Pediatric TB Intensive Houston, Texas
|
|
|
- Myrtle Lawrence
- 5 years ago
- Views:
Transcription

1 Pediatric TB Intensive Houston, Texas November 13, 2009 Extrapulmonary TB James B. McAuley MD MPH November 13, 2009 PEDIATRIC TB EXTRAPULMONARY DISEASE James B. McAuley MD MPH Rush University Medical Center Chicago, Illinois 1
2 Percent of Pediatric TB Cases by Age Group N=15,946 3 Age % Age < 1 9.2% Age 5-9 Age % 49.5% Pediatric TB Cases by Site of Disease, Pulmonary 71.1% Both 7.0% Extra pulmonary 21.9% Any extrapulmonary involvement* (totaling 28.9%) Lymphatic 18.9% Meningeal 3.1% Miliary 1.5% Bone & Joint 1.5% Other 3.9% *Any extrapulmonary involvement which includes cases that are extrapulmonary only and both Patients may have more than one disease site but are counted in mutually exclusive categories for surveillance purposes. 2
3 Percent of Pediatric TB Cases by Site of Disease*, N=15,946 5 Age < 1 n=1,471 Age 1-4 n=7, % 10.1% 75.2% 20.7% 7.2% 72.1% Age 5-9 n=3, % Age n=2, % 25.5% 27.0% 70.1% 67.1% Pulmonary Extrapulmonary Both Percent of Pediatric TB Cases with Any Extrapulmonary Involvement* by Age Group and Selected Sites of Disease, N=15,946 Age < 1 Age 1-4 Age 5-9 Age Site of Disease (n=1,471) (n=7,884) (n=3,691) (n=2,900) Lymphatic Meningeal Miliary Bone & Joint Other Total *Any extrapulmonary involvement includes extrapulmonary only and both 6 Note: Combine the total extrapulmonary percent shown with the pulmonary percent in slide #21 to obtain 100% for each age group. 3
4 Percent of TB Cases in Children Age < 1 Year With Any Extrapulmonary Involvement, N=1,471 Site of disease U.S. S-born Foreign-born Lymphatic 7.2% 17.7% Meningeal 7.8% 3.5% Miliary 5.8% 3.5% Bone & Joint 03% 0.3% 09% 0.9% Other 3.4% 1.8% Total 24.5%* 27.4%* *Any extrapulmonary involvement includes extrapulmonary only and both 7 Percent of TB Cases in Children Age 1 4 Years With Any Extrapulmonary Involvement, N=7,884 Site of disease U.S. S-born Foreign-born Lymphatic 19.4% 19.0% Meningeal 3.8% 2.0% Miliary 1.3% 1.0% Bone & Joint 11% 1.1% 20% 2.0% Other 2.7% 2.0% Total 28.3%* 26.0%* *Any Extrapulmonary involvement includes extrapulmonary only and both 8 4
5 Percent of TB Cases in Children Age 5 9 Years With Any Extrapulmonary Involvement, N=3,691 Site of disease U.S. S-born Foreign-born Lymphatic 23.1% 20.8% Meningeal 1.4% 1.0% Miliary 0.6% 0.6% Bone & Joint 16% 1.6% 21% 2.1% Other 4.1% 3.8% Total 30.8%* 28.3%* *Any Extrapulmonary involvement includes extrapulmonary only and both 9 Percent of TB Cases in Children Age Years With Any Extrapulmonary Involvement, N=2,900 Site of disease U.S. S-born Foreign-born Lymphatic 20.4% 18.1% Meningeal 1.6% 1.8% Miliary 1.5% 0.8% Bone & Joint 20% 2.0% 28% 2.8% Other 9.0% 7.3% Total 34.5%* 30.8%* *Any Extrapulmonary involvement includes extrapulmonary only and both 10 5
6 Pediatric TB Cases by HIV Status, * N=14,990 Information on HIV result is not available for the majority of pediatric TB cases (80.7%) Percent of pediatric TB cases with HIV positive test results, minimum estimate** (1.0%) Percent of pediatric cases with HIV positive test results of those patients with known results (5.1%) *California HIV data through 2004 only **Pediatric TB cases with positive HIV test results divided by all pediatric TB cases. California only reports positive HIV test results based on TB and AIDS registry matching; all other California TB cases are classified as Unknown. 11 Pediatric TB Chicago (n=498) % female 23% < 1yr 72% black 18% hispanic 5% white 6% foreign born 74% pulmonary 9% hilar nodes 9% lymph node (other) 3% miliary 6% meningitis 79% cultures sent 61% positive (261) Reinhard, Paul, McAuley, June 1997 Am J Med Sci 6
7 AFB Smears in Children Age (yrs) N AFB Done AFB + < % 23% % 16% % 12% % 20% TOTAL % 18% 1995 US Surveillance data, CDC AFB Culture in Children Age (yrs) N MTB Done MTB + < % 60% % 37% % 25% % 40% TOTAL % 41% 1995 US Surveillance data, CDC 7
8 Pediatric TB Chicago (n=498) community areas in Chicago 11.3 cases per 100,000 for African American SES variables only significant factors: percent below poverty percent unemployed percent female headed households Reinhard, Paul, McAuley, June 1997 Am J Med Sci Pathophysiology of Extrapulmonary TB Primary Infection TB reaches alveoli, replicates extra and intracellularly, lack of immediate host immune repsonse Replication intracellularly within macrophages, MTb prevents acidification of phagosome and multiplies for weeks within macrophages 8



9 Pathophysiology of Extrapulmonary TB Metastatic foci established in regional nodes, seed blood and travel to tissues favoring multiplication Alveolar macrophages secrete interleukins 12 and 18, which attracts CD4 cells, CD4 cells meet TB antigens on surface of infected macrophages and are transformed, proliferate and secrete gamma interferon TNF alpha stimulates granuloma formation and increases ability of Macrophages to kill MTb 9
10 TIMETABLE OF PEDIATRIC TB: from infection to disease Miliary and meningeal develop rapidly Adenopathy segmental Lymph node (cervical) Pleural effusion Skeletal Renal 1 12 months 2 12 months 2 12 months 3 9 months 6 months 2 years 1 5 years TST Positive window period Time From Exposure 10
11 Extrapulmonary Tuberculosis Proportion in all TB in USA : 7% (1963) to 18% (1987) to 20% (now) Increase maybe due to HIV infection More in minorities and foreign borns Lymphatic TB (30%) > Pleural TB (24%) > Bone and joint TB (10%) > Genitourinary TB (9%) > Miliary TB (8%) > Meningeal TB (6%) (New York, 1995) Case History 2 9/12 year old with fever and cough in August, treated as outpatient two months ago for pneumonia PMH of prematurity, tracheomalacia and tracheostomy Admitted, left lower lobe infiltrate, started on antibiotics, i seizure on hospital day 2 11
, protein=145, glucose=74")

