Chiropractic for pediatric development and adult health
|
|
|
- Sophie Banks
- 5 years ago
- Views:
Transcription
 846-7004 Items to bring to your first visit: All new patient paperwork filled out in advance Your automobile insurance policy o Claim number o Adjuster s name and")
1 Raleigh Specific Chiropractic Chiropractic for pediatric development and adult health 7721 Six Forks Rd. Suite 138 Raleigh, NC (919) Items to bring to your first visit: All new patient paperwork filled out in advance Your automobile insurance policy o Claim number o Adjuster s name and phone number o Contact your automobile insurance and open a medical claim 3 rd party automobile policy information o Claim number o Adjuster s name and phone number Your health insurance Your attorney information, if applicable
2 Patient Information -Our mission is to educate and adjust as many families as possible toward optimal health through natural chiropractic care- James K. Winget B.S. DC Jill R. Winget B.S. DC Date Patient No. Name S/S# - - First MI Last (Please Print) Address City: State Zip Home Phone # Work Phone # ext Cell # Sex: Female Male Age Birth Date Are you: Minor Single Married Divorced Widowed Separated Address: Your Employer: Occupation Business Address City State Zip Spouse's or parent's name Workplace Work number Other Person to contact in case of emergency Phone # Whom may we thank for referring you to us? Insurance Information Name of Primary Insurance Company involved Complete Name of the Insured Claims Adjustor's Name Claim# Address Phone# Attorney Information Name Phone# Address City State Zip Health Insurance This office will verify health insurance coverage for you. This is done as a courtesy for you, so please attach Insurance Card if available, and return to chiropractic assistant with this intake request CONFIDENTIAL 7721 Six Forks Rd Ste 138 Raleigh NC office (919) fax (919)
3
4
5 Raleigh Specific Chiropractic Chiropractic for pediatric development and adult health Patient Consents 7721 Six Forks Rd. Suite 138 Raleigh, NC (919) Consent for purposes of treatment, payment and healthcare operations I consent to the use or disclosure of my protected health information by Raleigh Specific Chiropractic for the purpose of diagnosing or providing treatment to me, obtaining payment for my health care bills, or to conduct health care operations of Raleigh Specific Chiropractic. I understand that diagnosis or treatment of me by Dr. James Winget or Dr. Jill Winget may be conditioned upon my consent as evidenced by my signature on this document. I understand I have the right to request a restriction. Raleigh Specific Chiropractic is not required to agree to the restriction I may request. However, if Raleigh Specific Chiropractic agrees to a restriction that I request, the restriction is binding on Raleigh Specific Chiropractic and on Drs. Winget. I have the right to revoke this consent, in writing, at any time, except to the extent that Dr. James/Jill Winget or Raleigh Specific Chiropractic has taken action in reliance on this consent. More information regarding this consent is available upon request. Open adjusting area It is the practice of this office to provide chiropractic care in an open adjusting environment. Open adjusting involves several patients being seen in the same adjusting area at the same time. Patients are within sight of one another, and some ongoing routine details of care are discussed within earshot of other patients and staff. This environment is used for ongoing care and is NOT the environment used for taking patient histories, performing examinations, or presenting reports of findings. These procedures are completed in a private, confidential setting. We are requesting this authorization of you due to various interpretations under federal law with respect to what is known as incidental disclosures of health information. It is our view that the kinds of matters related in an open adjusting environment are incidental matters. In the event you are someone else would not agree with us, we are providing this disclosure. The use of this format is intended to make your experience with our office more efficient and productive, as well as to enhance your access to quality health care and health information. If you choose not to be adjusted in an open adjusting environment, other arrangements will be made for you. Your decision will have no adverse effect on your care from Raleigh Specific Chiropractic or on your relationship with our staff. Your signature indicates your authorization of this activity. Your authorization may be revoked by you at any time. Revocation may be accomplished by advising us in writing of your desire to withdraw your authorization. Please allow a reasonable processing time for the change in our procedures to be completed. Contact It is our desire for our staff to use your name, address, and/or telephone number for the purpose of contacting you to advise you about health-related meetings, workshops, missed appointments and appointment reminders. The use of this information is intended to make your experience with our office more efficient and productive, as well as to further enhance your access to quality health care. If you choose not to authorize this information use, your decision will have no adverse effect on your care from Raleigh Specific Chiropractic or on your relationship with our staff. This office also occasionally posts stories and x-rays of current patients. If this situation presents itself in your case, this office will obtain specific permission from you for that purpose. Your signature indicates your authorization of this activity. Your authorization may be revoked by you at any time. Revocation may be accomplished by advising us in writing of your desire to withdraw your authorization. Please allow a reasonable processing time for the change in our procedures to be completed. Patient Name, Printed Patient Signature Date
6
7
8
9
10 Raleigh Specific Chiropractic Chiropractic for pediatric development and adult health 7721 Six Forks Rd. Suite 138 Raleigh, NC (919) Informed Consent for Chiropractic Care Raleigh Specific Chiropractic, Inc Chiropractic care, like all forms of health care, while offering considerable benefit may also provide some level of risk. This level of risk is most often very minimal, yet in rare cases injury has been associated with chiropractic care. The types of complications that have been reported secondary to chiropractic care include sprain/strain injuries, irritation of a disc condition, and rarely, fractures. One of the rarest complications associated with chiropractic care, occurring at a rate between one instance per one million to one per two million cervical spine (neck) adjustments may be a vertebral artery injury that could lead to stroke. Prior to receiving chiropractic care at this Chiropractic office, a health history and physical examination will be completed. These procedures are performed to assess your specific condition, your overall health and, in particular, your spine health. These procedures will assist us in determining if chiropractic care is needed, or if any further examinations or studies are needed. In addition, they will help us determine if there is any reason to modify your care or provide you with a referral to another health care provider. All relevant findings will be reported to you prior to beginning care. I understand and accept that there are risks associated with chiropractic care and give my consent to the examinations that the doctor deems necessary, and to the chiropractic care including spinal adjustments, as reported following my assessment. Patient Name (printed) Patient or legal Guardian Signature Witness Signature (office staff) Reviewed by Doctor Relationship to patient Date Date Date
Liberty Chiropractic Clinic Scarsdale Blvd., Houston, TX
 Liberty Chiropractic Clinic, -6154 Patient's Name Patient's Address City State Zip Code Age D.O.B. Single Married Divorced Widowed No. of children Occupation Employer Home Phone Work Phone Cell Phone Email
Liberty Chiropractic Clinic, -6154 Patient's Name Patient's Address City State Zip Code Age D.O.B. Single Married Divorced Widowed No. of children Occupation Employer Home Phone Work Phone Cell Phone Email
Natural Health Center
