Understanding the unmet medical needs with current ART
|
|
|
- Kelly Caldwell
- 5 years ago
- Views:
Transcription
1 Thanks: Polly Clayden, Francesca Conradie, Loyd Mulenga, Gary Maartens, Andrew Hill, David Ripin, Elli Katabira, Chris Duncombe, Nathan Ford, Marco Vitoria, WHO, Trip Gullik Industry: Gilead, Janssen, Viiv, Abbott, Merck, GSK Understanding the unmet medical needs with current ART Francois Venter Wits Reproductive Health & HIV Institute
2 28 approved drugs Up to 10 recommended first-line regimens
3
4 What is coming next from WHO??Test and Treat vs staying at 500?use of integrase inhibitors Both are linked
5 Major Guidelines for Initiation of Antiretroviral Therapy Guideline AIDS or HIV-Related Symptoms CD4+ Cell Count CD4+ Cell Count 200- CD4+ Cell Count 350- < 200/mm 3 350/mm 3 500/mm 3 CD4+ Cell Count > 500 cells/mm 3 DHHS-USA, 2014 Yes Yes Yes Yes 1 Yes 2 International AIDS Society-USA, 2014 Yes Yes Yes Yes 1 Yes 2 Brazil, 2014 Yes Yes Yes Yes 1 Yes 2 European AIDS Clinical Society, 2014 British HIV Association, 2014 World Health Organization, 2014 Yes Yes Yes Consider 3 Consider 3 Yes Yes Yes Consider 3 Defer 5 Yes Yes Yes Yes 4 Defer 5 (1) Strong strength recommendation based on observational data (A-II) (2) Moderate strength recommendation based on expert opinion (B-III). (3 ) But treat all symptomatic patients, HIV+ pregnant women, HBV co-infection, HCV co-infection, HIVAN, HIV related neurocognitive disorders, ITP, non-aids cancers (including HPV) and serodiscordant couples (4) Individuals with CD4 < 350 as a priority. (5) But treat all HIV+ pregnant women,tb co-infection with active disease and HBV co-infection with severe liver disease, and serodiscordant couples SA HIV Clinicians Society 2014 SA Government, 2015 Yes Yes Yes Defer Defer Yes Yes Yes Yes Defer

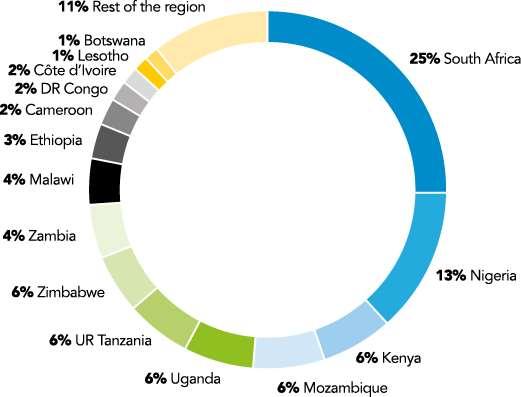
6 UNAIDS Gap Report 2014 <unaids.org>
7 ART Trials: Virologic Responses 114 studies through 2012, up to 3 years of f/u: ITT analyses 78% 43% Carr PLoS One 2014;9:e97482
8 ART Trials: Safety and Tolerability 114 studies, through 2012, up to 3 years of f/u: ITT analyses 14% 4% Carr PLoS One 2014;9:e97482
9 A widening menu of ARV use for treatment and prevention 34,000, Despite immediate increase from currently 17 million to 26 million people eligible for ART, the preventive effect will lead to decrease of number eligible after 2020 HIV+ IDU >500 HIV+ MSM > HIV+ FSW >500 Sero Discordant Couples >500 Pregnant women >500 Children HIV+ (aged 2-4) Adults HIV+/HBV+ > TB+/HIV+ >350 <350 not on ART Children in need (aged <2) - On ART (adults and children)
10 Pipeline Report

11 Think Many HIV testing programmes performing well issues such as TB and high VL less of an issue Pregnancy always an issue


12 So what we got?
13 Evolution of WHO ART Guidelines in Adults Topic When to start 1 st Line 8 options - AZT preferred 2 nd Line Boosted and non-boosted PIs CD4 200 CD4 200 CD Consider CD4 350 for TB 4 options - AZT preferred Boosted PIs -IDV/r LPV/r, SQV/r 8 options - AZT or TDFpreferred - d4t dose reduction Boosted PI - ATV/r, DRV/r, FPV/r LPV/r, SQV/r CD Irrespective CD4 for TB and HBV 6 options &FDCs - AZT or TDF preferred - d4t phase out Boosted PI - Heat stable FDC: ATV/r, LPV/r CD Irrespective CD4 for TB, HBV, PW and SDC - CD4 350 as priority 2 options & FDCs - TDF and EFV preferred across all populations Boosted PI - Heat stable FDC: ATV/r, LPV/r 3 rd Line None None None DRV/r, RAL, ETV DRV/r, RAL, ETV Viral Load Testing No Earlier initiation Simpler treatment Less toxic, more robust regimens No (Desirable) Yes (Tertiary centers) Better monitoring Yes (Phase in approach) Yes (preferred for monitoring, use of PoC, DBS) HIV/AIDS Department
14 Evolution of WHO ART Guidelines in Adults Topic When to start 1 st Line 8 options - AZT preferred 2 nd Line Boosted and non-boosted PIs CD4 200 CD4 200 CD Consider CD4 350 for TB 4 options - AZT preferred Boosted PIs -IDV/r LPV/r, SQV/r 8 options - AZT or TDFpreferred - d4t dose reduction Boosted PI - ATV/r, DRV/r, FPV/r LPV/r, SQV/r CD Irrespective CD4 for TB and HBV 6 options &FDCs - AZT or TDF preferred - d4t phase out Boosted PI - Heat stable FDC: ATV/r, LPV/r CD Irrespective CD4 for TB, HBV, PW and SDC - CD4 350 as priority 2 options & FDCs - TDF and EFV preferred across all populations Boosted PI - Heat stable FDC: ATV/r, LPV/r 3 rd Line None None None DRV/r, RAL, ETV DRV/r, RAL, ETV Viral Load Testing No Earlier initiation Simpler treatment Less toxic, more robust regimens No (Desirable) Yes (Tertiary centers) Better monitoring Yes (Phase in approach) Yes (preferred for monitoring, use of PoC, DBS) HIV/AIDS Department
15 Evolution of WHO ART Guidelines in Adults Topic When to start 1 st Line 8 options - AZT preferred 2 nd Line Boosted and non-boosted PIs CD4 200 CD4 200 CD Consider CD4 350 for TB 4 options - AZT preferred Boosted PIs -IDV/r LPV/r, SQV/r 8 options - AZT or TDFpreferred - d4t dose reduction Boosted PI - ATV/r, DRV/r, FPV/r LPV/r, SQV/r CD Irrespective CD4 for TB and HBV 6 options &FDCs - AZT or TDF preferred - d4t phase out Boosted PI - Heat stable FDC: ATV/r, LPV/r CD Irrespective CD4 for TB, HBV, PW and SDC - CD4 350 as priority 2 options & FDCs - TDF and EFV preferred across all populations Boosted PI - Heat stable FDC: ATV/r, LPV/r 3 rd Line None None None DRV/r, RAL, ETV DRV/r, RAL, ETV Viral Load Testing No Earlier initiation Simpler treatment Less toxic, more robust regimens No (Desirable) Yes (Tertiary centers) Better monitoring Yes (Phase in approach) Yes (preferred for monitoring, use of PoC, DBS) HIV/AIDS Department
16 Evolution of WHO ART Guidelines in Adults Topic When to start 1 st Line 8 options - AZT preferred 2 nd Line Boosted and non-boosted PIs CD4 200 CD4 200 CD Consider CD4 350 for TB 4 options - AZT preferred Boosted PIs -IDV/r LPV/r, SQV/r 8 options - AZT or TDFpreferred - d4t dose reduction Boosted PI - ATV/r, DRV/r, FPV/r LPV/r, SQV/r CD Irrespective CD4 for TB and HBV 6 options &FDCs - AZT or TDF preferred - d4t phase out Boosted PI - Heat stable FDC: ATV/r, LPV/r CD Irrespective CD4 for TB, HBV, PW and SDC - CD4 350 as priority 2 options & FDCs - TDF and EFV preferred across all populations Boosted PI - Heat stable FDC: ATV/r, LPV/r 3 rd Line None None None DRV/r, RAL, ETV DRV/r, RAL, ETV Viral Load Testing No Earlier initiation Simpler treatment Less toxic, more robust regimens No (Desirable) Yes (Tertiary centers) Better monitoring Yes (Phase in approach) Yes (preferred for monitoring, use of PoC, DBS) HIV/AIDS Department
17 Drug optimization Science evolved: smarter and better HIV treatment options are now available
 Increasing concern about CNS side")
18 In terms of first line therapy (TDF+XTC+EFV) Was 2013 just a brief harmonisation event? EFV now routinely substituted in developed world due to side effects (where TB less of a problem) Increasing concern about CNS side effects (also lipids, hepatitis, rash, gynaecomastia)
19 $ PPPY With limited resources, a public health approach needs to balance both costs and effectiveness in order to maximize efficiencies Drugs that have been prioritized as having clinical superiority have shown dramatic price reductions over short periods of time even since CADO in 2010 $400 $350 21% price reduction $300 $250 $200 $150 $100 $50 77% price reduction 72% price reduction $ EFV TDF ATV/r

20 TDF XTC EFV AZT XTC PI(lopinavir or atazanavir) XTC, other nukes Darunavir Raltegravir Etravirine
21 Currently available (or near-available) coformulated antiretroviral agents and regimens Agent D4T/3TC D4T/3TC/NVP ZDV/3TC ZDV/3TC/ABC LPV/RTV ATV/RTV DTG/ABC/3TC ABC/3TC TDF/XTC TDF/XTC/EFV TDF/FTC/RPV TDF/FTC/EVG/COBI Regimen Dual NRTI NNRTI + dual NRTI Dual NRTI Triple NRTI Boosted PI Boosted PI INSTI + dual NNRTI Dual NRTI Dual NRTI NNRTI + dual NRTI NNRTI + dual NRTI Dual NRTI + INSTI + booster 21
