Diagnosis of TB: Radiology David Finlay, MD
|
|
|
- Alexis Blair
- 6 years ago
- Views:
Transcription
1 TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1



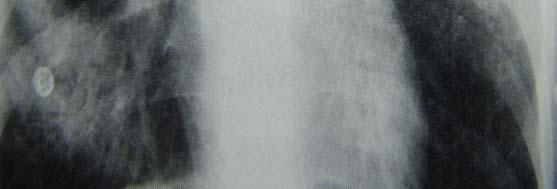
2 Primary Tuberculosis hilar or paratracheal lymphadenopathy with or without a parenchymal infiltrate is characteristic. bilateral lymphadenopathy in up to 15% lymphadenopathy may result in lobar atelectasis due to bronchial compression. 3 2





3 3

4 Primary Tuberculosis acquired by inhalation of airborne organisms right middle lobe, lower lobes most frequent focal pneumonitis, with caseous necrosis and lymphatic spread to ipsilateral hilar and mediastinal nodes most common radiographic appearance normal. 7 4

5 Primary tuberculosis immunity results in 90-95% 95% of patients with development of lung and hilar mediastinal granulomas, often calcified, which may or may not be visible on chest x-ray. 10 5




6 6
7 Primary tuberculosis may have hematogenous spread, which also becomes inactive and calcifies as immunity develops. Ghon lesion calcified nodule with parenchymal scar. Ranke complex Ghon lesion & calcified hilar node. 13 Primary Tuberculosis usually asymptomatic in 5-10% the infection is poorly controlled, resulting in progressive primary tuberculosis. 14 7


")
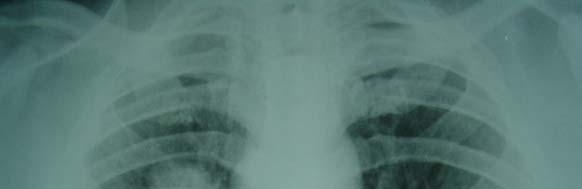
8 Progressive primary tuberculosis extensive cavitation of tuberculous pneumonia with endobronchial spread rupture of necrotic nodes into bronchi results in further endobronchial spread, as well as hematogenous spread pleural effusion (25%) hypersensitivity reaction. 15 8



9 Reactivation or Post Primary Tuberculosis as hypersensitivity develops, granulomas heal with calcification and fibrosis viable organisms may survive, and enter dormant phase reactivate at later date with immunosuppresion, stress, and/or reexposure 18 9
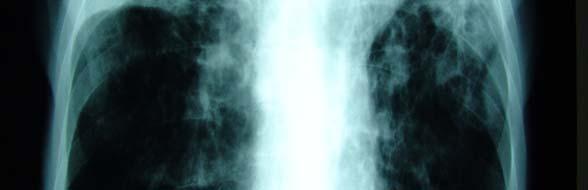
10 Reactivation tuberculosis characteristically have apical abnormalities.(up to 90%) usually posterior segment upper lobe. 19 Reactivation tuberculosis Radiographic findings patchy consolidation with streaky opacities (100%) primarily apical posterior upper lobes (90%) cavitation 45% bronchogenic spread of disease with ill-defined nodules (20-25%) fibrosis (30%) pleural effusion (20%) 20 10






11 11


12 Inactive vs. Active Tuberculosis may be impossible to tell on x-ray active disease suggested by focal consolidation with cavities in upper lobes or superior segment of lower lobes endobronchial spread due to active disease often results in poorly defined nodules between 5-10mm in size, acinar nodules if radiograph changes with treatment, active disease. lack of change on radiographs over 6 months suggests disease inactivity


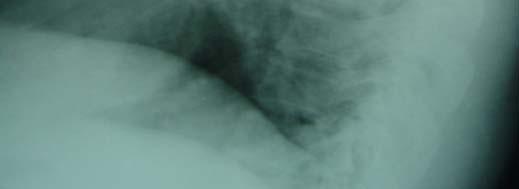
13 Pleural effusions primary TB (25%) hypersensitivity reaction to TB proteins organisms uncommonly isolated from fluid may be unassociated with obvious parenchymal disease on CXR 26 13






14 14

15 15



16 Pleural effusion post primary TB (20%) caused by rupture of a tuberculous cavity into the pleural space, causing empyema may cause bronchopleural fistula with air fluid levels often results in irreversible pleural thickening and calcification 31 16





17 17

 small")

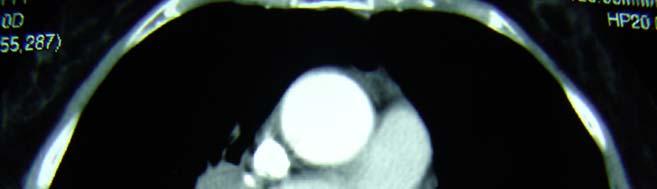
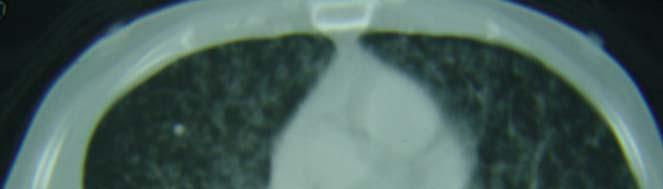
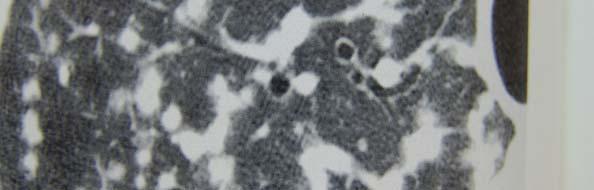
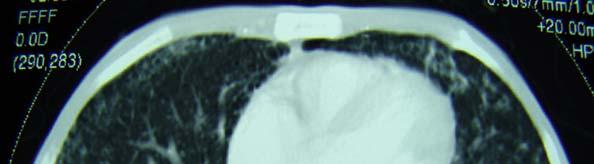
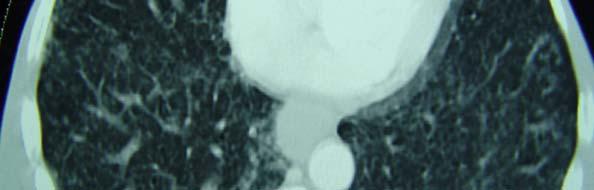
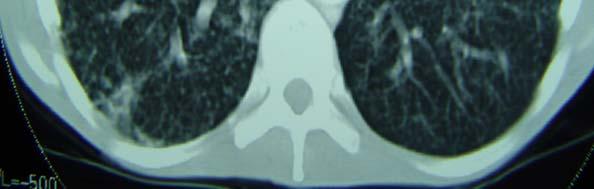
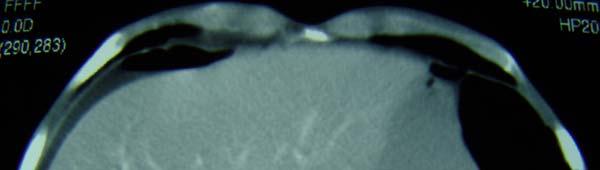
18 CT / HRCT findings airspace consolidation cavitation ill defined air space nodules (endobronchial spread) small diffuse nodules (miliary) due to hematogenous dissemination 36 18




19 19





20 20
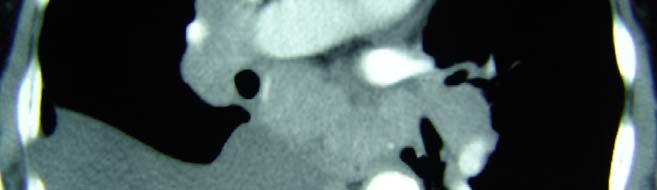
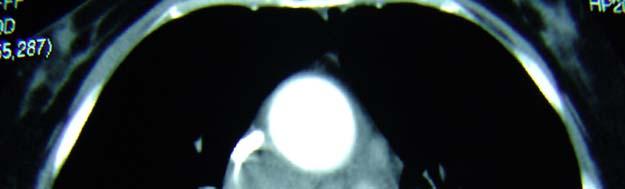
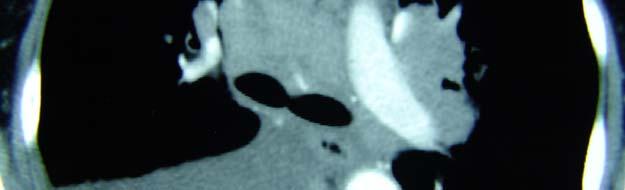
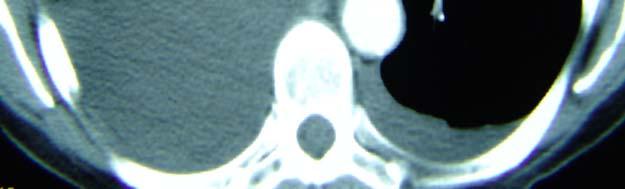
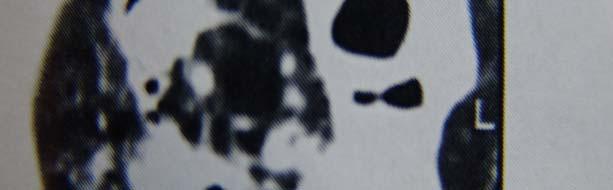
21 CT/ HRCT findings pleural effusion lymph node enlargement with central necrosis interlobular septal thickening bronchovascular distortion and impaction 42 21


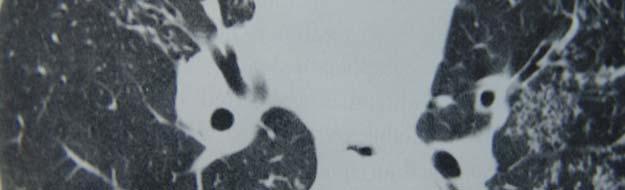
22 Tuberculous cavities usually have thick, irregular walls with treatment, walls thin and cavity shrinks and usually collapse 44 22





