Fever in Lupus. 21 st April 2014
|
|
|
- Myrtle Thomas
- 6 years ago
- Views:
Transcription
1 Fever in Lupus 21 st April 2014
2 Fever in lupus Cause of fever N= 487 % SLE fever Infection in SLE Active SLE and infection Tumor fever Miscellaneous 4 0.8
3 Crucial Question Infection or SLE or both? Opposite therapy Fatal sepsis can result with use of persistent high dose steroid in infection fever
4 Significant fever A documented temperature > 100F or 37.5C for at least 3 days



5 Define SLE fever No infection identified Diagnosis of Exclusion Follow up is must Features of active SLE Suppressed with hike in steroid No evidence of infection over next 2 weeks Physical examination and Investigations Decision may take a single OPD visit to 2 weeks
6 Case-1 F/20 Presenting complaints Fever from 3 months Cough and multiple joint pains from 2 weeks Symptoms started with cervical lymphadenopathy 8 months back FNAC s/o tuberculosis (no report available) Started on ATT but lymphnodes increased in number
7 Course After 5 months started having high grade fever associated with cough Fall in hb to 4 gm/dl 4 units PRBC Multiple small and large joint pain, swelling and EMS 1 hour 2 nd episode of fall in hb 2 unit of PRBC Reddish malar rash from 2 weeks USG abdomen Hepato-splenomegaly with multiple echogenic foci Admitted in pulmonary department d/t bilateral consolidation with pleural effusion
8 Course CT thorax showed Bilateral lower lobe and right middle lobe consolidation with b/l pleural effusion Treated with antibiotics * 3days no response By that time, ANA 4+ homogenous 1:160, Anti-ds DNA >300 IU/ml, C mg/dl, C mg/dl, TLC 3400, PCT ng/m, CRP 0.89 mg/dl, ESR 120 mm at 1 hr, Blood culture sterile
9 Transfer Started on 1 mg/kg prednisolone with antibiotic cover due to consolidation Repeat CRP 0.89 mg/dl, TLC repeated low, blood and urine culture negative Her symptoms improved, arthritis relieved, malar rash subsided, pleural effusion and chest symptoms and x-ray showed resolution in 10 days
10 Course Fever persisted high grade every 3 rd day As patient was taking 45 mg prednisolone (good amount!!) SLE fever unlikely Thoroughly evaluated with repeat cultures, Echo, USG abdomen hepatomegaly, Treated empirically with anti-malarial ACT orally Fever daily with increased frequency
11 Course Fundus showing b/l early papillo-edema, no signs of meningeal irritation CSF done normal, MRI brain normal Naprosyn 500 mg bd added, fever responded and subsided completely Likely SLE fever



12 Define Infection fever Clinically infection Culture, serology or clinical diagnosis Response to antibiotic therapy or reduction in Immuno-suppression No flare of lupus Next 4 months
13 Case-2 F/39 Diagnosed SLE 2010 minor organ At present on Azathioprine (2 mg/kg) and prednisolone 7.5 mg Presented with intermittent episodes of fever from oct 2013 Nov 2013 evaluated with admission
14 Nov 2013 No clinical localization for infection or disease activity CT Chest + abdomen normal Echo normal, CSF normal, Bone marrow normal dsdna high in 2010 is 61.2 C3 and C4 90 and 17 mg/dl ESR 20 and CRP 0.7, PCT no report TLC low 3200 Urine no pyuria but culture positive for pseudomonas, blood culture negative?sle fever steroid increased to 12.5 mg
15 Dec 2013 Non-resolving fever Gastroenterology opinion taken for liver biopsy as work-up for PUO But, then planned for a PET-CT Anti dsdna 48.6 IU/ml C3 and C4 100 and 23 mg/dl CRP 5.36 mg/dl, ESR 62 mm at 1 hour TLC low 3500 Steroid dose split to 7.5/5 mg M/E
16 Diagnosis PET-CT revealed abscess in lower pole right kidney Infection leading to fever


17 Define fever d/t both Clinical infection Culture, serology or clinical diagnosis Typical manifestations of SLE activity Response to both antibiotic therapy & increase in Immunosuppression
18 Case-3 M/ f/up SLE in remission off Azoran 1 year and 2.5 mg prdnisolone tapered from 3 months April Presented with fever, abdomen pain and loose stools and urine showing active sediments, complements low, ds DNA >200, PCT 2.10ng/ml, CRP <0.32 mg/dl, ESR 25 Developed Macrophage activation syndrome Treated with pulse steroid and 1 mg/kg prednisolone
19 After 1 month- may 2013 Fever relapse from 2 weeks with pain, swelling and redness in b/l thigh and buttock region MRI showing T2 enhancement of hamstrings, quadriceps and gluteal muscles Treated with vancomycin for 4 weeks and prednisolone reduced to 0.5 mg/kg Local symptoms improved but fever persisted with typical morning rise and decreases after morning steroid dose Steroid dose split fever subsided Complements normal, ds DNA 100, CRP/PCT not done
20 After 1 more month June 2013 Relapse of Fever 2 weeks with abdomen pain and right iliac fossa tenderness CECT abdomen multiple necrotic lymph node Started on ATT By 6 th day he developed multiple pockets of abscess in thigh and buttock region Aspirated pus positive for AFB
21 Define SLE fever No infection identified Diagnosis of Exclusion Follow up is must Features of active SLE Suppressed with hike in steroid No evidence of infection over next 2 weeks Physical examination and Investigations Decision may take a single OPD visit to 2 weeks
22 Suppressed with hike of steroid Two aspects Patient presents with fever and SLE diagnosis is made Follow up SLE patient presents with fever


23 Effect of steroid on fever in lupus Retrospective 22 patients suspected SLE fever 3 developed fatal sepsis at high dose
24 Effective steroid dose for SLE fever 80.6% in 1-5 days


25 Max ineffective steroid dose 5.3% still afebrile, 1 had MAS, 3 had lupus enceph
 13.")

26 Fever in follow up SLE patients 92 patients (60 renal and 32 non-renal) 13.2+/-8 months f/up Prednisolone 10mg in 82% of flare visits, 3 were receiving NSAIDs Fever is not associated with flare (only 1 patient)
27 Fever in follow up SLE patients 28 patients had significant fever One SLE fever - 20 mg OD 10 mg twice daily 5 had unexplained and resolved 22 had infection as a cause of fever Respiratory tract most commonly involved So, while on follow up and regular treatment, infection is much more likely to cause fever
28 Features of active SLE Normal CRP, Anti ds DNA raised, low complements, normal or low leucocyte count But does not rule out infection particularly in cases where both can co-exist!! So, is there some investigations that can look for infections in flare??
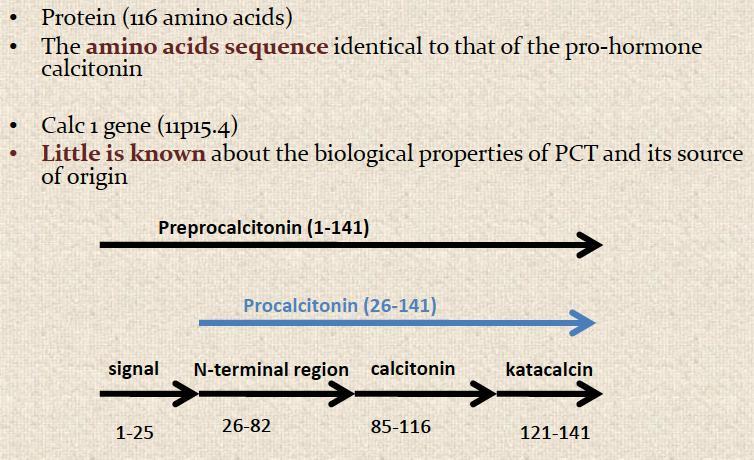
29 Pro-calcitonin
30 Pro-calcitonin (PCT) & lupus PCT levels marker for sepsis Higher (>2 ng/ml) in sepsis & septic shock Correlate with severity of sepsis Response to antibiotics Do not rise significantly in viral infections The Question - cut-off values in localized bacterial & fungal infections?
