Personalized Medicine in IBD
|
|
|
- Patrick Manning
- 6 years ago
- Views:
Transcription
1 Personalized Medicine in IBD Anita Afzali MD, MPH Assistant Professor of Medicine Director, Inflammatory Bowel Diseases Program University of Washington Harborview Medical Center CCFA April 2 nd, 2016
2 Disclosures Abbvie Consultant, Advisory Board UCB Consultant, Advisory Board Takeda Consultant Janssen Consultant Prometheus Consultant

3 What is Personalized Medicine?
4 Personalized Medicine Introduced in the 1970s Provides optimal medical care by using comprehensive pathophysiology-based information Prevent, diagnose and treat disease Custom-made for each individual patient
5 Right Patient, Right Treatment, Right Time Integration of clinical variables (i.e. age, gender), disease characteristics, genetic and conventional laboratory testing to guide treatment decisions Decrease risk of adverse events and disease complications Potential to optimize efficacy and outcomes
6 Spectrum of IBD Crohn s Disease Ulcerative Colitis Indeterminate Colitis
7 Spectrum of IBD Crohn s Disease Ulcerative Colitis Indeterminate Colitis

8 The -omes in IBD Pathogenesis Taken from Fiocchi C. Dig Dis 2015
9 Personalized Medicine IBDs are chronic complex diseases with multiple pathogenic components that interact with each other Complexity + interaction = unique molecular pathways only relevant to certain disease subtypes and individuals Not for entire IBD Population

10 Why do we need Personalized Medicine in IBD?


11 Exact Etiology Unknown: Inappropriate immune response Genetics Immune System/ Inflammation Environmental Influence Luminal microbial antigens/adjuvants CD=Crohn s disease; IBD=inflammatory bowel disease. Khor B, et al. Nature Cosnes J, et al. Gastroenterology
 that defend the body against attack from infections To eradicate infection, the immune system turns on, causes")
12 What is the Immune System? Cells (T cells, B cells, macrophages) that defend the body against attack from infections To eradicate infection, the immune system turns on, causes inflammation Once an infection is eliminated, the immune system knows how to turn itself off Photo courtesy of Scott Plevy, MD

13 Dysregulated Immune System In IBD, the off switch is broken Inflammation is a Key Aspect of IBD
14 IBD Medicine Cabinet Over-the-Counter Antibiotics 5-Aminosalicylates/Mesalamine Prednisone, Budesonide Immunomodulators AZA/6MP, MTX Biologics/Anti-TNFs/Anti-Adhesions
15 Biologics: Protein Target Specific Biologics:Anti-TNFs/Anti-Adhesions New Therapies have and will be designed to Target specific Inflammatory proteins (TNF best example) Genetic defects Microbial imbalances Directly target what is responsible for the disease process the inflammatory cascade

16 CHRONIC INFLAMMATION: PROTEINS CALLED CYTOKINES ARE THE LIGHT SWITCH TNF IL-1 IL-8 IL-12 IFN IL-4/IL-13 IL-1Ra TGF IL-10 On Off

17 Anti-TNFs in IBD Infliximab approved for CD 1998 Adalimumab for CD 2002 Certolizumab pegol for CD 2008 Infliximab approved for UC 2005 Adalimumab for UC 2012 Golimumab for UC 2013 Adapted from Curr Opin Rheumat 2014 Fausel R and Afzali A. Ther Clin Risk Manag 2015
18 Protein Target Specific: Biologics in IBD Revolutionized treatment and management of UC and CD Why do we use them? Very effective Reduces hospitalization, surgery Steroid free remission Improved quality of life Changes the natural history of disease** Limitations: costs, misinformation
19 Multiple Sclerosis Asthma Crohn s Disease Ulcerative Colitis Psoriasis Rheumatoid Arthritis

20 Rheumatoid Arthritis IBD TNF
21 Stages of Rheumatoid Arthritis Early Intermediate Late Courtesy of J. Cush, 2002
22 Mean change from baseline through 102 weeks Change in Joint Damage Mean through 102 Weeks Anti-TNF 14 Placebo 3 mg/kg qw8 3 mg/kg qw4 10 mg/kg qw8 10 mg/kg qw p < for each infliximab arm vs. placebo at week 30, 54, and 102 Baseline Week 30 Week 54 Week 102
23 n=19 n=35 n=19 n=35 n=20 n=22 n=20 n=22 n=45 n=55 n=45 n=55 n=131 n=98 n=131 n=98 % in CDAI Response or Remission Response and remission to Anti-TNF by disease duration 100% 90% 90% 80% 70% 60% 50% 40% 30% 37% 68% 37% 75% 50% 55% 36% 62% 36% 47% 29% 57% 33% 44% 24% 20% 10% 0% Sandborn WJ et al. Am J Gastro 2006 Colombel et al, NEJM 2007 <1 Year 1-<2 years 2-<5 years >=5 years Response Remission Placebo Response Placebo Remission PRECISE trial (certolizumab)
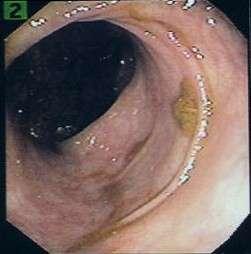

24 Anti-TNF: Endoscopic Healing



25 We Don t See the Deformities of the Intestines until Complication Early Intermediate Late Courtesy of J. Cush, 2002

26 Inflammation -> Fistula, Stricture Taken from M. Shaikhani MD
 or penetrating (70%) disease Cosnes J et al. Inflamm Bowel Dis.")
27 Cumulative Probability (%) THE EVOLUTION OF CROHN S DISEASE: INFLAMMATION LEADS TO DAMAGE Penetrating 70% Inflammatory Stricturing 18% Months Over a 20-year period, 88% risk of developing stricturing (18%) or penetrating (70%) disease Cosnes J et al. Inflamm Bowel Dis. 2002


28 Natural History Most Crohn s Patients Will Require Surgery Mekhjian HS et al. Gastro 1979.
29 Patients (%) Natural History Of Ulcerative Colitis n= Years after diagnosis Risk of colectomy: 24% after 10 years ~ 30% after 20 years Significant Increased risk of cancer Colectomy Disease activity Remission Adapted from Langholz E, et al. Gastroenterology 1994
30 Temporal trends of Colectomy in UC Kaplan GG et al. AJG 2012 Since introduction of biologic agents/anti-tnfs, decrease in total colectomy in UC patients
31 The Right Patient? Which Patients are at highest risk for disease complications? How do we choose the Right Patient for Early Appropriate intervention?
32 5-Yr Follow up of Crohn s Patients Variable Percent of Patients Non-disabling (n = 166) Disabling (n = 957) Male Independent Risk Factors Odds Ratio (95% CI) 2.1 (P = ) Age < 40 yr Disease location Small bowel only Small bowel & colon Colon only Smoker Systemic findings Perianal lesions Steroids for first flare (P = 0.01) 3.1 (P = ) Beaugerie L, et al. Gastroenterology
33 Percent Distribution of Patients and PPV of Independent Factors for Disabling CD 100 No factors (score = 0) 1 factor (score = 1) 80 2 factors (score = 2) All 3 factors (score = 3) Distribution of Patients Positive Predictive Value Beaugerie L, et al. Gastroenterology. 2006
34 Prognostic Value of Clinical Parameters Mild disease course Older age Higher education level Longer dz duration No smoking No rectal involvement Aggressive disease course Age at diagnosis <40 Perianal dz Weight loss >5kg Smoking Deep colonic ulcers Need for steroid use Extensive small bowel dz Early Appropriate Therapy Vermeire S, et al. Gut 2013
35 Additional Objective Measures: Associations of Serology and Disease Behavior Small Bowel Fibrostenosis Internal Perforating Surgery UClike Pouchitis ASCA X X X X anti-ompc X X anti-cbir1 X X X X anti-fla-x X X anti-a4- Fla2 X X panca X X Mow WS, et al. Gastroenterology Targan SR, et al. Gastroenterology Schoefer AM, et al. Inflamm Bowel Dis. 2009
36 Serology Predicts Progression to Surgery Survival estimates according to serology antibody sum Shortest time to CD-related surgery Dubinsky MC, et al. Clin Gastroenterol Hepatol. 2008
37 The Right Treatment? If at high risk for disease complications, How do we choose the Right Treatment?
38 IBD Treatment Strategy Top-down Strategy Early, appropriate use of biologic as initial treatment Induces rapid clinical response May enhance quality of life Step-up" Strategy Standard, sequential treatment for remission and maintenance Cost-effective Minimal side effects Biologics Immunemodulators - Azathioprine/6MP - MTX Anti-inflammatory Drugs Aminosalicylates Corticosteroids Surgery Surgery Biologics Immunemodulators - Azathioprine/6MP - MTX Corticosteroids Anti-inflammatory Drugs Aminosalicylates Corticosteroids Early Late Severe Moderate Mild






