PEDIATRIC HUMAN IMMUNO DEFICIENCY VIRUS. IAP UG Teaching slides
|
|
|
- Shauna Washington
- 5 years ago
- Views:
Transcription
1 PEDIATRIC HUMAN IMMUNO DEFICIENCY VIRUS 1
2 DISEASE BURDEN There were 3.2 million children living with HIV around the world with 90% residing in sub Saharan Africa Globally, between 2002 and 2013, there was a 58% reduction in the number of new HIV infections among children. More than 240,000 children were infected with HIV during Only 24% of children who needed antiretroviral treatment (ART) received it. 190,000 children died of AIDS related illnesses. 2
3 INDIA India has the third largest HIV epidemic in the world. National adult (15 49 years) HIV prevalence is estimated at 0.26% (0.22% 0.32%) in In 2015, adult HIV prevalence is estimated at0.30% among males and at 0.22% among females. The total number of people living with HIV (PLHIV)is estimated at lakhs in 2015 compared with lakhs in Children account for 6.54%, while two fifth (40.5%) of total HIV infections are among females. 3
4 INDIA India is estimated to have around 86 (56 129) thousand new HIV infections in 2015 showing 66% decline in new infections from 2000 and 32% decline from 2007 Children accounted for 12% of total new infections. Since 2007, when the number of AIDS related deaths (ARD) started to show a declining trend, the annual number of AIDS related deaths has declined by 54%. 4

5 DISTRIBUTION OF PEOPLE LIVING WITH HIV IN INDIA 5
6 ETIOLOGY Caused by HIV 1 and HIV 2 belong to Retroviridae. Single stranded RNA HIV 1 genome GAG viral core proteins like p24 POL viral enzymes like reverse transcriptase ENV envelope proteins gp120 and gp41 6
7 MODES OF TRANSMISSION IN CHILDREN Vertical can occur during intrauterine, intrapartum (most common)or through breast feeding. Rate of transmission from mother to child varies from 12% to 30% with figures as high as 50% reported from Africa. Blood Products 3 6% 7
8 MODES OF TRANSMISSION IN CHILDREN Other routes Sexual abuse Unsafe needles Sharps IVDU MSM Unknown 8
9 PATHOGENESIS 9
10 CLINICAL PATTERNS Three clinical patterns of HIV disease have been described in children (prior to HAART). Rapid progressors (15 25%) Symptomatic within first year. Short term progressors (60 80%) Symptomatic within 6 7 years. Long term progressors (<5%) Symptomatic within 8 10 years
11 CLINICAL FEATURES Clinical manifestations of HIV infection vary widely among infants, children and adolescents. 11
12 CLINICAL FEATURES CONT. Important manifestations occurring in infancy and childhood include : lymphadenopathy, hepatosplenomegaly, failure to thrive, chronic or recurrent diarrhea, recurrent pneumonia, oral thrush, 12
13 CLINICAL FEATURES CONT. Recurrent otitis media, Tuberculosis (TB), PCP, Pyrexia of unknown origin,etc. Recurrent bacterial infections, Chronic parotid swelling, Lymphoid interstitial pneumonitis (LIP) and Early onset progressive neurologic deterioration are manifestations seen more commonly in children as compared to adults. 13

14 WHO CLINICAL STAGING OF HIV 14

15 15

16 16

17 17

18 IMMUNE CLASSIFICATION 18
19 HIV NON SPECIFIC MANIFESTATIONS PUO > 1 mo Weight loss > 10% in 6 mo Diarrhea > 1 mo (10 50%) Failure to thrive & Growth retardation ( ~ 90%) Hepato/Spleno megaly Generalized Lymphadenopathy 19


20 20
21 OPPORTUNISTIC INFECTIONS Bacterial: Mycobacterial M. TB, MAI Rec. severe pyogenic infections Viral: OI CMV, Herpes, EBV Measles, Varicella, Molluscum Fungal: Candidiasis, C. Neoformans etc. Protozoal: PCP, Toxo., Cryptosporidium 30 50% of AIDS patients present with OI Recurrent infections rapid progression of disease 21
22 RECURRENT BACTERIAL INFECTIONS About 20% of AIDS defining illnesses. Recurrent, severe, systemic, non responsive Mainly capsular organisms Poor antibody response in spite of IgG levels Internal organ infections/abscess Sepsis Septic Arthritis Pneumonitis Pyo. Meningitis Organ abscesses SSTIs 2 episodes of invasive infections in 2 years 22
23 Candidiasis: Candidiasis is the most common fungal infection in HIV infected children. Oral nystatin suspension or clotrimazole can be used for treatment. Tuberculosis (TB) All forms of tuberculosis are seen in HIV infected children including pulmonary, lymph node and extrapulmonary tuberculosis 23
24 PNEUMOCYSTIS CARINII (JIROVECI) PNEUMONIA (PCP): This is the most common OI in infants. The highest occurrence is at age of 3 6 months. The infant presents with acute onset fever, dyspnoea, tachypnea, cough, cyanosis and marked hypoxia. 24
25 PNEUMOCYSTIS CARINII (JIROVECI) PNEUMONIA (PCP): Investigations: X ray Chest, PFT, Gallium Scan, The radiographic findings include interstitial infiltrates or diffuse alveolar disease (which progresses rapidly). GM stain sensitivity: Sputum (30%) BAL (60 90%) Biopsy (97%) Treatment is with intravenous cotrimoxazole


26 PCP PNEUMONIA PCP GM STAIN 26



27 SOME OTHER OI S 27

28 RESPIRATORY TRACT Lymphoid Interstitial Pneumonia (LIP): Prevalence 40 50%, less common in adults Commonly seen in vertically infected children Older child, insidious onset of dry cough, progressive dyspnea, clubbing? HIV RNA? EBV induced Investigations: X ray Chest, Lung biopsy Prognosis: Median survival mo after diagnosis 28
29 CENTRAL NERVOUS SYSTEM (CNS) HIV is a neurotropic virus and can cause primary CNS involvement. Neurological manifestations can be caused by the HIV itself, OIs, tumors or drugs. Presentation may be development delay in an infant, poor scholastic performance HIV encephalopathy needs early initiation of treatment with highly active anti retroviral therapy (HAART). 29
30 GASTROINTESTINAL AND HEPATIC MANIFESTATIONS: Candidiasis, periodontal disease, salivary gland disease, oral hairy leukoplakia and oral ulcerations can occur. Chronic or recurrent diarrhea with malabsorption, abdominal pain, dysphagia, and failure to thrive are common symptoms of gastrointestinal disease. HIV or AIDS enteropathy is the syndrome of malabsorption with partial villous atrophy caused by HIV infection to gut. Hepatomegaly is common. Fluctuating serum levels of transaminases with or without cholestasis is common
31 CARDIOVASCULAR SYSTEM The reasons for cardiac involvement can be HIV itself, intercurrent infections, immune mediated reactions and adverse effects of drug therapy (zidovudine). Usually the cardiac involvement is clinically silent. Dilated cardiomyopathy, left ventricular hypertrophy, pulmonary hypertension and congestive cardiac failure can occur
32 RENAL DISEASE Nephropathy is an unusual presenting symptom of HIV infection. Focal glomerulosclerosis (80%) progressing to renal failure in 6 9 months, mesangial hyperplasia (10 15%), segmental necrotizing glomerulonephritis and minimal change disease may be seen. Nephrotic syndrome is the most common manifestation of paediatric renal HIV disease

33 DERMATOLOGICAL DISORDERS Cutaneous manifestations are inflammatory or infectious disorders which are not necessarily unique Seborrheic dermatitis, severe eczema, recurrent or chronic episodes of HSV, herpes zoster, molluscum contagiosum, anogenital warts, candidial infections, tinea, onychomycosis, impetigo and scabies are common. 33
34 HEMATOLOGIC DISORDERS Anaemia is frequent (20 70%) and caused due to various reasons. Leukopenia occurs in almost one third of untreated cases (and neutropenia often occurs). Thrombocytopenia may occur in up to 20% of patients. Patients are predisposed for thrombosis due to: hyperviscosity (due to hypergammaglobulinemia) protein C and protein S deficiency 34
35 MALIGNANCIES & OTHER ORGAN INVOLVEMENT Malignancies: As compared to adults, malignant diseases are uncommon in children. Non Hodgkin lymphoma and primary CNS lymphoma are known to occur. Epstein Barr virus is associated with most lymphomas. Kaposi sarcoma (caused by human herpesvirus 8) is very rare in HIV infected children. Other organ involvement: HIV arthropathy, myopathy, rheumatologic, endocrine and metabolic disorders may also be seen
