Principles of laboratory diagnosis of M. tuberculosis. Anne-Marie Demers, MD, FRCPC 11 September 2017
|
|
|
- Stewart Chapman
- 5 years ago
- Views:
Transcription


1 Principles of laboratory diagnosis of M. tuberculosis Anne-Marie Demers, MD, FRCPC 11 September 2017
2 QUESTION Which statement is false? 1) A smear can only be on a concentrated specimen 2) It is normal for the TB laboratory to have some cultures that are reported as contaminated 3) Drug susceptibility testing can be done by genotypic (molecular) or phenotypic methods
3 Objectives Characteristics of mycobacteria Microbiology diagnosis of tuberculosis Phases of lab testing Specimen Collection Overview of most important tests Smear, Culture, Nucleic Acid Amplification Tests (NAATs), Drug Susceptibility Testing (DST) Reporting


4 Domain Phylum or Division Class Subclass Order Suborder Family Genus Bacteria Actinobacteria Actinobacteria Actinobacteridae Actinomycetales Corynebacterineae Mycobacteriaceae Mycobacterium CDC
 18 h Mycolic acids: special staining required Specific nutrients required Slow growth")
5 lipoarabinomannan (LAM) (lipopolysaccharide) Cell , DOI: ( /j.cell ) 18 h Mycolic acids: special staining required Specific nutrients required Slow growth
6 Mycobacterium mycobacterium.html 186 species Mycobacterium tuberculosis complex (MTBC) Nontuberculous Mycobacteria (NTM) MOTT (mycobacteria other than TB) M. leprae M. ulcerans (Buruli ulcer) M. tuberculosis M. bovis M. bovis BCG M. africanum Mycobacterium avium complex (MAC) M. kansasii M. marinum M. scrofulaceum M. fortuitum M. chelonei
7 > 95% DNA homology
8
9

10 TB Laboratory Diagnosis in children Why confirm the diagnosis? Clinical diagnosis not always easy Courtesy of E. Walters Guide treatment if MDR-TB Research


11 TB Laboratory Diagnosis Challenges In both adults and children TB diagnosis Respiratory specimens Quality/variability of specimen Infection control Culture still gold standard Costly, specialized labs Not perfect: contamination Long No real point of care test Xpert helps but other tests needed Variation in tests and procedures used, with many non-automated steps Compared to HIV diagnosis Diagnosis on blood specimen Rapid point of care tests
12 TB Laboratory Diagnosis in children Additional challenges: Paucibacillary nature of childhood TB Culture confirmed in 30% cases Specimen collection is invasive in young children Variety of specimens used Volumes collected often small Difficult to evaluate new diagnostic tests Tests evaluated in adult sputum applicable to gastric aspirate and other specimens?
13 Variability in TB labs Variability in procedures in TB labs worldwide Smear: auramine, ZN, Kinyoun Solid culture: LJ, 7H11 Variability due to individuals performing them e.g. smear reading, sputum processing Variability even for automated methods e.g. MGIT culture: automated and commercially available: however, identification of positive cultures varies Variability of diagnostic algorithms Culture or culture based DST not always done




14 Variety of TB diagnosis algorithms GLI Model TB Diagnostic Algorithms
15
, positive predictive value (ppv), and negative predictive value (npv).")
16 Figure 3. Relationship between prevalence (p), positive predictive value (ppv), and negative predictive value (npv). Own calculations based on a sensitivity of 90% and a specifity of 99%. Management In Health, 2010


17 Phases of laboratory testing Pre-Analytical Analytical Post-Analytical

18 Pre-analytical phase Decision of Test Specimen type Context Routine diagnostic / National TB Program Research Specimen collection and transport

19 Specimens Sputum Induced Sputum Potential specimens for bacteriological confirmation of PTB Slide courtesy of E. Walters
20 Specimens Respiratory vs non-respiratory Sputum (expectoraged, induced), Gastric aspirate/lavage, Naso-pharyngeal aspirate, Bronchoalveolar lavage (BAL), etc. Fine needle aspirate of lymphadenopathy, Cerebrospinal fluid (CSF), tissue, fluids, etc. Contaminated vs sterile From normally sterile sites vs from sites contaminated with normal flora Variability in collection methods Multiple specimens required

21 Gastric aspirate Collection of secretions swallowed overnight Naso-gastric tube inserted to aspirate stomach content after fasting Traditionally in hospital x 3 consecutive days Aspirate vs lavage Aspiration only Lavage using sterile water or saline. Dilution factor Inpatient vs outpatient Timing: Early morning Volume recommended: minimum 5-10 ml
22 Gastric aspirate Neutralisation of gastric aspirates with bicarbonates is recommended by many organisations including WHO, American Society of Microbiology Acid is detrimental to mycobacteria JCM 2013 Parashar et al. questioning need to neutralise GA specimens More research is needed Different neutralisation methods and formulations Solution vs solid/powder form Added by clinical team or by laboratory at reception Unless processing done < 4 hours of collection
23 Phases of laboratory testing Analytical




24
25 Specimen Processing Direct tests Culture Further tests if positive culture
 Cooling acid alcohol")

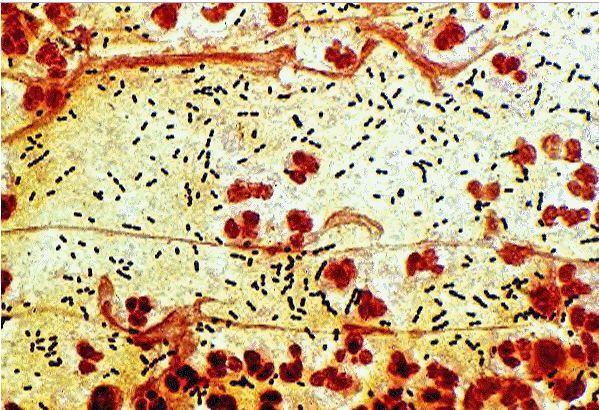
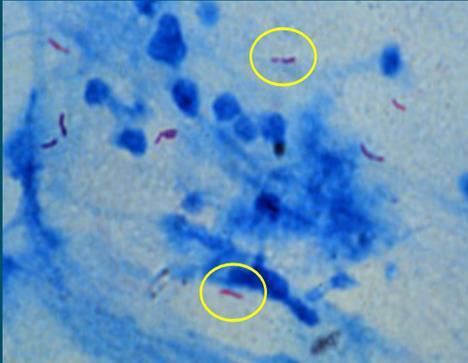
26 Smear microscopy Mycobacteria do not stain well with Gram stain Carbol fuschin stain: heat softens waxy lipid wall penetration of stain (mixture of dye and phenol) Cooling acid alcohol "decolouriser" poured over it acid removes carbol-fuschin from normal cells cold waxy coat of "acid fast" bacteria repel the decolouriser and remain stained: "acid fast" means acid cannot decolourise them

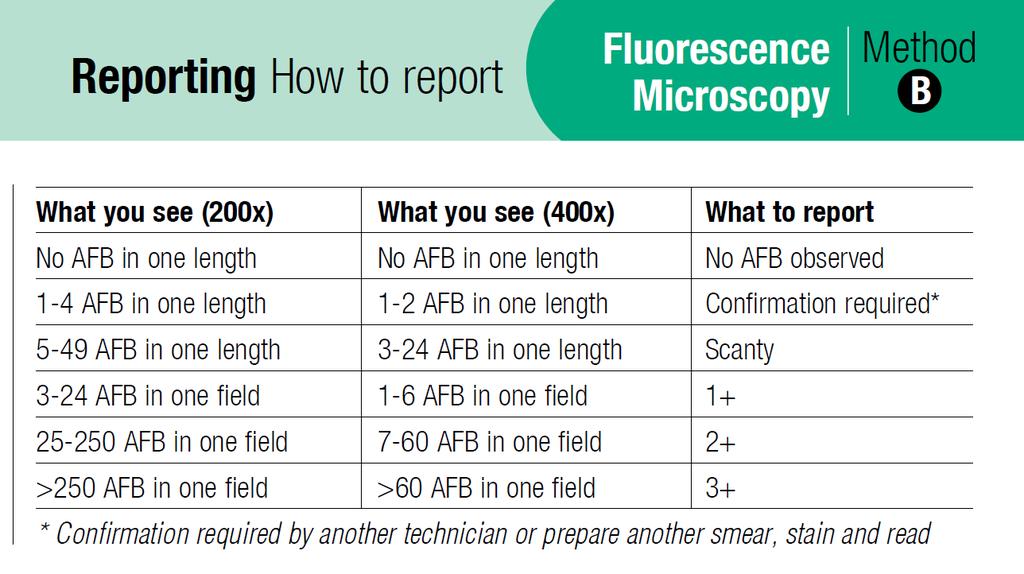
27 WHO Policy on Light Emitting Diode (LED) (2011): FM is 10% more sensitive and operational advantages Phased approach to change from brightfield to LED-based FM LED vs conventional FM: no dark room, less expensive lamps
28
29
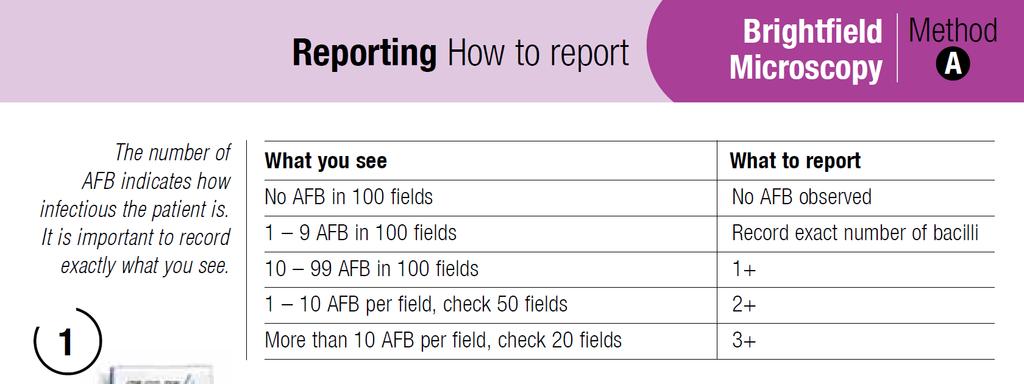
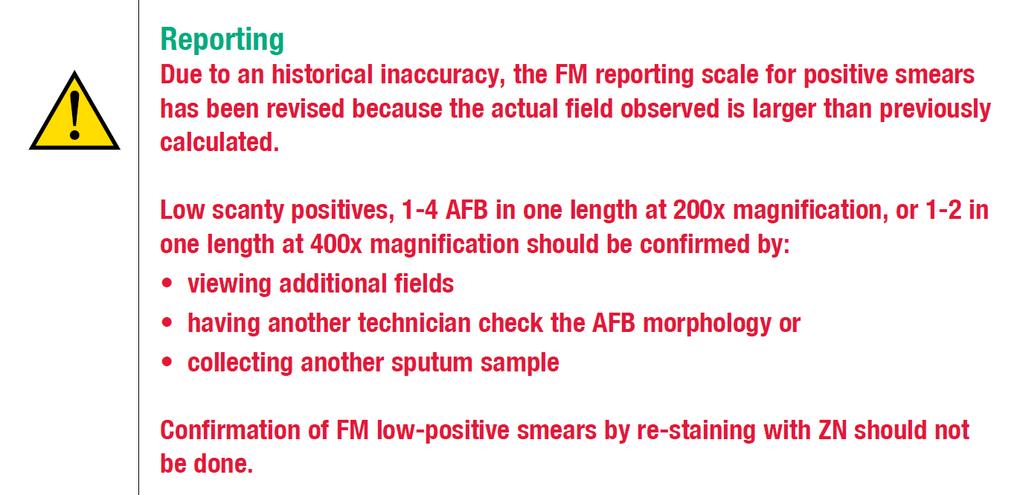
30 Test/Procedure Type/Example Smear microscopy Carbol-fuchsin: Ziehl-Neelsen (ZN), Kinyoun Fluorochrome: Auramine, Auramine-Rhodamine Done Directly on specimen: direct smear On specimen after processing: concentrated smear On culture if positive: ZN Sensitivity High bacterial load 5,000-10,000 AFB /ml is required for detection (culture detects 10 to 100 AFB / ml) Compared to culture: Se 20-80% 18% with processing (concentrated)* 10% with fluorescent vs conventional microscopy* Specificity All mycobacteria are acid fast Does not provide species identification Local prevalence of MTB and NTM determine the predictive values of a positive smear for MTB Cording suggestive of MTBC but also seen in some NTMs Turnaround time 24h Reporting WHO-IUATLD, ATS *Steingart Expert Rev. Anti Infect. Ther. 2007
31 Specimen Direct smear Direct tests Processing Concentrated smear Culture Further tests if positive culture Ziehl Neelsen on positive culture
32 Specimen Processing NALC-NaOH Digestion-Decontamination Direct tests Culture Further tests if positive culture