 Natural Health Center 420 Yucca Lane - Turpin, OK 73950 Tel. No. (580) 778-3310 / Cell No. (620) 391-5520 / Fax No. (580) 778-3340 Today s Date / / Application for Treatment Name: Birthdate: SS# Address:
Natural Health Center 420 Yucca Lane - Turpin, OK 73950 Tel. No. (580) 778-3310 / Cell No. (620) 391-5520 / Fax No. (580) 778-3340 Today s Date / / Application for Treatment Name: Birthdate: SS# Address:
Name Date / / Age Male/ Female Address City State Zip
 T 1 2 3 : Name _ Date / / Age Male/ Female Address City State Zip Phone: Home Cell Cell Phone Provider Email Address Date of Birth / / Occupation Employer Single / Married / Divorced / Widowed Spouse s
T 1 2 3 : Name _ Date / / Age Male/ Female Address City State Zip Phone: Home Cell Cell Phone Provider Email Address Date of Birth / / Occupation Employer Single / Married / Divorced / Widowed Spouse s
Name Date / / Age Male/Female Address City State Zip Phone: Home Cell Carrier (Ex: AT&T, Verizon)
") Name_ Date / / Age Male/Female Address City State Zip Phone: Home Cell Carrier (Ex: AT&T, Verizon) For reminders do you prefer Phone Calls, Text Messages or Emails? CALL ME / TEXT ME / EMAIL ME Email Address
Name_ Date / / Age Male/Female Address City State Zip Phone: Home Cell Carrier (Ex: AT&T, Verizon) For reminders do you prefer Phone Calls, Text Messages or Emails? CALL ME / TEXT ME / EMAIL ME Email Address
Initial Clinical History and Physical Form
 601 E FM 544, Suite 400, Murphy, TX, 75094 TEL: 972-442-4700 Initial Clinical History and Physical Form Patient Information Name: Age: of Birth: / / Sex: Male / Female Marital Status: Single Married Divorced
601 E FM 544, Suite 400, Murphy, TX, 75094 TEL: 972-442-4700 Initial Clinical History and Physical Form Patient Information Name: Age: of Birth: / / Sex: Male / Female Marital Status: Single Married Divorced
Who? When? Results? Please Mark P For In The Past OR Mark C For Currently Have:
 T, CD, E, C New Practice Member Application Name Date of Birth / / Age Male/Female Address City State Zip Phone: Cell Home Email Address Occupation Employer s Name Single / Married / Divorced / Widowed
T, CD, E, C New Practice Member Application Name Date of Birth / / Age Male/Female Address City State Zip Phone: Cell Home Email Address Occupation Employer s Name Single / Married / Divorced / Widowed
First Name Middle Last Today s Date / / Age Male/Female Date of Birth / / SS# - - Address City State ZIP Phone: Home Cell Phone Provider Address
 First Name Middle Last Today s Date / / Age Male/Female Date of Birth / / SS# - - Address City State ZIP Phone: Home Cell Phone Provider Email Address Do you have Medicaid? Y / N (present your card to
First Name Middle Last Today s Date / / Age Male/Female Date of Birth / / SS# - - Address City State ZIP Phone: Home Cell Phone Provider Email Address Do you have Medicaid? Y / N (present your card to
ADIO CHIROPRACTIC HEALTH PROFILE
 ADIO CHIROPRACTIC HEALTH PROFILE Name Date / / Age Male/Female Address City State Zip Phone: Home Cell_ Date of Birth / / Email Address For confirming appointments, would you prefer? EMAIL or TEXT CELL
ADIO CHIROPRACTIC HEALTH PROFILE Name Date / / Age Male/Female Address City State Zip Phone: Home Cell_ Date of Birth / / Email Address For confirming appointments, would you prefer? EMAIL or TEXT CELL
We Believe that you are Designed to be Extraordinary. (Office Use) Care Provider: Name: Date of birth (MM/DD/YY): Apt# City: Prov: PC:
 Care Provider: Name: Date of birth (MM/DD/YY): Apt# City: Prov: PC:") (Office Use) Care Provider: Name: Date of birth (MM/DD/YY): Mailing address: Apt# City: Prov: PC: Phone: h) c) Email: Do we have your permission to send you our weekly health newsletter? Y N **You can
(Office Use) Care Provider: Name: Date of birth (MM/DD/YY): Mailing address: Apt# City: Prov: PC: Phone: h) c) Email: Do we have your permission to send you our weekly health newsletter? Y N **You can
LIST YOUR HEALTH CONCERNS BELOW
 8209 Natures Way Unit 115 Lakewood Ranch, Florida 34202 (941) 877.1507 Name Date / / Age Male Female Address City State Zip Phone: Home Cell Cell Phone Provider Email Date of Birth / / Employer s Name
8209 Natures Way Unit 115 Lakewood Ranch, Florida 34202 (941) 877.1507 Name Date / / Age Male Female Address City State Zip Phone: Home Cell Cell Phone Provider Email Date of Birth / / Employer s Name
Who may we thank for referring you?
 NEW PRACTICE MEMBER APPLICATION Name Date of Birth / / Age Male/Female Address City State Zip Phone: Cell Home Social Security #: Email: Occupation Employer s Name Status: Single / Married / Divorced /
NEW PRACTICE MEMBER APPLICATION Name Date of Birth / / Age Male/Female Address City State Zip Phone: Cell Home Social Security #: Email: Occupation Employer s Name Status: Single / Married / Divorced /
New Practice Member Application
 New Practice Member Application Name Date of Birth / / Age Male/Female Address City State Zip Phone: Cell Home Social Security #: Email: Occupation Employer s Name Status: Single / Married / Divorced /
New Practice Member Application Name Date of Birth / / Age Male/Female Address City State Zip Phone: Cell Home Social Security #: Email: Occupation Employer s Name Status: Single / Married / Divorced /
PATIENT INFORMATION. Address City State Zip. Home Phone Work Phone Cell Phone Is it okay to contact you at work? Yes No. SSN - - DOB Age
 PATIENT INFORMATION Name Date Address City State Zip Home Phone Work Phone Cell Phone Is it okay to contact you at work? Yes No Carrier: E-mail @ SSN - - DOB Age Occupation: Employer: Marital Status: S
PATIENT INFORMATION Name Date Address City State Zip Home Phone Work Phone Cell Phone Is it okay to contact you at work? Yes No Carrier: E-mail @ SSN - - DOB Age Occupation: Employer: Marital Status: S
Practice Member Profile
 Practice Member Profile Please print Name: : Phone number: (H) (C) Cell provider: Address: City: State: Zip: of Birth: Age: Male Female (circle one) Marital Status: Name of Spouse: Number of Children:
Practice Member Profile Please print Name: : Phone number: (H) (C) Cell provider: Address: City: State: Zip: of Birth: Age: Male Female (circle one) Marital Status: Name of Spouse: Number of Children:
CIRCLE ALL CURRENT PROBLEMS YOU HAVE
 INSIDE OUT CHIROPRACTIC HEALTH PROFILE Name Date / / Age Male/Female Address City State Zip Phone: Home Cell_ Date of Birth / / Email Address For confirming appts, would you prefer? TEXT (cell carrier:
INSIDE OUT CHIROPRACTIC HEALTH PROFILE Name Date / / Age Male/Female Address City State Zip Phone: Home Cell_ Date of Birth / / Email Address For confirming appts, would you prefer? TEXT (cell carrier:
Physical Evidence Chiropractic 7035 Beracasa Way, Suite 103 Boca Raton Florida, Phone# (561) Fax# (561)
 Fax# (561)") 7035 Beracasa Way, Suite 103 Boca Raton Florida, 33433 Phone# (561)674-1217 Fax# (561)361-4999 Date File # PERSONAL HISTORY Last Name First Name middle Address City State Zip Date of Birth Age Social Security
7035 Beracasa Way, Suite 103 Boca Raton Florida, 33433 Phone# (561)674-1217 Fax# (561)361-4999 Date File # PERSONAL HISTORY Last Name First Name middle Address City State Zip Date of Birth Age Social Security
Welcome to our Family Chiropractic Office
 Welcome to our Family Chiropractic Office Thank you for choosing our office for chiropractic care. We are committed to providing your family with the highest quality of corrective and wellness chiropractic
Welcome to our Family Chiropractic Office Thank you for choosing our office for chiropractic care. We are committed to providing your family with the highest quality of corrective and wellness chiropractic
PATIENT ENTRANCE FORM
 PATIENT ENTRANCE FORM Name _ Date Address City/ Province Postal Code Home Telephone Work Telephone Email Address Would like email reminders for appointments? Yes No Date of Birth (Day/Month/Year) Age Marital
PATIENT ENTRANCE FORM Name _ Date Address City/ Province Postal Code Home Telephone Work Telephone Email Address Would like email reminders for appointments? Yes No Date of Birth (Day/Month/Year) Age Marital
New Practice Member Paperwork
 Cornerstone Family Chiropractic Health Information Form 928.237.9477 www.cfc4familyhealth.com 2225 E State Route 69 Suite A Prescott, AZ 86301 New Practice Member Paperwork This form is for adults only.