31 PCT, lupus & Infection Ann Rheum Dis Oct;60(10):988-9.
32 PCT to rule out infection Rule out = PCT of <0.17 ng/ml, NPV = 94% for infection Rule in = 100% specificity PCT>0.5 ng/ml and CRP>13 mg/dl poor sensitivity



33 CRP CRP - not elevated lupus flare Moderate rise - serositis and arthritis Levels are known to rise significantly in infections Considerable overlap But a margin to differentiate between the two
34 CRP to rule out infection CRP cutoff value 1.35 mg/dl 100% sensitive & 90% specific to detect infection
35 ROC of PCT & CRP 34 with infection and 39 with lupus flare
36 Markers of infection & flare
37 Infection and lupus


38 Infection morbidity & mortality

39 Infection & lupus
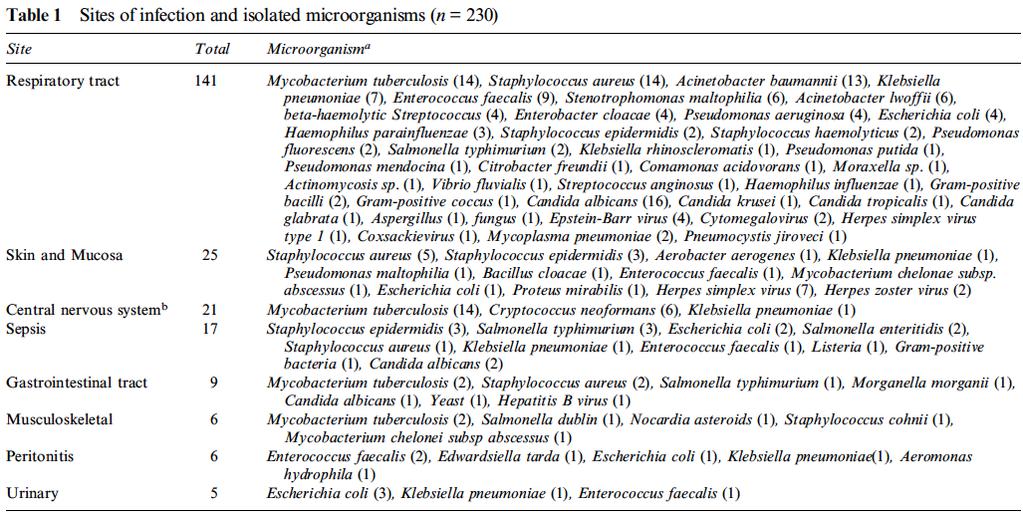
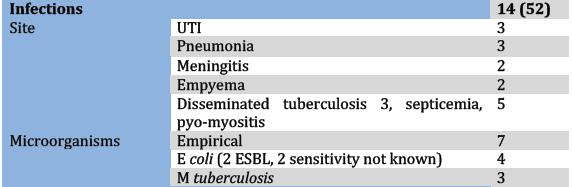
40 Sites and microorganisms
41 Summary Effective steroid dose can be > 40 mg Follow fever trends after steroid hike Follow up SLE patients infection PCT >2 ng/ml with fall on antibiotic likely infection PCT <0.17 ng/ml unlikely to be infection except viral Higher CRP infection CRP <1.35 mg/dl unlikely to be infection Features of active SLE in absence of evident infection
42 Take home message Infection is the most common cause SLE fever is diagnosis of exclusion Thank you
Systemic examination
 PROLONGED FEVER IN AN ADOLESCENT BOY Dr.Praveena Lionel, DNB PG, Dr.Kannan (HOD) Railway Hospital, Perambur History 11 yrs old adolescent boy was admitted with c/o Fever -1 wk Myalgia -1 wk Arthralgia
PROLONGED FEVER IN AN ADOLESCENT BOY Dr.Praveena Lionel, DNB PG, Dr.Kannan (HOD) Railway Hospital, Perambur History 11 yrs old adolescent boy was admitted with c/o Fever -1 wk Myalgia -1 wk Arthralgia
Case presentation. Dr REESAUL R
 Case presentation Dr REESAUL R Mr S. 25 years old Case 1 Ref on 06/ April /2006 to Chest Clinic from a private GP of Port Louis for : Cough + haemoptysis and dyspnoea Case 1(6/April/2006) Mr S Single 25
Case presentation Dr REESAUL R Mr S. 25 years old Case 1 Ref on 06/ April /2006 to Chest Clinic from a private GP of Port Louis for : Cough + haemoptysis and dyspnoea Case 1(6/April/2006) Mr S Single 25
RAPIDLY FAILING KIDNEYS. Dr Paul Johny 2 nd yr DNB Medicine Resident
 RAPIDLY FAILING KIDNEYS Dr Paul Johny 2 nd yr DNB Medicine Resident Mr Z 67yrs old Occupation : Retired officer from electricity board Chief complaints : Fever : 5 days Right lower limb swelling and pain
RAPIDLY FAILING KIDNEYS Dr Paul Johny 2 nd yr DNB Medicine Resident Mr Z 67yrs old Occupation : Retired officer from electricity board Chief complaints : Fever : 5 days Right lower limb swelling and pain
Clinical Radiological Pathological Conference
 Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
Dr. Venkateswari. R. Dr. Janani Sankar s unit Kanchi Kamakoti CHILDS Trust Hospital
 Dr. Venkateswari. R. Dr. Janani Sankar s unit Kanchi Kamakoti CHILDS Trust Hospital Acknowledgements: KKCTH Dr. Ramkumar Consultant Dermatologist Dr. Ramprakash Consultant Ophthalmologist Dr. Prasad Manne
Dr. Venkateswari. R. Dr. Janani Sankar s unit Kanchi Kamakoti CHILDS Trust Hospital Acknowledgements: KKCTH Dr. Ramkumar Consultant Dermatologist Dr. Ramprakash Consultant Ophthalmologist Dr. Prasad Manne
A RARE NEUROLOGICAL PRESENTATION OF SLE. Dr Yoganand M N Dr Prithvi P Nayak
 A RARE NEUROLOGICAL PRESENTATION OF SLE Dr Jayachandra Dr Yoganand M N Dr Prithvi P Nayak Presenter: Dr Shambhavi K R CHIEF COMPLAINTS A 30 year old lady hailing from Nepal presented to OPD with complaints
A RARE NEUROLOGICAL PRESENTATION OF SLE Dr Jayachandra Dr Yoganand M N Dr Prithvi P Nayak Presenter: Dr Shambhavi K R CHIEF COMPLAINTS A 30 year old lady hailing from Nepal presented to OPD with complaints
9/13/2015. Nothing to disclose
 Jared Bozeman Kathleen Luskin MD Bipin Thapa MD Medical College of Wisconsin Milwaukee, Wisconsin Nothing to disclose 24 Year old previously healthy woman presenting from OSH Fatigue Weakness Neck swelling
Jared Bozeman Kathleen Luskin MD Bipin Thapa MD Medical College of Wisconsin Milwaukee, Wisconsin Nothing to disclose 24 Year old previously healthy woman presenting from OSH Fatigue Weakness Neck swelling
Fever of unknown origin
 Fever of unknown origin Case B History of the present illness 75 years old women presented at our hospital with since months daily fevers between 38 to 39.5 Celsius (100.4-103.1 F) with night sweats. Her
Fever of unknown origin Case B History of the present illness 75 years old women presented at our hospital with since months daily fevers between 38 to 39.5 Celsius (100.4-103.1 F) with night sweats. Her
Case conference. Welcome Dr. Lawrence Tierney
 Case conference Welcome Dr. Lawrence Tierney Case: 18 year-old male CC) hamatomesis, Fever and cough HPI) 1 st admission One month ago, he admitted to our hospital because of hematemesis. He had weight
Case conference Welcome Dr. Lawrence Tierney Case: 18 year-old male CC) hamatomesis, Fever and cough HPI) 1 st admission One month ago, he admitted to our hospital because of hematemesis. He had weight
ENAL VEIN ROMBOSIS WHAT WAS IT? DR.JANANI SANKAR UNIT DR. KEDARI NAGARJUNA, DNB P KKCTH
 ENAL VEIN ROMBOSIS WHAT WAS IT? DR.JANANI SANKAR UNIT DR. KEDARI NAGARJUNA, DNB P KKCTH RESENTING COMPLAINTS: u 9 ¾ yrs, boy u Fever, Loose stools 10 days back u Right sided Abdominal pain+ NVESTIGATIONS
ENAL VEIN ROMBOSIS WHAT WAS IT? DR.JANANI SANKAR UNIT DR. KEDARI NAGARJUNA, DNB P KKCTH RESENTING COMPLAINTS: u 9 ¾ yrs, boy u Fever, Loose stools 10 days back u Right sided Abdominal pain+ NVESTIGATIONS
Table 2: Outcomes measured. Table 1: Intrapleural alteplase instillation therapy protocol
 ORIGINAL RESEARCH ARTICLE Intrapleural F brinolytic Therapy with Alteplase in Empyema Thoracis in Children conducted in the Department of Pediatric critical care and Pulmonology unit at our institution
ORIGINAL RESEARCH ARTICLE Intrapleural F brinolytic Therapy with Alteplase in Empyema Thoracis in Children conducted in the Department of Pediatric critical care and Pulmonology unit at our institution
Lung Cancer - Suspected
 Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
City Pediatric Meet-Dec 2011 SPECTRUM OF HLH. Spectrum of HLH. Dr.Revathi Raj s unit, Apollo Children s Hospital.