22 TDF XTC EFV AZT XTC PI(lopinavir or atazanavir) XTC, other nukes Darunavir Raltegravir Etravirine
 Well tolerated, FDCs galore,")
23 Tenofovir has taken over the world! 1st line recommendation by WHO; feature in EVERY guideline (some have ABC) Well tolerated, FDCs galore, daily Cheap (only alternative that is cheaper is d4t) Hep B for free
24 WHO Guidelines: 2013 Update Recommended Regimens NNRTI based EFV + (TDF/FTC or AZT/3TC) Alternative Regimens NNRTI based NVP + (TDF/FTC or AZT/3TC) 2013 Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection. WHO; 2013 June. 24
25 Changes in D4T, AZT & TDF use ( ) Between 2 to 4 million people using AZT containing regimen in WHO AMDS database, /15/2018 (preliminary data) 25
26 Now add PrEP TDF
27 Is API production capacity a potential treatment bottleneck? Situation of API production capacity for TDF and EFV with major API producers ( WHO API manufacturer survey, May 2013) Major parameters TDF EFV Number of API producers in API production capacity in 2012 (in metric tons)* >1,500 >2,210 Estimated number of patients using regimens containing the API in end of 2012 Number of patients that could be treated in end of ,500,000 3,700,000 >13,800,000 >10,000,000 (*) Data from some major manufacturers were not reported. The manufacturers also mentioned that they are all in the process of increasing capacity. WHO HIV/AMDS, 2014 (preliminary data)
 TDF EFV 2012 7 8 API production capacity in 2012 (in metric tons)* >1,500 >2,210")
28 Major parameters Number of API producers in Is API production capacity a potential treatment bottleneck? Situation of API production capacity for TDF and EFV with major API producers ( WHO API manufacturer survey, May 2013) TDF EFV API production capacity in 2012 (in metric tons)* >1,500 >2,210 Estimated number of patients using regimens containing the API in end of 2012 Number of patients that could be treated in end of 2012 Concern: API may become a huge problem if 20 by 20 AND PrEP come into play 3,500,000 3,700,000 >13,800,000 >10,000,000 (*) Data from some major manufacturers were not reported. The manufacturers also mentioned that they are all in the process of increasing capacity. WHO HIV/AMDS, 2014 (preliminary data)
29 Tenofovir alafenamide Slightly better safety profile than TDF ( at 10 or 25mg vs 300mg). But being tested as co-formulations Preliminary results promising will it simply replace TDF? Less API, less toxicity (?coformulations estimated availability to LMIC 2020) TDF analogue CHAI 200mg vs 300mg: may be available
30 Studies 104/111: Tenofovir Alafenamide Fumarate vs TDF in Treatment-Naive Pts Parallel, randomized, double-blind, active-controlled phase III studies Primary endpoint: HIV-1 RNA at Wk 48 Stratified by HIV-1 RNA, CD4+ cell count, geographic region Wk 48 Primary endpoint Wk 144 Treatment-naive HIV-infected pts with HIV-1 RNA 1000 copies/ml, egfr 50 ml/min (N = 1733) *10/200/150/150 mg once daily. 300/200/150/150 mg once daily. TAF/FTC/EVG/COBI* single-tablet regimen (n = 866) TDF/FTC/EVG/COBI single-tablet regimen (n = 867) Wohl DA, et al. CROI Abstract 113LB.
31 Pts (%) Studies 104/111: TAF Noninferior to Δ +2.0% (95% CI: -0.7% to +4.7) n = Virologic Success* Virologic Failure TDF at Week 48 TAF/FTC/EVG/COBI (n = 866) TDF/FTC/EVG/COBI (n = 867) No Data *HIV-1 RNA < 50 c/ml as defined by FDA Snapshot algorithm Discontinued for AE, death, or missing data. Wohl DA, et al. CROI Abstract 113LB. Reproduced with permission. 6 TAF also noninferior to TDF at Wk 48 in each study (104 and 111) Results similar across all baseline virologic and demographic subgroups 7 pts in TAF arm and 5 pts in TDF arm with NRTI resistance at VF 1 in TAF arm and 2 in TDF arm with combined M184V/I + K65R 5 pts in TAF arm and 3 pts in TDF arm with INSTI resistance at VF 0.9% in TAF arm and 1.5% in TDF arm discontinued due to AE CD4+ increases greater in TAF arm: 211 vs 181 (P =.024)
32 Mean Δ From BL in egfr, ml/min (Cockcroft-Gault) Renal Markers With TAF and TDF at Wk Smaller decreases in egfr with TAF [1] P < TAF/FTC/EVG/COBI (n = 866) TDF/FTC/EVG/COBI (n = 867) In separate single-arm trial of virologically suppressed pts with egfr ml/min switched to open-label TAF/FTC/EVG/COBI [2] 65% on TDF at BL At Wk 48 after switch: Smaller changes in proteinuria with TAF [1] Marker Time (Wks) Median % Change From BL in Urine Protein:Creatinine Ratio TAF (n = 866) TDF (n = 867) P Value Protein <.001 Albumin <.001 Retinol-binding protein <.001 β 2 -microglobulin < % maintained virologic suppression No change in egfr Reduction in proteinuria and markers of renal tubular function Improvement in hip and spine BMD 1. Sax P, et al. CROI Abstract 143. Reproduced with permission. 2. Pozniak A, et al. CROI Abstract 795.
33 Mean % Change From BL Studies 104/111: Significantly Smaller Decline in Hip and Spine BMD With TAF Significantly smaller decline in hip and spine BMD with TAF TAF/FTC/EVG/COBI (n = 866) TDF/FTC/EVG/COBI (n = 867) Change in Spine BMD Higher lipid levels with TAF, but TC:HDL-C ratio same as TDF [1] n n = 845 = 850 Wk P < Change in Hip BMD Wk P < Sax P, et al. CROI Abstract 143. Reproduced with permission.
34
35 What next on TDF? d4t study will part-answer bone and renal worries; otherwise, just wait TAF likely to replace it; TDF-CHAI 200mg Lower doses AZT, d4t; ABC, other drugs unlikely to displace it
36 TDF XTC EFV AZT XTC PI(lopinavir or atazanavir) XTC, other nukes Darunavir Raltegravir Etravirine

37 Efavirenz Daily, cheap, co-formulated, huge experience base, TB (and most everything else)-friendly EFV side effects predictable, treatable, substitutions easy Everyone pretty happy re teratogenicity
38 BUT Increasing recognition of CNS side effects -?Africans stoic? More nb in asymptomatics Rash, hepatitis, gynaecomastia, lipids ENCORE (Lancet 2013) 400mg vs 600mg less discontinuations, but very little change in side effects Concerns about 400 mg dose in PMTCT and TB
 For composite endpoint Only trend for completed/attempted suicide (17 events occured) EFV EFV-free Lack of association between use of")

39 Depression Meta-analysis n=5332, 4 RCT Efavirenz (6%) 2x higher risk for suicidality Rilpivirine (8%) Elvitegravir/COBI (5%) Raltegravir (6%) Atazanavir/r (2%) For composite endpoint Only trend for completed/attempted suicide (17 events occured) EFV EFV-free Lack of association between use of efavirenz and death from suicide: evidence from the D:A:D study #O315 Wednesday 5 November C. Smith; L. Ryom; A. d Arminio Monforte; P. Reiss; A. Mocroft; W. El-Sadr; R. Weber; M. Law; C. Sabin; J. Lundgren. Cohen et al., Lancet 2011; Molina et al, Lancet 2011; Elion et al., JAIDS 2013; Mollan et al, Ann Intern Med 2014

40 Alternatives Integrase inhibitors Rilprivirine
41 What about: Dolutegravir (raltegravir and elvitegravir expensive) Wunderkind of the moment 50 mg once-daily (in naïve patients) Very good efficacy Minimal toxicity Pregnancy category B Superior to EFV at 48 weeks in naïve patients SINGLE study (compared ABC/3TC/DTG with TDF/FTC/EFV. ) but safer, not virologically better Potential to be low cost and coformulated Walmsley SL et al. N Engl J Med. November 2013 FDA press statement. August 2013
42 What is the cost if we switch from EFV to DTG? Millions of patients will need to be switched (assuming stable patients on EFV will move, seems likely) huge undertaking and the manufacturing changes will likely be slightly chaotic Moving from EFV to DTG unlikely to be a big deal (?VL) ; reverse a problem Training how big an issue if all you lose is side effects??harmonisation between and within different countries private vs public sector, cross borders Pregnancy limited data TB studies are needed Studies largely done in men It s a new agent what happens if: it doesn t work in TB? Pregnancy? New side effect?

