This document must accompany the CAMPER MAIL-IN registration form
|
|
|
- Victor Mathews
- 5 years ago
- Views:
Transcription
1
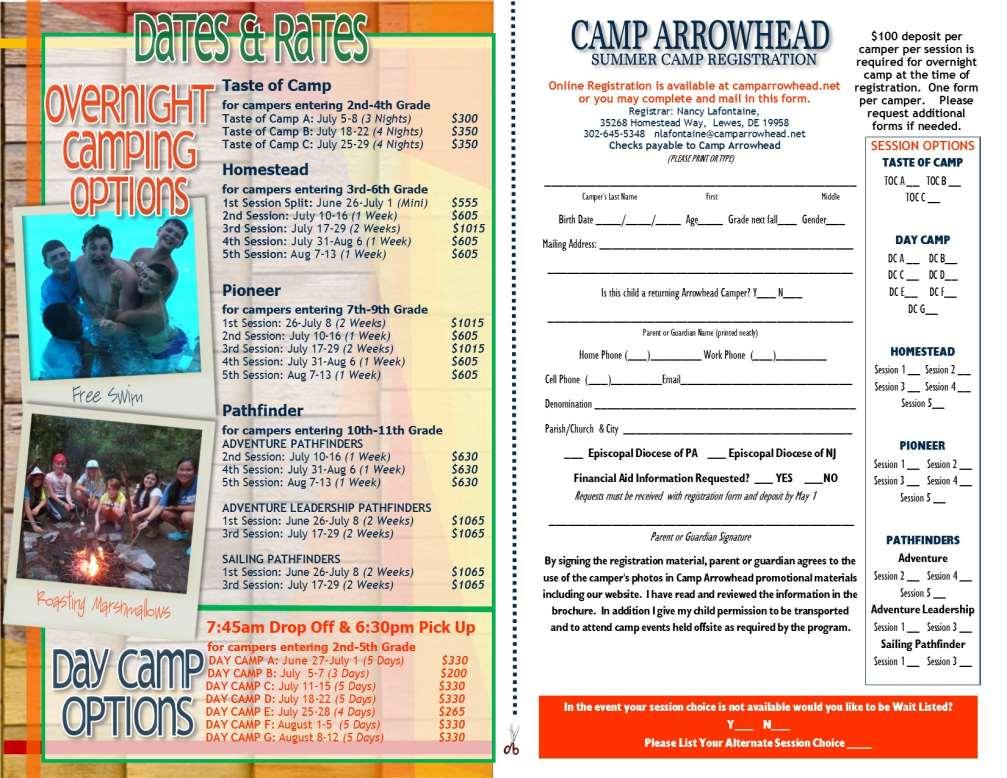
2 CAMP ARROWHEAD 2016 CAMPER HEALTH HISTORY MAIL-IN FORM Mail this form with CAMPER REGISTRATION to: Camp Arrowhead Attention: Nancy Lafontaine Homestead Way Lewes, DE Dates will attend camp: Camper Name: Male Female Birth Date: Grade entering in Sept. This document must accompany the CAMPER MAIL-IN registration form General Information Medical information must be provided for your child to attend camp. It is essential for the camp to have your child s current health information in order to be able to ensure the safety and well-being during your camper s stay at camp. All campers are required to have a physical within 12 months of attending camp. Camp physicals can sometimes be obtained at your local pharmacies or walk-in centers. Parent/Guardian to be contacted in case of illness: Name Relationship Phone Second Parent/Guardian or other emergency contact: Name Relationship Phone Camper s last exam date. ALLERGIES AND DIETARY RESTRICTIONS Does your child have any allergies? YES NO If yes, please circle and provide detailed information: FOOD ALLERGENS: Peanuts Soy Eggs Sesame seeds Milk DRUG ALLERGENS: Antibiotics Penicillin Sulfa drugs Tetracycline Analgesics Codeine Non-steroid antiinflammatory drugs (NSAIDs) Seafood (fish, crustaceans, shellfish) Tree nuts (almonds, cashews, hazelnuts, pistachios) Sulphites Wheat Mustard Antiseizure/Anticonvulsants Phenytoin Carbamazepine Chemotherapy Monoclonal antibody therapy Aspirin Ibuprofen PROVIDE DETAILS OF ALL CIRCLED: LIST ADDITIONAL FOODS, IF NEEDED PROVIDE DETAILS OF ALL CIRCLED: LIST ADDITIONAL DRUGS, IF NEEDED
3 ENVIRONMENTAL ALLERGENS: Pollen Trees Grass Weeds Dust mites Animal dander Mold Wood dust Ragweed Leaf litter PROVIDE DETAILS OF ALL CIRCLED: LIST ADDITIONAL, IF NEEDED Does your child require an EpiPen? YES NO If yes, provide details. IF YOUR CHILD REQUIRES AN EPIPEN, PLEASE PROVIDE ONE NON-EXPIRED EPIPEN WITH YOUR CAMPER S NAME ON THE EPIPEN. Does your child have any dietary restrictions? YES NO If yes, provide details. CAMPERS WITH DIETARY RESTRICTIONS MUST FILL OUT THE KITCHEN ALLERGY FROM LOCATED ON OUR MAIN CAMP WEBSITE PAGE. YOU ARE ALSO REQUIRED TO CONTACT OUR FOOD SERVICE MANAGER AT jfeaster@camparrowhead.net or ext 6 MEDICATIONS AND TREATMENTS PLEASE LIST ALL MEDICATION TO BE GIVEN WHILE AT CAMP ALL MEDICATION NAME DOSE SCHEDULE (Time of Day) DETAILS MEDICINE MUST BE BROUGHT IN ITS ORIGINAL PACKAGING Will your child require any treatments while at camp? YES NO Please explain what treatments(s) must be given to your child, including the frequency.
