The New Agents: Management of Experienced Patients and Resistance. Joel E. Gallant, MD, MPH Johns Hopkins University School of Medicine
|
|
|
- Bryan Booth
- 5 years ago
- Views:
Transcription
1 The New Agents: Management of Experienced Patients and Resistance Joel E. Gallant, MD, MPH Johns Hopkins University School of Medicine
2 T.D. 45 year old man with HIV infection diagnosed in 2000 On multiple non-suppressive ART regimens, including NRTIs, NNRTIs, PIs, with CD4 counts gradually dropping from high 400 s to low 200 s, VL 20K-100K His previous doctor said Don t worry about numbers, as long as you feel good! Now on ATV/r + EFV + TDF/FTC
3
4
5 When to Modify Therapy Studies to date show better responses with earlier switches, as well as viral evolution at low-level viremia
6 Without loss of 1 drug equivalent Without new mutation The Rate of Losing Future Treatment Options SCOPE cohort: Treatmentexperienced patients (n=106) Stable ART for 120 days 0.50 VL > 1000 c/ml 1 resistance mutation Resistance testing every 4 mos until ART modification new major PI mutation * 1 new NRTI mutation Any new mutation * Data are for PI-treated subjects (n = 71) Time (mos) New mutations at 1 year Any: 44% (95% CI 33 56) NRTI: 23% (95% CI 15 34) PI: 18% (95% CI 9 34) Hatano et al. 13 th CROI 2006; Poster Time (mos) Number of available ARVs from the following: ZDV, 3TC, ddi, ABC, TDF, EFV, IDV, NFV, SQV, RTV, APV, LPV
7 When to Modify Therapy Studies to date show better responses with earlier switches, as well as viral evolution at low-level viremia The risk of emergence of new mutations is highest in patients with little resistance
8 When to Modify Therapy Studies to date show better responses with earlier switches, as well as viral evolution at low-level viremia The risk of emergence of new mutations is highest in patients with little resistance The consequences of continued failure depend on the drugs being used: Rapid, high-level resistance: 3TC, FTC, NNRTIs Eventual, intermediate-level resistance: TDF, ABC Cumulative resistance over time: AZT, d4t, unboosted PIs Minimal resistance: boosted PIs (in PI-naïve pts)
9 Antiretroviral Agents Approved in the U.S. (April 2009) NRTIs NNRTIs PIs zidovudine (AZT) Retrovir & generic didanosine (ddi) Videx, Videx EC & generic nevirapine (NVP) Viramune delavirdine (DLV) Rescriptor saquinavir (SQV) Invirase indinavir (IDV) Crixivan stavudine (d4t) Zerit efavirenz (EFV) - Sustiva ritonavir (RTV) Norvir lamivudine (3TC) Epivir etravirine (ETR) - Intelence abacavir (ABC) Ziagen Nucleotide RTIs nelfinavir (NFV) Viracept emtricitabine (FTC) - Emtriva tenofovir DF (TDF) -Viread lopinavir/rtv (LPV/r) - Kaletra CCR5 Inhibitors Fusion Inhibitors atazanavir (ATV) - Reyataz maraviroc (MVC) - Selzentry enfuvirtide (ENF, T20) - Fuzeon fosamprenavir (FPV) - Lexiva Integrase Inhibitors raltegravir (RAL) - Isentress tipranavir (TPV) - Aptivus darunavir (DRV) - Prezista
10 Antiretroviral Agents Approved in the U.S. (April 2009) NRTIs NNRTIs PIs zidovudine (AZT) Retrovir & generic didanosine (ddi) Videx, Videx EC & generic nevirapine (NVP) Viramune delavirdine (DLV) Rescriptor saquinavir (SQV) Invirase indinavir (IDV) Crixivan stavudine (d4t) Zerit efavirenz (EFV) - Sustiva ritonavir (RTV) Norvir lamivudine (3TC) Epivir etravirine (ETR) - Intelence abacavir (ABC) Ziagen Nucleotide RTIs nelfinavir (NFV) Viracept emtricitabine (FTC) - Emtriva tenofovir DF (TDF) -Viread lopinavir/rtv (LPV/r) - Kaletra CCR5 Inhibitors Fusion Inhibitors atazanavir (ATV) - Reyataz maraviroc (MVC) - Selzentry enfuvirtide (ENF, T20) - Fuzeon fosamprenavir (FPV) - Lexiva Integrase Inhibitors raltegravir (RAL) - Isentress tipranavir (TPV) - Aptivus darunavir (DRV) - Prezista
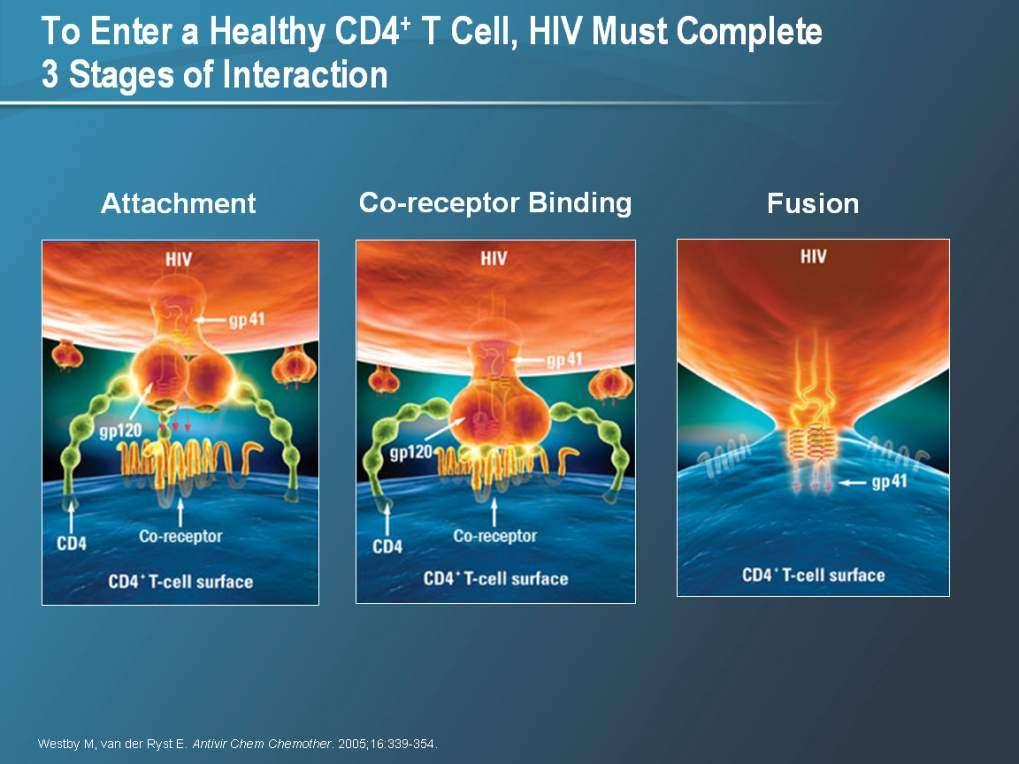
11 The HIV-1 Replication Cycle Protease Inhibitors RT = reverse transcriptase; LTR = long terminal repeat.
12 Resistance Patterns after PI Failure NFV: Unboosted PIs 30N: no cross-resistance 90M: cross-resistance SQV: 48V: no cross-resistance 90M: cross resistance ATV: 50L: no cross-resistance IDV: FPV Various mutations causing cross-resistance I54L/M, V32I + I47V: Variable cross-resistance RTV-Boosted PIs No PI resistance after failure of: LPV/r FPV/r SQV/r ATV/r DRV/r
13 ARTEMIS: DRV/r vs LPV/r in Treatment- Naive Patients Randomized, phase III, open-label study undertaken in 26 countries Week 48 primary endpoint Week 96 ART-naive patients with any CD4 count and VL > 2000 c/ml (N = 689) DRV/r 800/100 mg QD + TDF/FTC (n = 343) LPV/r 400/100mg BID or 800/200mg QD* + TDF/FTC (n = 346) Baseline disease characteristics in DRV/r vs LPV/r arms Median VL: 70,800 c/ml vs 62,100 c/ml Median CD4 count: 228 vs % of patients switched from capsule to tablet formulation of LPV/r during study; switch made according to local regulatory approval and drug availability *Dosing based on regulatory approval; 77% of patients received BID dosing. Mills A, et al. ICAAC/IDSA Abstract 1250c.
14 VL < 50 % [±SE] ARTEMIS: Week 96 Response to DRV/r vs LPV/r in Naive Patients Week 48: 96: Estimated difference in response vs LPV/RTV LPV/r for for noninferiority: PP: = 8.4% 5.6% (95% CI: 1.9% -0.1 to 11.3; 14.8%; P < P.001) <.001) Estimated difference in response vs LPV/RTV LPV/r for for superiority: ITT: = 8.3% 5.5% (95% CI: 1.8% -0.3 to 11.2; 14.7%; P = P.062) <.012) Superiority at Week 96 also observed when DRV/r (n = 343) compared with subset of patients treated with twice-daily LPV/r only (n = 258) 79% vs 72% (P =.038) Mills A, et al. ICAAC/IDSA Abstract 1250c. Primary endpoint 84% 78% Weeks DRV/r (n = 343) LPV/r (n = 346) 79% 71%
15 VFs (%) Virologic Failure Less Frequent with DRV/r than LPV/r 30 *p< /343 (11.7%) 59/346 (17.1%) Never suppressed Rebounders 0 DRV/r LPV/r *Pearson chi-square test ARTEMIS 96 week analyses
16 ARTEMIS: Resistance with Virologic Failure Number of patients, n DRV/r (n=343) LPV/r (n=346) VFs Paired genotypes Developing major (IAS-USA) PI RAMs Developing minor (IAS-USA) PI RAMs Developing major non-polymorphic PI RAMs Developing minor non-polymorphic PI RAMs Developing (IAS-USA) NRTI RAMs Paired phenotypes Loss of susceptibility to any PI* 0 0 Loss of susceptibility to FTC 1 4 Loss of susceptibility to TDF 0 0 *PREZISTA, LPV, APV, ATV, IDV, NFV, SQV and TPV 1. Johnson VA, et al. Top HIV Med 2007;15: Molina JM, et al. ICAAC/IDSA Abstract H-1250d Lathouwers E, et al. 7th EHDRW Poster 58
17 Median Change in VL at Wk 24 (log 10 copies/ml) Relationship of TPV Score to TPV Phenotype Results and Response TPV Score (n = 242) (n = 260) (n = 68) (n = 4) (n = 144) TPV Score Mutations 10V, 13V, 20M/R/V, 33F, 35G, 36I, 43T, 46L, 47V, 54A/M/V, 58E, 69K, 74P, 82L/T, 83D, 84V -3 *24-week data from patients in RESIST-1 and -2 given TPV/r. Valdez H, et al. Antivir Ther. 2005;10:S29
18 Pts With VL <50 c/ml (%) POWER 1 and 2: VL <50 c/ml at Week 48 (ITT-TLOVR) DRV/r 600/100 mg BID Control *P <.001 vs comparator PI/r 60 45%* 46%* % 10% Weeks Not all patients had reached Week 48 at the time of analysis; patients who had not reached Week 48 were censored at their last available visit Lazzarin A, et al. IAC Abstract TUAB0104
19 Patients With HIV RNA < 50 c/ml at Wk 24 (%) Patients With HIV RNA < 50 c/ml at Wk 24 (%) Effect of Baseline Resistance on Response to DRV 11 mutations associated with reduced response n = V11I, V32I, L33F, I47V, I50V, I54L, I54M, G73S, L76V, I84V and L89V Number of Primary PI Baseline Mutations Baseline fold-change strongest predictor of Week 24 response (Antivirogram) FC 10 FC Baseline DRV FC 13 n = FC > 40 DeMeyer S, et al. Antivir Ther. 2006;11:S83.
