Therapeutic Agents in Rheumatic and Inflammatory Diseases Drug Class Prior Authorization Protocol
|
|
|
- Ursula Manning
- 6 years ago
- Views:
Transcription

1 Therapeutic Agents in Rheumatic and Inflammatory Diseases Drug Class Prior Authorization Protocol Line of Business: Medi-Cal Effective Date: August 16, 2017 Revision Date: August 16, 2017 This policy has been developed through review of medical literature, consideration of medical necessity, generally accepted medical practice standards, and approved by the IEHP Pharmacy and Therapeutics Subcommittee. Drugs: Actemra (tocilizumab), Cimzia (certolizumab), Cosentyx (secukinumab), Enbrel (etanercept), Entyvio (vedolizumab), Humira (adalimumab), Inflectra (infliximab-dyyb), Kevzara (sarilumab), Kineret (anakinra), Orencia (abatacept), Otezla (apremilast), Remicade (infliximab), Simponi, Simponi Aria (golimumab), Stelara (ustekinumab), Taltz (ixekizumab), Tysabri (natalizumab), Xeljanz (tofacitinib) FDA Approved Indications: AS CD UC PP PsA RA HS MS UV pjia sjia Actemra (tocilizumab) IV IV Cimzia (certolizumab) Cosentyx (secukinumab) Enbrel (etanercept) Entyvio (vedolizumab) Inflectra (infliximab-dyyb) Humira (adalimumab) Kevzara (sarilumab) Kineret (anakinra) Orencia (abatacept) IV Otezla (apremilast) Remicade (infliximab) Simponi (golimumab) Simponi Aria (golimumab) Stelara (ustekinumab) Taltz (ixekizumab) Tysabri (natalizumab) Xeljanz (tofacitinib) AS = ankylosing spondylitis; CD = Crohn s disease; UC = ulcerative colitis; pjia = polyarticular juvenile idiopathic arthritis; sjia = systemic juvenile idiopathic arthritis; PP = plaque psoriasis; PsA = psoriatic arthritis; RA = rheumatoid arthritis; HS = Hidradenitis Suppurativa; MS = multiple sclerosis; UV = uveitis
2 Policy/Criteria: A. Drugs: Actemra (tocilizumab), Cimzia (certolizumab), Enbrel (etanercept), Humira (adalimumab), Inflectra (infliximab-dyyb), Kevzara (sarilumab), Kineret (anakinra), Orencia (abatacept), Remicade (infliximab), Renflexis (infliximab-abda), Simponi, Simponi Aria (golimumab), Xeljanz (tofacitinib) Diagnosis: a. Rheumatoid Arthritis Specialist: Rheumatologist Criteria: a. Trial and failure of at least one non-biologic DMARD (e.g. methotrexate, hydroxychloroquine, leflunomide, sulfasalazine, etc.) b. Failure or inadequate response to at least a 3-month treatment course of the two preferred biologic therapies: Enbrel and Humira, unless each were not tolerated or were contraindicated Authorization Duration: 12 months Re-Authorization Criteria: a. Documentation of meeting therapeutic goal (e.g. disease stability, improvement in daily activities and/or reduction in frequency of disease attacks) a. Requested dosage and administration are consistent with the FDA recommendations Formulary Status: a. Enbrel and Humira: Non-formulary preferred; PA applies b. Others: Non-formulary, PA applies B. Drugs: Cimzia (certolizumab), Cosentyx (secukinumab), Enbrel (etanercept), Humira (adalimumab), Inflectra (infliximab-dyyb), Remicade (infliximab), Renflexis (infliximab-abda), Simponi (golimumab) Diagnosis: a. Ankylosing Spondylitis Specialist: Rheumatologist Criteria:
3 a. Failure or clinically significant adverse effects to at least one-month treatment course of one NSAID at maximal recommended dose or maximally tolerated dose b. Failure or inadequate response to at least a 3-month treatment course of the two preferred biologic therapies: Enbrel and Humira, unless each were not tolerated or were contraindicated Authorization Duration: 12 months Re-Authorization Criteria: a. Documentation of meeting therapeutic goal (e.g. disease stability, improvement and/or reduction in frequency of disease attacks) b. Requested dosage and administration are consistent with the FDA recommendations Formulary Status: a. Enbrel and Humira: Non-formulary preferred; PA applies b. Others: Non-formulary, PA applies C. Drugs: Cimzia (certolizumab), Cosentyx (secukinumab), Enbrel (etanercept), Humira (adalimumab), Inflectra (infliximab-dyyb), Orencia (abatacept), Remicade (infliximab), Renflexis (infliximab-abda), Simponi (golimumab), Stelara (ustekinumab) Diagnosis: a. Psoriatic arthritis Specialist: Dermatologist, Rheumatologist Criteria: a. Trial and failure of at least one non-biologic DMARD (e.g. methotrexate, leflunomide, sulfasalazine, etc.) b. Failure or inadequate response to at least a 3-month treatment course of the two preferred biologic therapies: Enbrel and Humira, unless each were not tolerated or were contraindicated Authorization Duration: 12 months Re-Authorization Criteria: a. Documentation of meeting therapeutic goal (e.g. disease stability, improvement and/or reduction in frequency of disease attacks)
4 b. Requested dosage and administration are consistent with the FDA recommendations Formulary Status: a. Enbrel and Humira: Non-formulary preferred; PA applies b. Others: Non-formulary, PA applies D. Drugs: Cimzia (certolizumab), Entyvio (vedolizumab), Humira (adalimumab), Inflectra (infliximab-dyyb), Remicade (infliximab), Renflexis (infliximab-abda), Stelara (ustekinumab, Tysabri (natalizumab) Diagnosis: a. Crohn s Disease Specialist: Gastroenterologist Criteria: a. Failure or clinically significant adverse effects to an adequate course of corticosteroids (e.g. oral budesonide 9mg/day, prednisone 40-60mg daily) OR Documentation that patient has been unable to taper corticosteroid therapy without experiencing worsening of disease b. Treatment with at least a two-month course of DMARD (e.g. azathioprine, mercaptopurine or methotrexate) was not effective or not tolerated, unless all are contraindicated c. Failure or inadequate response to at least a 3-month treatment course of the preferred biologic therapies (see below), unless each were not tolerated or were contraindicated; i. Humira, then ii. iii. Cimzia, then Renflexis (pharmacy benefit, when supplied by pharmacy) OR Renflexis or Inflectra (medical benefit, e.g. J code) Authorization Duration: 12 months Re-Authorization Criteria: a. Documentation of meeting therapeutic goal (e.g. disease stability, improvement and/or reduction in frequency of disease attacks) b. Requested dosage and administration are consistent with the FDA recommendations
5 Formulary Status: a. Humira: Non-formulary preferred; PA applies b. Others: Non-formulary, PA applies E. Drugs: Cosentyx (secukinumab), Enbrel (etanercept), Humira (adalimumab), Inflectra (infliximab-dyyb), Remicade (infliximab), Renflexis (infliximab-abda), Stelara (ustekinumab), Taltz (ixekizumab) Diagnosis: a. Plaque psoriasis Specialist: Dermatologist, Rheumatologist Criteria: a. Documented psoriasis involvement of at least 10% of the body surface area OR Documented psoriasis involvement of the face, ears, hands, feet or genitalia OR Documented significant functional disability (i.e. unable to do daily activities) b. Trial and failure of at least one non-biologic DMARD (e.g. methotrexate, cyclosporine, azathioprine, etc.) c. Failure or inadequate response to at least a 3-month treatment course of the two preferred biologic therapies: Enbrel and Humira, unless each were not tolerated or were contraindicated Authorization Duration: 12 months Re-Authorization Criteria: a. Documentation of meeting therapeutic goal (e.g. disease stability, improvement and/or reduction in frequency of disease attacks) b. Requested dosage and administration are consistent with the FDA recommendations Formulary Status: a. Enbrel and Humira: Non-formulary preferred; PA applies b. Others: Non-formulary, PA applies
6 F. Drugs: Entyvio (vedolizumab), Humira (adalimumab), Inflectra (infliximab-dyyb), Remicade (infliximab), Renflexis (infliximab-abda), Simponi (golimumab) Diagnosis: a. Ulcerative colitis Specialist: Gastroenterologist Criteria: a. Failure or clinically significant adverse effects to at least two of the conventional therapies: i. An adequate course of corticosteroids (e.g. oral budesonide 9mg/day, prednisone 40-60mg daily or budesonide rectal) ii. At least one aminosalicylates (e.g. mesalamine, balsalazide, sulfasalazine) iii. Treatment with at least a two-month course of DMARD (e.g. azathioprine, mercaptopurine, methotrexate, sulfasalazine) was not effective or not tolerated, unless all are contraindicated b. Failure or inadequate response to at least a 2-month treatment course of the preferred biologic therapies (see below), unless each were not tolerated or were contraindicated. i. Humira, then ii. iii. Simponi, then Renflexis (pharmacy benefit, when supplied by pharmacy) OR Renflexis or Inflectra (medical benefit, e.g. J code) Authorization Duration: 12 months Re-Authorization Criteria: a. Documentation of meeting therapeutic goal (e.g. disease stability, improvement and/or reduction in frequency of disease attacks) b. Requested dosage and administration are consistent with the FDA recommendations Formulary Status: a. Humira: Non-formulary preferred; PA applies b. Others: Non-formulary, PA applies G. Drug: Humira (adalimumab) Diagnosis:
7 a. Non-Infectious Uveitis Specialist: Ophthalmologist, Rheumatologist Criteria: a. Failure or clinically significant adverse effects to at least one oral corticosteroids (e.g. prednisone) b. Failure or clinically significant adverse effects to at least one non-biologic DMARD (e.g. azathioprine, cyclosporine, methotrexate, mycophenolate mofetil, tacrolimus, etc.) Authorization Duration: 12 months Re-Authorization Criteria: a. Documentation of meeting therapeutic goal (e.g. disease stability, improvement and/or reduction in frequency of disease attacks) b. Requested dosage and administration are consistent with the FDA recommendations Formulary Status: Non-formulary preferred, PA applies H. Drug: Ilaris (canakinumab) Eligibility criteria: Check CCS eligibility Diagnosis: a. Cryopyrin-Associated Periodic Syndromes (CAPS): Familial cold autoinflammatory syndrome or Muckle-Wells syndrome OR b. Familial Mediterranean fever (FMF) OR c. Tumor necrosis factor receptor-1 associated periodic syndrome (TRAPS) OR Hyperimmunoglobulin D Syndrome (HIDS)/Mevalonate Kinase Deficiency (MKD) OR d. Systemic Juvenile Idiopathic Arthritis Specialist: Rheumatologist, Immunologist, specialist experienced in CAPS, FMF, TRAPS, HIDS or MKD Criteria:
8 a. CAPS: Familial cold autoinflammatory syndrome or Muckle-Wells syndrome: i. Documented genetic confirmation of mutation in NLRP3; ii. Documentation of significant functional impairment that limits daily living activities; b. Familial Mediterranean fever (FMF): i. Failure or clinically significant adverse effects to the alternative: colchicine c. TRAPS, HIDS or MKD: i. Confirmed diagnosis by specialist d. Systemic Juvenile Idiopathic Arthritis i. Failure or clinically significant adverse effects to: Actemra Kineret Authorization Duration: a. Pending CCS eligibility: 1 month b. Not CCS eligible: 12 months Re-Authorization Criteria: a. Documentation of meeting therapeutic goal (e.g. disease stability, improvement and/or reduction in frequency of disease attacks) b. Requested dosage and administration are consistent with the FDA recommendations Formulary Status: Non-formulary, PA applies I. Drug: Otezla (apremilast) Diagnosis: a. Plaque psoriasis OR b. Psoriatic arthritis Specialist: Dermatologist, Rheumatologist Criteria: a. Plaque psoriasis: i. Failure or clinically significant adverse effects to one of the preferred biologic therapy: Humira or Enbrel b. Psoriatic arthritis: i. Failure or clinically significant adverse effects to one of the preferred biologic therapy: Humira or Enbrel



9 Authorization Duration: a. 12 months Re-Authorization Criteria: a. Documentation of meeting therapeutic goal (e.g. disease stability, improvement and/or reduction in frequency of disease attacks) b. Requested dosage and administration are consistent with the FDA recommendations Formulary Status: Non-formulary, PA applies Clinical Evidence: 2015 American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis Table 1: Recommendation for the treatment of patients with early RA:



 defined as a")
10 Figure 1: 2015 American College of Rheumatology recommendations update for the treatment of early rheumatoid arthritis (RA) defined as a disease duration < 6 months.
