Stacey Dent, D.C., B.C.A.O Three Notch Rd. Unit 104 Hollywood, MD P: F: HarborBayChiropractic.
|
|
|
- Ashley Day
- 5 years ago
- Views:
Transcription

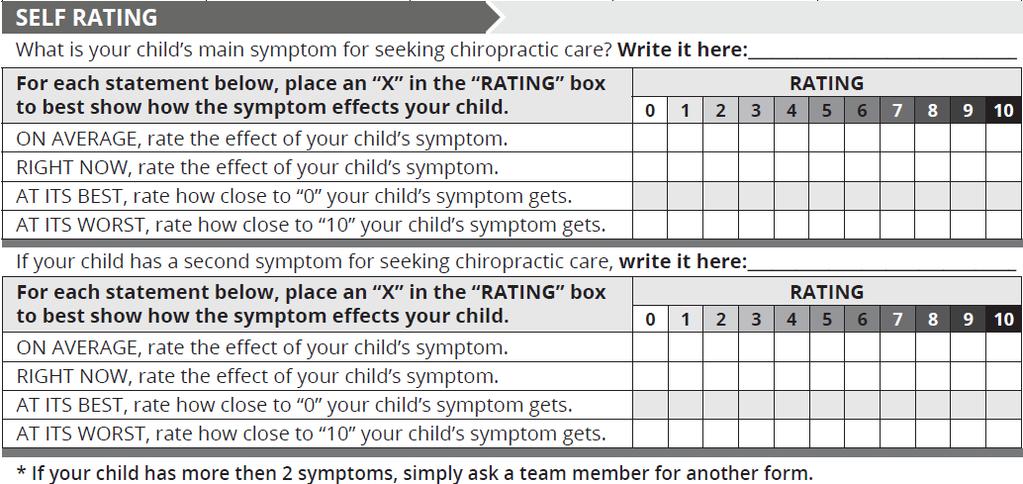
: I wish to be called at home work cell other (check all that apply) reguarding my child s care.")

1 Stacey Dent, D.C., B.C.A.O Three Notch Rd. Unit 104 Hollywood, MD P: F: HarborBayChiropractic.com Welcome to Harbor Bay Clinic of Chiropractic! (For any question that does not apply to you, simply respond N/A for Not Applicable.) Today s Date: Have you ever received chiropractic care? No Yes, (Name of Doctor): I wish to be called at home work cell other (check all that apply) reguarding my child s care. I do, I do not give permission to leave relevant medical inforamation on my answering machine or voice mail. I do, I do not want relevant medical information shared with the person who may answer the telephone. The name(s) of the individual(s) with whom you may leave pertenent information are: Method of Payment: Cash Check Credit Card (V, MC, Disc, AmEx) Do you have Medicare? Y N Insurance. Primary: Secondary:
2

3
4
5 CONDITION SELF SPOUSE SON(S) DAUGHTER(S) FATHER MOTHER SIBLING(S) Acid Reflux/GERD ADD/ADHD Anxiety Arthritis/Joint Pain Asthma/Allergies Autoimmune Disease Bed Wetting Birth Defect Cancer Colic Convulsions/Epilepsy Deceased Depression/Mood Changes Diabetes Digestive Problems Ear Problems/Hearing Loss Fibromyalgia/Muscle Pain Frequent Cold/Flu Gall Bladder Problems High/Low Blood Pressure HIV/AIDS Impotence/Sexual Dysfunction Kidney Problems Learning Disability Liver Problems Menstrual Dysfunction Migraines Neck Pain/Back Pain/Disc Problems Prostate Problems Sciatica Scoliosis Sinus/Drainage Problems Skin Problems Sleep Problems TMJ Dysfunction Tongue or Lip Tie Thyroid Problems Tremors Vertigo/Dizziness Vision Problems Other:
6 At Harbor Bay Clinic of Chiropractic the term Practice Member is used for those that have suffered either an injury or are seeking wellness rather than symptom management. A Practice Member is an active participant in his or her chiropractic care, and is therefore, invited to ask any questions or express any concerns that he or she may have. Practice members can expect quality service and leadership as they regain control of their health. First, a complete analysis of your spine will be administered to detect the presence of vertebral subluxations and to monitor your progress. Please read and sign this form stating that you understand the items explained below. If there is anything that is unclear please ask questions before you sign. If you refuse to sign this form the doctor reserves the right to refuse care. I hereby consent to give the doctor of chiropractic, and anyone working in the Harbor Bay Clinic of Chiropractic office, authorized by the chiropractor, permission and authority to care for my child (the minor listed here: for whom I am legally responsible). Chiropractic tests, diagnosis, analysis and adjustments are very safe and beneficial. However, in rare cases, underlying physical defects, deformities or pathologies may make an individual more prone to injury. It is the responsibility of the child s parent/guardian to make it known, or to learn through health care procedures if your child is suffering from latent pathological defects, illnesses, or deformities, which would otherwise not come to the attention of the chiropractor. The doctor of chiropractic will not give any treatment or care if she or he is aware that such care should not be used for a particular condition or circumstance. Your child s doctor of chiropractic is a licensed primary care provider, and is able to work with all other types of providers. I understand that if my child accepted as a Practice Member at Harbor Bay Clinic of Chiropractic, I am authorizing them to proceed with any treatment that they deem necessary. I understand that following the doctor s recommended care plan is essential to maximizing my child s healing and reaching optimal health through chiropractic. Furthermore, any questions that I have regarding chiropractic care, will be explained to me upon my request. Specific postural x-rays may be necessary for the identification of the location, type, and severity of any vertebral subluxations, as well as for the diagnosis and identification of latent or dangerous conditions requiring medical attention. X-rays may also be used to show progress after a period of recommended chiropractic care. At your request, you can receive a copy of your x-rays to a disc for the mandated fee of $5.00. By signing below, I authorize Harbor Bay Clinic of Chiropractic to perform diagnostic x-rays of my child if medically necessary. Select which is true for your female child: To the best of my knowledge, there is no chance that my child is pregnant at this time. I know or believe that my child may be pregnant at this time and therefore I DO NOT authorize Harbor Bay Clinic of Chiropractic to perform diagnostic x-rays of her. By signing below, I recognize that I am financially responsible for all services rendered to my child regardless of insurance or benefits. I further understand that any health insurance policy is an arrangement between me and my child s insurance carrier and that I may be required to pay for some or all of the fees charged to my child s account. I hereby authorize Harbor Bay Clinic of Chiropractic LLC to release all necessary information concerning my child s health condition to any billing company, insurance company, attorney, and/or adjuster in order to process any claim for reimbursement of charges incurred by my child. In addition I authorize Harbor Bay Clinic of Chiropractic LLC to release any information regarding my child s health condition to other health care providers involved in my child s care. This assignment will remain in effect until revoked by me in writing. I agree that a photocopy of this form is to be considered as valid as the original. I confirm that all information I have provided is true and correct to the best of my knowledge. I confirm that I have read and fully understand this agreement and authorize Harbor Bay Clinic of Chiropractic LLC to proceed with Chiropractic tests, diagnosis, analysis and adjustments.