 Uncle in")

12 Case History CSF: 107 WBC (84L), protein=145, glucose=74 MRI done, PPD placed Case History Aunt diagnosed with TB 10 months ago (lived in separate house) Uncle in hospital with pneumonia Child was not identified as a contact 9 year old sibling in school 12
13 CNS Tuberculosis Pathogenesis and clinical presentation Tuberculous meningitis (TBM) May produce damage to vessels, infarction of brain, edema, fibrosis Predilection: base of brain In AIDS: cerebral abscess or tuberculomas Space occupying sign: headache, seizure, paralysis, personality change, CN defects, neck stiffness, papilledema CNS Tuberculosis Diagnosis and Treatment CSF: clear or slightly opalescent; elevated protein and low glucose (virus: high) AFB and culture: limited Meningeal biopsy: difficult CT and MRI: helpful Tx: chemotherapy, surgery (hydrocephalus) and py, g y( y p ) steroids 13
14 CSF Findings in TB Meningitis Median WBC = 114 cells (20 530), 82% lymphocytes y (0 99 range) g) Median protein = 141 ( range) Median glucose = 30 (range 5 103) CSF values were not predictive of outcome Saitoh, Ped Infect Dis J, March 2005 CSF Microbiology in TB Meningitis, San Diego 9/20 (45%) positive CSF culture, 2/20 (10%) positive ii gastric aspirate culture 7/14 (50%) positive CSF TB pcr 14/20 (70%) had either CSF/gastric aspirate culture or CSF pcr positive Saitoh, Ped Infect Dis J, March
15 CSF Microbiology in TB Meningitis, Vietnam 107/132 (81%) with microbiologic confirmation: AFB smear sensitivity 52%, culture sensitivity 64% Multivariate analysis showed increased CSF volume increased sensitivity (> 6 ml gave 80% sensitivity) as did time examining slide (> 30 min) Thwaites, J Clin Micro, Jan 2004 CNS Imaging, San Diego Basal enhancement present on non contrast CT study 13/20 (68%) of children with definite TB CT findings did not correlate with long term neurological outcome Saitoh, Pediatr Infect Dis J. March


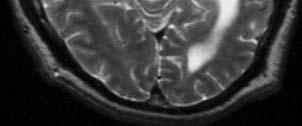
16 Typical MRI Findings Tuberculoma 32 16
17 Summary of Diagnostic Tests for CNS TB in Children TEST SENSITIVITY AFB smear gastric aspirate 5 10% AFB smear csf 0 50% Mycobacteria culture csf 0 64% Nucleic acid amplification 0 60% CSF TB PCR 0 60% Combination of CSF smear, or culture or NAA or PCR likely increases sensitivity, but NOT likely to greater than ~75%. Treatment Considerations Adjunct dexamethasone was associated with reduced d death (81/274, 32% vs. 112/271, 41%) and adverse events, but not disability in adolescents and adults with TB meningitis. Thwaites NEJM Oct Generally 1 2 mg/kg/day of prednisone given for 4 6 weeks 17
 Tuberculosis Lymphadenitis Differential Diagnosis Nontuberculous mycobacteria (young age, unilateral and normal CXR, MAI, M.")
18 Tuberculosis Lymphadenitis Most common form of extrapulmonary TB Peak age: children, recent shift to y/o High risk: Asians, female (2x to male), HIV Hilar, paratracheal and neck lymphnodes Self limited (>90%) Tuberculosis Lymphadenitis Differential Diagnosis Nontuberculous mycobacteria (young age, unilateral and normal CXR, MAI, M. scrofulum) Virus (CMV), toxoplasmosis, bartonella Neoplasm Tuberculin skin test, history and CXR Total excision biopsy pyand culture preferred for NTM adenitis Emerging consideration for medical therapy for NTM (typically MAI) 18
19 Tuberculosis Lymphadenitis Treatment Anti tuberculous chemotherapy for 6 months course (1 st line: pyrazinamide, isoniazid, rifampin; ethambutol if high rates of drug resistance) Surgical intervention generally to be avoided Steroids may be helpful with large nodes that are obstructing, particularly l in the chest Extra pulmonary Intrathoracic TB 19


20 Hilar adenopathy with infiltrate and collapse Collapse in a 9 year old 20

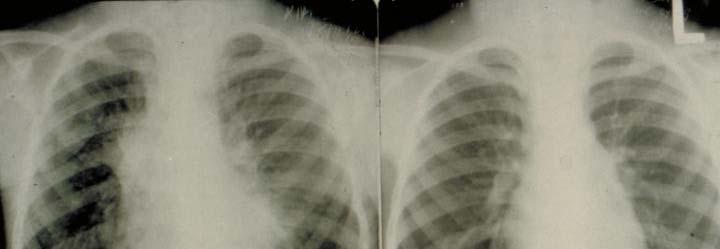
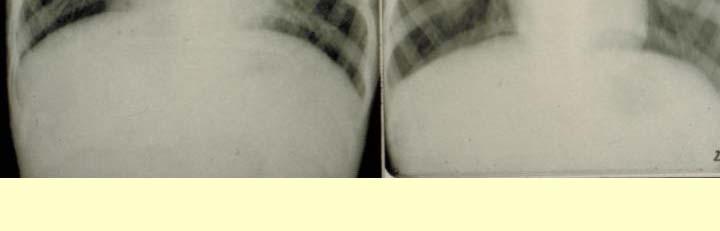
21 Hilar Adenopathy with Atelectasis Hilar Adenopathy 21
22 Hilar Disease in HIV Infected Person Treatment of Hilar Disease Often pulmonary disease as well Isolated TB adenopathy is paucibacillary ill and thus risk of resistance is low Nodes are slow to resolve, common error is to treat too long waiting for radiograph to resolve If the hilar nodes are too subtle to be clearly visible on plain radiographs, treating as for LTBI is unlikely to be a problem 22


