They re Scratching and You re Scratching Your Head: An Approach to the Diagnosis and Management of Acute and Chronic Urticaria
|
|
|
- Paula Bond
- 5 years ago
- Views:
Transcription
1 They re Scratching and You re Scratching Your Head: An Approach to the Diagnosis and Management of Acute and Chronic Urticaria Adelle R. Atkinson, MD, FRCPC Sea Courses May/June 2017
2 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or mechanical, including photocopying, recording, or information storage and retrieval systems without prior written permission of Sea Courses Inc. except where permitted by law. Sea Courses is not responsible for any speaker or participant s statements, materials, acts or omissions.
3 Learning Objectives At the end of this session, you will be able to: 1. Discuss the differential diagnoses of both acute and chronic urticaria 2. Describe the work-up and management of various forms of acute and chronic urticaria 3. describe an approach to the physical urticarias and their management
4 Acute and Chronic Urticaria

5 Definition Acute Urticaria The presence of hives every day or almost every day with a duration of less than 6 weeks Mast cell and basophil activation Chronic Urticaria The presence of hives every day or almost every day with a duration > 6 weeks But.Chronic Urticaria has to start somewhere, so patients need periodic re-evaluation
 time to resolution of symptoms presence of a viral illness exercise, heat, cold or")
6 Allergy - Diagnosis History specifics around the urticaria and whether there might have been a trigger (food, drug, environmental)? Associated angioedema action taken (antihistamines, epi-pen, 911) time to resolution of symptoms presence of a viral illness exercise, heat, cold or other physical triggers
7 Allergy - Diagnosis History continued Full review of systems for any other signs or symptoms of chronic disease thyroid disease, malignancy, autoimmunity, chronic viral infection etc. previous ingestions of the food/drug in question previous trials of therapy Personal and family history of atopy

8 Allergy - Diagnosis Physical Examination presence of existing allergic manifestations - angioedema, hives swollen nasal mucosa signs and symptoms of atopy Evidence of manifestations of any chronic disease
 Individual wheals usually fade within 24 to 48 hours with others")
9 Physical Examination CU lesions typically edematous pink or red wheals of variable size and shape with surrounding erythema and are usually pruritic Usually NOT painful or burning (more c/w vasculitis) Individual wheals usually fade within 24 to 48 hours with others forming

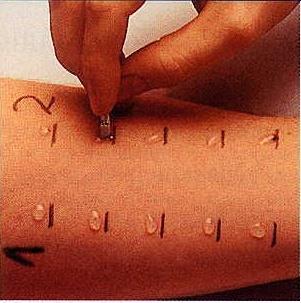
10 Skin Prick Testing



11 Skin Prick Testing Histamine Saline Peanut
12 Allergy - Diagnosis SPT must be tailored to each individual patient, one must not do a panel of screening tests looking for a positive reaction SPT is highly reproducible, and can be used for food, penicillin and environmental allergies the negative predictive value of SPT is very high in the order of 98 to 99% the PPV of SPT is variable -- unknown for penicillin and environmental, less than 50% for some foods
13 Allergy - Diagnosis Intracutaneous Testing used in most centres only with penicillin, vaccines and venom not used with environmental and food used after a negative SPT by doing an intradermal injection no good evidence that it adds to the SPT, many false positives needs to be compared with the gold standard Autologous Serum Skin Test (ASST) Utility not clear, only considered for CU Currently not routinely performed
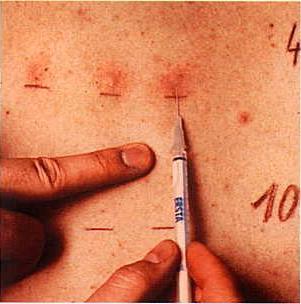
14 Intracutaneous testing
15 Allergy - Diagnosis Radioallergosorbent Test (RAST) in vitro test looking at specific IgE to specific allergens high negative predictive value positive predictive value low SPT more sensitive Offers some useful information and is particularly useful when SPT is not possible

16 Rast Testing
17 Rast Testing Anti-IgE Antigen IgE

18 Allergy - Diagnosis Double-Blind, Placebo- Controlled Food Challenge gold standard for the diagnosis of food allergy occasional false negatives must be done under supervision in a patient with a positive SPT and a questionable history a similar protocol has not been tried with penicillin
19 Acute Urticaria More likely to be associated with an identifiable condition Usually resolves spontaneously Needs a careful Hx and PE
20 Acute Urticaria Differential Diagnosis to consider after careful history and physical examination (and review of photos if available! especially if the patient is currently asymptomatic) Infections Viral, bacterial or parasitic IgE mediated reaction to: food, drugs Insect stings and bites Latex Blood products Direct mast cell activation Narcotics Muscle relaxants Vancomycin Radio contrast material Stinging nettle (urtica dioica) NSAIDS
21 Acute Urticaria Management Removal of offending agent First and second generation antihistamines Discussion with patients/families around the sedating side effects of first generation Brief course of oral steroids BUT there must be a plan as this is not a long term solution
22 Chronic Urticaria Less likely associated with an identifiable condition 0.5 to 5% of the general population May have both urticaria and angioedema occurring together or separately Histamine is the predominant mediator Activation of the coagulation cascade including increased prothrombin fragment F1 + 2 and D-dimer levels has been described and may be a marker of severity
23 Chronic Urticaria 30 50% of patients with CU produce specific IgG antibodies against the FcεR1αsubunit component of the high-affinity IgE receptor and 5 to 10% produce IgG antibodies against IgE itself Routine testing for food or inhalents, and extensive laboratory testing not recommended as it is not cost-effective and does not lead to improved patient outcomes Targeted laboratory testing based on Hx and PE is appropriate CBC and differential, ESR and/or CRP, liver enzymes, thyroid-stimulating hormone measurement This limited testing may be useful in patients with nothing in the history and physical to pick up rare cases (likely more in adults)
24 Chronic Urticaria Differential Diagnosis to consider after careful history and physical examination (and review of photos if available! especially if the patient is currently asymptomatic) Chronic idiopathic urticaria - majority Chronic viral infection ie: hepatitis B and C, EBV, HSV, Helicobacter pylori, helminthic parasitic infections Complement deficiencies Croyglobulinemia (eg. With Hepatitis C and CLL) Serum Sickness or other type III reactions Connective tissue diseases (SLE, JIA, thyroid disease) Endocrine disorders or hormonal therapies (eg. Ovarian tumors and OCP use) Mastocytosis/mastocytoma Urticarial vasculitis (hives usually last >24 hours) Malignancy
25 Chronic Urticaria But.. It is not recommended to do a workup for any of these disorders without evidence of additional features on history and physical examination tht suggest them Eg. Thyroid antibodies are frequently found in patients with CU and do not seem to be of clinical significance in the absence of associated clinical features Angioedema in the absence of urticaria goes down a different DDx pathway including: hereditary angioedema, ACE inhibitor associated angioedema etc.
26 Chronic Urticaria Management Avoid NSAIDs, heat, tight clothing No evidence to avoid any foods or other pseudoallergens
27 Stepwise Approach to the management of CIU 1. First-lie treatment is second-generation H1 antihistamines 2. Second-line therapy is up-dosing second-generation H1 antihistamins 3. Third-line treatment is omalizumab, recommended now before using Cyclosporin A 4. H2 antihistamines not included in the algorithm (case by case only) 5. Avoid first-generation H1 antihistamines based on benefitto-risk ratio 6. Corticosteroids considered only for short-term intervention; avoid as long-term treatment 7. Cyclosporin A for refractory CIU not responsive to other treatments
28 The Physical Urticarias

29 The Definition A subgroup of chronic urticaria (CU) Lesions reproducibly triggered by physical stimuli including: Cold Heat Physical pressure Vibration Water Sunlight exercise
 Can occur in isolation or with other chronic urticaria conditions Pathogenesis")
30 The Definition Physical stimulation incites the characteristic wheal and flare Can also cause angioedema Skin manifestations usually localized to the areas exposed to the stimuli (some systemic cases) Can occur in isolation or with other chronic urticaria conditions Pathogenesis unknown
31 Abijian et. al. Curr Allergy Asthma Rep 2012