4 Does your child regularly take any medications that will not be taken at camp? YES NO EXPLAIN OVER THE COUNTER MEDICATIONS May the following over-the-counter medications be given to your child while at camp? MEDICATION YES NO YES NO Acetaminophen (Tylenol) Anatacids Antibiotic Cream Antihistamines (Benadryl, Diphenhydramine) ASA (Aspirin) Calamine Lotion Cortaid Insect Repellent Pepto-Bismol Robitussin Robitussin DM Sting Swabs Sudafed Sunburn Spray or Ointment Dimetapp Ibuprofen Sunscreen Is there anything the camp needs to be aware of when giving any of the approved over-the-counter medications to your child? HEALTH HISTORY Has your child experienced, or is currently experiencing, any of the following conditions? If yes, please explain fully. Condition NO YES DETAILS ADD/ADHD HIVAIDS/ARC Asthma/Inhaler Back Pain or Injury Bedwetting Behavioral Issues Blackouts/Fainting Bleeding Disorder
5 CONDITION NO YES DETAILS CANCER Chest Pain Crohn s Colitis Concussion Constipation/Diarrhea Convulsions Depression Developmental Delays Diabetes Ear Infections Eating Disorder Epilepsy Frequent Colds Hay Fever Headaches Hearing Problems Heart Disease Hernia High Blood Pressure Irritable Bowel Syndrome Kidney Disease
6 CONDITION NO YES DETAILS LICE Menstrual Difficulties Mental Health Issues Neck Pain or Injury Nightmares/Terrors Pneumonia Respiratory Ailments Rheumatic Fever Seizures Sinus Infections Skin Problems Sleepwalking Sore Throats Speech Problems Stomach Aches Tonsillitis Ulcer Urinary Tract Infection Uses eye glasses or contacts Other
7 Has your child had any operations? YES NO If yes, please explain. Has your child ever been hospitalized or had a serious injury? YES NO If yes, please explain. Has your child had or currently has any of the following diseases? DISEASE Chicken Pox (Varciella) Mono (past 1 year) Hepatitis A Mumps Hepatitis B Rheumatic Fever Hepatitis C Scarlet Fever Measles (German) Whooping Cough Measles (Red) Fully explain any of the conditions above which your child is currently experiencing. Has your child been exposed to any communicable diseases within the last three months? YES No If yes, please explain. Does your child have any restrictions on activity? YES NO If yes, please explain. Will your child require any special assistance while at camp? YES NO If yes, please explain. Is there anything you would like to discuss with the camp staff? YES NO
8 HEALTH INSURANCE AND DOCTOR INFORMATION (ALL CAMPERS ARE REQUIRED TO SUBMIT A COPY OF THE FRONT AND BACK OF THE HAELTH INSURANCE CARD. THIS IS REQUIRED WHEN TAKING YOUR CAMPER FOR A DOCTOR S VISIT) Family Doctor Phone Family Dentist Phone MEDICAL INSURANCE Full Name of Policy Holder Policy Holder Phone Number HEALTH INSURANCE COMPANY INFORMATION INSURANCE COMPANY/PLAN NAME INSURANCE COMPANY PHONE NUMBER HEALTH INSURANCE POLICY NUMBER INSURANCE GROUP NAME OR NUMBER MEDICAL WAIVER Parent/Guardian Authorization for Health Care: This health history is correct and accurately reflects the health status of the camper to whom it pertains. The person described has permission to participate in all camp activities except as noted by me and/ or an examining physician. I give permission to the physician selected by the camp to order x-rays, routine tests, and treatment related to the health of my child for both routine health care and in emergency situations. If I cannot be reached in an emergency, as well as the emergency contact, I give my permission to the physician to hospitalize, secure proper treatment for, and order injection, anesthesia, or surgery for this child. I understand this information will be shared on a "need to know" basis with camp staff. I give permission to print this information. In addition the camp has permission to obtain a copy of my child's health record from providers who treat my child and theses providers may talk with the program's staff about my child's health status. If for any reason you cannot sign this waiver, contact the camp registrar at: or nlafontaine@camparrowhead.net. Parent/Guardian Signature Date
2016 CAMP REGISTRATION FORM Please mail this form together with payment of all camp fees to: Montlure Camp, PO Box 42705, Tucson, AZ
 2016 CAMP REGISTRATION FORM Please mail this form together with payment of all camp fees to: Montlure Camp, PO Box 42705, Tucson, AZ 85733-2705 Camper Information Camper Mailing Address: (First Name) (Nickname)
2016 CAMP REGISTRATION FORM Please mail this form together with payment of all camp fees to: Montlure Camp, PO Box 42705, Tucson, AZ 85733-2705 Camper Information Camper Mailing Address: (First Name) (Nickname)
Camp(s) attending Traditional. (Check all that apply) Name Date of Birth Age at camp Gender M / F Last First MI Circle One
 attending Traditional. (Check all that apply) Name Date of Birth Age at camp Gender M / F Last First MI Circle One") Arrival Date Departure Date 2016 CAMP HEALTH HISTORY & EXAMINATION FORM FOR CHILDREN, YOUTH & ADULTS Camp(s) attending Traditional (Check all that apply) r ETC Ranch Camp Specialty CIT Staff Young Leaders
Arrival Date Departure Date 2016 CAMP HEALTH HISTORY & EXAMINATION FORM FOR CHILDREN, YOUTH & ADULTS Camp(s) attending Traditional (Check all that apply) r ETC Ranch Camp Specialty CIT Staff Young Leaders
Doctor. Dentist. Mental Health. Other
 Page 1 Health Care Providers Specialty Name Telephone Number Doctor Dentist Orthodontist Mental Health Other May we contact your child s health care provider? Health Insurance Is your camper covered by
Page 1 Health Care Providers Specialty Name Telephone Number Doctor Dentist Orthodontist Mental Health Other May we contact your child s health care provider? Health Insurance Is your camper covered by
Medical History Records Form
 Medical History Records Form I am (please circle all that apply) Cincinnati Tradition member, staff or volunteer PERSONAL INFORMATION Last name: Middle initial: Sex Date of birth: Secondary phone number:
Medical History Records Form I am (please circle all that apply) Cincinnati Tradition member, staff or volunteer PERSONAL INFORMATION Last name: Middle initial: Sex Date of birth: Secondary phone number:
Calumet 2017 staff/trainee/volunteer Health History & Examination Form PO Box 236, West Ossipee, NH Fax
 Calumet 2017 staff/trainee/volunteer Health History & Examination Form PO Box 236, West Ossipee, NH 03890 The information on this form is to assist us in determining appropriate care for staff/trainees/volunteers.
Calumet 2017 staff/trainee/volunteer Health History & Examination Form PO Box 236, West Ossipee, NH 03890 The information on this form is to assist us in determining appropriate care for staff/trainees/volunteers.
Student Full Name: Date of Birth:
 Student Medical Form This form is to be completed for new students upon admission, and returning students prior to starting grades 3, 6, and 9. Students participating in athletics must complete form every
Student Medical Form This form is to be completed for new students upon admission, and returning students prior to starting grades 3, 6, and 9. Students participating in athletics must complete form every
CAMPER HEALTH HISTORY FORM 1
 CAMPER HEALTH HISTORY FORM 1 Developed and reviewed by: American Camp Association, American Academy of Pediatrics Council on School Health, & Association of Camp Nurses Mail this form to the address below
CAMPER HEALTH HISTORY FORM 1 Developed and reviewed by: American Camp Association, American Academy of Pediatrics Council on School Health, & Association of Camp Nurses Mail this form to the address below
Health History and Treatment Authorization Form Vanderkamp Center _ 337 Martin Road _ Cleveland, NY _
 Health History and Treatment Authorization Form Vanderkamp Center _ 337 Martin Road _ Cleveland, NY 13042 315-675-3651 _ vkcenter@vk.org of Program: Please return by: The information on this form is gathered
Health History and Treatment Authorization Form Vanderkamp Center _ 337 Martin Road _ Cleveland, NY 13042 315-675-3651 _ vkcenter@vk.org of Program: Please return by: The information on this form is gathered
,
 , o o o : : Girl Scouts, Hornets Nest Council 2018 Summer Camp Health/Permission Form SECTION ONE (must be completed every year for ALL campers) CAMPER INFORMATION Camp Session Name and Date: Camper Name
, o o o : : Girl Scouts, Hornets Nest Council 2018 Summer Camp Health/Permission Form SECTION ONE (must be completed every year for ALL campers) CAMPER INFORMATION Camp Session Name and Date: Camper Name
Let s Celebrate
 Let s Celebrate Girl Scouts of Western Ohio Health History and Medical Examination Form for Adults Health History: The more complete information you provide, the better we are able to work
