Introduction to. AcuColors. Karen Johnson, RN, MPH, Naturopath, CCP
|
|
|
- Alfred Wilson
- 5 years ago
- Views:
Transcription
1
2 Introduction to AcuColors Karen Johnson, RN, MPH, Naturopath, CCP

3 DISCLAIMER AcuColors does not provide medical advice, diagnosis or treatment. Content from AcuColors is not intended to be used for medical diagnosis or treatment. The information provided in this book is intended for general consumer understanding and self-improvement only. The information provided is not intended to be a substitute for professional medical advice. As health and nutrition research continuously evolves, we do not guarantee the accuracy, completeness, or timeliness of any information presented in this book.

4 AcuColors An Overview of Acucolors: Colored Light Healing on the Acupuncture points Learning Objectives: 1. Discover an alternative way of healing with Acucolors. 2. Master basic TCM Diagnostic methods to pinpoint meridian imbalances. 3. Learn how to apply colored light on the acupoints to heal the Body-Soul-Spirit levels. 4. Work through at least one health issue using the 3 Acucolors treatment techniques for whole holistic healing.

5 WHAT IS ACUCOLORS? A self-improvement health care program Incorporates many concepts from Traditional Chinese Medicine Addresses the whole person in Body, Soul and Spirit Uses colored light to heal and restore function on the cellular level of the body.

6 ACUCOLORS CAN ADDRESS: ADHD Anxiety Addictions Allergies Autoimmune issues BP & Heart Rate Concentration & Learning Childhood or Prenatal Trauma Digestion issues Detoxification Depression Emotional Issues Energy Blockages Fatigue Fever HA/Migraines Hormonal issues Pain Control Sinus Issues Skin problems Sleep problems Stress Weight control

7 ACUCOLORS ADDRESSES: the WHOLE Person in Body-Soul-Spirit Physical Body: The major focus of Western Medicine the Body is the physical vector which carries the Soul and the Spirit in this world. It needs nutrition and exercise to remain healthy and functional. It is subject to harm from accident or illness. (USE REGULATORY TREATMENTS.) Emotional Soul: The Soul is the psychological reflector of our emotions in an aura around the outside of the body. It supports our instinctive drive, and can act as mediator in bringing balance between the worldliness of the body and Godliness of the spirit. (USE SPECIFIC A-Z TREATMENTS.) Mind Spirit: The Spirit is our rational, intellectual director. It is our beliefs and our standards by which we interpret situations. The spirit mind can take control of the body matter. (REALIGN MERIDIAN PATHWAYS.)

8 The Meridians The Spirit, the information director, is located at the center of the meridian network of the body Meridians are energy pathways that carry vital information from the Spirit to the Soul and Body. The Yin meridians are paired with their opposing Yang pathways and become 5 main paired meridians, each having their own emotion and physical disease tendencies.
9 FIVE PAIRED MERIDIAN PATHWAYS SPIRITUAL MERIDIAN NETWORK (REALIGN MERIDIAN PATHWAYS.) MAIN SOUL EMOTION (USE SPECIFIC A-Z TREATMENTS.) PHYSICAL DISEASE TENDENCIES OF THE BODY (USE REGULATORY TREATMENTS.) Liver/Gall Bladder Lv/GB Stomach/Spleen St/Sp Kidney/Bladder Ki/Bl Lung/Large Intestine Lu/LI Heart/Small Intestine x/si Anger Worry Fear Sadness Love Allergies, Anxiety, Aphasia, Chronic Fatigue, Convulsions, Dizziness, Eye & Ear issues, Fever, Gallstones, Hip pain, Hypertension, Leg arthritis, Meningitis, Migraines, Mood disorders, Muscle Atrophy, Nausea, Numbness, PMS, Rib pain, Sciatica, Shoulder pain, Stroke, Tinnitus, Weakness Anemia, Anorexia, Diabetes, Food Poisoning, GERD, Glaucoma, Hives, IBS. Dyspepsia, Indigestion, Joint & Bone pain, Knee pain, Menstrual cramps, Muscle Spasms, Nausea, PMS, Smell or Taste issues, Sty, Toothache, Ulcers, Urinary Tract infections Anorexia, Arthritis, Bladder infections, Edema, Epilepsy, Fatigue, Foot pain, Hearing & Speech issues. Hiccups, IBS, Impotence, Joint pain, Knee, Leg, Low Back Pain, Low Libido, Muscle spasms, Osteoporosis, Premature Graying, Prostatitis, Rapid Pulse, Reproductive issues. Hereditary weaknesses, Respiratory ailments, Sciatica, Sexual dysfunction, Systemic diseases, Tinnitus. Urinary disorders, Vertigo Acne, Allergies. Asthma. Bell s Palsy, Bronchitis, Cold symptoms, Congestion, Cough, Cough. IBS, Crohn s, Depression, Diarrhea, Dry Skin, Eczema, Elbow pain, Fatigue, Flu, Immune deficiencies, Itching, Learning disorders, Nasal Obstruction, Sinus infection, Sneezing, Sore throat, Stress, Toothache, Ulcerative Colitis, Upper Back pain, Anemia, Blood Pressure/Heart rate & rhythm, Celiac disease, Chronic Cough; Shoulder & Neck pain. Sore Throat, Fatigue, Insomnia, Mouth sores, Mumps, Neuralgia, Nightmares. Fever, Numbness in fingers, Poor Circulation in arms & legs, Poor Memory, Sweating, Swollen Glands, TMJ syndrome.

10 WHY DO WE NEED ACUCOLORS? Emotions are part of our soul being. Normally, we express an emotion and immediately release it. What happens if we repress a negative emotion because we don t want to show it? The repressed emotion becomes trapped, blocking energy flow through the meridian channels of the body. When energy is blocked for extended periods of time, physical damage can occur at the cellular level of the body. AcuColors releases trapped emotions and opens up the blocked meridians allowing positive light energy to heal the cells of the body.


11 HEALING EFFECTS OF LIGHT ENERGY Dr. Fritz Albert Popp, Biophysicist found we emit biophotons 1974 which can be seen with Kirlian/Russian GDV camera: "We know today that man is essentially a being of light. And the modern science of photobiology... is presently proving this. In terms of healing... the implications are immense. We now know, for example, that... light can initiate, or arrest, cascade-like reactions in the cells, and that genetic cellular damage can be virtually repaired, within hours, by faint beams of light. We are still on the threshold of fully understanding the complex relationship between light and life, but we can now say, emphatically that the function of our entire metabolism is dependent on light.

12 Diagnostic Kirlian Photography Example Report From GDV camera.

13 GDV Chakra Report Shutting Down Overstressed
 5-4-3-2-1; Right Hand (RH) 1-2-3-4-5. 3. Check for Imbalance side to side.")
14 Fingertip Testing 1. Press firmly in the middle of the last digit of each finger, just under the round fingertip pad. Sharp pain that makes you want to yell OUCH! is a positive response. 2. Follow the testing in this order: Left Hand (LH) ; Right Hand (RH) Check for Imbalance side to side. If sore fingers are not the same on LH or RH, then there is a Laterality imbalance and need Corpus Callosum treatment. 4. When there is a T o F difference top to bottom, such as hot hands and cold feet, then there is a Polarity issue and a Vertical treatment is needed. BODY SYSTEM SENSITIVE FINGER(S) REGULATING FUNCTION FINGER CHART BY BODY SYSTEM Lymphatic Lv GB RH & LH Thumb(1 st ) Immune support & eliminate toxins thru lymphatic system. Nervous Sp St RH & LH Index (2 nd ) Transfer info between nerves & muscles for movement Musc Skel Ki Bl RH & LH Middle (3 rd ) Transfer info between nerves & muscles for movement Endocrine Lu LI RH & LH Ring (4 th ) Gland & Hormone Regulation Blood Ht SI RH & LH Little (5 th ) Circulation of oxygenated blood to the vital cells & organs PROBLEM Congestion Degeneration Degeneration Dysregulation Stagnation




15 HORIZONTAL & VERTICAL BALANCING Horizontal Treatment LOCATION: Corpus Callosum point, mid nose & upper lip. 20 sec on point INDICATION: Balances Side to Side. COLOR: Yellow Vertical Treatment LOCATION: Hypothalamus points in line with the pupils midway between hairline & eyebrows. Also GV2 at top of buttocks fold. 20 sec each point INDICATION: Balances Top to Bottom. COLOR:L=Orange; R=Blue: GV2=Or.ange
















16 TONGUE INSPECTION COLOR NORMAL: pink, flexible with a think clear coat & moisture VIOLET: (LvGB:Anger) venous stagnation, slow blood circulation, poor oxygenation RED: (KiBl:Fear) fever, vitamin deficiency, dehydration; the more red the more inflammation or acidity. This causes Stomach and Kidney damage. PALE (LuLI:Sadness) = Blood deficiency, Low BP, hypothyroid, metabolic deficiency leading to cold hands & feet, dehydration. REGION Dehydration GERD
 Blue indicates a weak heart. Blue-green shows a fungal infection. (HtSI) Red excess RBCs. If in nailbed, it confirms a heart problem.")
 b.")
17 NAILBED INSPECTION COLOR Yellow shows LvGB from impaired Lymph Drainage. Yellow, Green or Black can also mean a bacterial infection. Yellow with Pink base = Diabetes (SpSt) Blue indicates a weak heart. Blue-green shows a fungal infection. (HtSI) Red excess RBCs. If in nailbed, it confirms a heart problem. (HtSI) White could mean liver disease. ½ White ½ Pink = Kidney disease. Pale nailbed = Anemia (KiBl) ABNORMALITIES a. Longitudinal Ridges = FA deficiency, poor absorption of food, aging, kidney disorder, infection, arthritis (KiBl) b. Clubbing = depletion of O2 in blood, COPD, Celiac disease, IBS (LuLI) c. White spots = weak immune system d. Onychomycosis = systemic fungal e. Spoon nails = blood iron disorders