23 Chest Radiograph Pearls Hilar nodes, pleural disease extrapulmonary, few bacteria Cavitary disease many bacteria Parenchymal scars NOT active, only needs treatment for LTBI IF scar is > 2.5 cm Calcified node is functionally like a normal chest radiograph (very very few live AFB) Pleural TB 23



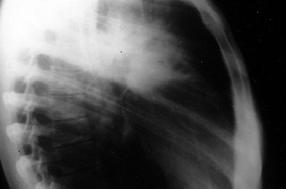
24 Extensive Pleural Disease Post Therapy 24



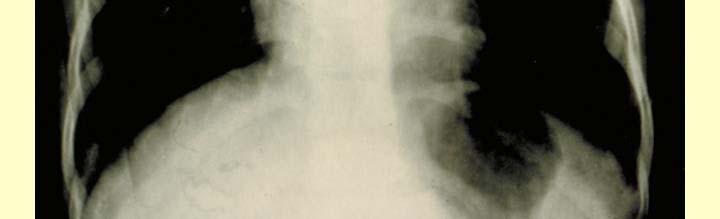
25 Pleural Tuberculosis Pericardial Tuberculosis 25



26 Case History 18 yo AA female with unremarkable PMH presents with 1 2 days of left breast swelling Enlarged, painful, no fever, left axillary pain PMH/SH sexually active, multiple partners, tobacco and non injection drug use 26
, Hgb = 10.")


27 Work Up WBC = 2.4 (65P/25L/8M), Hgb = 10.8, Platelets = 210 Chem 30 notable for: Na = 132, K = 4.1, TP = 7.5, alb = 3.2, cholesterol = 102 CXR 27




28 28


29 29


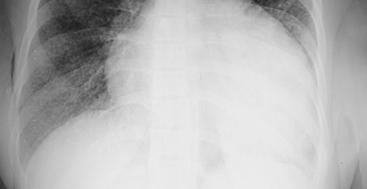
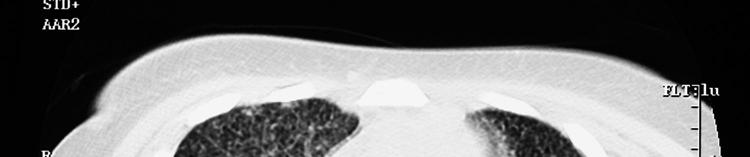
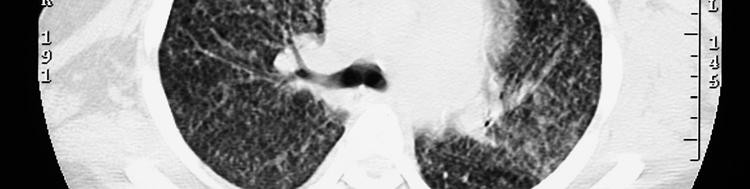
30 Diagnosis? HIV positive, CD4 = 20 MTb infection culture positive LN biopsy, sputum, pericarditis Miliary Tuberculosis 30



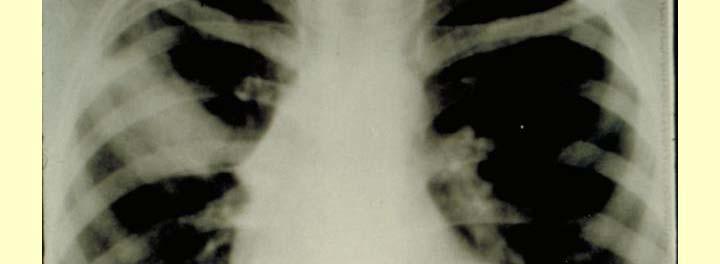
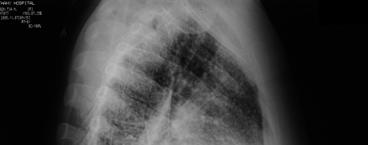
31 Miliary TB in a child Miliary TB child with hilar adenopathy 31


, steroids? 32")
32 Miliary TB Data from Malawi suggests 70% with Miliary TB will have disc abnormalities Miliary Tuberculosis Lympho hematogenous dissemination Infants and children: primary Elderly or HIV infection: reactivation Fever, weakness, anorexia, Wt loss, cough Dx: CXR, HRCT Tx: Chemotherapy for 9 12 months (HIV at least 12 months), steroids? 32
 80% (developing country) in")
 Treatment complicated by interaction")
33 HIV and Extrapulmonary TB Immunosuppression increases rate and dissemination and makes its symptoms atypical Outside US TB is greatest cause of death in y/o with AIDS; treatment of LTBI critical EPTB occurs in 25% (US) 80% (developing country) in HIV(+). Lymph node involvement most common, but miliary, CNS, or cutaneous TB are seen as in HIV( ) Treatment complicated by interaction of PI and rifampin, WHO recommends Rx TB first MDR TB, XDR TB Clinical and immunopathological course of HIV associated TB 33
34 Case History 3 year old with right arm pain two weeks after falling, no fever Uncle diagnosed with TB 15 months ago Child was not identified as a contact Afebrile, lytic lesion in proximal ulna US born, parents from India 67 Bone Spinal Tuberculosis 68 34