 City Pediatric Meet-Dec 2011 SPECTRUM OF HLH Spectrum of HLH Dr.Revathi Raj s unit, Apollo Children s Hospital. Case 1 4 month male child /thriving well Fever - 5 days with cough O/E hepatospenomegaly
City Pediatric Meet-Dec 2011 SPECTRUM OF HLH Spectrum of HLH Dr.Revathi Raj s unit, Apollo Children s Hospital. Case 1 4 month male child /thriving well Fever - 5 days with cough O/E hepatospenomegaly
3/25/2012. numerous micro-organismsorganisms
 Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
AUTOIMMUNE DISORDERS IN THE ACUTE SETTING
 AUTOIMMUNE DISORDERS IN THE ACUTE SETTING Diagnosis and Treatment Goals Aimee Borazanci, MD BNI Neuroimmunology Objectives Give an update on the causes for admission, clinical features, and outcomes of
AUTOIMMUNE DISORDERS IN THE ACUTE SETTING Diagnosis and Treatment Goals Aimee Borazanci, MD BNI Neuroimmunology Objectives Give an update on the causes for admission, clinical features, and outcomes of
62- year-old man presented with-
 62- year-old man presented with- High grade continued fever Extreme anorexia and vomiting 2 months BACKGROUND On 15 th March 2004, presented with- - severe pain, swelling, marked redness of ears, nose,
62- year-old man presented with- High grade continued fever Extreme anorexia and vomiting 2 months BACKGROUND On 15 th March 2004, presented with- - severe pain, swelling, marked redness of ears, nose,
From. The Department of Pediatrics Dr. Mehtas Hospital
 From The Department of Pediatrics Dr. Mehtas Hospital Case history A 12 yr old girl : Fever 5 days Redness of eyes & erythematous rashes over the body for 2 days Past: Febrile fits at 9 mo. Of age Afebrile
From The Department of Pediatrics Dr. Mehtas Hospital Case history A 12 yr old girl : Fever 5 days Redness of eyes & erythematous rashes over the body for 2 days Past: Febrile fits at 9 mo. Of age Afebrile
UNUSUAL PRESENTATIONS OF SYSTEMIC LUPUS ERYTHEMATOSUS
 UNUSUAL PRESENTATIONS OF SYSTEMIC LUPUS ERYTHEMATOSUS Presenter- Dr. Meghana B S Prof Dr. NAGARAJA B S Prof Dr. NIRMALA A C Dr. SIVARANJANI H Dr. B C PRAKASH Dr. MUMTAZ ALI KHAN A 60 year old lady, k/c/o
UNUSUAL PRESENTATIONS OF SYSTEMIC LUPUS ERYTHEMATOSUS Presenter- Dr. Meghana B S Prof Dr. NAGARAJA B S Prof Dr. NIRMALA A C Dr. SIVARANJANI H Dr. B C PRAKASH Dr. MUMTAZ ALI KHAN A 60 year old lady, k/c/o
High Impact Rheumatology
 High Impact Rheumatology Systemic Lupus Erythematosus Bernard Rubin, DO MPH Case 1: History A 45-year-old woman presents with severe dyspnea and cough. She was in excellent health until 4 weeks ago when
High Impact Rheumatology Systemic Lupus Erythematosus Bernard Rubin, DO MPH Case 1: History A 45-year-old woman presents with severe dyspnea and cough. She was in excellent health until 4 weeks ago when
Enlarging TB Lymph Node Improving or Deteriorating? History. History. Physical examination. Distribution of lymph nodes
 Enlarging TB Lymph Node Improving or Deteriorating? Dr. Lilian Lee Dr. Hamilton Hui Department of Paediatrics & Adolescent Medicine United Christian Hospital 30 August 2006 Enlarging TB lymph node - Improving
Enlarging TB Lymph Node Improving or Deteriorating? Dr. Lilian Lee Dr. Hamilton Hui Department of Paediatrics & Adolescent Medicine United Christian Hospital 30 August 2006 Enlarging TB lymph node - Improving
DISCUSSION BY: Dr M. R. Shakeebi, MD, Rheumatologist
 Case presentations Related to some Rheumatic Diseases Lab & Clinic i Programs, Tuesday, April 24, 2012 COORDINATOR: Dr M. Mahdi Mohammadi, LMD,PhD, Immunologist COORDINATOR: Dr M. Mahdi Mohammadi, LMD,PhD,
Case presentations Related to some Rheumatic Diseases Lab & Clinic i Programs, Tuesday, April 24, 2012 COORDINATOR: Dr M. Mahdi Mohammadi, LMD,PhD, Immunologist COORDINATOR: Dr M. Mahdi Mohammadi, LMD,PhD,
1 yr old girl presented with Fever on and off 3 months H/o frequent semisolid bulky stools 3 months Progressive abdominal distension 3 months Failure
 Dr Rajasree S Dr Srinivas S, Dr Bagdi RK, Dr Satheesh C Apollo Childrens Hospital, Chennai 1 yr old girl presented with Fever on and off 3 months H/o frequent semisolid bulky stools 3 months Progressive
Dr Rajasree S Dr Srinivas S, Dr Bagdi RK, Dr Satheesh C Apollo Childrens Hospital, Chennai 1 yr old girl presented with Fever on and off 3 months H/o frequent semisolid bulky stools 3 months Progressive
Acute Emergencies in Rheumatology
 Acute Emergencies in Rheumatology Clare Higgens Northwick Park hospital and St George s Hospital London Acute Rheumatological Emergencies The Acute Hot joint Inflammatory back pain.. Systemic lupus erythematosus(sle)
Acute Emergencies in Rheumatology Clare Higgens Northwick Park hospital and St George s Hospital London Acute Rheumatological Emergencies The Acute Hot joint Inflammatory back pain.. Systemic lupus erythematosus(sle)
Neuropsychiatric Systemic Lupus Erythematosus (NPSLE) Case presentations and topic discussion The Rheumatology Unit UMMC experience
 Case presentations and topic discussion The Rheumatology Unit UMMC experience") Neuropsychiatric Systemic Lupus Erythematosus (NPSLE) Case presentations and topic discussion The Rheumatology Unit UMMC experience References Sanna G, Bertolaccini ML. Neuropsychiatric manifestations
Neuropsychiatric Systemic Lupus Erythematosus (NPSLE) Case presentations and topic discussion The Rheumatology Unit UMMC experience References Sanna G, Bertolaccini ML. Neuropsychiatric manifestations
A TRICKY PROBLEM. Presenter-Dr Lakshmi PK
 A TRICKY PROBLEM Presenter-Dr Lakshmi PK Patient particulars 33 years old Male Resident of Andhra Pradesh Occupation-soldier Chief compliants Headache- 03 days Headache-global,throbbing type Associated
A TRICKY PROBLEM Presenter-Dr Lakshmi PK Patient particulars 33 years old Male Resident of Andhra Pradesh Occupation-soldier Chief compliants Headache- 03 days Headache-global,throbbing type Associated
EARNEST FERNANDES SLIDE SEMINAR CYTOCON 2012 BHUVANSESHWAR 02 Nov2012
 EARNEST FERNANDES SLIDE SEMINAR CYTOCON 2012 BHUVANSESHWAR 02 Nov2012 Dr Col U S Dinesh Professor SDM College of Medical Sciences & Hospital Dharwad(Karnataka) Case 1 62 year-old female presented with
EARNEST FERNANDES SLIDE SEMINAR CYTOCON 2012 BHUVANSESHWAR 02 Nov2012 Dr Col U S Dinesh Professor SDM College of Medical Sciences & Hospital Dharwad(Karnataka) Case 1 62 year-old female presented with
Diarrhoea on the AMU. Dr Chris Roseveare
 Diarrhoea on the AMU Dr Chris Roseveare The Society for Acute Medicine, Spring Meeting, Radisson Blu Hotel, Dublin 3-4 May 2012 Acute diarrhoea in developed countries adult populations Mainly a primary