32 The Background 0.5% of the general population has a PU Up to 25% of patients with CU have a PU

33 The History Duration & Frequency Description of the lesions (photos) Pruritis?/associated angioedema Context when the lesions occurred Management and response? History of atopy? Related to: Cold Heat Physical pressure Vibration Water Sunlight exercise

34 Simple Dermatographism (Urticaria Factitia) Most common form of PU Usually affects young adults Mean duration 6.5 years Development of itchy wheals induced by mild stroking, rubbing or scratching Whealing occurs quickly and lasts 0.5 to 2 hours
 Assess skin after 10 minutes Threshold")
35 Simple Dermatographism Provocation testing: (Urticaria Factitia) Rubbing the skin of the upper back or the volar of the forearm lightly with a smooth blunt object (dermographometer, tongue depressor) Assess skin after 10 minutes Threshold testing
36 Simple Dermatographism (Urticaria Factitia) Management: Symptom avoidance Avoid mechanical irritation, toweling after showering, light nonirritating clothing Second generation antihistamines (high doses) Leukotriene antagonists and/or H2 blockers Cyclosporin Omalizumab Narrow-band UV-B (need clinical trials)

37 Cholinergic Urticaria Up to 30% of cases of PU Lesions following a rise in body temperature (ie: exercise, hot bath) Symptoms decrease with age and eventually disappear Itchy, pinpoint wheals mostly on the limbs and trunk Last 15 to 60 minutes
38 Cholinergic Urticaria May also be induced by emotional stress and spicy foods and beverages May be due to antibodies to sweat Provocation testing: Moderate exercise on the treadmill to the point of sweating and 15 minutes beyond If the test is positive, passive warming test next (bath 42C) Passive warming differentiates from exercise induced urticaria/anaphylaxis Management: Avoidance 2 nd generation anti-histamines Desensitization protocols (regular exercise for eg.) Omalizumab Scopolamine Propanolol, anti-histamines, montelukast
, usually with a few hours delay (6 to 8) Frequently associated with severe burning and pain Flu-like symptoms, malaise,")
39 Delayed Pressure Urticaria Up to 1/3 of cases of PU (common in CU) Angioedema at sites of exposure to sustained pressure to the skin (belts, purse), usually with a few hours delay (6 to 8) Frequently associated with severe burning and pain Flu-like symptoms, malaise, arthralgia

40 Delayed Pressure Urticaria Proinflammatory cytokines, TNF etc. may be involved Provocation Testing: Apply pressure to the skin using weighted rods or a dermographometer Shoulder, upper back, things or volar survace of the forearm

41 Delayed Pressure Urticaria Postive test = red palpable swelling 6 hours later Threshold testing
42 Delayed Pressure Urticaria Management: Avoid mechanical pressure where possible Some reports of dapsone and sulfasalazine Non-sedating antihistamines High dose may be required (up to 4 times) Anti-leukotrienes have been tried

43 Cold-Induced Urticaria 5 to 30% of all PU Affects 2 sexes equally Release of inflammatory mediators after skin exposure to cold Occur within a few minutes of exposure Occur only in exposed areas Extensive cold contact ie: swimming may lead to systemic reactions (anaphylaxis)
44 Cold-Induced Urticaria May last from 5 to 8 years Provocation testing: Melting ice-cube in a thin plastic bag on the volar forearm for 5 minutes Assess response 10 minutes later Positive if test shows a palpable, visible wheal Usually pruritic and burning Threshold testing Management: Avoid ice-cold drinks Avoid very cold swimming pools/lakes Swim with a friend Prevention with 2 nd generation anti-histamines Usually higher than standard doses

45 Cold Induced Urticaria

46 Cold-Induced Urticaria Omalizumab, etanercept, anakinra Desensitization Decreasing the temperature of showers Maintenance through daily showers at lower temperature

47 Aquagenic Urticaria Rare < 100 cases described More common in women Onset after puberty Treatment with 2 nd generation antihistamines

48 Heat Contact Urticaria Rare (less than 100 cases described) Wheal after contact with temperatures that exceed those of the skin Lesions come a few minutes after exposure and resolve after 1 to 3 hours
49 Heat Contact Urticaria Provocation Testing: Local heat testing for 5 minutes at 45C Assess in 10 minutes Management: 2nd generation antihistamines Omalizumab (for difficult to treat patients)
50 Solar Urticaria/Vibratory Urticaria Solar Rare Whealing on exposure to UV light Systemic reactions can occur Prevention with 2 nd generation anti-histamines Desensitization Vibratory Rare Skin swellings and itching after exposure to vibration 2 nd generation antihistamines IVIG?
 More common in atopic individuals Typical symptoms of anaphylaxis: pruritis, urticaria, angioedema, flushing, shortness of")
51 Exercise-Induced Urticaria/Anaphylaxis 5 to 15% of all cases of anaphylaxis Induced by exercise with or without food (but not passive warming like Cholinergic urticaria) More common in atopic individuals Typical symptoms of anaphylaxis: pruritis, urticaria, angioedema, flushing, shortness of breath etc.
52 Exercise-Induced Urticaria/Anaphylaxis Provocation Testing: Exercise on treadmill supervised If food dependent suspected, NPO before one challenge but not the second Management: Avoid exercise in cold, hot or humid weather Avoid NSAIDs Avoid exercising outside in pollen season if seasonal atopy Avoid allergen if relevant (3 hours before and 1 hour after) 2 nd generation antihistamines (?as prophylaxis) Epinephrine autoinjector Exercise with a friend
53 Summary (What did we accomplish?) Here is what we said we would do: 1. Discuss the differential diagnoses of both acute and chronic urticaria 2. Describe the work-up and management of various forms of acute and chronic urticaria 3. describe an approach to the physical urticarias and their management