39 Treatment Approach Strategies Low risk of disease progression Top-down : may over-treat and expose patients to costs, risks of immunosuppression High risk of disease progression Step-up : may postpone adequate therapy in aggressive disease and results in disease progression, complications, morbidity

40 Update in the Evolution of Treatment Goals & Strategies Improved clinical symptoms Clinical remission Mucosal healing Steroid free remission Histologic remission Adapted CCFA Canada Webinar 2015
* p=0.028 P = 0.028 P p<0.001 < 0.001 p=0.035 P=0.")

41 SONIC Steroid-Free Clinical Remission at Week 50 All Randomized Patients (N=508)* p=0.028 P = P p<0.001 < p=0.035 P= /170 59/169 78/169 * Patients who did not enter the Study Extension were treated as non-responders Colombel JF et al. NEJM 2010

42 SUCCESS Steroid-Free Clinical Remission at Week 16 Panaccione R et al. Gastroenterology 2014
43 Combination Therapy in IBD: Use of Aza or MTX Better clinical outcomes Improved response to biologic therapy Decreased risk for antibody development Decreased need for steroids
44 The Right Treatment and Dose? One size doesn t fit all one dose isn t for all How do we choose the Right Dose?
45 Pharmacokinetics: How good drug works Factors More Drug Less Drug Males Body size Poor nutrition, albumin High inflammation, CRP X X X X Aza/MTX use X Presence of antibodies High baseline TNF levels Smoking X X X
46 OPTIMIZING TREATMENT For the Early Appropriate Patient Azathioprine 6-mercaptopurine Anti-TNFs Role of measuring metabolites and drug levels
47 Pharmacogenomics Using genetics to optimize medical therapy TPMT TPMT mutation Azathioprine 6-MP Azathioprine 6-MP Safe Toxic
48 Potential Utility of Metabolite Monitoring Identify Reasons for Non-Response 6TGN 6MMP Inadequate dose Non-adherence 6MMP shunting Drug Resistance
49 A New Era in IBD: Therapeutic Drug Monitoring (TDM) ~50% IBD patients will require dose modification or switch of treatment Symptoms may not be correlated with active inflammation (endoscopy vs CRP) Need to identify patients with Insufficient drug Anti-drug antibodies Causes other than active IBD
50 CRP mg/l CRP CRP mg/l CRP Association of CRP, ATI, Drug Level P= IFX_positive IFX- IFX+ ATI_positive ATI- ATI+ P= IFX- IFX < 3 μg/ml IFX_positive IFX+ IFX 3 μg/ml 52% lower CRP 59% higher CRP ATI- ATI ATI_positive ATI+ ATI+ Higher drug concentration levels associated with lower CRP Higher detectable antibodies associated with higher CRP Feagan B et al. Gastroenterology 2012
51 Therapeutic Drug Monitoring: Guide to optimize treatment High detectable antibodies Sub-therapeutic anti- TNF drug level Therapeutic drug level, low/no antibodies Change to another anti-tnf Increase dose or frequency of anti-tnf Evaluate by endoscopy/labs/imaging active or inactive disease? Afif W et al. Am J Gastro 2010
52 The Right Time? Timing is Everything.






53 Heart Disease
54 Treat to Target Symptomatic relief is NOT enough Need serial objective evaluation of inflammatory burden: Lab studies: CRP/ESR, Nutrition Endoscopic: colonoscopy, EGD, capsule Mucosal healing Radiologic: CAT or MRI scan Strictures, fistulas


55 Cumulative Probability (%) Timing for IBD Penetrating 70% Inflammatory Stricturing 18% Months Cosnes J et al. Inflamm Bowel Dis. 2002
56 Personalized Medicine Who is the Right Patient? What is the Right Treatment? When is the Right Time? The Art of Personalized Medicine in IBD

57 An Approach to Personalized Medicine First Visit: IBD Panel Serotype Genotype Phenotype What kind of IBD do you have? How will your disease progress? Predict adverse event Patient-specific treatment plan New, Integrated Target-Specific Therapy
58 Will IBD Medicine Be Personalized? Different pathogenesis, different therapies Genetic mutations Immunologic response to bacteria Clinical Phenotype Treatment NOD2 ASCA SB dz IBD - I A IL-23R Missing bacteria? Altered microbiota Mild SB dz Anti- IBD - II IL-23(?) UC - like IBD III Mild SB dz Probiotic Gene X Anti- CBir1 fistula IBD C IV? Courtesy of S Plevy


