Work-up of Respiratory Specimens Now you can breathe easier
|
|
|
- August Boyd
- 5 years ago
- Views:
Transcription
1 34 th Annual Meeting Southwestern Association of Clinical Microbiology Work-up of Respiratory Specimens Now you can breathe easier Yvette S. McCarter, PhD, D(ABMM) Director, Clinical Microbiology Laboratory UF Health Jacksonville Professor of Pathology University of Florida College of Medicine-Jacksonville


2 Disclosures No financial disclosures No discussion of off label uses Cat and parrot mommy 2
3 Objectives Discuss the value of the gram stained smear as a reliable rapid diagnostic tool and criteria for assessing specimen quality by microscopic screening. Describe recognition and reporting of organisms by genera rather than organism morphology. Discuss the criteria for and use of mixed flora in respiratory gram stains. Describe the Q score and Q234 systems and how they can be used to guide work up of lower respiratory tract cultures. Discuss the appropriate work up of bronchoalveolar lavage specimens. 3
4 The major goal of the clinical microbiology laboratory is to provide information of maximal clinical or epidemiological usefulness as rapidly as is consistent with acceptable accuracy and minimal cost. Jay P. Sanford, MD (1974) The culture of lower respiratory specimens may result in more unnecessary microbiologic effort than any other type of specimen. Raymond C. Bartlett, MD (1974) 4


5 Pathogenesis of Pneumonia Aspiration of colonizing flora Inhalation of aerosols Hematologic seeding 5
6 Oral Flora or Potential Pathogen? Oral Flora Corynebacterium spp. Coagulase negative staphylococci Staphylococcus aureus Neisseria spp. Haemophilus influenzae Streptococcus pneumoniae Moraxella catarrhalis Potential Pathogens Staphylococcus aureus Haemophilus influenzae Streptococcus pneumoniae Moraxella catarrhalis Gram negative bacilli Gram negative bacilli Oral flora CFU/mL 6
7 Utility of the Gram Stain Rapid, inexpensive, informational Evaluation of specimen quality Identify superficially contaminated specimens Enhance discrimination between samples with potential pathogens vs. colonizing flora Presumptive organism ID Guide rational selection of preliminary antibiotic therapy Guides interpretation of culture results 7
8 Utility of the Gram Stain Majority of the literature supports the clinical usefulness of gram stained sputum smears Wide range in reported sensitivity (35-96% and specificity (12-85%) Reference standard sputum culture Variable care in specimen collection Good quality specimen Multiple criteria for assessing Gram stain smears 8
9 Utility of the Gram Stain Sensitivity Specificity Population Comments Cao et al. J Infect Chemother 2004 Musher et al. CID 2004 Rosón et al. CID 2000 Anelavis et al. J Infect 2009 Blot et al. Am J Respir Crit Care Med 2000 Spn: 81% Hflu: 86% Mcat: 91% Spn: 98% Hflu: 95% Mcat: 98% Pediatric Spn: 57% NA Adult Included pts on antibiotics Spn: 57% Hflu: 82% Spn: 82% Hflu: 79% Saur: 76% GNR: 78% EA: 91% PTC: 70% Spn: 97% Hflu: 99% Spn: 93% Hflu: 96% Saur: 96% GNR: 95% EA: 64% PTC: 96% Adult (CAP) Adult (CAP) Adult (HAP) Presumptive Dx in 80% Specific criteria for Gram stain


10 Utility of the Gram Stain Gram stain DOES NOT diagnose the presence of pneumonia Once pneumonia diagnosed Gram stain is useful in determining probable etiologic agent 10
11 Utility of the Gram Stain Heineman et al J Clin Microbiol 6: % of the information gleaned from sputum cultures is clinically misleading in the absence of correlation with direct gram stain results Gleckman et al J Clin Microbiol 26: Selection of appropriate monotherapy 94% of the time when guided by bacterial morphotypes from the gram stain 11
12 Gram Stain Screening Criteria It all starts with a good smear Preparation Staining Standardization Consistent smear interpretation Establish quality of specimen Use interpretive comments 12
13 Gram Stain Screening Criteria Author (year) Method Minimum criteria Bartlett (1974) Sum of PMN/LPF (10-25, 1+; >25, 2+), mucus (1+); SEC (10-25, -1; >25, -2) Score of >0 Murray and Washington (1975) Geckler et al. (1977) Enumerate SEC/LPF <10 SEC/LPF <25 SEC/LPF Van Scoy (1977) Enumerate PMN/LPF >25 PMN/LPF Heineman and Radano (1979) Kalin et al Morris et al. (1993) Zaidi and Reller (1996) Ratio of PMN to SEC Enumerate SEC/LPF and presence/absence of organisms/oif Presence/absence of organisms/oif >10 PMN/SEC >5 PMN/SEC <10 SEC/LPF and organisms present Organisms present
14 Gram Stain Screening Criteria COLLECT DATE/TIME 2/10/ RESP CULTURE SPECIMEN: Sputum RECEIVE DATE/TIME 2/10/ REPORT STATUS: FINAL 2/10/15 DIRECT SMEAR SUGGESTS: No neutrophils Many squamous cells Not representative of lower respiratory tract secretions. Culture not performed. Please consult Microbiology if clinical considerations warrant complete processing of this specimen. (Specimen will be held 5 days). 14

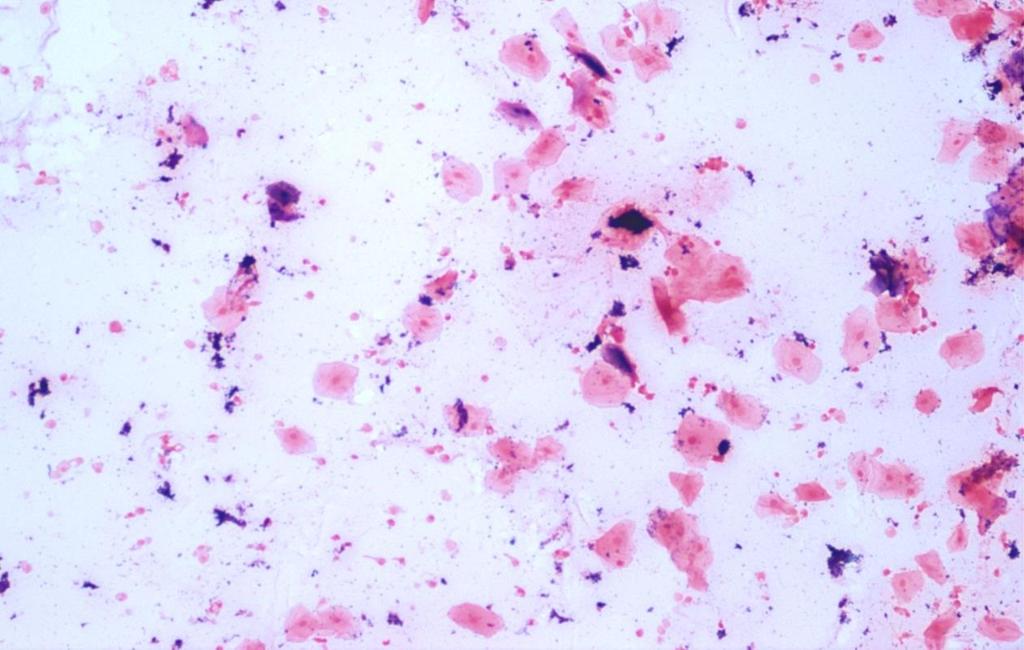
15 Poor Quality 14


16 Good Quality
17 Interpretation and Reporting of Organisms in Direct Smears Bartlett JAMA 247: Designation of organism genera more useful than description of organism morphology Bartlett et al Diagn Microbiol Infect Dis 14: Reliable differentiation of Gram negative bacilli Bacteroides or Haemophilus 95% Enteric Gram negative bacilli 82% Pseudomonas 56% 17

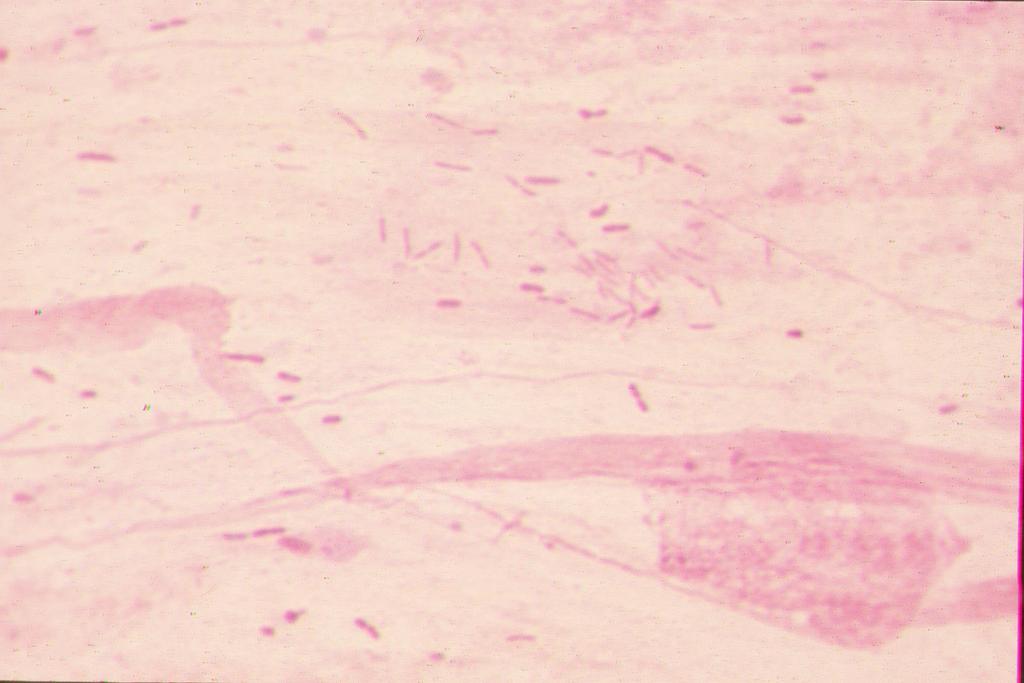
18 Enteric-like Gram negative bacilli Report only if 10 seen per oil immersion field 18

