ARTHRITIS ARTHRITIS. DR jp,asst prof,ich,mch,kottayam
|
|
|
- Hannah Ball
- 5 years ago
- Views:
Transcription
1 ARTHRITIS ARTHRITIS DR jp,asst prof,ich,mch,kottayam Arthritis is manifested as a swollen joint or a joint having at least 2 of the following conditions: limited range of motion, pain on movement (stress pain), or warmth overlying the joint. The assessment of a child with arthritis must enable differentiation between acute and chronic causes of arthritis and, particularly, recognition of those who may require urgent medical or surgical intervention. Juvenile idiopathic arthritis (JIA) is only one of the many causes of arthritis. This review covers the evaluation of a child with arthritis of one (mono) or several (poly) joints. POLYARTHRITIS The differential diagnosis of polyarthritis essentially includes infectious, inflammatory,and malignant causes. Although mechanical causes (eg, hypermobility and skeletal dysplasia) and diffuse idiopathic pain syndromes are considered in the differential diagnosis of polyarthralgia, they do not routinely cause polyarthritis. The review of systems and physical examination is critical to establishing a diagnosis because there are clues in the characteristics of the arthritis, fever, rash, and other system involvements that often provide the correct diagnosis When polyarthritis is the presenting complaint, in addition to the investigations outlined in Box 1 additional investigations may include serum C3 and C4 complement levels, serum levels of quantitative immunoglobulins, urinalysis, serologic testing for viralpathogens, swabs for gonococcal infection as indicated, ASO and anti DNase B titers, cardiac evaluation (electrocardiography and echocardiography), chest radiography, ANA titer, other autoantibodies (anti-
2 Ro, anti-la, anti-sm, anti-rnp, anti Scl 70), and antineutrophil cytoplasmic antibody Rheumatic Diseases Polyarthritis is a presenting feature of many rheumatic diseases including JIA, autoimmune connective tissue diseases, and systemic vasculitides. The most common cause of rheumatic diseases is polyarticular JIA (both RF negative and RF positive). Systemic JIA (SJIA) classically presents with a quotidian fever of at least 2 weeks duration. The typical pattern is once or twice daily spikes, with return to normal or even subnormal temperatures between spikes. In SJIA, the rash is evanescent, often occurring with the fever, which helps to distinguish this diagnosis from the rashes of erythema marginatum in ARF, palpable purpura in vasculitis, or Gottron papules in juvenile dermatomyositis. SLE commonly presents in adolescence with low-grade fevers, constitutional symptoms of anorexia, weight loss, malar rashes, and painful polyarthritis affecting both the large and small joints.32 Generally, the ANA titer is strongly positive in SLE but may also be positive in polyarticular JIA. Both SLE and SJIA can present with serositis and hepatosplenomegaly; however, the presence of nephritis, cytopenias, hypocomplementemia, anti-dsdna, and other autoantibodies differentiates SLE from SJIA Patients with systemic sclerosis and idiopathic inflammatory myositis frequently have mild nonpainful arthritis, but there are other clues to these diagnoses (weakness, heliotrope rashes, and Gottron papules seen in juvenile dermatomyositis and sclerotic skin changes; Raynaud phenomenon; skin and gum telangiectasias; respiratory symptoms; or gastrointestinal [GI] tract dysmotility seen in systemic sclerosis). MCTD is characterized by Raynaud phenomenon, myositis, polyarthritis and sclerodactyly with positive ANA titer and high titers of anti-rnp autoantibodies. The painful oligoarthritis or polyarthritis associated with Kawasaki disease can occur in up to one-third of patients and is typically observed in the subacute phase of the illness; however, it may also be seen in the acute phase.33 Arthritis is also seen in 75% of patients34 with Henoch-Scho nlein

3 purpura, but other features, such as lower extremity palpable purpura, abdominal pain, and nephritis, help to clarify this diagnosis. Pediatric sarcoidosis is a rare chronic noncaseating granulomatous disease characterized by arthritis, eczematous-like rash, anterior or posterior uveitis, and polyarthritis often associated with marked tenosynovitis.35 Fever, constitutional symptoms, hepatosplenomegaly, bone marrow involvement, and pulmonary manifestations are seen more with the adult-onset form of sarcoidosis.
4

5 Polyarthritis may also be a presenting feature of several of the autoinflammatory syndromes (familial Mediterranean fever, cryopyrinassociated periodic syndrome, hyperimmunoglobulinemia D syndrome

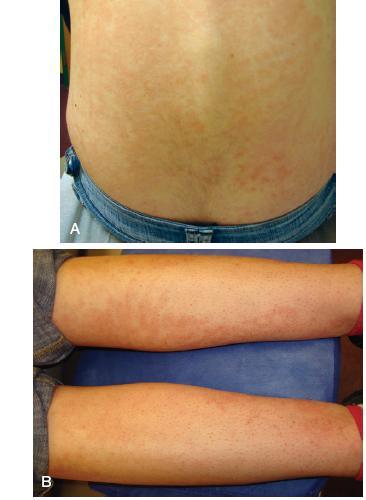
6 Systemic lupus erythematosus. A, Malar rash of systemic lupus erythematosus. Erythema, erosion, and atrophy are present. Note sparing of nasolabial folds. This patient also has a rash involving the forehead and chin. B, Lateral view shows ear involvement

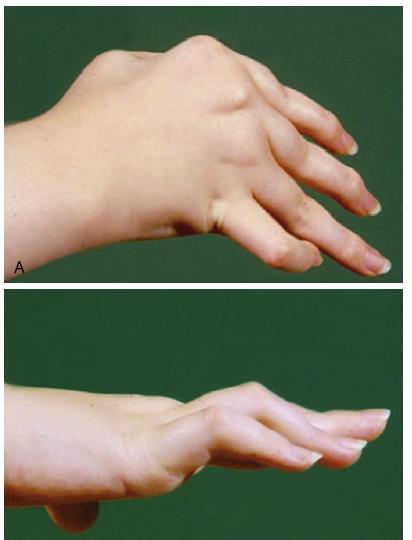
7 Juvenile idiopathic arthritis (JIA). A, Erythema of the knee in a patient with systemic-onset JIA (Still disease). B, Swelling and inflammation of the small joints of the hands in a patient with polyarticular JIA. Note the inability to fully extend the fingers. C, Swelling of the right thumb interphalangeal joint. D, Right knee swelling in a patient with pauciarticular JIA.
8


9 A, Gottron papules: Erythematous, atrophic skin changes overlying the metacarpophalangeal and proximal interphalangeal joints. B and C, Typical rash of JDM, as seen on B, the knees and C, the elbow. heliotrope rash
10 pathogens, swabs for gonococcal infection as indicated, ASO and anti DNase B
11 titers, cardiac evaluation (electrocardiography and echocardiography), chest radiography, ANA titer, other autoantibodies (anti-ro, anti-la, anti-sm, anti-rnp, anti Scl 70), and antineutrophil cytoplasmic antibody. Polyarthritis Related to Infection Bacterial pathogens Bacterial pathogens are generally associated with monoarthritis (septic joint).however, N gonorrhoeae is associated with fever, chills, vesiculopustular rashes,and migratory arthritis often accompanied by painful tenosynovitis. Purulent synovitis of several joints may be observed. Gonococcal arthritis usually develops inassociation with primary asymptomatic genitourinary tract infection or gonococcal infection of the throat or rectum. Thus, if suspected, cultures from the genital tract, throat, rectum, and any ve sicle in addition to the joint fluid should be obtained. The arthritis of infective endocarditis can precede other immune-mediated manifestations (Osler nodes, Janeway lesions, Roth spots) by weeks. This symmetric polyarthritis is thought to be an immune complex mediated process as demonstrated by the presence of hypocomplementemia, circulating immune complexes, and sometimes RFs.11 Reactive arthritis related to streptococcal infection: ARF and PSRA The diagnosis of ARF is established mainly on clinical grounds. The initial description of the clinical manifestations, now known as the Jones criteria, was revised most recently in The major criteria include (1) carditis, (2) polyarthritis, (3) chorea,(4) erythema marginatum, and (5) subcutaneous nodules. The minor criteria include(1) arthralgia (counted only when arthritis is not present), (2) fever, (3) elevated acutephase reactants, and (4) an electrocardiogram showing prolonged PR interval (firstdegreeheart block). Evidence of a preceding GAS infection is necessary for the diagnosisand indicates a high probability of ARF when present with 2 major manifestationsor 1 major and 2 minor manifestations.36 Evidence of prior GAS infection is necessary for the diagnosis of both ARF and PSRA. Microbiological confirmation can be obtained by throat culture or rapid antigen detection tests. However, both throat culture and rapid antigen detection tests cannot differentiate a true GAS infection from a carrier state, which can be found in as many as 15% of school-aged children.37
12 Confirmation of a recent GAS infection may also be achieved by serologic testing. A preceding GAS infection can be identified in the presence of elevated or increasing antistreptococcal antibody titers. The most commonlyused tests are ASO and anti DNase B. After the initial GAS infection, ASO titers begin to increase in 1 week and peak 3 to 6weeks later. Anti DNase B titers begin to increase in 1 to 2 weeks and peak 6 to 8 weeks after the infection. Elevated titers for both tests may persist for months after GAS infection.11 Differentiating between ARF and PSRA can be a challenge. PSRA tends to occur sooner after a streptococcal infection than the arthritis of ARF (7 10 vs days). The arthritis of ARF is typically migratory in nature, involving the large joints; is often associated with erythema over the joints and significant elevation in the acute phase reactants; and is dramatically responsive to NSAIDs. This is in contrast to the additive arthritis seen in PSRA, which tends to be more persistent, involves large and small joints and axial involvement, is associated with only moderate elevation in acute phase reactants, and is more resistant to NSAIDs.38 Viral pathogens Arthralgia and arthritis are well recognized and relatively common occurrences with viral infections. The most widely recognized viral-induced arthritis (in adults) is caused by parvovirus B19. This virus causes fifth disease/erythema infectiosum, a self-limited exanthem of childhood. Joint symptoms occur in about 10% of children and 60% of adults. In pediatrics, arthritis may be asymmetric and oligoarticular (<4 joints) in contrast to the acute-onset symmetric arthritis more commonly seen in adults.39 The diagnosis is made if circulating IgM antibodies to parvovirus are present. Treatment is supportive with NSAIDs. Although a primary rubella virus infection is associated with arthritis, a general pediatrician is more likely to observe arthritis associated with the rubella vaccine. Jointsymptoms usually develop approximately 2 weeks (10 28 days) after vaccination. Symmetric, migratory, and additive arthritis typically resolve within 2 to 4 weeks.11 Several herpesviruses, including varicella-zoster virus, Epstein-Barr virus, herpes simplex virus, and cytomegalovirus, have been associated with arthritis, in addition to hepatitis B and C. There are many immune phenomena related to human immunodeficiency virus infection, one of which is reactive arthritis.40
13 Other Important Diagnostic Considerations IBD can be associated with arthritis in 7% to 21% of children affected by this disease.11 There are 2 patterns of joint disease that can occur in association with IBD. The first pattern is involvement of the lower extremity joints, especially the ankles and knees. The activity of this peripheral arthritis tends to parallel the activity of the GI tract inflammation. Medical management is aimed at optimizing control of the GI tract inflammation, resulting in improvement in arthritis. The second pattern is of axial involvement and is often associated with HLA-B27. The involvement bears little relation to the GI disease. Clues to this would include a positive history of cramping abdominal pain, anorexia, diarrhea/hematochezia, weight loss, anemia, fever, or poor growth. As outlined earlier, malignancy should always be considered in the differential diagnosis of arthritis. Infiltration of the bone or synovium can mimic polyarthritis, although in most instances this is periarticular. ALL can cause polyarthritis as a result of leukemic infiltration into the synovium. In addition to constitutional symptoms, laboratory evaluation may show moderate to severe anemia or an elevation of the ESR, with a normal or low platelet count; a low WBC count; or high lactate dehydrogenase or uric acid levels. Serum sickness is an important consideration in the differential diagnosis of transient polyarthritis. Serum sickness is an immune complex mediated disease that is most commonly seen after a drug exposure (eg, cefaclor, penicillin, NSAIDs, thiazide diuretics, phenytoin). This disease is characterized by onset 7 to 14 days after exposure to an antigen, with the presenting symptoms of fever, arthralgia (two-thirds of patients), true arthritis (minority), myalgia, lymphadenopathy, and pruritic rash. The affected joints are characteristically quite tender to palpation and movement, with predominance of periarticular swelling, making it challenging to differentiate from true arthritis. The findings on CBC are nonspecific and may include neutropenia, reactive lymphocytes, mild thrombocytopenia, and eosinophilia. The ESR and CRP levels are frequently elevated, and hypoalbuminemia may be present in patients with edema. There may be mild proteinuria. C3, C4, and total hemolytic complement levels are often low, reflecting the consumptive process