59 UW Medicine Inflammatory Bowel Diseases Program THANK YOU!
Personalized Medicine in IBD: Where Are We in 2013
 Personalized Medicine in IBD: Where Are We in 2013 David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University Medical Center What is Personalized
Personalized Medicine in IBD: Where Are We in 2013 David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University Medical Center What is Personalized
Efficacy and Safety of Treatment for Pediatric IBD
 Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Assistant Professor of Clinical Pediatrics Division of Gastroenterology,
Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Assistant Professor of Clinical Pediatrics Division of Gastroenterology,
September 12, 2015 Millie D. Long MD, MPH, FACG
 Update on Biologic Therapy in 2015 September 12, 2015 Millie D. Long MD, MPH, FACG Assistant Professor of Medicine Inflammatory Bowel Disease Center University of North Carolina-Chapel Hill Outline Crohn
Update on Biologic Therapy in 2015 September 12, 2015 Millie D. Long MD, MPH, FACG Assistant Professor of Medicine Inflammatory Bowel Disease Center University of North Carolina-Chapel Hill Outline Crohn
Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease
 Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease The Case for Starting with Anti-TNFα Agents Maria Oliva-Hemker, M.D. Chief, Division of Pediatric Gastroenterology &
Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease The Case for Starting with Anti-TNFα Agents Maria Oliva-Hemker, M.D. Chief, Division of Pediatric Gastroenterology &
Beyond Anti TNFs: positioning of other biologics for Crohn s disease. Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center
 Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
Ali Keshavarzian MD Rush University Medical Center
 Treatment: Step Up or Top Down? Ali Keshavarzian MD Rush University Medical Center Questions What medication should IBD be treated with? Can we predict which patients with IBD are high risk? Is starting
Treatment: Step Up or Top Down? Ali Keshavarzian MD Rush University Medical Center Questions What medication should IBD be treated with? Can we predict which patients with IBD are high risk? Is starting
Crohn's Disease. The What, When, and Why of Treatment
 Crohn's Disease The What, When, and Why of Treatment Brian Feagan, MD, FACG Professor of Medicine and Epidemiology and Biostatistics Director, Robarts Clinical Trials Robarts Research Institute University
Crohn's Disease The What, When, and Why of Treatment Brian Feagan, MD, FACG Professor of Medicine and Epidemiology and Biostatistics Director, Robarts Clinical Trials Robarts Research Institute University
Efficacy and Safety of Treatment for Pediatric IBD
 Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Associate Professor of Clinical Pediatrics Division of Gastroenterology,
Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Associate Professor of Clinical Pediatrics Division of Gastroenterology,
Common Questions in Crohn s Disease Therapy. Case
 Common Questions in Crohn s Disease Therapy Jean-Paul Achkar, MD, FACG Kenneth Rainin Chair for IBD Research Cleveland Clinic Case 23 yo male with 1 year history of diarrhea, abdominal pain and 15 pound
Common Questions in Crohn s Disease Therapy Jean-Paul Achkar, MD, FACG Kenneth Rainin Chair for IBD Research Cleveland Clinic Case 23 yo male with 1 year history of diarrhea, abdominal pain and 15 pound
IBD Updates. Themes in IBD IBD management journey. New tools for therapeutic monitoring. First-line treatment in IBD
 IBD Updates Maria T. Abreu, MD University of Miami Miller School of Medicine Miami, Florida Themes in IBD 213 First-line treatment in IBD New tools for therapeutic monitoring Biologic therapy for CD and
IBD Updates Maria T. Abreu, MD University of Miami Miller School of Medicine Miami, Florida Themes in IBD 213 First-line treatment in IBD New tools for therapeutic monitoring Biologic therapy for CD and
Biologic Therapy for Inflammatory. Is Top-Down Too Top-Heavy? S. Devi Rampertab, MD, FACG, AGAF Associate Professor of Medicine University of Florida
 Biologic Therapy for Inflammatory Bowel Disease: Is Top-Down Too Top-Heavy? S. Devi Rampertab, MD, FACG, AGAF Associate Professor of Medicine University of Florida Learning Objectives Evaluate evidence
Biologic Therapy for Inflammatory Bowel Disease: Is Top-Down Too Top-Heavy? S. Devi Rampertab, MD, FACG, AGAF Associate Professor of Medicine University of Florida Learning Objectives Evaluate evidence
An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease. David A. Schwartz, MD
 An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University
An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University
How to Optimize Induction and Maintenance Responses: Definitions and Dosing Advances in Inflammatory Bowel Disease December 6, 2009
 How to Optimize Induction and Maintenance Responses: Definitions and Dosing 2009 Advances in Inflammatory Bowel Disease December 6, 2009 Fernando Velayos MD MPH University of California, San Francisco
How to Optimize Induction and Maintenance Responses: Definitions and Dosing 2009 Advances in Inflammatory Bowel Disease December 6, 2009 Fernando Velayos MD MPH University of California, San Francisco
Agenda. Predictive markers in IBD. Management of ulcerative colitis. Management of Crohn s disease
 Agenda Predictive markers in IBD Management of ulcerative colitis Management of Crohn s disease 2 Patients With UC (%) Distribution of UC Disease Severity at Presentation 1 Fulminant disease (9%) 8 6 4
Agenda Predictive markers in IBD Management of ulcerative colitis Management of Crohn s disease 2 Patients With UC (%) Distribution of UC Disease Severity at Presentation 1 Fulminant disease (9%) 8 6 4
CCFA. Crohns Disease vs UC: What is the best treatment for me? November
 CCFA Crohns Disease vs UC: What is the best treatment for me? November 8 2009 Ellen J. Scherl,, MD, FACP,AGAF Roberts Inflammatory Bowel Disease Center Weill Medical College Cornell University New York
CCFA Crohns Disease vs UC: What is the best treatment for me? November 8 2009 Ellen J. Scherl,, MD, FACP,AGAF Roberts Inflammatory Bowel Disease Center Weill Medical College Cornell University New York
Treatment Goals. Current Therapeutic Pyramids Crohn s Disease Ulcerative Colitis 11/14/10
 Current Management of IBD: From Conventional Agents to Biologics Stephen B. Hanauer, M.D. University of Chicago Treatment Goals Induce and maintain response/ remission Prevent complications Improve quality
Current Management of IBD: From Conventional Agents to Biologics Stephen B. Hanauer, M.D. University of Chicago Treatment Goals Induce and maintain response/ remission Prevent complications Improve quality
Join the conversation at #GIFORUMCCFA
 1 Join the conversation at #GIFORUMCCFA 2 Disclosures In accordance with the ACCME Standards for Commercial Support of CME, the speakers for this course have been asked to disclose to participants the
1 Join the conversation at #GIFORUMCCFA 2 Disclosures In accordance with the ACCME Standards for Commercial Support of CME, the speakers for this course have been asked to disclose to participants the
John F. Valentine, MD Inflammatory Bowel Disease Program University of Utah
 John F. Valentine, MD Inflammatory Bowel Disease Program University of Utah Hawaii 1/20/2017 DISCLOSURES Research Support: NIH, Pfizer, Celgene, AbbVie, Roche/Genentech, Takeda, CCFA OBJECTIVES Review
