ANCA-associated vasculitis. Vladimir Tesar Department of Nephrology, General University Hospital, Prague, Czech Republic
|
|
|
- Amice Henderson
- 5 years ago
- Views:
Transcription



1 ANCA-associated vasculitis Vladimir Tesar Department of Nephrology, General University Hospital, Prague, Czech Republic
2 Disclosure of Interests Abbvie, Amgen, Baxter, Bayer, Boehringer-Ingelheim, Calliditas, Chemocentryx, Daichi-Sankyo Fresenius Medical Care (consultancy, advisory board) KDIGO Controversies Conference on Glomerular Diseases November 16-19, 2017 Singapore
3 Outline of the lecture Anti-PR3 vs. anti-mpo disease, predictive value of renal biopsy? Initial therapy and relapse Plasma exchange Maintenance therapy Conclusions
4 Outline of the lecture Anti-PR3 vs. anti-mpo disease, predictive value of renal biopsy? Initial therapy and relapse Plasma exchange Maintenance therapy Conclusions
5 Revised CHCC nomenclature, 2012
6 Simplified clinicopathologic classification of AAV Jennette a Falk, Arthritis Rheum, 1994, 37: Granulomatosis with polyangiitis (GPA) formerly Wegener granulomatosis Microscopic polyangiitis (MPA) Eosinophilic granulomatosis with polyangiitis (EGPA) formerly Churg-Strauss syndrome Vasculitis with granulomas without asthma Vasculitis without asthma and granulomas Vasculitis with eosinophilia, astha and granulomas
7 Organ involvement in AAV

8 Prednisolone dose BVAS Anti-MPO ANCA associated with HLA-DQ, not HLA-DP, as it is in anti-pr3 ANCA

9 Anti-PR3 and anti-mpo disease have different presentation and outcome

10 Anti-PR3 and anti-mpo associated with different phenotypes (502 pts with AAV)
11 Footer only In 502 AAV pts relapse predicted by ANCA specificity and not CHCC and EMA clinical diagnosis AAV RLV GPA MPA KDIGO Controversies Conference on Glomerular Diseases November 16-19, 2017 Singapore
 KDIGO Controversies Conference on Glomerular Diseases November 16-19, 2017")
12 Footer only 40% out of 252 pts from CYCLOPS and IMPROVE developed at least one relapse Reduced risk of relapse - ANCA-negativity at switch to the maintenance therapy (anti-pr3, age, SCr, pulsed CPH, MMF maintenance) KDIGO Controversies Conference on Glomerular Diseases November 16-19, 2017 Singapore

13 Footer only In 9 studies ANCA and ANCA persistence only modestly predict future relapses Limited use to serial ANCA measurements during disease remission KDIGO Controversies Conference on Glomerular Diseases November 16-19, 2017 Singapore


14 New histologic classification of ANCA-associated glomerulonephritis
15 GFR well preserved in focal and (relatively in) crescentic GN, deteriorating in mixed and sclerotic GN



16 5-year renal survival in mixed GN better in other studies than in original cohort of Berden et al.
17 Validation studies Validation studies altogether in 1114 pts with AAV (784 Caucasian and 330 Asian) Conclusions: 1. classification generally validated (namely due to the difference between focal and sclerotic GN) 2. outcome in mixed GN generally better than in original study, no difference between crescentic and mixed GN 3. any difference driven namely by % of normal glomeruli, tubulointerstitial fibrosis and tubular atrophy (not part of classification) generally of importance 4. anti-mpo negative predictor, classification should be probably validated in anti-pr3 and anti-mpo disease separately 5. larger validation study warranted
18 Protocol renal rebiopsy in 17 pts with AAV

19 Necrosis and cellular crescents transform in fibrous crescents
20 Protocol renal rebiopsy in 17 pts with AAV

21 CD20+ cells disappeared, ale CD3+ cells persisted even in remission CD20+ buňky CD3+ buňky
22 Footer only In 174 pts from MEPEX and CYCYZAREM cumulative incidence of renal relapse at 5 yrs was 9.5%, risk in sclerotic class and with absence of interstitial infiltrates KDIGO Controversies Conference on Glomerular Diseases November 16-19, 2017 Singapore
23 Outline of the lecture Anti-PR3 vs. anti-mpo disease, predictive value of renal biopsy? Initial therapy and relapse Plasma exchange Maintenance therapy Conclusions
24 Wegener s granulomatosis outcome of untreated pts 1958 Walton outcome of untreated pts Walton,E.W.: Giant-cell granuloma of the respiratory tract (Wegeners granulomatosis). British Medical Journal, 2: , median survival: 5 months, majority of pts died of respiratory or renal failure 1983 Fauci, NIH, Bethesda, survival of untreated pts Fauci,A.S., et al.: Wegeners granulomatosis: prospective clinical and therapeutic experience with 85 patients for 21 years. Annals of Internal Medicine, 98: 76 85, median survival 5 months, 1-yr mortalita 82%, 2-yr mortalita 90%
25 Footer only Cyclophosphamide dramatic change of the outcome of patients < text > mean FU 8 yrs 91% marked improvement, 75% complete remission,13% mortality, 50% remissions with at least one relapse, 15-yr risk of bladder cancer 16% KDIGO Controversies Conference on Glomerular Diseases November 16-19, 2017 Singapore
26
27 EUVAS studies to minimize CPH exposure Early switch from CPH to AZA in generalized vasculitis does not increase the risk of relapses (within relatively short follow-up - CYCAZAREM) CPH pulses (lower cumulative dose of CPH) are as effective as induction treatment in generalized vasculitis (CYCLOPS) KDIGO Controversies Conference on Glomerular Diseases November 16-19, 2017 Singapore

28 In CYCAZAREM after median FU of 8.5 yrs there was a trend to relapse rate in pts switched early to AZA KDIGO Controversies Conference on Glomerular Diseases November 16-19, 2017 Singapore

29 In CYCLOPS there was risk of relapse in pulse CPH limb

30 Undertreatment shown to be one of the risk factors for relapses
31 First use of RTX in AAV - rapid response of BVAS, ANCA and CRP and stabilisation of renal function
32 65 consecutive pts with refractory AAV, 4 British centres MMF Lungs 50% Kidney 5% CYC

33 75% complete remission 23% partial remission 2% no response
34 RAVE study 194 pts with generalized AAV (2/3 with renal involvement - mean GFR 61 ml/min) randomized to either: 1) conventional treatment (CPH and CS, followed by AZA) 2) rituximab (plus CS, initially) for remission induction
35 RAVE study 64% of RTX pts vs. 53% of CPH pts reached the primary endpoint (non-inferiority) RTX more effective than CPH in inducing remission in relapsing disease: 67% vs. 42% reached the primary endpoint Rate of adverse events not different in both limbs

36 RITUXVAS study RTX vs. CPH in 44 pts with new AAV and renal involvement
37 RITUXVAS study RTX 4x 375 mg/m 2 CPH 2 pulses CPH 6 10 pulses followed by AZA

38 RITUXVAS study Cumulative incidence of remission Sustained remission: RTX 76% CPH 82% Increase of GFR at 12 months: RTX 19 ml/min CPH 15 ml/min
39
40

41 Subanalysis of 102 pts from RAVE study with renal involvement, no difference in remaining in remission and improvement of egfr RAVE study mean egrf 41 vs. 50 ml/min
 not different between RTX and")
42 In RITUXVAS survival (and relapse-free and ESRDfree survival) not different between RTX and CPH limb
43 Retrospective analysis of 37 pts with AAV and egfr 20 ml/min demonstrated similar efficacy of RTX with or without CPH

44 Analysis of 14 pts with severe renal AAV - good efficacy of RTX: all pts developed remission, egfr improved, treatment well tolerated

45 Efficacy of RTX compared in 59 pts with refractory AAV with either granulomatous vs vasculitic lesions, RTX better in vasculitic vs. (some) granulomatous manifestations Response rate 63%, relapse rate 40%

46 RAVE study 18-mo FU The strongest determinant of relapse risk was anti-pr3 positivity anti-mpo anti-pr3

47 Pts with anti-pr3 relapsing disease achieved remission more often following RTX compared to CPH after 6, 12 and 18 mo

48 Pts with anti-pr3 disease achieved complete remission after 6 mo following RTX more often compared to CPH Different treatment of anti-pr3 and anti-mpo disease?
 AEs mainly infections, hypogammaglobulinemia and")
49 Adverse events in 172 pts treated with RTX maintenance for a median 2.1 year (up to 7 years) AEs mainly infections, hypogammaglobulinemia and LON

50 RITUXVAS study Cumulative incidence of severe adverse events RTX 42% CYC 36%

51 RTX combined with low dose CPH in 23 pts with renal AAV Pts with SCr 500 µmol/l, AH and RTX treatment excluded
52 All pts achieved clinical remission within 6 weeks 3 major and 2 minor relapses occurred during a median FU of 39 mo (pts retreated with RTX for major relapses) Long-term remission, Putative steroid sparing platform

53 66 consecutive pts (AH, advanced CKD excluded) treated in one centre with RTX, low-dose CPH and CS Outcomes compared with matched controls from EUVAS studies At last FU (median 5 yrs) patient and renal survival 94% and 84%, respectively, major relapse rate 15%, median time to relapse 39 mo In matched EUVAS patients: risk of relapse ESRD mortality 2.2 higher, 4.8 higher, 3.5 higher

54 Activation of alternative complement pathway in AAV

55 Anti-C5 moab prevented necroses and crescent formation
56 67 pts with AAV randomized to: 1) Standard of care (SOC) control: Placebo + CYC or RTX + full starting dose of prednisone (60 mg), 2) CCX (avacopan) mg b.i.d. + CYC or RTX + reduced starting dose of prednisone (20 mg), or 3) CCX mg b.i.d. + CYC or RTX + no prednisone. Primary endpoint met: BVAS response (decrease of BVAS for at least 50%) at week 12 numerically superior and statistically non-inferior to SOC control (p = and p = 0.02) for each of the CCX168 groups vs. control