14 MONOARTHRITIS The differential diagnosis of monoarthritis includes entities in the broad categories of infection, postinfection, inflammation, malignancy, and trauma related to a systemic illness (A carefully conducted history taking and physical examination are the initial and most important steps in narrowing the differential diagnosis and guiding the diagnostic evaluation. History Taking Important aspects to be considered in the history taking are as follows: 1. Characteristics of the pain and/or stiffness (site, number of joints, severity, frequency, duration, pattern, and association of warmth or discoloration). Morning stiffness is a characteristic feature of inflammatory arthritis. Night pain should alert the clinician to a malignancy or an osteoid osteoma 2. Review of systems focused on the presence of fever or other constitutional symptoms (eg, weight loss, anorexia, night sweats, or nocturnal pain) 3. Precipitating factors: traumas, infections (streptococcal, enteric, viral), immunizations, medication exposures, and history of sexual activity 4. Travel to Lyme disease endemic or tuberculosis (TB)-endemic areas or other risk factors for TB (born in Africa, Asia, Latin America, or Eastern Europe; exposure to a person with TB; close contact with a person with a positive TB skin test result) 5. Presence of extra-articular features (diarrhea, urethral discharge, ocular symptoms, rash) 6. Personal or family history of a bleeding diathesis or HLA-B27 associated diseases (inflammatory bowel disease [IBD], acute anterior uveitis, psoriasis, j Physical Examination Abnormalities detected on physical examination are important clues to the diagnosis of monoarthritis. A detailed general physical examination should include growth parameters and vital signs. The presence of fever should alert the clinician to the potential for more severe conditions requiring urgent treatment (eg, septic arthritis).

15 On general examination, clues to underlying diagnosis include rash (psoriasis, viral exanthema), iritis (IBD or enthesitis-related arthritis), and hepatosplenomegaly /lymphadenopathy suggestive of malignancy. The musculoskeletal examination should include a review of all joints and examination of the gait but with a focus on the affected joints. A recently developed and validated tool is the pgals (pediatric Gait, Arms, Legs, Spine), which is a simple screening examination that can be performed in a few minutes (Fig. 1).1,2 The focused examination of the affected joint should include inspection of the skin for warmth, redness, swelling, and soft tissue involvement, using the contralateral side for comparison. Importantly, the distinction whether the swelling is of articular or extra-articular (eg, bursitis) origin must be made. Palpation of the surrounding bone is important because the presence of pinpoint bony tenderness is suggestive of fracture, osteomyelitis, or malignancy. Passive and active range of motion should be observed. An exquisite pain in the joint on range of motion or a joint that is severely restricted in its range of motion suggests an etiology other than inflammatory arthritis (eg, septic joint). In the presence of a significant trauma history, stress maneuvers for ligamentous instability should also be performed
16 Preliminary investigations that are to be considered for the evaluation of monoarthritis are presented in Box. Laboratory investigations of acute or chronic monoarthritis are performed to confirm the clinician s impression regarding the suspected diagnosis or to exclude conditions. A diagnosis of JIA is made based on history taking and physical examination and after exclusion of other causes. Laboratory Investigations Complete blood cell count (CBC) and differential white blood cell (WBC) count, inflammatory markers, and liver and renal functions should be considered in any child with monoarthritis. If the presentation is acute (<72 hours), a joint aspiration must be performed if the clinician is concerned about a septic joint, with the fluid sent for blood cell count, Gram stain, and culture. In addition, culture of the throat, blood, stool, and/or urine should be considered to identify a potential organism in the case of reactive arthritis. An acute presentation is also observed with hematologic and malignant diseases (eg, hemophilia and leukemia), highlighting the importance of CBC and coagulation studies. Antistreptolysin-O (ASO) and anti deoxyribonuclease B (anti DNase B) titers are useful to identify a recent streptococcal infection. In chronic monoarthritis, Lyme serology (when history is suggestive of an exposure) and antinuclear antibody (ANA) and rheumatoid factor (RF) titers should be considered. HLA-B27 testing is most relevant in chronic arthritis when the child is suspected of having a specific category of JIA (enthesitis-related arthritis), which is generally seen in boys older than 8 years and often associated with enthesitis, lumbosacral back pain, and a family history of HLA-B27 associated diseases (eg, IBD, ankylosing spondylitis). The presence of ANA or RF is neither necessary nor sufficient to make a diagnosis of JIA.3 ANA should not be used as a screening test for rheumatic illness in a primary care setting, because it may be positive in up to 15% of healthy children. ANA is used as a diagnostic test for children with probable systemic lupus erythematosus (SLE) ormixed connective tissue disease (MCTD) and other overlap-like illnesses.
17 In the context of JIA, a positive ANA titer is associated with a significantly increased risk of developing chronic anterior uveitis.4,5 RF has been associated with aging (>60 years), infections (bacterial endocarditis, hepatitis B or C, parasitic disease, viral infection), pulmonary disease (sarcoidosis, interstitial pulmonary fibrosis), malignancy, and primary biliary cirrhosis6 and thus is not a specific test for the diagnosis of rheumatic disease. Only 5% to 10% of patients with JIA have a positive RF, highlighting the lack of sensitivity for the diagnosis of JIA.7 A joint aspiration must be performed when a septic joint (bacterial) is suspected butis also recommended for the diagnosis of TB arthritis. The presence of hemarthrosis suggests coagulation disorder, trauma, or rare causes, including synovial hemangioma or pigmented villonodular synovitis.the more common and/or serious causes of monoarthritis are addressed in the following sections. Septic arthritis Septic arthritis is a medical emergency that requires prompt antibiotic therapy and orthopedic intervention (drainage and irrigation). This condition is estimated to account for 6.5% of all childhood arthritides.8 Septic arthritis results from direct puncture injury to a joint, hematogenous spread, or spread from a contiguous infection (eg, osteomyelitis or cellulitis). In children and adolescents, the most common causative agents are Staphylococcus aureus, group A streptococci (GAS), and Streptococcus pneumoniae.9,10 In children younger than 2 years, Haemophilus influenzae type B had been the most common pathogen identified, but vaccination of infants for H influenza has significantly decreased the frequency of infection with this organism.11 Other important agents are Salmonella in patients with sickle cell disease and Neisseria gonorrhoeae in sexually active adolescents. Kingella kingae has emerged as an important pathogen, particularly in children younger than 4 years.12,13 This organism grows better in aerobic conditions; hence synovial fluid and bone aspirates from patients should be inoculated in an aerobic blood culture system in addition to the traditional solid culture media.13,14 K kingae is difficult to isolate on routinely used solid culture media, which is why it is proposed that this organism may account for a significant portion of culture-negative cases of septic arthritis. Mycobacterium tuberculosis is an unusual causative agent of septic monoarthritis but must be considered in an atrisk individual.as
18 outlined earlier, the presence of fever, localized erythema, warmth, and significant pain on passive range of motion are highly suggestive of a septic joint. Children (particularly neonates) can present with pseudoparalysis of the affected limb. Investigations usually demonstrate an elevated WBC count (predominance of neutrophils) and inflammatory marker levels (erythrocyte sedimentation rate [ESR], C-reactive protein [CRP]). However, an urgent joint aspiration and a synovial fluid analysis with blood cell count and Gram stain is essential for the diagnosis. The causative agent is recovered in 50% to 70% of cases (blood or synovial fluid). Initial radiologic examination is not diagnostic and may demonstrate only soft tissue and capsular swelling. The characteristic findings of osteopenia and joint space loss may not be present until 10 days into the illness. Despite prompt recognition with appropriate surgical and antibiotic management, permanent damage is common. A septic hip joint is particularly vulnerable to early damage, with chronic debilitatingchanges seen within 24 to 48 hours if aspiration and treatment are delayed. Such a delay may result in avascular necrosis related to increased intra-articular pressure that compromises the blood vessels that supply the cartilage and femoral head. Reactive arthritis The term reactive arthritis refers to arthritis that develops during or after an infection elsewhere in the body but in which the microorganisms cannot be recovered from the joint. The classic organisms causing reactive arthritis are enteric (Campylobacter,Yersinia, Salmonella, Shigella) and genitourinary organisms (Chlamydia trachomatis). The triad of conjunctivitis, urethritis, and arthritis, formerly known as Reiter syndrome, may be seen after one of these infections. More recently, reactive arthritis has also been reported after infection with Mycoplasma pneumoniae15 and Chlamydia pneumoniae.16 Although the precise role of HLA-B27 in the development of arthritis isnot fully elucidated, there is a higher frequency of HLA-B27 positivity in patients who develop reactive arthritis after infection with one of these organisms.11 The generally short-lived arthritis may be monoarticular or polyarticular, involving the larger joints of the lower extremities; can be quite painful; and usually responds well to nonsteroidal antiinflammatory drugs (NSAIDs). In addition, acute rheumatic fever (ARF) and poststreptococcal reactive arthritis (PSRA) are postinfectious arthritidesand are discussed in the differential diagnosis of polyarthritis.