23 23
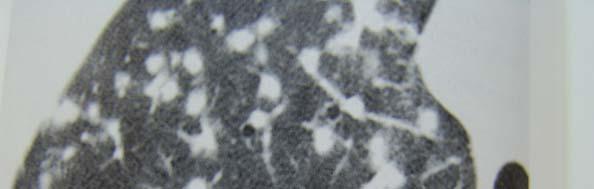
24 With treatment, increase in bronchovasular distortion, emphysema, fibrosis and bronchiectasis 47 HRCT findings of active disease Rosettes of centrilobular nodules, 2-10mm in diameter branching centrilobular opacities-- tree-inbud 48 24



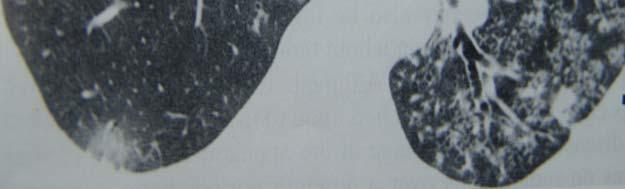
25 Tree in bud represents solid caseous material filling or surrounding terminal bronchioles or alveolar ducts. may coalesce, resulting in focal areas of bronchopneumonia usually reversible, resolving within 5-9 months of treatment 49 25



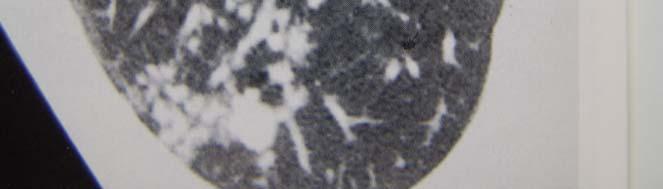
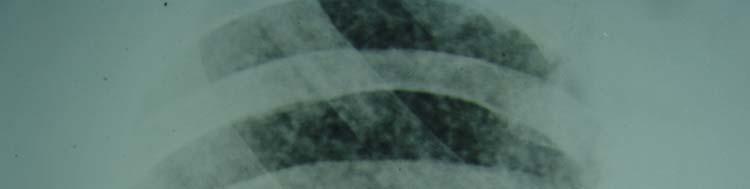
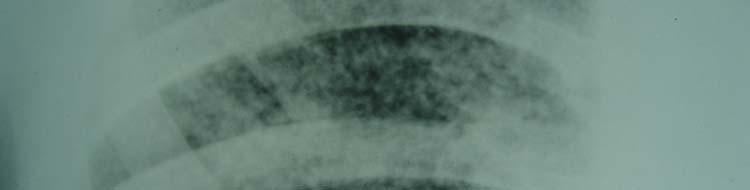
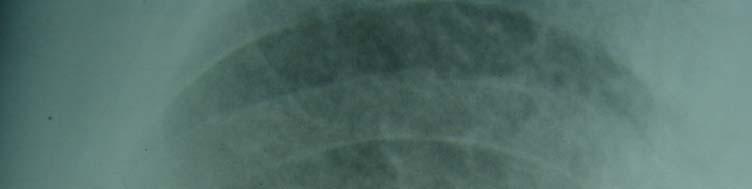
26 Miliary TB fine nodular or reticulonodular pattern, evenly distributed distinguished from endobronchial spread by uniform size of nodules and even distribution can occur with reactivation of progressive Primary TB 51 26


27 27


28 28
 57")
29 Lymphadenopathy more common in primary TB than post primary TB central necrosis particularly high incidence in AIDS, associated with rim enhancement (85%) 57 29
30 CT / HRCT more sensitive than chest radiography in detection and characterization of parenchymal and mediastinal disease, particularly in primary tuberculosis more accurately defines and characterizes lymphadenopathy 59 Reactivation TB complications pneumothorax due to cavity rapture into pleural space can also occur due to formation of subpleural blebs 60 30
31 Mycetomas (fungus balls) common in patients with cavitary tuberculosis colonization of cavities by aspergillus best shown by CT 61 Mycetoma intracavitary mass with an air-crescent sign changes position in cavity with prone/ decubitus scans not specific to tuberculous cavities (sarcoid, bulla, etc.) 62 31




32 32


33 33


34 TB and AIDS TB reported in up to 10% of AIDS patients radiographic appearance is more similar to primary TB, although reactivation is the most likely mechanism non cavitary consolidation in upper & lower regions associated with hilar / mediastinal lymphadenopathy 67 34





35 35
36 TB and AIDS atypical mycobacterial disease also commonly seen AIDS indicator disease in HIV patients with CD4 counts below 200 radiographic findings of TB in HIV/AIDs reflects extent of cellular immune compromise 71 TB and AIDS if CD4 count greater than 200, tuberculosis is indistinguishable from non-hiv patients (upper lobe cavitary infiltrates) if CD4 count less than 200, radiographic findings are similar to primary tuberculosis (80%) Dissemination is also more common in patients with greater degrees of immunocompromise, with miliary and extrapulmonary disease 72 36




37 37




38 38



39 TB and AIDS Normal CXR reported in up to 15% of AIDS / HIV patients with isolated TB CT much more sensitive in these cases 78 39
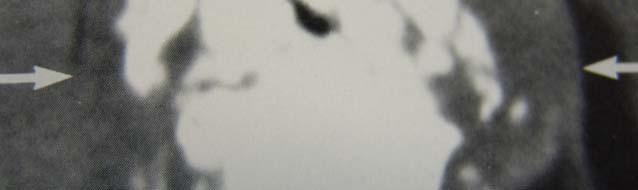
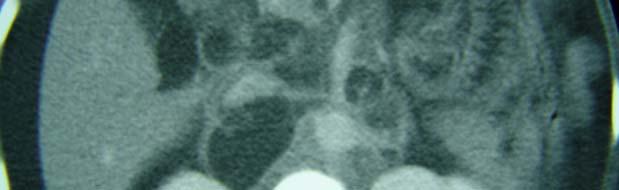
40 TB and AIDS 30-60% with tuberculosis have extra pulmonary foci, and only half of these have identifiable concomitant pulmonary infection abscesses of multiple organs including prostate, liver, spleen, chest and abdominal wall, and pancreas 79 Extrapulmonary manifestations of Tuberculosis exposure of superficial mucosal surfaces to infected respiratory secretions contiguous spread lymphohematogenous dissemination (especially in immunocompromised hosts) 80 40



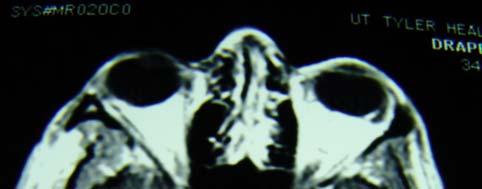
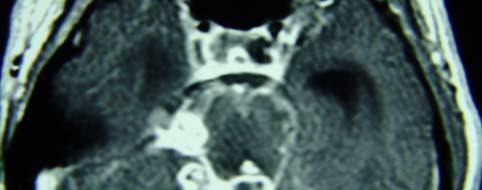
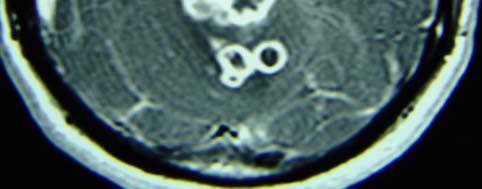
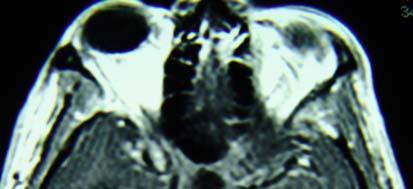
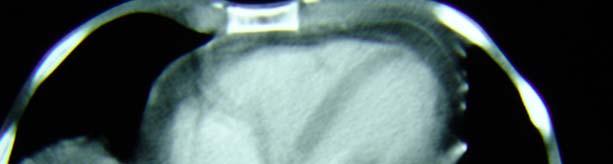
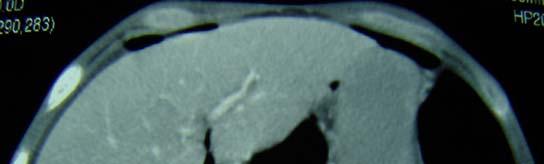
41 Hematogenous dissemination involves organ systems in proportion to blood flow spleen,liver,lungs, bone marrow, kidneys, adrenals, eyes splenomegaly or hepatomegaly with small abscesses meningitis, choroid plexus, pericarditis 82 41





