TB Intensive San Antonio, Texas
|
|
|
- Jennifer Chambers
- 5 years ago
- Views:
Transcription
1 TB Intensive San Antonio, Texas November 29-December 2, 2011 Pediatric TB Andrea Cruz, MD, MPH December 2, 2011 Andrea Cruz, MD, MPH has the following disclosures to make: No conflict of interests No relevant financial relationships with any commercial companies pertaining to this educational activity 1
2 An Introduction to Childhood Tuberculosis Andrea T. Cruz, MD/MPH Assistant Professor of Sections of Emergency Medicine & Infectious Disease Objectives To understand the definitions we use for childhood TB To know the common clinical and radiographic manifestations of childhood TB To understand the utility and limitations of available TB diagnostics To map out a plan of care (and know how to get help) for children with TB exposure, infection, and disease Page 3 2


3 Population Distribution World map showing territory size as a proportion of the world s population Page 4 Geography of TB World map showing territory size as a proportion of the world s TB cases found there Page 5 3



4 Famous People with TB JFK* Bronte (x3) Eleanor Roosevelt Fyodor Dostoyevsky Henry David Thoreau Nelson Mandela Ralph Waldo Emerson Simon Bolivar Franz Kafka King Tut John Keats *: possibly Edgar Allan Poe R.L. Stevenson Frederic Chopin Page 6 National Epidemiology: 2010 Data MMWR 2011;60:333 Page 7 4
")
5 Texas Epidemiology Harris County: cases cases cases cases cases cases 4-5 times the average national incidence Page 8 Definitions we use for TB Category Age Exam PPD/ IGRA CXR Contagious Treatment Exposure < 5 Never 1 drug, usually for 2 3 months (given by health department) Infection All + Never Usually 1 drug, given 6 9 months (given by family or health department) Disease All /+ +/ +/ Rarely Multiple drugs (3 4), given 6 12 months (always givenby health department) Nopatient with nontuberculous mycobacteria is contagious Page 9 5

6 Childhood TB Disease Sites Site* % of cases Median Age (years) Pulmonary Lymphatic Pleural Meningeal Bone/joint Miliary GU Peritoneal *: United States (almost all are normal hosts) Page 10 Risk of Progression from TB Infection to Disease by Age Peds in Review 2010;31:13 Page 11 6

7 Signs and Symptoms of Pulmonary TB Peds in Review 2010;31:13 Page 12 Available Diagnostic Tools Tool Older Generation Newer Generation Radiography CXR CT* Immune response Skin test Interferon assay Specimen Gastric aspirates Induced sputa collection PCR Sputum Other body fluids *CT is not the standard of care for the diagnosis of pulmonary TB, and is not necessary for the vast majority of children with pulmonary TB disease Page 13 7
8 One difference between adults & kids Modality Culture: Solid Adult Studies* Pedi Studies* Ratio adult to pedi Year of 1 st publication x 1967 Culture: x 1966 Liquid MODS x 2000 PPD/TST x 1907 IGRA x 1999 Xpert x 2010 PCR, all x 1990 *: PubMed Queries as of 7/27/11 Page 14 CXR Findings in Pediatric TB Hilar or mediastinal adenopathy Segmental/lobar infiltrates Calcifications (seen in 75-80% of children with pulmonary TB) Miliary disease Pleural effusions 15% of patients with TB disease will have normal CXRs Page 15 8





,")
, started on")
9 Intrathoracic Lymphadenopathy N.O Page 16 Lobar Infiltrates 9mo M presents to TB clinic with 23mm PPD done after grandfather diagnosed with smear positive pulmonary TB. Baby is asymptomatic, normal vital sg signs, s,go growing gwell. Admitted for LP (normal), gastric aspirates (smear negative), started on multidrug therapy for TB disease D.T Page 17 9




10 Collapse/Consolidation Pattern Lymph node collapses a bronchus, leading to distal atelectasis M.A Page 18 Calcifications Usually indicates disease present for 2 6 months W.C Page 19 10


11 Cavitary Lesions W.C Page 20 Cavitary Lesions Uncommon in children, but if see cavities, treat the child as contagious and take appropriate infection control precautions M.N Page 21 11




12 Cavitary Lesion 16yo M with very poorly controlled IDDM 2 months of productive cough, weight loss Smear-positive TB * DM is single most common predisposing medical condition in TX adults with TB disease J.A Int J Tuberc Lung Dis 2011;15:179 Page 22 Miliary Disease P.K Page 23 12



13 2003: 17yo WM with Crohn s, on anti TNFα therapy, negative baseline TST, developed miliary TB after 2 months C.A Page 24 Miliary TB with Tension Pneumothorax D.M Page 25 13



 J.")
14 Miliary TB in Spleen, Liver D.M Page 26 Pleural Effusions Often, children are very well appearing (vs. Staph empyemas) J.G Page 27 14
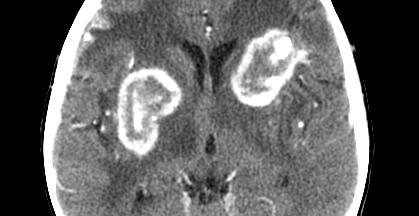

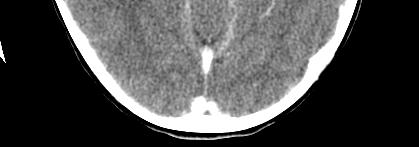
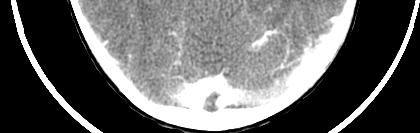

15 Tuberculomas W.C At initiation of therapy Page 28 After 2 months of therapy Tuberculous Pericarditis Page 29 15




16 Lymphadenopathy + Scrofuloderma Page 30 Paed Resp Rev 2007;8:107 Comparison: Nontuberculous Mycobacterial lymphadenopathy A.J T.O Page 31 16