11



")
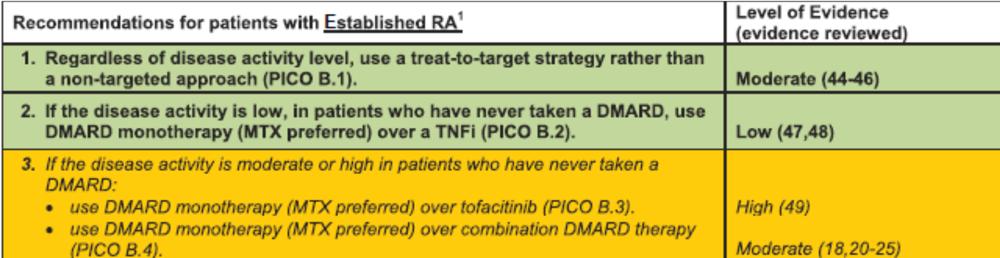
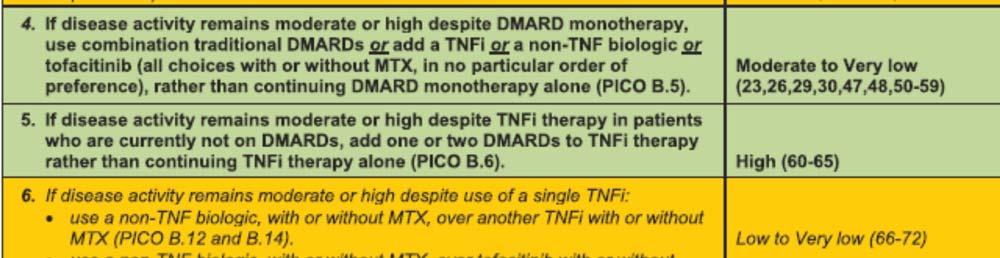
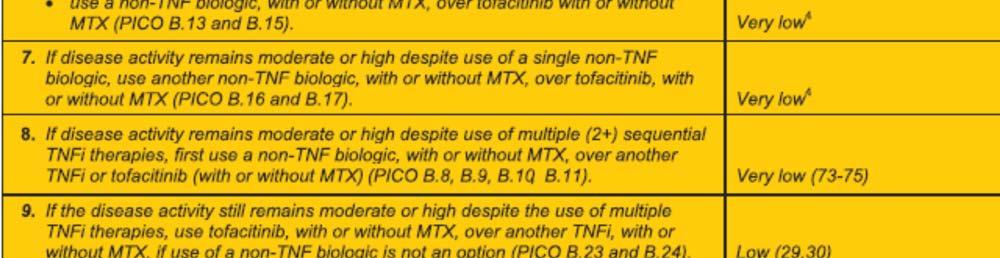
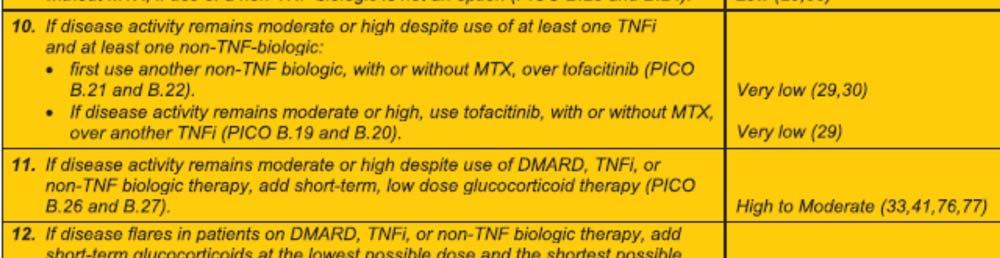
12 Table 2: Recommendation for the treatment of patients with established RA Figure 2: 2012 American College of Rheumatology (ACR) recommendations update for the treatment of established rheumatoid arthritis (RA) defined as a disease duration 6 months
 Systemic JIA with")
")
 monotherapy was recommended for a maximum period of 2 weeks as a therapeutic")
.")
13 Table 3: Recommendation in RA patients with high-risk comorbidities 2013 Update of the 2011 American College of Rheumatology Recommendations for the Treatment of Juvenile Idiopathic Arthritis (JIA) Systemic JIA with active systemic features and varying degrees of synovitis: Initial Therapeutic Options: Anakinra (Kineret) was recommended as one initial therapeutic option for patients with an physical global assessment (MD global) 5 irrespective of the active joint count (AJC), or a MD global <5 and an AJC >0 (level C). Systemic glucocorticoid (GC) monotherapy was recommended for a maximum period of 2 weeks as a therapeutic option for patients with an MD global <5 and an AJC >4 and for all patients with an MD global 5 irrespective of the AJC (Level C). Continuing GC as monotherapy for 1 month for patients with continued disease activity was inappropriate (Level D).
14 Initiating NSAID monotherapy in a patient without prior treatment was recommended as one approach for patients with an MD global <5 irrespective of the AJC (Level D). NSAID monotherapy was inappropriate for patients with an MD global 5 and an AJC >0 (Level D). Therapeutic Options for Continued Disease Activity Use of abatacept (Orencia) was recommended only for patients with an MD global 5 and an AJC >4 after a trial of both an IL-1 inhibitor [e.g. anakinra (Kineret)] and tocilizumab (Actemra) sequentially (level D). Anakinra was recommended for patients with continued disease activity after treatment with GC monotherapy (level A) or NSAID monotherapy (level C). Use of a calcineurin inhibitor was recommended only for patients with an MD global 5 and an AJC of 0 after a trial of both an IL-1 inhibitor and tocilizumab sequentially (level C). Canakinumab (Ilaris) was recommended for patients with continued disease activity after treatment with GC monotherapy (level A), methotrexate or leflunomide (level A), anakinra (level B) or tocilizumab (level C). GC monotherapy was recommended as an option following failed treatment with NSAID monotherapy for patients with an MD global <5 and an AJC >0 and for patients with an MD global 5 irrespective of the AJC (level C). Adjunct GC therapy at any point was appropriate to consider (level D). Intraarticular GC injection was recommended as adjunct therapy at any time (level C). Methotrexate (MTX) or leflunomide was recommended for patients with an MD global <5 and an AJC >0 after treatment with GC monotherapy (level C), an IL-1 inhibitor [e.g. anakinra (Kineret)] (level D) or tocilizumab (Actemra) (level D). Initiation of a TNF inhibitor was recommended for patients with an AJC >4 irrespective of the MD global after a trial of an IL-1 inhibitor or tocilizumab (level C). Initiation of a TNF inhibitor was recommended for patients with an AJC >0 irrespective of the MD global after a trial of both an IL-1 inhibitor and tocilizumab sequentially (level C). Systemic JIA without active systemic features and with varying degrees of active synovitis: Initial Therapeutic Options: Intraarticular GC injection was recommended as an initial treatment option for patients with an AJC 4 (level C). Initiation of MTX or leflunomide was recommended for patients with an AJC >4 (level C). Initiation of NSAID monotherapy in a patient without prior treatment for a maximum period of 1 month was recommended as one treatment approach for patients with an AJC>0 (level D). Continuing NSAID monotherapy for longer than 2 months for patients with continued disease activity was in appropriate (level D). Anakinra was recommended as a therapeutic option for patients with an AJC >4 following failed intraarticular injection or NSAID monotherapy (level B). Use of anakinra was also recommended for patients with an AJC >0 following treatment with MTX or leflunomide (level B).
15 Initiation of canakinumab was recommended for patients with an AJC >4 only after a trial of a DMARD plus anakinra or tocilizumab (level B), a DMARD plus a TNFinhibitor (level B) or abatacept (level C). Therapeutic Options for Continued Disease Activity: Use of abatacept was recommended for patients with an AJC >0 after treatment with MTX or leflunomide (level B), anakinra (level D) or tocilizumab (level D). Anakinra was recommended as a therapeutic option for patients with an AJC >4 following failed intraarticular injection of NSAID monotherapy (level B). Use of anakinra was also recommended for patients with an AJC >0 following treatment with MTX or leflunomide (level B). Initiation of canakinumab was recommended for patients with an AJC >4 only after a trial of a DMARD plus anakinra or tocilizumab (level B), a DMARD plus a TNFinhibitor (level B), or abatacept (level C). Use of MTX or leflunomide was recommended as an option for an AJC >0 following treatment with intraarticular injection (level C), NSAID monotherapy (level C), an IL-1 inhibitor (level D) or tocilizumab (level D). Initiation of a TNF inhibitor was recommended for patients with an AJC >0 after treatment with MTX or leflunomide (level C), anakinra (level D) or tocilizumab (level D). Initiation of tocilizumab was recommended for an AJC >0 following treatment with anakinra (level B) or MTX or leflunomide (level B). Systemic JIA with Features concerning for Macrophage Activation Syndrome (MAS): Initial Therapeutic Options: Use of anakinra was recommended as one therapeutic option for patients with features concerning for MAS (level C). Use of a calcineurin inhibitor was recommended as one therapeutic option for patients with features concerning for MAS (level C). Use of systemic GC monotherapy (administered by oral or intravenous route) was also recommended as a therapeutic option for patients with features concerning for MAS (level C). Continuing GC monotherapy for 2 weeks in patients with continued features concerning for MAS was inappropriate (level D).