36 HIV DIAGNOSIS UNDER 18 MONTHS Non-breast feeding infant Virological testing at 6 weeks Breast-feeding infant Virological testing at 6 weeks +ve test -ve test +ve test -ve test Retest 6-8 wks after stopping Breast-feeding Repeat +ve test Not HIV Infected Repeat +ve test +ve test -ve test HIV Infected HIV Infected 36 Repeat virological test if infant becomes symptomatic Not HIV Infected
37 HIV DIAGNOSIS OVER 18 MONTHS Non-breast feeding child Breast-feeding child HIV antibody test HIV antibody test Confirmed +ve test -ve test Confirmed +ve test -ve test Retest 6-8 wks after stopping breast-feeding HIV Infected Not HIV Infected HIV Infected Confirmed +ve test -ve test Refer for Rx, care & support Refer for Rx, care & support 37 Not HIV Infected
38 MANAGEMENT OF HIV High index of suspicion & timely diagnosis Growth monitoring & Nutritional advise Breast feeding vs. Replacement feeding Psycho social support Immunization Management of OI s & prophylaxis Anti retro viral therapy Prevention including PMTCT 38
39 HIV TREATMENT IMMUNISATION Asymptomatic HIV Give all vaccines Symptom. HIV? Live vaccines avoided BCG must in our country OPV safe IPV if available All killed/subunit vaccines Safe Monitor seroresponse Additional doses Passive prophylaxis VZIZ/Measles Ig 39
40 ARVT AIMS Immune preservation Slower disease progression Lesser infections Better physical growth Better neurodevelopment Prolong the life Improved quality of life? Cure in future 40 40
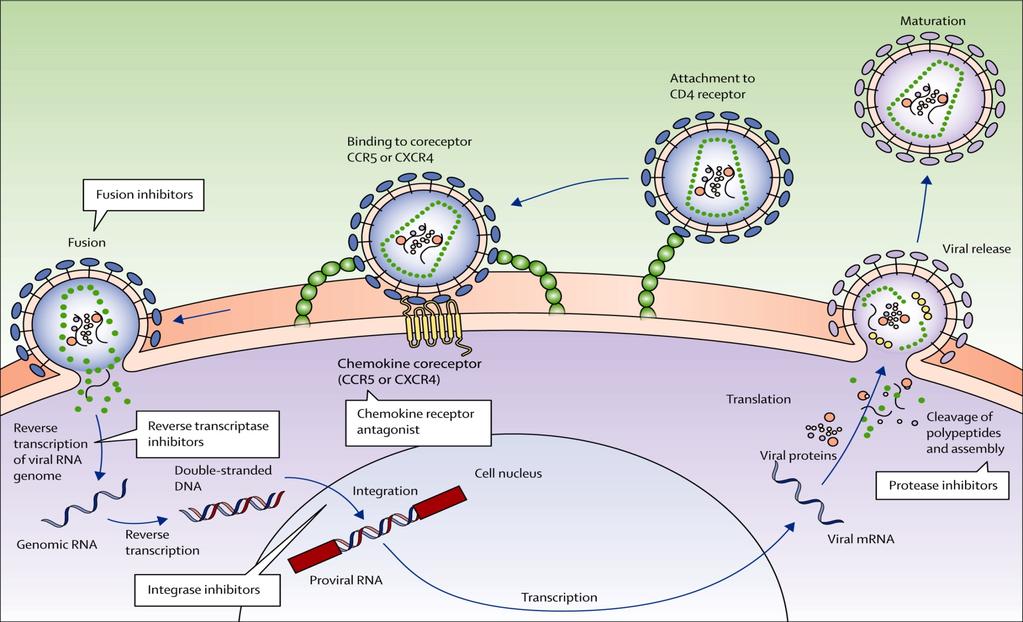
41 TYPES OF ANTIRETROVIRAL AGENTS 1. Nucleoside reverse transcriptase inhibitor Zidovudine Didanosine Stavudine Zalcitabine Lamivudine Abacavir 2. Non nucleoside reverse transcriptase inhibitor Nevirapine Delaviridine Efavirenz 3. Protease inhibitor Saquinavir Indinavir Ritonavir Nelfinavir Amprenavir Lopinavir 4. Newer drugs Fusion inhibitor 41
42 MECHANISM OF ACTION Nucleoside reverse transcriptase inhibitor Blocks the reverse transcriptase enzyme Non nucleoside reverse transcriptase inhibitor Blocks RT activity by binding adjacent to the enzymes active site Protease inhibitor Blocks HIV protease resulting in formation of immature, non infectious virion 42
43 NEWER ANTIRETROVIRALS Fusion Inhibitor T 20 Inhibits the fusion of HIV virion to the lymphocyte membrane Not available orally To be given either SC or IV twice daily 43
44 RECOMMENDATIONS FOR INITIATING ART IN INFANTS AND CHILDREN WHO Paediatric Stage Availability of CD4 cell measurements Age specific treatment recommendation <12 months 12 months 4 CD4 Treat all No CD4 3 CD4 Treat all Treat all, CD4 guided in those children with TB, LIP, OHL, thrombocytopenia No CD4 Treat all 2 CD4 CD4 guided No CD4 Do not treat 1 CD4 CD4 guided No CD4 Do not treat 44
45 RECOMMENDED FIRST LINE THERAPY Regimen of 2 NRTI plus 1 NNRTI AZT + 3TC + NVP/ EFV d4t + 3TC + NVP/ EFV ABC* + 3TC + NVP/ EFV EFV HIV and TB Not recommended < 3 yrs Adolescent girls ABC presently not available through the national program Never use AZT and d4t together AZT 1 st choice in non anemic children (Hb > 9 gm%) d4t 1 st choice in those who are anemic 45
46 ARVT MONITORING Clinical follow up CD 4 count & Viral load Baseline, at 6 wk.,18 24 wk., and then every 3 6 mo., SOS as required In vitro drug sensitivity Abn. results to be confirmed after 1 wk Don t test within 1 wk. of any infection 46
47 USING THE WHO CLINICAL STAGING SYSTEM FOR TREATMENT FAILURE WHO Clinical Stage on ART T 1 T 2 T 3 T 4 Management options Do not switch to other regimen Maintain scheduled follow up visits Treat and manage staging event Do not switch to other regimen Assess and offer adherence support Assess nutritional status and offer support Schedule earlier visit for clinical review Treat and manage staging event and monitor response Check if on treatment 24 weeks or more Assess and offer adherence support Assess nutritional status and offer support Check CD4 where available Consider switching regimen Institute more frequent follow up Assess and offer adherence support Assess nutritional status and offer support Document CD4 where available Switch regimen 47
48 WHO Paediatric Clinical Stage on ART T1 and T2 DECISION MAKING REGARDING SWITCHING TO SECOND LINE THERAPY Availability of CD4 measurements No CD4 CD4 Do not switch regimen Management options Consider switching regimen only if 2 or more values below age related threshold for severe immunodeficiency are available/ declining values? Increase clinical and CD4 follow up if CD4 approaches age related threshold for severe immunodeficiency T3 No CD4 Consider switching regimen CD4 Switching regimen is recommended if CD4 at or below age related threshold for severe immunodeficiency and particularly if child initially had good immune response to ART T4 No CD4 Switch regimen, regardless of CD4 CD4 48
49 ARVT DRUG INTERACTIONS NRTI : Antifungals, Aminoglycosides, Antacids (except ddi) AZT : TMP/SMX, Acyclovir ddc : IV Pentamidine ddi : Tetracyclines, Quinolones NNRTI & PI : Analgesics, Antihistaminic, Cizapride, Sedatives, Hypnotics, Rifampicin, Anticonvulsants 49
50 ARVT LONG TERM SIDE EFFECTS Altered Blood Sugar Diabetes Mellitus Raised S. Lipid levels Abnormal Body fat distribution Nephrocalcinosis Spontaneous bleeding in Hemophiliacs Hepatic damage Bone and joint effects 50
51 HIV PREVENTION No sex is the safest sex! Safe blood & blood products Disinfection Bleach, heat Universal precautions Gloves, protective measures, Hand washing Disposal of disposables Avoid mouth to mouth methods Post Exposure Prophylaxis HIV vaccine Prevention of PTCT 51
52 Five Phases of PMTCT Life skills STIs FP ANC VCT ARV Safe Delivery R.F E.BF PEP Social Support Phase alpha: Prevent Phase1: Inform Phase2: Prophylaxis Phase3: Infant Feeding Phase omega: Support 52
53 INFANT FEEDING ARV prophylaxis administered to the mother and infant reduces PTCT 5 to 20% of infants breastfed by HIV infected mothers are at risk of acquiring HIV Exclusive Replacement feeding / Exclusive BF along with ARV can reduce transmission significantly However top feeding especially bottle not safe in developing countries (diarrhea and LRTI) 53
54 INFANT FEEDING : HIV INFECTED MOTHERS WHO Recommendations Avoid all breastfeeding if replacement feeding is Acceptable Feasible Affordable Sustainable & Safe Otherwise, exclusive breastfeeding during the first months of life 54
55 INFANT FEEDING CONCLUSION INFORMED CHOICE BY MOTHER Decision depends on U5MR MMR HIV Prevalence, Demand by the mother Exclusive BF or RF Exclusive BF & early weaning RF Cow s milk with spoon 55
56 PPTCT PROTOCOLS India specific protocols: Initially AZT as per Thai protocol + BF choice Now sdnvp mother & Baby + BF choice Modifications required/suggested Mother on ART/In need of ART: Triple drug ART as per National Guidelines: < 2 % trans. Mother not in need of ART: Antenatal: AZT from 28 wk Intranatal: AZT + 3TC + sdnvp Postnatal: Mother: AZT + 3TC x 1 wk Baby: sdnvp + AZT x 1 wk Efficacy: < 2 % transmission risk 56
57 IF MOTHER COMES LATE If antenatal AZT taken for < 4 wk: AZT to baby for 4 wk instead of 1 wk If mother comes during labor: Intranatal and postnatal as before except AZT to baby for 4 wk instead of 1 wk If mother comes postpartum: Baby given the postnatal component except AZT for 4 wk instead of 1 wk Role of drugs for the duration of BF 57
58 UN FUTURE GOALS Target for decrease in MTCT 25% by % by 2010 We can do it We must do it We shall do it 58
59 POST EXP. PROPHYLAXIS (CDC 1998) Material infective - Yes Type of exposure M.M. /Broken skin Intact skin Percutaneous Small Volume Large Low risk No PEP High risk Offer Less severe Severity More severe Titer of HIV Low Offer Hig Basih c PEP Basic PEP, Expanded PEP if HIV titer high 59 Expanded PEP

60 THANK YOU 60
DR. SATTI A/RAHIM SATTI CONSULTANT PEDIATRICION
 A I D S IN CHILDREN BY DR. SATTI A/RAHIM SATTI CONSULTANT PEDIATRICION INTRODUCTION AIDS is the end stage of symptomatic HIV infection. HIV infection progresses more rapidly in children than in adults.