19 Hip monoarthritistransient synovitis of the hip Transient (toxic) synovitis (TS) of the hip presents as a painless limp or a painful hip or knee (referred pain) typically affecting boys younger than 4 years (occasionally up to 8 years). The cause of TS is unknown but it has been postulated to be related to previous infection, most commonly involving the upper respiratory tract. In a large incidence study of family practice visits for nontraumatic hip pain in children, which determined an incidence rate of per 100,000 person-years, TS had the highest incidence rate of all diagnoses considered (76.2 per 100,000 personyears). 17 On inspection, the child is generally well appearing (afebrile or only mildly elevated temperature) and can ambulate but may do so with a limp. The affected leg is often held in a position of external rotation and flexion. A few attempts have been made to develop redictors to differentiate septic arthritis from TS. A non weight bearing status, a history of fever, an ESR greater than 40 mm/h, and a WBC count greater than 12,000 cells/mm is highly predictive of septic arthritis.18,19 A radiograph of the affected area should be sought to rule out other pathologic conditions (eg, osteoid osteoma, fracture). Because the diagnosis of TSis one of exclusion, in the case of a child who looks well, with no fever and normal WBC count and ESR, conservative management with close follow-up (1 2 days) is sensible. If there is any concern for an infection being the cause of hip pain and limp (fever, abnormal ESR or WBC count, localized tenderness), an ultrasonography is recommended to document evidence of an effusion followed by a diagnostic aspiration (if an effusion is present).20with conservative use of NSAIDs and bed rest, this self-limited process tends to resolve in 3 to 10 days. It has been suggested that patients with TS should have a repeat radiography within 6 months to exclude Legg-Calve -Perthes (LCP) disease, which is estimated to be a complication of TS in 1% to 3% of cases. The recurrencerate is 4% to 17%, occurring mostly within 6 months. There has been no identified increased risk of developing JIA after a diagnosis of TS. When the presentation is one of monoarticular pain involving the hip, additional important considerations are slipped capital femoral epiphysis (SCFE) and LCP disease. Both these conditions are noninflammatory and not typically associated with arthritis. SCFE SCFE classically occurs in overweight boys aged 10 to 14 years or in children with endocrine disorders, such as hypothyroidism or pituitary
20 deficiencies (eg, growth hormone deficiency). SCFE is diagnosed radiographically. Both hips should be imaged because SCFE is bilateral in 30% of cases in which the presenting symptoms are unilateral. On diagnosis, an urgent referral should be made to orthopedics; in the meantime, the child should be non weight bearing and on bed rest and prescribed crutches. LCP syndrome LCP syndrome, an idiopathic avascular necrosis of the capital femoral epiphysis, typically affects boys aged between 4 and 10 years. A high index of suspicion is needed to make the diagnosis because initial radiographs are ften normal. At this early stage, magnetic resonance imaging (MRI) is most sensitive for the diagnosis, showing changes in the bone marrow related to hypoperfusion. Subsequently, radiographs show fragmentation and then healing of the femoral head, often with residualdeformity. Patients with LCP should be made non weight bearing, with an urgent referral to orthopedics. Treatment focuses on maintaining containment of the femoral head within the acetabulum with the use of abduction splints or, occasionally, surgically with an osteotomy of the proximal femur. Lyme disease Lyme arthritis is most commonly recognized in the Northeastern, Mid- Atlantic, and North-Central United States and less commonly in the West Coast and Southern Canada, attributable to the distribution of the whitetailed deer.21 This tick-borne illness is primarily caused by 3 species of the spirochete Borrelia burgdorferi. The clinical manifestations of Lyme disease vary but early disease manifestations include a flulike illness, rash (erythema migrans), lymphocytic meningitis, cranial nerve VII palsy, arthralgia, and rarely carditis. Arthritis is a late manifestation occurring months to years after the original infection. Often, the child is asymptomatic and may not recall having been bitten by a tick. This underscores the importance of eliciting a history of travel or residence in a Lyme-endemic area. The most frequently involved joint is the knee (intwo-thirds of cases), but any large joint may be affected,22 and more than one jointmay be involved at presentation. The arthritis may be painless and pisodic; however,chronic arthritis has been described in up to 18% of patients.23 The diagnosis is based on suggestive clinical characteristics in addition to confirmatorylaboratory tests. Indirect methods to detect infection are preferred over directdetection methods (cultures, stains, or polymerase chain reactions) because the latterhave higher rates of false-negative results and it often takes a prolonged period beforethe results are known. Of the indirect
21 methods, the enzyme immunoassay (enzymelinkedimmunosorbent assay) has high sensitivity and low pecificity and thus isused as a targeted screening test. In the case of a positive result, Western blot isthe confirmatory test with high specificity.11 Malignancy A malignancy must always be considered at the top of the differential diagnosis, evenif it can be immediately discounted. Clues that suggest a malignancy as the cause forarthritis include the following: pain out of keeping with the degree of arthritis, the child being irritable and difficult to examine, fever, lymphadenopathy or hepatosplenomegaly,leukocyte or platelet count that are lower than expected, bone pain, and metaphyseallucencies seen on the radiograph (Fig. 2).24 Joint involvement in malignancy tends to be oligoarticular (_4 joints) rather than polyarticular.25one study looking at the factors differentiating acute leukemia from chronic arthritisfound that the presence of a low WBC count (<4 _ 109/L), low-normal platelet count( _ 109/L), and history of nighttime pain was 100% specific and 85% sensitivefor the diagnosis of acute lymphoblastic leukemia (ALL).26 Moreover, when pain is thechief complaint of the patient, this may have a strong negative predictive value for thediagnosis of JIA. Isolated musculoskeletal pain, in the absence of other signs or symptoms,is almost never a presenting complaint in children with JIA, and, instead, children(with JIA) more commonly complain of joint swelling and/or gait disturbance.27jia Chronic arthritis is the most common rheumatic disease in children, affecting about in 1000 children worldwide.28 JIA is an umbrella term describing a group of rthritides of unknown etiology lasting more than 6 weeks in children younger than 16 ears.29 JIA is an important consideration in chronic monoarthritis because it is a significant cause of short-term and long-term disability. In addition, there is mounting evidence that early disease identification and treatment may lead to improved quality of life. The most frequently affected joints are the knee, ankle, wrist, and elbow. Chronic monoarthritis can be the presenting manifestation of oligoarthritis, enthesitis-related arthritis, and psoriatic arthritis. JIA rarely presents as monoarthritis involving the hip or shoulder. Consequently, there is a low threshold for further imaging (MRI) once an infectious cause has been ruled out. Up to 20% of children with JIA (oligoarthritis) may develop chronic anterior uveitis. Therefore, a slit lamp examination should be considered for a child with suspected JIA because detection of uveitis would support this diagnosis.
22 Other Important Diagnostic Considerations Hemophilia may cause recurrent monoarthritis. Chronic joint pain and damage is one of the most important causes of morbidity in this X-linked recessive coagulopathy. Hemorrhage into the soft tissues, particularly intramuscularly, may mimic hemarthrosis. Fig. The most commonly affected joints are the knees, elbows, and ankles. The classic presentation of hemarthrosis is one of acute onset of increasing fullness in a joint, with loss of range of motion.onexamination, the joint is warmand distended. Recurrent hemarthrosis can lead to bone and joint damage and early osteoarthritis, causing a significant effect on the patients quality of life. A rarer cause of hemarthrosis is pigmented villonodular synovitis, whichmayrepresent a benign neoplasm of the synovium. An acute or a chronic monoarthritis may easily be confused with extra-articular joint swelling, particularly around the knee joint. Bursitis is another important consideration in the approach to monoarthritis. A bursa is a synovial-lined sac designed to reduce friction between moving structures (eg, tendons rubbing against bones, ligaments, or other tendons). A bursa may communicate with the joint (eg, suprapatellar and popliteal); however, other bursae around the knee do not necessarily do so (eg, infrapatellar and medial collateral ligament). Bursitis typically presents with maximal tenderness at the site of the bursa and localized swelling. In the case of communication with the knee joint, a small joint effusion may also be observed. Although the prevalence of bursitis in childhood is low, it may be higher in athletes30 and patients with JIA.31 When bursitis is suspected, an MRI is the preferred imaging modality to confirm the diagnosis. It is important to distinguish between monoarthritis and bursitis because the treatment differs; bursitis may not respond to an intra-articular corticosteroid injection and may require a direct injection into the affected bursa.