33 Processing Normal respiratory flora M.tuberculosis 18 h
34 Test/Procedure Processing (Decontamination-Digestion) Type/Example NALC (N-acetyl L-cysteine)-NaOH (sodium hydroxide) Oxalic Acid Done Principle Directly on specimens from non-sterile sites Decontamination (NaOH): To eliminate contaminants as much as possible without affecting the viability of mycobacteria Digestion (NALC): To release mycobacteria trapped in specimen mucus To improve the decontamination process To facilitate concentration of the specimen Limitations Delicate procedure: if it is too harsh, the yield is affected, as mycobacteria are also killed; if too mild, specimens will be overgrown by other bacteria. Many manual steps. Optimal method for specimens other than sputum? Risk of cross-contamination Result Quality indicator N/A. Sediment or pellet obtained: used for smear, nucleic acid amplification test (NAAT) or culture Contamination rate: cultures overgrown by bacteria. Target: 3-5% (solid) and 8-10% (liquid)
35

36 or sediment
37 Specimen Processing Direct tests Culture Further tests if positive culture
 Nutrients:")


 MGIT tube: Middlebrook 7H9 broth")


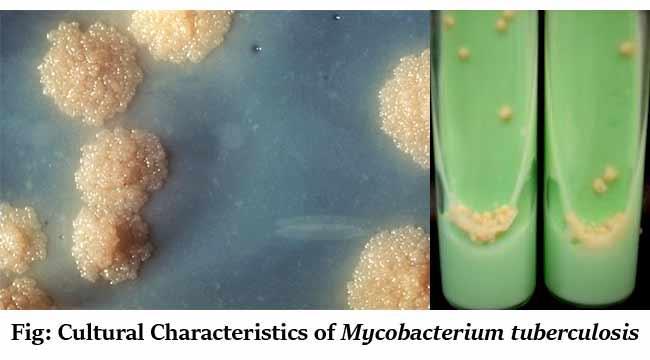
38 Lowenstein- Jensen (LJ) Middlebrook 7H10 or 7H11 agar (plate, tube) Nutrients: egg, potato, etc. LJ: Malachite green to inhibit bacteria Antibiotics can be added Middlebrook 7H9 broth MODS = Microscopic Observation Drug Susceptibility (Middlebrook 7H9 broth) MGIT tube: Middlebrook 7H9 broth + OADC enrichment: oleic acid, albumin, dextrose, catalase + PANTA antibiotic mixture (polymyxin B, amphotericin B, nalidixic acid, trimethoprim, azlocillin) Thin Layer Agar (TLA): Microscopic on agar

39

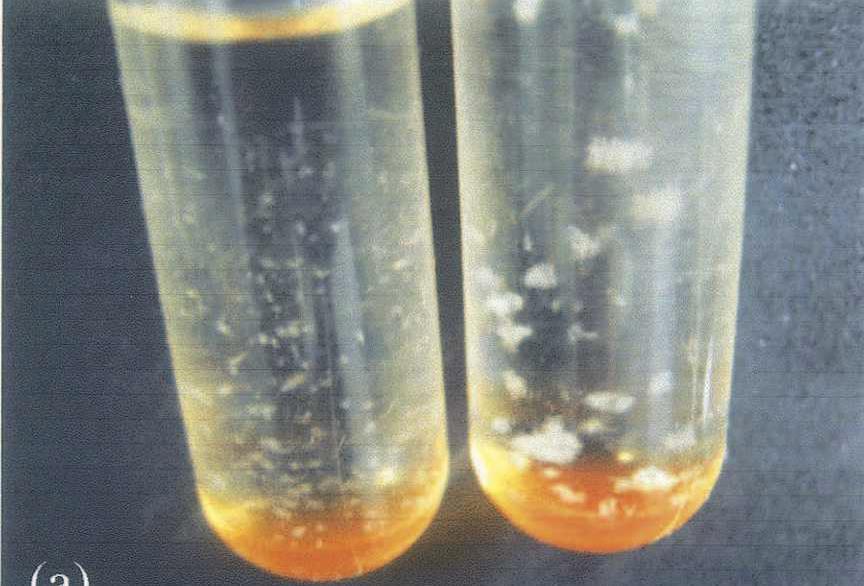
40 Mycobacterial Growth Indicator Tube BD BACTEC MGIT MGIT
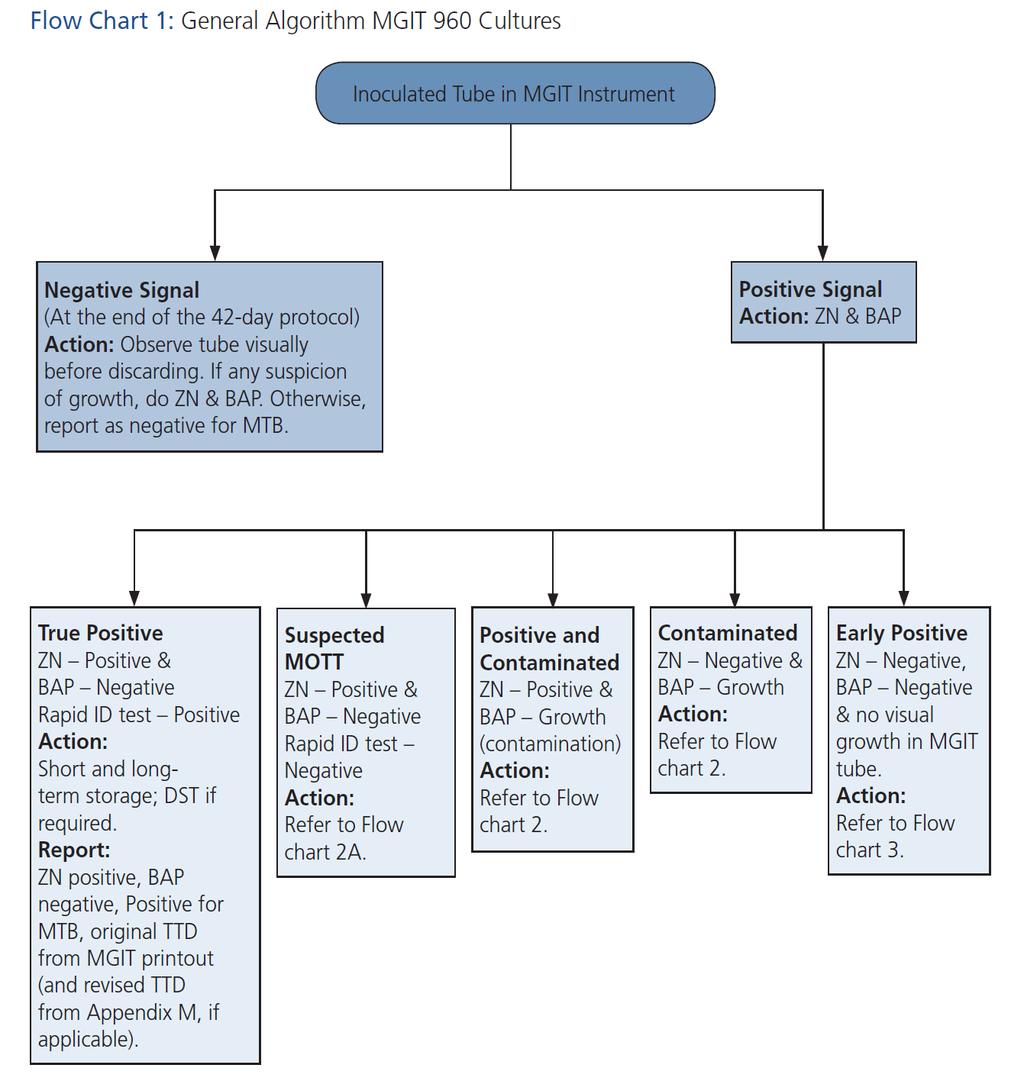
41 Test/Procedure Culture Type/Example Solid vs Liquid: Solid egg based: Lowenstein-Jensen (LJ), Ogawa Solid agar based: Middlebrook 7H10, 7H11 Liquid: Middlebrook 7H9 Manual vs Automated (ex: MGIT 960,VersaTREK,MB/BacT ALERT) Non-selective or selective (ex: 7H11S) Done On processed sample for non-sterile sites Directly on specimens for sterile sites Sensitivity Considered gold standard (liquid and solid) Detects 10 (liquid) to 100 (solid) TB bacilli / ml Specificity Depends on identification method Turn around time 8-10 days for smear-positive samples 2 6 weeks for smear-negative samples MGIT negative after 6 weeks (42 days). Solid often kept longer. Limitations MGIT susceptible to contamination Cost, expertise, biosafety, delays Reporting Qualitative: positive/negative for MTBC, etc. Quantitative: Solid: #colonies Liquid: time to detection (TTD)
42 Specimen Processing Direct tests Culture Further tests if positive culture


43 Identification of M. tuberculosis from liquid culture Automated system but manual steps for identification Identification test Ziehl-Neelsen Blood agar plate ZN: serpentine cords of varying length or district linear clumping
 Molecular methods DNA probes (Accuprobe MTBC) MPT64 antigen tests (lateral flow assays) Nucleic acid amplification tests (NAAT) Hain MTBDRplus done on")
44 Identification methods Biochemical tests Growth rate, morphology, pigmentation, combination of biochemical tests (nitrate, NAP, etc) abandoned No growth on medium with p-nitrobenzoic acid (PNB) High performance liquid chromatography (HPLC) Molecular methods DNA probes (Accuprobe MTBC) MPT64 antigen tests (lateral flow assays) Nucleic acid amplification tests (NAAT) Hain MTBDRplus done on positive culture Other methods
45 Test/Procedure Type/Example Principle MPT64 antigen test (Immunochromatographic tests, lateral flow assay tests) Capilia TB-Neo [Tauns Laboratories;Japan] SD Bioline s TB Ag MPT64 Rapid Test [South Korea] Becton Dickinson s TBcID[Maryland, USA] Detection of presence of the MTBC-specific protein MPT64 in culture isolates. Done On culture if positive (solid or liquid). Also works on contaminated cultures Sensitivity Detection limit 10 5 CFU/ml: done on positive culture High Se (92.4% 99.2%) Specificity High specificity (99-100%) Doesn t differentiate members of the MTBC Some substrains of M. bovis BCG lack MPT64 and will be negative Strains of microbes, such as S. aureus, that produce protein A may produce a false positive result Turn around time Reporting 15 minutes N/A. Part of the identification of positive cultures
46
47 Identification of mycobacteria Level of identification Identification as MTBC Differentiation within MTBC: not differentiated by Xpert MTB/RIF, Hain MTBDRplus Specialised testing LPA for MTBC differentiation, PCR Region of Differences, Sequencing Could be useful in the context of BCG studies NTM may or may not be identified to species level
48 Nucleic acid amplification tests (NAAT): Specimen GeneXpert Direct tests Processing GeneXpert LPA (Hain) Culture Further tests if positive culture LPA (Hain)
 e.g.")
49 Nucleic acid amplification tests (NAAT) Many commercially available Most used TB high burden countries: GeneXpert Line probe assays (LPA) e.g. Hain MTBDRplus Detection of MTB Detection of drug resistance
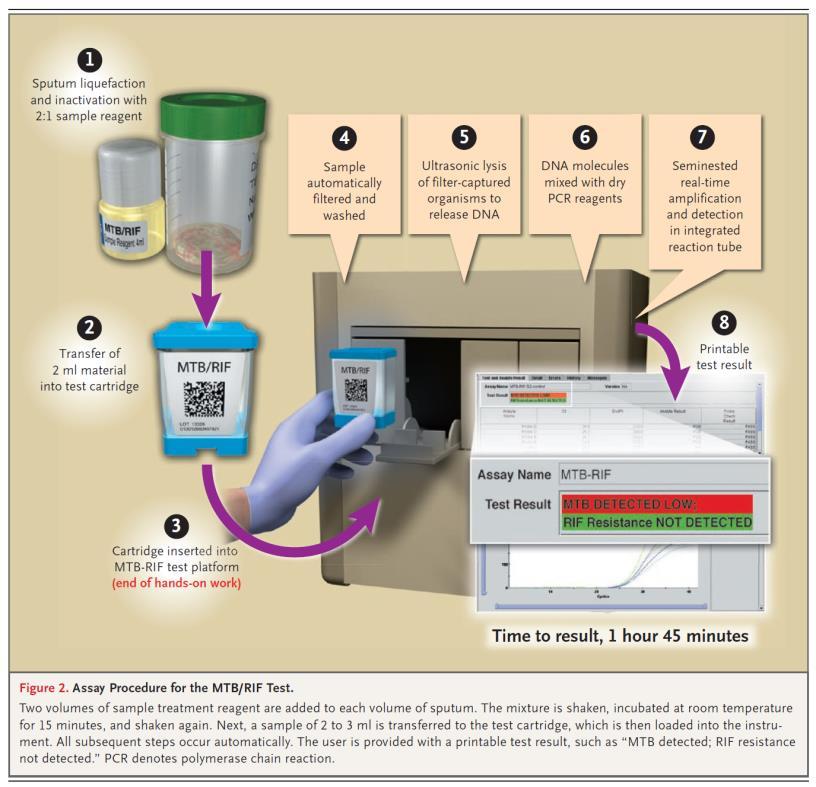
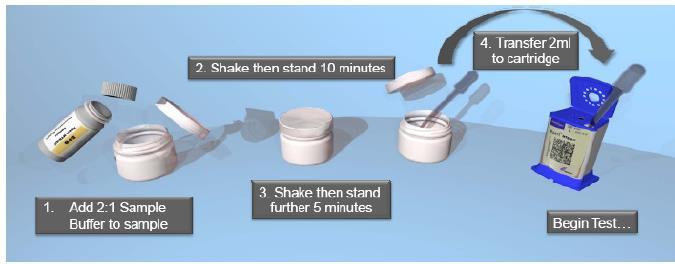
50
51
52 Test/Procedure Type/Example Principle Nucleic acid amplification test GeneXpert MTB/RIF (Cepheid) Cartridge-based assay that integrates sample preparation, amplification, and detection of DNA. Real time PCR using molecular beacons (5 probes). Designed to identify RIF resistance mutations in an 81-bp region of rpob gene: Rifampicin-resistance-determining region (RRDR) Done On direct specimen or processed specimen (sediment) Sensitivity Specificity Limitations Turn around time Cochrane adults 2014: For TB detection as smear replacement: Se 89% Sp 99% As add-on test after negative smear: Se 67% Sp 99% For RIF R detection: Se 95% Sp 98% Lancet Resp Med 2015 SR MA children: Compared to culture: Se 62% sputum 66% GL; Sp 98% For RIF R detection: Se 86% Sp 98% Initial high Se and Sp for detecting TB and DR, but afterwards concerns for false pos R other test to confirm DR (LPA, phenotypic). Also false negatives 2h