A I D S IN CHILDREN BY DR. SATTI A/RAHIM SATTI CONSULTANT PEDIATRICION INTRODUCTION AIDS is the end stage of symptomatic HIV infection. HIV infection progresses more rapidly in children than in adults.
PAEDIATRIC HIV INFECTION. Dr Ashendri Pillay Paediatric Infectious Diseases Specialist
 PAEDIATRIC HIV INFECTION Dr Ashendri Pillay Paediatric Infectious Diseases Specialist Paediatric HIV Infection Epidemiology Immuno-pathogenesis Antiretroviral therapy Transmission Diagnostics Clinical
PAEDIATRIC HIV INFECTION Dr Ashendri Pillay Paediatric Infectious Diseases Specialist Paediatric HIV Infection Epidemiology Immuno-pathogenesis Antiretroviral therapy Transmission Diagnostics Clinical
Clinical Manifestations of HIV
 HIV Symptoms Diane Havlir, MD Professor of Medicine and Chief, HIV/AIDS Division University of California, San Francisco (UCSF) WorldMedSchool; July 2, 2013 1 Clinical Manifestations of HIV! Result from
HIV Symptoms Diane Havlir, MD Professor of Medicine and Chief, HIV/AIDS Division University of California, San Francisco (UCSF) WorldMedSchool; July 2, 2013 1 Clinical Manifestations of HIV! Result from
medical monitoring: clinical monitoring and laboratory tests
 medical monitoring: clinical monitoring and laboratory tests Purpose of monitoring Check on the physical, psychological and emotional condition of the patient Detect other treatable conditions Identify
medical monitoring: clinical monitoring and laboratory tests Purpose of monitoring Check on the physical, psychological and emotional condition of the patient Detect other treatable conditions Identify
2. Clinical Manifestations (Pediatric HIV Infection)
") Page 1 of 6 HOUSTON ROMANIA SOUTHERN AFRICA MEXICO HOME CONTACT Friday, July 25, 2003 Pediatric HIV Infection by Mark W. Kline, M.D. 1. Introduction 2. Clinical Manifestations 3. Diagnosis 2. Clinical
Page 1 of 6 HOUSTON ROMANIA SOUTHERN AFRICA MEXICO HOME CONTACT Friday, July 25, 2003 Pediatric HIV Infection by Mark W. Kline, M.D. 1. Introduction 2. Clinical Manifestations 3. Diagnosis 2. Clinical
Human Immunodeficiency Virus. Acquired Immune Deficiency Syndrome AIDS
 Human Immunodeficiency Virus Acquired Immune Deficiency Syndrome AIDS Sudden outbreak in USA of opportunistic infections and cancers in young men in 1981 Pneumocystis carinii pneumonia (PCP), Kaposi s
Human Immunodeficiency Virus Acquired Immune Deficiency Syndrome AIDS Sudden outbreak in USA of opportunistic infections and cancers in young men in 1981 Pneumocystis carinii pneumonia (PCP), Kaposi s
HIV. Transmission modes. Transmission modes in children. Prevention of mother-to-child transmission of HIV. HIV identified in 1983
 Prevention of mother-to-child transmission of HIV HIV identified in 1983 HIV AIDS syndrome described in 1981 Kaposi s sarcoma, Pneumocystis jiroveci pnemumonia and wasting often combined Retrospectively,
Prevention of mother-to-child transmission of HIV HIV identified in 1983 HIV AIDS syndrome described in 1981 Kaposi s sarcoma, Pneumocystis jiroveci pnemumonia and wasting often combined Retrospectively,
INITIATING ART IN CHILDREN: Follow the six steps
 INITIATING ART IN CHILDREN: Follow the six steps STEP 1: DECIDE IF THE CHILD HAS CONFIRMED HIV INFECTION Child < 18 months: HIV infection is confirmed if the PCR is positive and the VL is more than 10,000
INITIATING ART IN CHILDREN: Follow the six steps STEP 1: DECIDE IF THE CHILD HAS CONFIRMED HIV INFECTION Child < 18 months: HIV infection is confirmed if the PCR is positive and the VL is more than 10,000
0% 0% 0% Parasite. 2. RNA-virus. RNA-virus
 HIV/AIDS and Treatment Manado, Indonesia 16 november HIV [e] EDUCATION HIV is a 1. DNA-virus 2. RNA-virus 3. Parasite 0% 0% 0% DNA-virus RNA-virus Parasite HIV HIV is a RNA-virus. HIV is an RNA virus which
HIV/AIDS and Treatment Manado, Indonesia 16 november HIV [e] EDUCATION HIV is a 1. DNA-virus 2. RNA-virus 3. Parasite 0% 0% 0% DNA-virus RNA-virus Parasite HIV HIV is a RNA-virus. HIV is an RNA virus which
Outline. Aim with PMTCT. How are children transmitted. Prevention of mother-to-child transmission of HIV. How does HIV transmit to children?
 Prevention of mother-to-child transmission of HIV Outline AimofPMTCT How HIV is transmitted to children Epidemiology of HIV in children How to reduce HIV transmission to children Guidelines Lars T. Fadnes
Prevention of mother-to-child transmission of HIV Outline AimofPMTCT How HIV is transmitted to children Epidemiology of HIV in children How to reduce HIV transmission to children Guidelines Lars T. Fadnes
THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2010
 THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2010 The South African Antiretroviral Treatment Guidelines 2010 Goals of the programme Achieve best health outcomes in the most cost-efficient manner
THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2010 The South African Antiretroviral Treatment Guidelines 2010 Goals of the programme Achieve best health outcomes in the most cost-efficient manner
TOWARDS ELIMINATION OF MOTHER TO CHILD TRANSMISSION OF HIV
 TOWARDS ELIMINATION OF MOTHER TO CHILD TRANSMISSION OF HIV Gladwel Muthoni KPA Conference 24 th April, 2018 OUTLINE Burden of HIV in PMTCT Mechanism and timing of Mother to Child Transmission (MTCT) Four
TOWARDS ELIMINATION OF MOTHER TO CHILD TRANSMISSION OF HIV Gladwel Muthoni KPA Conference 24 th April, 2018 OUTLINE Burden of HIV in PMTCT Mechanism and timing of Mother to Child Transmission (MTCT) Four
PHCP 403 by L. K. Sarki
 PHCP 403 by L. K. Sarki objectives To gain insight into the epidemiology of HIV To gain basic understanding of the etiology of HIV disease To know the clinical manifestations of the disease To gain a basic
PHCP 403 by L. K. Sarki objectives To gain insight into the epidemiology of HIV To gain basic understanding of the etiology of HIV disease To know the clinical manifestations of the disease To gain a basic
World Bank Training Program on HIV/AIDS Drugs
 World Bank Training Program on HIV/AIDS Drugs Training Module 3 Selection and Quantification based on the World Bank document Battling HIV/AIDS: A Decision Maker s Guide to the Procurement of Medicines
World Bank Training Program on HIV/AIDS Drugs Training Module 3 Selection and Quantification based on the World Bank document Battling HIV/AIDS: A Decision Maker s Guide to the Procurement of Medicines
Year 2002 Paper two: Questions supplied by Jo 1
 Year 2002 Paper two: Questions supplied by Jo 1 Question 9 A 37 year old man with known human immunodeficiency virus (HIV) infection for 10 years presents with severe renal colic for which he has no prior
Year 2002 Paper two: Questions supplied by Jo 1 Question 9 A 37 year old man with known human immunodeficiency virus (HIV) infection for 10 years presents with severe renal colic for which he has no prior
HIV Treatment Update. Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University
 HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
PAEDIATRIC ANTIRETROVIRAL THERAPY FOR THE GENERAL PRACTITIONER
 PAEDIATRIC ANTIRETROVIRAL THERAPY FOR THE GENERAL PRACTITIONER The care of HIV-infected children is somewhat different to that of adults, and although this poses some challenges, it should not impede paediatric
PAEDIATRIC ANTIRETROVIRAL THERAPY FOR THE GENERAL PRACTITIONER The care of HIV-infected children is somewhat different to that of adults, and although this poses some challenges, it should not impede paediatric
GUIDELINES FOR THE USE OF ANTIRETROVIRAL THERAPY IN PAPUA NEW GUINEA
 GUIDELINES FOR THE USE OF ANTIRETROVIRAL THERAPY IN PAPUA NEW GUINEA These guidelines were prepared for the Papua New Guinea National AIDS Council and the Papua New Guinea National Department of Health.