Let s Celebrate Girl Scouts of Western Ohio Health History and Medical Examination Form for Adults Health History: The more complete information you provide, the better we are able to work
GIRL FORM. Address City State Zip ( ) ( ) HEALTH INSURANCE INFORMATION Name of Insurance Company Address Insurance Company Phone Number
 ( ) HEALTH INSURANCE INFORMATION Name of Insurance Company Address Insurance Company Phone Number") : : GIRL FORM Girl Scouts, Hornets Nest Council 2018 Summer Camp Health/Permission Form Please Note: NO girl will be allowed to attend any camp without a completed and signed Summer Camp Health/Permission
: : GIRL FORM Girl Scouts, Hornets Nest Council 2018 Summer Camp Health/Permission Form Please Note: NO girl will be allowed to attend any camp without a completed and signed Summer Camp Health/Permission
THE CLEAR VIEW SCHOOL DAY TREATMENT CENTER BRIARCLIFF MANOR, NEW YORK ANNUAL HEALTH EXAMINATION (To be filled out by physician)
") THE CLEAR VIEW SCHOOL DAY TREATMENT CENTER 2016-2017 BRIARCLIFF MANOR, NEW YORK 10510 of Exam: ANNUAL HEALTH EXAMINATION (To be filled out by physician) Child's Name: of Birth: Physical Height Weight Blood
THE CLEAR VIEW SCHOOL DAY TREATMENT CENTER 2016-2017 BRIARCLIFF MANOR, NEW YORK 10510 of Exam: ANNUAL HEALTH EXAMINATION (To be filled out by physician) Child's Name: of Birth: Physical Height Weight Blood
THE CLEAR VIEW SCHOOL DAY TREATMENT CENTER BRIARCLIFF MANOR, NEW YORK ANNUAL HEALTH EXAMINATION (To be filled out by physician)
") THE CLEAR VIEW SCHOOL DAY TREATMENT CENTER 2016-2017 BRIARCLIFF MANOR, NEW YORK 10510 of Exam: ANNUAL HEALTH EXAMINATION (To be filled out by physician) Child's Name: of Birth: Physical Height Weight Blood
THE CLEAR VIEW SCHOOL DAY TREATMENT CENTER 2016-2017 BRIARCLIFF MANOR, NEW YORK 10510 of Exam: ANNUAL HEALTH EXAMINATION (To be filled out by physician) Child's Name: of Birth: Physical Height Weight Blood
Form C-MossRehab Camp Independence 2017-Medical Information
 Form C-MossRehab Camp Independence 2017-Medical Information DIRECTIONS FOR COMPLETION: Step 1. This form must be fully completed and signed by the applicant s physician. No substitutions of this form will
Form C-MossRehab Camp Independence 2017-Medical Information DIRECTIONS FOR COMPLETION: Step 1. This form must be fully completed and signed by the applicant s physician. No substitutions of this form will
PATIENT INFORMATION FORM (WOMEN ONLY)
") PATIENT INFORMATION FORM (WOMEN ONLY) Name: Age: Sex: Birthdate: / / SS # A. Describe briefly your present symptom(s) or the reason(s) for seeing the doctor today: B. Name all illnesses or conditions for
PATIENT INFORMATION FORM (WOMEN ONLY) Name: Age: Sex: Birthdate: / / SS # A. Describe briefly your present symptom(s) or the reason(s) for seeing the doctor today: B. Name all illnesses or conditions for
Dear Incoming Student:
 Dear Incoming Student: As the Director of Wellness Services, I want to welcome you to Nyack College! Our Staff is dedicated to providing you with quality health care. Our philosophy is based on the wellness
Dear Incoming Student: As the Director of Wellness Services, I want to welcome you to Nyack College! Our Staff is dedicated to providing you with quality health care. Our philosophy is based on the wellness
WELLNESS CENTER Student Health Services (434) FAX (434)
 FAX (434)") Page 1 WELLNESS CENTER Student Health Services (434) 223-6167 FAX (434) 223-7071 New Student Health Form The staff at Student Health are dedicated to providing you with high-quality health care designed
Page 1 WELLNESS CENTER Student Health Services (434) 223-6167 FAX (434) 223-7071 New Student Health Form The staff at Student Health are dedicated to providing you with high-quality health care designed
5. Statement of Applicant Health
 5. Statement of Applicant Health Applicant Name: Date of Examination: Height: Weight: Blood Type (If known): Physician must answer each of the following questions. To be completed by attending physician.
5. Statement of Applicant Health Applicant Name: Date of Examination: Height: Weight: Blood Type (If known): Physician must answer each of the following questions. To be completed by attending physician.
Camper Health History and Permission to Treat Name
 F O R R E S T E L R I D I N G office use only 1 2 3 4 5 6 & S P O R T S C A M P Camper Health History and Permission to Treat Name Last First Middle Birthdate Age at camp Grade in Fall Gender Male Female
F O R R E S T E L R I D I N G office use only 1 2 3 4 5 6 & S P O R T S C A M P Camper Health History and Permission to Treat Name Last First Middle Birthdate Age at camp Grade in Fall Gender Male Female
Child Health/Dental History Form
 Child Health/Dental History Form Patient s Name Nickname Date of Birth LAST FIRST INITIAL Parent s/guardian s Name Relationship to Patient Address PO OR MAILING ADDRESS CITY STATE ZIP CODE Phone Sex M
Child Health/Dental History Form Patient s Name Nickname Date of Birth LAST FIRST INITIAL Parent s/guardian s Name Relationship to Patient Address PO OR MAILING ADDRESS CITY STATE ZIP CODE Phone Sex M
A B O U T Y O U D E N T A L I N F O R M A T I O N
 1 A B O U T Y O U Full Name: Welcome to Voller Dentistry. We d like to get to know you better so that we can do our best to ensure your total oral health! Marital Status: Spouse s Name: Spouse s Occupation:
1 A B O U T Y O U Full Name: Welcome to Voller Dentistry. We d like to get to know you better so that we can do our best to ensure your total oral health! Marital Status: Spouse s Name: Spouse s Occupation:
Peninsula Puffers Asthma Camp 2019 Application
 Peninsula Puffers Asthma Camp 2019 Application Camp is for children, ages 8 to 14, who take medications daily for their asthma. Online Registration is available at www.aafaalaska.com CAMP DATES: June 9-
Peninsula Puffers Asthma Camp 2019 Application Camp is for children, ages 8 to 14, who take medications daily for their asthma. Online Registration is available at www.aafaalaska.com CAMP DATES: June 9-
PEDIATRIC REGISTRATION FORM
 MONTCLAIR HOMEOPATHY LLC Linda Corenthal Robins, M.D. Montclair, NJ 0704 Office 973-746-9888 www.montclairhomeopathy.com PEDIATRIC REGISTRATION FORM Referred by: Name Nickname Birth date Mother s Name
MONTCLAIR HOMEOPATHY LLC Linda Corenthal Robins, M.D. Montclair, NJ 0704 Office 973-746-9888 www.montclairhomeopathy.com PEDIATRIC REGISTRATION FORM Referred by: Name Nickname Birth date Mother s Name
PARTICIPANT APPLICATION FORM
 PARTICIPANT APPLICATION FORM Thank you for your interest in Camp Without Borders! Please carefully read and complete all areas of the application form. Applications must be submitted by the deadline to
PARTICIPANT APPLICATION FORM Thank you for your interest in Camp Without Borders! Please carefully read and complete all areas of the application form. Applications must be submitted by the deadline to
DIRECTIONS & PARKING. Robert Gramlich, MD Homeopath 8939 S. Sepulveda Blvd., Ste. 530 Los Angeles, CA Office (310)
") DIRECTIONS & PARKING Robert Gramlich, MD Homeopath 8939 S. Sepulveda Blvd., Ste. 530 Los Angeles, CA 90045 Office (310) 337.7315 From the North: Take 405 South, exit Howard Hughes Parkway and make a right
DIRECTIONS & PARKING Robert Gramlich, MD Homeopath 8939 S. Sepulveda Blvd., Ste. 530 Los Angeles, CA 90045 Office (310) 337.7315 From the North: Take 405 South, exit Howard Hughes Parkway and make a right
Client Registration Form
 Client Registration Form Personal Information Title: Mr. Mrs. Ms. Miss. Dr. First Name: Middle Name: Last Name: Date of Birth: Sex: Female Male Other Wt. Ht. Contact Details Street Address, appt., ste.,:
Client Registration Form Personal Information Title: Mr. Mrs. Ms. Miss. Dr. First Name: Middle Name: Last Name: Date of Birth: Sex: Female Male Other Wt. Ht. Contact Details Street Address, appt., ste.,:
Date First Name Middle Name Last Name. SSN Sex Birth Date Height Weight. Marital Status Spouse Name Number of Children. Address City State Zip
 PATIENT INFORMATION Date First Name Middle Name Last Name SSN Sex Birth Date Height Weight Marital Status Spouse Name Number of Children Address City State Zip Home Phone Cell Phone Email Emergency Relation
PATIENT INFORMATION Date First Name Middle Name Last Name SSN Sex Birth Date Height Weight Marital Status Spouse Name Number of Children Address City State Zip Home Phone Cell Phone Email Emergency Relation
INITIAL MEDICAL PACKET
 P a g e 1 INITIAL MEDICAL PACKET Name: Sport: Date: Last First Middle SSN: - - DOB: / / Age: Cell Phone: ( ) - Home Phone: ( ) - Family Physician: Phone: ( ) - Emergency contact: Name: Phone: ( ) - Relationship:
P a g e 1 INITIAL MEDICAL PACKET Name: Sport: Date: Last First Middle SSN: - - DOB: / / Age: Cell Phone: ( ) - Home Phone: ( ) - Family Physician: Phone: ( ) - Emergency contact: Name: Phone: ( ) - Relationship:
Home Number: ( ) Cell Number: ( ) SSN#: Address: Address: Date of Birth Sex. Place of Birth Marital Status: (Optional) (City & State)
 Cell Number: ( ) SSN#: Address: Address: Date of Birth Sex. Place of Birth Marital Status: (Optional) (City & State)") I. APPLICATION INSTRUCTIONS: School of Ultrasound Telephone (225) 756-3327 APPLICATION FOR APPOINTMENT AS STUDENT ULTRASOUND TECHNOLOGIST IN CARDIAC AND VASCULAR Applications for Admissions must include
I. APPLICATION INSTRUCTIONS: School of Ultrasound Telephone (225) 756-3327 APPLICATION FOR APPOINTMENT AS STUDENT ULTRASOUND TECHNOLOGIST IN CARDIAC AND VASCULAR Applications for Admissions must include
ADULT CASE HISTORY PLEASE PRINT IN INK OR TYPE ALL INFORMATION. Heaing Evaluation. Date of Birth: Gender: Spouse s Name: Spouse s Occupation:
 California State University, Fresno Speech, Language and Hearing Clinic 5310 North Campus Drive M/S PH 80 Fresno, California 93740-8019 (559) 278-2422 Fax (559) 278-5187 ADULT CASE HISTORY PLEASE PRINT
California State University, Fresno Speech, Language and Hearing Clinic 5310 North Campus Drive M/S PH 80 Fresno, California 93740-8019 (559) 278-2422 Fax (559) 278-5187 ADULT CASE HISTORY PLEASE PRINT
Eczema: also called atopic dermatitis; a chronic, itchy, scaly rash not due to a particular substance exposure
 Allergy is a condition in which the immune system causes sneezing, itching, rashes, and wheezing, or sometimes even life-threatening allergic reactions. The more you know about allergies, the better prepared
Allergy is a condition in which the immune system causes sneezing, itching, rashes, and wheezing, or sometimes even life-threatening allergic reactions. The more you know about allergies, the better prepared
Patient Medical History
 #3 1810, 8 th Street East, Saskatoon SK S7H0T6 Phone (306) 373-5209 Fax (306) 373 5207 Michelle Kormos, Osteopathy (current study) Patient Medical History Please complete the entire medical history and
#3 1810, 8 th Street East, Saskatoon SK S7H0T6 Phone (306) 373-5209 Fax (306) 373 5207 Michelle Kormos, Osteopathy (current study) Patient Medical History Please complete the entire medical history and
Employed? Yes No Employer Name. Occupation. Problem Onset Frequency Severity E.g. Headaches June times per week Mild / Moderate / Severe
 PLEASE NOTE: This file must be saved to your desktop before and after completing! PATIENT INFORMATION Date First Name SSN Sex Marital Status Middle Name Birth Date Last Name Height Spouse Name Address
PLEASE NOTE: This file must be saved to your desktop before and after completing! PATIENT INFORMATION Date First Name SSN Sex Marital Status Middle Name Birth Date Last Name Height Spouse Name Address
STUDENT HEALTH FORM. Name of Student Birth Date Sex (MM/DD/YY) Entrance Date (MM/DD/YY) Siblings in the School (names and grades)
 Entrance Date (MM/DD/YY) Siblings in the School (names and grades)") STUDENT HEALTH FORM If you are a new student enrolling at AISC, please attach a copy of the immunization records & proof of physical exam in the last 12 months & submit the complete form to: Sanja Ilic,
STUDENT HEALTH FORM If you are a new student enrolling at AISC, please attach a copy of the immunization records & proof of physical exam in the last 12 months & submit the complete form to: Sanja Ilic,
St Andrews Camp & Retreat Center
 Dear Campers, Parents, Guardians, and Friends: Medical Evaluation Camper When we think of resident camping, we should think of fun and excitement, yet even more importantly, at St. Andrews Camp, health
Dear Campers, Parents, Guardians, and Friends: Medical Evaluation Camper When we think of resident camping, we should think of fun and excitement, yet even more importantly, at St. Andrews Camp, health
Is your child on the BUPA School Medical Insurance Scheme?
 Section1 Student Forenames: Students Personal Medical Record Last Name: Date of Birth: Parental Address: Place of Birth: Fathers Address if Different: Phone Number: Email Address: Phone Number: Email Address:
Section1 Student Forenames: Students Personal Medical Record Last Name: Date of Birth: Parental Address: Place of Birth: Fathers Address if Different: Phone Number: Email Address: Phone Number: Email Address:
PATIENT INFORMATION Please print clearly and complete all blanks
 PATIENT INFORMATION Please print clearly and complete all blanks DATE: REFERRED BY: SEX: NAME: LAST FIRST MIDDLE BIRTHDATE: MAILING ADDRESS: CITY STATE ZIP TELEPHONE: CELL PHONE: WORK NUMBER: SS # MARITAL
PATIENT INFORMATION Please print clearly and complete all blanks DATE: REFERRED BY: SEX: NAME: LAST FIRST MIDDLE BIRTHDATE: MAILING ADDRESS: CITY STATE ZIP TELEPHONE: CELL PHONE: WORK NUMBER: SS # MARITAL
PATIENT REGISTRATION
 PATIENT REGISTRATION Last Name First Name MI Street Address City State Zip Code Social Security # - - Email Address Home Phone( ) Cell Phone( ) Sex Male Female of Birth Age Marital Status Married Single
PATIENT REGISTRATION Last Name First Name MI Street Address City State Zip Code Social Security # - - Email Address Home Phone( ) Cell Phone( ) Sex Male Female of Birth Age Marital Status Married Single
Florida School for the Deaf & the Blind
 Florida School for the Deaf & the Blind Do More. Be More. Achieve More. Applications should be mailed or faxed to: Florida School for the Deaf and the Blind Rebecca Falbo, Deaf Department Principal 207
Florida School for the Deaf & the Blind Do More. Be More. Achieve More. Applications should be mailed or faxed to: Florida School for the Deaf and the Blind Rebecca Falbo, Deaf Department Principal 207
Date First Name Middle Name Last Name. SSN Sex Birth Date Height Weight. Marital Status Spouse Name Number of Children. Address City State Zip
 PATIENT INFORMATION Date First Name Middle Name Last Name SSN Sex Birth Date Height Weight Marital Status Spouse Name Number of Children Address City State Zip Home Phone Cell Phone Email Emergency Relation
PATIENT INFORMATION Date First Name Middle Name Last Name SSN Sex Birth Date Height Weight Marital Status Spouse Name Number of Children Address City State Zip Home Phone Cell Phone Email Emergency Relation
Clarkson University Summer Camp Health Packet 2017 Camp(s) Attending: Dates:
 Attending: Dates:") Please print or type all information. Clarkson University Summer Camp Health Packet 2017 Camp(s) Attending: Dates: Camper s Information First Name: Last Name: Address: City: State: Zip Code: Country: Date
Please print or type all information. Clarkson University Summer Camp Health Packet 2017 Camp(s) Attending: Dates: Camper s Information First Name: Last Name: Address: City: State: Zip Code: Country: Date
New Patient Paperwork
 New Patient Paperwork NAME: Last: First: MI: Nickname: ADDRESS: Street: City: State: Zip: DOB: Male Female SSN#: - - Home: ( ) Work: ( ) Mobile: ( ) Email: If applicable, Spouse s Name: Emergency Contact
New Patient Paperwork NAME: Last: First: MI: Nickname: ADDRESS: Street: City: State: Zip: DOB: Male Female SSN#: - - Home: ( ) Work: ( ) Mobile: ( ) Email: If applicable, Spouse s Name: Emergency Contact
POPE JOHN PAUL II REGIONAL CATHOLIC ELEMENTARY CERTIFICATE OF IMMUNIZATION
 POPE JOHN PAUL II REGIONAL CATHOLIC ELEMENTARY DATE: STUDENT NAME: GRADE ENTERING PJPII: PHONE: DATE OF BIRTH: SCHOOL YEAR: CERTIFICATE OF IMMUNIZATION The Pennsylvania School Health Law states: The following
POPE JOHN PAUL II REGIONAL CATHOLIC ELEMENTARY DATE: STUDENT NAME: GRADE ENTERING PJPII: PHONE: DATE OF BIRTH: SCHOOL YEAR: CERTIFICATE OF IMMUNIZATION The Pennsylvania School Health Law states: The following
STUDENT HEALTH SERVICES 204 College Rd, Hampden-Sydney, VA 23943
 Page 1 STUDENT HEALTH SERVICES 204 College Rd, Hampden-Sydney, VA 23943 NEW STUDENT HEALTH FORM The staff at Student Health are dedicated to providing you with high-quality health care designed specifically
Page 1 STUDENT HEALTH SERVICES 204 College Rd, Hampden-Sydney, VA 23943 NEW STUDENT HEALTH FORM The staff at Student Health are dedicated to providing you with high-quality health care designed specifically
Part I: Health Form. This form is to be completed by the incoming student by July 15. Name: Date of Birth:
 Part I: Health Form This form is to be completed by the incoming student by July 15. Name: Date of Birth: Last First Middle MM/DD/YYYY Social Security #: Marital Status: ( ) Single ( ) Married ( ) Divorced
Part I: Health Form This form is to be completed by the incoming student by July 15. Name: Date of Birth: Last First Middle MM/DD/YYYY Social Security #: Marital Status: ( ) Single ( ) Married ( ) Divorced
We confirm that the above insurance information is correct.
 ATHLETE INFORMATION AND HEALTH QUESTIONNAIRE MISSOURI STATE UNIVERSITY SECTION 1 STUDENT-ATHLETE DEMOGRAPHIC INFORMATION FULL LEGAL NAME: Last: First: MI SS#: SPORT: DATE OF BIRTH: HOME PHONE: CELL PHONE:
ATHLETE INFORMATION AND HEALTH QUESTIONNAIRE MISSOURI STATE UNIVERSITY SECTION 1 STUDENT-ATHLETE DEMOGRAPHIC INFORMATION FULL LEGAL NAME: Last: First: MI SS#: SPORT: DATE OF BIRTH: HOME PHONE: CELL PHONE:
INSURANCE AND MANAGED CARE APPOINTMENT CANCELING POLICY
 The physicians and staff of New England Dermatology & Laser Center value and appreciate your selection of our office for your skin care. We are committed to providing you with the best possible service.
The physicians and staff of New England Dermatology & Laser Center value and appreciate your selection of our office for your skin care. We are committed to providing you with the best possible service.
Constant Daily. job children sex. bowels urinary 10 20% 30 40% 50 60% 70 80% 90% 100%
 Patient Name: Date: PRIMARY COMPLAINTS: Please list in order of most severe (#1) to least severe (#4). Sample complaints: Low Back, Left Knee, Right Shoulder, Neck, etc. You have the following complaints
Patient Name: Date: PRIMARY COMPLAINTS: Please list in order of most severe (#1) to least severe (#4). Sample complaints: Low Back, Left Knee, Right Shoulder, Neck, etc. You have the following complaints
PATIENT INFORMATION. Date: Patient Name: SS#: Address: City: State: Zip: Phone: (Home) (Work) (Cell)
 (Work) (Cell)") PATIENT INFORMATION Date: Patient Name: SS#: Address: City: State: Zip: Phone: (Home) (Work) (Cell) Email: Gender: Male ( ) Female ( ) Age: Birthdate: Marital Status: Married ( ) Widowed ( ) Single ( )
PATIENT INFORMATION Date: Patient Name: SS#: Address: City: State: Zip: Phone: (Home) (Work) (Cell) Email: Gender: Male ( ) Female ( ) Age: Birthdate: Marital Status: Married ( ) Widowed ( ) Single ( )
CAMP GLOW 2017 APPLICATION FORM
 Part I: Applicant Information: Name of Applicant: CAMP GLOW 2017 APPLICATION FORM Address: Date of Birth: Phone Number (s): Name of Person Completing this Application: Relation to Applicant: Organizational
Part I: Applicant Information: Name of Applicant: CAMP GLOW 2017 APPLICATION FORM Address: Date of Birth: Phone Number (s): Name of Person Completing this Application: Relation to Applicant: Organizational
Jones Co. Jr. College Sports Medicine Medical History Questionairre
 Jones Co. Jr. College Sports Medicine Medical History Questionairre DEMOGRAPHIC INFORMATION Full Name: Social Security #: - - Date of Birth: Sport: Year in School: Home Phone #: Cell Phone #: Parent/Guardian
Jones Co. Jr. College Sports Medicine Medical History Questionairre DEMOGRAPHIC INFORMATION Full Name: Social Security #: - - Date of Birth: Sport: Year in School: Home Phone #: Cell Phone #: Parent/Guardian
Date of Birth: Age: Sex: male female. Weight: Height: Address: Parents: Mother s Phone: (home) (cell) (work) Mother s
 (cell) (work) Mother s") *All information provided is kept in strict confidence Child s Name: Date: Date of Birth: Age: Sex: male female Weight: Height: Girls: Age at first period: Address: Parents: Mother s Phone: (home) (cell)
*All information provided is kept in strict confidence Child s Name: Date: Date of Birth: Age: Sex: male female Weight: Height: Girls: Age at first period: Address: Parents: Mother s Phone: (home) (cell)
PATIENT INFORMATION DENTAL HEALTH HISTORY
 PATIENT INFORMATION Welcome to Pristine Family and Implant Dentistry. We appreciate the confidence you place with us to provide dental services. To assist us in serving you, please complete the following
PATIENT INFORMATION Welcome to Pristine Family and Implant Dentistry. We appreciate the confidence you place with us to provide dental services. To assist us in serving you, please complete the following
MEDICAL HISTORY (To be filled in by patient)
") MEDICAL HISTORY Reason for Visit or Chief Complaint: Referred By: Present Illness: (To be filled in by Physician) I. Have you had any reactions, allergies or bad effects from any of the following: Serum
MEDICAL HISTORY Reason for Visit or Chief Complaint: Referred By: Present Illness: (To be filled in by Physician) I. Have you had any reactions, allergies or bad effects from any of the following: Serum
St. Louis Public School District PARENT PERMISSION FOR THE ADMINISTRATION OF OVER-THE- COUNTER MEDICATION
 St. Louis Public School District PARENT PERMISSION FOR THE ADMINISTRATION OF OVER-THE- COUNTER MEDICATION Listed below are nonprescription medications that the nurses can give to students only with parent
St. Louis Public School District PARENT PERMISSION FOR THE ADMINISTRATION OF OVER-THE- COUNTER MEDICATION Listed below are nonprescription medications that the nurses can give to students only with parent
Child Intake Form (To be completed by the parent or guardian and returned to the clinic) Phone: Select.
 Phone: Select.") NORTHEASTERN UNIVERSITY Speech, Language, and Hearing Center 30 Leon Street 503 Behrakis Health Science Center Boston, MA 02115 Ph: (617) 373-2492 Fx: (617) 373-8756 1 TODAY S DATE: Child Intake Form (To
NORTHEASTERN UNIVERSITY Speech, Language, and Hearing Center 30 Leon Street 503 Behrakis Health Science Center Boston, MA 02115 Ph: (617) 373-2492 Fx: (617) 373-8756 1 TODAY S DATE: Child Intake Form (To
New Patient Documentation. Name: (Last) (First) (Middle) Address: (Street) (Apt#) (City) (State) (Zip) Home Phone: ( ) Cell: ( ) Work: ( )
 (First) (Middle) Address: (Street) (Apt#) (City) (State) (Zip) Home Phone: ( ) Cell: ( ) Work: ( )") New Patient Documentation Name: (Last) (First) (Middle) Address: (Street) (Apt#) (City) (State) (Zip) Home Phone: ( ) Cell: ( ) Work: ( ) Age: Birthdate: E Email: Social: Sex: Male Female Height: Weight:
New Patient Documentation Name: (Last) (First) (Middle) Address: (Street) (Apt#) (City) (State) (Zip) Home Phone: ( ) Cell: ( ) Work: ( ) Age: Birthdate: E Email: Social: Sex: Male Female Height: Weight:
Patient s last name: First: Middle: Birth date: / / HISTORY Reason for consulting the doctor (describe your symptoms and complaint:
 Julie A. Wendt, MD, PLLC 21803 N. Scottsdale Rd, Ste 200 Scottsdale, AZ 85255 (480) 500-1902 PATIENT HEALTH QUESTIONNAIRE Today s date: Referring Doctor: Patient s last name: First: Middle: Birth date:
Julie A. Wendt, MD, PLLC 21803 N. Scottsdale Rd, Ste 200 Scottsdale, AZ 85255 (480) 500-1902 PATIENT HEALTH QUESTIONNAIRE Today s date: Referring Doctor: Patient s last name: First: Middle: Birth date:
Upper Iowa University Athletic Training. Name: Last First Middle. Home Address: Street Address City State Zip
 Upper Iowa University Athletic Training MEDICAL HISTORY Personal Data Name: Last First Middle Home Address: Street Address City State Zip School Address: Street Address City State Zip Home Phone #: Cell
Upper Iowa University Athletic Training MEDICAL HISTORY Personal Data Name: Last First Middle Home Address: Street Address City State Zip School Address: Street Address City State Zip Home Phone #: Cell
Medical Questionnaire
 Medical Questionnaire Date: Day Month Year Please answer these questions as completely as you can. We realize that this form is long, but the information in this form will be extremely valuable to us in
Medical Questionnaire Date: Day Month Year Please answer these questions as completely as you can. We realize that this form is long, but the information in this form will be extremely valuable to us in
Notto Chiropractic Health Center Patient Information
 Notto Chiropractic Health Center Patient Information Acct #: Name: Preferred Name: Address: City: State: Zip: Home Phone: ( ) - _. Work Phone: ( ) -. Who Referred You? In Case of Emergency: Phone Number:
Notto Chiropractic Health Center Patient Information Acct #: Name: Preferred Name: Address: City: State: Zip: Home Phone: ( ) - _. Work Phone: ( ) -. Who Referred You? In Case of Emergency: Phone Number:
Liver Health: Do you have liver problems? Yes No If so, please specify:
 Medical History General Last Name: First Name: Date of Birth: Age: Contact Number: Are you in good health to the best of your knowledge Medical Information: Please list any physicians you see and their
Medical History General Last Name: First Name: Date of Birth: Age: Contact Number: Are you in good health to the best of your knowledge Medical Information: Please list any physicians you see and their
Patient Name: Physician s Name Phone # Date of last physical Place a mark on yes or no to AIDS/HIV. Yes No Liver Disease.
 Patient Name: Date: HEALTH HISTORY Physician s Name Phone # Date of last physical Place a mark on yes or no to AIDS/HIV Heart Murmur Tuberculosis ANEMIA Heart Problems Tumor or growth on head/neck Arthritis,
Patient Name: Date: HEALTH HISTORY Physician s Name Phone # Date of last physical Place a mark on yes or no to AIDS/HIV Heart Murmur Tuberculosis ANEMIA Heart Problems Tumor or growth on head/neck Arthritis,
Institute for Continuing Theological Education Pontifical North American College
 Institute for Continuing Theological Education Pontifical North American College 00120 Vatican City State Europe Medical History and Physician s Report (Applicant completes pages 1-to-3 before taking this
Institute for Continuing Theological Education Pontifical North American College 00120 Vatican City State Europe Medical History and Physician s Report (Applicant completes pages 1-to-3 before taking this
Pharmacy and Referrals Pharmacy Name, Street Address & Telephone #: Primary Care Physician s Name, Location & Telephone #:
 Patient Registration Please Print Clearly Date: Last Name: First Name: Middle Initial: Sex: Date of Birth: / / Age: Social Security: - - Address: City: State: Zip Code - Circle Preferred Phone Number Home
Patient Registration Please Print Clearly Date: Last Name: First Name: Middle Initial: Sex: Date of Birth: / / Age: Social Security: - - Address: City: State: Zip Code - Circle Preferred Phone Number Home
MEDICAL HISTORY RECORD
 MEDICAL HISTORY RECORD Please print and complete all information. Case. Male Female Medicare. Medicaid. Today s Date Birthdate Last Name First Middle Daytime Phone Home Phone Address City Marital Status
MEDICAL HISTORY RECORD Please print and complete all information. Case. Male Female Medicare. Medicaid. Today s Date Birthdate Last Name First Middle Daytime Phone Home Phone Address City Marital Status
Last: First: MI: Nickname:
 New Patient Paperwork NAME: Last: First: MI: Nickname: ADDRESS: Street: City: State: Zip: DOB: Male Female SSN#: - - Home: ( ) Work: ( ) Mobile: ( ) Email: If applicable, Spouse s Name: Emergency Contact
New Patient Paperwork NAME: Last: First: MI: Nickname: ADDRESS: Street: City: State: Zip: DOB: Male Female SSN#: - - Home: ( ) Work: ( ) Mobile: ( ) Email: If applicable, Spouse s Name: Emergency Contact
CHILD INTAKE (Please Print Clearly)
") Jeremy Hayman, ND CHILD INTAKE (Please Print Clearly) Doctor of Naturopathic Medicine Child s name (First/Last) Date of birth (M/D/Y) Sex M F Referred by Who is filling out this form (name and relation)?
Jeremy Hayman, ND CHILD INTAKE (Please Print Clearly) Doctor of Naturopathic Medicine Child s name (First/Last) Date of birth (M/D/Y) Sex M F Referred by Who is filling out this form (name and relation)?
WELCOME TO THE MILLER CHIROPRACTIC CLINIC
 WELCOME TO THE MILLER CHIROPRACTIC CLINIC We are pleased that you have chosen to consult us regarding your health. In order to help us evaluate your condition thoroughly, please complete the following
WELCOME TO THE MILLER CHIROPRACTIC CLINIC We are pleased that you have chosen to consult us regarding your health. In order to help us evaluate your condition thoroughly, please complete the following
Welcome to our office!
 Vitality Chiropractic & Wellness Center 3348 Tyrone Blvd. St. Petersburg, FL 33710 WWW.DrWyckoff.com Phone (727) 381-7433 Fax (727) 381-7434 Welcome to our office! Please fill out our Health Record as
Vitality Chiropractic & Wellness Center 3348 Tyrone Blvd. St. Petersburg, FL 33710 WWW.DrWyckoff.com Phone (727) 381-7433 Fax (727) 381-7434 Welcome to our office! Please fill out our Health Record as
STUDENT HEALTH SERVICES IMMUNIZATION FORM FOR GUILFORD COLLEGE 5800 West Friendly Avenue Greensboro, NC 27410
 STUDENT HEALTH SERVICES IMMUNIZATION FORM FOR GUILFORD COLLEGE 5800 West Friendly Avenue Greensboro, NC 27410 P / 336-316-2194 F / 336-316-2184 A completed immunization record is required to be submitted
STUDENT HEALTH SERVICES IMMUNIZATION FORM FOR GUILFORD COLLEGE 5800 West Friendly Avenue Greensboro, NC 27410 P / 336-316-2194 F / 336-316-2184 A completed immunization record is required to be submitted
Dr. Sereena Uppal DC Michael Herrewig DC Doctor of Chiropractic th Avenue Surrey BC V4A 2H9 Tel: Fax:
 Dr. Sereena Uppal DC Michael Herrewig DC Doctor of Chiropractic 690 15355 24 th Avenue Surrey BC V4A 2H9 Tel: 604.541.9336 Fax: 604.541.9308 I. Patient Information Thank you for choosing our practice for
Dr. Sereena Uppal DC Michael Herrewig DC Doctor of Chiropractic 690 15355 24 th Avenue Surrey BC V4A 2H9 Tel: 604.541.9336 Fax: 604.541.9308 I. Patient Information Thank you for choosing our practice for
HEALTH HISTORY Since your well-being is our primary concern, please take the time to accurately answer the questions.