16 Figure 3: Treatment pathways for patients with active systemic features and varying degrees of synovitis Update of the 2011 American College of Rheumatology Recommendations for the Treatment of Juvenile Idiopathic Arthritis (JIA)




17 Figure 4: Treatment pathways for patients without active systemic features and with varying degrees of synovitis Update of the 2011 American College of Rheumatology Recommendations for the Treatment of Juvenile Idiopathic Arthritis (JIA)
18 2009 American College of Gastroenterology Practice Guidelines: Management of Crohn s Disease in Adults Patients with moderate to severe disease are treated with prednisone 40-60mg daily until resolution of symptoms and resumption of weight gain (generally 7-28 days) (grade A). Azathioprine and 6-mercaptopurine are effective for maintaining a steroid-induced remission (grade A), and parenteral methotrexate at a dose of 25mg/week is effective for steroid-dependent and steroid-refractory CD (grade B). The anti-tnf monoclonal antibodies, infliximab, adalimumab, and certolizumab-pegol are effective in the treatment of moderate to severe active CD in patients who have not responded despite complete and adequate therapy with a corticosteroid or an immunosuppressive agent (grade A). Infliximab monotherapy and infliximab combined with azathioprine are more effective than azathioprine in the treatment of patients with moderate to severe CD who have failed to respond to first-line therapy with mesalamine and/or corticosteroids (grade A). Infliximab, adalimumab, and certolizumab-pegol may be used as alternatives to steroid therapy in selected patients in whom corticosteroids are contraindicated or not desired (grade B). The anti-alpha 4 integrin antibody, natalizumab, is effective in the treatment of patients with moderate to severely active CD who have had an inadequate response or are unable to tolerate conventional CD therapies and anti-tnf monoclonal antibody therapy (grade A). Entyvio (vedolizumab) Vedolizumab, a humanized anti-alpha-4-beta-7 integrin monoclonal antibody, was FDAapproved for induction and maintenance therapy in adults with moderately to severely active ulcerative colitis, and for achieving (but not maintaining) clinical response and remission in adults with moderately to severely active Crohn s disease, who have had an inadequate response to at least one conventional therapy (e.g. TNF blocker, immunomodulator, glucocorticoids). Crohn s disease trial: In a double blind randomized trial, 368 patients were enrolled to receive either intravenous Entyvio (vedolizumab) or placebo. Concomitant stable dosages of aminosalicylates, corticosteroids (prednisone dosage 30mg/day or equivalent), and immunomodulators (azathioprine, 6-mercaptopurine or methotrexate) were permitted through Week 6. At week 6, 15% of patients taking Entyvio achieved clinically significant remission vs 7% with placebo (p= 0.041, primary end point). Nevertheless, there was no significant difference in CDAI-100 response ( 100 point decrease in CDAI score from baseline). o In addition, maintenance of remission was assessed at week 52 by enrolling a total of 461 patients who demonstrated clinical response at week 6 in either the induction trial or the following open label group. At week 52, remission rates were significantly higher in the vedolizumab group (39%) vs placebo (22%) (p=0.001). Ulcerative colitis trial: In a double blind randomized trial, 374 patients received either intravenous vedolizumab 300mg or placebo. Concomitant stable dosages of aminosalicylates, corticosteroids and immunomodulators (azathioprine or 6- mercaptopurine) were permitted through week 6. At week 6, the results demonstrated
19 statically significant higher rates of clinical response in vedolizumab (47%) vs placebo (26%) (p<0.001). Furthermore, statistically significant higher rates of clinical remission, improvement of endoscopic appearance of the mucosa and corticosteroid-free remission at week 52 were observed in the vedolizumab group. However, vedolizumab was associated with an increased risk for developing serious infections. Although no cases of progressive multifocal leukoencephalopathy (PML) have been reported in clinical trials, death has occurred in patients treated with another integrin receptor antagonist. A risk of PML cannot be ruled out Ulcerative Colitis Practice Guidelines in Adults: American College of Gastroenterology, Practice Parameters Committee Patients with mild to moderate distal colitis may be treated with oral aminosalicylates, topical mesalamine, or topical steroids (Evidence A). Topical mesalamine agents are superior to topical steroids or oral aminosalicylates (Evidence A). The combination of oral and topical aminosalicylates is more effective than either alone (Evidence A). The unusual patient who is refractory to all of the above agents at maximal doses, or who is systemically ill, may require treatment with oral prednisone in doses up to 40-60mg per day, or infliximab with an induction regimen of 5mg/kg at weeks 0, 2, and 6, although these two agents have not been studied specifically in patients with distal disease (Evidence C). Infliximab induction is an effective treatment for patients who are steroid refractory or steroid dependent despite adequate doses of a thiopurine, or who are intolerant to these medications. The infliximab induction dose is 5mg/kg given intravenously at weeks 0, 2, and 6 (Evidence A). Infliximab is contraindicated in patients with active infection, untreated latent TB, preexisting demyelinating disorder or optic neuritis, moderate to severe congestive heart failure, or current or recent malignancies. Infliximab is effective in maintaining improvement and remission in the patients responding to the infliximab induction regimen (Evidence A). The patient with severe colitis refractory to maximal oral treatment with prednisone, oral aminosalicylate drugs, and topical medications may be treated with infliximab 5mg/kg if urgent hospitalization is not necessary (Evidence A). Infliximab may also be effective in avoiding colectomy in patients failing intravenous steroids but its long-term efficacy is unknown in this setting (Evidence A) American Academy of Dermatology Guidelines of Care for the Management of Psoriasis and Psoriatic Arthritis Psoriasis without Psoriatic Arthritis: Recommended first line topical agents include corticosteroids, calcipotriene, calcitriol, calcipotriene-steroid combination, tazarotene (preferably in combination with a topical steroid), calcineurin inhibitors (flexures and face).
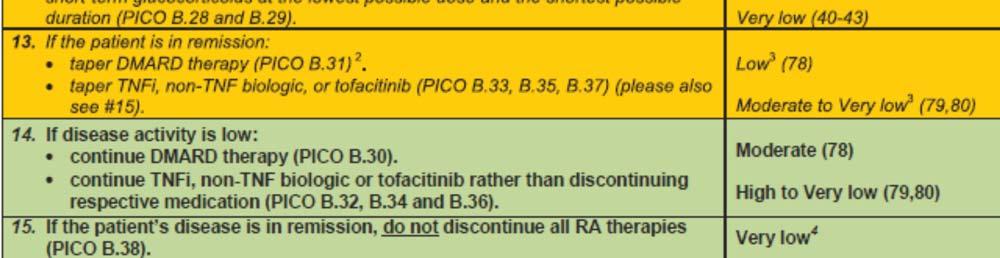
20 UV therapy remains an important therapeutic option for patients with moderate to severe disease. It is effective in the majority of patients, is cost-effective, and lacks systemic toxicities and immunosuppressive properties of systemic and biological treatments. Baseline screening, monitoring guidelines, absolute and relative contraindications, adverse events, and drug interactions of traditional systemic agents should be considered before initiating systemic agents. MTX remains the most widely used, logical first choice of systemic agent, because it is the most cost-effective systemic psoriasis agent with the longest safety follow-up data. Adverse effects include gastrointestinal side effects, hepatotoxicity, bone marrow suppression, acute pneumonitis and pulmonary fibrosis. Cyclosporine is particularly useful in the treatment of significant flares of psoriasis unresponsive to other therapies and as a bridging agent during the induction of other maintenance agents due to its rapid onset of action and marked efficacy. Intermittent short-term therapy with oral cyclosporine (12-16 weeks) is the most frequently recommended regimen, with treatment being withdrawn once significant improvement is achieved. Biologic agents are now routinely used when one or more traditional systemic agents fail to produce an adequate response or are not tolerated because of the presence of comorbidities. There is no specific sequence in which the currently available TNFα antagonists should be used. Although the strength of recommendation A is noted for the treatment of psoriasis using ustekinumab, compared with the TNF-alfa inhibitors which have now been available for more than 10 years, there is limited post-marketing safety data on ustekinumab. Its safety information is supplied by pooled analysis of phase II and phase III clinical trials. Psoriatic Arthritis: Mild PsA is most often managed with NSAIDs alone. If the psoriatic arthritis (PsA) is unresponsive after 2 to 3 months of therapy with NSAIDS, treatment with MTX should be considered. For patients with moderate to severe PsA, MTX, TNF-blockade, or combination of these therapies is considered first-line treatment. However, MTX is often used as first-line therapy before TNF- α blockade treatment, largely because of its significantly lower cost. Adalimumab, etanercept, golimumab and infliximab show similar efficacy for the signs and symptoms of PsA. On the other hand, infliximab clears cutaneous psoriasis in the highest proportion of patients and with the greatest rapidity, followed by adalimumab and then etanercept European League Against Rheumatism recommendations for the Management of Psoriatic Arthritis with Pharmacological Therapies In patients with psoriatic arthritis, non-steroidal anti-inflammatory drugs may be used to relieve musculoskeletal signs and symptoms. In patients with peripheral arthritis, particularly in those with many swollen joint, structural damage in the presence of inflammation, high erythrocyte sedimentation rate/c reactive protein and/or clinically relevant extra-articular manifestations, csdmards
21 should be considered at an early stage, with MTX preferred in those with relevant skin involvement. Local injection of glucocorticoids should be considered as adjunctive therapy in PsA; systemic glucocorticoids may be used with caution at the lowest effective dose. In patients with peripheral arthritis and an inadequate response to at least one csdmard, therapy with a bdmard, usually a TNFi, should be commenced. In patients with peripheral arthritis and an inadequate response to at least one csdmard, in whom TNFis are not appropriate, bdmards targeting interleukin (IL) 12/23 or IL-17 pathways may be considered. In patients with peripheral arthritis and an inadequate response to at least one csdmard, in whom bdmards are not appropriate, a tsdmard, such as a PDE4-inhibitor, may be considered. In patients with active enthesitis and/or dactylitis and insufficient response to NSAIDs or local glucocorticoid injections, therapy with a bdmard should be considered, which according to current practice is a TNFi. In patients with predominantly axial disease that is active and has insufficient response to NSAIDs, therapy with a bdmard should be considered, which according to current practice is a TNFi. In patients who fail to respond adequately to a bdmard, switching to another bdmard should be considered, including switching between TNFis.