Diarrhoea on the AMU Dr Chris Roseveare The Society for Acute Medicine, Spring Meeting, Radisson Blu Hotel, Dublin 3-4 May 2012 Acute diarrhoea in developed countries adult populations Mainly a primary
.,Dr Ali Alkazzaz Babylon collage of medicine 2016
 .,Dr Ali Alkazzaz Babylon collage of medicine 2016 Lupus history Lupus is the Latin word for wolf 1 st used medically in the 10 th century Described clinically in the 19 th century Butterfly rash in 1845
.,Dr Ali Alkazzaz Babylon collage of medicine 2016 Lupus history Lupus is the Latin word for wolf 1 st used medically in the 10 th century Described clinically in the 19 th century Butterfly rash in 1845
* MILIARY MOTTLING --
 * MILIARY MOTTLING -- RARE CAUSE DR ARATHI SRINIVASAN FELLOW IN PEDIATRIC HEMATO ONCOLOGY DR A ANDAL DEPARTMENT OF PEDIATRICS DR JULIUS XAVIER SCOTT DEPARTMENT OF PEDIATRIC HEMATO ONCOLOGY KANCHI KAMAKOTI
* MILIARY MOTTLING -- RARE CAUSE DR ARATHI SRINIVASAN FELLOW IN PEDIATRIC HEMATO ONCOLOGY DR A ANDAL DEPARTMENT OF PEDIATRICS DR JULIUS XAVIER SCOTT DEPARTMENT OF PEDIATRIC HEMATO ONCOLOGY KANCHI KAMAKOTI
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Pyrexia of unknown origin? Think still
 Pyrexia of unknown origin? Think still Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. DISCLAIMER
Pyrexia of unknown origin? Think still Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. DISCLAIMER
Additional file 2: Details of cohort studies and randomised trials
 Reference Randomised trials Ye et al. 2001 Abstract 274 R=1 WD=0 Design, numbers, treatments, duration Randomised open comparison of: (45 patients) 1.5 g for 3, 1 g for 3, then 0.5 to 0.75 g IV cyclophosphamide
Reference Randomised trials Ye et al. 2001 Abstract 274 R=1 WD=0 Design, numbers, treatments, duration Randomised open comparison of: (45 patients) 1.5 g for 3, 1 g for 3, then 0.5 to 0.75 g IV cyclophosphamide
Assessment of limping child (beware the child who does not weight bear at all):
:") Department of Paediatrics Clinical Guideline Acutely Limping Child and Septic Arthritis Assessment of limping child (beware the child who does not weight bear at all): History Careful history of any significant
Department of Paediatrics Clinical Guideline Acutely Limping Child and Septic Arthritis Assessment of limping child (beware the child who does not weight bear at all): History Careful history of any significant
Index No. All five (05) questions should be answered. All questions carry equal marks.
 questions should be answered. All questions carry equal marks.") POSTGRADUATE INSTITUTE OF MEDICINE UNIVERSITY OF COLOMBO POSTGRADUATE DIPLOMA IN TUBERCULOSIS & CHEST DISEASES EXAMINATION - MAY 2016 Date :- 4 th May 2016 PAPER I CASE HISTORIES Time :- 9.00 a.m. -11.00
POSTGRADUATE INSTITUTE OF MEDICINE UNIVERSITY OF COLOMBO POSTGRADUATE DIPLOMA IN TUBERCULOSIS & CHEST DISEASES EXAMINATION - MAY 2016 Date :- 4 th May 2016 PAPER I CASE HISTORIES Time :- 9.00 a.m. -11.00
MANAGEMENT OF TUBERCULOSIS IN NEONATES AND YOUNG INFANTS
 MANAGEMENT OF TUBERCULOSIS IN NEONATES AND YOUNG INFANTS A Bekker FIDSSA Conference, 2017 OUTLINE Case Perinatal TB Approach to the TB-exposed newborn MOM AND BABY S Born by NVD at peripheral hospital
MANAGEMENT OF TUBERCULOSIS IN NEONATES AND YOUNG INFANTS A Bekker FIDSSA Conference, 2017 OUTLINE Case Perinatal TB Approach to the TB-exposed newborn MOM AND BABY S Born by NVD at peripheral hospital
Bilateral Chest X-Ray Shadowing and Bilateral leg lesions - A case of Pulmonary Kaposi Sarcoma
 Article ID: WMC005047 ISSN 2046-1690 Bilateral Chest X-Ray Shadowing and Bilateral leg lesions - A case of Pulmonary Kaposi Sarcoma Peer review status: No Corresponding Author: Dr. Mohammad Fawad Khattak,
Article ID: WMC005047 ISSN 2046-1690 Bilateral Chest X-Ray Shadowing and Bilateral leg lesions - A case of Pulmonary Kaposi Sarcoma Peer review status: No Corresponding Author: Dr. Mohammad Fawad Khattak,
Morbidity Conference. Presented by 肝膽腸胃科張瀚文
 Morbidity Conference Presented by 肝膽腸胃科張瀚文 Chief Complaint General weakness for three days Present Illness This 63-year-old female with diabetes and on oral hypoglycemic agents presented with 3-day history
Morbidity Conference Presented by 肝膽腸胃科張瀚文 Chief Complaint General weakness for three days Present Illness This 63-year-old female with diabetes and on oral hypoglycemic agents presented with 3-day history
- Mycoplasma pneumoniae (MP): important respiratory pathogen in children that cause many upper and lower respiratory tract diseases, including
: important respiratory pathogen in children that cause many upper and lower respiratory tract diseases, including") KHOA DICH VU HO HAP - Mycoplasma pneumoniae (MP): important respiratory pathogen in children that cause many upper and lower respiratory tract diseases, including wheezing, coryza, bronchopneumonia. -
KHOA DICH VU HO HAP - Mycoplasma pneumoniae (MP): important respiratory pathogen in children that cause many upper and lower respiratory tract diseases, including wheezing, coryza, bronchopneumonia. -
Case 1: HER2 positive MBC. Sudeep Gupta Tata Memorial Centre
 Case 1: HER2 positive MBC Sudeep Gupta Tata Memorial Centre 54/F, postmenopausal First came to TMC on 3/8/15 Diagnosed in Jan 2015 Right breast mass Bones (L5 & S1), lung, spleen (upfront MBC) IDC grade
Case 1: HER2 positive MBC Sudeep Gupta Tata Memorial Centre 54/F, postmenopausal First came to TMC on 3/8/15 Diagnosed in Jan 2015 Right breast mass Bones (L5 & S1), lung, spleen (upfront MBC) IDC grade
Significance of Anti-C1q Antibodies in Patients with Systemic Lupus Erythematosus as A Marker of Disease Activity and Lupus Nephritis
 THE EGYPTIAN JOURNAL OF IMMUNOLOGY Vol. 23 (1), 2016 Page: 00-00 Significance of Anti-C1q Antibodies in Patients with Systemic Lupus Erythematosus as A Marker of Disease Activity and Lupus Nephritis 1
THE EGYPTIAN JOURNAL OF IMMUNOLOGY Vol. 23 (1), 2016 Page: 00-00 Significance of Anti-C1q Antibodies in Patients with Systemic Lupus Erythematosus as A Marker of Disease Activity and Lupus Nephritis 1
Case Report Pseudoseptic Arthritis: A Case Series and Review of the Literature
 Case Reports in Infectious Diseases Volume 2011, Article ID 942023, 4 pages doi:10.1155/2011/942023 Case Report Pseudoseptic Arthritis: A Case Series and Review of the Literature Brian P. Oppermann, 1
Case Reports in Infectious Diseases Volume 2011, Article ID 942023, 4 pages doi:10.1155/2011/942023 Case Report Pseudoseptic Arthritis: A Case Series and Review of the Literature Brian P. Oppermann, 1
Clinical Guidance. Kawasaki disease. Summary This guideline includes therapy and follow up including investigations (echocardiography, MRI).