54
Urticaria and Angioedema. Allergy and Immunology Awareness Program
 Urticaria and Angioedema Allergy and Immunology Awareness Program 1 Urticaria and Angioedema Allergy and Immunology Awareness Program Urticaria Commonly known as hives, urticarial is an itchy rash with
Urticaria and Angioedema Allergy and Immunology Awareness Program 1 Urticaria and Angioedema Allergy and Immunology Awareness Program Urticaria Commonly known as hives, urticarial is an itchy rash with
Managing urticaria in primary care
 Managing urticaria in primary care Tidman MJ. Managing urticaria in primary care. Practitioner 2015;259(1779)25-28 Dr Michael J. Tidman MD FRCP (Ed) FRCP (Lond) Consultant Dermatologist, Department of
Managing urticaria in primary care Tidman MJ. Managing urticaria in primary care. Practitioner 2015;259(1779)25-28 Dr Michael J. Tidman MD FRCP (Ed) FRCP (Lond) Consultant Dermatologist, Department of
DOES URTICARIA RULE YOUR LIFE?
 DOES URTICARIA RULE YOUR LIFE? Helpline 01322 619898 www.allergyuk.org The content of this leaflet was written and developed by Allergy UK. This leaflet is kindly supported by an unrestricted grant from
DOES URTICARIA RULE YOUR LIFE? Helpline 01322 619898 www.allergyuk.org The content of this leaflet was written and developed by Allergy UK. This leaflet is kindly supported by an unrestricted grant from
CHRONIC URTICARIA; IT S MORE THAN JUST ANTIHISTAMINES!
 CHRONIC URTICARIA; IT S MORE THAN JUST ANTIHISTAMINES! Randy D. Danielsen, PhD, PA, DFAAPA Dean & Professor Arizona School of Health Sciences A.T. Still University Ûr tĭ-kâr ē-ә Urticaria is characterized
CHRONIC URTICARIA; IT S MORE THAN JUST ANTIHISTAMINES! Randy D. Danielsen, PhD, PA, DFAAPA Dean & Professor Arizona School of Health Sciences A.T. Still University Ûr tĭ-kâr ē-ә Urticaria is characterized
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Urticaria These podcasts are designed to give medical students an overview of key topics in pediatrics. The audio versions
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Urticaria These podcasts are designed to give medical students an overview of key topics in pediatrics. The audio versions
Allergic Emergencies and Anaphylaxis. George Porfiris MD, CCFP(EM),FCFP TEGH
,FCFP TEGH") Allergic Emergencies and Anaphylaxis George Porfiris MD, CCFP(EM),FCFP TEGH Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Allergic Emergencies and Anaphylaxis George Porfiris MD, CCFP(EM),FCFP TEGH Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Update on urticaria Associate Professor Rohan Ameratunga Adapted for New Zealand from GLORIA Module 12: Urticaria
 Update on urticaria Associate Professor Rohan Ameratunga Adapted for New Zealand from GLORIA Module 12: Urticaria an educational program of Following this presentation you should be able to: Distinguish
Update on urticaria Associate Professor Rohan Ameratunga Adapted for New Zealand from GLORIA Module 12: Urticaria an educational program of Following this presentation you should be able to: Distinguish
Department of Paediatrics Clinical Guideline URTICARIA GUIDELINE BACKGROUND
 Department of Paediatrics Clinical Guideline URTICARIA GUIDELINE BACKGROUND This guideline is intended for use in A&E and general paediatric OPD to assist with the management of initial presentations of
Department of Paediatrics Clinical Guideline URTICARIA GUIDELINE BACKGROUND This guideline is intended for use in A&E and general paediatric OPD to assist with the management of initial presentations of
Urticaria. Appearance. Epidemiology [1] Aetiology [2]
![Urticaria. Appearance. Epidemiology [1] Aetiology [2]](/thumbs/72/67553487.jpg "Urticaria. Appearance. Epidemiology [1] Aetiology [2]") Page 1 of 5 View this article online at: patient.info/doctor/urticaria-pro Urticaria Urticaria, otherwise known as hives, is an itchy red blotchy rash resulting from swelling of the superficial part of
Page 1 of 5 View this article online at: patient.info/doctor/urticaria-pro Urticaria Urticaria, otherwise known as hives, is an itchy red blotchy rash resulting from swelling of the superficial part of
What s new (and old!) in food allergy. Adelle R. Atkinson, MD, FRCPC Sea Courses May/June 2017
 in food allergy. Adelle R. Atkinson, MD, FRCPC Sea Courses May/June 2017") What s new (and old!) in food allergy Adelle R. Atkinson, MD, FRCPC Sea Courses May/June 2017 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied,
What s new (and old!) in food allergy Adelle R. Atkinson, MD, FRCPC Sea Courses May/June 2017 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied,
FIT Board Review Corner April 2017
 FIT Board Review Corner April 2017 Welcome to the FIT Board Review Corner, prepared by Tammy Peng, MD, and Amar Dixit, MD, senior and junior representatives of ACAAI's Fellows-In-Training (FITs) to the
FIT Board Review Corner April 2017 Welcome to the FIT Board Review Corner, prepared by Tammy Peng, MD, and Amar Dixit, MD, senior and junior representatives of ACAAI's Fellows-In-Training (FITs) to the
Xolair. Xolair (omalizumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.45.02 Subject: Xolair Page: 1 of 6 Last Review Date: March 18, 2016 Xolair Description Xolair (omalizumab)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.45.02 Subject: Xolair Page: 1 of 6 Last Review Date: March 18, 2016 Xolair Description Xolair (omalizumab)
Xolair. Xolair (omalizumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.45.02 Subject: Xolair Page: 1 of 7 Last Review Date: September 15, 2016 Xolair Description Xolair (omalizumab)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.45.02 Subject: Xolair Page: 1 of 7 Last Review Date: September 15, 2016 Xolair Description Xolair (omalizumab)
COMMISSIONING POLICY RECOMMENDATION TREATMENT ADVISORY GROUP Policy agreed by North Lincolnshire CCG November 2012
 Drug, Treatment, Device name Omalizumab (Xolair; Novartis) COMMISSIONING POLICY RECOMMENDATION TREATMENT ADVISORY GROUP Policy agreed by North Lincolnshire CCG November 2012 Licensed indication Omalizumab
Drug, Treatment, Device name Omalizumab (Xolair; Novartis) COMMISSIONING POLICY RECOMMENDATION TREATMENT ADVISORY GROUP Policy agreed by North Lincolnshire CCG November 2012 Licensed indication Omalizumab
Mast Cell Mediators. Updates on Chronic Urticaria 11/1/2016. Urticaria: What happens in the skin?
 Urticaria: What happens in the skin? Updates on Chronic Urticaria Kent Woo, MD (USA) Allergy/Immunology Internal Medicine C A U S E MC, mast cell IgE Fc eri MC Release of Mediators Activation Vasodilation
Urticaria: What happens in the skin? Updates on Chronic Urticaria Kent Woo, MD (USA) Allergy/Immunology Internal Medicine C A U S E MC, mast cell IgE Fc eri MC Release of Mediators Activation Vasodilation
Skin prick testing: Guidelines for GPs
 INDEX Summary Offered testing but where Allergens precautions are taken Skin prick testing Other concerns Caution Skin testing is not useful in these following conditions When skin testing is uninterpretable
INDEX Summary Offered testing but where Allergens precautions are taken Skin prick testing Other concerns Caution Skin testing is not useful in these following conditions When skin testing is uninterpretable
Allergic Disorders. Allergic Disorders. IgE-dependent Release of Inflammatory Mediators. TH1/TH2 Paradigm
 Allergic Disorders Anne-Marie Irani, MD Virginia Commonwealth University Allergic Disorders IgE-mediated immune reactions Clinical entities include: asthma allergic rhinitis atopic dermatitis urticaria
Allergic Disorders Anne-Marie Irani, MD Virginia Commonwealth University Allergic Disorders IgE-mediated immune reactions Clinical entities include: asthma allergic rhinitis atopic dermatitis urticaria
Allergic Disorders. Allergic Disorders. IgE-dependent Release of Inflammatory Mediators. TH1/TH2 Paradigm