19 Gram negative coccobacilli suggestive of Haemophilus Report only if 10 seen per oil immersion field YM 19

20 Non-enteric Gram negative bacilli Report only if 10 seen per oil immersion field YM 20
21 21


22 Gram negative diplococci suggestive of Moraxella Report only if 25 seen per oil immersion field 22

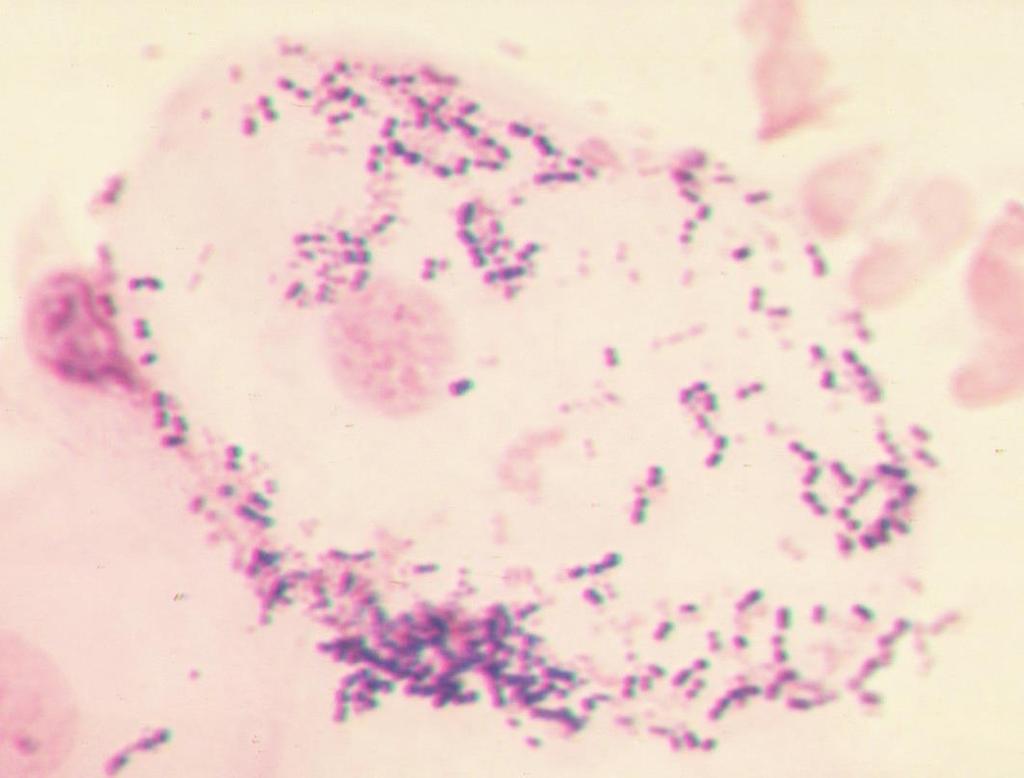
23 Gram positive cocci suggestive of Pneumococcus Report only if 25 pairs seen per oil immersion field YM 23

24 Gram positive cocci suggestive of Staphylococcus Report only if 50 seen per oil immersion field

25 Not Routinely Reported in Respiratory Gram Stains Gram positive cocci suggestive of Streptococcus


26 Not Routinely Reported in Respiratory Gram Stains Gram positive bacilli suggestive of Bacillus/Clostridium 26 Gram positive bacilli suggestive of Diphtheroids