57 67 pts with AAV randomized to RTX or CPH and either high dose sterois, avacopan + reduced steroid and avacopan without steroids Decrease pf BVAS faster in avacopan treated pts
 ** P < 0.01 for superiority of CCX168 vs.")
58 Decrease of albuminuria more expressed in pts treated with avacopan Urinary Albumin: Creatinine Ratio Percent Change from Baseline (Geometric Means) ** P < 0.01 for superiority of CCX168 vs. Control 61
 * P < 0.05 for CCX168 change or percent change from baseline vs.")
59 Rapid improvement of the quality of life in pts treated with avacopan (CCX168) * P < 0.05 for CCX168 change or percent change from baseline vs. Control 62
 ** P < 0.01, * P < 0.05 for CCX168 vs.")
60 Improvement of vitality (less fatigue) in pts on avacopan (CCX168) ** P < 0.01, * P < 0.05 for CCX168 vs. steroid control group
61 Adverse events possibly related to CS treatment Adverse Effect High Dose Steroids SOC (N=23) CCX168 + Low Dose Steroids (N=22) CCX168 + No Steroids (N=22) CCX168 Combined (N=44) Patients with Any Event 15 (65.2%) 4 (18.2%) 11 (50.0%) 15 (34.1%) * Psychiatric disorders 6 (26.1%) (6.8%) Serious infections 1 (4.3%) (4.5%) New onset/worsening 4 (17.4%) (2.3%) diabetes/hyperglycemia New onset/worsening 5 (21.7%) (22.7%) hypertension Weight gain >10 kg 2 (8.7%) (2.3%) Bone fractures 1 (4.3%) (0%) Cataracts 1 (4.3%) (0%) * P = 0.02 for CCX168 vs. SOC Control
62 Conclusions: Avacopan (CCX168) successful as steroid sparing drug during the induction phase of AAV ADVOCATE phase 3 trial with avacopan is currently ongoing
63 PEXIVAS recruited 700 pts with AAV a Scr > 200 µmol/l randomized also to standard-dose and reduced-dose corticosteroids (54% of the standard dose within 3 mo) Reduced-dose CS non-inferior in terms of both primary outcome (composite of the death and ESRD) and secondary outcomes (death, ESRD) significantly lower risk of serious infections at 1 year (HR = 0.70, p = 0.02) PEXIVAS
 malignancies in pts with cumulative")
64 High risk of late occurring ( yrs after CPH ) malignancies in pts with cumulative dose of CPH > 36 g


65 One-centre analysis of 323 pts with AAV 33 pts developed 45 malignancies CPH associated with increased risk of cancer, in RTX-treated pts similar risk of cancer as in general population
66
67
68
69 We recommend rituximab be used as an alternative initial treatment in patients with ANCA-associated vasculitis (1B) and be preferred in anti-pr3 positive patients (1B). We suggest rituximab be used only in those patients with severe renal disease in whom cyclophosphamide is contraindicated (2B)
70 We recommend that rituximab and corticosteroids be used as a first line treatment in patients with severe (major) relapse of ANCA vasculitis (1C), especially in anti-pr3 positive patients; as an alternative we recommend cyclophosphamide and corticosteroids
71 Outline of the lecture Anti-PR3 vs. anti-mpo disease, predictive value of renal biopsy? Initial therapy and relapse Plasma exchange Maintenance therapy Conclusions
72 In MEPEX trial 137 pts with AAV presenting with Scr > 500 µmol/l randomized either to PE or MP as an add-on treatment At 3 months 69% treated with PE compared to 49% treated with MP were alive and with independent renal function MEPEX
73
74 Metaanalysis - 9 studies, 387 pts, no impact on mortality in AAV
75 Plasma exchange had, however, significant impact on the rate of ESRD - decrease by 36%
76 Long-term FU of MEPEX: after a median FU of 3.95 yrs there was no difference in proportion of pts free of ESRD or death
77 Reduction of the risk of ESRD (0.64, confidence interval ) did not reach statistical significance
78 In MEPEX trial 137 pts with AAV presenting with Scr > 500 µmol/l randomized either to PE or MP as an add-on treatment At 3 months 69% treated with PE compared to 49% treated with MP were alive and with independent renal function MEPEX


79 No difference in renal recovery in 41 pts treated with ivcyp and PLEX compared with 37 pts PLEX treated pts from MEPEX

80 Much lower mortality in pts treated with ivcph compared to MEPEX pts

81 ESRD or death reduced only in PR3-ANCA positive pts
82
83 Plasma exchange - open questions Treatment of dialysis-dependent pts Treatment of pts with preserved renal function Treatment of pts with alveolar haemorrhage Different treatment of anti-pr3 and anti- MPO disease?

84 Footer only Single-center retrospective comparison of 24 pts with AAV treated with adjunct PE and with 24 age-, egfr- and disease activity- matched pts with standard treatment No difference in survival and dialysis-free survival KDIGO Controversies Conference on Glomerular Diseases November 16-19, 2017 Singapore
85 PEXIVAS recruited 700 pts with AAV a Scr > 200 µmol/l randomized to PE or no PE as an add-on treatment with a 2 yr FU, no effect on mortality and the risk of ESRD demonstrated in any of the studied subgroups PEXIVAS
86 Data from PEXIVAS will definitely modify these statements
87 Outline of the lecture Anti-PR3 vs. anti-mpo disease, predictive value of renal biopsy? Initial therapy and relapse Plasma exchange Maintenance therapy Conclusions
 of CS and AZA REMAIN KDIGO Controversies Conference on Glomerular Diseases November 16-19, 2017")
88 Footer only 110 pts with AAV mo after diagnosis in stable remission randomized to continuation (up to 48 mo) or withdrawal (at 24 mo) of CS and AZA REMAIN KDIGO Controversies Conference on Glomerular Diseases November 16-19, 2017 Singapore
89 Footer only Primary endpoint (survival without relapse within 48 mo) reached in 62.7% of pts in continuation vs. in 22% withdrawal limb REMAIN ESRD 7.8% vs. 0%, p = Survival without relapse 62.7% vs. 22%, OR 5.96 Survival without major relapse 35.3% vs. 13.5% KDIGO Controversies Conference on Glomerular Diseases November 16-19, 2017 Singapore

90 Footer only Relapse rate higher in patients ANCA positive at randomisation REMAIN KDIGO Controversies Conference on Glomerular Diseases November 16-19, 2017 Singapore

91 Footer only No significant difference in adverse event rate KDIGO Controversies Conference on Glomerular Diseases November 16-19, 2017 Singapore REMAIN
92 45 pts with c-anca positive AAV (75% with renal involvement) in remission after oral CPH randomized to 1-yr vs 4 yr maintenance with AZA No significant difference in relapse-free survival in both c-anca pos and neg pts KDIGO Controversies Conference on Glomerular Diseases November 16-19, 2017 Singapore

93 Study may have been underpowered to identify the difference, a trend to higher number of relapses in pts on standard vs extended AZA (46% vs. 25%) KDIGO Controversies Conference on Glomerular Diseases November 16-19, 2017 Singapore
94 Footer only at least some of the pts who reached remission of AAV require long-term immunosuppressive therapy to prevent recurrence of the disease KDIGO Controversies Conference on Glomerular Diseases November 16-19, 2017 Singapore

95 Outcome much better in pts treated with RTX preemptively
96 MAINRITSAN study 115 pts with AAV in remission randomized to RTX or AZA maintenance

97 MAINRITSAN study - renal involvement in 70% of pts
98 Significantly higher rate of (major) relapses in AZA limb 5% vs. 29% major relapses MAINRITSAN study
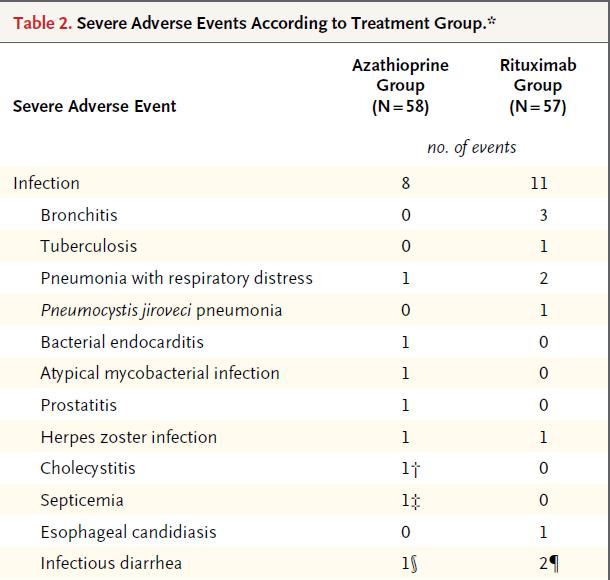
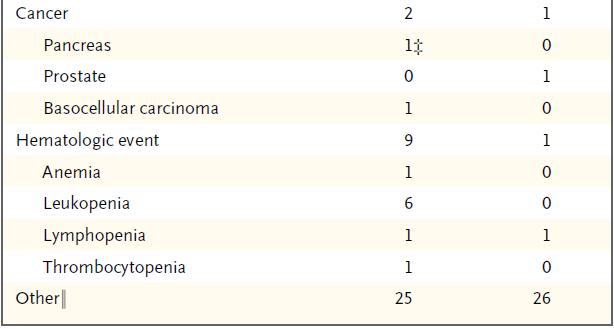

99 MAINRITSAN study no difference in SAE
 Major relapse-free survival- 71.9% vs. 49.4% (p = 0.")
100 60 mo FU of the MAINRITSAN study (RTX vs. AZA): 60-mo overall survival % vs. 93% (p = 0.045) All relapse-free survival % vs. 37.2% (p = 0.012) Major relapse-free survival- 71.9% vs. 49.4% (p = 0.003) No difference in AEs and corticosteroid doses Maintenance therapy with RTX remains superior to AZA even after 60 months