2/23/18. Disclosures. Rheumatic Diseases of Childhood. Making Room for Rheumatology. I have nothing to disclose. James J.
 Making Room for Rheumatology James J. Nocton, MD Disclosures I have nothing to disclose Rheumatic Diseases of Childhood Juvenile Idiopathic Arthritis (JIA) Systemic Lupus Erythematosus (SLE) Juvenile Dermatomyositis
Making Room for Rheumatology James J. Nocton, MD Disclosures I have nothing to disclose Rheumatic Diseases of Childhood Juvenile Idiopathic Arthritis (JIA) Systemic Lupus Erythematosus (SLE) Juvenile Dermatomyositis
SEPTIC ARTHRITIS. Dr Ahmed Husam Al Ahmed Rheumatologist SYRIA. University of Science and technology Hospital Sanaa Yemen 18/Dec/2014
 SEPTIC ARTHRITIS Dr Ahmed Husam Al Ahmed Rheumatologist SYRIA University of Science and technology Hospital Sanaa Yemen 18/Dec/2014 Objectives be able to define Septic Arthritis know what factors predispose
SEPTIC ARTHRITIS Dr Ahmed Husam Al Ahmed Rheumatologist SYRIA University of Science and technology Hospital Sanaa Yemen 18/Dec/2014 Objectives be able to define Septic Arthritis know what factors predispose
Types of osteoarthritis
 ARTHRITIS Osteoarthritis is a degenerative joint disease is the most common joint disorder. It is a frequent part of aging and is an important cause of physical disability in persons older than 65 years
ARTHRITIS Osteoarthritis is a degenerative joint disease is the most common joint disorder. It is a frequent part of aging and is an important cause of physical disability in persons older than 65 years
Physical examination of the musculosceletal- and nervous system. Pánczél Pál dr.
 Physical examination of the musculosceletal- and nervous system in the practice of internal medicine. Pánczél Pál dr. Bursae = sacks of the synovial membrane fulfilled with synovium. Localised between
Physical examination of the musculosceletal- and nervous system in the practice of internal medicine. Pánczél Pál dr. Bursae = sacks of the synovial membrane fulfilled with synovium. Localised between
Rheumatology 101 A Pediatrician s Guide
 Rheumatology 101 A Pediatrician s Guide Pediatric Staff and Alumni Day 2016 Dawn M. Wahezi, Yonit Sterba, Tamar Rubinstein Disclosures None Pick a Group Group 1 A child with a limp Group 2 ANA To test
Rheumatology 101 A Pediatrician s Guide Pediatric Staff and Alumni Day 2016 Dawn M. Wahezi, Yonit Sterba, Tamar Rubinstein Disclosures None Pick a Group Group 1 A child with a limp Group 2 ANA To test
PGALS: Approach to Child with Arthritis. Prof Chris Scott Paediatric Rheumatology
 PGALS: Approach to Child with Arthritis Prof Chris Scott Paediatric Rheumatology Introduction In a prospective study from The Royal Hospital for Sick Children, Edinburgh, every 58th child presented with
PGALS: Approach to Child with Arthritis Prof Chris Scott Paediatric Rheumatology Introduction In a prospective study from The Royal Hospital for Sick Children, Edinburgh, every 58th child presented with
Juvenile Idiopathic Arthritis (JIA)
") Juvenile Idiopathic Arthritis (JIA) Kaveh Ardalan, MD, MS Division of Rheumatology Ann & Robert H. Lurie Children s Hospital of Chicago Assistant Professor, Pediatrics and Medical Social Sciences Northwestern
Juvenile Idiopathic Arthritis (JIA) Kaveh Ardalan, MD, MS Division of Rheumatology Ann & Robert H. Lurie Children s Hospital of Chicago Assistant Professor, Pediatrics and Medical Social Sciences Northwestern
JuvenileIdiopathicArthritis. Dr Johan Siebert
 JuvenileIdiopathicArthritis Dr Johan Siebert 1 NORMAL DIARTHRODIAL JOINT Synovial is a thin membrane enclosing the joint space The joint space contains fluid that bathes the joint and reduces friction
JuvenileIdiopathicArthritis Dr Johan Siebert 1 NORMAL DIARTHRODIAL JOINT Synovial is a thin membrane enclosing the joint space The joint space contains fluid that bathes the joint and reduces friction
How do polyarthritis, polyarthralgias, and diffuse aches and pains differ?
 Approach to the patient with polyarthritis How do polyarthritis, polyarthralgias, and diffuse aches and pains differ? Polyarthritis is definite inflammation (swelling, tenderness, warmth) of more than
Approach to the patient with polyarthritis How do polyarthritis, polyarthralgias, and diffuse aches and pains differ? Polyarthritis is definite inflammation (swelling, tenderness, warmth) of more than
Non-inflammatory joint pain
 Non-inflammatory joint pain Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. INTRODUCTION Musculoskeletal
Non-inflammatory joint pain Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. INTRODUCTION Musculoskeletal
Department of Paediatrics Clinical Guideline. Guideline for the child with possible arthritis (joint swelling/pain, loss of function)
") Department of Paediatrics Clinical Guideline Guideline for the child with possible arthritis (joint swelling/pain, loss of function) Definition: Juvenile Idiopathic Arthritis (JIA) is defined as arthritis
Department of Paediatrics Clinical Guideline Guideline for the child with possible arthritis (joint swelling/pain, loss of function) Definition: Juvenile Idiopathic Arthritis (JIA) is defined as arthritis
Etiology: Pathogenesis Clinical manifestation Investigation Treatment Prognosis
 Etiology: Pathogenesis Clinical manifestation Investigation Treatment Prognosis JIA is the most common rheumatic disease in childhood and a major cause of chronic disability. Etiology: Unknown, but may
Etiology: Pathogenesis Clinical manifestation Investigation Treatment Prognosis JIA is the most common rheumatic disease in childhood and a major cause of chronic disability. Etiology: Unknown, but may
Department of Paediatrics Clinical Guideline
 Department of Paediatrics Clinical Guideline The child and young person with possible arthritis (joint swelling and/or pain, loss of function for >4 weeks) Definition: Juvenile Idiopathic Arthritis (JIA)
Department of Paediatrics Clinical Guideline The child and young person with possible arthritis (joint swelling and/or pain, loss of function for >4 weeks) Definition: Juvenile Idiopathic Arthritis (JIA)
Patient #1. Rheumatoid Arthritis. Rheumatoid Arthritis. 45 y/o female Morning stiffness in her joints >1 hour
 Patient #1 Rheumatoid Arthritis Essentials For The Family Medicine Physician 45 y/o female Morning stiffness in her joints >1 hour Hands, Wrists, Knees, Ankles, Feet Polyarticular, symmetrical swelling
Patient #1 Rheumatoid Arthritis Essentials For The Family Medicine Physician 45 y/o female Morning stiffness in her joints >1 hour Hands, Wrists, Knees, Ankles, Feet Polyarticular, symmetrical swelling
Juvenile Chronic Arthritis
 Juvenile Chronic Arthritis Dr. Christa Visser MBChB MMed (Med Phys) Diploma Musculoskeletal Medicine (UK), Member Society of Orthopaedic Medicine (UK) Childhood Arthritis JCA/JIA/JRA Remember Acute rheumatic
Juvenile Chronic Arthritis Dr. Christa Visser MBChB MMed (Med Phys) Diploma Musculoskeletal Medicine (UK), Member Society of Orthopaedic Medicine (UK) Childhood Arthritis JCA/JIA/JRA Remember Acute rheumatic
Objectives. Joint Pain. Case 1. Rheumatology for the Primary MD (Not just your grandmother s disease) 12/4/2010
 12/4/2010") Objectives Rheumatology for the Primary MD (Not just your grandmother s disease) Identify when it is appropriate to refer for rheumatologic evaluation Autoimmune/ Inflammatory v. noninflammatory disease
Objectives Rheumatology for the Primary MD (Not just your grandmother s disease) Identify when it is appropriate to refer for rheumatologic evaluation Autoimmune/ Inflammatory v. noninflammatory disease
APPROACH TO PATIENTS WITH POLYARTHRALGIA
 APPROACH TO PATIENTS WITH POLYARTHRALGIA Scott Vogelgesang, MD Division of Immunology University of Iowa No conflicts of interest DEFINITIONS Arthralgia joint pain with no evidence of inflammation Arthritis
APPROACH TO PATIENTS WITH POLYARTHRALGIA Scott Vogelgesang, MD Division of Immunology University of Iowa No conflicts of interest DEFINITIONS Arthralgia joint pain with no evidence of inflammation Arthritis
 www.fisiokinesiterapia.biz Peak onset between 20 and 30 years Form of spondyloarthritis (cause inflammation around site of ligament insertion into bone) and association with HLA-B27 Prevalence as high
www.fisiokinesiterapia.biz Peak onset between 20 and 30 years Form of spondyloarthritis (cause inflammation around site of ligament insertion into bone) and association with HLA-B27 Prevalence as high
RHEUMATOLOGY OVERVIEW. Carmelita J. Colbert, MD Assistant Professor of Medicine Division of Rheumatology Loyola University Medical Center
 RHEUMATOLOGY OVERVIEW Carmelita J. Colbert, MD Assistant Professor of Medicine Division of Rheumatology Loyola University Medical Center What is Rheumatology? Medical science devoted to the rheumatic diseases
RHEUMATOLOGY OVERVIEW Carmelita J. Colbert, MD Assistant Professor of Medicine Division of Rheumatology Loyola University Medical Center What is Rheumatology? Medical science devoted to the rheumatic diseases
Jeopardy. What s the rash? $100 $100 $100 $100 $100 $200 $200 $200 $200 $200 $300 $300 $300 $300 $300 $400 $400 $400 $400 $400
 Jeopardy Antibodies & more antibodies Aching joints What s the rash? Potpourri Image Challenge $100 $100 $100 $100 $100 $200 $200 $200 $200 $200 $300 $300 $300 $300 $300 $400 $400 $400 $400 $400 $500 $500
Jeopardy Antibodies & more antibodies Aching joints What s the rash? Potpourri Image Challenge $100 $100 $100 $100 $100 $200 $200 $200 $200 $200 $300 $300 $300 $300 $300 $400 $400 $400 $400 $400 $500 $500
Assessment of limping child (beware the child who does not weight bear at all):
:") Department of Paediatrics Clinical Guideline Acutely Limping Child and Septic Arthritis Assessment of limping child (beware the child who does not weight bear at all): History Careful history of any significant
Department of Paediatrics Clinical Guideline Acutely Limping Child and Septic Arthritis Assessment of limping child (beware the child who does not weight bear at all): History Careful history of any significant
A free online interactive information resource for clinicians.