GUIDELINES FOR THE USE OF ANTIRETROVIRAL THERAPY IN PAPUA NEW GUINEA These guidelines were prepared for the Papua New Guinea National AIDS Council and the Papua New Guinea National Department of Health.
HIV infection. Objectives. HIV is the Human Immunodeficiency Virus.
 9 HIV infection Objectives When you have completed this unit you should be able to: Define HIV infection and AIDS. Describe how children may become infected with HIV. Reduce the risk of mother-to-child
9 HIV infection Objectives When you have completed this unit you should be able to: Define HIV infection and AIDS. Describe how children may become infected with HIV. Reduce the risk of mother-to-child
 http://www.savinglivesuk.com/ HIV Awareness Study Morning 24 th November 2017 Agenda HIV Basics & Stages of HIV HIV Testing, Health Advising & Sexual Health Saving Lives Antiretroviral Medication Antenatal/Postnatal
http://www.savinglivesuk.com/ HIV Awareness Study Morning 24 th November 2017 Agenda HIV Basics & Stages of HIV HIV Testing, Health Advising & Sexual Health Saving Lives Antiretroviral Medication Antenatal/Postnatal
Principles of Antiretroviral Therapy
 Principles of Antiretroviral Therapy Ten Principles of Antiretroviral Therapy Skills Building Workshop: Clinical Management of HIV Infection and Antiretroviral Therapy, 11 th ICAAP, November 21st, 2011,
Principles of Antiretroviral Therapy Ten Principles of Antiretroviral Therapy Skills Building Workshop: Clinical Management of HIV Infection and Antiretroviral Therapy, 11 th ICAAP, November 21st, 2011,
Prokaryotic Biology. VIRAL STDs, HIV-1 AND AIDS
 Prokaryotic Biology VIRAL STDs, HIV-1 AND AIDS Prokaryotic Biology FROM THE CDC VIRAL STDs, HIV-1 AND AIDS VIRAL STDs & CONTACT VIRAL DISEASES A. GENITAL HERPES & COLD SORES 1. HERPES SIMPLEX VIRUS-2 (HHV-2)
Prokaryotic Biology VIRAL STDs, HIV-1 AND AIDS Prokaryotic Biology FROM THE CDC VIRAL STDs, HIV-1 AND AIDS VIRAL STDs & CONTACT VIRAL DISEASES A. GENITAL HERPES & COLD SORES 1. HERPES SIMPLEX VIRUS-2 (HHV-2)
Paediatric HIV. February
 Paediatric HIV February 2017 http://www.medcol.mw/e-learning-com-resources/paediatricinfectious-diseases/ Epidemiology Natural History Clinical presentation Diagnosis Staging Eligibility HAART Monitoring
Paediatric HIV February 2017 http://www.medcol.mw/e-learning-com-resources/paediatricinfectious-diseases/ Epidemiology Natural History Clinical presentation Diagnosis Staging Eligibility HAART Monitoring
OF HIV / AIDS EXPOSURE ACUTE HIV INFECTION (1-2W.) AIDS SEXUAL, BLOOD, VERTICAL Days to weeks(2-4w.) 5-8% *20-25%, 6y. *50%, 10y. *<5%, 2y.
 AIDS SEXUAL, BLOOD, VERTICAL Days to weeks(2-4w.) 5-8% *20-25%, 6y. *50%, 10y. *<5%, 2y.") Clinical Manifestations & Management of HIV Dr.Shervin Shokouhi Infectious Disease Specialist & Associate Professor of Shaheed Beheshti University of Medical Sciences 1 CLINICAL MANIFESTATIONS OF HIV /
Clinical Manifestations & Management of HIV Dr.Shervin Shokouhi Infectious Disease Specialist & Associate Professor of Shaheed Beheshti University of Medical Sciences 1 CLINICAL MANIFESTATIONS OF HIV /
WESTERN CAPE ART GUIDELINES PRESENTATION 2013
 WESTERN CAPE ART GUIDELINES PRESENTATION 2013 The WC guidelines are based on SA National ART guidelines dated 24th March 2013 Acknowledgement goes to members of the Adult and Paediatric HAST policy advisory
WESTERN CAPE ART GUIDELINES PRESENTATION 2013 The WC guidelines are based on SA National ART guidelines dated 24th March 2013 Acknowledgement goes to members of the Adult and Paediatric HAST policy advisory
TB & HIV CO-INFECTION IN CHILDREN. Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012
 TB & HIV CO-INFECTION IN CHILDREN Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012 Introduction TB & HIV are two of the leading causes of morbidity & mortality in children
TB & HIV CO-INFECTION IN CHILDREN Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012 Introduction TB & HIV are two of the leading causes of morbidity & mortality in children
Figure S1: Overview of PMTCT Options A and B. Prevention of Mother to Child HIV Transmission (PMTCT)
") Figure S1: Overview of PMTCT Options A and B Prevention of Mother to Child HIV Transmission (PMTCT) Option A: combined Antiretroviral therapy (ART) for all women meeting WHO 2010 criteria for initiation
Figure S1: Overview of PMTCT Options A and B Prevention of Mother to Child HIV Transmission (PMTCT) Option A: combined Antiretroviral therapy (ART) for all women meeting WHO 2010 criteria for initiation
Cryptococcosis of the Central Nervous System: Classical and Immune-Reconstitution Disease
 Cryptococcosis of the Central Nervous System: Classical and Immune-Reconstitution Disease Assist Prof. Somnuek Sungkanuparph Division of Infectious Diseases Faculty of Medicine Ramathibodi Hospital Mahidol
Cryptococcosis of the Central Nervous System: Classical and Immune-Reconstitution Disease Assist Prof. Somnuek Sungkanuparph Division of Infectious Diseases Faculty of Medicine Ramathibodi Hospital Mahidol
CUMULATIVE PERINATAL HIV EXPOSURE, AUSTRALIA. Date
 CUMULATIVE PERINATAL HIV EXPOSURE, AUSTRALIA 350 300 250 Number 200 150 100 50 0 1/01/1997 1/01/1998 1/01/1999 1/01/2000 31/12/2000 31/12/2001 31/12/2002 Date July 2004 Reported number of perinatally exposed
CUMULATIVE PERINATAL HIV EXPOSURE, AUSTRALIA 350 300 250 Number 200 150 100 50 0 1/01/1997 1/01/1998 1/01/1999 1/01/2000 31/12/2000 31/12/2001 31/12/2002 Date July 2004 Reported number of perinatally exposed
Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV. Ernesto Parra, M.D., M.P.H.
 Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV Ernesto Parra, M.D., M.P.H. Adjunct Associate Professor UTHSCSA Department of Pediatrics and Family and Community
Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV Ernesto Parra, M.D., M.P.H. Adjunct Associate Professor UTHSCSA Department of Pediatrics and Family and Community
BASIC HIV COURSE EXAMINATION
 [Pick the date] HU CFAR BASIC HIV COURSE EXAMINATION [Type the author name] The mission of the Harvard University Center for AIDS Research (HU CFAR) is to expand, promote, and facilitate collaborative,
[Pick the date] HU CFAR BASIC HIV COURSE EXAMINATION [Type the author name] The mission of the Harvard University Center for AIDS Research (HU CFAR) is to expand, promote, and facilitate collaborative,
INTEGRATING HIV INTO PRIMARY CARE
 INTEGRATING HIV INTO PRIMARY CARE ADELERO ADEBAJO, MD, MPH, AAHIVS, FACP NO DISCLOSURE 1.2 million people in the United States are living with HIV infection and 1 in 5 are unaware of their infection.
INTEGRATING HIV INTO PRIMARY CARE ADELERO ADEBAJO, MD, MPH, AAHIVS, FACP NO DISCLOSURE 1.2 million people in the United States are living with HIV infection and 1 in 5 are unaware of their infection.
Objectives. Outline. Section 1: Interaction between HIV and pregnancy. Effects of HIV on Pregnancy. Section 2: Mother-to-Child-Transmission (MTCT)
") Objectives Prevention of Mother-to-Child Transmission (PMTCT) Teen Club Community Partners Training Programme By the end of the session participants will be able to: 1. Identify factors affecting the transmission
Objectives Prevention of Mother-to-Child Transmission (PMTCT) Teen Club Community Partners Training Programme By the end of the session participants will be able to: 1. Identify factors affecting the transmission
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Sasisopin Kiertiburanakul, MD, MHS
 What s Newin Antiretroviral Therapy? Sasisopin Kiertiburanakul, MD, MHS Division of Infectious Diseases Department of Medicine Faculty of Medicine Ramathibodi Hospital Mahidol University Rotating RCPT,
What s Newin Antiretroviral Therapy? Sasisopin Kiertiburanakul, MD, MHS Division of Infectious Diseases Department of Medicine Faculty of Medicine Ramathibodi Hospital Mahidol University Rotating RCPT,
Immunodeficiency. (2 of 2)
") Immunodeficiency (2 of 2) Acquired (secondary) immunodeficiencies More common Many causes such as therapy, cancer, sarcoidosis, malnutrition, infection & renal disease The most common of which is therapy-related
Immunodeficiency (2 of 2) Acquired (secondary) immunodeficiencies More common Many causes such as therapy, cancer, sarcoidosis, malnutrition, infection & renal disease The most common of which is therapy-related
Immunodeficiencies HIV/AIDS
 Immunodeficiencies HIV/AIDS Immunodeficiencies Due to impaired function of one or more components of the immune or inflammatory responses. Problem may be with: B cells T cells phagocytes or complement
Immunodeficiencies HIV/AIDS Immunodeficiencies Due to impaired function of one or more components of the immune or inflammatory responses. Problem may be with: B cells T cells phagocytes or complement
HUMAN IMMUNODEFICIENCY VIRUS (HIV) AND AIDS
 AND AIDS") HUMAN IMMUNODEFICIENCY VIRUS (HIV) AND AIDS Mohamed Mahdi MD. MPH. Department of Infectology and Pediatric Immunology University of Debrecen (MHSC) 2015 Historical facts about HIV First presentation in
HUMAN IMMUNODEFICIENCY VIRUS (HIV) AND AIDS Mohamed Mahdi MD. MPH. Department of Infectology and Pediatric Immunology University of Debrecen (MHSC) 2015 Historical facts about HIV First presentation in
UPDATE TRAINING ARV TREATMENT GUIDELINES TRAINERS CASE STUDIES & ANSWER GUIDE
 UPDATE TRAINING ARV TREATMENT GUIDELINES TRAINERS CASE STUDIES & ANSWER GUIDE 3/13/2013 Contents Group Work Instructions... 2 PMTCT... 3 Case Study 1: Unbooked Pregnant Women... 3 Case Study 2: First ANC
UPDATE TRAINING ARV TREATMENT GUIDELINES TRAINERS CASE STUDIES & ANSWER GUIDE 3/13/2013 Contents Group Work Instructions... 2 PMTCT... 3 Case Study 1: Unbooked Pregnant Women... 3 Case Study 2: First ANC
Continuing Education for Pharmacy Technicians
 Continuing Education for Pharmacy Technicians HIV/AIDS TREATMENT Michael Denaburg, Pharm.D. Birmingham, AL Objectives: 1. Identify drugs and drug classes currently used in the management of HIV infected
Continuing Education for Pharmacy Technicians HIV/AIDS TREATMENT Michael Denaburg, Pharm.D. Birmingham, AL Objectives: 1. Identify drugs and drug classes currently used in the management of HIV infected
HIV IN PREGNANCY PANEL DISCUSSION
 HIV IN PREGNANCY PANEL DISCUSSION Introduction Transmission from HIV infected mother to baby is the key mode of HIV transmission in children Annually about 14,000 New HIV Infections occur among children
HIV IN PREGNANCY PANEL DISCUSSION Introduction Transmission from HIV infected mother to baby is the key mode of HIV transmission in children Annually about 14,000 New HIV Infections occur among children
TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011
 ART Treatment Guideline Training 31 st January to 4 th February, 2011") TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011 OUTLINE Background Global Incidence The Problem" The 3 I s Drug Resistant
TB/HIV CO-INFECTION ADULT & CHILDREN (INCLUDING INH PROPHYLAXIS) ART Treatment Guideline Training 31 st January to 4 th February, 2011 OUTLINE Background Global Incidence The Problem" The 3 I s Drug Resistant
MedChem 401~ Retroviridae. Retroviridae
 MedChem 401~ Retroviridae Retroviruses plus-sense RNA genome (!8-10 kb) protein capsid lipid envelop envelope glycoproteins reverse transcriptase enzyme integrase enzyme protease enzyme Retroviridae The
MedChem 401~ Retroviridae Retroviruses plus-sense RNA genome (!8-10 kb) protein capsid lipid envelop envelope glycoproteins reverse transcriptase enzyme integrase enzyme protease enzyme Retroviridae The
20 Years of Tears and Triumphs
 20 Years of Tears and Triumphs A Clinical Research Nurse s Perspective on HIV/AIDS Bobi Keenan, RN, ACRN Clinical Research Nurse UC Irvine Dept. of Medicine/Infectious Diseases Objectives 1. Understand
20 Years of Tears and Triumphs A Clinical Research Nurse s Perspective on HIV/AIDS Bobi Keenan, RN, ACRN Clinical Research Nurse UC Irvine Dept. of Medicine/Infectious Diseases Objectives 1. Understand
Update on global guidelines. and emerging issues on perinatal HIV prevention. WHO 2013 Consolidated ARV Guidelines
 WHO 2013 Consolidated ARV Guidelines Update on global guidelines H I V / A I D S DEPARTMENT and emerging issues on perinatal HIV prevention Children & HIV, St. Petersburg, Russia Sept 25-26, 2014 Dr. Nathan
WHO 2013 Consolidated ARV Guidelines Update on global guidelines H I V / A I D S DEPARTMENT and emerging issues on perinatal HIV prevention Children & HIV, St. Petersburg, Russia Sept 25-26, 2014 Dr. Nathan
43. Guidelines on Needle stick Injury
 43. Guidelines on Needle stick Injury The following information is abstracted from the South African Department of Health guidelines entitled: Management of Occupational Exposure to the Human Immunodeficiency
43. Guidelines on Needle stick Injury The following information is abstracted from the South African Department of Health guidelines entitled: Management of Occupational Exposure to the Human Immunodeficiency
0.14 ( 0.053%) UNAIDS 10% (94) ( ) (73-94/6 ) 8,920
 UNAIDS 10% (94) ( ) (73-94/6 ) 8,920") 0.14 UNAIDS 0.053% 2 250 60 10% 94 73 20 73-94/6 8,920 12 43 Public Health Service Task Force Recommendations 5-10% for Use of Antiretroviral Drugs in 10-20% Pregnant HIV-1-Infected Women for Maternal
0.14 UNAIDS 0.053% 2 250 60 10% 94 73 20 73-94/6 8,920 12 43 Public Health Service Task Force Recommendations 5-10% for Use of Antiretroviral Drugs in 10-20% Pregnant HIV-1-Infected Women for Maternal
be the presenting symptom of HIV-related illness. 4 CD4 cell count and CD4 cell percentage are key markers for determining disease progress and the ri
 Cutaneous Maniestations In HIV Positive Paediatric Patients Kondreddy B 1, Kuruvila M 2, Ullal KR 3, Bhat K 4 1 Resident, 2 Professor, 3 Senior Resident, Department of Dermatology, Venereology and Leprosy,
Cutaneous Maniestations In HIV Positive Paediatric Patients Kondreddy B 1, Kuruvila M 2, Ullal KR 3, Bhat K 4 1 Resident, 2 Professor, 3 Senior Resident, Department of Dermatology, Venereology and Leprosy,
CLAUDINE HENNESSEY & THEUNIS HURTER
 HIV/AIDS/TB CLAUDINE HENNESSEY & THEUNIS HURTER KEY TERMS Do these sound familiar? What strange terms do you hear in the clinics? Any others to add?? HIV AIDS Viral Load & suppression CD4 count Regimen
HIV/AIDS/TB CLAUDINE HENNESSEY & THEUNIS HURTER KEY TERMS Do these sound familiar? What strange terms do you hear in the clinics? Any others to add?? HIV AIDS Viral Load & suppression CD4 count Regimen
Clinical Education Initiative THE ROLE OF THE PRIMARY CARE CLINICIAN IN HIV CARE. Speaker: Antonia Urbina, MD
 Clinical Education Initiative Support@ceitraining.org THE ROLE OF THE PRIMARY CARE CLINICIAN IN HIV CARE Speaker: Antonia Urbina, MD 2/1/2017 The Role of the Primary Care Clinician in HIV Care [video transcript]
Clinical Education Initiative Support@ceitraining.org THE ROLE OF THE PRIMARY CARE CLINICIAN IN HIV CARE Speaker: Antonia Urbina, MD 2/1/2017 The Role of the Primary Care Clinician in HIV Care [video transcript]
Page 1. Outline. Outline. Building specialized knowledge: HIV. Biological interactions. Social aspects of the epidemic. Programmatic actions
 Harvard-Brazil Collaborative Public Health Field Course January 2014 Lecture # 8 Building specialized knowledge: HIV Aluisio Segurado Department of Infectious Diseases School of Medicine, University of
Harvard-Brazil Collaborative Public Health Field Course January 2014 Lecture # 8 Building specialized knowledge: HIV Aluisio Segurado Department of Infectious Diseases School of Medicine, University of
HIV Update Objectives. Epidemiology. Epidemiology, Transmission and Natural History. Transmission Risk by Exposure. Transmission 9/29/2014
 Objectives HIV Update 2014 Jay Sizemore, MD, MPH Medical Director Chattanooga CARES Assistant Professor UTCOM Chattanooga 2October 2014 Review HIV epidemiology and screening/testing guidelines Discuss
Objectives HIV Update 2014 Jay Sizemore, MD, MPH Medical Director Chattanooga CARES Assistant Professor UTCOM Chattanooga 2October 2014 Review HIV epidemiology and screening/testing guidelines Discuss
Understanding Viruses CHAPTER 38. Antiviral Agents. Understanding Viruses (cont'd) Viral Infections (cont'd) Viral Infections.