17 Cutaneous TB: Lupus vulgaris M.R Page 32 Skeletal TB Page 33 17





18 Pott s Disease J.M. 1/ yo F with 1yr of worsening hunchback (gibbous deformity). T5 destruction. Culture: M. bovis Clin Infect Dis 2005;41:515 Page 34 Immune System Recognition Tuberculin skin tests (PPD) Interferon gamma release assays (IGRA) Page 35 18

 Any")

19 PPD Placement No controls Need to see a wheal raised Page 36 Positive PPDs Generally, skin test conversion occurs within 2 months of contact Measure only induration, and record millimeters of induration (never record + or ) Any induration seen only in the first 24 hours should be ignored Induration after 72 hours counts; blistering also counts Page 37 19
20 What is a Positive PPD? 5 mm: HIV+ or other immunocompromise Contact with suspected source case Suspected TB disease 10 mm: Immigrants from high-prevalence areas Children under 4 years of age Children exposed to adults in high-risk categories Other immunocompromising conditions 15 mm: anyone, even without risk factors 2009 Red Book Page 38 Who does AAP Recommend Skin Testing? Universal skin testing is NOT recommended Initial PPD should be done before initiation of immunosuppressive therapy (including prolonged steroid usage, TNF-α antagonists) Annual PPDs: HIV+ or incarcerated Q2-3yr testing should be considered: high-risk Immediate PPD should be placed: As part of contact investigation CXR or clinical findings consistent with TB Children emigrating from endemic countries Children with travel history to or contact with persons from endemic countries 2009 Red Book Page 39 20
21 Validated Questions to Determine LTBI Risk Has a relative or contact had TB disease? Has a family member had a positive TB skin test? Was the child born in a high-risk country? Has your child traveled to a high-risk country for > 1 week? Should consider screening for risk factors at the initial visit and every 6 months thereafter in first 2 years of life 2001;107:e54; Red Book 2009 Page 40 PPD Limitations False positives: Exposure to mycobacteria other than TB BCG vaccine False negatives: Corticosteroid usage Other immunocompromise Viral suppression: measles, mumps, influenza Inter-observer variability Sliding scale for what is considered positive can be confusing Until very recently, lack of any confirmatory tests Page 41 21
22 PPD: Myths surrounding BCG Myth: PPDs will be positive in all patients who received BCG vaccination Reality: R 50% of infants receiving i BCG do not react to skin tests, and most of the rest stop reacting within 5 years Myth: PPDs can be neither placed nor interpreted in BCG recipients Reality: y different cut-off points for the skin test are not recommended based upon a child s BCG status Page 42 So, What Are Alternatives? Since 2005: 2 commercially available blood tests, interferon gamma release assays (IGRA) that offer more specificity than the skin test Page 43 22
 MMWR 2010;59(No.")
 Cross-reactivity with BCG Yes Unlikely Cross-reactivity with NTM Yes Less Likely Estimated sensitivity, TB in 75-90% 75-95% immunocompetent adults Estimated specificity, TB in 70-95%")
23 IGRAs Interferon-γ release assays (IGRAs) detect host response to Mycobacterium tuberculosis-specific antigens Two main tests currently FDAapproved: T-SPOT.TB QuantiFERON Q Gold In-Tube Offer several potential advantages over the tuberculin skin test (TST) MMWR 2010;59(No.RR 5):1 14 Page 44 Comparison of Skin Test & IGRA Characteristic TST IGRA Antigens studied Many -PPD ESAT-6, CFP-10, (TB-7.7) Cross-reactivity with BCG Yes Unlikely Cross-reactivity with NTM Yes Less Likely Estimated sensitivity, TB in 75-90% 75-95% immunocompetent adults Estimated specificity, TB in 70-95% % immunocompetent adults Distinguish between TB infection No No and TB disease Boosting Yes No Patient visits required Two One Page 45 Pediatr Infect Dis J 2006;25:941 23
24 IGRAs: Advantages One visit: optimal if adherence issues Decreased confusion about interpretation: one cutoff irrespective of age, immune status, and TB risk factors Enhanced specificity: optimal for BCG-immunized persons Page 46 IGRA: Limitations Indeterminate results: decrease the utility of a screening tool One cut-off: is this appropriate across risk strata? Unknown dynamics of when assays become positive Discordance: interpretation if TST and IGRA provide different results Limited pediatric data: especially for the most vulnerable risk groups Page 47 24
25 HIV-infected Children Sensitivity plummets with CD4 < 200 Sensitivity: TSPOT > QFN > TST We don t know the dynamics of IGRAs in HIV+ kids No association with QFN result and CD4 (but n=14 with + TST) Page 48 Malnourished Children 251 malnourished children, of whom 47% had helminthic infection (Ascaris, Trichuris) Test agreement: κ = 0.55 between TST and QuantiFERON 25% had indeterminate test results Degree of malnutrition and helminth infection were associated with indeterminate IGRA results 2010;126:e1522 Page 49 25
26 Cancer Center Patients 34 newly diagnosed children with cancer (S. Africa) TST vs. T-SPOT vs. QuantiFERON 7 were (+) with any test (less than expected) IGRAs had 12-15% indeterminate results In 1/5 of cases, TSPOT could not be completed because of low cell counts (controls failed) Multiple discordances: Between TST and both IGRAs Between the IGRAs Conclusion: no stand-alone test helpful in this population Int J Tuberc Lung Dis 2010;14:689 Page 50 Renal Patients Conversions and reversions of IGRAs seen Conversions: 22% and 27% for QFN and T-SPOT Reversions: 16% and 30% for QFN and T-SPOT Most studies suggest QFN is better for this group Indeterminate results range from 3-15% Results can be dramatically different if blood obtained pre- or post-dialysis IGRA should be done pre-dialysis Transpl Infect Dis 2009;11:28 / J Infect 2010;61:144 Page 51 26