 A free online interactive information resource for clinicians www.pmmonline.org The limping child Helen Foster Professor of Paediatric Rheumatology Newcastle University Honorary Consultant Great North
A free online interactive information resource for clinicians www.pmmonline.org The limping child Helen Foster Professor of Paediatric Rheumatology Newcastle University Honorary Consultant Great North
Musculoskeletal Referral Guidelines
 Musculoskeletal Referral Guidelines Introduction These guidelines have been developed to provide an integrated musculoskeletal service. They are based on reasonable clinical practice and will initially
Musculoskeletal Referral Guidelines Introduction These guidelines have been developed to provide an integrated musculoskeletal service. They are based on reasonable clinical practice and will initially
Joint Injuries and Disorders
 Joint Injuries and Disorders Introduction A joint is where two or more bones come together. Your joints include the knees, hips, elbows and shoulders. There are many types of joint disorders, including
Joint Injuries and Disorders Introduction A joint is where two or more bones come together. Your joints include the knees, hips, elbows and shoulders. There are many types of joint disorders, including
Juvenile Spondyloarthritis / Enthesitis Related Arthritis (SpA-ERA)
") www.printo.it/pediatric-rheumatology/gb/intro Juvenile Spondyloarthritis / Enthesitis Related Arthritis (SpA-ERA) Version of 2016 1. WHAT IS JUVENILE SPONDYLOARTHRITIS/ENTHESITIS- RELATED ARTHRITIS (SpA-ERA)
www.printo.it/pediatric-rheumatology/gb/intro Juvenile Spondyloarthritis / Enthesitis Related Arthritis (SpA-ERA) Version of 2016 1. WHAT IS JUVENILE SPONDYLOARTHRITIS/ENTHESITIS- RELATED ARTHRITIS (SpA-ERA)
The Limping Child: Differential Diagnosis
 The Limping Child: Differential Diagnosis Kathryn A Keeler, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics
The Limping Child: Differential Diagnosis Kathryn A Keeler, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics
Musculoskeletal Infection and Inflammation
 F.A. Davis: Advantage Musculoskeletal Infection and Inflammation(10.6.15) Page 1 Musculoskeletal Infection and Inflammation The musculoskeletal system is affected by infections and inflammatory conditions.
F.A. Davis: Advantage Musculoskeletal Infection and Inflammation(10.6.15) Page 1 Musculoskeletal Infection and Inflammation The musculoskeletal system is affected by infections and inflammatory conditions.
8/29/2012. Outline Juvenile idiopathic arthritis. 1. Classification-ILAR. 1. Classification-clinical diagnosis. 1. JIA classification
 Outline Juvenile idiopathic arthritis 1. Classification and symptoms (ILAR-International league of Associations for Rheumatology) 2. Imaging J. Herman Kan, M.D. Section chief, musculoskeletal imaging Edward
Outline Juvenile idiopathic arthritis 1. Classification and symptoms (ILAR-International league of Associations for Rheumatology) 2. Imaging J. Herman Kan, M.D. Section chief, musculoskeletal imaging Edward
A Patient s Guide to Transient Synovitis of the Hip in Children
 A Patient s Guide to Transient Synovitis of the Hip in Children 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet
A Patient s Guide to Transient Synovitis of the Hip in Children 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet
Disclosures. Rheumatological Approaches to Differential Diagnosis, Physical Examination, and Interpretation of Studies. None
 Rheumatological Approaches to Differential Diagnosis, Physical Examination, and Interpretation of Studies Sarah Goglin MD Assistant Professor of Medicine Division of Rheumatology Disclosures None 1 [footer
Rheumatological Approaches to Differential Diagnosis, Physical Examination, and Interpretation of Studies Sarah Goglin MD Assistant Professor of Medicine Division of Rheumatology Disclosures None 1 [footer
Is it Autoimmune or NOT! Presented to AONP! October 2015!
 Is it Autoimmune or NOT! Presented to AONP! October 2015! Four main jobs of immune system Detects Contains and eliminates Self regulates Protects Innate Immune System! Epithelial cells, phagocytic cells
Is it Autoimmune or NOT! Presented to AONP! October 2015! Four main jobs of immune system Detects Contains and eliminates Self regulates Protects Innate Immune System! Epithelial cells, phagocytic cells
Familial Mediterranean Fever
 www.printo.it/pediatric-rheumatology/gb/intro Familial Mediterranean Fever Version of 2016 1. WHAT IS FMF 1.1 What is it? Familial Mediterranean Fever (FMF) is a genetically transmitted disease. Patients
www.printo.it/pediatric-rheumatology/gb/intro Familial Mediterranean Fever Version of 2016 1. WHAT IS FMF 1.1 What is it? Familial Mediterranean Fever (FMF) is a genetically transmitted disease. Patients
A Tailored Approach to Uveitis and Associated Systemic Conditions Anthony DeWilde O.D.
 A Tailored Approach to Uveitis and Associated Systemic Conditions Anthony DeWilde O.D. I. Introduction II. III. IV. A. Why I am giving this talk B. What to take from lecture Diagnosis 1. Better understanding
A Tailored Approach to Uveitis and Associated Systemic Conditions Anthony DeWilde O.D. I. Introduction II. III. IV. A. Why I am giving this talk B. What to take from lecture Diagnosis 1. Better understanding
The Child with a Limp
 The Child with a Limp DR S Rajapaksa RCH CHIld with a limp Case: An 11 year old presents to ED with a 4 days history of a painful limp. He had been playing footie over the weekend and had fallen but then
The Child with a Limp DR S Rajapaksa RCH CHIld with a limp Case: An 11 year old presents to ED with a 4 days history of a painful limp. He had been playing footie over the weekend and had fallen but then
Diagnostic Dilemmas Between Viral and Bacterial Tonsillitis
 Diagnostic Dilemmas Between Viral and Bacterial Tonsillitis Round Table Moderator: Panelists: Edigar R. de Almeida Luiza Endo, Maria Helena Kiss, Renata di Francesco and Sílvio Luiz Zuquim Edigar R. de
Diagnostic Dilemmas Between Viral and Bacterial Tonsillitis Round Table Moderator: Panelists: Edigar R. de Almeida Luiza Endo, Maria Helena Kiss, Renata di Francesco and Sílvio Luiz Zuquim Edigar R. de
What organ system is involved? What is the pathology? What is the possible etiology?
 Johan van Rensburg What organ system is involved? What is the pathology? What is the possible etiology? Genetic Environmental What are the possible complications? How is the patient s functioning impaired?
Johan van Rensburg What organ system is involved? What is the pathology? What is the possible etiology? Genetic Environmental What are the possible complications? How is the patient s functioning impaired?
Kelley's Textbook of Rheumatology. 2 Volume Set. Text with Internet Access Code for Premium Consult Edition
 Kelley's Textbook of Rheumatology. 2 Volume Set. Text with Internet Access Code for Premium Consult Edition Firestein, G ISBN-13: 9781437717389 Table of Contents VOLUME I STRUCTURE AND FUNCTION OF BONE,
Kelley's Textbook of Rheumatology. 2 Volume Set. Text with Internet Access Code for Premium Consult Edition Firestein, G ISBN-13: 9781437717389 Table of Contents VOLUME I STRUCTURE AND FUNCTION OF BONE,
RHEUMATIC FEVER RHF-1. Disease name. Basis of diagnosis
 RHF-1 RHEUMATIC FEVER Disease name Disease Indicate whether this is an initial (i.e first) attack of rheumatic fever or a recurrent attack (an episode in a person with known past history of acute rheumatic
RHF-1 RHEUMATIC FEVER Disease name Disease Indicate whether this is an initial (i.e first) attack of rheumatic fever or a recurrent attack (an episode in a person with known past history of acute rheumatic
Rheumatoid Arthritis. Marge Beckman FALU, FLMI Vice President RGA Underwriting Quarterly Underwriting Meeting March 24, 2011
 Rheumatoid Arthritis Marge Beckman FALU, FLMI Vice President RGA Underwriting Quarterly Underwriting Meeting March 24, 2011 The security of experience. The power of innovation. www.rgare.com Case Study
Rheumatoid Arthritis Marge Beckman FALU, FLMI Vice President RGA Underwriting Quarterly Underwriting Meeting March 24, 2011 The security of experience. The power of innovation. www.rgare.com Case Study
Pediatric Orthopedic Pathology Pathology 2 Dr. Gary Mumaugh
 Pediatric Orthopedic Pathology Pathology 2 Dr. Gary Mumaugh Congenital Defects - Clubfoot (congenital equinovarus) Forefoot is adducted and supinated o Positional equinovarus o Idiopathic congenital equinovarus
Pediatric Orthopedic Pathology Pathology 2 Dr. Gary Mumaugh Congenital Defects - Clubfoot (congenital equinovarus) Forefoot is adducted and supinated o Positional equinovarus o Idiopathic congenital equinovarus
Rheumatic Fever And Post-streptococcal Reactive Arthritis
 www.printo.it/pediatric-rheumatology/gb/intro Rheumatic Fever And Post-streptococcal Reactive Arthritis Version of 2016 1. WHAT IS RHEUMATIC FEVER 1.1 What is it? Rheumatic fever is a disease caused by
www.printo.it/pediatric-rheumatology/gb/intro Rheumatic Fever And Post-streptococcal Reactive Arthritis Version of 2016 1. WHAT IS RHEUMATIC FEVER 1.1 What is it? Rheumatic fever is a disease caused by
Disclaimer. This is a broad survey and cannot cover all differential diagnoses or each condition in thorough detail
 Objectives Pediatric Infections: Differentiating Benign from Serious Eileen Klein, MD, MPH Rashes Infectious vs non-infectious Viral vs bacterial Respiratory and GI illnesses When do you treat When do
Objectives Pediatric Infections: Differentiating Benign from Serious Eileen Klein, MD, MPH Rashes Infectious vs non-infectious Viral vs bacterial Respiratory and GI illnesses When do you treat When do
Acute Osteomyelitis: similar to septic arthritis but up to 40% may be afebrile swelling overlying the bone & tenderness
 Osteomyelitis / Bone and Joint Infections Bone infections in children are usually from haematogenous bacterial seeding to a single joint, usually the lower limbs, but may be multifocal. Approximately 10%
Osteomyelitis / Bone and Joint Infections Bone infections in children are usually from haematogenous bacterial seeding to a single joint, usually the lower limbs, but may be multifocal. Approximately 10%
Essential Rheumatology. Dr Ellen Bruce Consultant Rheumatologist CMFT
 Essential Rheumatology Dr Ellen Bruce Consultant Rheumatologist CMFT Saving the best for last! Apparently people recall best the first and last thing they re told. Far too difficult to include everything.