7 This notice describes how health information about your child may be used and disclosed and how you can get access to your child s health information and records. Harbor Bay Clinic of Chiropractic LLC, understand the importance of privacy and we are commited to maintaining the confidentiality of your child s protected health information (PHI) in compliance with the Health Insurance Portability and Accountability Act of 1996 (HIPAA). We have developed office policies and procedures that protect your child s personal and health information when used within our office and any devices used to copy or transfer this data. We assure you that your child s information will only be shared as required and only for the purpose of administering your child s case and obtaining payment for services. Be assured that without your permission, your child s health information will not be used for any other purpose. The following ways are how your child s PHI may be used within our office to provide the best care and services possible: To provide treatment, obtain payment, and conduct health care operations. To schedule appointments and send reminders. To communicate with your child s family, friends, and/or caregivers with your authorization. As permitted or required by the law. The following describes your rights regarding your child s PHI. You may: Request to inspect any copy of your child s records. Request to amend incomplete or inaccurate information in your child s records. Receive an accounting of certain disclosures of your child s health information. Ask for additional privacy protections (although your request may be declined). Receive a paper copy of this notice. Harbor Bay Clinic of Chiropractic LLC, reserves the right to change this privacy policy as allowed by law and to make the new notice apply to health information already received as well as any information received in the future. A copy of our current notice is available upon request. The notice will display the effective date. If you believe that we have not properly respected the privacy of your child s PHI, you may notify our office by calling (301) , sending a letter to our office address or by ing info@harborbaychiropractic.com. I confirm that I have received and reviewed this notice and understand how health information about my child may be used and disclosed and how I can get access to my child s health information and records. Select an option below. I DO authorize Harbor Bay Clinic of Chiropractic to display testimonials, photographs and videos of my child in the office or on social media outlets. I understand that the purpose of sharing this information is to provide others with chiropractic education and give hope to those seeking answers to their health concerns. My consent remains in effect until revoked by me in writing. I DO NOT authorize Harbor Bay Clinic of Chiropractic to display testimonials, photographs and videos of my child in the office or on social media outlets at this time.
Today s Date: Have you ever received chiropractic care? No Yes, (Please list the City, State, & Doctor):
:") Tyler Leopardi D.C., Brittany Leopardi D.C. 1933 S. Narcoossee Rd. Saint Cloud, FL 34771 P: 321.430.3820 F:1.407.498.4051 info@avenueonechiropractic.com ADULT INTAKE FORM Discover Your True Health Potential.
Tyler Leopardi D.C., Brittany Leopardi D.C. 1933 S. Narcoossee Rd. Saint Cloud, FL 34771 P: 321.430.3820 F:1.407.498.4051 info@avenueonechiropractic.com ADULT INTAKE FORM Discover Your True Health Potential.
Today s Date: Have you ever received chiropractic care? No Yes, (Please list the City, State, & Doctor):
:") Evan Pridmore, D.C. 11227 Lebanon Rd. Mount Juliet, TN 37122 P: 615.583.9788 summitfamilychiropractictn.com ADULT INTAKE FORM Discover Your True Health Potential. Welcome to the Summit Family Chiropractic
Evan Pridmore, D.C. 11227 Lebanon Rd. Mount Juliet, TN 37122 P: 615.583.9788 summitfamilychiropractictn.com ADULT INTAKE FORM Discover Your True Health Potential. Welcome to the Summit Family Chiropractic
LIST YOUR HEALTH CONCERNS BELOW
 8209 Natures Way Unit 115 Lakewood Ranch, Florida 34202 (941) 877.1507 Name Date / / Age Male Female Address City State Zip Phone: Home Cell Cell Phone Provider Email Date of Birth / / Employer s Name
8209 Natures Way Unit 115 Lakewood Ranch, Florida 34202 (941) 877.1507 Name Date / / Age Male Female Address City State Zip Phone: Home Cell Cell Phone Provider Email Date of Birth / / Employer s Name
Who may we thank for referring you? Office Only LIST YOUR HEALTH CONCERNS BELOW. If you had the condition before, when? When did this episode start?
 Name Date / / Age Male / Female Address City State Zip Phone: Home Cell Cell Phone Provider Date of Birth / / Email Address Occupation Employer s Name Single / Married / Divorced / Widowed Spouse s Name
Name Date / / Age Male / Female Address City State Zip Phone: Home Cell Cell Phone Provider Date of Birth / / Email Address Occupation Employer s Name Single / Married / Divorced / Widowed Spouse s Name
SMITH CHIROPRACTIC HEALTH PROFILE Today s Date:
 SMITH CHIROPRACTIC HEALTH PROFILE Today s Date: Name: Age: Male/Female DOB: Address: City: State: Zip: Home Phone:_ Cell: Cell Phone Provider: SSN#: Email Address: Single/Married/Divorced/Widowed Spouse
SMITH CHIROPRACTIC HEALTH PROFILE Today s Date: Name: Age: Male/Female DOB: Address: City: State: Zip: Home Phone:_ Cell: Cell Phone Provider: SSN#: Email Address: Single/Married/Divorced/Widowed Spouse
Name Date / / Age Male/Female Address City State Zip Phone: Home Cell Carrier (Ex: AT&T, Verizon)
") Name_ Date / / Age Male/Female Address City State Zip Phone: Home Cell Carrier (Ex: AT&T, Verizon) For reminders do you prefer Phone Calls, Text Messages or Emails? CALL ME / TEXT ME / EMAIL ME Email Address
Name_ Date / / Age Male/Female Address City State Zip Phone: Home Cell Carrier (Ex: AT&T, Verizon) For reminders do you prefer Phone Calls, Text Messages or Emails? CALL ME / TEXT ME / EMAIL ME Email Address
Who may we thank for referring you?
 NEW PRACTICE MEMBER APPLICATION Name Date of Birth / / Age Male/Female Address City State Zip Phone: Cell Home Social Security #: Email: Occupation Employer s Name Status: Single / Married / Divorced /
NEW PRACTICE MEMBER APPLICATION Name Date of Birth / / Age Male/Female Address City State Zip Phone: Cell Home Social Security #: Email: Occupation Employer s Name Status: Single / Married / Divorced /
New Practice Member Application
 New Practice Member Application Name Date of Birth / / Age Male/Female Address City State Zip Phone: Cell Home Social Security #: Email: Occupation Employer s Name Status: Single / Married / Divorced /
New Practice Member Application Name Date of Birth / / Age Male/Female Address City State Zip Phone: Cell Home Social Security #: Email: Occupation Employer s Name Status: Single / Married / Divorced /
Who? When? Results? Please Mark P For In The Past OR Mark C For Currently Have:
 T, CD, E, C New Practice Member Application Name Date of Birth / / Age Male/Female Address City State Zip Phone: Cell Home Email Address Occupation Employer s Name Single / Married / Divorced / Widowed
T, CD, E, C New Practice Member Application Name Date of Birth / / Age Male/Female Address City State Zip Phone: Cell Home Email Address Occupation Employer s Name Single / Married / Divorced / Widowed
Sincerely, Dr. Justin & Woodbury Spine Staff
 Welcome to our office! We are sure that you will be provided the most appropriate and professional chiropractic care possible. Our most important goal is the constant improvement and maintenance of your
Welcome to our office! We are sure that you will be provided the most appropriate and professional chiropractic care possible. Our most important goal is the constant improvement and maintenance of your