 Viral Infections (cont'd) Viral Infections.") Understanding Viruses CHAPTER 38 Antiviral Agents Viral replication A virus cannot replicate on its own It must attach to and enter a host cell It then uses the host cell s energy to synthesize protein,
Understanding Viruses CHAPTER 38 Antiviral Agents Viral replication A virus cannot replicate on its own It must attach to and enter a host cell It then uses the host cell s energy to synthesize protein,
Structured Treatment Interruption in HIV Positive Patients. Leah Jackson, BScPhm Pharmacy Resident HIV Rotation January 23, 2007
 Structured Treatment Interruption in HIV Positive Patients Leah Jackson, BScPhm Pharmacy Resident HIV Rotation January 23, 2007 Objectives To become re-acquainted with the basics of HAART for HIV infection
Structured Treatment Interruption in HIV Positive Patients Leah Jackson, BScPhm Pharmacy Resident HIV Rotation January 23, 2007 Objectives To become re-acquainted with the basics of HAART for HIV infection
Measure #161: HIV/AIDS: Adolescent and Adult Patients with HIV/AIDS Who Are Prescribed Potent Antiretroviral Therapy
 Measure #161: HIV/AIDS: Adolescent and Adult Patients with HIV/AIDS Who Are Prescribed Potent Antiretroviral Therapy 2012 PHYSICIAN QUALITY REPTING OPTIONS F INDIVIDUAL MEASURES: REGISTRY ONLY DESCRIPTION:
Measure #161: HIV/AIDS: Adolescent and Adult Patients with HIV/AIDS Who Are Prescribed Potent Antiretroviral Therapy 2012 PHYSICIAN QUALITY REPTING OPTIONS F INDIVIDUAL MEASURES: REGISTRY ONLY DESCRIPTION:
HIV Infection in Pregnancy. Francis J. Ndowa WHO RHR/STI
 HIV Infection in Pregnancy Francis J. Ndowa WHO RHR/STI FJN_STI_2005 Department of reproductive health and research Département santé et recherche génésiques Session outline Effect of pregnancy on HIV
HIV Infection in Pregnancy Francis J. Ndowa WHO RHR/STI FJN_STI_2005 Department of reproductive health and research Département santé et recherche génésiques Session outline Effect of pregnancy on HIV
Lahey Clinic Internal Medicine Residency Program: Curriculum for Infectious Disease
 Lahey Clinic Internal Medicine Residency Program: Curriculum for Infectious Disease Faculty representative: Eva Piessens, MD, MPH Resident representative: Karen Ganz, MD Revision date: February 1, 2006
Lahey Clinic Internal Medicine Residency Program: Curriculum for Infectious Disease Faculty representative: Eva Piessens, MD, MPH Resident representative: Karen Ganz, MD Revision date: February 1, 2006
Tunisian recommendations on ART : process and results
 Second Arab Congress of Clinical Microbiology and Infectious Diseases May 24-26, 2012. Tunisian recommendations on ART : process and results M. BEN MAMOU UNAIDS Email: BenmamouM@unaids.org M. CHAKROUN
Second Arab Congress of Clinical Microbiology and Infectious Diseases May 24-26, 2012. Tunisian recommendations on ART : process and results M. BEN MAMOU UNAIDS Email: BenmamouM@unaids.org M. CHAKROUN
10/17/2015. Chapter 55. Care of the Patient with HIV/AIDS. History of HIV. HIV Modes of Transmission
 Chapter 55 Care of the Patient with HIV/AIDS All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. History of HIV Remains somewhat obscure The earlier
Chapter 55 Care of the Patient with HIV/AIDS All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. History of HIV Remains somewhat obscure The earlier
HIV basics. Katya Calvo Medical Director of Antimicrobial Stewardship
 HIV basics Katya Calvo Medical Director of Antimicrobial Stewardship Learning Objectives 1. Review of HIV epidemiology worldwide and locally 2. Review of recommendations on whom to screen 3. Work up of
HIV basics Katya Calvo Medical Director of Antimicrobial Stewardship Learning Objectives 1. Review of HIV epidemiology worldwide and locally 2. Review of recommendations on whom to screen 3. Work up of
TB/HIV Co-Infection. Tuberculosis and HIV
 TB Intensive Tyler, Texas June 2-4, 2010 TB/HIV Co-Infection Lisa Y Armitige, MD, PhD June 3, 2010 Tuberculosis and HIV Co-Infection Lisa Y Armitige, MD, PhD Medical Consultant Heartland National TB Center
TB Intensive Tyler, Texas June 2-4, 2010 TB/HIV Co-Infection Lisa Y Armitige, MD, PhD June 3, 2010 Tuberculosis and HIV Co-Infection Lisa Y Armitige, MD, PhD Medical Consultant Heartland National TB Center
The New National Guidelines. Feeding in the Context of HIV. Dr. Godfrey Esiru; National PMTCT Coordinator
 The New National Guidelines (2010) for PMTCT and Infant Feeding in the Context of HIV Dr. Godfrey Esiru; National PMTCT Coordinator Presentation outline Evolution of the PMTCT guidelines in Uganda Rational
The New National Guidelines (2010) for PMTCT and Infant Feeding in the Context of HIV Dr. Godfrey Esiru; National PMTCT Coordinator Presentation outline Evolution of the PMTCT guidelines in Uganda Rational
TORONTO GENERAL HOSPITAL HIV AMBULATORY CARE ROTATION
 TGH - ambulatory rotation page 1 of 5 TORONTO GENERAL HOSPITAL HIV AMBULATORY CARE ROTATION SITE: Immunodeficiency Clinic, Toronto General Hospital, University Health Network Location: 13 th floor, Norman
TGH - ambulatory rotation page 1 of 5 TORONTO GENERAL HOSPITAL HIV AMBULATORY CARE ROTATION SITE: Immunodeficiency Clinic, Toronto General Hospital, University Health Network Location: 13 th floor, Norman
Care and Treatment of Children and Adolescents with HIV - The Barbados Experience.