Essential Rheumatology Dr Ellen Bruce Consultant Rheumatologist CMFT Saving the best for last! Apparently people recall best the first and last thing they re told. Far too difficult to include everything.
The Child With a Limp
 KID WITH A LIMP Common in ED, common in Exams Differential diagnosis is very wide Most causes benign, but mustn't miss Septic arthritis Osteomyelitis Fractures / NAI SUFE (older, heavier children) The
KID WITH A LIMP Common in ED, common in Exams Differential diagnosis is very wide Most causes benign, but mustn't miss Septic arthritis Osteomyelitis Fractures / NAI SUFE (older, heavier children) The
Guideline on the clinical management of Henoch Schonlein Purpura (HSP)
") Guideline on the clinical management of Henoch Schonlein Purpura (HSP) Purpose To ensure a standardised approach in the management of children with HSP in southern Derbyshire. Scope The scope of this guideline
Guideline on the clinical management of Henoch Schonlein Purpura (HSP) Purpose To ensure a standardised approach in the management of children with HSP in southern Derbyshire. Scope The scope of this guideline
Dr. K. Brindha, M.D PG ESI PGIMSR, K.K Nagar, Chennai
 Dr. K. Brindha, M.D PG ESI PGIMSR, K.K Nagar, Chennai Case History 9 year old boy presented with a 3 week history of: Swelling of major lower limb joints Progression was additive (right ankle followed
Dr. K. Brindha, M.D PG ESI PGIMSR, K.K Nagar, Chennai Case History 9 year old boy presented with a 3 week history of: Swelling of major lower limb joints Progression was additive (right ankle followed
Acute rheumatic fever (ARF) Simple complement
 Simple complement") Acute rheumatic fever (ARF) Simple complement 1. The onset of acute rheumatic fever achieves the peak between the following ages: A. 3-7 years B. 5-15 years C. 13-17 years D. 2-10 years E. 10-18 years
Acute rheumatic fever (ARF) Simple complement 1. The onset of acute rheumatic fever achieves the peak between the following ages: A. 3-7 years B. 5-15 years C. 13-17 years D. 2-10 years E. 10-18 years
Rheumatoid Arthritis. Manish Relan, MD FACP RhMSUS Arthritis & Rheumatology Care Center. Jacksonville, FL (904)
") Rheumatoid Arthritis Manish Relan, MD FACP RhMSUS Arthritis & Rheumatology Care Center. Jacksonville, FL (904) 503-6999. 1 Disclosures Speaker Bureau: Abbvie 2 Objectives Better understand the pathophysiology
Rheumatoid Arthritis Manish Relan, MD FACP RhMSUS Arthritis & Rheumatology Care Center. Jacksonville, FL (904) 503-6999. 1 Disclosures Speaker Bureau: Abbvie 2 Objectives Better understand the pathophysiology
Test Name Results Units Bio. Ref. Interval
 135091662 Age 45 Years Gender Male 29/8/2017 120000AM 29/8/2017 100215AM 29/8/2017 110825AM Ref By Final RHEUMATOID AUTOIMMUNE COMREHENSIVE ANEL ANTI NUCLEAR ANTIBODY / FACTOR (ANA/ANF), SERUM ----- 20-60
135091662 Age 45 Years Gender Male 29/8/2017 120000AM 29/8/2017 100215AM 29/8/2017 110825AM Ref By Final RHEUMATOID AUTOIMMUNE COMREHENSIVE ANEL ANTI NUCLEAR ANTIBODY / FACTOR (ANA/ANF), SERUM ----- 20-60
Rheumatic Fever And Post-streptococcal Reactive Arthritis
 www.printo.it/pediatric-rheumatology/gb/intro Rheumatic Fever And Post-streptococcal Reactive Arthritis Version of 2016 1. WHAT IS RHEUMATIC FEVER 1.1 What is it? Rheumatic fever is a disease caused by
www.printo.it/pediatric-rheumatology/gb/intro Rheumatic Fever And Post-streptococcal Reactive Arthritis Version of 2016 1. WHAT IS RHEUMATIC FEVER 1.1 What is it? Rheumatic fever is a disease caused by
RHEUMATIC FEVER AND POST-STREPTOCOCCAL REACTIVE ARTHRITIS
 www.pediatric-rheumathology.printo.it RHEUMATIC FEVER AND POST-STREPTOCOCCAL REACTIVE ARTHRITIS What is it? Rheumatic fever has been defined as a disease triggered by infection caused by streptococcus.
www.pediatric-rheumathology.printo.it RHEUMATIC FEVER AND POST-STREPTOCOCCAL REACTIVE ARTHRITIS What is it? Rheumatic fever has been defined as a disease triggered by infection caused by streptococcus.
HEMORRHAGIC BULLOUS HENOCH- SCHONLEIN PURPURA: A CASE REPORT
 HEMORRHAGIC BULLOUS HENOCH- SCHONLEIN PURPURA: A CASE REPORT Nirmala Ponnuthurai, Sabeera Begum, Lee Bang Rom Paediatric Dermatology Unit, Institute of Paediatric, Hospital Kuala Lumpur, Malaysia Abstract
HEMORRHAGIC BULLOUS HENOCH- SCHONLEIN PURPURA: A CASE REPORT Nirmala Ponnuthurai, Sabeera Begum, Lee Bang Rom Paediatric Dermatology Unit, Institute of Paediatric, Hospital Kuala Lumpur, Malaysia Abstract
AUTOIMMUNE DISORDERS IN THE ACUTE SETTING
 AUTOIMMUNE DISORDERS IN THE ACUTE SETTING Diagnosis and Treatment Goals Aimee Borazanci, MD BNI Neuroimmunology Objectives Give an update on the causes for admission, clinical features, and outcomes of
AUTOIMMUNE DISORDERS IN THE ACUTE SETTING Diagnosis and Treatment Goals Aimee Borazanci, MD BNI Neuroimmunology Objectives Give an update on the causes for admission, clinical features, and outcomes of
Reading Test 1 Part A
 Reading Test 1 Part A Page 1 w Copy w Rights w. Reserved o e t ::: m www.oetmaterial.com a t e r i a l. c o m. a u Reading: Part A TIME LIMIT: 15 MINUTES Instructions: Complete the following summary using
Reading Test 1 Part A Page 1 w Copy w Rights w. Reserved o e t ::: m www.oetmaterial.com a t e r i a l. c o m. a u Reading: Part A TIME LIMIT: 15 MINUTES Instructions: Complete the following summary using
Patient with Musculo-skeletal Complaints - Summary
 Patient with Musculo-skeletal Complaints - Summary 1. Soft Tissue Rheumatism or Arthritis 2. Arthritis Monoarticular Polyarticular - :- (Asymmetrical) (Symetrical) :- -Crystals, Gout - Infective acute
Patient with Musculo-skeletal Complaints - Summary 1. Soft Tissue Rheumatism or Arthritis 2. Arthritis Monoarticular Polyarticular - :- (Asymmetrical) (Symetrical) :- -Crystals, Gout - Infective acute
Pyrexia of unknown origin? Think still
 Pyrexia of unknown origin? Think still Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. DISCLAIMER
Pyrexia of unknown origin? Think still Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. DISCLAIMER
Rheumatology Review Update in Internal Medicine COPYRIGHT. Robert H. Shmerling, M.D. Beth Israel Deaconess Medical Center.