 Allergic Disorders Anne-Marie Irani, MD Virginia Commonwealth University Allergic Disorders IgE-mediated immune reactions Clinical entities include: asthma allergic rhinitis atopic dermatitis urticaria
Allergic Disorders Anne-Marie Irani, MD Virginia Commonwealth University Allergic Disorders IgE-mediated immune reactions Clinical entities include: asthma allergic rhinitis atopic dermatitis urticaria
REFERRAL GUIDELINES - SUMMARY
 Clinical Immunology & Allergy Unit LEEDS TEACHING HOSPITALS NHS TRUST REFERRAL GUIDELINES - SUMMARY THESE GUIDELINES ARE DESIGNED TO ENSURE THAT PATIENTS REQUIRING SECONDARY CARE ARE SEEN EFFICIENTLY AND
Clinical Immunology & Allergy Unit LEEDS TEACHING HOSPITALS NHS TRUST REFERRAL GUIDELINES - SUMMARY THESE GUIDELINES ARE DESIGNED TO ENSURE THAT PATIENTS REQUIRING SECONDARY CARE ARE SEEN EFFICIENTLY AND
By the end of this lecture physicians will:
 No disclosure By the end of this lecture physicians will: 1. Be able to identify patients who need immune work-up. 2. Be able to recognize the manifestation of food allergies. 3. Be knowledgeable about
No disclosure By the end of this lecture physicians will: 1. Be able to identify patients who need immune work-up. 2. Be able to recognize the manifestation of food allergies. 3. Be knowledgeable about
Itch and Swelling update: Practical Approach to Urticaria & Angioedema
 Itch and Swelling update: Practical Approach to Urticaria & Angioedema Robert W Hostoffer, DO, LhD, FAAP, FACOP, FACOI, FCCP Program Director, Allergy/Immunology Fellowship Neha Sanan, DO Allergy & Immunology
Itch and Swelling update: Practical Approach to Urticaria & Angioedema Robert W Hostoffer, DO, LhD, FAAP, FACOP, FACOI, FCCP Program Director, Allergy/Immunology Fellowship Neha Sanan, DO Allergy & Immunology
Chapter 65 Allergy and Immunology for the Internist. ingestion provoke an IgE antibody response and clinical symptoms in sensitive individuals.
 Chapter 65 Allergy and Immunology for the Internist 1 I. Basic Information A. Definition of Allergens: Proteins of appropriate size that after inhalation, injection (e.g. drug, venom) or ingestion provoke
Chapter 65 Allergy and Immunology for the Internist 1 I. Basic Information A. Definition of Allergens: Proteins of appropriate size that after inhalation, injection (e.g. drug, venom) or ingestion provoke
Immunologic Mechanisms of Tissue Damage. (Immuopathology)
") Immunologic Mechanisms of Tissue Damage (Immuopathology) Immunopathology Exaggerated immune response may lead to different forms of tissue damage 1) An overactive immune response: produce more damage than
Immunologic Mechanisms of Tissue Damage (Immuopathology) Immunopathology Exaggerated immune response may lead to different forms of tissue damage 1) An overactive immune response: produce more damage than
Allergy Glossary of Terms
 Adrenaline (Epinephrine) Allergy Glossary of Terms Adrenaline is a natural hormone released in response to stress. When injected, adrenaline rapidly reverses the effects of a severe allergic reaction (anaphylaxis)
Adrenaline (Epinephrine) Allergy Glossary of Terms Adrenaline is a natural hormone released in response to stress. When injected, adrenaline rapidly reverses the effects of a severe allergic reaction (anaphylaxis)
Glossary of Terms ASCIA EDUCATION RESOURCES (AER) PATIENT INFORMATION
 PATIENT INFORMATION") Glossary of Terms Allergen A substance which can cause an allergic reaction. Allergen Immunotherapy A series of injections (shots) or sublingual drops are administered which contain the allergen such as
Glossary of Terms Allergen A substance which can cause an allergic reaction. Allergen Immunotherapy A series of injections (shots) or sublingual drops are administered which contain the allergen such as
Allergy Medicine James MacLean, M.D.
 Allergy Medicine 2018 James MacLean, M.D. Conflict of Interest Disclosures James A MacLean, MD FACAAI, FAAAAI None Objectives Identify the major causes of acute and chronic urticaria and angioedema Review
Allergy Medicine 2018 James MacLean, M.D. Conflict of Interest Disclosures James A MacLean, MD FACAAI, FAAAAI None Objectives Identify the major causes of acute and chronic urticaria and angioedema Review
Allergy Medicine James MacLean, M.D.
 Allergy Medicine 2019 James MacLean, M.D. Conflict of Interest Disclosures James A MacLean, MD FACAAI, FAAAAI None Objectives Identify the major causes of acute and chronic urticaria and angioedema Review
Allergy Medicine 2019 James MacLean, M.D. Conflict of Interest Disclosures James A MacLean, MD FACAAI, FAAAAI None Objectives Identify the major causes of acute and chronic urticaria and angioedema Review
Persia Pourshahnazari MD, FRCPC Clinical Immunology and Allergy November 3, 2018
 Persia Pourshahnazari MD, FRCPC Clinical Immunology and Allergy November 3, 2018 UBC couldn t get rid of me Medical school, Internal Medicine residency, Clinical Immunology and Allergy fellowship Current
Persia Pourshahnazari MD, FRCPC Clinical Immunology and Allergy November 3, 2018 UBC couldn t get rid of me Medical school, Internal Medicine residency, Clinical Immunology and Allergy fellowship Current
Perspectives in Primary Care: Evaluating and Managing Patients With Chronic Urticaria
 Perspectives in Primary Care: Evaluating and Managing Patients With Chronic Urticaria Please complete the preassessment located in your meeting handout before the program begins. Sponsorship and Support
Perspectives in Primary Care: Evaluating and Managing Patients With Chronic Urticaria Please complete the preassessment located in your meeting handout before the program begins. Sponsorship and Support
Allergic Conditions in Sports. Seth Smith, MD, CAQ-SM, PharmD TPC Course February 7, 2016
 Allergic Conditions in Sports Seth Smith, MD, CAQ-SM, PharmD TPC Course February 7, 2016 Goals and Objectives Describe diagnosis and management of exercise-induced bronchospasm/bronchoconstriction (EIB)
Allergic Conditions in Sports Seth Smith, MD, CAQ-SM, PharmD TPC Course February 7, 2016 Goals and Objectives Describe diagnosis and management of exercise-induced bronchospasm/bronchoconstriction (EIB)
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Xolair (omalizumab) Page 1 of 15 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Xolair (omalizumab) Prime Therapeutics will review Prior Authorization requests.
Xolair (omalizumab) Page 1 of 15 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Xolair (omalizumab) Prime Therapeutics will review Prior Authorization requests.
Do My Patient s Hives Always = Allergy? Julie Sterbank, DO Allergy & Immunology MetroHealth Medical Center
 Do My Patient s Hives Always = Allergy? Julie Sterbank, DO Allergy & Immunology MetroHealth Medical Center I do not have any financial or conflicts of interest to make regarding any of the items or conditions
Do My Patient s Hives Always = Allergy? Julie Sterbank, DO Allergy & Immunology MetroHealth Medical Center I do not have any financial or conflicts of interest to make regarding any of the items or conditions
EPIPEN INSERVICE Emergency Administration of Epinephrine for the Basic EMT. Michael J. Calice MD, FACEP St. Mary Mercy Hospital
 EPIPEN INSERVICE Emergency Administration of Epinephrine for the Basic EMT Michael J. Calice MD, FACEP St. Mary Mercy Hospital Case #1 NR is an 8 yo male c/o hot mouth and stomach ache after eating jelly
EPIPEN INSERVICE Emergency Administration of Epinephrine for the Basic EMT Michael J. Calice MD, FACEP St. Mary Mercy Hospital Case #1 NR is an 8 yo male c/o hot mouth and stomach ache after eating jelly
MANAGING COMMON PRESENTATIONS OF ALLERGY IN PRIMARY CARE. Helen Bourne Consultant Immunologist
 MANAGING COMMON PRESENTATIONS OF ALLERGY IN PRIMARY CARE Helen Bourne Consultant Immunologist AIMS Presentation of Allergic Disease in Adults Rhinitis/ Rhinoconjuctivitis Urticaria and Angioedema Food