 > soft tissue or muscle (4.")
35 Large Paraspinal Abscess with T 6 Destruction Bone and joint Tuberculosis Pott s disease Increasing since 1980s 13 25% HIV positive in several adult series Location: lumbar spine (29.5%) > thoracic spine (20.5%) > knee (13.2%) > hip (8.2%) > soft tissue or muscle (4.5%) (Los Angeles, ) Results from hematogenous dissemination 35
36 Bone and joint Tuberculosis Pathophysiology Invasion of joint space: direct or indirect Cartilage preservation Cold abscess and sinus tract formation Fibrosis and ankylosis, calcification Bone and joint Tuberculosis Clinical Presentation Tuberculous spondylitis Tb Tuberculous osteomyelitis i Tuberculous arthritis Tuberculous tensynovitis Tuberculous myositis 36
37 Bone and joint Tuberculosis Tuberculous spondylitis Most common, especially in developing countries Back pain and rigidity Vertebral body involvement and diskitis Kyphosis and paraplegia Bone and joint Tuberculosis Tuberculous osteomyelitis Initial: painful mass attached to bone with soft tissue swelling Predilection to metaphysis of long bones May extend to a joint Single in adults; multiple in children, elderly, immunosuppressive and HIV infection 37
38 Bone and joint Tuberculosis Tuberculous arthritis Large weight bearing joint like hip, knee Pifl Painful, ankylosed kl or swollen mono arthropathy, h limitation of motion Granulation, necrosis, narrowing of the joint space Has been reported in prosthesis infections Bone and joint Tuberculosis Tuberculous myositis More in immunosuppressed and AIDS Most with ih psoas muscle involvement extension from vertebral body Swelling, less pain; a solitary nodule with cold abscess, limitation of muscle function; iliac fossa pain or tenderness in some case 38
39 Bone and joint Tuberculosis Diagnosis and DDx DDx: collagen vascular arthritis and pyogenic arthritis; fungal infection; neoplasm Monoarthritis, chronic pain, minimal systemic signs Tuberculin skin test Plain radiography, open biopsy CT, MRI, CT guided fine needle aspiration biopsy Bone and joint Tuberculosis Treatment Early diagnosis Anti tuberculosis i drugs with ih minimal i operative intervention for abscess drainage (85 90% complete recovery) Operative decompression (laminectomy should be avoided), bracing may be helpful Arthroplasty 39
40 Genitourinary Tuberculosis Developing >> developed countries Ml/f Male/female=2:1, l most 20 40y/o (45 55y/o) Vague urinary tract symptoms: painless frequent micturition is common Microscopic hematuria: 50% Recurrent E. coli infection Urine WBC, suprapubic pain, hemospermia, painful testicular swelling: all rare Genitourinary Tuberculosis Diagnosis Tuberculin skin test Ui Urine examination i and culture Elevated ESR Plain film, IVP, percutaneous antegrade pyelography Limited value: endoscopy, biopsy, py, ultrasonography and CT 40
41 Genitourinary Tuberculosis Pathology Kidney: chronic parenchymal abscess, large renal calcification; may spread to ureter, bladder, seminal visicle Bladder: bullous granulation from ureteric orifice, obstruction; fistula to rectum Epididymis: bloodstream spread, present with discharging i sinus; may spread to testis Genitourinary Tuberculosis Treatment Anti tuberculous chemotherapy (effective) Surgery (>80%): nephrectomy, nephroureterectomy, epididymectomy and reconstructive surgery 41
42 Cutaneous Tuberculosis Uncommon (<1% in the west) Contagious, may spread by direct contact Exogenous source: Tuberculous chancre and prosector s wart Endogenous source (disseminated): scrofuloderma Hematogenous source: Lupus vulgaris and multiple soft tissue cold abscess (most in AIDS) Tuberculous masitis: most in y/o female as in our previous case Cutaneous Tuberculosis Diagnosis and Therapy Excisional biopsy for AFB stain and culture ELISA and PCR Tx: chemotherapy (3 4 drug) and surgery (excisional biopsy and debridement) 42