.") Clinical Guidance Kawasaki disease Summary This guideline includes therapy and follow up including investigations (echocardiography, MRI). Document Detail Document type Clinical Guideline Document name
Clinical Guidance Kawasaki disease Summary This guideline includes therapy and follow up including investigations (echocardiography, MRI). Document Detail Document type Clinical Guideline Document name
Example Clinician Educational Material for Providers of Immune Effector Cellular Therapy
 Example Clinician Educational Material for Providers of Immune Effector Cellular Therapy Disclaimer: This example is just one of many potential examples of clinician education material that can be provided
Example Clinician Educational Material for Providers of Immune Effector Cellular Therapy Disclaimer: This example is just one of many potential examples of clinician education material that can be provided
PNEUMONIA IN A PRESUMED IMMUNOCOMPETENT PATIENT
 Dr Marie Bruyneel and Deborah Konopnicki BVIKM/SBMIC November 8th, 2012 PNEUMONIA IN A PRESUMED IMMUNOCOMPETENT PATIENT Men, 54 years Emergency room on end october 2009 Sent by his family doctor for Influenza
Dr Marie Bruyneel and Deborah Konopnicki BVIKM/SBMIC November 8th, 2012 PNEUMONIA IN A PRESUMED IMMUNOCOMPETENT PATIENT Men, 54 years Emergency room on end october 2009 Sent by his family doctor for Influenza
Community Acquired Pneumonia. Abdullah Alharbi, MD, FCCP
 Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Dr Marie Bruyneel and Deborah Konopnicki. BVIKM/SBMIC November 8th, 2012
 Dr Marie Bruyneel and Deborah Konopnicki BVIKM/SBMIC November 8th, 2012 Men, 54 years Emergency room on end october 2009 Sent by his family doctor for Influenza A H1N1? Viral syndrom, cough, fever 39 (7j)
Dr Marie Bruyneel and Deborah Konopnicki BVIKM/SBMIC November 8th, 2012 Men, 54 years Emergency room on end october 2009 Sent by his family doctor for Influenza A H1N1? Viral syndrom, cough, fever 39 (7j)
TOCILIZUMAB FOR DIFFICULT TO TREAT IDIOPATHIC RETROPERITONEAL FIBROSIS. A PILOT TRIAL
 TOCILIZUMAB FOR DIFFICULT TO TREAT IDIOPATHIC RETROPERITONEAL FIBROSIS. A PILOT TRIAL Dr Augusto Vaglio, Dr Federica Maritati Unit of Nephrology, University Hospital of Parma, Via Gramsci 14, 43126 Parma
TOCILIZUMAB FOR DIFFICULT TO TREAT IDIOPATHIC RETROPERITONEAL FIBROSIS. A PILOT TRIAL Dr Augusto Vaglio, Dr Federica Maritati Unit of Nephrology, University Hospital of Parma, Via Gramsci 14, 43126 Parma
TUBERCULOSIS. By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi
 TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
When should we operate for recurrent diverticulitis. Savvas Papagrigoriadis MD MSc FRCS Consultant Colorectal Surgeon King's College Hospital
 When should we operate for recurrent diverticulitis Savvas Papagrigoriadis MD MSc FRCS Consultant Colorectal Surgeon King's College Hospital ASCRS Practice parameters for the Treatment of Acute Diverticulitis
When should we operate for recurrent diverticulitis Savvas Papagrigoriadis MD MSc FRCS Consultant Colorectal Surgeon King's College Hospital ASCRS Practice parameters for the Treatment of Acute Diverticulitis
Hths 2231 Laboratory 7 Infection
 Watch Movie: Meningitis Answer the movie questions on the worksheet. Complete activities 1-3. Activity #1: Go to the patho web page and click on activity 1. Click on Tutorials Click on Immunopathology
Watch Movie: Meningitis Answer the movie questions on the worksheet. Complete activities 1-3. Activity #1: Go to the patho web page and click on activity 1. Click on Tutorials Click on Immunopathology
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014
 Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 TB Case Presentation Andrea Cruz, MD, MPH August 14, 2014 Andrea Cruz, MD, MPH has the following disclosures to
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 TB Case Presentation Andrea Cruz, MD, MPH August 14, 2014 Andrea Cruz, MD, MPH has the following disclosures to
CASE-BASED SMALL GROUP DISCUSSION MHD II
 MHD II, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II Session 11 April 11, 2016 STUDENT COPY MHD II, Session 11, Student Copy Page 2 CASE HISTORY 1 Chief complaint: Our baby
MHD II, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II Session 11 April 11, 2016 STUDENT COPY MHD II, Session 11, Student Copy Page 2 CASE HISTORY 1 Chief complaint: Our baby
Long Case Set 02. Dr Raviraj Uppoor. Dr Sameer Shamshuddin. Consultant Radiologist Cumberland Infirmary, Carlisle, UK
 Long Case Set 02 www.frcrtutorials.com Dr Raviraj Uppoor MBBS, DMRD, DNB, FRCR Consultant Radiologist Cumberland Infirmary, Carlisle, UK Dr Sameer Shamshuddin MBBS, DMRD, FRCR Consultant Radiologist Royal
Long Case Set 02 www.frcrtutorials.com Dr Raviraj Uppoor MBBS, DMRD, DNB, FRCR Consultant Radiologist Cumberland Infirmary, Carlisle, UK Dr Sameer Shamshuddin MBBS, DMRD, FRCR Consultant Radiologist Royal
Hospital-acquired Pneumonia
 Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
1. Dengue An Overview. Dengue Expert Advisory Group
 1. Dengue An Overview Dengue Expert Advisory Group 1 Introduction Dengue Fever Dengue Hemorrhagic Fever Dengue Shock Syndrome 2 3 Dengue Virus Family : Flaviviridae Genus : Flavivirus Serotypes : DV1,
1. Dengue An Overview Dengue Expert Advisory Group 1 Introduction Dengue Fever Dengue Hemorrhagic Fever Dengue Shock Syndrome 2 3 Dengue Virus Family : Flaviviridae Genus : Flavivirus Serotypes : DV1,
A 43year old man presented with cough and breathlessness. Presented by Dr. Enayet-Ul-Islam Dhaka Medical College Hospital
 A 43year old man presented with cough and breathlessness Presented by Dr. Enayet-Ul-Islam Dhaka Medical College Hospital PARTICULARS OF THE PATIENT: Patients name : Mr. Md. Ismail,43 years. Address : Chittagong.