MANAGING COMMON PRESENTATIONS OF ALLERGY IN PRIMARY CARE Helen Bourne Consultant Immunologist AIMS Presentation of Allergic Disease in Adults Rhinitis/ Rhinoconjuctivitis Urticaria and Angioedema Food
Allergy Skin Prick Testing
 Allergy Skin Prick Testing What is allergy? The term allergy is often applied erroneously to a variety of symptoms induced by exposure to a wide range of environmental or ingested agents. True allergy
Allergy Skin Prick Testing What is allergy? The term allergy is often applied erroneously to a variety of symptoms induced by exposure to a wide range of environmental or ingested agents. True allergy
Angioedema. Disclosures. Question #1. Objectives. Question #3. Question #2 12/28/2015. Differentiate the various angioedema subtypes
 None Disclosures Jason Knuffman, M.D. Allergy and Clinical Immunology Quincy Medical Group Unity Point Health System Quincy, IL Objectives Question #1 Differentiate the various angioedema subtypes Identify
None Disclosures Jason Knuffman, M.D. Allergy and Clinical Immunology Quincy Medical Group Unity Point Health System Quincy, IL Objectives Question #1 Differentiate the various angioedema subtypes Identify
Coverage Criteria: Express Scripts, Inc. monograph dated 03/03/2010
 BENEFIT DESCRIPTION AND LIMITATIONS OF COVERAGE ITEM: PRODUCT LINES: COVERED UNDER: DESCRIPTION: CPT/HCPCS Code: Company Supplying: Setting: Xolair (omalizumab) Commercial HMO/PPO/CDHP HMO/PPO/CDHP: Rx
BENEFIT DESCRIPTION AND LIMITATIONS OF COVERAGE ITEM: PRODUCT LINES: COVERED UNDER: DESCRIPTION: CPT/HCPCS Code: Company Supplying: Setting: Xolair (omalizumab) Commercial HMO/PPO/CDHP HMO/PPO/CDHP: Rx
Lesson 17: Allergies & Anaphylaxis. Emergency Reference Guide p
 Lesson 17: Allergies & Anaphylaxis Emergency Reference Guide p. 25-30 Objectives Describe basics of allergic reactions & treatment Define anaphylaxis List signs & symptoms of anaphylaxis Describe conditions
Lesson 17: Allergies & Anaphylaxis Emergency Reference Guide p. 25-30 Objectives Describe basics of allergic reactions & treatment Define anaphylaxis List signs & symptoms of anaphylaxis Describe conditions
Hypersensitivity Reactions and Peanut Component Testing 4/17/ Mayo Foundation for Medical Education and Research. All rights reserved.
 1 Hello everyone. My name is Melissa Snyder, and I am the director of the Antibody Immunology Lab at the Mayo Clinic in Rochester, MN. I m so glad you are able to join me for a brief discussion about the
1 Hello everyone. My name is Melissa Snyder, and I am the director of the Antibody Immunology Lab at the Mayo Clinic in Rochester, MN. I m so glad you are able to join me for a brief discussion about the
Urticaria is a common, heterogeneous group of disorders
 SYMPOSIUM REPORT SUPPLEMENT A Summary of the New International EAACI/GA 2 LEN/EDF/ WAO Guidelines in Torsten Zuberbier, MD Abstract: is a heterogeneous group of disorders, especially acute and angiooedema
SYMPOSIUM REPORT SUPPLEMENT A Summary of the New International EAACI/GA 2 LEN/EDF/ WAO Guidelines in Torsten Zuberbier, MD Abstract: is a heterogeneous group of disorders, especially acute and angiooedema
Urticaria and Angioedema
 Urticaria and Angioedema This guideline, developed by Robbie Pesek, MD and Allison Burbank, MD, in collaboration with the ANGELS team, on July 23, 2013, is a significantly revised version of the guideline
Urticaria and Angioedema This guideline, developed by Robbie Pesek, MD and Allison Burbank, MD, in collaboration with the ANGELS team, on July 23, 2013, is a significantly revised version of the guideline
ALLERGY TESTING AND TREATMENT
 Status Active Medical and Behavioral Health Policy Section: Laboratory Policy Number: VI-02 Effective Date: 03/26/2014 Blue Cross and Blue Shield of Minnesota medical policies do not imply that members
Status Active Medical and Behavioral Health Policy Section: Laboratory Policy Number: VI-02 Effective Date: 03/26/2014 Blue Cross and Blue Shield of Minnesota medical policies do not imply that members
Shelley Westwood, RN, BSN
 Shelley Westwood, RN, BSN The body requires a constant supply of oxygen for survival. AMERICAN RED CROSS FIRST AID RESPONDING TO EMERGENCIES FOURTH EDITION Copyright 2006 by The American National Red Cross
Shelley Westwood, RN, BSN The body requires a constant supply of oxygen for survival. AMERICAN RED CROSS FIRST AID RESPONDING TO EMERGENCIES FOURTH EDITION Copyright 2006 by The American National Red Cross
While many people believe they may be allergic
 Focus on CME at the xxx University of Toronto The Truth Behind Allergies Peter Vadas, MD, PhD, FRCPC, FACP To be presented at the University of Toronto, Therapeutic Update, CME for Primary Care Today 2003,
Focus on CME at the xxx University of Toronto The Truth Behind Allergies Peter Vadas, MD, PhD, FRCPC, FACP To be presented at the University of Toronto, Therapeutic Update, CME for Primary Care Today 2003,
Path2220 INTRODUCTION TO HUMAN DISEASE ALLERGY. Dr. Erika Bosio
 Path2220 INTRODUCTION TO HUMAN DISEASE ALLERGY Dr. Erika Bosio Research Fellow Centre for Clinical Research in Emergency Medicine, Harry Perkins Institute of Medical Research University of Western Australia
Path2220 INTRODUCTION TO HUMAN DISEASE ALLERGY Dr. Erika Bosio Research Fellow Centre for Clinical Research in Emergency Medicine, Harry Perkins Institute of Medical Research University of Western Australia
알레르기질환관련 진단적검사의이해 분당서울대병원알레르기내과 김세훈
 알레르기질환관련 진단적검사의이해 2009. 8. 30. 분당서울대병원알레르기내과 김세훈 What is allergy? Von Pirquet(1906): Greek allos (altered) + ergos (response) Exposure to foreign antigen (allergen) beneficial Harmful altered response
알레르기질환관련 진단적검사의이해 2009. 8. 30. 분당서울대병원알레르기내과 김세훈 What is allergy? Von Pirquet(1906): Greek allos (altered) + ergos (response) Exposure to foreign antigen (allergen) beneficial Harmful altered response
KDIGO Conference San Francisco March KDIGO. Mechanisms of drug hypersensitivity. A. J. Bircher Dermatology/Allergology
 Conference San Francisco March 27 30 2014 Mechanisms of drug hypersensitivity A. J. Bircher Dermatology/Allergology University Hospital Basel Switzerland andreas.bircher@unibas.ch Disclosure of Interests
Conference San Francisco March 27 30 2014 Mechanisms of drug hypersensitivity A. J. Bircher Dermatology/Allergology University Hospital Basel Switzerland andreas.bircher@unibas.ch Disclosure of Interests
Is it allergy? Debbie Shipley
 Is it allergy? Debbie Shipley Topics Food Allergy and Eczema Hand Eczema and Patch Testing Urticaria Tackling Allergy Gell and Coombs classification Skin conditions with possible allergic component Allergy
Is it allergy? Debbie Shipley Topics Food Allergy and Eczema Hand Eczema and Patch Testing Urticaria Tackling Allergy Gell and Coombs classification Skin conditions with possible allergic component Allergy
Autologous Serum Skin Test in Chronic Idiopathic Urticaria: Prevalence, Correlation and Clinical Implications
 ASIAN PACIFIC JOURNAL OF ALLERGY AND IMMUNOLOGY (2006) 24: 201-206 Autologous Serum Skin Test in Chronic Idiopathic Urticaria: Prevalence, Correlation and Clinical Implications Kanokvalai Kulthanan, Sukhum
ASIAN PACIFIC JOURNAL OF ALLERGY AND IMMUNOLOGY (2006) 24: 201-206 Autologous Serum Skin Test in Chronic Idiopathic Urticaria: Prevalence, Correlation and Clinical Implications Kanokvalai Kulthanan, Sukhum
Immunology 2011 Lecture 23 Immediate Hypersensitivity 26 October
 Immunology 2011 Lecture 23 Immediate Hypersensitivity 26 October Allergic Reactions ( Immediate Hypersensitivity ) Hay fever, food, drug & animal allergies, reactions to bee stings, etc. Symptoms may include
Immunology 2011 Lecture 23 Immediate Hypersensitivity 26 October Allergic Reactions ( Immediate Hypersensitivity ) Hay fever, food, drug & animal allergies, reactions to bee stings, etc. Symptoms may include
Ailléirge Péidiatraiceach. Pediatric Allergy 3/9/2018. Disclosures & Conflicts Of Interest