43 TDF XTC EFV AZT XTC PI(lopinavir or atazanavir) XTC, other nukes Darunavir Raltegravir Etravirine
44 AZT Toxic???any role for AZT in future??? EARNEST does it matter what the nukes are? Could we recycle TDF/FTC?

45 TDF XTC EFV AZT XTC PI(lopinavir or atazanavir) XTC, other nukes Darunavir Raltegravir Etravirine
46 ?: Darunavir in 2 nd line Best PI better side effects If we get the dose down from 800/100? 600/100?400/100 lower cost, less side effects BUT will the virological potency be maintained? BUT is lopinavir all we need? EARNEST was very successful Will we even need a second line if DTG in 1 st? Studies planned

47 (Short term) future dream? (photo credit John Mellors)
48 Pill "A" to Pill "B" two single tablet regimens? Pill "A" TDF/3TC/EFV400 $100 Pill "B" DRV400/r/DTG $250 Two pills, used in sequence Simple treatment rule task shifting No overlapping drug resistance Mass generic production Low cost: $100 and $250 per person-year
49 Pill "A" to Pill "B" two single tablet regimens? Pill "A TAF/FTC/DTG (275mg) TDF/3TC/EFV400 $100 Pil?/FTC/darunavir (400mg)/rit 700+?) Pill "B" DRV400/r/DTG $250 TDF/3TC/EFV400 $100 Two pills, used in sequence Simple treatment rule task shifting No overlapping drug resistance Mass generic production Low cost: $100 and $250 per person-year



50 What about the children? Granules and sprinkles lpv/rit, raltegravir, others Low dose d4t planned ABC/TDF concerns

51 Conclusions New drugs likely to be in play in our area EFV 600mg -?if will be displaced

52
What next? Francois Venter. ART new drugs, new studies. Wits Reproductive Health & HIV Institute
 Thanks: Polly Clayden, Francesca Conradie, Loyd Mulenga, Gary Maartens, Andrew Hill, David Ripin, Elli Katabira, Chris Duncombe, Nathan Ford, Marco Vitoria, WHO Industry: Gilead, Janssen, ViivV Abbott,
Thanks: Polly Clayden, Francesca Conradie, Loyd Mulenga, Gary Maartens, Andrew Hill, David Ripin, Elli Katabira, Chris Duncombe, Nathan Ford, Marco Vitoria, WHO Industry: Gilead, Janssen, ViivV Abbott,
Unmet needs and challenges of current ART in South Africa. Michelle Moorhouse 21 Nov 2015
 Unmet needs and challenges of current ART in South Africa Michelle Moorhouse 21 Nov 2015 SA Snapshot Òct 2015 6-7 million HIV-positive: 18% world total, 25% of Southern Africa 3.2 on first line ART: consume
Unmet needs and challenges of current ART in South Africa Michelle Moorhouse 21 Nov 2015 SA Snapshot Òct 2015 6-7 million HIV-positive: 18% world total, 25% of Southern Africa 3.2 on first line ART: consume
Is current first line ART good enough? Francois Venter Wits Reproductive Health & HIV Research Institute
 Is current first line ART good enough? Francois Venter Wits Reproductive Health & HIV Research Institute Results: by April 2011 Budget: $3.5 billion 80% of 3,686 health facilities providing ARVs 50% ARV
Is current first line ART good enough? Francois Venter Wits Reproductive Health & HIV Research Institute Results: by April 2011 Budget: $3.5 billion 80% of 3,686 health facilities providing ARVs 50% ARV
Medical Challenges of HIV/AIDS pandemic: The WHO perspective. SOLTHIS HIV Forum
 Medical Challenges of HIV/AIDS pandemic: The WHO perspective SOLTHIS HIV Forum Marco Vitoria HIV/AIDS Department World Health Organization September 2013 Topic 2002 2003 2006 2010 2013 When to start 1
Medical Challenges of HIV/AIDS pandemic: The WHO perspective SOLTHIS HIV Forum Marco Vitoria HIV/AIDS Department World Health Organization September 2013 Topic 2002 2003 2006 2010 2013 When to start 1
The next generation of ART regimens
 The next generation of ART regimens By Gary Maartens Presented by Dirk Hagemeister Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI YASEKAPA UNIVERSITEIT VAN KAAPSTAD Current state
The next generation of ART regimens By Gary Maartens Presented by Dirk Hagemeister Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI YASEKAPA UNIVERSITEIT VAN KAAPSTAD Current state
Overview of 2013 WHO consolidated ARV guidelines and update plans. Marco Vitoria HIV/AIDS Department WHO Geneva September 2014
 AMDS ANNUAL STAKEHOLDERS AND PARTNERS MEETING Overview of 2013 WHO consolidated ARV guidelines and update plans Marco Vitoria HIV/AIDS Department WHO Geneva September 2014 AMDS ANNUAL STAKEHOLDERS AND
AMDS ANNUAL STAKEHOLDERS AND PARTNERS MEETING Overview of 2013 WHO consolidated ARV guidelines and update plans Marco Vitoria HIV/AIDS Department WHO Geneva September 2014 AMDS ANNUAL STAKEHOLDERS AND
What's new in the WHO ART guidelines How did markets react?
 WHO 2013 ARV Guidelines What's new in the WHO ART guidelines How did markets react? Dr. J. Perriëns Coordinator, HIV Technology and Commodities HIV department, WHO, Geneva When to start in adults Starting
WHO 2013 ARV Guidelines What's new in the WHO ART guidelines How did markets react? Dr. J. Perriëns Coordinator, HIV Technology and Commodities HIV department, WHO, Geneva When to start in adults Starting
Progress toward Universal ART Access: Innovations and Treatment 2.0. Marco Vitoria World Health Organization September 2013
 Progress toward Universal ART Access: Innovations and Treatment 2.0 Marco Vitoria World Health Organization September 2013 The need for scalable, more efficient treatment models Simpler drugs Point of
Progress toward Universal ART Access: Innovations and Treatment 2.0 Marco Vitoria World Health Organization September 2013 The need for scalable, more efficient treatment models Simpler drugs Point of
CADO/PADO: Update on 2015 WHO Consolidated guidelines Towards Treat All in the context of SDGs
 CADO/PADO: Update on 2015 WHO Consolidated guidelines Towards Treat All in the context of SDGs Meg Doherty, Treatment and Care Coordinator WHO HQ Outline What s new in ARV Guidelines Drug optimisation
CADO/PADO: Update on 2015 WHO Consolidated guidelines Towards Treat All in the context of SDGs Meg Doherty, Treatment and Care Coordinator WHO HQ Outline What s new in ARV Guidelines Drug optimisation
TDF containing ART: Efficacy and Safety. Dr Lloyd B. Mulenga Adult Infectious Diseases Centre University Teaching Hospital Lusaka, Zambia
 TDF containing ART: Efficacy and Safety Dr Lloyd B. Mulenga Adult Infectious Diseases Centre University Teaching Hospital Lusaka, Zambia 1 Indications Treatment of HIV-1 in combination with other antiretroviral
TDF containing ART: Efficacy and Safety Dr Lloyd B. Mulenga Adult Infectious Diseases Centre University Teaching Hospital Lusaka, Zambia 1 Indications Treatment of HIV-1 in combination with other antiretroviral
ART rapid scale up: the implications for patient care and retention. Dr Francesca Conradie Southern African HIV Clinicians Society
 ART rapid scale up: the implications for patient care and retention Dr Francesca Conradie Southern African HIV Clinicians Society Agenda Why do we need rapid scale up? Is there enough evidence for rapid
ART rapid scale up: the implications for patient care and retention Dr Francesca Conradie Southern African HIV Clinicians Society Agenda Why do we need rapid scale up? Is there enough evidence for rapid
PRIORITIES FOR HIV/AIDS PROCUREMENT AND PRODUCT DEVELOPMENT
 PRIORITIES FOR HIV/AIDS PROCUREMENT AND PRODUCT DEVELOPMENT Dr Chewe Luo MMed (Paeds), Mtrop Paed, PhD Senior Adviser and Team Leader Country Programme Scale up HIV Section Programme Division UNICEF, NY
PRIORITIES FOR HIV/AIDS PROCUREMENT AND PRODUCT DEVELOPMENT Dr Chewe Luo MMed (Paeds), Mtrop Paed, PhD Senior Adviser and Team Leader Country Programme Scale up HIV Section Programme Division UNICEF, NY
Switching ARV Regimens: Managing Toxicity and Improving Tolerability; Switches & Class-Sparing Approaches
 Switching ARV Regimens: Managing Toxicity and Improving Tolerability; Switches & Class-Sparing Approaches Harry W. Lampiris, MD Chief, Infectious Disease Section, San Francisco VA Medical Center Professor
Switching ARV Regimens: Managing Toxicity and Improving Tolerability; Switches & Class-Sparing Approaches Harry W. Lampiris, MD Chief, Infectious Disease Section, San Francisco VA Medical Center Professor
Clinical support for reduced drug regimens. David A Cooper The University of New South Wales Sydney, Australia
 Clinical support for reduced drug regimens David A Cooper The University of New South Wales Sydney, Australia Clinical support for reduced drug regimens First line optimisation Virological failure New