27 NEVER Reported in Respiratory Gram Stains Yeast 27
28 Mixed Flora Used only with respiratory specimens Use of objective criteria (# of organisms present per OIF) to distinguish resident flora or colonizers from potential pathogens: Morphology Call if: Gram negative bacilli Moraxella Staph 10 organisms/oif 25 organisms/oif 50 organisms/oif S. pneumoniae 25 pairs/oif Bartlett 1982 JAMA Wright et al Am J Med Normandin et al ASM C-91 28
29 Mixed Flora DIRECT SMEAR SUGGESTS: Cells: Moderate neutrophils No squamous cells Bacteria: Few Gram negative rods Many Gram positive diplococci Moderate Gram negative diplococci Few Gram positive rods Few Gram negative coccobacilli Rare Gram positive cocci in clusters Few yeast DIRECT SMEAR SUGGESTS: Cells: Moderate neutrophils No squamous cells Bacteria: Gram positive diplococci suggestive of Pneumococcus Mixed flora 29
30 Mixed Flora Criteria Morphology Call if: Gram negative bacilli 10 organisms/oif Moraxella 25 organisms/oif Staph 50 organisms/oif S. pneumoniae 25 pairs/oif Streptococcus Gram positive bacilli Yeast 30
31 Work up of Respiratory Cultures There are no clear guidelines for working up bacterial cultures Literature Colleagues There seems to be a need for some consistency when performing culture work up Uniformity in work up and reporting of bacterial isolates When to perform AST 31
32 Work up of Respiratory Cultures Specimen Quality Premise: PMN are an indication of infection or inflammation SEC indicate superficial contamination If a specimen contains a large amount of SEC, superficial contamination is likely The specimen should be recollected Extensive testing on heavily mixed cultures should not routinely be performed 32
33 Work up of Respiratory Cultures Q-Score System Q234 System Sharp, SE, et al Cumitech 7B, Lower Respiratory Tract Infections. ASM Press, Washington, DC 33
34 Work up of Respiratory Cultures Q-Score System (RC Bartlett, 1974) Q-SCORE = # of potential pathogens (PP) to work up Squamous cells (-) Report value Key: 0 = no cells 1 = 1-9/lpf 2 = 10-24/lpf 3 = >25/lpf Neutrophils (+) Q0 = no cult Q1 = 1PP Q2 = 2PP Q3 = 3PP
35 Work up of Respiratory Cultures Q-Score System Up to 3 organisms can be considered potential pathogens (PP) and be worked up (ID/AST) if from a good quality specimen (Q3) The lower quality of the specimen (e.g., the more SEC present) the fewer the organisms worked up (Q2, Q1) 35
36 Work up of Respiratory Cultures Q-Score System # PP in culture < Q-score: work up PP with ID/AST (2PP) (Q3) # PP in culture > Q-score: Look to Gram stain (3PP) (Q2) Work up PP that were seen in Gram stain with ID/AST If all PP in the culture are seen in Gram stain = do not work up; perform morphological identification (MID) 36
37 Work up of Respiratory Cultures Q234 System (SE Sharp, 2002) Gram stain Quality Check: PMN & SEC Reject any sputum for culture according to normal protocol Culture work up is based on number of PP present: 2 PP = Work up (< 2 PP) 4 PP = MID 3 PP = Look to Gram stain Work up to 2 PP if they are seen in the GS If all 3 PP are seen in the GS, MID all 3 NOTE: If mixed flora > PPs = MID PP 37
38 Example 1: Sputum GS: many PMN (+3), few SEC (-1), many enteric-like gram negative bacilli, many gram positive cocci suggestive of Staph, few Mixed flora (yeast) CULT: moderate P. aeruginosa, moderate E.coli, moderate Staph aureus, few yeast WORK UP: Q Score (Q2=2PP): Q234 (3PP): 38
39 Example 1: Sputum GS: many PMN (+3), few SEC (-1), many enteric-like gram negative bacilli, many gram positive cocci suggestive of Staph, few Mixed flora (yeast) CULT: moderate P. aeruginosa, moderate E.coli, moderate Staph aureus, few yeast WORK UP: Q Score (Q2=2PP): Work up E. coli and S. aureus MID P. aeruginosa; Report Mixed flora Q234 (3PP): 39
40 Example 1: Sputum GS: many PMN (+3), few SEC (-1), many enteric-like gram negative bacilli, many gram positive cocci suggestive of Staph, few Mixed flora (yeast) CULT: moderate P. aeruginosa, moderate E.coli, moderate Staph aureus, few yeast WORK UP: Q Score (Q2=2PP): Work up E. coli and S. aureus MID P. aeruginosa; Report Mixed flora Q234 (3PP): Work up E. coli and S. aureus MID P. aeruginosa; Report Mixed flora 40
41 Example 2: Sputum GS: many PMN (+3), moderate SEC (-2), many nonentericlike gram negative bacilli, moderate Mixed flora CULT: many P. aeruginosa, moderate Staph aureus, few viridans Strep, few Neisseria WORK UP: Q Score (Q1=1PP): Q234 (2PP): 41
42 Example 2: Sputum GS: many PMN (+3), moderate SEC (-2), many nonentericlike gram negative bacilli, moderate Mixed flora CULT: many P. aeruginosa, moderate Staph aureus, few viridans Strep, few Neisseria WORK UP: Q Score (Q1=1PP): Work up P. aeruginosa MID S. aureus; Report Mixed flora Q234 (2PP): 42
43 Example 2: Sputum GS: many PMN (+3), moderate SEC (-2), many nonentericlike gram negative bacilli, moderate Mixed flora CULT: many P. aeruginosa, moderate Staph aureus, few viridans Strep, few Neisseria WORK UP: Q Score (Q1=1PP): Work up P. aeruginosa MID S. aureus; Report Mixed flora Q234 (2PP): Work up P. aeruginosa and S. aureus Report Mixed flora 43
44 Example 3: Tracheal Aspirate GS: many PMN (+3), few SEC (-1), many Mixed flora (few enteric-like GNB; moderate gram positive cocci suggestive of Staph) CULT: moderate diphtheroids, moderate coag negative Staph, few E.coli, rare Staph aureus WORK UP: Q Score (Q2=2PP): Q234 (2PP): 44
45 Example 3: Tracheal Aspirate GS: many PMN (+3), few SEC (-1), many Mixed flora (few enteric-like GNB; moderate gram positive cocci suggestive of Staph) CULT: moderate diphtheroids, moderate coag negative Staph, few E.coli, rare Staph aureus WORK UP: Q score (Q2=2PP): Work up E. coli and S. aureus Report Mixed flora Q234 (2PP): 45
46 Example 3: Tracheal Aspirate GS: many PMN (+3), few SEC (-1), many Mixed flora (few enteric-like GNB; moderate gram positive cocci suggestive of Staph) CULT: moderate diphtheroids, moderate coag negative Staph, few E.coli, rare Staph aureus WORK UP: Q-Score (Q2=2PP): Work up E. coli and S. aureus Report Mixed flora Q234 (2PP): Report Mixed flora MID E. coli and S. aureus ** ** If mixed flora > PPs = MID PP 46
47 Premise for Q Systems Based on published prevalence of potential pathogen colonization of the oropharynx The more superficially contaminated the specimen, the higher the # of colonizing organisms present Quality of specimen is important in determining acceptability of specimen and extent of culture work up If organisms seen in smear, greater chance they are associated with an infective process 47
48 Q Systems Advantages Offers a consistent approach for interpreting cultures Based on specimen quality (primarily SEC) Based on organisms seen in Gram stain (organism seen on smear should be in a significant number in the specimen, 10 5 /ml) Limits number of organisms worked up from mixed cultures reporting of misleading information minimized 48
49 Q Systems Advantages No Potential Pathogen is ever ignored All potential pathogens reported (may not perform full ID/AST) Pathogens that some believe should ALWAYS BE WORKED UP (S. aureus, b-strep, P. aeruginosa ) are identified and always indicated on the report Can be modified to include screening for MRSA, VRE, etc. 49
50 Q Systems Advantages Guidelines The Q Systems offer guidelines for a systematic approach to culture interpretation These Guidelines are just that = Guidelines! Exceptions can be made Any concerned physician can consult with microbiology to have further work performed on any culture if clinically indicated 50
51 Bronchoalveolar Lavage What to do with the BAL Quantitate or not What quantity to work up What to do with that resident flora When to do susceptibility testing? 51
52 Bronchoalveolar Lavage Quantitative cultures of BAL specimens are imperfect predictors of the presence of pneumonia in mechanically-ventilated patients.* Quantitative cultures have a reported sensitivity and specificity of 91% and 78%, respectively.** Despite the limitations, there are no alternatives that are clearly better *Fujitani and Yu, Clin Infect Dis 43 Suppl 2:S106, 2006 **Mayhall, Emerg Infect Dis 7:200,
53 Bronchoalveolar Lavage Quantitative BAL Cultures Higher likelihood of pneumonia if there is at least one microorganism obtained at a concentration of 10 4 CFU/mL of lung fluid. * Commensal flora There should be no commensal flora at this site at concentrations 10 4 CFU/mL Commensal oral flora, when aspirated, can cause pneumonia Quantitation is used to determine whether this has occurred or not There should also be NO squamous epithelial cells present (this represents oral contamination) *Mayhall, Emerg Infect Dis 7:200, 2001; Baselski & Wunderink, Clin Microbiol Rev 7:533, 1994) 53
54 Bronchoalveolar Lavage IDSA/ATS guidelines for VAP "Significant growth of oropharyngeal commensals (viridans group streptococci, coagulase-negative staphylococci, Neisseria spp., and Corynebacterium spp.) from distal bronchial specimens is difficult to interpret, but these organisms can produce infection in immunocompromised hosts and some immunocompetent patients. Am J Respir Crit Care Med 171:388,
55 Bronchoalveolar Lavage Options for POTENTIAL PATHOGENS Cutoff Quantitate and perform ID/AST on potential pathogens if 10,000 for BAL and 1,000 for Brush using Q score or Q234 systems Quantitate and perform ID/AST on up to 3 potential pathogens if 10,000 for BAL and 1000 for Brush (if > 3 report MID) Option for POTENTIAL PATHOGENS < Cutoff Quantitate and report MID on any potential pathogens <10,000 for BAL and < 1,000 for Brush 55
56 Bronchoalveolar Lavage Options for ORAL FLORA #1 Quantitate total amount and report as Mixed flora If no SEC were seen on initial GS, for each OF isolate at 10,000 for BAL and 1,000 for Brush, report MID. #2 If no SEC were seen on initial GS, for each OF isolate at <10,000 for BAL and <1,000 for Brush, quantitate and report TOTAL AMOUNT of combined oral flora (i.e diphtheroids non hemolytic strep = 15,000 Mixed flora) If SEC were seen on initial GS (= contamination), quantitate and report Mixed flora regardless of amount present 56
57 Bronchoalveolar Lavage Oral Flora Option #1 Example Direct GS: Few PMN, No SEC, No organisms seen Culture grows 50,000 colonies/ml Staphylococcus aureus 15,000 colonies/ml Coag. neg staphylococci 15,000 colonies/ml a-streptococci (not Pneumo) REPORT: 50,000 colonies/ml S. aureus with AST 30,000 colonies/ml Mixed flora 57
58 Bronchoalveolar Lavage Option #2 Example (No SEC and MF 10,000) Direct GS: Few PMN, No SEC, No organisms seen Culture grows 50,000 colonies/ml Staphylococcus aureus 15,000 colonies/ml Coag. neg staphylococci 15,000 colonies/ml a-streptococci (not Pneumo) REPORT: 50,000 colonies/ml S. aureus with AST 15,000 colonies/ml Coag. neg staphylococci 15,000 colonies/ml a-streptococci (not Pneumo) Add message to contact Microbiology if work up is needed 58
59 Bronchoalveolar Lavage Option #2 Example (No SEC and MF <10,000) Direct GS: Few PMN, No SEC, No organisms seen Culture grows 50,000 colonies/ml Enterobacter spp. 25,000 colonies/ml Klebsiella spp. 8,000 colonies/ml Coag. neg staphylococci 7,000 colonies/ml a-streptococci (not Pneumo) REPORT: 50,000 colonies/ml Enterobacter (species) with AST 25,000 colonies/ml Klebsiella (species) with AST 15,000 colonies/ml Mixed flora 59
60 Bronchoalveolar Lavage Option #2 Example (SEC present) Direct GS: Moderate PMN, Few SEC, Many GPC/clusters Culture grows 50,000 colonies/ml Staphylococcus aureus 15,000 colonies/ml Coag. neg staphylococci 15,000 colonies/ml a-streptococci (not Pneumo) REPORT: 50,000 colonies/ml S. aureus with AST 30,000 colonies/ml Mixed flora 60
 Pick one of the Q s (Q systems) Report consistent and clinically-relevant respiratory culture results")
61 Conclusions Gram stain of direct respiratory specimens is useful DO IT WELL and USE IT Specimen quality assessment Rapid presumptive identification Guide culture work up Mind your P s and Q s Determine your P s (potential pathogens) Pick one of the Q s (Q systems) Report consistent and clinically-relevant respiratory culture results 61