 Ailléirge Péidiatraiceach Michael Zacharisen, M.D. Allergy/Immunology Pediatric Allergy Michael Zacharisen, M.D. Allergy/Immunology Disclosures & Conflicts Of Interest Green Bay Packer fan I drive a Jeep
Ailléirge Péidiatraiceach Michael Zacharisen, M.D. Allergy/Immunology Pediatric Allergy Michael Zacharisen, M.D. Allergy/Immunology Disclosures & Conflicts Of Interest Green Bay Packer fan I drive a Jeep
IMMUNOLOGY. Referral Guidelines NATIONAL REFERRAL GUIDELINES : IMMUNOLOGY. As above Specialist assessment is essential.
 PAGE 1 IMMUNOLOGY National PRIMARY IMMUNODEFICIENCY Primary immunodeficiency should be suspected in any patient with recurrent or persistent infection or unusual infection. Recurrent sinopulmonary infections
PAGE 1 IMMUNOLOGY National PRIMARY IMMUNODEFICIENCY Primary immunodeficiency should be suspected in any patient with recurrent or persistent infection or unusual infection. Recurrent sinopulmonary infections
Allergy & Urticaria. James MacLean, M.D.
 Allergy & Urticaria James MacLean, M.D. Conflict of Interest Disclosures James A MacLean, MD FACAAI, FAAAAI None Objectives Upon completion of this lecture the participant should be able to: Identify the
Allergy & Urticaria James MacLean, M.D. Conflict of Interest Disclosures James A MacLean, MD FACAAI, FAAAAI None Objectives Upon completion of this lecture the participant should be able to: Identify the
Hypersensitivity diseases
 Hypersensitivity diseases Downloaded from: StudentConsult (on 18 July 2006 11:40 AM) 2005 Elsevier Type-I Hypersensitivity Basic terms Type-I = Early= IgE-mediated = Atopic = Anaphylactic type of hypersensitivity
Hypersensitivity diseases Downloaded from: StudentConsult (on 18 July 2006 11:40 AM) 2005 Elsevier Type-I Hypersensitivity Basic terms Type-I = Early= IgE-mediated = Atopic = Anaphylactic type of hypersensitivity
OBJECTIVES DEFINITION TYPE I HYPERSENSITIVITY TYPES OF HYPERSENSITIVITY ACUTE ALLERGIC REACTION 11/5/2016
 OBJECTIVES ACUTE ALLERGIC REACTION Wei Zhao, MD, PhD Ambulatory Medical Director Children s Hospital of Richmond at VCU Associate Professor, Chief Chief, Division of Allergy and Immunology Virginia Commonwealth
OBJECTIVES ACUTE ALLERGIC REACTION Wei Zhao, MD, PhD Ambulatory Medical Director Children s Hospital of Richmond at VCU Associate Professor, Chief Chief, Division of Allergy and Immunology Virginia Commonwealth
Clinico - etiological study of chronic Urticaria and the role of autologous serum skin test in the diagnosis of chronic idiopathic Urticaria
 Original Article Clinico etiological study of chronic Urticaria and the role of autologous serum skin test in the diagnosis of chronic idiopathic Urticaria Swetha D, M Bhagya Rekha, S Srikanth, B.S.N.Reddy
Original Article Clinico etiological study of chronic Urticaria and the role of autologous serum skin test in the diagnosis of chronic idiopathic Urticaria Swetha D, M Bhagya Rekha, S Srikanth, B.S.N.Reddy
7/25/2016. Use of Epinephrine in the Community. Knowledge Amongst Paramedics. Knowledge Amongst Paramedics survey of 3479 paramedics
 Recognition & Management of Anaphylaxis in the Community S. Shahzad Mustafa, MD, FAAAAI Disclosures Speaker s bureau Genentech, Teva Consultant Genentech, Teva Outline Knowledge gap Definition Pathophysiology
Recognition & Management of Anaphylaxis in the Community S. Shahzad Mustafa, MD, FAAAAI Disclosures Speaker s bureau Genentech, Teva Consultant Genentech, Teva Outline Knowledge gap Definition Pathophysiology
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Xolair (omalizumab) Page 1 of 15 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Xolair (omalizumab) Prime Therapeutics will review Prior Authorization requests.
Xolair (omalizumab) Page 1 of 15 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Xolair (omalizumab) Prime Therapeutics will review Prior Authorization requests.
Scope of Practice Allergy Skin Testing in Australia In relation to revised Medicare Benefits Schedule item numbers effective 1 November 2018
 Scope of Practice Allergy Skin Testing in Australia In relation to revised Medicare Benefits Schedule item numbers effective 1 November 2018 A. Introduction The Australasian Society of Clinical Immunology
Scope of Practice Allergy Skin Testing in Australia In relation to revised Medicare Benefits Schedule item numbers effective 1 November 2018 A. Introduction The Australasian Society of Clinical Immunology
Immunology 2011 Lecture 23 Immediate Hypersensitivity 26 October
 Immunology 2011 Lecture 23 Immediate Hypersensitivity 26 October Allergic Reactions ( Immediate Hypersensitivity ) Hay fever, food, drug & animal allergies, reactions to bee stings, etc. Symptoms may include
Immunology 2011 Lecture 23 Immediate Hypersensitivity 26 October Allergic Reactions ( Immediate Hypersensitivity ) Hay fever, food, drug & animal allergies, reactions to bee stings, etc. Symptoms may include
INVESTIGATIONS & PROCEDURES IN PULMONOLOGY. Immunotherapy in Asthma Dr. Zia Hashim
 INVESTIGATIONS & PROCEDURES IN PULMONOLOGY Immunotherapy in Asthma Dr. Zia Hashim Definition Involves Administration of gradually increasing quantities of specific allergens to patients with IgE-mediated
INVESTIGATIONS & PROCEDURES IN PULMONOLOGY Immunotherapy in Asthma Dr. Zia Hashim Definition Involves Administration of gradually increasing quantities of specific allergens to patients with IgE-mediated
The management of chronic urticaria in primary care for adults and children
 The management of chronic urticaria in primary care for adults and children September Version 2.0 This supersedes version 1.0 Review due in September 2019 Document location DOCUMENT CONTROL Copies of this
The management of chronic urticaria in primary care for adults and children September Version 2.0 This supersedes version 1.0 Review due in September 2019 Document location DOCUMENT CONTROL Copies of this
Immunology. Lecture- 8
 Immunology Lecture- 8 Immunological Disorders Immunodeficiency Autoimmune Disease Hypersensitivities Immunodeficiency 1. Immunodeficiency --> abnormal production or function of immune cells, phagocytes,
Immunology Lecture- 8 Immunological Disorders Immunodeficiency Autoimmune Disease Hypersensitivities Immunodeficiency 1. Immunodeficiency --> abnormal production or function of immune cells, phagocytes,
Allergy/Immunology Marshall University Pediatrics
 Allergy/Immunology Marshall University Pediatrics Description: This is a clinical rotation about the most common chronic diseases affecting both children and adults. Residents will be introduced to allergy,
Allergy/Immunology Marshall University Pediatrics Description: This is a clinical rotation about the most common chronic diseases affecting both children and adults. Residents will be introduced to allergy,
Itchy, Scratchy, Red and Patchy: Derm tips for primary care. Robert Gniadecki, MD
 Itchy, Scratchy, Red and Patchy: Derm tips for primary care Robert Gniadecki, MD Faculty/Presenter Disclosure Faculty: Robert Gniadecki Relationships with financial sponsors: Grants/Research Support: N/A
Itchy, Scratchy, Red and Patchy: Derm tips for primary care Robert Gniadecki, MD Faculty/Presenter Disclosure Faculty: Robert Gniadecki Relationships with financial sponsors: Grants/Research Support: N/A
Tetsuji WAKUDA, Masanao SHIBASAKI,Tadashi TANITSU* National University Corporation, Tsukuba University of Technology *Cooperation with research
 NTUT Education of Disabilities, 2009 Vol. 7 Effects of Acupuncture on Control of Pruritus Associated with Atopic Dermatitis Course in Acupuncture and Moxibustion, Department of Health, Tsukuba University
NTUT Education of Disabilities, 2009 Vol. 7 Effects of Acupuncture on Control of Pruritus Associated with Atopic Dermatitis Course in Acupuncture and Moxibustion, Department of Health, Tsukuba University
The proposal is to add text/statements in red and to delete text/statements with strikethrough: POLICY