42 42



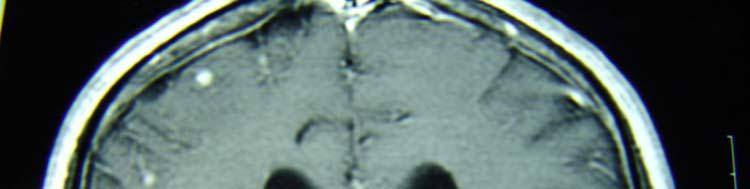
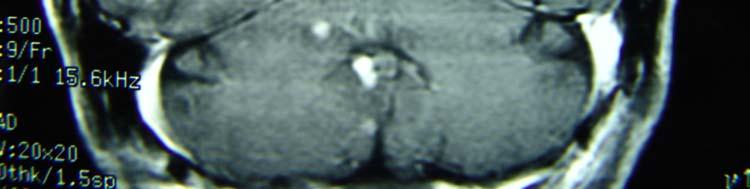
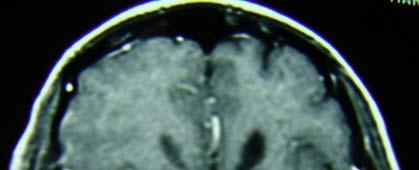
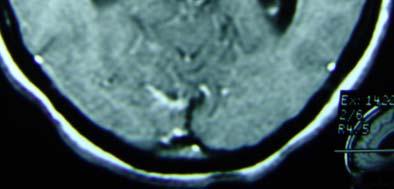
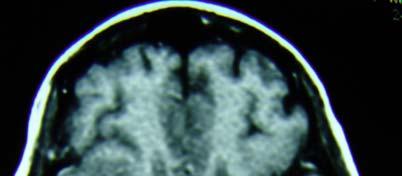
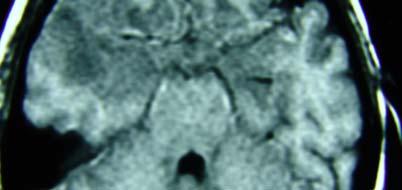
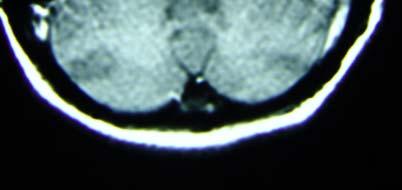
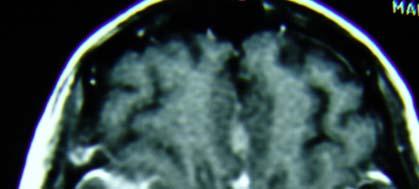
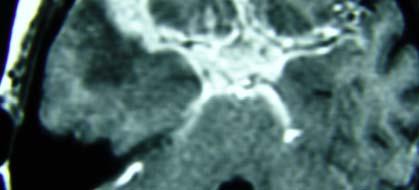
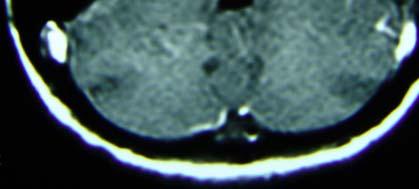
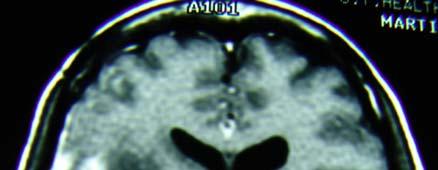
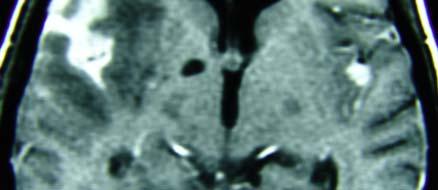
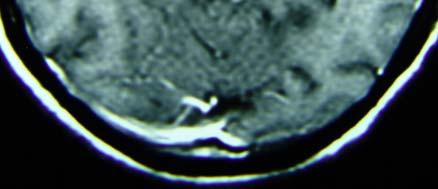
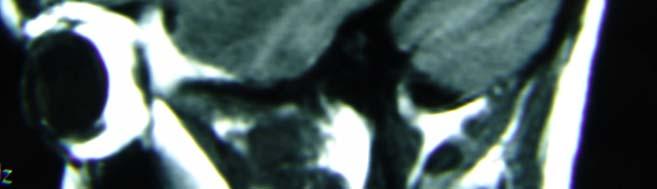
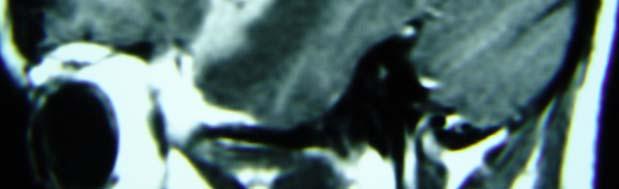
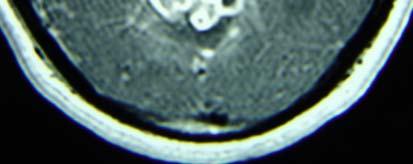
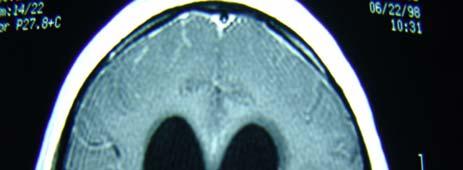
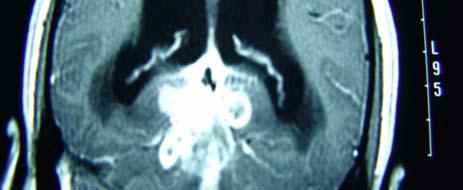
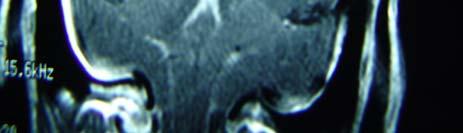
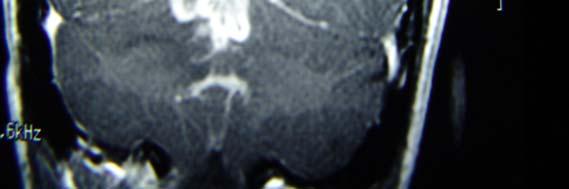
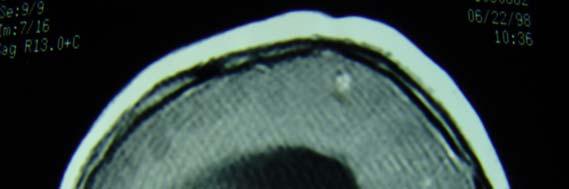
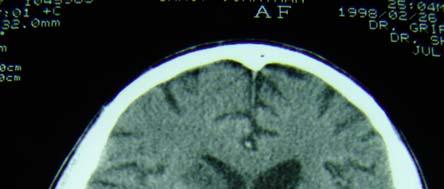
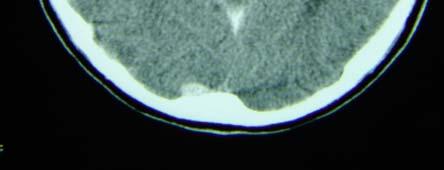
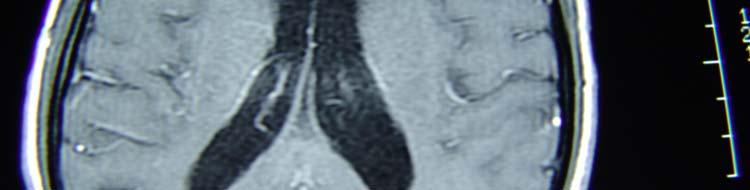
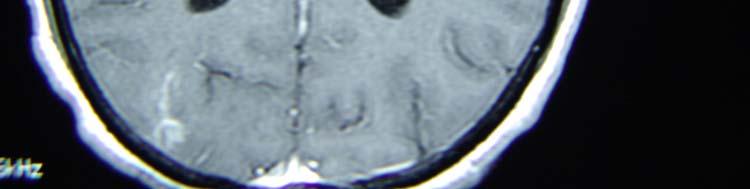
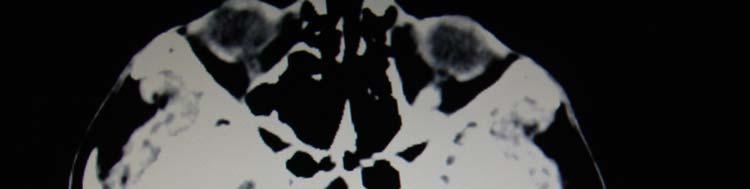
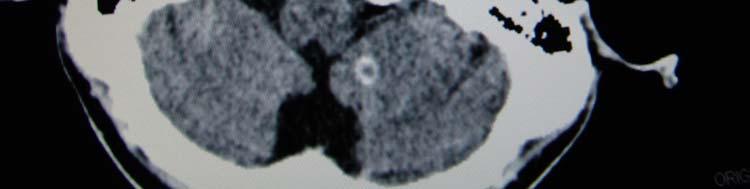
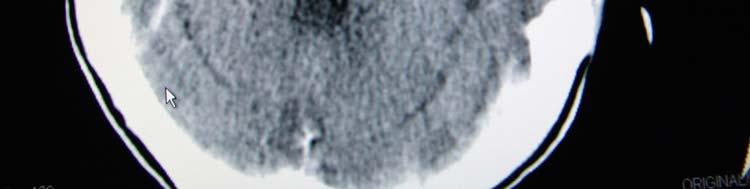
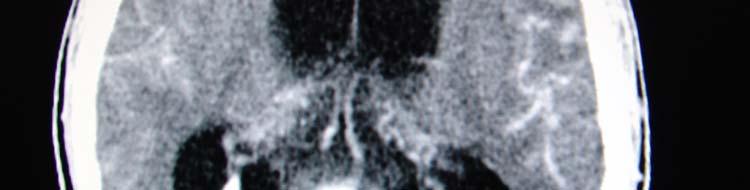
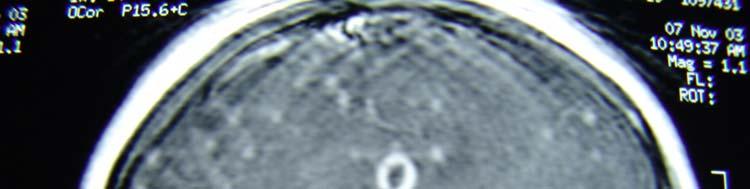
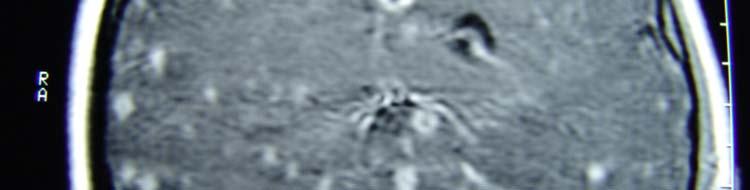
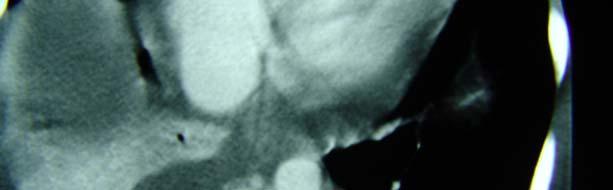
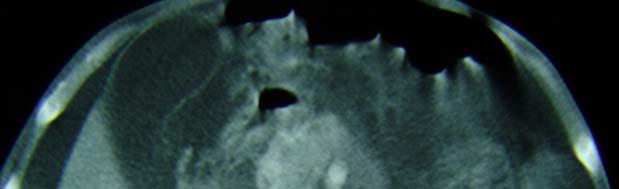
43 Hematogenous dissemination tuberculous meningitis thought to occur via rupture of a subependymal tubercle into the subarachroid space basal meninges most commonly involved Secondarily results in cortical and lacunar brain infarction, and spinal cord infarction 85 43
44 44
45 45