101 Rituximab higher cost partly offset by fewer relapses, side effects and FU expenses The cost of avoiding one relapse was 259 euros
102 69 pts treated with 2-yr RTX maintenance compared with 28 pts with RTX induction only Relapses in pts with early B cell return and reappearance of ANCA Relapse rate after RTX maintenance vs. after RTX induction only
103 Further RCTs with RTX in AAV MAINRITSAN 2 RTX maintenance given preemptively, or based on ANCA titre and reappearance of CD19 cells MAINRITSAN 3 RTX maintenance given for 18 compared to 46 mo RITAZAREM RTX maintenance in relapsing pts treated with RTX induction
104 Comparison Study of Two Rituximab Regimens in the Remission of ANCA Associated Vasculitis MAINRITSAN 2 NCT pts with ANCA-associated vasculitis (new or relapsing in remission after induction treatment) RTX maintenance regimen based on the ANCA titre and CD19 lymphocytes compared to preemptive RTX RTX given 1 g in the beginning, then 0.5 g each 6 months vs. based on ANCA titre and CD19 cells) Primary outcome measure: number of relapses (major and minor) within 28 mo

105 Results of MAINRITSAN2 study 14 (7.3%) vs. 8 (9.9%) relapses in tailored vs preemptive treatment (p = 0.2, n.s.) Median numbers of RTX infusion 3 vs. 5 Conclusion: both approaches similarly effective, fewer infusions and total RTX dose in tailored treatment limb
106 Rituximab Vasculitis Maintenance Study (RITAZAREM) NCT Main investigator: D Jayne 190 pts with relapsing AAV treated with RTX and CS and after 4 mo randomized to either RTX (a single dose every 4 mo for 2 yrs) or AZA and followed for 4 yrs Primary outcome measures: time to relapse (either minor or major relapse) from randomisation
107 In 69 pts treated with 2-year RTX maintenance Relapse rate after RTX withdrawal than after RTX induction only relapses in pts with early return of B cells and reappearance of ANCA
108 Comparison Between a Long Term and a Conventional Maintenance Treatment With Rituximab (MAINRITSAN3) NCT During FU of MAINRITSAN study, up to 30% of patients experienced a relapse 38 months after the last rituximab infusion (unpublished data), duration of RTX maintenanc treatment to be defined RTX maintenance of 18 mo will be compared with RTX maintenance of 46 mo in 116 pts with AAV in remission Primary outcome measures: vasculitis score 2003 (BVAS 2003 ) and relapse free survival rates (BVAS > 0)
109
110
111

