Correspondence should be addressed to Anna Linda Zignego;
|
|
|
- Dale Jenkins
- 5 years ago
- Views:
Transcription
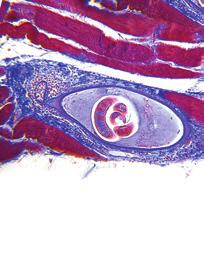
1 Case Reports in Immunology Volume 2015, Article ID , 5 pages Case Report Combined Treatment with Antiviral Therapy and Rituximab in Patients with Mixed Cryoglobulinemia: Review of the Literature and Report of a Case Using Direct Antiviral Agents-Based Antihepatitis C Virus Therapy Teresa Urraro, Laura Gragnani, Alessia Piluso, Alessio Fabbrizzi, Monica Monti, Elisa Fognani, Barbara Boldrini, Jessica Ranieri, and Anna Linda Zignego Center for Systemic Manifestations of Hepatitis Viruses (MASVE), Department of Experimental and Clinical Medicine, University of Florence, Lagro Brambilla 3, Florence, Italy Correspondence should be addressed to Anna Linda Zignego; a.zignego@dmi.unifi.it Received 26 September 2014; Revised 9 January 2015; Accepted 20 January 2015 Academic Editor: Lenin Pavón Copyright 2015 Teresa Urraro et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Mixed cryoglobulinemia (MC) is an autoimmune/b-cell lymphoproliferative disorder associated with Hepatitis C Virus (HCV) infection, manifesting as a systemic vasculitis. In the last decade, antiviral treatment (AT) with pegylated interferon (Peg-IFN) plus ribavirin (RBV) was considered the first therapeutic option for HCV-MC. In MC patients ineligible or not responsive to antivirals, the anti-cd20 monoclonal antibody rituximab (RTX) iseffective.acombinedatplusrtxwasalsosuggested.since the introduction of direct acting antivirals (DAAs), few data were published about MC and no data about a combined schedule. Here, we report a complete remission of MC after a sustained virological response following a combined RTX/Peg-IFN+RBV+DAA (boceprevir) treatment and review the literature about the combined RTX/AT. 1. Introduction Mixed cryoglobulinemia (MC) is both an autoimmune and B-cell lymphoproliferative disorder (LPD) characterized by immune complexes (cryoglobulins, CGs) that reversibly precipitate at low temperature [1]. In the large majority of cases, MC is triggered by Hepatitis C Virus (HCV) infection. HCV is both a hepatotropic and lymphotropic virus and may lead not only to liver diseases, but also to some lymphoproliferative disorders ranging from the benign MC to malignant B-cell non-hodgkin s lymphoma [2]. Small-to-medium sized vessel vasculitis is the pathological substrate of the MC-related clinical syndrome (MCS) [1]. Antiviral therapy (AT) has been indicated as first-line therapy in patients with mild-to-moderate HCV-related MCS. The use of IFN-α to treat MC was successfully proposed, even before HCV discovery, because of its antiproliferative and immunomodulatory effects [3]. However, the benefit was transient and relapses were very frequent after treatment discontinuation when viral eradication was not achieved [4 6]. Starting with the IFN monotherapy, the efficacy of AT progressively increased during two decades thanks to the use of Peg-IFN and RBV. The increased antiviral activity was associated with an increased clinical effectiveness in patients with MCS [2, 7, 8]. In severe cases and/or in patients intolerant or ineligible to AT, the usefulness and safety of anti-cd20 monoclonal antibody rituximab (RTX) have been clearly shown in several studies.rtxwasshowntobehighlyeffectiveinmodifying the dynamics of B cells by deleting expanded clones and markedly improving MCS in most cases [9 11]. Peg-IFN plus RBV has been considered the standard AT for about a decade [12]. Recently, the direct acting antiviral drugs (DAAs), inhibitor of the nonstructural 3/4A HCV protease, boceprevir (BOC), and telaprevir, in combination with Peg-IFN and RBV, have consistently increased the likelihood
2 2 Case Reports in Immunology Table 1: Main clinical and laboratory data before rituximab (RTXbaseline), 2 months after rituximab cycle (BOC-baseline), and at the end of follow-up after boceprevir-based antiviral therapy (post- BOC). RTXbaseline (June 2011) BOCbaseline (September 2011) Post-BOC (November 2013) Gender Female Age (years) 63 IL28b rs T/T Stiffness (kpa) HCV titer (IU 10 6 /ml) NEG ALT (IU/L) MC manifestations Clinical Purpura ++ Arthralgia ++ + Weakness ++ Peripheral neuropathy Raynaud syndrome Nephritis Sicca syndrome Laboratory Cryocrit (%) RF (IU/mL) 24 <10 <10 C4 (mg/dl) RTX: rituximab; BOC: boceprevir; MC: mixed cryoglobulinemia; IL28B: polymorphism of interleukin-28b; stiffness: liver stiffness as evaluated by transient elastography; kpa: kilopascal; IU: international units; ALT: alanine aminotransferase; RF: rheumatoid factor. Normal values: <40 IU/L; normal values: <10 IU/mL; normal values: from 10 to 40 mg/dl. of response in patients infected with HCV genotype 1 (Gt 1a or 1b) [13, 14]. Few data are still available for patients with HCV-related MCS treated with DAAs [15 18] and no clear information exists about the combination with RTX. Here we describe, for the first time, a case of HCVrelated MCS treated with the combination of RTX and BOCbased triple AT and review the available literature about the combination of RTX and anti-hcv therapy. 2. Case Report In May, 2010, a 63-year-old woman with a 30-year history of HCV (Gt 1b) chronic infection and harboring compensated liver cirrhosis with normal liver function tests and no signs of portal hypertension was evaluated at the MASVE Center of the University of Florence. The main clinical and laboratory data are detailed in Table 1.The analysis of cryocrit was performed in the MASVE laboratory at every medical appointment. Briefly, the patient blood was kept at C to avoid CGs precipitation; immediately after centrifugation, a special graduated glass tube (Wintrobe tube) has been filled with1.0mlofserum,placedat4 C, and examined after at least 7 days to assess the percentage of packed cryoglobulins. The reduction of C4 complement component and the RF levels was performed as routine tests by the Centralized Diagnostic Laboratory of the Careggi Hospital, Florence, Italy, by immunoturbidimetric method and immunoenzymatic assay, respectively. Since 2008, the patient showed a typical MCS [19] characterized by recurrent lower limb purpura, arthralgia/ arthritis of hands and shoulders, and burning paresthesia with bootie distribution. She repeatedly scored positive for mixed type II (polyclonal IgG/monoclonal IgMk) cryoglobulins as well as rheumatoid factor (RF), increased inflammatory markers, and low C4. The patient previously failed two Peg-IFNα-2b+RBV treatments. Her interleukin-28b (IL28b) genotype (rs ) was T/T, a negative predictor of response to IFN-based therapy [20]. In June 2010, the patient underwent treatment with RTX (1 g twice monthly) which led to a complete MCS clinical response, with improvement in all baseline clinical manifestations [21]. After recurrence of symptoms in July 2011, the treatment was repeated. Clinical conditions consistently improved and in September 2011 the patient underwent AT. The BOC-based treatment was chosen on the basis of negative predictors of response [12]and higher efficacy of triple therapy compared to dual one. After a 4-week lead-in phase with Peg-IFNα-2b (1.5 μg/ Kg/week, subcutaneously) plus RBV (800 mg/daily, orally), BOC was added (800 mg three times daily, orally) and triple therapy was continued for 44 weeks. Viremia disappeared 1 week after BOC administration and remained negative throughout therapy and follow-up (sustained virological response). The cryocrit scored negative during therapy and followup and C4 and RF remained persistently normal (Table 1 and Figure 1). During treatment, the patient did not experience purpura or arthritis. She developed anemia and neutropenia requiring administration of erythropoietin and granulokines and reduction of RBV (600 mg/daily). After therapy, the patient was regularly checked up every three months. During every scheduled check-up C4, RF, cryocrit levels as well as liver functional parameters, and viremia were evaluated (data not shown). We observed long-term clinical and virological response: after a 15-month follow-up, the patient no longer had purpura, arthritis, or other baseline symptoms. Persistence of mild xerostomia and xerophthalmia was occasionally treated with symptomatic drugs (Table 1). 3. Review of the Literature We performed a literature search on PubMed about combined/sequential treatment of MC (Table 2). In the first pilot study, Saadoun et al. treated 16 consecutive, unselected refractory HCV-MC patients with RTX followed by AT with Peg-IFN and RBV. 15/16 patients showed clinical improvement, with a good profile of safety [22].