46 46


47 47

48 48
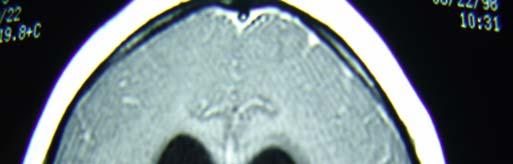
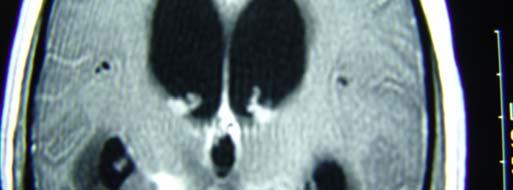
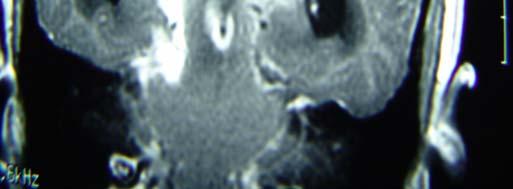
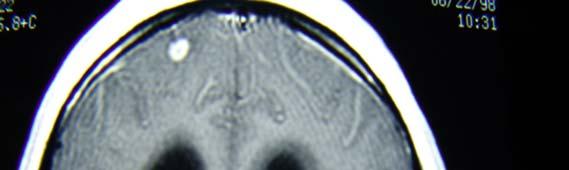

49 49



50 50






51 51


52 52


53 53



54 54



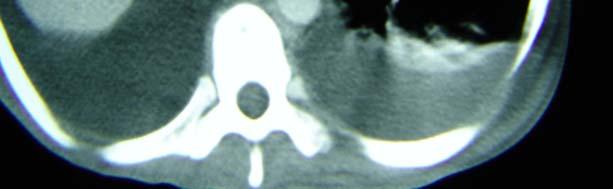
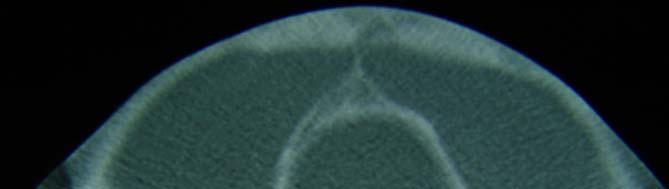
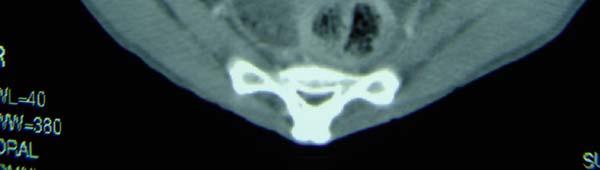
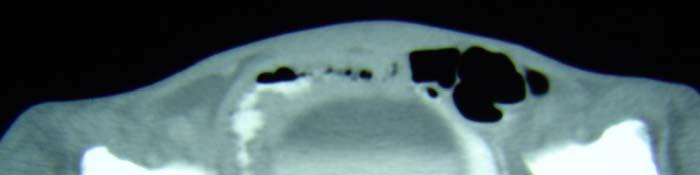
55 Bone involvement Potts disease Tuberculous spondylitis destructive lesions in spine primarily centered in vertebral discs, and secondarily involving vertebral end plates, resulting in kyphosis. May result in paravertebral abscess Cold abscess. Extends under anterior longitudinal ligament, involving multiple vertebra




56 56

57 Bone involvement also involves other joints hip, knee, tarsal joints cartilage destruction with articular defects
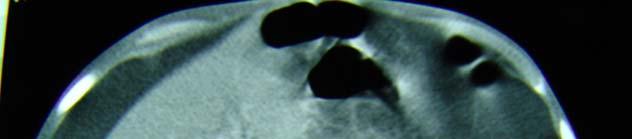
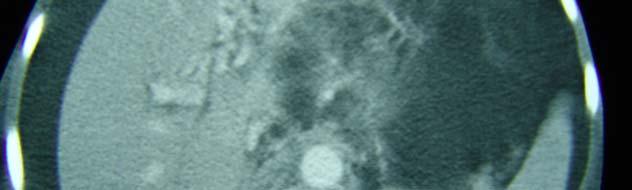
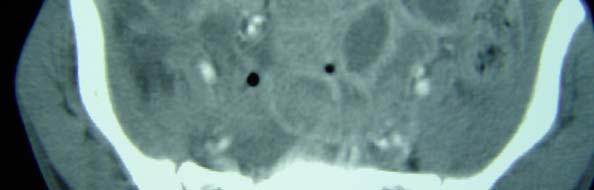
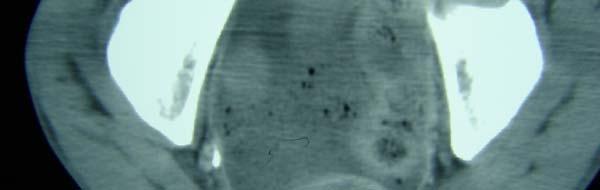
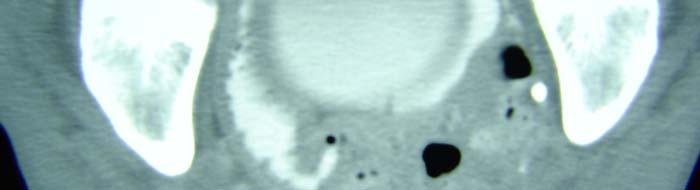
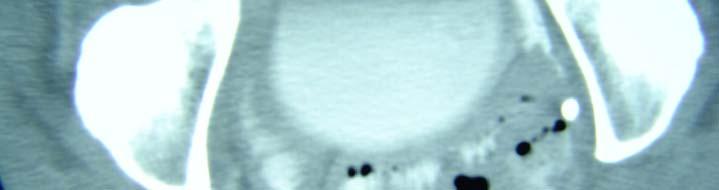
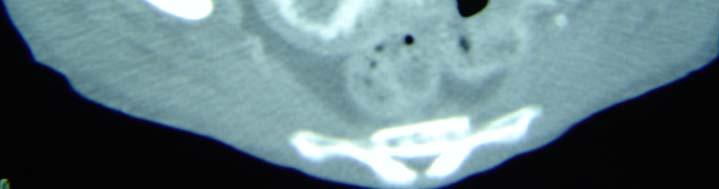
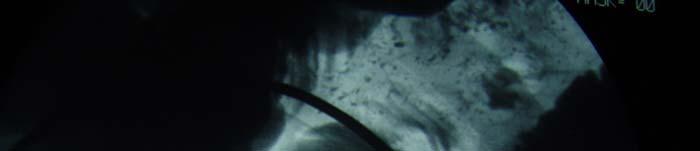
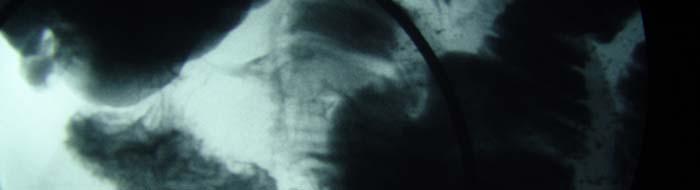
58 GI involvement increased incidence in AIDS ingestion of tuberculous sputum ileocecal area, ascending colon, most common sites 115 Tuberculous peritonitis complication of GI involvement ascites low density lymphadenopathy adhesions with bowel obstruction