Clinical support for reduced drug regimens David A Cooper The University of New South Wales Sydney, Australia Clinical support for reduced drug regimens First line optimisation Virological failure New
HIV Treatment Update. Anton Pozniak Consultant Physician, Director of HIV Services Chelsea and Westminster Hospital, London
 HIV Treatment Update Anton Pozniak Consultant Physician, Director of HIV Services Chelsea and Westminster Hospital, London Guidelines Nuke sparing Nukes Efavirenz placement as the gold standard ARV Role
HIV Treatment Update Anton Pozniak Consultant Physician, Director of HIV Services Chelsea and Westminster Hospital, London Guidelines Nuke sparing Nukes Efavirenz placement as the gold standard ARV Role
More Options, Some Opinions Initial Therapies for HIV Judith S. Currier, MD
 More Options, Some Opinions Initial Therapies for HIV Judith S. Currier, MD More Options, Some Opinions: Initial Therapies for HIV Judith S. Currier, MD University of California Los Angeles Los Angeles,
More Options, Some Opinions Initial Therapies for HIV Judith S. Currier, MD More Options, Some Opinions: Initial Therapies for HIV Judith S. Currier, MD University of California Los Angeles Los Angeles,
HIV - Therapy Principles
 HIV - Therapy Principles Manuel Battegay and Christine Katlama Basel, Switzerland and Paris, France Disclosure MB has received honoraria for advisory board participation from Gilead, MSD, Pfizer, ViiV
HIV - Therapy Principles Manuel Battegay and Christine Katlama Basel, Switzerland and Paris, France Disclosure MB has received honoraria for advisory board participation from Gilead, MSD, Pfizer, ViiV
HIV Update Allegra CPD Day Program Port Elizabeth Dr L E Nojoko
 HIV Update 2014 Allegra CPD Day Program Port Elizabeth 12-02-2014 Dr L E Nojoko Global estimates for adults and children 2011 People living with HIV 34.0 million [31.4 million 35.9 million] New HIV infections
HIV Update 2014 Allegra CPD Day Program Port Elizabeth 12-02-2014 Dr L E Nojoko Global estimates for adults and children 2011 People living with HIV 34.0 million [31.4 million 35.9 million] New HIV infections
Can we make first line ART better?
 Can we make first line ART better? Dr Angela Hartwig 8 th SA AIDS Conference, Durban Skills Building Session 15 June 2017 With thanks to Francois Venter and the people who gave him slides Characteristics
Can we make first line ART better? Dr Angela Hartwig 8 th SA AIDS Conference, Durban Skills Building Session 15 June 2017 With thanks to Francois Venter and the people who gave him slides Characteristics
Antiretroviral Treatment Strategies: Clinical Case Presentation
 Antiretroviral Treatment Strategies: Clinical Case Presentation Department of Internal Medicine, Far Eastern Memorial Hospital, New Taipei City, Taiwan Chia-Jui, Yang M.D Disclosure No conflicts of interests.
Antiretroviral Treatment Strategies: Clinical Case Presentation Department of Internal Medicine, Far Eastern Memorial Hospital, New Taipei City, Taiwan Chia-Jui, Yang M.D Disclosure No conflicts of interests.
HIV Treatment: State of the Art 2013
 HIV Treatment: State of the Art 2013 Daniel R. Kuritzkes, MD Chief, Division of Infectious Diseases Brigham and Women s Hospital Professor of Medicine Harvard Medical School Success of current ART Substantial
HIV Treatment: State of the Art 2013 Daniel R. Kuritzkes, MD Chief, Division of Infectious Diseases Brigham and Women s Hospital Professor of Medicine Harvard Medical School Success of current ART Substantial
Can we make first line ART better?
 Can we make first line ART better? Dr David Stead Treatment Optimization HIV Clinicians Society Workshop 25 November 2017 With thanks to Francois Venter and the people who gave him slides Characteristics
Can we make first line ART better? Dr David Stead Treatment Optimization HIV Clinicians Society Workshop 25 November 2017 With thanks to Francois Venter and the people who gave him slides Characteristics
Disclosures. Update on HIV Drug Therapy: A Case based Discussion. Case # 1: Dr. Grant has received grant support from BMS, Gilead, Janssen, and Viiv
 Disclosures Update on HIV Drug Therapy: A Case based Discussion Dr. Grant has received grant support from BMS, Gilead, Janssen, and Viiv Philip Grant Assistant Professor Division of Infectious Diseases
Disclosures Update on HIV Drug Therapy: A Case based Discussion Dr. Grant has received grant support from BMS, Gilead, Janssen, and Viiv Philip Grant Assistant Professor Division of Infectious Diseases
Treating HIV: When the Guidelines Don t Fit. Joel Gallant, MD, MPH. Southwest CARE Center Santa Fe, New Mexico
 Treating HIV: When the Guidelines Don t Fit Joel Gallant, MD, MPH Southwest CARE Center Santa Fe, New Mexico Johns Hopkins University School of Medicine University of New Mexico School of Medicine Disclosures
Treating HIV: When the Guidelines Don t Fit Joel Gallant, MD, MPH Southwest CARE Center Santa Fe, New Mexico Johns Hopkins University School of Medicine University of New Mexico School of Medicine Disclosures
Are the current doses of ARV correct. Richard Elion MD Associate Adjunct Clinical Professor of Medicine Johns Hopkins School of Medicine
 Are the current doses of ARV correct Richard Elion MD Associate Adjunct Clinical Professor of Medicine Johns Hopkins School of Medicine Can we lower doses of HIV meds safely? Consensus Panel in Alexandria
Are the current doses of ARV correct Richard Elion MD Associate Adjunct Clinical Professor of Medicine Johns Hopkins School of Medicine Can we lower doses of HIV meds safely? Consensus Panel in Alexandria
Antiretroviral Therapy in 2016
 Antiretroviral Therapy in 2016 Joel Gallant, MD, MPH Southwest CARE Center Santa Fe, NM University of New Mexico School of Medicine Johns Hopkins University School of Medicine Disclosures Consulting, Advisory
Antiretroviral Therapy in 2016 Joel Gallant, MD, MPH Southwest CARE Center Santa Fe, NM University of New Mexico School of Medicine Johns Hopkins University School of Medicine Disclosures Consulting, Advisory
ART Optimization (New emerging molecules) KPA PRE-CONFERENCE 24 th April 2018 Dr Justine Jelagat Odionyi (EGPAF)/Dr Virginia Karanja(CHS)
 KPA PRE-CONFERENCE 24 th April 2018 Dr Justine Jelagat Odionyi (EGPAF)/Dr Virginia Karanja(CHS)") ART Optimization (New emerging molecules) KPA PRE-CONFERENCE 24 th April 2018 Dr Justine Jelagat Odionyi (EGPAF)/Dr Virginia Karanja(CHS) Outline Introduction New ART molecules already adopted Dolutegravir
ART Optimization (New emerging molecules) KPA PRE-CONFERENCE 24 th April 2018 Dr Justine Jelagat Odionyi (EGPAF)/Dr Virginia Karanja(CHS) Outline Introduction New ART molecules already adopted Dolutegravir
Didactic Series. CROI 2014 Update. March 27, 2014
 Didactic Series CROI 2014 Update Christian Ramers, MD, MPH Family Health Centers of San Diego Ciaccio Memorial Clinic Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director,
Didactic Series CROI 2014 Update Christian Ramers, MD, MPH Family Health Centers of San Diego Ciaccio Memorial Clinic Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director,
Update on CADO/PADO: what are the challenges in using the current guidelines and foreseen ARV revisions: opportunities and challenges
 Update on CADO/PADO: what are the challenges in using the current guidelines and foreseen ARV revisions: opportunities and challenges Treatment and Care Team Meg Doherty, Marco Vitoria, Martina Penazzato,
Update on CADO/PADO: what are the challenges in using the current guidelines and foreseen ARV revisions: opportunities and challenges Treatment and Care Team Meg Doherty, Marco Vitoria, Martina Penazzato,
First line ART Rilpirivine A New NNRTI. Chris Jack Physician, Durdoc Centre ethekwini
 First line ART Rilpirivine A New NNRTI Chris Jack Physician, Durdoc Centre ethekwini Overview: Rilpirivine an option for ARV Naïve patients History Current guidelines Efficacy and Safety Tolerability /
First line ART Rilpirivine A New NNRTI Chris Jack Physician, Durdoc Centre ethekwini Overview: Rilpirivine an option for ARV Naïve patients History Current guidelines Efficacy and Safety Tolerability /
SA HIV Clinicians Society Adult ART guidelines