 Rheumatology Review Update in Internal Medicine Robert H. Shmerling, M.D. Beth Israel Deaconess Medical Center Boston MA Case #1 True statement(s) regarding etanercept and leflunomide, for the treatment
Rheumatology Review Update in Internal Medicine Robert H. Shmerling, M.D. Beth Israel Deaconess Medical Center Boston MA Case #1 True statement(s) regarding etanercept and leflunomide, for the treatment
Rheumatology Cases for the Internist
 Rheumatology Cases for the Internist Marc C. Hochberg, MD, MPH Professor of Medicine Head, Division of Rheumatology and Clinical Immunology Vice Chair, Department of Medicine University of Maryland School
Rheumatology Cases for the Internist Marc C. Hochberg, MD, MPH Professor of Medicine Head, Division of Rheumatology and Clinical Immunology Vice Chair, Department of Medicine University of Maryland School
Types of bone/joint infections. Bone and Joint Infections. Septic Arthritis. Pathogenesis. Pathogenesis. Bacterial arthritis: predisposing factors
 Bone and Joint Infections Types of bone/joint infections Arthritis (infective/septic) Osteomyelitis Prosthetic bone and joint infections Septic Arthritis Common destructive athroplasty Mono-articular Poly-articular
Bone and Joint Infections Types of bone/joint infections Arthritis (infective/septic) Osteomyelitis Prosthetic bone and joint infections Septic Arthritis Common destructive athroplasty Mono-articular Poly-articular
Following the bite of a mosquito infected with CHIKV, most individuals will
 3. CLINICAL 3A. Clinical Presentation of Acute Disease Following the bite of a mosquito infected with CHIKV, most individuals will present with symptomatic disease after an incubation period of 3-7 days
3. CLINICAL 3A. Clinical Presentation of Acute Disease Following the bite of a mosquito infected with CHIKV, most individuals will present with symptomatic disease after an incubation period of 3-7 days
MRI Features of Lyme Arthritis in Children
 Pediatric Imaging Ecklund et al. MRI of Lyme Arthritis in Children Kirsten Ecklund 1 Sigella Vargas 1 David Zurakowski 2 Robert P. Sundel 3 Ecklund K, Vargas S, Zurakowski D, Sundel RP Received June 30,
Pediatric Imaging Ecklund et al. MRI of Lyme Arthritis in Children Kirsten Ecklund 1 Sigella Vargas 1 David Zurakowski 2 Robert P. Sundel 3 Ecklund K, Vargas S, Zurakowski D, Sundel RP Received June 30,
Etiological Profile of Arthritis in Children between 6 Months and 12 Years of Age Admitted in a Tertiary Care Hospital
 Original Article DOI: 10.17354/ijss/2016/241 Etiological Profile of Arthritis in Children between 6 Months and 12 Years of Age Admitted in a Tertiary Care Hospital D Sivakumaran 1, M Krithiga 2 1 Associate
Original Article DOI: 10.17354/ijss/2016/241 Etiological Profile of Arthritis in Children between 6 Months and 12 Years of Age Admitted in a Tertiary Care Hospital D Sivakumaran 1, M Krithiga 2 1 Associate
A Patient s Guide to Limping in Children
 A Patient s Guide to Limping in Children 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet is compiled from a variety
A Patient s Guide to Limping in Children 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet is compiled from a variety
Joint Disorders. Musculoskeletal Disorders (Part B-2) Module 7 -Chapter 10. Overview Disorders of the Muscular System Disorders of the Skeletal System
 Module 7 -Chapter 10. Overview Disorders of the Muscular System Disorders of the Skeletal System") Musculoskeletal Disorders (Part B-2) Module 7 -Chapter 10 Overview Disorders of the Muscular System Disorders of the Skeletal System Susie Turner, MD 1/9/13 Joint Disorders Arthritis Inflammation of Joint
Musculoskeletal Disorders (Part B-2) Module 7 -Chapter 10 Overview Disorders of the Muscular System Disorders of the Skeletal System Susie Turner, MD 1/9/13 Joint Disorders Arthritis Inflammation of Joint
DISCUSSION BY: Dr M. R. Shakeebi, MD, Rheumatologist
 Case presentations Related to some Rheumatic Diseases Lab & Clinic i Programs, Tuesday, April 24, 2012 COORDINATOR: Dr M. Mahdi Mohammadi, LMD,PhD, Immunologist COORDINATOR: Dr M. Mahdi Mohammadi, LMD,PhD,
Case presentations Related to some Rheumatic Diseases Lab & Clinic i Programs, Tuesday, April 24, 2012 COORDINATOR: Dr M. Mahdi Mohammadi, LMD,PhD, Immunologist COORDINATOR: Dr M. Mahdi Mohammadi, LMD,PhD,
Focal Knee Swelling Clinical Presentation
 Focal Knee Swelling Clinical Presentation referral for MSK Triage History and Examination Baker's Cyst Medial or Lateral Focal Swelling Consider meniscal Cysts Bursitis Refer for Weight Bearing X-ray AP
Focal Knee Swelling Clinical Presentation referral for MSK Triage History and Examination Baker's Cyst Medial or Lateral Focal Swelling Consider meniscal Cysts Bursitis Refer for Weight Bearing X-ray AP
THE HIP. Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness.
 THE HIP Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness. Objectives Hip anatomy Causes of hip pain Hip exam Anatomy Bones Ilium Anterior Superior Iliac Spine
THE HIP Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness. Objectives Hip anatomy Causes of hip pain Hip exam Anatomy Bones Ilium Anterior Superior Iliac Spine
High Impact Rheumatology
 High Impact Rheumatology Systemic Lupus Erythematosus Bernard Rubin, DO MPH Case 1: History A 45-year-old woman presents with severe dyspnea and cough. She was in excellent health until 4 weeks ago when
High Impact Rheumatology Systemic Lupus Erythematosus Bernard Rubin, DO MPH Case 1: History A 45-year-old woman presents with severe dyspnea and cough. She was in excellent health until 4 weeks ago when
Osteomieliti STEOMIE
 OsteomielitiSTEOMIE Osteomyelitis is the inflammation of bone caused by pyogenic organisms. Major sources of infection: - haematogenous spread - tracking from adjacent foci of infection - direct inoculation
OsteomielitiSTEOMIE Osteomyelitis is the inflammation of bone caused by pyogenic organisms. Major sources of infection: - haematogenous spread - tracking from adjacent foci of infection - direct inoculation
TUBERCULOSIS OF HIP AND KNEE JOINT
 TUBERCULOSIS OF HIP AND KNEE JOINT TUBERCULOSIS OF HIP JOINT Occurrence-15% of all osteo articular tuber culosis Next common after spinal TB AETIO PATHOGENESIS Most common cause Mycobacterium tuberculosis
TUBERCULOSIS OF HIP AND KNEE JOINT TUBERCULOSIS OF HIP JOINT Occurrence-15% of all osteo articular tuber culosis Next common after spinal TB AETIO PATHOGENESIS Most common cause Mycobacterium tuberculosis
How to interpret and order rheumatology tests
 How to interpret and order rheumatology tests Kam Shojania, MD, FRCPC Clinical Professor and Head, UBC Division of Rheumatology Faculty/Presenter Disclosure Faculty: Kam Shojania Relationships with financial
How to interpret and order rheumatology tests Kam Shojania, MD, FRCPC Clinical Professor and Head, UBC Division of Rheumatology Faculty/Presenter Disclosure Faculty: Kam Shojania Relationships with financial
Rheumatology: 1. Is it arthritis?
 Clinical basics Rheumatology: 1. Is it arthritis? Stephanie Ensworth Case 1 A 29-year-old woman consults her physician 2 months after the birth of her second child because she woke one morning with pain
Clinical basics Rheumatology: 1. Is it arthritis? Stephanie Ensworth Case 1 A 29-year-old woman consults her physician 2 months after the birth of her second child because she woke one morning with pain
ERROR CORRECTION FORM
 Juvenile Idiopathic Arthritis Pre-HSCT Data Sequence Number: Registry Use Only Date of HSCT for which this form is being completed: HSCT type: autologous allogeneic, allogeneic, syngeneic unrelated related
Juvenile Idiopathic Arthritis Pre-HSCT Data Sequence Number: Registry Use Only Date of HSCT for which this form is being completed: HSCT type: autologous allogeneic, allogeneic, syngeneic unrelated related
CIBMTR Center Number: CIBMTR Recipient ID: RETIRED. Today s Date: Date of HSCT for which this form is being completed:
 Juvenile Idiopathic Arthritis Pre-HSCT Data Sequence Number: Date Received: Registry Use Only Today s Date: Date of HSCT for which this form is being completed: HSCT type: autologous allogeneic, allogeneic,
Juvenile Idiopathic Arthritis Pre-HSCT Data Sequence Number: Date Received: Registry Use Only Today s Date: Date of HSCT for which this form is being completed: HSCT type: autologous allogeneic, allogeneic,
INTERPRETATION OF LABORATORY TESTS IN RHEUMATIC DISEASE
 INTERPRETATION OF LABORATORY TESTS IN RHEUMATIC DISEASE Laboratory tests are an important adjunct in the clinical diagnosis of rheumatic diseases and are sometimes helpful in monitoring the activity of
INTERPRETATION OF LABORATORY TESTS IN RHEUMATIC DISEASE Laboratory tests are an important adjunct in the clinical diagnosis of rheumatic diseases and are sometimes helpful in monitoring the activity of
Where has SARA gone? Prof. David Kane Consultant Rheumatologist Beacon & Tallaght Hospitals. Clinical Professor in Rheumatology Trinity College Dublin
 Where has SARA gone? Prof. David Kane Consultant Rheumatologist Beacon & Tallaght Hospitals Clinical Professor in Rheumatology Trinity College Dublin 1 Reactive Arthritis Seronegative Asymmetrical Arthritis
Where has SARA gone? Prof. David Kane Consultant Rheumatologist Beacon & Tallaght Hospitals Clinical Professor in Rheumatology Trinity College Dublin 1 Reactive Arthritis Seronegative Asymmetrical Arthritis
Anthony DeWilde, O.D Linwood Blvd. Kansas City, MO x
 Anthony DeWilde, O.D. 4801 Linwood Blvd. Kansas City, MO 64128 816-861-4700 x 57411 anthony.dewilde@va.gov Uveitis and Glaucoma: The Seven Reasons Why IOP Can Increase in Uveitis (and What to do About
Anthony DeWilde, O.D. 4801 Linwood Blvd. Kansas City, MO 64128 816-861-4700 x 57411 anthony.dewilde@va.gov Uveitis and Glaucoma: The Seven Reasons Why IOP Can Increase in Uveitis (and What to do About