59 59


60 60






61 61

62 62



63 63



64 64





65 65
66 66




67 67
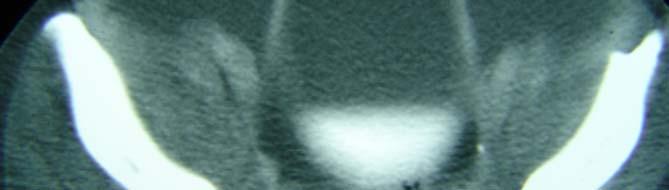
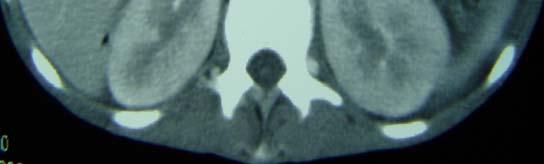
68 Urinary tract hematogenous spread to kidney hematuria, sterile pyuria 75% unilateral 135 Urinary tract tuberculomas form in renal parenchyma calcification Ureteral involvement develops from direct spread, resulting in stricture, and obstruction putty kidney tuberculous pyonephrosis autonephrectomy small, shrunken, calcified, scarred, and nonfunctional
69 Bladder involvement direct spread interstitial cystitis with thickened bladder wall ulceration also involves spinal opssicles and epididymus in males
David E. Griffith, MD has the following disclosures to make:
 Diagnosis of TB: Radiology David E. Griffith, MD March 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION David E. Griffith, MD has the following disclosures to make:
Diagnosis of TB: Radiology David E. Griffith, MD March 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION David E. Griffith, MD has the following disclosures to make:
TB Intensive Houston, Texas
 TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
PULMONARY TUBERCULOSIS RADIOLOGY
 PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
Tuberculosis: The Essentials
 Tuberculosis: The Essentials Kendra L. Fisher, MD, PhD THORACIC TUBERCULOSIS: THE BARE ESSENTIALS Kendra Fisher MD, FRCP (C) Department of Radiology Loma Linda University Medical Center TUBERCULOSIS ()
Tuberculosis: The Essentials Kendra L. Fisher, MD, PhD THORACIC TUBERCULOSIS: THE BARE ESSENTIALS Kendra Fisher MD, FRCP (C) Department of Radiology Loma Linda University Medical Center TUBERCULOSIS ()
Pediatric TB Intensive Houston, Texas October 14, 2013
 Pediatric TB Intensive Houston, Texas October 14, 2013 Radiologic Presentation of Childhood TB Susan D. John, MD, FACR October 14, 2013 Disclosures I have no disclosures or conflicts of interest to report
Pediatric TB Intensive Houston, Texas October 14, 2013 Radiologic Presentation of Childhood TB Susan D. John, MD, FACR October 14, 2013 Disclosures I have no disclosures or conflicts of interest to report
Pediatric TB Intensive Houston, Texas
 Pediatric TB Intensive Houston, Texas November 13, 2009 Radiographic Manifestations of Pediatric TB Susan D. John, MD, FACR November 13, 2009 Radiologic Presentation of Childhood TB Susan D. John, MD,
Pediatric TB Intensive Houston, Texas November 13, 2009 Radiographic Manifestations of Pediatric TB Susan D. John, MD, FACR November 13, 2009 Radiologic Presentation of Childhood TB Susan D. John, MD,
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
TB Radiology for Nurses Garold O. Minns, MD
 TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
Pathology of pulmonary tuberculosis. Dr: Salah Ahmed
 Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
How to Analyse Difficult Chest CT
 How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts
 Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
TB Intensive San Antonio, Texas November 29-December 2, 2011
 TB Intensive San Antonio, Texas November 29-December 2, 2011 Diagnosis of TB: Radiology Michael McCarthy, MD, FACR November 30, 2011 Michael McCarthy, MD, FACR has the following disclosures to make: No
TB Intensive San Antonio, Texas November 29-December 2, 2011 Diagnosis of TB: Radiology Michael McCarthy, MD, FACR November 30, 2011 Michael McCarthy, MD, FACR has the following disclosures to make: No
Tuberculosis - clinical forms. Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases
 Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
Chest Radiology Interpretation: Findings of Tuberculosis
 Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
TUBERCULOSIS. By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi
 TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
Original Article. Section: Radiology INTRODUCTION MATERIALS AND METHODS
 DOI: 10.21276/aimdr.2016.2.6.RD4 Original Article ISSN (O):2395-2822; ISSN (P):2395-2814 To Compare the Diagnostic Efficacy of HRCT Lung with Chest Radiographic Findings and Clinical Correlation with Microbiological
DOI: 10.21276/aimdr.2016.2.6.RD4 Original Article ISSN (O):2395-2822; ISSN (P):2395-2814 To Compare the Diagnostic Efficacy of HRCT Lung with Chest Radiographic Findings and Clinical Correlation with Microbiological
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS
 CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
Radiological Features of Mycobacterium tuberculosis TUBERCULE BACILLUS TUBERCULE BACILLUS DIAGNOSIS. Guy Richards. PATHOGENESIS of TUBERCULOSIS
 Radiological Features of Guy Richards Department of critical care Charlotte Maxeke Johannesburg Academic Hospital University of the Witwatersrand, Johannesburg, South Africa TUBERCULE BACILLUS Discovery
Radiological Features of Guy Richards Department of critical care Charlotte Maxeke Johannesburg Academic Hospital University of the Witwatersrand, Johannesburg, South Africa TUBERCULE BACILLUS Discovery
Tanya Van, M.D. has the following disclosures to make:
 Imaging of Pulmonary Mycobacterial TB Infection Tanya Van, M.D. April6, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Tanya Van, M.D. has the following disclosures to
Imaging of Pulmonary Mycobacterial TB Infection Tanya Van, M.D. April6, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Tanya Van, M.D. has the following disclosures to
Tuberculosis. By: Shefaa Q aqa
 Tuberculosis By: Shefaa Q aqa Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the
Tuberculosis By: Shefaa Q aqa Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the
An Image Repository for Chest CT
 An Image Repository for Chest CT Francesco Frajoli for the Chest CT in Antibody Deficiency Group An Image Repository for Chest CT he Chest CT in Antibody Deficiency Group is an international and interdisciplinary
An Image Repository for Chest CT Francesco Frajoli for the Chest CT in Antibody Deficiency Group An Image Repository for Chest CT he Chest CT in Antibody Deficiency Group is an international and interdisciplinary
Extraordinary Patterns of Tuberculosis
 Extraordinary Patterns of Tuberculosis E. Kadakovska Infectology Center of Latvia, Clinic of Tuberculosis and Lung Diseases, Diagnostics and Radiology Department 1 Target Importance of recognizing of tuberculosis
Extraordinary Patterns of Tuberculosis E. Kadakovska Infectology Center of Latvia, Clinic of Tuberculosis and Lung Diseases, Diagnostics and Radiology Department 1 Target Importance of recognizing of tuberculosis
Thoracic Sarcoidosis Imaging Updated: Jul 19, 2013
 Thoracic Sarcoidosis Imaging Updated: Jul 19, 2013 Overview Radiography Computed Tomography Magnetic Resonance Imaging Nuclear Imaging Show All Multimedia Library References Overview For patients with
Thoracic Sarcoidosis Imaging Updated: Jul 19, 2013 Overview Radiography Computed Tomography Magnetic Resonance Imaging Nuclear Imaging Show All Multimedia Library References Overview For patients with
Case 1 : Question. 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random
 Interesting case Case 1 Case 1 : Question 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random Case 1: Answer 1.1 What is the intralobular distribution? 1. Centrilobular
Interesting case Case 1 Case 1 : Question 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random Case 1: Answer 1.1 What is the intralobular distribution? 1. Centrilobular
Interpretation of Chest Radiographs Paul Christensen, MD 10/21/09. Diagnostic Evaluation. Medical Evaluation & CXR Interpretation.
 Diagnostic Evaluation Medical Evaluation & CXR Interpretation University of Michigan TB Consultant Washtenaw County Medical history Physical examination Testing for TB exposure (previously covered) Radiologic
Diagnostic Evaluation Medical Evaluation & CXR Interpretation University of Michigan TB Consultant Washtenaw County Medical history Physical examination Testing for TB exposure (previously covered) Radiologic
Acute and Chronic Lung Disease
 KATHOLIEKE UNIVERSITEIT LEUVEN Faculty of Medicine Acute and Chronic Lung Disease W De Wever, JA Verschakelen Department of Radiology, University Hospitals Leuven, Belgium Clinical utility of HRCT To detect
KATHOLIEKE UNIVERSITEIT LEUVEN Faculty of Medicine Acute and Chronic Lung Disease W De Wever, JA Verschakelen Department of Radiology, University Hospitals Leuven, Belgium Clinical utility of HRCT To detect
Lecture 3. Inflammatory Processes
 Lecture 3 Inflammatory Processes Process: Increased vascular permeability Water and cellular infiltrations Results: Abscess, ulceration, cavitation Penetration, perforation and fistula formation Scarring,
Lecture 3 Inflammatory Processes Process: Increased vascular permeability Water and cellular infiltrations Results: Abscess, ulceration, cavitation Penetration, perforation and fistula formation Scarring,
Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D.
 Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D. Department of Radiology, Korea University Guro Hospital, College of Medicine, Korea
Eun-Young Kang, M.D., Jae Wook Lee, M.D., Ji Yung Choo, M.D., Hwan Seok Yong, M.D., Ki Yeol Lee, M.D., Yu-Whan Oh, M.D. Department of Radiology, Korea University Guro Hospital, College of Medicine, Korea
Web Chapter 3. Image Gallery: Lesion detection on low dose chest CT
 Web Chapter 3 Image Gallery: Lesion detection on low dose chest CT Sarabjeet Singh, MD Mannudeep K. Kalra, MD *Eugene J. Mark, MD *James Stone, MD James H. Thrall, MD Department of Radiology and *Department
Web Chapter 3 Image Gallery: Lesion detection on low dose chest CT Sarabjeet Singh, MD Mannudeep K. Kalra, MD *Eugene J. Mark, MD *James Stone, MD James H. Thrall, MD Department of Radiology and *Department