 SA HIV Clinicians Society Adult ART guidelines In draft format Graeme Meintjes (on behalf of the guidelines committee) Selected topics When to start ART First-line Second-line Third-line Patients with
SA HIV Clinicians Society Adult ART guidelines In draft format Graeme Meintjes (on behalf of the guidelines committee) Selected topics When to start ART First-line Second-line Third-line Patients with
Efavirenz vs dolutegravir for 1st line ART: Is it time to change? The argument AGAINST. Graeme Meintjes University of Cape Town
 Efavirenz vs dolutegravir for 1st line ART: Is it time to change? The argument AGAINST Graeme Meintjes University of Cape Town Benefits of dolutegravir Superior efficacy in SINGLE trial Side effect profile
Efavirenz vs dolutegravir for 1st line ART: Is it time to change? The argument AGAINST Graeme Meintjes University of Cape Town Benefits of dolutegravir Superior efficacy in SINGLE trial Side effect profile
HIV Treatment Update. Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University
 HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
BHIVA antiretroviral treatment guidelines 2015
 BHIVA antiretroviral treatment guidelines 2015 Duncan Churchill Brighton & Sussex University Hospitals NHS Trust Laura Waters Mortimer Market Centre, CNWL Duncan Churchill GENERAL POINTS & WHEN TO START
BHIVA antiretroviral treatment guidelines 2015 Duncan Churchill Brighton & Sussex University Hospitals NHS Trust Laura Waters Mortimer Market Centre, CNWL Duncan Churchill GENERAL POINTS & WHEN TO START
Starting and Switching ART: 2016
 Starting and Switching ART: 2016 Luke Jerram Rajesh T. Gandhi, M.D. Massachusetts General Hospital Harvard Medical School Disclosures: grant support from EBSCO, Gilead, Merck, Viiv Thanks to Henry Sunpath,
Starting and Switching ART: 2016 Luke Jerram Rajesh T. Gandhi, M.D. Massachusetts General Hospital Harvard Medical School Disclosures: grant support from EBSCO, Gilead, Merck, Viiv Thanks to Henry Sunpath,
Didactic Series. CROI Update - II. Christian B. Ramers, MD, MPH Family Health Centers of San Diego Ciaccio Memorial Clinic 5/28/15
 Didactic Series CROI Update - II Christian B. Ramers, MD, MPH Family Health Centers of San Diego Ciaccio Memorial Clinic 5/28/15 ACCREDITATION STATEMENT: University of California, San Diego School of Medicine
Didactic Series CROI Update - II Christian B. Ramers, MD, MPH Family Health Centers of San Diego Ciaccio Memorial Clinic 5/28/15 ACCREDITATION STATEMENT: University of California, San Diego School of Medicine
Forecasting pipeline ARVs. Joseph Perriëns Sandeep Juneja Aastha Gupta
 Forecasting pipeline ARVs Joseph Perriëns Sandeep Juneja Aastha Gupta Presently: lack of visibility causes a gap between demand and generic production for new drugs Patent Holder R&D Marketing 3-4 yrs
Forecasting pipeline ARVs Joseph Perriëns Sandeep Juneja Aastha Gupta Presently: lack of visibility causes a gap between demand and generic production for new drugs Patent Holder R&D Marketing 3-4 yrs
Immediate Offer of HIV Treatment: How To Deliver on the Second 90 (including Supply Chain Management and Drug Stockouts)
") Immediate Offer of HIV Treatment: How To Deliver on the Second 90 (including Supply Chain Management and Drug Stockouts) Roselyne TOBY,MD, ID specialist Infectious Disease Unit/Yaounde Central Hospital
Immediate Offer of HIV Treatment: How To Deliver on the Second 90 (including Supply Chain Management and Drug Stockouts) Roselyne TOBY,MD, ID specialist Infectious Disease Unit/Yaounde Central Hospital
Antiretroviral Therapy: What to Start
 FLOWED: 05-14-2015 Chicago, IL: May 18, 2015 Antiretroviral Therapy: What to Start Eric S. Daar, MD Professor of Medicine David Geffen School of Medicine University of California Los Angeles Los Angeles,
FLOWED: 05-14-2015 Chicago, IL: May 18, 2015 Antiretroviral Therapy: What to Start Eric S. Daar, MD Professor of Medicine David Geffen School of Medicine University of California Los Angeles Los Angeles,
Bon Usage des Antirétroviraux dans l Infection par le VIH
 Bon Usage des Antirétroviraux dans l Infection par le VIH Pr. Jean-Michel Molina CHU St Louis, Assistance Publique Hôpitaux de Paris, INSERM U941 et Université Paris 7 Diderot, France 1 Liens d Intérêt
Bon Usage des Antirétroviraux dans l Infection par le VIH Pr. Jean-Michel Molina CHU St Louis, Assistance Publique Hôpitaux de Paris, INSERM U941 et Université Paris 7 Diderot, France 1 Liens d Intérêt
ARVs in Development: Where do they fit?
 The picture can't be displayed. ARVs in Development: Where do they fit? Daniel R. Kuritzkes, M.D. Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School Disclosures The speaker
The picture can't be displayed. ARVs in Development: Where do they fit? Daniel R. Kuritzkes, M.D. Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School Disclosures The speaker
STRIBILD (aka. The Quad Pill)
") NORTHWEST AIDS EDUCATION AND TRAINING CENTER STRIBILD (aka. The Quad Pill) Brian R. Wood, MD Medical Director, NW AETC ECHO Assistant Professor of Medicine, University of Washington Presentation prepared
NORTHWEST AIDS EDUCATION AND TRAINING CENTER STRIBILD (aka. The Quad Pill) Brian R. Wood, MD Medical Director, NW AETC ECHO Assistant Professor of Medicine, University of Washington Presentation prepared
HIV Treatment: New and Veteran Drugs Classes
 HIV Treatment: New and Veteran Drugs Classes Jonathan M Schapiro, MD National Hemophilia Center Stanford University School of Medicine Rome, March 2013 Overview Many excellent antiretroviral agents are
HIV Treatment: New and Veteran Drugs Classes Jonathan M Schapiro, MD National Hemophilia Center Stanford University School of Medicine Rome, March 2013 Overview Many excellent antiretroviral agents are
Rajesh T. Gandhi, M.D.
 HIV Treatment Guidelines: 2010 Rajesh T. Gandhi, M.D. Case 29 yo M with 8 weeks of cough and fever. Diagnosed with smear-positive pulmonary TB. HIV-1 antibody positive. CD4 count 361. HIV-1 RNA 23,000
HIV Treatment Guidelines: 2010 Rajesh T. Gandhi, M.D. Case 29 yo M with 8 weeks of cough and fever. Diagnosed with smear-positive pulmonary TB. HIV-1 antibody positive. CD4 count 361. HIV-1 RNA 23,000
HIV Clinical Management: Antiretroviral Therapy and Drug Resistance
 HIV Clinical Management: Antiretroviral Therapy and Drug Resistance Judith S. Currier, MD, MSc Professor of Medicine University of California, Los Angeles Disclosures: Research Grant from Theratechnologies
HIV Clinical Management: Antiretroviral Therapy and Drug Resistance Judith S. Currier, MD, MSc Professor of Medicine University of California, Los Angeles Disclosures: Research Grant from Theratechnologies
Drug toxicities: Safest PIs. Michelle Moorhouse 14 Apr 2016
 Drug toxicities: Safest PIs Michelle Moorhouse 14 Apr 2016 Impact of PIs on AIDS mortality CDC.gov. Epidemiology of HIV infection. Evolution of PIs http://www.clinicaloptions.com/hiv/treatment%20updates/boosted%20pis/interactive%20virtual%20presentation/slideset.aspx
Drug toxicities: Safest PIs Michelle Moorhouse 14 Apr 2016 Impact of PIs on AIDS mortality CDC.gov. Epidemiology of HIV infection. Evolution of PIs http://www.clinicaloptions.com/hiv/treatment%20updates/boosted%20pis/interactive%20virtual%20presentation/slideset.aspx
Prima linea: dovremmo evitare i PI nella terapia di prima linea per i loro effetti non desiderati? Giuseppina Liuzzi
 6 th INFECtivology TOday Paestum 15-16 -17 maggio 2014 Prima linea: dovremmo evitare i PI nella terapia di prima linea per i loro effetti non desiderati? Giuseppina Liuzzi Istituto Nazionale per le Malattie
6 th INFECtivology TOday Paestum 15-16 -17 maggio 2014 Prima linea: dovremmo evitare i PI nella terapia di prima linea per i loro effetti non desiderati? Giuseppina Liuzzi Istituto Nazionale per le Malattie
Simplifying Antiretroviral Therapy Regimens: It s not so simple
 Simplifying Antiretroviral Therapy Regimens: It s not so simple Jonathan Colasanti, MD, MSPH Division of Infectious Diseases Emory University School of Medicine Disclosures No Financial Disclosures Parts
Simplifying Antiretroviral Therapy Regimens: It s not so simple Jonathan Colasanti, MD, MSPH Division of Infectious Diseases Emory University School of Medicine Disclosures No Financial Disclosures Parts
Crafting an ART Regimen for Initiation or Salvage: Are NRTI s Necessary?