Cornerstone Family Chiropractic Health Information Form 928.237.9477 www.cfc4familyhealth.com 2225 E State Route 69 Suite A Prescott, AZ 86301 New Practice Member Paperwork This form is for adults only.
SEEDS OF HOPE FAMILY CHIROPRACTIC HEALTH HISTORY
 SEEDS OF HOPE FAMILY CHIROPRACTIC HEALTH HISTORY Welcome! PLEASE PRINT CLEARLY PERSONAL DATA Today s Date First name MI: Last name: Nickname Gender M F Age Date of Birth SS# (optional) Current address
SEEDS OF HOPE FAMILY CHIROPRACTIC HEALTH HISTORY Welcome! PLEASE PRINT CLEARLY PERSONAL DATA Today s Date First name MI: Last name: Nickname Gender M F Age Date of Birth SS# (optional) Current address
LIST YOUR HEALTH CONCERNS BELOW
 T 1 2 3 ROOTS CHIROPRACTIC HEALTH PROFILE In Name Date / / Age Male/Female Address City State Zip Phone: Home Cell Work Email Address Date of Birth / / Occupation Employer's Name Single / Married / Divorced
T 1 2 3 ROOTS CHIROPRACTIC HEALTH PROFILE In Name Date / / Age Male/Female Address City State Zip Phone: Home Cell Work Email Address Date of Birth / / Occupation Employer's Name Single / Married / Divorced
Who may we thank for referring you? Office Only LIST YOUR HEALTH CONCERNS BELOW. If you had the condition before, when? When did this episode start?
 Name Date / / Age Male / Female Address City State Zip Phone: Home Cell Cell Phone Provider Date of Birth / / Email Address Occupation Employer s Name Single / Married / Divorced / Widowed Spouse s Name
Name Date / / Age Male / Female Address City State Zip Phone: Home Cell Cell Phone Provider Date of Birth / / Email Address Occupation Employer s Name Single / Married / Divorced / Widowed Spouse s Name
Patient First Name: Last Name: Street Address: City: State: Zip Code. Mobile Phone: Home Phone: Work Phone:
 Dr. Beth Kozak Welcome! New Patient Information Form Please provide us with the following information: Patient First Name: Last Name: Street Address: City: State: Zip Code Mobile Phone: Home Phone: Work
Dr. Beth Kozak Welcome! New Patient Information Form Please provide us with the following information: Patient First Name: Last Name: Street Address: City: State: Zip Code Mobile Phone: Home Phone: Work
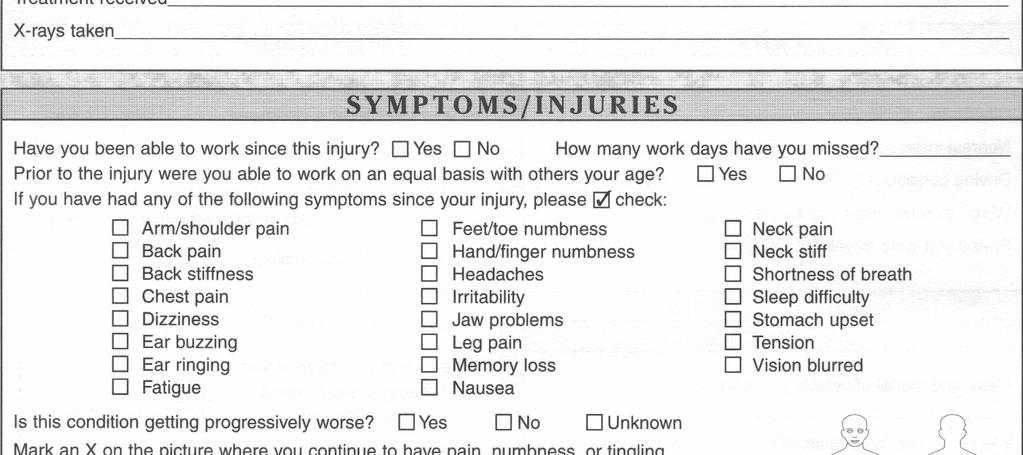
COMPLAINTS (Briefly describe each complaint by order of severity): HAVE YOU EVER HAD FALLS, AUTO ACCIDENTS OR INJURIES?
: HAVE YOU EVER HAD FALLS, AUTO ACCIDENTS OR INJURIES?") CORAL REEF CHIROPRACTIC CENTER, PA NAME (Last, First, Middle Initial) HOME PHONE TODAY S DATE COMPLETE ADDRESS (Include City, State & Zip) CELL PHONE DATE OF BIRTH OCCUPATION EMPLOYER NAME EMAIL AGE SEX
CORAL REEF CHIROPRACTIC CENTER, PA NAME (Last, First, Middle Initial) HOME PHONE TODAY S DATE COMPLETE ADDRESS (Include City, State & Zip) CELL PHONE DATE OF BIRTH OCCUPATION EMPLOYER NAME EMAIL AGE SEX
Welcome. In case of emergency, contact: Is condition due to an accident? [ ] Yes [ ] No
![Welcome. In case of emergency, contact: Is condition due to an accident? [ ] Yes [ ] No](/thumbs/89/99616722.jpg "Welcome. In case of emergency, contact: Is condition due to an accident? [ ] Yes [ ] No") Patient Information Welcome Who is responsible for this account? SSN Relationship to Patient Patient Name Insurance Co. Name: Preferred First Name Group #: ID #: Sex [ ] M [ ] F Age: Birthdate SS# Birthdate
Patient Information Welcome Who is responsible for this account? SSN Relationship to Patient Patient Name Insurance Co. Name: Preferred First Name Group #: ID #: Sex [ ] M [ ] F Age: Birthdate SS# Birthdate
Chiropractic Case History/Patient Information
 Chiropractic Case History/Patient Information 1 Date: Patient # Doctor: Name: Social Security # Home Phone: Address: City: State: Zip: E-mail address: Fax # Cell Phone: Age: Birth Date: Race: Marital:
Chiropractic Case History/Patient Information 1 Date: Patient # Doctor: Name: Social Security # Home Phone: Address: City: State: Zip: E-mail address: Fax # Cell Phone: Age: Birth Date: Race: Marital:
Address City State Zip Code
 Name Cell Phone Address City State Zip Code Date of Birth / / Male/Female Age Email SS# Number of Children Name of Children Employer Type of Work Marital Status Married Single Divorced Separated Widowed
Name Cell Phone Address City State Zip Code Date of Birth / / Male/Female Age Email SS# Number of Children Name of Children Employer Type of Work Marital Status Married Single Divorced Separated Widowed
Patient Information. Preferred Name: Date of Birth: SSN: Address: City: State: Zip: Phone: Cell/Home/Work (please circle one)
") Patient Information Name: First Last M.I. Date: Preferred Name: Date of Birth: SSN: Address: City: State: Zip: Email: Phone: Cell/Home/Work (please circle one) How did you hear about us? Door hanger, Fargo
Patient Information Name: First Last M.I. Date: Preferred Name: Date of Birth: SSN: Address: City: State: Zip: Email: Phone: Cell/Home/Work (please circle one) How did you hear about us? Door hanger, Fargo
LIST YOUR HEALTH CONCERNS BELOW
 Name Date / / Age Male/Female Address City State Zip Phone: Cell Cell Phone Provider Date of Birth / / Email Address Occupation Employer s Name Single/Married/Divorced/Widowed Spouse s Name Number of Children
Name Date / / Age Male/Female Address City State Zip Phone: Cell Cell Phone Provider Date of Birth / / Email Address Occupation Employer s Name Single/Married/Divorced/Widowed Spouse s Name Number of Children
Health Intake Form Connected Chiropractic 32 S. Rutherford Ave.