The Imaging Analysis of Pulmonary Sarcodiosis
 www.cancercellresearch.org ISSN: 2161-2609 Article The Imaging Analysis of Pulmonary Sarcodiosis Xin He, Chuanyu Zhang* Department of Radiology, Affiliated Hospital of Qingdao University, Qingdao, China
www.cancercellresearch.org ISSN: 2161-2609 Article The Imaging Analysis of Pulmonary Sarcodiosis Xin He, Chuanyu Zhang* Department of Radiology, Affiliated Hospital of Qingdao University, Qingdao, China
Typical and atypical findings of pulmonary sarcoidosis at high resolution CT
 Typical and atypical findings of pulmonary sarcoidosis at high resolution CT Poster No.: C-0169 Congress: ECR 2013 Type: Educational Exhibit Authors: L. Raposo Rodríguez, C. Mejía, B. Escobar Mallada,
Typical and atypical findings of pulmonary sarcoidosis at high resolution CT Poster No.: C-0169 Congress: ECR 2013 Type: Educational Exhibit Authors: L. Raposo Rodríguez, C. Mejía, B. Escobar Mallada,
Tuberculosis of the chest
 European Journal of Radiology 55 (2005) 158 172 Tuberculosis of the chest Luís Curvo-Semedo,Luísa Teixeira, Filipe Caseiro-Alves Department of Radiology, Hospitais da Universidade de Coimbra, Praceta Mota
European Journal of Radiology 55 (2005) 158 172 Tuberculosis of the chest Luís Curvo-Semedo,Luísa Teixeira, Filipe Caseiro-Alves Department of Radiology, Hospitais da Universidade de Coimbra, Praceta Mota
Pulmonary TB: HRCT findings
 Pulmonary TB: HRCT findings Tuberculosis: History BC 5000: Evidence of TB in neolithic man Jung-Gi Im, MD Department of Radiology Seoul National University Hospital BC 2900: Pyramid builders BC 1000 :
Pulmonary TB: HRCT findings Tuberculosis: History BC 5000: Evidence of TB in neolithic man Jung-Gi Im, MD Department of Radiology Seoul National University Hospital BC 2900: Pyramid builders BC 1000 :
Role of imaging (images) in my practice. Dr P Senthur Nambi Consultant Infectious Diseases
 in my practice. Dr P Senthur Nambi Consultant Infectious Diseases") Role of imaging (images) in my practice Dr P Senthur Nambi Consultant Infectious Diseases Medical images: My thoughts Images are just images Subject to the intellect of the interpreter View it in conjuction
Role of imaging (images) in my practice Dr P Senthur Nambi Consultant Infectious Diseases Medical images: My thoughts Images are just images Subject to the intellect of the interpreter View it in conjuction
Thoracic sarcoidosis: Pictoral review of typical and atypical findings
 Thoracic sarcoidosis: Pictoral review of typical and atypical findings Poster No.: C-0804 Congress: ECR 2010 Type: Educational Exhibit Topic: Chest Authors: A. Ferreira, J. Calha; Lisbon/PT Keywords: Sarcoidosis,
Thoracic sarcoidosis: Pictoral review of typical and atypical findings Poster No.: C-0804 Congress: ECR 2010 Type: Educational Exhibit Topic: Chest Authors: A. Ferreira, J. Calha; Lisbon/PT Keywords: Sarcoidosis,
Primary tuberculosis in a malnourished adolescent
 Primary tuberculosis in a malnourished adolescent Mazen Zawaideh 1*, Cherng Chao 2, Patricia Poole 2, John Naheedy 3 1. School of Medicine, University of California, San Diego, La Jolla, USA 2. Radiology
Primary tuberculosis in a malnourished adolescent Mazen Zawaideh 1*, Cherng Chao 2, Patricia Poole 2, John Naheedy 3 1. School of Medicine, University of California, San Diego, La Jolla, USA 2. Radiology
HRCT in Diffuse Interstitial Lung Disease Steps in High Resolution CT Diagnosis. Where are the lymphatics? Anatomic distribution
 Steps in High Resolution CT Diagnosis Pattern of abnormality Distribution of disease Associated findings Clinical history Tomás Franquet MD What is the diagnosis? Hospital de Sant Pau. Barcelona Secondary
Steps in High Resolution CT Diagnosis Pattern of abnormality Distribution of disease Associated findings Clinical history Tomás Franquet MD What is the diagnosis? Hospital de Sant Pau. Barcelona Secondary
Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations
 Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations TECHNICAL EVALUATION 1. Projection: AP/PA view To differentiate between AP & PA films,
Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations TECHNICAL EVALUATION 1. Projection: AP/PA view To differentiate between AP & PA films,
In Canada, there was a 25% reduction in incidence of genitourinary TB in the period compared with An interesting speculation
 Renal T B EPIDEMIOLOGY Young to middle age usually affected, rare in children Male : female ratio = 2:1 True prevalence and incidence not known as patients are usually asymptomatic With HIV pandemic, there
Renal T B EPIDEMIOLOGY Young to middle age usually affected, rare in children Male : female ratio = 2:1 True prevalence and incidence not known as patients are usually asymptomatic With HIV pandemic, there
Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations
: Pleuropulmonary Manifestations") 08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
Atypical radiologic appearances of pulmonary tuberculosis in non-hiv adult patients
 Atypical radiologic appearances of pulmonary tuberculosis in non-hiv adult patients Poster No.: R-0200 Congress: RANZCR-AOCR 2012 Type: Educational Exhibit Authors: K. N. Jeon, K. Bae, M. J. Park Keywords:
Atypical radiologic appearances of pulmonary tuberculosis in non-hiv adult patients Poster No.: R-0200 Congress: RANZCR-AOCR 2012 Type: Educational Exhibit Authors: K. N. Jeon, K. Bae, M. J. Park Keywords:
Long Case Set 02. Dr Raviraj Uppoor. Dr Sameer Shamshuddin. Consultant Radiologist Cumberland Infirmary, Carlisle, UK
 Long Case Set 02 www.frcrtutorials.com Dr Raviraj Uppoor MBBS, DMRD, DNB, FRCR Consultant Radiologist Cumberland Infirmary, Carlisle, UK Dr Sameer Shamshuddin MBBS, DMRD, FRCR Consultant Radiologist Royal
Long Case Set 02 www.frcrtutorials.com Dr Raviraj Uppoor MBBS, DMRD, DNB, FRCR Consultant Radiologist Cumberland Infirmary, Carlisle, UK Dr Sameer Shamshuddin MBBS, DMRD, FRCR Consultant Radiologist Royal
Tuberculosis Pathogenesis
 Tuberculosis Pathogenesis Renuka Khurana, MD, MPH May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Renuka Khurana, MD, MPH has the following disclosures
Tuberculosis Pathogenesis Renuka Khurana, MD, MPH May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Renuka Khurana, MD, MPH has the following disclosures
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
Case 1: Question. 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule
 HRCT WORK SHOP Case 1 Case 1: Question 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule Case 1: Question 1.2 What is the diagnosis? 1. Hypersensitivity
HRCT WORK SHOP Case 1 Case 1: Question 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule Case 1: Question 1.2 What is the diagnosis? 1. Hypersensitivity
Learning Radiology: Recognizing the Basics. Text with Student Consult Online Access Code
 Learning Radiology: Recognizing the Basics. Text with Student Consult Online Access Code Herring, W ISBN-13: 9780323074445 Table of Contents 1. Recognizing Anything The "colorful" world of radiology A
Learning Radiology: Recognizing the Basics. Text with Student Consult Online Access Code Herring, W ISBN-13: 9780323074445 Table of Contents 1. Recognizing Anything The "colorful" world of radiology A
Tuberculosis in Patients with End-Stage Renal Disease 1
 Tuberculosis in Patients with End-Stage Renal Disease 1 Hyo-Cheol Kim, M.D., Jin Mo Goo, M.D., Myung Jin Chung, M.D., Min Hoan Moon, M.D., Young Hwan Koh, M.D., and Jung-Gi Im, M.D. Purpose: The purpose
Tuberculosis in Patients with End-Stage Renal Disease 1 Hyo-Cheol Kim, M.D., Jin Mo Goo, M.D., Myung Jin Chung, M.D., Min Hoan Moon, M.D., Young Hwan Koh, M.D., and Jung-Gi Im, M.D. Purpose: The purpose
Chief Complain. For chemotherapy
 Chief Complain For chemotherapy Present Illness 93.12 Progressive weakness of R t arm for 1 year X-ray: peneative lesion over right proximal humorous Bone scan: multiple increased intake Biopsy of distal
Chief Complain For chemotherapy Present Illness 93.12 Progressive weakness of R t arm for 1 year X-ray: peneative lesion over right proximal humorous Bone scan: multiple increased intake Biopsy of distal
4/16/2017. Learning Objectives. Interpretation of the Chest Radiograph. Components. Production of the Radiograph. Density & Appearance
 Interpretation of the Arthur Jones, EdD, RRT Learning Objectives Identify technical defects in chest radiographs Identify common radiographic abnormalities This Presentation is Approved for 1 CRCE Credit
Interpretation of the Arthur Jones, EdD, RRT Learning Objectives Identify technical defects in chest radiographs Identify common radiographic abnormalities This Presentation is Approved for 1 CRCE Credit
Extrapulmonary Manifestations of Tuberculosis: A Radiologic Review
 Extrapulmonary Manifestations of Tuberculosis: A Radiologic Review Poster No.: C-1958 Congress: ECR 2014 Type: Authors: Educational Exhibit J. Isern 1, S. Llaverias Borrell 1, A. Olarte 1, E. Grive 1,
Extrapulmonary Manifestations of Tuberculosis: A Radiologic Review Poster No.: C-1958 Congress: ECR 2014 Type: Authors: Educational Exhibit J. Isern 1, S. Llaverias Borrell 1, A. Olarte 1, E. Grive 1,
10/17/2016. Nuts and Bolts of Thoracic Radiology. Objectives. Techniques
 Nuts and Bolts of Thoracic Radiology October 20, 2016 Carleen Risaliti Objectives Understand the basics of chest radiograph Develop a system for interpreting chest radiographs Correctly identify thoracic
Nuts and Bolts of Thoracic Radiology October 20, 2016 Carleen Risaliti Objectives Understand the basics of chest radiograph Develop a system for interpreting chest radiographs Correctly identify thoracic
Computed Tomography (CT) Scan Features of Pulmonary Drug-Resistant Tuberculosis in Non-HIV-Infected Patients
 Scan Features of Pulmonary Drug-Resistant Tuberculosis in Non-HIV-Infected Patients") Cronicon OPEN ACCESS EC BACTERIOLOGY AND VIROLOGY Research Article Computed Tomography (CT) Scan Features of Pulmonary Drug-Resistant Tuberculosis in Non-HIV-Infected Patients Ehsan Shahverdi 1 *, Ashkan
Cronicon OPEN ACCESS EC BACTERIOLOGY AND VIROLOGY Research Article Computed Tomography (CT) Scan Features of Pulmonary Drug-Resistant Tuberculosis in Non-HIV-Infected Patients Ehsan Shahverdi 1 *, Ashkan
Thoracic lung involvement in rheumatoid arthritis: Findings on HRCT
 Thoracic lung involvement in rheumatoid arthritis: Findings on HRCT Poster No.: C-2488 Congress: ECR 2015 Type: Educational Exhibit Authors: R. E. Correa Soto, M. J. Martín Sánchez, J. M. Fernandez 1 1
Thoracic lung involvement in rheumatoid arthritis: Findings on HRCT Poster No.: C-2488 Congress: ECR 2015 Type: Educational Exhibit Authors: R. E. Correa Soto, M. J. Martín Sánchez, J. M. Fernandez 1 1
Financial disclosure COMMON DIAGNOSES IN HRCT. High Res Chest HRCT. HRCT Pre test. I have no financial relationships to disclose. Anatomy Nomenclature
 Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
Currently, there are about 15 million TB patients including 11 million of working age.
 Currently, there are about 15 million TB patients including 11 million of working age. The vast majority of infected people (90%) the disease does not progress. Predicted by WHO in the next twenty years
Currently, there are about 15 million TB patients including 11 million of working age. The vast majority of infected people (90%) the disease does not progress. Predicted by WHO in the next twenty years
Exam 2 Respiratory Disorders
 Exam 2 Respiratory Disorders Common Cold Common Cold Pathology Common Cold Consequences Rhinosinusitis Rhinosinusitis Pathology Rhinosinusitis ostia can close due to Influenza (Flu) Influenza Pathology
Exam 2 Respiratory Disorders Common Cold Common Cold Pathology Common Cold Consequences Rhinosinusitis Rhinosinusitis Pathology Rhinosinusitis ostia can close due to Influenza (Flu) Influenza Pathology
Imaging Small Airways Diseases: Not Just Air trapping. Eric J. Stern MD University of Washington
 Imaging Small Airways Diseases: Not Just Air trapping Eric J. Stern MD University of Washington What we are discussing SAD classification SAD imaging with MDCT emphasis What is a small airway? Airway with
Imaging Small Airways Diseases: Not Just Air trapping Eric J. Stern MD University of Washington What we are discussing SAD classification SAD imaging with MDCT emphasis What is a small airway? Airway with
Pulmonary Aspergillosis
 May 2005 Pulmonary Aspergillosis Nancy Wei, Harvard Medical School, Year III Overview Pulmonary aspergillosis background information Patient presentations Common radiographic findings for each type of
May 2005 Pulmonary Aspergillosis Nancy Wei, Harvard Medical School, Year III Overview Pulmonary aspergillosis background information Patient presentations Common radiographic findings for each type of
Pneumocystis jirovecci pneumonia: from mild disease to a real disaster. A pictorial review of the different radiologic patterns in acute settings
 Pneumocystis jirovecci pneumonia: from mild disease to a real disaster. A pictorial review of the different radiologic patterns in acute settings Poster No.: C-1425 Congress: ECR 2017 Type: Educational
Pneumocystis jirovecci pneumonia: from mild disease to a real disaster. A pictorial review of the different radiologic patterns in acute settings Poster No.: C-1425 Congress: ECR 2017 Type: Educational
Surgical indications: Non-malignant pulmonary diseases. Punnarerk Thongcharoen
 Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
Pulmonary Sarcoidosis - Radiological Evaluation
 Original Research Article Pulmonary Sarcoidosis - Radiological Evaluation Jayesh Shah 1, Darshan Shah 2*, C. Raychaudhuri 3 1 Associate Professor, 2 1 st Year Resident, 3 Professor and HOD Radiology Department,
Original Research Article Pulmonary Sarcoidosis - Radiological Evaluation Jayesh Shah 1, Darshan Shah 2*, C. Raychaudhuri 3 1 Associate Professor, 2 1 st Year Resident, 3 Professor and HOD Radiology Department,
Dilemma of Thoracic Tuberculosis Vs. Sarcoidosis in TB Endemic Areas: An Imaging Approach
 Dilemma of Thoracic Tuberculosis Vs. Sarcoidosis in TB Endemic Areas: An Imaging Approach A. S. Bhalla, A. Das, A. GOYAL, P. NARANJE, R. GULERIA, G. C. KHILNANI ALL INDIA INSTITUTE OF MEDICAL SCIENCES
Dilemma of Thoracic Tuberculosis Vs. Sarcoidosis in TB Endemic Areas: An Imaging Approach A. S. Bhalla, A. Das, A. GOYAL, P. NARANJE, R. GULERIA, G. C. KHILNANI ALL INDIA INSTITUTE OF MEDICAL SCIENCES
Respiratory System الفريق الطبي االكاديمي
 Respiratory System الفريق الطبي االكاديمي Pathology sheet 5 Tuberculosis Done by: Ahmad Al-Sahele Introduction: as we know TB is caused by mycobacterium tubercolosis; now keep in your mind another microorganism
Respiratory System الفريق الطبي االكاديمي Pathology sheet 5 Tuberculosis Done by: Ahmad Al-Sahele Introduction: as we know TB is caused by mycobacterium tubercolosis; now keep in your mind another microorganism
Pictorial essay of unusual radiologic manifestations of pulmonary and airway metastasis at initial presentation of lung cancer
 Pictorial essay of unusual radiologic manifestations of pulmonary and airway metastasis at initial presentation of lung cancer Poster No.: C-2297 Congress: ECR 2012 Type: Educational Exhibit Authors: Y.
Pictorial essay of unusual radiologic manifestations of pulmonary and airway metastasis at initial presentation of lung cancer Poster No.: C-2297 Congress: ECR 2012 Type: Educational Exhibit Authors: Y.
Index. B Biological factors, 2 Brain stem encephalitis, Burkitt s lymphoma, 83, 105
 Index A Acquired immunodeficiency syndrome (AIDS) abdomen gallbladder complications, 97, 107 109 gastrointestinal complications, 96, 105 106 liver complications, 97, 107 109 neoplasm, 99, 110 111 pancreas
Index A Acquired immunodeficiency syndrome (AIDS) abdomen gallbladder complications, 97, 107 109 gastrointestinal complications, 96, 105 106 liver complications, 97, 107 109 neoplasm, 99, 110 111 pancreas
Pulmonary Pathology II. William Bligh-Glover M.D. Department of Anatomy, CWRU
 Pulmonary Pathology II William Bligh-Glover M.D. Department of Anatomy, CWRU Goals and Objectives Comprehend the etiology, pathogenesis/pathopysiology and consequences of pulmonary hypertension Distinguish
Pulmonary Pathology II William Bligh-Glover M.D. Department of Anatomy, CWRU Goals and Objectives Comprehend the etiology, pathogenesis/pathopysiology and consequences of pulmonary hypertension Distinguish
HIV related pulmonary infections. A radiologic pictorial review.
 HIV related pulmonary infections. A radiologic pictorial review. Poster No.: C-0836 Congress: ECR 2013 Type: Educational Exhibit Authors: N. Arcalis, P. Trallero, L. Berrocal Morales, S. Medrano, S. 1
HIV related pulmonary infections. A radiologic pictorial review. Poster No.: C-0836 Congress: ECR 2013 Type: Educational Exhibit Authors: N. Arcalis, P. Trallero, L. Berrocal Morales, S. Medrano, S. 1
X-Rays. Prepared by Prof.Dr. Magda Hassab Allah Assist.lecturer Marwa Al Hady
 X-Rays Prepared by Prof.Dr. Magda Hassab Allah Assist.lecturer Marwa Al Hady CHEST X-RAYS Normal Chest X-ray Comments on chest X ray includes examination of 1- Bony cage (ribs,clavicles &vertebral column
X-Rays Prepared by Prof.Dr. Magda Hassab Allah Assist.lecturer Marwa Al Hady CHEST X-RAYS Normal Chest X-ray Comments on chest X ray includes examination of 1- Bony cage (ribs,clavicles &vertebral column
Radiological spectrum of Thoracic Sequelae and Complications of Tuberculosis
 Radiological spectrum of Thoracic Sequelae and Complications of Tuberculosis Poster No.: P-0013 Congress: ESTI 2014 Type: Educational Poster Authors: B. Alami, O. Addou, M. Jaffal, M. Y. Alaoui Lamrani,
Radiological spectrum of Thoracic Sequelae and Complications of Tuberculosis Poster No.: P-0013 Congress: ESTI 2014 Type: Educational Poster Authors: B. Alami, O. Addou, M. Jaffal, M. Y. Alaoui Lamrani,
Interesting Cases. Pulmonary
 Interesting Cases Pulmonary 54M with prior history of COPD, hep B/C, and possible history of TB presented with acute on chronic dyspnea, and productive cough Hazy opacity overlying the left hemithorax
Interesting Cases Pulmonary 54M with prior history of COPD, hep B/C, and possible history of TB presented with acute on chronic dyspnea, and productive cough Hazy opacity overlying the left hemithorax
Spectrum of Cystic Lung Disease and its Mimics. Kathleen Jacobs MD and Elizabeth Weihe MD UC San Diego Medical Center, Department of Radiology
 Spectrum of Cystic Lung Disease and its Mimics Kathleen Jacobs MD and Elizabeth Weihe MD UC San Diego Medical Center, Department of Radiology No Financial Disclosures Learning Objectives 1. Review the
Spectrum of Cystic Lung Disease and its Mimics Kathleen Jacobs MD and Elizabeth Weihe MD UC San Diego Medical Center, Department of Radiology No Financial Disclosures Learning Objectives 1. Review the
Lung Cancer - Suspected
 Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Lung. 10/24/13 Chest X-ray: 2.9 cm mass like density in the inferior lingular segment worrisome for neoplasm. Malignancy cannot be excluded.
 Lung Case Scenario 1 A 54 year white male presents with a recent abnormal CT of the chest. The patient has a history of melanoma, kidney, and prostate cancers. 10/24/13 Chest X-ray: 2.9 cm mass like density
Lung Case Scenario 1 A 54 year white male presents with a recent abnormal CT of the chest. The patient has a history of melanoma, kidney, and prostate cancers. 10/24/13 Chest X-ray: 2.9 cm mass like density
56% of these were in south east Asia and west pacific region.