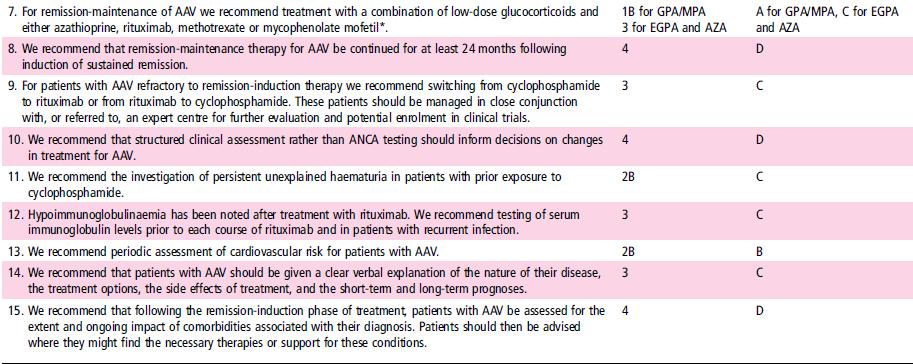
112 Maintenance treatment should be prolonged up to 48 months in pts who remain ANCA-positive (1B). We recommend rituximab or azathioprine as maintenance therapy, rituximab should be preferred in patients treated with rituximab induction (1B).
113 Outline of the lecture Anti-PR3 vs. anti-mpo disease, predictive value of renal biopsy? Initial therapy and relapse Plasma exchange Maintenance therapy Conclusions
114 Conclusions Anti-PR3 and anti-mpo pts should be probably treated differently Rituximab becomes first-line treatment in pts with major relapses and also in new pts with anti-pr3 disease, more data on pts with advanced kidney disease needed Rituximab is probably the best maintenance treatment (anti-pr3 vs. anti-mpo pts, doses, intervals, length of treatment) Corticosteroids should be (and can be) reduced, or replaced Effect of plasma exchange on ESRD not confirmed in PEXIVAS trial
115
Recent advances in management of Pulmonary Vasculitis. Dr Nita MB
 Recent advances in management of Pulmonary Vasculitis Dr Nita MB 23-01-2015 Overview of the seminar Recent classification of Vasculitis What is new in present classification? Trials on remission induction
Recent advances in management of Pulmonary Vasculitis Dr Nita MB 23-01-2015 Overview of the seminar Recent classification of Vasculitis What is new in present classification? Trials on remission induction
TREATMENT OF ANCA-ASSOCIATED VASCULITIS
 TREATMENT OF ANCA-ASSOCIATED VASCULITIS Loïc Guillevin Hôpital Cochin, Université Paris Descartes Cours DU, 11 mars 2016 1 Disclosure of interest regarding this presentation Roche has provided, in part,
TREATMENT OF ANCA-ASSOCIATED VASCULITIS Loïc Guillevin Hôpital Cochin, Université Paris Descartes Cours DU, 11 mars 2016 1 Disclosure of interest regarding this presentation Roche has provided, in part,
Lupus nephritis. Vladimir Tesar Department of Nephrology, General University Hospital, Prague, Czech Republic
 Lupus nephritis Vladimir Tesar Department of Nephrology, General University Hospital, Prague, Czech Republic Disclosure of Interests Abbvie, Amgen, Baxter, Bayer, Boehringer-Ingelheim, Calliditas, Chemocentryx,
Lupus nephritis Vladimir Tesar Department of Nephrology, General University Hospital, Prague, Czech Republic Disclosure of Interests Abbvie, Amgen, Baxter, Bayer, Boehringer-Ingelheim, Calliditas, Chemocentryx,
Tell me more about vasculitis. Lisa Willcocks Consultant in Nephrology and Vasculitis, Addenbrooke s Hospital
 Tell me more about vasculitis Lisa Willcocks Consultant in Nephrology and Vasculitis, Addenbrooke s Hospital Talk overview Case study ANCA-associated vasculitis What is ANCA vasculitis? What causes ANCA
Tell me more about vasculitis Lisa Willcocks Consultant in Nephrology and Vasculitis, Addenbrooke s Hospital Talk overview Case study ANCA-associated vasculitis What is ANCA vasculitis? What causes ANCA
ANCA+ VASCULITIDES CYCAZAREM,
 ANCA+ VASCULITIDES CYCAZAREM, q Comparison of 3 to 6 mo. oral CYC + CS then azathioprine or oral CYC for 12 mo.+ 10 mg/d CS. After 12 mo all the patients were treated with azathioprine q 150 patients followed
ANCA+ VASCULITIDES CYCAZAREM, q Comparison of 3 to 6 mo. oral CYC + CS then azathioprine or oral CYC for 12 mo.+ 10 mg/d CS. After 12 mo all the patients were treated with azathioprine q 150 patients followed
Plasma exchanges in ANCA-associated vasculitis
 Plasma exchanges in ANCA-associated vasculitis Xavier Puéchal, MD, PhD Centre de Référence des Maladies auto-immunes systémiques rares d Ile de France Hôpital Cochin Université Paris Descartes http://www.vascularites.org
Plasma exchanges in ANCA-associated vasculitis Xavier Puéchal, MD, PhD Centre de Référence des Maladies auto-immunes systémiques rares d Ile de France Hôpital Cochin Université Paris Descartes http://www.vascularites.org
RATIONALE. K Without therapy, ANCA vasculitis with GN is associated. K There is high-quality evidence for treatment with
 http://www.kidney-international.org chapter 13 & 2012 KDIGO Chapter 13: Pauci-immune focal and segmental necrotizing glomerulonephritis Kidney International Supplements (2012) 2, 233 239; doi:10.1038/kisup.2012.26
http://www.kidney-international.org chapter 13 & 2012 KDIGO Chapter 13: Pauci-immune focal and segmental necrotizing glomerulonephritis Kidney International Supplements (2012) 2, 233 239; doi:10.1038/kisup.2012.26
SMALL TO MEDIUM VASCULITIS: RENAL ASPECT RATANA CHAWANASUNTORAPOJ UPDATE IN INTERNAL MEDICINE 2018
 SMALL TO MEDIUM VASCULITIS: RENAL ASPECT RATANA CHAWANASUNTORAPOJ UPDATE IN INTERNAL MEDICINE 2018 OUTLINE Renal involvement in vasculitis Curr Rheumatol Rep 2013 Renal involvement in ANCA vasculitis GN***:
SMALL TO MEDIUM VASCULITIS: RENAL ASPECT RATANA CHAWANASUNTORAPOJ UPDATE IN INTERNAL MEDICINE 2018 OUTLINE Renal involvement in vasculitis Curr Rheumatol Rep 2013 Renal involvement in ANCA vasculitis GN***:
ANCA associated vasculitis in China
 ANCA associated vasculitis in China Min Chen Renal Division, Peking University First Hospital, Beijing 100034, P. R. China 1 General introduction of AAV in China Disease spectrum and ANCA type Clinical
ANCA associated vasculitis in China Min Chen Renal Division, Peking University First Hospital, Beijing 100034, P. R. China 1 General introduction of AAV in China Disease spectrum and ANCA type Clinical
Vascularites rénales associées aux ANCA
 Vascularites rénales associées aux ANCA Société Médicale des Hôpitaux de Paris 16 Mars 2012 Philippe Vanhille Néphrologie et Médecine Interne Hôpital de Valenciennes Classification of systemic vasculitis:
Vascularites rénales associées aux ANCA Société Médicale des Hôpitaux de Paris 16 Mars 2012 Philippe Vanhille Néphrologie et Médecine Interne Hôpital de Valenciennes Classification of systemic vasculitis:
Vascularites associées aux ANCA Traitement par le RITUXIMAB
 Vascularites associées aux ANCA Traitement par le RITUXIMAB Philippe Vanhille Néphrologie Médecine Interne Hôpital de Valenciennes Aix- en- Provence 2013 Cyclophosphamide therapy of severe systemic necrotizing
Vascularites associées aux ANCA Traitement par le RITUXIMAB Philippe Vanhille Néphrologie Médecine Interne Hôpital de Valenciennes Aix- en- Provence 2013 Cyclophosphamide therapy of severe systemic necrotizing
Managing Acute Medical Problems, Birmingham Vasculitis. David Jayne. University of Cambridge
 Managing Acute Medical Problems, Birmingham 2016 Vasculitis David Jayne University of Cambridge Disclosures Astra Zeneca, Aurinia, BIOGEN, Boehringer, Chemocentryx, Genzyme/Sanofi, GSK, Lilly, Medimmune,
Managing Acute Medical Problems, Birmingham 2016 Vasculitis David Jayne University of Cambridge Disclosures Astra Zeneca, Aurinia, BIOGEN, Boehringer, Chemocentryx, Genzyme/Sanofi, GSK, Lilly, Medimmune,
Jones slide di 23
 1 di 23 The patient with ANCA- associated vasculitis and pulmonary haemorrhage Rachel B Jones, Cambridge, UK Chairs:Hans-Joachim Anders, Munich, Germany Vladimir Tesar, Prague, Czech Republic Prof. Rachel
1 di 23 The patient with ANCA- associated vasculitis and pulmonary haemorrhage Rachel B Jones, Cambridge, UK Chairs:Hans-Joachim Anders, Munich, Germany Vladimir Tesar, Prague, Czech Republic Prof. Rachel
New Developments in ANCA-associated Vasculitis
 New Developments in ANCA-associated Vasculitis Second International Renal Conference Bruges, March 2018 Ulrich Specks, M.D. Connor Group Foundation Professor of Medicine Mayo Clinic College of Medicine
New Developments in ANCA-associated Vasculitis Second International Renal Conference Bruges, March 2018 Ulrich Specks, M.D. Connor Group Foundation Professor of Medicine Mayo Clinic College of Medicine
TREATMENT OF ANCA-ASSOCIATED VASCULITIS AN UPDATE. Loïc Guillevin. Hôpital Cochin, Université Paris Descartes. DU MALADIES SYSTEMIQUES, 7 March 2014
 TREATMENT OF ANCA-ASSOCIATED VASCULITIS AN UPDATE Loïc Guillevin Hôpital Cochin, Université Paris Descartes DU MALADIES SYSTEMIQUES, 7 March 2014 1 Disclosure of interest regarding this presentation Former
TREATMENT OF ANCA-ASSOCIATED VASCULITIS AN UPDATE Loïc Guillevin Hôpital Cochin, Université Paris Descartes DU MALADIES SYSTEMIQUES, 7 March 2014 1 Disclosure of interest regarding this presentation Former
Nierenbeteiligung bei Systemerkrankungen
 Nierenbeteiligung bei Systemerkrankungen ÖGN 2018 Irmgard Neumann www.vasculi*s.at Avacopan (CCX168) Small molecule, orally administered Highly selecgve C5aR inhibitor Prevented MPO- ANCA mediated GlomerulonephriGs
Nierenbeteiligung bei Systemerkrankungen ÖGN 2018 Irmgard Neumann www.vasculi*s.at Avacopan (CCX168) Small molecule, orally administered Highly selecgve C5aR inhibitor Prevented MPO- ANCA mediated GlomerulonephriGs
Annual Rheumatology & Therapeutics Review for Organizations & Societies
 Annual Rheumatology & Therapeutics Review for Organizations & Societies Update on Granulomatosis with Polyangiitis (Wegener s) Learning Objectives Identify the clinical features of granulomatosis with
Annual Rheumatology & Therapeutics Review for Organizations & Societies Update on Granulomatosis with Polyangiitis (Wegener s) Learning Objectives Identify the clinical features of granulomatosis with
EUVAS update June 5 th Marinka Twilt
 EUVAS update June 5 th 2012 Marinka Twilt Chapel Hill 2012 Classification Large Vessel Vasculitis (LVV) Medium Vessel Vasculitis (MVV) Small Vessel Vasculitis (SVV) Variable Vessel Vasculitis (VVV) Single
EUVAS update June 5 th 2012 Marinka Twilt Chapel Hill 2012 Classification Large Vessel Vasculitis (LVV) Medium Vessel Vasculitis (MVV) Small Vessel Vasculitis (SVV) Variable Vessel Vasculitis (VVV) Single
Rituximab treatment for ANCA-associated vasculitis in childhood
 Rituximab treatment for ANCA-associated vasculitis in childhood DISCLOSURE I have no relevant financial relationships to disclose Katharine Moore MD Nov 14, 2012 University of Colorado School of Medicine