 Corticosteroids used as adjunctive therapy for patients with TB meningitis and pericarditis If")
43 Other Extrapulmonary Otologic Tuberculosis Ocular Tuberculosis Cardiovascular Tuberculosis Tuberculous Peritonitis Tuberculous Enteritis more common in places with unpasteurized dairy consumption, M. bovis Tuberculosis of the liver and biliary tract Treatment Extrapulmonary TB Similar treatment regimen for pulmonary TB* 6 to 9 month regimens that include INH and RIF are effective (CNS 12+) Corticosteroids used as adjunctive therapy for patients with TB meningitis and pericarditis If PZA cannot be used in the initial phase, continuation i phase must be increased to 7 months 43
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas
 TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas March 7 9, Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012
 TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Pediatric TB Lisa Armitige, MD, PhD September 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
Pediatric TB Intensive Houston, Texas October 14, Extrapulmonary TB in Children Kim Connelly Smith, MD, MPH October 14, 2013
 Pediatric TB Intensive Houston, Texas October 14, 2013 Extrapulmonary TB in Children Kim Connelly Smith, MD, MPH October 14, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict
Pediatric TB Intensive Houston, Texas October 14, 2013 Extrapulmonary TB in Children Kim Connelly Smith, MD, MPH October 14, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict
Diagnosis of TB: Radiology David Finlay, MD
 TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017
 Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
TUBERCULOSIS. By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi
 TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
Errors in Dx and Rx of TB
 Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
TB Intensive San Antonio, Texas November 11 14, 2014
 TB Intensive San Antonio, Texas November 11 14, 2014 Extrapulmonary TB Linda Dooley, MD November 13, 2014 Linda Dooley, MD has the following disclosures to make: No conflict of interests No relevant financial
TB Intensive San Antonio, Texas November 11 14, 2014 Extrapulmonary TB Linda Dooley, MD November 13, 2014 Linda Dooley, MD has the following disclosures to make: No conflict of interests No relevant financial
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
David E. Griffith, MD has the following disclosures to make:
 Diagnosis of TB: Radiology David E. Griffith, MD March 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION David E. Griffith, MD has the following disclosures to make:
Diagnosis of TB: Radiology David E. Griffith, MD March 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION David E. Griffith, MD has the following disclosures to make:
CHAPTER 3: DEFINITION OF TERMS
 CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
Pathology of pulmonary tuberculosis. Dr: Salah Ahmed
 Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
Communicable Disease Control Manual Chapter 4: Tuberculosis
 Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
3/25/2012. numerous micro-organismsorganisms
 Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014
 Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 TB Case Presentation Andrea Cruz, MD, MPH August 14, 2014 Andrea Cruz, MD, MPH has the following disclosures to
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 TB Case Presentation Andrea Cruz, MD, MPH August 14, 2014 Andrea Cruz, MD, MPH has the following disclosures to
Pediatric TB Radiology: It s Not Black and White Part 2
 Experiencing technical difficulties? Please call Adobe Connect for technical assistance at 1-800-422-3623 Pediatric TB Radiology: It s Not Black and White Part 2 June 18, 2018 A National Webinar June 18,
Experiencing technical difficulties? Please call Adobe Connect for technical assistance at 1-800-422-3623 Pediatric TB Radiology: It s Not Black and White Part 2 June 18, 2018 A National Webinar June 18,
Pediatric TB Intensive Houston, Texas
 Pediatric TB Intensive Houston, Texas November 13, 2009 Radiographic Manifestations of Pediatric TB Susan D. John, MD, FACR November 13, 2009 Radiologic Presentation of Childhood TB Susan D. John, MD,
Pediatric TB Intensive Houston, Texas November 13, 2009 Radiographic Manifestations of Pediatric TB Susan D. John, MD, FACR November 13, 2009 Radiologic Presentation of Childhood TB Susan D. John, MD,
I. Demographic Information GENDER NUMBER OF CASES PERCENT OF CASES. Male % Female %
 San Joaquin County (SJC) in 03, (N=43) County Rate = 6. Cases per 00,000 Population I. Demographic Information Table I-A: TB cases by gender, SJC, 03 (N=43) GENDER NUMBER OF CASES Male 6 60.5% Female 7
San Joaquin County (SJC) in 03, (N=43) County Rate = 6. Cases per 00,000 Population I. Demographic Information Table I-A: TB cases by gender, SJC, 03 (N=43) GENDER NUMBER OF CASES Male 6 60.5% Female 7
TB in Children. Rene De Gama Block 10 Lectures 2012
 TB in Children Rene De Gama Block 10 Lectures 2012 Contents Epidemiology Transmission and pathogenesis Diagnosis of TB TB and HIV Management Epidemiology The year 2000 8.3 million new TB cases diagnosed
TB in Children Rene De Gama Block 10 Lectures 2012 Contents Epidemiology Transmission and pathogenesis Diagnosis of TB TB and HIV Management Epidemiology The year 2000 8.3 million new TB cases diagnosed
Pediatric TB Intensive Houston, Texas
 Pediatric TB Intensive Houston, Texas November 13, 2009 Treatment of Pediatric TB Jeffrey R. Starke, M.D. November 13, 2009 MANAGEMENT OF CHILDHOOD TUBERCULOSIS Jeffrey R. Starke, M.D. Professor of Pediatrics
Pediatric TB Intensive Houston, Texas November 13, 2009 Treatment of Pediatric TB Jeffrey R. Starke, M.D. November 13, 2009 MANAGEMENT OF CHILDHOOD TUBERCULOSIS Jeffrey R. Starke, M.D. Professor of Pediatrics
TB Intensive San Antonio, Texas November 29-December 2, 2011
 TB Intensive San Antonio, Texas November 29-December 2, 2011 Diagnosis of TB: Radiology Michael McCarthy, MD, FACR November 30, 2011 Michael McCarthy, MD, FACR has the following disclosures to make: No
TB Intensive San Antonio, Texas November 29-December 2, 2011 Diagnosis of TB: Radiology Michael McCarthy, MD, FACR November 30, 2011 Michael McCarthy, MD, FACR has the following disclosures to make: No
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Pediatric TB Intensive Houston, Texas October 14, 2013
 Pediatric TB Intensive Houston, Texas October 14, 2013 Radiologic Presentation of Childhood TB Susan D. John, MD, FACR October 14, 2013 Disclosures I have no disclosures or conflicts of interest to report
Pediatric TB Intensive Houston, Texas October 14, 2013 Radiologic Presentation of Childhood TB Susan D. John, MD, FACR October 14, 2013 Disclosures I have no disclosures or conflicts of interest to report
TB Radiology for Nurses Garold O. Minns, MD
 TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TB Intensive San Antonio, Texas August 7-10, 2012