 Tuberc ulosis Dr. ASAAD FARHAN ASSIST. PROF.PEDS. Learning objectives epidemiology Tuberculosis remains worlds deadliest communicable disease. TB is present in all regions of the world. WHO estimates that
Tuberc ulosis Dr. ASAAD FARHAN ASSIST. PROF.PEDS. Learning objectives epidemiology Tuberculosis remains worlds deadliest communicable disease. TB is present in all regions of the world. WHO estimates that
Pathology of Pneumonia
 Pathology of Pneumonia Dr. Atif Ali Bashir Assistant Professor of Pathology College of Medicine Majma ah University Introduction: 5000 sq meters of area.! (olympic track) Filters >10,000 L of air / day!
Pathology of Pneumonia Dr. Atif Ali Bashir Assistant Professor of Pathology College of Medicine Majma ah University Introduction: 5000 sq meters of area.! (olympic track) Filters >10,000 L of air / day!
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
August 2018 Imaging Case of the Month: Dyspnea in a 55-Year-Old Smoker. Michael B. Gotway, MD
 August 2018 Imaging Case of the Month: Dyspnea in a 55-Year-Old Smoker Michael B. Gotway, MD Department of Radiology Mayo Clinic Arizona Scottsdale, AZ USA Clinical History: A 55 year old woman presented
August 2018 Imaging Case of the Month: Dyspnea in a 55-Year-Old Smoker Michael B. Gotway, MD Department of Radiology Mayo Clinic Arizona Scottsdale, AZ USA Clinical History: A 55 year old woman presented
UERMMMC Department of Radiology. Basic Chest Radiology
 UERMMMC Department of Radiology Basic Chest Radiology PHYSICS DENSITIES BONE SOFT TISSUES WATER FAT AIR TELEROENTGENOGRAM Criteria for an Ideal Chest Radiograph 1. Upright 2. Posteroanterior View 3. Full
UERMMMC Department of Radiology Basic Chest Radiology PHYSICS DENSITIES BONE SOFT TISSUES WATER FAT AIR TELEROENTGENOGRAM Criteria for an Ideal Chest Radiograph 1. Upright 2. Posteroanterior View 3. Full
Bronchial syndrome. Atelectasis Draining bronchus Bronchiectasis
 Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
INTRATHORACIC TUBERCULOSIS IN CHILDREN
 DIAGNOSTIC ATLAS OF INTRATHORACIC TUBERCULOSIS IN CHILDREN A Guide For Low Income Countries 2003 International Union Against Tuberculosis and Lung Disease DIAGNOSTIC ATLAS OF INTRATHORACIC TUBERCULOSIS
DIAGNOSTIC ATLAS OF INTRATHORACIC TUBERCULOSIS IN CHILDREN A Guide For Low Income Countries 2003 International Union Against Tuberculosis and Lung Disease DIAGNOSTIC ATLAS OF INTRATHORACIC TUBERCULOSIS
ARDS - a must know. Page 1 of 14
 ARDS - a must know Poster No.: C-1683 Congress: ECR 2016 Type: Authors: Keywords: DOI: Educational Exhibit M. Cristian; Turda/RO Education and training, Edema, Acute, Localisation, Education, Digital radiography,
ARDS - a must know Poster No.: C-1683 Congress: ECR 2016 Type: Authors: Keywords: DOI: Educational Exhibit M. Cristian; Turda/RO Education and training, Edema, Acute, Localisation, Education, Digital radiography,
CHRONIC INFLAMMATION
 CHRONIC INFLAMMATION Chronic inflammation is an inflammatory response of prolonged duration often for months, years or even indefinitely. Its prolonged course is proved by persistence of the causative
CHRONIC INFLAMMATION Chronic inflammation is an inflammatory response of prolonged duration often for months, years or even indefinitely. Its prolonged course is proved by persistence of the causative
WANTED Manuscript supporting the prevailing paradigm of tuberculosis by any author DEAD or ALIVE $1,000 REWARD. 3 TB India HSCP
 A New Paradigm for the Pathogenesis of Pulmonary Tuberculosis Bronchogenic tuberculosis The missing link between primary and post-primary disease Robert Hunter MD, PhD Dept. of Pathology and Laboratory
A New Paradigm for the Pathogenesis of Pulmonary Tuberculosis Bronchogenic tuberculosis The missing link between primary and post-primary disease Robert Hunter MD, PhD Dept. of Pathology and Laboratory
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Barry Rabinovitch, MD, FRCP(C) Author Madhukar Pai, MD, PhD co-author and Series Editor Barry Rabinovitch is an assistant
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Barry Rabinovitch, MD, FRCP(C) Author Madhukar Pai, MD, PhD co-author and Series Editor Barry Rabinovitch is an assistant
Workshop Cyst & Lucency. How to Approach
 Workshop Cyst & Lucency How to Approach To Approach Cystic Lung Disease True cysts? Cavitary disease Cystic bronchiectasis Mosaic attenuation Subpleural cysts Bullae Paraseptal emphysema Honeycombing Birt
Workshop Cyst & Lucency How to Approach To Approach Cystic Lung Disease True cysts? Cavitary disease Cystic bronchiectasis Mosaic attenuation Subpleural cysts Bullae Paraseptal emphysema Honeycombing Birt
Immunocompromised patients. Immunocompromised patients. Immunocompromised patients
 Value of CT in Early Pneumonia in Immunocompromised Patients Nantaka Kiranantawat, PSU Preventative Factors Phagocyts Cellular immunity Humoral immunity Predisposing Factors Infection, Stress, Poor nutrition,
Value of CT in Early Pneumonia in Immunocompromised Patients Nantaka Kiranantawat, PSU Preventative Factors Phagocyts Cellular immunity Humoral immunity Predisposing Factors Infection, Stress, Poor nutrition,
September 2014 Imaging Case of the Month. Michael B. Gotway, MD. Department of Radiology Mayo Clinic Arizona Scottsdale, AZ
 September 2014 Imaging Case of the Month Michael B. Gotway, MD Department of Radiology Mayo Clinic Arizona Scottsdale, AZ Clinical History: A 57-year-old non-smoking woman presented to her physician as
September 2014 Imaging Case of the Month Michael B. Gotway, MD Department of Radiology Mayo Clinic Arizona Scottsdale, AZ Clinical History: A 57-year-old non-smoking woman presented to her physician as
CT Diagnosis of Pulmonary Wegener s Granulomatosis: A Case Report and Review of Literature
 CASE REPORT JIACM 2008; 9(4): 321-5 CT Diagnosis of Pulmonary Wegener s Granulomatosis: A Case Report and Review of Literature Shibani Mehra*, Shailendra Aggarwal Abstract The diagnosis of Wegener s granulomatosis
CASE REPORT JIACM 2008; 9(4): 321-5 CT Diagnosis of Pulmonary Wegener s Granulomatosis: A Case Report and Review of Literature Shibani Mehra*, Shailendra Aggarwal Abstract The diagnosis of Wegener s granulomatosis
Bronchogenic Carcinoma
 A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
Pediatric TB Radiology: It s Not Black and White Part 2
 Experiencing technical difficulties? Please call Adobe Connect for technical assistance at 1-800-422-3623 Pediatric TB Radiology: It s Not Black and White Part 2 June 18, 2018 A National Webinar June 18,
Experiencing technical difficulties? Please call Adobe Connect for technical assistance at 1-800-422-3623 Pediatric TB Radiology: It s Not Black and White Part 2 June 18, 2018 A National Webinar June 18,
Pulmonary TB Clinical Diagnosis
 Pulmonary TB Clinical Diagnosis Dr Onn Min Kon TB Clinics St Mary s Hospital + Hammersmith Hospital History back to basics Symptoms Ethnicity/ age Recent arrival/ travel history Contact history BCG history
Pulmonary TB Clinical Diagnosis Dr Onn Min Kon TB Clinics St Mary s Hospital + Hammersmith Hospital History back to basics Symptoms Ethnicity/ age Recent arrival/ travel history Contact history BCG history
Spinal infection. Outline ANATOMY 6/2/2017. Anatomy Pathogen
 Outline Spinal infection Pramot Tanutit, M.D. Department of Radiology, Songklanagarind Hospital Faculty of Medicine, Prince of Songkla University Anatomy Pathogen Pyogenic spondylodiscitis Tuberculous
Outline Spinal infection Pramot Tanutit, M.D. Department of Radiology, Songklanagarind Hospital Faculty of Medicine, Prince of Songkla University Anatomy Pathogen Pyogenic spondylodiscitis Tuberculous
General History. 林陳 珠 Female 69 years old 住院期間 : ~ Chief Complaint : sudden loss of conscious 5 minutes in the morning.
 General History 林陳 珠 Female 69 years old 住院期間 : 93.5.8~93.5.15 Chief Complaint : sudden loss of conscious for 2-52 5 minutes in the morning. General History DM under regular medical control for 10 years.
General History 林陳 珠 Female 69 years old 住院期間 : 93.5.8~93.5.15 Chief Complaint : sudden loss of conscious for 2-52 5 minutes in the morning. General History DM under regular medical control for 10 years.
Typical and Atypical Manifestations of Intrathoracic Sarcoidosis
 Typical and typical Manifestations of Intrathoracic Sarcoidosis Hyun Jin Park, MD 1 Jung Im Jung, MD 1 Myung Hee Chung, MD 1 Sun Wha Song, MD 1 Hyo Lim Kim, MD 1 Jun Hyun aik, MD 1 Dae Hee Han, MD 1 Ki
Typical and typical Manifestations of Intrathoracic Sarcoidosis Hyun Jin Park, MD 1 Jung Im Jung, MD 1 Myung Hee Chung, MD 1 Sun Wha Song, MD 1 Hyo Lim Kim, MD 1 Jun Hyun aik, MD 1 Dae Hee Han, MD 1 Ki
has the following disclosures to make:
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
Usual Interstitial pneumonia and Nonspecific Interstitial Pneumonia. Nitra and the Gangs.
 Usual Interstitial pneumonia and Nonspecific Interstitial Pneumonia Nitra and the Gangs. บทน ำและบทท ๓, ๑๐, ๑๒, ๑๓, ๑๔, ๑๕, ๑๗ Usual Interstitial Pneumonia (UIP) Most common & basic pathologic pattern
Usual Interstitial pneumonia and Nonspecific Interstitial Pneumonia Nitra and the Gangs. บทน ำและบทท ๓, ๑๐, ๑๒, ๑๓, ๑๔, ๑๕, ๑๗ Usual Interstitial Pneumonia (UIP) Most common & basic pathologic pattern
2015/4/14. Pneumonia. Diseases of Respiratory System Infection in the lung (distal airways, esp. alveoli) Lobar pneumonia.
 Lobar pneumonia.") Pneumonia Diseases of Respiratory System Infection in the lung (distal airways, esp. alveoli) 邓红浙江大学医学院病理学系 LUNG(reformed)5y-DH 1 hongdeng@zju.edu.cn Pathology (DH) 2 Pneumonia Bacteria pneumonia Viral
Pneumonia Diseases of Respiratory System Infection in the lung (distal airways, esp. alveoli) 邓红浙江大学医学院病理学系 LUNG(reformed)5y-DH 1 hongdeng@zju.edu.cn Pathology (DH) 2 Pneumonia Bacteria pneumonia Viral