 1.Neurogenic fibers- CNS weak 2.Lymphatic Congestion mucous 3.Hematochromia-- LvGB Pancreas issues 4.")
-- GI, GB issues; Pancreatic Blood Sugar issues; Diarrhea, Constipation, Flatulence (SpSt) 1.")
18 EYES Hematogenic (Brown eye)-- Glandular, Lymphatic congestion (LvGB) 1.Chronic Stress Rings -fibers buckle 2.Radii Solaris -toxic waste dump 3.Cholesterol Ring= too much cholesterol in blood. Lymphatic (Blue eye)-- Allergies, Overactive immune system; Colds, Sinus, Respiratory infections, GI disorders; Arthritis, Adrenal, Kidney & Thyroid problems (LuLI) 1.Neurogenic fibers- CNS weak 2.Lymphatic Congestion mucous 3.Hematochromia-- LvGB Pancreas issues 4.Scurf Rim-dark ring around outside of iris=skin circulation issues. Use dry skin brushing to increase circulation. Biliary ( Green Mixed Blue with Brown eye)-- GI, GB issues; Pancreatic Blood Sugar issues; Diarrhea, Constipation, Flatulence (SpSt) 1.Polyglandular endocrine 2.Lymphatic Rosary-congestion 3.Uric acid-=gout 4.Ballooning in Nerve Wreath- excess gas, hiatal hernia

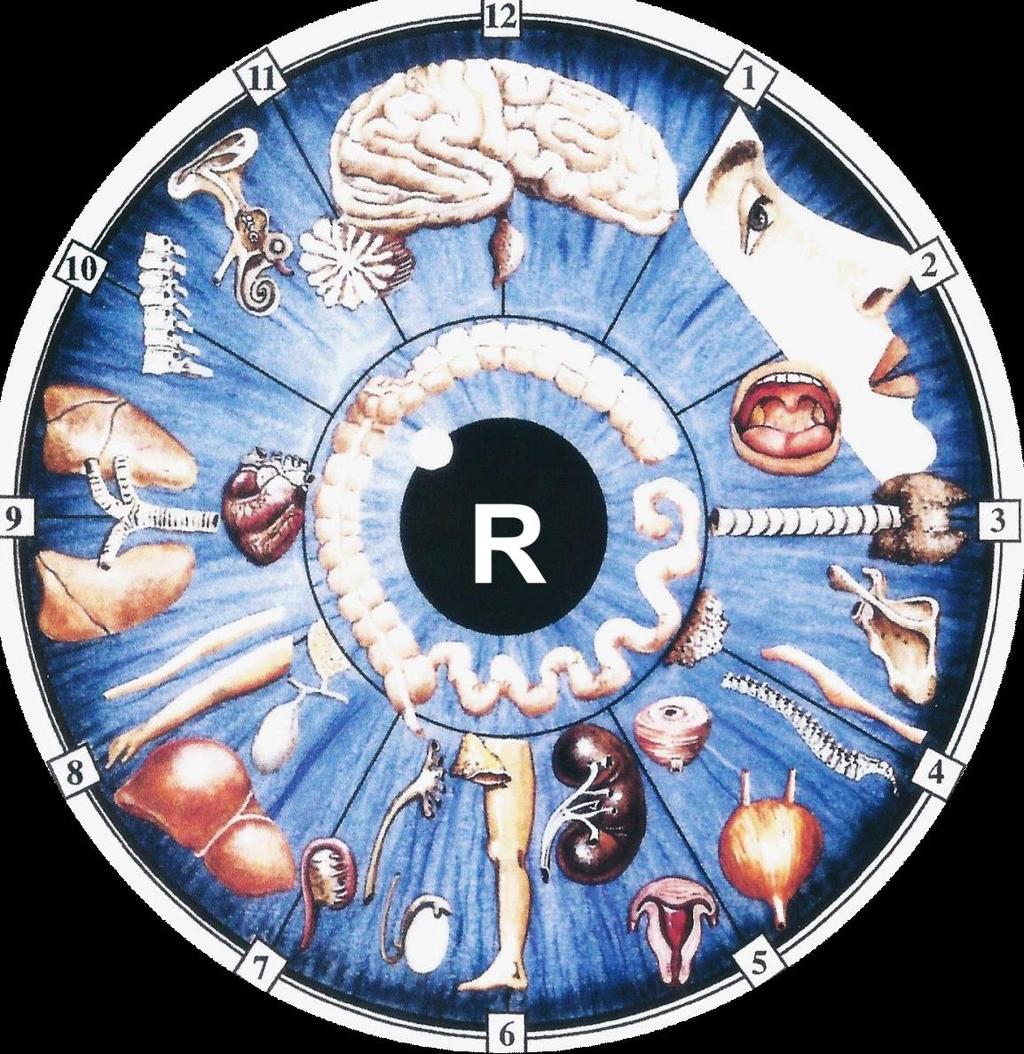
19 I RIDOLOGY P HOTOS R
. 2. EYE -inner corners Adenoids swollen, brown=chronic constipation, breast issues. Ki 3. NOSE - Red or swellings =Lu ; Red Nose tip=thyroid 4.")
20 FACE INSPECTION OBSERVE FOR CHANGES IN: Color darkened areas, pigment changes Shape --asymmetry Skin wrinkles, swelling Meridian Zones any changes over meridian areas 1. CHEEKBONE Swollen Blue-White color=diaphragm & CNS). 2. EYE -inner corners Adenoids swollen, brown=chronic constipation, breast issues. Ki 3. NOSE - Red or swellings =Lu ; Red Nose tip=thyroid 4. UPPER LIP -(heart fold) =Lighter & retractions are cardiac signs. 5. R LOWER LIP - swellings =Lv. 6. CENTER CHIN = pancreas. Pc includes genitals 7. L LOWER LIP =Sp. 8. LIPS = Narrow tight lips =mesenchymal issues. SI LI 9. CENTER UPPER LIP Acid folds of gas, bloating, metabolism- St 10. CENTER BROW Conflict Acid folds from stress & conflict. LvGB
 2. Treating specific health issues (A-Z) releases negative emotions in targeted organs. (Section 2) 3.")
21 Part II TREATMENTS Traditional Chinese Medicine (TCM) does not treat individual health conditions since they are only symptoms of greater energy imbalances in the body. 1. The Regulatory Treatments resynchronize the overall 5 paired meridian systems. (Section 1) 2. Treating specific health issues (A-Z) releases negative emotions in targeted organs. (Section 2) 3. Rebalancing the meridian systems cures the disease. (Section 3)


22 Sec 1: The Regulatory Treatments resynchronize the overall 5 paired meridian systems
23 Lymphatic THUMB (1st) FINGER Triple Triangles General Indications: For LvGB, Lymphatic issues, Acute Tonsillitis, Sinusitis, Appendicitis. To increase Lymphatic drainage & for detoxification. For any Chronic Lymphatic disease Hodgkin s Lymphoma, Lymphedema, Lymphocytosis, Heavy Metal Poisoning, Directions: Decide at which location you have the most tension, and treat that area regularly with the appropriate triangle below; otherwise, treat all 3 zones using the points on each triangle for an overall Detox treatment if you have multiple symptoms from each zone. Starting with #1 at the base of the neck, apply yellow to all 6 points for 20 seconds each. Triangle lines are only for visualization.
24 Nervous System Index (2nd) FINGER General Indications: Nervous System degenerative disorders such as Balance, Multiple Sclerosis (MS), Alzheimer s, Parkinson s, Epilepsy, and Stroke, Palsy or anything that affects memory and ability to perform daily activities. Directions: Starting with Blue # 1-7 for Nervous System Disorders (sore 2 nd Fingers). Apply appropriate colors for 20 seconds each.
25 Musculo Skeletal System Middle (3rd) FINGER General Indications: #3 Middle=Degenerative Disease of Bones & Muscles Arthritis, Fibromyalgia (FMS), Lupus (SLE), Myasthenia Gravis (MG), Osteoporosis, Sarcoma & Bone Cancer Directions: Starting with Red #1-5 for Musculoskeletal disorders (sore 3rd Fingers). Apply appropriate colors for 20 seconds each.
26 Endocrine RING (4TH) FINGER Chakra Balancing General Indications: For Endocrine disorders, such as Addison s, Adrenal Fatigue, Cushing s, Endometriosis, Diabetes, Graves, Hashimoto s Thyroiditis, PCOS (Polycystic Ovarian Syndrome). Directions: Starting at Root Chakra (Red), place appropriate color on each Chakra for 20 sec. During each light placement, think in your mind of a whirlwind spinning freely clockwise around that part of your body where the light is placed. The faster it spins the more balanced the chakra. The Chakras can spin either direction, but Clockwise tends to move outward and join other energy, while Counter Clockwise moves energy inward and tends to drain others energy. If one of the chakras will not move, try further meditation, visualizing with more intent a swirling motion. If there is still no movement, then suspect blockage(s). Look at the Gland and its Function in the chart above. If you know you already have issues with that gland, then this is further confirmation that you need to work with it to unblock the corresponding chakra. Each Chakra is linked to a gland. When you balance the chakra you help regulate the gland. Also, significant emotional trauma is imprinted in the Chakras; so when you balance the Chakras, you release negative emotions.
27 Blood/Immune Defense Little (5th) FINGER The Heart pumps vital nutrients throughout the whole body. The Small Intestine absorbs nutrients from ingested foods. These systems are dependent upon all the functions of the other 4 organ pairs Ex: If the Liver fuel filter, fails to sift out toxins, and the Lymphatic exhaust system backs up with waste, all of this pollution spills over into the blood causing toxic substances to be distributed all over the body in the form of RA, MS, Alzheimer s, etc. This is also your immune defense. So keep your engine running clean! General Indications To improve circulation & communication to all the body parts. For Heart diseases Hypertension, High Cholesterol, Enlarged Heart, Heart Attack, Palpitations. Congestive Heart Failure. For Lung Diseases COPD, Bronchitis, Asthma, Emphysema, Pneumonia, TB, Lung Cancer, Pulmonary Edema Directions: Place appropriate color on each point for 20 sec