A 43year old man presented with cough and breathlessness Presented by Dr. Enayet-Ul-Islam Dhaka Medical College Hospital PARTICULARS OF THE PATIENT: Patients name : Mr. Md. Ismail,43 years. Address : Chittagong.
Procalcitonin YUKON KUSKOKWIM HEALTH CORPORATION PRESENTED BY: CURT BUCHHOLZ, MD AUGUST 2017
 Procalcitonin YUKON KUSKOKWIM HEALTH CORPORATION PRESENTED BY: CURT BUCHHOLZ, MD AUGUST 2017 Procalcitonin (PCT) PCT isbeing studied as a biomarker for infection PCT consists of 116 amino
Procalcitonin YUKON KUSKOKWIM HEALTH CORPORATION PRESENTED BY: CURT BUCHHOLZ, MD AUGUST 2017 Procalcitonin (PCT) PCT isbeing studied as a biomarker for infection PCT consists of 116 amino
INTERSTITIAL LUNG DISEASE Dr. Zulqarnain Ashraf
 Indep Rev Jul-Dec 2018;20(7-12) Dr. Zulqarnain Ashraf IR-653 Abstract: ILD is a group of diseases affect interstitium of the lung. Repeated insult to the lung cause the interstitium to be damaged. Similarly
Indep Rev Jul-Dec 2018;20(7-12) Dr. Zulqarnain Ashraf IR-653 Abstract: ILD is a group of diseases affect interstitium of the lung. Repeated insult to the lung cause the interstitium to be damaged. Similarly
Unit II Problem 2 Pathology: Pneumonia
 Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Collar stud abscess an interesting case report
 Volume 2 issue 2 2012 ISSN 2250-0359 Collar stud abscess an interesting case report Kameshwaran Kannappan Punniyakodi * Balasubramanian Thiagarajan* *Stanley Medical College Chennai, Tamilnadu Abstract
Volume 2 issue 2 2012 ISSN 2250-0359 Collar stud abscess an interesting case report Kameshwaran Kannappan Punniyakodi * Balasubramanian Thiagarajan* *Stanley Medical College Chennai, Tamilnadu Abstract
What is Crohn's disease?
 What is Crohn's disease? Crohn's disease is a chronic inflammatory disorder that causes inflammation of the digestive tract. It can affect any area of the GI tract, from the mouth to the anus, but it most
What is Crohn's disease? Crohn's disease is a chronic inflammatory disorder that causes inflammation of the digestive tract. It can affect any area of the GI tract, from the mouth to the anus, but it most
PUO DIAGNOSTIC DILEMMA IN
 DIAGNOSTIC DILEMMA IN PUO DR.ARUN MOHAN.R 2 nd YEAR POST GRADUATE UNDER THE GUIDANCE OF PROF. DR. BHAKTHAVATCHALAM. N & DR. SRINIVASA. K. V DEPT. OF GENERAL MEDICINE DR.B.R.AMCH, BANGALORE. 1 HISTORY PATIENT
DIAGNOSTIC DILEMMA IN PUO DR.ARUN MOHAN.R 2 nd YEAR POST GRADUATE UNDER THE GUIDANCE OF PROF. DR. BHAKTHAVATCHALAM. N & DR. SRINIVASA. K. V DEPT. OF GENERAL MEDICINE DR.B.R.AMCH, BANGALORE. 1 HISTORY PATIENT
The X factor in a blue moon. Monique Lee Campbelltown Hospital
 The X factor in a blue moon Monique Lee Campbelltown Hospital Mrs MD 73 year old Increasing dyspnoea, hypoxia Recurrent lower respiratory tract infections Two hospital admissions parenteral antibiotics
The X factor in a blue moon Monique Lee Campbelltown Hospital Mrs MD 73 year old Increasing dyspnoea, hypoxia Recurrent lower respiratory tract infections Two hospital admissions parenteral antibiotics
General History. 林陳 珠 Female 69 years old 住院期間 : ~ Chief Complaint : sudden loss of conscious 5 minutes in the morning.
 General History 林陳 珠 Female 69 years old 住院期間 : 93.5.8~93.5.15 Chief Complaint : sudden loss of conscious for 2-52 5 minutes in the morning. General History DM under regular medical control for 10 years.
General History 林陳 珠 Female 69 years old 住院期間 : 93.5.8~93.5.15 Chief Complaint : sudden loss of conscious for 2-52 5 minutes in the morning. General History DM under regular medical control for 10 years.
CASE OF STAPH. AUREUS PNEUMONIA DR.VINAY BHOMIA MD
 CASE OF STAPH. AUREUS PNEUMONIA DR.VINAY BHOMIA MD PATIENT S HISTORY Ambalal Labana a male aged 40 yrs came with c/o -- High grade fever with rigors 7 days --cough with white expectoration 7 days --Breathlessness
CASE OF STAPH. AUREUS PNEUMONIA DR.VINAY BHOMIA MD PATIENT S HISTORY Ambalal Labana a male aged 40 yrs came with c/o -- High grade fever with rigors 7 days --cough with white expectoration 7 days --Breathlessness
Haematological Cancer Suspected (Adults & Children)
") Haematological Cancer Suspected (Adults & Children) Link to NICE guidelines: https://www.nice.org.uk/guidance/ng47 Patient of any age presents with symptoms of possible haematological cancer If 60 years
Haematological Cancer Suspected (Adults & Children) Link to NICE guidelines: https://www.nice.org.uk/guidance/ng47 Patient of any age presents with symptoms of possible haematological cancer If 60 years
Complicated echinococcal cyst to Biopsy or not to biopsy. V. Rusanov MR Kramer Pulmonary Institute, Rabin medical center
 Complicated echinococcal cyst to Biopsy or not to biopsy V. Rusanov MR Kramer Pulmonary Institute, Rabin medical center Case 1 84 y.o. Male, Iraq descend, past smoker 40 PY Medical History- HTN, Rheumatoid
Complicated echinococcal cyst to Biopsy or not to biopsy V. Rusanov MR Kramer Pulmonary Institute, Rabin medical center Case 1 84 y.o. Male, Iraq descend, past smoker 40 PY Medical History- HTN, Rheumatoid
Management of uveitis
 Management of uveitis DR. ANUPAMA KARANTH Anti-inflammatory agents -itis = inflammation Treatment : stop inflammation Use anti-inflammatory drugs Most potent of such agents : Corticosteroids Corticosteroids
Management of uveitis DR. ANUPAMA KARANTH Anti-inflammatory agents -itis = inflammation Treatment : stop inflammation Use anti-inflammatory drugs Most potent of such agents : Corticosteroids Corticosteroids
Case Presentation. Rafid Asfar, MD
 Case Presentation Rafid Asfar, MD Introduction ANCA associated vasculitis may be localized or systemic, and can involve the eyes Ocular manifestations can occur in the absence of systemic disease in persons
Case Presentation Rafid Asfar, MD Introduction ANCA associated vasculitis may be localized or systemic, and can involve the eyes Ocular manifestations can occur in the absence of systemic disease in persons
Patient #1. Rheumatoid Arthritis. Rheumatoid Arthritis. 45 y/o female Morning stiffness in her joints >1 hour
 Patient #1 Rheumatoid Arthritis Essentials For The Family Medicine Physician 45 y/o female Morning stiffness in her joints >1 hour Hands, Wrists, Knees, Ankles, Feet Polyarticular, symmetrical swelling
Patient #1 Rheumatoid Arthritis Essentials For The Family Medicine Physician 45 y/o female Morning stiffness in her joints >1 hour Hands, Wrists, Knees, Ankles, Feet Polyarticular, symmetrical swelling
To Study The Cinico-Radiological Features And Associated Co-Morbid Conditions
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 7 Ver. 16 (July. 2018), PP 58-62 www.iosrjournals.org To study the clinico-radiological features
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 7 Ver. 16 (July. 2018), PP 58-62 www.iosrjournals.org To study the clinico-radiological features
SYSTEMIC LUPUS ERYTHEMATOSUS: CURRENT CONCEPTS AND CLINICAL PEARLS. Dr Sheila Vasoo Consultant Division of Rheumatology NUHS
 SYSTEMIC LUPUS ERYTHEMATOSUS: CURRENT CONCEPTS AND CLINICAL PEARLS Dr Sheila Vasoo Consultant Division of Rheumatology NUHS Listen to the Patient Concepts Diagnosis Immunopathogenesis Clinical Pearls Disease
SYSTEMIC LUPUS ERYTHEMATOSUS: CURRENT CONCEPTS AND CLINICAL PEARLS Dr Sheila Vasoo Consultant Division of Rheumatology NUHS Listen to the Patient Concepts Diagnosis Immunopathogenesis Clinical Pearls Disease
Fever. National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital
 Fever National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital Case 1 4-month-old well-appearing girl admitted for croup and respiratory distress.