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Crafting an ART Regimen for Initiation or Salvage: Are NRTI s Necessary? Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Crafting an ART Regimen for Initiation or Salvage: Are NRTI s Necessary? Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical
First-Line Antiretroviral Therapy for Treatment and Prevention:
 First-Line Antiretroviral Therapy for Treatment and Prevention: The Past, Present and Future Best Options Joel Gallant, MD, MPH Johns Hopkins University School of Medicine IAS-USA Guidelines 7/2008: When
First-Line Antiretroviral Therapy for Treatment and Prevention: The Past, Present and Future Best Options Joel Gallant, MD, MPH Johns Hopkins University School of Medicine IAS-USA Guidelines 7/2008: When
L infettivologia del 3 millennio: AIDS ed altro
 L infettivologia del 3 millennio: AIDS ed altro VI Convegno Nazionale 15-16 -17 maggio 2014 Centro Congressi Hotel Ariston Paestum (SA) Nuove molecole ad azione anti-hiv Annalisa Saracino Clinica Malattie
L infettivologia del 3 millennio: AIDS ed altro VI Convegno Nazionale 15-16 -17 maggio 2014 Centro Congressi Hotel Ariston Paestum (SA) Nuove molecole ad azione anti-hiv Annalisa Saracino Clinica Malattie
Case 1 continued. Case 1 (cont) 12/8/16. MMAH Debate Panel Thursday, December 8, Case 1
 12/8/16. MMAH Debate Panel Thursday, December 8, Case 1") MMAH Debate Panel Thursday, December 8, 2016 Case 1 HPI 55 yo man with newly diagnosed HIV initiates care in your clinic. His CD4+ cell count is 600, with HIV VL=90,000 copies/ml. He is asymptomatic at
MMAH Debate Panel Thursday, December 8, 2016 Case 1 HPI 55 yo man with newly diagnosed HIV initiates care in your clinic. His CD4+ cell count is 600, with HIV VL=90,000 copies/ml. He is asymptomatic at
ARV Consolidated Guidelines 2015
 ARV Consolidated Guidelines 2015 This document outlines the draft list of PICO questions to support systematic review process for the 2015 ARV guidelines process. PICO questions are grouped by clinical
ARV Consolidated Guidelines 2015 This document outlines the draft list of PICO questions to support systematic review process for the 2015 ARV guidelines process. PICO questions are grouped by clinical
Treatment update. Bronagh McBrien June 2016
 Treatment update Bronagh McBrien June 2016 Speaker Name Bronagh McBrien Statement Received educational funding and support from Gilead, Merck, Boehringer Ingelheim, Janssen-Cilag Date : 27 June 2016 BHIVA
Treatment update Bronagh McBrien June 2016 Speaker Name Bronagh McBrien Statement Received educational funding and support from Gilead, Merck, Boehringer Ingelheim, Janssen-Cilag Date : 27 June 2016 BHIVA
DRUGS IN PIPELINE. Pr JC YOMBI UCL-AIDS REFERENCE CENTRE BREACH Sept 27, 2015
 DRUGS IN PIPELINE Pr JC YOMBI UCL-AIDS REFERENCE CENTRE BREACH Sept 27, 2015 N(t)RTI The Development of TAF TAF Delivers the High Potency of TDF While Minimizing Off- Target Kidney and Bone Side Effects
DRUGS IN PIPELINE Pr JC YOMBI UCL-AIDS REFERENCE CENTRE BREACH Sept 27, 2015 N(t)RTI The Development of TAF TAF Delivers the High Potency of TDF While Minimizing Off- Target Kidney and Bone Side Effects
CROI 2013: New Drugs for Treatment and PrEP
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER CROI 2013: New Drugs for Treatment and PrEP Brian R. Wood, MD Medical Director, NW AETC Project ECHO Assistant Professor of Medicine, University of Washington
NORTHWEST AIDS EDUCATION AND TRAINING CENTER CROI 2013: New Drugs for Treatment and PrEP Brian R. Wood, MD Medical Director, NW AETC Project ECHO Assistant Professor of Medicine, University of Washington
Pharmacological considerations on the use of ARVs in pregnancy
 Pharmacological considerations on the use of ARVs in pregnancy 11 th Residential Course on Clinical Pharmacology of Antiretrovirals Torino, 20-22 January 2016 Prof. David Burger, PharmD, PhD david.burger@radboudumc.nl
Pharmacological considerations on the use of ARVs in pregnancy 11 th Residential Course on Clinical Pharmacology of Antiretrovirals Torino, 20-22 January 2016 Prof. David Burger, PharmD, PhD david.burger@radboudumc.nl
Genotypic Resistance Testing in Routine Care in South Africa:
 Genotypic Resistance Testing in Routine Care in South Africa: Is the Juice Worth the Squeeze? Mark Siedner Africa Health Research Institute Harvard Medical School Conflicts of Interest^* No financial conflicts
Genotypic Resistance Testing in Routine Care in South Africa: Is the Juice Worth the Squeeze? Mark Siedner Africa Health Research Institute Harvard Medical School Conflicts of Interest^* No financial conflicts
The Dawn of the TLD Era
 The Dawn of the TLD Era 20th September 2018 Mark Siedner Africa Health Research Institute Harvard Medical School Outline: A Primer on Dolutegravir Do we really need more HIV drugs? The case for a new first-line
The Dawn of the TLD Era 20th September 2018 Mark Siedner Africa Health Research Institute Harvard Medical School Outline: A Primer on Dolutegravir Do we really need more HIV drugs? The case for a new first-line
What are the most promising opportunities for dose optimisation?
 What are the most promising opportunities for dose optimisation? Andrew Hill Liverpool University, UK Global Financial Crisis How can we afford to treat 15-30 million people with HIV in the future? Lowering
What are the most promising opportunities for dose optimisation? Andrew Hill Liverpool University, UK Global Financial Crisis How can we afford to treat 15-30 million people with HIV in the future? Lowering
Statistical issues in HIV trial design. Andrew Hill Senior Visiting Research Fellow Liverpool University
 Statistical issues in HIV trial design Andrew Hill Senior Visiting Research Fellow Liverpool University Type 1 error It is statistically significant! (after 100 different statistical tests) Type 1 error:
Statistical issues in HIV trial design Andrew Hill Senior Visiting Research Fellow Liverpool University Type 1 error It is statistically significant! (after 100 different statistical tests) Type 1 error:
Antiretroviral Treatment 2014
 Activity Code FM285 Antiretroviral Treatment 2014 Rajesh Gandhi, MD Masssachusetts General Hospital Disclosures: Educational grants to my institution from Janssen, Viiv, Abbott Learning Objectives Upon
Activity Code FM285 Antiretroviral Treatment 2014 Rajesh Gandhi, MD Masssachusetts General Hospital Disclosures: Educational grants to my institution from Janssen, Viiv, Abbott Learning Objectives Upon
Comprehensive Guideline Summary
 Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
HIV Treatment Evolution. Kimberly Y. Smith MD MPH Vice President and Head, Global Research and Medical Strategy Viiv Healthcare
 HIV Treatment Evolution Kimberly Y. Smith MD MPH Vice President and Head, Global Research and Medical Strategy Viiv Healthcare Overview of the Evolution of Antiretroviral Therapy Early Treatment 1987
HIV Treatment Evolution Kimberly Y. Smith MD MPH Vice President and Head, Global Research and Medical Strategy Viiv Healthcare Overview of the Evolution of Antiretroviral Therapy Early Treatment 1987
HIV Treatment Update 8/3/2015. When to Start. Disclosures
 8/3/215 HIV Treatment Update Joel Gallant, MD, MPH Southwest CARE Center Santa Fe, NM University of New Mexico School of Medicine Johns Hopkins University School of Medicine Disclosures Consulting, Advisory
8/3/215 HIV Treatment Update Joel Gallant, MD, MPH Southwest CARE Center Santa Fe, NM University of New Mexico School of Medicine Johns Hopkins University School of Medicine Disclosures Consulting, Advisory
Cases from the Clinic(ians): Case-Based Panel Discussion
: Case-Based Panel Discussion") Cases from the Clinic(ians): Case-Based Panel Discussion Michael S. Saag, MD Professor of Medicine The University of Alabama at Birmingham EDITED: 03-12-14 Learning Objectives After attending this presentation,
Cases from the Clinic(ians): Case-Based Panel Discussion Michael S. Saag, MD Professor of Medicine The University of Alabama at Birmingham EDITED: 03-12-14 Learning Objectives After attending this presentation,
Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV. Ernesto Parra, M.D., M.P.H.
 Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV Ernesto Parra, M.D., M.P.H. Adjunct Associate Professor UTHSCSA Department of Pediatrics and Family and Community
Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV Ernesto Parra, M.D., M.P.H. Adjunct Associate Professor UTHSCSA Department of Pediatrics and Family and Community
The Use of Integrase Inhibitors In Latin America: From Guidelines to the Real World Ernesto Martínez B., MD Internal Medicine, Infectious Diseases
 De afbeelding kan niet worden weergegeven. The Use of Integrase Inhibitors In Latin America: From Guidelines to the Real World Ernesto Martínez B., MD Internal Medicine, Infectious Diseases DISCLOSURE
De afbeelding kan niet worden weergegeven. The Use of Integrase Inhibitors In Latin America: From Guidelines to the Real World Ernesto Martínez B., MD Internal Medicine, Infectious Diseases DISCLOSURE
Antiretroviral Drugs
 Antiretroviral Drugs Dr Paddy Mallon UCD HIV Molecular Research Group Associate Dean for Research and Innovation UCD School of Medicine and Medical Science paddy.mallon@ucd.ie UCD School of Medicine &
Antiretroviral Drugs Dr Paddy Mallon UCD HIV Molecular Research Group Associate Dean for Research and Innovation UCD School of Medicine and Medical Science paddy.mallon@ucd.ie UCD School of Medicine &
Treatment Optimisation Community Condultation Feedback. KENLY SIKWESE AFRICAN COMMUNITY ADVISORY BOARD (AFROCAB) 3 rd May 2016
 3 rd May 2016") Treatment Optimisation Community Condultation Feedback KENLY SIKWESE AFRICAN COMMUNITY ADVISORY BOARD (AFROCAB) 3 rd May 2016 INTRODUCTION A brief history of ART 1987-90s AZT vecomes available ddi/ddc
Treatment Optimisation Community Condultation Feedback KENLY SIKWESE AFRICAN COMMUNITY ADVISORY BOARD (AFROCAB) 3 rd May 2016 INTRODUCTION A brief history of ART 1987-90s AZT vecomes available ddi/ddc
Switching antiretroviral therapy to safer strategies based on integrase inhibitors
 Switching antiretroviral therapy to safer strategies based on integrase inhibitors Dr Paddy Mallon UCD HIV Molecular Research Group UCD School of Medicine paddy.mallon@ucd.ie UCD School of Medicine & Medical
Switching antiretroviral therapy to safer strategies based on integrase inhibitors Dr Paddy Mallon UCD HIV Molecular Research Group UCD School of Medicine paddy.mallon@ucd.ie UCD School of Medicine & Medical
2009 Recommendations for Antiretroviral Therapy in Adults and Adolescents. When to Start and What ART to Use in 1 st and 2 nd Line December 2009
 2009 Recommendations for Antiretroviral Therapy in Adults and Adolescents When to Start and What ART to Use in 1 st and 2 nd Line December 2009 Historic Evolution of CD4 Criteria for ART Initiation in
2009 Recommendations for Antiretroviral Therapy in Adults and Adolescents When to Start and What ART to Use in 1 st and 2 nd Line December 2009 Historic Evolution of CD4 Criteria for ART Initiation in
WHO mission on ART optimization in Belarus March 30-31, April 1, 2016
 WHO mission on ART optimization in Belarus March 30-31, April 1, 2016 April, 2016 By Matti Ristola, Helsinki University Hospital, Finland, Valentin Rusovich, WHO Country Office, Belarus, Jens Lundgren
WHO mission on ART optimization in Belarus March 30-31, April 1, 2016 April, 2016 By Matti Ristola, Helsinki University Hospital, Finland, Valentin Rusovich, WHO Country Office, Belarus, Jens Lundgren
Management of ART Failure. EACS Advanced HIV Course 2015 Dr Nicky Mackie
 Management of ART Failure EACS Advanced HIV Course 2015 Dr Nicky Mackie Outline Defining treatment success Defining treatment failure Reasons for ART failure Management of ART failure Choice of second
Management of ART Failure EACS Advanced HIV Course 2015 Dr Nicky Mackie Outline Defining treatment success Defining treatment failure Reasons for ART failure Management of ART failure Choice of second
Update on HIV Drug Resistance. Daniel R. Kuritzkes, MD Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School
 Update on HIV Drug Resistance Daniel R. Kuritzkes, MD Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School Learning Objectives Upon completion of this presentation, learners
Update on HIV Drug Resistance Daniel R. Kuritzkes, MD Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School Learning Objectives Upon completion of this presentation, learners
WHEN TO START? CROI 2015: Focus on ART
 CROI 215: Focus on ART FORMATTED: 4-1-15 Washington, DC: May 13, 215 Roy M. Gulick, MD, MPH Gladys and Roland Harriman Professor of Medicine Chief, Division of Infectious Diseases Weill Cornell Medical
CROI 215: Focus on ART FORMATTED: 4-1-15 Washington, DC: May 13, 215 Roy M. Gulick, MD, MPH Gladys and Roland Harriman Professor of Medicine Chief, Division of Infectious Diseases Weill Cornell Medical
The impact of antiretroviral drugs on renal function
 The impact of antiretroviral drugs on renal function Professor Bruce Hendry Renal Medicine King s College London King s College Hospital NHS Foundation Trust 1 DISCLOSURES: BRUCE HENDRY I have received
The impact of antiretroviral drugs on renal function Professor Bruce Hendry Renal Medicine King s College London King s College Hospital NHS Foundation Trust 1 DISCLOSURES: BRUCE HENDRY I have received
2016 Perinatal Treatment Guidelines Update
 Mountain West AIDS Education and Training Center 2016 Perinatal Treatment Guidelines Update Shireesha Dhanireddy, MD Associate Professor of Medicine, University of Washington 2 November 2016 This presentation
Mountain West AIDS Education and Training Center 2016 Perinatal Treatment Guidelines Update Shireesha Dhanireddy, MD Associate Professor of Medicine, University of Washington 2 November 2016 This presentation
ART: The New, The Old and The Ugly
 ART: The New, The Old and The Ugly Our Current ARVS The Nucleoside/ Nucleotide Reverse Transcriptase Inhibitors (NRTIs/ NtRTIs) Abacavir Emtricitabine Lamivudine Stavudine Tenofovir Zidovudine The Non-Nucleoside
ART: The New, The Old and The Ugly Our Current ARVS The Nucleoside/ Nucleotide Reverse Transcriptase Inhibitors (NRTIs/ NtRTIs) Abacavir Emtricitabine Lamivudine Stavudine Tenofovir Zidovudine The Non-Nucleoside
Advancing Treatment 2.0: Progress on the 2013 Consolidated Guidelines What s new
 Advancing Treatment 2.0: Progress on the 2013 Consolidated Guidelines What s new H I V / A I D S D e p a r t m e n t WHO HQ Meg Doherty, MD, MPH, PhD Coordinator Treatment and Care November 5, 2012 1 Overview
Advancing Treatment 2.0: Progress on the 2013 Consolidated Guidelines What s new H I V / A I D S D e p a r t m e n t WHO HQ Meg Doherty, MD, MPH, PhD Coordinator Treatment and Care November 5, 2012 1 Overview
Tim Horn Deputy Executive Director, HIV & HCV Programs Treatment Action Group NASTAD Prevention and Care Technical Assistance Meeting Washington, DC
 Tim Horn Deputy Executive Director, HIV & HCV Programs Treatment Action Group NASTAD Prevention and Care Technical Assistance Meeting Washington, DC July 19, 2017 Pipeline is robust! Several drugs, coformulations,
Tim Horn Deputy Executive Director, HIV & HCV Programs Treatment Action Group NASTAD Prevention and Care Technical Assistance Meeting Washington, DC July 19, 2017 Pipeline is robust! Several drugs, coformulations,
Third Agent Advantages Disadvantages. Component Tenofovir/emtricitabine (TDF/FTC) 300/200 mg (coformulated with EFV as Atripla) 1 tab once daily
 300/200 mg (coformulated with EFV as Atripla) 1 tab once daily") Table I. Recommended and Alternative Antiretroviral Regimens (DHHS Guidelines, May 1, 2014) Recommended Regimens Nucleoside Analog Reverse Transcriptase Inhibitor (NRTI) Third Agent Advantages Disadvantages
Table I. Recommended and Alternative Antiretroviral Regimens (DHHS Guidelines, May 1, 2014) Recommended Regimens Nucleoside Analog Reverse Transcriptase Inhibitor (NRTI) Third Agent Advantages Disadvantages
Switching antiretroviral therapy to safer strategies based on integrase inhibitors. Pedro Cahn
 Switching antiretroviral therapy to safer strategies based on integrase inhibitors Pedro Cahn Disclosures Research Grants: Abbvie-Merck-Richmond-ViiV Advisory boards: Merck-Sandoz-ViiV Switching in Virologically
Switching antiretroviral therapy to safer strategies based on integrase inhibitors Pedro Cahn Disclosures Research Grants: Abbvie-Merck-Richmond-ViiV Advisory boards: Merck-Sandoz-ViiV Switching in Virologically
Optimizing ARV For Women
 Optimizing ARV For Women Kathleen E. Squires, MD W Paul and Ida H Havens Professor of Infectious Diseases Director, Division of Infectious Diseases Sidney Kimmel Medical College of Thomas Jefferson University
Optimizing ARV For Women Kathleen E. Squires, MD W Paul and Ida H Havens Professor of Infectious Diseases Director, Division of Infectious Diseases Sidney Kimmel Medical College of Thomas Jefferson University
Evolving HIV Treatment Paradigms What we need to know
 Evolving HIV Treatment Paradigms What we need to know Benjamin Young International Association of Providers of AIDS Care Washington, DC, USA Evolving HIV Treatment Paradigms When/who to treat Better medicines
Evolving HIV Treatment Paradigms What we need to know Benjamin Young International Association of Providers of AIDS Care Washington, DC, USA Evolving HIV Treatment Paradigms When/who to treat Better medicines
Tenofovir Alafenamide (TAF)
") Frontier AIDS Education and Training Center Tenofovir Alafenamide (TAF) Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical Director, Frontier AETC ECHO January 28, 2016
Frontier AIDS Education and Training Center Tenofovir Alafenamide (TAF) Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical Director, Frontier AETC ECHO January 28, 2016
SINGLE. Efficacy and safety of dolutegravir (DTG) in treatment-naïve subjects
 in treatment-naïve subjects") SINGLE Efficacy and safety of dolutegravir (DTG) in treatment-naïve subjects SE/HIV/0023/14 January 2014 PHASE III DTG TRIALS IN TREATMENT-NAÏVE ADULT SUBJECTS WITH HIV SINGLE 1 N=833 Phase III non-inferiority,
SINGLE Efficacy and safety of dolutegravir (DTG) in treatment-naïve subjects SE/HIV/0023/14 January 2014 PHASE III DTG TRIALS IN TREATMENT-NAÏVE ADULT SUBJECTS WITH HIV SINGLE 1 N=833 Phase III non-inferiority,
Real Life Experience of Dolutegravir and Lamivudine Dual Therapy As a Switching Regimen in HIVTR Cohort
 Real Life Experience of Dolutegravir and Lamivudine Dual Therapy As a Switching Regimen in HIVTR Cohort Yagci-Caglayik D 1, Gokengin D 2, Inan A 3, Ozkan-Ozdemir H 4, Inan D 5, Akbulut A 6, Korten V 1,
Real Life Experience of Dolutegravir and Lamivudine Dual Therapy As a Switching Regimen in HIVTR Cohort Yagci-Caglayik D 1, Gokengin D 2, Inan A 3, Ozkan-Ozdemir H 4, Inan D 5, Akbulut A 6, Korten V 1,
Qué anuncian los nuevos trials?