 Omalizumab DESCRIPTION Omalizumab is a recombinant DNA-derived humanized IgG1κ monoclonal antibody which selectively binds to immunoglobulin E (IgE). High serum levels of IgE are found in individuals with
Omalizumab DESCRIPTION Omalizumab is a recombinant DNA-derived humanized IgG1κ monoclonal antibody which selectively binds to immunoglobulin E (IgE). High serum levels of IgE are found in individuals with
HYPERSENSITIVITY REACTIONS D R S H O AI B R AZ A
 HYPERSENSITIVITY REACTIONS D R S H O AI B R AZ A HYPERSENSITIVITY REACTIONS Are exaggerated immune response upon antigenic stimulation Individuals who have been previously exposed to an antigen are said
HYPERSENSITIVITY REACTIONS D R S H O AI B R AZ A HYPERSENSITIVITY REACTIONS Are exaggerated immune response upon antigenic stimulation Individuals who have been previously exposed to an antigen are said
How to Successfully Manage Chronic Urticaria? & Tall Tales from Texas
 How to Successfully Manage Chronic Urticaria? & Tall Tales from Texas David A. Khan, MD Professor of Medicine and Pediatrics Allergy & Immunology Program Director 1 Disclosures Honoraria/Speakers Bureau
How to Successfully Manage Chronic Urticaria? & Tall Tales from Texas David A. Khan, MD Professor of Medicine and Pediatrics Allergy & Immunology Program Director 1 Disclosures Honoraria/Speakers Bureau
Anaphylaxis: The Atypical Varieties
 Anaphylaxis: The Atypical Varieties John Johnson, D.O., PGY-4 Allergy/Immunology Fellow University Hospitals of Cleveland Case Western Reserve University School of Medicine Disclosures: None What is Anaphylaxis?
Anaphylaxis: The Atypical Varieties John Johnson, D.O., PGY-4 Allergy/Immunology Fellow University Hospitals of Cleveland Case Western Reserve University School of Medicine Disclosures: None What is Anaphylaxis?
Food Allergies. (Demkin). That is approximately two million kids. That number only represents children, but
. That is approximately two million kids. That number only represents children, but") McCurry!1 Bailey McCurry Kennon Biology I Honors 1 May 2018 Food Allergies Food allergies are becoming more common in today s society. More people have allergies than you might think. Research says that
McCurry!1 Bailey McCurry Kennon Biology I Honors 1 May 2018 Food Allergies Food allergies are becoming more common in today s society. More people have allergies than you might think. Research says that
Allergic disorders in Mauritius with. stress on urticaria - angioedema
 Allergic disorders in Mauritius with stress on urticaria - angioedema Mauritius Climate Tropical maritime 20 S 58E Summer Hot, humid November- April Winter Cool, humid May October South Easterly winds
Allergic disorders in Mauritius with stress on urticaria - angioedema Mauritius Climate Tropical maritime 20 S 58E Summer Hot, humid November- April Winter Cool, humid May October South Easterly winds
Recognition & Management of Anaphylaxis in the Community. S. Shahzad Mustafa, MD, FAAAAI
 Recognition & Management of Anaphylaxis in the Community S. Shahzad Mustafa, MD, FAAAAI Disclosures None Outline Define anaphylaxis Pathophysiology Common causes Recognition and Management Definition Acute,
Recognition & Management of Anaphylaxis in the Community S. Shahzad Mustafa, MD, FAAAAI Disclosures None Outline Define anaphylaxis Pathophysiology Common causes Recognition and Management Definition Acute,
Perspectives in Primary Care: Evaluating and Managing Patients with Chronic Urticaria
 Saturday General Session Perspectives in Primary Care: Evaluating and Managing Patients with Chronic Urticaria Anne Marie Ditto, MD Associate Professor of Medicine Division of Allergy Immunology Northwestern
Saturday General Session Perspectives in Primary Care: Evaluating and Managing Patients with Chronic Urticaria Anne Marie Ditto, MD Associate Professor of Medicine Division of Allergy Immunology Northwestern
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: xolair_omalizumab 9/2003 11/2017 11/2018 11/2017 Description of Procedure or Service Asthma is a chronic
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: xolair_omalizumab 9/2003 11/2017 11/2018 11/2017 Description of Procedure or Service Asthma is a chronic
From now on we are going to deal with the clinical aspects of hypersensitivity reactions:
 In the name of Allah Hypersensitivity reactions Basic Immunology Introduction: The main role of the immune system is to discriminate between self & non self antigens. Although the immune system is supposed
In the name of Allah Hypersensitivity reactions Basic Immunology Introduction: The main role of the immune system is to discriminate between self & non self antigens. Although the immune system is supposed
Allergy overview. Mike Levin Division of Asthma and Allergy Department of Paediatrics University of Cape Town Red Cross Hospital
 Allergy overview Mike Levin Division of Asthma and Allergy Department of Paediatrics University of Cape Town Red Cross Hospital Adaptive Immune Responses Adaptive immune responses allow responses against
Allergy overview Mike Levin Division of Asthma and Allergy Department of Paediatrics University of Cape Town Red Cross Hospital Adaptive Immune Responses Adaptive immune responses allow responses against
INTERNATIONAL JOURNAL OF PHARMACEUTICAL RESEARCH AND BIO-SCIENCE
 Gajbhiye S,, 2014; Volume 3(4): 686-694 INTERNATIONAL JOURNAL OF PHARMACEUTICAL RESEARCH AND BIO-SCIENCE CHOLINERGIC URTICARIA: A REVIEW FROM PATHOPHYSIOLOGY, SYMPTOMS, SUBTYPES, DIAGNOSIS TO TREATMENT
Gajbhiye S,, 2014; Volume 3(4): 686-694 INTERNATIONAL JOURNAL OF PHARMACEUTICAL RESEARCH AND BIO-SCIENCE CHOLINERGIC URTICARIA: A REVIEW FROM PATHOPHYSIOLOGY, SYMPTOMS, SUBTYPES, DIAGNOSIS TO TREATMENT
contact activation in formation diseases 67 endothelial cells and kinin formation 73 processing and degradation 68 70
 Subject Index Adenosine, mast cell activation modulation 60 Age, risk factor 17, 18 Allergen elicitors 9, 10 insects, see Insect venom-induced microarrays for 136 overview of characteristics 23 recognition
Subject Index Adenosine, mast cell activation modulation 60 Age, risk factor 17, 18 Allergen elicitors 9, 10 insects, see Insect venom-induced microarrays for 136 overview of characteristics 23 recognition
Eczema: also called atopic dermatitis; a chronic, itchy, scaly rash not due to a particular substance exposure
 Allergy is a condition in which the immune system causes sneezing, itching, rashes, and wheezing, or sometimes even life-threatening allergic reactions. The more you know about allergies, the better prepared
Allergy is a condition in which the immune system causes sneezing, itching, rashes, and wheezing, or sometimes even life-threatening allergic reactions. The more you know about allergies, the better prepared
Myth: Prior Episodes Predict Future Reactions REALITY: No predictable pattern Severity depends on: Sensitivity of the individual Dose of the allergen
 Myth: Prior Episodes Predict Future Reactions REALITY: No predictable pattern Severity depends on: Sensitivity of the individual Dose of the allergen Anaphylaxis Fatalities Estimated 500 1000 deaths annually
Myth: Prior Episodes Predict Future Reactions REALITY: No predictable pattern Severity depends on: Sensitivity of the individual Dose of the allergen Anaphylaxis Fatalities Estimated 500 1000 deaths annually
VACCINE-RELATED ALLERGIC REACTIONS
 VACCINE-RELATED ALLERGIC REACTIONS Management of Anaphylaxis IERHA Immunization Program September 2016 VACCINE-RELATED ADVERSE EVENTS Local reactions pain, edema, erythema Systemic reactions fever, lymphadenopathy
VACCINE-RELATED ALLERGIC REACTIONS Management of Anaphylaxis IERHA Immunization Program September 2016 VACCINE-RELATED ADVERSE EVENTS Local reactions pain, edema, erythema Systemic reactions fever, lymphadenopathy
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Single Technology Appraisal (STA)