28 Sec 2: A-Z Special Health Treatments Allergies, Skin RELEASE NEGATIVE EMOTIONS IN TARGETED ORGANS Depression GI Disorders Jaw Issues Constipation Ear Disorders Heatstroke Kidney Problems Fever Insomnia Liver GB Issues

29 SECTION 3: MERIDIAN BALANCING REBALANCING THE MERIDIAN SYSTEMS CURES THE DISEASE. Meridians are energy pathways that link the outside physical body to the inside spirit body. The meridians are closely linked to the nervous system and the nerve pathways that feed every organ and part of the body, yet they also control the flow of chi throughout the whole body-soul-spirit. When a meridian is out of balance, symptoms will show up. From 5 Paired Meridian Pathway table, MigHA are from LvGB imbalance. HOW TO BRING MERIDIANS INTO BALANCE: Meridian Tracing: The energy of the Meridian pairs runs in opposition or Yin and Yang. Normally, the opposing forces keep the meridian pairs balanced, but occasionally the acupoints along one of the meridian pathways become physically or emotionally blocked causing a drop in energy in that pathway, while the opposing compensates with too much. An example of this is when the Liver meridian becomes blocked by anger causing migraines. There is a drop in energy in the Liver meridian which needs to be stimulated using the warm color Yellow. The Gall Bladder meridian tries to compensate with too much energy and needs to be sedated using the cool color Violet.
30 LIVER-GALL BLADDER THUMBS Anger is a powerful emotion that may produce migraine HAs, eye problems, myopathy or tendinitis. Meridian Underactive Warm Color Overactive Cool Color Liver Yellow Violet Gall Bladder Yellow Violet
31 STOMACH-SPLEEN INDEXES Ever heard of the Worry-Wart that ends up with stomach ulcers? Meridian Underactive Warm Color Overactive Cool Color Stomach Orange Blue Spleen Orange Blue
32 KIDNEY-BLADDER MIDDLES Fear and anxiety are common in young children and can even be transferred from the parents to the unborn child while in the womb. Meridian Underactive Warm Color Overactive Cool Color Kidney Red Green Bladder Red Green An additional step, stroking 5 times on the Kidney/Bladder lines on the feet can clear unwanted antepartum emotions. 1. Kidney Line 5x 3 rd toe to heel on bottom of L&R foot Orange 2. Bladder Line 5x 5 th toe bunion to heel on side of L&R foot Yellow
33 LUNG-LARGE INTESTINE RINGS Grief or sorrow will settle in the lungs. Meridian Underactive Warm Color Lung Orange Blue Large Intestine Orange Overactive Cool Color Blue
34 HEART-SMALL INTESTINE LITTLES The Heart should be full of Unconditional Love. This meridian should never be out of balance. If it is, then the others are as well, since the other 4 meridian pairs protect the Ht/SI at all costs. Meridian Underactive Warm Color Overactive Cool Color Heart Rose Turquoise Small Rose Turquoise Intestine

35 When there is light in the soul there will be beauty in the person. When there is beauty in the person, there will be harmony in the house. When there is harmony in the house, there will be order in the nation. When there is order in the nation, there will be peace in the world. --Old Chinese Proverb