20 TPV and DRV Mutations and Phenotypic Cut-offs Similarities and Differences in Key Mutations TPV 10V 13V 20M/R 33F 35G 36I 43T 46L 47V DRV 11I 32I 33F 47V TPV 54A/M/V 58E 69K 74P 82L/T 83D 84V 90M DRV 50V 54L/M 74P 76V 84V 89V Phenotypic Cutoffs Assay/ Cutoff Monogram: FC for Reduced Activity Monogram: FC for No Response Virco: FC for Maximal Response Virco: FC for Minimal Response TPV [1,2] 2 8 < DRV [3,4] < Coakley E, et al. Antivir Ther. 2006;11:S Bacheler L, et al. Euro Resistance Wkshp Abstract De Meyer S, et al. Antivir Ther. 2006;11:S Winters B, et al. Antivir Ther. 2006; 11:S180.
21 Tipranavir and Darunavir: Side Effects and Toxicity DRV/r Less diarrhea than LPV/r in TITAN More rash than LPV/r in TITAN TPV/r More hyperlipidemia than other PIs More hepatotoxicity than other PIs Intracranial hemorrhage (head surgery, head trauma, or bleed diathesis) If both drugs look equally active, DRV/r preferred
22 TITAN: DRV/r vs LPV/r in Experienced, LPV/r-Naive Patients Stratification by treatment site, use of NNRTI in OBR, and VL > or < 50,000 Week 48 prespecified primary analysis Week 96 Experienced, LPV-and DRV-naive patients with VL > 1000 (N = 595) DRV/r 600/100 mg bid + OBR (n = 298) LPV/r* 400/100 mg bid + OBR (n = 297) Arms well balanced at baseline except for proportion with > 2 active drugs in OBR: 65% DRV/r vs. 51% LPV/r LPV/r increased to 533/133 mg bid (caps) or 600/150 mg bid (for tabs) if NNRTI included in OBR. Valdez-Madruga J, et al. IAS Abstract TUAB101; Madruga JV, et al. Lancet. 2007;370:49-58
23 TITAN: VL < 50 c/ml at Week 48 by Baseline LPV Fold Change DRV/r met criteria for superiority to LPV/r in proportion of pts with VL < 50 c/ml in overall study population DRV/r noninferior but not superior in patients with baseline LPV FC 10 Patient Response, % DRV/r LPV/r DRV/r-LPV/r, % (95% CI)* Noninferiority P Value* Superiority P Value* Overall (n = 595) (3 to 19) < LPV FC 40 (n = 569) (2 to 18) < LPV FC 10 (n = 524) (-1 to 16) < *Estimated from logistic regression model including treatment and stratification factors: baseline VL and use of NNRTIs in OBR. Valdez-Madruga J, et al. IAS Abstract TUAB101. Madruga JV, et al. Lancet. 2007;370:49-58
24 Patients With VF (%) Patients With VF (%) TITAN: Virologic Failure Rates (ITT-TLOVR) Virologic failure = nonresponders and rebounders with VL > 400 c/ml All Patients 25 Mutations at failure: 20 LPV/r: 20/56 22% Patients With LPV FC 10 19% DRV/r: 6/ % 10 10% n = 31 n = 65 0 n = 26 n = 50 DRV/r (n = 298) LPV/r (n = 297) DRV/r (n = 263) LPV/r (n = 261) Valdez-Madruga J, et al. IAS Abstract TUAB101. Madruga JV, et al. Lancet. 2007;370:49-58
25 Primary PI mutations that developed in DRV/r group VFs 6 VFs developed primary PI mutation(s) V32I (n=3), I47V, and L76V (n=2), M46I, I54L and I54M (n=1) all but M46I are DRV RAMs 1 previously used 2 6 PIs LPV/r group 24 VFs developed primary PI mutation(s) M46I (n=9), L33F, I47V, and L76V (n=4), M46L, and V82A (n=3), V32I, I47A, and I84V (n=2), I50V, I54M, V82S, and L90M (n=1) all LPV RAMs 1 previously used 1 4 PI(s) 1 Johnson VA, et al. Top HIV Med 2007;15: TITAN 96 week analysis
26 VFs with loss of susceptibility to an ARV (%) VFs with loss of susceptibility to an ARV (%) Fewer VFs on DRV/r than on LPV/r lost susceptibility to PI or NRTI(s) in the treatment regimen, after excluding patients with baseline LPV FC 10 or prior use of 2 PIs Baseline LPV FC 10 Previous use of 1 PI DRV/r (n=33) LPV/r (n=55) DRV/r (n=23) LPV/r (n=40) p<0.001* 31% 17/55 p<0.01* p<0.05* p<0.05* 35% 15/ % 11/34 23% 9/ % 0/33 PI in regimen 6% 2/32 NRTI(s) in OBR % 0/23 PI in regimen 5% 1/22 NRTI(s) in OBR *Exact Chi-Squared Test; TITAN 96 week analysis
27 VFs with retained PI susceptibilitity (%) More VFs on DRV/r than on LPV/r retained susceptibility to PIs DRV/r LPV/r 20 0 DRV APV ATV IDV LPV SQV TPV susceptible at endpoint susceptible at baseline TITAN 96 week analysis
28 VFs with retained PI susceptibilitity (%) More VFs on DRV/r than on LPV/r retained susceptibility to PIs, after excluding patients with baseline LPV FC 10 or prior use of 2 PIs Baseline LPV FC 10 Previous use of 1 PI DRV/r LPV/r DRV APV ATV IDV LPV SQV TPV 0 DRV APV ATV IDV LPV SQV TPV susceptible at EP susceptible at BL TITAN 96 week analysis
29 The HIV-1 Replication Cycle RT Inhibitors RT = reverse transcriptase; LTR = long terminal repeat.
30 DUET-1 and -2: Etravirine + DRV/r- Containing OBR, Phase III Trials Week 24: primary endpoint Week 48: current analysis Week 96: planned follow-up HIV+ patients with virologic failure on current ART, history of 1 NNRTI mutation, 3 PI mutations, and VL > 5000 c/ml (DUET-1: N = 612; DUET-2: N = 491) ETR 200 mg twice daily + DRV/r-containing OBR* (DUET-1: n = 304; DUET-2: n = 295) Placebo + DRV/r-containing OBR* (DUET-1: n = 308; DUET-2: n = 296) *Investigator-selected OBR comprising DRV/r 600/100 mg twice daily + 2 NRTIs ± ENF. Cahn P, et al. IAC Abstract TUPE0047.
31 VL < 50 c/ml at Wk 48, % ± 95% CI DUET-1 and -2: Etravirine vs. Placebo in Treatment-Experienced Patients Mean CD4 change at Week 48 significantly greater in ETR arm: +98 vs +73 i 1,2] ETR (n = 599) ITT-TLOVR PBO (n = 604) 61% 40% P < Time (Weeks) 1. Haubrich R, et al. CROI Abstract 790; 2. Johnson M, et al. CROI Abstract 791;
32 Etravirine Resistance: Clinical Implications Effective against many NNRTI-resistant strains K103N does not decrease susceptibility (and may improve activity 1 ) Other NNRTI mutations vary in their effect on ETR activity Efficacy decreases with increasing NNRTI mutations No benefit with continued EFV or NVP therapy after failure Greater cross-resistance after failure of NVP than EFV 1 Don t continue EFV or NVP in a non-suppressive regimen Use genotypes drawn at time of NNRTI failure to assess ETR susceptibility 1. Marcelin AG, et al. CROI Abstract 645
33 Number of baseline ETR mutations DUET: Response (<50 c/ml) by Number of ETR mutations /161 64/147 73/121 59/157 38% 37/64 17/68 13/32 6/24 7/28 3/18 ETR + BR (n=406) 17% 25% 25% 25% Pts with VL <50 at Week 24 (%) PBO + BR (n=414) 41% 44% 58% 60% % V90I, K101E/P, A98G, V179D/F, L100I, G190A/S, V106I, Y181C/I/V Greatest added benefit with ETR vs. PBO seen in pts with <3 ETR mutations 86% of patients had <3 ETR mutations Excludes pts who used de-novo ENF or discontinued except for virological failure
34 New Weighted Scores for ETR Susceptibility Monogram 4: 100I, 101P, 181C/I 3: 138A/G, 179E, 190Q, 230L, 238N 2: 101E, 106A, 138K, 179L, 188L 1: 90I, 101H, 106M, 138Q, 179D/F/M, 181F, 190E/T, 221Y, 225H, 238T > 4 = reduced susceptibility 3: 181I/V Tibotec 2.5: 101P, 100I, 181C, 230L 1.5: 138A, 106I, 190S, 179F 1: 90I, 179D, 101E, 101H, 98G, 179T, 190A 0-2: 74% response : 52% response > 4: 38% response
 TBT score 1 MGR score 2 sensitive resistant sensitive resistant")
: A26 2. Benhamida J, et al.")
35 Methods A single cut-off was used to categorise samples as sensitive or with reduced susceptibility ( resistant ) TBT score 1 MGR score 2 sensitive resistant sensitive resistant These cut-offs were set at 2 for the Tibotec algorithm and 3 for the Monogram algorithm 1. Vingerhoets J, et al. Antivir Ther 2008;13(Suppl. 3): A26 2. Benhamida J, et al. Antivir Ther 2008;13(Suppl. 3): A142
36 The HIV-1 Replication Cycle Entry Inhibitors RT = reverse transcriptase; LTR = long terminal repeat.
37
 Emerge in later disease Associated with accelerated CD4 T-cell decline and disease progression CD4 CCR5 Berger EA, et")
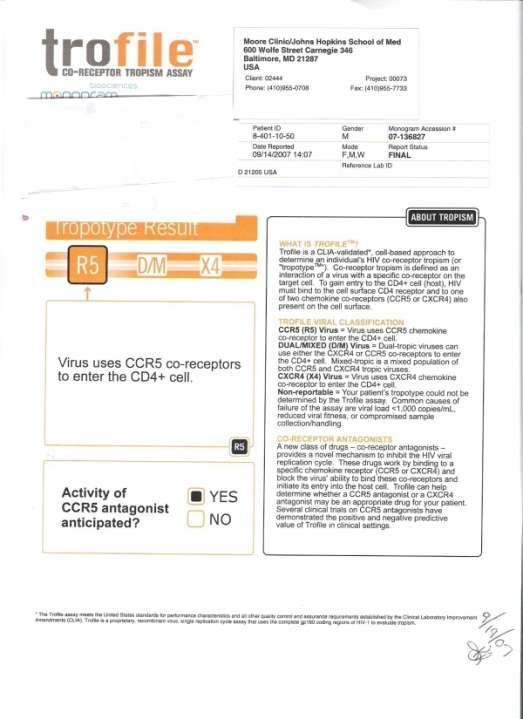
38 R5 Viruses Utilize the CCR5 co-receptor Also known as M-tropic or nonsyncytium inducing (NSI) Transmitted variants Prevalent in early disease Dual Viruses Can utilize either co-receptor X4 Viruses Utilize the CXCR4 co-receptor Also known as T-tropic or syncytium inducing (SI) Emerge in later disease Associated with accelerated CD4 T-cell decline and disease progression CD4 CCR5 Berger EA, et al. Nature. 1998;391:240. T-cell surface CXCR4
39 MOTIVATE-1 and -2: MVC + OBR vs Placebo + OBR, Phase III Trials 1:2:2 randomization; stratified by enfuvirtide use and VL< or 100,000 c/ml Week 48 Treatment-experienced HIV+ patients with R5-tropic virus only, VL 5000, stable or no ART for 4 wks, resistance to and/or 6 mos of 1 antiretroviral from 3 classes or 2 PIs (MOTIVATE 1: N = 601; MOTIVATE 2: N = 475) Placebo + OBR* (n = 209) MVC once daily (150 mg or 300 mg ) + OBR (n = 414) MVC twice daily (150 mg or 300 mg ) + OBR (n = 426) *OBR comprising 3-6 antiretroviral agents. Patients receiving PI (other than tipranavir) or delavirdine received 150 mg; all others received 300 mg. 1. Nelson M, et al. IAC Abstract TUPE Asmuth A, et al. IAC Abstract TUPE0050.
40 Patients (%) MOTIVATE 1 and 2: Maraviroc vs. Placebo in Experienced Patients with R5-tropic Virus Time (Weeks) PBO + OBT (n = 209) MVC QD + OBT (n = 414) MVC BID + OBT (n = 426) *P <.0001 vs PBO 45.5%* 43.2%* 16.7% Hardy D, et al. CROI Abstract 792.
41 Median CD4 Count Δ From Baseline Effect of Maraviroc on CD4 Count Analysis of MERIT study [1] Δ CD4 % 150 P =.004 for the difference over time % + 9.5% MVC + ZDV/3TC (n = 360) EFV + ZDV/3TC (n = 360) Weeks In separate study, addition of MVC in 9 patients with VL <50 but CD4 counts < 250 on current ART regimen did not significantly increase CD4count recovery with 5 mos of follow-up (P >.39) [2] 1. Lazzarin A, et al. ICAAC/IDSA Abstract Paez S, et al. ICAAC/IDSA Abstract 1247.

42 Emergence of D/M tropic virus on CCR5 antagonist therapy Treatment Start Failure Treatment Stop R5 R5 D/M D/M D/M D/M D/M D/M R5 R Time since first administration (days) R5 D/M X4 Non-functional clone Clonal and phylogenic analyses suggest emergent D/M tropic virus on CCR5 antagonists predominantly from pre-existing population Clinical implications of emerging D/M virus remain to be fully defined Lewis M, et al. XVI IHIVDRW, Barbados 2007, #56
43 Tropism in Experienced Patients as Identified by Trofile ( n= 6,857) Study/Source Population N R5 D/M X4 MOTIVATE 1 & 2 4 Experienced % 41% 3% TORO 1/2 5 Experienced % 46% 4% ACTG Experienced % 47% 4% SCOPE 7 Experienced % 39.5% 0.5% HOMER cohort 1 Naive % 18% <1% C & W cohort 2 Naive % 19% <1% Demarest 3 Naive % 12% 0% Pfizer Naive % 15% <1 1 Brumme ZL, et al. J Infect Dis. 2005;192: Moyle GJ, et al. J Infect Dis. 2005;191: Demarest J, et al. ICAAC Abstract H Coakley E, et al. 2nd Viral Entry Workshop, Abstract 8 5 Melby et al 13th CROI 2006 Abstract Wilkin T, et al. CROI Abstract Hunt et al. J Infect Dis. 2006;194:926-30
44 VL< 50 at Wee k 48 (%) Reanalysis of Virologic Efficacy in MERIT With Enhanced Tropism Assay Enhanced phenotypic tropism assay resulted in reclassification of 15% of patients from R5 to D/M at screening Noninferiority criteria (rates of HIV-1 RNA < 50 copies/ml) met when D/M patients excluded EFV+ ZDV/3TC MVC + ZDV/3TC Overall By Baseline VL MERIT MERIT-ES MERIT MERIT-ES < 100, ,000 < 100, , n= Saag M, et al. ICAAC/IDSA Abstract 1232a.
45 The Role of Maraviroc Requires screening with expensive tropism (Trofile) assay (currently ~$2000 per test) ~50% of experienced patients not candidates for MVC due to presence of D/M or X4 virus D/M or X4 virus can be missed if present at <0.3% with enhanced susceptibility assay Most likely to work in naïve patients, but little rationale for use in first-line regimens


46 The HIV-1 Replication Cycle Integrase Inhibitors RT = reverse transcriptase; LTR = long terminal repeat.
47 BENCHMRK-1 & -2: RAL in Treatment- Experienced Patients Randomized 2:1; stratified by ENF use/nonuse and resistance to 1 vs > 1 PI Week 16 primary analysis Week 96 current analysis Week 256 planned follow-up HIV-infected patients with tripleclass resistance and VL > 1000 RAL 400 mg BID + OBR* (BENCHMRK-1: n = 234; BENCHMRK-2: n = 232) (BENCHMRK-1: N = 352; BENCHMRK-2: N = 351) Placebo + OBR* (BENCHMRK-1: n = 118; BENCHMRK-2: n = 119) *Investigator-selected OBR based on baseline resistance data and history; inclusion of DRV and TPV permitted.
48 Patients (%) BENCHMRK-1: Raltegravir vs. Placebo in Experienced Patients % 65% P <.001 P < % 31% Weeks RAL n = PBO n = Cooper DA, et al. CROI Abstract 788.
49 Percent with HIV RNA <50 c/ml SWITCHMRK (Protocols 032 & 033): Percent with HIV RNA <50 C/mL (NC = F) % 90 87% 80 88% 70 (95% CI) : -6.6 (-14.4, 1.2) 81% (95% CI) : -5.8 (-12.2, 0.2) Protocol 032 Protocol Weeks Number of Contributing Patients Weeks RAL + ARTs LPV/r + ARTs Eron J, et al. CROI Abstract 70aLB
50 SWITCHMRK -1 and -2: Baseline Characteristics Characteristic RAL (n = 174) Protocol 032 Protocol 033 LPV/r (n = 174) RAL (n = 176) LPV/r (n = 178) Mean age Sex (% female) Race (% nonwhite) VL 50 (%) Mean CD4 count LPV/r use 1 yr (%) Med. Yrs of previous ART (range) 3.3 ( ) 3.6 ( ) 3.7 ( ) 4.6 ( ) Med. # of previous ARV drugs (range) 5.0 ( ) 5.0 ( ) 5.5 ( ) 6.0 ( ) Eron J, et al. CROI Abstract 70aLB.
51 BENCHMRK 1 & 2: Evolution from N155 to Q148 Mutations Over Time Virologic failure in 105/462 patients receiving RAL 94 had baseline & virologic failure samples 30 had no genetic changes 64 (68%) failures in current analysis First Genotype (n = 64) 27% % % Mixed 92 Second Genotype (n = 51) 53% Hazuda D, et al. ICAAC/IDSA Abstract 898.

52 Integrase Assay Determines RAL Susceptibility Phenotypic integrase resistance assay now commercially available Amplification threshold: VL > 500 Biological cutoff for RAL is FC > 1.5 Does not detail genotypic mutations Fransen S, et al. ICAAC/IDSA Abstract 1214.
53 The Role of Raltegravir Combined with other active drugs in experienced patients with resistant virus To replace other agents in patients experiencing toxicity Consider activity of other agents in the regimen Be especially careful when switching from a PI/r to RAL As alternative to PI therapy in patients failing initial NNRTI regimen As alternative to NNRTIs or PIs for initial therapy
54 Sequencing Options after First Failure 2 NRTIs + NNRTI NRTIs + ETR Assess susceptibility to both NRTIs and ETR PI/r + ETR ETR Not recommended in combination with PIs other than DRV/r and SQV/r. Assess ETR susceptibility RAL+ ETR Low-barrier drugs. Would require proof of ETR susceptibility PI + RAL Full activity of both agents regardless of resistance. May be possible without RTV boosting (e.g. RAL + ATV) NRTIs + PI/r Likely to be effective because of PI/r regardless of NRTI resistance.
55 Treating the Highly Experienced Patient Step 1: How Many Active Drugs are Available? Raltegravir: Assume activity if naïve to integrase inhibitors Darunavir or tipranavir: Assess susceptibility with phenotype, virtual phenotype, or cumulative genotype Etravirine: Assess ETR susceptibility, preferably using genotypes obtained at failure of prior NNRTIs Maraviroc: Assess tropism Enfuvirtide: Necessary in select cases(d/m-tropic with crossresistance to DRV and ETR) NRTIs: Resistance likely. May have partial activity, but rarely count as fully active agents.
56 Treating the Highly Experienced Patient Step 2: How Many Drugs do you Need? Clinical trials suggest that patients should be treated with at least 2 fully active drugs
57 Patients,% MOTIVATE 1 & 2: VL < 50 at Wk 24 by Number of Active Drugs in OBR N = PBO + OBR MVC QD + OBR MVC BID + OBR Combined Analysis: MOTIVATE 1 and Number of active drugs in OBR Nelson M, et al. CROI Abstract 104aLB. Lalezari J, et al. CROI Abstract 104bLB.
58 BENCHMRK-1 & -2: Undetectable VL at Week 48, Overall and by GSS RAL Overall By GSS: n PBO Rates of virologic suppression also greater with RAL vs PBO when analyzed by baseline PSS Similar results when assessing PSS by number of fully active drugs and by number of fully or partially active drugs Patients (%) 1. Cooper DA, et al. CROI Abstract 788; 2. Steigbigel R, et al. CROI Abstract 789.
59 12/36 0/35 121/203 51/ / /305 VL < 50 c/ml at Wk 48, % DUET-1 and -2: VL < 50 at Wk 48, by Active Agents in OBR 100 ETR (n = 599) PBO (n = 604) # of Active Agents in OBR by PSS (DRV active if FC < 40) Haubrich R, et al. CROI Abstract 790; 2. Johnson M, et al. CROI Abstract 791; 3. Winters B, et al. CROI Abstract 873.
60 Treating the Highly Experienced Patient Step 2: How Many Drugs do you Need? Clinical trials suggest that patients should be treated with at least 2 fully active drugs Considerations: Partial susceptibility (PIs, ETR) Low-level D/M or X4 virus (MVC) NRTI resistance common. Are NRTIs necessary? To be determined by ACTG 5241
61
62
63 T.D. RAL: Naïve to integrase inhibitors: expect full susceptibility DRV/r: Phenotypic fold-change 13. Intermediate susceptibility range = Expect good activity MVC: Has R5-tropic virus (by original assay). Expect good activity ETR: Was not available when he started his regimen. Monogram score = 3 (101H= L=2): expect activity Tibotec score = 1 (101H=1): expect activity
64 T.D. T.D. was started on a regimen of DRV/r + RAL + MVC He tolerated it well and has now been on therapy for over 1 years His VL is <50, and his CD4 count is 535.
65 The Goal of Therapy The goal of therapy is virologic suppression to <50 c/ml in all patients. -DHHS & IAS-USA Guidelines 1.US Department of Health and Human Services. Available at: Accessed May 7, Hammer S, et al. JAMA. 2006;296:
66 The Next Drugs? Rilpivirine: NNRTI with promise for initial therapy. Probable cross-resistance with ETR Elvitegravir: Once-daily boosted integrase inhibitor. Cross-resistance with RAL Vicriviroc: Once-daily boosted CCR5 inhibitor. Will be ineffective in patients who fail MVC with D/M-tropic virus

67
68 Helpful Resources Johns Hopkins HIV Guide: (http: Medical Management of HIV Infection J.G. Bartlett & J.E. Gallant Other useful websites: Clinical Care Options: Medscape: Stanford HIV Resistance Database: DHHS Guidelines:
Management of Treatment-Experienced Patients: New Agents and Rescue Strategies. Joel E. Gallant, MD, MPH Johns Hopkins University School of Medicine
 Management of Treatment-Experienced Patients: New Agents and Rescue Strategies Joel E. Gallant, MD, MPH Johns Hopkins University School of Medicine When to Modify Therapy! Studies to date show better responses
Management of Treatment-Experienced Patients: New Agents and Rescue Strategies Joel E. Gallant, MD, MPH Johns Hopkins University School of Medicine When to Modify Therapy! Studies to date show better responses
Nobel /03/28. HIV virus and infected CD4+ T cells
 Mechanism of HIV drug resistance. Rodrigo Brindeiro / Amilcar Tanuri Laboratório de Virologia Molecular UFRJ 2 -Asso ciate Research Scientist, Internatio nal Center fo r Aids Care and Treatment Programs-ICAP,
Mechanism of HIV drug resistance. Rodrigo Brindeiro / Amilcar Tanuri Laboratório de Virologia Molecular UFRJ 2 -Asso ciate Research Scientist, Internatio nal Center fo r Aids Care and Treatment Programs-ICAP,
Northwest AIDS Education and Training Center Educating health care professionals to provide quality HIV care
 Northwest AIDS Education and Training Center Educating health care professionals to provide quality HIV care www.nwaetc.org The Northwest AIDS Education and Training Center (NW AETC), located at the University
Northwest AIDS Education and Training Center Educating health care professionals to provide quality HIV care www.nwaetc.org The Northwest AIDS Education and Training Center (NW AETC), located at the University
HIV Drugs and the HIV Lifecycle
 HIV Drugs and the HIV Lifecycle Together, we can change the course of the HIV epidemic one woman at a time. #onewomanatatime #thewellproject All HIV drugs work by interrupting different steps in HIV's
HIV Drugs and the HIV Lifecycle Together, we can change the course of the HIV epidemic one woman at a time. #onewomanatatime #thewellproject All HIV drugs work by interrupting different steps in HIV's
MEDICAL COVERAGE GUIDELINES ORIGINAL EFFECTIVE DATE: 03/07/18 SECTION: DRUGS LAST REVIEW DATE: 02/19/19 LAST CRITERIA REVISION DATE: ARCHIVE DATE:
 FUZEON (enfuvirtide) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
FUZEON (enfuvirtide) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
HIV Treatment: New and Veteran Drugs Classes
 HIV Treatment: New and Veteran Drugs Classes Jonathan M Schapiro, MD National Hemophilia Center Stanford University School of Medicine Rome, March 2013 Overview Many excellent antiretroviral agents are
HIV Treatment: New and Veteran Drugs Classes Jonathan M Schapiro, MD National Hemophilia Center Stanford University School of Medicine Rome, March 2013 Overview Many excellent antiretroviral agents are
Second-Line Therapy NORTHWEST AIDS EDUCATION AND TRAINING CENTER
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Second-Line Therapy David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, Division of Infectious Diseases University of Washington Presentation
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Second-Line Therapy David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, Division of Infectious Diseases University of Washington Presentation
HIV Pharmacology 101ish - 202ish: New HIV Clinicians Workshop
 HIV Pharmacology 101ish - 202ish: New HIV Clinicians Workshop Parya Saberi, PharmD, MAS The Medical Management of HIV/AIDS December 2012 Objectives What are commonly used ARVs and where do they work in
HIV Pharmacology 101ish - 202ish: New HIV Clinicians Workshop Parya Saberi, PharmD, MAS The Medical Management of HIV/AIDS December 2012 Objectives What are commonly used ARVs and where do they work in
Josep Mallolas Hospital Clínic Barcelona
 Nuevos paradigmas en la infección VIH Josep Mallolas Hospital Clínic Barcelona 1. Do you believe, I have to start ARV therapy? Incidence and Mortality of AIDS in Spain HIV and NON-AIDS complications HIV
Nuevos paradigmas en la infección VIH Josep Mallolas Hospital Clínic Barcelona 1. Do you believe, I have to start ARV therapy? Incidence and Mortality of AIDS in Spain HIV and NON-AIDS complications HIV
HIV MEDICATIONS AT A GLANCE. Atripla 600/200/300 mg tablet tablet daily. Complera 200/25/300 mg tablet tablet daily
 HIV MEDICATIONS AT A GLANCE Generic Name Trade Name Strength DIN Usual Dosage Single Tablet Regimen (STR) Products Efavirenz/ Emtricitabine/ rilpivirine/ elvitegravir/ cobicistat/ alafenamide Emtricitabine/
HIV MEDICATIONS AT A GLANCE Generic Name Trade Name Strength DIN Usual Dosage Single Tablet Regimen (STR) Products Efavirenz/ Emtricitabine/ rilpivirine/ elvitegravir/ cobicistat/ alafenamide Emtricitabine/
The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines
 The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines I. Boucoiran, T. Lee, K. Tulloch, L. Sauve, L. Samson, J. Brophy, M. Boucher and D. Money For and
The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines I. Boucoiran, T. Lee, K. Tulloch, L. Sauve, L. Samson, J. Brophy, M. Boucher and D. Money For and
COMPREHENSIVE ANTIRETROVIRAL TABLE: ADULT DOSING, DOSAGE FORM MODIFICATIONS, ADVERSE REACTIONS and INTERACTION POTENTIAL
 Generic Name COMPREHENSIVE ANTIRETROVIRAL TABLE: NUCLOESIDE/TIDE REVERSE TRANSCRIPTASE INHIBITORS (N(t)RTIs) Abacavir ABC (Ziagen) Didanosine ddi (Videx EC) Emtricitabine FTC (Emtriva) Lamivudine 3TC (Epivir)
Generic Name COMPREHENSIVE ANTIRETROVIRAL TABLE: NUCLOESIDE/TIDE REVERSE TRANSCRIPTASE INHIBITORS (N(t)RTIs) Abacavir ABC (Ziagen) Didanosine ddi (Videx EC) Emtricitabine FTC (Emtriva) Lamivudine 3TC (Epivir)
THE HIV LIFE CYCLE. Understanding How Antiretroviral Medications Work
 THE HIV LIFE CYCLE Understanding How Antiretroviral Medications Work DEFINITIONS Host: The animal or cell that another organism lives in. In HIV human CD4 T-cells are the host for HIV. Nucleus: The core
THE HIV LIFE CYCLE Understanding How Antiretroviral Medications Work DEFINITIONS Host: The animal or cell that another organism lives in. In HIV human CD4 T-cells are the host for HIV. Nucleus: The core
Comprehensive Guideline Summary
 Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
WOMENS INTERAGENCY HIV STUDY ANTIRETROVIRAL DOSAGE FORM SECTION A. GENERAL INFORMATION
 WOMENS INTERAGENCY HIV STUDY ANTIRETROVIRAL DOSAGE FORM SECTION A. GENERAL INFORMATION A1. PARTICIPANT ID: ENTER NUMBER HERE - - - ONLY IF ID LABEL IS NOT AVAILABLE A2. VISIT #: A3. VERSION DATE: 1 0 /
WOMENS INTERAGENCY HIV STUDY ANTIRETROVIRAL DOSAGE FORM SECTION A. GENERAL INFORMATION A1. PARTICIPANT ID: ENTER NUMBER HERE - - - ONLY IF ID LABEL IS NOT AVAILABLE A2. VISIT #: A3. VERSION DATE: 1 0 /
Selected Issues in HIV Clinical Trials
 Selected Issues in HIV Clinical Trials Judith S. Currier, M.D., MSc Professor of Medicine Division of Infectious Diseases University of California, Los Angeles Issues Evolving Global and Domestic Epidemic
Selected Issues in HIV Clinical Trials Judith S. Currier, M.D., MSc Professor of Medicine Division of Infectious Diseases University of California, Los Angeles Issues Evolving Global and Domestic Epidemic
ART and Prevention: What do we know?