") Thank you for agreeing to give us a statement on your organisation s view of the technology and the way it should be used in the NHS. Healthcare professionals can provide a unique perspective on the technology
Thank you for agreeing to give us a statement on your organisation s view of the technology and the way it should be used in the NHS. Healthcare professionals can provide a unique perspective on the technology
Five things to know about anaphylaxis
 Five things to know about anaphylaxis Magdalena Berger, MD FRCPC Allergist and Clinical Immunologist New Brunswick Internal Medicine Update April 22, 2016 Disclosures None relevant to this presentation
Five things to know about anaphylaxis Magdalena Berger, MD FRCPC Allergist and Clinical Immunologist New Brunswick Internal Medicine Update April 22, 2016 Disclosures None relevant to this presentation
xx Xolair 150 MG SOLR (GENENTECH)
") Omalizumab NDC CODE(S) 50242-0040-xx Xolair 150 MG SOLR (GENENTECH) DESCRIPTION Omalizumab is a recombinant DNA-derived humanized IgG1κ monoclonal antibody which selectively binds to immunoglobulin E (IgE).
Omalizumab NDC CODE(S) 50242-0040-xx Xolair 150 MG SOLR (GENENTECH) DESCRIPTION Omalizumab is a recombinant DNA-derived humanized IgG1κ monoclonal antibody which selectively binds to immunoglobulin E (IgE).
Idiopathic Anaphylaxis. Paul A. Greenberger, MD, FAAAAI 2/28/2014 Course # 1605
 Idiopathic Anaphylaxis Paul A. Greenberger, MD, FAAAAI 2/28/2014 Course # 1605 Objectives Review definition and classification of idiopathic anaphylaxis Consider the differential diagnosis Critique lab
Idiopathic Anaphylaxis Paul A. Greenberger, MD, FAAAAI 2/28/2014 Course # 1605 Objectives Review definition and classification of idiopathic anaphylaxis Consider the differential diagnosis Critique lab
Seasonal Allergic Rhinoconjunctivitis
 Seasonal Allergic Rhinoconjunctivitis Allergic rhinoconjunctivitis is a common condition. Most patients can achieve good symptom control through allergen avoidance and pharmacotherapy with non-sedating
Seasonal Allergic Rhinoconjunctivitis Allergic rhinoconjunctivitis is a common condition. Most patients can achieve good symptom control through allergen avoidance and pharmacotherapy with non-sedating
Allergy Management Policy
 Allergy Management Policy Food Allergy People with allergies have over-reactive immune systems that target otherwise harmless elements of our diet and environment. During an allergic reaction to food,
Allergy Management Policy Food Allergy People with allergies have over-reactive immune systems that target otherwise harmless elements of our diet and environment. During an allergic reaction to food,
Allergy Medications. Antihistamines. are very safe. Although usually taken as tablets, they may be prescribed as a liquid or syrup for young children
 The treatments prescribed for allergy control the symptoms and reactions; they do not cure the condition. However, using treatments as prescribed can show a huge change in a patient s health, mood and
The treatments prescribed for allergy control the symptoms and reactions; they do not cure the condition. However, using treatments as prescribed can show a huge change in a patient s health, mood and
2012/12/5. Principle of the management of urticaria. The efficacy of systemic steroid on urticaria depends of subtypes urticaria
 6 December 2012: 13:3015:00 G.04 (HICC) The Hyderabad International Convention Centre (HICC) in Hyderabad, India WISC 2012; WAO International Scientific Conference Postgraduate Course 16: URTICARIA & ANGIOEDEMA
6 December 2012: 13:3015:00 G.04 (HICC) The Hyderabad International Convention Centre (HICC) in Hyderabad, India WISC 2012; WAO International Scientific Conference Postgraduate Course 16: URTICARIA & ANGIOEDEMA
IMMUNOTHERAPY IN ALLERGIC RHINITIS
 Rhinology research Chair Weekly Activity, King Saud University IMMUNOTHERAPY IN ALLERGIC RHINITIS E V I D E N C E D - B A S E O V E R V I E W O F T H E R U L E O F I M M U N O T H E R A P Y I N A L L E
Rhinology research Chair Weekly Activity, King Saud University IMMUNOTHERAPY IN ALLERGIC RHINITIS E V I D E N C E D - B A S E O V E R V I E W O F T H E R U L E O F I M M U N O T H E R A P Y I N A L L E
Anaphylaxis: Treatment in the Community
 : Treatment in the Community is likely if a patient who, within minutes of exposure to a trigger (allergen), develops a sudden illness with rapidly progressing skin changes and life-threatening airway
: Treatment in the Community is likely if a patient who, within minutes of exposure to a trigger (allergen), develops a sudden illness with rapidly progressing skin changes and life-threatening airway
URTICARIA DIAGNOSIS. *Tadech Boonpiyathad, Wat Mitthamsiri, Panitan Pradubpongsa, Atik Sangasapaviliya
 URTICARIA DIAGNOSIS *Tadech Boonpiyathad, Wat Mitthamsiri, Panitan Pradubpongsa, Atik Sangasapaviliya Division of Allergy and Clinical Immunology, Department of Medicine, Phramongkutklao Hospital, Bangkok,
URTICARIA DIAGNOSIS *Tadech Boonpiyathad, Wat Mitthamsiri, Panitan Pradubpongsa, Atik Sangasapaviliya Division of Allergy and Clinical Immunology, Department of Medicine, Phramongkutklao Hospital, Bangkok,
Acute and Chronic Urticaria, Including New Treatment Options
 Acute and Chronic Urticaria, Including New Treatment Options Charles V. Klucka, D.O. Florida Osteopathic Medical Association, District XI October 19, 2018 Disclosures I have no relevant financial relationships
Acute and Chronic Urticaria, Including New Treatment Options Charles V. Klucka, D.O. Florida Osteopathic Medical Association, District XI October 19, 2018 Disclosures I have no relevant financial relationships
Clinical and Experimental Allergy
 doi: 10.1111/j.1365-2222.2007.02678.x Clinical and Experimental Allergy, 37, 631 650 Journal compilation c 2007 Blackwell Publishing Ltd SPECIAL ARTICLE BSACI guidelines for the management of chronic urticaria
doi: 10.1111/j.1365-2222.2007.02678.x Clinical and Experimental Allergy, 37, 631 650 Journal compilation c 2007 Blackwell Publishing Ltd SPECIAL ARTICLE BSACI guidelines for the management of chronic urticaria
EPI PEN TRAINING KAREN, RN, BSN FARGO SOUTH SCHOOL NURSE
 EPI PEN TRAINING KAREN, RN, BSN FARGO SOUTH SCHOOL NURSE Why use an Epipen? Anaphylaxis Anaphylaxis is a severe, potentially lifethreatening allergic reaction caused by contact with certain triggers CAUSES
EPI PEN TRAINING KAREN, RN, BSN FARGO SOUTH SCHOOL NURSE Why use an Epipen? Anaphylaxis Anaphylaxis is a severe, potentially lifethreatening allergic reaction caused by contact with certain triggers CAUSES
Foundations in Microbiology Seventh Edition
 Lecture PowerPoint to accompany Foundations in Microbiology Seventh Edition Talaro Chapter 16 To run the animations you must be in Slideshow View. Use the buttons on the animation to play, pause, and turn
Lecture PowerPoint to accompany Foundations in Microbiology Seventh Edition Talaro Chapter 16 To run the animations you must be in Slideshow View. Use the buttons on the animation to play, pause, and turn
4/12/18. Refractory Chronic Urticaria: When Omalizumab Fails. Objectives. Disclosures
 Refractory Chronic Urticaria: When Omalizumab Fails David A. Khan, MD Professor of Medicine and Pediatrics Allergy & Immunology Program Director 1 Disclosures n Research Grants n NIH n Honoraria n UpToDate,
Refractory Chronic Urticaria: When Omalizumab Fails David A. Khan, MD Professor of Medicine and Pediatrics Allergy & Immunology Program Director 1 Disclosures n Research Grants n NIH n Honoraria n UpToDate,
Systemic Allergic & Immunoglobulin Disorders
 Systemic Allergic & Immunoglobulin Disorders Bryan L. Martin, DO, MMAS, FACAAI, FAAAAI, FACP, FACOI Emeritus Professor of Medicine and Pediatrics President, American College of Allergy, Asthma & Immunology
Systemic Allergic & Immunoglobulin Disorders Bryan L. Martin, DO, MMAS, FACAAI, FAAAAI, FACP, FACOI Emeritus Professor of Medicine and Pediatrics President, American College of Allergy, Asthma & Immunology