Vasculitis and the Dermatologist: General approach, pitfalls, and pearls
|
|
|
- Kristina Manning
- 6 years ago
- Views:
Transcription

1 Vasculitis and the Dermatologist: General approach, pitfalls, and pearls Robert G. Micheletti, MD Assistant Professor of Dermatology and Medicine Director, Cutaneous Vasculitis Clinic, Penn Vasculitis Center Co-Director, Inpatient Dermatology Consult Service University of Pennsylvania
2 Vasculitis Definition Inflammation and destruction of blood vessels resulting in tissue damage Diagnosis depends on characteristic clinical findings and histology clinical-pathologic correlation Clinical morphology correlates with the size of the affected blood vessels such that disorders are classified according to vessel size 2
3 Vasculitis Classification Affected Vessels Classification Subclassification Small Cutaneous small vessel (leukocytoclastic) vasculitis Small vessel vasculitis special types Idiopathic Infectious Medication exposure Inflammatory (CTD) Small and medium Cryoglobulinemic Types II and III ANCA-associated IgA Vasculitis (Henoch-Schonlein) Urticarial vasculitis Acute hemorrhagic edema of infancy Erythema elevatum diutinum EGPA (Churg-Strauss), Microscopic Polyangiitis, GPA (Wegener) Medium Polyarteritis nodosa (PAN) Benign cutaneous form Systemic form Large Temporal arteritis Takayasu arteritis 3
4 Vasculitis Classification: The size of involved vessels is predictive Using the skin exam alone, we can narrow the differential diagnosis considerably 4

5 Vasculitis Classification: The size of involved vessels is predictive Nerves: Not typically involved Nerves: Wrist or foot drop (mononeuritis multiplex) 5
6 Small Vessel Vasculitis Terminology Regardless of the terminology used, these lesions are a symptom rather than a disease entity in and of themselves In other words, to diagnose skin-limited vasculitis, one must first rule out systemic manifestations (renal, joint, GI) and underlying conditions that affect management and prognosis Patients may also start with skin-limited disease and develop other manifestations over time, necessitating close follow-up I use the term small vessel vasculitis of the skin initially 6


7 Small Vessel Vasculitis Presentation In the case of palpable purpura: The small vessel involvement accounts for the small size of the lesions Complement cascade and inflammation account for palpability and symptomatology RBC extravasation results in nonblanching purpura The effect of gravity on immune complex deposition accounts for lesion distribution Think small vessel vasculitis or overlap conditions which can affect small vessels 7

8 Small Vessel Vasculitis Presentation Absent are manifestations more typical of medium vessel vasculitis: Subcutaneous nodules Livedo reticularis Retiform purpura Larger hemorrhagic bullae More significant ulceration and necrosis If such lesions are seen, suspect medium vessel vasculitis or vasculitis overlapping small and medium vessels: Cutaneous or systemic polyarteritis nodosa ANCA-associated vasculitis Cryoglobulinemic vasculitis If there is both palpable purpura and medium vessel manifestations, suspect ANCA or Cryo vasculitis 8
9 Small Vessel Vasculitis Work-Up When a patient presents with lesions suspicious for vasculitis, initial work-up should try to answer three basic questions: 1) Are the lesions due to vasculitis? 2) Are other organ systems involved? 3) Are there findings which help establish a particular diagnosis? 9
10 Small Vessel Vasculitis Work-Up The diagnosis of vasculitis can be confirmed by biopsy showing leukocytoclasis and fibrinoid necrosis of small vessels A well-established but not old lesion (1-2 days) should be biopsied; lesions are dynamic timing and location are critical Tissue eosinophilia may suggest drug-induced vasculitis Depth or severity of inflammation may predict systemic involvement or even underlying malignancy Arch Dermatol 2006;142: Br J Dermatol 2014;171(6):
11 Small Vessel Vasculitis Work-Up Direct immunofluorescence should be performed (fresh lesion) IgA vasculitis is a special category (Henoch-Schonlein purpura) with more frequent renal, GI, and joint involvement IgM may correlate with renal involvement, or cryoglobulinemia C3 or IgG at the DEJ (lupus band test) may suggest hypocomplimentemic urticarial vasculitis and underlying SLE J Am Acad Dermatol 2010;63(6):
12 Small Vessel Vasculitis Work-Up Biopsy should be performed whenever possible; even the most astute clinician can be fooled by mimickers of vasculitis Beware path reports that have leukocytoclasis or perivascular neutrophils but not fibrinoid necrosis; read the fine print Beware mimickers with secondary vasculitis (bug bites, ulcers, trauma, neutrophilic dermatosis, etc.) Clinical-pathologic correlation is key 12
13 Small Vessel Vasculitis Differential Differential Diagnosis of Purpuric Macules and Papules: Skin-limited small vessel vasculitis IgA vasculitis Cryoglobulinemic vasculitis ANCA-associated vasculitis Arthropod bites Macular purpura due to trauma, skin fragility, or anticoagulation Platelet dysfunction or deficiency Pigmented purpuric dermatosis Cholesteral emboli Septic emboli Livedoid vasculopathy 13
14 Small Vessel Vasculitis Work-Up When a patient presents with lesions suspicious for vasculitis, initial work-up should try to answer three basic questions: 1) Are the lesions due to vasculitis? 2) Are other organ systems involved? 3) Are there findings which help establish a particular diagnosis? 14
15 Small Vessel Vasculitis Work-Up A thorough ROS and physical exam should be performed, along with basic labs and those dictated by history / exam Vasculitis may be confined to the skin, but systemic vasculitis and underlying disease states / triggers must be excluded 15

16 Small Vessel Vasculitis Etiologies 16
17 Small Vessel Vasculitis Etiologies Antibiotics, particularly B-lactams, are common culprits, but almost any drug or additive can cause vasculitis Upper respiratory infections, group A Strep, and Hepatitis C are common causes, but numerous infectious triggers are reported Determining a specific cause can be difficult Clin Pediatr 2007;46:451. J Am Acad Dermatol 1994;30(5 Pt 2):
18 Small Vessel Vasculitis Etiologies Vasculitis can also be a presenting sign of connective tissue disease, most often lupus or Sjogren syndrome Such cases may be associated with more significant internal involvement Clin Dermatol 2006;24(5): Curr Rheumatol Rep 2014;16(9):

19 Small Vessel Vasculitis Work-Up A careful history and review of systems is essential for separating patients with skin-limited vasculitis from those with more significant systemic involvement or underlying disease 19
20 Symptoms/Signs of Systemic Vasculitis Organ System Symptoms Signs Work-up Constitutional HEENT Fever, chills, sweats, weight loss, fatigue Hair loss, dry eyes/mouth, eye pain, oral/nasal ulcers, sinusitis, epistaxis Fever Iritis, sinus tenderness, otitis, lymphadenopathy CBC, ESR, CRP, ANA Cardiovascular CP, orthopnea, PND Gallop, rub, edema ECG, echo Pulmonary SOB, cough, hemoptysis, wheeze Crackles, wheeze, rhonchi Gastrointestinal Abd pain, melena, N/V Abd tenderness, hepatosplenomegaly ANCA, ophtho exam, laryngoscopy CXR Fecal occult blood, LFTs Musculoskeletal Joint pains, muscle aches Joint swelling X-ray, ultrasound Renal Hematuria, frothy urine Hypertension, lower extremity edema Neuro Paresthesias, numbness, weakness Foot/wrist drop, reflexes, sensation, proprioception BMP, UA, urine sediment, UProt/Cr Nerve conduction studies 20
21 Small Vessel Vasculitis Work-Up In most cases of small vessel vasculitis of the skin, significant systemic manifestations are unlikely Arthralgias are fairly common during flares, but frank synovitis or arthritis is rare and suggests systemic disease Other symptoms (e.g. constitutional, neurological, pulmonary) are red flags for other types of systemic vasculitis If one or more of these symptoms is present, a targeted workup should proceed to identify potentially severe extracutaneous manifestations 21
22 Small Vessel Vasculitis Work-Up No standard protocol for this workup exists (data emerging), but it should be guided by clinical signs and symptoms Most episodes are skin-limited and resolve within 3-4 weeks Not every test need be ordered in every patient Avoid ordering unnecessary tests, as false positive or irrelevant results can be confusing However, serious internal organ dysfunction does rarely occur 22
23 Most common trap Ordering too little (e.g. ignore systemic symptoms or fail to order urinalysis) Ordering too much (e.g. low-positive ANA or APLA that should never have been ordered) 23
24 Small Vessel Vasculitis Work-Up When the presentation is straightforward and ROS negative, nothing more than a CBC, BMP, and UA (with micro) may be required Of these tests, the urinalysis is most essential; the presence of glomerulonephritis is most likely to change management 24
25 Small Vessel Vasculitis Work-Up Additional indiscriminate work-up is unlikely to be helpful Review of biopsy-proven small vessel vasculitis cases: ESR/CRP are rarely normal (<10%) and therefore rarely helpful ANCA and SPEP rarely abnormal (<5%); order only when indicated Screening radiographs (CXR, CT, angio) essentially never positive 25
26 Small Vessel Vasculitis Work-Up But additional work-up is indicated when there is concern for systemic involvement or other types of vasculitis Fecal occult blood test in those with abdominal pain or GI bleed A chest x-ray or chest CT if cough or dyspnea Any other organ-specific targeted workup should proceed based on review of systems and examination By definition, if skin lesions suggestive of med or small-to-medium vessel vasculitis are present (e.g. retiform purpura), appropriate work-up for those conditions (e.g. cryo, AAV, PAN) should ensue 26
27 Small Vessel Vasculitis Work-Up For those with concerning symptoms or chronic / recurrent lesions with no obvious cause, reasonable workup includes: CBC, BMP, urinalysis, and LFTs Infectious serologies, including hepatitis B and C, HIV, antistreptolysin-o Rheumatologic workup, including ANA and RF (which screens for rheumatoid arthritis and is a surrogate for mixed cryoglobulins) Second-level tests include: SPEP / immunofixation to look for evidence of a paraprotein C3 and C4 levels, which may be low in urticarial vasculitis or systemic lupus and signal more significant systemic involvement ANCAs, which are strongly suggestive of ANCA-assoc vasculitis Cryoglobulins 27
28 Small Vessel Vasculitis Work-Up Summary: Straightforward case, negative ROS: CBC, BMP, UA w/ micro, +/- CXR and fecal occult blood Unclear trigger, other symptoms: above labs plus HBV, HCV, HIV, ASO, ANA, RF Second level tests: C3/C4, ANCA, Cryos, SPEP Any other work-up warranted by presenting signs / symptoms 28
29 Small Vessel Vasculitis Management Initial therapy (and prognosis) are dictated by the work-up: More aggressive systemic therapy is necessary in the case of renal or other organ involvement Treat / address underlying condition 29
30 Small Vessel Vasculitis Management If systemic involvement has been excluded, the treatment of skin-limited vasculitis should be symptom-focused Because most cases are minimally symptomatic and selflimited, aggressive immunosuppression is generally not advisable (I rarely use prednisone for skin-only disease) Rest and elevation Compression stockings Topical steroids for itch relief 30
31 Small Vessel Vasculitis Management Systemic therapy is indicated if severe, intractable, or recurrent (8-10% become chronic) For discomfort, ulceration, and psychosocial impact For any episode that is not self-limited and lasts longer than a few weeks, even if relatively asymptomatic Unfortunately, there is a dearth of high-quality data: Only one small RCT, for colchicine All else is case reports and expert opinion (dapsone, azathioprine, others) Adequate dose and duration of therapy are likely important Complete resolution or cure of chronic small vessel vasculitis may be elusive, but chronic systemic glucocorticoids usually not indicated 31
32 A Randomized Multicenter Study for Isolated Skin Vasculitis (ARAMIS) Colchicine, dapsone, azathioprine 32