27 Diabetics Adult type II diabetics with culture-positive TB* QFN: 70% sensitive T-SPOT: 93% sensitive Seemed to perform as well as TST * DM is single most common predisposing medical condition in TX adults with TB disease Int J Tuberc Lung Dis 2011;15:179 Page 52 TST preferred, IGRA acceptable Children < 5 years of age IGRA preferred, TST acceptable BCG recipients Groups with historically low rates of return for TST reading MMWR 2010;59:RR 5 Page 53 27
28 Either IGRA or TST can be used Contact investigations Surveillance programs for healthcare workers MMWR 2010;59:RR 5 Page 54 Both TST and IGRA should be considered Initial IGRA indeterminate i t or borderline When initial test (TST or IGRA) is negative and: There exists clinical suspicion for TB disease Risk of infection, progression, and poor outcome higher When initial test (TST or IGRA) is positive and: Need additional evidence to increase compliance Healthy persons with low risk for both infection and disease progression MMWR 2010;59:RR 5 Page 55 28




29 What to do with discordant results? In patients in whom disease is suspected or at high risk for progression from infection, treat if any test positive For patients without risk factors, treat if the more specific test is positive Page 56 Case: A.N. (2010) 19mo M presents with fever, altered mentation. No medical history or known contacts with TB. Page 57 29
30 Case: A.N. (2010) CSF WBC RBC Protein Glucose Smear AFB Cx Source EVD 15 17, LP < 20 PPD: 0 mm QuantiFERON: indeterminate T-SPOT: wicked positive Mother s (now former) boyfriend found to have pulmonary TB after contact investigation Page 58 Acid-Fast Culture Yield Specimen Culture Yield Sputum/gastric aspirate 30-40% Lymphatic tissue 75% Pleural fluid 20-40% Cerebrospinal fluid 20-50% Pericardial fluid 0-42% Ascitic fluid 30% Skin biopsy 20-50% Skeletal biopsy 75% Paed Resp Rev 2007;8:107 Page 59 30
 Try new methods of obtaining cultures Page 60 Gastric Aspirates Inpatient procedure Overnight")
31 So, Our Culture Yield is Horrible; Now What? Great contact investigations to identify source cases for our patients (cultures by proxy) Try new methods of obtaining cultures Page 60 Gastric Aspirates Inpatient procedure Overnight fasting Lavage with NS if volume < 20cc Generally done qam x3 Inpatient costs substantial AFB smear yield: minimal AFB Culture yield: 20-30% Page 61 31




32 Induced Sputum Outpatient procedure 2-3h fasting gperiod Pretreated with salmeterol; nebulized saline, then CPT given Nasopharynx suctioned One specimen sufficient Minimal costs AFB smear yield: 50% AFB Culture yield: 25-30% Lancet. 2005;365:130 Page 62 Page 63 Photo courtesy of Paul Mullan, M.D. 32

33 TB Infection Control In the mid-1990s, TCH began to require that adults and adolescents accompanying inpatient children with suspected tuberculosis undergo chest radiography to rule- out infectious pulmonary TB A previous report from TCH [Muñoz et al. Infect Control Hosp Epidemiol 2002;23: ] demonstrated that 15% of the adults accompanying hospitalized children with suspected tuberculosis had previously undiagnosed pulmonary TB Results from this study also showed that no healthcare worker who cared for a child with tuberculosis became infected [conversion of the TST] Infect Control Hosp Epidemiol 2002;23:568 and 2011;32:188 Page 64 When do we worry about it? Older adolescents Children with certain findings on CXR Producing sputum Any draining skin lesions Infect Control Hosp Epidemiol 2011;32:188 Page 65 33
 for patient Keep patient in room Page")

34 If we are worried, what do we do? N95 respirator for you Simple facemask (not N95) for patient Keep patient in room Page 66 History of Drug-Resistant TB Drug Year Introduced Year of 1 st Documented Resistance Streptomycin Isoniazid Pyrazinamide Ethambutol Rifampin Fluoroquinolones Page 67 34



35 Total drugs to treat pan-susceptible TB Page 68 Total drugs to treat 1 case of multidrug-resistant (MDR)* TB *MDR: resistant to at least INH and Rifampin XDR (extensively drug resistant): Page MDR 69 + resistance to fluoroquinolones + injectable agents 35


36 DOTS (directly observed therapy, short course): administration of medications to persons with TB disease by dispassionate 3 rd party Standard d d of care for TB disease in the United States Provided free of charge to patient Removes some barriers to care Increases adherence, thereby decreasing risk of selecting out for drug resistant organisms by sporadic medication usage Photos courtesy of Manish Shah, MD Page 70 Treatment TB exposure TB infection TB disease Page 71 36

 pending repeat skin testing Children > 4 yrs of age")

37 TB Exposure Children < 5 years of age with a negative PPD, normal CXR and examination exposed to contact with suspected TB Provide chemoprophylaxis in the window period (8-10 weeks) pending repeat skin testing Children > 4 yrs of age also need sequential skin testing, but no window chemoprophylaxis Page 72 Why Do We Do This? To Prevent This: E.Q Page 73 37
38 Why do we treat TB infection? Risk of developing TB disease with untreated + PPD: 5-10% lifetime risk in most patients 40% risk in infants 5-10% annual risk in HIV-infected patients ½ of lifetime risk in 1 st 1-2 yrs after PPD conversion Remainder of risk evenly spread over lifetime We can reduce risk by 90-95% with INH Page 74 Red Book Statement on TB Infection All infants, children, and adolescents who have a positive PPD result but no evidence of TB disease and who have never received antituberculosis therapy should be considered for INH unless resistance to INH is suspected or a specific contraindication exists Red Book 2009, p691 Page 75 38

39 How is LTBI different in children? Risk of disease progression Identifying time of infection Identification of source case Medication tolerance Page 76 Risk of Progression to Disease, Stratified by Patient Age Risk of disease progression in adults: 1 13% lifetime risk in Review 2010;31:13 Page 77 NEJM 2011;364:15 39