Pauciarticular juvenile rheumatoid arthritis: clinical and immunogenetic aspects
 Ann. rheum. Dis. (1979), 38, Supplement p. 79 Pauciarticular juvenile rheumatoid arthritis: clinical and immunogenetic aspects CHESTER W. FINK, AND PETER STASTNY From the University of Texas Southwestern
Ann. rheum. Dis. (1979), 38, Supplement p. 79 Pauciarticular juvenile rheumatoid arthritis: clinical and immunogenetic aspects CHESTER W. FINK, AND PETER STASTNY From the University of Texas Southwestern
REFERRAL GUIDELINES: RHEUMATOLOGY
 Outpatient Page 1 1 REFERRAL GUIDELINES: RHEUMATOLOGY Date of birth Demographic Contact details (including mobile phone) Clinical Reason for referral Duration of symptoms Essential Referral Content Referring
Outpatient Page 1 1 REFERRAL GUIDELINES: RHEUMATOLOGY Date of birth Demographic Contact details (including mobile phone) Clinical Reason for referral Duration of symptoms Essential Referral Content Referring
Rheumatoid Arthritis
 Rheumatoid Arthritis What is rheumatoid arthritis? Rheumatoid arthritis (RA) is an autoimmune disease that causes chronic inflammation of the joints. Rheumatoid arthritis can also cause inflammation of
Rheumatoid Arthritis What is rheumatoid arthritis? Rheumatoid arthritis (RA) is an autoimmune disease that causes chronic inflammation of the joints. Rheumatoid arthritis can also cause inflammation of
A CRP B FBC C LFT D blood culture E uric acid
 1 A 39 year old lady with rheumatoid arthritis is admitted to hospital with a hot, swollen and painful right knee. Which is the most important blood test? A CRP B FBC C LFT D blood culture E uric acid
1 A 39 year old lady with rheumatoid arthritis is admitted to hospital with a hot, swollen and painful right knee. Which is the most important blood test? A CRP B FBC C LFT D blood culture E uric acid
Rheumatoid arthritis and Psoriatic arthritis: a guide for Primary Care. Nina Flavin, MD Rheumatology Confluence Health April 13 th, 2018
 Rheumatoid arthritis and Psoriatic arthritis: a guide for Primary Care Nina Flavin, MD Rheumatology Confluence Health April 13 th, 2018 No Disclosures Objectives Recognize early signs of RA/PsA what to
Rheumatoid arthritis and Psoriatic arthritis: a guide for Primary Care Nina Flavin, MD Rheumatology Confluence Health April 13 th, 2018 No Disclosures Objectives Recognize early signs of RA/PsA what to
Diagnostic Tests in Rheumatic Disease: What s Old, What s New & What s Useful? COPYRIGHT
 Diagnostic Tests in Rheumatic Disease: What s Old, What s New & What s Useful? Robert H. Shmerling, M.D. Beth Israel Deaconess Medical Center Boston, MA Diagnostic Tests in Rheumatic Disease: What's Old,
Diagnostic Tests in Rheumatic Disease: What s Old, What s New & What s Useful? Robert H. Shmerling, M.D. Beth Israel Deaconess Medical Center Boston, MA Diagnostic Tests in Rheumatic Disease: What's Old,
A Patient s Guide to Lyme Disease
 A Patient s Guide to Lyme Disease 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 DISCLAIMER: The information in this booklet is compiled from a variety of sources.
A Patient s Guide to Lyme Disease 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 DISCLAIMER: The information in this booklet is compiled from a variety of sources.
Budsakorn Darawankul, MD. Maharat Nakhon Ratchasima Hospital
 Budsakorn Darawankul, MD. Maharat Nakhon Ratchasima Hospital Outline What is ANA? How to detect ANA? Clinical application Common autoantibody in ANA diseases Outline What is ANA? How to detect ANA? Clinical
Budsakorn Darawankul, MD. Maharat Nakhon Ratchasima Hospital Outline What is ANA? How to detect ANA? Clinical application Common autoantibody in ANA diseases Outline What is ANA? How to detect ANA? Clinical
The diagnostic challenge of joint pain part 2
 Musculoskeletal 407 The diagnostic challenge of joint pain part 2 Polyarthralgia is a common presentation in primary care. Because chronic arthritides may present abruptly, they need to be considered in
Musculoskeletal 407 The diagnostic challenge of joint pain part 2 Polyarthralgia is a common presentation in primary care. Because chronic arthritides may present abruptly, they need to be considered in
Review Article. Appraoch to Patients with Polyarticular Symptoms. Introduction. Raymond WS Wong
 Review Article Appraoch to Patients with Polyarticular Symptoms Raymond WS Wong Abstract: Keywords: Polyarticular symptoms represent the most common symptom complex resulting in referral to a rheumatologist
Review Article Appraoch to Patients with Polyarticular Symptoms Raymond WS Wong Abstract: Keywords: Polyarticular symptoms represent the most common symptom complex resulting in referral to a rheumatologist
History Taking and the Musculoskeletal Examination
 History Taking and the Musculoskeletal Examination Introduction A thorough rheumatologic assessment is performed within the context of a good general evaluation of the patient. The patient should be undressed
History Taking and the Musculoskeletal Examination Introduction A thorough rheumatologic assessment is performed within the context of a good general evaluation of the patient. The patient should be undressed
APR-DRG Description Ave Charge
 Abdominal Pain 16,500.25 2.8 6,000.09 Acute & Subacute Endocarditis 15,339.30 3.0 5,113.10 Acute Myocardial Infarction 17,687.46 2.6 6,802.87 Alcohol Abuse & Dependence 19,126.64 4.2 4,553.96 Alcoholic
Abdominal Pain 16,500.25 2.8 6,000.09 Acute & Subacute Endocarditis 15,339.30 3.0 5,113.10 Acute Myocardial Infarction 17,687.46 2.6 6,802.87 Alcohol Abuse & Dependence 19,126.64 4.2 4,553.96 Alcoholic
Articular disease of the hand - the target joint approach
 Articular disease of the hand - the target joint approach Poster No.: C-1817 Congress: ECR 2016 Type: Educational Exhibit Authors: R. R. Domingues Madaleno 1, A. P. Pissarra 1, I. Abreu 2, A. Canelas 1,
Articular disease of the hand - the target joint approach Poster No.: C-1817 Congress: ECR 2016 Type: Educational Exhibit Authors: R. R. Domingues Madaleno 1, A. P. Pissarra 1, I. Abreu 2, A. Canelas 1,
COMMON VARIABLE IMMUNODEFICIENCY
 COMMON VARIABLE IMMUNODEFICIENCY This booklet is intended for use by patients and their families and should not replace advice from a clinical immunologist. 1 COMMON VARIABLE IMMUNODEFICIENCY Also available
COMMON VARIABLE IMMUNODEFICIENCY This booklet is intended for use by patients and their families and should not replace advice from a clinical immunologist. 1 COMMON VARIABLE IMMUNODEFICIENCY Also available
Approach to Arthritis
 Approach to Arthritis Dr. V. Krishnamurthy M. D., D. M. (Rheumatology) Rheumatologist, Chennai Meenakshi Multispecialty Hospital Rheumatologist, Meenakshi Academy of Higher Education (MAHER), Apollo Specialty
Approach to Arthritis Dr. V. Krishnamurthy M. D., D. M. (Rheumatology) Rheumatologist, Chennai Meenakshi Multispecialty Hospital Rheumatologist, Meenakshi Academy of Higher Education (MAHER), Apollo Specialty
Paediatrica Indonesiana
 VOLUME 46 March - April 2006 NUMBER 3-4 Case Report Juvenile rheumatoid arthritis associated with uveitis in a 4-year-old girl Made Sukmawati, Hendra Santoso, Niti Susila Juvenile rheumatoid arthritis
VOLUME 46 March - April 2006 NUMBER 3-4 Case Report Juvenile rheumatoid arthritis associated with uveitis in a 4-year-old girl Made Sukmawati, Hendra Santoso, Niti Susila Juvenile rheumatoid arthritis
When is it Rheumatoid Arthritis When to Refer
 When is it Rheumatoid Arthritis When to Refer Nancy A. Brown, DO Spring 2015 When is it Rheumatoid Arthritis When to Refer Learning objectives To review the definition and epidemiology of Rheumatoid Arthritis
When is it Rheumatoid Arthritis When to Refer Nancy A. Brown, DO Spring 2015 When is it Rheumatoid Arthritis When to Refer Learning objectives To review the definition and epidemiology of Rheumatoid Arthritis
Chapter 2. Overview of ankylosing spondylitis
 Chapter 2 Overview of ankylosing spondylitis The concept and classification of spondyloarthritis The term spondyloarthritis (SpA) comprises AS, reactive arthritis, arthritis/spondylitis associated with
Chapter 2 Overview of ankylosing spondylitis The concept and classification of spondyloarthritis The term spondyloarthritis (SpA) comprises AS, reactive arthritis, arthritis/spondylitis associated with
Rheumatoid Arthritis. Rheumatoid Arthritis. RCS 6080 Medical and Psychosocial Aspects of Rehabilitation Counseling. Rheumatic Diseases
 RCS 6080 Medical and Psychosocial Aspects of Rehabilitation Counseling Rheumatic Diseases The prevalence of rheumatoid arthritis in most Caucasian populations approaches 1% among adults 18 and over and
RCS 6080 Medical and Psychosocial Aspects of Rehabilitation Counseling Rheumatic Diseases The prevalence of rheumatoid arthritis in most Caucasian populations approaches 1% among adults 18 and over and
Growing Pains in Children 1.0 Contact Hour Presented by: CEU Professor
 Growing Pains in Children 1.0 Contact Hour Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2008 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution of these
Growing Pains in Children 1.0 Contact Hour Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2008 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution of these
OSTEOMYELITIS. If it occurs in adults, then the axial skeleton is the usual site.
 OSTEOMYELITIS Introduction Osteomyelitis is an acute or chronic inflammatory process of the bone and its structures secondary to infection with pyogenic organisms. Pathophysiology Osteomyelitis may be
OSTEOMYELITIS Introduction Osteomyelitis is an acute or chronic inflammatory process of the bone and its structures secondary to infection with pyogenic organisms. Pathophysiology Osteomyelitis may be