:106-13. Autoimmun Rev 2013;12(10):1016-21.")
33 IgA Vasculitis (Henoch- Schonlein Purpura) Most common in children Viral URI or Strep pharyngitis often precede onset by 1-2w Overall, 40% due to infection Drug trigger in around 20% Consider paraneoplasia in adults (90% male) Medicine 2014;93(2): Autoimmun Rev 2013;12(10): J Am Acad Dermatol 2006;55(Suppl 5):S65-70.
34 IgA Vasculitis Management Management depends on severity of cutaneous and systemic symptoms, employing the same agents (colchicine, dapsone) Cochrane review showed no benefit of early steroids at the time of diagnosis for preventing renal complications of IgA vasculitis: Prophylactic steroids are not recommended They do ameliorate joint and abdominal pain and accelerate resolution of renal symptoms, if they develop J Pediatr 2006;149(2): Cochrane Database Syst Rev 2009;(3):CD
35 IgA Vasculitis Prognosis Prognosis is favorable but depends on severity of renal disease; lasts up to 6 months in 1/3 of cases Persistent nephropathy occurs in 8%, progressive renal failure in 1-3% 31% of adult patients experience renal insufficiency during the course of disease Those with hematuria or proteinuria should be carefully followed Medicine 2014;93(2): Lancet 2007;369(9566): Arch Dis Child 2010;95(11): J Am Soc Nephrol. 2002; 13:
36 Questions How do you treat/prevent and monitor for renal involvement in Henoch Schonlein Purpura (IgA vasculitis)? Frequent UA w/ micro and BP monitoring for at least 6 months; renal involvement usually develops within 1 month No benefit to prophylactic steroids, but are indicated if renal complications develop Lancet 2007;369(9566): Arch Dis Child 2010;95(11):
37 Urticarial Vasculitis As many as 5-10% of chronic urticaria patients Red flags : Lesions last >24 hours (not evanescent) Burn rather than itch Resolve with bruise-like marks Systemic symptoms like fever, arthralgias Lack of response to antihistamines Courtesy of Dr. Misha Rosenbach 37
38 Urticarial Vasculitis Red flags should prompt a biopsy small vessel vasculitis Work-UP: ROS and physical exam Basic labs, UA, etc. C3 and C4 levels

39 Normocomplimentemic Urticarial Vasculitis Patients with normal compliment levels: Skin-limited and selfresolving Best considered a subset of cutaneous small-vessel vasculitis 39
 Obstructive pulmonary disease (20%) GI symptoms (20%) Glomerulonephritis Hypocomplimentemic urticarial vasculitis syndrome")
40 Hypocomplimentemic Urticarial Vasculitis Patients with low C3 and C4 complement levels: Much more likely to have: Systemic lupus (>50%) Arthritis (50%) Obstructive pulmonary disease (20%) GI symptoms (20%) Glomerulonephritis Hypocomplimentemic urticarial vasculitis syndrome (HUVS)
41 Cryoglobulinemic Vasculitis (small/medium) Cryoglobulins: cold-precipitable circulating immunoglobulins Can cause vasculopathy (vascular occlusion) or vasculitis (vascular inflammation) 41

42 Cryoglobulinemic Vasculitis (small/medium) Type Composition Association Pathophys Manifestations I II III Monoclonal IgM or IgG Monoclonal IgM against Polyclonal IgG Polyclonal IgM against Polyclonal IgG Lymphoprolif. disorders HCV, HIV, HBV, autoimmune disease, also lymphoprolif. disorders Vascular occlusion / vasculopathy Vasculitis Raynaud s, retiform purpura, gangrene, acrocyanosis Palpable purpura, arthralgias, peripheral neuropathy, glomerulonephritis *Mixed cryos (Type II and III) are antibodies which bind to the Fc (crystallizable) region of other antibodies; this is referred to as rheumatoid factor activity Fc 42
 Check HCV, HIV, HBV, SPEP")
43 Cryoglobulinemic Vasculitis Rheumatoid factor (RF) is the poor man s cryos (+ in >70%) Cryoglobulins often falsely negative Draw during flare, keep warm, transport immediately, repeat if negative Complement levels usually low (90%) Check HCV, HIV, HBV, SPEP 43
44 Cryoglobulinemic Vasculitis (small/medium) Underlying infectious or autoimmune process causes B-cell stimulation and expansion, essential to disease pathogenesis Most common disease association is hepatitis C (70-90%) Half of HCV patients have circulating cryos; 15% develop symptoms Cryoglobulin-antibody immune complexes form and deposit in vessel walls, activating complement Skin, joints, and nerves most frequently involved: Hallmark is a mixed small and medium vessel vasculitis with a predilection for dependent and cold-exposed sites 44

45 Mixed small and medium vessel manifestations --palpable purpura --retiform purpura --livedo reticularis --cold-induced acrocyanosis 45
46 Questions What lab test is a good screening tool for cryo vasculitis? Rheumatoid factor (RF) Positive in almost all patients and usually highly elevated 46
47 ANCA-Associated Vasculitis (small/medium) The ANCA-associated vasculitides Granulomatosis with polyangiitis (GPA), formerly Wegener s Eosinophilic granulomatosis with polyangiitis (EGPA), formerly Churg-Strauss Micoscopic polyangiitis (MPA) have overlapping features, characteristically the pulmonary-renal syndrome of pulmonary hemorrhage and necrotizing glomerulonephritis 47
48 ANCA-Associated Vasculitis (small/medium) With the advent of ANCA testing, these diseases can be diagnosed with 85% sensitivity and 98% specificity But, ANCA testing can also be a source of confusion; it is worth reviewing the interpretation of this test 48
49 ANCA Testing Patient serum is incubated on a slide with ethanol-fixed human neutrophils Binding is measured using indirect immunofluorescence, and the staining pattern is noted by the technician 49
50 ANCA Testing The two major IF patterns associated with vasculitis are: C-ANCA, in which staining is diffuse throughout the cytoplasm P-ANCA, in which staining is perinuclear A third, atypical pattern may be seen; can be confused with P-ANCA 50
51 ANCA Testing A number of limitations: Subjective nature of visual interpretation of the IF pattern Lack of standardization and reference for normal range Staining patterns can be seen in other conditions besides vasculitis (sensitive but not specific) 51


52 ANCA Testing C-ANCA: Relatively specific for GPA and MPA P-ANCA: Can be seen in EGPA, MPA Inflammatory rheumatic disease (e.g. SLE, RA), IBD, CF, anti-gbm, and drug-induced vasculitis Atypical ANCA: Suspect drug, IBD, rheumatic disease, other Both C-ANCA and P-ANCA: Suspect drug-induced vasculitis 52
53 ANCA Testing For these reasons, positive immunofluorescence is confirmed by ELISA; these antibodies are what is really relevant in vasculitis: C-ANCA P-ANCA PR3 (proteinase 3) antibodies MPO (myeloperoxidase) antibodies ELISA is less sensitive, but more specific, higher positive predictive value Both antigens are located in the granules of neutrophils Antibodies to other antigens account for non- MPO, non-pr3 ANCAs, atypical ANCAs 53
54 ANCA Testing The optimal approach to testing is therefore to screen for ANCA with IIF and confirm positive results using PR3 and MPO ELISA When ANCAs are ordered, the lab should report back both IIF and ELISA reflexively; a positive ANCA is incomplete without ELISA results 54
55 ANCA Testing ANCAs are most useful when confirmed with ELISA, appropriate clinical features, and histology, in which case they are sensitive and specific 55



56 Granulomatosis with Polyangiitis AKA Wegener s Initial presentation (90%): rhinorrhea, severe sinusitis, etc. Courtesy of Dr. Antoine Sreih Courtesy of Dr. Antoine Sreih Courtesy of Dr. Antoine Sreih 56
 Glomerulonephritis (85%)")
 Mix of small and med vessel")
57 Granulomatosis with Polyangiitis Cough, dyspnea, and chest pain: Pulmonary infiltrates (70%) Glomerulonephritis (85%) Cutaneous findings (50%): Palpable purpura Ulcers Subcutaneous nodules (extensor surfaces) Mix of small and med vessel manifestations 57

58 Churg-Strauss nodules / PNGD Central necrosis is typical Courtesy of Dr. Douglas Pugliese
 Granulomatous vasculitis of the skin, nerves, lungs, heart, liver, spleen, kidneys, intestines 50% are ANCA negative When positive, 75% are P-ANCA / MPO Courtesy of")
59 Eosinophilic Granulomatosis with Polyangiitis AKA Churg-Strauss 1) Allergic rhinitis, nasal polyps, adult-onset asthma 2) After several years, fever and peripheral eosinophilia develop Eosinophilic pneumonia and gastroenteritis 3) Granulomatous vasculitis of the skin, nerves, lungs, heart, liver, spleen, kidneys, intestines 50% are ANCA negative When positive, 75% are P-ANCA / MPO Courtesy of Dr. Antoine Sreih 59
60 Question How do you interpret positive ANCA results? ANCA is merely an operator-dependent immunofluorescence test Positive C or P-ANCA must be confirmed by ELISA to be specific for vasculitis Discordant results suggest other causes of ANCA positivity, such as drug-induced vasculitis or IBD, should be considered 60
61 Question Does a negative ANCA exclude ANCA-associated vasculitis? 30% of MPA patients and 50% of EGPA patients are ANCA negative Up to 10% of GPA patients (particularly those with limited disease) may have negative ANCA ANCA status may change over time 61
62 Case Example The finding of medium vessel vasculitis suggests polyarteritis nodosa The patient s fever, malaise, myalgias, abdominal symptoms, and hypertension are concerning for systemic PAN 62
63
64 Case Example Laboratory work-up: CBC and CMP unremarkable HBV, HCV, HIV negative ANCA negative ESR 16, CRP <0.5 Urinalysis w/ 2-5 RBCs 64
65 Case Example What work-up would you get next? CT Angiogram (Abd/Pelvis): Subtle vascular changes: mild narrowing of proximal common hepatic and proximal splenic artery; mild dilation of the distal splenic artery; mild dilation of the distal bilateral common iliac arteries; focal mild narrowing in the proximal left common iliac Imaging (angiography) showing aneurysmal dilation and narrowing of vessels can be crucial to the diagnosis of PAN Patient begun on systemic steroids 65
66 Vasculitis Classification Affected Vessels Classification Subclassification Small Cutaneous small vessel (leukocytoclastic) vasculitis Small vessel vasculitis special types Idiopathic Infectious Medication exposure Inflammatory (CTD) Small and medium Cryoglobulinemic Types II and III ANCA-associated IgA Vasculitis (Henoch-Schonlein) Urticarial vasculitis Acute hemorrhagic edema of infancy Erythema elevatum diutinum EGPA (Churg-Strauss), Microscopic Polyangiitis, GPA (Wegener) Medium Polyarteritis nodosa (PAN) Benign cutaneous form Systemic form Large Temporal arteritis Takayasu arteritis 66
67 Medium Vessel Vasculitis (Polyarteritis Nodosa) Medium-sized arteries and veins Systemic symptoms include: Fever and weight loss (90%) Arthralgia / arthritis (75%) Peripheral neuritis (75%) with foot drop Renal involvement (50%) with hypertension GI involvement (40%) with abdominal pain, bleeding Stroke, myocardial infarction, intestinal infarction Spares the lungs 67



68 Polyarteritis Nodosa Skin lesions are seen in 60% of patients with systemic PAN medium vessel manifestations Retiform purpura Ulcers Digital necrosis Livedo reticularis 5-10mm subcutaneous nodules distributed along blood vessels Courtesy of Dr. Misha Rosenbach Biopsies be deep enough to sample medium vessels in the subcutis 68


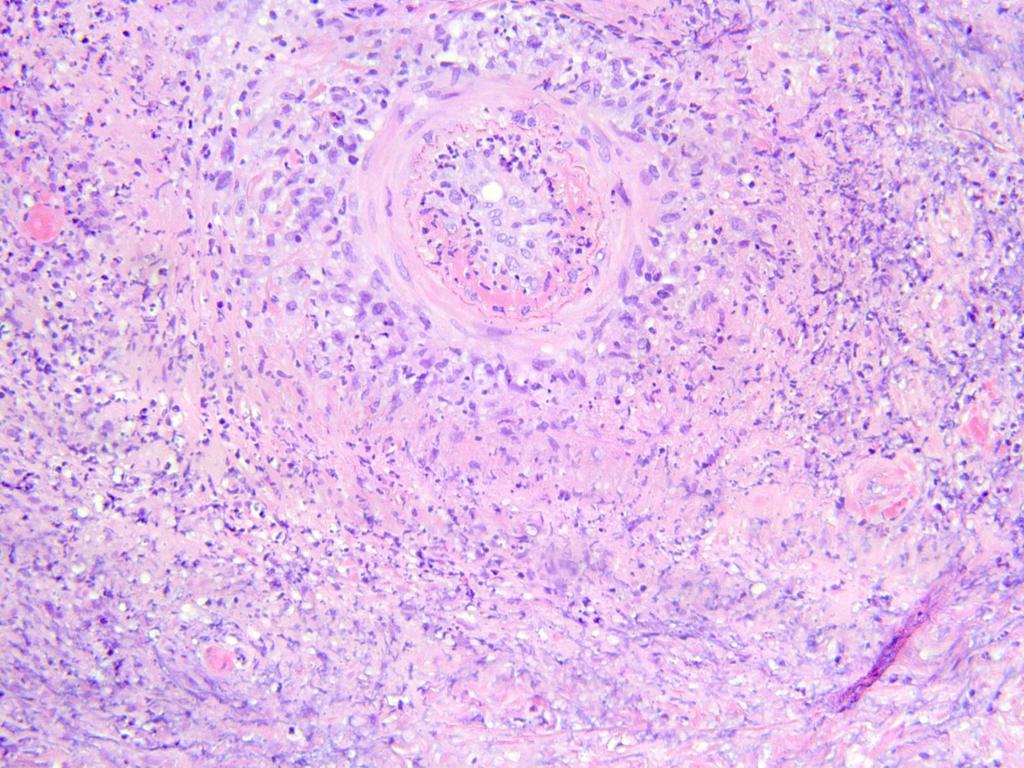
69 Polyarteritis Nodosa Fibrinoid necrosis of medium-sized vessels, thrombus, neutrophils Multiple microaneurysms on angiogram N Engl J Med 2006; 355:2574
70 Questions What are the characteristic renal manifestations of polyarteritis nodosa? Hypertension from renal artery aneurysms A lack of hematuria on urinalysis does not rule out renal PAN 70
71 Questions How does benign cutaneous PAN differ from systemic PAN? Characteristic skin lesions (livedo, nodules, ulcers), but no significant systemic manifestations Systemic renal, GI, and cardiac complications can develop over time, even >10 years later (very rare) 71
72 Summary Use the physical exam, clinical acumen to your advantage Always confirm vasculitis with biopsy; clin-path correlation is key Don t over-order labs in straightforward cases of small vessel vasculitis Let review of systems and exam guide systemic work-up Urinalysis with micro is of paramount importance Monitor UA and blood pressure periodically while active rash, especially (and frequently) in IgA vasculitis 72
73 Summary Learn to use selected laboratory tests when they are indicated Low C3 and C4 signify a worse prognosis in urticarial vasculitis RF is a good screening tool for cryo vasculitis (poor man s cryos) ANCA results must be confirmed with PR3 and MPO ELISA; they are just one piece of the diagnostic puzzle Evaluate for systemic PAN with a CT-angiogram; renal involvement manifests with hypertension, not hematuria Disease severity must guide management Vasculitis can be difficult, but a systematic clinical and diagnostic approach leads to successful diagnosis and management 73
74 A Randomized Multicenter Study for Isolated Skin Vasculitis (ARAMIS) Colchicine, dapsone, azathioprine 74
75 Clinical Transcriptomics in Systemic Vasculitis (CUTIS) Multi-center observational study to evaluate histopathology and transcriptome of cutaneous lesions in idiopathic vasculitis Describe systematically the histopathology of cutaneous vasculitis Perform gene expression profiling on lesional skin to define novel pathways to aid classification and targeted therapies 75


76 The Dermatology Foundation has supported & advanced my career.
77 Thank you Cutaneous Vasculitis Clinic, Penn Vasculitis Center University of Pennsylvania
PAEDIATRIC VASCULITIS
 PAEDIATRIC VASCULITIS Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. OUTLINE Introduction
PAEDIATRIC VASCULITIS Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. OUTLINE Introduction
Vasculitis. Edward Dwyer, M.D. Division of Rheumatology. Vasculitis
 Edward Dwyer, M.D. Division of Rheumatology VASCULITIS is a primary inflammatory disease process of the vasculature Determinants of the Clinical Manifestations of : Target organ involved Size of vessel
Edward Dwyer, M.D. Division of Rheumatology VASCULITIS is a primary inflammatory disease process of the vasculature Determinants of the Clinical Manifestations of : Target organ involved Size of vessel
Dr Rodney Itaki Lecturer Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology
 Vasculitis Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Disease Spectrum Hypersensitivity vasculitis/microscopic
Vasculitis Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Disease Spectrum Hypersensitivity vasculitis/microscopic
Mohammad Reza Shakibi M.D Kerman university of medical sciences (KMU) Shafa Hospital, Rheumatology ward
 Shafa Hospital, Rheumatology ward") VASCULITIS SYNDROMES Mohammad Reza Shakibi M.D Kerman university of medical sciences (KMU) Shafa Hospital, Rheumatology ward ILLUSTRATED CASE 1 A 56 years old lady refered me for prolonged fever, arthritis
VASCULITIS SYNDROMES Mohammad Reza Shakibi M.D Kerman university of medical sciences (KMU) Shafa Hospital, Rheumatology ward ILLUSTRATED CASE 1 A 56 years old lady refered me for prolonged fever, arthritis
Atlas of the Vasculitic Syndromes
 CHAPTER e40 Atlas of the Vasculitic Syndromes Carol A. Langford Anthony S. Fauci Diagnosis of the vasculitic syndromes is usually based upon characteristic histologic or arteriographic findings in a patient
CHAPTER e40 Atlas of the Vasculitic Syndromes Carol A. Langford Anthony S. Fauci Diagnosis of the vasculitic syndromes is usually based upon characteristic histologic or arteriographic findings in a patient
Case Presentation VASCULITIS. Case Presentation. Case Presentation. Vasculitis
 Case Presentation VASCULITIS The patient is a 24 year old woman who presented to the emergency room with left-sided weakness. She was confused and complained of a severe headache. She was noted to have
Case Presentation VASCULITIS The patient is a 24 year old woman who presented to the emergency room with left-sided weakness. She was confused and complained of a severe headache. She was noted to have
VASCULITIS. Case Presentation. Case Presentation
 VASCULITIS Case Presentation The patient is a 24 year old woman who presented to the emergency room with left-sided weakness. She was confused and complained of a severe headache. She was noted to have
VASCULITIS Case Presentation The patient is a 24 year old woman who presented to the emergency room with left-sided weakness. She was confused and complained of a severe headache. She was noted to have
SHO Teaching. Dr. Amir Bhanji Consultant Nephrologist, Q.A hospital, Portsmouth
 SHO Teaching Vasculitis Renal medicine Dr. Amir Bhanji Consultant Nephrologist, Q.A hospital, Portsmouth OUTLINE What is vasculitis Causes Classification Brief look into ANCA Associated Vasculitis (AAV)
SHO Teaching Vasculitis Renal medicine Dr. Amir Bhanji Consultant Nephrologist, Q.A hospital, Portsmouth OUTLINE What is vasculitis Causes Classification Brief look into ANCA Associated Vasculitis (AAV)
Disclosures. Rheumatological Approaches to Differential Diagnosis, Physical Examination, and Interpretation of Studies. None
 Rheumatological Approaches to Differential Diagnosis, Physical Examination, and Interpretation of Studies Sarah Goglin MD Assistant Professor of Medicine Division of Rheumatology Disclosures None 1 [footer
Rheumatological Approaches to Differential Diagnosis, Physical Examination, and Interpretation of Studies Sarah Goglin MD Assistant Professor of Medicine Division of Rheumatology Disclosures None 1 [footer
CUTANEOUS VASCULITIS. Katharine Warburton ST6 Dermatology
 CUTANEOUS VASCULITIS Katharine Warburton ST6 Dermatology AIMS Clinical cases introduction The theory Categorising cutaneous vasculitis Features presenting in the skin Mimics/pitfalls How to initially manage
CUTANEOUS VASCULITIS Katharine Warburton ST6 Dermatology AIMS Clinical cases introduction The theory Categorising cutaneous vasculitis Features presenting in the skin Mimics/pitfalls How to initially manage
Vasculitis local: systemic
 Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated 2- infectious
Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated 2- infectious
Vasculitis and Vasculitides. OMONDI OYOO Physician/Rheumatologist; Senior Lecturer, Department of Medicine University of Nairobi
 Vasculitis and Vasculitides OMONDI OYOO Physician/Rheumatologist; Senior Lecturer, Department of Medicine University of Nairobi Definition Presence of leucocytes in the vessel wall with reactive damage
Vasculitis and Vasculitides OMONDI OYOO Physician/Rheumatologist; Senior Lecturer, Department of Medicine University of Nairobi Definition Presence of leucocytes in the vessel wall with reactive damage
Annual Rheumatology & Therapeutics Review for Organizations & Societies
 Annual Rheumatology & Therapeutics Review for Organizations & Societies Update on Granulomatosis with Polyangiitis (Wegener s) Learning Objectives Identify the clinical features of granulomatosis with
Annual Rheumatology & Therapeutics Review for Organizations & Societies Update on Granulomatosis with Polyangiitis (Wegener s) Learning Objectives Identify the clinical features of granulomatosis with
Vasculitis local: systemic
 Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated inflammation
Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated inflammation
HEMORRHAGIC BULLOUS HENOCH- SCHONLEIN PURPURA: A CASE REPORT
 HEMORRHAGIC BULLOUS HENOCH- SCHONLEIN PURPURA: A CASE REPORT Nirmala Ponnuthurai, Sabeera Begum, Lee Bang Rom Paediatric Dermatology Unit, Institute of Paediatric, Hospital Kuala Lumpur, Malaysia Abstract
HEMORRHAGIC BULLOUS HENOCH- SCHONLEIN PURPURA: A CASE REPORT Nirmala Ponnuthurai, Sabeera Begum, Lee Bang Rom Paediatric Dermatology Unit, Institute of Paediatric, Hospital Kuala Lumpur, Malaysia Abstract
A number of factors point to the likelihood of a person with RA developing RV:
 What is rheumatoid vasculitis (RV)? Rheumatoid vasculitis (RV) is a rare but serious complication of rheumatoid arthritis (RA) an inflammatory disease that causes severe joint pain and damage, and can
What is rheumatoid vasculitis (RV)? Rheumatoid vasculitis (RV) is a rare but serious complication of rheumatoid arthritis (RA) an inflammatory disease that causes severe joint pain and damage, and can
Overview. = inflammation of vessel wall. Symptoms and signs depend on the tissue of which the vessels are affected
 Vasculitis (1+2) Overview = inflammation of vessel wall Symptoms and signs depend on the tissue of which the vessels are affected Often with systemic symptoms fever, myalgia, arthralgia, malaise etc. Most
Vasculitis (1+2) Overview = inflammation of vessel wall Symptoms and signs depend on the tissue of which the vessels are affected Often with systemic symptoms fever, myalgia, arthralgia, malaise etc. Most
Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis
 GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
December 6, 2010 Asthma and Rheumatic Disorders and Vasculitis
 December 6, 2010 Asthma and Rheumatic Disorders and Vasculitis Lanny J. Rosenwasser, M.D. Dee Lyons/Missouri Endowed Chair in Immunology Research Professor of Pediatrics Allergy-Immunology Division Childrens
December 6, 2010 Asthma and Rheumatic Disorders and Vasculitis Lanny J. Rosenwasser, M.D. Dee Lyons/Missouri Endowed Chair in Immunology Research Professor of Pediatrics Allergy-Immunology Division Childrens
AN OVERVIEW OF ANCA-ASSOCIATED VASCULITIS
 GRANULOMATOSIS WITH POLYANGIITIS (GPA), MICROSCOPIC POLYANGIITIS (MPA), and EOSINOPHILIC GRANULOMATOSIS WITH POLYANGIITIS (EGPA) AN OVERVIEW OF ANCA-ASSOCIATED VASCULITIS What is ANCA-associated Vasculitis?
GRANULOMATOSIS WITH POLYANGIITIS (GPA), MICROSCOPIC POLYANGIITIS (MPA), and EOSINOPHILIC GRANULOMATOSIS WITH POLYANGIITIS (EGPA) AN OVERVIEW OF ANCA-ASSOCIATED VASCULITIS What is ANCA-associated Vasculitis?
2/23/18. Disclosures. Rheumatic Diseases of Childhood. Making Room for Rheumatology. I have nothing to disclose. James J.
 Making Room for Rheumatology James J. Nocton, MD Disclosures I have nothing to disclose Rheumatic Diseases of Childhood Juvenile Idiopathic Arthritis (JIA) Systemic Lupus Erythematosus (SLE) Juvenile Dermatomyositis
Making Room for Rheumatology James J. Nocton, MD Disclosures I have nothing to disclose Rheumatic Diseases of Childhood Juvenile Idiopathic Arthritis (JIA) Systemic Lupus Erythematosus (SLE) Juvenile Dermatomyositis
CENTRAL NERVOUS SYSTEM VASCULITIS
 What is central nervous system (CNS) vasculitis? Central nervous system (CNS) vasculitis is among a family of rare disorders characterized by inflammation of the blood vessels, which restricts blood flow
What is central nervous system (CNS) vasculitis? Central nervous system (CNS) vasculitis is among a family of rare disorders characterized by inflammation of the blood vessels, which restricts blood flow
VASCULITIC SYNDROMES. Howard L. Feinberg, D.O., F.A.C.O.I., F.A.C.R. OPSC 2018
 VASCULITIC SYNDROMES Howard L. Feinberg, D.O., F.A.C.O.I., F.A.C.R. OPSC 2018 2012 REVISED CHAPEL HILL CONSENSUS CONFERENCE Large vessel Takayasu arteritis Giant cell arteritis Medium Vessel Polyarteritis
VASCULITIC SYNDROMES Howard L. Feinberg, D.O., F.A.C.O.I., F.A.C.R. OPSC 2018 2012 REVISED CHAPEL HILL CONSENSUS CONFERENCE Large vessel Takayasu arteritis Giant cell arteritis Medium Vessel Polyarteritis
CIC Edizioni Internazionali. Cutaneous vasculitides and vasculopathies. Review. Giampiero Girolomoni Paolo Rosina. severity.
 Review Cutaneous vasculitides and vasculopathies Giampiero Girolomoni Paolo Rosina Department of Medicine Section of Dermatology University of Verona, Italy Address for correspondence: Paolo Rosina, MD
Review Cutaneous vasculitides and vasculopathies Giampiero Girolomoni Paolo Rosina Department of Medicine Section of Dermatology University of Verona, Italy Address for correspondence: Paolo Rosina, MD
The Vasculitis Syndromes
 The Vasculitis Syndromes Definition Inflammation and damage of blood vessels Single organ skin Several organ systems Primary Secondary Heterogeneity Overlap Primary Vasculitis Syndromes Wegener s granulomatosis
The Vasculitis Syndromes Definition Inflammation and damage of blood vessels Single organ skin Several organ systems Primary Secondary Heterogeneity Overlap Primary Vasculitis Syndromes Wegener s granulomatosis
Diagnostic Procedures for Vasculitis
 Diagnostic Procedures for Vasculitis Toshiharu Matsumoto, MD Clinical Professor of Department of Diagnostic Pathology Juntendo University Nerima Hospital, Tokyo, Japan Introduction In 1994, the International
Diagnostic Procedures for Vasculitis Toshiharu Matsumoto, MD Clinical Professor of Department of Diagnostic Pathology Juntendo University Nerima Hospital, Tokyo, Japan Introduction In 1994, the International
GRANULOMATOSIS WITH POLYANGIITIS
 What is granulomatosis with polyangiitis (GPA)? Granulomatosis with polyangiitis (GPA) is a form of vasculitis a family of rare disorders characterized by inflammation of the blood vessels, which can restrict
What is granulomatosis with polyangiitis (GPA)? Granulomatosis with polyangiitis (GPA) is a form of vasculitis a family of rare disorders characterized by inflammation of the blood vessels, which can restrict
ANCA associated vasculitis in China
 ANCA associated vasculitis in China Min Chen Renal Division, Peking University First Hospital, Beijing 100034, P. R. China 1 General introduction of AAV in China Disease spectrum and ANCA type Clinical
ANCA associated vasculitis in China Min Chen Renal Division, Peking University First Hospital, Beijing 100034, P. R. China 1 General introduction of AAV in China Disease spectrum and ANCA type Clinical
GIANT CELL ARTERITIS. Page 1 of 6 Reproduction of this material requires written permission of the Vasculitis Foundation. Copyright 2018.
 What is giant cell arteritis (GCA)? Giant cell arteritis (GCA) is a form of vasculitis a family of rare disorders characterized by inflammation of the blood vessels, which can restrict blood flow and damage
What is giant cell arteritis (GCA)? Giant cell arteritis (GCA) is a form of vasculitis a family of rare disorders characterized by inflammation of the blood vessels, which can restrict blood flow and damage
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A ANCA vasculitis. See Antineutrophil cytoplasmic antibody associated (ANCA) vasculitis Angiography 54 Antineutrophil cytoplasmic antibody correlation
Note: Page numbers of article titles are in boldface type. A ANCA vasculitis. See Antineutrophil cytoplasmic antibody associated (ANCA) vasculitis Angiography 54 Antineutrophil cytoplasmic antibody correlation
RARE JUVENILE PRIMARY SYSTEMIC VASCULITIS
 www.pediatric-rheumathology.printo.it RARE JUVENILE PRIMARY SYSTEMIC VASCULITIS WHAT IS IT? Vasculitis is an inflammation of blood vessels. Vasculitides cover a wide group of diseases. Primary vasculitis
www.pediatric-rheumathology.printo.it RARE JUVENILE PRIMARY SYSTEMIC VASCULITIS WHAT IS IT? Vasculitis is an inflammation of blood vessels. Vasculitides cover a wide group of diseases. Primary vasculitis
Vasculitis (Polyarteritis Nodosa, Microscopic Polyangiitis, Wegener s Granulomatosis, Henoch- Schönlein Purpura)
") Vasculitis (Polyarteritis Nodosa, Microscopic Polyangiitis, Wegener s Granulomatosis, Henoch- Schönlein Purpura) J. Charles Jennette Ronald J. Falk The kidneys are affected by a variety of systemic vasculitides
Vasculitis (Polyarteritis Nodosa, Microscopic Polyangiitis, Wegener s Granulomatosis, Henoch- Schönlein Purpura) J. Charles Jennette Ronald J. Falk The kidneys are affected by a variety of systemic vasculitides
Rheumatology Primer: What Labs and When
 Rheumatology Primer: What Labs and When Irina Konon, MD Department of Internal Medicine Division of Rheumatology Medical College of Wisconsin Disclosures None 1 Objective Discuss principles of laboratory
Rheumatology Primer: What Labs and When Irina Konon, MD Department of Internal Medicine Division of Rheumatology Medical College of Wisconsin Disclosures None 1 Objective Discuss principles of laboratory
Management of Acute Vasculitis. CMT teaching 3 rd June 2015 Caroline Wroe
 Management of Acute Vasculitis CMT teaching 3 rd June 2015 Caroline Wroe Vasculitis pub quiz Match the date with the event Dr Peter McBride, Scottish Otolaryngologist describes a disease of rapid destruction
Management of Acute Vasculitis CMT teaching 3 rd June 2015 Caroline Wroe Vasculitis pub quiz Match the date with the event Dr Peter McBride, Scottish Otolaryngologist describes a disease of rapid destruction
THE TIP OF THE ICEBERG SAMER BOLIS, DO PGY-3 LEHIGH VALLEY HEALTH NETWORK, ALLENTOWN PA
 THE TIP OF THE ICEBERG SAMER BOLIS, DO PGY-3 LEHIGH VALLEY HEALTH NETWORK, ALLENTOWN PA Case The patient is a 48 year-old female, who recently returned from a trip to Puerto Rico. She presents to the ED
THE TIP OF THE ICEBERG SAMER BOLIS, DO PGY-3 LEHIGH VALLEY HEALTH NETWORK, ALLENTOWN PA Case The patient is a 48 year-old female, who recently returned from a trip to Puerto Rico. She presents to the ED
Case Presentation. Rafid Asfar, MD
 Case Presentation Rafid Asfar, MD Introduction ANCA associated vasculitis may be localized or systemic, and can involve the eyes Ocular manifestations can occur in the absence of systemic disease in persons
Case Presentation Rafid Asfar, MD Introduction ANCA associated vasculitis may be localized or systemic, and can involve the eyes Ocular manifestations can occur in the absence of systemic disease in persons
Small Vessel Vasculitis
 Banff- Rocky Mountain Barry Kassen, MD, FRCPC,FACP Head, Division of Internal Medicine UBC/VGH/SPH Acting Head, Division of Community Internal Medicine November, 2009 Objectives 1. To understand small
Banff- Rocky Mountain Barry Kassen, MD, FRCPC,FACP Head, Division of Internal Medicine UBC/VGH/SPH Acting Head, Division of Community Internal Medicine November, 2009 Objectives 1. To understand small
EDITORIAL. Issue Seventeen, October Editorial Team. Issue Seventeen. Info link
 EDITORIAL, October 2004 Welcome to the Spring 2004 Edition of InfoLink. The feature article in this edition has been written by Dr Rodger Laurent, Head of Department, PaLMS Rheumatology Laboratory. The
EDITORIAL, October 2004 Welcome to the Spring 2004 Edition of InfoLink. The feature article in this edition has been written by Dr Rodger Laurent, Head of Department, PaLMS Rheumatology Laboratory. The
Done by: Shatha Khtoum
 Done by: Shatha Khtoum Overview Vasculitis -Vasculitis is a general term for vessel wall inflammation -Symptoms and signs depend on the tissue of which the vessels are affected. (slide 2) -There are usually
Done by: Shatha Khtoum Overview Vasculitis -Vasculitis is a general term for vessel wall inflammation -Symptoms and signs depend on the tissue of which the vessels are affected. (slide 2) -There are usually
*HSP is a common vasculitis of small vessels with cutaneous & systemic complications. Its etiology is unknown& often follows URTIs.
 BY Introduction The disease is eponymously named after Eduard heinrich Henoch (1820-1910), a German pediatrician, and his teacher Johann Lukas Schonlein (1793-1864), who described it in the 1860s. Cont
BY Introduction The disease is eponymously named after Eduard heinrich Henoch (1820-1910), a German pediatrician, and his teacher Johann Lukas Schonlein (1793-1864), who described it in the 1860s. Cont
ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS. Myriam Farah, MD, FRCPC
 ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS Myriam Farah, MD, FRCPC Clinical Assistant Professor Division of Nephrology, University of British Columbia November 2016 1. How to recognize acute
ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS Myriam Farah, MD, FRCPC Clinical Assistant Professor Division of Nephrology, University of British Columbia November 2016 1. How to recognize acute
A clinical syndrome, composed mainly of:
 Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Crescentic Glomerulonephritis (RPGN)
") Crescentic Glomerulonephritis (RPGN) Background Rapidly progressive glomerulonephritis (RPGN) is defined as any glomerular disease characterized by extensive crescents (usually >50%) as the principal histologic
Crescentic Glomerulonephritis (RPGN) Background Rapidly progressive glomerulonephritis (RPGN) is defined as any glomerular disease characterized by extensive crescents (usually >50%) as the principal histologic
Rituximab treatment for ANCA-associated vasculitis in childhood
 Rituximab treatment for ANCA-associated vasculitis in childhood DISCLOSURE I have no relevant financial relationships to disclose Katharine Moore MD Nov 14, 2012 University of Colorado School of Medicine
Rituximab treatment for ANCA-associated vasculitis in childhood DISCLOSURE I have no relevant financial relationships to disclose Katharine Moore MD Nov 14, 2012 University of Colorado School of Medicine
Vasculitides in Surgical Neuropathology Practice
 Vasculitides in Surgical Neuropathology Practice USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS
Vasculitides in Surgical Neuropathology Practice USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS
High Impact Rheumatology
 High Impact Rheumatology Systemic Lupus Erythematosus Bernard Rubin, DO MPH Case 1: History A 45-year-old woman presents with severe dyspnea and cough. She was in excellent health until 4 weeks ago when
High Impact Rheumatology Systemic Lupus Erythematosus Bernard Rubin, DO MPH Case 1: History A 45-year-old woman presents with severe dyspnea and cough. She was in excellent health until 4 weeks ago when
Small Vessel Vasculitis
 Small Vessel Vasculitis Paul A Brogan Professor of Vasculitis and Consultant Paediatric Rheumatologist Department of Rheumatology Institute of Child Health and Great Ormond St Hospital, London UK P.brogan@ucl.ac.uk
Small Vessel Vasculitis Paul A Brogan Professor of Vasculitis and Consultant Paediatric Rheumatologist Department of Rheumatology Institute of Child Health and Great Ormond St Hospital, London UK P.brogan@ucl.ac.uk
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
AUTOIMMUNE DISORDERS IN THE ACUTE SETTING
 AUTOIMMUNE DISORDERS IN THE ACUTE SETTING Diagnosis and Treatment Goals Aimee Borazanci, MD BNI Neuroimmunology Objectives Give an update on the causes for admission, clinical features, and outcomes of
AUTOIMMUNE DISORDERS IN THE ACUTE SETTING Diagnosis and Treatment Goals Aimee Borazanci, MD BNI Neuroimmunology Objectives Give an update on the causes for admission, clinical features, and outcomes of
Disclaimer. This is a broad survey and cannot cover all differential diagnoses or each condition in thorough detail
 Objectives Pediatric Infections: Differentiating Benign from Serious Eileen Klein, MD, MPH Rashes Infectious vs non-infectious Viral vs bacterial Respiratory and GI illnesses When do you treat When do
Objectives Pediatric Infections: Differentiating Benign from Serious Eileen Klein, MD, MPH Rashes Infectious vs non-infectious Viral vs bacterial Respiratory and GI illnesses When do you treat When do
Annual Rheumatology & Therapeutics Review for Organizations & Societies
 Annual Rheumatology & Therapeutics Review for Organizations & Societies Update on Granulomatosis with Polyangiitis (Wegener s) Philip Seo, MD, MHS Director, Johns Hopkins Vasculitis Center Director, Johns
Annual Rheumatology & Therapeutics Review for Organizations & Societies Update on Granulomatosis with Polyangiitis (Wegener s) Philip Seo, MD, MHS Director, Johns Hopkins Vasculitis Center Director, Johns
CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS
 CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS DR ANNIE JOJO, Dr Seethalekshmy N V, Dr Nanda Kachare DEPARTMENT OF PATHOLOGY, AMRITA INSTITUTE OF MEDICAL SCIENCES, KOCHI. 54 yrs female,
CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS DR ANNIE JOJO, Dr Seethalekshmy N V, Dr Nanda Kachare DEPARTMENT OF PATHOLOGY, AMRITA INSTITUTE OF MEDICAL SCIENCES, KOCHI. 54 yrs female,
TAKAYASU S ARTERITIS. Second-stage symptoms include:
 What is Takayasu s arteritis (TAK)? Takayasu s arteritis (TAK) is a form of vasculitis a family of rare disorders characterized by inflammation of the blood vessels, which can restrict blood flow and damage
What is Takayasu s arteritis (TAK)? Takayasu s arteritis (TAK) is a form of vasculitis a family of rare disorders characterized by inflammation of the blood vessels, which can restrict blood flow and damage
ST - segment Elevation Myocardial Infarction complicating an atypical Kawasaki disease
 ST - segment Elevation Myocardial Infarction complicating an atypical Kawasaki disease Raluca PRISECARU, Marc VINCENT, Steven VERCAUTEREN Brussels Heart Center, Brussels, Belgium Disclosure None Clinical
ST - segment Elevation Myocardial Infarction complicating an atypical Kawasaki disease Raluca PRISECARU, Marc VINCENT, Steven VERCAUTEREN Brussels Heart Center, Brussels, Belgium Disclosure None Clinical
HENOCH SCHÖNLEIN PURPURA (VASCULAR PURPURA, ANAPHYLACTOID PURPURA) IN CHILDREN Single choice tests (SC)
 IN CHILDREN Single choice tests (SC)") HENOCH HÖNLEIN PURPURA (VAULAR PURPURA, ANAPHYLACTOID PURPURA) IN CHILDREN Single choice tests () 1. Choose the type of bleeding characteristic for the Henoch Schönlein purpura (vascular purpura, anaphylactoid
HENOCH HÖNLEIN PURPURA (VAULAR PURPURA, ANAPHYLACTOID PURPURA) IN CHILDREN Single choice tests () 1. Choose the type of bleeding characteristic for the Henoch Schönlein purpura (vascular purpura, anaphylactoid
29 Glomerular disease: an overview
 29 Glomerular : an overview Renal Extra-renal Neurological changes Clinical syndromes pressure Sore throat (streptococcal) Rash Cardiac valve lesions Hemoptysis Asymptomatic or Acute Glomerulonephritis
29 Glomerular : an overview Renal Extra-renal Neurological changes Clinical syndromes pressure Sore throat (streptococcal) Rash Cardiac valve lesions Hemoptysis Asymptomatic or Acute Glomerulonephritis
A. Smržová. III. Interní klinika FN Olomouc nefrologická, revmatologická a endokrinologická
 A. Smržová III. Interní klinika FN Olomouc nefrologická, revmatologická a endokrinologická Systemic vasculitis destructive inflamatory of the walls of blood vessels. Pathologist Inflammatory destruction
A. Smržová III. Interní klinika FN Olomouc nefrologická, revmatologická a endokrinologická Systemic vasculitis destructive inflamatory of the walls of blood vessels. Pathologist Inflammatory destruction
Case Presentation. By Eman El Sharkawy Ass. Professor of cardiology Alexandria University
 Case Presentation By Eman El Sharkawy Ass. Professor of cardiology Alexandria University 6m old baby girl Past history : - At the age of 2m attack of fever, diarrhea, mouth ulcers, difficult breast feeding
Case Presentation By Eman El Sharkawy Ass. Professor of cardiology Alexandria University 6m old baby girl Past history : - At the age of 2m attack of fever, diarrhea, mouth ulcers, difficult breast feeding
Glomerular pathology in systemic disease
 Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
VASCULITIS AND VASCULOPATHY
 VASCULITIS AND VASCULOPATHY Mantosh S. Rattan @CincyKidsRad facebook.com/cincykidsrad Disclosure No relevant financial disclosures Outline Overview Referral pathways MR imaging Case examples Vasculitis
VASCULITIS AND VASCULOPATHY Mantosh S. Rattan @CincyKidsRad facebook.com/cincykidsrad Disclosure No relevant financial disclosures Outline Overview Referral pathways MR imaging Case examples Vasculitis
Vasculitis. Seth Mark Berney, MD Professor of Medicine Chief, Division of Rheumatology University of Arkansas for Medical Sciences
 Vasculitis Seth Mark Berney, MD Professor of Medicine Chief, Division of Rheumatology University of Arkansas for Medical Sciences History A 50 year old white male with a history of intravenous drug use
Vasculitis Seth Mark Berney, MD Professor of Medicine Chief, Division of Rheumatology University of Arkansas for Medical Sciences History A 50 year old white male with a history of intravenous drug use
Dr. Rai Muhammad Asghar Head of Paediatric Department BBH Rawalpindi
 Dr. Rai Muhammad Asghar Head of Paediatric Department BBH Rawalpindi Acute Post streptococcal Glomerulonephritis Sudden onset of Gross hematuria Edema Hypertension Renal insufficiency Cause of AGN Post
Dr. Rai Muhammad Asghar Head of Paediatric Department BBH Rawalpindi Acute Post streptococcal Glomerulonephritis Sudden onset of Gross hematuria Edema Hypertension Renal insufficiency Cause of AGN Post
FAQ Identifying and enrolling participants
 FAQ Identifying and enrolling participants WHO IS ELIGIBLE - CASES? Patients with a new diagnosis of primary systemic vasculitis Patients suitable as cases are over 18 years with a new presentation or
FAQ Identifying and enrolling participants WHO IS ELIGIBLE - CASES? Patients with a new diagnosis of primary systemic vasculitis Patients suitable as cases are over 18 years with a new presentation or
VCRC-OMERACT ANCA-Vasculitis Outcome Measure Initiative Comparative Outcome Measure Exercise-Training Cases
 Introduction to Training Cases The purpose of this preliminary exercise is to familiarize you with the rules and logistics of the five instruments under study. Please do not read the Training Cases until
Introduction to Training Cases The purpose of this preliminary exercise is to familiarize you with the rules and logistics of the five instruments under study. Please do not read the Training Cases until
KAWASAKI DISEASE. What is Kawasaki disease? Causes
 What is Kawasaki disease? Kawasaki disease is a form of vasculitis a family of rare disorders characterized by inflammation of the blood vessels, which can restrict blood flow and damage vital organs and
What is Kawasaki disease? Kawasaki disease is a form of vasculitis a family of rare disorders characterized by inflammation of the blood vessels, which can restrict blood flow and damage vital organs and
vasculitis Patomorfologia vasculitis (arteritis) caused by infections vasculitis (arteritis) caused by infections
 caused by infections vasculitis (arteritis) caused by infections") Patomorfologia Lecture 12 prof hab. n. med. Andrzej Marszałek VASCULITIS infectious vasculitis non-infectious causes: Aspergillus Rickettsiae vasculitis (arteritis) caused by infections Mucormycosis syphylis
Patomorfologia Lecture 12 prof hab. n. med. Andrzej Marszałek VASCULITIS infectious vasculitis non-infectious causes: Aspergillus Rickettsiae vasculitis (arteritis) caused by infections Mucormycosis syphylis
SMALL TO MEDIUM VASCULITIS: RENAL ASPECT RATANA CHAWANASUNTORAPOJ UPDATE IN INTERNAL MEDICINE 2018
 SMALL TO MEDIUM VASCULITIS: RENAL ASPECT RATANA CHAWANASUNTORAPOJ UPDATE IN INTERNAL MEDICINE 2018 OUTLINE Renal involvement in vasculitis Curr Rheumatol Rep 2013 Renal involvement in ANCA vasculitis GN***:
SMALL TO MEDIUM VASCULITIS: RENAL ASPECT RATANA CHAWANASUNTORAPOJ UPDATE IN INTERNAL MEDICINE 2018 OUTLINE Renal involvement in vasculitis Curr Rheumatol Rep 2013 Renal involvement in ANCA vasculitis GN***:
AKI Case study -Vasculitis. Sarah Mackie Renal Practice Development Nurse King s College Hospital - London
 AKI Case study -Vasculitis Sarah Mackie Renal Practice Development Nurse King s College Hospital - London What is vasculitis Vasculitis refers to inflammation of the blood vessels, including arteries,
AKI Case study -Vasculitis Sarah Mackie Renal Practice Development Nurse King s College Hospital - London What is vasculitis Vasculitis refers to inflammation of the blood vessels, including arteries,
Vasculitis Prof. Dr. med. Katharina Glatz Pathologie
 Vasculitis 08-21-2018 Prof. Dr. med. Katharina Glatz Pathologie Agenda Anatomy and histology Vasculitis: Chapel Hill Classification Examples Giant cell arteritis Single organ vasculitis Artery or Vein?
Vasculitis 08-21-2018 Prof. Dr. med. Katharina Glatz Pathologie Agenda Anatomy and histology Vasculitis: Chapel Hill Classification Examples Giant cell arteritis Single organ vasculitis Artery or Vein?
Diagnostic Tests in Rheumatic Disease: What s Old, What s New & What s Useful? COPYRIGHT
 Diagnostic Tests in Rheumatic Disease: What s Old, What s New & What s Useful? Robert H. Shmerling, M.D. Beth Israel Deaconess Medical Center Boston, MA Diagnostic Tests in Rheumatic Disease: What's Old,
Diagnostic Tests in Rheumatic Disease: What s Old, What s New & What s Useful? Robert H. Shmerling, M.D. Beth Israel Deaconess Medical Center Boston, MA Diagnostic Tests in Rheumatic Disease: What's Old,
APPROACH TO PATIENTS WITH POLYARTHRALGIA
 APPROACH TO PATIENTS WITH POLYARTHRALGIA Scott Vogelgesang, MD Division of Immunology University of Iowa No conflicts of interest DEFINITIONS Arthralgia joint pain with no evidence of inflammation Arthritis
APPROACH TO PATIENTS WITH POLYARTHRALGIA Scott Vogelgesang, MD Division of Immunology University of Iowa No conflicts of interest DEFINITIONS Arthralgia joint pain with no evidence of inflammation Arthritis
CHECK LIST FORM-MONTH 27 (Please note Month 27 is from enrolment not randomisation)
") CHECK LIST FORM-MONTH 27 (Please note Month 27 is from enrolment not randomisation) Participant Initials: Date of Birth: Were the following forms completed for this visit? Follow Up Form Done t Done BVASWG
CHECK LIST FORM-MONTH 27 (Please note Month 27 is from enrolment not randomisation) Participant Initials: Date of Birth: Were the following forms completed for this visit? Follow Up Form Done t Done BVASWG
Guideline on the clinical management of Henoch Schonlein Purpura (HSP)
") Guideline on the clinical management of Henoch Schonlein Purpura (HSP) Purpose To ensure a standardised approach in the management of children with HSP in southern Derbyshire. Scope The scope of this guideline
Guideline on the clinical management of Henoch Schonlein Purpura (HSP) Purpose To ensure a standardised approach in the management of children with HSP in southern Derbyshire. Scope The scope of this guideline
Direct immunofluorescence testing in vasculitis A single institution experience with Henoch-Schönlein purpura
 Received: 11 August 2017 Revised: 21 September 2017 Accepted: 29 September 2017 DOI: 10.1111/cup.13054 ORIGINAL ARTICLE Direct immunofluorescence testing in vasculitis A single institution experience with
Received: 11 August 2017 Revised: 21 September 2017 Accepted: 29 September 2017 DOI: 10.1111/cup.13054 ORIGINAL ARTICLE Direct immunofluorescence testing in vasculitis A single institution experience with
Scleritis LEN V KOH OD
 Scleritis LEN V KOH OD 2014 PUCO 1 Introduction A painful, destructive, and potentially blinding disorder Highly symptomatic High association with systemic disease Immunosuppresssive agents 2014 PUCO 2
Scleritis LEN V KOH OD 2014 PUCO 1 Introduction A painful, destructive, and potentially blinding disorder Highly symptomatic High association with systemic disease Immunosuppresssive agents 2014 PUCO 2
Vasculitis Update. A selective review of what s new. Dr Jonathan Akikusa MBBS FRACP
 Vasculitis Update A selective review of what s new Dr Jonathan Akikusa MBBS FRACP Consultant Paediatric Rheumatologist Royal Children s Hospital, Melbourne Honorary Research Fellow Murdoch Children s Research
Vasculitis Update A selective review of what s new Dr Jonathan Akikusa MBBS FRACP Consultant Paediatric Rheumatologist Royal Children s Hospital, Melbourne Honorary Research Fellow Murdoch Children s Research
BSD Self Assessment Workshop 7 th July 2013 CASE 27 RAC6123
 BSD Self Assessment Workshop 7 th July 2013 CASE 27 RAC6123 M55. 4/7 tender lesions on knee, legs and arms. Also iritis/ weight loss/headache, synovitis.?vasculitis. Sarcoidosis. Biopsy from left elbow
BSD Self Assessment Workshop 7 th July 2013 CASE 27 RAC6123 M55. 4/7 tender lesions on knee, legs and arms. Also iritis/ weight loss/headache, synovitis.?vasculitis. Sarcoidosis. Biopsy from left elbow
Vasculitis. Marwan Adwan. 4 th year MBBS. Consultant Rheumatologist. MBChB, MRCPI, MSc, MRCP (rheum)
") Vasculitis 4 th year MBBS Marwan Adwan MBChB, MRCPI, MSc, MRCP (rheum) Consultant Rheumatologist Case 1 A 45 man presents with 3 wk hx of fever, fatigue, malaise, abdo pain and polyarthralgia. He noticed
Vasculitis 4 th year MBBS Marwan Adwan MBChB, MRCPI, MSc, MRCP (rheum) Consultant Rheumatologist Case 1 A 45 man presents with 3 wk hx of fever, fatigue, malaise, abdo pain and polyarthralgia. He noticed
CHECK LIST FORM-SCREENING
 CHECK LIST FORM-SCREENING Participant Initials: Date of Birth: Evaluation Date: Were the following forms completed for this visit? Eligibility Form Done t Done Baseline medical History Form Done t Done
CHECK LIST FORM-SCREENING Participant Initials: Date of Birth: Evaluation Date: Were the following forms completed for this visit? Eligibility Form Done t Done Baseline medical History Form Done t Done
Clinical Case Conference Tuesday August 25, 2015 Dana Assis, MD
 Clinical Case Conference Tuesday August 25, 2015 Dana Assis, MD CC: LE swelling and pain for three weeks HPI: 71F hx HTN, DM (A1c 9.6), HFrEF (45%), asthma, OA, cryptogenic cirrhosis p/w bilateral lower
Clinical Case Conference Tuesday August 25, 2015 Dana Assis, MD CC: LE swelling and pain for three weeks HPI: 71F hx HTN, DM (A1c 9.6), HFrEF (45%), asthma, OA, cryptogenic cirrhosis p/w bilateral lower