John F. Valentine, MD Inflammatory Bowel Disease Program University of Utah Hawaii 1/20/2017 DISCLOSURES Research Support: NIH, Pfizer, Celgene, AbbVie, Roche/Genentech, Takeda, CCFA OBJECTIVES Review
Update on Biologics in Ulcerative Colitis. Scott Plevy, MD University of North Carolina Chapel Hill, NC
 Update on Biologics in Ulcerative Colitis Scott Plevy, MD University of North Carolina Chapel Hill, NC Objectives Discuss the latest advances in the pharmacologic management of ulcerative colitis Describe
Update on Biologics in Ulcerative Colitis Scott Plevy, MD University of North Carolina Chapel Hill, NC Objectives Discuss the latest advances in the pharmacologic management of ulcerative colitis Describe
Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy
 Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy Stephen B. Hanauer, MD University of Chicago Potential Conflicts: Centocor/Schering, Abbott, UCB, Elan, Berlex, PDL Goals of Treatment
Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy Stephen B. Hanauer, MD University of Chicago Potential Conflicts: Centocor/Schering, Abbott, UCB, Elan, Berlex, PDL Goals of Treatment
Positioning New Therapies
 Positioning New Therapies Stephen Hanauer, MD Professor of Medicine Medical Director, Digestive Disease Center Northwestern Medicine Chicago, Illinois Speaker Disclosure Stephen Hanauer, MD has disclosed
Positioning New Therapies Stephen Hanauer, MD Professor of Medicine Medical Director, Digestive Disease Center Northwestern Medicine Chicago, Illinois Speaker Disclosure Stephen Hanauer, MD has disclosed
Recent Advances in the Management of Refractory IBD
 Recent Advances in the Management of Refractory IBD Raina Shivashankar, M.D. Assistant Professor of Medicine Division of Gastroenterology and Hepatology Thomas Jefferson University Philadelphia, PA Outline
Recent Advances in the Management of Refractory IBD Raina Shivashankar, M.D. Assistant Professor of Medicine Division of Gastroenterology and Hepatology Thomas Jefferson University Philadelphia, PA Outline
Mono or Combination Therapy with. Individualized Approach
 Mono Combination Therapy with Biologics i in IBD: Developing an Individualized Approach David T. Rubin, MD, FACG Co-Direct, Inflammaty Bowel Disease Center Fellowship Program Direct University of Chicago
Mono Combination Therapy with Biologics i in IBD: Developing an Individualized Approach David T. Rubin, MD, FACG Co-Direct, Inflammaty Bowel Disease Center Fellowship Program Direct University of Chicago
Biologics in IBD. Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College
 Biologics in IBD Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College Case 30 year old man diagnosed with ulcerative proctitis diagnosed in 2003 Had been maintained
Biologics in IBD Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College Case 30 year old man diagnosed with ulcerative proctitis diagnosed in 2003 Had been maintained
Azathioprine for Induction and Maintenance of Remission in Crohn s Disease
 Azathioprine for Induction and Maintenance of Remission in Crohn s Disease William J. Sandborn, MD Chief, Division of Gastroenterology Director, UCSD IBD Center Objectives Azathioprine as induction and
Azathioprine for Induction and Maintenance of Remission in Crohn s Disease William J. Sandborn, MD Chief, Division of Gastroenterology Director, UCSD IBD Center Objectives Azathioprine as induction and
Fibrotic complications of inflammatory bowel disease
 January 27th 2017, 8th Gastro Foundation Weekend for Fellows; Spier Hotel & Conference Centre, Stellenbosch Fibrotic complications of inflammatory bowel disease Gerhard Rogler, Department of Gastroenterology
January 27th 2017, 8th Gastro Foundation Weekend for Fellows; Spier Hotel & Conference Centre, Stellenbosch Fibrotic complications of inflammatory bowel disease Gerhard Rogler, Department of Gastroenterology
Optimizing Immunomodulators and
 Optimizing Immunomodulators and Biologics i in Inflammatory Bowel Disease Sunanda Kane, MD, MSPH, FACG Professor of Medicine Division of Gastroenterology and Hepatology Mayo Clinic Rochester, Minnesota,
Optimizing Immunomodulators and Biologics i in Inflammatory Bowel Disease Sunanda Kane, MD, MSPH, FACG Professor of Medicine Division of Gastroenterology and Hepatology Mayo Clinic Rochester, Minnesota,
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
Medical Therapy for Pediatric IBD: Efficacy and Safety
 Medical Therapy for Pediatric IBD: Efficacy and Safety Betsy Maxwell, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Pediatric IBD: Defining Remission
Medical Therapy for Pediatric IBD: Efficacy and Safety Betsy Maxwell, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Pediatric IBD: Defining Remission
Anne Griffiths MD, FRCPC. SickKids Hospital, University of Toronto. Buenos Aires, August 16, 2014
 Management and Medical Therapies for Crohn disease: strategies to enhance mucosal healing Anne Griffiths MD, FRCPC SickKids Hospital, University of Toronto Buenos Aires, August 16, 2014 New onset Crohn
Management and Medical Therapies for Crohn disease: strategies to enhance mucosal healing Anne Griffiths MD, FRCPC SickKids Hospital, University of Toronto Buenos Aires, August 16, 2014 New onset Crohn
COPYRIGHT. Inflammatory Bowel Disease What Every Clinician Needs to Know. Adam S. Cheifetz, MD. Director, Center for Inflammatory Bowel Disease
 Inflammatory Bowel Disease What Every Clinician Needs to Know Adam S. Cheifetz, MD Director, Center for Inflammatory Bowel Disease Beth Israel Deaconess Medical Center Associate Professor of Medicine Harvard
Inflammatory Bowel Disease What Every Clinician Needs to Know Adam S. Cheifetz, MD Director, Center for Inflammatory Bowel Disease Beth Israel Deaconess Medical Center Associate Professor of Medicine Harvard
Disease behavior in adult patients- are there predictors for stricture or fistula formation?
 Disease behavior in adult patients- are there predictors for stricture or fistula formation? Falk Symposium 168, Madrid, Spain Iris Dotan, M.D., Head, IBD Center, Department of Gastroenterology and Liver
Disease behavior in adult patients- are there predictors for stricture or fistula formation? Falk Symposium 168, Madrid, Spain Iris Dotan, M.D., Head, IBD Center, Department of Gastroenterology and Liver
Strategies for changing the course of Crohn s disease
 Strategies for changing the course of Crohn s disease Maria T. Abreu, MD University of Miami Miller School of Medicine Miami, Florida Where we are now and where we want to be Diagnosis (usually endoscopy)
Strategies for changing the course of Crohn s disease Maria T. Abreu, MD University of Miami Miller School of Medicine Miami, Florida Where we are now and where we want to be Diagnosis (usually endoscopy)
Latest Treatment Updates for Ulcerative Colitis: Evolving Treatment Goals
 Latest Treatment Updates for Ulcerative Colitis: Evolving Treatment Goals Stephen Hanauer, MD Professor of Medicine Medical Director, Digestive Disease Center Northwestern Medicine Chicago, Illinois Speaker
Latest Treatment Updates for Ulcerative Colitis: Evolving Treatment Goals Stephen Hanauer, MD Professor of Medicine Medical Director, Digestive Disease Center Northwestern Medicine Chicago, Illinois Speaker
5/2/2018 SHOULD DEEP REMISSION BE A TREATMENT GOAL? YES! Disclosures: R. Balfour Sartor, MD
 5/2/218 SHOULD DEEP REMISSION BE A TREATMENT GOAL? YES! Disclosures: R. Balfour Sartor, MD Grant support for preclinical studies: Janssen, Gusto Global, Vedanta, Artizan BALFOUR SARTOR, MD DISTINGUISHED
5/2/218 SHOULD DEEP REMISSION BE A TREATMENT GOAL? YES! Disclosures: R. Balfour Sartor, MD Grant support for preclinical studies: Janssen, Gusto Global, Vedanta, Artizan BALFOUR SARTOR, MD DISTINGUISHED