 ART and Prevention: What do we know? Biomedical Issues Trip Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Cornell Medical College New York City ART for Prevention:
ART and Prevention: What do we know? Biomedical Issues Trip Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Cornell Medical College New York City ART for Prevention:
A Fatal Imbalance. Tropical diseases: 18 new drugs (incl. 8 for malaria) 1.3% 21 new drugs for neglected diseases. Tuberculosis: 3 new drugs
 1.3% 21 new drugs for neglected diseases. Tuberculosis: 3 new drugs") ADDRESSING GAPS IN INNOVATION FOR NEGLECTED PATIENTS: DNDI ANDPEDIATRIC HIV/AIDS Rachel Cohen, Regional Executive Director, DNDi North America Proposals for a Global Innovation System that Responds to
ADDRESSING GAPS IN INNOVATION FOR NEGLECTED PATIENTS: DNDI ANDPEDIATRIC HIV/AIDS Rachel Cohen, Regional Executive Director, DNDi North America Proposals for a Global Innovation System that Responds to
Continuing Education for Pharmacy Technicians
 Continuing Education for Pharmacy Technicians HIV/AIDS TREATMENT Michael Denaburg, Pharm.D. Birmingham, AL Objectives: 1. Identify drugs and drug classes currently used in the management of HIV infected
Continuing Education for Pharmacy Technicians HIV/AIDS TREATMENT Michael Denaburg, Pharm.D. Birmingham, AL Objectives: 1. Identify drugs and drug classes currently used in the management of HIV infected
Selected Issues in HIV Clinical Trials
 Selected Issues in HIV Clinical Trials Judith S. Currier, M.D., MSc Professor of Medicine Division of Infectious Diseases University of California, Los Angeles Issues Evolving Global and Domestic Epidemic
Selected Issues in HIV Clinical Trials Judith S. Currier, M.D., MSc Professor of Medicine Division of Infectious Diseases University of California, Los Angeles Issues Evolving Global and Domestic Epidemic
Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV. Ernesto Parra, M.D., M.P.H.
 Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV Ernesto Parra, M.D., M.P.H. Adjunct Associate Professor UTHSCSA Department of Pediatrics and Family and Community
Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV Ernesto Parra, M.D., M.P.H. Adjunct Associate Professor UTHSCSA Department of Pediatrics and Family and Community
HIV Drug Resistance Update 2007
 HIV Drug Resistance Update 27 Harry Lampiris, MD Associate Professor of Clinical Medicine, UCSF Infectious Disease Section Department of Medicine San Francisco VA Medical Center Outline Indications for
HIV Drug Resistance Update 27 Harry Lampiris, MD Associate Professor of Clinical Medicine, UCSF Infectious Disease Section Department of Medicine San Francisco VA Medical Center Outline Indications for
Principles of HIV Drug Resistance: Resistance to New Drug Classes. Mark A Wainberg McGill University AIDS Centre Montreal, Quebec, Canada
 Principles of HIV Drug Resistance: Resistance to New Drug Classes Mark A Wainberg McGill University AIDS Centre Montreal, Quebec, Canada Why Is It Important to Understand HIV Drug Resistance? 1. Resistance
Principles of HIV Drug Resistance: Resistance to New Drug Classes Mark A Wainberg McGill University AIDS Centre Montreal, Quebec, Canada Why Is It Important to Understand HIV Drug Resistance? 1. Resistance
Medscape's Antiretroviral Pocket Guide for the Treatment of HIV Infection
 Table 3. Characteristics of Nucleoside Reverse Transcriptase Inhibitors (NRTIs) Generic Name (Abbreviation) / Trade Name Abacavir (ABC) / Ziagen Trizivir with ZDV + 3TC Epzicom with 3TC Didanosine (ddi)
Table 3. Characteristics of Nucleoside Reverse Transcriptase Inhibitors (NRTIs) Generic Name (Abbreviation) / Trade Name Abacavir (ABC) / Ziagen Trizivir with ZDV + 3TC Epzicom with 3TC Didanosine (ddi)
Antiretroviral Dosing in Renal Impairment
 Protease Inhibitors (PIs) Atazanavir Reyataz hard capsules 300 mg once daily taken with ritonavir 100 mg once daily No dosage adjustment is needed for atazanavir in renal impairment Atazanavir use in haemodialysis
Protease Inhibitors (PIs) Atazanavir Reyataz hard capsules 300 mg once daily taken with ritonavir 100 mg once daily No dosage adjustment is needed for atazanavir in renal impairment Atazanavir use in haemodialysis
ANTIRETROVIRAL TREATMENTS (Part 1of
 CCR5 CO-RECEPTOR ANTAGONISTS maraviroc (MVC) Selzentry 25mg, 75mg, FUSION INHIBITORS 20mg/mL ANTIRETROVIRAL TREATMENTS (Part 1of 5) oral soln enfuvirtide (ENF, T-20) Fuzeon 90mg/mL pwd for SC inj after
CCR5 CO-RECEPTOR ANTAGONISTS maraviroc (MVC) Selzentry 25mg, 75mg, FUSION INHIBITORS 20mg/mL ANTIRETROVIRAL TREATMENTS (Part 1of 5) oral soln enfuvirtide (ENF, T-20) Fuzeon 90mg/mL pwd for SC inj after
COMPREHENSIVE ANTIRETROVIRAL TABLE: ADULT DOSING**, DOSAGE FORM MODIFICATIONS, ADVERSE REACTIONS and INTERACTION POTENTIAL
 COMPREHENSIVE ANTIRETROVIRAL TABLE: NUCLOESIDE/TIDE REVERSE TRANSCRIPTASE INHIBITORS (N(t)RTIs) Abacavir ABC (Ziagen) Didanosine ddi (Videx EC) Emtricitabine FTC (Emtriva) Lamivudine 3TC (Epivir) Stavudine
COMPREHENSIVE ANTIRETROVIRAL TABLE: NUCLOESIDE/TIDE REVERSE TRANSCRIPTASE INHIBITORS (N(t)RTIs) Abacavir ABC (Ziagen) Didanosine ddi (Videx EC) Emtricitabine FTC (Emtriva) Lamivudine 3TC (Epivir) Stavudine
Human Immunodeficiency Virus (HIV) and Acquired Immune Deficiency Syndrome (AIDS) in the Long Term Care Setting Part 2: HIV Medications
 and Acquired Immune Deficiency Syndrome (AIDS) in the Long Term Care Setting Part 2: HIV Medications") Human Immunodeficiency Virus (HIV) and Acquired Immune Deficiency Syndrome (AIDS) in the Long Term Care Setting Part 2: HIV Medications Carrie Allen PharmD, CGP, BCPS, BCPP, CCHP Overview - Part 2: HIV
Human Immunodeficiency Virus (HIV) and Acquired Immune Deficiency Syndrome (AIDS) in the Long Term Care Setting Part 2: HIV Medications Carrie Allen PharmD, CGP, BCPS, BCPP, CCHP Overview - Part 2: HIV
Pharmacological considerations on the use of ARVs in pregnancy
 Pharmacological considerations on the use of ARVs in pregnancy 11 th Residential Course on Clinical Pharmacology of Antiretrovirals Torino, 20-22 January 2016 Prof. David Burger, PharmD, PhD david.burger@radboudumc.nl
Pharmacological considerations on the use of ARVs in pregnancy 11 th Residential Course on Clinical Pharmacology of Antiretrovirals Torino, 20-22 January 2016 Prof. David Burger, PharmD, PhD david.burger@radboudumc.nl
Criteria for Oral PrEP
 Oral PrEP New Drugs Roy M. Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Medical College of Cornell University New York City Safe Criteria for Oral PrEP Penetrates
Oral PrEP New Drugs Roy M. Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Medical College of Cornell University New York City Safe Criteria for Oral PrEP Penetrates
Switching ARV Regimens: Managing Toxicity and Improving Tolerability; Switches & Class-Sparing Approaches
 Switching ARV Regimens: Managing Toxicity and Improving Tolerability; Switches & Class-Sparing Approaches Harry W. Lampiris, MD Chief, Infectious Disease Section, San Francisco VA Medical Center Professor
Switching ARV Regimens: Managing Toxicity and Improving Tolerability; Switches & Class-Sparing Approaches Harry W. Lampiris, MD Chief, Infectious Disease Section, San Francisco VA Medical Center Professor
Antiretroviral Therapy
 Antiretroviral Therapy Scott M. Hammer, M.D. 1986 1990 ZDV monorx 1990 1995 Alternative NRTI monorx Combination NRTI Rx Introduction of NNRTI s Antiretroviral resistance Pathogenetic concepts Evolution
Antiretroviral Therapy Scott M. Hammer, M.D. 1986 1990 ZDV monorx 1990 1995 Alternative NRTI monorx Combination NRTI Rx Introduction of NNRTI s Antiretroviral resistance Pathogenetic concepts Evolution
HIV in in Women Women
 HIV in Women Susan L. Koletar, MD The Ohio State University How Many of These Women Have HIV? Answer: I don t really know Google Search: Photos of Groups of Women Pub Med Search: HIV and Women 22,732
HIV in Women Susan L. Koletar, MD The Ohio State University How Many of These Women Have HIV? Answer: I don t really know Google Search: Photos of Groups of Women Pub Med Search: HIV and Women 22,732
2 nd Line Treatment and Resistance. Dr Rohit Talwani & Dr Dave Riedel 12 th June 2012
 2 nd Line Treatment and Resistance Dr Rohit Talwani & Dr Dave Riedel 12 th June 2012 Overview Basics of Resistance Treatment failure Strategies to manage treatment failure Mutation Definition: A change
2 nd Line Treatment and Resistance Dr Rohit Talwani & Dr Dave Riedel 12 th June 2012 Overview Basics of Resistance Treatment failure Strategies to manage treatment failure Mutation Definition: A change
Addressing Pediatric Needs of the Most Neglected: next steps
 Addressing Pediatric Needs of the Most Neglected: next steps An updated overview of DNDi Pediatric Focus Nathalie Strub Wourgaft (Medical Director) Janice Lee (HIV Pediatric Clinical Manager) A Fatal Imbalance
Addressing Pediatric Needs of the Most Neglected: next steps An updated overview of DNDi Pediatric Focus Nathalie Strub Wourgaft (Medical Director) Janice Lee (HIV Pediatric Clinical Manager) A Fatal Imbalance
WOMEN'S INTERAGENCY HIV STUDY METABOLIC STUDY: MS01 SPECIMEN COLLECTION FORM
 WOMEN'S INTERAGENCY HIV STUDY METABOLIC STUDY: MS01 SPECIMEN COLLECTION FORM ID LABEL HERE ---> VERSION DATE 10/01/07 - - - VISIT #: FORM COMPLETED BY: A1. DATE OF BLOOD DRAW: / / M D Y A2. Do you take
WOMEN'S INTERAGENCY HIV STUDY METABOLIC STUDY: MS01 SPECIMEN COLLECTION FORM ID LABEL HERE ---> VERSION DATE 10/01/07 - - - VISIT #: FORM COMPLETED BY: A1. DATE OF BLOOD DRAW: / / M D Y A2. Do you take
HIV Integrase Inhibitors: Current and Future Use. Douglas G. Fish, MD Albany Medical College Cali, Colombia March 13, 2008
 HIV Integrase Inhibitors: Current and Future Use Douglas G. Fish, MD Albany Medical College Cali, Colombia March 13, 2008 Which of the following statements about raltegravir is false? a) Raltegravir is