36 For Further Information: The website has a copy of this presentation and a link to my Amazon e-books.
By Karen E Johnson, RN, MPH, Naturopath
 By Karen E Johnson, RN, MPH, Naturopath DISCLAIMER AcuColors does not provide medical advice, diagnosis or treatment. Content from AcuColors is not intended to be used for medical diagnosis or treatment.
By Karen E Johnson, RN, MPH, Naturopath DISCLAIMER AcuColors does not provide medical advice, diagnosis or treatment. Content from AcuColors is not intended to be used for medical diagnosis or treatment.
Introduction THE PHYSICAL BODY
 Introduction THE PHYSICAL BODY Traditional Chinese Medicine (TCM) teaches us that the whole person includes 3 entities the Body, the Soul and the Spirit. When disease strikes, it affects all 3, not just
Introduction THE PHYSICAL BODY Traditional Chinese Medicine (TCM) teaches us that the whole person includes 3 entities the Body, the Soul and the Spirit. When disease strikes, it affects all 3, not just
AN INTRODUCTION TO. KAREN E JOHNSON, RN, MPH, CCP, NATUROPATH
 AN INTRODUCTION TO AcuColors KAREN E JOHNSON, RN, MPH, CCP, NATUROPATH WWW.ACUCOLORS.COM karen@acucolors.com Text copyright @ 2016 Karen E Johnson All rights reserved. Without limiting the rights under
AN INTRODUCTION TO AcuColors KAREN E JOHNSON, RN, MPH, CCP, NATUROPATH WWW.ACUCOLORS.COM karen@acucolors.com Text copyright @ 2016 Karen E Johnson All rights reserved. Without limiting the rights under
On a scale of 1 10 ("10" being optimal health) please rate where you feel your health is in the the areas below:
 please rate where you feel your health is in the the areas below:") Healthcare History djp Pure-Health wellness centre www.pure-health.com Wellness Profile General Health On a scale of 1 10 ("10" being optimal health) please rate where you feel your health is in the the
Healthcare History djp Pure-Health wellness centre www.pure-health.com Wellness Profile General Health On a scale of 1 10 ("10" being optimal health) please rate where you feel your health is in the the
What do you believe is causing your most important health concern?
 Intake form Name Today s Date Date of Birth Address City Phone Postal Code Email Primary Health Care Provider Emergency Contact Phone Note: By providing your email address you are giving us consent to
Intake form Name Today s Date Date of Birth Address City Phone Postal Code Email Primary Health Care Provider Emergency Contact Phone Note: By providing your email address you are giving us consent to
Inner Balance Acupuncture
 Patient Information Inner Balance Acupuncture 274 Southland Drive, Suite 101, Lexington, KY 40503 859-595-2164 www.acupunctureky.com Name: Today s date: Age: Male Female Marital status: Date of Birth:
Patient Information Inner Balance Acupuncture 274 Southland Drive, Suite 101, Lexington, KY 40503 859-595-2164 www.acupunctureky.com Name: Today s date: Age: Male Female Marital status: Date of Birth:
Medical History Form
 General: Medical History Form 1. Chief Complaint: What are the main health concerns you wish to address? 2. Current and Past Treatment: Have you received treatment for these problems? Yes No, if yes, which:
General: Medical History Form 1. Chief Complaint: What are the main health concerns you wish to address? 2. Current and Past Treatment: Have you received treatment for these problems? Yes No, if yes, which:
Patient Information. Marital Status (Single, Married, Life Partner, Divorced, Widowed) CHIEF COMPLAINT
 CHIEF COMPLAINT") Patient Information Name Date Home Address City State Zip Phone E-mail Address Cell Phone: Business Address City State Zip Phone Occupation Place of Birth Date of Birth Age Height Weight Soc. Sec. # Sex
Patient Information Name Date Home Address City State Zip Phone E-mail Address Cell Phone: Business Address City State Zip Phone Occupation Place of Birth Date of Birth Age Height Weight Soc. Sec. # Sex
Shiatsu Intake Form PURCHASED PRODUCT/SERVICE. Date of Birth Age Height Weight. Home Address City State ZIP
 Shiatsu Intake Form DATE PURCHASED PRODUCT/SERVICE FIRST NAME LAST NAME Date of Birth Age Height Weight Home Address City State ZIP Home Phone Cell Phone Email Name of Emergency Contact Would you like
Shiatsu Intake Form DATE PURCHASED PRODUCT/SERVICE FIRST NAME LAST NAME Date of Birth Age Height Weight Home Address City State ZIP Home Phone Cell Phone Email Name of Emergency Contact Would you like
Emotional Relationships Social Life Sexually Recreation
 Name Date Address City State Zip Married Single Partner Divorced Widowed Date of Birth SS# Email Work Phone Home Phone Cell Phone Occupation Referred by Emergency Contact Family Physician Contact May we
Name Date Address City State Zip Married Single Partner Divorced Widowed Date of Birth SS# Email Work Phone Home Phone Cell Phone Occupation Referred by Emergency Contact Family Physician Contact May we
Acupuncture Health History Page 1 of 5
 General Contact Information Acupuncture Health History Page 1 of 5 Name: Date of Birth: Address: City: Postal Code: Contact Numbers#: Home #: Email: (By checking you give David E. Chung Permission to email
General Contact Information Acupuncture Health History Page 1 of 5 Name: Date of Birth: Address: City: Postal Code: Contact Numbers#: Home #: Email: (By checking you give David E. Chung Permission to email
Patient Intake Form for Allegany Ear, Nose, & Throat
 Patient Intake Form for Allegany Ear, se, & Throat Patient Name: What brings you to the office today? Who is your primary care doctor? Please list your current medications: Are you allergic to any medications?
Patient Intake Form for Allegany Ear, se, & Throat Patient Name: What brings you to the office today? Who is your primary care doctor? Please list your current medications: Are you allergic to any medications?
Essential Wellness Of Illinois, LLC Health History Questionnaire Christine A. Renz L.Ac., Dipl OM, MSTOM
 Name Date Address City State Zip Home Phone Cell Fax Email Emergency Contact Emergency Number Date of Birth Age Sex Height Weight Lbs Marital Status Occupation Who referred you to this office? Name of
Name Date Address City State Zip Home Phone Cell Fax Email Emergency Contact Emergency Number Date of Birth Age Sex Height Weight Lbs Marital Status Occupation Who referred you to this office? Name of
Johanna M. Hoeller, DC PS
 ENTRANCE FORM Birth date: Height: Weight: Emergency Contact: Emergency Contact Phone: ( ) Spouse/Partner or Parent s name: Children s names: Occupation (Your): Employer: Address: City/State/Zip: Phone:
ENTRANCE FORM Birth date: Height: Weight: Emergency Contact: Emergency Contact Phone: ( ) Spouse/Partner or Parent s name: Children s names: Occupation (Your): Employer: Address: City/State/Zip: Phone:
Caspian Acupuncture -- Health History Form Anita Tayyebi EAMP, LAc. 652 SW 150 th St Burien WA 98166
 Frist Name Last: Date Phone (H) (C) (W) E-mail Address City State Zip Age DOB Place of Birth _ Marital/Partnership Status Preferred Gender Pronoun _ Profession Family Physician Telephone # Referred By
Frist Name Last: Date Phone (H) (C) (W) E-mail Address City State Zip Age DOB Place of Birth _ Marital/Partnership Status Preferred Gender Pronoun _ Profession Family Physician Telephone # Referred By
The Rehabilitation Institute Cancer Rehabilitation
 DO NOT DRILL The Rehabilitation Institute Cancer Rehabilitation STAR Patient Intake Form Your Name: Date: Your date of birth: Age: Who referred you (if a healthcare provider, please provide address)? Doctors
DO NOT DRILL The Rehabilitation Institute Cancer Rehabilitation STAR Patient Intake Form Your Name: Date: Your date of birth: Age: Who referred you (if a healthcare provider, please provide address)? Doctors
Metabolic Assessment Form
 Metabolic Assessment Form Approach Wellness and Aesthetics 200 Forsythe Street Fayetteville, NC 28303 Office: (910) 322-7368 Fax: (910) 483-5796 www.tawellness.net Name: Age: Sex: Date: Part 1: Please
Metabolic Assessment Form Approach Wellness and Aesthetics 200 Forsythe Street Fayetteville, NC 28303 Office: (910) 322-7368 Fax: (910) 483-5796 www.tawellness.net Name: Age: Sex: Date: Part 1: Please
Sound View Acupuncture and Chinese Herbs 5410 California Ave SW, #202, Seattle, WA
 Sound View Acupuncture and Chinese Herbs 5410 California Ave SW, #202, Seattle, WA 98136 206.200.3595 Today s date Name Legal name (if different) Phone (primary) (secondary) Address City State Zip Email
Sound View Acupuncture and Chinese Herbs 5410 California Ave SW, #202, Seattle, WA 98136 206.200.3595 Today s date Name Legal name (if different) Phone (primary) (secondary) Address City State Zip Email
BACK TO BASICS HEALTH & NUTRITION COMPREHENSIVE HEALTH HISTORY
 BACK TO BASICS HEALTH & NUTRITION COMPREHENSIVE HEALTH HISTORY Thank you for choosing Back To Basics Health & Nutrition to assist you with your natural health care. The ability to draw effective conclusions
BACK TO BASICS HEALTH & NUTRITION COMPREHENSIVE HEALTH HISTORY Thank you for choosing Back To Basics Health & Nutrition to assist you with your natural health care. The ability to draw effective conclusions
06/09/2005 Medical history and intake form
 Medical history and intake form Please complete this form as accurately as possible - it helps to provide you with the best possible treatment. Address including postcode Contact numbers Home/work/mobile
Medical history and intake form Please complete this form as accurately as possible - it helps to provide you with the best possible treatment. Address including postcode Contact numbers Home/work/mobile