Fever National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital Case 1 4-month-old well-appearing girl admitted for croup and respiratory distress.
PITFALLS IN THE DIAGNOSIS OF SKELETAL TUBERCULOSIS IN CHILDREN
 PITFALLS IN THE DIAGNOSIS OF SKELETAL TUBERCULOSIS IN CHILDREN DR.JANANI SANKAR SENIOR CONSULTANT - PEDIATRICS DEPARTMENT OF PEDIATRICS & PEDIATRIC ORTHOPEDICS KANCHI KAMAKOTI CHILDS TRUST HOSPITAL CHENNAI,
PITFALLS IN THE DIAGNOSIS OF SKELETAL TUBERCULOSIS IN CHILDREN DR.JANANI SANKAR SENIOR CONSULTANT - PEDIATRICS DEPARTMENT OF PEDIATRICS & PEDIATRIC ORTHOPEDICS KANCHI KAMAKOTI CHILDS TRUST HOSPITAL CHENNAI,
The Child with HIV and a Fever 1
 The Child with HIV and a Fever 1 Author: Andrew Riordan Amanda Williams Date of preparation: August 2003 Date reviewed: February 2012 Next review date: February 2014 Contents 1. Introduction 2. HIV disease
The Child with HIV and a Fever 1 Author: Andrew Riordan Amanda Williams Date of preparation: August 2003 Date reviewed: February 2012 Next review date: February 2014 Contents 1. Introduction 2. HIV disease
Outcome of Severe Malaria in Endemic Zone - Study From a District Hospital of Bangladesh
 Dr. Md. AMIR HOSSAIN Department of Medicine Rangamati General Hospital Deputed to BSMMU, Dhaka. Outcome of Severe Malaria in Endemic Zone - Study From a District Hospital of Bangladesh 1 INTRODUCTION In
Dr. Md. AMIR HOSSAIN Department of Medicine Rangamati General Hospital Deputed to BSMMU, Dhaka. Outcome of Severe Malaria in Endemic Zone - Study From a District Hospital of Bangladesh 1 INTRODUCTION In
Case Presentation. Dr.N.Bhanu teja Final year postgraduate Department of pulmonology
 Case Presentation Dr.N.Bhanu teja Final year postgraduate Department of pulmonology A 60 year old male patient resident of miryalguda referred to pulmonary medicine outpatient department with complaints
Case Presentation Dr.N.Bhanu teja Final year postgraduate Department of pulmonology A 60 year old male patient resident of miryalguda referred to pulmonary medicine outpatient department with complaints
Benlysta (belimumab) Prior Authorization Criteria Program Summary
 Prior Authorization Criteria Program Summary") Benlysta (belimumab) Prior Authorization Criteria Program Summary This prior authorization applies to Commercial, NetResults A series, NetResults F series and Health Insurance Marketplace formularies.
Benlysta (belimumab) Prior Authorization Criteria Program Summary This prior authorization applies to Commercial, NetResults A series, NetResults F series and Health Insurance Marketplace formularies.
Indications for use of Infliximab
 Indications for use of Infliximab Moscow, June 10 th 2006 Prof. Dr. Dr. Gerhard Rogler Klinik und Poliklinik für Innere Medizin I Universität Regensburg Case report 1989: Diagnosis of Crohn s disease of
Indications for use of Infliximab Moscow, June 10 th 2006 Prof. Dr. Dr. Gerhard Rogler Klinik und Poliklinik für Innere Medizin I Universität Regensburg Case report 1989: Diagnosis of Crohn s disease of
FAMILIAL MEDITERRANEAN FEVER (FMF) RAKAN TELFAH not MD, not PHD
 RAKAN TELFAH not MD, not PHD") FAMILIAL MEDITERRANEAN FEVER (FMF) RAKAN TELFAH not MD, not PHD FMF Is a hereditary autoinflammatory disease caused by mutations in Mediterranean fever gene (MEFV). It is inherited in an autosomal recessive
FAMILIAL MEDITERRANEAN FEVER (FMF) RAKAN TELFAH not MD, not PHD FMF Is a hereditary autoinflammatory disease caused by mutations in Mediterranean fever gene (MEFV). It is inherited in an autosomal recessive
TB or Not TB That is the Question. Yunus Moosa Department of Infectious Diseases UKZN
 TB or Not TB That is the Question Yunus Moosa Department of Infectious Diseases UKZN Case: Mr. DN 42 yr. Male HIV on ART since 2006 and HPT - perindopril 1/12 prior to admission -fever, cough and cervical
TB or Not TB That is the Question Yunus Moosa Department of Infectious Diseases UKZN Case: Mr. DN 42 yr. Male HIV on ART since 2006 and HPT - perindopril 1/12 prior to admission -fever, cough and cervical
The Dr. Jae Yang Lecture: An Overview of the Radiographic Picture of TB
 The Dr. Jae Yang Lecture: An Overview of the Radiographic Picture of TB Harvey H. Wong, MD FRCPC MScCH Assistant Professor Department of Medicine Division of Respirology University of Toronto Financial
The Dr. Jae Yang Lecture: An Overview of the Radiographic Picture of TB Harvey H. Wong, MD FRCPC MScCH Assistant Professor Department of Medicine Division of Respirology University of Toronto Financial
Antibiotic Protocols for Paediatrics Steve Biko Academic Hospital
 Antibiotic Protocols for Paediatrics Steve Biko Academic Hospital Respiratory tract infections in children Uncomplicated URTI A child with a cold should not receive an antibiotic Paracetamol (15 mg/kg/dose
Antibiotic Protocols for Paediatrics Steve Biko Academic Hospital Respiratory tract infections in children Uncomplicated URTI A child with a cold should not receive an antibiotic Paracetamol (15 mg/kg/dose
Lofgren's syndrome A case report
 Open Journal of Clinical & Medical Case Reports Lofgren's syndrome A case report Volume 3 (2017) Issue 24 ISSN 2379-1039 Mohammad Iqbal KM; Thara Pratap; Muhammed Jasim Abdul Jalal*; Chippy Eldhose; Shani
Open Journal of Clinical & Medical Case Reports Lofgren's syndrome A case report Volume 3 (2017) Issue 24 ISSN 2379-1039 Mohammad Iqbal KM; Thara Pratap; Muhammed Jasim Abdul Jalal*; Chippy Eldhose; Shani
1. Introduction Algorithm: Infant with Fever 0-28 Days Algorithm: Infant with Fever Days...3
 These guidelines are designed to assist clinicians and are not intended to supplant good clinical judgement or to establish a protocol for all patients with this condition. MANAGEMENT OF FEVER 38 C (100.4F)
These guidelines are designed to assist clinicians and are not intended to supplant good clinical judgement or to establish a protocol for all patients with this condition. MANAGEMENT OF FEVER 38 C (100.4F)
Osteomieliti STEOMIE
 OsteomielitiSTEOMIE Osteomyelitis is the inflammation of bone caused by pyogenic organisms. Major sources of infection: - haematogenous spread - tracking from adjacent foci of infection - direct inoculation
OsteomielitiSTEOMIE Osteomyelitis is the inflammation of bone caused by pyogenic organisms. Major sources of infection: - haematogenous spread - tracking from adjacent foci of infection - direct inoculation