 Care and Treatment of Children and Adolescents with HIV - The Barbados Experience. M. Anne St John Consultant, Department of Paediatrics Queen Elizabeth Hospital, Barbados Hon Professor, Child Health,
Care and Treatment of Children and Adolescents with HIV - The Barbados Experience. M. Anne St John Consultant, Department of Paediatrics Queen Elizabeth Hospital, Barbados Hon Professor, Child Health,
OI prophylaxis When to start, when to stop. Eva Raphael, MD MPH Family and community medicine, pgy-2 University of California, San Francisco
 OI prophylaxis When to start, when to stop Eva Raphael, MD MPH Family and community medicine, pgy-2 University of California, San Francisco Learning Objectives o Recognize when to start OI prophylaxis
OI prophylaxis When to start, when to stop Eva Raphael, MD MPH Family and community medicine, pgy-2 University of California, San Francisco Learning Objectives o Recognize when to start OI prophylaxis
Imunodeficiency states
 Imunodeficiency states Primary Caused by defined genetic defects Usually rare, but severe (exception: IgA deficiency) Secondary Consequence of some other disease, treatment, environmental factors Usually
Imunodeficiency states Primary Caused by defined genetic defects Usually rare, but severe (exception: IgA deficiency) Secondary Consequence of some other disease, treatment, environmental factors Usually
Antiviral Chemotherapy
 Viruses are intimate intracellular parasites and their destruction may cause destruction of infected cells. Many virus infections were considered to be self-limited. Most of the damage to cells in virus
Viruses are intimate intracellular parasites and their destruction may cause destruction of infected cells. Many virus infections were considered to be self-limited. Most of the damage to cells in virus
The Global HIV Epidemic. Jerome Larkin, MD
 The Global HIV Epidemic Jerome Larkin, MD Outline Global Epidemiology Natural History of HIV Antiretroviral Therapy Malaria Tuberculosis Prevention of Mother to Child Transmission Post-Exposure Prophylaxis
The Global HIV Epidemic Jerome Larkin, MD Outline Global Epidemiology Natural History of HIV Antiretroviral Therapy Malaria Tuberculosis Prevention of Mother to Child Transmission Post-Exposure Prophylaxis
Malaysian Consensus Guidelines on Antiretroviral Therapy Cheng Joo Thye Hospital Raja Permaisuri Bainun Ipoh
 Malaysian Consensus Guidelines on Antiretroviral Therapy 2017 Cheng Joo Thye Hospital Raja Permaisuri Bainun Ipoh Acknowledgement Table of contents Evolution of when to initiate therapy ART improves survival
Malaysian Consensus Guidelines on Antiretroviral Therapy 2017 Cheng Joo Thye Hospital Raja Permaisuri Bainun Ipoh Acknowledgement Table of contents Evolution of when to initiate therapy ART improves survival
Prevention of mother-to-child transmission of HIV. Lars Thore Fadnes Centre for International Health
 Prevention of mother-to-child transmission of HIV Lars Thore Fadnes Centre for International Health HIV HIV identified in 1983 AIDS syndrome described in 1981 Kaposi s sarcoma, Pneumocystis jiroveci pnemumonia
Prevention of mother-to-child transmission of HIV Lars Thore Fadnes Centre for International Health HIV HIV identified in 1983 AIDS syndrome described in 1981 Kaposi s sarcoma, Pneumocystis jiroveci pnemumonia
PROVIDING EXCELLENT PRIMARY CARE FOR PATIENTS LIVING WITH HIV
 PROVIDING EXCELLENT PRIMARY CARE FOR PATIENTS LIVING WITH HIV Madhuri Lad, DO, FACOI, AAHIVS Clinical Assistant Professor OSU Department of Internal Medicine OBJECTIVES Demographics Definitions Diagnosis
PROVIDING EXCELLENT PRIMARY CARE FOR PATIENTS LIVING WITH HIV Madhuri Lad, DO, FACOI, AAHIVS Clinical Assistant Professor OSU Department of Internal Medicine OBJECTIVES Demographics Definitions Diagnosis
POST-EXPOSURE PROPHYLAXIS, PRE-EXPOSURE PROPHYLAXIS, & TREATMENT OF HIV
 POST-EXPOSURE PROPHYLAXIS, PRE-EXPOSURE PROPHYLAXIS, & TREATMENT OF HIV DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none
POST-EXPOSURE PROPHYLAXIS, PRE-EXPOSURE PROPHYLAXIS, & TREATMENT OF HIV DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none
TB Intensive Tyler, Texas December 2-4, Tuberculosis and HIV Co-Infection. Lisa Y. Armitige, MD, PhD. December 4, 2008.
 TB Intensive Tyler, Texas December 2-4, 2008 Tuberculosis and HIV Co-Infection Lisa Y. Armitige, MD, Ph.D. December 4, 2008 Tuberculosis and HIV Co Infection Lisa Y. Armitige, MD, PhD Assistant Professor
TB Intensive Tyler, Texas December 2-4, 2008 Tuberculosis and HIV Co-Infection Lisa Y. Armitige, MD, Ph.D. December 4, 2008 Tuberculosis and HIV Co Infection Lisa Y. Armitige, MD, PhD Assistant Professor
Improving accessibility to antiretroviral drugs: A south-south collaboration
 Improving accessibility to antiretroviral drugs: A south-south collaboration Jaideep A Gogtay MD Cipla Ltd Mumbai jgogtay@cipla.com Adults and children estimated to be living with HIV at the end of 2000
Improving accessibility to antiretroviral drugs: A south-south collaboration Jaideep A Gogtay MD Cipla Ltd Mumbai jgogtay@cipla.com Adults and children estimated to be living with HIV at the end of 2000
Outline. A 41 Year-old Male COMMON PITFALLS IN HIV/AIDS MANAGEMENT: A CASE-BASED APPROACH. Q1: What anti-fungal regimen would you start?
 Outline COMMON PITFALLS IN HIV/AIDS MANAGEMENT: A CASE-BASED APPROACH Considerations for antiretroviral use in patients with coinfections Concerning and how to manage drug-drug interactions ARV-other drugs
Outline COMMON PITFALLS IN HIV/AIDS MANAGEMENT: A CASE-BASED APPROACH Considerations for antiretroviral use in patients with coinfections Concerning and how to manage drug-drug interactions ARV-other drugs
The Italian AIDS Epidemic Supports The Chemical AIDS Theory. Daniele Mandrioli
 The Italian AIDS Epidemic Supports The Chemical AIDS Theory Daniele Mandrioli EPIDEMIOLOGY France Population: 65.073.482 AIDS Incidence: 16/million Germany Population: 82.438.000 AIDS Incidence: 4/million
The Italian AIDS Epidemic Supports The Chemical AIDS Theory Daniele Mandrioli EPIDEMIOLOGY France Population: 65.073.482 AIDS Incidence: 16/million Germany Population: 82.438.000 AIDS Incidence: 4/million
Pediatric HIV Update NORTHWEST AIDS EDUCATION AND TRAINING CENTER
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Pediatric HIV Update Christian B. Ramers, MD, MPH Assistant Medical Director, Family Health Centers of San Diego HIV/HCV Distance Education Specialist - NWAETC,
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Pediatric HIV Update Christian B. Ramers, MD, MPH Assistant Medical Director, Family Health Centers of San Diego HIV/HCV Distance Education Specialist - NWAETC,
Chapter 22. Autoimmune and Immunodeficiency Diseases
 Chapter 22 Autoimmune and Immunodeficiency Diseases Autoimmune Diseases Failures of self-tolerance Immune system fails to distinguish selfantigens from foreign antigens This results in the immune system
Chapter 22 Autoimmune and Immunodeficiency Diseases Autoimmune Diseases Failures of self-tolerance Immune system fails to distinguish selfantigens from foreign antigens This results in the immune system
The HIV positive Child handout. Heidelberg October 2017 Dr. Charlotte Adamczick
 The HIV positive Child handout Heidelberg October 2017 Dr. Charlotte Adamczick Outline of the presentation 1. Some facts 2. The infected patient: early and late presentation 3. Treatment of the HIV related
The HIV positive Child handout Heidelberg October 2017 Dr. Charlotte Adamczick Outline of the presentation 1. Some facts 2. The infected patient: early and late presentation 3. Treatment of the HIV related
Overview of HIV. LTC Paige Waterman
 Overview of HIV LTC Paige Waterman Outline Background and Epidemiology HIV Virology, Transmission, and Pathogenesis Acute HIV infection HIV Diagnostics Management of Health Care Personnel Exposed to HIV
Overview of HIV LTC Paige Waterman Outline Background and Epidemiology HIV Virology, Transmission, and Pathogenesis Acute HIV infection HIV Diagnostics Management of Health Care Personnel Exposed to HIV
James Nuttall Paediatric Infectious Diseases Unit Red Cross Children s Hospital
 James Nuttall Paediatric Infectious Diseases Unit Red Cross Children s Hospital Paediatric HIV Infection Symposium, August 21, 2010, Red Cross Children s Hospital Overview of talk The 2010 paediatric guidelines
James Nuttall Paediatric Infectious Diseases Unit Red Cross Children s Hospital Paediatric HIV Infection Symposium, August 21, 2010, Red Cross Children s Hospital Overview of talk The 2010 paediatric guidelines
Introduction: WHO recommends that criteria for starting ART be defined in national protocols and that these
 ISSN: 0975-766X Available Online through Research Article www.ijptonline.com HEALTH PROFILE OF HIV POSITIVE INDIVIDUALS AT ANTI RETROVIRAL TREATMENT CENTRE, KADAPA DISTRICT Dr.K.Chandra Sekhar *, Dr. K.J.Kishore
ISSN: 0975-766X Available Online through Research Article www.ijptonline.com HEALTH PROFILE OF HIV POSITIVE INDIVIDUALS AT ANTI RETROVIRAL TREATMENT CENTRE, KADAPA DISTRICT Dr.K.Chandra Sekhar *, Dr. K.J.Kishore
Guidelines for Antiretroviral Therapy in Zimbabwe. The National Drug and Therapeutic Policy Advisory Committee (NDTPAC) December, 2003
 December, 2003") Guidelines for Antiretroviral Therapy in Zimbabwe The National Drug and Therapeutic Policy Advisory Committee (NDTPAC) December, 2003 Ministry of Health and Child Welfare, Republic of Zimbabwe Further
Guidelines for Antiretroviral Therapy in Zimbabwe The National Drug and Therapeutic Policy Advisory Committee (NDTPAC) December, 2003 Ministry of Health and Child Welfare, Republic of Zimbabwe Further
Rajesh T. Gandhi, M.D.