HIV Integrase Inhibitors: Current and Future Use Douglas G. Fish, MD Albany Medical College Cali, Colombia March 13, 2008 Which of the following statements about raltegravir is false? a) Raltegravir is
History (August 2010) Therapy for Experienced Patients. History (September 2010) History (November 2010) 12/2/11
 Therapy for Experienced Patients. History (September 2010) History (November 2010) 12/2/11") (August 2010) Therapy for Experienced Patients Hiroyu Hatano, MD, MHS Assistant Professor of Medicine University of California San Francisco Medical Management of AIDS December 2011 42M HIV (CD4=450, VL=6250,
(August 2010) Therapy for Experienced Patients Hiroyu Hatano, MD, MHS Assistant Professor of Medicine University of California San Francisco Medical Management of AIDS December 2011 42M HIV (CD4=450, VL=6250,
HIV medications HIV medication and schedule plan
 Living with HIV (human immunodeficiency virus) It may be scary to find out that you re HIV-positive or have AIDS. Coping with this news may be difficult. Although HIV is a serious infection, people with
Living with HIV (human immunodeficiency virus) It may be scary to find out that you re HIV-positive or have AIDS. Coping with this news may be difficult. Although HIV is a serious infection, people with
ART: The New, The Old and The Ugly
 ART: The New, The Old and The Ugly Our Current ARVS The Nucleoside/ Nucleotide Reverse Transcriptase Inhibitors (NRTIs/ NtRTIs) Abacavir Emtricitabine Lamivudine Stavudine Tenofovir Zidovudine The Non-Nucleoside
ART: The New, The Old and The Ugly Our Current ARVS The Nucleoside/ Nucleotide Reverse Transcriptase Inhibitors (NRTIs/ NtRTIs) Abacavir Emtricitabine Lamivudine Stavudine Tenofovir Zidovudine The Non-Nucleoside
Approach for the Newly Diagnosed HIV Positive Patient
 Approach for the Newly Diagnosed HIV Positive Patient Jason E. Farley, PhD, MPH, ANP-BC, FAAN, AACRN Associate Professor & NP, Johns Hopkins University School of Nursing & Medicine Director, AETC Adult-Gerontology
Approach for the Newly Diagnosed HIV Positive Patient Jason E. Farley, PhD, MPH, ANP-BC, FAAN, AACRN Associate Professor & NP, Johns Hopkins University School of Nursing & Medicine Director, AETC Adult-Gerontology
Genotyping and Drug Resistance in Clinical Practice. Case Studies
 Genotyping and Drug Resistance in Clinical Practice Case Studies 12/02 40 year old Hispanic male Dx with HIV 1995 + Hx of PCP > 1x, HepC Medication history: AZT, Crixivan, Videx EC, Sustiva, Zerit, Ziagen,
Genotyping and Drug Resistance in Clinical Practice Case Studies 12/02 40 year old Hispanic male Dx with HIV 1995 + Hx of PCP > 1x, HepC Medication history: AZT, Crixivan, Videx EC, Sustiva, Zerit, Ziagen,
Susan L. Koletar, MD
 HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
Kiat Ruxrungtham. Professor of Medicine Chulalongkorn University, and HIV-NAT, Thai Red Cross AIDS Research Centre
 Kiat Ruxrungtham Professor of Medicine Chulalongkorn University, and HIV-NAT, Thai Red Cross AIDS Research Centre www.iasusa.org; www.aidsinfo.nih.gov; www.clinicaloptions.com; www.clinicaloptions.com/hiv
Kiat Ruxrungtham Professor of Medicine Chulalongkorn University, and HIV-NAT, Thai Red Cross AIDS Research Centre www.iasusa.org; www.aidsinfo.nih.gov; www.clinicaloptions.com; www.clinicaloptions.com/hiv
Somnuek Sungkanuparph, M.D.
 HIV Drug Resistance Somnuek Sungkanuparph, M.D. Associate Professor Division of Infectious Diseases Department of Medicine Faculty of Medicine Ramathibodi Hospital Mahidol University Adjunct Professor
HIV Drug Resistance Somnuek Sungkanuparph, M.D. Associate Professor Division of Infectious Diseases Department of Medicine Faculty of Medicine Ramathibodi Hospital Mahidol University Adjunct Professor
Management of patients with antiretroviral treatment failure: guidelines comparison
 The editorial staff Management of patients with antiretroviral treatment failure: guidelines comparison A change of therapy should be considered for patients if they experience sustained rebound in viral
The editorial staff Management of patients with antiretroviral treatment failure: guidelines comparison A change of therapy should be considered for patients if they experience sustained rebound in viral
HIV THERAPY STRATEGIES FOR THIRD LINE. issues to consider when faced with few drug options
 STRATEGIES FOR THIRD LINE HIV THERAPY issues to consider when faced with few drug options A PUBLICATION FROM Information, Inspiration and Advocacy for People Living With HIV/AIDS MAY 2008 Most people living
STRATEGIES FOR THIRD LINE HIV THERAPY issues to consider when faced with few drug options A PUBLICATION FROM Information, Inspiration and Advocacy for People Living With HIV/AIDS MAY 2008 Most people living
MDR HIV and Total Therapeutic Failure. Douglas G. Fish, MD Albany Medical College Albany, New York Cali, Colombia March 30, 2007
 MDR HIV and Total Therapeutic Failure Douglas G. Fish, MD Albany Medical College Albany, New York Cali, Colombia March 30, 2007 Objectives Case study Definitions Fitness Pathogenesis of resistant virus
MDR HIV and Total Therapeutic Failure Douglas G. Fish, MD Albany Medical College Albany, New York Cali, Colombia March 30, 2007 Objectives Case study Definitions Fitness Pathogenesis of resistant virus
HIV Treatment: State of the Art 2013
 HIV Treatment: State of the Art 2013 Daniel R. Kuritzkes, MD Chief, Division of Infectious Diseases Brigham and Women s Hospital Professor of Medicine Harvard Medical School Success of current ART Substantial
HIV Treatment: State of the Art 2013 Daniel R. Kuritzkes, MD Chief, Division of Infectious Diseases Brigham and Women s Hospital Professor of Medicine Harvard Medical School Success of current ART Substantial
Friday afternoon Programme
 Friday afternoon Programme Pharmacology and TDM Dr Marta Boffito Consultant Physician, C&W Resistance to new anti-retrovirals Dr Steve Taylor Consultant Physician, Birmingham HIVPA Annual Conference 2008
Friday afternoon Programme Pharmacology and TDM Dr Marta Boffito Consultant Physician, C&W Resistance to new anti-retrovirals Dr Steve Taylor Consultant Physician, Birmingham HIVPA Annual Conference 2008
Treatment strategies for the developing world
 David A Cooper National Centre in HIV Epidemiology and Clinical Research The University of New South Wales Sydney, Australia First line standard of care First line in the developing world First line failure
David A Cooper National Centre in HIV Epidemiology and Clinical Research The University of New South Wales Sydney, Australia First line standard of care First line in the developing world First line failure
When to Start ART. Reduction in HIV transmission. ? Reduction in HIV-associated inflammation and associated complications» i.e. CV disease, neuro, etc
 When to Start ART Exact CD4 count at which to initiate therapy not known, but evidence points to starting at higher counts Current recommendation: ART for all patients with CD4 count of
When to Start ART Exact CD4 count at which to initiate therapy not known, but evidence points to starting at higher counts Current recommendation: ART for all patients with CD4 count of
New Frontiers for Treatment Strategies for HIV Care
 New Frontiers for Treatment Strategies for HIV Care Eric S. Daar, MD Chief, Division of HIV Medicine Harbor-UCLA Medical Center Professor of Medicine David Geffen School of Medicine at UCLA Disclosures:
New Frontiers for Treatment Strategies for HIV Care Eric S. Daar, MD Chief, Division of HIV Medicine Harbor-UCLA Medical Center Professor of Medicine David Geffen School of Medicine at UCLA Disclosures:
0.14 ( 0.053%) UNAIDS 10% (94) ( ) (73-94/6 ) 8,920
 UNAIDS 10% (94) ( ) (73-94/6 ) 8,920") 0.14 UNAIDS 0.053% 2 250 60 10% 94 73 20 73-94/6 8,920 12 43 Public Health Service Task Force Recommendations 5-10% for Use of Antiretroviral Drugs in 10-20% Pregnant HIV-1-Infected Women for Maternal
0.14 UNAIDS 0.053% 2 250 60 10% 94 73 20 73-94/6 8,920 12 43 Public Health Service Task Force Recommendations 5-10% for Use of Antiretroviral Drugs in 10-20% Pregnant HIV-1-Infected Women for Maternal
JULUCA (dolutegravir sodium-rilpivirine hydrochloride) oral tablet
 oral tablet") JULUCA (dolutegravir sodium-rilpivirine hydrochloride) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
JULUCA (dolutegravir sodium-rilpivirine hydrochloride) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
BHIVA Best of CROI Feedback Meetings. London Birmingham North West England Cardiff Gateshead Edinburgh
 BHIVA Best of CROI Feedback Meetings London Birmingham North West England Cardiff Gateshead Edinburgh BHIVA Best of CROI Feedback Meetings 2010 ANTIRETROVIRAL TREATMENT STRATEGIES AND NEW DRUGS A5202:
BHIVA Best of CROI Feedback Meetings London Birmingham North West England Cardiff Gateshead Edinburgh BHIVA Best of CROI Feedback Meetings 2010 ANTIRETROVIRAL TREATMENT STRATEGIES AND NEW DRUGS A5202:
30 Years of HIV: An Update on Treatment Guidelines and Beyond
 8/3/212 Conflict of Interest Declaration 3 Years of HIV: An Update on Treatment Guidelines and Beyond Blake Max, PharmD, AAHIVE Clinical Associate Professor University of Illinois at Chicago College of
8/3/212 Conflict of Interest Declaration 3 Years of HIV: An Update on Treatment Guidelines and Beyond Blake Max, PharmD, AAHIVE Clinical Associate Professor University of Illinois at Chicago College of
/AIDS HIV/ HIV Overview. Nelson L. Michael, MD, PhD Division of Retrovirology Walter Reed Army Institute of Research US Military HIV Research Program
 /AIDS HIV/ HIV Overview Nelson L. Michael, MD, PhD Division of Retrovirology Walter Reed Army Institute of Research US Military HIV Research Program www.hivresearch.org 1 WRAIR Tropical Medicine Course
/AIDS HIV/ HIV Overview Nelson L. Michael, MD, PhD Division of Retrovirology Walter Reed Army Institute of Research US Military HIV Research Program www.hivresearch.org 1 WRAIR Tropical Medicine Course
Virological suppression and PIs. Diego Ripamonti Malattie Infettive - Bergamo