 HEALTH HISTORY Since your well-being is our primary concern, please take the time to accurately answer the questions. Date: Patient Full Name: DOB: Sex: M / F Social Security #: Address: Home #: Cell #:
HEALTH HISTORY Since your well-being is our primary concern, please take the time to accurately answer the questions. Date: Patient Full Name: DOB: Sex: M / F Social Security #: Address: Home #: Cell #:
PATIENT REGISTRATION PATIENT NAME: DOB: SS#: CITY: STATE: ZIP: CELL PHONE: EMPLOYER: EMPLOYER PHONE: ( ) EMERGENCY CONTACT PH# ( ) RELATIONSHIP:
 EMERGENCY CONTACT PH# ( ) RELATIONSHIP:") PATIENT NAME: DOB: SS#: NAME OF PARENTS (if patient is a minor) PATIENT REGISTRATION HOME ADDRESS HOME PHONE: CITY: STATE: ZIP: CELL PHONE: MAILING ADDRESS (if different) CITY: STATE: ZIP: EMPLOYER: EMPLOYER
PATIENT NAME: DOB: SS#: NAME OF PARENTS (if patient is a minor) PATIENT REGISTRATION HOME ADDRESS HOME PHONE: CITY: STATE: ZIP: CELL PHONE: MAILING ADDRESS (if different) CITY: STATE: ZIP: EMPLOYER: EMPLOYER
Adult Health History Summary
 Adult Health History Summary Name Age Date of Birth Address City Province Postal Code Phone (home) (cell) Occupation Email May we contact you via email? YES NO Emergency Contact Phone # How did you hear
Adult Health History Summary Name Age Date of Birth Address City Province Postal Code Phone (home) (cell) Occupation Email May we contact you via email? YES NO Emergency Contact Phone # How did you hear
Southwestern Community College Extension Education Fire & Rescue Training Programs Student Medical Form
 Jerry Sutton Public Safety Training Center 225 Industrial Park Loop Franklin, NC 28734 (828) 306- -2428 www.southwesterncc.edu/content/public-safety-training Southwestern Community College Extension Education
Jerry Sutton Public Safety Training Center 225 Industrial Park Loop Franklin, NC 28734 (828) 306- -2428 www.southwesterncc.edu/content/public-safety-training Southwestern Community College Extension Education
Family Self-Care and Over the Counter Medications Program. Sponsored by: FAHC Department of Pharmacy
 Family Self-Care and Over the Counter Medications Program Sponsored by: FAHC Department of Pharmacy What are Over the Counter Medications? Nonprescription medications and products Often referred to as
Family Self-Care and Over the Counter Medications Program Sponsored by: FAHC Department of Pharmacy What are Over the Counter Medications? Nonprescription medications and products Often referred to as
Patient Name: Date / Time of Appt: at
 12422 South 450 East, Suite C, Draper, UT 84020 (801) 553-1900 Fax (801) 553-9995 Patient Name: Date / Time of Appt: at Duane J. Harris, MD and the staff of Intermountain Allergy & Asthma of Draper welcome
12422 South 450 East, Suite C, Draper, UT 84020 (801) 553-1900 Fax (801) 553-9995 Patient Name: Date / Time of Appt: at Duane J. Harris, MD and the staff of Intermountain Allergy & Asthma of Draper welcome
Date of Birth Work Phone # ( ) Home Phone # ( ) Emergency Contact # ( )
 Home Phone # ( ) Emergency Contact # ( )") Please complete the following form in order to provide us with the background information we require to ensure you receive comprehensive care. It should take 15-20 minutes. Contact Information: Name Occupation
Please complete the following form in order to provide us with the background information we require to ensure you receive comprehensive care. It should take 15-20 minutes. Contact Information: Name Occupation
STUDENT MEDICATIONS If your child is accepted, he or she must bring all prescription medications in their original pharmacy container.
 TEXAS SCHOOL FOR THE BLIND AND VISUALLY IMPAIRED STUDENT MEDICAL / DIETARY HISTORY FORM Information for Parent: So that we can safely care for your child, please provide complete and specific information
TEXAS SCHOOL FOR THE BLIND AND VISUALLY IMPAIRED STUDENT MEDICAL / DIETARY HISTORY FORM Information for Parent: So that we can safely care for your child, please provide complete and specific information
Feil & Oppenheimer Psychological Services
 Feil & Oppenheimer Psychological Services 260 Waseca Ave. Barrington, RI 02806 401-245-4040 Fax: 401-245-1240 feiloppenheimer@gmail.com Adult Patient Questionnaire Name: Today's Date: Address: Home Phone:
Feil & Oppenheimer Psychological Services 260 Waseca Ave. Barrington, RI 02806 401-245-4040 Fax: 401-245-1240 feiloppenheimer@gmail.com Adult Patient Questionnaire Name: Today's Date: Address: Home Phone:
VGCC VANCE-GRANVILLE COMMUNITY COLLEGE
 Student Medical Form VGCC VANCE-GRANVILLE COMMUNITY COLLEGE STUDENT MEDICAL FORM VANCE-GRANVILLE COMMUNITY COLLEGE INSTRUCTIONS FOR COMPLETING STUDENT MEDICAL FORM 1. Complete the four-page insert: Physical
Student Medical Form VGCC VANCE-GRANVILLE COMMUNITY COLLEGE STUDENT MEDICAL FORM VANCE-GRANVILLE COMMUNITY COLLEGE INSTRUCTIONS FOR COMPLETING STUDENT MEDICAL FORM 1. Complete the four-page insert: Physical
For Students Who are Deaf or Hard of Hearing
 For Students Who are Deaf or Hard of Hearing June 3 - June 15, 2018 Driver Education for Students Who are Deaf or Hard of Hearing Two-week Long Summer School for Eligible Ohio Teens Columbus, OH The Ohio
For Students Who are Deaf or Hard of Hearing June 3 - June 15, 2018 Driver Education for Students Who are Deaf or Hard of Hearing Two-week Long Summer School for Eligible Ohio Teens Columbus, OH The Ohio
Chiropractic Registration and History
 Chiropractic Registration and History 1. Patient Information Name: Birthdate: SS/HIC/Patient ID #: Address: City: State: Zip: Phone: Cell: E-Mail: Sex: M F (Circle) Minor Single Married Divorced Separated
Chiropractic Registration and History 1. Patient Information Name: Birthdate: SS/HIC/Patient ID #: Address: City: State: Zip: Phone: Cell: E-Mail: Sex: M F (Circle) Minor Single Married Divorced Separated
PATIENT DATA SHEET GENERAL INFORMATION DATE ( ) ( ) ( ) HOME PHONE WORK PHONE CELL PHONE
 ( ) ( ) HOME PHONE WORK PHONE CELL PHONE") PATIENT DATA SHEET GENERAL INFORMATION / / DATE LAST NAME FIRST NAME MIDDLE INITIAL ADDRESS CITY STATE ZIP CODE ( ) ( ) ( ) HOME PHONE WORK PHONE CELL PHONE EMAIL ADDRESS SEX MALE FEMALE (PLEASE CIRCLE)
PATIENT DATA SHEET GENERAL INFORMATION / / DATE LAST NAME FIRST NAME MIDDLE INITIAL ADDRESS CITY STATE ZIP CODE ( ) ( ) ( ) HOME PHONE WORK PHONE CELL PHONE EMAIL ADDRESS SEX MALE FEMALE (PLEASE CIRCLE)
Name Age DOB Sex M F Your relationship status: Single Married Life partner Widowed Address
 Today s Date Contact Information Name Age DOB Sex M F Your relationship status: Single Married Life partner Widowed Address Phone numbers and E-mail (please check numbers to call or leave a message) Home
Today s Date Contact Information Name Age DOB Sex M F Your relationship status: Single Married Life partner Widowed Address Phone numbers and E-mail (please check numbers to call or leave a message) Home
Address: City: Postal Code: Emergency Contact: Phone# Relationship: Who may we thank for referring you to this office?