Essential Rheumatology. Dr Ellen Bruce Consultant Rheumatologist CMFT
 Essential Rheumatology Dr Ellen Bruce Consultant Rheumatologist CMFT Saving the best for last! Apparently people recall best the first and last thing they re told. Far too difficult to include everything.
Essential Rheumatology Dr Ellen Bruce Consultant Rheumatologist CMFT Saving the best for last! Apparently people recall best the first and last thing they re told. Far too difficult to include everything.
Undifferentiated Connective Tissue Disease and Overlap Syndromes. Mark S. Box, MD
 Undifferentiated Connective Tissue Disease and Overlap Syndromes Mark S. Box, MD Overlap Syndromes As many as 25% of patients with rheumatic diseases with systemic symptoms cannot be definitely diagnosed
Undifferentiated Connective Tissue Disease and Overlap Syndromes Mark S. Box, MD Overlap Syndromes As many as 25% of patients with rheumatic diseases with systemic symptoms cannot be definitely diagnosed
Case conference. Welcome Dr. Lawrence Tierney
 Case conference Welcome Dr. Lawrence Tierney Case: 18 year-old male CC) hamatomesis, Fever and cough HPI) 1 st admission One month ago, he admitted to our hospital because of hematemesis. He had weight
Case conference Welcome Dr. Lawrence Tierney Case: 18 year-old male CC) hamatomesis, Fever and cough HPI) 1 st admission One month ago, he admitted to our hospital because of hematemesis. He had weight
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome.
 Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
ARTHRITIS FOUNDATION VASCULITIS
 ARTHRITIS FOUNDATION Registered Nonprofit Organisation - No. 002-847 NPO Helpline No: 0861 30 30 30 VASCULITIS This information leaflet is published by the Arthritis Foundation as part of our continuing
ARTHRITIS FOUNDATION Registered Nonprofit Organisation - No. 002-847 NPO Helpline No: 0861 30 30 30 VASCULITIS This information leaflet is published by the Arthritis Foundation as part of our continuing
Managing Acute Medical Problems, Birmingham Vasculitis. David Jayne. University of Cambridge
 Managing Acute Medical Problems, Birmingham 2016 Vasculitis David Jayne University of Cambridge Disclosures Astra Zeneca, Aurinia, BIOGEN, Boehringer, Chemocentryx, Genzyme/Sanofi, GSK, Lilly, Medimmune,
Managing Acute Medical Problems, Birmingham 2016 Vasculitis David Jayne University of Cambridge Disclosures Astra Zeneca, Aurinia, BIOGEN, Boehringer, Chemocentryx, Genzyme/Sanofi, GSK, Lilly, Medimmune,
Goals of this talk. Morbilliform. Common Morphologies in the Hospital 11/7/2017. Hospital Based Dermatology: Common and Tough Consult Cases
 Hospital Based Dermatology: Common and Tough Consult Cases Lindy P. Fox MD Associate Professor of Clinical Dermatology Director, Hospital Consultation Service University of California, San Francisco lindy.fox@ucsf.edu
Hospital Based Dermatology: Common and Tough Consult Cases Lindy P. Fox MD Associate Professor of Clinical Dermatology Director, Hospital Consultation Service University of California, San Francisco lindy.fox@ucsf.edu
Henoch Schonlein Purpura
 CHILDREN S SERVICES Henoch Schonlein Purpura Definition A vasculitic syndrome of small vessels classically characterised by a purpuric rash, abdominal pain, arthritis, and nephritis. Platelet count and
CHILDREN S SERVICES Henoch Schonlein Purpura Definition A vasculitic syndrome of small vessels classically characterised by a purpuric rash, abdominal pain, arthritis, and nephritis. Platelet count and
AN APPROACH TO HEMATURIA. Dr Saima Ali
 AN APPROACH TO HEMATURIA Dr Saima Ali Definition Microscopic hematuria hematuria is defined as the presence of 5 or more RBCs per high-power field in 3 of 3 consecutive centrifuged specimens obtained at
AN APPROACH TO HEMATURIA Dr Saima Ali Definition Microscopic hematuria hematuria is defined as the presence of 5 or more RBCs per high-power field in 3 of 3 consecutive centrifuged specimens obtained at
ANTI NEUTROPHIL CYTOPLASMIC ANTIBODY (ANCA) TESTING GUIDELINES
 TESTING GUIDELINES") ANTI NEUTROPHIL CYTOPLASMIC ANTIBODY (ANCA) TESTING GUIDELINES Version: 1.0 Ratified by: Clinical Biochemistry Senior Staff Group Date ratified: Name of originator/author: Director responsible for implementation:
ANTI NEUTROPHIL CYTOPLASMIC ANTIBODY (ANCA) TESTING GUIDELINES Version: 1.0 Ratified by: Clinical Biochemistry Senior Staff Group Date ratified: Name of originator/author: Director responsible for implementation:
Granulomatosis with Polyangiitis (Wegener s)
") August 2011 Granulomatosis with Polyangiitis (Wegener s) Andrew Noll, Harvard Medical School, Year III Agenda Patient presentation Overview of granulomatosis with polyangiitis (Wegener s), abbreviated
August 2011 Granulomatosis with Polyangiitis (Wegener s) Andrew Noll, Harvard Medical School, Year III Agenda Patient presentation Overview of granulomatosis with polyangiitis (Wegener s), abbreviated
Differential Diagnosis of Neuropathies and Compression. Dr Ashwin Pinto Consultant Neurologist Wessex Neurological Centre
 Differential Diagnosis of Neuropathies and Compression Dr Ashwin Pinto Consultant Neurologist Wessex Neurological Centre Outline of talk Mononeuropathies median and anterior interosseous nerve ulnar nerve
Differential Diagnosis of Neuropathies and Compression Dr Ashwin Pinto Consultant Neurologist Wessex Neurological Centre Outline of talk Mononeuropathies median and anterior interosseous nerve ulnar nerve
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
Scott Vogelgesang, MD Division of Rheumatology/Immunology University of Iowa
 Scott Vogelgesang, MD Division of Rheumatology/Immunology University of Iowa Basic Concepts ANA DsDNA Sm RNP SSA SSB RF/CCP ESR/CRP ANCA Cases Summary Rheumatology Tests Lie and Mislead! Rheumatology Rally
Scott Vogelgesang, MD Division of Rheumatology/Immunology University of Iowa Basic Concepts ANA DsDNA Sm RNP SSA SSB RF/CCP ESR/CRP ANCA Cases Summary Rheumatology Tests Lie and Mislead! Rheumatology Rally
Dr P Sigwadi 30 May 2012
 Dr P Sigwadi 30 May 2012 Introduction Haematuria Positive blood on urine dipstick 5 red blood cells/ microliter of urine Prevalence Gross haematuria ( macroscopic) 0.13 % Microscopic- 1.5% Haematuria +
Dr P Sigwadi 30 May 2012 Introduction Haematuria Positive blood on urine dipstick 5 red blood cells/ microliter of urine Prevalence Gross haematuria ( macroscopic) 0.13 % Microscopic- 1.5% Haematuria +
Revised 2017 international consensus on testing of ANCAs in granulomatosis with polyangiitis and microscopic polyangiitis.
 Revised 2017 international consensus on testing of ANCAs in granulomatosis with polyangiitis and microscopic polyangiitis. Bossuyt X, Cohen Tervaert JW, Arimura Y, Blockmans D, Flores-Suárez LF, Guillevin
Revised 2017 international consensus on testing of ANCAs in granulomatosis with polyangiitis and microscopic polyangiitis. Bossuyt X, Cohen Tervaert JW, Arimura Y, Blockmans D, Flores-Suárez LF, Guillevin
A RARE NEUROLOGICAL PRESENTATION OF SLE. Dr Yoganand M N Dr Prithvi P Nayak
 A RARE NEUROLOGICAL PRESENTATION OF SLE Dr Jayachandra Dr Yoganand M N Dr Prithvi P Nayak Presenter: Dr Shambhavi K R CHIEF COMPLAINTS A 30 year old lady hailing from Nepal presented to OPD with complaints
A RARE NEUROLOGICAL PRESENTATION OF SLE Dr Jayachandra Dr Yoganand M N Dr Prithvi P Nayak Presenter: Dr Shambhavi K R CHIEF COMPLAINTS A 30 year old lady hailing from Nepal presented to OPD with complaints
A CRP B FBC C LFT D blood culture E uric acid
 1 A 39 year old lady with rheumatoid arthritis is admitted to hospital with a hot, swollen and painful right knee. Which is the most important blood test? A CRP B FBC C LFT D blood culture E uric acid
1 A 39 year old lady with rheumatoid arthritis is admitted to hospital with a hot, swollen and painful right knee. Which is the most important blood test? A CRP B FBC C LFT D blood culture E uric acid
Dhanalakshmi.R II yr MD Stanley medical college
 Dhanalakshmi.R II yr MD Stanley medical college 10 Yr old female child - abdominal pain & vomiting for 1 day. Diffuse in nature, moderate in intensity, not related to food intake & radiates to back. No
Dhanalakshmi.R II yr MD Stanley medical college 10 Yr old female child - abdominal pain & vomiting for 1 day. Diffuse in nature, moderate in intensity, not related to food intake & radiates to back. No
Review Article. Current concepts in Anti-Neutrophil Cytoplasmic Antibody (ANCA) associated Vasculitis. Milind Aurangabadkar
 associated Vasculitis. Milind Aurangabadkar") Review Article Vidarbha Journal of Internal Medicine Volume 23 July 207 Current concepts in Anti-Neutrophil Cytoplasmic Antibody (ANCA) associated Vasculitis Milind Aurangabadkar ABSTRACT Anti-neutrophil
Review Article Vidarbha Journal of Internal Medicine Volume 23 July 207 Current concepts in Anti-Neutrophil Cytoplasmic Antibody (ANCA) associated Vasculitis Milind Aurangabadkar ABSTRACT Anti-neutrophil