22 Figure 5: 2015 EULAR Algorithm for Treatment of Psoriatic Arthritis
23 2016 Update of the ASAS/EULAR Recommendations for the Management of Axial Spondyloarthritis The primary goal of treating the patient with axspa is to maximize long-term healthrelated quality of life through control of symptoms and inflammation, prevention of progressive structural damage, preservation/normalization of function and social participation. The treatment of patients with axspa should be individualized according to the current signs and symptoms of the disease (axial, peripheral, extra-articular manifestation) and the patient characteristics including comorbidities and psychosocial factors. Disease monitoring of patients with axspa should include patient-reported outcomes, clinical findings, laboratory tests and imaging, all with the appropriate instruments and relevant to the clinical presentation. The frequency of monitoring should be an individual basis depending on symptoms, severity and treatment. Patient should be educated about axspa and encouraged to exercise on a regular basis and stop smoking; physical therapy should be considered. Patient suffering from pain and stiffness should use an NSAID as first-line drug treatment up to the maximum dose, taking risks and benefits into account. For patients who respond well to NSAIDs continuous use is preferred if symptomatic otherwise. Analgesics, such as paracetamol and opioid-like drugs, might be considered for residual pain after previously recommended treatments have failed, are contraindicated and/or poorly tolerated. Glucocorticoid injections directed to the local site of musculoskeletal inflammation may be considered. Patients with axial disease should not receive long-term treatment with systemic glucocorticoids. Patients with purely axial disease should normally not be treated with csdmards; sulfasalazine may be considered in patients with peripheral arthritis. bdmards should be considered in patients with persistently high disease activity despite conventional treatments; current practice is to start with TNFi therapy. If TNFi therapy fails, switching to another TNFi or an anti-il-17 therapy should be considered. If a patient is in sustained remission, tapering of a bdmard can be considered. Inflectra (infliximab-dyyb) The U.S. Food and Drug Administration approved Inflectra (infliximab-dyyb), a biosimilar to Remicade (infliximab) in April 5, Inflectra is approved and can be prescribed by a health care professional for the treatment of: o Adult patients and pediatric patients (ages six years and older) with moderately to severely active Crohn s disease who have had an inadequate response to conventional therapy; o Adult patients with moderately to severely active ulcerative colitis who have had an inadequate response to conventional therapy;
24 o Patients with moderately to severely active rheumatoid arthritis in combination with methotrexate; o Patients with active ankylosing spondylitis (arthritis of the spine); o Patients with active psoriatic arthritis; o Adult patients with chronic severe plaque psoriasis. The FDA s approval of Inflectra is based on review of evidence that included structural and functional characterization, animal study data, human pharmacokinetic and pharmacodynamics data, clinical immunogenicity data and other clinical safety and effectiveness data that demonstrates Inflectra is biosimilar to Remicade. Inflectra has been approved as biosimilar, not as an interchangeable product. The most common expected side effects of Inflectra include respiratory infections, such as sinus infections and sore throat, headache, coughing and stomach pain. Infusion reactions can happen up to two hours after an infusion. Symptoms of infusion reactions may include fever, chills, chest pain, low blood pressure or high blood pressure, shortness of breath, rash and itching. Inflectra contains a Boxed Warning to alert health care professionals and patients about an increased risk of serious infections leading to hospitalization or death, including tuberculosis, bacterial sepsis, invasive fungal infections (such as histoplasmosis) and others. The Boxed Warning also notes that lymphoma and other malignancies, some fatal, have been reported in children and adolescent patients treated with tumor necrosis factor blockers, including infliximab products such as Inflectra. Other serious side effects may include liver injury, blood problems, lupus-like syndrome, psoriasis, and in rare cases nervous system disorders. The drug must be dispensed with a patient Medication Guide that describes important information about its uses and risks. Xeljanz (tofacitinib) Xeljanz (tofacitinib), a janus kinase (JAK) inhibitor, interferes with the JAK-STAT signaling pathway and therefore the development of inflammation associated with rheumatoid arthritis. Fleischmann et al (2012) conducted a phase 3, double-blind, placebo-controlled, parallel-group, 6 month study. Patients (n = 611) were randomly assigned to tofacitinib 5 mg twice daily, tofacitinib 10 mg twice daily, 3 months of placebo and 3 months of tofacitinib 5 mg twice daily, or 3 months of placebo and tofacitinib 10 mg twice daily. The three primary endpoints were a 20% improvement in the American College of Rheumatology scale (ACR 20), change from baseline in the Health Assessment Questionnaire Disability Index (HAQ-DI) score (score range from 0 to 3), and percentage of patients with a Disease Activity Score for 28-joint counts of less than 2.6 (score range from 0 to 9.4) based on the erythrocyte sedimentation rate (DAS28-4[ESR]). By month 3, patients in the tofacitinib groups had a higher percentage of improvement in the ACR20 (p < 0.001) and greater reductions from baseline in the HAQ-DI score (p <0.001). The percentage of patients with a DAS28-4[ESR] less than 2.6 was not significantly greater in the tofacitinib groups, 5 mg and 10 mg, compared to placebo (p = 0.62 and p = 0.10, respectively). Six patients receiving tofacitinib developed serious infections. Tofacitinib treatment was associated with increased levels of low-density lipoprotein (LDL) cholesterol levels and decreased neutrophil counts. Common adverse events included headache and upper respiratory tract infections.
25 In a 12 month, phase III clinical trial, van Vollenhoven et al (2012) compared tofacitinib and adalimumab in patients who were receiving methotrexate. Patients (n = 717) were randomly assigned to tofacitinib 5 mg twice daily, tofacitinib 10 mg twice daily, adalimumab 40 mg every 2 weeks, or placebo. Those who did not receive a 20% reduction from baseline in the number of swollen and tender joints were transitioned to either tofacitinib 5 mg or 10 mg at month 3 and month 6. The three primary endpoints were a 20% improvement at months 6 in the American College of Rheumatology scale (ACR 20), change from baseline to month 3 in the Health Assessment Questionnaire Disability Index (HAQ-DI) score (score range from 0 to 3), and percentage of patients at month 6 who had a Disease Activity Score for 28-joint counts of less than 2.6 (score range from 0 to 9.4) based on the erythrocyte sedimentation rate (DAS28-4[ESR]). At month 6, the ACR 20 response rates were higher among the tofacitinib and adalimumab groups compared to placebo (p < 0.001). In addition, the percentage of patients with a DAS28-4[ESR] below 2.6 in both active treating groups was higher than placebo. At month 3, reductions in the HAQ-DI were greater among the tofacitinib and adalimumab groups compared to placebo. Adverse events were found more frequently with tofacitinib than placebo. While tofacitinib demonstrated superiority to placebo, the study was not designed to directly evaluate the efficacy of tofacitinib compared to adalimumab. Currently, studies have not shown any biologic DMARDs or JAK-inhibitor, tofacitinib, to be more effective than another in the treatment of rheumatoid arthritis. However, the safety profile for tofacitinib is limited relative to other alternatives. During clinical trials, tofacitinib was associated with an increased risk of serious infections, including opportunistic infections, tuberculosis, cancers and lymphoma. The most common adverse effects were upper respiratory tract infections, headache, diarrhea, and inflammation of the nasal passage and the upper part of the pharynx. References: 1. Enbrel [package insert]. Thousand Oaks, CA: Amgen and Wyeth Pharmaceuticals; Menter A, Korman N, Elmets C, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis. J Am Acad Dermatol 2010; 65(1) 3. Ringold S, Weiss PF, Beukelman T, et al Update of the 2011 American College of Rheumatology Recommendations for the Treatment of Juvenile Idiopathic Arthritis. Arthritis & Rheumatism. 2013; 65(10): Singh, JA, Saag, KG, Bridges JR SL, et al American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis. Arthritis Rheumatol. doi: /art U.S. Food and Drug Administration. FDA News Release. April 5, Available at Accessed October 18, Van der Heijde D, Ramiro S, Landewé R, et al update of the ASAS-EULAR management recommendations for axial spondyloarthritis. Annals of the Rheumatic Diseases Published Online First: 13 January doi: /annrheumdis
26 7. Gossec L, Smolen JS, Ramiro S, et al. European League Against Rheumatism (EULAR) recommendations for the management of psoriatic arthritis with pharmacological therapies: 2015 update. Annals of the Rheumatic Diseases Published Online First: 07 December doi: /annrheumdis Lichtenstein GR, Hanauer SB, et al. Am J Gastroenterol 2009; 104: ; doi: /ajg ; published online 6 January Kornbluth, A, Sacher, DB, et al. Am J Gastroenterol 2010; 105: ; doi: /ajg ; published online 12 January Change Control Date Change 08/16/2017 Added Renflexis (biosimilar to Remicade) as NF preferred over Inflectra for Crohn s/ulcerative Collitis when billed as pharmacy benefit. On parity with Inflectra for Crohn s/ulcerative Collitis when billed as a medical benefit. Revised criteria for Crohn s/ulcerative Collitis and added reauthorization criteria Added criteria and re-authorization criteria for Ilaris
Drug Class Prior Authorization Criteria Therapeutic Agents in Rheumatic and Inflammatory Diseases
 Drug Class Prior Authorization Criteria Therapeutic Agents in Rheumatic and Inflammatory Diseases Line of Business: Medicaid P & T Approval Date: August 16, 2017 Effective Date: August 16, 2017 This policy
Drug Class Prior Authorization Criteria Therapeutic Agents in Rheumatic and Inflammatory Diseases Line of Business: Medicaid P & T Approval Date: August 16, 2017 Effective Date: August 16, 2017 This policy
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Otezla (apremilast) Page 1 of 7 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Otezla (apremilast) Prime Therapeutics will review Prior Authorization requests Prior
Otezla (apremilast) Page 1 of 7 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Otezla (apremilast) Prime Therapeutics will review Prior Authorization requests Prior
1 P a g e. Systemic Juvenile Idiopathic Arthritis (SJIA) (1.3) Patients 2 years of age and older with active systemic juvenile idiopathic arthritis.