40 Pinpointing time of infection Most young children are by definition new converters So, this is best opportunity to prevent future disease: ½ of lifetime risk is in first 1-2 years after TST conversion Risk substantively higher for infants Page 78 Children have circumscribed social networks Often the person who infected the child is a caregiver/relative Easier to identify source case, and child is unlikely to have > 1 source case NEJM 2011;364:730 Page 79 40


41 Medication Tolerance : 5% risk of side effects in children Most minor abdominal pain without elevation in LFTs 3.3% 3% risk of elevated LFTs in 1970s with INH+RIF Adults: 2006;117:e148; 1983;72:491 Page NEJM ;364:15 IJTLD 2010;14:1374 Take home messages: educate families on side effects low threshold for checking LFTs if symptomatic screen for LTBI judiciously 2008;121:e1732 Page 81 41

42 Chest 2010;137:737 Page 82 TB Prevention Isoniazid (INH) = mainstay of therapy mg/kg single daily dose if given by family mg/kg twice weekly if given by health department Duration: 9 months Alternative: rifampin x 6 months If person around child with TB is known to have INH-resistant disease or if child is INH-intolerant Page 83 42
43 LTBI Treatment Pearls Use INH suspension only in children < 5 kg Otherwise, give tablets that can be crushed & mixed with food Compliance with 9 months of INH averages a bit over 50%; be skeptical Use health department to administer medications to high-risk patients: infants, immunocompromised children, recent contacts When children aren t tolerating INH, the problem is more often with the parent than the child Routine LFTs not indicated unless: concomitant administration of other hepatotoxic drugs; pre-existing liver disease; or signs/symptoms of hepatitis Page 84 Therapy for TB Disease Start 4-drug therapy (a change from 2006 Red Book) INH, rifampin (RIF), pyrazinamide (PZA), and ethambutol (EMB); INH/RIF are the backbone of therapy Use PZA only during 1 st 2 months for susceptible TB This is your shortening agent : consolidate from 9 to 6 months of therapy Stop EMB once culture results known, if have pan-susceptible TB This is your insurance in case you have drug-resistant TB Anticipate minimum 6 month therapy, and we often extend it to longer periods, especially for extrapulmonary disease Always administered by directly observed therapy (DOT) 2009 Red Book Page 85 43
44 Notes on TB Drugs Drug Side Effects Other notes INH Peripheral neuropathy; seizures in B6 helps prevent neuropathy and is overdose only treatment for INH seizures, but doesn t prevent hepatotoxicity RIF Orange discoloration of secretions; inactivates oral contraceptives; many drug interactions Please warn of Longhorn orange urine! PZA Can increase uric acid gout symptoms; rash Of 1 st line drugs, greatest association with hepatotoxicity EMB Optic neuritis, red green color blindness Despite side effects, has very poor CNS penetrance and not used for meningitis *All primarily hepatically metabolized, except EMB, which is also renally excreted Peds in Review 2010;31:13 Page 86 Conclusions Screen all children for TB risk factors via questionnaire Traditional culture techniques are of much lower yield in children as compared with adults Newer diagnostic assays have recently become available, but are not without their own limitations IGRAs offer improved specificity, not sensitivity, compared to PPDs There is no substitute for a comprehensive history to elicit TB risk factors It is impossible to effectively manage childhood TB without close cooperation with an effective public health infrastructure Page 87 44
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017
 Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management
 TB Nurse Case Management San Antonio, Texas March 2-4, 2011 Pediatric TB Andrea T. Cruz, MD, MPH March 2, 2011 Andrea Cruz, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas March 2-4, 2011 Pediatric TB Andrea T. Cruz, MD, MPH March 2, 2011 Andrea Cruz, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Pediatric TB Lisa Armitige, MD, PhD September 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB Nurse Case Management San Antonio, Texas March 7 9, Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012
 TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Intensive San Antonio, Texas August 7-10, 2012
 TB Intensive San Antonio, Texas August 7-10, 2012 An Introduction to Childhood Tuberculosis Kim Smith, MD, MPH August 10, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Intensive San Antonio, Texas August 7-10, 2012 An Introduction to Childhood Tuberculosis Kim Smith, MD, MPH August 10, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]
![CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]](/thumbs/89/99628771.jpg "CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]") CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT] QUESTION: : Which children in the United States should get a tuberculin skin test? Do questionnaires really work? Jeffrey
CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT] QUESTION: : Which children in the United States should get a tuberculin skin test? Do questionnaires really work? Jeffrey
Management of Pediatric Tuberculosis in New Jersey
 Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
TB Intensive San Antonio, Texas
 TB Intensive San Antonio, Texas August 2-5, 2011 Pediatric TB Jeffrey Starke, MD August 5, 2011 Jeffrey Starke, MD has the following disclosures to make: Is on a data safety monitoring board for Hoffman
TB Intensive San Antonio, Texas August 2-5, 2011 Pediatric TB Jeffrey Starke, MD August 5, 2011 Jeffrey Starke, MD has the following disclosures to make: Is on a data safety monitoring board for Hoffman
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015
 Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Pediatric TB Intensive Houston, Texas October 14, 2013
 Pediatric TB Intensive Houston, Texas October 14, 2013 Diagnosis and Management of Tuberculosis in Adolescents Andrea T. Cruz, MD, MPH Sections of Infectious Diseases & Emergency Medicine October 14, 2013