Application for Patient
 Application for Patient First Name: M.I.: Last Name: Date: Address: City: State: Zip: SS#: - - Age: DOB: / / Male / Female Email: Home #: Cell # Work # Primary Care Physician: Do we have permission to
Application for Patient First Name: M.I.: Last Name: Date: Address: City: State: Zip: SS#: - - Age: DOB: / / Male / Female Email: Home #: Cell # Work # Primary Care Physician: Do we have permission to
Practice Member Profile
 Practice Member Profile Please print Name: : Phone number: (H) (C) Cell provider: Address: City: State: Zip: of Birth: Age: Male Female (circle one) Marital Status: Name of Spouse: Number of Children:
Practice Member Profile Please print Name: : Phone number: (H) (C) Cell provider: Address: City: State: Zip: of Birth: Age: Male Female (circle one) Marital Status: Name of Spouse: Number of Children:
ADIO CHIROPRACTIC HEALTH PROFILE
 ADIO CHIROPRACTIC HEALTH PROFILE Name Date / / Age Male/Female Address City State Zip Phone: Home Cell_ Date of Birth / / Email Address For confirming appointments, would you prefer? EMAIL or TEXT CELL
ADIO CHIROPRACTIC HEALTH PROFILE Name Date / / Age Male/Female Address City State Zip Phone: Home Cell_ Date of Birth / / Email Address For confirming appointments, would you prefer? EMAIL or TEXT CELL
Name Date / / Age Male/ Female Address City State Zip
 T 1 2 3 : Name _ Date / / Age Male/ Female Address City State Zip Phone: Home Cell Cell Phone Provider Email Address Date of Birth / / Occupation Employer Single / Married / Divorced / Widowed Spouse s
T 1 2 3 : Name _ Date / / Age Male/ Female Address City State Zip Phone: Home Cell Cell Phone Provider Email Address Date of Birth / / Occupation Employer Single / Married / Divorced / Widowed Spouse s
CIRCLE ALL CURRENT PROBLEMS YOU HAVE
 INSIDE OUT CHIROPRACTIC HEALTH PROFILE Name Date / / Age Male/Female Address City State Zip Phone: Home Cell_ Date of Birth / / Email Address For confirming appts, would you prefer? TEXT (cell carrier:
INSIDE OUT CHIROPRACTIC HEALTH PROFILE Name Date / / Age Male/Female Address City State Zip Phone: Home Cell_ Date of Birth / / Email Address For confirming appts, would you prefer? TEXT (cell carrier:
LIST YOUR HEALTH CONCERNS BELOW
 LOCATION COMING SOON Lakewood Ranch, FL 32402 941.877.1507 Name Date / / Age Male/Female Address City State Zip Phone: Home Cell Cell Phone Provider Email Date of Birth / / Employer s Name Position Single
LOCATION COMING SOON Lakewood Ranch, FL 32402 941.877.1507 Name Date / / Age Male/Female Address City State Zip Phone: Home Cell Cell Phone Provider Email Date of Birth / / Employer s Name Position Single
HEALTH RECORD REASON FOR THIS VISIT ABOUT YOU ABOUT YOUR SPOUSE HEALTH HABITS EXPERIENCE WITH CHIROPRACTIC
 HEALTH RECORD ABOUT YOU REASON FOR THIS VISIT Name Address City State Zip _Home phone Birth date Cell Phone Age Gender Number of children Employer Work address Work phone Occupation Marital Status Social
HEALTH RECORD ABOUT YOU REASON FOR THIS VISIT Name Address City State Zip _Home phone Birth date Cell Phone Age Gender Number of children Employer Work address Work phone Occupation Marital Status Social
New Practice Member Paperwork
 Cornerstone Family Chiropractic Health Information Form 928.237.9477 www.cfc4familyhealth.com 2225 E State Route 69 Suite A Prescott, AZ 86301 New Practice Member Paperwork This form is for adults only.
Cornerstone Family Chiropractic Health Information Form 928.237.9477 www.cfc4familyhealth.com 2225 E State Route 69 Suite A Prescott, AZ 86301 New Practice Member Paperwork This form is for adults only.
LIST YOUR HEALTH CONCERNS BELOW
 Name Date / / Age Male/Female Address City State Zip Phone: Cell Cell Phone Provider Date of Birth / / Email Address Occupation Employer s Name Single/Married/Divorced/Widowed Spouse s Name Number of Children
Name Date / / Age Male/Female Address City State Zip Phone: Cell Cell Phone Provider Date of Birth / / Email Address Occupation Employer s Name Single/Married/Divorced/Widowed Spouse s Name Number of Children
Welcome To Our Office
 Welcome To Our Office Mission Statement Our office is dedicated to educating and adjusting as many families as possible towards optimal health through natural chiropractic care. We believe the greatest
Welcome To Our Office Mission Statement Our office is dedicated to educating and adjusting as many families as possible towards optimal health through natural chiropractic care. We believe the greatest
Chiropractic Case History/Patient Information
 Chiropractic Case History/Patient Information 1 Date: Patient # Doctor: Name: Social Security # Home Phone: Address: City: State: Zip: E-mail address: Fax # Cell Phone: Age: Birth Date: Race: Marital:
Chiropractic Case History/Patient Information 1 Date: Patient # Doctor: Name: Social Security # Home Phone: Address: City: State: Zip: E-mail address: Fax # Cell Phone: Age: Birth Date: Race: Marital:
PERSONAL INFORMATION. First Name: M.I.: Last Name: Preferred Name: Social Security Number: Address: City / State / Zip:
 ADULT INTAKE FORM Date: PERSONAL INFORMATION First Name: M.I.: Last Name: Preferred Name: Social Security Number: Address: City / State / Zip: Cell Phone: ( ) Alternate Phone: ( Text Reminders: Y N Before
ADULT INTAKE FORM Date: PERSONAL INFORMATION First Name: M.I.: Last Name: Preferred Name: Social Security Number: Address: City / State / Zip: Cell Phone: ( ) Alternate Phone: ( Text Reminders: Y N Before
COMPLAINTS (Briefly describe each complaint by order of severity): HAVE YOU EVER HAD FALLS, AUTO ACCIDENTS OR INJURIES?
: HAVE YOU EVER HAD FALLS, AUTO ACCIDENTS OR INJURIES?") CORAL REEF CHIROPRACTIC CENTER, PA NAME (Last, First, Middle Initial) HOME PHONE TODAY S DATE COMPLETE ADDRESS (Include City, State & Zip) CELL PHONE DATE OF BIRTH OCCUPATION EMPLOYER NAME EMAIL AGE SEX
CORAL REEF CHIROPRACTIC CENTER, PA NAME (Last, First, Middle Initial) HOME PHONE TODAY S DATE COMPLETE ADDRESS (Include City, State & Zip) CELL PHONE DATE OF BIRTH OCCUPATION EMPLOYER NAME EMAIL AGE SEX
Child s Name Birth Date / / Age. Mother's Name. Father's Name. Phone: Home Cell. Address. Address Number & Street City State Zip
 Welcome! Thank you for choosing our practice for your health needs. Your first visit to our center is an opportunity for us to learn all about you. If you have any questions or concerns, do not hesitate
Welcome! Thank you for choosing our practice for your health needs. Your first visit to our center is an opportunity for us to learn all about you. If you have any questions or concerns, do not hesitate
ADULT CHIROPRACTIC INTAKE FORM
 ADULT CHIROPRACTIC INTAKE FORM Welcome to our office! It is well known that families who maintain strong, healthy, wellaligned spines have greatly improved health. People whose spines are not healthy and
ADULT CHIROPRACTIC INTAKE FORM Welcome to our office! It is well known that families who maintain strong, healthy, wellaligned spines have greatly improved health. People whose spines are not healthy and
General Information: (Circle One) (Circle One) Primary Insured's Information Skip if you are primary
 (Circle One) Primary Insured's Information Skip if you are primary") General Information: First Name: Middle Initial: Last Name: Suffix: Called Name: Street Address: City: State: Zip Code: Home Phone: ( ) - Work Phone: ( ) - Cell Phone: ( ) - Email Address: Marital Status:
General Information: First Name: Middle Initial: Last Name: Suffix: Called Name: Street Address: City: State: Zip Code: Home Phone: ( ) - Work Phone: ( ) - Cell Phone: ( ) - Email Address: Marital Status:
Personal Information. Reason for Seeking Care. What is your reason for seeking care at Strive Chiropractic?
 Adult Intake Form Date: Personal Information First Name: M.I.: Last Name: Preferred Name: Social Security Number: Address: City / State / Zip: Cell Phone: ( ) Alternate Phone: ( ) Text Reminders: Y N Before
Adult Intake Form Date: Personal Information First Name: M.I.: Last Name: Preferred Name: Social Security Number: Address: City / State / Zip: Cell Phone: ( ) Alternate Phone: ( ) Text Reminders: Y N Before
COMPLETE THIS PAGE FOR CHILDREN 4-8 YEARS OF AGE ASTHMA EAR INFECTIONS SORE THROAT BED WETTING HEADACHES UPSET STOMACH
 COMPLETE THIS PAGE FOR CHILDREN 4-8 YEARS OF AGE CHILD S CURRENT HEALTH STATUS DURING PREGNANCY DID YOU USE: DRUGS/MEDICATIONS TOBACCO/ALCOHOL IF YES, DESCRIBE YOUR DELIVERY: CHILD S HEALTH HISTORY INSTRUCTIONS:
COMPLETE THIS PAGE FOR CHILDREN 4-8 YEARS OF AGE CHILD S CURRENT HEALTH STATUS DURING PREGNANCY DID YOU USE: DRUGS/MEDICATIONS TOBACCO/ALCOHOL IF YES, DESCRIBE YOUR DELIVERY: CHILD S HEALTH HISTORY INSTRUCTIONS:
Current Health Information
 Name: : / / Current Health Information List your health concerns below: Health Concerns: (List according to severity) Rate of Severity 1 = Mild 10 = Unbear able When did the Symptom s Start? Are the Symptoms
Name: : / / Current Health Information List your health concerns below: Health Concerns: (List according to severity) Rate of Severity 1 = Mild 10 = Unbear able When did the Symptom s Start? Are the Symptoms
3. How Long Has This Been An Issue?
 NEW PATIENT INTAKE FORM Aspire Chiropractic 124 W Harwood Rd. Ste. B Hurst, TX 76054 Name: Occupation: DOB: Age: Sex: Male Female Employer: Marital Status: Single Married Other Name/Age of Kids: Phone:
NEW PATIENT INTAKE FORM Aspire Chiropractic 124 W Harwood Rd. Ste. B Hurst, TX 76054 Name: Occupation: DOB: Age: Sex: Male Female Employer: Marital Status: Single Married Other Name/Age of Kids: Phone:
First Name Middle Last Today s Date / / Age Male/Female Date of Birth / / SS# - - Address City State ZIP Phone: Home Cell Phone Provider Address
 First Name Middle Last Today s Date / / Age Male/Female Date of Birth / / SS# - - Address City State ZIP Phone: Home Cell Phone Provider Email Address Do you have Medicaid? Y / N (present your card to
First Name Middle Last Today s Date / / Age Male/Female Date of Birth / / SS# - - Address City State ZIP Phone: Home Cell Phone Provider Email Address Do you have Medicaid? Y / N (present your card to
SPARROW FAMILY CHIROPRACTIC
 Whom may we thank for referring you to this office? SPARROW FAMILY CHIROPRACTIC Today s Date: PATIENT DEMOGRAPHICS PM#: Name: Birth Date: - - Age: Male Female Address: City: State: Zip: E-mail Address:
Whom may we thank for referring you to this office? SPARROW FAMILY CHIROPRACTIC Today s Date: PATIENT DEMOGRAPHICS PM#: Name: Birth Date: - - Age: Male Female Address: City: State: Zip: E-mail Address:
Describe the pain and it s location:
 WELCOME TO ZIVKOVIC CHIROPRACTIC CENTER DATE: Please print clearly and fill in completely. ABOUT YOU: Patient Name:_ What do you prefer to be called:_ SS# Street Address City State Zip Date of Birth: Age:
WELCOME TO ZIVKOVIC CHIROPRACTIC CENTER DATE: Please print clearly and fill in completely. ABOUT YOU: Patient Name:_ What do you prefer to be called:_ SS# Street Address City State Zip Date of Birth: Age:
Carter Physiotherapy, PLLC Patient Contact Information
 Carter Physiotherapy, PLLC Patient Contact Information Patient Name Today s Date Address City State Zip DOB Age Gender Marital Status Cell Phone Home Phone Email Employer Occupation Parent/Guardian/Spouse
Carter Physiotherapy, PLLC Patient Contact Information Patient Name Today s Date Address City State Zip DOB Age Gender Marital Status Cell Phone Home Phone Email Employer Occupation Parent/Guardian/Spouse
LIST YOUR HEALTH CONCERNS BELOW
 T 1 2 3 ROOTS CHIROPRACTIC HEALTH PROFILE In Name Date / / Age Male/Female Address City State Zip Phone: Home Cell Work Email Address Date of Birth / / Occupation Employer's Name Single / Married / Divorced
T 1 2 3 ROOTS CHIROPRACTIC HEALTH PROFILE In Name Date / / Age Male/Female Address City State Zip Phone: Home Cell Work Email Address Date of Birth / / Occupation Employer's Name Single / Married / Divorced
ABOUT YOU CHIROPRACTIC EXPERIENCE REASON FOR THIS VISIT ABOUT YOUR SPOUSE HEALTH HABITS
 NAME: ABOUT YOU WHO REFERRED YOU TO OUR OFFICE? CHIROPRACTIC EXPERIENCE ADDRESS: CITY: HOME PHONE: STATE/ZIP CODE: CELL PHONE: How did you hear about our office? NEWSPAPER SIGN YELLOW PAGES COMMUNITY EVENT
NAME: ABOUT YOU WHO REFERRED YOU TO OUR OFFICE? CHIROPRACTIC EXPERIENCE ADDRESS: CITY: HOME PHONE: STATE/ZIP CODE: CELL PHONE: How did you hear about our office? NEWSPAPER SIGN YELLOW PAGES COMMUNITY EVENT
CHIROPRACTIC EXPERIENCE ABOUT YOU REASON FOR THIS VISIT HEALTH HABITS MEDICATIONS YOU TAKE SUPPLEMENTS YOU TAKE
 ABOUT YOU CHIROPRACTIC EXPERIENCE NAME: ADDRESS: CITY: HOME PHONE: EMAIL ADDRESS: STATE/ZIP CODE: CELL PHONE: WHO REFERRED YOU TO OUR OFFICE? HAVE YOU SEEN OR HEARD OF OUR OFFICE BECAUSE OF ( ALL THAT
ABOUT YOU CHIROPRACTIC EXPERIENCE NAME: ADDRESS: CITY: HOME PHONE: EMAIL ADDRESS: STATE/ZIP CODE: CELL PHONE: WHO REFERRED YOU TO OUR OFFICE? HAVE YOU SEEN OR HEARD OF OUR OFFICE BECAUSE OF ( ALL THAT
APPLICATION FOR CARE AT LAUNCH CHIROPRACTIC
 Whom may we thank for referring you to this office? APPLICATION FOR CARE AT LAUNCH CHIROPRACTIC Today s Date: HRN: PATIENT DEMOGRAPHICS Name: DOB: Age: Male Female Address: City: State: Zip: E-mail: Home
Whom may we thank for referring you to this office? APPLICATION FOR CARE AT LAUNCH CHIROPRACTIC Today s Date: HRN: PATIENT DEMOGRAPHICS Name: DOB: Age: Male Female Address: City: State: Zip: E-mail: Home
Address City State Zip Code
 Name Cell Phone Address City State Zip Code Date of Birth / / Male/Female Age Email SS# Number of Children Name of Children Employer Type of Work Marital Status Married Single Divorced Separated Widowed
Name Cell Phone Address City State Zip Code Date of Birth / / Male/Female Age Email SS# Number of Children Name of Children Employer Type of Work Marital Status Married Single Divorced Separated Widowed
APPLICATION FOR CARE AT OPTIMAL HEALTH CHIROPRACTIC
 Today s Date: APPLICATION FOR CARE AT OPTIMAL HEALTH CHIROPRACTIC PATIENT DEMOGRAPHICS Name: Birth Date: / / Age: Male Female Address: City: State: Zip: E-mail Address: Home Phone: Cell Phone: Martial
Today s Date: APPLICATION FOR CARE AT OPTIMAL HEALTH CHIROPRACTIC PATIENT DEMOGRAPHICS Name: Birth Date: / / Age: Male Female Address: City: State: Zip: E-mail Address: Home Phone: Cell Phone: Martial
Home Sleep Test (HST) Instructions
 Instructions") Home Sleep Test (HST) Instructions 1. Your physician has ordered an unattended home sleep test (HST) to diagnose or rule out sleep apnea. This test cannot diagnose any other sleep disorders. 2. This device
Home Sleep Test (HST) Instructions 1. Your physician has ordered an unattended home sleep test (HST) to diagnose or rule out sleep apnea. This test cannot diagnose any other sleep disorders. 2. This device
Revelation Chiropractic Health Profile
 Revelation Chiropractic Health Profile Name Date / Age Male / Female Address Apt City Zip Phone Numbers: Home Cell Circle best number to reach you at: Home Cell Date of Birth / / Occupation Email Address
Revelation Chiropractic Health Profile Name Date / Age Male / Female Address Apt City Zip Phone Numbers: Home Cell Circle best number to reach you at: Home Cell Date of Birth / / Occupation Email Address
Address (if different from above):
:") Lee H. Baker, DDS 1243 Augusta West Pkwy Augusta, GA 30909 (706) 855-8989-Phone (706) 855-0321-Fax www.drleebaker.com Welcome to our practice! In order to know you and your child better, please complete
Lee H. Baker, DDS 1243 Augusta West Pkwy Augusta, GA 30909 (706) 855-8989-Phone (706) 855-0321-Fax www.drleebaker.com Welcome to our practice! In order to know you and your child better, please complete
Welcome to our Family Chiropractic Office
 Welcome to our Family Chiropractic Office Thank you for choosing our office for chiropractic care. We are committed to providing your family with the highest quality of corrective and wellness chiropractic
Welcome to our Family Chiropractic Office Thank you for choosing our office for chiropractic care. We are committed to providing your family with the highest quality of corrective and wellness chiropractic
Child s Legal Name: Nickname: Male Female. Birth Date: Age: School: Grade: FATHER STEPMOTHER GUARDIAN? Insured s Name: D.O.B. Social Security #:
 Welcome Welcome to our practice! We strive to make each of your child s visits pleasant and comfortable. Our goal is to teach your child oral habits which will help keep their smile beautiful for their
Welcome Welcome to our practice! We strive to make each of your child s visits pleasant and comfortable. Our goal is to teach your child oral habits which will help keep their smile beautiful for their
Health and History Assessment ACCOUNT #: HIPPA: CTT:
 ACTION Chiropractor LLC Health and History Assessment ACCOUNT #: HIPPA: CTT: NAME: SEX: M/ F BIRTHDATE: / / ADDRESS: CITY: STATE: Zip: PHONE # s: HOME: ( ) WORK: ( ) CELL: ( ) HEIGHT: WEIGHT: MARITAL STATUS:
ACTION Chiropractor LLC Health and History Assessment ACCOUNT #: HIPPA: CTT: NAME: SEX: M/ F BIRTHDATE: / / ADDRESS: CITY: STATE: Zip: PHONE # s: HOME: ( ) WORK: ( ) CELL: ( ) HEIGHT: WEIGHT: MARITAL STATUS:
New Patient Information
 Patient's Street Address: Home Phone: Cell Phone: of Birth: / / New Patient Information State: Name of Person Responsible for This Account: E-Mail Address: Zip Code: Work Phone: SSN: Do You Have Dental
Patient's Street Address: Home Phone: Cell Phone: of Birth: / / New Patient Information State: Name of Person Responsible for This Account: E-Mail Address: Zip Code: Work Phone: SSN: Do You Have Dental
Restored Life Wellness
 Restored Life Wellness C E N T E R PERSONAL INFORMATION Child s First Name: M.I.: Last Name: Preferred Name: Address: City/State/Zip: Birth Age: Sex: M F # of Siblings: Sibling(s) Names & Ages: Parents
Restored Life Wellness C E N T E R PERSONAL INFORMATION Child s First Name: M.I.: Last Name: Preferred Name: Address: City/State/Zip: Birth Age: Sex: M F # of Siblings: Sibling(s) Names & Ages: Parents
634 N. STATE STREET, WESTERVILLE OH, (614) 901-WELL
 901-WELL") eas 634 N. STATE STREET, WESTERVILLE OH, 43082 (614) 901-WELL www.abilitychiro.com Name: Age: Date: Address: City: State: Zip Code: Alternate Address: City: State: Zip Code: Cell Phone: ( ) Cell Phone
eas 634 N. STATE STREET, WESTERVILLE OH, 43082 (614) 901-WELL www.abilitychiro.com Name: Age: Date: Address: City: State: Zip Code: Alternate Address: City: State: Zip Code: Cell Phone: ( ) Cell Phone
Pediatric Intake Form
 Pediatric Intake Form Date: Personal Information Child s First Name: M.I.: Last Name: Preferred Name: Social Security Number: Address: City / State / Zip: Birth Date: Age: Sex: M F # of Siblings: Sibling(s)
Pediatric Intake Form Date: Personal Information Child s First Name: M.I.: Last Name: Preferred Name: Social Security Number: Address: City / State / Zip: Birth Date: Age: Sex: M F # of Siblings: Sibling(s)
MASSAGE INTAKE FORM PATIENT S PREFERED NAME DATE COMPLETED
 MASSAGE INTAKE FORM PATIENT S PREFERED NAME DATE COMPLETED Patient Information Name: DOB: / / Gender: M F Home Address: Home Phone: City, State, Zip: Work Phone: Email Address: Cell Phone: I do not want
MASSAGE INTAKE FORM PATIENT S PREFERED NAME DATE COMPLETED Patient Information Name: DOB: / / Gender: M F Home Address: Home Phone: City, State, Zip: Work Phone: Email Address: Cell Phone: I do not want
Welcome to the Dynamic Essence tribe!
 Welcome to the Dynamic Essence tribe! 746 Wealthy St SE Grand Rapids, MI 49503 P: 989.573.1170 DynamicEssenceChiropractic@gmail.com We empower you to reclaim your power. Elevate your unique expression.
Welcome to the Dynamic Essence tribe! 746 Wealthy St SE Grand Rapids, MI 49503 P: 989.573.1170 DynamicEssenceChiropractic@gmail.com We empower you to reclaim your power. Elevate your unique expression.
Patient First Name: Last Name: Street Address: City: State: Zip Code. Mobile Phone: Home Phone: Work Phone:
 Dr. Beth Kozak Welcome! New Patient Information Form Please provide us with the following information: Patient First Name: Last Name: Street Address: City: State: Zip Code Mobile Phone: Home Phone: Work
Dr. Beth Kozak Welcome! New Patient Information Form Please provide us with the following information: Patient First Name: Last Name: Street Address: City: State: Zip Code Mobile Phone: Home Phone: Work
Dr. Janet L. Yarger 510 Baxter Road, Suite 8, Chesterfield, MO
 Registration Form Date: / / Name: Social Security #: - - Address: City: State: Zip Code: Home Phone #: ( ) - Age: Date of Birth / / Cell Phone #: ( ) - Best Phone to call you at: HOME/CELL/WORK Email Address:
Registration Form Date: / / Name: Social Security #: - - Address: City: State: Zip Code: Home Phone #: ( ) - Age: Date of Birth / / Cell Phone #: ( ) - Best Phone to call you at: HOME/CELL/WORK Email Address:
LIST YOUR HEALTH CONCERNS BELOW
 Date / / HEALTH PROFILE T C E X Name D.O.B. / / Age Male/Female Address City State Zip Phone: Home Cell Cell Phone Carrier: Email Address Occupation Employer s Name _ Single / Married / Divorced / Widowed
Date / / HEALTH PROFILE T C E X Name D.O.B. / / Age Male/Female Address City State Zip Phone: Home Cell Cell Phone Carrier: Email Address Occupation Employer s Name _ Single / Married / Divorced / Widowed
Luker Chiropractic Health Questionnaire
 Luker Chiropractic Health Questionnaire Name: D.O.B.: Address: City: State: Zip: Home Phone: Cell: Email: Male/Female Marital Status: M W D S Age: SS# Occupation: Employer: Spouse Name: # of Children:
Luker Chiropractic Health Questionnaire Name: D.O.B.: Address: City: State: Zip: Home Phone: Cell: Email: Male/Female Marital Status: M W D S Age: SS# Occupation: Employer: Spouse Name: # of Children:
Chiropractic Health Dr. Art Vanderhoef
 Patient Information Form Chiropractic Health Dr. Art Vanderhoef File # Name Address City State Zip Home Phone ( ) Work Phone ( ) Cell Phone ( ) Email Address How do you prefer to be contacted? Mail Home
Patient Information Form Chiropractic Health Dr. Art Vanderhoef File # Name Address City State Zip Home Phone ( ) Work Phone ( ) Cell Phone ( ) Email Address How do you prefer to be contacted? Mail Home
Liberty Chiropractic Clinic Scarsdale Blvd., Houston, TX
 Liberty Chiropractic Clinic, -6154 Patient's Name Patient's Address City State Zip Code Age D.O.B. Single Married Divorced Widowed No. of children Occupation Employer Home Phone Work Phone Cell Phone Email
Liberty Chiropractic Clinic, -6154 Patient's Name Patient's Address City State Zip Code Age D.O.B. Single Married Divorced Widowed No. of children Occupation Employer Home Phone Work Phone Cell Phone Email
HEALING HANDS CHIROPRACTIC, LLC 3 Hall Ave Wallingford, CT healinghandsdc.com
 HEALING HANDS CHIROPRACTIC, LLC 3 Hall Ave Wallingford, CT 06492 203-626-9994 healinghandsdc.com Child Intake Form PERSONAL INFORMATION Date Child s Name: Address Gender M F Age Birthdate City State Zip
HEALING HANDS CHIROPRACTIC, LLC 3 Hall Ave Wallingford, CT 06492 203-626-9994 healinghandsdc.com Child Intake Form PERSONAL INFORMATION Date Child s Name: Address Gender M F Age Birthdate City State Zip
New Patient Form Welcome!
 New Patient Form Welcome! Last First Middle Initial DOB Address City ST ZIP Phone (H) (C) Email Occupation Employer Relationship Status S M W D Spouse s Name DOB Children s Names and Ages Have you had
New Patient Form Welcome! Last First Middle Initial DOB Address City ST ZIP Phone (H) (C) Email Occupation Employer Relationship Status S M W D Spouse s Name DOB Children s Names and Ages Have you had
Welcome to. Active Health Chiropractic
 Dr. Darrell Voll, DC CACCP Welcome to Active Health Chiropractic Thank you for choosing our office. We are committed to providing you and your family with the highest quality of chiropractic care available
Dr. Darrell Voll, DC CACCP Welcome to Active Health Chiropractic Thank you for choosing our office. We are committed to providing you and your family with the highest quality of chiropractic care available
Dr. Charles E. Copeland, DC Highland Chiropractic
 Highland Chiropractic Name: Birth Date: / / Gender M / F Occupation: Address: Employer: City: State: Zip: How did you hear about us? Home Phone: ( ) - Preferred Phone to Contact Work Phone: ( ) - Home
Highland Chiropractic Name: Birth Date: / / Gender M / F Occupation: Address: Employer: City: State: Zip: How did you hear about us? Home Phone: ( ) - Preferred Phone to Contact Work Phone: ( ) - Home
Physical Evidence Chiropractic 7035 Beracasa Way, Suite 103 Boca Raton Florida, Phone# (561) Fax# (561)
 Fax# (561)") 7035 Beracasa Way, Suite 103 Boca Raton Florida, 33433 Phone# (561)674-1217 Fax# (561)361-4999 Date File # PERSONAL HISTORY Last Name First Name middle Address City State Zip Date of Birth Age Social Security
7035 Beracasa Way, Suite 103 Boca Raton Florida, 33433 Phone# (561)674-1217 Fax# (561)361-4999 Date File # PERSONAL HISTORY Last Name First Name middle Address City State Zip Date of Birth Age Social Security
Who may we thank for referring you? When did this episode start?
 NEW PRACTICE MEMBER APPLICATION Name Date / / Age Male/Female Address City State Zip Phone: Home Cell_ Date of Birth / / Email Address For confirming appointments, would you prefer? EMAIL or TEXT CELL
NEW PRACTICE MEMBER APPLICATION Name Date / / Age Male/Female Address City State Zip Phone: Home Cell_ Date of Birth / / Email Address For confirming appointments, would you prefer? EMAIL or TEXT CELL
APPLICATION FOR CARE AT CORE CHIROPRACTIC
 Whom may we thank for referring you to this office? APPLICATION FOR CARE AT CORE CHIROPRACTIC Today s Date: HRN: PATIENT DEMOGRAPHICS Name: Birth Date: - - Age: Male Female Address: City: State: Zip: E-mail
Whom may we thank for referring you to this office? APPLICATION FOR CARE AT CORE CHIROPRACTIC Today s Date: HRN: PATIENT DEMOGRAPHICS Name: Birth Date: - - Age: Male Female Address: City: State: Zip: E-mail
New Patient Information
 New Patient Information Bloomfield Children s Dentistry 6405 Telegraph Road Bloomfield Hills, MI 48301 In order to get to know your family better, and to provide you with the best service, we ask that
New Patient Information Bloomfield Children s Dentistry 6405 Telegraph Road Bloomfield Hills, MI 48301 In order to get to know your family better, and to provide you with the best service, we ask that
APPLICATION FOR CARE AT LAUNCH CHIROPRACTIC
 Whom may we thank for referring you to this office? APPLICATION FOR CARE AT LAUNCH CHIROPRACTIC Today s Date: PATIENT DEMOGRAPHICS HRN: Name: Birth Date: - - Age: o Male o Female Address: City: State:
Whom may we thank for referring you to this office? APPLICATION FOR CARE AT LAUNCH CHIROPRACTIC Today s Date: PATIENT DEMOGRAPHICS HRN: Name: Birth Date: - - Age: o Male o Female Address: City: State:
New Practice Member Application
 a New Practice Member Application PATIENT DEMOGRAPHICS Name Date of Birth / / Age Male/Female Address City State Zip Phone: Cell Home Cellular Provider Email Address Occupation Employer s Name Single /
a New Practice Member Application PATIENT DEMOGRAPHICS Name Date of Birth / / Age Male/Female Address City State Zip Phone: Cell Home Cellular Provider Email Address Occupation Employer s Name Single /
APPLICATION FOR CARE AT Raleigh Specific Chiropractic
 Whom may we thank for referring you to this office? Today s : PATIENT DEMOGRAPHICS APPLICATION FOR CARE AT Raleigh Specific Chiropractic HRN: Name: Birth : - - Age: Male Female Address: City: State: Zip:
Whom may we thank for referring you to this office? Today s : PATIENT DEMOGRAPHICS APPLICATION FOR CARE AT Raleigh Specific Chiropractic HRN: Name: Birth : - - Age: Male Female Address: City: State: Zip:
PATIENT FEE SCHEDULE As of January 1, 2017
 TERMS OF ACCEPTANCE When a patient seeks chiropractic care and we accept such a patient for care, it is essential for both to be working towards the same objective. Chiropractic has only one goal. It is
TERMS OF ACCEPTANCE When a patient seeks chiropractic care and we accept such a patient for care, it is essential for both to be working towards the same objective. Chiropractic has only one goal. It is
New Member Contact Information
 New Member Contact Information Date: Social Security #: - - File Number: First Name: Middle Initial: Last Name: Age: Birth Date: / / Gender: M F Marital Status: S M D W Home Address: Home Phone: - - City,
New Member Contact Information Date: Social Security #: - - File Number: First Name: Middle Initial: Last Name: Age: Birth Date: / / Gender: M F Marital Status: S M D W Home Address: Home Phone: - - City,
Date of Birth: Sex: O Male O Female Marital Status? O M O W O D O S. Chiropractic Care
 Basic Information Full Name: Address: City: State: Zip: Cell: Home: Work: Date of Birth: Sex: O Male O Female Marital Status? O M O W O D O S Email: Occupation: Emergency Contact: Phone: Children: O No
Basic Information Full Name: Address: City: State: Zip: Cell: Home: Work: Date of Birth: Sex: O Male O Female Marital Status? O M O W O D O S Email: Occupation: Emergency Contact: Phone: Children: O No
DENTAL QUESTIONNAIRE
 Name: (First) (Last) (Preferred) Birthdate: (Month) (Day) (Year) Gender: Male Female Address: City: Prov: Postal Code: Cell Phone: (Number will be used for confirmation of appointments) Email Address:
Name: (First) (Last) (Preferred) Birthdate: (Month) (Day) (Year) Gender: Male Female Address: City: Prov: Postal Code: Cell Phone: (Number will be used for confirmation of appointments) Email Address:
Dr. Fawn Shaffer, DC 565 McElhattan Drive Lock Haven, PA (570)
") PATIENT Dr. Fawn Shaffer, DC 565 McElhattan Drive Lock Haven, PA 17745 (570) 748-3590 PERSONAL INFORMATION: Please Circle: Mr. Mrs. Ms. Miss Dr. Male Female Name: Nickname: Age: DOB: Address: City/State/
PATIENT Dr. Fawn Shaffer, DC 565 McElhattan Drive Lock Haven, PA 17745 (570) 748-3590 PERSONAL INFORMATION: Please Circle: Mr. Mrs. Ms. Miss Dr. Male Female Name: Nickname: Age: DOB: Address: City/State/
PATIENT INFORMATION SHEET PERSON RESPONSIBLE FOR PAYMENT OF THIS ACCOUNT
 PATIENT INFORMATION SHEET Referred By: Patient s Name: SSN: Date of Birth: Address: City/Zip: Phone #: Sex: M / F Marital Status: M / S / W / D No. of Dependents: Email Address: Emergency Contact Person:
PATIENT INFORMATION SHEET Referred By: Patient s Name: SSN: Date of Birth: Address: City/Zip: Phone #: Sex: M / F Marital Status: M / S / W / D No. of Dependents: Email Address: Emergency Contact Person:
New Practice Member Application
 i New Practice Member Application PATIENT DEMOGRAPHICS Name Date of Birth / / Age Male/Female Address City State Zip Phone: Cell Home Would you like to receive text reminders for your appointments? Cellular
i New Practice Member Application PATIENT DEMOGRAPHICS Name Date of Birth / / Age Male/Female Address City State Zip Phone: Cell Home Would you like to receive text reminders for your appointments? Cellular
JACKSONVILLE SPEECH & HEARING CENTER PATIENT INFORMATION FORM PEDIATRIC (CHILD) - AUDIOLOGY Please Print
 - AUDIOLOGY Please Print") JACKSONVILLE SPEECH & HEARING CENTER PATIENT INFORMATION FORM PEDIATRIC (CHILD) - AUDIOLOGY Please Print Referring Physician: Child s (Patient) Name: LAST FIRST MIDDLE Gender: Male Female Date of Birth:
JACKSONVILLE SPEECH & HEARING CENTER PATIENT INFORMATION FORM PEDIATRIC (CHILD) - AUDIOLOGY Please Print Referring Physician: Child s (Patient) Name: LAST FIRST MIDDLE Gender: Male Female Date of Birth:
Welcome to Manna Family Chiropractic!
 Welcome to Manna Family Chiropractic! Today s date Who should we thank for referring you here? Is your visit today regarding you, or your whole family? Family Just Me Your name Date of Birth Street Address
Welcome to Manna Family Chiropractic! Today s date Who should we thank for referring you here? Is your visit today regarding you, or your whole family? Family Just Me Your name Date of Birth Street Address
APPLICATION FOR CARE AT VICTORY HEALTH CENTER
 217 Fox Road Knoxville, TN 37922 865 357 2600 victoryknoxville@gmail.com Whom may we thank for referring you to this office? APPLICATION FOR CARE AT VICTORY HEALTH CENTER Today s : PATIENT DEMOGRAPHICS
217 Fox Road Knoxville, TN 37922 865 357 2600 victoryknoxville@gmail.com Whom may we thank for referring you to this office? APPLICATION FOR CARE AT VICTORY HEALTH CENTER Today s : PATIENT DEMOGRAPHICS
CONDITIONS OF SERVICES RENDERED
 CONDITIONS OF SERVICES RENDERED FINANCIAL AGREEMENT: I agree, whether I sign as agent or as patient, that in consideration of the services to be rendered to the patient, I hereby individually obligate
CONDITIONS OF SERVICES RENDERED FINANCIAL AGREEMENT: I agree, whether I sign as agent or as patient, that in consideration of the services to be rendered to the patient, I hereby individually obligate
APPLICATION FOR CARE
 3023 Eastland Blvd. Suite 101 Clearwater, FL 33761 Ph: 727-797-9900 Fax: 727-797-7695 APPLICATION FOR CARE Date: Name: Address: City, State, Zip: Home Phone: Work Phone: Cell Phone: Email Address: Birth
3023 Eastland Blvd. Suite 101 Clearwater, FL 33761 Ph: 727-797-9900 Fax: 727-797-7695 APPLICATION FOR CARE Date: Name: Address: City, State, Zip: Home Phone: Work Phone: Cell Phone: Email Address: Birth
Gordley Family Chiropractic Clinic Patient Introduction Card. First Name MI Last Name Date Address Married Single Mailing Address City State Zip Code
 Gordley Family Chiropractic Clinic Patient Introduction Card First Name MI Last Name Date Address Married Single Mailing Address Phone City State Zip Code Birth Date Social Security Number Employed By
Gordley Family Chiropractic Clinic Patient Introduction Card First Name MI Last Name Date Address Married Single Mailing Address Phone City State Zip Code Birth Date Social Security Number Employed By
NEW PATIENT PAPERWORK
 NEW PATIENT PAPERWORK Welcome! Please fill out the necessary paperwork provided. It is our pleasure to serve you and your family. How did you find out about us? If It was a friend or doctor, please list
NEW PATIENT PAPERWORK Welcome! Please fill out the necessary paperwork provided. It is our pleasure to serve you and your family. How did you find out about us? If It was a friend or doctor, please list
Life Story. Vital Information. Street City State Zip. Home Phone: May we leave a message? Cell Phone: Emergency Contact
 Today s date: Life Story Patient Number Vital Information Patient s Name I prefer to be called Marital Status Spouse/Partner Name Birth date: Age: Adderss Street City State Zip Email Home Phone: May we
Today s date: Life Story Patient Number Vital Information Patient s Name I prefer to be called Marital Status Spouse/Partner Name Birth date: Age: Adderss Street City State Zip Email Home Phone: May we
Please list medications and dosage (including non-prescriptions) you are currently taking or have taken recently:
 you are currently taking or have taken recently:") Name: DOB: Today s Date: Primary Care Doctor: Referring Physician: What is the primary reason for today s visit? Medical History Please list medications and dosage (including non-prescriptions) you are
Name: DOB: Today s Date: Primary Care Doctor: Referring Physician: What is the primary reason for today s visit? Medical History Please list medications and dosage (including non-prescriptions) you are
Patient Information Form
 Patient Information Name: First Middle Last Address: City: State: Zip: Telephone: Home Cell Work Date of Birth: Social Security Number: (SSN is only needed if getting super-bills for potential insurance
Patient Information Name: First Middle Last Address: City: State: Zip: Telephone: Home Cell Work Date of Birth: Social Security Number: (SSN is only needed if getting super-bills for potential insurance
Welcome To Corporate Chiropractic Works!