Mucosal healing: does it really matter?
 Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does it really matter? Professor Jean-Frédéric Colombel, New York, USA Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does
Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does it really matter? Professor Jean-Frédéric Colombel, New York, USA Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does
Crohn s Disease: Should We Treat Based on Symptoms or Based on Objective Markers of Inflammation?
 Crohn s Disease: Should We Treat Based on Symptoms or Based on Objective Markers of Inflammation? Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology and Hepatology Mayo Clinic
Crohn s Disease: Should We Treat Based on Symptoms or Based on Objective Markers of Inflammation? Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology and Hepatology Mayo Clinic
Choosing and Positioning Biologic Therapy for Crohn s Disease: (Still) Looking for the Crystal Ball
 Looking for the Crystal Ball") Choosing and Positioning Biologic Therapy for Crohn s Disease: (Still) Looking for the Crystal Ball Siddharth Singh, MD, MS Assistant Professor of Medicine Division of Gastroenterology Division of Biomedical
Choosing and Positioning Biologic Therapy for Crohn s Disease: (Still) Looking for the Crystal Ball Siddharth Singh, MD, MS Assistant Professor of Medicine Division of Gastroenterology Division of Biomedical
Selby Inflamm Bowel Dis. 2008:14:
 Medical Management of Inflammatory Bowel Disease Freddy Caldera D.O. Assistant Professor Division of Gastroenterology Objectives Discuss Crohn s disease and Ulcerative Colitis Discuss Medications for Inflammatory
Medical Management of Inflammatory Bowel Disease Freddy Caldera D.O. Assistant Professor Division of Gastroenterology Objectives Discuss Crohn s disease and Ulcerative Colitis Discuss Medications for Inflammatory
Drug Level Monitoring in IBD. Objectives
 Drug Level Monitoring in IBD Corey A. Siegel, MD, MS Director, Dartmouth-Hitchcock IBD Center Associate Professor of Medicine, Geisel School of Medicine at Dartmouth Objectives Review non-biologic drug
Drug Level Monitoring in IBD Corey A. Siegel, MD, MS Director, Dartmouth-Hitchcock IBD Center Associate Professor of Medicine, Geisel School of Medicine at Dartmouth Objectives Review non-biologic drug
Predicting the natural history of IBD. Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium
 Predicting the natural history of IBD Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium Patient 1 Patient 2 Age 22 Frequent cramps and diarrhea for 6 months Weight
Predicting the natural history of IBD Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium Patient 1 Patient 2 Age 22 Frequent cramps and diarrhea for 6 months Weight
Disclosures. What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists
 What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists Disclosures No financial relationships to disclose. 1 Learning Objectives Case 24M with ileocolonic
What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists Disclosures No financial relationships to disclose. 1 Learning Objectives Case 24M with ileocolonic
Emerging g therapies for IBD: A practical approach to positioning. Sequential Therapies for IBD
 Emerging g therapies for IBD: A practical approach to positioning Stephen B. Hanauer, MD Sequential Therapies for IBD Disease Severity at Presentation Severe Anti-TNF +/IS Cyclosporine (UC) Colectomy (UC)
Emerging g therapies for IBD: A practical approach to positioning Stephen B. Hanauer, MD Sequential Therapies for IBD Disease Severity at Presentation Severe Anti-TNF +/IS Cyclosporine (UC) Colectomy (UC)
Severe IBD: What to Do When Anti- TNFs Don t Work?
 Severe IBD: What to Do When Anti- TNFs Don t Work? David T. Rubin, MD, FACG Professor of Medicine Co-Director, Inflammatory Bowel Disease Center Interim Chief, Section of Gastroenterology, Hepatology and
Severe IBD: What to Do When Anti- TNFs Don t Work? David T. Rubin, MD, FACG Professor of Medicine Co-Director, Inflammatory Bowel Disease Center Interim Chief, Section of Gastroenterology, Hepatology and
Available Data on Pediatric Exposure Response a Clinician s Perspective
 Available Data on Pediatric Exposure Response a Clinician s Perspective Marla Dubinsky, MD Professor of Pediatrics and Medicine Chief Pediatric GI and Nutrition Co-Director Susan and Leonard Feinstein
Available Data on Pediatric Exposure Response a Clinician s Perspective Marla Dubinsky, MD Professor of Pediatrics and Medicine Chief Pediatric GI and Nutrition Co-Director Susan and Leonard Feinstein
Optimizing the effectiveness of anti-tnf therapy in paediatric IBD
 Optimizing the effectiveness of anti-tnf therapy in paediatric IBD Anne Griffiths MD, FRCPC Co-Lead, Inflammatory Bowel Disease Center Northbridge Chair in IBD Hospital for Sick Children, Professor of
Optimizing the effectiveness of anti-tnf therapy in paediatric IBD Anne Griffiths MD, FRCPC Co-Lead, Inflammatory Bowel Disease Center Northbridge Chair in IBD Hospital for Sick Children, Professor of
Withdrawal of drug therapy in patients with quiescent Crohn s disease
 Withdrawal of drug therapy in patients with quiescent Crohn s disease DR. JEAN-FRÉDÉRIC COLOMBEL DIRECTOR OF THE IBD CENTER, ICAHN SCHOOL OF MEDICINE AT MOUNT SINAI, NEW YORK, USA Withdrawal of drug therapy
Withdrawal of drug therapy in patients with quiescent Crohn s disease DR. JEAN-FRÉDÉRIC COLOMBEL DIRECTOR OF THE IBD CENTER, ICAHN SCHOOL OF MEDICINE AT MOUNT SINAI, NEW YORK, USA Withdrawal of drug therapy
IBD Understanding Your Medications. Thomas V. Aguirre, MD Santa Barbara GI Consultants
 IBD Understanding Your Medications Thomas V. Aguirre, MD Santa Barbara GI Consultants IBD Understanding Your Medications (& Your Doctor) Thomas V. Aguirre, MD Santa Barbara GI Consultants Disclosure I
IBD Understanding Your Medications Thomas V. Aguirre, MD Santa Barbara GI Consultants IBD Understanding Your Medications (& Your Doctor) Thomas V. Aguirre, MD Santa Barbara GI Consultants Disclosure I
OPTIMAL USE OF IMMUNOMODULATORS AND BIOLOGICS Edward V. Loftus, Jr., MD, FACG
 1C: Advances in Inflammatory Bowel Disease OPTIMAL USE OF IMMUNOMODULATORS AND BIOLOGICS Edward V. Loftus, Jr., MD, FACG narrow interpretation of this presentation topic would A be a discussion of dosing
1C: Advances in Inflammatory Bowel Disease OPTIMAL USE OF IMMUNOMODULATORS AND BIOLOGICS Edward V. Loftus, Jr., MD, FACG narrow interpretation of this presentation topic would A be a discussion of dosing
Immunogenicity of Biologic Agents and How to Prevent Sensitization
 Immunogenicity of Biologic Agents and How to Prevent Sensitization William J. Sandborn, MD Professor and Chief, Division of Gastroenterology Director, UCSD IBD Center La Jolla, California, USA Learning
Immunogenicity of Biologic Agents and How to Prevent Sensitization William J. Sandborn, MD Professor and Chief, Division of Gastroenterology Director, UCSD IBD Center La Jolla, California, USA Learning
Association Between Plasma Concentrations of Certolizumab Pegol and Endoscopic Outcomes of Patients With Crohn's Disease
 Association Between Plasma Concentrations of Certolizumab Pegol and Endoscopic Outcomes of Patients With Crohn's Disease Jean Frédéric Colombel, William J. Sandborn, Matthieu Allez, Jean Louis Dupas, Olivier
Association Between Plasma Concentrations of Certolizumab Pegol and Endoscopic Outcomes of Patients With Crohn's Disease Jean Frédéric Colombel, William J. Sandborn, Matthieu Allez, Jean Louis Dupas, Olivier