Rituximab treatment for ANCA-associated vasculitis in childhood DISCLOSURE I have no relevant financial relationships to disclose Katharine Moore MD Nov 14, 2012 University of Colorado School of Medicine
Year In Review: VasculitisPers. Disclosures. Learning Objectives. none 4/16/2018. Describe new medications for the treatment of vasculitis
 Year In Review: VasculitisPers Cailin Sibley, M.D., M.H.S. Director, Vasculitis Clinic April 27 th, 2018 NTEREST DISCLOSURE Disclosures none Learning Objectives Describe new medications for the treatment
Year In Review: VasculitisPers Cailin Sibley, M.D., M.H.S. Director, Vasculitis Clinic April 27 th, 2018 NTEREST DISCLOSURE Disclosures none Learning Objectives Describe new medications for the treatment
Clinical Commissioning Policy: Rituximab For ANCA Vasculitis. December Reference : NHSCB/ A3C/1a
 Clinical Commissioning Policy: Rituximab For ANCA Vasculitis December 2012 Reference : NHSCB/ A3C/1a NHS Commissioning Board Clinical Commissioning Policy: Rituximab For The Treatment Of Anti-Neutrophil
Clinical Commissioning Policy: Rituximab For ANCA Vasculitis December 2012 Reference : NHSCB/ A3C/1a NHS Commissioning Board Clinical Commissioning Policy: Rituximab For The Treatment Of Anti-Neutrophil
Treatment of Severe Renal Disease in ANCA Positive and Negative Small Vessel Vasculitis with Rituximab
 American Journal of Nephrology Original Report: Patient-Oriented, Translational Research Am J Nephrol 2015;41:296301 Received: March 12, 2015 Accepted: May 6, 2015 Published online: June 2, 2015 Treatment
American Journal of Nephrology Original Report: Patient-Oriented, Translational Research Am J Nephrol 2015;41:296301 Received: March 12, 2015 Accepted: May 6, 2015 Published online: June 2, 2015 Treatment
Atypical IgA Nephropathy
 Atypical IgA Nephropathy Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA XXXIII Chilean Congress of Nephrology, Hypertension and Transplantation Puerto Varas, Chile October 6, 2016 IgA
Atypical IgA Nephropathy Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA XXXIII Chilean Congress of Nephrology, Hypertension and Transplantation Puerto Varas, Chile October 6, 2016 IgA
Small Vessel Vasculitis
 Small Vessel Vasculitis Paul A Brogan Professor of Vasculitis and Consultant Paediatric Rheumatologist Department of Rheumatology Institute of Child Health and Great Ormond St Hospital, London UK P.brogan@ucl.ac.uk
Small Vessel Vasculitis Paul A Brogan Professor of Vasculitis and Consultant Paediatric Rheumatologist Department of Rheumatology Institute of Child Health and Great Ormond St Hospital, London UK P.brogan@ucl.ac.uk
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Jones RB, Cohen Tervaert JW, Hauser T, et al. Rituximab versus
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Jones RB, Cohen Tervaert JW, Hauser T, et al. Rituximab versus
Optimizing the Therapeutic Strategies in ANCA-Associated Vasculitis Single Centre Experience with International Randomized Trials
 Prague Medical Report / Vol. 107 (2006) No. 2, p. 199 212 199) Optimizing the Therapeutic Strategies in ANCA-Associated Vasculitis Single Centre Experience with International Randomized Trials Vaňková
Prague Medical Report / Vol. 107 (2006) No. 2, p. 199 212 199) Optimizing the Therapeutic Strategies in ANCA-Associated Vasculitis Single Centre Experience with International Randomized Trials Vaňková
SHO Teaching. Dr. Amir Bhanji Consultant Nephrologist, Q.A hospital, Portsmouth
 SHO Teaching Vasculitis Renal medicine Dr. Amir Bhanji Consultant Nephrologist, Q.A hospital, Portsmouth OUTLINE What is vasculitis Causes Classification Brief look into ANCA Associated Vasculitis (AAV)
SHO Teaching Vasculitis Renal medicine Dr. Amir Bhanji Consultant Nephrologist, Q.A hospital, Portsmouth OUTLINE What is vasculitis Causes Classification Brief look into ANCA Associated Vasculitis (AAV)
Where a licence is displayed above, please note the terms and conditions of the licence govern your use of this document.
 Rituximab for treatment of severe renal disease in ANCA associated vasculitis Geetha, Duvuru; Hruskova, Zdenka; Segelmark, Marten; Hogan, Jonathan; Morgan, Matthew; Cavero, Teresa; Eriksson, Per; Seo,
Rituximab for treatment of severe renal disease in ANCA associated vasculitis Geetha, Duvuru; Hruskova, Zdenka; Segelmark, Marten; Hogan, Jonathan; Morgan, Matthew; Cavero, Teresa; Eriksson, Per; Seo,
Long-term outcome of patients with ANCAassociated vasculitis treated with plasma exchange: a retrospective, single-centre study
 Frausová et al. Arthritis Research & Therapy (2016) 18:168 DOI 10.1186/s13075-016-1055-5 RESEARCH ARTICLE Open Access Long-term outcome of patients with ANCAassociated vasculitis treated with plasma exchange:
Frausová et al. Arthritis Research & Therapy (2016) 18:168 DOI 10.1186/s13075-016-1055-5 RESEARCH ARTICLE Open Access Long-term outcome of patients with ANCAassociated vasculitis treated with plasma exchange:
Evidence-based therapy for the ANCAassociated vasculitides: what do the trials. show so far? Clinical Trial Outcomes
 associo far? Evidence-based therapy for the ANCAassociated vasculitides: what do the trials show so far? Anti-neutrophil cytoplasm antibody-associated vasculitides are rare multisystem inflammatory diseases
associo far? Evidence-based therapy for the ANCAassociated vasculitides: what do the trials show so far? Anti-neutrophil cytoplasm antibody-associated vasculitides are rare multisystem inflammatory diseases
Repeat protocol renal biopsy in ANCA-associated renal vasculitis
 NDT Advance Access published February 26, 2014 Nephrol Dial Transplant (2014) 0: 1 5 doi: 10.1093/ndt/gfu042 Original Article Repeat protocol renal biopsy in ANCA-associated renal vasculitis Zdenka Hruskova
NDT Advance Access published February 26, 2014 Nephrol Dial Transplant (2014) 0: 1 5 doi: 10.1093/ndt/gfu042 Original Article Repeat protocol renal biopsy in ANCA-associated renal vasculitis Zdenka Hruskova
The European and French networks. Christian Pagnoux, MD, MSc, MPH Mount Sinai Hospital, Toronto, Canada Cochin Hospital, Paris, France
 The European and French networks Christian Pagnoux, MD, MSc, MPH Mount Sinai Hospital, Toronto, Canada Cochin Hospital, Paris, France French Vasculitis Study Group December 1980: L. Guillevin no research,
The European and French networks Christian Pagnoux, MD, MSc, MPH Mount Sinai Hospital, Toronto, Canada Cochin Hospital, Paris, France French Vasculitis Study Group December 1980: L. Guillevin no research,
Management of Acute Vasculitis. CMT teaching 3 rd June 2015 Caroline Wroe
 Management of Acute Vasculitis CMT teaching 3 rd June 2015 Caroline Wroe Vasculitis pub quiz Match the date with the event Dr Peter McBride, Scottish Otolaryngologist describes a disease of rapid destruction
Management of Acute Vasculitis CMT teaching 3 rd June 2015 Caroline Wroe Vasculitis pub quiz Match the date with the event Dr Peter McBride, Scottish Otolaryngologist describes a disease of rapid destruction
New Evidence reports on presentations given at EULAR Rituximab for the Treatment of Rheumatoid Arthritis and Vasculitis
 New Evidence reports on presentations given at EULAR 2011 Rituximab for the Treatment of Rheumatoid Arthritis and Vasculitis Report on EULAR 2011 presentations Anti-TNF failure and response to rituximab
New Evidence reports on presentations given at EULAR 2011 Rituximab for the Treatment of Rheumatoid Arthritis and Vasculitis Report on EULAR 2011 presentations Anti-TNF failure and response to rituximab
EULAR/ERA-EDTA recommendations for the management of ANCAassociated
 EULAR/ERA-EDTA recommendations for the management of ANCAassociated vasculitis Dr. Meharunnisha Syed III year DNB Resident (General Medicine) Narayana Health-MSH Fifteen recommendations were developed,
EULAR/ERA-EDTA recommendations for the management of ANCAassociated vasculitis Dr. Meharunnisha Syed III year DNB Resident (General Medicine) Narayana Health-MSH Fifteen recommendations were developed,
Renal involvement in vasculitis
 Renal involvement in vasculitis Renal involvement in vasculitis Stephen Marks Consultant Paediatric Nephrologist Great Ormond Street Hospital for Children and UCL Institute of Child Health, London, UK.
Renal involvement in vasculitis Renal involvement in vasculitis Stephen Marks Consultant Paediatric Nephrologist Great Ormond Street Hospital for Children and UCL Institute of Child Health, London, UK.
End-stage renal disease in ANCA-associated vasculitis
 Nephrol Dial Transplant (2017) 32: 248 253 doi: 10.1093/ndt/gfw046 Advance Access publication 6 April 2016 End-stage renal disease in ANCA-associated vasculitis Sergey Moiseev 1, Pavel Novikov 1, David
Nephrol Dial Transplant (2017) 32: 248 253 doi: 10.1093/ndt/gfw046 Advance Access publication 6 April 2016 End-stage renal disease in ANCA-associated vasculitis Sergey Moiseev 1, Pavel Novikov 1, David
Efficacy and Safety of Rituximab in the Treatment of Rheumatoid Arthritis and ANCA-associated Vasculitis
 New Evidence reports on presentations given at ACR/ARHP 2010 Efficacy and Safety of Rituximab in the Treatment of Rheumatoid Arthritis and ANCA-associated Vasculitis Report on ACR/ARHP 2010 presentations
New Evidence reports on presentations given at ACR/ARHP 2010 Efficacy and Safety of Rituximab in the Treatment of Rheumatoid Arthritis and ANCA-associated Vasculitis Report on ACR/ARHP 2010 presentations
Antineutrophil cytoplasm antibody associated vasculitis: recent developments
 mini review http://www.kidney-international.org & 2013 International Society of Nephrology Antineutrophil cytoplasm antibody associated vasculitis: recent developments Shunsuke Furuta 1 and David R.W.
mini review http://www.kidney-international.org & 2013 International Society of Nephrology Antineutrophil cytoplasm antibody associated vasculitis: recent developments Shunsuke Furuta 1 and David R.W.