3 Case Reports in Immunology 3 Viremia (UI/mL) 1.00E E E E E E E + 01 RF (IU/mL), C4 (mg/dl), and cryocrit (%) E w3 w4 w5 w6 w7 w8 w12 w17 w20 w24 w30 w34 w38 w43 w47 f. up 1 m f. up 2 m f. up 3 m f. up 5 m f. up 6 m f. up 9 m f. up 15 m 0 June 2011 September 2011 November 2013 (a) (b) Figure 1: (a) Viral kinetics: a slight decrease in serum HCV RNA values was observed during the lead-in phase. Soon after the introduction of boceprevir (week 4), a drastic reduction in viremia was observed, with complete negativization at week 5. The vertical dashed line represents the introduction of boceprevir; the horizontal continuous line indicates the detection limit of the HCV RNA test (15 IU/mL). IU: international units; ml: milliliter; w: week; f. up: follow up; m: month. (B) Cryocrit C4 and RF kinetics during the combined therapy (RTX+Peg- IFN+RBV+BOC). The time points considered are (1) before rituximab (June 2011), (2) two months after rituximab cycle (September 2011; triple therapy baseline), and (3) end of the follow-up after boceprevir-based antiviral therapy (November 2013). After RTX therapy cryocrit, C4 and RF normalized and remained persistently normal. (e)cryocrit;( ) rheumatoid factor; ( ) C4. RF: rheumatoid factor; normal values: <10IU/mL;normalvaluesofC4:from10to40mg/dL. Table 2: Combined treatment with antiviral therapy and rituximab in MC patients: review of the literature. Author Patients Main indication Regimen Saadoun et al., 2008 [22] Terrier et al., 2009 [23] Dammacco et al., 2010 [24] Saadoun et al., 2010 [25] Ignatova et al., 2014 [26] 16 Refractory MC 20 Severe MC MC (naïve patients) MC (unselected) 6 SevereMC (RTX 375 mg/sqm 4 Peg IFNα2b + +RBV ++ after a month) (RTX 375 mg/sqm 4or1gr 2 Peg IFNα2b + +RBV ++ after a month) CT (RTX 375 mg/sqm 4weekly+two5 monthly inf. + Peg IFNα2b + or α2a RBV ++ ) (RTX 375 mg/sqm 4or1gr 2 Peg IFNα2b + or α2a +++ +RBV ++ after a month) (RTX n.d. dose Peg IFNα +RBV ++ after a month) Therapy outcome (CR/PR/NR) AEs (10/6/1) 2 (16/3/1) 4 (12/5/5) 3 (28/9/1) 5 + (n.d./n.d./n.d.) MC: mixed cryoglobulinemia; : sequential treatment; CT: combined treatment; CR: complete response, PR: partial response, NR: no response; AEs: adverse events (requiring antiviral treatment interruption); n.d.: not determined mcg/kg weekly; ++ weight-based; mcg weekly. One worsening of peripheral neuropathy case and 1 flare of psoriasis case. Two hematologic toxicity cases; 1 flare of psoriasis case; 1 hepatocarcinoma case. One severe anemia case; 2 grade 4 neutropenia cases. + Two hematologic toxicity cases; 1 depression case; 1 flare of psoriasis cases; 1 neuropathy case. n.d.
4 4 Case Reports in Immunology A subsequent study of Terrier et al. comprised 32 severe HCV-MCS patients, treated either with RTX monotherapy (12 patients) or with RTX followed by AT (20 patients, 11 already included in the previous pilot study). The authors reported the efficacy of RTX, with a better response in RTX/Peg-IFN+RBV group [23]. In 2010 Dammacco et al. and Saadoun et al. published two studies on the use of RTX and AT with Peg-IFN+RBV according to a combined [24]or sequential[25]scheme. In the first study, 37 HCV-MCS patients, naïve for IFNs or previous administration of immunosuppressive drugs, were randomized to get a RTX/Peg-IFN+RBV treatment (22 patients) or Peg-IFN+RBV (15 patients, controls) [24]. Patients in the first group obtained a significantly higher rate of complete and sustained response, without increase of adverse events. Inthesecondstudy,aprospective,nonrandomisedcohort study of 93 patients, Saadoun et al. found that combined therapy reduced the clinical remission time, improved renal response rate, and led to higher rates of cryoglobulin clearance and clonal VH1-69+B cell suppression than Peg- IFN+RBV alone [25]. In a recent letter, Ignatova and coworkers described 18 patients who underwent AT with Peg-IFN+RBV. In six subjects, RTX was administered 1 month before AT in order to treat severe MC. Data of this report confirm that AT increases the relapse-free survival compared with standard immunosuppression or RTX alone and that combined RTX/AT schedule can be useful in moderate/severe MC [26, 27]. 4. Discussion Patients response to AT has been shown to be lower in HCV patients with MC than without, after both double (Peg-IFN+RBV) and BOC-based triple therapy [15, 28]. The reasons for a lower propensity to eradicate HCV are unknown but are possibly related to a stronger involvement of lymphatic cells (especially B-cell) by the infection in MC [1] leading to more consistent viral reservoirs and, when using DAAs, a higher risk of viral mutations. The usefulness and safety of RTX in MC have been clearly shown in numerous studies, including also patients with advanced liver disease [11, 21, 29 31], even if most patients treated with RTX-monotherapy experienced vasculitis relapse following B-cell recovery [23]. Combined therapy with RTX plus Peg-IFN+RBV, according to a sequential or contemporary scheme, has previously provided an improvement of clinical response and higher cryoglobulinclearancethanpeg-ifn+rbv,intheabsence of increasing adverse events [23 25, 32]. The pathogenetic bases could be linked to the association of cooperating mechanisms,liketheviraleradicationandthedepletion of the pathological B-cell clones. Furthermore, the B-cell depletion could favor the elimination of a viral reservoir. On the other hand, the clinical improvement obtained with RTX treatment could make eligible to AT patients previously not eligible. Interestingly, in our previous study on 35 HCV chronically infected subjects, the only MCS patient who persistently responded to treatment was the one excluded from the comparative analysis owing to a recent treatment with RTX [15]. In the same study we showed a sudden decrease in cryocrit together with the rapid decrease of viremia due to the introduction of BOC, stressing the role exerted by viral replication in MC pathogenesis [15]. In conclusion, we are reporting here the first description of a safe and highly efficacious combination of RTX and BOC-based AT in a patient with cryoglobulinemic vasculitis. The persistent response was both virological and clinical. Our previous observation of a low rate of virological response in MCS patients may increase the interest of this report which seems to agree with the hypothesis of a key role played by B cells as HCV reservoirs. Such an observation appears toconfirmthepositiveeffectofacombinedtherapeutic approach also when using DAA-dependent AT. These results were, however, obtained in a single case and further studies based on significant numbers of patients are needed in order to confirm our observations in the specific setting of patients with HCV-related MC. Conflict of Interests All the authors declare no conflict of interests. Acknowledgments This work was supported by grants from the Istituto Toscano Tumori (ITT) and Ente Cassa di Risparmio di Firenze ; Laura Gragnani is supported by a 2015 fellowship Fondazione Umberto Veronesi ; Elisa Fognani is supported by an AIRC fellowship. References [1] A. L. Zignego, L. Gragnani, C. Giannini, and G. Laffi, The hepatitis C virus infection as a systemic disease, Internal and Emergency Medicine,vol.7,supplement3,pp.S201 S208,2012. [2] A. L. Zignego, C. Giannini, and L. Gragnani, HCV and lymphoproliferation, Clinical and Developmental Immunology,vol. 2012, Article ID , 8 pages, [3] L.Bonomo,M.Casato,A.Afeltra,andD.Caccavo, Treatment of idiopathic mixed cryoglobulinemia with alpha interferon, The American Medicine, vol.83,no.4,pp , [4] C. Ferri, E. Marzo, G. Longombardo et al., Interferon-α in mixed cryoglobulinemia patients: a randomized, crossovercontrolled trial, Blood, vol. 81, no. 5, pp , [5] R.Misiani,P.Bellavita,D.Fenilietal., Interferonalfa-2atherapy in cryoglobulinemia associated with hepatitis C virus, The New England Medicine, vol.330,no.11,pp , [6] V. M. Lauta and A. de Sangro, Long-term results regarding the use of recombinant interferon alpha-2b in the treatment of II type mixed essential cryoglobulinemia, Medical Oncology,vol. 12, no. 4, pp , 1995.