62 Questions 62
Work up of Respiratory & Wound Cultures:
 Work up of Respiratory & Wound Cultures: Culture work up 2 Systematic approaches 1 Work up of Respiratory & Wound Cultures Resident flora Colonizing organisms Pathogens 2 Work up of Respiratory & Wound
Work up of Respiratory & Wound Cultures: Culture work up 2 Systematic approaches 1 Work up of Respiratory & Wound Cultures Resident flora Colonizing organisms Pathogens 2 Work up of Respiratory & Wound
Acceptability of Sputum Specimens
 JOURNAL OF CLINICAL MICROBIOLOGY, Oct. 1982, p. 627-631 0095-1137/82/100627-05$02.00/0 Copyright C 1982, American Society for Microbiology Vol. 16, No. 4 Comparison of Six Different Criteria for Judging
JOURNAL OF CLINICAL MICROBIOLOGY, Oct. 1982, p. 627-631 0095-1137/82/100627-05$02.00/0 Copyright C 1982, American Society for Microbiology Vol. 16, No. 4 Comparison of Six Different Criteria for Judging
Babak Valizadeh, DCLS
 Laboratory Diagnosis of Bacterial Infections of the Respiratory Tract Babak Valizadeh, DCLS 1391. 02. 05 2012. 04. 25 Babak_Valizadeh@hotmail.com Biological Safety Cabinet Process specimens in biological
Laboratory Diagnosis of Bacterial Infections of the Respiratory Tract Babak Valizadeh, DCLS 1391. 02. 05 2012. 04. 25 Babak_Valizadeh@hotmail.com Biological Safety Cabinet Process specimens in biological
Unit II Problem 2 Microbiology Lab: Pneumonia
 Unit II Problem 2 Microbiology Lab: Pneumonia - What are the steps needed to obtain a proper sputum specimen? You need the following: A wide-mouth labeled container. Gloves. Water. Mouth wash + tissues.
Unit II Problem 2 Microbiology Lab: Pneumonia - What are the steps needed to obtain a proper sputum specimen? You need the following: A wide-mouth labeled container. Gloves. Water. Mouth wash + tissues.
References Required document for Laboratory Accreditation by the College of American Pathologists.
 Subject Culture: Lower Respiratory Tract Index Number Lab-3375 Section Laboratory Subsection Microbiology Category Departmental Contact Sarah Stoner Last Revised 9/11/2017 References Required document
Subject Culture: Lower Respiratory Tract Index Number Lab-3375 Section Laboratory Subsection Microbiology Category Departmental Contact Sarah Stoner Last Revised 9/11/2017 References Required document
Lower Respiratory Tract Infection
 Lower Respiratory Tract Infection - Clinical Diseases and etiologic agents -Sample Collection and transport -Direct Smear (interpretation and Report) -Culture methods (interpretation and Report) The culture
Lower Respiratory Tract Infection - Clinical Diseases and etiologic agents -Sample Collection and transport -Direct Smear (interpretation and Report) -Culture methods (interpretation and Report) The culture
HEALTHCARE-ASSOCIATED PNEUMONIA: EPIDEMIOLOGY, MICROBIOLOGY & PATHOPHYSIOLOGY
 HEALTHCARE-ASSOCIATED PNEUMONIA: EPIDEMIOLOGY, MICROBIOLOGY & PATHOPHYSIOLOGY David Jay Weber, M.D., M.P.H. Professor of Medicine, Pediatrics, & Epidemiology Associate Chief Medical Officer, UNC Health
HEALTHCARE-ASSOCIATED PNEUMONIA: EPIDEMIOLOGY, MICROBIOLOGY & PATHOPHYSIOLOGY David Jay Weber, M.D., M.P.H. Professor of Medicine, Pediatrics, & Epidemiology Associate Chief Medical Officer, UNC Health
Correlation of Sputum Gram Stain and Sputum Culture for Respiratory Tract Infections in a Tertiary Care Hospital, Ballari, India
 International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 6 (2017) pp. 3008-3012 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.606.357
International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 6 (2017) pp. 3008-3012 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.606.357
Sputum Screening by Nomarski Interference Contrast
 JOURNAL OF CLINICAL MICROBIOLOGY, Apr. 1979, p. 520-524 0095-1137/79/04-0520/05$02.00/0 Vol. 9, No. 4 Sputum Screening by Nomarski Interference Contrast Microscopy DAVID F. WELCH AND MICHAEL T. KELLYt*
JOURNAL OF CLINICAL MICROBIOLOGY, Apr. 1979, p. 520-524 0095-1137/79/04-0520/05$02.00/0 Vol. 9, No. 4 Sputum Screening by Nomarski Interference Contrast Microscopy DAVID F. WELCH AND MICHAEL T. KELLYt*
Culture of Throat, Sputum and Other Respiratory Specimens
 Culture of Throat, Sputum and Other Respiratory Specimens Carol Spiegel, Ph.D., D(ABMM) Professor of Pathology and Laboratory Medicine at the UW School of Medicine and Public Health and Director of Clinical
Culture of Throat, Sputum and Other Respiratory Specimens Carol Spiegel, Ph.D., D(ABMM) Professor of Pathology and Laboratory Medicine at the UW School of Medicine and Public Health and Director of Clinical
The Bacteriology of Bronchiectasis in Australian Indigenous children
 The Bacteriology of Bronchiectasis in Australian Indigenous children Kim Hare, Amanda Leach, Peter Morris, Heidi Smith-Vaughan, Anne Chang Presentation outline What is bronchiectasis? Our research at Menzies
The Bacteriology of Bronchiectasis in Australian Indigenous children Kim Hare, Amanda Leach, Peter Morris, Heidi Smith-Vaughan, Anne Chang Presentation outline What is bronchiectasis? Our research at Menzies
ANWICU knowledge
 ANWICU knowledge www.anwicu.org.uk This presenta=on is provided by ANWICU We are a collabora=ve associa=on of ICUs in the North West of England. Permission to provide this presenta=on has been granted
ANWICU knowledge www.anwicu.org.uk This presenta=on is provided by ANWICU We are a collabora=ve associa=on of ICUs in the North West of England. Permission to provide this presenta=on has been granted
INTRODUCTION TO UPPER RESPIRATORY TRACT DISEASES
 Upper Respiratory Tract Infections Return to Syllabus INTRODUCTION TO UPPER RESPIRATORY TRACT DISEASES General Goal: To know the major mechanisms of defense in the URT, the major mechanisms invaders use
Upper Respiratory Tract Infections Return to Syllabus INTRODUCTION TO UPPER RESPIRATORY TRACT DISEASES General Goal: To know the major mechanisms of defense in the URT, the major mechanisms invaders use
CHEST VOLUME 117 / NUMBER 4 / APRIL, 2000 Supplement
 CHEST VOLUME 117 / NUMBER 4 / APRIL, 2000 Supplement Evidence-Based Assessment of Diagnostic Tests for Ventilator- Associated Pneumonia* Executive Summary Ronald F. Grossman, MD, FCCP; and Alan Fein, MD,
CHEST VOLUME 117 / NUMBER 4 / APRIL, 2000 Supplement Evidence-Based Assessment of Diagnostic Tests for Ventilator- Associated Pneumonia* Executive Summary Ronald F. Grossman, MD, FCCP; and Alan Fein, MD,
POLICY FOR TREATMENT OF LOWER RESPIRATORY TRACT INFECTIONS
 POLICY F TREATMENT OF LOWER RESPIRATY TRACT INFECTIONS Written by: Dr M Milupi, Consultant Microbiologist Date: June 2018 Approved by: The Drugs & Therapeutics Committee Date: July 2018 Implementation
POLICY F TREATMENT OF LOWER RESPIRATY TRACT INFECTIONS Written by: Dr M Milupi, Consultant Microbiologist Date: June 2018 Approved by: The Drugs & Therapeutics Committee Date: July 2018 Implementation
Normal Human Flora. (Human Microbiome) Dr.Sarmad M.H. Zeiny Baghdad College of Medicine
 Dr.Sarmad M.H. Zeiny Baghdad College of Medicine") Normal Human Flora (Human Microbiome) Dr.Sarmad M.H. Zeiny Baghdad College of Medicine 2014-2015 Objectives Describe important human normal flora. Demonstrate the epidemiology of human normal flora. Determine
Normal Human Flora (Human Microbiome) Dr.Sarmad M.H. Zeiny Baghdad College of Medicine 2014-2015 Objectives Describe important human normal flora. Demonstrate the epidemiology of human normal flora. Determine
Hospital Acquired Pneumonias
 Hospital Acquired Pneumonias Hospital Acquired Pneumonia ( HAP ) Hospital acquired pneumonia ( HAP ) is defined as an infection of the lung parenchyma developing during hospitalization and not present
Hospital Acquired Pneumonias Hospital Acquired Pneumonia ( HAP ) Hospital acquired pneumonia ( HAP ) is defined as an infection of the lung parenchyma developing during hospitalization and not present
Blood culture 壢新醫院 病理檢驗科 陳啟清技術主任
 Blood culture 壢新醫院 病理檢驗科 陳啟清技術主任 A Positive Blood Culture Clinically Important Organism Failure of host defenses to contain an infection at its primary focus Failure of the physician to effectively eradicate,
Blood culture 壢新醫院 病理檢驗科 陳啟清技術主任 A Positive Blood Culture Clinically Important Organism Failure of host defenses to contain an infection at its primary focus Failure of the physician to effectively eradicate,
V. Reporting UNIVERSITY HEALTH NETWORK/MOUNT SINAI HOSPITAL, DEPARTMENT OF MICROBIOLOGY
 Version: 1.0 CURRENT 1 of 26 TABLE OF CONTENTS Urinary Tract Infection Workup I. Introduction... 3 II. Specimen Collection and Transplant... 4 III. Reagents/Materials/Media... 4 IV. Procedure... 4 Asymptomatic
Version: 1.0 CURRENT 1 of 26 TABLE OF CONTENTS Urinary Tract Infection Workup I. Introduction... 3 II. Specimen Collection and Transplant... 4 III. Reagents/Materials/Media... 4 IV. Procedure... 4 Asymptomatic
BACTERIOLOGY PROGRAMME AND PLAN OF TEACHING 3 rd Semester (academic year )
") BACTERIOLOGY PROGRAMME AND PLAN OF TEACHING 3 rd Semester (academic year 2012-2013) 19. 10. 2012. Introduction in microbiology, bacterial taxonomy, general bacterial prop Bacterial structures, biosynthesis
BACTERIOLOGY PROGRAMME AND PLAN OF TEACHING 3 rd Semester (academic year 2012-2013) 19. 10. 2012. Introduction in microbiology, bacterial taxonomy, general bacterial prop Bacterial structures, biosynthesis