 TB Intensive San Antonio, Texas August 7-10, 2012 An Introduction to Childhood Tuberculosis Kim Smith, MD, MPH August 10, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Intensive San Antonio, Texas August 7-10, 2012 An Introduction to Childhood Tuberculosis Kim Smith, MD, MPH August 10, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests
Interpretation of Chest Radiographs Paul Christensen, MD 10/21/09. Diagnostic Evaluation. Medical Evaluation & CXR Interpretation.
 Diagnostic Evaluation Medical Evaluation & CXR Interpretation University of Michigan TB Consultant Washtenaw County Medical history Physical examination Testing for TB exposure (previously covered) Radiologic
Diagnostic Evaluation Medical Evaluation & CXR Interpretation University of Michigan TB Consultant Washtenaw County Medical history Physical examination Testing for TB exposure (previously covered) Radiologic
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Life Cycle of M. tuberculosis
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
has the following disclosures to make:
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
TUBERCULOSIS. Pathogenesis and Transmission
 TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Global Impact of TB
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
Pediatric TB Theresa Barton, MD
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Pediatric TB Theresa Barton, MD December 9, 2009 Pediatric Tuberculosis Tess Barton, MD Assistant Professor of Pediatrics UT Southwestern
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Pediatric TB Theresa Barton, MD December 9, 2009 Pediatric Tuberculosis Tess Barton, MD Assistant Professor of Pediatrics UT Southwestern
Dr Francis Ogaro MTRH ELDORET
 Dr Francis Ogaro MTRH ELDORET TB in children often severe, disseminated and can progress rapidly and with poor outcome TB diagnosis in children has relied on clinical, imaging, microscopy and TST findings.
Dr Francis Ogaro MTRH ELDORET TB in children often severe, disseminated and can progress rapidly and with poor outcome TB diagnosis in children has relied on clinical, imaging, microscopy and TST findings.
TB, or NOT TB? A Tough Question in Kids!
 TB, or NOT TB? A Tough Question in Kids! Brian Lee, MD Pediatric Tuberculosis Program Division of Infectious Diseases Ken Martin, MD Division of Radiology Overview Illustrate the range of clinical scenarios
TB, or NOT TB? A Tough Question in Kids! Brian Lee, MD Pediatric Tuberculosis Program Division of Infectious Diseases Ken Martin, MD Division of Radiology Overview Illustrate the range of clinical scenarios
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
PULMONARY TUBERCULOSIS RADIOLOGY
 PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
Diagnosis of tuberculosis in children
 Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Diagnosis & Medical Case Management of TB Disease. Lisa Armitige, MD, PhD October 22, 2015
 Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
TB Intensive Houston, Texas October 15-17, 2013
 TB Intensive Houston, Texas October 15-17, 2013 Tuberculosis in Children Kim Connelly Smith, MD, MPH October 16, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Intensive Houston, Texas October 15-17, 2013 Tuberculosis in Children Kim Connelly Smith, MD, MPH October 16, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
Diagnosis and Medical Management of TB Disease. Quratulian Annie Kizilbash, MD, MPH March 17, 2015
 Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
TB & HIV CO-INFECTION IN CHILDREN. Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012
 TB & HIV CO-INFECTION IN CHILDREN Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012 Introduction TB & HIV are two of the leading causes of morbidity & mortality in children
TB & HIV CO-INFECTION IN CHILDREN Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012 Introduction TB & HIV are two of the leading causes of morbidity & mortality in children
Pediatric Drug-Resistant TB in China
 Pediatric Drug-Resistant TB in China Shuihua Lu,Tao Li Shanghai Public Health Clinical Center Jan.18,2013 A MDR-TB CASE A four and a half years old boy, spent 4 yeas of his life in hospital. His childhood
Pediatric Drug-Resistant TB in China Shuihua Lu,Tao Li Shanghai Public Health Clinical Center Jan.18,2013 A MDR-TB CASE A four and a half years old boy, spent 4 yeas of his life in hospital. His childhood
HISTORY TB = 25% ADULT DEATHS EGYPTIAN MUMMIES: SPINAL TB. 17 th -18th CENTURIES- URBANIZATION MID 24
 HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY INDUSTRIALIZATION TB = 25% ADULT DEATHS GERM THEORY OF DISEASE KOCH S BACILLUS-1883 PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS
HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY INDUSTRIALIZATION TB = 25% ADULT DEATHS GERM THEORY OF DISEASE KOCH S BACILLUS-1883 PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS
Algorithmic Approaches to Child TB Management in Resource-limited Settings
 Algorithmic Approaches to Child TB Management in Resource-limited Settings Steve Graham Centre for International Child Health University of Melbourne Department of Paediatrics Royal Children s Hospital
Algorithmic Approaches to Child TB Management in Resource-limited Settings Steve Graham Centre for International Child Health University of Melbourne Department of Paediatrics Royal Children s Hospital
HISTORY TB = 25% ADULT DEATHS MID 24 PRE-ANTIBIOTIC ERA
 PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS & REST CAVITARY DISEASE & COLLAPSE THERAPY FRESH AIR, SUNSHINE-ROOFTOPS SOLARIA HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY
PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS & REST CAVITARY DISEASE & COLLAPSE THERAPY FRESH AIR, SUNSHINE-ROOFTOPS SOLARIA HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY
Tuberculosis - clinical forms. Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases
 Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
Analysis. Answers. Action. Saturday Night Fever. Shaka Brown Capital Congress
 Saturday Night Fever Shaka Brown Capital Congress Shaka Zulu October 31, 2012 SICK SUCKS How my illness started October 2013 August to October 2013 Symptoms: Severe fatigue Night sweats Low grade fever
Saturday Night Fever Shaka Brown Capital Congress Shaka Zulu October 31, 2012 SICK SUCKS How my illness started October 2013 August to October 2013 Symptoms: Severe fatigue Night sweats Low grade fever
Research in Tuberculosis: Translation into Practice
 Case History Research in Tuberculosis: Translation into Practice This is a 6-year6 year-old Bosnian male, who presented to ER with one-week history of fever and occasional vomiting. No cough, difficulty
Case History Research in Tuberculosis: Translation into Practice This is a 6-year6 year-old Bosnian male, who presented to ER with one-week history of fever and occasional vomiting. No cough, difficulty
Tuberculosis. By: Shefaa Q aqa