 CLAYTON PARK CHIROPRACTIC CENTRE INC. Suite 11-117 Kearney Lake Road Halifax, Nova Scotia B3M 4N9 (902) 443-5669 phone (902) 443-9419 fax info@claytonparkchiro.ca For Office Use Only: Bilaterals L R PERSONAL
CLAYTON PARK CHIROPRACTIC CENTRE INC. Suite 11-117 Kearney Lake Road Halifax, Nova Scotia B3M 4N9 (902) 443-5669 phone (902) 443-9419 fax info@claytonparkchiro.ca For Office Use Only: Bilaterals L R PERSONAL
* Health Insurance Verification Form, submitted on line. Click on link. Mandatory Health Insurance Verification Form
 Residential Student: The Health Office welcomes you to residential living. It is our goal in collaboration with Residential Life, Safety, and Security, and the Dean of Students to promote health and wellness
Residential Student: The Health Office welcomes you to residential living. It is our goal in collaboration with Residential Life, Safety, and Security, and the Dean of Students to promote health and wellness
CARY HOLISTIC HEALTH, LLC. Thank you for scheduling an appointment with Cary Holistic Health. Maggie Thibodeau, ND
 Maggie Thibodeau, ND CARY HOLISTIC HEALTH, LLC 222 Ashville Avenue, Suite 10 / Cary, NC 27518 (919) 858-1004 / CaryHolisticHealth.com Thank you for scheduling an appointment with. We are located at 222
Maggie Thibodeau, ND CARY HOLISTIC HEALTH, LLC 222 Ashville Avenue, Suite 10 / Cary, NC 27518 (919) 858-1004 / CaryHolisticHealth.com Thank you for scheduling an appointment with. We are located at 222
A Progression of Seemingly Unrelated Symptoms. Identifying and Managing Potential Allergic Food and Respiratory Sensitivities
 A Progression of Seemingly Unrelated Symptoms Identifying and Managing Potential Allergic Food and Respiratory Sensitivities Talk to your doctor if you or your loved one have experienced or is currently
A Progression of Seemingly Unrelated Symptoms Identifying and Managing Potential Allergic Food and Respiratory Sensitivities Talk to your doctor if you or your loved one have experienced or is currently
HEALTH HISTORY Since your well-being is our primary concern, please take the time to accurately answer the questions.
 HEALTH HISTORY Since your well-being is our primary concern, please take the time to accurately answer the questions. Date: Patient Full Name: DOB: Sex: M / F Social Security #: Address: Home #: Cell #:
HEALTH HISTORY Since your well-being is our primary concern, please take the time to accurately answer the questions. Date: Patient Full Name: DOB: Sex: M / F Social Security #: Address: Home #: Cell #:
«Think on... Allergies and allergens» First training session
 Training Report Form «Think on... Allergies and allergens» First training session Tasks: 1-1 to 1-5 This training session was performed by Group:..........................................................
Training Report Form «Think on... Allergies and allergens» First training session Tasks: 1-1 to 1-5 This training session was performed by Group:..........................................................
The Center For Healthy Living & Longevity Keri Topouzian, D.O. Fax:
 The Center For Healthy Living & Longevity Keri Topouzian, D.O. Fax: 248.792.0345 Pediatric Health Questionnaire Today s Date: / / BLOOD TYPE: Patient Name: Birth date: / / Age: Mother s Name Father s Name
The Center For Healthy Living & Longevity Keri Topouzian, D.O. Fax: 248.792.0345 Pediatric Health Questionnaire Today s Date: / / BLOOD TYPE: Patient Name: Birth date: / / Age: Mother s Name Father s Name
HEALTH OFFICE, Poughkeepsie, NY Residential Student:
 Residential Student: The Health Office welcomes you to residential living. It is our goal in collaboration with Residential Life, Safety, and Security, and the Dean of Students to promote health and wellness
Residential Student: The Health Office welcomes you to residential living. It is our goal in collaboration with Residential Life, Safety, and Security, and the Dean of Students to promote health and wellness
PATIENT MEDICAL HISTORY
 Patients Name: PATIENT MEDICAL HISTORY Address: Date of Last Visit: Date of Med History City: State: Zip: Email: Home Phone: Work Phone: Birth Date: Social Security No: Marital Status: Primary Dental Guarantor:
Patients Name: PATIENT MEDICAL HISTORY Address: Date of Last Visit: Date of Med History City: State: Zip: Email: Home Phone: Work Phone: Birth Date: Social Security No: Marital Status: Primary Dental Guarantor:
UCCM ANISHNAABE POLICE SERVICE EMPLOYMENT VISION REPORT
 APPLICANT NAME: UCCM ANISHNAABE POLICE SERVICE EMPLOYMENT VISION REPORT REACTION ACCOM. LIGHT PUPILS EQUAL UNEQUAL FUNDI FIELDS OF VISION COLOUR (TEST USED) WITHOUT GLASSES NEAR FAR WITH GLASSES RIGHT
APPLICANT NAME: UCCM ANISHNAABE POLICE SERVICE EMPLOYMENT VISION REPORT REACTION ACCOM. LIGHT PUPILS EQUAL UNEQUAL FUNDI FIELDS OF VISION COLOUR (TEST USED) WITHOUT GLASSES NEAR FAR WITH GLASSES RIGHT
Naturopathic & Acupuncture Intake Form (Age 14+)
") Dr. Katie Thomson Aitken BAS, ND Dr. Alaina Gair, B.Sc., ND 86 Norfolk St., Guelph 519-827-0040 Contact Information Naturopathic & Acupuncture Intake Form (Age 14+) Name: Gender: Age: Birth Date (dd/mm/yy):
Dr. Katie Thomson Aitken BAS, ND Dr. Alaina Gair, B.Sc., ND 86 Norfolk St., Guelph 519-827-0040 Contact Information Naturopathic & Acupuncture Intake Form (Age 14+) Name: Gender: Age: Birth Date (dd/mm/yy):
Chiropractic Case History/Patient Information
 1 Chiropractic Case History/Patient Information Name: Social Security # Home Phone: Address: City: State: Zip: E-mail address: Cell Phone: Age: Birth Date: Race: Marital Status: [M] [S ][W] [D] Occupation:
1 Chiropractic Case History/Patient Information Name: Social Security # Home Phone: Address: City: State: Zip: E-mail address: Cell Phone: Age: Birth Date: Race: Marital Status: [M] [S ][W] [D] Occupation:
Pharmacy and Referrals Pharmacy Name, Street Address & Telephone #: Primary Care Physician s Name, Location & Telephone #:
 Patient Registration Please Print Clearly Date: Last Name: First Name: Middle Initial: Sex: Date of Birth: / / Age: Social Security: - - Address: City: State: Zip Code - Home Phone #: Work Phone #: Cell
Patient Registration Please Print Clearly Date: Last Name: First Name: Middle Initial: Sex: Date of Birth: / / Age: Social Security: - - Address: City: State: Zip Code - Home Phone #: Work Phone #: Cell
Avicenna Acupuncture PEDIATRIC INTAKE FORM (BIRTH TO 5 YEARS)
") PEDIATRIC INTAKE FORM (BIRTH TO 5 YEARS) Date: Address: City: State: Zip: Parents Name: Telephone (cell): Parent s work #: Parent s email address: Date of Birth: Gender: How did you hear about this clinic?
PEDIATRIC INTAKE FORM (BIRTH TO 5 YEARS) Date: Address: City: State: Zip: Parents Name: Telephone (cell): Parent s work #: Parent s email address: Date of Birth: Gender: How did you hear about this clinic?