 HIV Treatment Guidelines: 2010 Rajesh T. Gandhi, M.D. Case 29 yo M with 8 weeks of cough and fever. Diagnosed with smear-positive pulmonary TB. HIV-1 antibody positive. CD4 count 361. HIV-1 RNA 23,000
HIV Treatment Guidelines: 2010 Rajesh T. Gandhi, M.D. Case 29 yo M with 8 weeks of cough and fever. Diagnosed with smear-positive pulmonary TB. HIV-1 antibody positive. CD4 count 361. HIV-1 RNA 23,000
Newly diagnosed HIV patient. Dr. Heila Redpath 06 FEBRUARY 2014
 Newly diagnosed HIV patient Dr. Heila Redpath 06 FEBRUARY 2014 PRIMARY HIV INFECTION: SEROCONVERSION SYMPTOMATIC HIV INFECTION AND AIDS ASYMPTOMATIC LATENT INFECTION CLOSED CIRCLES: CD4 cells OPEN
Newly diagnosed HIV patient Dr. Heila Redpath 06 FEBRUARY 2014 PRIMARY HIV INFECTION: SEROCONVERSION SYMPTOMATIC HIV INFECTION AND AIDS ASYMPTOMATIC LATENT INFECTION CLOSED CIRCLES: CD4 cells OPEN
Updates on Revised Antiretroviral Treatment Guidelines Overview 27 March 2013
 Updates on Revised Antiretroviral Treatment Guidelines 2013 Overview 27 March 2013 Introduction of Fixed Dose combination (FDC) FDCs will be available in facilities on 1 April 2013 The FDC ARV that will
Updates on Revised Antiretroviral Treatment Guidelines 2013 Overview 27 March 2013 Introduction of Fixed Dose combination (FDC) FDCs will be available in facilities on 1 April 2013 The FDC ARV that will
Treatment experience in South Africa. Dr Ian Sanne Clinical HIV Research Unit University of the Witwatersrand
 Treatment experience in South Africa Dr Ian Sanne Clinical HIV Research Unit University of the Witwatersrand Overview South African Prevalence Adherence Combination ddi + d4t Nevirapine Hepatotoxicity
Treatment experience in South Africa Dr Ian Sanne Clinical HIV Research Unit University of the Witwatersrand Overview South African Prevalence Adherence Combination ddi + d4t Nevirapine Hepatotoxicity
Paediatric ART: eligibility criteria and first line regimens. (revised) Dave le Roux 13 August 2016
 Dave le Roux 13 August 2016") Paediatric ART: eligibility criteria and first line regimens (revised) Dave le Roux 13 August 2016 Outline Eligibility criteria for starting ART Evolving evidence for earlier ART W Cape, National, WHO
Paediatric ART: eligibility criteria and first line regimens (revised) Dave le Roux 13 August 2016 Outline Eligibility criteria for starting ART Evolving evidence for earlier ART W Cape, National, WHO
Ch 18 Infectious Diseases Affecting Cardiovascular and Lymphatic Systems
 Ch 18 Infectious Diseases Affecting Cardiovascular and Lymphatic Systems Highlight Disease: Malaria World s dominant protozoal disease. Four species of Plasmodium: P. falciparum (malignant), P. vivax (begnin),
Ch 18 Infectious Diseases Affecting Cardiovascular and Lymphatic Systems Highlight Disease: Malaria World s dominant protozoal disease. Four species of Plasmodium: P. falciparum (malignant), P. vivax (begnin),
Medical monitoring: Clinical monitoring and laboratory tests
 medical monitoring: clincial monitoring and laboratory tests: 1 medical monitoring: clinical monitoring and laboratory tests Medical monitoring: Clinical monitoring and laboratory tests Aims This section
medical monitoring: clincial monitoring and laboratory tests: 1 medical monitoring: clinical monitoring and laboratory tests Medical monitoring: Clinical monitoring and laboratory tests Aims This section
HIV Lecture. Anucha Apisarnthanarak, MD Division of Infectious Diseases Thammasart University Hospital
 HIV Lecture Anucha Apisarnthanarak, MD Division of Infectious Diseases Thammasart University Hospital End-2001 global estimates for children and adults People living with HIV/AIDS New HIV infections in
HIV Lecture Anucha Apisarnthanarak, MD Division of Infectious Diseases Thammasart University Hospital End-2001 global estimates for children and adults People living with HIV/AIDS New HIV infections in
Opportunistic infections in the era of cart, still a problem in resource-limited settings
 Opportunistic infections in the era of cart, still a problem in resource-limited settings Cristiana Oprea Victor Babes Clinical Hospital for Infectious and Tropical Diseases, Bucharest, Romania Assessment
Opportunistic infections in the era of cart, still a problem in resource-limited settings Cristiana Oprea Victor Babes Clinical Hospital for Infectious and Tropical Diseases, Bucharest, Romania Assessment
GOALS AND OBJECTIVES INFECTIOUS DISEASE
 GOALS AND OBJECTIVES INFECTIOUS DISEASE Infectious Disease and HIV Overview: The Infectious Diseases Program at the University of Southern California prepares trainees for the management of problems in
GOALS AND OBJECTIVES INFECTIOUS DISEASE Infectious Disease and HIV Overview: The Infectious Diseases Program at the University of Southern California prepares trainees for the management of problems in
Overview of HIV WRAIR- GEIS 'Operational Clinical Infectious Disease' Course
 Overview of HIV WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED Acknowledgments - Dr. Christina Polyak - Dr. Julie Ake Disclaimer The views expressed in this presentation are
Overview of HIV WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED Acknowledgments - Dr. Christina Polyak - Dr. Julie Ake Disclaimer The views expressed in this presentation are
2nd line failure, provincial evaluation process for 3rd line therapy, 3rd line treatment options James Nuttall
 2nd line failure, provincial evaluation process for 3rd line therapy, 3rd line treatment options James Nuttall Paediatric Infectious Diseases Unit, Red Cross War Memorial Children s Hospital & University
2nd line failure, provincial evaluation process for 3rd line therapy, 3rd line treatment options James Nuttall Paediatric Infectious Diseases Unit, Red Cross War Memorial Children s Hospital & University
HIV in Obstetrics and Gynecology
 FAST FACTS HIV in Obstetrics and Gynecology Indispensable Guides to Clinical by J Richard Smith, Naomi Low-Beer and Bruce A Barron Practice HIV infection 7 Managing infected women 13 Preconceptual care
FAST FACTS HIV in Obstetrics and Gynecology Indispensable Guides to Clinical by J Richard Smith, Naomi Low-Beer and Bruce A Barron Practice HIV infection 7 Managing infected women 13 Preconceptual care
Updates on Paediatric HIV DCH 2018
 Updates on Paediatric HIV DCH 2018 Dr James Nuttall Paediatric Infectious Diseases Unit Red Cross War Memorial Children s Hospital & University of Cape Town james.nuttall@uct.ac.za HIV
Updates on Paediatric HIV DCH 2018 Dr James Nuttall Paediatric Infectious Diseases Unit Red Cross War Memorial Children s Hospital & University of Cape Town james.nuttall@uct.ac.za HIV
HIV 101: Overview of the Physiologic Impact of HIV and Its Diagnosis Part 2: Immunologic Impact of HIV and its Effects on the Body
 HIV 101: Overview of the Physiologic Impact of HIV and Its Diagnosis Part 2: Immunologic Impact of HIV and its Effects on the Body Melissa Badowski, PharmD, BCPS, AAHIVP Clinical Assistant Professor University
HIV 101: Overview of the Physiologic Impact of HIV and Its Diagnosis Part 2: Immunologic Impact of HIV and its Effects on the Body Melissa Badowski, PharmD, BCPS, AAHIVP Clinical Assistant Professor University
WHO/Euro Report of the Technical Consultation on Clinical Staging of HIV/AIDS and HIV/AIDS Case Definitions for Surveillance
 WHO/EURO REPORT OF THE TECHNICAL CONSULTATION ON CLINICAL STAGING OF HIV/AIDS AND HIV/AIDS CASE DEFINITIONS FOR SURVEILLANCE Copenhagen, Denmark 24 26 May 2005 WHO/Euro Report of the Technical Consultation
WHO/EURO REPORT OF THE TECHNICAL CONSULTATION ON CLINICAL STAGING OF HIV/AIDS AND HIV/AIDS CASE DEFINITIONS FOR SURVEILLANCE Copenhagen, Denmark 24 26 May 2005 WHO/Euro Report of the Technical Consultation
AIDS at 25. Epidemiology and Clinical Management MID 37
 AIDS at 25 Epidemiology and Clinical Management Blood HIV Transmission transfusion injection drug use Sexual Intercourse heterosexual male to male Perinatal intrapartum breast feeding Regional HIV and
AIDS at 25 Epidemiology and Clinical Management Blood HIV Transmission transfusion injection drug use Sexual Intercourse heterosexual male to male Perinatal intrapartum breast feeding Regional HIV and