 Tuberculosis By: Shefaa Q aqa Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the
Tuberculosis By: Shefaa Q aqa Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the
Pediatric TB Intensive Houston, Texas October 14, 2013
 Pediatric TB Intensive Houston, Texas October 14, 2013 Diagnosis and Management of Tuberculosis in Adolescents Andrea T. Cruz, MD, MPH Sections of Infectious Diseases & Emergency Medicine October 14, 2013
Pediatric TB Intensive Houston, Texas October 14, 2013 Diagnosis and Management of Tuberculosis in Adolescents Andrea T. Cruz, MD, MPH Sections of Infectious Diseases & Emergency Medicine October 14, 2013
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB in the Correctional Setting Florence, Arizona October 7, 2014
 TB in the Correctional Setting Florence, Arizona October 7, 2014 Diagnosis and Treatment of TB Disease Renuka Khurana, MBBS, MPH October 7, 2014 Renuka Khurana, MSSB, MPH has the following disclosures
TB in the Correctional Setting Florence, Arizona October 7, 2014 Diagnosis and Treatment of TB Disease Renuka Khurana, MBBS, MPH October 7, 2014 Renuka Khurana, MSSB, MPH has the following disclosures
Tuberculosis Pathogenesis
 Tuberculosis Pathogenesis Renuka Khurana, MD, MPH May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Renuka Khurana, MD, MPH has the following disclosures
Tuberculosis Pathogenesis Renuka Khurana, MD, MPH May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Renuka Khurana, MD, MPH has the following disclosures
Diagnosis of TB in Children. Dr Jacquie Narotso Oliwa
 Diagnosis of TB in Children Dr Jacquie Narotso Oliwa 1 Objectives To identify the common clinical presentations of TB in children Overview of diagnostic measures To understand a simplified approach to
Diagnosis of TB in Children Dr Jacquie Narotso Oliwa 1 Objectives To identify the common clinical presentations of TB in children Overview of diagnostic measures To understand a simplified approach to
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
Gary Reubenson 16 October 2012 PAEDIATRIC TUBERCULOSIS: AN OVERVIEW IN 40 MINUTES!!
 Gary Reubenson 16 October 2012 PAEDIATRIC TUBERCULOSIS: AN OVERVIEW IN 40 MINUTES!! DECLARATION No relevant conflicts of interest to declare OVERVIEW Burden of disease & epidemiology Pathogenesis (not
Gary Reubenson 16 October 2012 PAEDIATRIC TUBERCULOSIS: AN OVERVIEW IN 40 MINUTES!! DECLARATION No relevant conflicts of interest to declare OVERVIEW Burden of disease & epidemiology Pathogenesis (not
TB in Children. The diagnostic challenge. Ralph Diedericks Red Cross Hospital
 TB in Children The diagnostic challenge Ralph Diedericks Red Cross Hospital TB in children Brief epidemiology Clinical issues in primary TB Cases Rates of TB infection 2005 TST survey reported a TB prevalence
TB in Children The diagnostic challenge Ralph Diedericks Red Cross Hospital TB in children Brief epidemiology Clinical issues in primary TB Cases Rates of TB infection 2005 TST survey reported a TB prevalence
Extrapulmonary Tuberculosis
 Extrapulmonary Tuberculosis Timothy H. Dellit, MD Professor, UW Allergy & Infectious Diseases Associate Medical Director Harborview Medical Center No financial conflicts Tuberculosis in King County1995-2014
Extrapulmonary Tuberculosis Timothy H. Dellit, MD Professor, UW Allergy & Infectious Diseases Associate Medical Director Harborview Medical Center No financial conflicts Tuberculosis in King County1995-2014
Enlarging TB Lymph Node Improving or Deteriorating? History. History. Physical examination. Distribution of lymph nodes
 Enlarging TB Lymph Node Improving or Deteriorating? Dr. Lilian Lee Dr. Hamilton Hui Department of Paediatrics & Adolescent Medicine United Christian Hospital 30 August 2006 Enlarging TB lymph node - Improving
Enlarging TB Lymph Node Improving or Deteriorating? Dr. Lilian Lee Dr. Hamilton Hui Department of Paediatrics & Adolescent Medicine United Christian Hospital 30 August 2006 Enlarging TB lymph node - Improving
Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
HISTORY TB = 25% ADULT DEATHS PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS & REST CAVITARY DISEASE & COLLAPSE THERAPY FRESH AIR, SUNSHINE-ROOFTOPS SOLARIA
 PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS & REST CAVITARY DISEASE & COLLAPSE THERAPY FRESH AIR, SUNSHINE-ROOFTOPS SOLARIA HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY
PRE-ANTIBIOTIC ERA SANATORIUM REGIMENS & REST CAVITARY DISEASE & COLLAPSE THERAPY FRESH AIR, SUNSHINE-ROOFTOPS SOLARIA HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY
INDUSTRIALIZATION TB = 25% ADULT DEATHS
 HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY INDUSTRIALIZATION TB = 25% ADULT DEATHS 1 GERM THEORY OF DISEASE KOCH S BACILLUS-1883 PRE-ANTIBIOTIC ERA SANATORIUM
HISTORY EGYPTIAN MUMMIES: SPINAL TB 17 th -18th CENTURIES- URBANIZATION 19th CENTURY INDUSTRIALIZATION TB = 25% ADULT DEATHS 1 GERM THEORY OF DISEASE KOCH S BACILLUS-1883 PRE-ANTIBIOTIC ERA SANATORIUM
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
TB and Comorbidities Adriana Vasquez, MD April 12, 2018
 TB and Comorbidities Adriana Vasquez, MD April 12, 2018 TB Nurse Case Management April 10 12, 2018 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Adriana Vasquez, MD has the following disclosures to make:
TB and Comorbidities Adriana Vasquez, MD April 12, 2018 TB Nurse Case Management April 10 12, 2018 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Adriana Vasquez, MD has the following disclosures to make:
9 month old with stridor, cough, low-grade fever, mild hypoxia
 9 month old with stridor, cough, low-grade fever, mild hypoxia 3 months of age CXR normal Scenarios: Pregnant woman with + PPD Next steps? CXR negative, asymptomatic: treat for LTBI after delivery (INH
9 month old with stridor, cough, low-grade fever, mild hypoxia 3 months of age CXR normal Scenarios: Pregnant woman with + PPD Next steps? CXR negative, asymptomatic: treat for LTBI after delivery (INH
Tuberculosis Elimination: The Role of the Infection Preventionist
 Tuberculosis Elimination: The Role of the Infection Preventionist Preface: What Happens when Health Care Professionals are not familiar with TB? A 15 year old student was diagnosed with highly infectious
Tuberculosis Elimination: The Role of the Infection Preventionist Preface: What Happens when Health Care Professionals are not familiar with TB? A 15 year old student was diagnosed with highly infectious
Extra pulmonary Tuberculosis
 Extra pulmonary Tuberculosis SHANNON KASPERBAUER, MD NATIONAL JEWISH HEALTH DENVER TB COURSE APRIL 2019 Disclosures Insmed: speaker, advisory board, investigator No relevant disclosures for this talk Objectives
Extra pulmonary Tuberculosis SHANNON KASPERBAUER, MD NATIONAL JEWISH HEALTH DENVER TB COURSE APRIL 2019 Disclosures Insmed: speaker, advisory board, investigator No relevant disclosures for this talk Objectives
Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts
 Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
Recognizing MDR-TB in Children. Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention February 2016
 Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
Tuberculosis: A Provider s Guide to
 Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
Pediatric Tuberculosis
 Pediatric Tuberculosis Kim Connelly Smith, MD, MPH April 7, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Kim Connelly Smith, MD, MPH has the following disclosures to
Pediatric Tuberculosis Kim Connelly Smith, MD, MPH April 7, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Kim Connelly Smith, MD, MPH has the following disclosures to
56% of these were in south east Asia and west pacific region.
 Tuberc ulosis Dr. ASAAD FARHAN ASSIST. PROF.PEDS. Learning objectives epidemiology Tuberculosis remains worlds deadliest communicable disease. TB is present in all regions of the world. WHO estimates that
Tuberc ulosis Dr. ASAAD FARHAN ASSIST. PROF.PEDS. Learning objectives epidemiology Tuberculosis remains worlds deadliest communicable disease. TB is present in all regions of the world. WHO estimates that
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013
 Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Characteristics of Mycobacterium
 Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
Management of Pediatric Tuberculosis in New Jersey
 Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
Peripheral mycobacterial lymphadenitis (TB, NTM and BCG)
") Peripheral mycobacterial lymphadenitis (TB, NTM and BCG) H Simon Schaaf Desmond Tutu TB Centre, Department of Paediatrics and Child Health, Stellenbosch University, Cape Town, South Africa Questions Peripheral
Peripheral mycobacterial lymphadenitis (TB, NTM and BCG) H Simon Schaaf Desmond Tutu TB Centre, Department of Paediatrics and Child Health, Stellenbosch University, Cape Town, South Africa Questions Peripheral
At the end of this session, participants will be able to:
 Advanced Concepts in Pediatric Tuberculosis: Infection Control, Source Case and Contact Investigation Ana M. Alvarez, M.D. Associate Professor Division of Pediatric Infectious Diseases and Immunology University
Advanced Concepts in Pediatric Tuberculosis: Infection Control, Source Case and Contact Investigation Ana M. Alvarez, M.D. Associate Professor Division of Pediatric Infectious Diseases and Immunology University
TB in the Patient with HIV
 TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
The Diagnosis of Active TB. Deborah McMahan, MD TB Intensive September 28, 2017
 The Diagnosis of Active TB Deborah McMahan, MD TB Intensive September 28, 2017 Agenda Epidemiology Big picture Conditions that Should Make You Suspicious Which test? Eeenie meenie miny mo Radiographic
The Diagnosis of Active TB Deborah McMahan, MD TB Intensive September 28, 2017 Agenda Epidemiology Big picture Conditions that Should Make You Suspicious Which test? Eeenie meenie miny mo Radiographic
TB Nurse Case Management Waukesha, Wisconsin March 31 April 2, Pediatric TB Michelle Hulse, MD April 1, 2009
 TB Nurse Case Management Waukesha, Wisconsin March 31 April 2, 2009 Pediatric TB Michelle Hulse, MD April 1, 2009 Pediatric Tuberculosis HNTC Nurse Case Management Course April 1, 2009 Waukesha, Wisconsin
TB Nurse Case Management Waukesha, Wisconsin March 31 April 2, 2009 Pediatric TB Michelle Hulse, MD April 1, 2009 Pediatric Tuberculosis HNTC Nurse Case Management Course April 1, 2009 Waukesha, Wisconsin
TB Intensive San Antonio, Texas December 1-3, 2010
 TB Intensive San Antonio, Texas December 1-3, 2010 TB Pathogenesis and Transmission Lynn Horvath, MD; TCID December 1, 2010 Tuberculosis Pathogenesis Lynn L. Horvath, MD, FACP, FIDSA Associate Professor
TB Intensive San Antonio, Texas December 1-3, 2010 TB Pathogenesis and Transmission Lynn Horvath, MD; TCID December 1, 2010 Tuberculosis Pathogenesis Lynn L. Horvath, MD, FACP, FIDSA Associate Professor
Urinary Schistosomiasis: Urological manifestations &complications. Dr MJ Engelbrecht Department of Urology
 Urinary Schistosomiasis: Urological manifestations &complications Dr MJ Engelbrecht Department of Urology Clinical presentation Three clinical stages Swimmer s itch Acute schistosomiasis Chronic schistosomiasis
Urinary Schistosomiasis: Urological manifestations &complications Dr MJ Engelbrecht Department of Urology Clinical presentation Three clinical stages Swimmer s itch Acute schistosomiasis Chronic schistosomiasis
Latent TB Infection (LTBI) Strategies for Detection and Management
 Strategies for Detection and Management") Latent TB Infection (LTBI) Strategies for Detection and Management Patrick T. Dowling MD,MPH Professor and Chair Dept of Family Medicine David Geffen School of Medicine at UCLA Pri-Med March 29 2014 Pdowling@mednet.ucla.edu
Latent TB Infection (LTBI) Strategies for Detection and Management Patrick T. Dowling MD,MPH Professor and Chair Dept of Family Medicine David Geffen School of Medicine at UCLA Pri-Med March 29 2014 Pdowling@mednet.ucla.edu
MYCOBACTERIUM. Mycobacterium Tuberculosis (Mtb) nontuberculous mycobacteria (NTM) Mycobacterium lepray
 nontuberculous mycobacteria (NTM) Mycobacterium lepray") MYCOBACTERIUM nontuberculous mycobacteria (NTM) Mycobacterium Tuberculosis (Mtb) Mycobacterium lepray 1-tubercle bacilli are thin 2- straight rods 3- obligate aerobes 4- derive energy from the oxidation
MYCOBACTERIUM nontuberculous mycobacteria (NTM) Mycobacterium Tuberculosis (Mtb) Mycobacterium lepray 1-tubercle bacilli are thin 2- straight rods 3- obligate aerobes 4- derive energy from the oxidation
PEDIATRIC TUBERCULOSIS. Objectives. Children are not just small adults. Pediatric Tuberculosis 1
 PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
TB: A Supplement to GP CLINICS
 TB: A Supplement to GP CLINICS Chapter 10: Childhood Tuberculosis: Q&A For Primary Care Physicians Author: Madhukar Pai, MD, PhD Author and Series Editor What is Childhood TB and who is at risk? India
TB: A Supplement to GP CLINICS Chapter 10: Childhood Tuberculosis: Q&A For Primary Care Physicians Author: Madhukar Pai, MD, PhD Author and Series Editor What is Childhood TB and who is at risk? India
Epidemiology and diagnosis of MDR-TB in children H Simon Schaaf
 Epidemiology and diagnosis of MDR-TB in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Definitions
Epidemiology and diagnosis of MDR-TB in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Definitions
Scott Lindquist MD MPH Tuberculosis Medical Consultant Washington State DOH and Kitsap County Health Officer
 Tuberculosis in the 21 st Century Scott Lindquist MD MPH Tuberculosis Medical Consultant Washington State DOH and Kitsap County Health Officer Feedback Poll In my opinion, the recent media coverage of
Tuberculosis in the 21 st Century Scott Lindquist MD MPH Tuberculosis Medical Consultant Washington State DOH and Kitsap County Health Officer Feedback Poll In my opinion, the recent media coverage of