 (1.3) Patients 2 years of age and older with active systemic juvenile idiopathic arthritis.") LENGTH OF AUTHORIZATION: Initial: 3 months for Crohn s or Ulcerative Colitis; 1 year for all other indications. Renewal: 1 year dependent upon medical records supporting response to therapy and review
LENGTH OF AUTHORIZATION: Initial: 3 months for Crohn s or Ulcerative Colitis; 1 year for all other indications. Renewal: 1 year dependent upon medical records supporting response to therapy and review
Regulatory Status FDA- approved indication: Simponi and Simponi ARIA are tumor necrosis factor (TNF) blockers indicated for the treatment of: (2-3)
 blockers indicated for the treatment of: (2-3)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.51 Subject: Simponi / Simponi ARIA Page: 1 of 9 Last Review Date: March 16, 2018 Simponi / Simponi
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.51 Subject: Simponi / Simponi ARIA Page: 1 of 9 Last Review Date: March 16, 2018 Simponi / Simponi
Amjevita (adalimumab-atto)
") *- Florida Healthy Kids Amjevita (adalimumab-atto) Override(s) Prior Authorization Quantity Limit Medications Amjevita 20 mg/0.4 ml prefilled syringe Amjevita (adalimumab-atto) 40 mg/0.8 ml 2 #* ^ prefilled
*- Florida Healthy Kids Amjevita (adalimumab-atto) Override(s) Prior Authorization Quantity Limit Medications Amjevita 20 mg/0.4 ml prefilled syringe Amjevita (adalimumab-atto) 40 mg/0.8 ml 2 #* ^ prefilled
Pharmacy Management Drug Policy
 SUBJECT: Inflammatory Conditions Clinical Review Prior Authorization (CRPA) Rx and Medical Drugs POLICY NUMBER: PHARMACY-73 EFFECTIVE DATE: 01/01/2018 LAST REVIEW DATE: 06/11/2018 If the member s subscriber
SUBJECT: Inflammatory Conditions Clinical Review Prior Authorization (CRPA) Rx and Medical Drugs POLICY NUMBER: PHARMACY-73 EFFECTIVE DATE: 01/01/2018 LAST REVIEW DATE: 06/11/2018 If the member s subscriber
Biologics for Autoimmune Diseases
 Biologics for Autoimmune Diseases Goal(s): Restrict use of biologics to OHP funded conditions and according to OHP guidelines for use. Promote use that is consistent with national clinical practice guidelines
Biologics for Autoimmune Diseases Goal(s): Restrict use of biologics to OHP funded conditions and according to OHP guidelines for use. Promote use that is consistent with national clinical practice guidelines
INFLIXIMAB Remicade (infliximab), Inflectra (infliximab-dyyb), Ixifi* (infliximabqbtx), Renflexis (infliximab-abda)
, Inflectra (infliximab-dyyb), Ixifi* (infliximabqbtx), Renflexis (infliximab-abda)") Pre - PA Allowance None Prior-Approval Requirements Diagnoses Patient must have ONE of the following: 6 years of age or older 1. Moderate to severe Crohn s disease (CD) a. Patient has fistulizing disease
Pre - PA Allowance None Prior-Approval Requirements Diagnoses Patient must have ONE of the following: 6 years of age or older 1. Moderate to severe Crohn s disease (CD) a. Patient has fistulizing disease
Cimzia. Cimzia (certolizumab pegol) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.50.11 Section: Prescription Drugs Effective Date: April 1, 2018 Subject: Cimzia Page: 1 of 5 Last Review
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.50.11 Section: Prescription Drugs Effective Date: April 1, 2018 Subject: Cimzia Page: 1 of 5 Last Review
Regulatory Status FDA- approved indication: Simponi and Simponi ARIA are tumor necrosis factor (TNF) blockers indicated for the treatment of:
 blockers indicated for the treatment of:") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.51 Subject: Simponi / Simponi ARIA Page: 1 of 8 Last Review Date: March 17, 2017 Simponi / Simponi
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.51 Subject: Simponi / Simponi ARIA Page: 1 of 8 Last Review Date: March 17, 2017 Simponi / Simponi
Regulatory Status FDA-approved indications: Entyvio is an α4β7integrin receptor antagonist indicated for: (1)
") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.50.12 Subject: Entyvio Page: 1 of 7 Last Review Date: September 20, 2018 Entyvio Description Entyvio
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.50.12 Subject: Entyvio Page: 1 of 7 Last Review Date: September 20, 2018 Entyvio Description Entyvio
Amjevita (adalimumab-atto) CG-DRUG-64, CG-DRUG-65
 CG-DRUG-64, CG-DRUG-65") Market DC Amjevita (adalimumab-atto) CG-DRUG-64, CG-DRUG-65 Override(s) Prior Authorization Quantity Limit Medications Amjevita 20 mg/0.4 ml prefilled syringe Amjevita (adalimumab-atto) 40 mg/0.8 ml 2
Market DC Amjevita (adalimumab-atto) CG-DRUG-64, CG-DRUG-65 Override(s) Prior Authorization Quantity Limit Medications Amjevita 20 mg/0.4 ml prefilled syringe Amjevita (adalimumab-atto) 40 mg/0.8 ml 2
Stelara. Stelara (ustekinumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.90.04 Subject: Stelara Page: 1 of 9 Last Review Date: September 20, 2018 Stelara Description Stelara
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.90.04 Subject: Stelara Page: 1 of 9 Last Review Date: September 20, 2018 Stelara Description Stelara
Infusible Biologics Medical Policy Prior Authorization Program Summary
 Infusible Biologics Medical Policy Prior Authorization Program Summary Precertification/Prior Authorization may be required under certain plans. Please verify each member s benefits. OBJECTIVE The intent
Infusible Biologics Medical Policy Prior Authorization Program Summary Precertification/Prior Authorization may be required under certain plans. Please verify each member s benefits. OBJECTIVE The intent
Cyltezo (adalimumab-adbm) CG-DRUG-64, CG-DRUG-65
 CG-DRUG-64, CG-DRUG-65") Market DC Cyltezo (adalimumab-adbm) CG-DRUG-64, CG-DRUG-65 Override(s) Prior Authorization Quantity Limit Medications Cyltezo (adalimumab-adbm) 40 mg/0.8 ml prefilled syringe #* ^ Approval Duration 1 year
Market DC Cyltezo (adalimumab-adbm) CG-DRUG-64, CG-DRUG-65 Override(s) Prior Authorization Quantity Limit Medications Cyltezo (adalimumab-adbm) 40 mg/0.8 ml prefilled syringe #* ^ Approval Duration 1 year
Medication Policy Manual. Topic: Xeljanz, tofacitinib Date of Origin: January 21, 2013
 Medication Policy Manual Policy No: dru289 Topic: Xeljanz, tofacitinib Date of Origin: January 21, 2013 Committee Approval Date: January 19, 2015 Next Review Date: January 2016 Effective Date: April 1,
Medication Policy Manual Policy No: dru289 Topic: Xeljanz, tofacitinib Date of Origin: January 21, 2013 Committee Approval Date: January 19, 2015 Next Review Date: January 2016 Effective Date: April 1,
C. Assess clinical response after the first three months of treatment.
 Government Health Plan (GHP) of Puerto Rico Authorization Criteria Tumor Necrosis Factor Alpha (TNFα) Adalimumab (Humira ) Managed by MCO Section I. Prior Authorization Criteria A. Physician must submit
Government Health Plan (GHP) of Puerto Rico Authorization Criteria Tumor Necrosis Factor Alpha (TNFα) Adalimumab (Humira ) Managed by MCO Section I. Prior Authorization Criteria A. Physician must submit
Regulatory Status FDA-approved indication: Orencia is a selective T cell costimulation modulator indicated for: (1)
") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.18 Subject: Orencia Page: 1 of 8 Last Review Date: March 16, 2018 Orencia Description Orencia (abatacept)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.18 Subject: Orencia Page: 1 of 8 Last Review Date: March 16, 2018 Orencia Description Orencia (abatacept)
Pharmacy Management Drug Policy
 SUBJECT: Cimzia (Certolizumab pegol) - for Ankylosing Spondylitis, Crohn s Disease, Psoriatic Arthritis and Rheumatoid Arthritis POLICY NUMBER: PHARMACY-07 EFFECTIVE DATE: 5/2009 LAST REVIEW DATE: 6/13/2018
SUBJECT: Cimzia (Certolizumab pegol) - for Ankylosing Spondylitis, Crohn s Disease, Psoriatic Arthritis and Rheumatoid Arthritis POLICY NUMBER: PHARMACY-07 EFFECTIVE DATE: 5/2009 LAST REVIEW DATE: 6/13/2018
Simponi / Simponi ARIA (golimumab)
") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.51 Subject: Simponi / Simponi ARIA Page: 1 of 6 Last Review Date: September 15, 2016 Simponi / Simponi
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.51 Subject: Simponi / Simponi ARIA Page: 1 of 6 Last Review Date: September 15, 2016 Simponi / Simponi
Medication Policy Manual. Topic: Otezla, apremilast Date of Origin: May 9, 2014
 Medication Policy Manual Policy No: dru342 Topic: Otezla, apremilast Date of Origin: May 9, 2014 Committee Approval Date: January 19, 2015 Next Review Date: January 2016 Effective Date: April 1, 2015 IMPORTANT
Medication Policy Manual Policy No: dru342 Topic: Otezla, apremilast Date of Origin: May 9, 2014 Committee Approval Date: January 19, 2015 Next Review Date: January 2016 Effective Date: April 1, 2015 IMPORTANT
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: golimumab_simponi 8/2013 2/2018 2/2019 3/2018 Description of Procedure or Service Golimumab (Simponi and
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: golimumab_simponi 8/2013 2/2018 2/2019 3/2018 Description of Procedure or Service Golimumab (Simponi and
Cimzia. Cimzia (certolizumab pegol) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.50.11 Subject: Cimzia Page: 1 of 5 Last Review Date: December 8, 2017 Cimzia Description Cimzia (certolizumab
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.50.11 Subject: Cimzia Page: 1 of 5 Last Review Date: December 8, 2017 Cimzia Description Cimzia (certolizumab
Biologic Immunomodulators Prior Authorization with Quantity Limit Program Summary
 Biologic Immunomodulators Prior Authorization with Quantity Limit Program Summary Biologic Immunomodulators Prior Authorization with Quantity Limit (with a preferred option) OBJECTIVE The intent of the
Biologic Immunomodulators Prior Authorization with Quantity Limit Program Summary Biologic Immunomodulators Prior Authorization with Quantity Limit (with a preferred option) OBJECTIVE The intent of the
Cosentyx. Cosentyx (secukinumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.90.11 Subject: Cosentyx Page: 1 of 7 Last Review Date: September 20, 2018 Cosentyx Description Cosentyx
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.90.11 Subject: Cosentyx Page: 1 of 7 Last Review Date: September 20, 2018 Cosentyx Description Cosentyx
Cimzia. Cimzia (certolizumab pegol) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Cimzia Page: 1 of 5 Last Review Date: March 17, 2017 Cimzia Description Cimzia (certolizumab pegol)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Cimzia Page: 1 of 5 Last Review Date: March 17, 2017 Cimzia Description Cimzia (certolizumab pegol)
Regulatory Status FDA-approved indication: Orencia is a selective T cell co-stimulation modulator indicated for: (1)
") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Orencia Page: 1 of 9 Last Review Date: September 20, 2018 Orencia Description Orencia (abatacept)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Orencia Page: 1 of 9 Last Review Date: September 20, 2018 Orencia Description Orencia (abatacept)
Clinical Policy: Certolizumab (Cimzia) Reference Number: PA.CP.PHAR.247 Effective Date: 01/18 Last Review Date: 08/17 Line of Business: Medicaid
 Reference Number: PA.CP.PHAR.247 Effective Date: 01/18 Last Review Date: 08/17 Line of Business: Medicaid") Clinical Policy: (Cimzia) Reference Number: PA.CP.PHAR.247 Effective Date: 01/18 Last Review Date: 08/17 Line of Business: Medicaid Coding Implications Revision Log Description (Cimzia ) is a tumor necrosis
Clinical Policy: (Cimzia) Reference Number: PA.CP.PHAR.247 Effective Date: 01/18 Last Review Date: 08/17 Line of Business: Medicaid Coding Implications Revision Log Description (Cimzia ) is a tumor necrosis
Remicade (infliximab), Inflectra (infliximab-dyyb), Renflexis (infliximababda)
, Inflectra (infliximab-dyyb), Renflexis (infliximababda)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.50.02 Subject: Infliximab Page: 1 of 13 Last Review Date: December 8, 2017 Infliximab Description Remicade
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.50.02 Subject: Infliximab Page: 1 of 13 Last Review Date: December 8, 2017 Infliximab Description Remicade
Coverage Criteria: Express Scripts, Inc. monograph dated 12/15/ months or as otherwise noted by indication
 BENEFIT DESCRIPTION AND LIMITATIONS OF COVERAGE ITEM: PRODUCT LINES: COVERED UNDER: DESCRIPTION: CPT/HCPCS Code: Company Supplying: Setting: Kineret (anakinra subcutaneous injection) Commercial HMO/PPO/CDHP
BENEFIT DESCRIPTION AND LIMITATIONS OF COVERAGE ITEM: PRODUCT LINES: COVERED UNDER: DESCRIPTION: CPT/HCPCS Code: Company Supplying: Setting: Kineret (anakinra subcutaneous injection) Commercial HMO/PPO/CDHP
Immune Modulating Drugs Prior Authorization Request Form
 Patient: HPHC member ID #: Requesting provider: Phone: Servicing provider: Diagnosis: Contact for questions (name and phone #): Projected start and end date for requested Requesting provider NPI: Fax:
Patient: HPHC member ID #: Requesting provider: Phone: Servicing provider: Diagnosis: Contact for questions (name and phone #): Projected start and end date for requested Requesting provider NPI: Fax:
Xeljanz. Xeljanz, Xeljanz XR (tofacitinib) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.24 Subject: Xeljanz Page: 1 of 6 Last Review Date: March 16, 2018 Xeljanz Description Xeljanz, Xeljanz
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.24 Subject: Xeljanz Page: 1 of 6 Last Review Date: March 16, 2018 Xeljanz Description Xeljanz, Xeljanz
Otezla. Otezla (apremilast) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Otezla Page: 1 of 5 Last Review Date: March 16, 2018 Otezla Description Otezla (apremilast) Background
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Otezla Page: 1 of 5 Last Review Date: March 16, 2018 Otezla Description Otezla (apremilast) Background
CIMZIA (certolizumab pegol)
") Pre - PA Allowance None Prior-Approval Requirements Age Diagnoses 18 years of age or older Patient must have ONE of the following: 1. Moderate to severe Crohn s Disease (CD) a. Inadequate response, intolerance
Pre - PA Allowance None Prior-Approval Requirements Age Diagnoses 18 years of age or older Patient must have ONE of the following: 1. Moderate to severe Crohn s Disease (CD) a. Inadequate response, intolerance
Prior Authorization Conditions for Approval of Humira (adalimumab) Website Form Submit request via: Fax
 Website Form Submit request via: Fax") Prior Authorization Conditions for Approval of Humira (adalimumab) Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 All requests for Humira (adalimumab) require a prior
Prior Authorization Conditions for Approval of Humira (adalimumab) Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 All requests for Humira (adalimumab) require a prior
Inflectra (infliximab-dyyb), Remicade (infliximab), Renflexis (infliximab-abda) DRUG CG-DRUG-64
, Remicade (infliximab), Renflexis (infliximab-abda) DRUG CG-DRUG-64") Inflectra (infliximab-dyyb), Remicade (infliximab), Renflexis (infliximab-abda) DRUG.00002 CG-DRUG-64 Override(s) Prior Authorization *Washington Medicaid See State Specific Mandates Medications Inflectra
Inflectra (infliximab-dyyb), Remicade (infliximab), Renflexis (infliximab-abda) DRUG.00002 CG-DRUG-64 Override(s) Prior Authorization *Washington Medicaid See State Specific Mandates Medications Inflectra
Regulatory Status FDA-approved indication: Humira and Amjevita are tumor necrosis factor (TNF) blockers indicated for the treatment of: (2-3)
 blockers indicated for the treatment of: (2-3)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.29 Subject: Humira Page: 1 of 10 Last Review Date: June 22, 2017 Humira Description Humira (adalimumab),
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.29 Subject: Humira Page: 1 of 10 Last Review Date: June 22, 2017 Humira Description Humira (adalimumab),
Infliximab/Infliximab-dyyb DRUG.00002
 Infliximab/Infliximab-dyyb DRUG.00002 Override(s) Prior Authorization Step Therapy Medications Remicade (infliximab) Inflectra (inflectra-dyyb) Approval Duration 1 year Comment Intravenous administration
Infliximab/Infliximab-dyyb DRUG.00002 Override(s) Prior Authorization Step Therapy Medications Remicade (infliximab) Inflectra (inflectra-dyyb) Approval Duration 1 year Comment Intravenous administration
Humira (adalimumab) DRUG.00002
 DRUG.00002") Humira (adalimumab) DRUG.00002 Override(s) Prior Authorization Quantity Limit Approval Duration 1 year Medications Humira 10 mg/0.2 ml syringe Humira pediatric Crohn s Disease starter pack 40 mg/0.8 ml
Humira (adalimumab) DRUG.00002 Override(s) Prior Authorization Quantity Limit Approval Duration 1 year Medications Humira 10 mg/0.2 ml syringe Humira pediatric Crohn s Disease starter pack 40 mg/0.8 ml
Clinical Policy: Abatacept (Orencia) Reference Number: ERX.SPA.123 Effective Date:
 Reference Number: ERX.SPA.123 Effective Date:") Clinical Policy: (Orencia) Reference Number: ERX.SPA.123 Effective Date: 10.01.16 Last Review Date: 05.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Orencia) Reference Number: ERX.SPA.123 Effective Date: 10.01.16 Last Review Date: 05.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Actemra. Actemra (tocilizumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.12 Subject: Actemra Page: 1 of 13 Last Review Date: September 20, 2018 Actemra Description Actemra
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.12 Subject: Actemra Page: 1 of 13 Last Review Date: September 20, 2018 Actemra Description Actemra
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: abatacept_orencia 4/2008 2/2018 2/2019 2/2018 Description of Procedure or Service Abatacept (Orencia ), a
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: abatacept_orencia 4/2008 2/2018 2/2019 2/2018 Description of Procedure or Service Abatacept (Orencia ), a
ADALIMUMAB Generic Brand HICL GCN Exception/Other ADALIMUMAB HUMIRA GUIDELINES FOR USE INITIAL CRITERIA (NOTE: FOR RENEWAL CRITERIA SEE BELOW)
") Generic Brand HICL GCN Exception/Other ADALIMUMAB HUMIRA 24800 GUIDELINES FOR USE INITIAL CRITERIA (NOTE: FOR RENEWAL CRITERIA SEE BELOW) 1. Does the patient have a diagnosis of moderate to severe rheumatoid
Generic Brand HICL GCN Exception/Other ADALIMUMAB HUMIRA 24800 GUIDELINES FOR USE INITIAL CRITERIA (NOTE: FOR RENEWAL CRITERIA SEE BELOW) 1. Does the patient have a diagnosis of moderate to severe rheumatoid
Clinical Policy: Etanercept (Enbrel) Reference Number: PA.CP.PHAR.250 Effective Date: 01/18 Last Review Date: 08/17 Line of Business: Medicaid
 Reference Number: PA.CP.PHAR.250 Effective Date: 01/18 Last Review Date: 08/17 Line of Business: Medicaid") Clinical Policy: (Enbrel) Reference Number: PA.CP.PHAR.250 Effective Date: 01/18 Last Review Date: 08/17 Line of Business: Medicaid Coding Implications Revision Log Description (Enbrel ) is tumor necrosis
Clinical Policy: (Enbrel) Reference Number: PA.CP.PHAR.250 Effective Date: 01/18 Last Review Date: 08/17 Line of Business: Medicaid Coding Implications Revision Log Description (Enbrel ) is tumor necrosis
Remicade. Remicade (infliximab), Inflectra (infliximab-dyyb) Description
, Inflectra (infliximab-dyyb) Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.50.02 Subsection: Gastrointestinal nts Original Policy Date: May 20, 2011 Subject: Remicade Page: 1 of
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.50.02 Subsection: Gastrointestinal nts Original Policy Date: May 20, 2011 Subject: Remicade Page: 1 of
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Infliximab (Remicade), Infliximab-dyyb (Inflectra), and Infliximab-abda (Renflexis) Reference Number: ERX.SPA.160 Effective Date: 10.01.16 Last Review Date: 05.18 Revision Log See Important
Clinical Policy: Infliximab (Remicade), Infliximab-dyyb (Inflectra), and Infliximab-abda (Renflexis) Reference Number: ERX.SPA.160 Effective Date: 10.01.16 Last Review Date: 05.18 Revision Log See Important
Remicade (infliximab) Inflectra (infliximab-dyyb) Renflexis (infliximab-abda)
 Inflectra (infliximab-dyyb) Renflexis (infliximab-abda)") DRUG POLICY BENEFIT APPLICATION Remicade (infliximab) Inflectra (infliximab-dyyb) Renflexis (infliximab-abda) Benefit determinations are based on the applicable contract language in effect at the time
DRUG POLICY BENEFIT APPLICATION Remicade (infliximab) Inflectra (infliximab-dyyb) Renflexis (infliximab-abda) Benefit determinations are based on the applicable contract language in effect at the time
INFLIXIMAB Remicade (infliximab), Inflectra (infliximab-dyyb), Renflexis (infliximab-abda)
, Inflectra (infliximab-dyyb), Renflexis (infliximab-abda)") RATIONALE FOR INCLUSION IN PA PROGRAM Background Remicade, Renflexis and Inflectra are tumor necrosis factor (TNFα) blockers. Tumor necrosis factor is an endogenous protein that regulates a number of physiologic
RATIONALE FOR INCLUSION IN PA PROGRAM Background Remicade, Renflexis and Inflectra are tumor necrosis factor (TNFα) blockers. Tumor necrosis factor is an endogenous protein that regulates a number of physiologic
Drugs and Applicable Coding: J-code: Enbrel-J1438; Humira-J0135; Remicade-J1745; Inflectra-Q5102; Cimzia-J0718; Simponi-J1602 Renflexis - pending
 Policy Subject: Anti-TNF Agents Policy Number: SHS PBD16 Category: Rheumatology & Autoimmune Policy Type: Medical Pharmacy Department: Pharmacy Product (check all that apply): Group HMO/POS Individual
Policy Subject: Anti-TNF Agents Policy Number: SHS PBD16 Category: Rheumatology & Autoimmune Policy Type: Medical Pharmacy Department: Pharmacy Product (check all that apply): Group HMO/POS Individual
MEDICAL COVERAGE GUIDELINES ORIGINAL EFFECTIVE DATE: 04/09/18 SECTION: DRUGS LAST REVIEW DATE: LAST CRITERIA REVISION DATE: 09/05/18 ARCHIVE DATE:
 ILARIS (canakinumab) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
ILARIS (canakinumab) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
Corporate Medical Policy
 Corporate Medical Policy Infliximab, Infliximab-dyyb, Infliximab-abda File Name: Origination: Last CAP Review: Next CAP Review: Last Review: infliximab 5/2002 2/2018 2/2019 7/2018 Description of Procedure
Corporate Medical Policy Infliximab, Infliximab-dyyb, Infliximab-abda File Name: Origination: Last CAP Review: Next CAP Review: Last Review: infliximab 5/2002 2/2018 2/2019 7/2018 Description of Procedure
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Biologic Immunomodulators Therapy Page 1 of 26 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Biologic Immunomodulators Therapy (Pharmacy Benefit Only) Prime Therapeutics
Biologic Immunomodulators Therapy Page 1 of 26 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Biologic Immunomodulators Therapy (Pharmacy Benefit Only) Prime Therapeutics
Remicade. Remicade (infliximab), Inflectra (infliximab-dyyb) Description
, Inflectra (infliximab-dyyb) Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Remicade Page: 1 of 9 Last Review Date: June 22, 2017 Remicade Description Remicade (infliximab),
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Remicade Page: 1 of 9 Last Review Date: June 22, 2017 Remicade Description Remicade (infliximab),
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 1041-8 Program Prior Authorization/Notification Medication Humira (adalimumab) P&T Approval Date 1/2007, 6/2008, 4/2009, 6/2009,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 1041-8 Program Prior Authorization/Notification Medication Humira (adalimumab) P&T Approval Date 1/2007, 6/2008, 4/2009, 6/2009,
Cimzia (certolizumab pegol)
") DRUG POLICY BENEFIT APPLICATION Cimzia (certolizumab pegol) Benefit determinations are based on the applicable contract language in effect at the time the services were rendered. Exclusions, limitations
DRUG POLICY BENEFIT APPLICATION Cimzia (certolizumab pegol) Benefit determinations are based on the applicable contract language in effect at the time the services were rendered. Exclusions, limitations
Xeljanz (tofacitinib), Xeljanz XR (tofacitinib extended-release)
, Xeljanz XR (tofacitinib extended-release)") Market DC Xeljanz (tofacitinib), Xeljanz XR (tofacitinib extended-release) Override(s) Prior Authorization Quantity Limit Medications Xeljanz (tofacitinib) Approval Duration 1 year Quantity Limit May be
Market DC Xeljanz (tofacitinib), Xeljanz XR (tofacitinib extended-release) Override(s) Prior Authorization Quantity Limit Medications Xeljanz (tofacitinib) Approval Duration 1 year Quantity Limit May be
Drug Effectiveness Review Project Summary Report Biologics (Targeted Immune Modulators)
") Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Infliximab Remicade (infliximab) Inflectra (infliximab-dyyb) Renflexis (infliximab-abda)
 Inflectra (infliximab-dyyb) Renflexis (infliximab-abda)") Infliximab Remicade (infliximab) Inflectra (infliximab-dyyb) Renflexis (infliximab-abda) Line(s) of Business: HMO; PPO; QUEST Integration Akamai Advantage Original Effective Date: 11/18/2003 Current Effective
Infliximab Remicade (infliximab) Inflectra (infliximab-dyyb) Renflexis (infliximab-abda) Line(s) of Business: HMO; PPO; QUEST Integration Akamai Advantage Original Effective Date: 11/18/2003 Current Effective
ACTEMRA (tocilizumab)
") Pre - PA Allowance None Prior-Approval Requirements Diagnoses Patient must have ONE of the following: 1. Active Polyarticular Juvenile Idiopathic Arthritis (PJIA) b. Patient has an intolerance or has experienced
Pre - PA Allowance None Prior-Approval Requirements Diagnoses Patient must have ONE of the following: 1. Active Polyarticular Juvenile Idiopathic Arthritis (PJIA) b. Patient has an intolerance or has experienced
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: infliximab_remicade 5/2002 2/2017 2/2018 2/2017 Description of Procedure or Service Infliximab (REMICADE
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: infliximab_remicade 5/2002 2/2017 2/2018 2/2017 Description of Procedure or Service Infliximab (REMICADE
Remicade (infliximab) DRUG.00002
 DRUG.00002") Applicability/Effective Date *- Florida Healthy Kids Remicade (infliximab) DRUG.00002 Override(s) Prior Authorization Step Therapy Medications Remicade (infliximab) Approval Duration 1 year Comment Intravenous
Applicability/Effective Date *- Florida Healthy Kids Remicade (infliximab) DRUG.00002 Override(s) Prior Authorization Step Therapy Medications Remicade (infliximab) Approval Duration 1 year Comment Intravenous
certolizumab pegol (Cimzia )
") Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
ORENCIA (ABATACEPT) INJECTION FOR INTRAVENOUS INFUSION
 INJECTION FOR INTRAVENOUS INFUSION") UnitedHealthcare Community Plan Medical Benefit Drug Policy ORENCIA (ABATACEPT) INJECTION FOR INTRAVENOUS INFUSION Policy Number: CS2018D0039J Effective Date: March 1, 2018 Table of Contents Page INSTRUCTIONS
UnitedHealthcare Community Plan Medical Benefit Drug Policy ORENCIA (ABATACEPT) INJECTION FOR INTRAVENOUS INFUSION Policy Number: CS2018D0039J Effective Date: March 1, 2018 Table of Contents Page INSTRUCTIONS
HARVARD PILGRIM HEALTH CARE RECOMMENDED MEDICATION REQUEST GUIDELINES HUMIRA PEDIATRIC
 Generic Brand HICL GCN Exception/Other ADALIMUMAB HUMIRA 24800 HUMIRA PEDIATRIC GUIDELINES FOR USE INITIAL CRITERIA (NOTE: FOR RENEWAL CRITERIA SEE BELOW) 1. Is the patient currently taking Humira? If
Generic Brand HICL GCN Exception/Other ADALIMUMAB HUMIRA 24800 HUMIRA PEDIATRIC GUIDELINES FOR USE INITIAL CRITERIA (NOTE: FOR RENEWAL CRITERIA SEE BELOW) 1. Is the patient currently taking Humira? If
Regulatory Status FDA-approved indication: Humira and Amjevita are tumor necrosis factor (TNF) blockers indicated for the treatment of: (2-3)
 blockers indicated for the treatment of: (2-3)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.29 Subject: Humira Page: 1 of 13 Last Review Date: September 20, 2018 Humira Description Humira (adalimumab),
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.29 Subject: Humira Page: 1 of 13 Last Review Date: September 20, 2018 Humira Description Humira (adalimumab),
DRAFT. Therapeutic Class Code: D6A, S2J, S2M, S2Q, Z2U, Z2Z, S2Z, L1A, S2V, Z2V, D6K Therapeutic Class Description: Injectable Immunomodulators
 AFT Therapeutic Class Code: D6A, S2J, S2M, S2Q, Z2U, Z2Z, S2Z, L1A, S2V, Z2V, D6K Therapeutic Class Description: Injectable Immunomodulators Medication Generic Code Number(s) NDC Number(s) Actemra SQ 35486
AFT Therapeutic Class Code: D6A, S2J, S2M, S2Q, Z2U, Z2Z, S2Z, L1A, S2V, Z2V, D6K Therapeutic Class Description: Injectable Immunomodulators Medication Generic Code Number(s) NDC Number(s) Actemra SQ 35486
Drug Class Review Targeted Immune Modulators
 Drug Class Review Targeted Immune Modulators Final Update 5 Report June 2016 The purpose of reports is to make available information regarding the comparative clinical effectiveness and harms of different
Drug Class Review Targeted Immune Modulators Final Update 5 Report June 2016 The purpose of reports is to make available information regarding the comparative clinical effectiveness and harms of different
First Name. Specialty: Fax. First Name DOB: Duration:
 Prescriber Information Last ame: First ame DEA/PI: Specialty: Phone - - Fax - - Member Information Last ame: First ame Member ID umber DOB: - - Medication Information: Drug ame and Strength: Diagnosis:
Prescriber Information Last ame: First ame DEA/PI: Specialty: Phone - - Fax - - Member Information Last ame: First ame Member ID umber DOB: - - Medication Information: Drug ame and Strength: Diagnosis:
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Biologic Immunomodulators Therapy Page 1 of 34 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Biologic Immunomodulators Therapy (Pharmacy Benefit Only) Prime Therapeutics
Biologic Immunomodulators Therapy Page 1 of 34 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Biologic Immunomodulators Therapy (Pharmacy Benefit Only) Prime Therapeutics
Carelirst.+.V Family of health care plans
 Carelirst.+.V Family of health care plans CVS Caremark POLICY Document for ACTEMRA The overall objective of this policy is to support the appropriate and cost effective use of the medication, specific
Carelirst.+.V Family of health care plans CVS Caremark POLICY Document for ACTEMRA The overall objective of this policy is to support the appropriate and cost effective use of the medication, specific
Regulatory Status FDA-approved indication: Humira and Amjevita are tumor necrosis factor (TNF) blockers indicated for the treatment of: (2-3)
 blockers indicated for the treatment of: (2-3)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.29 Subject: Humira Page: 1 of 14 Last Review Date: June 22, 2018 Humira Description Humira (adalimumab),
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.29 Subject: Humira Page: 1 of 14 Last Review Date: June 22, 2018 Humira Description Humira (adalimumab),
HARVARD PILGRIM HEALTH CARE RECOMMENDED MEDICATION REQUEST GUIDELINES
 Generic Brand HICL GCN Exception/Other GOLIMUMAB SIMPONI 22533, 22536, 34697, 35001 ROUTE = SUBCUTANE. GUIDELINES FOR USE INITIAL CRITERIA (NOTE: FOR RENEWAL CRITERIA SEE BELOW) 1. Is the request for a
Generic Brand HICL GCN Exception/Other GOLIMUMAB SIMPONI 22533, 22536, 34697, 35001 ROUTE = SUBCUTANE. GUIDELINES FOR USE INITIAL CRITERIA (NOTE: FOR RENEWAL CRITERIA SEE BELOW) 1. Is the request for a
Prior Authorization Conditions for Approval of Enbrel (etanercept) Website Form Submit request via: Fax
 Website Form Submit request via: Fax") Prior Authorization Conditions for Approval of Enbrel (etanercept) Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 All requests for Enbrel (etanercept) require a prior
Prior Authorization Conditions for Approval of Enbrel (etanercept) Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 All requests for Enbrel (etanercept) require a prior
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2018 P 1017-7 Program Prior Authorization/Notification Medication Cimzia (certolizumab) P&T Approval Date 1/2007, 6/2008, 4/2009, 6/2009,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2018 P 1017-7 Program Prior Authorization/Notification Medication Cimzia (certolizumab) P&T Approval Date 1/2007, 6/2008, 4/2009, 6/2009,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2018 P 1097-7 Program Prior Authorization/Notification Medication *Stelara (ustekinumab) *This program applies to the subcutaneous formulation
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2018 P 1097-7 Program Prior Authorization/Notification Medication *Stelara (ustekinumab) *This program applies to the subcutaneous formulation
SIMPONI ARIA (GOLIMUMAB) INJECTION FOR INTRAVENOUS INFUSION
 INJECTION FOR INTRAVENOUS INFUSION") UnitedHealthcare Commercial Medical Benefit Drug Policy SIMPONI ARIA (GOLIMUMAB) INJECTION FOR INTRAVENOUS INFUSION Policy Number: PHA031 Effective Date: March 1, 2019 Table of Contents Page COVERAGE RATIONALE...
UnitedHealthcare Commercial Medical Benefit Drug Policy SIMPONI ARIA (GOLIMUMAB) INJECTION FOR INTRAVENOUS INFUSION Policy Number: PHA031 Effective Date: March 1, 2019 Table of Contents Page COVERAGE RATIONALE...
Fml Limits. Azathioprine (Imuran) 50mg, 75mg, 100mg - $26.85 Cyclosporine, 25mg, 100mg. $ Leflunomide (Arava) 10mg Tablet - $144.
 50mg, 75mg, 100mg - $26.85 Cyclosporine, 25mg, 100mg. $ Leflunomide (Arava) 10mg Tablet - $144.") MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Rheumatoid Arthritis (RA) P&T DATE: 2/15/2017 CLASS: Rheumatology/Anti-inflammatory Disorders REVIEW HISTORY 2/16, 5/15,
MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Rheumatoid Arthritis (RA) P&T DATE: 2/15/2017 CLASS: Rheumatology/Anti-inflammatory Disorders REVIEW HISTORY 2/16, 5/15,
Clinical Policy: Certolizumab (Cimzia) Reference Number: ERX.SPA.167 Effective Date:
 Reference Number: ERX.SPA.167 Effective Date:") Clinical Policy: (Cimzia) Reference Number: ERX.SPA.167 Effective Date: 10.01.16 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Cimzia) Reference Number: ERX.SPA.167 Effective Date: 10.01.16 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: Certolizumab (Cimzia) Reference Number: ERX.SPA.167 Effective Date:
 Reference Number: ERX.SPA.167 Effective Date:") Clinical Policy: (Cimzia) Reference Number: ERX.SPA.167 Effective Date: 1.1.16 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal information.
Clinical Policy: (Cimzia) Reference Number: ERX.SPA.167 Effective Date: 1.1.16 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal information.
Circle Yes or No Y N. [If no, skip to question 7.] 2. Does the patient have a diagnosis of ulcerative colitis? Y N. [If no, skip to question 4.
![Circle Yes or No Y N. [If no, skip to question 7.] 2. Does the patient have a diagnosis of ulcerative colitis? Y N. [If no, skip to question 4.](/thumbs/85/91758188.jpg "Circle Yes or No Y N. [If no, skip to question 7.] 2. Does the patient have a diagnosis of ulcerative colitis? Y N. [If no, skip to question 4.") 06/01/2016 Prior Authorization AETA BETTER HEALTH OF MICHIGA (MEDICAID) Humira (MI88) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign
06/01/2016 Prior Authorization AETA BETTER HEALTH OF MICHIGA (MEDICAID) Humira (MI88) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign
Regulatory Status FDA-approved indication: Humira and its biosimilars are tumor necrosis factor (TNF) blockers indicated for the treatment of: (2-5)
 blockers indicated for the treatment of: (2-5)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.29 Subject: Humira Page: 1 of 13 Last Review Date: November 30, 2018 Humira Description Humira (adalimumab),
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.29 Subject: Humira Page: 1 of 13 Last Review Date: November 30, 2018 Humira Description Humira (adalimumab),
RHEUMATOID ARTHRITIS DRUGS
 Rheumatology Biologics Criteria from the Exceptional Access Program RHEUMATOID ARTHRITIS DRUGS DRUG NAME BRS REIMBURSED DOSAGE FORM/ STRENGTH Adalimumab Humira 40 mg/0.8 syringe and 40mg/0.8 pen for Anakinra
Rheumatology Biologics Criteria from the Exceptional Access Program RHEUMATOID ARTHRITIS DRUGS DRUG NAME BRS REIMBURSED DOSAGE FORM/ STRENGTH Adalimumab Humira 40 mg/0.8 syringe and 40mg/0.8 pen for Anakinra
Pharmacy Prior Authorization
 Pharmacy Prior Authorization MERC CARE PLA (MEDICAID) Humira (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and date. Fax
Pharmacy Prior Authorization MERC CARE PLA (MEDICAID) Humira (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and date. Fax
The Medical Letter. on Drugs and Therapeutics
 The Medical Letter publications are protected by US and international copyright laws. Forwarding, copying or any other distribution of this material is strictly prohibited. For further information call:
The Medical Letter publications are protected by US and international copyright laws. Forwarding, copying or any other distribution of this material is strictly prohibited. For further information call:
Center for Evidence-based Policy
 P&T Committee Brief Targeted Immune Modulators: Comparative Drug Class Review Alison Little, MD Center for Evidence-based Policy Oregon Health & Science University 3455 SW US Veterans Hospital Road, SN-4N
P&T Committee Brief Targeted Immune Modulators: Comparative Drug Class Review Alison Little, MD Center for Evidence-based Policy Oregon Health & Science University 3455 SW US Veterans Hospital Road, SN-4N
Orencia (abatacept) DRUG.00040
 DRUG.00040") Market DC Orencia (abatacept) DRUG.00040 Override(s) Prior Authorization Quantity Limit Approval Duration 1 year Medications Comments Quantity Limit Orencia (abatacept) - AGP, VA MCD only 4 vials per 28
Market DC Orencia (abatacept) DRUG.00040 Override(s) Prior Authorization Quantity Limit Approval Duration 1 year Medications Comments Quantity Limit Orencia (abatacept) - AGP, VA MCD only 4 vials per 28
Medical Policy An Independent Licensee of the Blue Cross and Blue Shield Association
 Biologic Immunomodulators Therapy Page 1 of 28 Medical Policy An Independent Licensee of the Blue Cross and Blue Shield Association Title: See also: Biologic Immunomodulators Therapy (Pharmacy Benefit
Biologic Immunomodulators Therapy Page 1 of 28 Medical Policy An Independent Licensee of the Blue Cross and Blue Shield Association Title: See also: Biologic Immunomodulators Therapy (Pharmacy Benefit
Clinical Policy: Infliximab (Remicade, Inflectra, Renflexis) Reference Number: CP.PHAR.254
 Reference Number: CP.PHAR.254") Clinical Policy: Infliximab (Remicade, Inflectra, Renflexis) Reference Number: CP.PHAR.254 Effective Date: 07/16 Last Review Date: 07/17 Coding Implications Revision Log See Important Reminder at the end
Clinical Policy: Infliximab (Remicade, Inflectra, Renflexis) Reference Number: CP.PHAR.254 Effective Date: 07/16 Last Review Date: 07/17 Coding Implications Revision Log See Important Reminder at the end
Clinical Policy: Certolizumab (Cimzia) Reference Number: CP.PHAR.247 Effective Date: 08/16 Last Review Date: 08/17 Line of Business: Medicaid
 Reference Number: CP.PHAR.247 Effective Date: 08/16 Last Review Date: 08/17 Line of Business: Medicaid") Clinical Policy: (Cimzia) Reference Number: CP.PHAR.247 Effective Date: 08/16 Last Review Date: 08/17 Line of Business: Medicaid Coding Implications Revision Log See Important Reminder at the end of this
Clinical Policy: (Cimzia) Reference Number: CP.PHAR.247 Effective Date: 08/16 Last Review Date: 08/17 Line of Business: Medicaid Coding Implications Revision Log See Important Reminder at the end of this
Subject: Vedolizumab (Entyvio ) Infusion
 Infusion") 09-J2000-18 Original Effective Date: 09/15/14 Reviewed: 09/12/18 Revised: 01/15/19 Subject: Vedolizumab (Entyvio ) Infusion THIS MEDICAL COVERAGE GUIDELINE IS NOT AN AUTHORIZATION, CERTIFICATION, EXPLANATION
09-J2000-18 Original Effective Date: 09/15/14 Reviewed: 09/12/18 Revised: 01/15/19 Subject: Vedolizumab (Entyvio ) Infusion THIS MEDICAL COVERAGE GUIDELINE IS NOT AN AUTHORIZATION, CERTIFICATION, EXPLANATION
Drug Class Update with New Drug Evaluation: Biologics for Autoimmune Conditions
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
1. Does the patient have a diagnosis of moderate to severe polyarticular juvenile idiopathic arthritis (PJIA)?
?") Humira (adalimumab) Medication Request Form (MRF) for Healthy Indiana Plan (HIP) and Hoosier Healthwise (HHW) FAX TO: (858) 790-7100 c/o MedImpact Healthcare Systems, Inc. Attn: Prior Authorization Department
Humira (adalimumab) Medication Request Form (MRF) for Healthy Indiana Plan (HIP) and Hoosier Healthwise (HHW) FAX TO: (858) 790-7100 c/o MedImpact Healthcare Systems, Inc. Attn: Prior Authorization Department
Carefirst.+.V Family of health care plans
 Carefirst.+.V Family of health care plans CVS care mark POLICY Document for ENTYVIO The overall objective of this policy is to support the appropriate and cost effective use of the medication, specific
Carefirst.+.V Family of health care plans CVS care mark POLICY Document for ENTYVIO The overall objective of this policy is to support the appropriate and cost effective use of the medication, specific
Pharmacy Prior Authorization
 Pharmacy Prior Authorization AETA BETTER HEALTH PESLVAIA & AETA BETTER HEALTH KIDS Humira (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information,
Pharmacy Prior Authorization AETA BETTER HEALTH PESLVAIA & AETA BETTER HEALTH KIDS Humira (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information,
Regulatory Status FDA-approved indication: Orencia is a selective T cell costimulation modulator indicated for: (1)
") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.18 Subject: Orencia Page: 1 of 6 Last Review Date: December 8, 2017 Orencia Description Orencia (abatacept)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.18 Subject: Orencia Page: 1 of 6 Last Review Date: December 8, 2017 Orencia Description Orencia (abatacept)
Stelara. Stelara (ustekinumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.90.04 Subject: Stelara Page: 1 of 6 Last Review Date: December 8, 2017 Stelara Description Stelara (ustekinumab)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.90.04 Subject: Stelara Page: 1 of 6 Last Review Date: December 8, 2017 Stelara Description Stelara (ustekinumab)
Clinical Policy: Biologic DMARDs Reference Number: CP.CPA.194 Effective Date: Last Review Date: Line of Business: Commercial
 Clinical Policy: Reference Number: CP.CPA.194 Effective Date: 01.01.18 Last Review Date: 12.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important regulatory
Clinical Policy: Reference Number: CP.CPA.194 Effective Date: 01.01.18 Last Review Date: 12.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important regulatory
Regulatory Status FDA-approved indication: Enbrel and Erelzi are tumor necrosis factor (TNF) blockers indicated for the treatment of: (2-3)
 blockers indicated for the treatment of: (2-3)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.27 Subject: Enbrel Page: 1 of 8 Last Review Date: March 16, 2018 Enbrel Description Enbrel (etanercept),
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.27 Subject: Enbrel Page: 1 of 8 Last Review Date: March 16, 2018 Enbrel Description Enbrel (etanercept),