 Virological suppression and PIs Diego Ripamonti Malattie Infettive - Bergamo Ritonavir-boosted PIs Boosted PIs: 3 drugs in one The intrinsic antiretroviral activity Viral suppression and high baseline
Virological suppression and PIs Diego Ripamonti Malattie Infettive - Bergamo Ritonavir-boosted PIs Boosted PIs: 3 drugs in one The intrinsic antiretroviral activity Viral suppression and high baseline
Quick Reference Guide to Antiretrovirals. Guide to Antiretroviral Agents
 Author: Malte Schütz, MD June 1, 2002 Quick Reference Guide to Antiretrovirals Regular updates to this publication are posted on the Medscape Web site at http://hiv.medscape.com/updates/quickguide. Please
Author: Malte Schütz, MD June 1, 2002 Quick Reference Guide to Antiretrovirals Regular updates to this publication are posted on the Medscape Web site at http://hiv.medscape.com/updates/quickguide. Please
The Use of Resistance Testing in HIV
 The Use of Resistance Testing in HIV Dushyantha Jayaweera, M.D., M.R.C.O.G., F.A.C.P. Professor in Clinical Medicine Division of Infectious Diseases University of Miami Miller School of Medicine Viral
The Use of Resistance Testing in HIV Dushyantha Jayaweera, M.D., M.R.C.O.G., F.A.C.P. Professor in Clinical Medicine Division of Infectious Diseases University of Miami Miller School of Medicine Viral
Susan L. Koletar, MD
 HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
The ART of Managing Drug-Drug Interactions in Patients with HIV
 The ART of Managing Drug-Drug Interactions in Patients with HIV Bradley L. Smith, Pharm.D. smith.bradley1@mayo.edu Pharmacy Grand Rounds December 19, 2017 2017 MFMER slide-1 Presentation Objectives Describe
The ART of Managing Drug-Drug Interactions in Patients with HIV Bradley L. Smith, Pharm.D. smith.bradley1@mayo.edu Pharmacy Grand Rounds December 19, 2017 2017 MFMER slide-1 Presentation Objectives Describe
Update on HIV Drug Resistance. Daniel R. Kuritzkes, MD Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School
 Update on HIV Drug Resistance Daniel R. Kuritzkes, MD Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School Learning Objectives Upon completion of this presentation, learners
Update on HIV Drug Resistance Daniel R. Kuritzkes, MD Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School Learning Objectives Upon completion of this presentation, learners
Antiretrovial Crushable/Liquid Formulation Chart
 Antiretrovial Crushable/Liquid Formulation Chart Eliza Dollard, PharmD; Nafeesa Chin-Beckford, PharmD; Laura Aragon, PharmD Last Updated: 04/2016 Agent How Supplied Crushable Status **Products listed in
Antiretrovial Crushable/Liquid Formulation Chart Eliza Dollard, PharmD; Nafeesa Chin-Beckford, PharmD; Laura Aragon, PharmD Last Updated: 04/2016 Agent How Supplied Crushable Status **Products listed in
Optimizing the treatment
 PIs are the real world answer for: Optimizing the treatment Sergio Lo Caputo Malattie Infettive - Azienda Sanitaria Firenze Evolution of ARVs DARUNAVIR PI ETRAVIRINA NNRTI DOLUTEGRAVIR INI POTENZA E ALTA
PIs are the real world answer for: Optimizing the treatment Sergio Lo Caputo Malattie Infettive - Azienda Sanitaria Firenze Evolution of ARVs DARUNAVIR PI ETRAVIRINA NNRTI DOLUTEGRAVIR INI POTENZA E ALTA
Pharmacology Update Alice Tseng, Pharm.D., FCSHP Vancouver May 11, 2005
 Pharmacology Update 2005 Alice Tseng, Pharm.D., FCSHP Vancouver May 11, 2005 I m having a Maalox moment!!! Gastric Hypoacidity in HIV 20% incidence in HIV (unrelated to CD 4 ) Antacids, ddi tablets, H2-blockers
Pharmacology Update 2005 Alice Tseng, Pharm.D., FCSHP Vancouver May 11, 2005 I m having a Maalox moment!!! Gastric Hypoacidity in HIV 20% incidence in HIV (unrelated to CD 4 ) Antacids, ddi tablets, H2-blockers
Overview of HIV WRAIR- GEIS 'Operational Clinical Infectious Disease' Course
 Overview of HIV WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED Acknowledgments - Dr. Christina Polyak - Dr. Julie Ake Disclaimer The views expressed in this presentation are
Overview of HIV WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED Acknowledgments - Dr. Christina Polyak - Dr. Julie Ake Disclaimer The views expressed in this presentation are
HIV Overview. Mary Marovich, MD, DTMH Division of Retrovirology Walter Reed Army Ins?tute of Research US Military HIV Research Program
 HIV Overview Mary Marovich, MD, DTMH Division of Retrovirology Walter Reed Army Ins?tute of Research US Military HIV Research Program www.hivresearch.org 1 Outline HIV Virology, Transmission, and Pathogenesis
HIV Overview Mary Marovich, MD, DTMH Division of Retrovirology Walter Reed Army Ins?tute of Research US Military HIV Research Program www.hivresearch.org 1 Outline HIV Virology, Transmission, and Pathogenesis
Overview of HIV. LTC Paige Waterman
 Overview of HIV LTC Paige Waterman Outline Background and Epidemiology HIV Virology, Transmission, and Pathogenesis Acute HIV infection HIV Diagnostics Management of Health Care Personnel Exposed to HIV
Overview of HIV LTC Paige Waterman Outline Background and Epidemiology HIV Virology, Transmission, and Pathogenesis Acute HIV infection HIV Diagnostics Management of Health Care Personnel Exposed to HIV
SELECTING THE BEST ART FOR EACH PATIENT
 SELECTING THE BEST ART FOR EACH PATIENT Corklin R Steinhart, MD, PhD Head, Global Medical Directors ViiV Healthcare CNVX/HIVP/0025/16 5th Asian Conference on Hepatitis & AIDS 第五届亚洲肝炎与艾滋病学术会议 28-29 May
SELECTING THE BEST ART FOR EACH PATIENT Corklin R Steinhart, MD, PhD Head, Global Medical Directors ViiV Healthcare CNVX/HIVP/0025/16 5th Asian Conference on Hepatitis & AIDS 第五届亚洲肝炎与艾滋病学术会议 28-29 May
Second and third line paediatric ART strategies
 Second and third line paediatric ART strategies Dr. Marape Marape Assistant Professor Ohio University School of Health Professions Gaborone, Botswana Marape Marape MB, BCh, BAO, MPH, PhD Assistant Professor
Second and third line paediatric ART strategies Dr. Marape Marape Assistant Professor Ohio University School of Health Professions Gaborone, Botswana Marape Marape MB, BCh, BAO, MPH, PhD Assistant Professor
Update on Antiretroviral Treatment for HIV Infection 2008
 Update on Antiretroviral Treatment for HIV Infection 2008 Janet Gilmour MD FRCP(C) Clinical Associate Professor of Medicine University of Calgary November 2008 Disclosure and Acknowledgements Disclosure:
Update on Antiretroviral Treatment for HIV Infection 2008 Janet Gilmour MD FRCP(C) Clinical Associate Professor of Medicine University of Calgary November 2008 Disclosure and Acknowledgements Disclosure:
Resistance Workshop. 3rd European HIV Drug
 3rd European HIV Drug Resistance Workshop March 30-April 1 st, 2005 Christine Hughes, PharmD Clinical Associate Professor Faculty of Pharmacy & Pharmaceutical Sciences University of Alberta Tenofovir resistance
3rd European HIV Drug Resistance Workshop March 30-April 1 st, 2005 Christine Hughes, PharmD Clinical Associate Professor Faculty of Pharmacy & Pharmaceutical Sciences University of Alberta Tenofovir resistance
Antiretroviral Treatment Strategies: Clinical Case Presentation
 Antiretroviral Treatment Strategies: Clinical Case Presentation Department of Internal Medicine, Far Eastern Memorial Hospital, New Taipei City, Taiwan Chia-Jui, Yang M.D Disclosure No conflicts of interests.
Antiretroviral Treatment Strategies: Clinical Case Presentation Department of Internal Medicine, Far Eastern Memorial Hospital, New Taipei City, Taiwan Chia-Jui, Yang M.D Disclosure No conflicts of interests.
Case # 1. Case #1 (cont d)
") Antiretroviral Therapy Management: Expert Panel Discussion George Beatty Susa Coffey Steve O Brien December 3, 2011 Moderated by Annie Luetkemeyer Case # 1 38 y.o. man, CD4 =350, VL=340K, new to your clinic
Antiretroviral Therapy Management: Expert Panel Discussion George Beatty Susa Coffey Steve O Brien December 3, 2011 Moderated by Annie Luetkemeyer Case # 1 38 y.o. man, CD4 =350, VL=340K, new to your clinic
 Page 1 of 5 ENLGLISH / ESPAÑOL / PORTUGUÉS / FRANÇAIS Share 3 Drug Chart for HIV Treatment CURRENT EDITION ABOUT SENSE BACK ISSUES MSMGF HOME CONTACT US There are a number of antiretroviral (ARV) medications
Page 1 of 5 ENLGLISH / ESPAÑOL / PORTUGUÉS / FRANÇAIS Share 3 Drug Chart for HIV Treatment CURRENT EDITION ABOUT SENSE BACK ISSUES MSMGF HOME CONTACT US There are a number of antiretroviral (ARV) medications
Selecting an Initial Antiretroviral Therapy (ART) Regimen
 Regimen") Selecting an Initial Antiretroviral Therapy (ART) Regimen An HIV Diagnosis is a Call to Action In support of the NYSDOH AIDS Institute s January 2018 call to action for patients newly diagnosed with HIV,
Selecting an Initial Antiretroviral Therapy (ART) Regimen An HIV Diagnosis is a Call to Action In support of the NYSDOH AIDS Institute s January 2018 call to action for patients newly diagnosed with HIV,
HIV - Therapy Principles
 HIV - Therapy Principles Manuel Battegay and Christine Katlama Basel, Switzerland and Paris, France Disclosure MB has received honoraria for advisory board participation from Gilead, MSD, Pfizer, ViiV
HIV - Therapy Principles Manuel Battegay and Christine Katlama Basel, Switzerland and Paris, France Disclosure MB has received honoraria for advisory board participation from Gilead, MSD, Pfizer, ViiV
Disclosures. Update on HIV Drug Therapy: A Case based Discussion. Case # 1: Dr. Grant has received grant support from BMS, Gilead, Janssen, and Viiv
 Disclosures Update on HIV Drug Therapy: A Case based Discussion Dr. Grant has received grant support from BMS, Gilead, Janssen, and Viiv Philip Grant Assistant Professor Division of Infectious Diseases
Disclosures Update on HIV Drug Therapy: A Case based Discussion Dr. Grant has received grant support from BMS, Gilead, Janssen, and Viiv Philip Grant Assistant Professor Division of Infectious Diseases
Approach to a Patient Newly Diagnosed with HIV, Including ART Basics Rajesh T. Gandhi, M.D.
 Approach to a Patient Newly Diagnosed with HIV, Including ART Basics Rajesh T. Gandhi, M.D. Disclosures: grant support from Gilead, Roche, EBSCO Objectives Apply current guidelines to initial evaluation
Approach to a Patient Newly Diagnosed with HIV, Including ART Basics Rajesh T. Gandhi, M.D. Disclosures: grant support from Gilead, Roche, EBSCO Objectives Apply current guidelines to initial evaluation
Supplementary information
 Supplementary information Dose-response Curve Slope Sets Class-Specific Limits on Inhibitory Potential of Anti-HIV Drugs Lin Shen 1,2, Susan Peterson 1, Ahmad R. Sedaghat 1, Moira A. McMahon 1,2, Marc
Supplementary information Dose-response Curve Slope Sets Class-Specific Limits on Inhibitory Potential of Anti-HIV Drugs Lin Shen 1,2, Susan Peterson 1, Ahmad R. Sedaghat 1, Moira A. McMahon 1,2, Marc
When to start, when to switch ART and monitoring of ARV side effects
 When to start, when to switch ART and monitoring of ARV side effects Thanomsak Anekthananon, MD Faculty of Medicine Siriraj Hospital September 4, 2009 Recommended Websites Free e-book: HIV Medicine 2007
When to start, when to switch ART and monitoring of ARV side effects Thanomsak Anekthananon, MD Faculty of Medicine Siriraj Hospital September 4, 2009 Recommended Websites Free e-book: HIV Medicine 2007
Update on HIV-1 Drug Resistance and Tropism Testing
 Update on HIV-1 Drug Resistance and Tropism Testing Daniel R. Kuritzkes, MD Section of Retroviral Therapeutics Brigham and Women s Hospital Harvard Medical School ACTHIV 2011: A State-of-the-Science Conference
Update on HIV-1 Drug Resistance and Tropism Testing Daniel R. Kuritzkes, MD Section of Retroviral Therapeutics Brigham and Women s Hospital Harvard Medical School ACTHIV 2011: A State-of-the-Science Conference
Crafting an ART Regimen for Initiation or Salvage: Are NRTI s Necessary?
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Crafting an ART Regimen for Initiation or Salvage: Are NRTI s Necessary? Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Crafting an ART Regimen for Initiation or Salvage: Are NRTI s Necessary? Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical
Objectives. HIV Treatment in Recently In 1996 the introduction of protease inhibitors decreasing the death rate of those infected by 50%.
 Objectives Identify modes HIV transmission and methods of prevention. HIV Treatment in 2010 Lisa D. Inge, Pharm.D., BCPS, AAHIVE Assistant Director, Jacksonville Campus Clinical Assistant Professor University
Objectives Identify modes HIV transmission and methods of prevention. HIV Treatment in 2010 Lisa D. Inge, Pharm.D., BCPS, AAHIVE Assistant Director, Jacksonville Campus Clinical Assistant Professor University
HIV for the Non-ID Pharmacist
 Disclosures HIV for the Non-ID Pharmacist I have nothing to disclose at this time Carmen Faulkner-Fennell, PharmD, BCPS (AQ-ID) Clinical Pharmacy Specialist--Infectious Diseases Greenville Hospital System
Disclosures HIV for the Non-ID Pharmacist I have nothing to disclose at this time Carmen Faulkner-Fennell, PharmD, BCPS (AQ-ID) Clinical Pharmacy Specialist--Infectious Diseases Greenville Hospital System
Didactic Series. Update: 2012 HIV Treatment Guidelines. Daniel Lee, MD August 30, 2012
 Didactic Series Update: 2012 HIV Treatment Guidelines Daniel Lee, MD August 30, 2012 ACCREDITATION STATEMENT: University of California, San Diego School of Medicine is accredited by the Accreditation Council
Didactic Series Update: 2012 HIV Treatment Guidelines Daniel Lee, MD August 30, 2012 ACCREDITATION STATEMENT: University of California, San Diego School of Medicine is accredited by the Accreditation Council
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 3 November 2010
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 3 November 2010 ISENTRESS 400 mg, film-coated tablet B/60 (CIP code: 383 084-8) Applicant: MSD-CHIBRET raltegravir
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 3 November 2010 ISENTRESS 400 mg, film-coated tablet B/60 (CIP code: 383 084-8) Applicant: MSD-CHIBRET raltegravir
Are the current doses of ARV correct. Richard Elion MD Associate Adjunct Clinical Professor of Medicine Johns Hopkins School of Medicine
 Are the current doses of ARV correct Richard Elion MD Associate Adjunct Clinical Professor of Medicine Johns Hopkins School of Medicine Can we lower doses of HIV meds safely? Consensus Panel in Alexandria
Are the current doses of ARV correct Richard Elion MD Associate Adjunct Clinical Professor of Medicine Johns Hopkins School of Medicine Can we lower doses of HIV meds safely? Consensus Panel in Alexandria
VIKING STUDIES Efficacy and safety of dolutegravir in treatment-experienced subjects
 VIKING STUDIES Efficacy and safety of dolutegravir in treatment-experienced subjects IL/DLG/0040/14 June 2014 GSK (Israel) Ltd. Basel 25, Petach Tikva. Tel-03-9297100 Medical information service: il.medinfo@gsk.com
VIKING STUDIES Efficacy and safety of dolutegravir in treatment-experienced subjects IL/DLG/0040/14 June 2014 GSK (Israel) Ltd. Basel 25, Petach Tikva. Tel-03-9297100 Medical information service: il.medinfo@gsk.com
Antiretroviral Therapy: New Drugs, New Formulations, New Ideas, New Strategies
 Antiretroviral Therapy: ew Drugs, ew Formulations, ew Ideas, ew Strategies Prof. Ian Sanne Director Clinical HIV Research Unit University of the Witwatersrand and Managing Director Right to Care Why We
Antiretroviral Therapy: ew Drugs, ew Formulations, ew Ideas, ew Strategies Prof. Ian Sanne Director Clinical HIV Research Unit University of the Witwatersrand and Managing Director Right to Care Why We
What are the most promising opportunities for dose optimisation?
 What are the most promising opportunities for dose optimisation? Andrew Hill Liverpool University, UK Global Financial Crisis How can we afford to treat 15-30 million people with HIV in the future? Lowering
What are the most promising opportunities for dose optimisation? Andrew Hill Liverpool University, UK Global Financial Crisis How can we afford to treat 15-30 million people with HIV in the future? Lowering
HIV Update. Divya Ahuja, MD Associate Professor of Medicine University of South Carolina School of Medicine
 HIV Update Divya Ahuja, MD Associate Professor of Medicine University of South Carolina School of Medicine Rates of Diagnoses of HIV Infection among Adults and Adolescents, 2012 United States and 6 Dependent
HIV Update Divya Ahuja, MD Associate Professor of Medicine University of South Carolina School of Medicine Rates of Diagnoses of HIV Infection among Adults and Adolescents, 2012 United States and 6 Dependent
12th European AIDS Conference / EACS ARV Therapies and Therapeutic Strategies A CME Newsletter
 EACS 2009 11-14, November 2009 Cologne, Germany Course Director Jürgen K. Rockstroh, MD Co-Chairman, 12th European AIDS Conference Professor, University of Bonn Bonn, Germany Faculty Calvin Cohen, MD,
EACS 2009 11-14, November 2009 Cologne, Germany Course Director Jürgen K. Rockstroh, MD Co-Chairman, 12th European AIDS Conference Professor, University of Bonn Bonn, Germany Faculty Calvin Cohen, MD,
Simplifying HIV Treatment Now and in the Future
 Simplifying HIV Treatment Now and in the Future David M. Hachey, Pharm.D., AAHIVP Professor Idaho State University Department of Family Medicine Nothing Disclosure 1 Objectives List current first line
Simplifying HIV Treatment Now and in the Future David M. Hachey, Pharm.D., AAHIVP Professor Idaho State University Department of Family Medicine Nothing Disclosure 1 Objectives List current first line
Nothing to disclose.
 Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital HIV UPDATE FOR THE PRIMARY CARE PROVIDER Nothing to disclose. 1 Outline Epidemiology Screening / testing for HIV
Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital HIV UPDATE FOR THE PRIMARY CARE PROVIDER Nothing to disclose. 1 Outline Epidemiology Screening / testing for HIV
Antiretroviral Pregnancy Registry
 Preterm Birth, low birth weight and fetal antiretroviral exposure: Estimated gestational age and birth weight data from singleton live births, 1989 through 31 January 2009 K. Beckerman, J. Albano, M. Martinez-Tristani,
Preterm Birth, low birth weight and fetal antiretroviral exposure: Estimated gestational age and birth weight data from singleton live births, 1989 through 31 January 2009 K. Beckerman, J. Albano, M. Martinez-Tristani,
Didactic Series. Switching Regimens in the Setting of Virologic Suppression
 Didactic Series Switching Regimens in the Setting of Virologic Suppression Craig Ballard, PharmD, AAHIVP UC San Diego Health Owen Clinic June 14 th, 2018 1 Learning Objectives 1) Describe DHHS guidelines
Didactic Series Switching Regimens in the Setting of Virologic Suppression Craig Ballard, PharmD, AAHIVP UC San Diego Health Owen Clinic June 14 th, 2018 1 Learning Objectives 1) Describe DHHS guidelines
HIV Treatment Update. Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University
 HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start