A 2-Year Study of Gram Stain Competency Assessment in 40 Clinical Laboratories
 Microbiology and Infectious Disease / GRAM STAIN COMPETENCY ASSESSMENT A 2-Year Study of Gram Stain Competency Assessment in 40 Clinical Laboratories Nancy Goodyear, PhD, 1 Sara Kim, PhD, 2,3 Mary Reeves,
Microbiology and Infectious Disease / GRAM STAIN COMPETENCY ASSESSMENT A 2-Year Study of Gram Stain Competency Assessment in 40 Clinical Laboratories Nancy Goodyear, PhD, 1 Sara Kim, PhD, 2,3 Mary Reeves,
PULMONARY EMERGENCIES
 EMERGENCIES I. Pneumonia A. Bacterial Pneumonia (most common cause of a focal infiltrate) 1. Epidemiology a. Accounts for up to 10% of hospital admissions in the U.S. b. Most pneumonias are the result
EMERGENCIES I. Pneumonia A. Bacterial Pneumonia (most common cause of a focal infiltrate) 1. Epidemiology a. Accounts for up to 10% of hospital admissions in the U.S. b. Most pneumonias are the result
Diagnosis of Ventilator- Associated Pneumonia: Where are we now?
 Diagnosis of Ventilator- Associated Pneumonia: Where are we now? Gary French Guy s & St. Thomas Hospital & King s College, London BSAC Guideline 2008 Masterton R, Galloway A, French G, Street M, Armstrong
Diagnosis of Ventilator- Associated Pneumonia: Where are we now? Gary French Guy s & St. Thomas Hospital & King s College, London BSAC Guideline 2008 Masterton R, Galloway A, French G, Street M, Armstrong
Skin reactivity to autologous bacteria isolated from respiratory tract of patients with obstructive pulmonary disease
 Skin reactivity to autologous bacteria 149 Original Article Skin reactivity to autologous bacteria isolated from respiratory tract of patients with obstructive pulmonary disease J. Halasa 1, M. Halasa
Skin reactivity to autologous bacteria 149 Original Article Skin reactivity to autologous bacteria isolated from respiratory tract of patients with obstructive pulmonary disease J. Halasa 1, M. Halasa
Hospital-acquired Pneumonia
 Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
ISF criteria (International sepsis forum consensus conference of infection in the ICU) Secondary peritonitis
 Secondary peritonitis") Appendix with supplementary material. This appendix was part of the submitted manuscript and has been peer reviewed. It is posted as supplied by the authors. Supplementary Tables Table S1. Definitions
Appendix with supplementary material. This appendix was part of the submitted manuscript and has been peer reviewed. It is posted as supplied by the authors. Supplementary Tables Table S1. Definitions
Optimizing MALDI-TOF Use. Clinical Impact Laboratory Impact
 Optimizing MALDI-TOF Use Clinical Impact Laboratory Impact Christine C. Ginocchio, PhD, MT (ASCP) Clinical Professor of Medicine Hofstra North Shore-LIJ School of Medicine, NY VP, Global Microbiology Affairs,
Optimizing MALDI-TOF Use Clinical Impact Laboratory Impact Christine C. Ginocchio, PhD, MT (ASCP) Clinical Professor of Medicine Hofstra North Shore-LIJ School of Medicine, NY VP, Global Microbiology Affairs,
Critical Care Nursing Theory. Pneumonia. - Pneumonia is an acute infection of the pulmonary parenchyma
 - is an acute infection of the pulmonary parenchyma - is a common infection encountered by critical care nurses when it complicates the course of a serious illness or leads to acute respiratory distress.
- is an acute infection of the pulmonary parenchyma - is a common infection encountered by critical care nurses when it complicates the course of a serious illness or leads to acute respiratory distress.
ESCMID Online Lecture Library. by author
 Microbiological evaluation: how to report the results Alvaro Pascual MD, PhD Infectious Diseases and Clinical Microbiology Unit. University Hospital Virgen Macarena University of Sevilla BSI management
Microbiological evaluation: how to report the results Alvaro Pascual MD, PhD Infectious Diseases and Clinical Microbiology Unit. University Hospital Virgen Macarena University of Sevilla BSI management
Staphylococci. Gram stain: gram positive cocci arranged in clusters.
 Microbiology lab Respiratory system Third medical year Lab contents: Gram positive bacteria (Staphylococcus and Streptococcus spp), two types of filamentous fungi (Aspergillus and Penicillium spp), and
Microbiology lab Respiratory system Third medical year Lab contents: Gram positive bacteria (Staphylococcus and Streptococcus spp), two types of filamentous fungi (Aspergillus and Penicillium spp), and
Usefulness of Gram staining of tracheal aspirates in initial therapy for ventilator-associated pneumonia in extremely preterm neonates
 (2010) 30, 270 274 r 2010 Nature Publishing Group All rights reserved. 0743-8346/10 $32 www.nature.com/jp ORIGINAL ARTICLE Usefulness of Gram staining of tracheal aspirates in initial therapy for ventilator-associated
(2010) 30, 270 274 r 2010 Nature Publishing Group All rights reserved. 0743-8346/10 $32 www.nature.com/jp ORIGINAL ARTICLE Usefulness of Gram staining of tracheal aspirates in initial therapy for ventilator-associated
Normal Flora PROF. HANAN HABIB DEPARTMENT OF PATHOLOGY COLLEGE OF MEDICINE, KSU
 Normal Flora PROF. HANAN HABIB DEPARTMENT OF PATHOLOGY COLLEGE OF MEDICINE, KSU Objectives 1. Define the terms: Normal Flora, Resident flora, Transient flora and carrier state 2. Know the origin of normal
Normal Flora PROF. HANAN HABIB DEPARTMENT OF PATHOLOGY COLLEGE OF MEDICINE, KSU Objectives 1. Define the terms: Normal Flora, Resident flora, Transient flora and carrier state 2. Know the origin of normal
CAP, HCAP, HAP, VAP. 1. In 1898, William Osler described community-acquired pneumonia as:
 1. In 1898, William Osler described community-acquired pneumonia as: Brad Sharpe, M.D. Professor of Clinical Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu I have no relevant financial
1. In 1898, William Osler described community-acquired pneumonia as: Brad Sharpe, M.D. Professor of Clinical Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu I have no relevant financial
Bacteria causing respiratory tract infections
 Editing file Bacteria causing respiratory tract infections Objectives : Recognize signs & symptoms of different bacterial respiratory tract infections Be able to come up with a short differential to relevant
Editing file Bacteria causing respiratory tract infections Objectives : Recognize signs & symptoms of different bacterial respiratory tract infections Be able to come up with a short differential to relevant
Pathology of Pneumonia
 Pathology of Pneumonia Dr. Atif Ali Bashir Assistant Professor of Pathology College of Medicine Majma ah University Introduction: 5000 sq meters of area.! (olympic track) Filters >10,000 L of air / day!
Pathology of Pneumonia Dr. Atif Ali Bashir Assistant Professor of Pathology College of Medicine Majma ah University Introduction: 5000 sq meters of area.! (olympic track) Filters >10,000 L of air / day!
M E D I C A L L A B O R A T O R Y
 M E D I C A L L A B O R A T O R Y E V A L U A T I O N PARTICIPANT SUMMARY 2 0 1 7 Microbiology 2017 MLE-M1 Total Commitment to Education and Service Provided by ACP, Inc. Evaluation Criteria... 2 Microbiology
M E D I C A L L A B O R A T O R Y E V A L U A T I O N PARTICIPANT SUMMARY 2 0 1 7 Microbiology 2017 MLE-M1 Total Commitment to Education and Service Provided by ACP, Inc. Evaluation Criteria... 2 Microbiology
The Clinical Significance of Blood Cultures. Presented BY; Cindy Winfrey, MSN, RN, CIC, DON- LTC TM, VA- BC TM
 The Clinical Significance of Blood Cultures Presented BY; Cindy Winfrey, MSN, RN, CIC, DON- LTC TM, VA- BC TM OVERVIEW Blood cultures are considered an important laboratory tool used to diagnose serious
The Clinical Significance of Blood Cultures Presented BY; Cindy Winfrey, MSN, RN, CIC, DON- LTC TM, VA- BC TM OVERVIEW Blood cultures are considered an important laboratory tool used to diagnose serious
Validation of sputum Gram stain for treatment of community-acquired pneumonia and healthcare-associated pneumonia: a prospective observational study
 Fukuyama et al. BMC Infectious Diseases 2014, 14:534 RESEARCH ARTICLE Open Access Validation of sputum Gram stain for treatment of community-acquired pneumonia and healthcare-associated pneumonia: a prospective
Fukuyama et al. BMC Infectious Diseases 2014, 14:534 RESEARCH ARTICLE Open Access Validation of sputum Gram stain for treatment of community-acquired pneumonia and healthcare-associated pneumonia: a prospective
PEACEHEALTH LABORATORIES
 360-414-2306 www.peacehealthlabs.org Critical Values Call List - Longview Critical values are reported per the criteria published below. Laboratory results meeting these criteria indicate potential life-threatening
360-414-2306 www.peacehealthlabs.org Critical Values Call List - Longview Critical values are reported per the criteria published below. Laboratory results meeting these criteria indicate potential life-threatening
Nosocomial Pneumonia. <5 Days: Non-Multidrug-Resistant Bacteria
 Nosocomial Pneumonia Meredith Deutscher, MD Troy Schaffernocker, MD Ohio State University Burden of Hospital-Acquired Pneumonia Second most common nosocomial infection in the U.S. 5-10 episodes per 1000
Nosocomial Pneumonia Meredith Deutscher, MD Troy Schaffernocker, MD Ohio State University Burden of Hospital-Acquired Pneumonia Second most common nosocomial infection in the U.S. 5-10 episodes per 1000