New Patient Form. Patient Demographics. Emergency Information. Employment Information. Page 1 of 7. Family Health Chiropractic Care
 Page 1 of 7 Patient Demographics First Name* Last Name* Date Of Birth* Home Phone* Mobile Phone Phone Gender* Email Preferred Communication Street Address 1* Street Addresss 2 Zip* City* State* Emergency
Page 1 of 7 Patient Demographics First Name* Last Name* Date Of Birth* Home Phone* Mobile Phone Phone Gender* Email Preferred Communication Street Address 1* Street Addresss 2 Zip* City* State* Emergency
PATIENT INFORMATION FORM (WOMEN ONLY)
") PATIENT INFORMATION FORM (WOMEN ONLY) Name: Age: Sex: Birthdate: / / SS # A. Describe briefly your present symptom(s) or the reason(s) for seeing the doctor today: B. Name all illnesses or conditions for
PATIENT INFORMATION FORM (WOMEN ONLY) Name: Age: Sex: Birthdate: / / SS # A. Describe briefly your present symptom(s) or the reason(s) for seeing the doctor today: B. Name all illnesses or conditions for
PATIENT MEDICAL HISTORY INTAKE FORM
 Northgate Professional Center 1985 Main Street, Suite 209 Springfield, Massachusetts 01103 Tel; 413-455-1081 Fax; 413-391-7489 www.marimedconsults.com PATIENT MEDICAL HISTORY INTAKE FORM Patient Information:
Northgate Professional Center 1985 Main Street, Suite 209 Springfield, Massachusetts 01103 Tel; 413-455-1081 Fax; 413-391-7489 www.marimedconsults.com PATIENT MEDICAL HISTORY INTAKE FORM Patient Information:
Natalie Kilheeney L.Ac., Dipl. OM Licensed Acupuncturist & Herbalist
 *All information is important to your intake and valuable to your personal treatment plan. Please answer as thorough as possible. Patient Information: Name: Date: / / (First Middle Last) Address: City:
*All information is important to your intake and valuable to your personal treatment plan. Please answer as thorough as possible. Patient Information: Name: Date: / / (First Middle Last) Address: City:
Eastern Body Therapy
 2310 Eastern Body Therapy 6th Avenue San Diego, CA 92101 (619)772-4002 Personal Information Name Date of injury/illness Address: Apt. City State Zip Home phone: ( ) Work Phone: ( ) E-mail: Social Security
2310 Eastern Body Therapy 6th Avenue San Diego, CA 92101 (619)772-4002 Personal Information Name Date of injury/illness Address: Apt. City State Zip Home phone: ( ) Work Phone: ( ) E-mail: Social Security
Initial Consultation
 Today s Date: Initial Consultation Thank you for choosing Apollo Health and Wellness. Please take your time to fill out this form. It will help us to concentrate on areas of your health that need attention
Today s Date: Initial Consultation Thank you for choosing Apollo Health and Wellness. Please take your time to fill out this form. It will help us to concentrate on areas of your health that need attention
Nutrition Consultation Intake Form Please write or print clearly
 Artemis in the City, LLC Danielle Heard, MS, MS, HHC Clinical & Functional Nutritionist ph: 866-330-5421 fx: 212-535-3234 www.artemisinthecity.com Nutrition Consultation Intake Form Please write or print
Artemis in the City, LLC Danielle Heard, MS, MS, HHC Clinical & Functional Nutritionist ph: 866-330-5421 fx: 212-535-3234 www.artemisinthecity.com Nutrition Consultation Intake Form Please write or print
Facial Assessment. Color. Lines in the Skin.
 Facial Assessment Color. Red. Heat, inflammation, upward movement. White. Closure of capillaries, cold, shock, downward/inward movement. Blue. Lack of oxygen. Purple. Stagnation, bruises. Yellow. Liver,
Facial Assessment Color. Red. Heat, inflammation, upward movement. White. Closure of capillaries, cold, shock, downward/inward movement. Blue. Lack of oxygen. Purple. Stagnation, bruises. Yellow. Liver,
The Rehabilitation Institute Cancer Rehabilitation
 DO NOT DRILL The Rehabilitation Institute Cancer Rehabilitation Patient Intake Form Your Name: Date: Your date of birth: Age: Who referred you (if a healthcare provider, please provide address)? Doctors
DO NOT DRILL The Rehabilitation Institute Cancer Rehabilitation Patient Intake Form Your Name: Date: Your date of birth: Age: Who referred you (if a healthcare provider, please provide address)? Doctors
WELLNESS HISTORY. Patient s Name: Date
 u:\share\sr dr\wellness history1 08-08-13 1 WELLNESS HISTORY Patient s Name: Date 1) Have you ever been to Acupuncturist? Yes No If Yes: Currently In the past, When: Did it help? What treatment did you
u:\share\sr dr\wellness history1 08-08-13 1 WELLNESS HISTORY Patient s Name: Date 1) Have you ever been to Acupuncturist? Yes No If Yes: Currently In the past, When: Did it help? What treatment did you
Dr. Andrea Gri B.Kin, ND Doctor of Naturopathic Medicine Phone: Fax: Peter Robertson Blvd, Brampton ON L6R 1T4
 Dr. Andrea Gri B.Kin, ND Doctor of Naturopathic Medicine Phone: 905-793- 8868 Fax: 905-793- 8957 630 Peter Robertson Blvd, Brampton ON L6R 1T4 ADULT INTAKE FORM Name: (Last) (First) (Preferred Name) Address:
Dr. Andrea Gri B.Kin, ND Doctor of Naturopathic Medicine Phone: 905-793- 8868 Fax: 905-793- 8957 630 Peter Robertson Blvd, Brampton ON L6R 1T4 ADULT INTAKE FORM Name: (Last) (First) (Preferred Name) Address:
New Patient Medical History Intake Form
 New Patient Medical History Intake Form Name: Todays Date: / / Date of Birth: / / Age: Gender: M / F Marital Status: S M D W Address: City: State: Zip Code Primary Ph.# (cell, hm, wk) Email Address 2nd
New Patient Medical History Intake Form Name: Todays Date: / / Date of Birth: / / Age: Gender: M / F Marital Status: S M D W Address: City: State: Zip Code Primary Ph.# (cell, hm, wk) Email Address 2nd
ABUNDANT HEALTH CHIROPRACTIC New Patient Form PERSONAL INFORMATION. Name: Gender: M F Today's Date: / / Birth Date: / / Age: Social Security #: - -
 ABUNDANT HEALTH CHIROPRACTIC New Patient Form PERSONAL INFORMATION Name: Gender: M F Today's Date: / / Birth Date: / / Age: Social Security : - - Home Address: City, State, Zip: Home Phone: ( ) Work Phone:
ABUNDANT HEALTH CHIROPRACTIC New Patient Form PERSONAL INFORMATION Name: Gender: M F Today's Date: / / Birth Date: / / Age: Social Security : - - Home Address: City, State, Zip: Home Phone: ( ) Work Phone:
How much do you know about illnesses or health problems for your parents, grandparents, brothers, sisters, and/or children? 1 A lot Some None at all
 Family Health History Please answer each question as honestly as possible. There are no right or wrong answers to nay of the questions. It is important that you answer as many questions as you can. We
Family Health History Please answer each question as honestly as possible. There are no right or wrong answers to nay of the questions. It is important that you answer as many questions as you can. We
PATIENT HEALTH QUESTIONNAIRE Radiation Oncology
 REVIEWED DATE / INITIALS Safety: Yes No Are you at risk for falls? Do you have a Pacemaker? Females; Is there a possibility you may be pregnant? Allergies: Yes No If YES, please list medication allergies:
REVIEWED DATE / INITIALS Safety: Yes No Are you at risk for falls? Do you have a Pacemaker? Females; Is there a possibility you may be pregnant? Allergies: Yes No If YES, please list medication allergies:
NEW PATIENT HEALTH HISTORY
 NEW PATIENT HEALTH HISTORY Debra Joan Wood, Lic Ac, MAcOM Acupuncture and Herbs Please help me provide you with a complete evaluation by taking the time to fill out this questionnaire carefully. If there
NEW PATIENT HEALTH HISTORY Debra Joan Wood, Lic Ac, MAcOM Acupuncture and Herbs Please help me provide you with a complete evaluation by taking the time to fill out this questionnaire carefully. If there
Patient History Form
 Patient History Form Advanced Directive Care Plan? Yes No Name: Birth date: / / Address: Age: Sex: F M STREET DAY YEAR Telephone: Home ( ) CITY STATE DAY YEAR MARITAL STATUS: Divorced Separated Alive/Age
Patient History Form Advanced Directive Care Plan? Yes No Name: Birth date: / / Address: Age: Sex: F M STREET DAY YEAR Telephone: Home ( ) CITY STATE DAY YEAR MARITAL STATUS: Divorced Separated Alive/Age
Premium Specialty: Pediatrics
 Premium Specialty: Pediatrics Credentialed Specialties include: Adolescent Medicine, Pediatric Adolescent, and Pediatrics This document is designed to be used in conjunction with the UnitedHealth Premium
Premium Specialty: Pediatrics Credentialed Specialties include: Adolescent Medicine, Pediatric Adolescent, and Pediatrics This document is designed to be used in conjunction with the UnitedHealth Premium
ACUPUNCTURE INTAKE FORM
 , ND ACUPUNCTURE INTAKE FORM Thank you for taking the time to complete the following new patient forms. Given this form is extensive, it plays an integral role in achieving our mutual goal of your optimal
, ND ACUPUNCTURE INTAKE FORM Thank you for taking the time to complete the following new patient forms. Given this form is extensive, it plays an integral role in achieving our mutual goal of your optimal
Medical History Form
 Medical History Form NAME DOB / / TODAY S DATE MEDICAL HISTORY What medical Conditions do you have? Select all that apply, or write in if not listed: Diabetes High Blood Pressure Thyroid Disorder Heart
Medical History Form NAME DOB / / TODAY S DATE MEDICAL HISTORY What medical Conditions do you have? Select all that apply, or write in if not listed: Diabetes High Blood Pressure Thyroid Disorder Heart
RHEUMATOLOGY PATIENT HISTORY FORM
 !! RAMOS RHEUMATOLOGY, PC RHEUMATOLOGY PATIENT HISTORY FORM Date: / / NAME: Birthdate: / / Last First M. I. Age: Sex: F M Marital status: Never married Married Divorced Separated Widowed Partnered/significant
!! RAMOS RHEUMATOLOGY, PC RHEUMATOLOGY PATIENT HISTORY FORM Date: / / NAME: Birthdate: / / Last First M. I. Age: Sex: F M Marital status: Never married Married Divorced Separated Widowed Partnered/significant
Adult Health History Summary
 Adult Health History Summary Name Age Date of Birth Address City Province Postal Code Phone (home) (cell) Occupation Email May we contact you via email? YES NO Emergency Contact Phone # How did you hear
Adult Health History Summary Name Age Date of Birth Address City Province Postal Code Phone (home) (cell) Occupation Email May we contact you via email? YES NO Emergency Contact Phone # How did you hear
Alivia Acupuncture Clinic, LLC. Address. City State Zip. . Occupation Employer. Emergency contact Relationship. Primary Care provider Phone
 Alivia Acupuncture Clinic, LLC Karla Sourasky Olmos, L. Ac Patient Information Name Age Date of birth Address City State Zip Email Home Phone Work phone Cell Phone Marital Status Single Married Divorced
Alivia Acupuncture Clinic, LLC Karla Sourasky Olmos, L. Ac Patient Information Name Age Date of birth Address City State Zip Email Home Phone Work phone Cell Phone Marital Status Single Married Divorced
Medical Intake Form. Patient Name: Age : Date of Birth: Gender: Female Male Marital Status: #Children: Address: City: State: Zip:
 Date: Patient Name: Age : Date of Birth: Gender: Female Male Marital Status: #Children: Address: City: State: Zip: Home Phone: Cell Phone: Work Phone: E-mail: Person to Contact in Case of Emergency: Relationship
Date: Patient Name: Age : Date of Birth: Gender: Female Male Marital Status: #Children: Address: City: State: Zip: Home Phone: Cell Phone: Work Phone: E-mail: Person to Contact in Case of Emergency: Relationship
PATIENT HEALTH QUESTIONNAIRE Radiation Oncology
 REVIEWED DATE / INITIALS Safety: Are you at risk for falls? Do you have a Pacemaker? Females; Is there a possibility you may be pregnant? Allergies: If YES, please list medication allergies: Do you have
REVIEWED DATE / INITIALS Safety: Are you at risk for falls? Do you have a Pacemaker? Females; Is there a possibility you may be pregnant? Allergies: If YES, please list medication allergies: Do you have
LECOM Health Ophthalmology
 Patient Name: Date of Birth: New Patient Questionnaire Your answers will be used by your healthcare provider get an accurate history of your medical conditions and ocular concerns. If you are uncomfortable
Patient Name: Date of Birth: New Patient Questionnaire Your answers will be used by your healthcare provider get an accurate history of your medical conditions and ocular concerns. If you are uncomfortable
Carlette Zottola Lac, MSTOM Acupuncture New Patient Intake Form. Patient Information. Emergency Contact Information.
 Carlette Zottola Lac, MSTOM Acupuncture New Patient Intake Form Patient Information Name: Date of Birth: Age: Gender(please circle) M or F Occupation: Address: City, State, Zip: Email: Home Phone: Cell
Carlette Zottola Lac, MSTOM Acupuncture New Patient Intake Form Patient Information Name: Date of Birth: Age: Gender(please circle) M or F Occupation: Address: City, State, Zip: Email: Home Phone: Cell
New Patient Questionnaire. Name DOB Date
 Medical History (This refers to medical problems that have already been diagnosed or treated. Please explain how this is treated, such as diet, medication, surgery, etc.) Condition Abnormal Pap smear Alcohol
Medical History (This refers to medical problems that have already been diagnosed or treated. Please explain how this is treated, such as diet, medication, surgery, etc.) Condition Abnormal Pap smear Alcohol
Oriental Medicine Questionnaire
 Oriental Medicine Questionnaire Date: Name: DOB Sex: M F SS# Address: City State Zip Cell Phone: Home Phone: Business Phone Occupation: Height: Weight: Who referred you to this office? 1.What brought you
Oriental Medicine Questionnaire Date: Name: DOB Sex: M F SS# Address: City State Zip Cell Phone: Home Phone: Business Phone Occupation: Height: Weight: Who referred you to this office? 1.What brought you
Please fill out the following form in as much detail as possible. Please Print. Name. Address. City State Zip. Home Phone Office Phone.
 CASE NO. Please fill out the following form in as much detail as possible. Please Print Date Name Address City State Zip Home Phone Office Phone E-mail Address Age Date of Birth Occupation Sex (M) (F)
CASE NO. Please fill out the following form in as much detail as possible. Please Print Date Name Address City State Zip Home Phone Office Phone E-mail Address Age Date of Birth Occupation Sex (M) (F)
New Patient Packet. Patient Name: DOB: Age: Address: City: State: Zip: Address: City: State: Zip: Name: Address: Phone: Fax:
 New Patient Packet Patient Name: DOB: Age: Sex: Male / Female Height: Weight: PHYSICIAN CARE Primary Care Physician: Address: City: State: Zip: Phone: Fax: Referring Physician (if different from PCP):
New Patient Packet Patient Name: DOB: Age: Sex: Male / Female Height: Weight: PHYSICIAN CARE Primary Care Physician: Address: City: State: Zip: Phone: Fax: Referring Physician (if different from PCP):
Laser Vein Center Thomas Wright MD Page 1 of 4
 Demographics Laser Vein Center Thomas Wright MD Page 1 of 4 Patient Name: Address: City, St, Zip Primary Phone: Alternate: DOB: Social Security #: Insurance Information Primary Insurance ID# Group# Subscriber
Demographics Laser Vein Center Thomas Wright MD Page 1 of 4 Patient Name: Address: City, St, Zip Primary Phone: Alternate: DOB: Social Security #: Insurance Information Primary Insurance ID# Group# Subscriber
CONTENTS. Preface. Introduction. The Gem Sticks. Working with the Hand Rod or Pendulum. Types of Therapy. Gemstone Reflexology By Nora Kircher
 Gemstone Reflexology By Nora Kircher CONTENTS Preface Introduction The Gem Sticks Amethyst Aventurine Fluorite Heliotrope Rock Crystal Rose Quartz Rutile Quartz Sodalite Working with the Hand Rod or Pendulum
Gemstone Reflexology By Nora Kircher CONTENTS Preface Introduction The Gem Sticks Amethyst Aventurine Fluorite Heliotrope Rock Crystal Rose Quartz Rutile Quartz Sodalite Working with the Hand Rod or Pendulum
Camas Acupuncture & Nutrition Stephanie Meinhold, LAc 405 NE 6 th Avenue Camas, WA P F
 Patient Information Camas Acupuncture & Nutrition General Information Name: Date: Address: City: State: Zip Code: Phone (H): (W): Cell: Email: Appt reminders via text? Y N via email? Y N Date of Birth:
Patient Information Camas Acupuncture & Nutrition General Information Name: Date: Address: City: State: Zip Code: Phone (H): (W): Cell: Email: Appt reminders via text? Y N via email? Y N Date of Birth:
DHATU ASSESSMENT. Total the number of symptoms for each tissue category. 1. BLOOD PLASMA (RASA). The clear, serum portion of the blood.
. The clear, serum portion of the blood.") DHATU ASSESSMENT Total the number of symptoms for each tissue category. 1. BLOOD PLASMA (RASA). The clear, serum portion of the blood. Excessively dry skin Dehydration Premature graying of the hair Cold
DHATU ASSESSMENT Total the number of symptoms for each tissue category. 1. BLOOD PLASMA (RASA). The clear, serum portion of the blood. Excessively dry skin Dehydration Premature graying of the hair Cold
Bridges Family Wellness PC. New Patient Intake. Bridges Family Wellness Intake Form SE Lake Rd, Suite 102 Milwaukie, OR
 New Patient Intake Bridges Family Wellness Intake Form Full Name: * What is your birthdate? MM/DD/YYYY * What is your gender identity? * Home address: * Cell Phone * Other Phone number(s): Emergency Contact
New Patient Intake Bridges Family Wellness Intake Form Full Name: * What is your birthdate? MM/DD/YYYY * What is your gender identity? * Home address: * Cell Phone * Other Phone number(s): Emergency Contact
Symptom Review (page 1) Name Date
 Name Date") v2.4, 2/13 JonathanTreasure.com Botanical Medicine & Cancer Herb Drug Interactions Herbalism 3.0 Symptom Review (page 1) Name Date INSTRUCTIONS Please read each section below carefully and, after each
v2.4, 2/13 JonathanTreasure.com Botanical Medicine & Cancer Herb Drug Interactions Herbalism 3.0 Symptom Review (page 1) Name Date INSTRUCTIONS Please read each section below carefully and, after each
The TMJ Therapy Effects of Joint Manipulation
 The overall postural structure associated with TMJ disorders is part of the The TMJ Therapy concern. Chiropractic manipulation has helped realign the joints in your TMJ, neck, and low back and along with
The overall postural structure associated with TMJ disorders is part of the The TMJ Therapy concern. Chiropractic manipulation has helped realign the joints in your TMJ, neck, and low back and along with
Headache Follow-up Visit Form
 !1 Headache Follow-up Visit Form We will be unable to see you unless this form is completely filled out. We appreciate your thoroughness. Name DOB Age Today s Date Referring doctor: Primary doctor: Neurologist:
!1 Headache Follow-up Visit Form We will be unable to see you unless this form is completely filled out. We appreciate your thoroughness. Name DOB Age Today s Date Referring doctor: Primary doctor: Neurologist:
Name: Date of birth: Address: City: State: Zip: Phone: (day) (evening): (cell): address: Occupation: Who referred you/how did you hear about us?
 (evening): (cell): address: Occupation: Who referred you/how did you hear about us?") Name: Date of birth: Address: City: State: Zip: Phone: (day) (evening): (cell): Email address: Occupation: Who referred you/how did you hear about us? Your primary health care provider: Phone: Emergency
Name: Date of birth: Address: City: State: Zip: Phone: (day) (evening): (cell): Email address: Occupation: Who referred you/how did you hear about us? Your primary health care provider: Phone: Emergency
MEDICAL INFORMATION. SECTION 1: Pharmacy Information. Pharmacy Name and Address: Pharmacy Phone Number: SECTION 2: Social History
 MEDICAL INFORMATION TODAY S DATE: SOCIAL SECURITY NUMBER: PATIENT NAME: BIRTHDAY: HEIGHT: WEIGHT: AGE: WHO REFERRED YOU? RACE: PRIMARY CARE PHYSICIAN: SEX: DOCTOR S ADDRESS: SECTION 1: Pharmacy Information
MEDICAL INFORMATION TODAY S DATE: SOCIAL SECURITY NUMBER: PATIENT NAME: BIRTHDAY: HEIGHT: WEIGHT: AGE: WHO REFERRED YOU? RACE: PRIMARY CARE PHYSICIAN: SEX: DOCTOR S ADDRESS: SECTION 1: Pharmacy Information
THE MANY SYMPTOMS ROOTED IN HORMONE IMBALANCES
 abdominal pain acne aging process accelerated allergies, including asthma, hives, rashes, sinus congestion anemia (blood hemoglobin low) anorexia anovulatory (no ovulation) anxiety anxious depression appetite
abdominal pain acne aging process accelerated allergies, including asthma, hives, rashes, sinus congestion anemia (blood hemoglobin low) anorexia anovulatory (no ovulation) anxiety anxious depression appetite
New Client Health & Wellness Paper Work
 Nutritionally Yours Health Solutions 604 Macy Drive, Roswell GA 30076 678-372-2913 / alanepnd@gmail.com New Client Health & Wellness Paper Work Today's Date Patient Name: _ Parents Name (if patient is
Nutritionally Yours Health Solutions 604 Macy Drive, Roswell GA 30076 678-372-2913 / alanepnd@gmail.com New Client Health & Wellness Paper Work Today's Date Patient Name: _ Parents Name (if patient is
Questionnaire for Lipedema Patients
 Questionnaire for Lipedema Patients Name Date of diagnosis Date Name of physician making diagnosis Do you also have lymphedema? What areas of the body are affected? Outside of thighs Inner thighs Knees
Questionnaire for Lipedema Patients Name Date of diagnosis Date Name of physician making diagnosis Do you also have lymphedema? What areas of the body are affected? Outside of thighs Inner thighs Knees
MERIDIAN SYMPTOMOLOGY
 MERIDIAN SYMPTOMOLOGY According to Fukushima Kodo and Shudo Denmai a Summation by Jake Paul Fratkin, OMD Originally published in North American Journal of Oriental Medicine, Vol. 5, No. 12, March, 1998.
MERIDIAN SYMPTOMOLOGY According to Fukushima Kodo and Shudo Denmai a Summation by Jake Paul Fratkin, OMD Originally published in North American Journal of Oriental Medicine, Vol. 5, No. 12, March, 1998.
Balanced Healing Acupuncture, LLC
 Balanced Healing Acupuncture, LLC Intake Form NAME: Last First: GENDER: Date of Birth / / Age Email Address Address City State Zip Code Preferred Phone Number Cell Home Work Preferred Method of Communication:
Balanced Healing Acupuncture, LLC Intake Form NAME: Last First: GENDER: Date of Birth / / Age Email Address Address City State Zip Code Preferred Phone Number Cell Home Work Preferred Method of Communication:
Address: City: Postal Code: Emergency Contact: Phone# Relationship: Who may we thank for referring you to this office?
 CLAYTON PARK CHIROPRACTIC CENTRE INC. Suite 11-117 Kearney Lake Road Halifax, Nova Scotia B3M 4N9 (902) 443-5669 phone (902) 443-9419 fax info@claytonparkchiro.ca For Office Use Only: Bilaterals L R PERSONAL
CLAYTON PARK CHIROPRACTIC CENTRE INC. Suite 11-117 Kearney Lake Road Halifax, Nova Scotia B3M 4N9 (902) 443-5669 phone (902) 443-9419 fax info@claytonparkchiro.ca For Office Use Only: Bilaterals L R PERSONAL
Tongue Evaluation. Body Color. Including colors at different locations. Indications. Body temperature regulation.
 Tongue Evaluation Christopher Rodgers, Student Body. Refers to the overall appearance including muscles, arteries, and veins. Associations. Conditions of the cardiovascular, nervous, reproductive, urinary
Tongue Evaluation Christopher Rodgers, Student Body. Refers to the overall appearance including muscles, arteries, and veins. Associations. Conditions of the cardiovascular, nervous, reproductive, urinary
Patient Name Date of Birth MALE / FEMALE Date. Left handed or Right handed. Marital Status: Single Married Divorced Widowed Children?
 PH NEW PATIENT HISTORY Patient Name Date of Birth MALE / FEMALE Date Occupation: Left handed or Right handed Marital Status: Single Married Divorced Widowed Children? Y or N # Previous Treating Physician:
PH NEW PATIENT HISTORY Patient Name Date of Birth MALE / FEMALE Date Occupation: Left handed or Right handed Marital Status: Single Married Divorced Widowed Children? Y or N # Previous Treating Physician:
Medical History Form
 Medical History Form Full Name Title: Mr/Mrs/Ms/Miss Address Date of Birth Date Telephone: Mobile: Email: How did you hear about the Garden of health? G.P s Name and Address Are you currently seeing your
Medical History Form Full Name Title: Mr/Mrs/Ms/Miss Address Date of Birth Date Telephone: Mobile: Email: How did you hear about the Garden of health? G.P s Name and Address Are you currently seeing your
Sentelligent Medical Intuitive Body Scan
 Sentelligent Medical Intuitive Body Scan 1 1) Ask for presenting symptoms. Get clear channel and set sacred space. 2) Ask if any resistance or interference. 3) Ask Source to provide information only on
Sentelligent Medical Intuitive Body Scan 1 1) Ask for presenting symptoms. Get clear channel and set sacred space. 2) Ask if any resistance or interference. 3) Ask Source to provide information only on
My energy is lower than I would like it to. I feel exhausted after exercising or physical activity.
 SYMPTOMS Questionnaire Duplicate your answer across all of the 5 boxes that aren t blocked out. See example ENERGY My energy is lower than I would like it to be. I feel exhausted after exercising or physical
SYMPTOMS Questionnaire Duplicate your answer across all of the 5 boxes that aren t blocked out. See example ENERGY My energy is lower than I would like it to be. I feel exhausted after exercising or physical
Horse Meridians & Ting Points
 Horse Meridians & Ting Points Just like the Chakras are the main energy centers, the Meridians are the major pathways. They help to determine where the energy travels through the body. If these pathways
Horse Meridians & Ting Points Just like the Chakras are the main energy centers, the Meridians are the major pathways. They help to determine where the energy travels through the body. If these pathways
Dr. Sereena Uppal DC Michael Herrewig DC Doctor of Chiropractic th Avenue Surrey BC V4A 2H9 Tel: Fax:
 Dr. Sereena Uppal DC Michael Herrewig DC Doctor of Chiropractic 690 15355 24 th Avenue Surrey BC V4A 2H9 Tel: 604.541.9336 Fax: 604.541.9308 I. Patient Information Thank you for choosing our practice for
Dr. Sereena Uppal DC Michael Herrewig DC Doctor of Chiropractic 690 15355 24 th Avenue Surrey BC V4A 2H9 Tel: 604.541.9336 Fax: 604.541.9308 I. Patient Information Thank you for choosing our practice for
Bodily Conditions Rooted in Hormone Imbalance
 Check this list for all conditions that apply to you. The total possible score is 209. Count the number of symptoms you check. The higher your score, the more likely you need to address hormone imbalances.
Check this list for all conditions that apply to you. The total possible score is 209. Count the number of symptoms you check. The higher your score, the more likely you need to address hormone imbalances.
NEW PATIENT QUESTIONNAIRE
 Consultant Name: NEW PATIENT QUESTIONNAIRE Health Care Analysis CONGRATULATIONS! You ve taken an important step in your commitment to managing your weight. We look forward to working with you. Our Program
Consultant Name: NEW PATIENT QUESTIONNAIRE Health Care Analysis CONGRATULATIONS! You ve taken an important step in your commitment to managing your weight. We look forward to working with you. Our Program
PLEASE COMPLETE ALL SECTIONS OF THIS FORM
 PLEASE COMPLETE ALL SECTIONS OF THIS FORM Patient Name: Date of Birth: Referring Doctor? (Name, telephone number and address) Chief Complaint: Why have you come here? How did it start? What are the symptoms?
PLEASE COMPLETE ALL SECTIONS OF THIS FORM Patient Name: Date of Birth: Referring Doctor? (Name, telephone number and address) Chief Complaint: Why have you come here? How did it start? What are the symptoms?
Acupuncture. The Art of Healing with Needles
 Acupuncture The Art of Healing with Needles What is Acupuncture? Strategic placement of needles to stimulate acupoints on meridians to restore proper flow of Qi and Blood and balance of Yin and Yang to
Acupuncture The Art of Healing with Needles What is Acupuncture? Strategic placement of needles to stimulate acupoints on meridians to restore proper flow of Qi and Blood and balance of Yin and Yang to
Chiropractic Patient Admittance Form
 Chiropractic Patient Admittance Form PERSONAL INFORMATION Last Name: Given Name: Initial: Address: City/Province: Postal Code: Home Phone: Work Phone: Cell: E-mail Address: Date of Birth (D/MM/YYYY): Male
Chiropractic Patient Admittance Form PERSONAL INFORMATION Last Name: Given Name: Initial: Address: City/Province: Postal Code: Home Phone: Work Phone: Cell: E-mail Address: Date of Birth (D/MM/YYYY): Male
DETOXIFICATION SUPPORT
 DETOXIFICATION SUPPORT with Jodi Cohen, NTP, Founder www.vibrantblueoils.com Key Points SUPPORT the detoxification organs BEFORE starting a detoxification program. This includes digestive healing efforts
DETOXIFICATION SUPPORT with Jodi Cohen, NTP, Founder www.vibrantblueoils.com Key Points SUPPORT the detoxification organs BEFORE starting a detoxification program. This includes digestive healing efforts
Who is filling out this intake form? Self Spouse Parent Guardian
 Office Use Only: Reviewed with Patient Data Entry Scan & File Date: Date: Date: Initials: Initials: Initials: Today s Date: Who is filling out this intake form? Self Spouse Parent Guardian If you are not
Office Use Only: Reviewed with Patient Data Entry Scan & File Date: Date: Date: Initials: Initials: Initials: Today s Date: Who is filling out this intake form? Self Spouse Parent Guardian If you are not
Luo Vessels, Cutaneous and Muscle Regions
 Chapter 3 Luo Vessels, Cutaneous and Muscle Regions 1 Characteristics of Luo Vessels Connect external/internal pairs Distribute qi throughout the body Harmonize circulation 2 In all, there are fifteen
Chapter 3 Luo Vessels, Cutaneous and Muscle Regions 1 Characteristics of Luo Vessels Connect external/internal pairs Distribute qi throughout the body Harmonize circulation 2 In all, there are fifteen
Patient Information. Vibrant Health Acupuncture & Wellness Center, LLC 260 Gateway Drive, Suite 7B Bel Air, Maryland
 Patient Information Vibrant Health Acupuncture & Wellness Center, LLC 260 Gateway Drive, Suite 7B Bel Air, Maryland 21014 410-913-8322 Patient Name: Date of Birth: Age: Male: Female: Single: Married: Separated:
Patient Information Vibrant Health Acupuncture & Wellness Center, LLC 260 Gateway Drive, Suite 7B Bel Air, Maryland 21014 410-913-8322 Patient Name: Date of Birth: Age: Male: Female: Single: Married: Separated:
CURRENT HEALTH CONDITIONS. Patient Name: Date:
 Patient Name: Date: Is this your first pregnancy? 0 Yes 0 No - If not, please tell us about your previous pregnancy and/or birth experience(s). (Duration, frtervent/ons, etc) Do you plan to follow the
Patient Name: Date: Is this your first pregnancy? 0 Yes 0 No - If not, please tell us about your previous pregnancy and/or birth experience(s). (Duration, frtervent/ons, etc) Do you plan to follow the
Health Intake Form. Name: Prefer Name: Date: City: State: Zip Code: Gender: M F. Telephone # (home): (work): (Cell):
: (work): (Cell):") Health Intake Form Name: Prefer Name: Date: Address: Age: City: State: Zip Code: Gender: M F Telephone # (home): (work): (Cell): Email Address: Date of Birth: Marital Status: Married Separated Divorced
Health Intake Form Name: Prefer Name: Date: Address: Age: City: State: Zip Code: Gender: M F Telephone # (home): (work): (Cell): Email Address: Date of Birth: Marital Status: Married Separated Divorced
Amarillo Surgical Group Doctor: Date:
 Office Visit Information (General Surgery) Amarillo Surgical Group Doctor: Date: Patient s Information Name: Last First Middle Social Security #: Date of Birth: Age Gender: [ Male / Female ] Marital Status:
Office Visit Information (General Surgery) Amarillo Surgical Group Doctor: Date: Patient s Information Name: Last First Middle Social Security #: Date of Birth: Age Gender: [ Male / Female ] Marital Status:
The information you provide us will greatly help us provide the highest quality and most comprehensive care for you.
 Rheumatology (circle location of appointment) 111 Hundertmark Rd. Suite 115N 560 S. Maple St. Suite 400 place patient label here Chaska, MN 55318 Waconia, MN 55387 952-361-2450 952-361-2450 The information
Rheumatology (circle location of appointment) 111 Hundertmark Rd. Suite 115N 560 S. Maple St. Suite 400 place patient label here Chaska, MN 55318 Waconia, MN 55387 952-361-2450 952-361-2450 The information
Have a healthy discussion. Use this guide to start a. conversation. with your. healthcare provider
 Have a healthy discussion Use this guide to start a conversation with your healthcare provider MAKE THE CONVERSATION COUNT Here are some things you may want to reflect on and discuss with your healthcare
Have a healthy discussion Use this guide to start a conversation with your healthcare provider MAKE THE CONVERSATION COUNT Here are some things you may want to reflect on and discuss with your healthcare
Introduction of Korean Acupuncture focusing on Saam Five Element Acupuncture and Facial Acupuncture
 Introduction of Korean Acupuncture focusing on Saam Five Element Acupuncture and Facial Acupuncture Sanghoon Lee MD(Korean Medicine), MPH, PhD, DiplAc, LAc.(USA) Professor of Acupuncture & Moxibustion
Introduction of Korean Acupuncture focusing on Saam Five Element Acupuncture and Facial Acupuncture Sanghoon Lee MD(Korean Medicine), MPH, PhD, DiplAc, LAc.(USA) Professor of Acupuncture & Moxibustion
Condition #2: What is the next important condition you would like help with, and how long ago did it begin?:
 NAME _ Please take the time to fill this form out completely. The more information we have, the better we can assist you, and will make better use of your initial visit. What is the main problem you would
NAME _ Please take the time to fill this form out completely. The more information we have, the better we can assist you, and will make better use of your initial visit. What is the main problem you would
CASE HISTORY. Address: City: State: Zip: Date of Birth: Age: address: Occupation: Employer: Spouse's Employer: Referred by:
 CASE HISTORY Account #: Please complete this form using your keyboard, then print it using the print function of your browser. You can then sign the form and bring it with you to your first appointment.
CASE HISTORY Account #: Please complete this form using your keyboard, then print it using the print function of your browser. You can then sign the form and bring it with you to your first appointment.
California Chiropractic Boshears, Inc Yucaipa Blvd., Yucaipa Ca Phone: (909) Fax : (909)
 Fax : (909)") California Chiropractic Boshears, Inc. 35191 Yucaipa Blvd., Yucaipa Ca. 92399 Phone: (909) 790-5005 Fax : (909) 790-5009 Patient Information Date: Name: Address: Home Phone: Work Phone: Sex: Male or Female
California Chiropractic Boshears, Inc. 35191 Yucaipa Blvd., Yucaipa Ca. 92399 Phone: (909) 790-5005 Fax : (909) 790-5009 Patient Information Date: Name: Address: Home Phone: Work Phone: Sex: Male or Female
Medication Allergies
 **PLEASE CHECK IN 15 MINUTES PRIOR TO APPOINTMENT WITH FORMS COMPLETED** Primary Provider at Ocotillo Internal Medicine Other Physicians you see: Jonathan Hackenyos, D.O. 1. Cheryl Maurice, M.D. 2. 3.
**PLEASE CHECK IN 15 MINUTES PRIOR TO APPOINTMENT WITH FORMS COMPLETED** Primary Provider at Ocotillo Internal Medicine Other Physicians you see: Jonathan Hackenyos, D.O. 1. Cheryl Maurice, M.D. 2. 3.
BROADWAY SPORTS & INTERNAL MEDICINE, P.S TH AVE NE SUITE 202 BELLEVUE, WA P: F:
 BROADWAY SPORTS & INTERNAL MEDICINE, P.S. 1600 116 TH AVE NE SUITE 202 BELLEVUE, WA 98004 P: 206 215-2288 F:206 215-2289 MEDICAL HISTORY QUESTIONNAIRE Date Name Date of Birth HT WT Current Medical Complaints
BROADWAY SPORTS & INTERNAL MEDICINE, P.S. 1600 116 TH AVE NE SUITE 202 BELLEVUE, WA 98004 P: 206 215-2288 F:206 215-2289 MEDICAL HISTORY QUESTIONNAIRE Date Name Date of Birth HT WT Current Medical Complaints
Symptom Questionnaire
 Symptom Questionnaire The following questionnaire is a general assessment of your health developed by Dr Royal Lee D.D.S. Each grouping represents a particular area of your body that may be causing you
Symptom Questionnaire The following questionnaire is a general assessment of your health developed by Dr Royal Lee D.D.S. Each grouping represents a particular area of your body that may be causing you
Longevitology Toronto Canada Questions. A: Two compulsory questions: B: 102 Questions
 Longevitology Toronto Canada - 102 Questions A: Two compulsory questions: What is Longevitology? Longevitology is the knowledge to receive the cosmic energy so as to strengthen the Chi in human body, thus
Longevitology Toronto Canada - 102 Questions A: Two compulsory questions: What is Longevitology? Longevitology is the knowledge to receive the cosmic energy so as to strengthen the Chi in human body, thus
1. Have you ever had or now have: 2. Have you ever had or now have:
 1. Have you ever had or now have: 2. Have you ever had or now have: Yes No Please Check each item no blanks CARDIOVASCULAR Yes No Often Seldom 1. Chronic or frequent colds 1. Shortness of breath with normal
1. Have you ever had or now have: 2. Have you ever had or now have: Yes No Please Check each item no blanks CARDIOVASCULAR Yes No Often Seldom 1. Chronic or frequent colds 1. Shortness of breath with normal
Patient History Form
 Patient Personal Information Name: Date: Age: Occupation: Employer's name: Briefly describe your daily activities at work: Sex: male female Marital Status: single married divorced widowed Spouse's name:
Patient Personal Information Name: Date: Age: Occupation: Employer's name: Briefly describe your daily activities at work: Sex: male female Marital Status: single married divorced widowed Spouse's name:
2. Approx. Date of Onset: 3. Approx. Date of Onset:
 Healthy Balance Lisa A. Dulac, L.Ac. Acupuncture Patient Intake Form Present Health Concerns: Please list your most important health concerns in order of their significance. 1. Approx. Date of Onset: 2.
Healthy Balance Lisa A. Dulac, L.Ac. Acupuncture Patient Intake Form Present Health Concerns: Please list your most important health concerns in order of their significance. 1. Approx. Date of Onset: 2.
Past Medical History. Chief Complaint: Patient Name: Appointment Date: Page 1
 Appointment Date: Page 1 Chief Complaint: (Please write reason, symptoms, condition or diagnosis that prompts your appointment) Past Medical History PERSONAL SKIN HISTORY YES NO Yes - Details Melanoma
Appointment Date: Page 1 Chief Complaint: (Please write reason, symptoms, condition or diagnosis that prompts your appointment) Past Medical History PERSONAL SKIN HISTORY YES NO Yes - Details Melanoma