 Qué anuncian los nuevos trials? XVII Curso Nacional VIH/SIDA Sociedad Chilena de Infectología Agosto 2014 Dr. Carlos Beltrán Hospital Barros Luco Trudeau Universidad de Santiago Grupo SidaChile El presente
Qué anuncian los nuevos trials? XVII Curso Nacional VIH/SIDA Sociedad Chilena de Infectología Agosto 2014 Dr. Carlos Beltrán Hospital Barros Luco Trudeau Universidad de Santiago Grupo SidaChile El presente
2017 NSTC Annual Meeting Eric Daar April 18, 2017
 Antiretroviral Therapy Update for TB Clinicians Eric S. Daar, M.D. Chief, Division of HIV Medicine Harbor-UCLA Medical Center Professor of Medicine David Geffen School of Medicine at UCLA Grants Consultant
Antiretroviral Therapy Update for TB Clinicians Eric S. Daar, M.D. Chief, Division of HIV Medicine Harbor-UCLA Medical Center Professor of Medicine David Geffen School of Medicine at UCLA Grants Consultant
Professor Jeffery Lennox
 BHIVA AUTUMN CONFERENCE 2014 Including CHIVA Parallel Sessions Professor Jeffery Lennox Emory University School of Medicine Atlanta, Georgia, USA 9-10 October 2014, Queen Elizabeth II Conference Centre,
BHIVA AUTUMN CONFERENCE 2014 Including CHIVA Parallel Sessions Professor Jeffery Lennox Emory University School of Medicine Atlanta, Georgia, USA 9-10 October 2014, Queen Elizabeth II Conference Centre,
State of the ART: Integrase Inhibitors Clinical Data. Juan Berenguer Hospital General Universitario Gregorio Marañón (IiSGM) Madrid, Spain
 Madrid, Spain") State of the ART: Integrase Inhibitors Clinical Data Juan Berenguer Hospital General Universitario Gregorio Marañón (IiSGM) Madrid, Spain Disclosures Consulting fees and honoraria Gilead, Janssen, MSD,
State of the ART: Integrase Inhibitors Clinical Data Juan Berenguer Hospital General Universitario Gregorio Marañón (IiSGM) Madrid, Spain Disclosures Consulting fees and honoraria Gilead, Janssen, MSD,
Antiretroviral Therapy: Current Recommendations, New Drugs, and Novel Strategies. Joel Gallant, MD, MPH Johns Hopkins University School of Medicine
 Antiretroviral Therapy: Current Recommendations, New Drugs, and Novel Strategies Joel Gallant, MD, MPH Johns Hopkins University School of Medicine Initial Regimen: DHHS Guidelines 3/27/2012 Preferred Regimens
Antiretroviral Therapy: Current Recommendations, New Drugs, and Novel Strategies Joel Gallant, MD, MPH Johns Hopkins University School of Medicine Initial Regimen: DHHS Guidelines 3/27/2012 Preferred Regimens
Is dolutegravir a magic bullet for HIV/TB programmes?
 Francois Venter Is dolutegravir a magic bullet for HIV/TB programmes? March 2018 Thanks Michelle Moorhouse, Graeme Meintjes, Gary Maartens, Celicia Serenata, Andy Hill, Polly Clayden, Gloria Maimela, Tom
Francois Venter Is dolutegravir a magic bullet for HIV/TB programmes? March 2018 Thanks Michelle Moorhouse, Graeme Meintjes, Gary Maartens, Celicia Serenata, Andy Hill, Polly Clayden, Gloria Maimela, Tom
HIV Treatment for Adults and Adolescents. Stefano Vella MD Istituto Superiore di Sanità - Rome - Italy
 HIV Treatment for Adults and Adolescents Stefano Vella MD Istituto Superiore di Sanità - Rome - Italy www.ias2013.org Kuala Lumpur, Malaysia, 30 June - 3 July 2013 PLHIV in need of ART WHO 2013 Guidelines
HIV Treatment for Adults and Adolescents Stefano Vella MD Istituto Superiore di Sanità - Rome - Italy www.ias2013.org Kuala Lumpur, Malaysia, 30 June - 3 July 2013 PLHIV in need of ART WHO 2013 Guidelines
Management of patients with antiretroviral treatment failure: guidelines comparison
 The editorial staff Management of patients with antiretroviral treatment failure: guidelines comparison A change of therapy should be considered for patients if they experience sustained rebound in viral
The editorial staff Management of patients with antiretroviral treatment failure: guidelines comparison A change of therapy should be considered for patients if they experience sustained rebound in viral
COMPETING INTEREST OF FINANCIAL VALUE
 BHIVA AUTUMN CONFERENCE 2012 Including CHIVA Parallel Sessions Dr Ian Williams University College London Medical School COMPETING INTEREST OF FINANCIAL VALUE > 1,000: Speaker Name Statement Ian Williams
BHIVA AUTUMN CONFERENCE 2012 Including CHIVA Parallel Sessions Dr Ian Williams University College London Medical School COMPETING INTEREST OF FINANCIAL VALUE > 1,000: Speaker Name Statement Ian Williams
Abstract PS8/2. Double-blind treatment phase D/C/F/TAF. + matching D/C + F/TDF placebo D/C/F/TAF. D/C + F/TDF + matching D/C/F/TAF placebo
 WEEK 8 RESULTS OF AMBER: A PHASE 3, RANDOMISED, DOUBLE-BLIND TRIAL IN ANTIRETROVIRAL TREATMENT (ART)-NAÏVE HIV--INFECTED ADULTS TO EVALUATE THE EFFICACY AND SAFETY OF THE ONCE-DAILY, SINGLE-TABLET REGIMEN
WEEK 8 RESULTS OF AMBER: A PHASE 3, RANDOMISED, DOUBLE-BLIND TRIAL IN ANTIRETROVIRAL TREATMENT (ART)-NAÏVE HIV--INFECTED ADULTS TO EVALUATE THE EFFICACY AND SAFETY OF THE ONCE-DAILY, SINGLE-TABLET REGIMEN
Treatment and Care: Product portfolio
 Treatment and Care: Product portfolio Dr Paula Munderi MRC/UVRI Uganda Research Unit on AIDS EDCTP Stakeholder Meeting on HIV/AIDS 3-4 September 2013 Summary Brief overview HIV Treatment Pipeline Key Questions
Treatment and Care: Product portfolio Dr Paula Munderi MRC/UVRI Uganda Research Unit on AIDS EDCTP Stakeholder Meeting on HIV/AIDS 3-4 September 2013 Summary Brief overview HIV Treatment Pipeline Key Questions
2009 Revisions of WHO ART Guidelines. November 2009
 2009 Revisions of WHO ART Guidelines November 2009 Guidelines Development Process 01/09 2009 WHO ART guideline revision process Scope of the work 03/09 WHO Guideline review committee approval 04/09 05/09
2009 Revisions of WHO ART Guidelines November 2009 Guidelines Development Process 01/09 2009 WHO ART guideline revision process Scope of the work 03/09 WHO Guideline review committee approval 04/09 05/09