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 3 October 2012
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 3 October 2012 REMICADE 100 mg, powder for concentrate for solution for infusion B/1 vial (CIP code: 562 070-1) Applicant:
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 3 October 2012 REMICADE 100 mg, powder for concentrate for solution for infusion B/1 vial (CIP code: 562 070-1) Applicant:
The future of IBD therapeutic research
 The future of IBD therapeutic research Jean-Frederic Colombel, MD Director Susan and Leonard Feinstein IBD Clinical Center Icahn School of Medicine, Mount Sinai Hospital New York J-F Colombel has served
The future of IBD therapeutic research Jean-Frederic Colombel, MD Director Susan and Leonard Feinstein IBD Clinical Center Icahn School of Medicine, Mount Sinai Hospital New York J-F Colombel has served
Personalized Medicine: IBD
 Use of Anti-TNF Antibodies and Other Serologies for Managing IBD Christopher J. Shepela, MD, MS Assistant Professor of Medicine University of Minnesota Medical Director at Digestive Disease Center at Regions
Use of Anti-TNF Antibodies and Other Serologies for Managing IBD Christopher J. Shepela, MD, MS Assistant Professor of Medicine University of Minnesota Medical Director at Digestive Disease Center at Regions
Treating to Achieve a Target and Disease Monitoring in 2015: State of the Art
 Treating to Achieve a Target and Disease Monitoring in 2015: State of the Art David T. Rubin, MD The Joseph B. Kirsner Professor of Medicine Chief, Section of Gastroenterology, Hepatology and Nutrition
Treating to Achieve a Target and Disease Monitoring in 2015: State of the Art David T. Rubin, MD The Joseph B. Kirsner Professor of Medicine Chief, Section of Gastroenterology, Hepatology and Nutrition
New treatment options in UC. Rob Bryant IBD Consultant Royal Adelaide Hospital
 New treatment options in UC Rob Bryant IBD Consultant Royal Adelaide Hospital Talk Outline 1. Raising expectations 2. Optimising UC therapy 3. Clinical trials 4. What s new on the PBS? 5. Questions 1.
New treatment options in UC Rob Bryant IBD Consultant Royal Adelaide Hospital Talk Outline 1. Raising expectations 2. Optimising UC therapy 3. Clinical trials 4. What s new on the PBS? 5. Questions 1.
New Perspectives on the Diagnosis and Management of IBD. Disclosures
 New Perspectives on the Diagnosis and Management of IBD Joel R. Rosh, MD Director, Pediatric Gastroenterology Goryeb Children's Hospital/Atlantic Health Professor of Pediatrics Icahn School of Medicine
New Perspectives on the Diagnosis and Management of IBD Joel R. Rosh, MD Director, Pediatric Gastroenterology Goryeb Children's Hospital/Atlantic Health Professor of Pediatrics Icahn School of Medicine
CROHN'S DISEASE/ULCERATIVE COLITIS TREATMENT ALGORITHM
 CROHN'S DISEASE/ULCERATIVE COLITIS TREATMENT ALGORITHM Crohn's Disease Ulcerative Colitis Steroids x 2 No prior AZA/6-MP Biologic Agent AZA/6-MP STEP-UP MANAGEMENT APPROACH Advantages Patients attain remission
CROHN'S DISEASE/ULCERATIVE COLITIS TREATMENT ALGORITHM Crohn's Disease Ulcerative Colitis Steroids x 2 No prior AZA/6-MP Biologic Agent AZA/6-MP STEP-UP MANAGEMENT APPROACH Advantages Patients attain remission
Indications for use of Infliximab
 Indications for use of Infliximab Moscow, June 10 th 2006 Prof. Dr. Dr. Gerhard Rogler Klinik und Poliklinik für Innere Medizin I Universität Regensburg Case report 1989: Diagnosis of Crohn s disease of
Indications for use of Infliximab Moscow, June 10 th 2006 Prof. Dr. Dr. Gerhard Rogler Klinik und Poliklinik für Innere Medizin I Universität Regensburg Case report 1989: Diagnosis of Crohn s disease of
Crohn s
 Crohn s Disease David T. Rubin, MD, AGAF Joseph B. Kirsner Professor of Medicine Chief, Section of Gastroenterology, Hepatology, and Nutrition Co-Director, Digestive Diseases Center @IBDMD Disclosures
Crohn s Disease David T. Rubin, MD, AGAF Joseph B. Kirsner Professor of Medicine Chief, Section of Gastroenterology, Hepatology, and Nutrition Co-Director, Digestive Diseases Center @IBDMD Disclosures
How to use infliximab?
 How to use infliximab? Séverine Vermeire, MD, PhD Division of Gastroenterology University Hospital Gasthuisberg Leuven The how to use infliximab rules Before starting IFX: try optimizing chances for response!
How to use infliximab? Séverine Vermeire, MD, PhD Division of Gastroenterology University Hospital Gasthuisberg Leuven The how to use infliximab rules Before starting IFX: try optimizing chances for response!
The Refractory Crohn s Disease
 The Refractory Crohn s Disease Patient David T. Rubin, MD, FACG Professor of Medicine Co-Director, Inflammatory Bowel Disease Center Interim Chief, Section of Gastroenterology, Hepatology and Nutrition
The Refractory Crohn s Disease Patient David T. Rubin, MD, FACG Professor of Medicine Co-Director, Inflammatory Bowel Disease Center Interim Chief, Section of Gastroenterology, Hepatology and Nutrition
Crohn's Disease. The What, When, and Why of Treatment
 Crohn's Disease The What, When, and Why of Treatment Gary R. Lichtenstein, MD, FACG Professor of Medicine Director, Inflammatory Bowel Disease Program University of Pennsylvania Philadelphia, PA In my
Crohn's Disease The What, When, and Why of Treatment Gary R. Lichtenstein, MD, FACG Professor of Medicine Director, Inflammatory Bowel Disease Program University of Pennsylvania Philadelphia, PA In my
PEDIATRIC INFLAMMATORY BOWEL DISEASE
 PEDIATRIC INFLAMMATORY BOWEL DISEASE Alexis Rodriguez, MD Pediatric Gastroenterology Advocate Children s Hospital Disclosers Abbott Nutrition - Speaker Inflammatory Bowel Disease Chronic inflammatory disease
PEDIATRIC INFLAMMATORY BOWEL DISEASE Alexis Rodriguez, MD Pediatric Gastroenterology Advocate Children s Hospital Disclosers Abbott Nutrition - Speaker Inflammatory Bowel Disease Chronic inflammatory disease
Dr David Epstein Vincent Pallotti Hospital and University of Cape Town
 Inflammatory Bowel Disease Management in South Africa in 2016 Pharmaceutical Care Management Association Dr David Epstein Vincent Pallotti Hospital and University of Cape Town Inflammatory Bowel Disease
Inflammatory Bowel Disease Management in South Africa in 2016 Pharmaceutical Care Management Association Dr David Epstein Vincent Pallotti Hospital and University of Cape Town Inflammatory Bowel Disease
Perianal and Fistulizing Crohn s Disease: Tough Management Decisions. Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic
 Perianal and Fistulizing Crohn s Disease: Tough Management Decisions Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic Talk Overview Background Assessment and Classification
Perianal and Fistulizing Crohn s Disease: Tough Management Decisions Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic Talk Overview Background Assessment and Classification
Preventing post-operative recurrence
 Oxford Inflammatory Bowel Disease MasterClass Preventing post-operative recurrence Dr Oliver Brain Oxford Disclosures Presented at IEE, Oxford 2013 AbbVie sponsored meeting Talk Outline Risk factors for
Oxford Inflammatory Bowel Disease MasterClass Preventing post-operative recurrence Dr Oliver Brain Oxford Disclosures Presented at IEE, Oxford 2013 AbbVie sponsored meeting Talk Outline Risk factors for
Clinical Trials in IBD. Bruce Yacyshyn MD Professor of Medicine Division of Digestive Diseases
 Clinical Trials in IBD Bruce Yacyshyn MD Professor of Medicine Division of Digestive Diseases Objectives Today s discussion will address the following topics: Similarities and differences between Crohn