Infected cardiac-implantable electronic devices: diagnosis, and treatment
 Infected cardiac-implantable electronic devices: diagnosis, and treatment The incidence of infection following implantation of cardiac implantable electronic devices (CIEDs) is increasing at a faster rate
Infected cardiac-implantable electronic devices: diagnosis, and treatment The incidence of infection following implantation of cardiac implantable electronic devices (CIEDs) is increasing at a faster rate
Myositis and Your Lungs
 Myositis and Your Lungs 2013 TMA Annual Patient Meeting Louisville, Kentucky Chester V. Oddis, MD University of Pittsburgh Director, Myositis Center Myositis Heterogeneous group of autoimmune syndromes
Myositis and Your Lungs 2013 TMA Annual Patient Meeting Louisville, Kentucky Chester V. Oddis, MD University of Pittsburgh Director, Myositis Center Myositis Heterogeneous group of autoimmune syndromes
SELECTED INFECTIONS ACQUIRED DURING TRAVELLING IN NORTH AMERICA. Lin Li, MD August, 2012
 SELECTED INFECTIONS ACQUIRED DURING TRAVELLING IN NORTH AMERICA Lin Li, MD August, 2012 Case 1 32 year old male working in Arizona; on leave back in Singapore Presented to hospital A for fever x (7-10)
SELECTED INFECTIONS ACQUIRED DURING TRAVELLING IN NORTH AMERICA Lin Li, MD August, 2012 Case 1 32 year old male working in Arizona; on leave back in Singapore Presented to hospital A for fever x (7-10)
Key Difference - Pleural Effusion vs Pneumonia
 Difference Between Pleural Effusion and Pneumonia www.differencebetween.com Key Difference - Pleural Effusion vs Pneumonia Pleural effusion and pneumonia are two conditions that affect our respiratory
Difference Between Pleural Effusion and Pneumonia www.differencebetween.com Key Difference - Pleural Effusion vs Pneumonia Pleural effusion and pneumonia are two conditions that affect our respiratory
Delayed response to anti-tuberculosis treatment in a patient on infliximab
 Respiratory Medicine (2005) 99, 648 652 CASE REPORT Delayed response to anti-tuberculosis treatment in a patient on infliximab Elina Vlachaki a, Kostas Psathakis a,, Kostas Tsintiris a, Alexios Iliopoulos
Respiratory Medicine (2005) 99, 648 652 CASE REPORT Delayed response to anti-tuberculosis treatment in a patient on infliximab Elina Vlachaki a, Kostas Psathakis a,, Kostas Tsintiris a, Alexios Iliopoulos
Role of imaging (images) in my practice. Dr P Senthur Nambi Consultant Infectious Diseases
 in my practice. Dr P Senthur Nambi Consultant Infectious Diseases") Role of imaging (images) in my practice Dr P Senthur Nambi Consultant Infectious Diseases Medical images: My thoughts Images are just images Subject to the intellect of the interpreter View it in conjuction
Role of imaging (images) in my practice Dr P Senthur Nambi Consultant Infectious Diseases Medical images: My thoughts Images are just images Subject to the intellect of the interpreter View it in conjuction
Pediatric TB Radiology: It s Not Black and White Part 2
 Experiencing technical difficulties? Please call Adobe Connect for technical assistance at 1-800-422-3623 Pediatric TB Radiology: It s Not Black and White Part 2 June 18, 2018 A National Webinar June 18,
Experiencing technical difficulties? Please call Adobe Connect for technical assistance at 1-800-422-3623 Pediatric TB Radiology: It s Not Black and White Part 2 June 18, 2018 A National Webinar June 18,
Diarrhoea for the Acute Physician
 Diarrhoea for the Acute Physician STEPHEN INNS GASTROENTEROLOGIST AND PHYSICIAN HUTT VALLEY DHB August 2013 Outline Case History 1 Initial assessment of acute diarrhoea Management of fulminant UC Management
Diarrhoea for the Acute Physician STEPHEN INNS GASTROENTEROLOGIST AND PHYSICIAN HUTT VALLEY DHB August 2013 Outline Case History 1 Initial assessment of acute diarrhoea Management of fulminant UC Management
Fever and rash in children. Haider Arishi MD Consultant, pediatrics and infectious diseases Director, infection control program
 Fever and rash in children Haider Arishi MD Consultant, pediatrics and infectious diseases Director, infection control program objectives To understand importance of fever and rash. To discuss the clinical
Fever and rash in children Haider Arishi MD Consultant, pediatrics and infectious diseases Director, infection control program objectives To understand importance of fever and rash. To discuss the clinical
Management of Nephrotic Syndrome
 Management of Nephrotic Syndrome 1. Introduction Incidence 2-4/100,000. Boys > girls 3:2; age of onset 2-6 years 80% of cases in children is due to minimal change (MCD) of which 80% will respond to steroid
Management of Nephrotic Syndrome 1. Introduction Incidence 2-4/100,000. Boys > girls 3:2; age of onset 2-6 years 80% of cases in children is due to minimal change (MCD) of which 80% will respond to steroid
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
Chronic Cough An Unusual Presentation. Dr Sourabh Jain Department of Respiratory Medicine
 Chronic Cough An Unusual Presentation Dr Sourabh Jain Department of Respiratory Medicine A 72 years old male from Pune, non smoker, with no co-morbidities Chief Complaints : Chronic cough with scanty mucoid
Chronic Cough An Unusual Presentation Dr Sourabh Jain Department of Respiratory Medicine A 72 years old male from Pune, non smoker, with no co-morbidities Chief Complaints : Chronic cough with scanty mucoid
9/25/2013 SYSTEMIC LUPUS ERYTHEMATOSUS (SLE)
") SYSTEMIC LUPUS ERYTHEMATOSUS (SLE) 1 Other Types of Lupus Discoid Lupus Erythematosus Lupus Pernio --- Sarcoidosis Lupus Vulgaris --- Tuberculosis of the face Manifestations of SLE Fever Rashes Arthritis
SYSTEMIC LUPUS ERYTHEMATOSUS (SLE) 1 Other Types of Lupus Discoid Lupus Erythematosus Lupus Pernio --- Sarcoidosis Lupus Vulgaris --- Tuberculosis of the face Manifestations of SLE Fever Rashes Arthritis
Scleritis LEN V KOH OD
 Scleritis LEN V KOH OD 2014 PUCO 1 Introduction A painful, destructive, and potentially blinding disorder Highly symptomatic High association with systemic disease Immunosuppresssive agents 2014 PUCO 2
Scleritis LEN V KOH OD 2014 PUCO 1 Introduction A painful, destructive, and potentially blinding disorder Highly symptomatic High association with systemic disease Immunosuppresssive agents 2014 PUCO 2