Pediatric TB Intensive Houston, Texas October 14, 2013 Diagnosis and Management of Tuberculosis in Adolescents Andrea T. Cruz, MD, MPH Sections of Infectious Diseases & Emergency Medicine October 14, 2013
TB Intensive Houston, Texas October 15-17, 2013
 TB Intensive Houston, Texas October 15-17, 2013 Tuberculosis in Children Kim Connelly Smith, MD, MPH October 16, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Intensive Houston, Texas October 15-17, 2013 Tuberculosis in Children Kim Connelly Smith, MD, MPH October 16, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
PEDIATRIC TUBERCULOSIS
 PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
PEDIATRIC TUBERCULOSIS. Objectives. Children are not just small adults. Pediatric Tuberculosis 1
 PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
Pediatric Tuberculosis
 Pediatric Tuberculosis Kim Connelly Smith, MD, MPH April 7, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Kim Connelly Smith, MD, MPH has the following disclosures to
Pediatric Tuberculosis Kim Connelly Smith, MD, MPH April 7, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Kim Connelly Smith, MD, MPH has the following disclosures to
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Global Impact of TB
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB in Corrections Phoenix, Arizona
 TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
TB Intensive San Antonio, Texas November 11 14, 2014
 TB Intensive San Antonio, Texas November 11 14, 2014 Interferon Gamma Release Assays Lisa Armitige, MD, PhD November 12, 2014 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of
TB Intensive San Antonio, Texas November 11 14, 2014 Interferon Gamma Release Assays Lisa Armitige, MD, PhD November 12, 2014 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of
New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents
 New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea
New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea
Contact Investigation and Prevention in the USA
 Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
has the following disclosures to make:
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Life Cycle of M. tuberculosis
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of tuberculosis in children
 Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
TUBERCULOSIS. Pathogenesis and Transmission
 TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TB Intensive Houston, Texas October 15-17, 2013
 TB Intensive Houston, Texas October 15-17, 2013 Interferon Gamma Release Assays (IGRA s) Lisa Armitige, MD, PhD October 16, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
TB Intensive Houston, Texas October 15-17, 2013 Interferon Gamma Release Assays (IGRA s) Lisa Armitige, MD, PhD October 16, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
Diagnosis and Medical Management of TB Disease. Quratulian Annie Kizilbash, MD, MPH March 17, 2015
 Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
Approaches to LTBI Diagnosis
 Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014
 Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014 Interferon Gamma Release Assays: Understanding the Test David Griffith, BA, MD April 11, 2014 David Griffith, BA, MD has the following
Evaluation and Treatment of TB Contacts Tyler, Texas April 11, 2014 Interferon Gamma Release Assays: Understanding the Test David Griffith, BA, MD April 11, 2014 David Griffith, BA, MD has the following
Communicable Disease Control Manual Chapter 4: Tuberculosis
 Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Errors in Dx and Rx of TB
 Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
Diagnosis & Medical Case Management of TB Disease. Lisa Armitige, MD, PhD October 22, 2015
 Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Pediatric TB Theresa Barton, MD
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Pediatric TB Theresa Barton, MD December 9, 2009 Pediatric Tuberculosis Tess Barton, MD Assistant Professor of Pediatrics UT Southwestern
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Pediatric TB Theresa Barton, MD December 9, 2009 Pediatric Tuberculosis Tess Barton, MD Assistant Professor of Pediatrics UT Southwestern
Childhood Tuberculosis Some Basic Issues. Jeffrey R. Starke, M.D. Baylor College of Medicine
 Childhood Tuberculosis Some Basic Issues Jeffrey R. Starke, M.D. Baylor College of Medicine TUBERCULOSIS IS A SOCIAL DISEASE WITH MEDICAL IMPLICATIONS THE GREAT PARADOX OF TUBERCULOSIS A CAUTIONARY TALE
Childhood Tuberculosis Some Basic Issues Jeffrey R. Starke, M.D. Baylor College of Medicine TUBERCULOSIS IS A SOCIAL DISEASE WITH MEDICAL IMPLICATIONS THE GREAT PARADOX OF TUBERCULOSIS A CAUTIONARY TALE
Gary Reubenson 16 October 2012 PAEDIATRIC TUBERCULOSIS: AN OVERVIEW IN 40 MINUTES!!
 Gary Reubenson 16 October 2012 PAEDIATRIC TUBERCULOSIS: AN OVERVIEW IN 40 MINUTES!! DECLARATION No relevant conflicts of interest to declare OVERVIEW Burden of disease & epidemiology Pathogenesis (not
Gary Reubenson 16 October 2012 PAEDIATRIC TUBERCULOSIS: AN OVERVIEW IN 40 MINUTES!! DECLARATION No relevant conflicts of interest to declare OVERVIEW Burden of disease & epidemiology Pathogenesis (not
The Origin of Swine Flu
 How the Heck Do You Diagnose Tuberculosis in Children, Anyway? Jeffrey R. Starke, M.D. Professor and Vice Chairman of Pediatrics Baylor College of Medicine Houston, Texas USA The Origin of Swine Flu MAIN
How the Heck Do You Diagnose Tuberculosis in Children, Anyway? Jeffrey R. Starke, M.D. Professor and Vice Chairman of Pediatrics Baylor College of Medicine Houston, Texas USA The Origin of Swine Flu MAIN
Northwestern Polytechnic University
 Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
10/3/2017. Updates in Tuberculosis. Global Tuberculosis, WHO 2015 report. Objectives. Disclosures. I have nothing to disclose
 Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
CHAPTER 3: DEFINITION OF TERMS
 CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 IGRA s and Their Use in TB Nurse NCM Lisa Armitige, MD, PhD July 18, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 IGRA s and Their Use in TB Nurse NCM Lisa Armitige, MD, PhD July 18, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict
Pediatric Tuberculosis. Ann M. Loeffler, MD Pediatric TB Consultant Curry International Tuberculosis Center
 Pediatric Tuberculosis Ann M. Loeffler, MD Pediatric TB Consultant Curry International Tuberculosis Center Introduction Basic situations in which children are evaluated Diagnosis and treatment of latent
Pediatric Tuberculosis Ann M. Loeffler, MD Pediatric TB Consultant Curry International Tuberculosis Center Introduction Basic situations in which children are evaluated Diagnosis and treatment of latent
Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University
 Lloyd Friedman, M.D. Milford Hospital Yale University") Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University Tuberculosis Estimates USA World Infection 15,000,000 2,000,000,000
Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University Tuberculosis Estimates USA World Infection 15,000,000 2,000,000,000
Disclosures. Current Issues and Controversies in Child and Adolescent Tuberculosis 02/24/2016. NSTC 2016 Annual Meeting
 Current Issues and Controversies in Child and Adolescent Tuberculosis Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea Cruz, M.D.] Disclosures Dr.
Current Issues and Controversies in Child and Adolescent Tuberculosis Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea Cruz, M.D.] Disclosures Dr.
Pediatric TB Intensive Houston, Texas
 Pediatric TB Intensive Houston, Texas November 13, 2009 Treatment of Pediatric TB Jeffrey R. Starke, M.D. November 13, 2009 MANAGEMENT OF CHILDHOOD TUBERCULOSIS Jeffrey R. Starke, M.D. Professor of Pediatrics
Pediatric TB Intensive Houston, Texas November 13, 2009 Treatment of Pediatric TB Jeffrey R. Starke, M.D. November 13, 2009 MANAGEMENT OF CHILDHOOD TUBERCULOSIS Jeffrey R. Starke, M.D. Professor of Pediatrics
LTBI in Special Populations John Nava, MD October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 LTBI in Special Populations John Nava, MD October 5, 2010 2 Treatment of Latent TB Infection in Special Populations John
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 LTBI in Special Populations John Nava, MD October 5, 2010 2 Treatment of Latent TB Infection in Special Populations John
Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, TB Nurse Case Management September 12 14, 2017
 Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Jeffrey R. Starke, M.D. has the following disclosures to make:
 AAP 2018 Red Book Tuberculosis: IGRAs and Treatment of TB Infection Jeffrey R. Starke, M.D. May 31, 2018 AAP 2018 Red Book Childhood Tuberculosis: IGRAs and Treatment of TB Infection May 31, 2018 WEBINAR
AAP 2018 Red Book Tuberculosis: IGRAs and Treatment of TB Infection Jeffrey R. Starke, M.D. May 31, 2018 AAP 2018 Red Book Childhood Tuberculosis: IGRAs and Treatment of TB Infection May 31, 2018 WEBINAR
TB in the Patient with HIV
 TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
Disclosures. Updates in TB for the PCP: Opportunities for Prevention. Objectives PART 1: WHY TEST? 4/14/2016. None
 Disclosures Updates in TB for the PCP: Opportunities for Prevention None Pennan Barry, MD, MPH Chief, Surveillance and Epidemiology, California TB Control Branch Assistant Clinical Professor, Division
Disclosures Updates in TB for the PCP: Opportunities for Prevention None Pennan Barry, MD, MPH Chief, Surveillance and Epidemiology, California TB Control Branch Assistant Clinical Professor, Division
Tuberculosis (TB) Fundamentals for School Nurses
 Fundamentals for School Nurses") Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Tuberculosis: A Provider s Guide to
 Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
At the end of this session, participants will be able to:
 Advanced Concepts in Pediatric Tuberculosis: Infection Control, Source Case and Contact Investigation Ana M. Alvarez, M.D. Associate Professor Division of Pediatric Infectious Diseases and Immunology University
Advanced Concepts in Pediatric Tuberculosis: Infection Control, Source Case and Contact Investigation Ana M. Alvarez, M.D. Associate Professor Division of Pediatric Infectious Diseases and Immunology University
New Tuberculosis Guidelines. Jason Stout, MD, MHS
 New Tuberculosis Guidelines Jason Stout, MD, MHS Two New Sets of Guidelines Treatment of Drug-Susceptible Tuberculosis Clinical Infectious Diseases 2016; 63(7): e147-e195 Diagnosis of Tuberculosis in Adults
New Tuberculosis Guidelines Jason Stout, MD, MHS Two New Sets of Guidelines Treatment of Drug-Susceptible Tuberculosis Clinical Infectious Diseases 2016; 63(7): e147-e195 Diagnosis of Tuberculosis in Adults
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013
 Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2014
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and Infectious Disease UT Health Northeast
 Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
TUBERCULOSIS. Presented By: Public Health Madison & Dane County
 TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI)
") Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI) CURTIS FOWLER MPT,PA C ASSISTANT CLINICAL PROFESSOR UNIVERSITY OF THE PACIFIC Learning objectives Recognize the appropriate
Evaluation and Management of the Patient with Latent Tuberculosis Infection (LTBI) CURTIS FOWLER MPT,PA C ASSISTANT CLINICAL PROFESSOR UNIVERSITY OF THE PACIFIC Learning objectives Recognize the appropriate
Targeted Testing and the Diagnosis of. Latent Tuberculosis. Infection and Tuberculosis Disease
 Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
I. Demographic Information GENDER NUMBER OF CASES PERCENT OF CASES. Male % Female %
 San Joaquin County (SJC) in 03, (N=43) County Rate = 6. Cases per 00,000 Population I. Demographic Information Table I-A: TB cases by gender, SJC, 03 (N=43) GENDER NUMBER OF CASES Male 6 60.5% Female 7
San Joaquin County (SJC) in 03, (N=43) County Rate = 6. Cases per 00,000 Population I. Demographic Information Table I-A: TB cases by gender, SJC, 03 (N=43) GENDER NUMBER OF CASES Male 6 60.5% Female 7
TB Intensive Tyler, Texas December 2-4, 2008
 TB Intensive Tyler, Texas December 2-4, 2008 Interferon Gamma Releasing Assays: Diagnosing TB in the 21 st Century Peter Barnes, MD December 2, 2008 TOPICS Use of interferon-gamma release assays (IGRAs)
TB Intensive Tyler, Texas December 2-4, 2008 Interferon Gamma Releasing Assays: Diagnosing TB in the 21 st Century Peter Barnes, MD December 2, 2008 TOPICS Use of interferon-gamma release assays (IGRAs)
TB Prevention Who and How to Screen
 TB Prevention Who and How to Screen 4.8.07. IUATLD 1st Asia Pacific Region Conference 2007 Dr Cynthia Chee Dept of Respiratory Medicine / TB Control Unit Tan Tock Seng Hospital, Singapore Cycle of Infection
TB Prevention Who and How to Screen 4.8.07. IUATLD 1st Asia Pacific Region Conference 2007 Dr Cynthia Chee Dept of Respiratory Medicine / TB Control Unit Tan Tock Seng Hospital, Singapore Cycle of Infection
Pre-Treatment Evaluation. Treatment of Latent TB Infection (LTBI) Initiating Treatment: Patient Education. Before initiating treatment for LTBI:
 Initiating Treatment: Patient Education. Before initiating treatment for LTBI:") Pre-Treatment Evaluation Before initiating treatment for LTBI: Treatment of Latent TB Infection (LTBI) Amee Patrawalla, MD Associate Professor, New Jersey Medical School Attending Physician, NJMS Global
Pre-Treatment Evaluation Before initiating treatment for LTBI: Treatment of Latent TB Infection (LTBI) Amee Patrawalla, MD Associate Professor, New Jersey Medical School Attending Physician, NJMS Global
Tuberculosis Update. Topics to be Addressed
 Tuberculosis Update Robert M. Jasmer, M.D. University of California, San Francisco TB Control Section, San Francisco Department of Public Health Topics to be Addressed TB in the USA Screening recommendations
Tuberculosis Update Robert M. Jasmer, M.D. University of California, San Francisco TB Control Section, San Francisco Department of Public Health Topics to be Addressed TB in the USA Screening recommendations
Latent TB Infection (LTBI) Strategies for Detection and Management
 Strategies for Detection and Management") Latent TB Infection (LTBI) Strategies for Detection and Management Patrick T. Dowling MD,MPH Professor and Chair Dept of Family Medicine David Geffen School of Medicine at UCLA Pri-Med March 29 2014 Pdowling@mednet.ucla.edu
Latent TB Infection (LTBI) Strategies for Detection and Management Patrick T. Dowling MD,MPH Professor and Chair Dept of Family Medicine David Geffen School of Medicine at UCLA Pri-Med March 29 2014 Pdowling@mednet.ucla.edu
Diagnosis Latent Tuberculosis. Disclosures. Case
 Diagnosis Latent Tuberculosis Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention September 2016 1 Disclosures
Diagnosis Latent Tuberculosis Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention September 2016 1 Disclosures
The Diagnosis of Active TB. Deborah McMahan, MD TB Intensive September 28, 2017
 The Diagnosis of Active TB Deborah McMahan, MD TB Intensive September 28, 2017 Agenda Epidemiology Big picture Conditions that Should Make You Suspicious Which test? Eeenie meenie miny mo Radiographic
The Diagnosis of Active TB Deborah McMahan, MD TB Intensive September 28, 2017 Agenda Epidemiology Big picture Conditions that Should Make You Suspicious Which test? Eeenie meenie miny mo Radiographic
TB in Children. Rene De Gama Block 10 Lectures 2012
 TB in Children Rene De Gama Block 10 Lectures 2012 Contents Epidemiology Transmission and pathogenesis Diagnosis of TB TB and HIV Management Epidemiology The year 2000 8.3 million new TB cases diagnosed
TB in Children Rene De Gama Block 10 Lectures 2012 Contents Epidemiology Transmission and pathogenesis Diagnosis of TB TB and HIV Management Epidemiology The year 2000 8.3 million new TB cases diagnosed
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Michael J. Huey, MD. NYSCHA Annual Meeting WE-2, October 19, 2016
 Michael J. Huey, MD Assistant Vice President and Executive Director Emory University Student Health Services Associate Professor, Family and Preventive Medicine Emory University School of Medicine President-elect
Michael J. Huey, MD Assistant Vice President and Executive Director Emory University Student Health Services Associate Professor, Family and Preventive Medicine Emory University School of Medicine President-elect
Latent TB Infection (LTBI)
") Latent TB Infection (LTBI) Diagnosis & Treatment of Latent TB Infection (LTBI) Amee Patrawalla MD MPH Assistant Professor UMDNJ-New Jersey Medical School Infection with Mycobacterium tuberculosis without
Latent TB Infection (LTBI) Diagnosis & Treatment of Latent TB Infection (LTBI) Amee Patrawalla MD MPH Assistant Professor UMDNJ-New Jersey Medical School Infection with Mycobacterium tuberculosis without
Latent TB, TB and the Role of the Health Department
 Latent TB, TB and the Role of the Health Department Elaine Darnall, RN, BSN, CIC TB Nurse Consultant Illinois Dept of Public Health March 21, 2018 Elaine Darnall has disclosed that there is no actual or
Latent TB, TB and the Role of the Health Department Elaine Darnall, RN, BSN, CIC TB Nurse Consultant Illinois Dept of Public Health March 21, 2018 Elaine Darnall has disclosed that there is no actual or
TB Intensive San Antonio, Texas May 7-10, 2013
 TB Intensive San Antonio, Texas May 7-10, 2013 TB in the HIV Patient Lisa Armitige, MD, PhD May 09, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests No relevant
TB Intensive San Antonio, Texas May 7-10, 2013 TB in the HIV Patient Lisa Armitige, MD, PhD May 09, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests No relevant
Case Management of the TB/HIV Infected Patient
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Case Management of the TB/HIV Infected Patient Sarah Hoffman, MPH, MSN, ACRN December 9, 2009 TB/HIV: Considerations in the Care of the Coinfected
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Case Management of the TB/HIV Infected Patient Sarah Hoffman, MPH, MSN, ACRN December 9, 2009 TB/HIV: Considerations in the Care of the Coinfected
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease Barbara J Seaworth MD Medical Director Heartland National TB Center Professor of Medicine University of Texas Health Center Tyler Barbara J Seaworth MD has
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease Barbara J Seaworth MD Medical Director Heartland National TB Center Professor of Medicine University of Texas Health Center Tyler Barbara J Seaworth MD has
Tuberculosis and Diabetes Dec. 10, 2009 Dean Schillinger, M.D. and Gisela Schecter, M.D., M.P.H. 1 of 18
 Screening, Diagnosis, and Treatment of TB in Persons with Diabetes Dean Schillinger, M.D. University of California San Francisco CA Diabetes Program Gisela Schecter, M.D., M.P.H. TB Control Branch CA Department
Screening, Diagnosis, and Treatment of TB in Persons with Diabetes Dean Schillinger, M.D. University of California San Francisco CA Diabetes Program Gisela Schecter, M.D., M.P.H. TB Control Branch CA Department
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 PAGE 1 of 7 References Related ACA Standards 4 th Edition Standards for Adult Correctional Institutions 4-4350, 4-4355 These guidelines are based on the recommendations of the American Thoracic Society
PAGE 1 of 7 References Related ACA Standards 4 th Edition Standards for Adult Correctional Institutions 4-4350, 4-4355 These guidelines are based on the recommendations of the American Thoracic Society
European Respiratory Society Congress Barcelona President Award. Dr Walther Guerrero Ciquero
 TUBERCULOSIS Homework European Respiratory Society Congress Barcelona 2010 President Award Dr Walther Guerrero Ciquero ERS will continue to honour his memory through a Fellowship bearing his name. Stop
TUBERCULOSIS Homework European Respiratory Society Congress Barcelona 2010 President Award Dr Walther Guerrero Ciquero ERS will continue to honour his memory through a Fellowship bearing his name. Stop
CDC Immigration Requirements: Tuberculosis Screening for Children
 CDC Immigration Requirements: Tuberculosis Screening for Children Ann M. Loeffler, M.D. Curry International TB Center San Francisco, CA March, 2013 Atlanta, Georgia CDC Immigration Requirements: Tuberculosis
CDC Immigration Requirements: Tuberculosis Screening for Children Ann M. Loeffler, M.D. Curry International TB Center San Francisco, CA March, 2013 Atlanta, Georgia CDC Immigration Requirements: Tuberculosis
Research in Tuberculosis: Translation into Practice
 Case History Research in Tuberculosis: Translation into Practice This is a 6-year6 year-old Bosnian male, who presented to ER with one-week history of fever and occasional vomiting. No cough, difficulty
Case History Research in Tuberculosis: Translation into Practice This is a 6-year6 year-old Bosnian male, who presented to ER with one-week history of fever and occasional vomiting. No cough, difficulty
HIV prevalance in TB cases
 TUBERCULOSIS HIV prevalance in TB cases Top 5 AIDS indicative diseases; EUR, 2003 58% 35% 25% 11% 7% TB HIV wasting s. Candidiasis Rec. pneumonia HIV encephal. 26% 25% 31% 31% 16% 8% 7% 16% 14% 10% TB
TUBERCULOSIS HIV prevalance in TB cases Top 5 AIDS indicative diseases; EUR, 2003 58% 35% 25% 11% 7% TB HIV wasting s. Candidiasis Rec. pneumonia HIV encephal. 26% 25% 31% 31% 16% 8% 7% 16% 14% 10% TB
TB Nurse Case Management San Antonio, Texas April 9-11, 2013
 TB Nurse Case Management San Antonio, Texas April 9-11, 2013 TB / Dose Counting Rachel Munoz, RN. TB Nurse Case Manager/Nurse Consultant Austin/Travis County Health Department April 10, 2013 Rachel Munoz,
TB Nurse Case Management San Antonio, Texas April 9-11, 2013 TB / Dose Counting Rachel Munoz, RN. TB Nurse Case Manager/Nurse Consultant Austin/Travis County Health Department April 10, 2013 Rachel Munoz,
The Most Widely Misunderstood Test of All
 The Most Widely Misunderstood Test of All Lee B. Reichman, MD, MPH NJMS Global Tuberculosis Institute History of Treatment of Latent Tuberculosis Infection For more than 4 decades, treatment of persons
The Most Widely Misunderstood Test of All Lee B. Reichman, MD, MPH NJMS Global Tuberculosis Institute History of Treatment of Latent Tuberculosis Infection For more than 4 decades, treatment of persons
Treatment of Active Tuberculosis
 Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
Tuberculosis in Children and Adolescents 2017
 Tuberculosis in Children and Adolescents 2017 George D. McSherry, MD Division of Infectious Diseases Penn State Children s Hospital and Pediatric Section Northeastern Regional Training and Medical Consultation
Tuberculosis in Children and Adolescents 2017 George D. McSherry, MD Division of Infectious Diseases Penn State Children s Hospital and Pediatric Section Northeastern Regional Training and Medical Consultation
Dr Francis Ogaro MTRH ELDORET
 Dr Francis Ogaro MTRH ELDORET TB in children often severe, disseminated and can progress rapidly and with poor outcome TB diagnosis in children has relied on clinical, imaging, microscopy and TST findings.
Dr Francis Ogaro MTRH ELDORET TB in children often severe, disseminated and can progress rapidly and with poor outcome TB diagnosis in children has relied on clinical, imaging, microscopy and TST findings.
TB is Global. Latent TB Infection (LTBI) Sharing the Care: Working Together. September 24, 2014
 Sharing the Care: Working Together. September 24, 2014") Sharing the Care: Working Together to Meet the Challenge of TB Presented by: Barbara Cole, RN, PHN, MSN Director, Disease Control County of Riverside Department of Public Health Curry International TB
Sharing the Care: Working Together to Meet the Challenge of TB Presented by: Barbara Cole, RN, PHN, MSN Director, Disease Control County of Riverside Department of Public Health Curry International TB
ESCMID Online Lecture Library. by author
 Tuberculosis prevention in immunodepressed patients M. Carmen Fariñas Álvarez Infectious Diseases.H.U.Marqués de Valdecilla University of Cantabria, Spain DISCLOSURES I have no potential conflicts with
Tuberculosis prevention in immunodepressed patients M. Carmen Fariñas Álvarez Infectious Diseases.H.U.Marqués de Valdecilla University of Cantabria, Spain DISCLOSURES I have no potential conflicts with