320 MBIO Microbial Diagnosis. Aljawharah F. Alabbad Noorah A. Alkubaisi 2017
 320 MBIO Microbial Diagnosis Aljawharah F. Alabbad Noorah A. Alkubaisi 2017 Pathogens of the Urinary tract The urinary system is composed of organs that regulate the chemical composition and volume of
320 MBIO Microbial Diagnosis Aljawharah F. Alabbad Noorah A. Alkubaisi 2017 Pathogens of the Urinary tract The urinary system is composed of organs that regulate the chemical composition and volume of
Healthcare-associated infections acquired in intensive care units
 SURVEILLANCE REPORT Annual Epidemiological Report for 2015 Healthcare-associated infections acquired in intensive care units Key facts In 2015, 11 788 (8.3%) of patients staying in an intensive care unit
SURVEILLANCE REPORT Annual Epidemiological Report for 2015 Healthcare-associated infections acquired in intensive care units Key facts In 2015, 11 788 (8.3%) of patients staying in an intensive care unit
Cell counting (EtBr) Before cell-lysis. Cell-lysis by 3% SDS beads beating. After cell-lysis
 Before cell-lysis. Cell-lysis by 3% SDS beads beating. After cell-lysis") Key words Sample Cell counting (EtBr) DNA extraction Cell-lysis by 3% SDS beads beating Before cell-lysis After cell-lysis Cell-lysis efficiency (Maintained70%) PCR PCR amplification of partial fragments
Key words Sample Cell counting (EtBr) DNA extraction Cell-lysis by 3% SDS beads beating Before cell-lysis After cell-lysis Cell-lysis efficiency (Maintained70%) PCR PCR amplification of partial fragments
Bacterial Identification
 JOURNAL OF CLINICAL MICROBIOLOGY, July 1994, p. 1757-1762 0095-1137/94/$04.00+0 Copyright C 1994, American Society for Microbiology Vol. 32, No. 7 Clinical Impact of Rapid In Vitro Susceptibility Testing
JOURNAL OF CLINICAL MICROBIOLOGY, July 1994, p. 1757-1762 0095-1137/94/$04.00+0 Copyright C 1994, American Society for Microbiology Vol. 32, No. 7 Clinical Impact of Rapid In Vitro Susceptibility Testing
Respiratory Tract Infections
 JOURNAL OF CLINICAL MICROBIOLOGY, May 1987, p. 758-762 0095-1137/87/050758-05$02.00/0 Copyright 1987, American Society for Microbiology Vol. 25, No. 5 Nonvalue of Sputum Culture in the Management of Lower
JOURNAL OF CLINICAL MICROBIOLOGY, May 1987, p. 758-762 0095-1137/87/050758-05$02.00/0 Copyright 1987, American Society for Microbiology Vol. 25, No. 5 Nonvalue of Sputum Culture in the Management of Lower
Discrepancies in the recovery of bacteria from multiple sinuses in acute and chronic sinusitis
 Journal of Medical Microbiology (2004), 53, 879 885 DOI 10.1099/jmm.0.45655-0 Short Communication Correspondence Itzhak Brook ib6@georgetown.edu Received 1 March 2004 Accepted 18 May 2004 Discrepancies
Journal of Medical Microbiology (2004), 53, 879 885 DOI 10.1099/jmm.0.45655-0 Short Communication Correspondence Itzhak Brook ib6@georgetown.edu Received 1 March 2004 Accepted 18 May 2004 Discrepancies
BACTERIOLOGY OF POSTOPERATIVE PNEUMONIA EOLE STUDY Dupont H ICM 2003, 29,
 Pneumonies: classification Pneumonies communautaires Pneumonies associées aux soins Non nosocomiales Nosocomiales Malade ventilé précoces tardives Malade non ventilé The concept of Health Care Associated
Pneumonies: classification Pneumonies communautaires Pneumonies associées aux soins Non nosocomiales Nosocomiales Malade ventilé précoces tardives Malade non ventilé The concept of Health Care Associated
Community Acquired & Nosocomial Pneumonias
 Community Acquired & Nosocomial Pneumonias IDSA/ATS 2007 & 2016 Guidelines José Luis González, MD Clinical Assistant Professor of Medicine Outline Intro - Definitions & Diagnosing CAP treatment VAP & HAP
Community Acquired & Nosocomial Pneumonias IDSA/ATS 2007 & 2016 Guidelines José Luis González, MD Clinical Assistant Professor of Medicine Outline Intro - Definitions & Diagnosing CAP treatment VAP & HAP
Respiratory Pathogen Panel TEM-PCR Test Code:
 Respiratory Pathogen Panel TEM-PCR Test Code: 220000 Tests in this Panel Enterovirus group Human bocavirus Human coronavirus (4 types) Human metapneumovirus Influenza A - Human influenza Influenza A -
Respiratory Pathogen Panel TEM-PCR Test Code: 220000 Tests in this Panel Enterovirus group Human bocavirus Human coronavirus (4 types) Human metapneumovirus Influenza A - Human influenza Influenza A -
Streptococci facultative anaerobe
 THE GENUS STREPTOCOCCUS The genus Streptococcus obtains Gram-positive cocci, nonmotile, nonsporeforming, arranged mostly in chains or in pairs. Most species are facultative anaerobes. Some of streptococci
THE GENUS STREPTOCOCCUS The genus Streptococcus obtains Gram-positive cocci, nonmotile, nonsporeforming, arranged mostly in chains or in pairs. Most species are facultative anaerobes. Some of streptococci
THE MICROBIOLOGICAL PROFILE OF VENTILATOR ASSOCIATED PNEUMONIA.
 THE MICROBIOLOGICAL PROFILE OF VENTILATOR ASSOCIATED PNEUMONIA. Dr. Poonam C. Sharma, Dr. S. S. Raut, Dr. S. R. More, Dr. V. S. Rathod, Dr. V. M. Gujar. 1. Post Graduate Student, Department of Microbiology,
THE MICROBIOLOGICAL PROFILE OF VENTILATOR ASSOCIATED PNEUMONIA. Dr. Poonam C. Sharma, Dr. S. S. Raut, Dr. S. R. More, Dr. V. S. Rathod, Dr. V. M. Gujar. 1. Post Graduate Student, Department of Microbiology,
Anatomy kidney ureters bladder urethra upper lower
 Urinary tract Anatomy The urinary tract consists of the kidney, ureters, bladder, and urethra. Urinary tract infections can be either: upper or lower based primarily on the anatomic location of the infection.
Urinary tract Anatomy The urinary tract consists of the kidney, ureters, bladder, and urethra. Urinary tract infections can be either: upper or lower based primarily on the anatomic location of the infection.
Community Acquired Pneumonia. Background & Rationale to North American Guidelines. Lionel Mandell MD FRCPC Brussels Belgium
 Community Acquired Pneumonia Background & Rationale to North American Guidelines Lionel Mandell MD FRCPC Brussels Belgium Consider Impact of the disease Issues to reflect upon Impact of the Disease 3-4
Community Acquired Pneumonia Background & Rationale to North American Guidelines Lionel Mandell MD FRCPC Brussels Belgium Consider Impact of the disease Issues to reflect upon Impact of the Disease 3-4
심사사례 성균관의대강북삼성병원감염내과 염준섭
 폐렴및호흡기질환의치료와 심사사례 성균관의대강북삼성병원감염내과 염준섭 서 론 미국 : 매년 560만명의환자발생 -- 20% 입원 사망률 - 외래에서치료가능한환자 : 1-5% - 입원치료가필요한환자 : 25% - 국내 ( 사망원인통계결과 ) : 2001년 ; 6.1명 /10만명, 1991년 ; 5.1명 /10만명 50-90% 가외래에서치료 30-40% 는원인을밝혀내지못함
폐렴및호흡기질환의치료와 심사사례 성균관의대강북삼성병원감염내과 염준섭 서 론 미국 : 매년 560만명의환자발생 -- 20% 입원 사망률 - 외래에서치료가능한환자 : 1-5% - 입원치료가필요한환자 : 25% - 국내 ( 사망원인통계결과 ) : 2001년 ; 6.1명 /10만명, 1991년 ; 5.1명 /10만명 50-90% 가외래에서치료 30-40% 는원인을밝혀내지못함
Blood cultures in ED. Dr Sebastian Chang MBBS FACEM
 Blood cultures in ED Dr Sebastian Chang MBBS FACEM Why do we care about blood cultures? blood cultures are the most direct method for detecting bacteraemia in patients a positive blood culture: 1. can
Blood cultures in ED Dr Sebastian Chang MBBS FACEM Why do we care about blood cultures? blood cultures are the most direct method for detecting bacteraemia in patients a positive blood culture: 1. can
Monitoring of Enhanced Surveillance for Severe and Fatal Pneumonia, 1 st January 31 st March 2015
 Monitoring of Enhanced Surveillance for Severe and Fatal Pneumonia, 1 st January 31 st March 2015 1. The cumulative cases report since December 2010 and cases report during January to March 2015 During
Monitoring of Enhanced Surveillance for Severe and Fatal Pneumonia, 1 st January 31 st March 2015 1. The cumulative cases report since December 2010 and cases report during January to March 2015 During
Central Nervous System Infection
 Central Nervous System Infection Lingyun Shao Department of Infectious Diseases Huashan Hospital, Fudan University Definition Meningitis: an inflammation of the arachnoid membrane, the pia mater, and the
Central Nervous System Infection Lingyun Shao Department of Infectious Diseases Huashan Hospital, Fudan University Definition Meningitis: an inflammation of the arachnoid membrane, the pia mater, and the
Pneumonia (PNEU) and Ventilator-Associated Pneumonia (VAP) Prevention. Basics of Infection Prevention 2-Day Mini-Course 2016
 and Ventilator-Associated Pneumonia (VAP) Prevention. Basics of Infection Prevention 2-Day Mini-Course 2016") Pneumonia (PNEU) and Ventilator-Associated Pneumonia (VAP) Prevention Basics of Infection Prevention 2-Day Mini-Course 2016 Objectives Differentiate long term care categories of respiratory infections
Pneumonia (PNEU) and Ventilator-Associated Pneumonia (VAP) Prevention Basics of Infection Prevention 2-Day Mini-Course 2016 Objectives Differentiate long term care categories of respiratory infections
Epidemiology of Infectious Complications of H1N1 Influenza Virus Infection
 Epidemiology of Infectious Complications of H1N1 Influenza Virus Infection Lyn Finelli, DrPH, MS Lead, Influenza Surveillance and Outbreak Response Epidemiology and Prevention Branch Influenza Division
Epidemiology of Infectious Complications of H1N1 Influenza Virus Infection Lyn Finelli, DrPH, MS Lead, Influenza Surveillance and Outbreak Response Epidemiology and Prevention Branch Influenza Division
Guidelines for workup of Throat and Genital Cultures