 Health Intake Form Connected Chiropractic 32 S. Rutherford Ave. Johnstown, CO 80534 (970) 587-7029 Name: Date: Address: City: State: Zip: Cell Ph: Home Ph: Work Ph: Best Number to contact you: Home Work
Health Intake Form Connected Chiropractic 32 S. Rutherford Ave. Johnstown, CO 80534 (970) 587-7029 Name: Date: Address: City: State: Zip: Cell Ph: Home Ph: Work Ph: Best Number to contact you: Home Work
Home Sleep Test (HST) Instructions
 Instructions") Home Sleep Test (HST) Instructions 1. Your physician has ordered an unattended home sleep test (HST) to diagnose or rule out sleep apnea. This test cannot diagnose any other sleep disorders. 2. This device
Home Sleep Test (HST) Instructions 1. Your physician has ordered an unattended home sleep test (HST) to diagnose or rule out sleep apnea. This test cannot diagnose any other sleep disorders. 2. This device
Patient Intake Form Gray Chiropractic Health Clinic LLC 360 East International Airport Road, Suite #4 Anchorage, Alaska (907)
") Patient Intake Form Gray Chiropractic Health Clinic LLC 360 East International Airport Road, Suite #4 Anchorage, Alaska 99518 (907)563-7700 PATIENT DEMOGRAPHICS Today's Date: *** PLEASE WRITE IN BLACK
Patient Intake Form Gray Chiropractic Health Clinic LLC 360 East International Airport Road, Suite #4 Anchorage, Alaska 99518 (907)563-7700 PATIENT DEMOGRAPHICS Today's Date: *** PLEASE WRITE IN BLACK
LIST YOUR HEALTH CONCERNS BELOW
 LOCATION COMING SOON Lakewood Ranch, FL 32402 941.877.1507 Name Date / / Age Male/Female Address City State Zip Phone: Home Cell Cell Phone Provider Email Date of Birth / / Employer s Name Position Single
LOCATION COMING SOON Lakewood Ranch, FL 32402 941.877.1507 Name Date / / Age Male/Female Address City State Zip Phone: Home Cell Cell Phone Provider Email Date of Birth / / Employer s Name Position Single
Current Health Information
 Name: : / / Current Health Information List your health concerns below: Health Concerns: (List according to severity) Rate of Severity 1 = Mild 10 = Unbear able When did the Symptom s Start? Are the Symptoms
Name: : / / Current Health Information List your health concerns below: Health Concerns: (List according to severity) Rate of Severity 1 = Mild 10 = Unbear able When did the Symptom s Start? Are the Symptoms
CHIROPRACTIC, PLLC. & Wellness Center. Terms of Acceptance
 CHIROPRACTIC, PLLC & Wellness Center Terms of Acceptance When a member of Vital Chiropractic Center seeks chiropractic health care and we accept a member for such care, it is essential for both to be working
CHIROPRACTIC, PLLC & Wellness Center Terms of Acceptance When a member of Vital Chiropractic Center seeks chiropractic health care and we accept a member for such care, it is essential for both to be working
Revelation Chiropractic Health Profile
 Revelation Chiropractic Health Profile Name Date / Age Male / Female Address Apt City Zip Phone Numbers: Home Cell Circle best number to reach you at: Home Cell Date of Birth / / Occupation Email Address
Revelation Chiropractic Health Profile Name Date / Age Male / Female Address Apt City Zip Phone Numbers: Home Cell Circle best number to reach you at: Home Cell Date of Birth / / Occupation Email Address
SMITH CHIROPRACTIC HEALTH PROFILE Today s Date:
 SMITH CHIROPRACTIC HEALTH PROFILE Today s Date: Name: Age: Male/Female DOB: Address: City: State: Zip: Home Phone:_ Cell: Cell Phone Provider: SSN#: Email Address: Single/Married/Divorced/Widowed Spouse
SMITH CHIROPRACTIC HEALTH PROFILE Today s Date: Name: Age: Male/Female DOB: Address: City: State: Zip: Home Phone:_ Cell: Cell Phone Provider: SSN#: Email Address: Single/Married/Divorced/Widowed Spouse
Chiropractic Health Dr. Art Vanderhoef
 Patient Information Form Chiropractic Health Dr. Art Vanderhoef File # Name Address City State Zip Home Phone ( ) Work Phone ( ) Cell Phone ( ) Email Address How do you prefer to be contacted? Mail Home
Patient Information Form Chiropractic Health Dr. Art Vanderhoef File # Name Address City State Zip Home Phone ( ) Work Phone ( ) Cell Phone ( ) Email Address How do you prefer to be contacted? Mail Home
FRAME CHIROPRACTIC South Price Road, Suite D-110 Tempe, Arizona Phone: Fax:
 3330 South Price Road, Suite D-110 Tempe, Arizona 85282 Phone: 480.345.2080 Fax: 480.345.2199 W E L C O M E ABOUT YOU (please print) Today s Date: Patient Name: DOB: Age: SS#: Mailing Address: City: State:
3330 South Price Road, Suite D-110 Tempe, Arizona 85282 Phone: 480.345.2080 Fax: 480.345.2199 W E L C O M E ABOUT YOU (please print) Today s Date: Patient Name: DOB: Age: SS#: Mailing Address: City: State:
Health and History Assessment ACCOUNT #: HIPPA: CTT:
 ACTION Chiropractor LLC Health and History Assessment ACCOUNT #: HIPPA: CTT: NAME: SEX: M/ F BIRTHDATE: / / ADDRESS: CITY: STATE: Zip: PHONE # s: HOME: ( ) WORK: ( ) CELL: ( ) HEIGHT: WEIGHT: MARITAL STATUS:
ACTION Chiropractor LLC Health and History Assessment ACCOUNT #: HIPPA: CTT: NAME: SEX: M/ F BIRTHDATE: / / ADDRESS: CITY: STATE: Zip: PHONE # s: HOME: ( ) WORK: ( ) CELL: ( ) HEIGHT: WEIGHT: MARITAL STATUS:
Welcome To Our Office
 Welcome To Our Office Mission Statement Our office is dedicated to educating and adjusting as many families as possible towards optimal health through natural chiropractic care. We believe the greatest
Welcome To Our Office Mission Statement Our office is dedicated to educating and adjusting as many families as possible towards optimal health through natural chiropractic care. We believe the greatest
Dr. Charles E. Copeland, DC Highland Chiropractic
 Highland Chiropractic Name: Birth Date: / / Gender M / F Occupation: Address: Employer: City: State: Zip: How did you hear about us? Home Phone: ( ) - Preferred Phone to Contact Work Phone: ( ) - Home
Highland Chiropractic Name: Birth Date: / / Gender M / F Occupation: Address: Employer: City: State: Zip: How did you hear about us? Home Phone: ( ) - Preferred Phone to Contact Work Phone: ( ) - Home
Acknowledgment of Clinic Terms
 Acknowledgment of Clinic Terms Our GOAL The goal of CHIRO-FIT, Inc. is to detect and correct subluxations of the spine and body. We do not focus on the treatment of pain and disease, instead aim to help
Acknowledgment of Clinic Terms Our GOAL The goal of CHIRO-FIT, Inc. is to detect and correct subluxations of the spine and body. We do not focus on the treatment of pain and disease, instead aim to help
PATIENT INTAKE FORM Health & Wellness
 PATIENT INTAKE FORM Health & Wellness GRAFFEO CHIROPRACTIC CLINIC Joseph Graffeo, DC, PC Date: ABOUT YOU 16248 NE Glisan St Portland, OR 97230 First Name Last Name Middle Name Email Address Street Address
PATIENT INTAKE FORM Health & Wellness GRAFFEO CHIROPRACTIC CLINIC Joseph Graffeo, DC, PC Date: ABOUT YOU 16248 NE Glisan St Portland, OR 97230 First Name Last Name Middle Name Email Address Street Address
Name First Middle Initial Last Today s Date. Address Street City State Zip. Primary Phone # Cell # . Your Occupation Employer
 Name First Middle Initial Last Today s Date Address Street City State Zip Date of Birth Age Social Security # Sex: Male Female mm/dd/year Primary Phone # Cell # Email Emergency Contact Name Number Marital
Name First Middle Initial Last Today s Date Address Street City State Zip Date of Birth Age Social Security # Sex: Male Female mm/dd/year Primary Phone # Cell # Email Emergency Contact Name Number Marital
Describe the pain and it s location:
 WELCOME TO ZIVKOVIC CHIROPRACTIC CENTER DATE: Please print clearly and fill in completely. ABOUT YOU: Patient Name:_ What do you prefer to be called:_ SS# Street Address City State Zip Date of Birth: Age:
WELCOME TO ZIVKOVIC CHIROPRACTIC CENTER DATE: Please print clearly and fill in completely. ABOUT YOU: Patient Name:_ What do you prefer to be called:_ SS# Street Address City State Zip Date of Birth: Age:
Welcome to the Dynamic Essence tribe!