53 For RIF R detection: Se 95% Sp 98% If pooled accuracy are applied to a hypothetical cohort of 1000 individuals where: 15% of those with symptoms are rifampicin resistant: Xpert MTB/RIF would correctly identify 143 individuals as RIF R and miss 8 cases correctly identify 833 individuals as RIF S and misclassify 17 individuals as R 5% of those with symptoms are rifampicin resistant, Xpert MTB/RIF would correctly identify 48 individuals as RIF R and miss 3 cases correctly identify 931 individuals as RIF S and misclassify 19 individuals as R
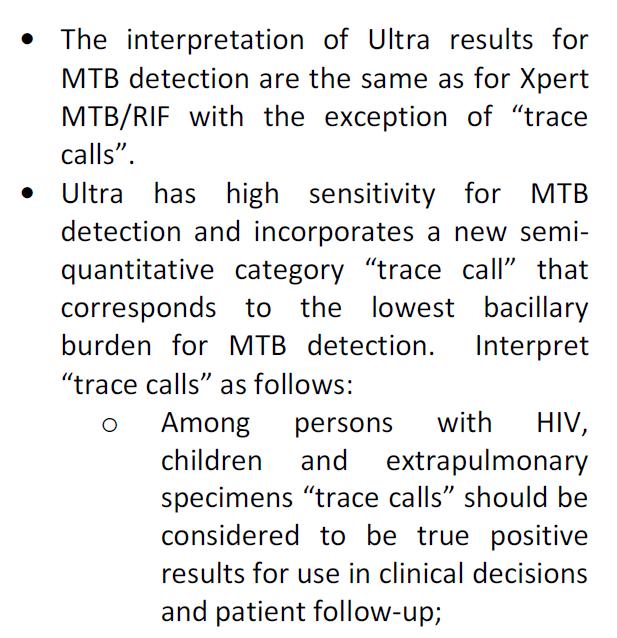
54 Xpert MTB/RIF Ultra Improved limit of detection 16 CFU/ml vs 114 CFU/ml Xpert MTB/RIF Culture ~ Smear microscopy ~ An additional semi-quantitative category ( trace ) to take into account the higher sensitivity Lowest bacillary burden for TB detection Updated categories: high, medium, low, very low and trace
55 Ultra Ultra vs standard Xpert in 1520 adults Se Ultra 5% higher than Xpert Highest in smear negative patients and HIV infected Sp Ultra 3.2% lower than Xpert Lowest in patients with history of TB. Detects non-viable bacilli. Problem in high endemic setting. The impact of increased sensitivity results in decreased specificity for TB detection and becomes a trade-off between increased diagnosis and overtreatment As good accuracy for RIF detection
56 Ultra For EPTB and paediatric TB: Se due to trace-call Se Ultra 95% vs 45% Xpert in TBM Se Ultra 71% vs 47% Xpert resp specimens children Positive Xpert Negative Culture
57
58
59 Nucleic acid amplification tests (NAAT): Specimen GeneXpert Direct tests Processing GeneXpert LPA (Hain) Culture Further tests if positive culture LPA (Hain)
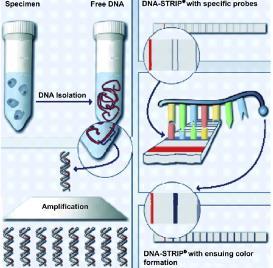
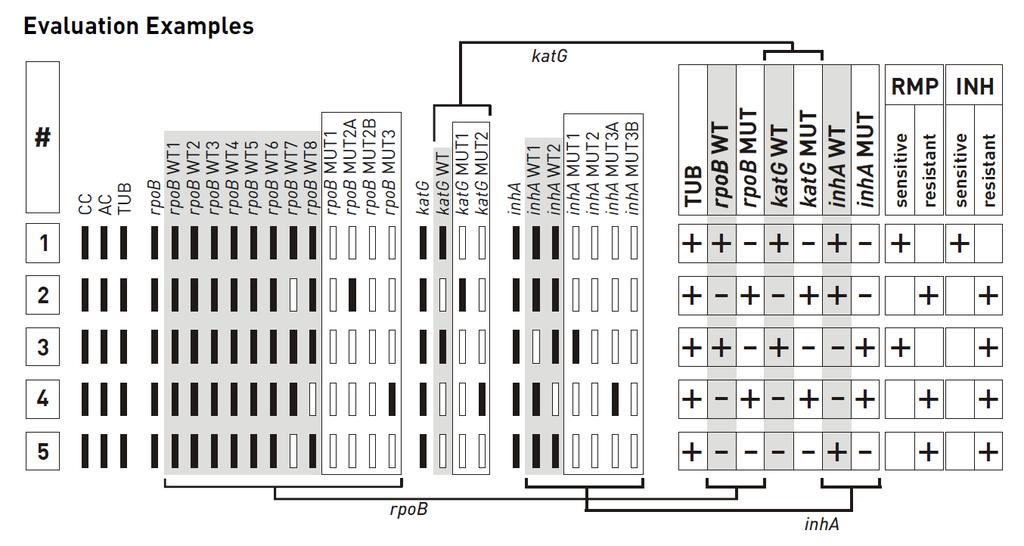
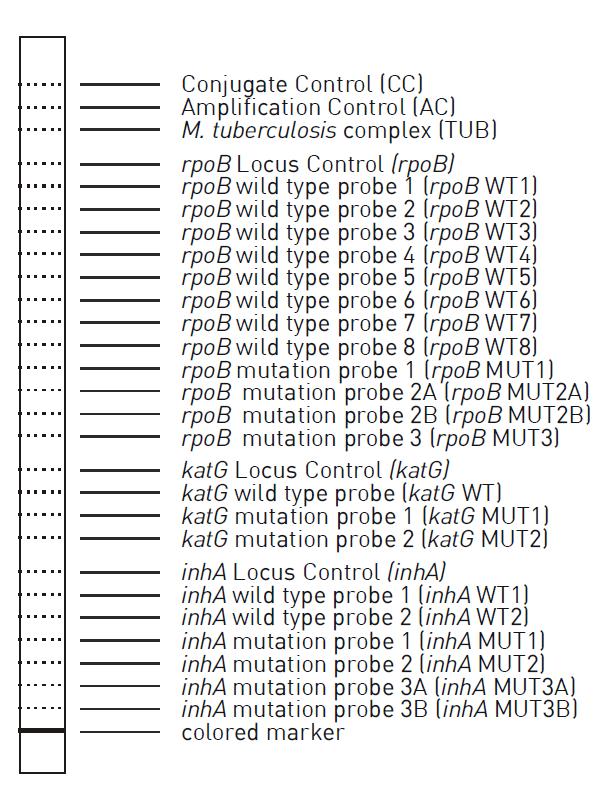
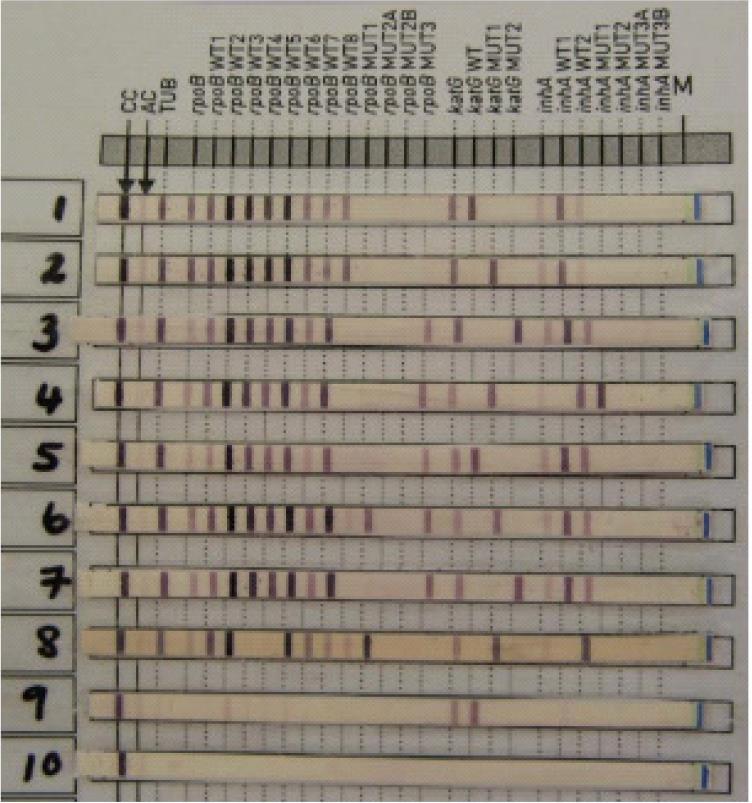
60 Test/Procedure Nucleic acid amplification test: Line Probe Assays Type/Example Hain MTBDRplus to detect MDR-TB by detecting mutations in rpob gene (RIF) and katg and inha (INH) Hain MTBDRsl to detect XDR-TB by detecting mutations in genes for susceptibility to FQs (ofloxacin, moxi, levo) and second line injectable drugs (SLIDs; amikacin, kanamycin,and capreomycin) Principle Hybridization of labeled amplicons (amplified by PCR from M. tuberculosis DNA present in patient specimens) to oligonucleotide probes arranged on a membrane strip Done On processed specimen (sediment) from smear positive or negative patient OR on positive culture Sensitivity Specificity See next slides Limitations Open tube format: possible cross contamination Requires appropriate laboratory infrastructure and equipment Reading strips: possible subjectivity LPAs are less sensitive for the detection of isoniazid resistance Turn around time 24-48h