 Guidelines for workup of Throat and Genital Cultures 1 Acute Pharyngitis By far the most common infection of the upper respiratory tract Viral infection is by far the most common cause of pharyngitis The
Guidelines for workup of Throat and Genital Cultures 1 Acute Pharyngitis By far the most common infection of the upper respiratory tract Viral infection is by far the most common cause of pharyngitis The
Community Acquired Pneumonia. Abdullah Alharbi, MD, FCCP
 Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
PNEUMONIA. I. Background 6 th most common cause of death in U.S. Most common cause of infection related mortality
 Page 1 of 8 September 4, 2001 Donald P. Levine, M.D. University Health Center Suite 5C Office: 577-0348 dlevine@intmed.wayne.edu Assigned reading: pages 153-160; 553-563 PNEUMONIA the most widespread and
Page 1 of 8 September 4, 2001 Donald P. Levine, M.D. University Health Center Suite 5C Office: 577-0348 dlevine@intmed.wayne.edu Assigned reading: pages 153-160; 553-563 PNEUMONIA the most widespread and
The Chain of Infection
 The Chain of Infection As healthcare professionals, it is important to understand two facts about infection: 1.The various ways infection can be transmitted. 2. The ways the infection chain can be broken.
The Chain of Infection As healthcare professionals, it is important to understand two facts about infection: 1.The various ways infection can be transmitted. 2. The ways the infection chain can be broken.
320 MBIO Microbial Diagnosis. Aljawharah F. Alabbad Noorah A. Alkubaisi 2017
 320 MBIO Microbial Diagnosis Aljawharah F. Alabbad Noorah A. Alkubaisi 2017 Blood Culture What is a blood culture? A blood culture is a laboratory test in which blood is injected into bottles with culture
320 MBIO Microbial Diagnosis Aljawharah F. Alabbad Noorah A. Alkubaisi 2017 Blood Culture What is a blood culture? A blood culture is a laboratory test in which blood is injected into bottles with culture
Prospective Study of the Usefulness of Sputum Gram Stain in the Initial Approach to Community-Acquired Pneumonia Requiring Hospitalization
 869 Prospective Study of the Usefulness of Sputum Gram Stain in the Initial Approach to Community-Acquired Pneumonia Requiring Hospitalization Beatriz Rosón, Jordi Carratalà, Ricard Verdaguer, Jordi Dorca,
869 Prospective Study of the Usefulness of Sputum Gram Stain in the Initial Approach to Community-Acquired Pneumonia Requiring Hospitalization Beatriz Rosón, Jordi Carratalà, Ricard Verdaguer, Jordi Dorca,
INVESTIGATING: WOUND INFECTION
 INVESTIGATING: WOUND INFECTION Diagnosing infection in surgical and other wounds involves nurses being able to observe the clinical signs in a wound rather than simply obtaining positive microbiology results
INVESTIGATING: WOUND INFECTION Diagnosing infection in surgical and other wounds involves nurses being able to observe the clinical signs in a wound rather than simply obtaining positive microbiology results
Surveillance of Healthcare Associated Infections in Scottish Intensive Care Units
 Surveillance of Healthcare Associated Infections in Scottish Intensive Care Units Annual report of data from January 2010 to December 2010 Scottish Intensive Care Society Audit Group 1 Health Protection
Surveillance of Healthcare Associated Infections in Scottish Intensive Care Units Annual report of data from January 2010 to December 2010 Scottish Intensive Care Society Audit Group 1 Health Protection
CHOWDHURY MRA 1, AZAD KAK 2, HOSSAIN MZ 3, SARDAR MH 4, SIDDIQUI MR 5, SAAD S 6, RAHMAN MM 7
 ORIGINAL ARTICLES MICROBIAL ASPECT OF ASPIRATION PNEUMONIA IN PATIENTS WITH ALTERED CONSCIOUSNESS ADMITTED IN DHAKA MEDICAL COLLEGE HOSPITAL, BANGLADESH CHOWDHURY MRA 1, AZAD KAK 2, HOSSAIN MZ 3, SARDAR
ORIGINAL ARTICLES MICROBIAL ASPECT OF ASPIRATION PNEUMONIA IN PATIENTS WITH ALTERED CONSCIOUSNESS ADMITTED IN DHAKA MEDICAL COLLEGE HOSPITAL, BANGLADESH CHOWDHURY MRA 1, AZAD KAK 2, HOSSAIN MZ 3, SARDAR
MECHANISMS. Dr. WILLIAM J. BENJAMIN. Eye Physiology & Ocular Prosthetics Laboratory. School of Optometry
 OCULAR DEFENSE MECHANISMS Dr. WILLIAM J. BENJAMIN Eye Physiology & Ocular Prosthetics Laboratory University of Alabama at Birmingham School of Optometry Presented at the UAB School of Optometry as Part
OCULAR DEFENSE MECHANISMS Dr. WILLIAM J. BENJAMIN Eye Physiology & Ocular Prosthetics Laboratory University of Alabama at Birmingham School of Optometry Presented at the UAB School of Optometry as Part
Routine endotracheal cultures for the prediction of sepsis in ventilated babies
 Archives of Disease in Childhood, 1989, 64, 34-38 Routine endotracheal cultures for the prediction of sepsis in ventilated babies T A SLAGLE, E M BIFANO, J W WOLF, AND S J GROSS Department of Pediatrics,
Archives of Disease in Childhood, 1989, 64, 34-38 Routine endotracheal cultures for the prediction of sepsis in ventilated babies T A SLAGLE, E M BIFANO, J W WOLF, AND S J GROSS Department of Pediatrics,
Protocols for Laboratory Verification of Performance of the BioFire FilmArray Pneumonia Panel
 Protocols for Laboratory Verification of Performance of the BioFire FilmArray Pneumonia Panel Laboratory Protocols for Use with a ZeptoMetrix NATtrol Verification Panel Purpose The Clinical Laboratory
Protocols for Laboratory Verification of Performance of the BioFire FilmArray Pneumonia Panel Laboratory Protocols for Use with a ZeptoMetrix NATtrol Verification Panel Purpose The Clinical Laboratory
Diagnostic approach and microorganism resistance pattern in UTI Yeva Rosana, Anis Karuniawati, Yulia Rosa, Budiman Bela
 Diagnostic approach and microorganism resistance pattern in UTI Yeva Rosana, Anis Karuniawati, Yulia Rosa, Budiman Bela Microbiology Department Medical Faculty, University of Indonesia Urinary Tract Infection
Diagnostic approach and microorganism resistance pattern in UTI Yeva Rosana, Anis Karuniawati, Yulia Rosa, Budiman Bela Microbiology Department Medical Faculty, University of Indonesia Urinary Tract Infection
Cefotaxime Rationale for the EUCAST clinical breakpoints, version th September 2010
 Cefotaxime Rationale for the EUCAST clinical breakpoints, version 1.0 26 th September 2010 Foreword EUCAST The European Committee on Antimicrobial Susceptibility Testing (EUCAST) is organised by the European
Cefotaxime Rationale for the EUCAST clinical breakpoints, version 1.0 26 th September 2010 Foreword EUCAST The European Committee on Antimicrobial Susceptibility Testing (EUCAST) is organised by the European
Normal Flora. CLS 212: Medical Microbiology
 Normal Flora CLS 212: Medical Microbiology Relationships between Organisms Symbiosis Permanent association between two different organisms. Neutralism Two organisms living together, and neither is affected
Normal Flora CLS 212: Medical Microbiology Relationships between Organisms Symbiosis Permanent association between two different organisms. Neutralism Two organisms living together, and neither is affected
Microbiology products. Liofilchem Chromatic
 ET Microbiology products M IC R O PL A N www.liofilchem.net Liofilchem Chromatic c h ro m o g e n i c c u l t u re m e d i a LIOFILCHEM s.r.l. Via Scozia, Zona Industriale 64026 Roseto degli Abruzzi (Te)
ET Microbiology products M IC R O PL A N www.liofilchem.net Liofilchem Chromatic c h ro m o g e n i c c u l t u re m e d i a LIOFILCHEM s.r.l. Via Scozia, Zona Industriale 64026 Roseto degli Abruzzi (Te)
JMSCR Vol 04 Issue 12 Page December 2016
 www.jmscr.igmpublication.org Impact Factor 5.244 Index Copernicus Value: 83.27 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v4i12.124 COPD: Microbial Pattern in Acute Exacerbation
www.jmscr.igmpublication.org Impact Factor 5.244 Index Copernicus Value: 83.27 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v4i12.124 COPD: Microbial Pattern in Acute Exacerbation
EDUCATIONAL COMMENTARY - CLUE CELL MORPHOLOGY: DIAGNOSTIC CONSIDERATIONS
 EDUCATIONAL COMMENTARY - CLUE CELL MORPHOLOGY: DIAGNOSTIC CONSIDERATIONS Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE
EDUCATIONAL COMMENTARY - CLUE CELL MORPHOLOGY: DIAGNOSTIC CONSIDERATIONS Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE
EDUCATIONAL COMMENTARY THROAT CULTURES LEARNING OUTCOMES. Upon completion of this exercise, the participant should be able to:
 EDUCATIONAL COMMENTARY THROAT CULTURES LEARNING OUTCOMES Upon completion of this exercise, the participant should be able to: distinguish three types of hemolysis produced by bacterial colonies. discuss
EDUCATIONAL COMMENTARY THROAT CULTURES LEARNING OUTCOMES Upon completion of this exercise, the participant should be able to: distinguish three types of hemolysis produced by bacterial colonies. discuss
Received 30 March 2005; returned 16 June 2005; revised 8 September 2005; accepted 12 September 2005
 Journal of Antimicrobial Chemotherapy (2005) 56, 1047 1052 doi:10.1093/jac/dki362 Advance Access publication 20 October 2005 Evaluation of PPI-0903M (T91825), a novel cephalosporin: bactericidal activity,
Journal of Antimicrobial Chemotherapy (2005) 56, 1047 1052 doi:10.1093/jac/dki362 Advance Access publication 20 October 2005 Evaluation of PPI-0903M (T91825), a novel cephalosporin: bactericidal activity,
CONSIDERATIONS IN UTI DETECTION AND POTENTIAL IMPACT ON ANTIBIOTIC STEWARDSHIP