5 Case Reports in Immunology 5 [7]P.Cacoub,L.Gragnani,C.Comarmond,andA.L.Zignego, Extrahepatic manifestations of chronic hepatitis C virus infection, Digestive and Liver Disease,vol.46,pp.S165 S173,2014. [8]A.L.Zignego,L.Gragnani,A.Pilusoetal., Virus-driven autoimmunity and lymphoproliferation: the example of HCV infection, Expert Review of Clinical Immunology, vol. 11, no. 1, pp , [9] F. Zaja, S. de Vita, C. Mazzaro et al., Efficacy and safety of rituximab in type II mixed cryoglobulinemia, Blood,vol.101,no. 10, pp , [10] M. Pietrogrande, S. de Vita, A. L. Zignego et al., Recommendations for the management of mixed cryoglobulinemia syndrome in hepatitis C virus-infected patients, Autoimmunity Reviews,vol.10,no.8,pp ,2011. [11] S. De Vita, L. Quartuccio, M. Isola et al., A randomized controlled trial of rituximab for the treatment of severe cryoglobulinemic vasculitis, Arthritis and Rheumatism,vol.64,no.3,pp , [12] European Association for the Study of the Liver, EASL clinical practice guidelines: management of hepatitis C virus infection, Hepatology, vol. 55, no. 2, pp , [13]F.Poordad,J.McConeJr.,B.R.Baconetal., Boceprevirfor untreated chronic HCV genotype 1 infection, The New England Medicine, vol. 364, no. 13, pp , [14] I.M.Jacobson,J.G.McHutchison,G.Dusheikoetal., Telaprevir for previously untreated chronic hepatitis C virus infection, The New England Medicine,vol.364,no.25,pp , [15] L. Gragnani, A. Fabbrizzi, E. Triboli et al., Triple antiviral therapy in hepatitis C virus infection with or without mixed cryoglobulinaemia: a prospective, controlled pilot study, Digestive and Liver Disease,vol.46,no.9,pp ,2014. [16] D. Saadoun, M. R. Rigon, V. Thibault et al., Peg-IFNα/ribavirin/protease inhibitor combination in hepatitis C virus associated mixed cryoglobulinemia vasculitis: results at week 24, Annals of the Rheumatic Diseases, vol.73,no.5,pp , [17] S.DeNicola,A.Aghemo,M.R.Campiseetal., Telaprevirina patient with chronic hepatitis C and cryoglobulinemic glomerulonephritis, Antiviral Therapy, vol. 19, no. 5, pp , [18] D. Saadoun, M. Resche Rigon, S. Pol et al., PegIFNα/ribavirin/protease inhibitor combination in severe hepatitis C virus-associated mixed cryoglobulinemia vasculitis, Hepatology,vol.62,no.1,pp.24 30,2015. [19] S. De Vita, F. Soldano, M. Isola et al., Preliminary classification criteria for the cryoglobulinaemic vasculitis, Annals of the Rheumatic Diseases, vol. 70, no. 7, pp , [20] A. Piluso, C. Giannini, E. Fognani et al., Value of IL28B genotyping in patients with HCV-related mixed cryoglobulinemia: results of a large, prospective study, Viral Hepatitis, vol.20,no.4,pp.e107 e114,2013. [21] A. Petrarca, L. Rigacci, P. Caini et al., Safety and efficacy of rituximab in patients with hepatitis C virus-related mixed cryoglobulinemia and severe liver disease, Blood, vol. 116, no. 3, pp , [22] D.Saadoun,M.Resche-Rigon,D.Sene,L.Perard,A.Karras,and P. Cacoub, Rituximab combined with Peg-interferon-ribavirin in refractory hepatitis C virus-associated cryoglobulinaemia vasculitis, Annals of the Rheumatic Diseases,vol.67, no.10,pp , [23] B. Terrier, D. Saadoun, D. Sène et al., Efficacy and tolerability of rituximab with or without PEGylated interferon alfa-2b plus ribavirin in severe hepatitis C virus-related vasculitis: a long-term followup study of thirty-two patients, Arthritis & Rheumatism,vol.60,no.8,pp ,2009. [24] F. Dammacco, F. A. Tucci, G. Lauletta et al., Pegylated interferon-α, ribavirin, and rituximab combined therapy of hepatitis C virus-related mixed cryoglobulinemia: a long-term study, Blood,vol.116,no.3,pp ,2010. [25] D. Saadoun, M. R. Rigon, D. Sene et al., Rituximab plus Peginterferon-alpha/ribavirin compared with Peg-interferonalpha/ribavirin in hepatitis C-related mixed cryoglobulinemia, Blood,vol.116,no.3,pp , ,2010. [26] T.Ignatova,O.Chernova,P.Novikov,andS.Moiseev, HCVassociated cryoglobulinaemic vasculitis: triple/dual antiviral treatment and/or rituximab? Annals of the Rheumatic Diseases, vol.73,no.9,articlee58,2014. [27] D. Saadoun and P. Cacoub, HCV-associated cryoglobulinemic vasculitis: triple/dual antiviral treatment and/or rituximab? Reply to the comment by Ignatova et al, Annals of the Rheumatic Diseases,vol.73,no.9,articlee59,2014. [28] L.Gragnani,E.Fognani,A.Pilusoetal., Long-termeffectof HCV eradication in patients with mixed cryoglobulinemia: A prospective, controlled, open-label, cohort study, Hepatology, [29] F. Zaja, D. Russo, G. Fuga, F. Patriarca, A. Ermacora, and M. Baccarani, Rituximab for the treatment of type II mixed cryoglobulinemia, Haematologica, vol. 84, no. 12, pp , [30]D.Sansonno,V.deRe,G.Lauletta,F.A.Tucci,M.Boiocchi, and F. Dammacco, Monoclonal antibody treatment of mixed cryoglobulinemia resistant to interferon α with an anti-cd20, Blood,vol.101,no.10,pp ,2003. [31] C. Ferri, P. Cacoub, C. Mazzaro et al., Treatment with rituximab in patients with mixed cryoglobulinemia syndrome: results of multicenter cohort study and review of the literature, Autoimmunity Reviews, vol. 11, no. 1, pp , [32] E. Mauro, M. Pedata, A. Ermacora, and C. Mazzaro, An additional line of therapy with pegylated interferon and ribavirin after rituximab in a patient with hepatitis C virus-related mixed cryoglobulinaemia and indolent non-hodgkin s lymphoma previously treated with interferon, Blood Transfusion, vol. 10, no. 1, pp , 2012.










6 MEDIATORS of INFLAMMATION The Scientific World Journal Gastroenterology Research and Practice Diabetes Research International Endocrinology Immunology Research Disease Markers Submit your manuscripts at BioMed Research International PPAR Research Obesity Ophthalmology Evidence-Based Complementary and Alternative Medicine Stem Cells International Oncology Parkinson s Disease Computational and Mathematical Methods in Medicine AIDS Behavioural Neurology Research and Treatment Oxidative Medicine and Cellular Longevity
Department of Internal Medicine, Pordenone General Hospital, Italy; 2
 Le Infezioni in Medicina, n. 4, 337-341, Caso clinico Case reports Recombinant Human Erythropoietin (RHuEpo) and Granular Colony Stimulating Factor (G-CSF) in hepatitis C virus (HCV) related to mixed cryoglobulinaemia
Le Infezioni in Medicina, n. 4, 337-341, Caso clinico Case reports Recombinant Human Erythropoietin (RHuEpo) and Granular Colony Stimulating Factor (G-CSF) in hepatitis C virus (HCV) related to mixed cryoglobulinaemia
Prior Authorization Guideline
 Prior Authorization Guideline Guideline Name Olysio (simeprevir) Formulary UnitedHealthcare Community & State Formulary Note Approval Date 2/19/2014 Revision Date 7/9/2014 1. Indications Drug Name: Olysio
Prior Authorization Guideline Guideline Name Olysio (simeprevir) Formulary UnitedHealthcare Community & State Formulary Note Approval Date 2/19/2014 Revision Date 7/9/2014 1. Indications Drug Name: Olysio
CHRONIC HCV TREATMENT: In Special Populations.
 CHRONIC HCV TREATMENT: In Special Populations. By Taher EL-ZANATY Prof. of Internal Medicine CAIRO UNIVERSITY Introduction: HCV is the major cause of chronic hepatitis in Egypt. Its end stage is liver
CHRONIC HCV TREATMENT: In Special Populations. By Taher EL-ZANATY Prof. of Internal Medicine CAIRO UNIVERSITY Introduction: HCV is the major cause of chronic hepatitis in Egypt. Its end stage is liver
Case Report Successful Antiviral Triple Therapy in a Longstanding Refractory Hepatitis C Virus Infection with an Acute Kidney Injury
 Case Reports in Nephrology, Article ID 308729, 4 pages http://dx.doi.org/10.1155/2014/308729 Case Report Successful Antiviral Triple Therapy in a Longstanding Refractory Hepatitis C Virus Infection with
Case Reports in Nephrology, Article ID 308729, 4 pages http://dx.doi.org/10.1155/2014/308729 Case Report Successful Antiviral Triple Therapy in a Longstanding Refractory Hepatitis C Virus Infection with
Hepatitis C: Management of Previous Non-responders with First Line Protease Inhibitors
 Hepatitis C: Management of Previous Non-responders with First Line Protease Inhibitors Fred Poordad, MD The Texas Liver Institute Clinical Professor of Medicine University of Texas Health Science Center
Hepatitis C: Management of Previous Non-responders with First Line Protease Inhibitors Fred Poordad, MD The Texas Liver Institute Clinical Professor of Medicine University of Texas Health Science Center
Peg-IFNα/ribavirin/protease inhibitor combination in hepatitis C virus associated mixed cryoglobulinemia vasculitis: results at week 24
 EXTENDED REPORT Peg-IFNα/ribavirin/protease inhibitor combination in hepatitis C virus associated mixed cryoglobulinemia vasculitis: results at week 24 David Saadoun, 1,2 M Resche Rigon, 3 V Thibault,
EXTENDED REPORT Peg-IFNα/ribavirin/protease inhibitor combination in hepatitis C virus associated mixed cryoglobulinemia vasculitis: results at week 24 David Saadoun, 1,2 M Resche Rigon, 3 V Thibault,
5/12/2016. Learning Objectives. Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients
 5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
Hepatitis C virus (HCV) is a major health problem
 is a major health problem") AMERICAN ASSOCIATION FOR THE STUDY OFLIVERD I S E ASES HEPATOLOGY, VOL. 64, NO. 5, 2016 Prospective Study of Guideline-Tailored Therapy With Direct-Acting Antivirals for Hepatitis C Virus-Associated Mixed
AMERICAN ASSOCIATION FOR THE STUDY OFLIVERD I S E ASES HEPATOLOGY, VOL. 64, NO. 5, 2016 Prospective Study of Guideline-Tailored Therapy With Direct-Acting Antivirals for Hepatitis C Virus-Associated Mixed
Hepatitis C Management and Treatment
 Hepatitis C Management and Treatment Kaya Süer Near East University Faculty of Medicine Infectious Diseases and Clinical Microbiology 1 Discovery of Hepatitis C Key facts Hepatitis C: the virus can cause
Hepatitis C Management and Treatment Kaya Süer Near East University Faculty of Medicine Infectious Diseases and Clinical Microbiology 1 Discovery of Hepatitis C Key facts Hepatitis C: the virus can cause
CRIOGLOBULINEMIA MISTA E LINFOMI NELL ERA DEI DAAs DI II GENERAZIONE. Anna Linda Zignego
 CRIOGLOBULINEMIA MISTA E LINFOMI NELL ERA DEI DAAs DI II GENERAZIONE Anna Linda Zignego Eur J Gastroenterol Hepatol, 2017 MC: in the setting of HCV-related pathologies, a typically female disease Direct
CRIOGLOBULINEMIA MISTA E LINFOMI NELL ERA DEI DAAs DI II GENERAZIONE Anna Linda Zignego Eur J Gastroenterol Hepatol, 2017 MC: in the setting of HCV-related pathologies, a typically female disease Direct
ASSAYS UTILZIED TO MONITOR HCV AND ITS TREATMENT
 ASSAYS UTILZIED TO MONITOR HCV AND ITS TREATMENT Mitchell L Shiffman, MD Liver Institute of Virginia Bon Secours Health System Richmond and Newport News, VA Liver Institute of Virginia Education, Research
ASSAYS UTILZIED TO MONITOR HCV AND ITS TREATMENT Mitchell L Shiffman, MD Liver Institute of Virginia Bon Secours Health System Richmond and Newport News, VA Liver Institute of Virginia Education, Research
Prior Authorization Guideline
 Prior Authorization Guideline Guideline Name Sovaldi (sofosbuvir) Formulary UnitedHealthcare Community & State Formulary Note Approval Date 2/19/2014 Revision Date 7/8/2014 1. Indications Drug Name: Sovaldi
Prior Authorization Guideline Guideline Name Sovaldi (sofosbuvir) Formulary UnitedHealthcare Community & State Formulary Note Approval Date 2/19/2014 Revision Date 7/8/2014 1. Indications Drug Name: Sovaldi
considered for patients with cryoglobulinemic kidney diseases. (Weak)
") http://www.kidney-international.org & 2008 DIGO Guideline 5: Diagnosis and management of kidney diseases associated with HCV infection idney International (2008) 73 (Suppl 109), S69 S77; doi:10.1038/ki.2008.88
http://www.kidney-international.org & 2008 DIGO Guideline 5: Diagnosis and management of kidney diseases associated with HCV infection idney International (2008) 73 (Suppl 109), S69 S77; doi:10.1038/ki.2008.88
Should Elderly CHC Patients (>70 years old) be Treated?
 be Treated?") Should Elderly CHC Patients (>70 years old) be Treated? Deepak Amarapurkar Consultant Gastroenterologist & Hepatologist Bombay Hospital & Medical Research Center, Mumbai & Jagjivanram Western Railway Hospital,
Should Elderly CHC Patients (>70 years old) be Treated? Deepak Amarapurkar Consultant Gastroenterologist & Hepatologist Bombay Hospital & Medical Research Center, Mumbai & Jagjivanram Western Railway Hospital,
SECTION 1: OLYSIO with (PEGASYS) AND RIBAVIRIN SECTION 2: OLYSIO with (PEGINTRON) AND RIBAVIRIN RATIONALE FOR INCLUSION IN PA PROGRAM
 AND RIBAVIRIN SECTION 2: OLYSIO with (PEGINTRON) AND RIBAVIRIN RATIONALE FOR INCLUSION IN PA PROGRAM") SECTION 1: OLYSIO with (PEGASYS) AND RIBAVIRIN SECTION 2: OLYSIO with (PEGINTRON) AND RIBAVIRIN RATIONALE FOR INCLUSION IN PA PROGRAM SECTION 1: OLYSIO with (PEGASYS) AND RIBAVIRIN Background Hepatitis
SECTION 1: OLYSIO with (PEGASYS) AND RIBAVIRIN SECTION 2: OLYSIO with (PEGINTRON) AND RIBAVIRIN RATIONALE FOR INCLUSION IN PA PROGRAM SECTION 1: OLYSIO with (PEGASYS) AND RIBAVIRIN Background Hepatitis
Treatment of Hepatitis C in HIV-Coinfected Patients. Vincent Soriano Department of Infectious Diseases Hospital Carlos III Madrid, Spain
 Treatment of Hepatitis C in HIV-Coinfected Patients Vincent Soriano Department of Infectious Diseases Hospital Carlos III Madrid, Spain Estimated no. of persons infected with HIV and hepatitis viruses
Treatment of Hepatitis C in HIV-Coinfected Patients Vincent Soriano Department of Infectious Diseases Hospital Carlos III Madrid, Spain Estimated no. of persons infected with HIV and hepatitis viruses
Oral combination therapy: future hepatitis C virus treatment? "Lancet Oct 30;376(9751): Oral combination therapy with a nucleoside
: Oral combination therapy with a nucleoside") Author manuscript, published in "Journal of Hepatology 2011;55(4):933-5" DOI : 10.1016/j.jhep.2011.04.018 Oral combination therapy: future hepatitis C virus treatment? Commentary article on the following
Author manuscript, published in "Journal of Hepatology 2011;55(4):933-5" DOI : 10.1016/j.jhep.2011.04.018 Oral combination therapy: future hepatitis C virus treatment? Commentary article on the following
Length of Authorization: 8-16 weeks. Requires PA: All direct-acting antivirals for treatment of Hepatitis C. Approval Criteria
 Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure appropriate
Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure appropriate
Clinical Cases Hepatitis C Naïve Patients. Rafael Esteban Liver Unit. Hospital General Universitari Vall Hebron. Barcelona.
 Clinical Cases Hepatitis C Naïve Patients Rafael Esteban Liver Unit. Hospital General Universitari Vall Hebron. Barcelona. Case study 1 27 year old woman, Diagnosed with Chronic Hepatitis C 3 years ago
Clinical Cases Hepatitis C Naïve Patients Rafael Esteban Liver Unit. Hospital General Universitari Vall Hebron. Barcelona. Case study 1 27 year old woman, Diagnosed with Chronic Hepatitis C 3 years ago
Treatment of genotype 4 patient. with cirrhosis. Vincent LEROY Clinique Universitaire d Hépato-Gastroentérologie INSERM U823 CHU de Grenoble
 Treatment of genotype 4 patient with cirrhosis Vincent LEROY Clinique Universitaire d Hépato-Gastroentérologie INSERM U823 CHU de Grenoble Clinical case 52 year-old patient Intra-venous drug user 1987-1989
Treatment of genotype 4 patient with cirrhosis Vincent LEROY Clinique Universitaire d Hépato-Gastroentérologie INSERM U823 CHU de Grenoble Clinical case 52 year-old patient Intra-venous drug user 1987-1989
29th Viral Hepatitis Prevention Board Meeting
 29th Viral Hepatitis Prevention Board Meeting Madrid, November 2006 Treatment of chronic hepatitis C José M. Sánchez-Tapias Liver Unit Hospital Clínic University of Barcelona Spain CHRONIC HEPATITIS C
29th Viral Hepatitis Prevention Board Meeting Madrid, November 2006 Treatment of chronic hepatitis C José M. Sánchez-Tapias Liver Unit Hospital Clínic University of Barcelona Spain CHRONIC HEPATITIS C
CURRENT TREATMENTS. Mitchell L Shiffman, MD Director Liver Institute of Virginia. Richmond and Newport News, VA, USA
 CURRENT TREATMENTS FOR HCV Mitchell L Shiffman, MD Director Liver Institute of Virginia Bon Secours Health System Richmond and Newport News, VA, USA Liver Institute of Virginia Education, Research and
CURRENT TREATMENTS FOR HCV Mitchell L Shiffman, MD Director Liver Institute of Virginia Bon Secours Health System Richmond and Newport News, VA, USA Liver Institute of Virginia Education, Research and
Professor Patrice Cacoub
 Five Nations Conference on HIV and Hepatitis in partnership with Professor Patrice Cacoub La Pitié-Salpêtrière Hospital, Paris, France HCV and its Extra Hepatic Manifestations: From Immune- to Inflammatory-Related
Five Nations Conference on HIV and Hepatitis in partnership with Professor Patrice Cacoub La Pitié-Salpêtrière Hospital, Paris, France HCV and its Extra Hepatic Manifestations: From Immune- to Inflammatory-Related
How to optimize current therapy for GT1 patients Shortened therapy with IFNa-based therapy
 How to optimize current therapy for GT1 patients Shortened therapy with IFNa-based therapy Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Leber- und Studienzentrum
How to optimize current therapy for GT1 patients Shortened therapy with IFNa-based therapy Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Leber- und Studienzentrum
Management of CHC G1 patients who are relapsers or non-responders to Peg IFN and RBV therapy: Wait or Triple Therapy?
 Management of CHC G1 patients who are relapsers or non-responders to Peg IFN and RBV therapy: Wait or Triple Therapy? Prof. Teerha Piratvisuth NKC Institute of Gastroenterology and Hepatology Prince of
Management of CHC G1 patients who are relapsers or non-responders to Peg IFN and RBV therapy: Wait or Triple Therapy? Prof. Teerha Piratvisuth NKC Institute of Gastroenterology and Hepatology Prince of
Protease inhibitor based triple therapy in treatment experienced patients
 Protease inhibitor based triple therapy in treatment experienced patients Universitätsklinikum Leipzig Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Leber
Protease inhibitor based triple therapy in treatment experienced patients Universitätsklinikum Leipzig Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Leber
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Hepatitis C First Generation Agents Page 1 of 16 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C First Generation Agents - Through Preferred
Hepatitis C First Generation Agents Page 1 of 16 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C First Generation Agents - Through Preferred
Express Scripts, Inc. monograph dated 5/25/2011; selected revision 6/1/2011
 BENEFIT DESCRIPTION AND LIMITATIONS OF COVERAGE ITEM: PRODUCT LINES: COVERED UNDER: DESCRIPTION: CPT/HCPCS Code: Company Supplying: Setting: Coverage Criteria: Approval Period: Victrelis (boceprevir capsules)
BENEFIT DESCRIPTION AND LIMITATIONS OF COVERAGE ITEM: PRODUCT LINES: COVERED UNDER: DESCRIPTION: CPT/HCPCS Code: Company Supplying: Setting: Coverage Criteria: Approval Period: Victrelis (boceprevir capsules)
HCV Treat now! Robert G Gish MD. Professor Consultant Stanford University
 HCV Treat now! Robert G Gish MD Professor Consultant Stanford University Steering committee and Executive Board NVHR National Viral Hepatitis Roundtable Founding Member CEVHAP Singapore Viral Hepatitis
HCV Treat now! Robert G Gish MD Professor Consultant Stanford University Steering committee and Executive Board NVHR National Viral Hepatitis Roundtable Founding Member CEVHAP Singapore Viral Hepatitis
Pegylated Interferon Agents for Hepatitis C
 Applicable X X X X X X X Pegylated Interferon Agents for Hepatitis C Override(s) Prior Authorization Quantity Limit Initial for Monotherapy or Combination with Ribavirin based on Genotype, Status, or Co-Infection
Applicable X X X X X X X Pegylated Interferon Agents for Hepatitis C Override(s) Prior Authorization Quantity Limit Initial for Monotherapy or Combination with Ribavirin based on Genotype, Status, or Co-Infection
Hepatitis C Virus Clinical Criteria Update September 18, For: New York State Medicaid
 Hepatitis C Virus Clinical Criteria Update September 18, 2014 For: New York State Medicaid 1 Purpose Characterize the place in therapy for the agents utilized for management of chronic hepatitis C (CHC)
Hepatitis C Virus Clinical Criteria Update September 18, 2014 For: New York State Medicaid 1 Purpose Characterize the place in therapy for the agents utilized for management of chronic hepatitis C (CHC)
Simeprevir + PEG + RBV in Treatment-Naïve Genotype 1 QUEST-1 Trial
 Phase 3 Treatment Naïve Simeprevir + in Treatment-Naïve Genotype 1 QUEST-1 Trial Jacobson IM, et al. Lancet. 2014;384:403-13. Simeprevir + PEG + Ribavirin for Treatment-Naïve HCV GT1 QUEST-1 Trial QUEST-1
Phase 3 Treatment Naïve Simeprevir + in Treatment-Naïve Genotype 1 QUEST-1 Trial Jacobson IM, et al. Lancet. 2014;384:403-13. Simeprevir + PEG + Ribavirin for Treatment-Naïve HCV GT1 QUEST-1 Trial QUEST-1
ةي : لآا ةرقبلا ةروس
 سورة البقرة: اآلية HCV RELAPSERS AND NONRESPONDERS: How to deal with them? BY Prof. Mohamed Sharaf-Eldin Prof. of Hepatology and Gastroenterology Tanta University Achieving SVR The ability to achieve a
سورة البقرة: اآلية HCV RELAPSERS AND NONRESPONDERS: How to deal with them? BY Prof. Mohamed Sharaf-Eldin Prof. of Hepatology and Gastroenterology Tanta University Achieving SVR The ability to achieve a
Length of Authorization: 8-16 weeks. Requires PA: All direct-acting antivirals for treatment of Hepatitis C. Approval Criteria
 Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure appropriate
Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure appropriate
Safety of Treatment in Cirrhotics in the Era of New Antiviral Therapies for Hepatitis C Virus
 Safety of Treatment in Cirrhotics in the Era of New Antiviral Therapies for Hepatitis C Virus JEFFREY NADELSON MD, ALAN EPSTEIN MD, THOMAS SEPE MD BOSTON UNIVERSITY SCHOOL OF MEDICINE ROGER WILLIAMS MEDICAL
Safety of Treatment in Cirrhotics in the Era of New Antiviral Therapies for Hepatitis C Virus JEFFREY NADELSON MD, ALAN EPSTEIN MD, THOMAS SEPE MD BOSTON UNIVERSITY SCHOOL OF MEDICINE ROGER WILLIAMS MEDICAL
UNIVERSITY OF MEDICINE AND PHARMACY OF CRAIOVA DOCTORAL SCHOOL DOCTORAL THESIS
 UNIVERSITY OF MEDICINE AND PHARMACY OF CRAIOVA DOCTORAL SCHOOL DOCTORAL THESIS PHARMACOGENETICS AND THE APPLICATION OF SINGLE NUCLEOTIDE POLYMORPHISMS IN RESPONSE TO PEGYLATED INTERFERON AND RIBAVIRIN
UNIVERSITY OF MEDICINE AND PHARMACY OF CRAIOVA DOCTORAL SCHOOL DOCTORAL THESIS PHARMACOGENETICS AND THE APPLICATION OF SINGLE NUCLEOTIDE POLYMORPHISMS IN RESPONSE TO PEGYLATED INTERFERON AND RIBAVIRIN
Treatment Options in HCV Relapsers and Nonresponders. Raymond T. Chung, M.D.
 Session IV Treatment Options in HCV Relapsers and Nonresponders Raymond T. Chung, M.D. Director of Hepatology, Massachusetts General Hospital, Associate Professor of Medicine, Harvard Medical School, Boston,
Session IV Treatment Options in HCV Relapsers and Nonresponders Raymond T. Chung, M.D. Director of Hepatology, Massachusetts General Hospital, Associate Professor of Medicine, Harvard Medical School, Boston,
Treatment with the New Direct Acting Antivirals for Hepatitis C
 Treatment with the New Direct Acting Antivirals for Hepatitis C Mary Olson, DNP, ANP-BC Clinical Trials Program Director Weill Cornell Medical College The Center for the Study of Hepatitis C Objectives
Treatment with the New Direct Acting Antivirals for Hepatitis C Mary Olson, DNP, ANP-BC Clinical Trials Program Director Weill Cornell Medical College The Center for the Study of Hepatitis C Objectives
CASE STUDY. Adverse Events in treatment chronic hepatitis C patients with PegInterferon and Ribavirin What would your management decision be?
 Adverse Events in treatment chronic hepatitis C patients with PegInterferon and Ribavirin What would your management decision be? CASE STUDY Pham Thi Thu Thuy MD, PhD Ho Chi Minh City Vietnam Serious Adverse
Adverse Events in treatment chronic hepatitis C patients with PegInterferon and Ribavirin What would your management decision be? CASE STUDY Pham Thi Thu Thuy MD, PhD Ho Chi Minh City Vietnam Serious Adverse
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Hepatitis B / Hepatitis C Peg-interferon Page 1 of 20 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis B / Hepatitis C Peg-interferon Hepatitis
Hepatitis B / Hepatitis C Peg-interferon Page 1 of 20 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis B / Hepatitis C Peg-interferon Hepatitis
Emerging Approaches for the Treatment of Hepatitis C Virus
 Emerging Approaches for the Treatment of Hepatitis C Virus Gap Analysis 1 Physicians may not be sufficiently familiar with the latest guidelines for chronic HCV treatment, including the initiation and
Emerging Approaches for the Treatment of Hepatitis C Virus Gap Analysis 1 Physicians may not be sufficiently familiar with the latest guidelines for chronic HCV treatment, including the initiation and
DAA-based treatment in cirrhotic and post-transplanted patients. Audrey Coilly, MD Hôpital Paul Brousse, Villejuif, France
 DAA-based treatment in cirrhotic and post-transplanted patients Audrey Coilly, MD Hôpital Paul Brousse, Villejuif, France Cirrhosis and transplantation 2 populations with similar issues Hepatic impairment
DAA-based treatment in cirrhotic and post-transplanted patients Audrey Coilly, MD Hôpital Paul Brousse, Villejuif, France Cirrhosis and transplantation 2 populations with similar issues Hepatic impairment
The role of triple therapy with protease inhibitors in hepatitis C virus genotype 1na «ve patients
 The role of triple therapy with protease inhibitors in hepatitis C virus genotype 1na «ve patients David R. Nelson Clinical and Translational Science Institute, University of Florida, FL, USA Liver International
The role of triple therapy with protease inhibitors in hepatitis C virus genotype 1na «ve patients David R. Nelson Clinical and Translational Science Institute, University of Florida, FL, USA Liver International
Introduction. The ELECTRON Trial
 63rd AASLD November 9-13, 12 Boston, Massachusetts Faculty Douglas T. Dieterich, MD Professor of Medicine and Director of CME Department of Medicine Director of Outpatient Hepatology Division of Liver
63rd AASLD November 9-13, 12 Boston, Massachusetts Faculty Douglas T. Dieterich, MD Professor of Medicine and Director of CME Department of Medicine Director of Outpatient Hepatology Division of Liver
Length of Authorization: 8-16 weeks. Requires PA: All direct-acting antivirals for treatment of Hepatitis C. Approval Criteria
 Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the medical evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure
Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the medical evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Hepatitis C First Generation Agents Page 1 of 18 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C First Generation Agents - Through Preferred
Hepatitis C First Generation Agents Page 1 of 18 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C First Generation Agents - Through Preferred
Treatment of chronic hepatitis C in HIV co-infected patients
 Treatment of chronic hepatitis C in HIV co-infected patients Vicente Soriano Department of Infectious Diseases Hospital Carlos III, Madrid, Spain The most prevalent chronic viral infections in humans HBV
Treatment of chronic hepatitis C in HIV co-infected patients Vicente Soriano Department of Infectious Diseases Hospital Carlos III, Madrid, Spain The most prevalent chronic viral infections in humans HBV
Topic: Sovaldi, sofosbuvir Date of Origin: March 14, Committee Approval Date: August 15, 2014 Next Review Date: March 2015
 Medication Policy Manual Policy No: dru332 Topic: Sovaldi, sofosbuvir Date of Origin: March 14, 2014 Committee Approval Date: August 15, 2014 Next Review Date: March 2015 Effective Date: October 1, 2014
Medication Policy Manual Policy No: dru332 Topic: Sovaldi, sofosbuvir Date of Origin: March 14, 2014 Committee Approval Date: August 15, 2014 Next Review Date: March 2015 Effective Date: October 1, 2014
General Statement for Drugs for the Treatment of Hepatitis C
 General Statement for Drugs for the Treatment of Hepatitis C Use the following criteria to determine patient eligibility for subsidisation under the PBS for hepatitis C treating agents. By writing a PBS
General Statement for Drugs for the Treatment of Hepatitis C Use the following criteria to determine patient eligibility for subsidisation under the PBS for hepatitis C treating agents. By writing a PBS
Hepatitis C: Management of Treatment Naïve Patients with First Line Protease Inhibitors
 Hepatitis C: Management of Treatment Naïve Patients with First Line Protease Inhibitors Eric Lawitz, MD, AGAF, CPI The Texas Liver Institute Clinical Professor of Medicine University of Texas Health Science
Hepatitis C: Management of Treatment Naïve Patients with First Line Protease Inhibitors Eric Lawitz, MD, AGAF, CPI The Texas Liver Institute Clinical Professor of Medicine University of Texas Health Science
Hepatitis: A Global Health. Concern
 Chapter 5 Hepatitis: A Global Health Extra-Hepatic Manifestations of Hepatitis C Virus Infection Clodoveo Ferri*; Michele Colaci 1 ; DiliaGiuggioli 1 1 Rheumatology Unit, University of Modena and Reggio
Chapter 5 Hepatitis: A Global Health Extra-Hepatic Manifestations of Hepatitis C Virus Infection Clodoveo Ferri*; Michele Colaci 1 ; DiliaGiuggioli 1 1 Rheumatology Unit, University of Modena and Reggio
Tratamiento de la Hepatitis C Rafael Esteban Hospital General Universitario Valle de Hebrón Barcelona
 Tratamiento de la Hepatitis C Rafael Esteban Hospital General Universitario Valle de Hebrón Barcelona rrent HCV Therapy 8% % sustained response 6% 4% 2% % 54-61% 41% 34% 25% 16% 6% IFN 24w IFN 48w Peg
Tratamiento de la Hepatitis C Rafael Esteban Hospital General Universitario Valle de Hebrón Barcelona rrent HCV Therapy 8% % sustained response 6% 4% 2% % 54-61% 41% 34% 25% 16% 6% IFN 24w IFN 48w Peg
Review Article Interferon Treatment of Hepatitis C Reinfection after Liver Transplantation: A Meta-Analysis
 Gastroenterology Research and Practice Volume 215, Article ID 2632, 8 pages http://dx.doi.org/1.1155/215/2632 Review Article Interferon Treatment of Hepatitis C Reinfection after Liver Transplantation:
Gastroenterology Research and Practice Volume 215, Article ID 2632, 8 pages http://dx.doi.org/1.1155/215/2632 Review Article Interferon Treatment of Hepatitis C Reinfection after Liver Transplantation:
Chronic Hepatitis C. Risk Factors
 Chronic Hepatitis C The hepatitis C virus is one of the most important causes of chronic liver disease in the United States. Almost 4 million Americans or 1.8 percent of the U.S. population have an antibody
Chronic Hepatitis C The hepatitis C virus is one of the most important causes of chronic liver disease in the United States. Almost 4 million Americans or 1.8 percent of the U.S. population have an antibody
Optimal ltherapy in non 1 genotypes:
 Optimal ltherapy in non 1 genotypes: genotype 2 and 3 patients Antonio Craxì GI & Liver Unit, Di.Bi.M.I.S. University of Palermo, Italy craxanto@unipa.it Peg IFN alpha plus ribavirin : SVR rate of >80%
Optimal ltherapy in non 1 genotypes: genotype 2 and 3 patients Antonio Craxì GI & Liver Unit, Di.Bi.M.I.S. University of Palermo, Italy craxanto@unipa.it Peg IFN alpha plus ribavirin : SVR rate of >80%
Intron A (interferon alfa-2b) with ribavirin, (Moderiba, Rebetol, Ribasphere, RibaTab, ribavirin tablets/capsules - all strengths)
 with ribavirin, (Moderiba, Rebetol, Ribasphere, RibaTab, ribavirin tablets/capsules - all strengths)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.06 Subject: Intron A Ribavirin Page: 1 of 6 Last Review Date: March 18, 2016 Intron A Ribavirin Description
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.06 Subject: Intron A Ribavirin Page: 1 of 6 Last Review Date: March 18, 2016 Intron A Ribavirin Description
Pierluigi Toniutto Clinica di Medicina Interna Azienda Ospedaliero Universitaria Udine
 Pierluigi Toniutto Clinica di Medicina Interna Azienda Ospedaliero Universitaria Udine Il sottoscritto dichiara di non aver avuto negli ultimi 12 mesi conflitto d interesse in relazione a questa presentazione
Pierluigi Toniutto Clinica di Medicina Interna Azienda Ospedaliero Universitaria Udine Il sottoscritto dichiara di non aver avuto negli ultimi 12 mesi conflitto d interesse in relazione a questa presentazione
REQUEST FOR PRIOR AUTHORIZATION Hepatitis C Treatments
 Fax completed form to: 866-940-7328 Prior Authorization Phone Number: 800-310-6826 IA Medicaid Member ID # Patient name Date of Birth Patient address Patient phone Provider NPI Prescriber name Phone Prescriber
Fax completed form to: 866-940-7328 Prior Authorization Phone Number: 800-310-6826 IA Medicaid Member ID # Patient name Date of Birth Patient address Patient phone Provider NPI Prescriber name Phone Prescriber
Intron A Hepatitis C. Intron A (interferon alfa-2b) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.05 Subject: Intron A Hepatitis C Page: 1 of 5 Last Review Date: November 30, 2018 Intron A Hepatitis
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.05 Subject: Intron A Hepatitis C Page: 1 of 5 Last Review Date: November 30, 2018 Intron A Hepatitis
Dr. Siddharth Srivastava
 Dr. Siddharth Srivastava MD, DM (Gastroenterology) Associate Professor GIPMER, New Delhi Rashtriya Gaurav Award 2013 for work on hepatitis B and C Set up Liver clinic at GIPMER and in charge EUS laboratory.
Dr. Siddharth Srivastava MD, DM (Gastroenterology) Associate Professor GIPMER, New Delhi Rashtriya Gaurav Award 2013 for work on hepatitis B and C Set up Liver clinic at GIPMER and in charge EUS laboratory.
Appendix This appendix was part of the submitted manuscript and has been peer reviewed. It is posted as supplied by the authors.
 Appendix This appendix was part of the submitted manuscript and has been peer reviewed. It is posted as supplied by the authors. Appendix to: Thompson AJV; Expert panel representing the Gastroenterological
Appendix This appendix was part of the submitted manuscript and has been peer reviewed. It is posted as supplied by the authors. Appendix to: Thompson AJV; Expert panel representing the Gastroenterological
EASL Clinical Practice Guidelines: Management of hepatitis C virus infection
 Clinical Practice Guidelines EASL Clinical Practice Guidelines: Management of hepatitis C virus infection European Association for the Study of the Liver Introduction Hepatitis C virus (HCV) infection
Clinical Practice Guidelines EASL Clinical Practice Guidelines: Management of hepatitis C virus infection European Association for the Study of the Liver Introduction Hepatitis C virus (HCV) infection
SYNOPSIS Final Clinical Study Report for Study AI444031
 Name of Sponsor/Company: Bristol-Myers Squibb Name of Finished Product: Name of Active Ingredient: () Individual Study Table Referring to the Dossier (For National Authority Use Only) SYNOPSIS for Study
Name of Sponsor/Company: Bristol-Myers Squibb Name of Finished Product: Name of Active Ingredient: () Individual Study Table Referring to the Dossier (For National Authority Use Only) SYNOPSIS for Study
Phase 3. Treatment Experienced. Ledipasvir-Sofosbuvir +/- Ribavirin in HCV Genotype 1 ION-2. Afdhal N, et al. N Engl J Med. 2014;370:
 Phase 3 Treatment Experienced Ledipasvir-Sofosbuvir +/- Ribavirin in HCV Genotype 1 ION-2 Afdhal N, et al. N Engl J Med. 2014;370:1483-93. Ledipasvir-Sofosbuvir +/- Ribavirin in Treatment-Experienced HCV
Phase 3 Treatment Experienced Ledipasvir-Sofosbuvir +/- Ribavirin in HCV Genotype 1 ION-2 Afdhal N, et al. N Engl J Med. 2014;370:1483-93. Ledipasvir-Sofosbuvir +/- Ribavirin in Treatment-Experienced HCV
Research Article Clinical Outcome of a Novel Anti-CD6 Biologic Itolizumab in Patients of Psoriasis with Comorbid Conditions
 Dermatology Research and Practice Volume 2, Article ID 13326, 4 pages http://dx.doi.org/.1155/2/13326 Research Article Clinical Outcome of a Novel Anti-CD6 Biologic Itolizumab in Patients of Psoriasis
Dermatology Research and Practice Volume 2, Article ID 13326, 4 pages http://dx.doi.org/.1155/2/13326 Research Article Clinical Outcome of a Novel Anti-CD6 Biologic Itolizumab in Patients of Psoriasis
Program Disclosure. Provider is approved by the California Board of Registered Nursing, Provider #13664, for 1.5 contact hours.
 Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint-sponsorship
Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint-sponsorship
Over the past decade, the introduction of
 MANAGEMENT OF CHRONIC HEPATITIS C IN HIV-INFECTED PATIENTS: CLINICAL EXPERIENCE WITH PEGYLATED INTERFERON α PLUS RIBAVIRIN Raymond T. Chung, MD* ABSTRACT Coinfection with hepatitis C virus (HCV) is common
MANAGEMENT OF CHRONIC HEPATITIS C IN HIV-INFECTED PATIENTS: CLINICAL EXPERIENCE WITH PEGYLATED INTERFERON α PLUS RIBAVIRIN Raymond T. Chung, MD* ABSTRACT Coinfection with hepatitis C virus (HCV) is common
-HCV genome is about 9400 nucleotides long, it is ssrna and positive sense -the 10 viral proteins are first made as a large polyprotein -individual
 2013: HCV Genome -HCV genome is about 9400 nucleotides long, it is ssrna and positive sense -the 10 viral proteins are first made as a large polyprotein -individual proteins are released from polyprotein
2013: HCV Genome -HCV genome is about 9400 nucleotides long, it is ssrna and positive sense -the 10 viral proteins are first made as a large polyprotein -individual proteins are released from polyprotein
Transplantation. Professor Didier. Centre Hépatobiliaire, Hépatobiliaire, C.H.B.
 Treatment Treatment of of Hepatitis Hepatitis C C in in Liver Liver Transplantation Transplantation Professor Professor Didier Didier Samuel Samuel Centre Centre Hépatobiliaire, Hépatobiliaire, Inserm
Treatment Treatment of of Hepatitis Hepatitis C C in in Liver Liver Transplantation Transplantation Professor Professor Didier Didier Samuel Samuel Centre Centre Hépatobiliaire, Hépatobiliaire, Inserm
Efficacy and safety of protease inhibitors for sever hepatitis C recurrence after liver transplantation: a first multicentric experience
 Efficacy and safety of protease inhibitors for sever hepatitis C recurrence after liver transplantation: a first multicentric experience A. Coilly, B. Roche, J. Dumortier, D. Botta-Fridlund, V. Leroy,
Efficacy and safety of protease inhibitors for sever hepatitis C recurrence after liver transplantation: a first multicentric experience A. Coilly, B. Roche, J. Dumortier, D. Botta-Fridlund, V. Leroy,
A Practical Guide to Hepatitis C Management
 A Practical Guide to Hepatitis C Management David C. Wolf, M.D., FACP, FACG, AGAF Medical Director of Liver Transplantation Westchester Medical Center Professor of Clinical Medicine New York Medical College
A Practical Guide to Hepatitis C Management David C. Wolf, M.D., FACP, FACG, AGAF Medical Director of Liver Transplantation Westchester Medical Center Professor of Clinical Medicine New York Medical College
MEDIC CENTER. Case 2
 Case 2 Case history 57 year old Vietnamese man He lives in HCM city and works as a engineer The patient presented in July 2012 with fatigue Diagnosed with HCV in 2004 Negative for both HBV and HIV antibodies
Case 2 Case history 57 year old Vietnamese man He lives in HCM city and works as a engineer The patient presented in July 2012 with fatigue Diagnosed with HCV in 2004 Negative for both HBV and HIV antibodies
Hepatitis C (Direct Acting Antiviral Medications for Treatment of Hepatitis C) Fibrosis Score Requirement QUEST Integration
 Fibrosis Score Requirement QUEST Integration") Hepatitis C (Direct Acting Antiviral Medications for Treatment of Hepatitis C) Fibrosis Score Requirement QUEST Integration Policy Number: Original Effective Date: MM.04.036 06/01/2015 Lines of Business:
Hepatitis C (Direct Acting Antiviral Medications for Treatment of Hepatitis C) Fibrosis Score Requirement QUEST Integration Policy Number: Original Effective Date: MM.04.036 06/01/2015 Lines of Business:
SASKATCHEWAN FORMULARY BULLETIN Update to the 62nd Edition of the Saskatchewan Formulary
 April 1, 2017 Bulletin #165 ISSN 1923-0761 SASKATCHEWAN FORMULARY BULLETIN Update to the 62nd Edition of the Saskatchewan Formulary Related Information for Prescribers: Only prescribers who have completed
April 1, 2017 Bulletin #165 ISSN 1923-0761 SASKATCHEWAN FORMULARY BULLETIN Update to the 62nd Edition of the Saskatchewan Formulary Related Information for Prescribers: Only prescribers who have completed
Glecaprevir-Pibrentasvir in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2)
") Phase 3 Treatment-Experienced in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2) in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2): Study Features MAGELLAN-1 (Part 2) Trial Design: Randomized,
Phase 3 Treatment-Experienced in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2) in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2): Study Features MAGELLAN-1 (Part 2) Trial Design: Randomized,
SVR Updates from the 2013 EASL
 Updates from the 2013 EASL By Tracy Swan, Treatment Action Group Streamlining HCV Treatment Treatment for hepatitis C virus (HCV) is becoming simpler, shorter, and more effective. All-oral combinations
Updates from the 2013 EASL By Tracy Swan, Treatment Action Group Streamlining HCV Treatment Treatment for hepatitis C virus (HCV) is becoming simpler, shorter, and more effective. All-oral combinations
All Hands on Deck: Taking on Hepatitis C in Tennessee
 All Hands on Deck: Taking on Hepatitis C in Tennessee Cody A. Chastain, MD Assistant Professor of Medicine Viral Hepatitis Program Division of Infectious Diseases Vanderbilt University Medical Center Cody.a.Chastain@Vanderbilt.edu
All Hands on Deck: Taking on Hepatitis C in Tennessee Cody A. Chastain, MD Assistant Professor of Medicine Viral Hepatitis Program Division of Infectious Diseases Vanderbilt University Medical Center Cody.a.Chastain@Vanderbilt.edu
PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline
 PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline Preferred Regimen Based on Diagnosis: Mavyret (glecaprevir/pibrentasvir ) Non-Preferred: Daklinza (daclatasvir) Epclusa (sofosbuvir/velpatasvir)
PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline Preferred Regimen Based on Diagnosis: Mavyret (glecaprevir/pibrentasvir ) Non-Preferred: Daklinza (daclatasvir) Epclusa (sofosbuvir/velpatasvir)
Approved regimens for cirrhotic patients
 5th Workshop on HCV THERAPY ADVANCES New antivirals in clinical practice Approved regimens for cirrhotic patients Amsterdam, 4-5 december 2015 Disease burden in Spain 400000 350000 300000 F0 Peak cirrhosis
5th Workshop on HCV THERAPY ADVANCES New antivirals in clinical practice Approved regimens for cirrhotic patients Amsterdam, 4-5 december 2015 Disease burden in Spain 400000 350000 300000 F0 Peak cirrhosis
Hepatitis C Resistance Associated Variants (RAVs)
") Hepatitis C Resistance Associated Variants (RAVs) Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Nothing to disclose Disclosure
Hepatitis C Resistance Associated Variants (RAVs) Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Nothing to disclose Disclosure
Survival and Prognostic Factors in Mixed Cryoglobulinemia: Data from 246 Cases
 diseases Article Survival and Prognostic Factors in Mixed Cryoglobulinemia: Data from 246 Cases Cesare Mazzaro 1, Luigino Dal Maso 2, Endri Mauro 3, Valter Gattei 1, Michela Ghersetti 2, Pietro Bulian
diseases Article Survival and Prognostic Factors in Mixed Cryoglobulinemia: Data from 246 Cases Cesare Mazzaro 1, Luigino Dal Maso 2, Endri Mauro 3, Valter Gattei 1, Michela Ghersetti 2, Pietro Bulian
Review Article HCV and Lymphoproliferation
 Hindawi Publishing Corporation Clinical and Developmental Immunology Volume 2012, Article ID 980942, 8 pages doi:10.1155/2012/980942 Review Article HCV and Lymphoproliferation Anna Linda Zignego, 1, 2
Hindawi Publishing Corporation Clinical and Developmental Immunology Volume 2012, Article ID 980942, 8 pages doi:10.1155/2012/980942 Review Article HCV and Lymphoproliferation Anna Linda Zignego, 1, 2
Hepatits C Criteria Direct Acting Antiviral Medications
 Hepatits C Criteria Direct Acting Antiviral Medications Harvoni-Formulary PA required 1. Is the patient being treated for a funded condition by the Oregon Health Plan? 2. Does the member have a diagnosis
Hepatits C Criteria Direct Acting Antiviral Medications Harvoni-Formulary PA required 1. Is the patient being treated for a funded condition by the Oregon Health Plan? 2. Does the member have a diagnosis
Optimal Treatment with Boceprevir. Michael Manns
 Optimal Treatment with Boceprevir Michael Manns 6th Paris Hepatitis Conference, 14th January 2013 Acknowledgements Benjamin Maasoumy Optimal Patient Selection Defining the Ideal Candidate Treatment Urgency
Optimal Treatment with Boceprevir Michael Manns 6th Paris Hepatitis Conference, 14th January 2013 Acknowledgements Benjamin Maasoumy Optimal Patient Selection Defining the Ideal Candidate Treatment Urgency
Assessing the patient with a new diagnosis of Hepatitis C LAUREN MYERS MMSC, PA-C OREGON HEALTH & SCIENCE UNIVERSITY
 Assessing the patient with a new diagnosis of Hepatitis C LAUREN MYERS MMSC, PA-C OREGON HEALTH & SCIENCE UNIVERSITY Disclosures Nothing to Disclose Assessing the patient with a new diagnosis of Hepatitis
Assessing the patient with a new diagnosis of Hepatitis C LAUREN MYERS MMSC, PA-C OREGON HEALTH & SCIENCE UNIVERSITY Disclosures Nothing to Disclose Assessing the patient with a new diagnosis of Hepatitis
Treating now vs. post transplant
 Resistance with treatment failure Treating now vs. post transplant Pros (for treating pre transplant) If SVR efficacy means Better quality of life Removal from waiting list No post transplant recurrence
Resistance with treatment failure Treating now vs. post transplant Pros (for treating pre transplant) If SVR efficacy means Better quality of life Removal from waiting list No post transplant recurrence
Treating HCV Genotype 2 & 3
 Treating HCV Genotype 2 & 3 3rd Workshop on HCV Therapy Advances, Rome 14.12.2013 Christoph Sarrazin Klinikum der J. W. Goethe-Universität Frankfurt am Main, Germany HCV Genotypes 2 & 3 Laurel and Hardy
Treating HCV Genotype 2 & 3 3rd Workshop on HCV Therapy Advances, Rome 14.12.2013 Christoph Sarrazin Klinikum der J. W. Goethe-Universität Frankfurt am Main, Germany HCV Genotypes 2 & 3 Laurel and Hardy
Case report Telaprevir in a patient with chronic hepatitis C and cryoglobulinemic glomerulonephritis
 Antiviral Therapy 04; 9:57 5 (doi:.85/imp684) Case report Telaprevir in a patient with chronic hepatitis C and cryoglobulinemic glomerulonephritis Stella De Nicola, Alessio Aghemo *, Maria Rosaria Campise,
Antiviral Therapy 04; 9:57 5 (doi:.85/imp684) Case report Telaprevir in a patient with chronic hepatitis C and cryoglobulinemic glomerulonephritis Stella De Nicola, Alessio Aghemo *, Maria Rosaria Campise,
Pharmacological management of viruses in obese patients
 Cubist Pharmaceuticals The Shape of Cures to Come Pharmacological management of viruses in obese patients Dr. Dimitar Tonev, Medical Director UKINORD 1 Disclosures } The author is a pharmaceutical physician
Cubist Pharmaceuticals The Shape of Cures to Come Pharmacological management of viruses in obese patients Dr. Dimitar Tonev, Medical Director UKINORD 1 Disclosures } The author is a pharmaceutical physician
ABCs of Hepatitis C: What s New. The Long-Awaited New Era: Protease Inhibitors for HCV Genotype 1
 ABCs of Hepatitis C: What s New ACG Postgraduate Course Washington, DC October 30, 2011 Ira M. Jacobson, M.D. Vincent Astor Professor of Medicine Chief, Division of Gastronterology and Hepatology Medical
ABCs of Hepatitis C: What s New ACG Postgraduate Course Washington, DC October 30, 2011 Ira M. Jacobson, M.D. Vincent Astor Professor of Medicine Chief, Division of Gastronterology and Hepatology Medical
Antiviral agents in HCV
 Antiviral agents in HCV : Upcoming Therapeutic Options Su Jong Yu, M.D., Ph.D. Department of Internal Medicine, Liver Research Institute, Seoul National University College of Medicine Estimated 170 Million
Antiviral agents in HCV : Upcoming Therapeutic Options Su Jong Yu, M.D., Ph.D. Department of Internal Medicine, Liver Research Institute, Seoul National University College of Medicine Estimated 170 Million
Abbreviated Class Update: Hepatitis C
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Bristol-Myers Squibb. HCV Full Development Portfolio Overview. Richard Bertz Int Workshop CP HIV Meeting Amsterdam, Netherlands 24 April 2013
 Bristol-Myers Squibb HCV Full Development Portfolio Overview Richard Bertz Int Workshop CP HIV Meeting Amsterdam, Netherlands 24 April 2013 1 BMS Agents in Clinical Development: DAAs and INF Lambda Lambda
Bristol-Myers Squibb HCV Full Development Portfolio Overview Richard Bertz Int Workshop CP HIV Meeting Amsterdam, Netherlands 24 April 2013 1 BMS Agents in Clinical Development: DAAs and INF Lambda Lambda
Handelsbanken November Bertil Samuelsson VP Discovery Research Rein Piir CFO / IR
 Handelsbanken November 18 2009 Bertil Samuelsson VP Discovery Research Rein Piir CFO / IR Pipeline Project Indication(s) Partners/- date of Explorati Optimiz agreement Terms Medivir's markets ve phase
Handelsbanken November 18 2009 Bertil Samuelsson VP Discovery Research Rein Piir CFO / IR Pipeline Project Indication(s) Partners/- date of Explorati Optimiz agreement Terms Medivir's markets ve phase
Correspondence should be addressed to Martin J. Bergman;
 Autoimmune Diseases Volume 2013, Article ID 367190, 7 pages http://dx.doi.org/10.1155/2013/367190 Research Article Composite Indices Using 3 or 4 Components of the Core Data Set Have Similar Predictive
Autoimmune Diseases Volume 2013, Article ID 367190, 7 pages http://dx.doi.org/10.1155/2013/367190 Research Article Composite Indices Using 3 or 4 Components of the Core Data Set Have Similar Predictive
HEPATITIS C VIRUS (HCV) GENOTYPE TESTING
 GENOTYPE TESTING") CLINICAL GUIDELINES For use with the UnitedHealthcare Laboratory Benefit Management Program, administered by BeaconLBS HEPATITIS C VIRUS (HCV) GENOTYPE TESTING Policy Number: PDS - 027 Effective Date:
CLINICAL GUIDELINES For use with the UnitedHealthcare Laboratory Benefit Management Program, administered by BeaconLBS HEPATITIS C VIRUS (HCV) GENOTYPE TESTING Policy Number: PDS - 027 Effective Date:
HEPATITIS C UPDATES. Sanaa S. Said 10 th April, 2014
 HEPATITIS C UPDATES Sanaa S. Said 10 th April, 2014 CONTENTS Introduction Epidemiology Transmission and Natural history Kenyan guidelines What is new? References INTRODUCTION Hepacivirus genus, Flaviviridae
HEPATITIS C UPDATES Sanaa S. Said 10 th April, 2014 CONTENTS Introduction Epidemiology Transmission and Natural history Kenyan guidelines What is new? References INTRODUCTION Hepacivirus genus, Flaviviridae
Arvind R. Murali, MD Assistant Professor of Medicine Gastroenterology & Hepatology Organ Transplant Center UIHC, Carver College of Medicine
 Arvind R. Murali, MD Assistant Professor of Medicine Gastroenterology & Hepatology Organ Transplant Center UIHC, Carver College of Medicine No financial disclosures No conflicts of interest No affiliations
Arvind R. Murali, MD Assistant Professor of Medicine Gastroenterology & Hepatology Organ Transplant Center UIHC, Carver College of Medicine No financial disclosures No conflicts of interest No affiliations
Triple therapy with telaprevir or boceprevir: management of side effects
 Triple therapy with telaprevir or boceprevir: management of side effects Universitätsklinikum Leipzig Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Leber
Triple therapy with telaprevir or boceprevir: management of side effects Universitätsklinikum Leipzig Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Leber
Intron A Hepatitis B. Intron A (interferon alfa-2b) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.01 Subject: Intron A Hepatitis B Page: 1 of 7 Last Review Date: November 30, 2018 Intron A Hepatitis
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.01 Subject: Intron A Hepatitis B Page: 1 of 7 Last Review Date: November 30, 2018 Intron A Hepatitis