61
62
63 RIF resistance WHO Policy update LPA INH RIF 2016 Test accuracy LPA for direct testing compared with phenotypic RIF DST (done on sputum): Sensitivity: 0.96 (95% CI: ) Specificity: 0.98 (95% CI: ) Test accuracy LPA for indirect testing compared with phenotypic RIF DST (done on culture): Sensitivity: 0.97 (95% CI: ) Specificity: 0.99 (95% CI: )
64 INH resistance Resistance-conferring mutations in inha and katg genes account 90% of INH R detected by phenotypic DST Test accuracy LPA for direct testing compared with phenotypic INH DST (done on sputum): Sensitivity: 0.89 (95% CI: ) Specificity: 0.98 (95% CI: ) Test accuracy LPA for indirect testing compared with phenotypic INH DST (done on culture): Sensitivity: 0.91 (95% CI: ) Specificity: 1.00 (95% CI: ) Conventional culture-based DST should be used in the follow-up evaluation of patients with a high risk for INH R and a negative LPA result, especially in settings with a high pre-test probability of INH R A 90% prevalence of INH R likely in a population of MDRTB patients when a patient is diagnosed by the Xpert MTB/RIF assay


65 Hain MTBDRsl
66 VERSION 1 (compared to culture based DST) 26 studies FQ R: direct testing, MTBDRsl Se 86.2% Sp 98.6% smear-positive specimen FQ R: indirect testing, MTBDRsl Se 85.6% Sp 98.5% smear-positive specimen SLID R: direct testing, MTBDRsl Se 87.0% Sp 99.5% smear-positive specimen SLID R: indirect testing, MTBDRsl Se 76.5% Sp 99.1% smear-positive specimen XDR-TB: direct testing, MTBDRsl Se 69.4% Sp 99.4% smear-positive specimen XDR-TB: indirect testing, MTBDRsl Se 70.9% Sp 98.8% smear-positive specimen VERSION 2 (compared to culture based DST) 1 study FQ R: direct testing, MTBDRsl Se 97% Sp 98% smear-positive specimen Se 80% Sp 100% smear-negative specimen SLID R: direct testing, MTBDRsl Se 89% Sp 90% smear-positive specimen Se 80% Sp 100% smear-negative specimen XDR-TB: direct testing, MTBDRsl Se 79% Sp 97% smear-positive specimen Se 50% Sp 100% smear-negative specimen
67 2016
68
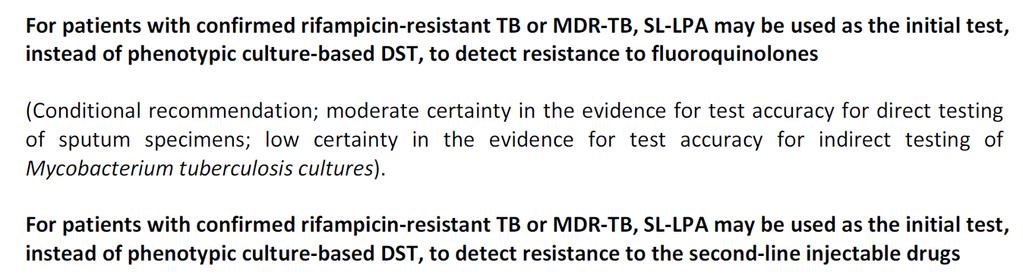
69 Line Probe Assays First-line line probe assay (FL-LPA) Detects MTB and assesses resistance to RIF and INH Commercial examples of this test: GenoType MTBDRplus (Hain Lifescience, Germany) NTM+MDRTB Detection Kit (NIPRO Corporation, Japan) WHO: FL-LPA is suitable for use on culture isolates and AFB smear-positive sputum specimens Second-line line probe assays (SL-LPA) Detects MTB and assesses resistance to FQs and SLIDs Commercial example of this test: GenoType MTBDRsl test (Hain Lifescience, Germany) WHO: Diagnostic accuracy is similar when SL-LPA is performed directly on sputum or from cultured isolates. SL- LPA can be used on smear-positive or smear-negative specimens although a higher indeterminate rate will occur when testing smear-negative specimens.
70
71 Specimen Processing Direct tests Drug susceptibility testing (DST) Culture Further tests if positive culture Drug susceptibility testing (DST)
72 Drug susceptibility testing (DST) Genotypic (molecular) testing is based on detecting the presence of wild-type sequences or mutations in genes known to be associated with antibiotic susceptibility or resistance Can be done on sample or on positive culture GeneXpert LPA: Hain MTBDRplus and MTBDRsl Whole genome sequencing
 or on culture (indirect) On liquid culture or on solid culture Methods: proportion method (most used), absolute concentration")
73 Drug susceptibility testing (DST) Phenotypic testing is based on whether or not the organism can grow in the presence of the antibiotic. Can be done: On sample (direct) or on culture (indirect) On liquid culture or on solid culture Methods: proportion method (most used), absolute concentration method, and resistant ratio method
74 %20line%20drugs.pdf
75 Plate bacteria on media containing No drugs Critical concentrations of a drug Incubate for 3 weeks Count colonies Isolate is R if the # of colonies on drug-containing media is >1% of the colonies on drug-free media
76 The isolate is considered resistant if the number of colonies in the drug quadrant is equal to or more than 1% of that in the control quadrant
.")

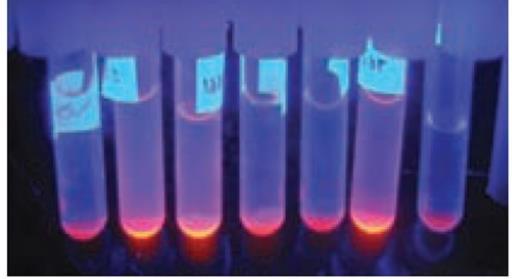
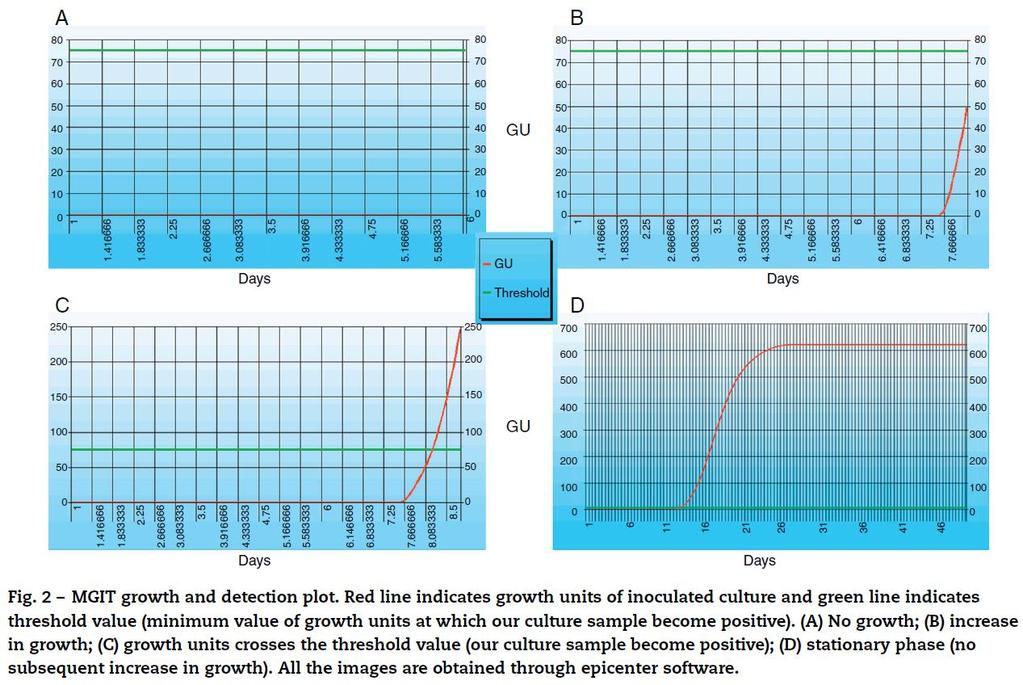
77 MGIT DST is a modified proportion method Results in 4-14 days after the test is set up The method is based on the fluorescence produced from reduced oxygen in the MGIT medium due to microbial growth. The fluorescence generated is then converted to growth units (GU). In general, more GU indicates more growth. When the growth control generates GU to 400 within 4-14 days, the DST is valid for interpretation: If a drug-containing MGIT tube yields GU<100, the organism is interpreted as being susceptible If GU is 100, the organism is considered resistant. Growth Control tube STR INH RIF EMB

78 Minimum inhibitory concentration (MIC) is the lowest concentration of an antimicrobial drug that will inhibit the visible growth of a microorganism
79 Drug susceptibility testing (DST) Discordants Different genotypic tests Different phenotypic tests Genotypic and phenotypic tests Clinical response to treatment Difficult to compare different methods done in different laboratories on different specimens Complex and evolving field Role for both phenotypic and genotypic methods Phenotypic DST still considered gold standard for now

80 Gold standard
81
82 Specimen Processing Direct tests Whole genome sequencing Culture Further tests if positive culture Whole genome sequencing
83 Phases of laboratory testing Post-Analytical
84 Lab report Important to understand what tests are done Challenging Requires understanding of the different tests done in the TB laboratory Results can be complex, especially for MDR-TB when drug susceptibility results done by different methods Verify results for all specimens collected Verify final reports Contact laboratory if unclear
85 Specimen Processing Direct tests Culture Further tests if positive culture Questions?
86 QUESTION Which statement is false? 1) A smear can only be on a concentrated specimen 2) It is normal for the TB laboratory to have some cultures that are reported as contaminated 3) Drug susceptibility testing can be done by genotypic (molecular) or phenotypic methods
TB 101 Disease, Clinical Assessment and Lab Testing
 TB 101 Disease, Clinical Assessment and Lab Testing Pacific Islands Tuberculosis Controllers Association Conference (PITCA) Clinical Laboratory Breakout None Disclosure Objectives Be able to list and explain
TB 101 Disease, Clinical Assessment and Lab Testing Pacific Islands Tuberculosis Controllers Association Conference (PITCA) Clinical Laboratory Breakout None Disclosure Objectives Be able to list and explain
Ken Jost, BA, has the following disclosures to make:
 Diagnosis of TB Disease: Laboratory Ken Jost, BA May 10, 2017 TB Intensive May 9-12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Ken Jost, BA, has the following disclosures to make: No conflict
Diagnosis of TB Disease: Laboratory Ken Jost, BA May 10, 2017 TB Intensive May 9-12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Ken Jost, BA, has the following disclosures to make: No conflict
TB Intensive San Antonio, Texas November 11 14, 2014
 TB Intensive San Antonio, Texas November 11 14, 2014 Diagnosis of TB: Laboratory Ken Jost, BA November 12, 2014 Ken Jost, BA has the following disclosures to make: No conflict of interests No relevant
TB Intensive San Antonio, Texas November 11 14, 2014 Diagnosis of TB: Laboratory Ken Jost, BA November 12, 2014 Ken Jost, BA has the following disclosures to make: No conflict of interests No relevant
Diagnosis of TB: Laboratory Ken Jost Tuesday April 9, 2013
 TB Nurse Case Management San Antonio, Texas April 9-11, 2013 Diagnosis of TB: Laboratory Ken Jost Tuesday April 9, 2013 Ken Jost has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas April 9-11, 2013 Diagnosis of TB: Laboratory Ken Jost Tuesday April 9, 2013 Ken Jost has the following disclosures to make: No conflict of interests No relevant
TB/HIV 2 sides of the same coin. Dr. Shamma Shetye, MD Microbiology Metropolis Healthcare, Mumbai
 TB/HIV 2 sides of the same coin Dr. Shamma Shetye, MD Microbiology Metropolis Healthcare, Mumbai Global- Tb new cases Diagnosis-Microscopy ZN,Flourescent microscopy(fm) Rapid, inexpensive test Specificity>95%
TB/HIV 2 sides of the same coin Dr. Shamma Shetye, MD Microbiology Metropolis Healthcare, Mumbai Global- Tb new cases Diagnosis-Microscopy ZN,Flourescent microscopy(fm) Rapid, inexpensive test Specificity>95%
Diagnosis of TB: Laboratory Ken Jost Tuesday April 1, 2014
 TB Nurse Case Management San Antonio, Texas April 1 3, 2014 Diagnosis of TB: Laboratory Ken Jost Tuesday April 1, 2014 Ken Jost, BA has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas April 1 3, 2014 Diagnosis of TB: Laboratory Ken Jost Tuesday April 1, 2014 Ken Jost, BA has the following disclosures to make: No conflict of interests No relevant
MIC = Many Inherent Challenges Sensititre MIC for Antimicrobial Susceptibility Testing of Mycobacterium tuberculosis complex
 MIC = Many Inherent Challenges Sensititre MIC for Antimicrobial Susceptibility Testing of Mycobacterium tuberculosis complex Marie Claire Rowlinson, PhD D(ABMM) Florida Bureau of Public Health Laboratories
MIC = Many Inherent Challenges Sensititre MIC for Antimicrobial Susceptibility Testing of Mycobacterium tuberculosis complex Marie Claire Rowlinson, PhD D(ABMM) Florida Bureau of Public Health Laboratories
Stacy White, PhD May 12, TB for Community Providers. Phoenix, Arizona
 Role of the Laboratory in TB Diagnosis Stacy White, PhD May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Stacy White, PhD has the following disclosures
Role of the Laboratory in TB Diagnosis Stacy White, PhD May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Stacy White, PhD has the following disclosures
Mycobacterial cell wall. Cell Cycle Lengths. Outline of Laboratory Methods. Laboratory Methods
 Laboratory Methods Cell Cycle Lengths Generation time (hrs) Days needed for 26 generations (colony) E. coli 0.33 0.36 Nancy Connell, PhD Professor, nfectious Disease Department of Medicine Center for Emerging
Laboratory Methods Cell Cycle Lengths Generation time (hrs) Days needed for 26 generations (colony) E. coli 0.33 0.36 Nancy Connell, PhD Professor, nfectious Disease Department of Medicine Center for Emerging
TB Laboratory for Nurses
 TB Laboratory for Nurses Shea Rabley, RN, MN Consultant Mayo Clinic Center for Tuberculosis 2014 MFMER slide-1 Disclosures None 2014 MFMER slide-2 Objectives Participants will be able to: 1. Name 2 safety
TB Laboratory for Nurses Shea Rabley, RN, MN Consultant Mayo Clinic Center for Tuberculosis 2014 MFMER slide-1 Disclosures None 2014 MFMER slide-2 Objectives Participants will be able to: 1. Name 2 safety
CDPH - CTCA Joint Guidelines Guideline for Micobacteriology Services In California
 CDPH - CTCA Joint Guidelines Guideline for Micobacteriology Services In California These guidelines are intended to be used as an educational aid to help clinicians make informed decisions about patient
CDPH - CTCA Joint Guidelines Guideline for Micobacteriology Services In California These guidelines are intended to be used as an educational aid to help clinicians make informed decisions about patient
Overview of Mycobacterial Culture, Identification, and Drug Susceptibility Testing
 Overview of Mycobacterial Culture, Identification, and Drug Susceptibility Testing 1. Essentials for the Mycobacteriology Laboratory: Promoting Quality Practices 1.1 Overview: Mycobacterial Culture, Identification,
Overview of Mycobacterial Culture, Identification, and Drug Susceptibility Testing 1. Essentials for the Mycobacteriology Laboratory: Promoting Quality Practices 1.1 Overview: Mycobacterial Culture, Identification,
Drug susceptibility testing for tuberculosis KRISTEN DICKS, MD, MPH DUKE UNIVERSITY MEDICAL CENTER
 Drug susceptibility testing for tuberculosis KRISTEN DICKS, MD, MPH DUKE UNIVERSITY MEDICAL CENTER Outline Drug resistant TB: definitions and epidemiology How does TB become resistant? Current drug susceptibility
Drug susceptibility testing for tuberculosis KRISTEN DICKS, MD, MPH DUKE UNIVERSITY MEDICAL CENTER Outline Drug resistant TB: definitions and epidemiology How does TB become resistant? Current drug susceptibility
TB Nurse Case Management. March 7-9, Diagnosis of TB: Ken Jost Wednesday March 7, 2012
 TB Nurse Case Management San Antonio, Texas March 7-9, 2012 Diagnosis of TB: Laboratory Ken Jost Wednesday March 7, 2012 Ken Jost has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas March 7-9, 2012 Diagnosis of TB: Laboratory Ken Jost Wednesday March 7, 2012 Ken Jost has the following disclosures to make: No conflict of interests No relevant
DST for detection of DR TB - roll out of Xpert in South Africa and overview of other technologies: what are the gaps?
 DST for detection of DR TB - roll out of Xpert in South Africa and overview of other technologies: what are the gaps? Mark Nicol Division of Medical Microbiology and Institute for Infectious Diseases and
DST for detection of DR TB - roll out of Xpert in South Africa and overview of other technologies: what are the gaps? Mark Nicol Division of Medical Microbiology and Institute for Infectious Diseases and
Epidemiology and diagnosis of MDR-TB in children H Simon Schaaf
 Epidemiology and diagnosis of MDR-TB in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Definitions
Epidemiology and diagnosis of MDR-TB in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Definitions
WELCOME. Lab Talk: What a Nurse Hears. April 18, NTNC Annual Meeting Lab Talk: What a Nurse Hears
 Lab Talk: What a Lab Talk: What a Max Salfinger, MD, FIDSA, FAAM Executive Director, Advanced Diagnostic Laboratories Laboratory Director, Mycobacteriology & Pharmacokinetics National Jewish Health Lisa
Lab Talk: What a Lab Talk: What a Max Salfinger, MD, FIDSA, FAAM Executive Director, Advanced Diagnostic Laboratories Laboratory Director, Mycobacteriology & Pharmacokinetics National Jewish Health Lisa
Diagnosis of drug resistant TB
 Diagnosis of drug resistant TB Megan Murray, MD, ScD Harvard School of Public Health Brigham and Women s Hospital Harvard Medical School Broad Institute Global burden of TB 9 million new cases year 2 million
Diagnosis of drug resistant TB Megan Murray, MD, ScD Harvard School of Public Health Brigham and Women s Hospital Harvard Medical School Broad Institute Global burden of TB 9 million new cases year 2 million
Laboratory Diagnostic Techniques. Hugo Donaldson Consultant Microbiologist Imperial College Healthcare NHS Trust
 Laboratory Diagnostic Techniques Hugo Donaldson Consultant Microbiologist Imperial College Healthcare NHS Trust Learning Objectives 1) When to consider a diagnosis of TB 2) When to consider a referral
Laboratory Diagnostic Techniques Hugo Donaldson Consultant Microbiologist Imperial College Healthcare NHS Trust Learning Objectives 1) When to consider a diagnosis of TB 2) When to consider a referral
A retrospective evaluation study of diagnostic accuracy of Xpert MTB/RIF assay, used for detection of Mycobacterium tuberculosis in Greece
 Örebro University School of Health and Medical Science Biomedical Laboratory Science Programme 180 credits Degree project in biomedical laboratory science, advanced course, 15 credits May 21, 2015 A retrospective
Örebro University School of Health and Medical Science Biomedical Laboratory Science Programme 180 credits Degree project in biomedical laboratory science, advanced course, 15 credits May 21, 2015 A retrospective
Frances Jamieson, MD and Kevin May, BSc November 15 th,
 Frances Jamieson, MD and Kevin May, BSc November 15 th, 2016 1 TB Elimination: Back To Basics Financial Interest Disclosure (over the past 24 months) Dr. Frances amieson Company Speaker Advisory Research
Frances Jamieson, MD and Kevin May, BSc November 15 th, 2016 1 TB Elimination: Back To Basics Financial Interest Disclosure (over the past 24 months) Dr. Frances amieson Company Speaker Advisory Research
Xpert MTB/RIF Ultra: Understanding this new diagnostic and who will have access to it
 Xpert MTB/RIF Ultra: Understanding this new diagnostic and who will have access to it Angela Starks, PhD Chief, Laboratory Branch Division of TB Elimination Matt Bankowski, PhD, MS, D(ABMM), HCLD/CC(ABB)
Xpert MTB/RIF Ultra: Understanding this new diagnostic and who will have access to it Angela Starks, PhD Chief, Laboratory Branch Division of TB Elimination Matt Bankowski, PhD, MS, D(ABMM), HCLD/CC(ABB)
When good genes go bad
 When good genes go bad Dr Kessendri Reddy NHLS Tygerberg Hospital Division of Clinical Microbiology Fakulteit Geneeskunde en Gesondheidswetenskappe Faculty of Medicine and Health Sciences Overview Cases
When good genes go bad Dr Kessendri Reddy NHLS Tygerberg Hospital Division of Clinical Microbiology Fakulteit Geneeskunde en Gesondheidswetenskappe Faculty of Medicine and Health Sciences Overview Cases
The ABC s of AFB s Laboratory Testing for Tuberculosis. Gary Budnick Connecticut Department of Public Health Mycobacteriology Laboratory
 The ABC s of AFB s Laboratory Testing for Tuberculosis Gary Budnick Connecticut Department of Public Health Mycobacteriology Laboratory Laboratory TAT Goals Case Study Specimen Collection Testing Contact
The ABC s of AFB s Laboratory Testing for Tuberculosis Gary Budnick Connecticut Department of Public Health Mycobacteriology Laboratory Laboratory TAT Goals Case Study Specimen Collection Testing Contact
Diagnosis and Management of Active Tuberculosis
 Diagnosis and Management of Active Tuberculosis Zelalem Temesgen, MD FIDSA AAHIVS 2013 MFMER slide-1 Disclosures None 2013 MFMER slide-2 Objectives By the end of this session, participants should be able
Diagnosis and Management of Active Tuberculosis Zelalem Temesgen, MD FIDSA AAHIVS 2013 MFMER slide-1 Disclosures None 2013 MFMER slide-2 Objectives By the end of this session, participants should be able
How best to structure a laboratory network with new technologies
 How best to structure a laboratory network with new technologies Cristina Gutierrez, MD, PhD Uniting to scale up TB care in Central Asia 14 and 15 April 2011 Tashkent, Uzbekistan New laboratory diagnostics
How best to structure a laboratory network with new technologies Cristina Gutierrez, MD, PhD Uniting to scale up TB care in Central Asia 14 and 15 April 2011 Tashkent, Uzbekistan New laboratory diagnostics
CULTURE OR PCR WHAT IS
 CULTURE OR PCR WHAT IS BEST FOR AFRICA? Peter R Mason BRTI TB IN AFRICA GLOBAL 9 MILLION NEW CASES/YR 1.5 MILLION TB DEATHS AFRICA 95% TB DEATHS IN LMIC 9/22 HIGH BURDEN COUNTRIES IN AFRICA STRONG LINK
CULTURE OR PCR WHAT IS BEST FOR AFRICA? Peter R Mason BRTI TB IN AFRICA GLOBAL 9 MILLION NEW CASES/YR 1.5 MILLION TB DEATHS AFRICA 95% TB DEATHS IN LMIC 9/22 HIGH BURDEN COUNTRIES IN AFRICA STRONG LINK
Microscopic Morphology in Smears Prepared from MGIT Broth Medium for Rapid Presumptive Identification of Mycobacterium tuberculosis
 Annals of Clinical & Laboratory Science, vol. 33, no. 2, 2003 179 Microscopic Morphology in Smears Prepared from MGIT Broth Medium for Rapid Presumptive Identification of Mycobacterium tuberculosis complex,
Annals of Clinical & Laboratory Science, vol. 33, no. 2, 2003 179 Microscopic Morphology in Smears Prepared from MGIT Broth Medium for Rapid Presumptive Identification of Mycobacterium tuberculosis complex,
Online Annexes (5-8)
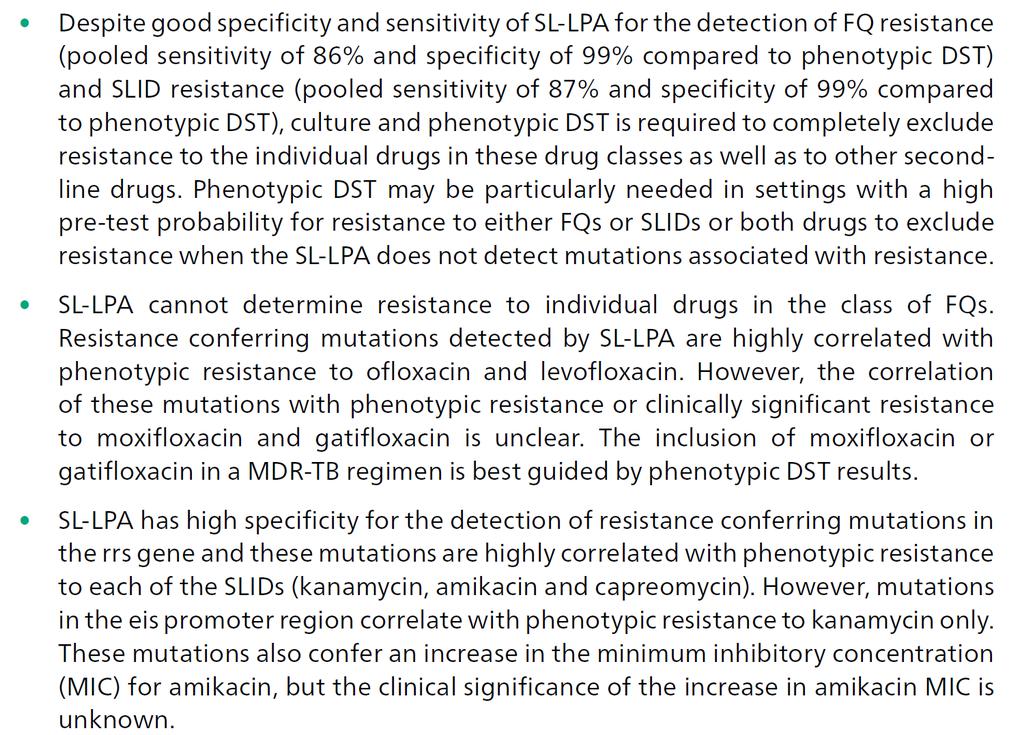
") Online Annexes (5-8) to WHO Policy guidance: The use of molecular line probe assay for the detection of resistance to second-line anti-tuberculosis drugs THE END TB STRATEGY Online Annexes (5-8) to WHO
Online Annexes (5-8) to WHO Policy guidance: The use of molecular line probe assay for the detection of resistance to second-line anti-tuberculosis drugs THE END TB STRATEGY Online Annexes (5-8) to WHO
Evaluation of the Microscopic-Observation. Drug-Susceptibility Assay Drugs Concentration for Detection Of Multidrug-Resistant Tuberculosis
 Evaluation of the Microscopic-Observation Drug-Susceptibility Assay Drugs Concentration for Detection Of Multidrug-Resistant Tuberculosis ABSTRACT New diagnostic tools are urgently needed to interrupt
Evaluation of the Microscopic-Observation Drug-Susceptibility Assay Drugs Concentration for Detection Of Multidrug-Resistant Tuberculosis ABSTRACT New diagnostic tools are urgently needed to interrupt
PCR and direct amplification for tuberculosis diagnosis. Emmanuelle CAMBAU University Paris Diderot, APHP, Saint Louis-Lariboisière Hospital,
 PCR and direct amplification for tuberculosis diagnosis Emmanuelle CAMBAU University Paris Diderot, APHP, Saint Louis-Lariboisière Hospital, Paris, France Educational Workshop 05- ECCMID 2015 Copenhagen
PCR and direct amplification for tuberculosis diagnosis Emmanuelle CAMBAU University Paris Diderot, APHP, Saint Louis-Lariboisière Hospital, Paris, France Educational Workshop 05- ECCMID 2015 Copenhagen
Receipt within 1 day of specimen collection. Report AFB b smear result within 1 day from receipt of specimen
 Recommendation Promote rapid delivery of specimens to the laboratory Use fluorescent acid-fast staining and promptly transmit results by phone, FAX, or electronically Identify growth as acid-fast and use
Recommendation Promote rapid delivery of specimens to the laboratory Use fluorescent acid-fast staining and promptly transmit results by phone, FAX, or electronically Identify growth as acid-fast and use
Objectives. TB Laboratory Methods
 TB Laboratory Methods Beverly Metchock, Dr.P.H., D(ABMM) Team Leader, Reference Laboratory, Mycobacteriology Laboratory Branch February 2011 Objectives General overview of mycobacteriology (TB) lab practices
TB Laboratory Methods Beverly Metchock, Dr.P.H., D(ABMM) Team Leader, Reference Laboratory, Mycobacteriology Laboratory Branch February 2011 Objectives General overview of mycobacteriology (TB) lab practices
Research Methods for TB Diagnostics. Kathy DeRiemer, PhD, MPH University of California, Davis Shanghai, China: May 8, 2012
 Research Methods for TB Diagnostics Kathy DeRiemer, PhD, MPH University of California, Davis Shanghai, China: May 8, 2012 Overview Why do we need good TB diagnostics? What works? What doesn t work? How
Research Methods for TB Diagnostics Kathy DeRiemer, PhD, MPH University of California, Davis Shanghai, China: May 8, 2012 Overview Why do we need good TB diagnostics? What works? What doesn t work? How
MYCOBACTERIA. Pulmonary T.B. (infect bird)
") MYCOBACTERIA SPP. Reservoir Clinical Manifestation Mycobacterium tuberculosis Human Pulmonary and dissem. T.B. M. lepra Human Leprosy M. bovis Human & cattle T.B. like infection M. avium Soil, water, birds,
MYCOBACTERIA SPP. Reservoir Clinical Manifestation Mycobacterium tuberculosis Human Pulmonary and dissem. T.B. M. lepra Human Leprosy M. bovis Human & cattle T.B. like infection M. avium Soil, water, birds,
Online Annexes (5-8)
") 2016 Online Annexes (5-8) to WHO Policy guidance: The use of molecular line probe assay for the detection of resistance to second-line anti-tuberculosis drugs 1 Contents: Annex 5: GRADE summary of findings
2016 Online Annexes (5-8) to WHO Policy guidance: The use of molecular line probe assay for the detection of resistance to second-line anti-tuberculosis drugs 1 Contents: Annex 5: GRADE summary of findings
Frances Morgan, PhD October 21, Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS
 The Laboratory s Role in Caring for Patients Diagnosed with TB Frances Morgan, PhD October 21, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
The Laboratory s Role in Caring for Patients Diagnosed with TB Frances Morgan, PhD October 21, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Role of the Laboratory in TB Diagnosis and Management
 Role of the Laboratory in TB Diagnosis and Management Michael Pentella, Ph.D., D(ABMM), CIC Associate Director University Hygienic Lab Clinical Associate Professor, College of Public Health, University
Role of the Laboratory in TB Diagnosis and Management Michael Pentella, Ph.D., D(ABMM), CIC Associate Director University Hygienic Lab Clinical Associate Professor, College of Public Health, University
INTENSIFIED TB CASE FINDING
 INTENSIFIED TB CASE FINDING My friends call me Intensified Case Finding (ICF) I undertake regularly screening all people with, or at high risk of HIV, for symptoms of TB in health care facilities, communities
INTENSIFIED TB CASE FINDING My friends call me Intensified Case Finding (ICF) I undertake regularly screening all people with, or at high risk of HIV, for symptoms of TB in health care facilities, communities
WSLH Testing and Surveillance Updates
 WSLH Testing and Surveillance Updates Wisconsin Mycobacteriology Laboratory Network annual conference November 4, 2015, Madison, WI Updates Outline Collection and Transport Smear and Culture Nucleic Acid
WSLH Testing and Surveillance Updates Wisconsin Mycobacteriology Laboratory Network annual conference November 4, 2015, Madison, WI Updates Outline Collection and Transport Smear and Culture Nucleic Acid
Research Article Factors Associated with Missed Detection of Mycobacterium tuberculosis by Automated BACTEC MGIT 960 System
 BioMed Research International Volume 2016, Article ID 5972021, 4 pages http://dx.doi.org/10.1155/2016/5972021 Research Article Factors Associated with Missed Detection of Mycobacterium tuberculosis by
BioMed Research International Volume 2016, Article ID 5972021, 4 pages http://dx.doi.org/10.1155/2016/5972021 Research Article Factors Associated with Missed Detection of Mycobacterium tuberculosis by
Laboratory Diagnosis and Antimicrobial Susceptibility Testing of Mycobacterium tuberculosis Complex. Objectives
 Laboratory Diagnosis and Antimicrobial Susceptibility Testing of Mycobacterium tuberculosis Complex Marie-Claire Rowlinson, PhD D(ABMM) Calin Chiribau, PhD, MT(ASCP) Florida Bureau of Public Health Laboratories
Laboratory Diagnosis and Antimicrobial Susceptibility Testing of Mycobacterium tuberculosis Complex Marie-Claire Rowlinson, PhD D(ABMM) Calin Chiribau, PhD, MT(ASCP) Florida Bureau of Public Health Laboratories
Evaluation of Genxpert Real Time PCR POC in the Diagnosis of Multidrug Resistant TB Among Patients Attending NTBLTC Saye-Zaria Nigeria
 RESEARCH ARTICLE Open Access Journal of Infectious Diseases and Pathogenesis ISSN 577-7939 Evaluation of Genxpert Real Time PCR POC in the Diagnosis of Multidrug Resistant TB Among Patients Attending NTBLTC
RESEARCH ARTICLE Open Access Journal of Infectious Diseases and Pathogenesis ISSN 577-7939 Evaluation of Genxpert Real Time PCR POC in the Diagnosis of Multidrug Resistant TB Among Patients Attending NTBLTC
Online Annexes (2-4)
") Online Annexes (2-4) to WHO Policy update: The use of molecular line probe assays for the detection of resistance to isoniazid and rifampicin THE END TB STRATEGY Online Annexes (2-4) to WHO Policy update:
Online Annexes (2-4) to WHO Policy update: The use of molecular line probe assays for the detection of resistance to isoniazid and rifampicin THE END TB STRATEGY Online Annexes (2-4) to WHO Policy update:
Xpert MTB/RIF Training. Indira Soundiram 2012
 Xpert MTB/RIF Training Indira Soundiram 2012 A Better Way to Platform Design GeneXpert Infinity-48 GeneXpert Module GX-I GX-II GX-IV GX-XVI 2 Defining Molecular Diagnostics Any Test Any Time Any Sample
Xpert MTB/RIF Training Indira Soundiram 2012 A Better Way to Platform Design GeneXpert Infinity-48 GeneXpert Module GX-I GX-II GX-IV GX-XVI 2 Defining Molecular Diagnostics Any Test Any Time Any Sample
Public Health Mycobacteriology (TB) Laboratory Testing Services
 Laboratory Testing Services") Public Health Mycobacteriology (TB) Laboratory Testing Services Gary Budnick Supervising Microbiologist Connecticut Department of Public Health Laboratory Branch Hartford, Connecticut Specimen Collection
Public Health Mycobacteriology (TB) Laboratory Testing Services Gary Budnick Supervising Microbiologist Connecticut Department of Public Health Laboratory Branch Hartford, Connecticut Specimen Collection
Guidelines for Tuberculosis Control in New Zealand 2010 Chapter 11: Mycobacteriology: Laboratory Methods and Standards
 Guidelines for Tuberculosis Control in New Zealand 2010 Chapter 11: Mycobacteriology: Laboratory Methods and Standards Ministry of Health. 2010. Guidelines for Tuberculosis Control in New Zealand 2010.
Guidelines for Tuberculosis Control in New Zealand 2010 Chapter 11: Mycobacteriology: Laboratory Methods and Standards Ministry of Health. 2010. Guidelines for Tuberculosis Control in New Zealand 2010.
Rapid Diagnostic Techniques for Identifying Tuberculosis Ken Jost November 13, 2008
 Tuberculosis Updates for Clinicians San Antonio, Texas November 13, 2008 Rapid Diagnostic Techniques for Identifying Tuberculosis Ken Jost November 13, 2008 Rapid Diagnostic Techniques for Identifying
Tuberculosis Updates for Clinicians San Antonio, Texas November 13, 2008 Rapid Diagnostic Techniques for Identifying Tuberculosis Ken Jost November 13, 2008 Rapid Diagnostic Techniques for Identifying
POSITIONING OF TB DX : TIERED SYSTEM, INTEGRATED APPROACH
 POSITIONING OF TB DX : TIERED SYSTEM, INTEGRATED APPROACH Akos Somoskövi, M.D., Ph.D. and Giorgio Roscigno, M.D. ANNUAL GLI MEETING, 4 th OCTOBER 2010 MERIEUX FOUNDATION, ANNECY Integrated Laboratory Network
POSITIONING OF TB DX : TIERED SYSTEM, INTEGRATED APPROACH Akos Somoskövi, M.D., Ph.D. and Giorgio Roscigno, M.D. ANNUAL GLI MEETING, 4 th OCTOBER 2010 MERIEUX FOUNDATION, ANNECY Integrated Laboratory Network
Harmonizing the Use of Molecular & Culture-based DST of Mycobacterium tuberculosis
 Harmonizing the Use of Molecular & Culture-based DST of Mycobacterium tuberculosis Grace Lin, MS. Research Scientist grace.lin@cdph.ca.gov APHL 8 th TB Lab Conference San Diego 8-19-13 Harmonizing? There
Harmonizing the Use of Molecular & Culture-based DST of Mycobacterium tuberculosis Grace Lin, MS. Research Scientist grace.lin@cdph.ca.gov APHL 8 th TB Lab Conference San Diego 8-19-13 Harmonizing? There
Molecular assays in Tuberculosis. Jatin Yegurla Junior resident
 Molecular assays in Tuberculosis Jatin Yegurla Junior resident 17-3-2018 Contents Introduction TB-PCR Line Probe assay (LPA) GenoType MTBDRsl test (Second line LPA) Xpert MTB/RIF (GeneXpert) (CB-NAAT)
Molecular assays in Tuberculosis Jatin Yegurla Junior resident 17-3-2018 Contents Introduction TB-PCR Line Probe assay (LPA) GenoType MTBDRsl test (Second line LPA) Xpert MTB/RIF (GeneXpert) (CB-NAAT)
TB is Local. Barry Chin, Boston Globe, 10/15/2008. * BUT only in appropriate setting
 Diagnosis of Tuberculosis 2012 New Tools, Tricks, Thinking? John Bernardo, M.D. Pulmonary Section, Boston University School of Medicine Massachusetts Department of Public Health Objectives To review the
Diagnosis of Tuberculosis 2012 New Tools, Tricks, Thinking? John Bernardo, M.D. Pulmonary Section, Boston University School of Medicine Massachusetts Department of Public Health Objectives To review the
The MODS Assay for Detection of TB and TB Drug Resistance: A Multi-center Study
 The MODS Assay for Detection of TB and TB Drug Resistance: A Multi-center Study microscopic observation drug susceptibility Susan E. Dorman, MD Johns Hopkins University Afranio L. Kritski, MD, PhD Federal
The MODS Assay for Detection of TB and TB Drug Resistance: A Multi-center Study microscopic observation drug susceptibility Susan E. Dorman, MD Johns Hopkins University Afranio L. Kritski, MD, PhD Federal
of clinical laboratory diagnosis in Extra-pulmonary Tuberculosis
 New approaches and the importance of clinical laboratory diagnosis in Extra-pulmonary Tuberculosis Bahrmand.AR, Hadizadeh Tasbiti.AR, Saifi.M, Yari.SH, Karimi.A, Fateh.A, Tuberculosis Dept. Pasteur Institute
New approaches and the importance of clinical laboratory diagnosis in Extra-pulmonary Tuberculosis Bahrmand.AR, Hadizadeh Tasbiti.AR, Saifi.M, Yari.SH, Karimi.A, Fateh.A, Tuberculosis Dept. Pasteur Institute
Mycobacteria Diagnostic Testing in Manitoba. Dr. Michelle Alfa Medical Director, DSM Clin Micro Discipline
 Mycobacteria Diagnostic Testing in Manitoba Dr. Michelle Alfa Medical Director, DSM Clin Micro Discipline Acknowlegements: Assunta Rendina: Charge Tech HSC Lab Joyce Wolf & Dr. Meenu Sharma: NML Dr. Kanchana
Mycobacteria Diagnostic Testing in Manitoba Dr. Michelle Alfa Medical Director, DSM Clin Micro Discipline Acknowlegements: Assunta Rendina: Charge Tech HSC Lab Joyce Wolf & Dr. Meenu Sharma: NML Dr. Kanchana
Diagnosis of Tuberculosis by GeneXpert MTB/RIF Assay Technology: A Short Review
 International Journal of Advanced Microbiology and Health Research www.ijamhr.com Volume 1; Issue 1; September 2017; Page No. 20-24 Review Article Diagnosis of Tuberculosis by GeneXpert MTB/RIF Assay Technology:
International Journal of Advanced Microbiology and Health Research www.ijamhr.com Volume 1; Issue 1; September 2017; Page No. 20-24 Review Article Diagnosis of Tuberculosis by GeneXpert MTB/RIF Assay Technology:
Health Care Worker Training on Roll Out New TB Diagnostic Test. Prepared by: City Health (J Caldwell) & NHLS (M Bosman & I Noordien)
 & NHLS (M Bosman & I Noordien)") Health Care Worker Training on Roll Out New TB Diagnostic Test Prepared by: City Health (J Caldwell) & NHLS (M Bosman & I Noordien) Overview Specimen Collection Investigations to request Sorting & registering
Health Care Worker Training on Roll Out New TB Diagnostic Test Prepared by: City Health (J Caldwell) & NHLS (M Bosman & I Noordien) Overview Specimen Collection Investigations to request Sorting & registering
Diagnosis of tuberculosis in children
 Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Communication between clinician and laboratory Molecular detection of M. tuberculosis complex
 3 Laboratory 3rd edition contributors: PENNAN M. BARRY, MD, MPH & SHOU-YEAN GRACE LIN, MS General information on TB laboratory work..................... 32 Molecular methods for detection of M. tuberculosis
3 Laboratory 3rd edition contributors: PENNAN M. BARRY, MD, MPH & SHOU-YEAN GRACE LIN, MS General information on TB laboratory work..................... 32 Molecular methods for detection of M. tuberculosis
GLI model TB diagnostic algorithms
 GLI model TB diagnostic algorithms GLI model TB diagnostic algorithms Revised June 2018 Contents Acknowledgements Abbreviations v vi Background 1 Algorithm 1: Preferred algorithm for universal patient
GLI model TB diagnostic algorithms GLI model TB diagnostic algorithms Revised June 2018 Contents Acknowledgements Abbreviations v vi Background 1 Algorithm 1: Preferred algorithm for universal patient
Molecular diagnosis of MDR-TB using GenoType MTBDRplus 96 assay in Ibadan, Nigeria
 Niger. J. Physiol. Sci. 28(December 2013) 187 191 www.njps.com.ng Molecular diagnosis of MDR-TB using GenoType MTBDRplus 96 assay in Ibadan, Nigeria * 1 Kehinde A.O. and 2 Adebiyi, E.O. Department of Medical
Niger. J. Physiol. Sci. 28(December 2013) 187 191 www.njps.com.ng Molecular diagnosis of MDR-TB using GenoType MTBDRplus 96 assay in Ibadan, Nigeria * 1 Kehinde A.O. and 2 Adebiyi, E.O. Department of Medical
AFB Identification Texas Approach
 AFB Identification Texas Approach Ken Jost Texas Department of State Health Services 6th National Conference on Laboratory Aspects of TB June 21, 2010 DSHS-Austin TB Lab Customers & Samples Year 2009 175
AFB Identification Texas Approach Ken Jost Texas Department of State Health Services 6th National Conference on Laboratory Aspects of TB June 21, 2010 DSHS-Austin TB Lab Customers & Samples Year 2009 175
TB Nurse Case Management Davenport, Iowa September 27 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Role of the Laboratory in the TB Diagnosis and Management Michael Pentella, PhD, MS, SM(ASCP), CIC, D(ABMM) September 27, 2011 Michael Pentella,
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Role of the Laboratory in the TB Diagnosis and Management Michael Pentella, PhD, MS, SM(ASCP), CIC, D(ABMM) September 27, 2011 Michael Pentella,
Mycobacteria & Tuberculosis PROF.HANAN HABIB & PROF ALI SOMILY DEPRTMENT OF PATHOLOGY, MICROBIOLOGY UNIT COLLEGE OF MEDICINE
 Mycobacteria & Tuberculosis PROF.HANAN HABIB & PROF ALI SOMILY DEPRTMENT OF PATHOLOGY, MICROBIOLOGY UNIT COLLEGE OF MEDICINE Objectives l Recognize that tuberculosis as a chronic disease mainly affecting
Mycobacteria & Tuberculosis PROF.HANAN HABIB & PROF ALI SOMILY DEPRTMENT OF PATHOLOGY, MICROBIOLOGY UNIT COLLEGE OF MEDICINE Objectives l Recognize that tuberculosis as a chronic disease mainly affecting
Characteristics of Mycobacterium
 Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
IDENTIFICATION OF M. tuberculosis
 Rev. 1 Pag. 1 di 7 Destinatari: Personale del Settore Diagnosi Microbiologica Avanzata e Settore Ricerca Micobatteri CONTENT 1. SCOPE 2. APPLICATION 3. DEFINITIONS AND ABBREVIATIONS 4. RESPONSIBILITIES
Rev. 1 Pag. 1 di 7 Destinatari: Personale del Settore Diagnosi Microbiologica Avanzata e Settore Ricerca Micobatteri CONTENT 1. SCOPE 2. APPLICATION 3. DEFINITIONS AND ABBREVIATIONS 4. RESPONSIBILITIES
Int.J.Curr.Microbiol.App.Sci (2018) 7(5):
 7(5):") International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 7 Number 05 (2018) Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2018.705.239
International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 7 Number 05 (2018) Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2018.705.239
Introduction. Diagnosis of extrapulmonaryand paediatric tuberculosis. Extrapulmonary tuberculosis EPTB SASCM WORKSHOP 2014/05/24
 Diagnosis of extrapulmonaryand paediatric tuberculosis AW Dreyer Centre for Tuberculosis NICD Introduction Part of the global efforts to control tuberculosis (TB) include improving case detection, especially
Diagnosis of extrapulmonaryand paediatric tuberculosis AW Dreyer Centre for Tuberculosis NICD Introduction Part of the global efforts to control tuberculosis (TB) include improving case detection, especially
Research Article Use of Genotype MTBDRplus Assay for Diagnosis of Multidrug-Resistant Tuberculosis in Nepal
 Hindawi International Scholarly Research Notices Volume 2017, Article ID 1635780, 5 pages https://doi.org/10.1155/2017/1635780 Research Article Use of Genotype MTBDRplus Assay for Diagnosis of Multidrug-Resistant
Hindawi International Scholarly Research Notices Volume 2017, Article ID 1635780, 5 pages https://doi.org/10.1155/2017/1635780 Research Article Use of Genotype MTBDRplus Assay for Diagnosis of Multidrug-Resistant
Tuberculosis Reference Laboratory, NIDCH, Mahakhali, Dhaka.
 Bangladesh J Med Microbiol 2011; 05 (02): 06-10 Bangladesh Society of Medical Microbiologists Original Article A rapid Drug Susceptibility Test (DST) for detection of Multi-Drug Resistant (MDR) Mycobacterium
Bangladesh J Med Microbiol 2011; 05 (02): 06-10 Bangladesh Society of Medical Microbiologists Original Article A rapid Drug Susceptibility Test (DST) for detection of Multi-Drug Resistant (MDR) Mycobacterium
Comparison of the Xpert MTB/RIF Assay and Real-time PCR for the Detection of Mycobacterium tuberculosis
 Available online at www.annclinlabsci.org Annals of Clinical & Laboratory Science, vol. 45, no. 3, 2015 327 Comparison of the Xpert MTB/RIF Assay and Real-time PCR for the Detection of Mycobacterium tuberculosis
Available online at www.annclinlabsci.org Annals of Clinical & Laboratory Science, vol. 45, no. 3, 2015 327 Comparison of the Xpert MTB/RIF Assay and Real-time PCR for the Detection of Mycobacterium tuberculosis
Nucleic Acid Amplification Testing for the Diagnosis of TB
 Roche Nucleic Acid Amplification Testing for the Diagnosis of TB David Warshauer, PhD Deputy Director, Communicable Diseases Wisconsin State Laboratory of Hygiene 19 th /20 th Century Traditional Algorithm
Roche Nucleic Acid Amplification Testing for the Diagnosis of TB David Warshauer, PhD Deputy Director, Communicable Diseases Wisconsin State Laboratory of Hygiene 19 th /20 th Century Traditional Algorithm
AN EVALUATION OF CURRENT DIAGNOSTIC METHODS FOR TUBERCLOSIS IN RESOURCE-POOR AREAS AND A PROPOSAL FOR A MORE SENSITIVE TEST. Helen Marya McGuirk
 AN EVALUATION OF CURRENT DIAGNOSTIC METHODS FOR TUBERCLOSIS IN RESOURCE-POOR AREAS AND A PROPOSAL FOR A MORE SENSITIVE TEST by Helen Marya McGuirk B.S., Microbiology, University of Georgia, 2007 Submitted
AN EVALUATION OF CURRENT DIAGNOSTIC METHODS FOR TUBERCLOSIS IN RESOURCE-POOR AREAS AND A PROPOSAL FOR A MORE SENSITIVE TEST by Helen Marya McGuirk B.S., Microbiology, University of Georgia, 2007 Submitted
GLI model TB diagnostic algorithms
 GLI model TB diagnostic algorithms GLI model TB diagnostic algorithms March 2017 Contents Acknowledgements Abbreviations v vi Background 1 Algorithm 1: Preferred algorithm for universal patient access
GLI model TB diagnostic algorithms GLI model TB diagnostic algorithms March 2017 Contents Acknowledgements Abbreviations v vi Background 1 Algorithm 1: Preferred algorithm for universal patient access
Diagnosis of Extra Pulmonary Tuberculosis By Using Xpert MTB/RIF Assay (CBNAAT) And MGIT Liquid Culture.
 And MGIT Liquid Culture.") IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 9 Ver. 10 (September. 2018), PP 65-70 www.iosrjournals.org Diagnosis of Extra Pulmonary Tuberculosis
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 9 Ver. 10 (September. 2018), PP 65-70 www.iosrjournals.org Diagnosis of Extra Pulmonary Tuberculosis
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
THE ROLE OF THE LABORATORY
 TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE NOVEMBER 1-4, 2016 THE ROLE OF THE LABORATORY LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe three
TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE NOVEMBER 1-4, 2016 THE ROLE OF THE LABORATORY LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe three
THE ROLE OF THE LABORATORY
 TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE THE ROLE OF THE LABORATORY LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe three laboratory methods
TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE THE ROLE OF THE LABORATORY LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe three laboratory methods
The Clinical Impact of Rapid Nucleic Acid Amplification Tests for Detection of M. tuberculosis
 The Clinical Impact of Rapid Nucleic Acid Amplification Tests for Detection of M. tuberculosis DR. PHYLLIS DELLA-LATTA, D(ABMM), FAAM DIRECTOR, CLINICAL MICROBIOLOGY SERVICE PROFESSOR, CLINICAL PATHOLOGY
The Clinical Impact of Rapid Nucleic Acid Amplification Tests for Detection of M. tuberculosis DR. PHYLLIS DELLA-LATTA, D(ABMM), FAAM DIRECTOR, CLINICAL MICROBIOLOGY SERVICE PROFESSOR, CLINICAL PATHOLOGY
CDC s Approach to Fast Track Laboratory Diagnosis for Persons at Risk of Drug Resistant TB: Molecular Detection of Drug Resistance (MDDR) Service
 Service") CDC s Approach to Fast Track Laboratory Diagnosis for Persons at Risk of Drug Resistant TB: Molecular Detection of Drug Resistance (MDDR) Service Beverly Metchock, DrPH, D(ABMM) Team Lead, Reference Laboratory
CDC s Approach to Fast Track Laboratory Diagnosis for Persons at Risk of Drug Resistant TB: Molecular Detection of Drug Resistance (MDDR) Service Beverly Metchock, DrPH, D(ABMM) Team Lead, Reference Laboratory
Medical Bacteriology- lecture 13. Mycobacterium Actinomycetes
 Medical Bacteriology- lecture 13 Mycobacterium Actinomycetes Mycobacterium tuberculosis Large, very weakly gram positive rods, Obligate aerobes, related to Actinomycetes, non spore forming, non motile
Medical Bacteriology- lecture 13 Mycobacterium Actinomycetes Mycobacterium tuberculosis Large, very weakly gram positive rods, Obligate aerobes, related to Actinomycetes, non spore forming, non motile
Medical Bacteriology- Lecture 10. Mycobacterium. Actinomycetes. Nocardia
 Medical Bacteriology- Lecture 10 Mycobacterium Actinomycetes Nocardia 1 Mycobacterium Characteristics - Large, very weakly gram positive rods - Obligate aerobes, related to Actinomycetes - Catalase positive
Medical Bacteriology- Lecture 10 Mycobacterium Actinomycetes Nocardia 1 Mycobacterium Characteristics - Large, very weakly gram positive rods - Obligate aerobes, related to Actinomycetes - Catalase positive
TB Updates for the Physician Rochester, Minnesota June 19, 2009
 TB Updates for the Physician Rochester, Minnesota June 19, 2009 Mycobacterial Laboratory Science Update Nancy L. Wengenack, Ph.D. Associate Professor of Laboratory Medicine and Pathology Division of Clinical
TB Updates for the Physician Rochester, Minnesota June 19, 2009 Mycobacterial Laboratory Science Update Nancy L. Wengenack, Ph.D. Associate Professor of Laboratory Medicine and Pathology Division of Clinical
The Lancet Infectious Diseases
 Xpert MTB/RIF Ultra for detection of Mycobacterium tuberculosis and rifampicin resistance: a prospective multicentre diagnostic accuracy study Susan E Dorman, Samuel G Schumacher, David Alland et al. 2017
Xpert MTB/RIF Ultra for detection of Mycobacterium tuberculosis and rifampicin resistance: a prospective multicentre diagnostic accuracy study Susan E Dorman, Samuel G Schumacher, David Alland et al. 2017
General Session IV - Dale Schwab April 20, 2017
 The Culture of Clinical Commercial Labs Presented by: Dale Schwab PhD, Senior Scientific Director, Infectious Disease April 20, 2017 Objectives Challenges for the reference laboratory in MTB diagnosis/opportunities
The Culture of Clinical Commercial Labs Presented by: Dale Schwab PhD, Senior Scientific Director, Infectious Disease April 20, 2017 Objectives Challenges for the reference laboratory in MTB diagnosis/opportunities
Diagnosis of tuberculosis
 Diagnosis of tuberculosis Madhukar Pai, MD, PhD Assistant Professor, Epidemiology McGill University, Montreal, Canada madhukar.pai@mcgill.ca Global TB Case Detection A major concern 2.6 million new smear
Diagnosis of tuberculosis Madhukar Pai, MD, PhD Assistant Professor, Epidemiology McGill University, Montreal, Canada madhukar.pai@mcgill.ca Global TB Case Detection A major concern 2.6 million new smear
NAAT in the Clinical Laboratory and Impact on Infection Control 9 th National Conference on Laboratory Aspects of Tuberculosis APHL
 NAAT in the Clinical Laboratory and Impact on Infection Control 9 th National Conference on Laboratory Aspects of Tuberculosis APHL Susan Novak-Weekley, S(M), ASCP, Ph.D., D(ABMM) Director of Microbiology,
NAAT in the Clinical Laboratory and Impact on Infection Control 9 th National Conference on Laboratory Aspects of Tuberculosis APHL Susan Novak-Weekley, S(M), ASCP, Ph.D., D(ABMM) Director of Microbiology,
Comparison of recoveries of Mycobacterium tuberculosis using the automated BACTEC MGIT 960 System and Lowenstein Jensen medium
 Comparison of recoveries of Mycobacterium tuberculosis using the automated System and Lowenstein Jensen medium Mo. A.AL-Mazini T. Bukeet A. Abdul Kareem Coll. of Sci./ Unive Basrah Abstract We examined
Comparison of recoveries of Mycobacterium tuberculosis using the automated System and Lowenstein Jensen medium Mo. A.AL-Mazini T. Bukeet A. Abdul Kareem Coll. of Sci./ Unive Basrah Abstract We examined
TB NAAT testing at the Los Angeles County Public Health Laboratory
 TB NAAT testing at the Los Angeles County Public Health Laboratory Hector Rivas Public Health Microbiology Supervisor II Los Angeles County Public Health Laboratory hrivas@ph.lacounty.gov April 2012 1
TB NAAT testing at the Los Angeles County Public Health Laboratory Hector Rivas Public Health Microbiology Supervisor II Los Angeles County Public Health Laboratory hrivas@ph.lacounty.gov April 2012 1
Rapid Diagnosis and Detection of Drug Resistance in Tuberculosis
 Rapid Diagnosis and Detection of Drug Resistance in Tuberculosis YAM Wing-Cheong 任永昌 Department of Microbiology The University of Hong Kong Tuberculosis Re-emerging problem in industrialized countries
Rapid Diagnosis and Detection of Drug Resistance in Tuberculosis YAM Wing-Cheong 任永昌 Department of Microbiology The University of Hong Kong Tuberculosis Re-emerging problem in industrialized countries
Detection of Multidrug Resistance and Characterization of Mutations in Mycobacterium tuberculosis Isolates in Raichur District, India
 International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 10 (2017) pp. 1543-1549 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.610.185
International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 10 (2017) pp. 1543-1549 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.610.185
Towards Harmonization of Mycobacteriology in TB Trials. Study 31/ACTG 5349 Key Elements of Mycobacteriology Laboratory Procedures
 Study 31/ACTG 5349 Key Elements of Mycobacteriology Laboratory Procedures: Towards Harmonization of Mycobacteriology in TB Trials Title Author(s) Study 31/ACTG 5349 Key Elements of Mycobacteriology Laboratory
Study 31/ACTG 5349 Key Elements of Mycobacteriology Laboratory Procedures: Towards Harmonization of Mycobacteriology in TB Trials Title Author(s) Study 31/ACTG 5349 Key Elements of Mycobacteriology Laboratory
Diagnosis of drug-resistant tuberculosis disease in children: A practical approach
 Diagnosis of drug-resistant tuberculosis disease in children: A practical approach Carlos M. Perez-Velez, MD Banner Good Samaritan Medical Center University of Arizona College of Medicine Phoenix 31 October
Diagnosis of drug-resistant tuberculosis disease in children: A practical approach Carlos M. Perez-Velez, MD Banner Good Samaritan Medical Center University of Arizona College of Medicine Phoenix 31 October
BMC Infectious Diseases
 BMC Infectious Diseases This Provisional PDF corresponds to the article as it appeared upon acceptance. Fully formatted PDF and full text (HTML) versions will be made available soon. Rapid screening of
BMC Infectious Diseases This Provisional PDF corresponds to the article as it appeared upon acceptance. Fully formatted PDF and full text (HTML) versions will be made available soon. Rapid screening of
Original Article Evaluation of Xpert MTB/RIF in detection of pulmonary and extrapulmonary tuberculosis cases in China
 Int J Clin Exp Pathol 2017;10(4):4847-4851 www.ijcep.com /ISSN:1936-2625/IJCEP0045802 Original Article Evaluation of Xpert MTB/RIF in detection of pulmonary and extrapulmonary tuberculosis cases in China
Int J Clin Exp Pathol 2017;10(4):4847-4851 www.ijcep.com /ISSN:1936-2625/IJCEP0045802 Original Article Evaluation of Xpert MTB/RIF in detection of pulmonary and extrapulmonary tuberculosis cases in China
MYCOBACTERIOLOGY INTRODUCTION RANGE OF LABORATORY SERVICES
 MYCOBACTERIOLOGY INTRODUCTION The Central Tuberculosis Laboratory (CTBL) of the Department of Pathology provides laboratory diagnosis of tuberculosis (TB) and other mycobacterial diseases for all hospitals,
MYCOBACTERIOLOGY INTRODUCTION The Central Tuberculosis Laboratory (CTBL) of the Department of Pathology provides laboratory diagnosis of tuberculosis (TB) and other mycobacterial diseases for all hospitals,
Mycobacteriology William H. Benjamin, Jr.
 Mycobacteriology William H. Benjamin, Jr. William H. Benjamin, PhD Department of Pathology UAB 1 Mycobacteria sp. Acid Fast Bacilli (AFB) Mycolic acids (C78-91) Waxes Obligate aerobes Slow growing days
Mycobacteriology William H. Benjamin, Jr. William H. Benjamin, PhD Department of Pathology UAB 1 Mycobacteria sp. Acid Fast Bacilli (AFB) Mycolic acids (C78-91) Waxes Obligate aerobes Slow growing days
NOLA TB TIMES. TB Diagnostics A Special Issue. on TB Diagnosis 101. Diagnostic Discrepancy Data. Comprehensive Approach
 NOLA TB TIMES Volume 1, No 3 February 2016 TB Diagnostics A Special Issue on TB Diagnosis 101 Happy New Year and Happy Mardi Gras to everyone! We already have seven presumptive cases of tuberculosis (TB)
NOLA TB TIMES Volume 1, No 3 February 2016 TB Diagnostics A Special Issue on TB Diagnosis 101 Happy New Year and Happy Mardi Gras to everyone! We already have seven presumptive cases of tuberculosis (TB)
Chapter 4 Diagnosis of Tuberculosis Disease
 Chapter 4 Diagnosis of Tuberculosis Disease Table of Contents Chapter Objectives.... 75 Introduction.... 77 Medical Evaluation.......................................................... 78 Chapter Summary...
Chapter 4 Diagnosis of Tuberculosis Disease Table of Contents Chapter Objectives.... 75 Introduction.... 77 Medical Evaluation.......................................................... 78 Chapter Summary...