Clinical Case Conference Tuesday August 25, 2015 Dana Assis, MD
 Clinical Case Conference Tuesday August 25, 2015 Dana Assis, MD CC: LE swelling and pain for three weeks HPI: 71F hx HTN, DM (A1c 9.6), HFrEF (45%), asthma, OA, cryptogenic cirrhosis p/w bilateral lower
Clinical Case Conference Tuesday August 25, 2015 Dana Assis, MD CC: LE swelling and pain for three weeks HPI: 71F hx HTN, DM (A1c 9.6), HFrEF (45%), asthma, OA, cryptogenic cirrhosis p/w bilateral lower
Clinical research in adult vasculitis. Calgary October 8 th, 2015
 Clinical research in adult vasculitis Calgary October 8 th, 2015 Disclosures Consulting and speaker fees Hoffmann-La Roche BMS Advisory boards Hoffmann-La Roche GSK Educational subventions (CanVasc) Hoffmann-La
Clinical research in adult vasculitis Calgary October 8 th, 2015 Disclosures Consulting and speaker fees Hoffmann-La Roche BMS Advisory boards Hoffmann-La Roche GSK Educational subventions (CanVasc) Hoffmann-La
Wegener s Granulomatosis JUN-KI PARK
 Wegener s Granulomatosis JUN-KI PARK Definition History Epidemiology Clinical symptoms Pathophysiology Treatment Wegener granulomatosis (WG) is a complex, immunemediated disorder, which along with microscopic
Wegener s Granulomatosis JUN-KI PARK Definition History Epidemiology Clinical symptoms Pathophysiology Treatment Wegener granulomatosis (WG) is a complex, immunemediated disorder, which along with microscopic
anti-neutrophil cytoplasmic antibody, myeloperoxidase, microscopic polyangiitis, cyclophosphamide, corticosteroid
 Online publication June 24, 2009 ANCA JMAAV 1 2 ANCA JMAAV MPO-ANCA 18 17 50 J Jpn Coll Angiol, 2009, 49: 53 61 anti-neutrophil cytoplasmic antibody, myeloperoxidase, microscopic polyangiitis, cyclophosphamide,
Online publication June 24, 2009 ANCA JMAAV 1 2 ANCA JMAAV MPO-ANCA 18 17 50 J Jpn Coll Angiol, 2009, 49: 53 61 anti-neutrophil cytoplasmic antibody, myeloperoxidase, microscopic polyangiitis, cyclophosphamide,
Avacopan in addition to standard of care for ANCA-associated vasculitis
 EVIDENCE BRIEFING DECEMBER 2018 Avacopan in addition to standard of care for ANCA-associated vasculitis NIHRIO ID 24160 NICE ID 10023 Developer/Company ChemoCentryx and Vifor Pharma UK Ltd UKPS ID N/A
EVIDENCE BRIEFING DECEMBER 2018 Avacopan in addition to standard of care for ANCA-associated vasculitis NIHRIO ID 24160 NICE ID 10023 Developer/Company ChemoCentryx and Vifor Pharma UK Ltd UKPS ID N/A
Protocol Version 2.0 Synopsis
 Protocol Version 2.0 Synopsis Title Short Title Plasma exchange and glucocorticoid dosing in anti-neutrophil cytoplasm antibody associated vasculitis: a randomized controlled trial. PEXIVAS PEXIVAS Clinical
Protocol Version 2.0 Synopsis Title Short Title Plasma exchange and glucocorticoid dosing in anti-neutrophil cytoplasm antibody associated vasculitis: a randomized controlled trial. PEXIVAS PEXIVAS Clinical
ENFERMEDADES AUTOINMUNES SISTÉMICAS. Dr. J. María Pego Reigosa
 ENFERMEDADES AUTOINMUNES SISTÉMICAS Dr. J. María Pego Reigosa ABSTRACT NUMBER: 888 PHASE 3 TRIAL RESULTS WITH BLISIBIMOD, A SELECTIVE INHIBITOR OF B-CELL ACTIVATING FACTOR, IN SUBJECTS WITH MODERATE-TO-SEVERE
ENFERMEDADES AUTOINMUNES SISTÉMICAS Dr. J. María Pego Reigosa ABSTRACT NUMBER: 888 PHASE 3 TRIAL RESULTS WITH BLISIBIMOD, A SELECTIVE INHIBITOR OF B-CELL ACTIVATING FACTOR, IN SUBJECTS WITH MODERATE-TO-SEVERE
Rate of infections in severe necrotising vasculitis patients treated with cyclophosphamide induction therapy: a meta-analysis
 Rate of infections in severe necrotising vasculitis patients treated with cyclophosphamide induction therapy: a meta-analysis M. Jung 1, L. Barra 2 1 Division of Rheumatology, Department of Medicine, University
Rate of infections in severe necrotising vasculitis patients treated with cyclophosphamide induction therapy: a meta-analysis M. Jung 1, L. Barra 2 1 Division of Rheumatology, Department of Medicine, University
Systemerkrankungen mit Nierenbeteiligung
 Systemerkrankungen mit Nierenbeteiligung ÖGN Fuschl 2012 Irmgard Neumann Wilhelminenspital Wien Induktions-Therapie Generalisiert CYC i.v. pulse = CYC oral CYCLOPS, de Groot, Ann Int Med 2009 RIT vs CYC
Systemerkrankungen mit Nierenbeteiligung ÖGN Fuschl 2012 Irmgard Neumann Wilhelminenspital Wien Induktions-Therapie Generalisiert CYC i.v. pulse = CYC oral CYCLOPS, de Groot, Ann Int Med 2009 RIT vs CYC
Early plasma exchange improves outcome in PR3-ANCA-positive renal vasculitis
 Early plasma exchange improves outcome in PR3-ANCA-positive renal vasculitis J.W. Gregersen 1, T. Kristensen 1, S.R.P. Krag 2, H. Birn 1, P. Ivarsen 1 1 Department of Nephrology, 2 Department of Pathology,
Early plasma exchange improves outcome in PR3-ANCA-positive renal vasculitis J.W. Gregersen 1, T. Kristensen 1, S.R.P. Krag 2, H. Birn 1, P. Ivarsen 1 1 Department of Nephrology, 2 Department of Pathology,
Review Article. Current concepts in Anti-Neutrophil Cytoplasmic Antibody (ANCA) associated Vasculitis. Milind Aurangabadkar
 associated Vasculitis. Milind Aurangabadkar") Review Article Vidarbha Journal of Internal Medicine Volume 23 July 207 Current concepts in Anti-Neutrophil Cytoplasmic Antibody (ANCA) associated Vasculitis Milind Aurangabadkar ABSTRACT Anti-neutrophil
Review Article Vidarbha Journal of Internal Medicine Volume 23 July 207 Current concepts in Anti-Neutrophil Cytoplasmic Antibody (ANCA) associated Vasculitis Milind Aurangabadkar ABSTRACT Anti-neutrophil
Small Vessel Vasculitis
 Banff- Rocky Mountain Barry Kassen, MD, FRCPC,FACP Head, Division of Internal Medicine UBC/VGH/SPH Acting Head, Division of Community Internal Medicine November, 2009 Objectives 1. To understand small
Banff- Rocky Mountain Barry Kassen, MD, FRCPC,FACP Head, Division of Internal Medicine UBC/VGH/SPH Acting Head, Division of Community Internal Medicine November, 2009 Objectives 1. To understand small
Older patients with ANCA-associated vasculitis and dialysis dependent renal failure: a retrospective study
 Manno et al. BMC Nephrology (2015) 16:88 DOI 10.1186/s12882-015-0082-9 RESEARCH ARTICLE Open Access Older patients with ANCA-associated vasculitis and dialysis dependent renal failure: a retrospective
Manno et al. BMC Nephrology (2015) 16:88 DOI 10.1186/s12882-015-0082-9 RESEARCH ARTICLE Open Access Older patients with ANCA-associated vasculitis and dialysis dependent renal failure: a retrospective
TITLE: Rituximab for Granulomatosis with Polyangiitis or Microscopic Polyangiitis: A Review of the Clinical and Cost-effectiveness
 TITLE: Rituximab for Granulomatosis with Polyangiitis or Microscopic Polyangiitis: A Review of the Clinical and Cost-effectiveness DATE: 28 January 2015 CONTEXT AND POLICY ISSUES Granulomatosis with polyangiitis
TITLE: Rituximab for Granulomatosis with Polyangiitis or Microscopic Polyangiitis: A Review of the Clinical and Cost-effectiveness DATE: 28 January 2015 CONTEXT AND POLICY ISSUES Granulomatosis with polyangiitis
ANCA-associated vasculitis with renal involvement: an outcome analysis
 NDT Advance Access published April 6, Nephrol Dial Transplant () 1 of 9 DOI: 1.193/ndt/gfh161 Original Article ANCA-associated vasculitis with renal involvement: an outcome analysis Sven Weidner 1, Steffen
NDT Advance Access published April 6, Nephrol Dial Transplant () 1 of 9 DOI: 1.193/ndt/gfh161 Original Article ANCA-associated vasculitis with renal involvement: an outcome analysis Sven Weidner 1, Steffen
Chapter 4: Steroid-resistant nephrotic syndrome in children Kidney International Supplements (2012) 2, ; doi: /kisup.2012.
 2, ; doi: /kisup.2012.") http://www.kidney-international.org & 2012 KDIGO Chapter 4: Steroid-resistant nephrotic syndrome in children Kidney International Supplements (2012) 2, 172 176; doi:10.1038/kisup.2012.17 INTRODUCTION This
http://www.kidney-international.org & 2012 KDIGO Chapter 4: Steroid-resistant nephrotic syndrome in children Kidney International Supplements (2012) 2, 172 176; doi:10.1038/kisup.2012.17 INTRODUCTION This
EudraCT number: Page 8 of 42
 EudraCT number: 2012-001102-14 Page 8 of 42 5 Trial Synopsis Title Sponsor name North American Sponsor Disease Under Investigation An international, open label, randomised, controlled trial comparing rituximab
EudraCT number: 2012-001102-14 Page 8 of 42 5 Trial Synopsis Title Sponsor name North American Sponsor Disease Under Investigation An international, open label, randomised, controlled trial comparing rituximab
Renal outcome of kidney-transplantation in Korean recipients with ANCA-associated vasculitis
 Renal outcome of kidney-transplantation in Korean recipients with ANCA-associated vasculitis E.S. Park, S.S. Ahn, S.M. Jung, J.J. Song, Y.-B. Park, S.-W. Lee Division of Rheumatology, Department of Internal
Renal outcome of kidney-transplantation in Korean recipients with ANCA-associated vasculitis E.S. Park, S.S. Ahn, S.M. Jung, J.J. Song, Y.-B. Park, S.-W. Lee Division of Rheumatology, Department of Internal
EudraCT number: Page 9 of 46
 EudraCT number: 2012-001102-14 Page 9 of 46 5 Trial Synopsis Title Sponsor name North American Sponsor Japan Sponsor Ireland Sponsor Disease Under Investigation An international, open label, randomised,
EudraCT number: 2012-001102-14 Page 9 of 46 5 Trial Synopsis Title Sponsor name North American Sponsor Japan Sponsor Ireland Sponsor Disease Under Investigation An international, open label, randomised,
Long-term follow-up of patients with severe ANCAassociated vasculitis comparing plasma exchange to intravenous methylprednisolone treatment is unclear
 http://www.kidney-international.org & 2013 International Society of Nephrology Long-term of patients with severe ANCAassociated vasculitis comparing plasma exchange to intravenous methylprednisolone treatment
http://www.kidney-international.org & 2013 International Society of Nephrology Long-term of patients with severe ANCAassociated vasculitis comparing plasma exchange to intravenous methylprednisolone treatment