Clinical Trials in IBD Bruce Yacyshyn MD Professor of Medicine Division of Digestive Diseases Objectives Today s discussion will address the following topics: Similarities and differences between Crohn
Personalized Medicine. Selecting the Right First-line Biologic Agent. Gene Expression Profiles Crohn s Disease. The Right Treatment
 Personalized Medicine Selecting the Right First-line Biologic Agent William Tremaine, M.D. Maxine and Jack Zarrow Professor Mayo Clinic Rochester, MN, USA The Right Treatment Pretreatment Genomic Analysis
Personalized Medicine Selecting the Right First-line Biologic Agent William Tremaine, M.D. Maxine and Jack Zarrow Professor Mayo Clinic Rochester, MN, USA The Right Treatment Pretreatment Genomic Analysis
Definitions. Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency)
") CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
Therapy for Inflammatory Bowel Disease
 Therapy for Inflammatory Bowel Disease Jonathan P. Terdiman, MD Professor of Clinical Medicine Clinical Director, Center for Colitis and Crohn s Disease University of California San Francisco, CA UC: Current
Therapy for Inflammatory Bowel Disease Jonathan P. Terdiman, MD Professor of Clinical Medicine Clinical Director, Center for Colitis and Crohn s Disease University of California San Francisco, CA UC: Current
Implementation of disease and safety predictors during disease management in UC
 Implementation of disease and safety predictors during disease management in UC DR ARIELLA SHITRIT DIGESTIVE DISEASES INSTITUTE SHAARE ZEDEK MEDICAL CENTER JERUSALEM Case presentation A 52 year old male
Implementation of disease and safety predictors during disease management in UC DR ARIELLA SHITRIT DIGESTIVE DISEASES INSTITUTE SHAARE ZEDEK MEDICAL CENTER JERUSALEM Case presentation A 52 year old male
How do I choose amongst medicines for inflammatory bowel disease. Maria T. Abreu, MD
 How do I choose amongst medicines for inflammatory bowel disease Maria T. Abreu, MD Overview of IBD Pathogenesis Bacterial Products Moderately Acutely Inflamed Chronic Inflammation = IBD Normal Gut Mildly
How do I choose amongst medicines for inflammatory bowel disease Maria T. Abreu, MD Overview of IBD Pathogenesis Bacterial Products Moderately Acutely Inflamed Chronic Inflammation = IBD Normal Gut Mildly
Management of Refractory Crohn s Disease
 Management of Refractory Crohn s Disease @IBDMD David T. Rubin, MD, FACG, FASGE Joseph B. Kirsner Professor of Medicine Chief, Section of Gastroenterology, Hepatology and Nutrition Disclosures Consultant
Management of Refractory Crohn s Disease @IBDMD David T. Rubin, MD, FACG, FASGE Joseph B. Kirsner Professor of Medicine Chief, Section of Gastroenterology, Hepatology and Nutrition Disclosures Consultant
Understanding Inflammatory Bowel Diseases: What Every Patient Needs to Know
 Understanding Inflammatory Bowel Diseases: What Every Patient Needs to Know An educational program for patients, families and caregivers living with Crohn s disease and ulcerative colitis. Dr. William
Understanding Inflammatory Bowel Diseases: What Every Patient Needs to Know An educational program for patients, families and caregivers living with Crohn s disease and ulcerative colitis. Dr. William
Positioning Biologics in Ulcerative Colitis
 Positioning Biologics in Ulcerative Colitis Bruce E. Sands, MD, MS Acting Chief, Gastrointestinal Unit Massachusetts General Hospital Associate Professor of Medicine Harvard Medical School Sequential Therapies
Positioning Biologics in Ulcerative Colitis Bruce E. Sands, MD, MS Acting Chief, Gastrointestinal Unit Massachusetts General Hospital Associate Professor of Medicine Harvard Medical School Sequential Therapies
Optimal Use of Immunomodulators and Biologics
 3/17/214 Optimal Use of Immunomodulators and Biologics Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology and Hepatology Mayo Clinic Rochester, Minnesota, U.S.A. Loftus Disclosures
3/17/214 Optimal Use of Immunomodulators and Biologics Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology and Hepatology Mayo Clinic Rochester, Minnesota, U.S.A. Loftus Disclosures
IBD :- a new era of diagnostics and therapy Dr Martyn Dibb Consultant Luminal Gastroenterologist Royal Liverpool University Hospital
 IBD :- a new era of diagnostics and therapy Dr Martyn Dibb Consultant Luminal Gastroenterologist Royal Liverpool University Hospital Aims To understand the aetiology of IBD To understand the impact that
IBD :- a new era of diagnostics and therapy Dr Martyn Dibb Consultant Luminal Gastroenterologist Royal Liverpool University Hospital Aims To understand the aetiology of IBD To understand the impact that
Crohn s Disease: A New Approach to an Old Problem
 Management of Postoperative Crohn s Disease: A New Approach to an Old Problem Miguel Regueiro, M.D. Associate Professor of Medicine Associate Chief for Education Clinical Head and Co-Director, IBD Center
Management of Postoperative Crohn s Disease: A New Approach to an Old Problem Miguel Regueiro, M.D. Associate Professor of Medicine Associate Chief for Education Clinical Head and Co-Director, IBD Center
My Child Has Inflammatory Bowel Disease : Why? What now? What s next?
 My Child Has Inflammatory Bowel Disease : Why? What now? What s next? George M. Zacur, M.D., M.S. Clinical Assistant Professor Department of Pediatrics and Communicable Diseases Division of Gastroenterology
My Child Has Inflammatory Bowel Disease : Why? What now? What s next? George M. Zacur, M.D., M.S. Clinical Assistant Professor Department of Pediatrics and Communicable Diseases Division of Gastroenterology
Use of extrapolation in small clinical trials:
 Use of extrapolation in small clinical trials: Infliximab for pediatric ulcerative colitis Jessica J. Lee, MD, MMSc Medical Officer Division of Gastroenterology and Inborn Errors Products CDER/ FDA 1 Learning
Use of extrapolation in small clinical trials: Infliximab for pediatric ulcerative colitis Jessica J. Lee, MD, MMSc Medical Officer Division of Gastroenterology and Inborn Errors Products CDER/ FDA 1 Learning
Crohn's Disease. The What, When, and Why of Treatment
 Crohn's Disease The What, When, and Why of Treatment Sunanda Kane, MD, FACG Professor of Medicine Department of Gastroenterology and Hepatology Mayo Clinic Rochester, MN In my lecture today, I will be
Crohn's Disease The What, When, and Why of Treatment Sunanda Kane, MD, FACG Professor of Medicine Department of Gastroenterology and Hepatology Mayo Clinic Rochester, MN In my lecture today, I will be
Moderately to severely active ulcerative colitis
 Adalimumab in the Treatment of Moderate-to-Severe Ulcerative Colitis: ULTRA 2 Trial Results Sandborn WJ, van Assche G, Reinisch W, et al. Adalimumab induces and maintains clinical remission in patients
Adalimumab in the Treatment of Moderate-to-Severe Ulcerative Colitis: ULTRA 2 Trial Results Sandborn WJ, van Assche G, Reinisch W, et al. Adalimumab induces and maintains clinical remission in patients
To help protect your privacy, PowerPoint prevented this external picture from being automatically downloaded. To download and display this picture,
 To help protect your privacy, PowerPoint prevented this external picture from being automatically downloaded. To download and display this picture, click Options in the Message Bar, and then click Enable
To help protect your privacy, PowerPoint prevented this external picture from being automatically downloaded. To download and display this picture, click Options in the Message Bar, and then click Enable
Anti tumor necrosis factor (TNF) agents have