 CONSIDERATIONS IN UTI DETECTION AND POTENTIAL IMPACT ON ANTIBIOTIC STEWARDSHIP ERIN H. GRAF, PHD, D(ABMM) Director, Infectious Disease Diagnostics Laboratory Assistant Professor, Clinical Pathology and
CONSIDERATIONS IN UTI DETECTION AND POTENTIAL IMPACT ON ANTIBIOTIC STEWARDSHIP ERIN H. GRAF, PHD, D(ABMM) Director, Infectious Disease Diagnostics Laboratory Assistant Professor, Clinical Pathology and
SURVEILLANCE BLOODSTREAM INFECTIONS IN BELGIAN HOPITALS ( SEP ) RESULTS ANNUAL REPORT data
 RESULTS ANNUAL REPORT data") SURVEILLANCE BLOODSTREAM INFECTIONS IN BELGIAN HOPITALS ( SEP ) RESULTS ANNUAL REPORT data 2000-2014 SEP Workgroup Meeting 24 June 2015 Dr. Naïma Hammami Dr. Marie-Laurence Lambert naima.hammami@wiv-isp.be
SURVEILLANCE BLOODSTREAM INFECTIONS IN BELGIAN HOPITALS ( SEP ) RESULTS ANNUAL REPORT data 2000-2014 SEP Workgroup Meeting 24 June 2015 Dr. Naïma Hammami Dr. Marie-Laurence Lambert naima.hammami@wiv-isp.be
Lab 4. Blood Culture (Media) MIC AMAL-NORA-ALJAWHARA 1
 MIC AMAL-NORA-ALJAWHARA 1") Lab 4. Blood Culture (Media) 2018 320 MIC AMAL-NORA-ALJAWHARA 1 Blood Culture 2018 320 MIC AMAL-NORA-ALJAWHARA 2 What is a blood culture? A blood culture is a laboratory test in which blood is injected
Lab 4. Blood Culture (Media) 2018 320 MIC AMAL-NORA-ALJAWHARA 1 Blood Culture 2018 320 MIC AMAL-NORA-ALJAWHARA 2 What is a blood culture? A blood culture is a laboratory test in which blood is injected
Poor Predictive Ability of Urinalysis and Microscopic Examination to Detect Urinary Tract Infection
 Microbiology and Infectious Disease / POOR PREDICTIVE ABILITY OF URINALYSIS Poor Predictive Ability of Urinalysis and Microscopic Examination to Detect Urinary Tract Infection Joy D. Van Nostrand, MS,
Microbiology and Infectious Disease / POOR PREDICTIVE ABILITY OF URINALYSIS Poor Predictive Ability of Urinalysis and Microscopic Examination to Detect Urinary Tract Infection Joy D. Van Nostrand, MS,
Macroscopic Purulence, Leukocyte Counts, and Bacterial Morphotypes in Relation to Culture Findings for Sinus
 JOURNAL OF CLINICAL MICROBIOLOGY, OCt. 1988, p. 1926-1933 0095-1137/88/101926-08$02.00/0 Copyright 1988, American Society for Microbiology Vol. 26, No. 10 Macroscopic Purulence, Leukocyte Counts, and Bacterial
JOURNAL OF CLINICAL MICROBIOLOGY, OCt. 1988, p. 1926-1933 0095-1137/88/101926-08$02.00/0 Copyright 1988, American Society for Microbiology Vol. 26, No. 10 Macroscopic Purulence, Leukocyte Counts, and Bacterial
Airway Bacterial Concentrations and Exacerbations of Chronic Obstructive Pulmonary Disease
 Airway Bacterial Concentrations and Exacerbations of Chronic Obstructive Pulmonary Disease Sanjay Sethi 1,2, Rohin Sethi 2, Karen Eschberger 2, Phyllis Lobbins 3, Xueya Cai 4, Brydon J. B. Grant 1,2, and
Airway Bacterial Concentrations and Exacerbations of Chronic Obstructive Pulmonary Disease Sanjay Sethi 1,2, Rohin Sethi 2, Karen Eschberger 2, Phyllis Lobbins 3, Xueya Cai 4, Brydon J. B. Grant 1,2, and
Treatment of febrile neutropenia in patients with neoplasia
 Treatment of febrile neutropenia in patients with neoplasia George Samonis MD, PhD Medical Oncologist Infectious Diseases Specialist Professor of Medicine The University of Crete, Heraklion,, Crete, Greece
Treatment of febrile neutropenia in patients with neoplasia George Samonis MD, PhD Medical Oncologist Infectious Diseases Specialist Professor of Medicine The University of Crete, Heraklion,, Crete, Greece
Study of etiological factors and sensitivity pattern in CSOM
 Indian Journal of Basic and Applied Medical Research; December 2015: Vol.-5, Issue- 1, P. 766-770 766-771 Original article: Study of etiological factors and sensitivity pattern in CSOM Paresh Chavan, G
Indian Journal of Basic and Applied Medical Research; December 2015: Vol.-5, Issue- 1, P. 766-770 766-771 Original article: Study of etiological factors and sensitivity pattern in CSOM Paresh Chavan, G
MICROBIOLOGY SPECIMEN COLLECTION MANUAL
 Lee Memorial Health System Lee County, FL CLINICAL LABORATORY MICROBIOLOGY SPECIMEN COLLECTION MANUAL ACID FAST CULTURE Specimen Type see Specimen Chart ACID FAST STAIN see Specimen Chart Acid Fast stain
Lee Memorial Health System Lee County, FL CLINICAL LABORATORY MICROBIOLOGY SPECIMEN COLLECTION MANUAL ACID FAST CULTURE Specimen Type see Specimen Chart ACID FAST STAIN see Specimen Chart Acid Fast stain
Diagnostic Value of Sputum Gram s Stain and Sputum Culture in Lower Respiratory Tract Infections in a Tertiary Care Hospital
 International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 7 (2017) pp. 4310-4314 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.607.448
International Journal of Current Microbiology and Applied Sciences ISSN: 2319-7706 Volume 6 Number 7 (2017) pp. 4310-4314 Journal homepage: http://www.ijcmas.com Original Research Article https://doi.org/10.20546/ijcmas.2017.607.448
HOSPITAL INFECTION CONTROL
 HOSPITAL INFECTION CONTROL Objectives To be able to define hospital acquired infections discuss the sources and routes of transmission of infections in a hospital describe methods of prevention and control
HOSPITAL INFECTION CONTROL Objectives To be able to define hospital acquired infections discuss the sources and routes of transmission of infections in a hospital describe methods of prevention and control
Pneumonia Aetiology Why is it so difficult to distinguish pathogens from innocent bystanders?
 Pneumonia Aetiology Why is it so difficult to distinguish pathogens from innocent bystanders? David Murdoch Department of Pathology University of Otago, Christchurch Outline Background Diagnostic challenges
Pneumonia Aetiology Why is it so difficult to distinguish pathogens from innocent bystanders? David Murdoch Department of Pathology University of Otago, Christchurch Outline Background Diagnostic challenges
Pressure Injury Complications: Diagnostic Dilemmas
 Pressure Injury Complications: Diagnostic Dilemmas Aimée D. Garcia, MD, CWS, FACCWS Associate Professor, Department of Medicine, Geriatrics Section Baylor College of Medicine Medical Director, Wound Clinic
Pressure Injury Complications: Diagnostic Dilemmas Aimée D. Garcia, MD, CWS, FACCWS Associate Professor, Department of Medicine, Geriatrics Section Baylor College of Medicine Medical Director, Wound Clinic
Infective endocarditis
 Infective endocarditis Today's lecture is about infective endocarditis, the Dr started the lecture by asking what are the most common causative agents of infective endocarditis? 1-Group A streptococci
Infective endocarditis Today's lecture is about infective endocarditis, the Dr started the lecture by asking what are the most common causative agents of infective endocarditis? 1-Group A streptococci
Pneumonia Community-Acquired Healthcare-Associated
 Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
VITEK MS Implementation of Mass Spectrometry
 VITEK MS Implementation of Mass Spectrometry Willson Jang, Technical Leader wljang@providencehealth.bc.ca Microbiology & Virology Laboratory Providence Health Care St. Paul s Hospital October 23, 2013
VITEK MS Implementation of Mass Spectrometry Willson Jang, Technical Leader wljang@providencehealth.bc.ca Microbiology & Virology Laboratory Providence Health Care St. Paul s Hospital October 23, 2013
Pradeep Morar, MD; Zvoru Makura, MD; Andrew Jones, MD; Paul Baines, MD; Andrew Selby, MD; Julie Hughes, RGN; and Rick van Saene, MD
 Topical Antibiotics on Tracheostoma Prevents Exogenous Colonization and Infection of Lower Airways in Children* Pradeep Morar, MD; Zvoru Makura, MD; Andrew Jones, MD; Paul Baines, MD; Andrew Selby, MD;
Topical Antibiotics on Tracheostoma Prevents Exogenous Colonization and Infection of Lower Airways in Children* Pradeep Morar, MD; Zvoru Makura, MD; Andrew Jones, MD; Paul Baines, MD; Andrew Selby, MD;
Microbial Flora of Normal Human Body Dr. Kaya Süer. Near East University Medical Faculty Infectious Diseases and Clinical Microbiology
 Microbial Flora of Normal Human Body Dr. Kaya Süer Near East University Medical Faculty Infectious Diseases and Clinical Microbiology Normal Microbial Flora Skin Conjunctivae Oral Cavity Upper respiratory
Microbial Flora of Normal Human Body Dr. Kaya Süer Near East University Medical Faculty Infectious Diseases and Clinical Microbiology Normal Microbial Flora Skin Conjunctivae Oral Cavity Upper respiratory
Gram staining of protected pulmonary specimens in the early diagnosis of ventilator-associated pneumonia
 British Journal of Anaesthesia 85 (5): 735±9 (2000) Gram staining of protected pulmonary specimens in the early diagnosis of ventilator-associated pneumonia O. Mimoz *, A. Karim, J. X. Mazoit, A. Edouard,
British Journal of Anaesthesia 85 (5): 735±9 (2000) Gram staining of protected pulmonary specimens in the early diagnosis of ventilator-associated pneumonia O. Mimoz *, A. Karim, J. X. Mazoit, A. Edouard,
Isolation of Staphylococcus aureus from sputum in cystic fibrosis
 Journal of Clinical Pathology, 1978, 31, 913-918 Isolation of Staphylococcus aureus from sputum in cystic fibrosis P. D. SPARHAM, D. I. LOBBAN, AND D. C. E. SPELLER From the Bacteriology Department, Bristol
Journal of Clinical Pathology, 1978, 31, 913-918 Isolation of Staphylococcus aureus from sputum in cystic fibrosis P. D. SPARHAM, D. I. LOBBAN, AND D. C. E. SPELLER From the Bacteriology Department, Bristol