 Welcome To Corporate Chiropractic Works! When a person seeks the services of a chiropractor, it is important to fully understand the purpose and intent of that particular chiropractor and the chiropractic
Welcome To Corporate Chiropractic Works! When a person seeks the services of a chiropractor, it is important to fully understand the purpose and intent of that particular chiropractor and the chiropractic
Family First Chiropractic
 Personal Information Title: (Check one) Mr. Mrs. Ms. Miss Other First Name Middle Initial Last Name Street City State Zip Code Email Home Phone ( ) - Cell Phone ( ) - Date of Birth / / Sex: Male Female
Personal Information Title: (Check one) Mr. Mrs. Ms. Miss Other First Name Middle Initial Last Name Street City State Zip Code Email Home Phone ( ) - Cell Phone ( ) - Date of Birth / / Sex: Male Female
Family First Chiropractic
 Family First Chiropractic Personal Information Title: (Check one) Mr. Mrs. Ms. Miss Other First Name Middle Initial Last Name Street City State Zip Code Email Home Phone ( ) - Cell Phone ( ) - Date of
Family First Chiropractic Personal Information Title: (Check one) Mr. Mrs. Ms. Miss Other First Name Middle Initial Last Name Street City State Zip Code Email Home Phone ( ) - Cell Phone ( ) - Date of
Chiropractic Case History/Patient Information
 Family Chiropractic and Wellness. 1 Chiropractic Case History/Patient Information Date: Patient # Name: Social Security # Home Phone: Address: City: State: Zip: E-mail address: Fax # Cell Phone: Birth
Family Chiropractic and Wellness. 1 Chiropractic Case History/Patient Information Date: Patient # Name: Social Security # Home Phone: Address: City: State: Zip: E-mail address: Fax # Cell Phone: Birth
MEDICAL HISTORY FORM
 MEDICAL HISTORY FORM Patient Name: Date of Birth: Date: Email: Address: Emergency Contact (name, relationship to patient, & phone): Height: Weight: Right/Left Hand Dominant: [ ] Male [ ] Female What area
MEDICAL HISTORY FORM Patient Name: Date of Birth: Date: Email: Address: Emergency Contact (name, relationship to patient, & phone): Height: Weight: Right/Left Hand Dominant: [ ] Male [ ] Female What area
WEBSTER CHIROPRACTIC CARE
 WEBSTER CHIROPRACTIC CARE Name: Address: City: Zip Code: Marital Status: M S Phone: Cell: Age of Birth Email: May we contact you or send helpful health information via Email? Yes or No Would you like E-mail
WEBSTER CHIROPRACTIC CARE Name: Address: City: Zip Code: Marital Status: M S Phone: Cell: Age of Birth Email: May we contact you or send helpful health information via Email? Yes or No Would you like E-mail
th Street Urbandale, IA YOST
 YfC 3993 100th Street Urbandale, IA 50322 515.278.YOST www.yostfamilychiropractic.com Demographics: Language (Primary) Race: Unspecified American Indian or Alaska Native Black or African American Other
YfC 3993 100th Street Urbandale, IA 50322 515.278.YOST www.yostfamilychiropractic.com Demographics: Language (Primary) Race: Unspecified American Indian or Alaska Native Black or African American Other
New Practice Member Forms
 New Practice Member Forms Name Date Age Male Female Address City State Zip Phone: Home Cell Cell Phone Provider E-mail SSN Birthday Date of Occupation Employer s Name Single Married Divorced Widowed Spouse
New Practice Member Forms Name Date Age Male Female Address City State Zip Phone: Home Cell Cell Phone Provider E-mail SSN Birthday Date of Occupation Employer s Name Single Married Divorced Widowed Spouse
Pregnant Patient Introduction Form Form
 1820 S. Westnedge Ave. Suite #1. Kalamazoo, MI 49008 269.344.5551 antoniottichiropractic.com Form : Patient name: Address: Estimated Due : Home Phone: INTRODUCTION MEDICAL HISTORY City, State, Zip: Work
1820 S. Westnedge Ave. Suite #1. Kalamazoo, MI 49008 269.344.5551 antoniottichiropractic.com Form : Patient name: Address: Estimated Due : Home Phone: INTRODUCTION MEDICAL HISTORY City, State, Zip: Work
Chiropractic for pediatric development and adult health
 Raleigh Specific Chiropractic Chiropractic for pediatric development and adult health 7721 Six Forks Rd. Suite 138 Raleigh, NC 27615 (919) 846-7004 Items to bring to your first visit: All new patient paperwork
Raleigh Specific Chiropractic Chiropractic for pediatric development and adult health 7721 Six Forks Rd. Suite 138 Raleigh, NC 27615 (919) 846-7004 Items to bring to your first visit: All new patient paperwork
PATIENT INTAKE FORM Health & Wellness
 PATIENT INTAKE FORM Health & Wellness GRAFFEO CHIROPRACTIC CLINIC Joseph Graffeo, DC, PC Date: ABOUT YOU 16248 NE Glisan St Portland, OR 97230 First Name Last Name Middle Name Email Address Street Address
PATIENT INTAKE FORM Health & Wellness GRAFFEO CHIROPRACTIC CLINIC Joseph Graffeo, DC, PC Date: ABOUT YOU 16248 NE Glisan St Portland, OR 97230 First Name Last Name Middle Name Email Address Street Address
Welcome to our Office!
 Welcome to our Office! Please fill out our Health Record as completely and accurate as possible. If you have any questions, please don t hesitate to ask one of our qualified team members. It is our pleasure
Welcome to our Office! Please fill out our Health Record as completely and accurate as possible. If you have any questions, please don t hesitate to ask one of our qualified team members. It is our pleasure