Paediatric anti-neutrophil cytoplasmic antibody (ANCA) -associated vasculitis: an update on renal management
 -associated vasculitis: an update on renal management") Pediatr Nephrol (2018) 33:25 39 DOI 10.1007/s00467-016-3559-2 REVIEW Paediatric anti-neutrophil cytoplasmic antibody (ANCA) -associated vasculitis: an update on renal management Lucy A Plumb 1 & Louise
Pediatr Nephrol (2018) 33:25 39 DOI 10.1007/s00467-016-3559-2 REVIEW Paediatric anti-neutrophil cytoplasmic antibody (ANCA) -associated vasculitis: an update on renal management Lucy A Plumb 1 & Louise
Case Rep Nephrol Urol 2013;3: DOI: / Published online: January 27, 2013
 Published online: January 27, 2013 1664 5510/13/0031 0016$38.00/0 This is an Open Access article licensed under the terms of the Creative Commons Attribution- NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license),
Published online: January 27, 2013 1664 5510/13/0031 0016$38.00/0 This is an Open Access article licensed under the terms of the Creative Commons Attribution- NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license),
Rheumatology Advance Access published March 7, Induction treatment of ANCA-associated vasculitis with a single dose of rituximab
 Original article Rheumatology Advance Access published March 7, 2014 RHEUMATOLOGY 262 doi:10.1093/rheumatology/ket489 Induction treatment of ANCA-associated vasculitis with a single dose of rituximab Tabitha
Original article Rheumatology Advance Access published March 7, 2014 RHEUMATOLOGY 262 doi:10.1093/rheumatology/ket489 Induction treatment of ANCA-associated vasculitis with a single dose of rituximab Tabitha
Pharmacy Management Drug Policy
 SUBJECT: : Nucala (mepolizumab), Cinqair (reslizumab), & Fasenra (benralizumab) POLICY NUMBER: Pharmacy-62 EFFECTIVE DATE: 12/15 LAST REVIEW DATE: 3/5/2018 If the member s subscriber contract excludes
SUBJECT: : Nucala (mepolizumab), Cinqair (reslizumab), & Fasenra (benralizumab) POLICY NUMBER: Pharmacy-62 EFFECTIVE DATE: 12/15 LAST REVIEW DATE: 3/5/2018 If the member s subscriber contract excludes
Update and Review on Vasculitis. Ramona Raya, MD ACP Internal Medicine Congress August 7, 2015
 Update and Review on Vasculitis Ramona Raya, MD ACP Internal Medicine Congress August 7, 2015 Outline Classification and nomenclature updates Small vessel vasculitis Pathophysiology Diagnosis Management/therapeutic
Update and Review on Vasculitis Ramona Raya, MD ACP Internal Medicine Congress August 7, 2015 Outline Classification and nomenclature updates Small vessel vasculitis Pathophysiology Diagnosis Management/therapeutic
Updates from the 15 th ANCA workshop
 Updates from the 15 th ANCA workshop Christian Pagnoux, MD, MSc, MPH Mount Sinai Hospital, Toronto, Canada Cochin Hospital, Paris, France Nataliya Milman, MD Ottawa, Canada Simon Carette, MD, MPhil, FRCP
Updates from the 15 th ANCA workshop Christian Pagnoux, MD, MSc, MPH Mount Sinai Hospital, Toronto, Canada Cochin Hospital, Paris, France Nataliya Milman, MD Ottawa, Canada Simon Carette, MD, MPhil, FRCP
IRACON Management of Lupus Nephritis: Old is gold, New is Trendy
 IRACON 2016 Management of Lupus Nephritis: Old is gold, New is Trendy First episode of LN (III/IV): Induction Low dose is equally considerable as high dose CYC Switch to the other agent if no improvement
IRACON 2016 Management of Lupus Nephritis: Old is gold, New is Trendy First episode of LN (III/IV): Induction Low dose is equally considerable as high dose CYC Switch to the other agent if no improvement
Everyday Vasculitis (or what questions do we get asked most!) Lucy Smyth Renal Consultant
 Lucy Smyth Renal Consultant") Everyday Vasculitis (or what questions do we get asked most!) Lucy Smyth Renal Consultant What is it? Why have I got it? How can we treat it? Why do I feel like I do? What do the blood tests mean? Will
Everyday Vasculitis (or what questions do we get asked most!) Lucy Smyth Renal Consultant What is it? Why have I got it? How can we treat it? Why do I feel like I do? What do the blood tests mean? Will
PAEDIATRIC VASCULITIS
 PAEDIATRIC VASCULITIS Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. OUTLINE Introduction
PAEDIATRIC VASCULITIS Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. OUTLINE Introduction
Lupus Related Kidney Diseases. Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017
 Lupus Related Kidney Diseases Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017 Financial Disclosures MedImmune Lupus Nephritis Kidney Biopsy Biomarkers
Lupus Related Kidney Diseases Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017 Financial Disclosures MedImmune Lupus Nephritis Kidney Biopsy Biomarkers
Glucocorticoids and Relapse and Infection Rates in Anti-Neutrophil Cytoplasmic Antibody Disease
 Article Glucocorticoids and Relapse and Infection Rates in Anti-Neutrophil Cytoplasmic Antibody Disease JulieAnne G. McGregor, Susan L. Hogan, Yichun Hu, Caroline E. Jennette, Ronald J. Falk, and Patrick
Article Glucocorticoids and Relapse and Infection Rates in Anti-Neutrophil Cytoplasmic Antibody Disease JulieAnne G. McGregor, Susan L. Hogan, Yichun Hu, Caroline E. Jennette, Ronald J. Falk, and Patrick
Pauci-immune glomerulonephritis: does negativity of antineutrophilic cytoplasmic antibodies matters?
 International Journal of Rheumatic Diseases 2016; 19: 74 81 ORIGINAL ARTICLE Pauci-immune glomerulonephritis: does negativity of antineutrophilic cytoplasmic antibodies matters? Aman SHARMA, 1, * Ritambra
International Journal of Rheumatic Diseases 2016; 19: 74 81 ORIGINAL ARTICLE Pauci-immune glomerulonephritis: does negativity of antineutrophilic cytoplasmic antibodies matters? Aman SHARMA, 1, * Ritambra
New biomarkers for ANCA-associated Vasculitis? Juliana Bordignon Draibe
 New biomarkers for ANCA-associated Vasculitis? Juliana Bordignon Draibe Summary Introduction Antibodies: ANCAs, Anti-LAMP-2, Anti-moesin B and T lymphocytes Markers of vascular activation: complement,
New biomarkers for ANCA-associated Vasculitis? Juliana Bordignon Draibe Summary Introduction Antibodies: ANCAs, Anti-LAMP-2, Anti-moesin B and T lymphocytes Markers of vascular activation: complement,
Russia Dialysis Society Peterhof, Russia June 8, 2016
 Russia Dialysis Society Peterhof, Russia June 8, 2016 TREATMENT OF GLOMERULONEPHRITIS XV Северо-Западная ( AAV, SLE, Нефрологическая Membranous) Школа What s changed in the past decade? William Couser,
Russia Dialysis Society Peterhof, Russia June 8, 2016 TREATMENT OF GLOMERULONEPHRITIS XV Северо-Западная ( AAV, SLE, Нефрологическая Membranous) Школа What s changed in the past decade? William Couser,
AN OVERVIEW OF ANCA-ASSOCIATED VASCULITIS
 GRANULOMATOSIS WITH POLYANGIITIS (GPA), MICROSCOPIC POLYANGIITIS (MPA), and EOSINOPHILIC GRANULOMATOSIS WITH POLYANGIITIS (EGPA) AN OVERVIEW OF ANCA-ASSOCIATED VASCULITIS What is ANCA-associated Vasculitis?
GRANULOMATOSIS WITH POLYANGIITIS (GPA), MICROSCOPIC POLYANGIITIS (MPA), and EOSINOPHILIC GRANULOMATOSIS WITH POLYANGIITIS (EGPA) AN OVERVIEW OF ANCA-ASSOCIATED VASCULITIS What is ANCA-associated Vasculitis?
ANCA-associated systemic vasculitis (AASV)
") PAPER 2007 Royal College of Physicians of Edinburgh ANCA-associated systemic vasculitis (AASV) 1 DC Kluth, 2 J Hughes 1 Reader in Nephrology, MRC Centre for Inflammation Research, University of Edinburgh,
PAPER 2007 Royal College of Physicians of Edinburgh ANCA-associated systemic vasculitis (AASV) 1 DC Kluth, 2 J Hughes 1 Reader in Nephrology, MRC Centre for Inflammation Research, University of Edinburgh,
Annals of the Rheumatic Diseases 2011; 70(3):
:") Long-term patient survival in ANCA-associated vasculitis Oliver Floßmann Annelies Berden Kirsten de Groot Chris Hagen Lorraine Harper Caroline Heijl Peter Höglund David Jayne Raashid Luqmani Alfred Mahr
Long-term patient survival in ANCA-associated vasculitis Oliver Floßmann Annelies Berden Kirsten de Groot Chris Hagen Lorraine Harper Caroline Heijl Peter Höglund David Jayne Raashid Luqmani Alfred Mahr
Estimating Renal Survival Using the ANCA-Associated GN Classification
 Estimating Renal Survival Using the ANCA-Associated GN Classification Marc Hilhorst, Benjamin Wilde, Peter van Breda Vriesman, Pieter van Paassen, and Jan Willem Cohen Tervaert, for the Limburg Renal Registry
Estimating Renal Survival Using the ANCA-Associated GN Classification Marc Hilhorst, Benjamin Wilde, Peter van Breda Vriesman, Pieter van Paassen, and Jan Willem Cohen Tervaert, for the Limburg Renal Registry
Additional file 2: Details of cohort studies and randomised trials
 Reference Randomised trials Ye et al. 2001 Abstract 274 R=1 WD=0 Design, numbers, treatments, duration Randomised open comparison of: (45 patients) 1.5 g for 3, 1 g for 3, then 0.5 to 0.75 g IV cyclophosphamide
Reference Randomised trials Ye et al. 2001 Abstract 274 R=1 WD=0 Design, numbers, treatments, duration Randomised open comparison of: (45 patients) 1.5 g for 3, 1 g for 3, then 0.5 to 0.75 g IV cyclophosphamide
Renal transplantation in anti-neutrophil cytoplasmic antibody-associated vasculitis
 Nephrol Dial Transplant (2015) 30: i159 i163 doi: 10.1093/ndt/gfu328 Advance Access publication 16 October 2014 Full Review Renal transplantation in anti-neutrophil cytoplasmic antibody-associated vasculitis
Nephrol Dial Transplant (2015) 30: i159 i163 doi: 10.1093/ndt/gfu328 Advance Access publication 16 October 2014 Full Review Renal transplantation in anti-neutrophil cytoplasmic antibody-associated vasculitis
Improved prognosis in Norwegian patients with glomerulonephritis associated with anti-neutrophil cytoplasmic antibodies
 Nephrol Dial Transplant (2015) 30: i67 i75 doi: 10.1093/ndt/gfv008 Advance Access publication 17 February 2015 Original Article Improved prognosis in Norwegian patients with glomerulonephritis associated
Nephrol Dial Transplant (2015) 30: i67 i75 doi: 10.1093/ndt/gfv008 Advance Access publication 17 February 2015 Original Article Improved prognosis in Norwegian patients with glomerulonephritis associated