 agents have") Achieving Clinical Response and Remission in Moderate-to-Severe Ulcerative Colitis With Golimumab Sandborn WJ, Feagan BG, Marano C, et al; PURSUIT-SC Study Group. Subcutaneous golimumab induces clinical
Achieving Clinical Response and Remission in Moderate-to-Severe Ulcerative Colitis With Golimumab Sandborn WJ, Feagan BG, Marano C, et al; PURSUIT-SC Study Group. Subcutaneous golimumab induces clinical
Slide 1 Medications in inflammatory bowel disease a primer for health care providers. Slide 2. Slide 3 Theory of pathogenesis. IBD - epidemiology
 Slide 1 Medications in inflammatory bowel disease a primer for health care providers Athos Bousvaros, MD Associate director Inflammatory Bowel Disease Center Boston Children s Hospital 617 355 2962 Slide
Slide 1 Medications in inflammatory bowel disease a primer for health care providers Athos Bousvaros, MD Associate director Inflammatory Bowel Disease Center Boston Children s Hospital 617 355 2962 Slide
Disease Management Strategies for Moderate to Severe IBD in Adults
 Disease Management Strategies for Moderate to Severe IBD in Adults Alyssa Parian, MD Assistant Professor of Medicine Johns Hopkins University April 21, 2016 Outline Overview of IBD Treatments (Benefits/Risks)
Disease Management Strategies for Moderate to Severe IBD in Adults Alyssa Parian, MD Assistant Professor of Medicine Johns Hopkins University April 21, 2016 Outline Overview of IBD Treatments (Benefits/Risks)
Approaches to Inflammatory Bowel Disease
 2:15 3pm Best Approach to Inflammatory Bowel Disease SPEAKER Maria Abreu, MD Presenter Disclosure Information The following relationships exist related to this presentation: Maria Abreu, MD, receives consulting
2:15 3pm Best Approach to Inflammatory Bowel Disease SPEAKER Maria Abreu, MD Presenter Disclosure Information The following relationships exist related to this presentation: Maria Abreu, MD, receives consulting
Biologics in 2016: How Do We Select the Most Appropriate Agent? Gary R. Lichtenstein, MD, FACG University of PA School of Medicine Philadelphia, PA
 Biologics in 2016: How Do We Select the Most Appropriate Agent? Gary R. Lichtenstein, MD, FACG University of PA School of Medicine Philadelphia, PA Overview Indications and Drug Selection Contraindications
Biologics in 2016: How Do We Select the Most Appropriate Agent? Gary R. Lichtenstein, MD, FACG University of PA School of Medicine Philadelphia, PA Overview Indications and Drug Selection Contraindications
Latest Treatment Updates for Crohn s Disease: Tailoring Therapy David G. Binion, M.D.
 Latest Treatment Updates for Crohn s Disease: Tailoring Therapy David G. Binion, M.D. Co-Director, IBD Center Director, Nutrition Support Service UPMC Presbyterian Hospital Division of Gastroenterology,
Latest Treatment Updates for Crohn s Disease: Tailoring Therapy David G. Binion, M.D. Co-Director, IBD Center Director, Nutrition Support Service UPMC Presbyterian Hospital Division of Gastroenterology,
Primer On Personalized Medicine
 Primer On Personalized Medicine Sandeep Gupta MD FACG FASGE AGAF Prashanth Porayette MD PhD Pediatric Gastroenterology, Hepatology, Nutrition, Riley Hospital for Children, Indianapolis, IN 46202 Disclosures:
Primer On Personalized Medicine Sandeep Gupta MD FACG FASGE AGAF Prashanth Porayette MD PhD Pediatric Gastroenterology, Hepatology, Nutrition, Riley Hospital for Children, Indianapolis, IN 46202 Disclosures:
Progress in Inflammatory Bowel Disease
 Progress in Inflammatory Bowel Disease Gary R Lichtenstein, MD Director, Center for IBD University of Pennsylvania School of Medicine Hospital of the University of PA Philadelphia, PA Disclosure Research,
Progress in Inflammatory Bowel Disease Gary R Lichtenstein, MD Director, Center for IBD University of Pennsylvania School of Medicine Hospital of the University of PA Philadelphia, PA Disclosure Research,
Percent Cumulative. Probability. Penetrating. Inflammatory. Stricturing. Months Patients at risk N =
 Fistulizing Crohn s Disease Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology & Hepatology Mayo Clinic Rochester, Minnesota, USA Outline Fistulizing Crohn s Etiology Incidence
Fistulizing Crohn s Disease Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology & Hepatology Mayo Clinic Rochester, Minnesota, USA Outline Fistulizing Crohn s Etiology Incidence
Diagnostic and Therapeutic Approaches to Dysplasia in Inflammatory Bowel Diseases
 Diagnostic and Therapeutic Approaches to Dysplasia in Inflammatory Bowel Diseases Parakkal Deepak, M.B.B.S., M.S. Assistant Professor of Medicine Division of Gastroenterology John T. Milliken Department
Diagnostic and Therapeutic Approaches to Dysplasia in Inflammatory Bowel Diseases Parakkal Deepak, M.B.B.S., M.S. Assistant Professor of Medicine Division of Gastroenterology John T. Milliken Department
5-ASA Therapy, Steroids and Antibiotics in Inflammatory Bowel Disease
 5-ASA Therapy, Steroids and Antibiotics in Inflammatory Bowel Disease David T. Rubin, MD Associate Professor of Medicine Co-Director, Inflammatory Bowel Disease Center University it of Chicago Medical
5-ASA Therapy, Steroids and Antibiotics in Inflammatory Bowel Disease David T. Rubin, MD Associate Professor of Medicine Co-Director, Inflammatory Bowel Disease Center University it of Chicago Medical
Addressing Risks and Benefits In IBD
 Addressing Risks and Benefits In IBD Gil Y. Melmed, MD, MS Assistant Professor of Medicine, Cedars-Sinai Medical Center David Geffen School of Medicine at UCLA www.nomorecrohnsdisease.com "Jaw Dropping
Addressing Risks and Benefits In IBD Gil Y. Melmed, MD, MS Assistant Professor of Medicine, Cedars-Sinai Medical Center David Geffen School of Medicine at UCLA www.nomorecrohnsdisease.com "Jaw Dropping
Fistulizing Crohn s Disease: The Aggressive Approach
 Fistulizing Crohn s Disease: The Aggressive Approach Bruce E. Sands, MD, MS MGH Crohn s and Colitis Center and Gastrointestinal Unit Massachusetts General Hospital Boston, USA Case Presentation: Summary
Fistulizing Crohn s Disease: The Aggressive Approach Bruce E. Sands, MD, MS MGH Crohn s and Colitis Center and Gastrointestinal Unit Massachusetts General Hospital Boston, USA Case Presentation: Summary
Best Practices in the Diagnosis and Treatment of Inflammatory Bowel Disease
 Mark Lazarev, MD November 14, 2013 Assistant Professor of Medicine, Johns Hopkins University School of Medicine Best Practices in the Diagnosis and Treatment of Inflammatory Bowel Disease 1 Talk outline
Mark Lazarev, MD November 14, 2013 Assistant Professor of Medicine, Johns Hopkins University School of Medicine Best Practices in the Diagnosis and Treatment of Inflammatory Bowel Disease 1 Talk outline
Mucosal Healing in Crohn s Disease. Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium
 Mucosal Healing in Crohn s Disease Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium Mucosal Lesions in CD: General Features CD can affect the entire GI tract
Mucosal Healing in Crohn s Disease Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium Mucosal Lesions in CD: General Features CD can affect the entire GI tract
Understanding Inflammatory Bowel Diseases (IBD):
:") Understanding Inflammatory Bowel Diseases (IBD): What Every Patient Needs to Know William H Holderman, MD Digestive Health Specialists Tacoma, WA Today s Objectives Define IBD, its potential causes and
Understanding Inflammatory Bowel Diseases (IBD): What Every Patient Needs to Know William H Holderman, MD Digestive Health Specialists Tacoma, WA Today s Objectives Define IBD, its potential causes and