 Welcome to the Dynamic Essence tribe! 746 Wealthy St SE Grand Rapids, MI 49503 P: 989.573.1170 DynamicEssenceChiropractic@gmail.com We empower you to reclaim your power. Elevate your unique expression.
Welcome to the Dynamic Essence tribe! 746 Wealthy St SE Grand Rapids, MI 49503 P: 989.573.1170 DynamicEssenceChiropractic@gmail.com We empower you to reclaim your power. Elevate your unique expression.
Patient Information Form
 Patient Information Name: First Middle Last Address: City: State: Zip: Telephone: Home Cell Work Date of Birth: Social Security Number: (SSN is only needed if getting super-bills for potential insurance
Patient Information Name: First Middle Last Address: City: State: Zip: Telephone: Home Cell Work Date of Birth: Social Security Number: (SSN is only needed if getting super-bills for potential insurance
PATIENT REGISTRATION
 PATIENT REGISTRATION Last Name First Name MI Street Address City State Zip Code Social Security # - - Email Address Home Phone( ) Cell Phone( ) Sex Male Female of Birth Age Marital Status Married Single
PATIENT REGISTRATION Last Name First Name MI Street Address City State Zip Code Social Security # - - Email Address Home Phone( ) Cell Phone( ) Sex Male Female of Birth Age Marital Status Married Single
Physical Evidence Chiropractic 7035 Beracasa Way Suite 103 Boca Raton FL, Phone# (561) Fax# (561)
 Fax# (561)") 7035 Beracasa Way Suite 103 Boca Raton FL, 33433 Phone# (561)361-4888 Fax# (561)361-4999 Date File # PERSONAL HISTORY Last Name First Name Address City State Zip Date of Birth Age Social Security # Circle
7035 Beracasa Way Suite 103 Boca Raton FL, 33433 Phone# (561)361-4888 Fax# (561)361-4999 Date File # PERSONAL HISTORY Last Name First Name Address City State Zip Date of Birth Age Social Security # Circle
Welcome To Corporate Chiropractic Works!
 Welcome To Corporate Chiropractic Works! When a person seeks the services of a chiropractor, it is important to fully understand the purpose and intent of that particular chiropractor and the chiropractic
Welcome To Corporate Chiropractic Works! When a person seeks the services of a chiropractor, it is important to fully understand the purpose and intent of that particular chiropractor and the chiropractic
Rise Chiropractic 239 S. French Broad Ave Asheville, NC
 Rise Chiropractic 239 S. French Broad Ave Asheville, NC 28801 828.989.8369 1 Name: of Birth: Age: Sex: M F Address: City/State: Zip: Phone: (H) (W) (C) SS# Email: Occupation: Employer: Marital Status:
Rise Chiropractic 239 S. French Broad Ave Asheville, NC 28801 828.989.8369 1 Name: of Birth: Age: Sex: M F Address: City/State: Zip: Phone: (H) (W) (C) SS# Email: Occupation: Employer: Marital Status:
What s the name of your position?
 What s the name of your position? What are some basic work responsibilities (e.g primarily front desk/administration, light lifting or heavy liftingplease indicate pounds)? CONSENT FORM FOR USE AND DISCLOSURE
What s the name of your position? What are some basic work responsibilities (e.g primarily front desk/administration, light lifting or heavy liftingplease indicate pounds)? CONSENT FORM FOR USE AND DISCLOSURE
3. How Long Has This Been An Issue?
 NEW PATIENT INTAKE FORM Aspire Chiropractic 124 W Harwood Rd. Ste. B Hurst, TX 76054 Name: Occupation: DOB: Age: Sex: Male Female Employer: Marital Status: Single Married Other Name/Age of Kids: Phone:
NEW PATIENT INTAKE FORM Aspire Chiropractic 124 W Harwood Rd. Ste. B Hurst, TX 76054 Name: Occupation: DOB: Age: Sex: Male Female Employer: Marital Status: Single Married Other Name/Age of Kids: Phone:
Pregnant Patient Introduction Form Form
 1820 S. Westnedge Ave. Suite #1. Kalamazoo, MI 49008 269.344.5551 antoniottichiropractic.com Form : Patient name: Address: Estimated Due : Home Phone: INTRODUCTION MEDICAL HISTORY City, State, Zip: Work
1820 S. Westnedge Ave. Suite #1. Kalamazoo, MI 49008 269.344.5551 antoniottichiropractic.com Form : Patient name: Address: Estimated Due : Home Phone: INTRODUCTION MEDICAL HISTORY City, State, Zip: Work
PERSONAL INFORMATION. Date of Birth Age (Last) (First) (M.I.) Address City/State Zip. Phone # Home Work Cell
 (First) (M.I.) Address City/State Zip. Phone # Home Work Cell") *If the reason for your visit is due to a worker s compensation injury or an automobile accident, please inform the front desk immediately. PERSONAL INFORMATION of Birth Age (Last) (First) (M.I.) Address
*If the reason for your visit is due to a worker s compensation injury or an automobile accident, please inform the front desk immediately. PERSONAL INFORMATION of Birth Age (Last) (First) (M.I.) Address
Patient Profile. Full Name: Address: Work Phone: Date of Birth: Social Security #: (Circle One) Full Time / Part Time. Emergency Contact: Number:
 Full Time / Part Time. Emergency Contact: Number:") Patient Profile Full Name: Address: City: State: Zip Code: Home Phone: Cell Phone: Work Phone: Date of Birth: Social Security #: Email Address: Employer: (Circle One) Full Time / Part Time Emergency Contact:
Patient Profile Full Name: Address: City: State: Zip Code: Home Phone: Cell Phone: Work Phone: Date of Birth: Social Security #: Email Address: Employer: (Circle One) Full Time / Part Time Emergency Contact:
New Patient Form Welcome!
 New Patient Form Welcome! Last First Middle Initial DOB Address City ST ZIP Phone (H) (C) Email Occupation Employer Relationship Status S M W D Spouse s Name DOB Children s Names and Ages Have you had
New Patient Form Welcome! Last First Middle Initial DOB Address City ST ZIP Phone (H) (C) Email Occupation Employer Relationship Status S M W D Spouse s Name DOB Children s Names and Ages Have you had
Cascadia Chiropractic Centre
 Name: Address: Dr. Simpson Leung Cascadia Chiropractic Centre New Patient Information & Clinical Record Date: City: Province: Postal Code: Phone: Cell: Work Phone: Date of Birth: E-mail Address: Care Card
Name: Address: Dr. Simpson Leung Cascadia Chiropractic Centre New Patient Information & Clinical Record Date: City: Province: Postal Code: Phone: Cell: Work Phone: Date of Birth: E-mail Address: Care Card
CONDITIONS OF SERVICES RENDERED
 CONDITIONS OF SERVICES RENDERED FINANCIAL AGREEMENT: I agree, whether I sign as agent or as patient, that in consideration of the services to be rendered to the patient, I hereby individually obligate
CONDITIONS OF SERVICES RENDERED FINANCIAL AGREEMENT: I agree, whether I sign as agent or as patient, that in consideration of the services to be rendered to the patient, I hereby individually obligate
Child s Legal Name: Nickname: Male Female. Birth Date: Age: School: Grade: FATHER STEPMOTHER GUARDIAN? Insured s Name: D.O.B. Social Security #:
 Welcome Welcome to our practice! We strive to make each of your child s visits pleasant and comfortable. Our goal is to teach your child oral habits which will help keep their smile beautiful for their
Welcome Welcome to our practice! We strive to make each of your child s visits pleasant and comfortable. Our goal is to teach your child oral habits which will help keep their smile beautiful for their
LIST YOUR HEALTH CONCERNS BELOW
 Date / / HEALTH PROFILE T C E X Name D.O.B. / / Age Male/Female Address City State Zip Phone: Home Cell Cell Phone Carrier: Email Address Occupation Employer s Name _ Single / Married / Divorced / Widowed
Date / / HEALTH PROFILE T C E X Name D.O.B. / / Age Male/Female Address City State Zip Phone: Home Cell Cell Phone Carrier: Email Address Occupation Employer s Name _ Single / Married / Divorced / Widowed
Patient Intake Form Gray Chiropractic Health Clinic LLC 360 East International Airport Road, Suite #4 Anchorage, Alaska (907)
") Patient Intake Form Gray Chiropractic Health Clinic LLC 360 East International Airport Road, Suite #4 Anchorage, Alaska 99518 (907)563 7700 PATIENT DEMOGRAPHICS Today's Date: Name: Birth Date: Age: Male
Patient Intake Form Gray Chiropractic Health Clinic LLC 360 East International Airport Road, Suite #4 Anchorage, Alaska 99518 (907)563 7700 PATIENT DEMOGRAPHICS Today's Date: Name: Birth Date: Age: Male
Dr. Janet L. Yarger 510 Baxter Road, Suite 8, Chesterfield, MO
 Registration Form Date: / / Name: Social Security #: - - Address: City: State: Zip Code: Home Phone #: ( ) - Age: Date of Birth / / Cell Phone #: ( ) - Best Phone to call you at: HOME/CELL/WORK Email Address:
Registration Form Date: / / Name: Social Security #: - - Address: City: State: Zip Code: Home Phone #: ( ) - Age: Date of Birth / / Cell Phone #: ( ) - Best Phone to call you at: HOME/CELL/WORK Email Address:
Lions Sight & Hearing Foundation Phone: Fax: Hearing Aid: Request for assistance
 Lions Sight & Hearing Foundation Phone: 602-954-1723 Fax: 602-954-1768 Hearing Aid: Request for assistance 3427 N 32 nd Street office use only Date received Case number Applicant: (Name; please print clearly)
Lions Sight & Hearing Foundation Phone: 602-954-1723 Fax: 602-954-1768 Hearing Aid: Request for assistance 3427 N 32 nd Street office use only Date received Case number Applicant: (Name; please print clearly)
Personal Information. Reason for Seeking Care. What is your reason for seeking care at Strive Chiropractic?
 Adult Intake Form Date: Personal Information First Name: M.I.: Last Name: Preferred Name: Social Security Number: Address: City / State / Zip: Cell Phone: ( ) Alternate Phone: ( ) Text Reminders: Y N Before
Adult Intake Form Date: Personal Information First Name: M.I.: Last Name: Preferred Name: Social Security Number: Address: City / State / Zip: Cell Phone: ( ) Alternate Phone: ( ) Text Reminders: Y N Before
Our office is located at 2030 Drew Street, Clearwater FL, We are on Drew Street, in between N.E Old Coachman Road and Hercules Avenue.
 Dear New Patient, Thank you for choosing Dennis M. Lox, M.D to participate in your healthcare. We realize that you could have chosen any other office, so we are honored that you have chosen us. While Dr.
Dear New Patient, Thank you for choosing Dennis M. Lox, M.D to participate in your healthcare. We realize that you could have chosen any other office, so we are honored that you have chosen us. While Dr.
Welcome to Manna Family Chiropractic!
 Welcome to Manna Family Chiropractic! Today s date Who should we thank for referring you here? Is your visit today regarding you, or your whole family? Family Just Me Your name Date of Birth Street Address
Welcome to Manna Family Chiropractic! Today s date Who should we thank for referring you here? Is your visit today regarding you, or your whole family? Family Just Me Your name Date of Birth Street Address
General Information: (Circle One) (Circle One) Primary Insured's Information Skip if you are primary
 (Circle One) Primary Insured's Information Skip if you are primary") General Information: First Name: Middle Initial: Last Name: Suffix: Called Name: Street Address: City: State: Zip Code: Home Phone: ( ) - Work Phone: ( ) - Cell Phone: ( ) - Email Address: Marital Status:
General Information: First Name: Middle Initial: Last Name: Suffix: Called Name: Street Address: City: State: Zip Code: Home Phone: ( ) - Work Phone: ( ) - Cell Phone: ( ) - Email Address: Marital Status:
Welcome to our Office!
 Welcome to our Office! Please fill out our Health Record as completely and accurate as possible. If you have any questions, please don t hesitate to ask one of our qualified team members. It is our pleasure
Welcome to our Office! Please fill out our Health Record as completely and accurate as possible. If you have any questions, please don t hesitate to ask one of our qualified team members. It is our pleasure
Which physician are you scheduled to see? Scheduled Appointment Date: As a reminder: Please arrive minutes prior to your scheduled appointment.
 Which physician are you scheduled to see? Scheduled Appointment : As a reminder: Please arrive 15-20 minutes prior to your scheduled appointment. Please bring the following on the day of your scheduled
Which physician are you scheduled to see? Scheduled Appointment : As a reminder: Please arrive 15-20 minutes prior to your scheduled appointment. Please bring the following on the day of your scheduled
GARDEN STATE SLEEP CENTER REGISTRATION FORM PATIENT INFORMATION:
 GARDEN STATE SLEEP CENTER REGISTRATION FORM (Please Print) Today s Date: Primary Care Physician: PATIENT INFORMATION: Last Name: First: Middle: Mr. Miss Dr. Mrs. Ms. Marital Status (Please check one) Single
GARDEN STATE SLEEP CENTER REGISTRATION FORM (Please Print) Today s Date: Primary Care Physician: PATIENT INFORMATION: Last Name: First: Middle: Mr. Miss Dr. Mrs. Ms. Marital Status (Please check one) Single
JACKSONVILLE SPEECH & HEARING CENTER PATIENT INFORMATION FORM PEDIATRIC (CHILD) - AUDIOLOGY Please Print
 - AUDIOLOGY Please Print") JACKSONVILLE SPEECH & HEARING CENTER PATIENT INFORMATION FORM PEDIATRIC (CHILD) - AUDIOLOGY Please Print Referring Physician: Child s (Patient) Name: LAST FIRST MIDDLE Gender: Male Female Date of Birth:
JACKSONVILLE SPEECH & HEARING CENTER PATIENT INFORMATION FORM PEDIATRIC (CHILD) - AUDIOLOGY Please Print Referring Physician: Child s (Patient) Name: LAST FIRST MIDDLE Gender: Male Female Date of Birth:
PATIENT FEE SCHEDULE As of January 1, 2017
 TERMS OF ACCEPTANCE When a patient seeks chiropractic care and we accept such a patient for care, it is essential for both to be working towards the same objective. Chiropractic has only one goal. It is
TERMS OF ACCEPTANCE When a patient seeks chiropractic care and we accept such a patient for care, it is essential for both to be working towards the same objective. Chiropractic has only one goal. It is
NPM INTAKE FORM. Home Phone No.: Work Phone No.: Cell Phone:
 NPM INTAKE FORM INFORMATION: Name: Chosen Name (What would you like to be called?): Address: Date: Age: City/State/Zip: Home Phone No.: Work Phone No.: Cell Phone: Email Address: Date of Birth: Occupation:
NPM INTAKE FORM INFORMATION: Name: Chosen Name (What would you like to be called?): Address: Date: Age: City/State/Zip: Home Phone No.: Work Phone No.: Cell Phone: Email Address: Date of Birth: Occupation:
Luker Chiropractic Health Questionnaire
 Luker Chiropractic Health Questionnaire Name: D.O.B.: Address: City: State: Zip: Home Phone: Cell: Email: Male/Female Marital Status: M W D S Age: SS# Occupation: Employer: Spouse Name: # of Children:
Luker Chiropractic Health Questionnaire Name: D.O.B.: Address: City: State: Zip: Home Phone: Cell: Email: Male/Female Marital Status: M W D S Age: SS# Occupation: Employer: Spouse Name: # of Children:
CONTINUUM CHIROPRACTIC ADULT HEALTH HISTORY FORM
 CONTINUUM CHIROPRACTIC ADULT HEALTH HISTORY FORM Today s Date PERSONAL DATA Legal Name Preferred Name Age Date of Birth Height Weight Home Address City State Zip Home phone ( ) Business Phone ( ) Cell
CONTINUUM CHIROPRACTIC ADULT HEALTH HISTORY FORM Today s Date PERSONAL DATA Legal Name Preferred Name Age Date of Birth Height Weight Home Address City State Zip Home phone ( ) Business Phone ( ) Cell
Application for Patient
 Application for Patient First Name: M.I.: Last Name: Date: Address: City: State: Zip: SS#: - - Age: DOB: / / Male / Female Email: Home #: Cell # Work # Primary Care Physician: Do we have permission to
Application for Patient First Name: M.I.: Last Name: Date: Address: City: State: Zip: SS#: - - Age: DOB: / / Male / Female Email: Home #: Cell # Work # Primary Care Physician: Do we have permission to
PERSONAL INFORMATION. First Name: M.I.: Last Name: Preferred Name: Social Security Number: Address: City / State / Zip:
 ADULT INTAKE FORM Date: PERSONAL INFORMATION First Name: M.I.: Last Name: Preferred Name: Social Security Number: Address: City / State / Zip: Cell Phone: ( ) Alternate Phone: ( Text Reminders: Y N Before
ADULT INTAKE FORM Date: PERSONAL INFORMATION First Name: M.I.: Last Name: Preferred Name: Social Security Number: Address: City / State / Zip: Cell Phone: ( ) Alternate Phone: ( Text Reminders: Y N Before
634 N. STATE STREET, WESTERVILLE OH, (614) 901-WELL
 901-WELL") eas 634 N. STATE STREET, WESTERVILLE OH, 43082 (614) 901-WELL www.abilitychiro.com Name: Age: Date: Address: City: State: Zip Code: Alternate Address: City: State: Zip Code: Cell Phone: ( ) Cell Phone
eas 634 N. STATE STREET, WESTERVILLE OH, 43082 (614) 901-WELL www.abilitychiro.com Name: Age: Date: Address: City: State: Zip Code: Alternate Address: City: State: Zip Code: Cell Phone: ( ) Cell Phone
HEALTH RECORD REASON FOR THIS VISIT ABOUT YOU ABOUT YOUR SPOUSE HEALTH HABITS EXPERIENCE WITH CHIROPRACTIC
 HEALTH RECORD ABOUT YOU REASON FOR THIS VISIT Name Address City State Zip _Home phone Birth date Cell Phone Age Gender Number of children Employer Work address Work phone Occupation Marital Status Social
HEALTH RECORD ABOUT YOU REASON FOR THIS VISIT Name Address City State Zip _Home phone Birth date Cell Phone Age Gender Number of children Employer Work address Work phone Occupation Marital Status Social
First Name: Middle Initial: Last Name: Address Line 1: Address Line 2: Home Phone: ( ) - Work Phone: ( ) - Sex: Female Male Other
 - Work Phone: ( ) - Sex: Female Male Other") Date: Bella Vita Chiropractic & Wellness 610 Eastbury Drive Suite 3 Iowa City, IA 52245 (319) 887.6992 Title: Mr. Mrs. Ms Miss First Name: Middle Initial: Last Name: Address Line 1: Address Line 2: City:
Date: Bella Vita Chiropractic & Wellness 610 Eastbury Drive Suite 3 Iowa City, IA 52245 (319) 887.6992 Title: Mr. Mrs. Ms Miss First Name: Middle Initial: Last Name: Address Line 1: Address Line 2: City:
Cascadia Chiropractic Centre
 Name: Cascadia Chiropractic Centre New Patient Information & Clinical Record Date: Date of Birth: Your age: Care Card #: Address: City/Prov: Postal Code: Phone: Cell: Work Phone: E-mail Address: Marital
Name: Cascadia Chiropractic Centre New Patient Information & Clinical Record Date: Date of Birth: Your age: Care Card #: Address: City/Prov: Postal Code: Phone: Cell: Work Phone: E-mail Address: Marital
Family First Chiropractic
 Personal Information Title: (Check one) Mr. Mrs. Ms. Miss Other First Name Middle Initial Last Name Street City State Zip Code Email Home Phone ( ) - Cell Phone ( ) - Date of Birth / / Sex: Male Female
Personal Information Title: (Check one) Mr. Mrs. Ms. Miss Other First Name Middle Initial Last Name Street City State Zip Code Email Home Phone ( ) - Cell Phone ( ) - Date of Birth / / Sex: Male Female
The Spinal Tuning Chiropractic Center s Health Profile Application and Practice Entrance & Policy Forms. Table Of Contents:
 The Spinal Tuning Chiropractic Center s Health Profile Application and Practice Entrance & Policy Forms Table Of Contents: Health Profile Application, Pages 1&2: This standard health profile application
The Spinal Tuning Chiropractic Center s Health Profile Application and Practice Entrance & Policy Forms Table Of Contents: Health Profile Application, Pages 1&2: This standard health profile application
APPLICATION FOR SERVICES
 APPLICATION FOR SERVICES CLIENT - PERSONAL INFORMATION First Name M.I. Last Name Today s Street Address City State Zip Birth date Home phone (ok to leave msg? Y - N) Cell phone (ok to leave msg? Y - N
APPLICATION FOR SERVICES CLIENT - PERSONAL INFORMATION First Name M.I. Last Name Today s Street Address City State Zip Birth date Home phone (ok to leave msg? Y - N) Cell phone (ok to leave msg? Y - N
Patient Name: 1831 N. Belcher RD Suite C3 Clearwater, FL Phone: Fax: Authorization to Release Protected Information Da
 Patient Name: 1831 N. Belcher RD Suite C3 Clearwater, FL 33765 Phone: 727-754-4959 Fax: 727-754-5910 Authorization to Release Protected Information Date of Birth: Instructions: Following section to be
Patient Name: 1831 N. Belcher RD Suite C3 Clearwater, FL 33765 Phone: 727-754-4959 Fax: 727-754-5910 Authorization to Release Protected Information Date of Birth: Instructions: Following section to be
New Patient Paperwork
 New Patient Paperwork Date: Phone: Patient: Last Name First Name Initial Street Address: City/State/Zip Code: Sex: M F Age: Birthdate: Single Married Widowed Separated Divorced Email: Newsletter? Y N Insured
New Patient Paperwork Date: Phone: Patient: Last Name First Name Initial Street Address: City/State/Zip Code: Sex: M F Age: Birthdate: Single Married Widowed Separated Divorced Email: Newsletter? Y N Insured
TRANSITION OF CARE APPLICATION
 Dear Member: Thank you for enrolling in MedStar Medicare Choice. You may currently be receiving services from healthcare providers that are not part of the MedStar Medicare Choice Provider Network. An
Dear Member: Thank you for enrolling in MedStar Medicare Choice. You may currently be receiving services from healthcare providers that are not part of the MedStar Medicare Choice Provider Network. An
th Street Urbandale, IA YOST
 YfC 3993 100th Street Urbandale, IA 50322 515.278.YOST www.yostfamilychiropractic.com Demographics: Language (Primary) Race: Unspecified American Indian or Alaska Native Black or African American Other
YfC 3993 100th Street Urbandale, IA 50322 515.278.YOST www.yostfamilychiropractic.com Demographics: Language (Primary) Race: Unspecified American Indian or Alaska Native Black or African American Other
Revitalize, Regenerate & Restore Office of Dr. Kashi Rai. Health Coaching Packet
 1 Health Coaching Packet A health coach is knowledgeable in the process of health behavior modification. We work in partnership with our clients to assist them to enhance personal accountability, set goals
1 Health Coaching Packet A health coach is knowledgeable in the process of health behavior modification. We work in partnership with our clients to assist them to enhance personal accountability, set goals
Rupp Chiropractic FAMILY PHYSICIAN FEMALES: ARE YOU PREGNANT, OR A CHANCE YOU MIGHT BE PREGNANT? YES / NO HOW WERE YOU REFERRED TO OUR OFFICE?
 PATIENT INFORMATION NAME DATE ADDRESS CITY STATE ZIP HOME # CELL # WORK # E MAIL ADDRESS SOCIAL SECURITY # I WOULD LIKE TO RECEIVE EMAIL APPOINTMENT REMINDERS [YES] [NO] RACE: AMERICAN INDIAN ALASKA NATIVE
PATIENT INFORMATION NAME DATE ADDRESS CITY STATE ZIP HOME # CELL # WORK # E MAIL ADDRESS SOCIAL SECURITY # I WOULD LIKE TO RECEIVE EMAIL APPOINTMENT REMINDERS [YES] [NO] RACE: AMERICAN INDIAN ALASKA NATIVE
Sincerely, Dr. Justin & Woodbury Spine Staff
 Welcome to our office! We are sure that you will be provided the most appropriate and professional chiropractic care possible. Our most important goal is the constant improvement and maintenance of your
Welcome to our office! We are sure that you will be provided the most appropriate and professional chiropractic care possible. Our most important goal is the constant improvement and maintenance of your
CORNERSTONE PAIN MANAGEMENT
 SECONDARY INSURANCE PRIMARY INSURANCE CORNERSTONE PAIN MANAGEMENT PATIENT INFORMATION First Name: Dr. Mr. Mrs. Ms. Miss MI: Last Name: Social Security: Age: Date of Birth: Gender: Address: City: State:
SECONDARY INSURANCE PRIMARY INSURANCE CORNERSTONE PAIN MANAGEMENT PATIENT INFORMATION First Name: Dr. Mr. Mrs. Ms. Miss MI: Last Name: Social Security: Age: Date of Birth: Gender: Address: City: State:
Tell Us About Your Child. Who is Accompanying Your Child Today? Parent Information. Primary Dental Insurance
 1 Today s Date: 2 (225) 664-2646 (225) 664-2640 (fax) 245 VETERANS BLVD. DENHAM SPRINGS, LA 70726 Who is Accompanying Your Child Today? Name: Relation: Do you have legal custody of this child? Yes No Tell
1 Today s Date: 2 (225) 664-2646 (225) 664-2640 (fax) 245 VETERANS BLVD. DENHAM SPRINGS, LA 70726 Who is Accompanying Your Child Today? Name: Relation: Do you have legal custody of this child? Yes No Tell
Patient Name Date of Birth / / Today s Date / /
 Dr. Mark Valente Dr. Andy Indresano Board Certified, Fellowship Trained Phone. 972.707.0005 Fax. 888.992.6199 DISCspine.com New Patient Intake Form Name First MI Last Street Address Apt # _ City _ State
Dr. Mark Valente Dr. Andy Indresano Board Certified, Fellowship Trained Phone. 972.707.0005 Fax. 888.992.6199 DISCspine.com New Patient Intake Form Name First MI Last Street Address Apt # _ City _ State
Initial Visit Forms. Life in Motion Chiropractic & Wellness 6139 Route 96 -Suite 1 Farmington, NY (585)
") Initial Visit Forms 6139 Route 96 -Suite 1 Patient Name: Patient Intake Form Name: Date: Address: City: State: Zip: Home #: ( ) Cell #: ( ) Work #: ( ) E-mail: Preferred method of contact: Date of Birth:
Initial Visit Forms 6139 Route 96 -Suite 1 Patient Name: Patient Intake Form Name: Date: Address: City: State: Zip: Home #: ( ) Cell #: ( ) Work #: ( ) E-mail: Preferred method of contact: Date of Birth:
CHIROPRACTIC NEW PATIENT FORM REASON FOR VISIT
 DR. ANN IZARD, B.COMM, DC DOCTOR OF CHIROPRACTIC 4353 HASTINGS STREET BURNABY, BC V5C 2J7 TEL: 604.293.2941 FAX: 604.298.2941 WWW.BHIHC.COM WWW.ANNIZARD.COM FULL NAME: DATE OF BIRTH (DD/MM/YYYY): STREET
DR. ANN IZARD, B.COMM, DC DOCTOR OF CHIROPRACTIC 4353 HASTINGS STREET BURNABY, BC V5C 2J7 TEL: 604.293.2941 FAX: 604.298.2941 WWW.BHIHC.COM WWW.ANNIZARD.COM FULL NAME: DATE OF BIRTH (DD/MM/YYYY): STREET
Access Endodontics Marat Tselnik, DDS -PRACTICE LIMITED TO ENDODONTICS-
 Access Endodontics Marat Tselnik, DDS -PRACTICE LIMITED TO ENDODONTICS- REFERRED BY: TODAY S DATE: PATIENT NAME HOME PHONE (LAST) (FIRST) (MIDDLE) E-MAIL CELL PHONE HOME ADDRESS (STREET) (CITY) (STATE)
Access Endodontics Marat Tselnik, DDS -PRACTICE LIMITED TO ENDODONTICS- REFERRED BY: TODAY S DATE: PATIENT NAME HOME PHONE (LAST) (FIRST) (MIDDLE) E-MAIL CELL PHONE HOME ADDRESS (STREET) (CITY) (STATE)