Technology appraisal guidance Published: 26 March 2014 nice.org.uk/guidance/ta308
 Rituximab in combination with glucocorticoids for treating antineutrophil cytoplasmic antibody- associated vasculitis Technology appraisal guidance Published: 26 March 2014 nice.org.uk/guidance/ta308 NICE
Rituximab in combination with glucocorticoids for treating antineutrophil cytoplasmic antibody- associated vasculitis Technology appraisal guidance Published: 26 March 2014 nice.org.uk/guidance/ta308 NICE
IgA-Nephropathy: an update on treatment Jürgen Floege
 IgA-Nephropathy: an update on treatment Jürgen Floege Division of Nephrology & Immunology juergen.floege@rwth-aachen.de Floege & Feehally, Nat Rev Nephrol 2013 Floege & Eitner, J Am Soc Nephrol. 2011 If
IgA-Nephropathy: an update on treatment Jürgen Floege Division of Nephrology & Immunology juergen.floege@rwth-aachen.de Floege & Feehally, Nat Rev Nephrol 2013 Floege & Eitner, J Am Soc Nephrol. 2011 If
Considering the early proactive switch from a CNI to an mtor-inhibitor (Case: Male, age 34) Josep M. Campistol
 Josep M. Campistol") Considering the early proactive switch from a CNI to an mtor-inhibitor (Case: Male, age 34) Josep M. Campistol Patient details Name DOB ESRD Other history Mr. B.I.B. 12 January 1975 (34yo) Membranous GN
Considering the early proactive switch from a CNI to an mtor-inhibitor (Case: Male, age 34) Josep M. Campistol Patient details Name DOB ESRD Other history Mr. B.I.B. 12 January 1975 (34yo) Membranous GN
The CARI Guidelines Caring for Australasians with Renal Impairment. Membranous nephropathy role of steroids GUIDELINES
 Membranous nephropathy role of steroids Date written: July 2005 Final submission: September 2005 Author: Merlin Thomas GUIDELINES There is currently no data to support the use of short-term courses of
Membranous nephropathy role of steroids Date written: July 2005 Final submission: September 2005 Author: Merlin Thomas GUIDELINES There is currently no data to support the use of short-term courses of
New Ideas. Better Medicines. Presentation to Investors. January 2019
 New Ideas. Better Medicines. Presentation to Investors January 2019 Forward Looking Statements 2 This presentation contains forward looking statements that involve substantial risks and uncertainties.
New Ideas. Better Medicines. Presentation to Investors January 2019 Forward Looking Statements 2 This presentation contains forward looking statements that involve substantial risks and uncertainties.
The CARI Guidelines Caring for Australasians with Renal Impairment. Idiopathic membranous nephropathy: use of other therapies GUIDELINES
 Idiopathic membranous nephropathy: use of other therapies Date written: July 2005 Final submission: September 2005 Author: Merlin Thomas GUIDELINES No recommendations possible based on Level I or II evidence
Idiopathic membranous nephropathy: use of other therapies Date written: July 2005 Final submission: September 2005 Author: Merlin Thomas GUIDELINES No recommendations possible based on Level I or II evidence
ANCA Glomerulonephritis and Vasculitis
 CJASN epress. Published on August 25, 2017 as doi: 10.2215/CJN.02500317 ANCA Glomerulonephritis and Vasculitis J. Charles Jennette and Patrick H. Nachman Abstract ANCA vasculitis has an associated autoimmune
CJASN epress. Published on August 25, 2017 as doi: 10.2215/CJN.02500317 ANCA Glomerulonephritis and Vasculitis J. Charles Jennette and Patrick H. Nachman Abstract ANCA vasculitis has an associated autoimmune
Sponsored document from American Journal of Kidney Diseases
 Sponsored document from American Journal of Kidney Diseases Prediction of ESRD in Pauci-immune Necrotizing Glomerulonephritis: Quantitative Histomorphometric Assessment and Serum Creatinine Clara J. Day
Sponsored document from American Journal of Kidney Diseases Prediction of ESRD in Pauci-immune Necrotizing Glomerulonephritis: Quantitative Histomorphometric Assessment and Serum Creatinine Clara J. Day
Rapidly progressive glomerulonephritis. Alan Salama UCL Centre for Nephrology Royal Free Hospital
 Rapidly progressive glomerulonephritis Alan Salama UCL Centre for Nephrology Royal Free Hospital Remember this. AKI Acute tubular injury Not all AKI is caused by sepsis or volume depletion AKI is caused
Rapidly progressive glomerulonephritis Alan Salama UCL Centre for Nephrology Royal Free Hospital Remember this. AKI Acute tubular injury Not all AKI is caused by sepsis or volume depletion AKI is caused
The CARI Guidelines Caring for Australasians with Renal Impairment. Specific management of IgA nephropathy: role of steroid therapy GUIDELINES
 Specific management of IgA nephropathy: role of steroid therapy Date written: July 2005 Final submission: September 2005 Author: Merlin Thomas GUIDELINES Steroid therapy may protect against progressive
Specific management of IgA nephropathy: role of steroid therapy Date written: July 2005 Final submission: September 2005 Author: Merlin Thomas GUIDELINES Steroid therapy may protect against progressive
Lupus and Your Kidneys. Michael P. Madaio, MD Professor of Medicine Chairman of Medicine Medical College of Georgia Augusta, Georgia
 Lupus and Your Kidneys Michael P. Madaio, MD Professor of Medicine Chairman of Medicine Medical College of Georgia Augusta, Georgia Kidney Inflammation and Abnormal Function as a Result of Lupus (Lupus
Lupus and Your Kidneys Michael P. Madaio, MD Professor of Medicine Chairman of Medicine Medical College of Georgia Augusta, Georgia Kidney Inflammation and Abnormal Function as a Result of Lupus (Lupus
Prediction of ESRD in Pauci-immune Necrotizing Glomerulonephritis: Quantitative Histomorphometric Assessment and Serum Creatinine
 ORIGINAL INVESTIGATIONS Pathogenesis and Treatment of Kidney Disease Prediction of ESRD in Pauci-immune Necrotizing Glomerulonephritis: Quantitative Histomorphometric Assessment and Serum Creatinine Clara
ORIGINAL INVESTIGATIONS Pathogenesis and Treatment of Kidney Disease Prediction of ESRD in Pauci-immune Necrotizing Glomerulonephritis: Quantitative Histomorphometric Assessment and Serum Creatinine Clara
Vasculitis. Edward Dwyer, M.D. Division of Rheumatology. Vasculitis
 Edward Dwyer, M.D. Division of Rheumatology VASCULITIS is a primary inflammatory disease process of the vasculature Determinants of the Clinical Manifestations of : Target organ involved Size of vessel
Edward Dwyer, M.D. Division of Rheumatology VASCULITIS is a primary inflammatory disease process of the vasculature Determinants of the Clinical Manifestations of : Target organ involved Size of vessel
Rituximab (MabThera) maintenance therapy for granulomatosis with polyangiitis (GPA) and microscopic polyangiitis (MPA)
 maintenance therapy for granulomatosis with polyangiitis (GPA) and microscopic polyangiitis (MPA)") NIHR Innovation Observatory Evidence Briefing: August 2017 Rituximab (MabThera) maintenance therapy for granulomatosis with polyangiitis (GPA) and microscopic polyangiitis (MPA) NIHRIO (HSRIC) ID: 12979
NIHR Innovation Observatory Evidence Briefing: August 2017 Rituximab (MabThera) maintenance therapy for granulomatosis with polyangiitis (GPA) and microscopic polyangiitis (MPA) NIHRIO (HSRIC) ID: 12979
Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis
 GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
Chapter 6: Idiopathic focal segmental glomerulosclerosis in adults Kidney International Supplements (2012) 2, ; doi: /kisup.2012.
 2, ; doi: /kisup.2012.") http://www.kidney-international.org chapter 6 & 2012 KDIGO Chapter 6: Idiopathic focal segmental glomerulosclerosis in adults Kidney International Supplements (2012) 2, 181 185; doi:10.1038/kisup.2012.19
http://www.kidney-international.org chapter 6 & 2012 KDIGO Chapter 6: Idiopathic focal segmental glomerulosclerosis in adults Kidney International Supplements (2012) 2, 181 185; doi:10.1038/kisup.2012.19
Renal transplantation
 NEPHROLOGY 2008; 13, S37 S43 doi:10.1111/j.1440-1797.2008.00996.x Renal transplantation Date written: November 2006 Final submission: July 2007 Author: Nigel Toussaint GUIDELINES No recommendations possible
NEPHROLOGY 2008; 13, S37 S43 doi:10.1111/j.1440-1797.2008.00996.x Renal transplantation Date written: November 2006 Final submission: July 2007 Author: Nigel Toussaint GUIDELINES No recommendations possible
LONG-TERM OUTCOME OF PATIENTS WITH LUPUS NEPHRITIS: A SINGLE CENTER EXPERIENCE
 & LONG-TERM OUTCOME OF PATIENTS WITH LUPUS NEPHRITIS: A SINGLE CENTER EXPERIENCE Senija Rašić 1 *, Amira Srna 1, Snežana Unčanin 1, Jasminka Džemidžić 1, Damir Rebić 1, Alma Muslimović 1, Maida Rakanović-Todić
& LONG-TERM OUTCOME OF PATIENTS WITH LUPUS NEPHRITIS: A SINGLE CENTER EXPERIENCE Senija Rašić 1 *, Amira Srna 1, Snežana Unčanin 1, Jasminka Džemidžić 1, Damir Rebić 1, Alma Muslimović 1, Maida Rakanović-Todić
NEWS RELEASE Genentech Contacts: Media: Joe St. Martin (650) Investor: Karl Mahler Thomas Kudsk Larsen (973)
 Investor: Karl Mahler Thomas Kudsk Larsen (973)") NEWS RELEASE Genentech Contacts: Media: Joe St. Martin (650) 467-6800 Investor: Karl Mahler 011 41 61 687 8503 Thomas Kudsk Larsen (973) 235-3655 Biogen Idec Contacts: Media: Christina Chan (781) 464-3260
NEWS RELEASE Genentech Contacts: Media: Joe St. Martin (650) 467-6800 Investor: Karl Mahler 011 41 61 687 8503 Thomas Kudsk Larsen (973) 235-3655 Biogen Idec Contacts: Media: Christina Chan (781) 464-3260
ENFERMEDADES AUTOINMUNES SISTÉMICAS. Dr. José María Pego Reigosa
 ENFERMEDADES AUTOINMUNES SISTÉMICAS Dr. José María Pego Reigosa ABSTRACT NUMBER: 2754 Comparison of Individually Tailored vs Systematic Rituximab Regimens to Maintain ANCA-Associated Vasculitis Remissions:
ENFERMEDADES AUTOINMUNES SISTÉMICAS Dr. José María Pego Reigosa ABSTRACT NUMBER: 2754 Comparison of Individually Tailored vs Systematic Rituximab Regimens to Maintain ANCA-Associated Vasculitis Remissions: