Briefing Document. FDA Pulmonary - Allergy Drugs Advisory Committee
|
|
|
- Solomon Jackson
- 5 years ago
- Views:
Transcription

1 FDA Advisory Committee Briefing Materials Page 1 of 157 Briefing Document FDA Pulmonary - Allergy Drugs Advisory Committee Ivacaftor for the Treatment of Cystic Fibrosis in Patients Age 6 Years and Older with an R117H-CFTR Mutation in the CFTR Gene NDA /S-014 Date of Document: 16 September 2014 AVAILABLE FOR PUBLIC DISCLOSURE WITHOUT REDACTION Sponsor: 50 Northern Avenue Boston, MA , USA
2 FDA Advisory Committee Briefing Materials Page 2 of 157 TABLE OF CONTENTS Table of Contents... 2 List of Tables... 5 List of Figures... 8 List of Abbreviations Executive Summary Introduction Scientific Background Cystic Fibrosis Diagnosis of Cystic Fibrosis Clinical Consequences Lung Disease Level of Chloride Transport and CF Disease Characteristics Treatments for Cystic Fibrosis R117H Mutation Prevalence Clinical Characteristics Complex Allele Ivacaftor Overview Mechanism of Action Overview of Clinical Development Program Results for Previously Studied Mutations Efficacy Safety R117H Mutation: In Vitro Data Regulatory History of R117H Development Program Overview of Clinical Studies in Patients with R117H Mutation Study Designs Study Entry Criteria Study Objectives and Endpoints Data Monitoring Committee Stopping of Study Statistical Methods Study Sample Size Datasets Analyzed Statistical Tests Primary Efficacy Variable (Percent Predicted FEV 1 ) Complete Case Set Analyses Multiplicity Adjustment Subgroup Analyses Ad Hoc Analyses Study Study Population and Efficacy Results Study
3 FDA Advisory Committee Briefing Materials Page 3 of Patient Disposition Demographic and Baseline Characteristics Pharmacokinetics Efficacy: Full Analysis Set Primary Efficacy Endpoint Secondary Efficacy Endpoints Tertiary Efficacy Endpoints Efficacy: Full Analysis Set Subgroups Overview of Subgroup Results Subgroup Baseline Characteristics Patients 18 Years of Age Patients 12 to 17 Years of Age Patients 6 to 11 Years of Age Study Patient Disposition Demographics and Baseline Characteristics Efficacy Full Analysis Set Patients 18 Years of Age Patients 12 to 17 Years of Age Patients 6 to 11 Years of Age Safety Study Summary of Adverse Events Common Adverse Events Common Adverse Events in Safety Set Common Adverse Events by Age Subgroups Adverse Events by Severity Deaths, Other Serious Adverse Events, and Adverse Events Leading to Discontinuation of Study Drug Laboratory Evaluations, Vital Signs, and Other Safety Evaluations Liver-Related Parameters Electrocardiogram Data Safety in Special Populations and Situations Study Post-Marketing Pharmacovigilance Activities Benefits and Risks References Appendices Kalydeco USPI CFQ-R Supplemental Tables and Figures Comparison of Entry Criteria: Studies 102, 103, 111, and Demographic and Baseline Characteristics Concomitant Medications Efficacy Results
4 FDA Advisory Committee Briefing Materials Page 4 of Study 110 Primary Endpoint: Sensitivity Analyses Study 110: Figure of Time to First Pulmonary Exacerbation, FAS Study 110: Tabular Summary of Change from Baseline and Treatment Difference, FAS and Subgroups Study 110: Changes in Inflammatory Mediator Concentrations, FAS Study
5 FDA Advisory Committee Briefing Materials Page 5 of 157 List of Tables Table 1 Efficacy Endpoint Results, Full Analysis Set Table 2 Study 110: Baseline Characteristics; Full Analysis Set and Age Subgroups. 19 Table 3 Study 110: Efficacy Endpoint Results, Full Analysis Set, Patients 18 Years of Age Table 4 Study 110: Pulmonary Exacerbation Incidence and Event Rates; Patients 18 Years of Age Table 5 Study 112: Absolute Change in Percent Predicted FEV 1 from Study 112 Baseline to Week 12, Full Analysis Set, 18 Years of Age Table 6 Study 110: Efficacy Endpoint Results, Full Analysis Set, Patients 6 to 11 Years of Age Table 7 Study 112: Absolute Change from Baseline (At the End of Washout) to Week 12 in Percent Predicted FEV 1, Full Analysis Set, Patients 6 to 11 Years of Age Table 8 Study 110: Summary of Adverse Event Incidence, Safety Set Table 9 Drugs Commonly Used for Patients With Cystic Fibrosis (Antimicrobials Excluded) Table 10 Baseline Characteristics of Patients in Studies of Ivacaftor in Different Populations (G551D, Non-G551D Severe Gating, F508del Homozygous) Table 11 Pulmonary and Extrapulmonary Endpoints: Treatment Difference (Ivacaftor vs Placebo) for Different Patient Populations (G551D, Non-G551D Severe Gating, F508del Homozygous) Table 12 Incidence of Most Common Adverse Events in All Patients; 48-Week, Placebo-Controlled, Phase 3 Studies in Patients Age 6 Years and Older With G551D Mutation Table 13 Incidence of Most Common Adverse Events by Age; 48-Week, Placebo-Controlled, Phase 3 Studies in Patients Age 6 Years and Older With G551D Mutation Table 14 Overview of Adverse Events by Age; 48-Week, Placebo-Controlled, Phase 3 Studies in Patients Age 6 Years and Older With G551D Mutation Table 15 Most Common Serious Adverse Events by Age; 48-Week, Placebo-Controlled, Phase 3 Studies in Patients Age 6 Years and Older With G551D Mutation Table 16 Incidence of Transaminase Elevations: Placebo-Controlled, Phase 3 Studies in Patients Age 6 Years and Older With G551D Mutation and Phase 2 Study in Patients Age 12 Years and Older Homozygous for F508del Mutation Table 17 Channel Gating Activity, Single Channel Conductance, and Total Chloride Transport With and Without Ivacaftor in Cells Expressing G551D-CFTR or R117H-CFTR Table 18 Studies 110 and 112: Key Aspects of Study Designs Table 19 Principal Entry Criteria of Study Table 20 Studies 110 and 112: Objectives and Prespecified Primary and Secondary Endpoints Table 21 Study 110: Demographics and Baseline Characteristics, Full Analysis Set... 72
6 FDA Advisory Committee Briefing Materials Page 6 of 157 Table 22 Study 110: Absolute Change From Baseline in Percent Predicted FEV 1 by MMRM, Full Analysis Set Table 23 Study 110: Secondary Efficacy Endpoints; Full Analysis Set Table 24 Study 110: Absolute Change in FEV 1 (L); Full Analysis Set Table 25 Study 110: Baseline Characteristics; FAS, Age Subgroup, Poly-T Variant Subgroup Table 26 Study 110: Baseline Disease Characteristics, Age Subgroups Table 27 Study 110: Efficacy Endpoint Results; Patients 18 Years of Age Table 28 Study 110: Absolute Change in FEV 1 (L); Patients 18 Years of Age Table 29 Study 110: Pulmonary Exacerbation Incidence and Event Rates; Patients 18 Years of Age Table 30 Study 110: Efficacy Endpoint Results; Patients 6 to 11 Years of Age Table 31 Study 110: Absolute Change in FEV 1 (L); Patients 6 to 11 Years of Age Table 32 Study 110: Percent Predicted FEV 1 Values at Screening, Day 1, and Week 24; Full Analysis Set, Patients 6 to 11 Years of Age (Inclusive) Table 33 Study 110: Absolute Change From Screening in Percent Predicted FEV 1 by MMRM; Full Analysis Set, Patients 6 to 11 Years of Age Table 34 Study 112: Absolute Change from Baseline to Week 2 and Week 12 in Percent Predicted FEV 1, Full Analysis Set Table 35 Study 112: Results for Efficacy Endpoints: Mean (SD) Changes from Study 112 Baseline, Full Analysis Set Table 36 Study 112: Absolute Change in Percent Predicted FEV 1 from Study 112 Baseline; Full Analysis Set, 18 Years of Age Table 37 Study 112: Results for Efficacy Endpoints: Mean (SD) Changes from Study 112 Baseline, Full Analysis Set, Patients 18 Years of Age Table 38 Study 112: Efficacy Results; Patient in 12 to 17 Year Old Age Group Table 39 Study 112: Absolute Change from Study 112 Baseline in Percent Predicted FEV 1, Full Analysis Set, Patients 6 to 11 Years of Age Table 40 Study 112: Results for Efficacy Endpoints: Mean (SD) Changes from Study 112 Baseline, Full Analysis Set, 6 to 11 Years of Age Table 41 Study 110: Summary of Adverse Event Incidence, Safety Set Table 42 Table 43 Study 110: Adverse Events Occurring in At Least 10% of Patients in Either Treatment Group by System Organ Class and Preferred Term, Safety Set Study 110: Adverse Events Occurring in At Least 15% of Patients in Either Treatment Group by System Organ Class, Preferred Term, and Age Subgroups, Safety Set Table 44 Study 110: Adverse Events Reviewed for Association with FEV 1 Changes in Patients Age 6 to 11 Years Table 45 Study 110: Serious Adverse Events; Safety Set and Age Subgroups Table 46 Study 110: Maximum On-Treatment Liver Function Test Results, Safety Set Table 47 Study 112: Serious Adverse Events Table Principal Inclusion Criteria and Enrollment of Patients with Cystic Fibrosis in Phase 3 Placebo-controlled Studies of Ivacaftor Table Study 112: Demographics and Baseline Characteristics, Full Analysis Set. 144
7 FDA Advisory Committee Briefing Materials Page 7 of 157 Table Study 110: Concomitant Medications Received by At Least 15% of Patients in Any Treatment Group, Full Analysis Set Table Study 110: Absolute Change From Baseline in Percent Predicted FEV 1, Sensitivity Analysis, Full Analysis Set Table Study 110: Percent Predicted FEV 1 ; Absolute Change from Baseline and Treatment Difference; Full Analysis Set and Subgroups Table Study 110: Sweat Chloride (mmol/l); Change From Baseline; Full Analysis Set and Subgroups Table Study 110: CFQ-R Respiratory Domain Score (Points); Absolute Change from Baseline; Full Analysis Set and Subgroups Table Study 110: Absolute Change From Baseline in Inflammatory Mediator and Log-Transformed Inflammatory Mediator Concentrations by MMRM, Full Analysis Set
8 FDA Advisory Committee Briefing Materials Page 8 of 157 List of Figures Figure 1 Studies 110 and 112: Schematic of Study Designs Figure 2 Study 110: Absolute Change from Baseline in Percent Predicted FEV 1 ; Patients 18 Years of Age Figure 3 Studies 110 and 112: Absolute Change from Baseline in Percent Predicted Figure 4 FEV 1 ; Patients 18 Years of Age Studies 110 and 112: Absolute Change from Baseline in Percent Predicted FEV 1 ; Patients 6 to 11 Years of Age Figure 5 Pathophysiologic Cascade of CF Disease Figure 6 Clinical Manifestations of CF Occur Throughout the Body Figure 7 Lung Disease is Progressive in People with CF Figure 8 CFTR Chloride Transport is Determined by CFTR Quantity and CFTR Function Figure 9 Level of CFTR Dysfunction Relates to Disease Phenotype Figure 10 Current Therapies Target the Downstream Manifestations of CF Figure 11 Comparison of F508del Homozygous and R117H Phenotype Figure 12 Prevalence of Lung Disease with Normal Percent Predicted FEV 1 and Percent Predicted FEV 1 in Different Age Groups of Patients in the US with the R117H Mutation Figure 13 Percent Predicted FEV 1 by Age Cohorts for CF Patients in US With an R117H-CFTR Mutation Figure 14 Percent Predicted FEV 1 <90% and 90%, by Age Cohort, for CF Patients in US With an R117H-CFTR Mutation Figure 15 Ivacaftor Mechanism of Action Figure 16 Effect of Ivacaftor on Channel Gating Activity of G551D-CFTR Figure 17 Study 102 (Trial 1) and Study 103 (Trial 2): Mean Absolute Change from Baseline in Percent Predicted FEV 1 in Patients With the G551D-CFTR Mutation Figure 18 Studies 110 and 112: Schematic of Study Designs Figure 19 Study 110: Patient Disposition Figure 20 Ivacaftor Exposure (C min ) by Age for Patient With the R117H Mutation (Study 110) or With CFTR Mutations That Cause Severe Gating Defects (Studies 102, 103, and 111) Figure 21 Figure 22 Figure 23 Figure 24 Figure 25 Study 110: Absolute Change in Percent Predicted FEV 1, Sweat Chloride, Rate of change in BMI, and CFQ-R Respiratory Domain Score; Full Analysis Set Study 110: Absolute Change in Percent Predicted FEV 1 from Baseline Through Week 24, by MMRM; FAS Subgroups Study 110: Absolute Change in Sweat Chloride from Baseline Through Week 24; FAS Subgroups Study 110: Absolute Change in Percent Predicted FEV 1 ; Patients 18 Years of Age Study 110: Absolute Change in CFQ-R Respiratory Domain Score; Patients 18 Years of Age... 87
9 FDA Advisory Committee Briefing Materials Page 9 of 157 Figure 26 Study 110: Treatment Difference in Mean Absolute Change from Baseline in Percent Predicted FEV 1 Through Week 24 by Subpopulations, Full Analysis Set, Patients 18 Years of Age Figure 27 Study 110: Waterfall Plot of Absolute Change from Baseline at Week 24 in Percent Predicted FEV 1 for Patients 18 Years of Age Receiving Ivacaftor: R117H-5T Versus R117H-7T Figure 28 Study 110: Waterfall Plot of Absolute Change from Baseline at Week 24 in Percent Predicted FEV 1 for Patients 18 Years of Age With R117H-7T Figure 29 Study 110: Absolute Change From Baseline in Percent Predicted FEV 1 and CFQ-R Respiratory Domain Score; Patients 6 to 11 Years Figure 30 Study 110: Individual Patient Results for Absolute Change from Baseline in Percent Predicted FEV 1 ; Full Analysis Set, Patients 6 to 11 Years of Age Figure 31 Study 110: Individual Patient Results for Percent Predicted FEV 1 at Screening, Run-In, and Baseline; Patients 6 to 11 Years of Age Figure 32 Study 112 Ivacaftor Arm: Patient Disposition Through Week Figure 33 Study 110 and 112: Absolute Change in Percent Predicted FEV 1, FAS Figure 34 Studies 110 and 112: Absolute Change in Percent Predicted FEV 1 and CFQ-R Respiratory Domain Score, Patients 18 Years of Age Figure 35 Studies 110 and 112: Absolute Change in Percent Predicted FEV 1, Patients 6 to 11 Years of Age Figure 36 Studies 110 and 112: Individual Patient Results for Percent Predicted FEV 1 ; Patients 6 to 11 Years of Age Figure 13-1 Study 110: Time to First Pulmonary Exacerbation, Full Analysis Set Figure 13-2 Figure 13-3 Study 112: Waterfall Plot of Absolute Change From Baseline in Percent Predicted FEV 1 at Week 12 by Treatment in Study 112, Full Analysis Set, 18 Years of Age Study 110 and Study 112: Mean (±SE) Absolute Change from Baseline in Percent Predicted FEV1 (%) by Visit; Full Analysis Set, 6 to 11 Year Subgroup Excluding Patient with Pulmonary Exacerbation
10 FDA Advisory Committee Briefing Materials Page 10 of 157 LIST OF ABBREVIATIONS Abbreviation AE ALT AST ATP BMI CCS CF CFF CFTR CFTR CFQ-R CI CL/F C min ECG EU FDA F508del FAS FEV 1 FRT G178R G551D or G551D- CFTR G551D or G551D- CFTR G551S G970R G1244E G1349D HBE HRCT LFT LS MCID MedDRA MMRM P aeruginosa PK Term adverse event alanine aminotransferase aspartate aminotransferase adenosine triphosphate body mass index complete case set cystic fibrosis Cystic Fibrosis Foundation (US) cystic fibrosis transmembrane conductance regulator (gene) cystic fibrosis transmembrane conductance regulator (protein) Cystic Fibrosis Questionnaire-Revised confidence interval apparent (oral) clearance minimum observed concentration Electrocardiogram European Union Food and Drug Administration CFTR mutation with an in-frame deletion of a phenylalanine codon corresponding to position 508 of the wild-type protein full analysis set forced expiratory volume in 1 second Fischer rat thyroid CFTR missense mutation that results in the replacement of a glycine residue at position 178 of CFTR with an arginine residue CFTR missense mutation that results in the replacement of a glycine residue at position 551 of CFTR with an aspartic acid residue CFTR protein with a replacement of a glycine residue at position 551 with an aspartic acid residue CFTR missense mutation that results in the replacement of a glycine residue at position 551 of CFTR with a serine residue CFTR missense mutation that results in the replacement of a glycine residue at position 970 of CFTR with an arginine residue CFTR missense mutation that results in the replacement of a glycine residue at position 1244 of CFTR with a glutamic acid residue CFTR missense mutation that results in the replacement of a glycine residue at position 1349 of CFTR with an aspartic acid residue human bronchial epithelial high-resolution computed tomography liver function test least squares minimal clinically important difference Medical Dictionary for Regulatory Activities mixed-effects model for repeated measures Pseudomonas aeruginosa pharmacokinetic, pharmacokinetics
11 FDA Advisory Committee Briefing Materials Page 11 of 157 Abbreviation Term PKA protein kinase A PT preferred term q12h every 12 hours R117H a missense mutation that results in the replacement of an arginine residue at position 117 of CFTR with a histidine residue R117H or R117H- CFTR CFTR protein with the replacement of an arginine residue normally found at position 117 of the wild-type protein with a histidine residue R117H-5T CFTR allele with an R117H mutation and a 5T poly-t variant R117H-7T CFTR allele with an R117H mutation and a 7T poly-t variant S549N CFTR missense mutation that results in the replacement of a serine residue at position 549 of CFTR with an asparagine residue S549R CFTR missense mutation that results in the replacement of a serine residue at position 549 of CFTR with an arginine residue S1251N CFTR missense mutation that results in the replacement of a serine residue at position 1251 of CFTR with an asparagine residue S1255P CFTR missense mutation that results in the replacement of a serine residue at position 1255 of CFTR with a proline residue SAE serious adverse event SD standard deviation SE standard error of the mean snda supplemental New Drug Application SOC system organ class ULN upper limit of normal URTI upper respiratory tract infection US United States USPI US Prescribing Information
12 FDA Advisory Committee Briefing Materials Page 12 of EXECUTIVE SUMMARY Indication for KALYDECO (Ivacaftor) KALYDECO (ivacaftor) is a cystic fibrosis transmembrane conductance regulator (CFTR) potentiator. KALYDECO is the first medicine that treats the underlying cause of cystic fibrosis (CF). KALYDECO is currently approved in the US for the treatment of CF in patients age 6 years and older who have one of the following mutations in the CFTR gene: G551D, G1244E, G1349D, G178R, G551S, S1251N, S1255P, S549N, or S549R. Vertex submitted a supplemental New Drug Application (snda) for the approval of KALYDECO for the treatment of cystic fibrosis (CF) in patients age 6 years and older who have an R117H mutation in the CFTR gene. In the US, approximately 500 people with CF have the R117H mutation and are age 6 years or older. The current USPI is provided in Appendix CF is a progressive, life-threatening disease that affects approximately 30,000 people in the US. CF is caused by defective or missing CFTR protein that results from mutations in the CFTR gene. The CFTR protein is an epithelial chloride channel that aids in regulating salt and water absorption and secretion in multiple organs, including lungs, pancreas, and sweat glands. Decreased CFTR chloride transport results in the multisystem pathology associated with CF. Lung disease is the primary cause of morbidity and mortality in people with CF. 1,2 Destructive cycles of inflammation, recurrent chronic infection, and irreversible lung damage are characteristic of CF, and start to occur before measurable decreases in lung function (percent predicted FEV 1 ) are apparent. Lung disease leads to a progressive loss of lung function that ultimately results in respiratory failure. It is important to appreciate that CF patients with normal FEV 1 often have significant irreversible lung disease. 38,39,40,41 Section 3 provides additional information about CF. The rate of CF disease progression generally correlates with the extent of loss of CFTR chloride transport. The amount of chloride transported by the CFTR protein is a function of the quantity of CFTR protein at the cell surface, the channel gating of the CFTR protein (the amount of time the CFTR protein channel is open and can transport chloride), and the channel conductance of the CFTR protein (rate at which chloride passes through the open channel). The mutations that cause CF result in decreased quantity and/or function of the CFTR protein. 3,4,5 A complete or near complete loss of CFTR chloride transport referred to as minimal function of CFTR results in CF characterized by an early onset and relatively rapid disease progression. Examples of mutations that result in minimal CFTR function are F508del and the mutations for which ivacaftor is currently approved (e.g., G551D). A less complete loss of CFTR-mediated chloride transport referred to as residual function of CFTR often results in CF that is more slowly progressive but reaches a severe disease stage and causes premature death. R117H is a mutation that results in residual CFTR function. A
13 FDA Advisory Committee Briefing Materials Page 13 of 157 study of patients enrolled in the CFF registry between 1996 and 2002 found a median age of death of 24 years for patients with mutations that result in minimal CFTR function and 38 years for patients who have a CFTR mutation that results in residual CFTR function. 65 People with CF who have the R117H mutation are a small subset of the CF population with a significant unmet medical need. The R117H mutation is present in about 700 CF patients in the US, including about 500 people age 6 years of age older. 1,6 The R117H mutation has variable penetrance: people with the R117H mutation have a heterogeneous clinical presentation and progression, ranging from asymptomatic to CF The clinical consequences of R117H are influenced by the length of the poly-thymidine (poly-t) tract, another region of the CFTR gene, that is on the same allele (in cis) as the R117H mutation. The poly-t tract can occur as 1 of 3 variants (5T, 7T, or 9T). The lower the number of thymidine repeats, the less functional CFTR protein that is synthesized. 11 R117H-5T will likely cause disease, R117H-7T is less likely to cause disease, and R117H-9T is highly unlikely to cause disease. 7,8 Heterogeneity of clinical presentation also exists within the R117H-5T and R117H-7T populations, due to factors such as inter-patient variability in the effect of a given poly-t variant on the amount of functional CFTR protein synthesized Although R117H-7T is less likely than R117H-5T to cause disease, some people with R117H-7T develop CF. 8,14 While R117H with the 5T or 7T polymorphism is often associated with a slower progression of clinical symptoms relative to the mutations for which ivacaftor is currently approved, patients with the R117H mutation who develop CF have progressive disease, with premature mortality and considerable morbidity. Data from patients included in the US CFF Registry show a progressive loss of lung function (percent predicted FEV 1 ) in people with the R117H mutation, and evidence of lung disease that may be present before measurable decreases in lung function. 6 Section 4 provides additional information about the clinical characteristics of patients with the R117H mutation and the R117H mutation and poly-t tract. Ivacaftor is the only approved treatment that targets the underlying cause of CF. Ivacaftor, an orally bioavailable small molecule, is a first-in-class therapy and the only approved treatment that targets the underlying cause of CF the dysfunctional CFTR protein. Ivacaftor increases CFTR chloride transport by potentiating the channel open probability (gating) of the CFTR protein at the cell surface. Other treatments for CF target the downstream consequences of diminished CFTR function, such as lung disease or pancreatic insufficiency. There is no cure for CF. In the US, ivacaftor has orphan drug, fast track, and breakthrough therapy designations. The effectiveness and safety of ivacaftor has been established in people with CF who have other CFTR mutations that cause defects in CFTR channel gating. The CFTR mutations for which ivacaftor is currently approved cause defects in channel gating that result in minimal CFTR function. The clinical development program for ivacaftor initially focused on the G551D mutation, the most prevalent of these mutations. In vitro,
14 FDA Advisory Committee Briefing Materials Page 14 of 157 ivacaftor increased the open probability of G551D-CFTR and increased chloride transport in human bronchial epithelial cells derived from people with the G551D mutation. In vitro to in vivo translation was demonstrated: in patients age 6 years and older with the G551D mutation, ivacaftor increased CFTR chloride transport, as evidenced by decreases in sweat chloride concentration during ivacaftor treatment. This pharmacodynamic effect translated into clinical benefit in adults, adolescents, and children 6 to 11 years of age. In patients with the G551D mutation, the treatment effect for absolute change in percent predicted FEV 1 through Week 24 (the primary endpoint) was 10.6 percentage points (P <0.0001) in patients 12 years of age and 12.5 percentage points (P <0.0001) in patients 6 to 11 years of age. Ivacaftor treatment also resulted in substantial and sustained clinical benefit in other pulmonary endpoints and in extrapulmonary endpoints, including measures of nutritional status (weight, body mass index). Translation of in vitro to in vivo results was also demonstrated for the other 8 CFTR mutations for which ivacaftor is approved in the US. The safety profile of ivacaftor is based on data from more than 1100 patients age 6 years and older who were treated with ivacaftor for up to 3 years in clinical trials and on post-marketing data for more than 2000 patients age 6 years and older, accounting for more than 1,045,000 person-days of post-marketing exposure. Of the patients with post-marketing exposure, approximately 390 are age 6 to 11 years, accounting for more than 197,000 person-days. The safety profile, which has remained consistent with long-term use, appears similar between children and adults and between patients with different CFTR mutations. In placebo-controlled studies in patients with the G551D mutation, the incidence of serious adverse events (SAEs) was lower in patients treated with ivacaftor than in patients treated with placebo. In 48-week, placebo-controlled studies in patients with the G551D mutation, the most common adverse events (AEs) that had a higher incidence in ivacaftor-treated patients than in placebo-treated patients were headache, oropharyngeal pain, upper respiratory tract infection, nasal congestion, abdominal pain, nasopharyngitis, diarrhea, rash, nausea, and dizziness. 15 For the approval of ivacaftor for treatment of CF in patients with the G551D mutation, separate placebo-controlled studies were conducted for patients 6 to 11 years of age (52 patients) and patients >12 years of age (161 patients). The other mutations currently approved for ivacaftor treatment in the US have a lower prevalence than G551D and were evaluated in a single placebo-controlled study in 39 patients aged 6 years and older. (In the US, about 1100 people with CF age 6 years or older have the G551D mutation or one of the other CFTR mutations for which ivacaftor is currently approved in the US.) Analyses of data from patients with the G551D mutation treated with ivacaftor for up to 144 weeks in clinical trials confirmed the favorable safety profile of ivacaftor and demonstrated that the benefits on endpoints such as FEV 1, weight/bmi, respiratory symptoms, and pulmonary exacerbation were sustained. 16 In addition, the annualized rate of decline in percent predicted FEV 1 was lower for these patients (-0.81 ± 0.36) than for a homozygous F508del control population from the US CFF registry (-1.73 ± 0.17). 17 Data from the US CF Foundation GOAL study (G551D Observational Study), which assessed the impact of ivacaftor post-approval, showed comparable benefits on many of the endpoints assessed in the pivotal trials and a pre-to-post treatment reduction in hospitalization rates from 27% to 8% (P<0.001) and a reduction in P aeruginosa positive culture rates from 52% to 34% (P<0.001) during a 6-month period. 18
15 FDA Advisory Committee Briefing Materials Page 15 of 157 Further information about ivacaftor results for previously studied mutations is provided in Section 5.4 and in the USPI in Appendix The mechanism of action of ivacaftor for R117H-CFTR is the same as that proven to be clinically effective for G551D-CFTR and other mutations approved for ivacaftor treatment. The R117H mutation results in CFTR protein with a gating defect (decreased open probability) and a conductance defect (decreased current amplitude). The gating defect is the dominant defect: R117H-CFTR has 22% of normal CFTR open probability and 88% of normal CFTR current amplitude. The R117H-CFTR gating defect is less severe than the G551D-CFTR gating defect (3% of normal CFTR open probability). As described above, the clinical consequences of the R117H mutation are influenced by another region of the CFTR gene (the poly-t tract), which affects the amount of functional CFTR protein produced. The combined effect of the gating defect (leading to lower open probability) and the reduction in the amount of functional CFTR protein produced leads to the loss of chloride transport that can result in CF lung disease in R117H patients. In vitro, ivacaftor increased R117H-CFTR channel gating activity, as measured by an increase in the channel open probability. The increase in open probability resulted in an increase in chloride transport: in human bronchial epithelial cells derived from people with the R117H-5T/F508del genotype, ivacaftor increased chloride transport from 26% of normal CFTR to 38% of normal CFTR. See Section 6 for further details about in vitro results. The clinical program for people with the R117H mutation was designed to assess the efficacy and safety of ivacaftor in this small patient population. The efficacy and safety of ivacaftor in patients with the R117H mutation was evaluated in Study 110, a double-blind, placebo-controlled study, and Study 112, an ongoing, open-label, rollover study in which Study 110 patients could enroll after participating in Study 110 (Figure 1). Final results are available from Study 110. Interim analysis results are available from Study 112 (efficacy results through Week 12, and SAE data from the pharmacovigilance database). Both studies were conducted in the US and in the European Union (EU). Figure 1 Studies 110 and 112: Schematic of Study Designs
16 FDA Advisory Committee Briefing Materials Page 16 of 157 Both studies used an ivacaftor dosage of 150 mg every 12 hours, which is the recommended dosage in the KALYDECO USPI. Study drug treatment was in addition to the patient s usual prescribed CF therapy. Study 110 Study 110 enrolled patients 6 years of age and older who had an R117H mutation on at least one allele, a confirmed diagnosis of CF (chronic sinopulmonary disease and sweat chloride 60 mmol/l or 2 CF-causing mutations), and percent predicted FEV 1 of 40% to 105% (patients 6 to 11 years of age) and 40% to 90% (patients 12 years of age and older). The upper limit of percent predicted FEV 1 was higher for patients 6 to 11 years of age than for patients 12 years of age and older to aid in the recruitment of children. The Study 110 sample size a minimum of 40 to a maximum of 80 patients was primarily driven by feasibility considerations in this rare population. Randomization was stratified by age (6 to 11, 12 to 17, and 18 years) and percent predicted FEV 1 (<70%, 70% to 90%, and >90%), as these factors were anticipated to have an influence on the outcomes. The primary endpoint of Study 110 was the absolute change in percent predicted FEV 1 through Week 24. Secondary endpoints were changes in body mass index (BMI), sweat chloride concentrations, cystic fibrosis questionnaire-revised (CFQ-R) respiratory domain score, time to first pulmonary exacerbation, and safety. Efficacy analyses were prespecified to use the Full Analysis Set (FAS), defined as all randomized patients who received at least 1 dose of study drug. The primary analysis for the primary efficacy endpoint was based on a mixed effects model for repeated measures (MMRM). The model included absolute change from baseline in percent predicted FEV 1 as the dependent variable, treatment, visit (Weeks 2, 4, 8, 16, and 24), and treatment-by-visit interaction as fixed effects, and patient as a random effect, with adjustment for the continuous baseline values of age and percent predicted FEV 1. Prespecified subgroup analyses (without multiplicity adjustment) were conducted for baseline characteristics (age group, percent predicted FEV 1, geographic region, sex, P aeruginosa infection status, and poly-t variant). After enrollment at the high end of the prespecified range had been achieved, with a projection of at least 65 patients of the 40 to 80 planned to be randomized, Vertex made the decision to stop Study 110. This decision was based on a number of factors, including study feasibility and timelines. The rate of enrollment had slowed considerably despite multiple efforts to extend patient recruitment. Notably, 70 patients randomized in the study represents about 15% of the size of the US population of patients 6 years of age and older who have the R117H mutation. Eight patients were still enrolled in the study at the time of study closure, all of whom had received at least 2 weeks of study drug treatment, and all of whom enrolled in Study 112, the 2-year open-label study of ivacaftor. The MMRM analyses for Study110 included all available data from the study, including data for the 8 patients who did not complete the full 24 weeks of treatment in Study 110. A Complete Case Set analysis (excluding these 8 patients) yielded comparable results to the FAS.
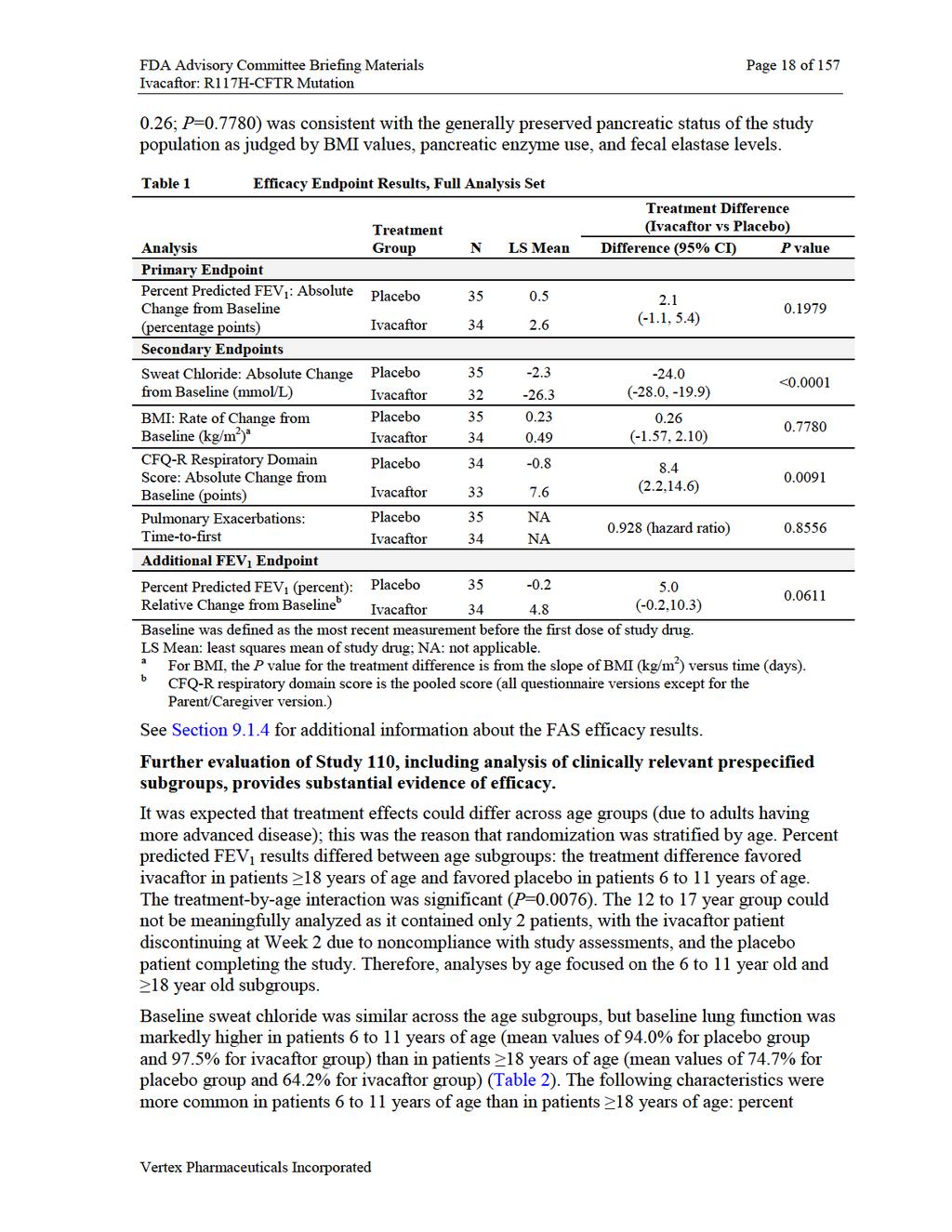
17 FDA Advisory Committee Briefing Materials Page 17 of 157 Study 112 An interim analysis of Study 112 was conducted to provide additional information about the effect of ivacaftor in patients with the R117H mutation following a washout period at the end of Study 110. While limited by its open-label design, Study 112 provides two sets of supportive data for ivacaftor treatment in patients with the R117H mutation: patients treated with ivacaftor in Study 110 (ivacaftor/ivacaftor group) patients treated with placebo in Study 110 (placebo/ivacaftor group) Summary statistics and ad hoc analyses were conducted to evaluate the change from baseline for percent predicted FEV 1, sweat chloride, and CFQ-R respiratory domain score. Because this was an open-label study, these endpoints were evaluated based on change from the Study 112 baseline within each group (all patients, patients treated with placebo in Study 110, and patients treated with ivacaftor in Study 110). See Section 8 for further information about the design and methods of analysis for the clinical studies in patients with the R117H mutation. The patients enrolled in Study 110 included a substantial portion of the available patient population. The Study 110 FAS included 69 patients; 59 of these patients completed 24 weeks of treatment, 8 patients were in the treatment period when the study was stopped, and 2 patients discontinued treatment (1 due to noncompliance, 1 due to pregnancy). At baseline, the 69 patients in Study 110 had a mean sweat chloride value of about 70 mmol/l and a mean percent predicted FEV 1 of 72.9% (range: 32.5% to 105.5%). The patients had well-preserved BMIs (mean overall: 23.8 kg/m 2 ), and a high proportion were pancreatic sufficient as judged by fecal elastase-1 measurements. Seventeen patients were 6 to 11 years of age, 2 were 12 to 17 years of age, and 50 were 18 years of age. Fifteen of the patients 6 to 11 years of age were in the US, representing 12.6% of the 119 of the CF patients in the US with the R117H mutation aged 6 to 11 years. Thirty-seven patients 18 years of age were in the US, representing 21.3% of the 173 patients in the US with the R117H mutation, had percent predicted FEV 1 <90%, and were age 18 years. Sixty-five of the Study 110 patients enrolled in the ivacaftor arm of Study 112. The population in Study 112 is therefore a representative group of the patients in Study 110. See Sections and for additional disposition and baseline data. Study 110 failed the primary endpoint. The treatment difference for the primary endpoint (absolute change in percent predicted FEV 1 from baseline through Week 24) for the FAS was 2.1 percentage points, which failed to reach statistical significance (95% CI: -1.1, 5.4; P=0.1979) (Table 1). Treatment differences favored ivacaftor at all treatment period time points. Substantial treatment differences in favor of ivacaftor were seen for the secondary endpoints of absolute change from baseline in sweat chloride concentrations and CFQ-R respiratory domain scores. The treatment difference for CFQ-R respiratory domain score was twice the minimal clinically important difference (4 points). The result for rate of change in BMI (treatment difference
18
19 FDA Advisory Committee Briefing Materials Page 19 of 157 predicted FEV 1 >90%; absence of Pseudomonas aeruginosa infection; poly-t variant 7T. Despite normal lung function as measured by percent predicted FEV 1, the Study 110 patients who were 6 to 11 years of age had medical histories that included CF lung disease. Table 2 Study 110: Baseline Characteristics; Full Analysis Set and Age Subgroups Age Treatment N Sweat Chloride (mmol/l) Mean (range) Percent Predicted FEV 1 (%) Mean (range) Number of Patients With Percent Predicted FEV 1 >90% n (%) BMI (kg/m 2 ) Mean (range) All (full Placebo (22.5 to 108.8) 70.2 (3.4, 102.8) 6 (17.1) (13.64, 37.83) analysis set) Ivacaftor ; N=32 (22.5, 120.0) 75.7 (32.5, 105.5) 7 (20.6) (14.37, 42.87) 18 years Placebo (35.5 to 102.3) 62.2 (37.4 to 85.8) (17.04 to 37.83) Ivacaftor , N=23 (23.3 to 120.0) 67.0 (32.5 to 92.6) 1 (4.2) (21.50 to 42.87) 12 to 17 Placebo years Ivacaftor to 11 years Placebo (22.5 to 108.8) 94.0 (80.0 to 102.8) 6 (75.0) (13.64 to 21.50) Ivacaftor , N=8 (33.0 to 100.5) 97.5 (84.1 to 105.5) 6 (66.7) (14.37 to 24.69) Efficacy results for patients 18 years of age and patients 6 to 11 years of age are summarized below. See Section for an overview of results for all subgroups, and Section for a summary of baseline characteristics of the subgroups. Efficacy results for adult patients, a clinically relevant subgroup that comprised 72.5% of the patients in Study 110, were positive and consistent. The clinical benefit of ivacaftor in patients 18 years of age was demonstrated by the clinically relevant treatment difference for absolute change in percent predicted FEV 1 (5 percentage points) and CFQ-R respiratory domain score. The treatment difference for CFQ-R respiratory domain score was more than 3 times the minimal clinically important difference (4 points). Sweat chloride showed a substantial treatment effect (-21.9 mmol/l).
20

 placebo patient 18 years of age had at least a 7.5 percentage point increase, compared to 33.3% of ivacaftor patients 18 years of age.")
21 FDA Advisory Committee Briefing Materials Page 21 of 157 Figure 2 Study 110: Absolute Change from Baseline in Percent Predicted FEV 1 ; Patients 18 Years of Age Data are observed means. Baseline was defined as the most recent measurement before the first dose of study drug. A responder analysis provides additional evidence of the ivacaftor treatment effect: 54.2% of ivacaftor patients 18 years of age had at least a 5 percentage point increase from baseline in percent predicted FEV 1, compared with 15.4% of placebo patients 18 years of age. Only 1 (3.8%) placebo patient 18 years of age had at least a 7.5 percentage point increase, compared to 33.3% of ivacaftor patients 18 years of age. Results for pulmonary exacerbations were supportive of efficacy: measures of pulmonary exacerbations, including markers for more clinically severe events, numerically favored ivacaftor (Table 4). Table 4 Study 110: Pulmonary Exacerbation Incidence and Event Rates; Patients 18 Years of Age Parameter Number of: Placebo (N=26) Ivacaftor (N=24) Duration in Study Days on study All pulmonary exacerbations Patients with events Events (event rate) 17 (0.748) 13 (0.556) Requiring hospitalization Patients with events 6 2 Events 7 2 Requiring IV antibiotic therapy Patients with events 6 2 Events 8 2 Pulmonary exacerbation includes events that met the protocol definition of pulmonary exacerbations (treatment with new or changed antibiotic therapy for 4 sinopulmonary signs/symptoms).
22 FDA Advisory Committee Briefing Materials Page 22 of 157 Interim analysis results from Study 112, an open-label rollover study, provide supportive evidence of the efficacy of ivacaftor in adults. Study 112 results for patients 18 years of age are closely comparable to results for this group of patients in Study 110. A clinically relevant and statistically significant treatment response for the absolute change in percent predicted FEV 1 occurred for both the placebo/ivacaftor and ivacaftor/ivacaftor groups. The absolute change from baseline for both groups was about 5 percentage points (Table 5), which is comparable to the treatment difference seen in Study 110 for patients 18 years of age. Table 5 Study 112: Absolute Change in Percent Predicted FEV 1 from Study 112 Baseline to Week 12, Full Analysis Set, 18 Years of Age Study Population N Mean Change from Baseline P Value a (Within Group) Overall < Placebo/Ivacaftor Ivacaftor/Ivacaftor Notes: Baseline was defined as the most recent measurement before intake of the first dose of study drug in Study 112. This measurement was taken at the Day 1 Visit for Study 112, which was also the Follow-up Visit of Study 110. Age is the baseline age in Study 110. a P values are based on the one-sample t-test. Figure 3 shows the absolute change from baseline in percent predicted FEV 1 for Studies 110 and 112, illustrating the on-off-on effect of ivacaftor treatment. In the ivacaftor/ivacaftor treatment group, percent predicted FEV 1 values increased during ivacaftor treatment in Study 110, decreased during the washout period, and increased when ivacaftor treatment was restarted in Study 112. Figure 3 also shows the increase in the placebo/ivacaftor group, which was comparable to that for the ivacaftor/ivacaftor group.
23 FDA Advisory Committee Briefing Materials Page 23 of 157 Figure 3 Studies 110 and 112: Absolute Change from Baseline in Percent Predicted FEV 1 ; Patients 18 Years of Age Note: Data are observed means; change from baseline for both studies was calculated as the change from the Study 110 baseline. The totality of data in the subgroup of patients 18 years of age, which comprised 72.5% of patients in Study 110, demonstrates the efficacy of ivacaftor in patients with the R117H mutation. Study 110 results for patients 18 years of age were replicated in Study 112. There is a good rationale for a difference in outcomes between age groups given that adults had more advanced lung disease at baseline. Additional information about efficacy results in patients 18 years of age is provided in Section (Study 110) and Section (Study 112). In the small subgroup of patients age 6 to 11 years old, the treatment difference for percent predicted FEV 1 favored placebo; however, based on further analyses, this does not represent a clinically relevant signal. In patients 6 to 11 years of age (8 patients treated with placebo and 9 patients treated with ivacaftor), the treatment difference for absolute change in percent predicted FEV 1 favored placebo (treatment difference: -6.3 percentage points; Table 6). The CFQ-R respiratory domain also favored placebo; however, there was no consistent trend in results across time points. Sweat chloride concentration showed a substantial treatment difference in favor of ivacaftor, consistent with the adult population.
24
 to Week 12 was 6.5 percentage points (P = 0.0806).")
25 FDA Advisory Committee Briefing Materials Page 25 of 157 Results from an interim analysis of Study 112 did not show a negative effect of ivacaftor on percent predicted FEV 1 in patients 6 to 11 years of age. In patients 6 to 11 years of age, the absolute change in percent predicted FEV 1 from the start of Study 112 (after washout) to Week 12 was 6.5 percentage points (P = ). Increases in percent predicted FEV 1 occurred in both the placebo/ivacaftor group and the ivacaftor/ivacaftor group. Table 7 Study 112: Absolute Change from Baseline (At the End of Washout) to Week 12 in Percent Predicted FEV 1, Full Analysis Set, Patients 6 to 11 Years of Age Study Population N Mean Change from Baseline P Value a (Within Group) Overall Placebo/Ivacaftor Ivacaftor/Ivacaftor Notes: Baseline was defined as the most recent measurement before intake of the first dose of study drug in Study 112. This measurement was taken at the Day 1 Visit for Study 112, which was also the Follow-up Visit of Study 110. Age is the baseline age in Study 110. a P values are based on the one-sample t-test. Figure 4 Studies 110 and 112: Absolute Change from Baseline in Percent Predicted FEV 1 ; Patients 6 to 11 Years of Age Note: Data are observed means; change from baseline for both studies was calculated as the change from the Study 110 baseline. See Section for further details about the Study 112 efficacy results in patients 6 to 11 years of age.
26 FDA Advisory Committee Briefing Materials Page 26 of 157 Different results in age subgroups were not due to pharmacokinetics or to lack of a pharmacodynamic effect. Ivacaftor exposure in patients in Study 110 was consistent with exposure in previous clinical trials in other CF populations (see Section 9.1.3). Baseline sweat chloride levels were similar for the age subgroup, and sweat chloride results showed consistent, substantial changes for all subgroups, indicating that the differences in FEV 1 response were not driven by a difference in effect on CFTR function. Ivacaftor s safety profile is favorable, consistent, and well established. Safety results in patients with the R117H mutation were comparable to those in patients age 6 years and older with other CFTR mutations who have been treated with ivacaftor for up to 3 years. Study 110 In Study 110, the incidence of AEs considered related to study drug, incidence of SAEs, and incidence of AEs leading to study drug interruption were lower in the ivacaftor group than the placebo group (Table 8). There were no deaths and no AEs that led to study drug discontinuation. Table 8 Study 110: Summary of Adverse Event Incidence, Safety Set Placebo (N = 35) n (%) Ivacaftor (N = 34) n (%) Patients With At least 1 AE 35 (100.0) 32 (94.1) At least 1 related AE 7 (20.0) 3 (8.8) At least 1 severe (grade 3) AE 5 (14.4) 1 (2.9) At least 1 AE leading to death 0 0 At least 1 SAE 6 (17.1) 4 (11.8) At least 1 related SAE 0 0 At least 1 AE leading to study drug interruption 2 (5.7) 1 (2.9) At least 1 AE leading to study drug withdrawal 0 0 Note: Related includes the categories possibly related to study drug and related to study drug. AEs for which the incidence was at least 5 percentage points higher with ivacaftor than placebo treatment were nasal congestion, oropharyngeal pain, abdominal pain, wheezing, upper airway cough syndrome, bacterial disease carrier, influenza-like illness, and abdominal discomfort. The most common SAE in both treatment groups was infective pulmonary exacerbation of CF (incidence of 8.8% in the ivacaftor group and 17.1% in the placebo group). All SAEs of infective pulmonary exacerbation of CF resolved without study drug discontinuation, and none were considered to be related to study drug. Results for clinical laboratory parameters (serum chemistry, hematology, coagulation studies), vital signs, physical examinations, and electrocardiograms (ECGs) showed minor differences between the ivacaftor and placebo groups that were not considered to be clinically meaningful. There were no clinically relevant differences in safety results between patients 6 to 11 years of age and patients 18 years of age.
27 FDA Advisory Committee Briefing Materials Page 27 of 157 Study 112 SAE data are available from ongoing Study 112; 8 of the 65 patients had an SAE, and the most common SAE was infective pulmonary exacerbation of CF. See Section 10 for further details about ivacaftor safety results in Studies 110 and 112. The totality of the evidence provides a positive benefit/risk assessment for patients with the R117H mutation and supports approval of ivacaftor for the treatment of CF in patients age 6 years and older who have an R117H mutation in the CFTR gene The R117H mutation is present in about 700 people with CF in the US, including about 500 people age 6 years and older. 1 No currently approved treatments are available to treat the underlying cause of disease in this patient population, in whom disease progresses with advancing age. The R117H patient population is challenging to study, given the rarity of the mutation and heterogeneity in clinical presentation and progression. The patients enrolled in Study 110 represented a substantial proportion of the R117H patient population in the US. Ivacaftor treatment increased CFTR chloride transport in patients with the R117H mutation, including all subgroups, as evidenced by substantial reductions in sweat chloride concentrations. The effect size was similar between the poly T variants (5T and 7T). This is consistent with ivacaftor s unique mechanism of action, which targets CFTR dysfunction the underlying cause of CF. This mechanism of action has been proven to be effective in people with other CFTR mutations that cause a defect in channel gating. Despite the failed primary endpoint in Study 110, a biologically understandable and clinically consistent pattern of results demonstrates that ivacaftor provided clinical benefit for patients 18 years of age and had a favorable safety profile for all patients studied. In patients 18 years of age with the R117H mutation, ivacaftor demonstrated consistent, clinically meaningful benefit: Ivacaftor treatment resulted in sustained, clinically significant increases in lung function (FEV 1 ) and CFQ-R respiratory domain score in Study 110. Measures of pulmonary exacerbations, including markers for more clinically severe events, favored ivacaftor in Study 110. Improvements in FEV 1 were reduced when ivacaftor treatment was withdrawn during a blinded washout period at the end of Study 110, and then were restored in Study 112 after reintroduction of ivacaftor treatment. Percent predicted FEV 1 results in Study 112 for patients 18 years of age were closely comparable to results in Study 110 for patients 18 years of age. The totality of data in this subgroup, which comprised 72.5% of the patients in Study 110, supports the efficacy of ivacaftor in patients with the R117H mutation. The safety experience in the R117H population was favorable and consistent with the well-established safety profile that is based on more than 1100 patients treated with ivacaftor in clinical trials and post-marketing exposure for more than 2000 patients. In R117H patients, no unique safety concerns were apparent, no adverse events resulted in discontinuation of
28 FDA Advisory Committee Briefing Materials Page 28 of 157 ivacaftor, and adverse events that were severe and/or serious were infrequent. Similar to the safety profile observed in placebo-controlled studies for the currently approved mutations, the incidence of SAEs in Study 110 was lower for ivacaftor treatment group than the placebo treatment group. Across all sources, the most common adverse events involve the respiratory, infectious, gastrointestinal, or nervous systems. Ivacaftor for the treatment of CF in patients age 6 years and older with the R117H mutation meets the regulatory criteria for extrapolation of efficacy from adult patients to pediatric patients. Therefore, extrapolation of efficacy to children is appropriate. The disease process is similar, and there were comparable exposures and safety profiles in pediatric and adult patients. Ivacaftor was pharmacodynamically active in pediatric patients, as evidenced by decreases in sweat chloride concentrations during ivacaftor treatment. Ivacaftor was well-tolerated in pediatric patients. Despite the lung function as measured by FEV 1 being in the normal range in the small number of pediatric patients in Study 110, some children and adolescents have lung disease that is not evident based on FEV 1 measurements, and some patients with the R117H mutation have more rapidly progressing disease. These patients have the potential to benefit from ivacaftor treatment. This is a small group of patients that could best be identified based on the individual assessment of clinicians. In summary, the totality of data provides substantial evidence of effectiveness, and the benefit:risk profile supports approval of ivacaftor in patients age 6 years and older who have an R117H mutation in the CFTR gene.
29 FDA Advisory Committee Briefing Materials Page 29 of INTRODUCTION KALYDECO (ivacaftor) is a cystic fibrosis transmembrane conductance regulator (CFTR) potentiator. KALYDECO is currently approved in the US for the treatment of CF in patients age 6 years and older who have one of the following mutations in the CFTR gene: G551D, G1244E, G1349D, G178R, G551S, S1251N, S1255P, S549N, or S549R. Vertex submitted a supplemental New Drug Application (snda) for the approval of KALYDECO for the treatment of cystic fibrosis (CF) in patients age 6 years and older who have an R117H mutation in the CFTR gene. In the US, about 500 people with CF have the R117H mutation and 6 years of age or older. The current USPI is provided in Appendix SCIENTIFIC BACKGROUND Summary CF is a progressive, life-threatening disease that affects about 30,000 people in the US. CF is caused by defective or missing CFTR protein that results from mutations in the CFTR gene. Newborn screening for mutations in the CFTR gene is now routine practice in the US. The CFTR protein is an epithelial chloride channel that aids in regulating salt and water absorption and secretion in multiple organs, including lungs, pancreas, and sweat glands. Decreased CFTR chloride transport results in the multisystem pathology associated with CF. In people with CF, the primary cause of morbidity and mortality is lung disease. The lung disease is characterized by inflammation and recurrent, chronic infections that lead to progressive loss in lung function, ultimately resulting in respiratory failure. Evidence of lung disease is apparent as early as 3 years of age, and occurs before decreases in lung function (percent predicted FEV 1 ) are apparent. The structural lung damage caused by CF is regarded as irreversible, and therefore avoiding or slowing the progression of structural damage is a key therapeutic goal. The rate of CF disease progression generally correlates with the extent of loss of CFTR chloride transport. The amount of chloride transported by the CFTR protein is a function of the quantity of CFTR protein at the cell surface, the channel gating of the CFTR protein (amount of time the CFTR protein channel is open and can transport chloride), and the channel conductance of the CFTR protein (rate at which chloride passes through the open channel). With the exception of ivacaftor, pharmacologic treatments for CF target the downstream consequences of diminished CFTR function, such as lung disease or pancreatic insufficiency.
30 FDA Advisory Committee Briefing Materials Page 30 of Cystic Fibrosis CF is an autosomal recessive, progressive, and life-threatening genetic disease most common in the Caucasian population. CF affects approximately 75,000 individuals in North America, Europe, and Australia, including approximately 30,000 people in the United States (US). 1,19,20,21 Among people in the US with CF, the median age of death is 27 years. 1 CF is caused by loss-of-function mutations in the CFTR gene that result in decreased quantity and/or function of the CFTR protein at the cell surface. 22 The CFTR protein is an epithelial chloride channel responsible for aiding in the regulation of salt and water absorption and secretion in multiple organs, including lungs, pancreas, intestinal tract, biliary tract, sweat glands, and vas deferens. 2,23-26 More than 1900 CFTR mutations have been identified, 27 although not all of these mutations cause CF. 3.2 Diagnosis of Cystic Fibrosis The diagnosis of CF is suggested by the presence of 1 or more characteristic clinical features, a history of CF in a sibling, or a positive newborn screening test result, and is confirmed by laboratory evidence of abnormal CFTR protein function (a positive sweat chloride test) or by genotyping analysis. 28,29 Genotyping for mutations in the CFTR gene is now routine practice in many countries, including the US. Since the introduction and continued advances of newborn screening, many patients with CF are identified through a positive screen test and subsequently diagnosed within the first neonatal year. 29 In the US, more than 61% of people with CF who were diagnosed in 2012 were found because of an abnormal newborn screen. 1 Elevated sweat chloride concentrations are a hallmark of CF and are used for diagnostic purposes. Sweat chloride concentrations 60 mmol/l are considered indicative of CF; intermediate sweat chloride values in the range of 40 to 59 mmol/l are also observed in patients with CF; and a sweat chloride concentration 39 mmol/l is generally considered normal, although CF patients have also been identified with these values (particularly in the very young, where 30 mmol/l may be considered normal Clinical Consequences The CFTR protein is located in the apical membrane of epithelial cells in multiple organs, including lungs, pancreas, intestinal tract, biliary tract, sweat glands, and vas deferens. The decrease in chloride transport in these organs results in the multisystem pathology associated with CF (Figure 5).




31 FDA Advisory Committee Briefing Materials Page 31 of 157 Figure 5 Pathophysiologic Cascade of CF Disease Source: Rowe SM et al. N Engl J Med. 2005;352: ; Ratjen. Respir Care. 2009;54: Clinical manifestations of CF occur throughout the body (Figure 6). 2 Figure 6 Clinical Manifestations of CF Occur Throughout the Body Source: O Sullivan BP, Freedman SD. Lancet. 2009;373:


32 FDA Advisory Committee Briefing Materials Page 32 of Lung Disease Although CF is a multi-system disease, the primary cause of morbidity and mortality is lung disease. 1,2 In the lungs, the dysfunction of the CFTR protein leads to obstruction of airways with thick mucus, chronic bacterial infections, and damaging inflammatory responses, which are thought to play a role in causing irreversible structural changes. Chronic infection with P. aeruginosa leads to faster progression of lung disease and a shortened survival. 30,31 Thus, lung disease in patients with CF is characterized by inflammation and recurrent and chronic infections leading to progressive loss in pulmonary function and respiratory failure. People with CF typically experience a progressive loss of lung function (Figure 9). 1 Figure 7 Lung Disease is Progressive in People with CF Source: US CFF Registry; 2012 FEV 1 obtained from spirometry is a reflection of the extent of airway obstruction and is the most clinically accepted measure of pulmonary function and disease progression in CF. 32,33 Per US regulatory guidance, FEV 1 is also the recommended primary clinical endpoint in efficacy studies for CF 34 and chronic obstructive pulmonary disease. 35 However, FEV 1 is an indirect measure of lung structure and is insensitive to detect localized or small airway damage. 36,37 Lung damage (from any disease, not just CF) can be significant before airflow is affected. It is important to appreciate that CF patients with preserved FEV 1 may not have entirely healthy lungs. Studies over the past 2 decades using high-resolution computed tomography (HRCT) have shown lung damage (such as airway wall thickening and bronchiectasis) in patients with CF despite normal or stable lung function as measured by FEV HRCT studies in infants with CF that were diagnosed by newborn screening, but were considered clinically healthy, indicate that structural lung damage is common even very early in disease progression In a cohort of 81 well-treated CF infants in Australia diagnosed by newborn screening, by the age of 3 years, 84% had evidence of bronchiectasis (on computed tomography scan), indicating that irreversible structural changes had occurred; 69% had evidence of gas trapping (on computed tomography scan); and 10% had Pseudomonas aeruginosa infection. 45 This is consistent with the results of inflammatory marker studies that have found that airway inflammation begins in infancy

33 FDA Advisory Committee Briefing Materials Page 33 of 157 The presence of airway inflammation signals the beginning of the destructive cycles of chronic inflammation, infection, and irreversible lung damage that are characteristic of CF lung disease. 49 A study of the longitudinal development of P. aeruginosa infection in children with CF found that 29% of the infants developed nonmucoid infection in the first 6 months of life; overall, the median age for nonmucoid P. aeruginosa infection was 1.0 years, and the transition from nonmucoid to mucoid P. aeruginosa infection was 13.0 years. 50 Chronic (mucoid) P. aeruginosa infection is considered the major limiting factor in survival for patients with CF Level of Chloride Transport and CF Disease Characteristics The amount of chloride transported by the CFTR protein is a function of the quantity of CFTR protein at the cell surface, the channel gating of the CFTR protein (the amount of time the CFTR protein channel is open and can transport chloride), and the channel conductance of the CFTR protein (rate at which chloride passes through the open channel) (Figure 8). 3-5 Figure 8 CFTR Chloride Transport is Determined by CFTR Quantity and CFTR Function The loss-of-function mutations that cause CF result in decreased quantity and/or function of the CFTR protein. As for other ion channels, gating of the CFTR channel is measured by open probability, and conductance of the CFTR channel is measured by current amplitude. By definition, a CFTR form that has lower open probability than normal CFTR has a gating defect. By definition, a CFTR form that has lower current amplitude than normal CFTR has a conductance defect. Some CFTR mutations reduce both the quantity and function of CFTR (e.g., F508del) or cause defects in both channel gating and channel conductance (e.g., R117H). 3 In people with CF, the rate of CF disease progression generally correlates with the extent of loss of CFTR chloride transport (Figure 8). A complete or near complete loss of CFTR-mediated chloride transport referred to as minimal function of CFTR results in CF characterized by an early onset and relatively rapid disease progression, with a median
.")
.")
34 FDA Advisory Committee Briefing Materials Page 34 of 157 age of death of 24 years for patients in the US (registry data from 1996 to 2002). 65 Examples of mutations that result in minimal CFTR function are F508del and the mutations with a defect in channel gating for which Kalydeco is currently approved (e.g., G551D). A less complete loss of CFTR-mediated chloride transport referred to as residual function of CFTR often results in CF that is more slowly progressive but that may still reach a severe disease stage and cause premature death, with median age of death of 38 years for patients in the US (registry data from 1996 to 2002). 65 There is no consensus in the field about the precise definition of minimal versus residual CFTR function, but there is consensus that there 3, 57 is residual CFTR function associated with R117H both in vitro and in vivo. Figure 9 Level of CFTR Dysfunction Relates to Disease Phenotype Source: Strausbaugh, Clin Chest Med 2007; McKone et al, Chest 2006; McKone et al, Lancet 2003; Noone et al, Gastroenterology 2001; Noone et al, Am J Respir Crit Care Med 2000; Davis et al, Am J Respir Crit Care Med CF is an autosomal recessive disease. Individuals with mutations on both CFTR alleles that result in minimal CFTR function have an early onset, more rapidly progressive disease phenotype. Individuals who have 1 allele with a mutation that results in minimal CFTR function and 1 allele with a mutation that results in residual CFTR function generally have a more slowly progressive disease phenotype. Individuals who have a CF-causing mutation on only one allele do not have CF, even if that mutation results in minimal CFTR function. While CF disease phenotype is largely determined by the CFTR mutations, other factors such as modifier genes and environmental factors also affect disease progression and severity. A CFTR potentiator, such as ivacaftor, may benefit individuals who are homozygous for a CFTR mutation that responds to the potentiator and individuals who are heterozygous and have one CFTR allele that responds to the potentiator. While, on average, the rate of disease progression is slower in patients who have residual CFTR function than in patients with minimal CFTR function, there is heterogeneity in these patients and some patients with residual CFTR function reach an advanced stage of disease at

35 FDA Advisory Committee Briefing Materials Page 35 of 157 a younger age. Importantly, structural damage caused in the lungs is regarded as irreversible, and therefore preventing or slowing the progression of structural damage is a key therapeutic goal. 3.6 Treatments for Cystic Fibrosis There is no cure for CF. With the exception of ivacaftor, pharmacologic treatments for CF target the downstream consequences of diminished CFTR function (Figure 10). Figure 10 Current Therapies Target the Downstream Manifestations of CF Source: Ratjen. Respir Care. 2009; 54: ; Jones et al. Drugs. 2009; 69: ; Davis et al., Am J Respir Crit Care Med. 1996; 154: Table 9 shows drugs commonly used for patients with CF, excluding antimicrobials. Antibmicrobials such as tobramycin (TOBI Podhaler is indicated for the management of CF patients with Pseudomonas aeruginosa), and aztreonam for inhalation solution (Cayston ; indicated to improve respiratory symptoms in CF patients with Pseudomonas aeruginosa) are also commonly used for the treatment of CF patients.

36 FDA Advisory Committee Briefing Materials Page 36 of 157 Table 9 Drugs Commonly Used for Patients With Cystic Fibrosis (Antimicrobials Excluded) Source: FDA briefing document; Pulmonary-Allergy Drugs Advisory Committee Meeting, 30 January 2013 For the drugs commonly used for patients with CF and for which there is an FDA-approved CF indication related to respiratory function, increases achieved in percent predicted FEV 1 are summarized below. Note that some of these results are reported as relative change and some are reported as absolute change, which affects the magnitude of the result. (See Section 5.3 for an explanation of absolute change versus relative change.) Dornase alpha: the overall mean relative increase from baseline in FEV 1 during 6 months of therapy was 5.8% at the 2.5 mg once daily dose level and 5.6% at the 2.5 mg twice daily dose level. This study was conducted in CF patients 5 years of age and older with a baseline forced vital capacity 40% predicted and who were receiving standard therapies for CF. (Source: Pulmozyme USPI; dated October 2010). Tobramycin: Treatment with TOBI Podhaler and placebo resulted in relative increases in percent predicted FEV 1 of 12.54% and 0.09%, respectively, at the end of the first 28-day cycle of treatment (least squares mean difference = 12.44%; 95% CI: 4.89, 20.00; P=0.002). Analysis of absolute changes in percent predicted FEV 1 showed a treatment difference of 6.90% (95% CI: 2.40, 11.40). These studies were conducted in patients 6 to 21 years of age with FEV 1 within the range of 25% to 80% (inclusive), and >90% of patients received concomitant therapies for CF (Source: TOBI Podhaler USPI; dated April 2014). Aztreonam: In a placebo-controlled study, the treatment difference for percent change in FEV 1 (L) at Day 28 was statistically significant at 10% (95% CI: 6%, 14%). The study enrolled patients with a mean baseline percent predicted FEV 1 of 55%, and patients were receiving standard care for CF, including drugs for obstructive airway disease. (Source: CAYSTON USPI; dated 2012). Published results of clinical studies of aztreonam in patients with CF aged 6 years and older reported treatment differences of 6.6% and 10.2% for relative change in percent predicted FEV 1. 58,59 Patients in these studies received concomitant therapies for CF and had a mean percent predicted FEV 1 of 55% at baseline.
37 FDA Advisory Committee Briefing Materials Page 37 of R117H MUTATION Summary The R117H mutation is present in about 700 people with CF in the US, including about 500 people age 6 years and older. While R117H is often associated with delayed onset of clinical symptoms relative to the mutations for which ivacaftor is currently approved, CF patients with the R117H mutation have progressive disease, with premature mortality and considerable morbidity. About 50% of patients with the R117H mutation who are age 6 to 11 years have early clinical evidence of lung disease (lung infection; treatment for lung disease; antibiotic treatment and/or pulmonary exacerbation; respiratory diagnosis), with an additional 7% of patients in this age group already having FEV 1 90% predicted. The declines in FEV 1 are progressive. Compared with patients who are F508del homozygous or who carry one of the mutations for which ivacaftor is currently approved, patients with the R117H mutation have lower sweat chloride levels, a lower incidence of pancreatic insufficiency, and a slower progression of lung disease, consistent with the presence of some functional CFTR. As a result of advances in newborn screening, individuals with an R117H mutation are being identified earlier in life, often before the onset of advanced gastrointestinal or pulmonary manifestations. The patient population with the R117H mutation is heterogeneous, due in part to polymorphisms in the polythymidine sequence (poly-t tract) that is on the same CFTR allele as the R117H mutation. The length of the poly T tract (5T, 7T, or 9T) affects the splicing efficiency of CFTR mrna, which affects the amount of functional CFTR protein synthesized (5T<7T <9T). CF patients with the R117H mutation have a high unmet medical need, particularly for therapies that target the underlying cause of CF. 4.1 Prevalence The R117H mutation is present in approximately 2% to 3% of patients with CF in the US and European Union (EU). 1,60-63 The 2013 US Cystic Fibrosis Foundation (CFF) registry (which includes more than 90% of people in the US with CF) included approximately 700 people with the R117H mutation. 1 Of these 700, about 500 are 6 years of age. 1,6 4.2 Clinical Characteristics The R117H mutation has variable penetrance: people with the R117H mutation have a heterogeneous clinical presentation and progression, ranging from asymptomatic to classic CF. 7-10,64 The clinical consequences of R117H are influenced by another region of the CFTR gene (the poly-t tract), which affects the amount of functional CFTR protein produced (see Section 4.3). Nonetheless, patients who develop CF and have the R117H mutation have a reduced median life expectancy, with a median age of death of 38 years for CF patients in the US who carry


38 FDA Advisory Committee Briefing Materials Page 38 of 157 this type of mutation (mutation with residual CFTR function; US registry data from 1996 to 2002). 65 Compared with patients with CF who are F508del homozygous or who carry one of the mutations for which ivacaftor is currently approved, people with the R117H mutation have lower sweat chloride levels, a lower incidence of pancreatic insufficiency, and a slower progression of lung disease (Figure 11). 9 Patients homozygous for the F508del-CFTR mutation have a mean sweat chloride concentration of 104 mmol/l, compared with a mean sweat chloride concentration of 60 mmol/l for patients with an R117H-CFTR mutation. 9 This is consistent with the minimal and residual CFTR function associated with these CFTR genotypes. Figure 11 Comparison of F508del Homozygous and R117H Phenotype Source: Source: CFF and Johns Hopkins Hospital. Clinical and Functional Translation of CFTR (CFTR2) Database. Historically, due to the slower progression of disease, many individuals with an R117H-CFTR mutation were not diagnosed with CF until the late childhood or adult years, when the disease had progressed and symptoms became more evident. Recently this has changed because of advances in newborn screening. As a result, more individuals with an R117H-CFTR mutation are now identified earlier in life, often before the onset of advanced gastrointestinal or pulmonary manifestations. 14,70 A study of 4 children followed for up to 30 months after having been identified through prenatal screening or newborn screening as having the F508del/R117H-7T genotype, and who had normal or borderline sweat chloride levels, found that all 4 children had pulmonary infection with CF-related organisms and had abnormalities detected on chest x-ray, and 1 child had pulmonary symptoms. 66 A study of 10 children 1 to 7 years of age with the F508del/R117H-7 genotype found that the majority had pulmonary infection with CF-related organisms and all had abnormalities detected on chest x-ray (e.g., bronchial wall thickening). 67 As for other CFTR mutations that cause CF, the R117H mutation is associated with reduced lung function, gradually progressive obstructive lung disease, recurrent sinusitis and bronchitis, and increasing frequency of hospitalizations due to pulmonary disease. 68-,69,70
. In the 12 to 17 year old subgroup, 17% of patients have percent predicted FEV 1 <90%, and this increases to 59% of patients 18 years of age.")

39 FDA Advisory Committee Briefing Materials Page 39 of 157 Data from the US CFF Registry show evidence of lung disease and decreased percent predicted FEV 1 even in patients 6 to 11 years of age, and a progression of reduced FEV 1 with age (Figure 12). In the 12 to 17 year old subgroup, 17% of patients have percent predicted FEV 1 <90%, and this increases to 59% of patients 18 years of age. 6 Figure 12 Prevalence of Lung Disease with Normal Percent Predicted FEV 1 and Percent Predicted FEV 1 in Different Age Groups of Patients in the US with the R117H Mutation Source: CFF Registry; 2011 dataset Figure 13 shows percent predicted FEV 1 results by age cohort for patients with the R117H mutation who are included in the CFF registry, further illustrating the progressive loss of lung function with age. 6


40 FDA Advisory Committee Briefing Materials Page 40 of 157 Figure 13 Percent Predicted FEV 1 by Age Cohorts for CF Patients in US With an R117H-CFTR Mutation Source: CFF Registry Data, 2011; data on file at Vertex. An analysis of 2011 CFF registry data, providing the number of patients with percent predicted FEV 1 <90% or 90%, by age cohort is provided in Figure Figure 14 Percent Predicted FEV 1 <90% and 90%, by Age Cohort, for CF Patients in US With an R117H-CFTR Mutation Source: CFF Registry Data, 2011
41 FDA Advisory Committee Briefing Materials Page 41 of Complex Allele The R117H mutation has variable penetrance: people with the R117H mutation have a heterogeneous clinical presentation and progression, ranging from asymptomatic to classic CF. 7,8,9,10 The clinical consequences of R117H are influenced by the length of the poly-t tract, another region of the CFTR gene, that is in cis (on the same allele) with the R117H mutation. The length of the poly-t tract affects the splicing efficiency of CFTR mrna, and thus the amount of functional CFTR protein synthesized. 11 The poly-t tract can occur as 1 of 3 variants (5T, 7T, or 9T). The lower the number of thymidine repeats, the less functional CFTR protein that is synthesized. 11 R117H-5T will likely cause disease, R117H-7T is less likely to cause disease, and R117H-9T is highly unlikely to cause disease.7,8 Heterogeneity of clinical presentation also exists within the R117H-5T and R117H-7T populations, due to factors such as inter-patient variability in the effect of a given poly-t variant on CFTR mrna splicing efficiency. 12,12,13 The mechanism by which poly-t variants result in less functional CFTR protein on the cell surface by decreasing the amount of functional CFTR protein synthesized differs from that of the F508del, the most prevalent CFTR mutation. F508del causes a defect in the processing and trafficking of the CFTR protein and results in little-to-no CFTR at the cell surface While CFTR genotyping can provide the patient's poly-t variant genotype, it cannot specify which CFTR allele each variant was located on. Determining which variant is in cis with the R117H mutation requires genotyping both parents or analyzing the patient s genotype using allele-specific long-range polymerase chain reaction, which is not a routine component of CFTR genotyping. Although patients with an R117H-7T allele are generally less likely to develop CF disease than those with the R117H-5T allele, some people with the R117H-7T allele develop CF. 8,14 A study of Australasian individuals found that some patients with R117H-7T had clinical signs of CF, including decreased percent predicted FEV 1. 8 The Cystic Fibrosis Foundation consensus report Guidelines for Diagnosis of Cystic Fibrosis in Newborns through Older Adults states that infants with R117H-7T are at sufficiently high risk for lung disease to merit clinical monitoring in a CF care center. 29
42 FDA Advisory Committee Briefing Materials Page 42 of IVACAFTOR Summary Ivacaftor is the only approved treatment that targets the underlying cause of CF. Ivacaftor increases CFTR chloride transport by potentiating the channel open probability (gating) of the CFTR protein at the cell surface. In the US, ivacaftor is approved for treatment of CF in patients age 6 years and older who have one of the following mutations in the CFTR gene: G551D, G1244E, G1349D, G178R, G551S, S1251N, S1255P, S549N, and S549R. This population includes about 1100 people in the US. The currently approved mutations all result in defects in CFTR gating, which decrease the open probability of the CFTR chloride channel (amount of time channel is open and can transport chloride). The ability of ivacaftor to increase chloride transport by increasing CFTR open probability was demonstrated in vitro for these mutations. Translation of in vitro to in vivo results was demonstrated for the G551D mutation and the other 8 mutations for which ivacaftor is approved in the US: ivacaftor treatment decreased sweat chloride concentration, demonstrating that ivacaftor increases CFTR chloride transport in CF patients. Ivacaftor treatment has been proven to result in clinical benefit in adults, adolescents, and children 6 to 11 years of age. In patients with the G551D mutation, the ivacaftor treatment effect for absolute change in percent predicted FEV 1 through Week 24 was 10.6 percentage points (P <0.0001) in patients 12 years of age and 12.5 percentage points (P <0.0001) in patients 6 to 11 years of age. Ivacaftor treatment also resulted in substantial and sustained clinical benefit in other pulmonary endpoints and in extrapulmonary endpoints, including measures of nutritional status (weight, body mass index). Ivacaftor is very well-tolerated, with a safety profile that appears similar in children and adults and that has remained consistent with long-term use. Adverse events that have been associated with ivacaftor have generally been mild to moderate in severity, and not treatment-limiting. In placebo-controlled studies, the overall incidence of SAEs has been lower in patients treated with ivacaftor than in patients treated with placebo. In 48-week, placebo-controlled studies in patients with the G551D mutation, AEs that had a higher incidence in ivacaftor-treated patients than in placebo treated patients were headache, oropharyngeal pain, upper respiratory tract infection, nasal congestion, abdominal pain, nasopharyngitis, diarrhea, and rash. As of 23 July 2014, the pharmacovigilance safety database for ivacaftor includes post-marketing exposure for more than 2000 patients, accounting for more than 1,045,000 person-days of exposure, 390 are age 6 to 11 years, accounting for more than 197,000 person-days of exposure. Post-marketing safety data are consistent with those from clinical studies and the established safety profile of ivacaftor.

43 FDA Advisory Committee Briefing Materials Page 43 of Overview Ivacaftor is a first-in-class therapy that potentiates the activity of the CFTR protein. Ivacaftor is currently the only approved treatment for patients with CF that targets the underlying cause of the disease. In the US, Kalydeco (ivacaftor) was granted Fast Track Designation on 04 May 2006, Orphan Drug Designation (Designation No ) on 20 December 2006, and Breakthrough Therapy Designation on 13 November In January 2012, Kalydeco was approved by the FDA for the treatment of CF in patients age 6 years and older who have a G551D mutation in the CFTR gene. In February 2014, the FDA approved Kalydeco for the following 8 CFTR gating mutations: G1244E, G1349D, G178R, G551S, S1251N, S1255P, S549N, and S549R. The current Kalydeco UPSI is provided in Appendix Kalydeco is also approved in Australia, Canada, the EU, Liechtenstein, Switzerland, and New Zealand. This section of the document describes the mechanism of action of ivacaftor, the clinical development program, and in vitro and clinical data for previously studied mutations. The previously studied mutations result in minimal CFTR function and early onset of CF disease. The term severe gating defects is used to refer to mutations with a gating defect that result in minimal CFTR function. (See Section 3.1 for information about minimal and residual function and CF disease progression.) 5.2 Mechanism of Action Ivacaftor increases CFTR chloride transport by potentiating the channel open probability (gating) of the CFTR protein at the cell surface (Figure 15). Figure 15 Ivacaftor Mechanism of Action
 and current channel amplitude (conductance).")
44 FDA Advisory Committee Briefing Materials Page 44 of 157 The effect of ivacaftor on the open probability of G551D-CFTR, a CFTR form with a gating defect that results in minimal CFTR function, can be directly measured to assess ion channel open probability (gating) and current channel amplitude (conductance). Studies using membrane patches excised from Fischer rat thyroid (FRT) cells expressing normal and G551D-CFTR show that in the absence of ivacaftor, the open probability of G551D-CFTR is <5% of normal CFTR. With the addition of ivacaftor, in the presence of protein kinase A (PKA) and adenosine triphosphate (ATP), G551D-CFTR channel open probability is substantially increased (Figure 16 shows patch clamp tracing; see Table 17 for quantitative summary of results). Figure 16 Effect of Ivacaftor on Channel Gating Activity of G551D-CFTR Source: Van Goor et al. 71 Representative patch-clamp tracings for normal CFTR or G551D-CFTR mutation in an excised plasma membrane patch from Fischer rat thyroid (FRT) cells expressing the G551D-CFTR mutation or normal CFTR. To activate CFTR, the cytoplasmic surface (bath solution) was exposed to 75 nm PKA and 1 mm ATP (baseline) before application of 10 μm ivacaftor. 5.3 Overview of Clinical Development Program A CFTR potentiator, such as ivacaftor, may benefit individuals who are homozygous for a CFTR mutation that responds to the potentiator and individuals who are heterozygous and have one CFTR allele that responds to the potentiator. Because ivacaftor s mechanism of action is to increase the open probability of CFTR at the cell surface, the clinical development program initially focused on the population of CF patients who have a G551D-CFTR gating mutation and then evaluated CF patients who have non-g551d-cftr gating mutations that result in minimal CFTR function. These mutations do not affect the quantity of CFTR at the cell surface but decrease the function of the CFTR: they decrease the gating activity of the channel, resulting in a decreased open probability (decreased amount of time the channel is open and can transport chloride). The clinical development program also evaluated patients who are homozygous for the F508del mutation; this population represents about 50% of the US CF patient population. The F508del mutation results in little to no CFTR at the cell surface, and the very small amount of CFTR at the cell surface exhibits defective channel gating and more rapid turnover than normal CFTR The primary efficacy endpoint in Phase 3 studies was the absolute change from baseline in percent predicted FEV 1. Secondary efficacy endpoints included absolute changes in sweat chloride, measures of nutritional function (weight, BMI), CFQ-R respiratory domain score (a patient reported outcome measure) and time to first pulmonary exacerbation.
45 FDA Advisory Committee Briefing Materials Page 45 of 157 Absolute change is calculated as the difference between two values: For values that are percentages (such as percent predicted FEV 1 ), the units for absolute change are percentage points. Relative change expresses the absolute change as a percentage of the first value: 5.4 Results for Previously Studied Mutations Clinical development of ivacaftor for the currently approved mutations was supported by in vitro studies showing that (1) ivacaftor increased the open probability of these CFTR forms; and (2) ivacaftor increased chloride transport of these CFTR forms Efficacy For the approval of ivacaftor for treatment of CF in patients with the G551D mutation, separate placebo-controlled studies were conducted for patients 6 to 11 years of age (52 patients) and patients 12 years of age (161 patients). The other mutations currently approved for ivacaftor treatment in the US have a lower prevalence than G551D and were evaluated in a single placebo-controlled study in 39 patients aged 6 years and older. (In the US, about 1100 people with CF age 6 years or older have the G551D mutation or one of the other CFTR mutations for which ivacaftor is currently approved in the US.) Table 10 summarizes baseline disease characteristics for studies of ivacaftor in patients with mutations that cause severe gating defects (Studies 102, 103, and 111) and in patients homozygous for the F508del-CFTR mutation (Study 104). These genotypes result in CFTR with minimal CFTR function, and thus are associated with early progression of CF. Baseline characteristics for patients in Studies 102, 103, 111, and 104 were consistent with a population of patients with this CF phenotype, including mean sweat chloride levels of approximately 100 mmol/l. Table 10 Baseline Characteristics of Patients in Studies of Ivacaftor in Different Populations (G551D, Non-G551D Severe Gating, F508del Homozygous) G551D 6 to 11 Yr Study 103 (N=52) G551D 12 Yr Study 102 (N=161) Non-G551D Severe Gating 6 Yr Study111 (N=39) a F508del Homozygous 12 Yr Study 104 (N=140) Endpoint Sweat chloride (mmol/l) N=48 N=152 N=139 mean (SD) (11.92) (10.28) 97.5 (18.58) (9.83) ppfev 1 mean (SD) 84.2 (18.06) 63.6 (16.43) 78.4 (20.98) 78.7 (22.95) <70%, n (%) 12 (23.1) 94 (58.4) 13 (33.3) 53 (37.9) 70%, n (%) NA 67 (41.6) NA NA 70% to 90%, n (%) 18 (34.6) NA 12 (30.8) 40 (28.6)
46
47 FDA Advisory Committee Briefing Materials Page 47 of 157 Table 11 summarizes efficacy results for ivacaftor in patients with mutations that cause severe gating defects (G551D mutation: Studies 102, 103; other mutations that cause severe gating defects; Study 111) and in patients homozygous for the F508del mutation (Study 104). Ivacaftor showed treatment benefit for pulmonary and extrapulmonary endpoints in patients with the G551D mutation and patients with other mutations that cause severe gating defects. In patients homozygous for the F508del-CFTR mutation, the estimated treatment difference was 1.72 percentage points (95% CI: -0.6; 4.1) for the absolute change in percent predicted FEV 1 and mmol/l (P=0.0384) for the absolute change in sweat chloride. These results were not unexpected because F508del results in a little to no CFTR on the cell surface, such that there are insufficient channels to potentiate, and therefore the increase in channel open probability resulting from ivacaftor treatment is insufficient to provide a substantial increase in chloride transport or measurable clinical benefit. For this mutation, combination therapy, with a CFTR corrector (increases trafficking to the cell surface) as well as a potentiator (to increase open probability) will be required Table 11 Endpoint Absolute Change from Baseline: Sweat chloride ppfev 1 (percentage points) CFQ-R Respiratory Domain Score Body Weight BMI-for-age Z-score Pulmonary and Extrapulmonary Endpoints: Treatment Difference (Ivacaftor vs Placebo) for Different Patient Populations (G551D, Non- G551D Severe Gating, F508del Homozygous) G551D 12 Yr Study 102 (N=78 Pbo; N=83 Iva) N=74 P; N=78 I mmol/l P< N=78 P, N=83 I 10.6 P< N=71 P; N=80 I 8.1 points P< N=78 P, N=83 I 2.8 kg P< N=23 P; N=24 I 0.34 points P= G551D 6 to 11 Yr Study 103 (N=26 Pbo; N=26 Iva) N= 23 P; N=23 I mmol/l P< N=25 P; N=26 I 12.5 P< N=25 P; N=26 I 6.1 points P= N=26 P, N=26 I 1.9 kg P< N=26 P, N=26 I 0.34 points P= Non-G551D Severe Gating 6 Yr Study111 (N=37 Pbo; N=38 Iva) a N=38 P; N=37 I mmol/l P< N=37 P; N=38 I 10.7 P< N=37 P; N=38 I 9.6 points P< N=37 P; N=38 I 1.7 kg P< N=17 P; N=19 I 0.28 points P= F508del Homozygous 12 Yr Study 104 (N=28 Pbo; N=112 Iva) N=28 P; N=109 I -2.9 mmol/l P= N=28 P; N=111 I 1.7 P= N=28 P; N=111 I 1.3 points P= N=28 P; N=112 I kg P= N=7 P; N=56 I 0.06 points P= P=placebo; I=ivacaftor. Note: Treatment difference (model-based) = effect of ivacaftor effect of placebo. Results are shown for the primary efficacy endpoint analysis (through Week 24 for Studies 102 and 103; through Week 8 for Study 111; through Week 16 for Study 104). Given the time course of response to ivacaftor, results can be compared across studies. a Study 111 was a crossover study; patients were randomized to 1 of 2 treatment sequences (ivacaftor then placebo or placebo then ivacaftor; treatment periods were separated by a 4- to 8-week washout period). b Pooled adults/adolescent adult/adolescent and 12- to 13-year old CFQ R versions in Study Studies 102 and Study ; child version in Study 103.; and pooled adult/adolescent, 12- to 13-year-old version, and child version in Study 111. c BMI-for-age z-scores were only determined for patients age 20 years or less in Studies 102, 111, and 104.
48 FDA Advisory Committee Briefing Materials Page 48 of 157 Ivacaftor has sustained efficacy that has translated into real-world benefits. Study 105, an open-label safety study, confirmed the favorable safety profile of ivacaftor and also demonstrated that the benefits on endpoints such as FEV 1, weight/bmi, respiratory symptoms, and pulmonary exacerbations were sustained up to 144 weeks. 16 An analysis of the annualized rate of decline in percent predicted FEV 1 in patients treated with ivacaftor for 2 to 3 years during Phase 3 clinical trials (Studies 102/103 and 105) compared to a homozygous F508del control population (propensity-score-matched; 1:5 matching ratio) was presented at the European Cystic Fibrosis Congress in The rate of decline in percent predicted FEV 1 was lower in patients treated with ivacaftor for 2 to 3 years (-0.81 ± 0.36) than in the matched controls (-1.73 ± 0.17); this difference was statistically significant (P<0.02). Data from the G551D Observational Study (GOAL) run by the CF Foundation assessed the impact of ivacaftor in post-approval usage. In addition to showing comparable benefits on many of the endpoints assessed in the pivotal trials, this study provided evidence for a pre-to-post treatment reduction in hospitalization rates across 6 months from 27% to 8% (P<0.001) and a reduction in P aeruginosa positive culture rates across 6 months from 52% to 34% (P<0.001). 18 These data demonstrate the important benefits that ivacaftor treatment can provide Safety The safety profile of ivacaftor is based on data from clinical trials and from the pharmacovigilance safety database, which has collected AE information from spontaneous and solicited sources for more than 2 years, since the first approval in the US in January The clinical trials safety database includes placebo-controlled safety data for up to 48 weeks in patients 6 years and older with a G551D mutation, followed by open-label safety data in patients who received ivacaftor for up to 3 years. Of the more than 2000 patients with postmarketing exposure, 390 are age 6 to 11 years, accounting for more than 197,000 person-days of exposure. Since approval, there have been no significant changes to the established safety profile overall or for any age subgroup. Overall, ivacaftor is very well-tolerated, with a safety profile that appears similar in children and adults and that has remained consistent with long-term use. Adverse events that have been associated with ivacaftor have generally been mild to moderate in severity, and not treatment-limiting. In placebo-controlled studies, the incidence of SAEs was lower in patients treated with ivacaftor than in patients treated with placebo. Table 12 shows the incidence of the most common AEs in 48-week, placebo-controlled studies in patients with the G551D mutation. The majority of these AEs are common in CF patients. Adverse events with a higher incidence in ivacaftor-treated patients than in placebo treated patients were headache, oropharyngeal pain, upper respiratory tract infection, nasal congestion, abdominal pain, nasopharyngitis, diarrhea, and rash.
49 FDA Advisory Committee Briefing Materials Page 49 of 157 Table 12 Incidence of Most Common Adverse Events in All Patients; 48-Week, Placebo-Controlled, Phase 3 Studies in Patients Age 6 Years and Older With G551D Mutation Preferred Term Note: the most common adverse events associated with ivacaftor are in bold font Placebo N = 104 % Ivacaftor N = 109 % Cystic fibrosis lung a Cough Headache Oropharyngeal pain Upper respiratory tract infection Nasal congestion Abdominal pain Nasopharyngitis Pyrexia Productive cough Diarrhea Rash 7 13 Nausea Vomiting Rales This table includes data from Studies 102 and 103. Events in bold font had a higher incidence in the ivacaftor group than in the placebo group. a CF lung is a previous MedDRA preferred term for infective pulmonary exacerbation of CF. Table 13 shows the incidence of most common AEs in 48-week, placebo-controlled studies in patients with the G551D mutation, by age subgroup. The AE profile was similar in patients 12 years of age (Study 102) and patients 6 to 11 years of age (Study 103), in terms of which AEs were more frequent with ivacaftor than with placebo treatment. The treatment difference in the incidence of diarrhea was higher in patients 6 to 11 years of age (0 placebo; 12% ivacaftor) than in patients 12 years of age (13% placebo; 13% ivacaftor), although the incidence of diarrhea in ivacaftor-treated patients was lower in patients 6 to 11 years old than in patients 12 years old.
50 FDA Advisory Committee Briefing Materials Page 50 of 157 Table 13 Preferred Term Note: the most common adverse events associated with ivacaftor are in bold font Incidence of Most Common Adverse Events by Age; 48-Week, Placebo-Controlled, Phase 3 Studies in Patients Age 6 Years and Older With G551D Mutation Age 6 to 11 Years (Study 103) Age 12 Years (Study 102) Placebo N = 26 % Ivacaftor N = 26 % Placebo N = 78 % Ivacaftor N = 83 % Cystic fibrosis lung a Cough Headache Oropharyngeal pain Upper respiratory tract infection Nasal congestion Abdominal pain Nasopharyngitis Pyrexia Productive cough Diarrhea Rash Nausea Vomiting Rales This table includes data from Studies 102 and 103. Events in bold font had a higher incidence in the ivacaftor group than in the placebo group in one at least one of the studies. a CF lung is a previous MedDRA preferred term for infective pulmonary exacerbation of CF. AEs that were serious or that led to discontinuation of treatment were less frequent in ivacaftor-treated patients than in placebo-treated patients age 12 years and older. The same trend was seen in patients age 6 to 11 years, although the incidences were lower due to the lower incidence of pulmonary exacerbations (Table 14). Table 14 Category Overview of Adverse Events by Age; 48-Week, Placebo-Controlled, Phase 3 Studies in Patients Age 6 Years and Older With G551D Mutation Age 12 Years (Study 102) Age 6 to 11 Years (Study 103) Placebo N = 78 n (%) Ivacaftor N = 83 n (%) Placebo N = 26 n (%) Ivacaftor N = 26 n (%) Patients with AEs leading to death Patients with SAEs 33 (42) 20 (24) 6 (23) 5 (19) Patients with Grade 3 or 4 AEs 16 (21) 18 (22) 5 (19) 4 (15) Patients with AEs leading to study drug withdrawal SAE: serious adverse event 4 (5) 1 (1) 1 (4) 0
51 FDA Advisory Committee Briefing Materials Page 51 of 157 Table 15 shows the most common SAEs in 48-week, placebo-controlled studies in patients with the G551D mutation, by age subgroup. In both age subgroups, the most common SAE was CF lung, which had a lower incidence in ivacaftor-treated patients than in placebo-treated patients. SAEs of hemoptysis occurred only in patients 12 years, and had a lower incidence in ivacaftor-treated patients than in placebo-treated patients. Table 15 Category Preferred Term Most Common Serious Adverse Events by Age; 48-Week, Placebo-Controlled, Phase 3 Studies in Patients Age 6 Years and Older With G551D Mutation Age 12 Years (Study 102) Age 6 Through 11 Years (Study 103) Placebo N = 78 n (%) Ivacaftor N = 83 n (%) Placebo N = 26 n (%) Ivacaftor N = 26 n (%) Any serious adverse event 33 (42) 20 (24) 6 (23) 5 (19) Cystic fibrosis lung a 26 (33) 11 (13) 3 (12) 2 (8) Hemoptysis 4 (5) 1 (1) 0 0 Hypoglycemia 0 2 (2) 0 0 Productive cough (4) 1 (4) a CF lung is a previous MedDRA preferred term for infective pulmonary exacerbation of CF. Table 16 shows the incidence of transaminase elevations in the 48-week, placebo-controlled studies in patients age 6 years and older with the G551D mutation (Studies 102 and 103) and the Phase 2 study in patients 12 years or older who are homozygous for the F508del mutation(study 104). Transaminase elevations occurred in a small number of placebo-treated and ivacaftor-treated patients, and the incidence of these elevations was similar in the placebo and ivacaftor groups. Table 16 Incidence of Transaminase Elevations: Placebo-Controlled, Phase 3 Studies in Patients Age 6 Years and Older With G551D Mutation and Phase 2 Study in Patients Age 12 Years and Older Homozygous for F508del Mutation ALT or AST Maximum Elevation Placebo N =132 Incidence (%) Ivacaftor N=221 Incidence (%) >3 ULN 8 6 >5 ULN 2 3 >8 ULN 2 2 This table includes data for Studies 102, 103, and 104. Source: USPI; ALT: alanine aminotransferase; AST: aspartate aminotransferase; ULN: upper limit of normal Overall, the clinical features, including time to onset, concomitant factors, progression and resolution of liver function test (LFT) elevations, were similar between the placebo and ivacaftor groups. In all instances, the elevations in transaminases were reversible, and the role of ivacaftor in contributing to the transaminase elevations uncertain. No patients met
52 FDA Advisory Committee Briefing Materials Page 52 of 157 Hy s Law criteria. As a conservative measure, monitoring of LFTs on a quarterly basis during the first year of treatment was proposed and has been part of the ivacaftor labeling since initial approval. Lens opacities (cataracts), first observed in a nonclinical study involving juvenile rats, was identified as a potential safety concern with ivacaftor, though the relevance of the finding to humans is uncertain. The initial juvenile rat findings of nuclear cataracts were considered species and developmental age-specific, and unlikely relevant to humans. Similar findings of cataract have not been observed in other toxicology studies involving ivacaftor administered to older rats and dogs. However, ophthalmologic examinations have been included in ongoing ivacaftor clinical studies in children 2 to 11 years of age, and a post-marketing eye safety study has been initiated In conclusion, the safety profile in patients age 6 years and older who have the G551D mutation and who have been treated with ivacaftor for up to 3 years has remained consistent. Ivacaftor is very well-tolerated, with no new safety concerns emerging with longer-term use. The safety profile has also remained consistent and favorable in several recently completed studies, including the Phase 3 study in patients 6 years and older with non-g551d severe gating mutations (Study 111). See the USPI in Section 13.1 for further details about the ivacaftor safety profile. Worldwide Marketing Experience Ivacaftor is approved Australia, Canada, the EU, Liechtenstein, New Zealand, Switzerland, and the US. The pharmacovigilance safety database has collected AE information from spontaneous and solicited sources for more than 2 years, since the first approval in the US in January As of 23 July 2014, the pharmacovigilance safety database includes postmarketing exposure for more than 2000 patients, accounting for more than 1,045,000 person-days of exposure. Of the patients with postmarketing exposure, approximately 390 are age 6 to 11 years, accounting for more than 197,000 person-days of exposure. Ivacaftor appears to remain well-tolerated in the post-marketing setting in patients age 6 and older, with the type and incidence of AEs seen generally consistent with the established safety profile for ivacaftor. Since approval, there have been no significant changes to the overall safety profile from either clinical studies or post-marketing sources.
53 FDA Advisory Committee Briefing Materials Page 53 of R117H MUTATION: IN VITRO DATA Summary The R117H mutation results in CFTR protein with a gating defect (decreased open probability) and a conductance defect (decreased current amplitude). The gating defect is the dominant defect: R117H-CFTR has 22% of normal CFTR open probability and 88% of normal CFTR current amplitude. The R117H-CFTR gating defect is less severe than the G551D-CFTR gating defect (3% of normal CFTR open probability). R117H-CFTR has residual chloride transport. In vitro, ivacaftor increased R117H-CFTR channel gating activity, as measured by an increase in the channel open probability. The increase in open probability resulted in an increase in chloride transport, from 26% of normal CFTR chloride transport to 38% of normal CFTR chloride transport. Ivacaftor had no effect on R117H-CFTR channel conductance. The mechanism of action of ivacaftor on R117H increasing CFTR channel open probability is the same as that proven to be clinically effective for G551D and the other gating mutations currently approved for ivacaftor. As for G551D and for the 8 other mutations for which ivacaftor is approved in the US, in vitro data supported development of ivacaftor for the R117H patient population. Consistent with results published in Nature in 1993, which showed that the open probability of R117H was 28% that of normal CFTR and the current amplitude of R117H was 86% that of normal CFTR, 3 in vitro studies conducted by Vertex showed that the R117H mutation results in gating and conductance defects, that the gating defect is the predominant defect, and that R117H-CFTR has residual chloride transport (Table 17). Ivacaftor significantly increased the level of chloride transport of R117H-CFTR but had no effect on the channel current amplitude of R117H-CFTR. Results for the G551D mutation are shown for comparison; as described in Section 5.2, ivacaftor increased the channel open probability of G551D-CFTR, and thus increased chloride transport of G551D-CFTR. The mechanism of action of ivacaftor for R117H-CFTR increasing channel open probability is the same as that proven to be clinically effective in G551D-CFTR and in the other 8 mutations for which ivacaftor is indicated in the US. The ability of ivacaftor to potentiate channel gating activity of different CFTR forms indicates that the action of ivacaftor is independent of the location of the CFTR mutation within the protein. The only stipulation is that a sufficient amount of CFTR is at the cell surface (because ivacaftor potentiates CFTR on the cell surface). The R117H human bronchial epithelial (HBE) cells carried 5T variant, which reduces the amount of CFTR protein on the cell surface (see Section 4.3).
54 FDA Advisory Committee Briefing Materials Page 54 of 157 Table 17 CFTR Form Channel Gating Activity, Single Channel Conductance, and Total Chloride Transport With and Without Ivacaftor in Cells Expressing G551D-CFTR or R117H-CFTR Channel Open Probability (Gating) (% Normal CFTR FRT Cells Channel Current Amplitude (Conductance) (% Normal CFTR) HBE Cells Total Chloride Transport (% Normal CFTR) No Ivacaftor Ivacaftor No Ivacaftor Ivacaftor No Ivacaftor Ivacaftor R117H 22 ± 1 a 42 ± 2 b 88 ± 1 a 86 ± 3 26 ± 2 a 38 ± 4 b G551D 3 ± 1 a 28 ± 5 b 104 ± ± 3 5 ± 1 a 48 ± 4 b Source: Module 2.5/Table 4 In all experiments, once a stable baseline was reached, 3 µm ivacaftor was added acutely during the recording. Channel open probability and single channel current amplitude were quantified by single-channel, patch-clamp electrophysiology using FRT cells expressing normal-cftr, R117H-CFTR, or G551D-CFTR. To activate CFTR, 75 nm protein kinase A was added in the presence of 1 mm ATP. Recordings were obtained at a holding potential of 80 mv. Total chloride transport was quantified by Ussing chamber electrophysiology using HBE cells derived from people without CF and from CF patients who had the F508del mutation on one CFTR allele and the R117H or G551D mutation on the second CFTR allele. The 5T variant was in cis with the R117H mutation. To activate CFTR, a maximally effective concentration of forskolin (10 µm) was added to activate adenylate cyclase and increase camp-dependent stimulation of protein kinase A. All data shown are the mean ± SEM (standard error of the mean) normalized to the activity of normal CFTR and expressed as % normal. Statistical significance: a P<0.001 vs. normal CFTR; b P<0.05 with ivacaftor vs. no ivacaftor. Given the in vitro results, it was anticipated that the improvement in CFTR activity with ivacaftor would be less in patients with the R117H mutation than in the patients with the G551D-CFTR mutation. However, even a modest change in CFTR function can affect the CF disease phenotype (Figure 9). 7 REGULATORY HISTORY OF R117H DEVELOPMENT PROGRAM The Study 110 design was finalized after obtaining advice from the FDA. The study was started in July 2012 and completed in October A Type B pre-snda meeting was held between Vertex and the FDA in March 2014 to discuss the results of the study and the possibility of filing an snda for KALYDECO for the treatment of CF patients age 18 years who have an R117H mutation. During this meeting, the Agency advised that an additional efficacy study may be needed since Study 110 did not meet the primary objective. Additionally, the FDA noted the apparent decline in FEV 1 in the subgroup of pediatric patients but conveyed that with positive data in an enriched subgroup, current guidance would support extrapolation to the age range evaluated in Study 110 (ages 6 years and older) based on pharmacokinetic and safety data. After the pre-snda meeting, to obtain additional data to support the snda submission, Vertex conducted an interim analysis of Study 112, an ongoing, open-label study of ivacaftor that enrolled patients from Study 110. In Study 110, there was a 3- to 4-week washout period between the last dose of study drug (placebo or ivacaftor) and the follow-up visit before patients are enrolled to Study 112. The follow-up visit of Study 110 was the baseline visit for Study 112. There was an apparent on-off treatment effect observed in the washout period of
55 FDA Advisory Committee Briefing Materials Page 55 of 157 Study 110, and an off-on treatment effect demonstrated rapidly in Study 112, providing corroborating evidence to the results from Study 110. Based on a thorough understanding of the results from Study 110 and the interim analysis results of Study 112, Vertex considers Study 110 and 112 provide sufficient evidence to support approval of ivacaftor in the CF patients with an R117H mutation. Subsequently, an snda was filed in June 2014 to seek approval of the indication for the treatment of CF in patients age 18 years and older who have an R117H mutation in the CFTR gene. Under the breakthrough designation, Vertex continuously received constructive guidance from the Agency throughout ivacaftor development in the R117H population and during review of the snda. Additionally, as noted by the FDA during the pre-snda meeting, the ICH E11 guidance allows for efficacy extrapolation to pediatrics from adult data, when the drug product is used for the same indication (s) in adults and pediatric patients, the disease process is similar in adults and pediatric patients, and the outcome of therapy is likely to be comparable. These criteria are applicable in this case. The data from the R117H clinical program continued to be explored and examined carefully, particularly the pediatric data. Data exploration for the subgroup of pediatric patients revealed lack of a clinically meaningful negative effect on lung function in children, no evidence of a safety issue and a pharmacodynamic response as measured by sweat chloride. Therefore, in August 2014, Vertex amended the proposed indication to seek approval for the treatment of CF in patients age 6 years and older who have an R117H mutation in the CFTR gene. An Advisory Committee Meeting with Pulmonary-Allergy Drugs Advisory Committee (PADAC) was scheduled on 21 October 2014 to discuss this application.
56 FDA Advisory Committee Briefing Materials Page 56 of OVERVIEW OF CLINICAL STUDIES IN PATIENTS WITH R117H MUTATION Summary Two studies evaluated the efficacy and safety of ivacaftor in patients with the R117H mutation: Study 110, a double-blind, placebo-controlled study, and Study 112, an ongoing, open-label study in which Study 110 patients could enroll after participating in Study 110. Patients who enrolled in Study 112 had a 3- to 4-week washout period between the last dose of study drug in Study 110 and the first dose of ivacaftor in Study 112. Both studies used an ivacaftor dosage of 150 mg q12h, which is the recommended dosage for the currently approved mutations. Treatment in Studies 110 and Study 112 was in addition to the patient s usual prescribed CF therapy. Study 110 enrolled patients 6 years of age and older with an R117H mutation on at least one allele, a confirmed diagnosis of CF (chronic sinopulmonary disease and sweat chloride 60 mmol/l or 2 CF-causing mutations), and percent predicted FEV 1 of 40% to 105% (patients 6 to 11 years of age) and 40% to 90% (patients 12 years of age and older). The US study sites were accredited CFF Therapeutics Development Network trial centers. Randomization in Study 110 was stratified by age (6 to 11, 12 to 17, and 18 years) and percent predicted FEV 1 (<70%, 70% to 90%, and >90%), since these factors were anticipated to have an influence on the outcomes. The primary endpoint of Study 110 was the absolute change in percent predicted FEV 1 through Week 24 of treatment. Secondary endpoints were changes in BMI, sweat chloride concentrations, CFQ-R respiratory domain score, time to first pulmonary exacerbation, and safety. The Study 110 sample size was primarily driven by feasibility considerations in this rare population with an enrollment of a minimum of 40 to a maximum of 80 patients. Efficacy analyses were conducted using the Full Analysis Set (FAS), defined as all randomized patients who received at least one dose of study drug. The primary analysis for the primary efficacy variable was based on a mixed effects model for repeated measures (MMRM). The model included absolute change from baseline in percent predicted FEV 1 as the dependent variable, treatment, visit, and treatment-by-visit interaction as fixed effects, and patient as a random effect, with adjustment for the continuous baseline values of age and percent predicted FEV 1. Subgroup analyses were prespecified (without multiplicity adjustment).
57 FDA Advisory Committee Briefing Materials Page 57 of 157 As planned in the protocol, an interim analysis (IA) for safety and efficacy was done for DMC review after 40 patients completed the Week 8 Visit. Vertex clinical study personnel remained blinded to IA results. To control the overall type I error rate, a Bonferroni-type adjustment was applied. This reflected an allocated significance of for the IA. The significance level for the final analysis was set at because enrollment was not stopped after the IA. 8.1 Study Designs Two studies were conducted to evaluate ivacaftor in patients with an R117H-CFTR mutation: Study 110 and Study 112. A schematic of the designs of the studies is provided in Figure 18. Final results are available from Study 110. Interim analysis results are available from Study 112 (efficacy results through Week 12, and SAE data from the pharmacovigilance database). Both studies were conducted in the US and in the European Union (EU). Figure 18 Studies 110 and 112: Schematic of Study Designs Note: Study 112 also included an observational arm in which patients did not receive ivacaftor. Of the 67 Study 110 patients who enrolled in Study 112, 65 enrolled in the ivacaftor arm and 2 enrolled in the observational arm. Both studies used an ivacaftor dosage of 150 mg every 12 hours (q12h), which is the dose used in previous clinical studies in patients 6 years of age and older and is the recommended dosage in the USPI for patients 6 years of age and older. Treatment in Studies 110 and Study 112 was in addition to the patient s usual prescribed CF therapy (which was to remain stable throughout the study). Patients were first enrolled in Study 110, a prospectively randomized placebo-controlled study, and after completing Study 110, had the option to enroll in Study 112, an open-label study. Study 110 patients who completed their assigned duration of treatment in Study 110 were eligible to enroll in the ivacaftor arm of Study 112; other Study 110 patients were eligible to enroll in the observational arm of Study 112 in which patients would not receive ivacaftor or any other study drug. Of the 69 FAS patients in Study 110, 67 enrolled in Study 112: 65 patients in the ivacaftor arm, and 2 patients in the observational arm. The Study 112 interim analysis efficacy results include data from the ivacaftor arm (see Section 9.2) and SAE data from the ivacaftor and observational arms (see Section 10.2).
58 FDA Advisory Committee Briefing Materials Page 58 of 157 The Study 112 interim analysis included data for the 65 Study 110 patients enrolled in the ivacaftor arm, and took place after all ongoing patients from Study 110 who entered the ivacaftor arm completed the Week 12 visit. Study 110 had a 3- to 4-week washout period between the last dose of study drug (placebo or ivacaftor) and the follow-up visit. The follow-up visit of Study 110 was the baseline visit for Study 112. Therefore, patients were off all study drug for 3 to 4 weeks before their first dose of ivacaftor in Study 112. As a result, Study 112 provided an opportunity to re-establish an ivacaftor response in patients who had been treated with ivacaftor in Study 110 and to assess an ivacaftor response patients treated with placebo in Study 110. The US study sites (24 of the 26 sites with patients treated in Study 110) were accredited CFF Therapeutics Development Network trial centers. Key aspects of the study designs are summarized in Table 18. The duration of treatment in Study 110, ivacaftor dosage, and randomization ratio are the same as in Studies102 and 103, the pivotal Phase 3 studies of patients with the G551D mutation. (See Section 5.4 for additional information about those studies.) Table 18 Studies 110 and 112: Key Aspects of Study Designs Category Study 110 Study 112 Phase Phase 3 Phase 3 Design double-blind, placebo-controlled, parallel group open-label, ivacaftor treatment (the study also includes an observation arm but those data were not included in the interim analysis) Population 6 years of age and older; R117H mutation on at least one allele Patients enrolled in Study 110 a Duration of treatment 24 weeks last dose of study drug was 3 to 4 weeks before the Follow-up Visit; Follow-up visit of Study 110 was baseline visit for Study weeks (the snda included data from an interim analysis conducted at 12 weeks) Ivacaftor dosage 150 mg q12h 150 mg q12h Method of assigning patients to treatment groups Randomization; 1:1 ratio (placebo:ivacaftor) Ivacaftor arm: Patients who completed their assigned study drug treatment duration in Study 110. Observational arm: Patients who prematurely discontinued study drug treatment and received at least 4 weeks of treatment in Study 110; who completed Study 110 and chose to enroll in the observational arm; or who completed Study 110 but did not meet the inclusion criteria of the ivacaftor arm. Randomization stratification Stratified by age (6 to 11 years, 12 to 17 years, and 18 years) and percent predicted FEV 1 (<70%, 70% to 90%, and >90%). Not applicable Study sites 26 sites in the US EU b Patients from Study 110 enrolled at 24 sites in the US and the EU
59 FDA Advisory Committee Briefing Materials Page 59 of 157 Table 18 Studies 110 and 112: Key Aspects of Study Designs Category Study 110 Study 112 Study status Completed; final results available Ongoing; results from Week 12 interim analysis available a Study 112 is also enrolling patients from clinical studies of ivacaftor in patients with other CFTR mutations; however, data from those patients were not included in the interim analysis. b Study 110 had 27 sites that enrolled and randomized patients, and 26 sites with patients that were randomized and treated with study drug(placebo or ivacaftor). One patient was randomized to placebo but not dosed (the patient was randomized based on their percent predicted FEV 1 value at screening, but had a percent predicted value of 115% at baseline, and therefore was not dosed) Specific guidelines were provided for inhaled antibiotics to minimize confounding effects of concomitant use on the results of the study. For Study 110, patients who were taking inhaled hypertonic saline at the time of study entry should have remained on hypertonic saline through the Follow-up Visit; patients who were not taking inhaled hypertonic saline at the time of study entry should have remained off hypertonic saline through the Follow-up Visit. Use of hypertonic saline was allowed in Study Study Entry Criteria Study 110 was conducted in patients aged 6 years and older with a confirmed diagnosis of CF, the R117H-CFTR mutation on at least one allele, and FEV 1 40% predicted of normal for age, sex, and height by the Hankinson 73 or Wang 74 equations. Eligibility criteria were designed to enroll a population that was generally representative of the patient population and thus allowed for particularly well-preserved lung function in children. The principal inclusion criteria are provided in Table 19. The study enrolled only patients with FEV 1 equal to or more than 40% predicted because lower levels of lung function may have a significant component of irreversible lung structural damage (i.e., bronchiectasis) and because those patients are also more medically unstable. The upper limit of percent predicted FEV 1 was higher for patients 6 to 11 years of age (105%) than for patients 12 years of age and older (90%) to aid the recruitment of children. The criteria for diagnosis of CF and percent predicted FEV 1 are same as those used in the pivotal Phase 3 studies in patients with the G551D mutation Exclusion criteria were designed to decrease potential confounders of study endpoint evaluations and to align with criteria used in previous studies of ivacaftor. Table 19 Principal Entry Criteria of Study 110 Inclusion Criteria Confirmed diagnosis of CF 75 CFTR mutation Age Percent predicted FEV 1 chronic sinopulmonary disease AND sweat chloride value 60 mmol/l by quantitative pilocarpine iontophoresis or 2 CF-causing mutations (all as documented in the patient s medical record) R117H 6 years and older 40% to 105% (inclusive) for patients 6 to 11 years 40% to 90% (inclusive) for patients 12 years
60 FDA Advisory Committee Briefing Materials Page 60 of 157 Table 19 Principal Entry Criteria of Study 110 Exclusion Criteria CFTR mutation CF disease not stable G551D, G178R, G551S, S549N, S549R, G970R, G1244E, S1251N, S1255P, or G1349D An acute upper or lower respiratory infection, pulmonary exacerbation, or changes in therapy (including antibiotics) for pulmonary disease within 4 weeks before Day 1 (first dose of study drug) Colonization with organisms associated with a more rapid decline in pulmonary status (e.g., Burkholderia cenocepacia, Burkholderia dolosa, and Mycobacterium abscessus) at screening Notes: Hankinson 73 and Wang 74 equations were used to calculate percent predicted FEV 1. For male patients, the Wang standard was applied for patients 6 to 17 years of age, and the Hankinson standard was applied for patients 18 years and older. For female patients, the Wang standard was applied for patients 6 to 15 years of age, and the Hankinson standard was applied for patients 16 years and older. 8.3 Study Objectives and Endpoints The objectives and pre-specified primary and secondary endpoints for Studies 110 and 112 are provided in Table 20. In Study 110, efficacy assessments were done at baseline (before first dose of study drug), at Weeks 2, 4, 8, 16, and 24 of the treatment period, and at the follow-up visit (3 to 4 weeks after the last dose of study drug). In Study 112, efficacy assessments were done at baseline (i.e., follow-up visit of Study 110) and at Weeks 2 and 12 of the treatment period. Table 20 Studies 110 and 112: Objectives and Prespecified Primary and Secondary Endpoints Category Study 110 Study 112 Objectives Primary Evaluate the efficacy of ivacaftor in patients with CF who have the R117H-CFTR mutation To evaluate the safety of long-term ivacaftor treatment in patients with CF Secondary Evaluate the safety of ivacaftor in patients with CF who have the R117H-CFTR mutation To evaluate the efficacy of long-term ivacaftor treatment in patients with CF Endpoints Primary a Absolute change from baseline in percent predicted FEV 1 through Week 24 Secondary Change from baseline in BMI (rate of change over 24 weeks) at Week 24 Change from baseline in sweat chloride through Week 24 Change from baseline in the CFQ-R respiratory domain through Week 24 Time to first pulmonary exacerbation Safety, as determined by AEs, clinical laboratory values, electrocardiogram (ECG), ophthalmologic examinations, and vital signs Safety, as determined by AEs, clinical laboratory values, ECG, ophthalmologic examinations, and vital signs a Absolute change from baseline in percent predicted FEV 1 through Week 24 Change from baseline in sweat chloride Change from baseline in CFQ-R respiratory domain For the interim analysis included in the snda, the only safety data analyzed from Study 112 were SAEs.
61 FDA Advisory Committee Briefing Materials Page 61 of 157 According to regulatory guidance, FEV 1 is the recommended primary clinical endpoint in efficacy studies for CF 34 and chronic obstructive pulmonary disease. 35 Improvement in FEV 1 has served as the primary efficacy measure in definitive CF clinical studies, including those of ivacaftor. 76,77 As in previous Phase 3 studies of ivacaftor, the primary endpoint in Study 110 was absolute change in percent predicted FEV 1. Based on the response observed in Studies 102 and 103, a 24-week treatment period was selected for Study 110, although Studies 102 and 103 support that the effects of ivacaftor on sweat chloride, lung function, and other endpoint scan be seen as early as 2 weeks after the start of treatment. The CFQ-R is a CF-specific patient-reported-outcome (PRO) instrument that has been used as a primary endpoint for regulatory approval and was used in previous Phase 3 studies of ivacaftor. The CFQ-R respiratory domain includes questions about coughing, the presence of mucus, and ease of breathing. Scores range from 0 to 100, with higher scores indicating better health. A difference of 4 points in the respiratory domain score is considered the minimal clinically important difference (MCID). 81 A copy of the CFQ-R is provided in Appendix As in previous Phase 3 studies of ivacaftor, for efficacy analyses, a pulmonary exacerbation was defined in the protocol as a new or change in antibiotic therapy for any 4 or more signs or symptoms (e.g., change in sputum, new or increased hemoptysis, increased cough, increased dyspnea; sinus pain or tenderness, radiographic changes indicative of pulmonary infection). In Study 112, safety was the primary endpoint. Measures of efficacy including percent predicted FEV 1, sweat chloride response, and the CFQ-R respiratory domain score were secondary endpoints. 8.4 Data Monitoring Committee A data monitoring committee (DMC), independent of Vertex, conducted planned reviews of the study data. During the execution of the study there were two DMC reviews. The first was for safety which supported continued enrollment. The second review took place after 40 patients completed 8 weeks of treatment and was performed for safety and efficacy with a pre-specified stopping rule specified by Vertex in the event of strong efficacy results. Since the rule was not met, and there was no safety reason to halt the study, the DMC recommended continuing the study without any modifications. 8.5 Stopping of Study 110 About 6 weeks after the second DMC review, Vertex made the decision to stop the study. Vertex made this decision based on a number of factors, including study feasibility and timelines, while taking all necessary steps to ensure study integrity and patient protection. Enrollment at the high end of the prespecified range had been achieved, with a projection of at last 65 patients of the 40 to 80 planned to be randomized. In addition, the rate of enrollment had slowed considerably despite multiple efforts to extend patient recruitment. Notably, 70 patients randomized in the study represents about 15% of the size of the US population of patients 6 years of age and older who have the R117H mutation. Prior to the decision to stop enrollment, blinded review of data from the study was performed by a statistician not involved in study conduct to confirm that FEV 1 variability (without regard to treatment effect) was consistent with statistical powering assumptions. In addition,
62 FDA Advisory Committee Briefing Materials Page 62 of 157 blinded review of individual patient FEV 1 profiles indicated that FEV 1 patterns remained largely stable following 2 weeks on study drug. At the time the decision was made to stop the study, 6 of the 8 patients ultimately affected by the decision to stop the study (see below) were not yet randomized, so no data about these 6 patients was available. Eight patients were still enrolled in the study and receiving blinded study treatment at the time the study was stopped. All of these patients had received at least 2 weeks of study drug treatment in Study 110, and had at least one post-baseline FEV 1 measurement. These patients were given the opportunity to enroll in Study 112, the 2-year open-label study of ivacaftor, and all 8 patients made the decision to enroll in that study following a 3 to 4 week washout phase. An MMRM analysis, which is a standard statistical approach for handling missing data, was used as the primary analytical method for Study 110. Thus, the analysis of Study 110 included all available data from the study, including data from patients who did not complete a full 24 weeks of treatment. Of all the possible FEV 1 assessments that could be taken in Study 110, 94% were available for analysis. A Complete Case Set (CCS) analysis that excluded the patients who did not complete 24 weeks of treatment yielded comparable results to the Full Analysis Set (FAS) (see Section ). 8.6 Statistical Methods Study Sample Size The Study 110 sample size a minimum of 40 to a maximum of 80 patients was primarily driven by feasibility considerations in this rare population. Use of a range for the sample size is consistent with Study 111, the Phase 3 study in patients with non-g551d gating mutations (sample size for that study was a minimum of 20 and a maximum of 40 patients) Datasets Analyzed Full Analysis Set (FAS): The FAS was defined as all randomized patients who received at least 1 dose of study drug (placebo or ivacaftor). Patients were analyzed according to the study drug to which they were assigned. Complete Case Set (CCS): The CCS included all FAS patients who had the opportunity to complete the full 24-week treatment period. CCS analyses were performed for the primary and secondary endpoints to assess the effect of early termination of the study. Criteria used to assign patients to the CCS were determined before clinical data lock. Safety Set: The Safety Set included all patients who received at least 1 dose of study drug (placebo or ivacaftor) Statistical Tests Based on the results from Studies 102, 103, and 111, the effects of ivacaftor on FEV 1, sweat chloride concentrations, and CF-related respiratory symptoms were anticipated to be rapid in onset and sustained. Therefore, an MMRM, which analyzed data from all patients (including those who had less than 24 weeks of ivacaftor treatment) was used as the primary analysis method in Study 110. A linear mixed-effects model was used to determine the treatment difference in weight gain at 24 weeks.
63 FDA Advisory Committee Briefing Materials Page 63 of 157 As planned in the protocol, an interim analysis (IA) for safety and efficacy was carried out for DMC review after 40 patients completed the Week 8 Visit. Vertex clinical study personnel remained blinded to IA results. To control the overall type I error rate, a Bonferroni-type adjustment was applied. This reflected an allocated significance of for the IA. The significance level for the final analysis was set at as enrollment was not stopped after the IA. Because the treatment comparison for the primary analysis was not statistically significant, P-values for other analyses need to be interpreted with caution to avoid inflation of the Type I error. Nominal P-values for these analyses are presented because they are helpful in assessing the magnitude of the treatment difference relative to variability, but P-values of 0.05 or less should be viewed with caution when being considered as confirmatory evidence of treatment effect Primary Efficacy Variable (Percent Predicted FEV 1 ) Percent predicted FEV 1 is the ratio of FEV 1 (L) to the predicted FEV 1 (L), expressed as a percentage. Predicted FEV 1 (L) was calculated using the Hankinson 73 and Wang 74 standards. For male patients, the Wang standard was applied for patients 6 to 17 years of age, and the Hankinson standard was applied for patients 18 years and older. For female patients, the Wang standard was applied for patients 6 to 15 years of age, and the Hankinson standard was applied for patients 16 years and older. Hankinson Normal Values (HNVs) were calculated for FEV 1, FVC, FEF 25-75%, and 2 2 HNV b FEV 1 /FVC% using the equation: 0 b1 Age b2 Age b3 Height. Height is given in centimeters, age is given in years, and the coefficients b 0, b 1, b 2, and b 3 are determined based on patient s sex, race, and age group. Wang Normal Values (WNVs) were calculated for FEV 1, FVC, FEF 25-75%, and FEV 1 /FVC using the equation: WNV exp( ln(height)) WNV exp( ln( Height)). Height is given in meters, and the coefficients α and β are determined based on patient s sex, race, and age Primary Analysis of Primary Variable The primary analysis for the primary efficacy variable was based on a mixed-effects model for repeated measures (MMRM). 82 The model included absolute change from baseline in percent predicted FEV 1 as the dependent variable, treatment (ivacaftor versus placebo), visit (Week 2, Week 4, Week 8, Week 16, and Week 24), and treatment-by-visit interaction as fixed effects, and patient as a random effect, with adjustment for the continuous baseline values of age and percent predicted FEV 1. In the model, visit was treated as a class variable and a compound symmetry covariance matrix was assumed to model the within-patient variability. Denominator degrees of freedom for the F-test for fixed effects was estimated using the Kenward-Roger approximation. 83 With a mixed-effects model as the primary analysis model based on restricted maximum likelihood estimation and assuming conditional fixed and random effects, data were assumed missing at random and no imputation of missing data was carried out The main effect of treatment obtained from the model was interpreted as the average treatment difference (effect of ivacaftor) across all post-baseline visits. This was a weighted
64 FDA Advisory Committee Briefing Materials Page 64 of 157 average of the treatment difference across all post-baseline visits. The estimated mean treatment difference, a 95% confidence interval (CI), and a 2-sided P-value were provided. The consistency of treatment difference over different visits was evaluated using the above model. If there was evidence of a qualitative treatment-by-visit interaction, a descriptive summary of the treatment difference for each visit was to be used to identify the nature of the interaction Sensitivity Analyses The following sensitivity analyses of the primary variable were performed. Nonparametric analysis: Stratified Wilcoxon rank-sum test (Van Elteren test) on the mean change from baseline in percent predicted FEV 1, stratified by baseline values of age group ( 18 years of age, 12 to 17 years [inclusive], 6 to 11 years [inclusive]) and percent predicted FEV 1 (<70%, 70% to 90%, and >90%). If the number of patients in a stratum was less than 5 patients per treatment group, the stratum was collapsed with others to create meaningful comparison categories. With a mixed-effects model as the primary analysis model, no imputation of missing data was done. However, the following sensitivity analyses were conducted to assess the impact of missing efficacy evaluations on the treatment difference estimated through MMRM: Pattern mixture model (PMM): If there was more than 10% missing data in either treatment group, assessment of the effect of missing patterns on treatment difference and an overall treatment difference were obtained. Dropout reason-based multiple imputation: For patients who terminated from treatment before the end of the analysis period for any of the following reasons: AE, noncompliance with study procedures, death, physician decision, or required prohibited medication, missing measurements were imputed using a multiple imputation method. Complete data were analyzed using ANCOVA and MI ANALYZE; multiple-imputation was performed to remedy loss of variance information. The imputation distribution for the missing change in percent predicted FEV 1 from baseline at Week 24 was a normal distribution. All randomized patients were classified as Completer, Dropout Category 1, or Dropout Category 2, based on the following rules: o Completer: Patients completed 24 weeks treatment duration o Dropout Category 1: Patients discontinued treatment due to AEs, noncompliance with study requirements, death, physician decision, or requires prohibited medication. o Dropout Category 2: Patients discontinued treatment due to all other reasons, including study termination Complete Case Set Analyses Prespecified CCS analyses were conducted for the primary and key secondary endpoints to assess the impact of early stopping of the study, which resulted in 8 patients being unable to complete the full 24-week treatment period.
65 FDA Advisory Committee Briefing Materials Page 65 of Multiplicity Adjustment To ensure adequate control for the overall Type I error rate, a sequential procedure for testing both the primary endpoint and secondary endpoints was specified in the statistical analysis plan. The primary endpoint and key secondary endpoints were tested in sequence with α = : 1. Test 1: The primary efficacy endpoint will be tested at significance level α. 2. Test 2 : If a statistically significant result is obtained from Test 1, change from baseline in BMI at Week 24 and change from baseline in sweat chloride through Week 24 will be tested using Hochberg s step-up procedure at significance level α. 3. Test 3 : If a statistically significant result is obtained from Test 2, change from baseline in CFQ-R respiratory domain score through Week 24 and time-to-first pulmonary exacerbation will be tested using Hochberg s step-up procedure. Other analyses and testing of secondary efficacy endpoints were not controlled for Type I error Subgroup Analyses Subgroup analyses were prespecified (without multiplicity adjustment) to examine the consistency of treatment difference across subgroups. If an adequate sample size (i.e., 5 patients in both treatment groups) was available in any of the subgroups, a model-based analysis similar to that described for the primary analysis was conducted within the subgroup. Minimally, summary statistics were provided by treatment group at each visit. With the exception of the analysis by poly T variant, the subgroups were the same as those analyzed in previous Phase 3 studies of ivacaftor: age group at baseline ( 18 years, 12 to 17 years [inclusive], and 6 to 11 years [inclusive]) percent predicted FEV 1 at baseline (<70%, 70% to 90% [inclusive], and >90%) geographic region (North America and Europe) sex (Female and Male) P aeruginosa infection status at baseline (Yes [infected] and No [not infected]) R117H poly-t variant (5T, 7T, 9T) Ad Hoc Analyses Following database lock, ad hoc analyses were carried out to gain a better understanding of the main study results. These analyses were primarily focused on understanding any potential differences in results due to patient age, baseline percent predicted FEV 1, and R117H allele poly-t variant.
66 FDA Advisory Committee Briefing Materials Page 66 of Study 112 In the Study 112 Week 12 interim analysis, summary statistics and additional ad hoc analyses for evaluation of absolute change from baseline in percent predicted FEV 1 using the following methods, for the overall population, and patients aged 18 years and patients aged 6 to 11 years were conducted: Change from Study 112 baseline to Week 12 for the FAS using a one-sample t-test; Change from Study 112 baseline to Week 12 for patients who were treated with placebo in Study 110 (placebo/ivacaftor group) using a one-sample t-test; and Change from Study 112 baseline to Week 12 for patients who were treated with ivacaftor in Study 110 (ivacaftor/ivacaftor group) using a one-sample t-test. These endpoints were measured in an open-label setting and therefore are not directly comparable to the previously reported results. Summary statistics for sweat chloride concentrations and CFQ-R respiratory domain were calculated but no inferential analyses were performed because these outcomes had robust changes in the placebo-controlled comparison in Study 110.
67 FDA Advisory Committee Briefing Materials Page 67 of STUDY POPULATION AND EFFICACY RESULTS Summary Study 110 Patient Disposition The Study 110 FAS included 69 patients; 59 of these patients completed 24 weeks of treatment, 8 patients did not complete 8 weeks of treatment because the study was stopped by the sponsor, and 2 patients discontinued study drug treatment (1 due to noncompliance, 1 due to pregnancy). Patient Baseline Characteristics Of the 69 patients in the FAS, 50 (72.5%) were 18 years of age, 2 were 12 to 17 years of age, and 17 (24.6%) were 6 to 11 years of age. The sample size of 50 patients for the 18 year old subgroup exceeded the minimum sample size that had been defined for the entire study (40 patients). Baseline characteristics for the FAS were consistent with the known characteristics of the R117H patient population. The mean sweat chloride value was about 70 mmol/l; patients had well preserved BMIs (mean: 23.8 kg/m 2 ) and a high proportion were pancreatic sufficient as judged by a low incidence or pancreatic enzyme replacement therapy and by fecal elastase-1 measurements. The mean (SD) percent predicted FEV 1 was 72.9% (range: 32.5% to 105.5%). Pharmacokinetics Ivacaftor exposure in patients in Study 110 was consistent with exposure in previous clinical trials in other CF populations. Efficacy: FAS (69 patients) The result for the primary endpoint (treatment difference in absolute change in percent predicted FEV 1 from baseline through Week 24) for the FAS was 2.1 (95% CI: -1.1, 5.4), which failed to reach statistical significance (P=0.1979). Treatment differences favored ivacaftor at all treatment period time points. Substantial treatment differences were seen for the secondary endpoints of absolute change from baseline in sweat chloride concentrations (treatment difference: mmol/l; P<0.0001) and CFQ-R respiratory domain scores (treatment difference: 8.4 points; P=0.0091). The treatment difference for CFQ-R respiratory domain score was twice the MCID. The treatment difference for rate of change in BMI was 0.26 (P=0.7780), and the treatment difference for time-to-first pulmonary exacerbation (hazard ratio) was (P=0.8556). Efficacy: FAS Subgroups Percent predicted FEV 1 results showed a pattern of a more positive response to ivacaftor in patient subgroups with markers of more disease progression. Results differed between the age subgroups: the treatment difference favored ivacaftor in patients 18 years of age and favored placebo in patients 6 to 11 years of age. Due to these discrepant results, the data were explored thoroughly in the age subgroups.
68 FDA Advisory Committee Briefing Materials Page 68 of 157 Baseline sweat chloride levels were similar for the age subgroups, and sweat chloride results showed consistent, substantial changes for all subgroups, indicating that the differences in FEV 1 response were not driven by a difference in effect on CFTR function. The following characteristics were more common in patients 6 to 11 years of age than in patients 18 years of age: percent predicted FEV 1 >90%; P aeruginosa infection status: no (not infected); poly-t variant: 7T. Advances in newborn screening likely contributed to greater representation of the 7T poly-t variant in the pediatric subgroup since more individuals with an R117H-CFTR mutation are now identified earlier in life, often before the onset of advanced gastrointestinal or pulmonary manifestations. Baseline percent predicted FEV 1 was >90% in 1 of the 50 patients age 18 years and in 12 of the 17 patients aged 6 to 11 years. Efficacy: Patients 18 Years of Age (50 patients) The clinical benefit of ivacaftor in patients 18 years of age was demonstrated by the clinically relevant treatment difference for absolute change from baseline in percent predicted FEV 1 (5 percentage points; 95% CI: 1.1, 8.8; P=0.0119) and the secondary endpoints of absolute change from baseline in sweat chloride ( mmol/l; 95% CI: , -17.3; P<0.0001) and CFQ-R respiratory domain score (12.64 points; 95% CI: 5.02, ; P=0.0017). The treatment difference for CFQ-R respiratory domain score was more than 3 times the MCID. An FEV 1 responder analysis supports that patients benefited meaningfully from ivacaftor treatment: 54.2% of ivacaftor patients had an increase of at least 5 percentage points, compared with 15.4% of placebo patients. After the last dose of ivacaftor in Study 110, while treatment assignments were still blinded, percent predicted FEV 1 decreased substantially in ivacaftor-treated patients, providing further evidence of the effect of ivacaftor on lung function in patients 18 years of age. Measures of pulmonary exacerbations, including markers for more clinically severe events, favored ivacaftor. The totality of data in this subgroup, which comprised 72.5% of enrolled patients, supports the efficacy of ivacaftor in patients with the R117H mutation. The efficacy of ivacaftor treatment was further supported by results of Study 112 (described below). Efficacy: Patients 12 to 17 Years of Age (2 patients) One patient was randomized to placebo, and 1 patient was randomized to ivacaftor. The patient in the placebo group completed 24 weeks of treatment; the baseline percent predicted FEV 1 value was 88.7%, and the absolute change at Week 24 was 7.5 percentage points. The ivacaftor patient discontinued treatment after the Week 2 Visit because of noncompliance. At the Week 2 visit, there was no substantial change in percent predicted FEV 1, but the absolute change in sweat chloride was mmol/l. Efficacy: Patients 6 to 11 Years of Age (17 patients) In the small subgroup of patients 6 to 11 years of age, the treatment difference for the absolute change from baseline in percent predicted FEV 1 favored placebo (-6.3 percentage points; 95% CI: -12.0, -0.7; P=0.0301).
69 FDA Advisory Committee Briefing Materials Page 69 of 157 Sweat chloride concentrations showed a substantial treatment difference in favor of ivacaftor (-27.6 mmol/l, 95% CI: -37.2, -18.1; P<0.0001). CFQ-R respiratory domain score results favored placebo (treatment difference: points; 95% CI: , 3.41; P=0.1856); however, there was no consistent trend in the results across the treatment period time points. The treatment difference for rate of change in BMI was kg/m 2 (95% CI: , 2.014; P=0.8693). In both the placebo and ivacaftor treatment groups, the mean percent predicted FEV 1 was >93% at all time points. Detailed analysis and review of data in this small subgroup of 17 patients, 9 of whom were treated with ivacaftor, led to the conclusion that ivacaftor had a lack of effect on FEV 1 rather than a negative effect, and that the results do not represent a clinically relevant signal: o o o o o baseline percent predicted FEV 1 values were normal (ivacaftor group mean baseline value: 97.5%), which made improvements in percent predicted FEV 1 challenging to demonstrate although there were numerical changes in percent predicted FEV 1 values during the treatment period, intra-patient values were variable both before and after dosing within what is generally a normal range of pulmonary function the treatment difference favoring placebo was due to an increase in percent predicted FEV1 values in the placebo group (LS mean change of 3.5 percentage points) combined with a modest decrease in the ivacaftor group (LS mean change of -2.8 percentage points) the sample size of the population was very small, and as a consequence, the effect of outliers was magnified there were no trends in AEs or other evidence of the FEV 1 decline in the ivacaftor group being associated with a safety signal In addition, as described below, data from Study 112 did not replicate the negative effect of ivacaftor in patients 6 to 11 years of age Study 112 Of the 69 FAS patients in Study 110, 65 patients enrolled in the ivacaftor arm of Study 112, and 64 of these patients completed 12 weeks of ivacaftor treatment in Study 112. The baseline value for the Study 112 efficacy analyses was the Day 1 Visit for Study 112, which was also the Follow-up Visit for Study 110. Patients had their last dose of study drug (ivacaftor or placebo) 3 to 4 weeks before this visit. After the start of ivacaftor treatment, both the placebo/ivacaftor and ivacaftor/ivacaftor groups (i.e., patients treated with placebo in Study 110 and patients treated with ivacaftor in Study 110) had clinically relevant and statistically significant treatment responses for absolute change from baseline in percent predicted FEV 1. For the population overall, the mean change from baseline was 5.45 percentage points (P< for within-group comparison).
70 FDA Advisory Committee Briefing Materials Page 70 of 157 In patients 18 years of age, results for the absolute change from baseline in percent predicted FEV 1 were closely comparable to results for this group of patients in Study 110, both for patients in the placebo/ivacaftor group mean change from baseline: 5.5 percentage points; P=0.0016) and for patients in the ivacaftor/ivacaftor group (mean change from baseline: 4.7 percentage points; P=0.0036). In patients 6 to 11 years of age, the mean overall absolute change in percent predicted FEV1 from baseline to Week 12 was 6.5 percentage points (P = ). For patients treated with placebo in Study 110, the mean change from baseline at Week 12 was 3.6 percentage points; for patients treated with ivacaftor in Study 110, the mean change from baseline was 9.8 percentage points. The 9.8 percentage point difference was driven by the patient who a pulmonary exacerbation SAE in Study 110 and whose percent predicted FEV 1 value increased to the Study 110 baseline value during treatment with ivacaftor in Study 112. Therefore Study 112 provided supportive evidence of the efficacy of ivacaftor treatment in adults and did not show a negative effect of ivacaftor on percent predicted FEV 1 values in patients 6 to 11 years of age. 9.1 Study Patient Disposition A total of 108 patients were screened, and 70 of these patients were enrolled and randomized in a 1:1 ratio to placebo or ivacaftor treatment. Of the 70 randomized patients, 69 received at least 1 dose of study drug and were included in the FAS. One patient was randomized to placebo but not dosed (the patient was randomized based on their percent predicted FEV 1 value at screening, but had a percent predicted value of 115% at baseline, and therefore was not dosed). Patient disposition data for the FAS are presented in Figure 19. All patients, including the 8 patients who did not have the opportunity to complete 24 weeks of treatment, were included in the Study 110 FAS and contributed to the MMRM efficacy analyses. In Study 110, 94% of the planned spirometry assessments from baseline through Week 24 were obtained and analyzed (390 of the 414 planned spirometry data assessments). * In Study 112, 99% of the planned spirometry assessments from baseline through Week 12 were obtained and analyzed (192 of the 195 planned spirometry assessments). * Study 110: 69 patients, each with 6 scheduled assessments (baseline and Weeks 2, 4, 8, 16, and 24) = 414; Study 112: 65 patients, each with 2 scheduled assessments (baseline and Weeks 1 and 12) = 195.
71 FDA Advisory Committee Briefing Materials Page 71 of 157 Figure 19 Study 110: Patient Disposition a Discontinuations: 1 ivacaftor patient discontinued at week 2 due to noncompliance and 1 ivacaftor patient discontinued between weeks 16 and 24 because of pregnancy. b Eight patients did not complete 24 weeks of treatment because the study was terminated early by the sponsor. For these 8 patients, the last Treatment Period study visit was Week 2 for 2 patients, Week 4 for 1 patient, Week 8 for 3 patients, and Week 16 for 2 patients. These patients were considered to have completed their assigned treatment duration, and all 8 enrolled in the ivacaftor arm of Study Demographic and Baseline Characteristics Demographic and baseline characteristics of patients in Study 110 were consistent with registry data and published literature (see Section 4). The mean sweat chloride value was about 70 mmol/l. Patients had well-preserved BMIs (mean overall: 23.8 kg/m 2 ) and a high proportion were pancreatic sufficient as assessed by a low rate of pancreatic enzyme replacement therapy use (pancreatin: 11.6%; pancrelipase: 5.8%) and a high rate of fecal elastase μg/g (87.0%). The inter-patient variability for these measures was large, as would be expected for a mutation with varying clinical consequences. Of the 69 patients in the FAS, 50 (72%) were 18 years of age, 2 were 12 to 17 years of age, and 17 (25%) were 6 to 11 years of age. Of the 2 patients 12 to 17 years of age, the placebo patient completed the study and the ivacaftor patient discontinued at Week 2 due to noncompliance. The sample size of 50 patients for the 18 year old subgroup exceeded the minimum sample size that had been defined for the entire study (40 patients). Fifteen of the 17 patients 6 to 11 years of age were from the US, and 37 of 50 patients 18 years old from the US. Baseline percent predicted FEV 1 and BMI were slightly higher in the ivacaftor group than in the placebo group, and baseline sweat chloride and P aeruginosa infection rate were slightly lower for the ivacaftor group than the placebo group. The R117H-5T variant was more prevalent in the placebo group (placebo: 27 of 34 patients; ivacaftor: 21 of 33 patients).
72 FDA Advisory Committee Briefing Materials Page 72 of 157 To assess the potential imbalance among key baseline parameters, a logistic regression analysis with stepwise model selection was used. Region was found to be imbalanced (P-value = ) and the poly-t status may have been slightly imbalanced (P-value=0.0585), while the other parameters (age, sex, baseline percent predicted FEV 1, baseline BMI, baseline sweat chloride, baseline CFQ-R, baseline fecal elastase-1 and P aeruginosa infection status at baseline) were not found to be imbalanced. Fisher s exact test was also used to assess the imbalance of poly-t status and region, and the results were not significant at 0.05 significance level. * Table 21 Study 110: Demographics and Baseline Characteristics, Full Analysis Set Variable Region, n (%) Placebo N = 35 Ivacaftor N = 34 Overall N = 69 United States 30 (85.7) 24 (70.6) 54 (78.3) Europe 5 (14.3) 10 (29.4) 15 (21.7) Sex, n (%) Male 15 (42.9) 15 (44.1) 30 (43.5) Female 20 (57.1) 19 (55.9) 39 (56.5) Race, n (%) White 35 (100.0) 34 (100.0) 69 (100.0) Age (years) N Mean Standard deviation Median Minimum Maximum Age Group (years), n (%) 6 to 11 (inclusive) 8 (22.9) 9 (26.5) 17 (24.6) 12 to 17 (inclusive) 1 (2.9) 1 (2.9) 2 (2.9) (74.3) 24 (70.6) 50 (72.5) * To address the potential imbalance of the poly-t status and region, the primary efficacy endpoint was analyzed using an MMRM similar to the primary model plus the poly-t status and region as additional covariates. The estimate of the treatment difference was 2.27 (95% CI: -1.12, 5.66) which is consistent with the primary analysis outcome (see Section ).
73 FDA Advisory Committee Briefing Materials Page 73 of 157 Table 21 Study 110: Demographics and Baseline Characteristics, Full Analysis Set Variable CFTR Poly-T Variant a, n 5T on R117H allele Placebo N = 35 Ivacaftor N = 34 5T/5T T/7T Overall N = 69 5T/9T T on R117H allele 7T/5T T/7T T/9T Sweat Chloride (mmol/l) N Mean Standard deviation Median Minimum Maximum Percent Predicted FEV 1 N Mean Standard deviation Median Minimum Maximum Percent Predicted FEV 1, n (%) <70% 15 (42.9) 13 (38.2) 28 (40.6) 70% to 90% 14 (40.0) 14 (41.2) 28 (40.6) >90% 6 (17.1) 7 (20.6) 13 (18.8) BMI (kg/m 2 ) N Mean Standard deviation Median Minimum Maximum P aeruginosa Infection Status, n (%) Yes 19 (54.3) 15 (44.1) 34 (49.3) No 16 (45.7) 19 (55.9) 35 (50.7)
74 FDA Advisory Committee Briefing Materials Page 74 of 157 Table 21 Study 110: Demographics and Baseline Characteristics, Full Analysis Set Variable Fecal Elastase-1, n (%) Placebo N = 35 Ivacaftor N = 34 Overall N = 69 <200 µg/g 5 (14.3) 2 (5.9) 7 (10.1) 200 µg/g 28 (80.0) 32 (94.1) 60 (87.0) Missing 2 (5.7) -- 2 (2.9) Notes: All results displayed are Baseline results. Baseline was defined as the most recent measurement before intake of the first dose of study drug. Baseline sweat chloride was the average of Run-in and Day 1. BMI: Body Mass Index = Weight/(Height*Height) (kg/m2). Weight-for-age z-score and BMI-for-age z-score were calculated by using National Center for Health Statistics (NCHS) growth charts. Z-scores were defined as missing if the patient is over 240 months old at the time of assessment. a The poly-t variant on the R117H allele was derived for 15 patients where this information was missing and the patient had either R117H/F508DEL or R117H/R117H. Subsequent to the use of this derivation, all patients with F508del were confirmed by long-range PCR to have the 9T variant, validating the method of derivation. The most commonly reported concomitant medications were for management of CF complications. Use of concomitant medications by at least 15% of patients while receiving placebo or ivacaftor was similar with the exceptions of paracetamol (placebo: 37.1%; ivacaftor: 11.8%), pancreatin (placebo: 20.0%; ivacaftor: 2.9%), and salbutamol (placebo: 80.0%; ivacaftor: 64.7%). Table in Appendix summarizes concomitant medications received by at least 15% of patients while receiving placebo or ivacaftor Pharmacokinetics A population PK model was successfully developed based on the prior model for ivacaftor and incorporating data from Study 110. Body weight was the covariate that most influenced the apparent (oral) clearance (CL/F) of ivacaftor, consistent with the previous model. Gender and patient status (CF versus healthy subjects) did not account for variability in ivacaftor PK in a clinically meaningful manner. Age was also not a clinically important covariate after accounting for body size. Ivacaftor CL/F was reduced 21% for patients with the R117H-CFTR mutation relative to the non-r117h CF population (including patients with other mutations that cause gating defects and F508del homozygotes). However, this difference in the CL/F estimate should be interpreted with caution, because data for the R117H patients came from a single study, and therefore factors such as study design and inherent inter-study variability may contribute to the difference in CL/F. Ivacaftor exposure in patients in Study 110 was consistent with exposure in previous clinical trials in other CF populations.
75 FDA Advisory Committee Briefing Materials Page 75 of 157 Figure 20 Ivacaftor Exposure (C min ) by Age for Patient With the R117H Mutation (Study 110) or With CFTR Mutations That Cause Severe Gating Defects (Studies 102, 103, and 111) C min : minimum observed concentration *Includes CFTR mutations G551D, G178R, G551S, G549N, S549R, G970R, G1244E, S1251N, S1255P, G1349D Efficacy: Full Analysis Set Primary Efficacy Endpoint Results for the primary endpoint (the absolute change from baseline in percent predicted FEV 1 through Week 24) failed to reach statistical significance (Table 22). While not achieving statistical significance, treatment differences favored ivacaftor at all treatment period time points. The gains seen in percent predicted FEV 1 for the ivacaftor group during the treatment period reversed in the follow-up period when the patients were no longer receiving ivacaftor, providing some evidence of a positive treatment effect (Figure 21).
76 FDA Advisory Committee Briefing Materials Page 76 of 157 Table 22 Study 110: Absolute Change From Baseline in Percent Predicted FEV 1 by MMRM, Full Analysis Set Absolute Change Treatment Difference Visit or Time Treatment Sample Statistics From Baseline a (Ivacaftor vs Placebo) Period Group N Mean N LS Mean Difference (95% CI) P value Baseline Placebo Ivacaftor Overall Placebo Post-baseline Ivacaftor (-1.1, 5.4) LS Mean: least squares mean Note: Sample statistics are unadjusted results. Mean values are percentages. Absolute change from baseline values and treatment difference values are percentage points. Treatment difference is ivacaftor placebo. A positive difference favors ivacaftor. a Estimates were obtained from MMRM with absolute change from baseline as the dependent variable; with treatment group, categorical visit (Weeks 2, 4, 8, 16, and 24) and treatment by visit interaction as fixed effects; with patient as a random effect; and with adjustment for the continuous baseline value of age and percent predicted FEV 1 using compound symmetry covariance matrix. Sensitivity Analysis of Primary Efficacy Variable To assess the robustness of the primary analyses, three sensitivity analyses were conducted as described in Section The stratified Wilcoxon rank sum test was used to detect the treatment difference if the underlying normality assumption was not met. Both ANCOVA model with missing data imputed using multiple imputation and pattern mixture model were carried out to assess treatment difference by considering the impact of missing data. Results of the sensitivity analyses were consistent with the results of the primary analysis (Table in Section ). The absolute change from baseline was greater for the ivacaftor group than the placebo group for all analyses, but was not statistically significant. Complete Case Set Analysis of Primary Efficacy Variable Results of the CCS analyses were consistent with results of the FAS analyses: the treatment difference for percent predicted FEV 1 for the CCS was 2.7 (95% CI: -0.4, 5.8; P=0.0875), and as described above, the treatment difference for the FAS was 2.1 percentage points (95% CI: -1.1, 5.4; P = ). The difference between the CCS and FAS results was driven by notable pulmonary exacerbations that occurred in 3 of the 8 patients who were excluded from the CCS (but included in the FAS) Secondary Efficacy Endpoints Table 23 shows FAS results for secondary efficacy endpoints. Ivacaftor treatment effects were seen for the secondary endpoints of absolute change from baseline in sweat chloride concentrations and CFQ-R respiratory domain scores. The change in sweat chloride was rapid and sustained, consistent with previous experience in other populations. The magnitude of the treatment difference for sweat chloride was not as large as that achieved with the G551D mutation; however, given the difference in baseline levels for the G551D and R117H populations (mean values of about 100 mmol/l and 70 mmol/l, respectively), sweat chloride concentrations were similar for the two populations during ivacaftor treatment.
77 FDA Advisory Committee Briefing Materials Page 77 of 157 The treatment difference for change from baseline in the CFQ-R respiratory domain score (8.4 points) exceeded the MCID (4 points). 81 A responder analysis of the relative percentage of patients who attained the MCID in CFQ-R respiratory domain score of 4 points revealed that 41.2% of ivacaftor patients versus 28.6% of placebo patients achieved this meaningful level of improvement. The result for rate of change in BMI (treatment difference 0.26; P=0.7780) was not unexpected given the generally preserved pancreatic status of the study population as judged by the high BMIs and based on pancreatic enzyme use/fecal elastase levels. Similarly, it is not surprising that no strong pulmonary exacerbation signal was seen in this small population of patients with the R117H mutation, which has a relatively low rate of pulmonary exacerbations during a 24-week period. Table 23 Study 110: Secondary Efficacy Endpoints; Full Analysis Set Sample Statistics Absolute Change From Baseline Treatment Difference (Ivacaftor vs Placebo) Visit or Time Period Treatment Difference Group N Mean N LS Mean (95% CI) P value Absolute Change From Baseline in Sweat Chloride (mmol/l) by MMRM Baseline Placebo Ivacaftor Overall Post-baseline Placebo Ivacaftor (-28.0, -19.9) < Rate of Change From Baseline in BMI (kg/m 2 ) by LMM a Baseline Placebo Ivacaftor Week 24 Placebo Ivacaftor (-1.57, 2.10) Absolute Change From Baseline in Pooled CFQ-R Respiratory Domain Score (points) by MMRM b Baseline Placebo Ivacaftor Overall Post-baseline Placebo Ivacaftor (2.2,14.6) Pulmonary Exacerbations: Time to First (Hazard Ratio) Placebo 35 Not applicable Ivacaftor 34 Not applicable (hazard ratio) Note: Sample statistics are unadjusted results. Difference is Ivacaftor Placebo. A negative difference in sweat chloride favors ivacaftor. Positives differences in BMI and CFQ-R respiratory domain favor ivacaftor. Estimated hazard ratio between ivacaftor and placebo of a value <1 favors ivacaftor. LS Mean: least squares mean a P value for the treatment difference is from the slope of BMI (kg/m 2 ) versus time (days). b CFQ-R results are pooled results (all questionnaire versions except for the Parent/Caregiver version). Figures of the results for percent predicted FEV 1, sweat chloride, and CFQ-R respiratory domain, and rate of change in BMI are shown in Figure 21. Figure 13-1 in Appendix shows the Kaplan-Meier plot of time-to-first pulmonary exacerbation for the FAS.






 Sweat")

78 FDA Advisory Committee Briefing Materials Page 78 of 157 Figure 21 Study 110: Absolute Change in Percent Predicted FEV 1, Sweat Chloride, Rate of change in BMI, and CFQ-R Respiratory Domain Score; Full Analysis Set A) Percent Predicted FEV 1 B) Sweat Chloride C) BMI D) CFQ-R Respiratory Domain Score
79 FDA Advisory Committee Briefing Materials Page 79 of 157 The treatment difference for absolute change from baseline in FEV 1 was 97 ml (P=0.0632) (Table 24), which is very close to the clinically relevant treatment effect for chronic obstructive pulmonary disease proposed by Cazzole et al. 84 (100 to140 ml). Table 24 Study 110: Absolute Change in FEV 1 (L); Full Analysis Set Sample Statistics Absolute Change From Baseline a Treatment Difference (Ivacaftor vs Placebo) Visit or Time Period Treatment Difference Group N Mean N LS Mean (95% CI) P value Baseline Placebo Ivacaftor Overall Post-baseline Placebo Ivacaftor (-0.006, 0.200) Note: Sample statistics are unadjusted results. Difference is Ivacaftor Placebo. A positive difference favors ivacaftor. LS Mean: least squares mean a Estimates were obtained from MMRM with dependent variable absolute change from baseline, with treatment group, categorical visit (Weeks 2, 4, 8, 16, and 24) and treatment by visit interaction as fixed effects, patient as random effect, and with adjustment for the continuous baseline value of age and FEV 1, using compound symmetry covariance matrix. Although there was no significant difference in time-to-first pulmonary exacerbation (Table 23), there was a trend toward less severe pulmonary exacerbations with ivacaftor treatment. The ivacaftor group also had fewer AEs and SAEs of infective pulmonary exacerbations of CF than the placebo group (see Section 10.1). Because all pulmonary exacerbations that met the protocol-defined criteria occurred in patients 18 years of age, these data are summarized in Section (efficacy endpoint results for patients 18 years of age) Tertiary Efficacy Endpoints Absolute changes from baseline in concentrations and log-transformed concentrations of inflammatory mediators (leukocytes, CRP, IgG, and IL-8) were tertiary endpoints. Generally, the decrease in inflammatory mediator concentrations was greater for the ivacaftor group than for the placebo group (Table in Appendix ) Efficacy: Full Analysis Set Subgroups Overview of Subgroup Results To further understand the FAS results, analyses of subgroups were reviewed (age, sex, geographic region, percent predicted FEV 1 at baseline, P aeruginosa infection status at baseline, and poly-t variant). The subgroup analyses were prespecified and included in the statistical analysis plan, and with the exception of poly-t variant and P. aeruginosa infection status, are standard subgroup analyses conducted for all Phase 3 studies of ivacaftor. Percent predicted FEV 1 results (Figure 22) showed a pattern of a more positive response to ivacaftor in patients with the markers of more disease progression (lower percent predicted FEV 1, presence of an R117H-5T allele). The most striking difference in percent predicted FEV 1 response was for the age subgroups: the treatment difference favored ivacaftor in the subgroup of patients 18 years of age and
 were in the 12 to 17 year old stratum.")
80 FDA Advisory Committee Briefing Materials Page 80 of 157 favored placebo in patients 6 to 11 years of age. The treatment-by-age interaction was significant (P=0.0076). Only 2 patients (one in each treatment arm) were in the 12 to 17 year old stratum. Due to discrepant results in patients 6 to 11 years versus patients 18 years, the data were explored thoroughly in these subgroups. Figure 22 Study 110: Absolute Change in Percent Predicted FEV 1 from Baseline Through Week 24, by MMRM; FAS Subgroups Note: Estimates were obtained from MMRM with dependent variable absolute change from baseline, with treatment, visit, status (geographic region, sex, age, percent predicted FEV1, P aeruginosa infection status; or poly T variant), treatment-by-visit interaction, and treatment-by-status interaction as fixed effects, patient as a random effect adjusted for the continuous baseline values of age and percent predicted FEV 1, using a compound symmetry covariance matrix. a P-value is from the main treatment difference. Analysis of ivacaftor exposure showed that appropriate exposures were obtained in patients 6 to 11 years of age and in patients 18 years of age (Figure 20). Sweat chloride results showed consistent, substantial changes for all subgroups, indicating that ivacaftor potentiated CFTR activity in all subgroups (Figure 23), indicating that the differences in FEV 1 response were not driven by a lack of effect on CFTR function.


81 FDA Advisory Committee Briefing Materials Page 81 of 157 Figure 23 Study 110: Absolute Change in Sweat Chloride from Baseline Through Week 24; FAS Subgroups Additional results of subgroup analyses are provided in supplemental tables in Appendix (percent predicted FEV 1 : Table 13-52; sweat chloride: Table 13-53; CFQ-R respiratory domain score: Table 13-54) Subgroup Baseline Characteristics To further evaluate the efficacy results, baseline disease characteristics of age subgroups and poly-t variant subgroups were reviewed (Table 25). Baseline sweat chloride was similar across the subgroups. However, differences in lung function were observed, with patients 6 to 11 years of age having higher percent predicted FEV 1 values than older patients. The R117H patients 6 to 11 years of age had relatively well-preserved lung function at baseline (mean percent predicted FEV 1 values of 94.0% for the placebo arm and 97.5% for the ivacaftor arm). This is not surprising for patients with the R117H mutation, in whom disease progresses with age, and where despite symptoms, patients can still have very well preserved airflow. However, as described below, additional factors may have led to the pediatric population having a more favorable prognosis, and potentially being less sensitive to a therapeutic intervention. Therefore it could be very challenging to demonstrate an effect on FEV 1 in the 6 to 11 year old subgroup, particularly given the small sample size (9 patients treated with ivacaftor). Patients with the 7T variant had higher percent predicted FEV 1 values than patients with the 5T variant, consistent with the known effect of these polymorphisms.
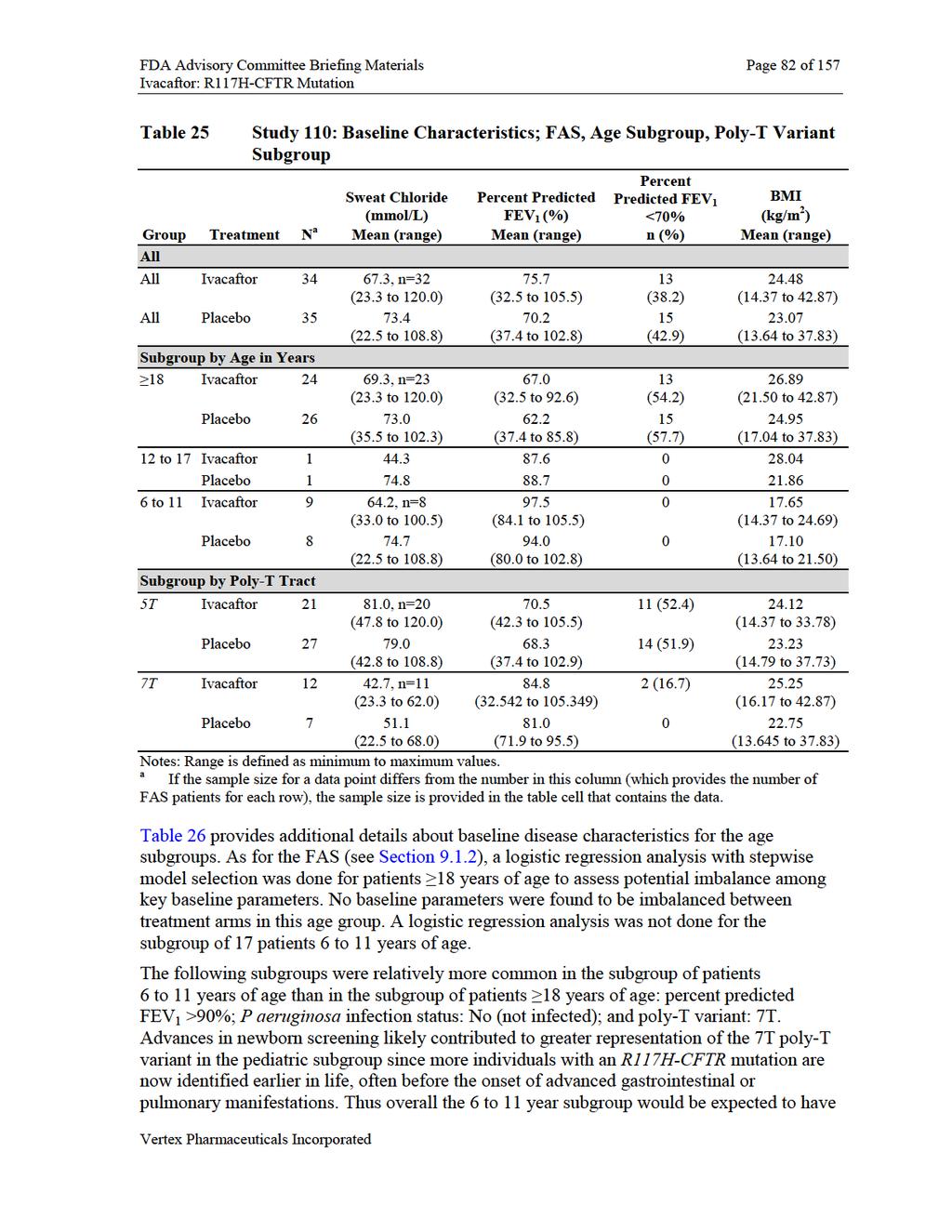
82
83 FDA Advisory Committee Briefing Materials Page 83 of 157 a less active disease profile than the subgroup of patients 18 years of age, where the proportion of R117H-7T patients was substantially lower (10 out of 50 patients). Table 26 Variable Study 110: Baseline Disease Characteristics, Age Subgroups FAS: All Ages N = 69 FAS: 6 to 11 Yr N=17 FAS: 12 to 17 Yr N=2 FAS: 18 Yr N=50 Percent Predicted FEV 1 N Mean Not determined 64.5 Standard deviation Not determined 14.9 Median Not determined 66.5 Minimum Maximum Percent Predicted FEV 1, n (%) <70% 28 (40.6) (56.0) 70% to 90% 28 (40.6) 5 (29.4) 2 (100.0) 21 (42.0) >90% 13 (18.8) 12 (70.6) 0 1 (2.0) P aeruginosa Infection Status, n (%) Yes 34 (49.3) 2 (11.8) 0 32 (64.0) No 35 (50.7) 15 (88.2) 2 (100.0) 18 (36.0) Fecal Elastase-1, n (%) <200 µg/g 7 (10.1) (14.0) 200 µg/g 60 (87.0) 16 (94.1) 2 (100.0) 42 (84.0) Missing 2 (2.9) 1 (5.9) 0 1 (2.0) CFTR Poly-T Variant a, n 5T on R117H allele T/5T T/7T T/9T T on R117H allele T/5T T/7T T/9T Notes: All results displayed are Baseline results. Baseline was defined as the most recent measurement before intake of the first dose of study drug. Baseline sweat chloride was the average of Run-in and Day 1. BMI: Body Mass Index = Weight/(Height*Height) (kg/m2). Weight-for-age z-score and BMI-for-age z-score were calculated by using National Center for Health Statistics (NCHS) growth charts. Z-scores were defined as missing if the patient is over 240 months old at the time of assessment. a The poly-t variant for the R117H allele was derived for patients where this information was missing and the patient had either R117H/F508DEL or R117H/R117H (Study 110 CSR/Section ) While entry criteria required all patients to have CF, the entry criterion for upper limit of percent predicted FEV 1 for patients 6 to 11 years of age (105%) was higher than that for patients 12 years of age (90%). The difference in entry criteria for percent predicted FEV 1, combined with the progression of CF in the R117H patient population, contributed to a heterogeneous study population in which CF disease was more advanced in older patients than in younger patients.
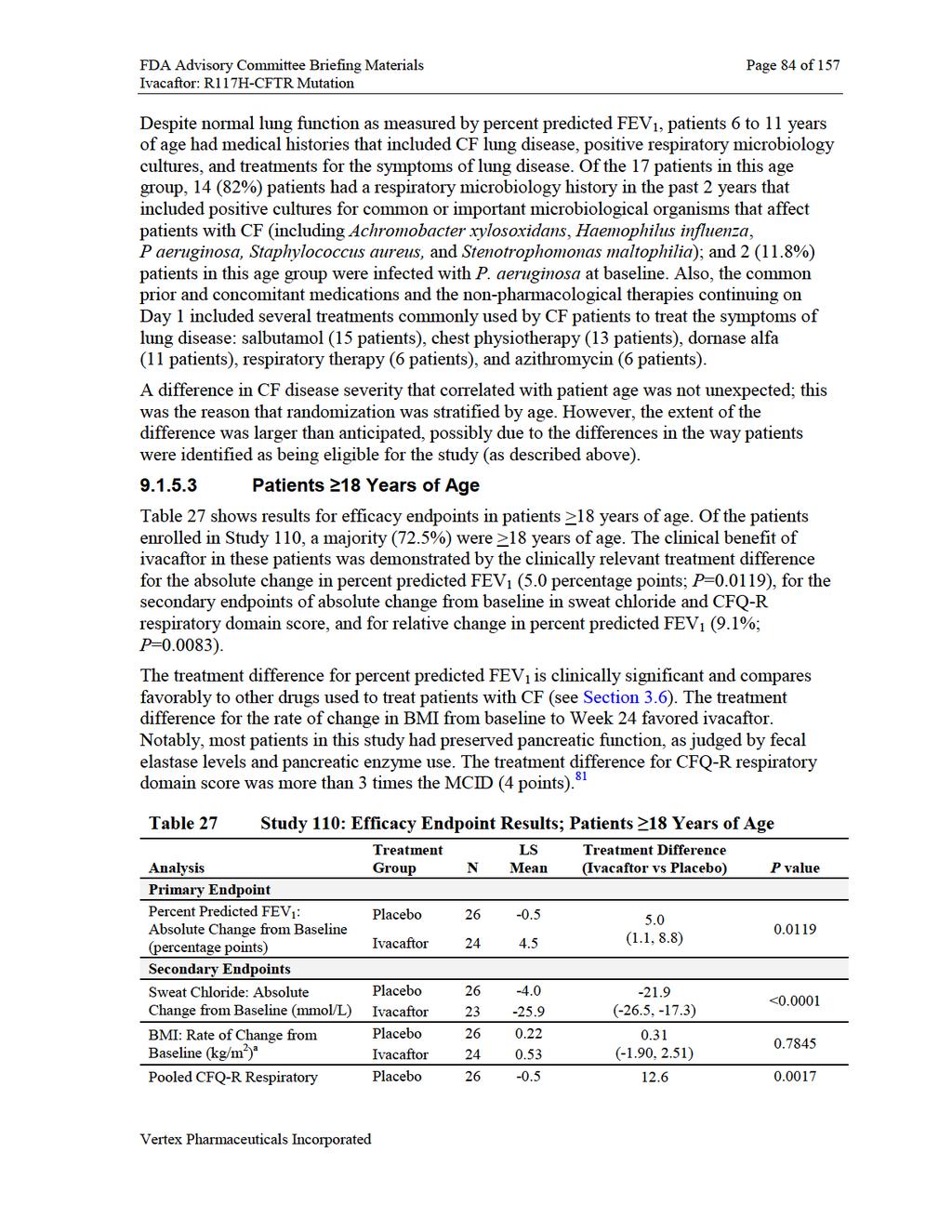
84
85

 Absolute")

86 FDA Advisory Committee Briefing Materials Page 86 of 157 Figure 24 Study 110: Absolute Change in Percent Predicted FEV 1 ; Patients 18 Years of Age A) Absolute Change from Baseline B) Responder Analysis of Absolute Change from Baseline Through Week 24
 (Table 28), which is more than the clinically relevant treatment effect for COPD proposed by Cazzole et al. 84 (100 to 140 ml).")
 P value Baseline Placebo 26 2.164 Ivacaftor 24 2.440 Overall Post-baseline Placebo 26 2.178 26-0.014 0.168 Ivacaftor 24 2.610 24 0.154 (0.034, 0.302) 0.")
87 FDA Advisory Committee Briefing Materials Page 87 of 157 The treatment difference for absolute change from baseline in FEV 1 was 168 ml (P=0.0153) (Table 28), which is more than the clinically relevant treatment effect for COPD proposed by Cazzole et al. 84 (100 to 140 ml). Table 28 Study 110: Absolute Change in FEV 1 (L); Patients 18 Years of Age Sample Statistics Absolute Change From Baseline a Treatment Difference (Ivacaftor vs Placebo) Visit or Time Period Treatment Difference Group N Mean N LS Mean (95% CI) P value Baseline Placebo Ivacaftor Overall Post-baseline Placebo Ivacaftor (0.034, 0.302) Note: Sample statistics are unadjusted results. Difference is Ivacaftor Placebo. A positive difference favors ivacaftor. LS Mean: least squares mean a Estimates were obtained from MMRM with dependent variable absolute change from baseline, with treatment group, categorical visit (Weeks 2, 4, 8, 16, and 24) and treatment by visit interaction as fixed effects, patient as random effect, and with adjustment for the continuous baseline value of age and FEV 1, using compound symmetry covariance matrix. The absolute change from baseline in the CFQ-R respiratory domain score showed a clear treatment difference (Figure 25), and the treatment difference through Week 24 was triple the MCID. Figure 25 Study 110: Absolute Change in CFQ-R Respiratory Domain Score; Patients 18 Years of Age
88 FDA Advisory Committee Briefing Materials Page 88 of 157 The low number of patients with pulmonary exacerbations precluded inferential statistical analysis of time-to-first pulmonary exacerbation for the subgroup of patients age 18 years. However, all protocol-defined pulmonary exacerbations occurred in patients 18 years of age *, and measures of pulmonary exacerbations, including markers for more clinically severe events numerically favored ivacaftor (Table 29). In addition, the ivacaftor group had fewer pulmonary exacerbation AEs and SAEs than the placebo group (see Section ). Table 29 Study 110: Pulmonary Exacerbation Incidence and Event Rates; Patients 18 Years of Age Parameter Statistic Placebo N=26 Ivacaftor N=24 Duration in study Total days in study All pulmonary exacerbations Patients with events Events (event rate) 17 (0.748) 13 (0.556) Requiring hospitalization Patients with events 6 2 Events 7 2 Requiring IV antibiotic therapy Patients with events 6 2 Events 8 2 Notes: Estimates were obtained from negative binomial regression with the number of events as the dependent variable, treatment as fixed effects, and adjustments for baseline percent predicted FEV 1 and age, with log (time on study) a an offset. Negative binomial regression was conducted only when the number of patients with events in each treatment group was 5 and the models converged. Pulmonary exacerbation includes events that met the protocol definition of pulmonary exacerbations (treatment with new or changed antibiotic therapy for 4 sinopulmonary signs/symptoms). * The pulmonary exacerbation SAE in the pediatric patient that was associated with a decline of 26 percentage points in percent predicted FEV 1 did not meet the protocol-defined criteria for pulmonary exacerbation (a new or change in antibiotic therapy for 4 specified signs/symptoms; see Section 8.3 for explanation of criteria).
.")
89 FDA Advisory Committee Briefing Materials Page 89 of 157 Ivacaftor treatment resulted in consistent and substantial improvements over placebo for the absolute change in percent predicted FEV 1 in patients age 18 years of age, regardless of disease severity, sex, geographic region, and P aeruginosa infection status at baseline (Figure 26). Figure 26 Study 110: Treatment Difference in Mean Absolute Change from Baseline in Percent Predicted FEV 1 Through Week 24 by Subpopulations, Full Analysis Set, Patients 18 Years of Age Note: A positive treatment different favors ivacaftor. Analysis of the >90% predicted subgroup was not performed as there was only 1 patient in this subgroup. The treatment difference in absolute change from baseline in percent predicted FEV 1 for patients 18 years of age with R117H-5T was 5.9 percentage points (P = ). An MMRM analysis conducted for the 10 patients 18 years of age who had R117H-7T did not show an overall post-baseline treatment difference (0.04 percentage points, P = ). However, a waterfall plot analysis of individual patient responses at Week 24 suggests that some patients with R117H-7T may have responded to ivacaftor treatment (Figure 27 and Figure 28).
90 FDA Advisory Committee Briefing Materials Page 90 of 157 Figure 27 Study 110: Waterfall Plot of Absolute Change from Baseline at Week 24 in Percent Predicted FEV 1 for Patients 18 Years of Age Receiving Ivacaftor: R117H-5T Versus R117H-7T 25 5 T ( N = 1 6 ) 7 T ( N = 4 ) A b s o l u t e C h a n g e ( % ) Figure 28 Study 110: Waterfall Plot of Absolute Change from Baseline at Week 24 in Percent Predicted FEV 1 for Patients 18 Years of Age With R117H-7T A b s o l u t e C h a n g e ( % ) P la c e b o ( N = 4 ) Iv a c a fto r ( N = 4 )
91
92



 Percent Predicted FEV 1 B)")
93 FDA Advisory Committee Briefing Materials Page 93 of 157 Figure 29 Study 110: Absolute Change From Baseline in Percent Predicted FEV 1 and CFQ-R Respiratory Domain Score; Patients 6 to 11 Years A) Percent Predicted FEV 1 B) CFQ-R Respiratory Domain
94 FDA Advisory Committee Briefing Materials Page 94 of 157 The treatment difference for absolute change from baseline in FEV 1 was -69 ml (P=0.2381) (Table 28). Table 31 Study 110: Absolute Change in FEV 1 (L); Patients 6 to 11 Years of Age Sample Statistics Absolute Change From Baseline a Treatment Difference (Ivacaftor vs Placebo) Visit or Time Period Treatment Difference Group N Mean N LS Mean (95% CI) P value Baseline Placebo Ivacaftor Overall Post-baseline Placebo Ivacaftor (-0.189, 0.052) Note: Sample statistics are unadjusted results. Difference is Ivacaftor Placebo. A negative difference favors ivacaftor. LS Mean: least squares mean a Estimates were obtained from MMRM with dependent variable absolute change from baseline, with treatment group, categorical visit (Weeks 2, 4, 8, 16, and 24) and treatment by visit interaction as fixed effects, patient as random effect, and with adjustment for the continuous baseline value of age and FEV 1, using compound symmetry covariance matrix. Data for 6 to 11 year old patients were thoroughly reviewed and analyzed to evaluate possible reasons for the FEV 1 results, both at the level of individual patients and for the overall subgroup. Detailed review of data in this subgroup of 17 patients led to the conclusion that ivacaftor had a lack of effect on FEV 1 rather than a negative effect, and that the results do not represent a clinically relevant signal: baseline percent predicted FEV 1 values were normal (ivacaftor group mean baseline value: 97.5%; see Table 25), which made improvements in percent predicted FEV 1 challenging to demonstrate although there were numerical changes in percent predicted FEV 1 values during the treatment period, intra-patient values were variable both before and after dosing within what is generally a normal range of pulmonary function (see Figure 30) the treatment difference favoring placebo was due to an increase in percent predicted FEV 1 values in the placebo group (LS mean change of 3.5 percentage points) combined with a modest decrease in the ivacaftor group (LS mean change of -2.8 percentage points) the sample size of the population was very small, and as a consequence, the effect of outliers was magnified there were no trends in AEs or other evidence of the FEV 1 decrease in the ivacaftor group being associated with a safety signal Additional details about the percent predicted FEV 1 results in patients 6 to 11 years of age are provided below. Percent predicted FEV 1 increased in the placebo group: Individual patient percent predicted FEV 1 data were reviewed (values over time; change from baseline over time: Figure 30). The data suggest an increase in the placebo group during the first few weeks of treatment that was sustained through the 24 weeks of treatment. The placebo response observed in patients age
.")

95 FDA Advisory Committee Briefing Materials Page 95 of to 11 years old is different from that seen for placebo-treated patients in previous ivacaftor studies, even those performed in children (e.g., see Figure 17). The decrease in percent predicted FEV 1 in the ivacaftor group was driven by a patient with a pulmonary exacerbation SAE and minor decreases or stable values in other patients: Although the placebo response drove much of the observed differences in the pediatric population, the ivacaftor treated patients did have very modest falls in percent predicted FEV 1. And as mentioned above, 1 patient in the ivacaftor group had a substantial decline in percent predicted FEV 1 at Week 16 (26 percentage points) that coincided with an SAE of pulmonary exacerbation (see Figure 30). This patient remained on ivacaftor and had another substantial decline in FEV 1 during the follow-up period (47 percentage points). The patient enrolled in the ivacaftor arm of Study 112, and his FEV 1 returned to baseline during ivacaftor treatment in Study 112. The next worse response in the 6 to 11 year old subgroup in Study 110 was a patient who had a baseline of percent predicted and an average of percent predicted postdose, ending at percent predicted at Week 24. Aside from these 2 patients, all other 6 to 11 year old patients had less than a 5 percentage point relative change (comparing postdose average to baseline), and 3 patients had average percent predicted FEV 1 values >100% during the 24-week treatment period. Figure 30 Study 110: Individual Patient Results for Absolute Change from Baseline in Percent Predicted FEV 1 ; Full Analysis Set, Patients 6 to 11 Years of Age Variability in FEV 1 values before start of study drug dosing may have affected results: Comparison of percent predicted FEV 1 values at Screening and Day 1 (Baseline) shows that in the placebo group, many patients had a decrease in percent predicted FEV 1 between Screening and Baseline, and a number of ivacaftor patients had an increase in percent predicted FEV 1 between Screening and Baseline (Figure 31 and Table 32).
 Patient Treatment Group Screening Baseline (Day 1)")

96 FDA Advisory Committee Briefing Materials Page 96 of 157 Figure 31 Study 110: Individual Patient Results for Percent Predicted FEV 1 at Screening, Run-In, and Baseline; Patients 6 to 11 Years of Age Table 32 Study 110: Percent Predicted FEV 1 Values at Screening, Day 1, and Week 24; Full Analysis Set, Patients 6 to 11 Years of Age (Inclusive) Patient Treatment Group Screening Baseline (Day 1) Week 24 1 Placebo Placebo Placebo Placebo Placebo Not available 6 Placebo Placebo Placebo Ivacaftor Ivacaftor Ivacaftor Ivacaftor Not available 13 Ivacaftor Ivacaftor Ivacaftor Ivacaftor Not available 17 Ivacaftor Note: "Not available" indicates the patient did not complete 24 weeks of treatment.
97 FDA Advisory Committee Briefing Materials Page 97 of 157 Based on the observed changes in between screening and baseline, an analysis was done to evaluate the absolute change in percent predicted FEV 1 from screening (instead of from baseline) (Table 33). In this analysis, no treatment difference with a P-value of <0.05 was found at any time point, including overall post-baseline. Therefore, the changes between the screening visit and baseline (Day 1) appeared to contribute to the observed treatment difference in the primary endpoint in patients 6 to 11 years of age. Table 33 Study 110: Absolute Change From Screening in Percent Predicted FEV 1 by MMRM; Full Analysis Set, Patients 6 to 11 Years of Age Absolute Change Treatment Difference Visit or Time Treatment Sample Statistics From Baseline a (Ivacaftor vs Placebo) Period Group N Mean N LS Mean Difference (95% CI) P value b Screening Placebo Ivacaftor Week 2 Placebo Ivacaftor (-13.6, 2.1) Week 4 Placebo Ivacaftor (-13.8, 2.1) Week 8 Placebo Ivacaftor (-9.4, 6.8) Week 16 Placebo Ivacaftor (-12.2, 4.0) Week 24 Placebo Ivacaftor (-12.5, 3.9) Overall Placebo Post-Baseline Ivacaftor (-11.3, 2.8) Note: Sample statistics are unadjusted results. Difference is ivacaftor placebo. A positive difference favors ivacaftor. LS Mean: least squares mean a Estimates were obtained from MMRM with absolute change from screening as the dependent variable; with treatment, categorical visit (Weeks 2, 4, 8, 16, and 24), and treatment by visit interaction as fixed effects; with patient as a random effect; and with adjustment for the continuous baseline value of percent predicted FEV 1 using compound symmetry covariance matrix. b P value for Overall Post-baseline is from the main treatment difference; P values at individual visits are from linear contrasts between the 2 treatments effects at the given visit. FEV 1 trends not associated with AEs or safety concerns: An in-depth review of AEs in 6 to11 year olds was conducted, with a particular focus on respiratory AEs. There were no AEs in 6 to 11 year old patients to suggest the presence of bronchospasm, nor were there other events that would suggest a clinically significant adverse effect of ivacaftor. See Section 10.1 for further information about the safety results in Study 110. A broader review of the totality of pediatric experience with ivacaftor has never suggested any evidence for a pulmonary tolerability concern overall, nor more specifically in the 6 to 11 year age group. Conclusion: Analysis and review of individual patient efficacy and safety data led to the conclusion that the results do not represent a clinically relevant signal. Results of Study 112 also support this conclusion (see Section ).


98 FDA Advisory Committee Briefing Materials Page 98 of 157 Potentially, because of the slower disease progression and because lung function had not yet substantially declined in the 6 to 11 year old patients, an improvement in lung function was not detected with spirometry. However, having shown that ivacaftor does improve CFTR function in patients 6 to 11 years of age, as evidenced by the sweat chloride results, there is a biologic and mechanistic rationale for concluding that a patient in this age group who has more advanced disease or has suffered a decline in lung function would benefit from ivacaftor treatment, just as the adult patients have. 9.2 Study Patient Disposition Patients who completed their assigned study drug treatment in Study 110 were offered the opportunity to enroll in the open-label treatment arm of Study 112, where they would receive ivacaftor. This section of the document presents interim analysis results for these patients through Week 12 of ivacaftor treatment. Of the 69 FAS patients in Study 110, 65 enrolled in the ivacaftor arm of Study 112. The population in Study 112 is therefore a suitably representative group and not a biased group of good responders. In the description of Study112 results, placebo/ivacaftor refers to patients treated with placebo in Study 110, and ivacaftor/ivacaftor refers to patients treated with ivacaftor in Study 110. Of the 65 patients enrolled in the ivacaftor arm of Study 112, 64 patients completed at least 12 weeks of treatment in Study 112, and 1 patient (in the ivacaftor/ivacaftor group) discontinued between Week 2 and 12 because she was moving to a different country. Figure 32 Study 112 Ivacaftor Arm: Patient Disposition Through Week 12 a One patient refused further dosing with ivacaftor in Study 112 because she was moving to a different country.
99 FDA Advisory Committee Briefing Materials Page 99 of Demographics and Baseline Characteristics Given that 65 of the 67 eligible patients from Study 110 enrolled in the ivacaftor arm of Study 112, the Study 112 FAS demographic and baseline characteristics were comparable to those in Study 110. A summary of demographic data and baseline characteristics is provided in Table I Appendix For the FAS in Study 112, mean baseline percent predicted FEV 1 values were comparable for the placebo/ivacaftor and ivacaftor/ivacaftor groups; baseline sweat chloride levels were lower in the ivacaftor/ivacaftor group than in the placebo/ivacaftor group Efficacy The baseline value was the Day 1 Visit for Study 112, which was also the Follow-up Visit for Study 110. Patients took their last dose of study drug (ivacaftor or placebo) 3 to 4 weeks before this visit Full Analysis Set Both the placebo/ivacaftor and ivacaftor/ivacaftor groups had a clinically relevant and statistically significant treatment response in the FAS primary endpoint (absolute change from baseline in percent predicted FEV 1 ) (Table 34). For the overall population, the mean change from baseline to Week 12 was 5.5 percentage points (P<0.0001; within-group comparison). The slight difference in results between the placebo/ivacaftor and ivacaftor/ivacaftor groups (absolute change at Week 12 of 5.0 percentage points versus 6.0 percentage points) was driven by the ivacaftor/ivacaftor patient who had a decrease in percent predicted FEV 1 associated with a pulmonary exacerbation SAE in Study 110 and whose values returned to Study 110 baseline levels during ivacaftor treatment in Study 112. Table 34 Study 112: Absolute Change from Baseline to Week 2 and Week 12 in Percent Predicted FEV 1, Full Analysis Set Study Population Study 112 Visit N Mean Change from Baseline P Value a (Within Group) Overall Week Week < Placebo/Ivacaftor Week Week Ivacaftor/Ivacaftor Week Week Notes: Baseline was defined as the most recent measurement before intake of the first dose of study drug in Study 112. This measurement was taken at the Day 1 Visit for Study 112, which was also the Follow-up Visit of Study 110, and which occurred 3 to 4 weeks after the last dose of study drug in Study 110. a P values are based on the one-sample t-test. The washout period between the end of study drug dosing in Study 110 and the start of ivacaftor dosing in Study 112 allowed evaluation of the effect of stopping and re-starting ivacaftor treatment (on-off-on effect). During this washout period, Study 110 treatment assignments were still blinded. In patients who had been treated with ivacaftor in Study 110, FEV 1 levels decreased between Week 24 and the follow-up visit (when ivacaftor treatment was stopped), and then increased again when ivacaftor treatment was resumed in Study 112 (Figure 33), providing additional
, and the magnitude and time course of response was")
100 FDA Advisory Committee Briefing Materials Page 100 of 157 evidence of the effect of ivacaftor on percent predicted FEV 1. Patients who had been treated with placebo in Study 110 showed an increase in FEV 1 when ivacaftor treatment was started in Study 112 (Figure 33), and the magnitude and time course of response was similar to that of patients treated with ivacaftor in Study 110. Figure 33 Study 110 and 112: Absolute Change in Percent Predicted FEV 1, FAS Note: Data are observed means. Absolute change from baseline was calculated using the Study 110 baseline value. Absolute change from baseline in percent predicted FEV 1, sweat chloride, and CFQ-R respiratory domain showed substantial improvements during ivacaftor treatment in both groups (Table 35).
101 FDA Advisory Committee Briefing Materials Page 101 of 157 Table 35 Study 112: Results for Efficacy Endpoints: Mean (SD) Changes from Study 112 Baseline, Full Analysis Set Study Placebo/Ivacaftor Ivacaftor/Ivacaftor Overall Visit N Mean (SD) N Mean (SD) N Mean (SD) Week (6.7) (9.4) (8.0) Endpoint Percent Predicted FEV 1: Absolute Change from Baseline (percentage points) Week (7.7) (10.4) (8.9) Sweat Chloride: Week (9.1) (12.3) (10.7) Absolute Change from Baseline (mmol/l) a CFQ-R Respiratory Week (19.2) (15.7) (17.9) Domain Score: Absolute Change from Week (14.0) (21.4) (18.0) Baseline (points) b SD: standard deviation Notes: Baseline was defined as the most recent measurement before intake of the first dose of study drug in Study 112. This measurement was taken at the Day 1 Visit for Study 112, which was also the Follow-up Visit of Study 110, and which occurred 3 to 4 weeks after the last dose of study drug in Study 110. a Sweat chloride was only collected at the Baseline and the Week 2 Visit. b Pooled was defined as all questionnaire versions except for the parent/caregiver version Patients 18 Years of Age The results of Study 112 for patients 18 years of age are closely comparable to results for this age group of patients in Study 110. There was a clinically relevant and statistically significant treatment response for percent predicted FEV 1 in patients 18 years of age for both the placebo/ivacaftor and ivacaftor/ivacaftor groups, and the magnitude of the increase at Week 12 was about 5 percentage points for both groups (Table 36). Table 36 Study 112: Absolute Change in Percent Predicted FEV 1 from Study 112 Baseline; Full Analysis Set, 18 Years of Age Study Population Study 112 Visit N Mean Change from Baseline P Value a (Within Group) Overall Week < Week < Placebo/Ivacaftor Week Week Ivacaftor/Ivacaftor Week Week Notes: Baseline was defined as the most recent measurement before intake of the first dose of study drug in Study 112. This measurement was taken at the Day 1 Visit for Study 112, which was also the Follow-up Visit of Study 110, and which occurred 3 to 4 weeks after the last dose of study drug in Study 110. Age is the baseline age in Study 110. a P values are based on the one-sample t-test. In addition, absolute change from baseline in sweat chloride and absolute change from baseline in CFQ-R respiratory domain score showed substantial improvements during ivacaftor treatment in both the placebo/ivacaftor and ivacaftor/ivacaftor groups (statistical
102 FDA Advisory Committee Briefing Materials Page 102 of 157 testing was not conducted on these assessments). Summary statistics for the efficacy endpoints are shown in Table 37. Table 37 Study 112: Results for Efficacy Endpoints: Mean (SD) Changes from Study 112 Baseline, Full Analysis Set, Patients 18 Years of Age Study Placebo/Ivacaftor Ivacaftor/Ivacaftor Overall Visit N Mean (SD) N Mean (SD) N Mean (SD) Week (7.0) (4.6) (6.0) Endpoint Percent Predicted FEV 1: Absolute Change from Baseline Week (7.9) (6.4) (7.2) (percentage points) Sweat Chloride: Week (8.7) (11.5) (10.2) Absolute Change from Baseline (mmol/l) a CFQ-R Respiratory Week (21.3) (15.8) (18.9) Domain Score: Absolute Change from Week (14.5) (22.7) (18.6) Baseline (points) b SD: standard deviation Notes: Baseline is defined as the most recent measurement before the first dose of study drug in Study 112. This measurement was taken at the Day 1 Visit for Study 112, which was also the Follow-up Visit of Study 110, and which occurred 3 to 4 weeks after the last dose of study drug in Study 110. Age is the baseline age in Study 110. a b Sweat chloride was only collected at the Baseline and the Week 2 Visit. All patients 18 years of age used the Adolescents and Adults version of the CFQ-R. Figure 34A shows the absolute change in percent predicted FEV 1 in Studies 110 and 112 for patients 18 years of age, and Figure 34B shows the absolute change in CFQ-R respiratory domain score in Studies 110 and 112 for patients 18 years of age. After the last dose of study drug in Study 110, while treatment assignments were still blinded, percent predicted FEV 1 decreased substantially in ivacaftor-treated patients, providing further evidence of the treatment effect of ivacaftor on lung function in patients 18 years of age. During ivacaftor treatment in Study 112, both groups of patients those treated with placebo in Study 110 and those treated with ivacaftor in Study 110 had increases in percent predicted FEV 1 by Week 2 of treatment. The increase at Week 12 in the ivacaftor/ivacaftor group was consistent with the FEV 1 value at Week 24 in Study 110, and the increase in the placebo/ivacaftor group, who were newly exposed to ivacaftor, was similar to the increase in the ivacaftor/ivacaftor treated patients. CFQ-R respiratory domain scores followed the same pattern as the FEV 1 results: values decreased in ivacaftor-treated patients in Study 110, after the last dose of study drug (when treatment assignments were still blinded), values decreased in patients in the ivacaftor/ivacaftor group. During ivacaftor treatment in Study 112, both ivacaftor/ivacaftor and placebo/ivacaftor groups had increases in CFQ-R respiratory domain scores.

 Percent Predicted FEV 1 B) CFQ-R")

103 FDA Advisory Committee Briefing Materials Page 103 of 157 Figure 34 Studies 110 and 112: Absolute Change in Percent Predicted FEV 1 and CFQ-R Respiratory Domain Score, Patients 18 Years of Age A) Percent Predicted FEV 1 B) CFQ-R Respiratory Domain Score Note: Data are observed means. Absolute change from baseline was calculated using the Study 110 baseline value.
104 FDA Advisory Committee Briefing Materials Page 104 of Patients 12 to 17 Years of Age The 17-year-old patient who was in the placebo group in Study 110 enrolled in the ivacaftor arm of Study 112. In Study 112, the patient s sweat chloride concentrations decreased and percent predicted FEV 1 levels increased (Table 38). Table 38 Study 112: Efficacy Results; Patient in 12 to 17 Year Old Age Group Percent Predicted CFQ-R Respiratory Sweat Chloride Study 112 Time Point FEV 1 Domain Score (Points) (mmol/l) Baseline Week Week Notes: Baseline was defined as the most recent measurement before intake of the first dose of study drug in Study 112. This measurement was taken at the Day 1 Visit for Study 112, which was also the Follow-up Visit of Study 110, and which occurred 3 to 4 weeks after the last dose of study drug in Study Patients 6 to 11 Years of Age Statistical result for the absolute change from baseline in percent predicted FEV 1 for patients 6 to 11 years of age are presented in Table 39. The mean overall absolute change in percent predicted FEV 1 from baseline to Week 12 in patients 6 to 11 years of age was 6.5 percentage points (P = ). The mean absolute change in percent predicted FEV 1 from baseline to Week 12 was 3.6 percentage points for the placebo/ivacaftor group and 9.8 percentage points for the ivacaftor/ivacaftor group. The difference between the groups was driven by the patient in the ivacaftor/ivacaftor group who had a substantial decline in percent predicted FEV 1 during Study 110 that coincided with an SAE of pulmonary exacerbation (discussed in Section ). This patient resumed ivacaftor treatment, and percent predicted FEV 1 values returned to baseline during Study 112, driving the larger response observed in the ivacaftor/ivacaftor group compared to the placebo/ivacaftor group. This patient also had a similar effect on the CFQ-R respiratory domain results. To evaluate the effect of this patient on the FEV 1 results, the Study 112 data were reanalyzed with this patient excluded (Figure 13-3 in Appendix ). The results showed a mean change from baseline to Week 12 of 3.4 percentage points (P<0.0567). Table 39 Study 112: Absolute Change from Study 112 Baseline in Percent Predicted FEV 1, Full Analysis Set, Patients 6 to 11 Years of Age Study Population Study 112 Visit N Mean Change from Baseline P Value a (Within Group) Overall Week Week Placebo/Ivacaftor Week Week Ivacaftor/Ivacaftor Week Week Notes: Baseline was defined as the most recent measurement before intake of the first dose of study drug in Study 112. This measurement was taken at the Day 1 Visit for Study 112, which was also the Follow-up Visit of Study 110, and which occurred 3 to 4 weeks after the last dose of study drug in Study 110. Age is the baseline age in Study 110.
105 FDA Advisory Committee Briefing Materials Page 105 of 157 Table 39 Study 112: Absolute Change from Study 112 Baseline in Percent Predicted FEV 1, Full Analysis Set, Patients 6 to 11 Years of Age Study Population Study 112 Visit N Mean Change from Baseline P Value a (Within Group) a P values are based on the one-sample t-test. Summary statistics for the efficacy endpoints are shown in Table 37. Treatment with ivacaftor resulted in a substantial reduction in sweat chloride concentration in both the placebo/ivacaftor and the ivacaftor/ivacaftor groups. Table 40 Study 112: Results for Efficacy Endpoints: Mean (SD) Changes from Study 112 Baseline, Full Analysis Set, 6 to 11 Years of Age Study Placebo/Ivacaftor Ivacaftor/Ivacaftor Overall Visit N Mean (SD) N Mean (SD) N Mean (SD) Week (2.0) (17.6) (13.0) Endpoint Percent Predicted FEV 1: Absolute Change from Baseline Week (7.8) (17.9) (13.3) (percentage points) Sweat Chloride: Week (9.9) (12.3) (10.6) Absolute Change from Baseline (mmol/l) a CFQ-R Respiratory Week (12.9) (14.8) (15.3) Domain Score: Absolute Change from Week (11.3) (17.8) (16.9) Baseline (points) b SD: standard deviation Notes: Baseline was defined as the most recent measurement before intake of the first dose of study drug in Study 112. This measurement was taken at the Day 1 Visit for Study 112, which was also the Follow-up Visit of Study 110, and which occurred 3 to 4 weeks after the last dose of study drug in Study 110. Age is the baseline age in Study 110. a b Sweat chloride was only collected at the Baseline and the Week 2 Visit. Pooled was defined as all questionnaire versions except for the parent/caregiver version. Figure 35 shows the absolute change in percent predicted FEV 1 for Studies 110 and 112 for patients 6 to 11 years of age.

106 FDA Advisory Committee Briefing Materials Page 106 of 157 Figure 35 Studies 110 and 112: Absolute Change in Percent Predicted FEV 1, Patients 6 to 11 Years of Age Note: Data are observed means. Absolute change from baseline was calculated using the Study 110 baseline value. Percent predicted FEV 1 results for individual patients, including the screening and run-in values in Study 110, are shown in Figure 36. The Study 112 results support the conclusions for Study 112 that FEV 1 values were variable within a generally normal range of pulmonary function.

107 FDA Advisory Committee Briefing Materials Page 107 of 157 Figure 36 Studies 110 and 112: Individual Patient Results for Percent Predicted FEV 1 ; Patients 6 to 11 Years of Age
108 FDA Advisory Committee Briefing Materials Page 108 of SAFETY Summary The safety profile of patients age 6 years and older with the R117H mutation was comparable to that observed in prior ivacaftor Phase 2b/3studies and post-marketing experience. The incidence of AEs considered related to study drug, incidence of SAEs, and incidence of AEs leading to study drug interruption were lower for ivacaftor-treated patients than for placebo-treated patients. There were no deaths and no AEs that led to study drug discontinuation. AEs for which the incidence was at least 5 percentage points higher with ivacaftor than placebo treatment were nasal congestion, oropharyngeal pain, abdominal pain, wheezing, upper airway cough syndrome, bacterial disease carrier, influenza-like illness, and abdominal discomfort. The most common SAE in both treatment groups was infective pulmonary exacerbation of CF; the incidence was higher in the placebo group than in the ivacaftor group. There were no clinically relevant differences in safety in patients 6 to 11 years of age compared with patients 18 years of age. Results for clinical laboratory parameters (serum chemistry, hematology, coagulation studies), vital signs, physical examinations, and electrocardiograms (ECGs) showed minor differences between the ivacaftor and placebo groups that were not considered to be clinically meaningful. SAE data are available from ongoing Study 112; 8 of the 65 patients had an SAE, and the most common SAE was infective pulmonary exacerbation of CF Study Summary of Adverse Events Overall, the safety profile of patients age 6 years and older with the R117H mutation was similar to that observed in prior ivacaftor Phase 2b/3studies and post-marketing experience (see Section 5.4.2). Ivacaftor appeared to be very well-tolerated in patients with the R117H mutation, with no new safety signals apparent. The incidence of AEs considered related to study drug, incidence of SAEs, and incidence of AEs leading to study drug interruption were lower in the ivacaftor-treated patients than in placebo-treated patients (Table 41). All SAEs were considered by the investigator to be not related to the study drug. There were no deaths and no AEs events that led to study drug discontinuation.
109 FDA Advisory Committee Briefing Materials Page 109 of 157 Table 41 Study 110: Summary of Adverse Event Incidence, Safety Set Placebo (N = 35) n (%) Ivacaftor (N = 34) n (%) Patients With At least 1 AE 35 (100.0) 32 (94.1) At least 1 related AE 7 (20.0) 3 (8.8) At least 1 AE leading to death 0 0 At least 1 related AE leading to death 0 0 At least 1 SAE 6 (17.1) 4 (11.8) At least 1 severe (grade 3) AE 5 (14.3) 1 (2.8) At least 1 related SAE 0 0 At least 1 AE leading to study drug interruption 2 (5.7) 1 (2.9) At least 1 related AE leading to study drug interruption 1 (2.9) 0 At least 1 AE leading to study drug withdrawal 0 0 Note: Related includes the Possibly Related and Related to study drug categories Common Adverse Events Common Adverse Events in Safety Set AEs that occurred in at least 10% of patients in either treatment group are presented by system organ class (SOC) and preferred term (PT) in Table 42. AEs for which the incidence was at least 5 percentage points higher with ivacaftor than placebo treatment were (in order of decreasing difference between groups) nasal congestion, oropharyngeal pain, abdominal pain, wheezing, upper airway cough syndrome, bacterial disease carrier, influenza-like illness, and abdominal discomfort. AEs for which the incidence was at least 5 percentage points higher with placebo treatment than ivacaftor treatment were (in order of decreasing difference between groups) hemoptysis, arthralgia, pyrexia, rales, sinusitis, nasal mucosal disorder, sinus congestion, viral upper respiratory tract infection (URTI), pain, dizziness, blood potassium increased, dehydration, attention deficit/hyperactivity disorder, hypersensitivity, constipation, and URTI. Table 42 Study 110: Adverse Events Occurring in At Least 10% of Patients in Either Treatment Group by System Organ Class and Preferred Term, Safety Set Placebo (N = 35) n (%) Ivacaftor (N = 34) n (%) System Organ Class Preferred Term Patients with any AEs 35 (100.0) 32 (94.1) Infections and infestations 24 (68.6) 21 (61.8) Infective pulmonary exacerbation of CF 14 (40.0) 13 (38.2) Upper respiratory tract infection 5 (14.3) 3 (8.8) Sinusitis 5 (14.3) 2 (5.9)
110 FDA Advisory Committee Briefing Materials Page 110 of 157 Table 42 Study 110: Adverse Events Occurring in At Least 10% of Patients in Either Treatment Group by System Organ Class and Preferred Term, Safety Set Placebo (N = 35) n (%) Ivacaftor (N = 34) n (%) System Organ Class Preferred Term Respiratory, thoracic, and mediastinal disorders 19 (54.3) 18 (52.9) Cough 9 (25.7) 10 (29.4) Sputum increased 4 (11.4) 5 (14.7) Nasal congestion 2 (5.7) 5 (14.7) Oropharyngeal pain 2 (5.7) 5 (14.7) Wheezing 1 (2.9) 4 (11.8) Hemoptysis 6 (17.1) 0 Gastrointestinal disorders 13 (37.1) 13 (38.2) Diarrhea 4 (11.4) 5 (14.7) Abdominal pain 0 4 (11.8) Vomiting 4 (11.4) 3 (8.8) General disorders and administration site conditions 11 (31.4) 7 (20.6) Pyrexia 6 (17.1) 2 (5.9) Nervous system disorders 9 (25.7) 6 (17.6) Headache 5 (14.3) 6 (17.6) Musculoskeletal and connective tissue disorders 8 (22.9) 2 (5.9) Arthralgia 4 (11.4) 0 Notes: SOC and PT within SOC were sorted in descending order of frequency in the ivacaftor column. A patient with multiple events within an SOC or within a PT was counted only once within an SOC or PT, respectively. Adverse events were coded from MedDRA, Version Common Adverse Events by Age Subgroups AEs that occurred in at least 15% of patients in either treatment group for patients 18 years and 6 to 11 years of age at baseline are presented in Table 43. Among patients aged 12 to 17 years, 1 patient received placebo treatment and 1 patient received ivacaftor treatment. The patient in the ivacaftor group had no AEs; neither patient had SAEs. Because there were only 2 patients in this subgroup, the AE results for these patients are not included in Table 43. In the 18 years of age subgroup, AEs that occurred in at least 15% of patients in either treatment group and for which the incidence was higher (>2 patients difference) with ivacaftor than placebo were nasal congestion, oropharyngeal pain, and wheezing. AEs that occurred in at least 15% of patients in either treatment group for which the incidence was higher (>2 patients difference) with placebo than ivacaftor were URTI and hemoptysis. Among patients aged 6 to 11 years, there were no AEs that occurred in at least 15% of patients in either treatment group for which the difference between treatment groups was >2 patients. The efficacy section (Section 9) discussed pulmonary exacerbations as an efficacy endpoint; these exacerbations were formally defined in the protocol and analyzed accordingly. Adverse events of pulmonary exacerbations, however, were reported by investigators without adhering to such clear and precise definitions. Consistent with the overall safety population,
111 FDA Advisory Committee Briefing Materials Page 111 of 157 infective pulmonary exacerbation of CF and cough were the most common AEs in patients 18 years of age in both treatment groups; the incidence of both events was higher among patients 18 years of age than among patients 6 to 11 years of age: The incidence of infective pulmonary exacerbation of CF in the 18 years of age subgroup was 45.8% (11 patients, 14 events) in the ivacaftor group and 50.0% (13 patients, 23 events) in the placebo group. In the 6 to 11 years subgroup, the incidence of infective pulmonary exacerbation of CF was 22.2% (2 patients, 3 events) in the ivacaftor group and 12.5% (1 patient, 1 event) in the placebo group. The incidence of cough in the 18 years of age subgroup was 37.5% (9 patients, 12 events) in the ivacaftor group and 26.9% (7 patients, 8 events) in the placebo group compared to 11.1% (1 patient, 2 events) in the ivacaftor group and 12.5% (1 patient, 2 events) in the placebo group in the 6 to 11 years subgroup. The higher incidence of infective pulmonary exacerbation of CF and cough in the 18 years of age subgroup compared to the 6 to 11 years subgroup is not unexpected because patients in the 18 years of age subgroup had a higher baseline disease severity as evident by mean percent predicted FEV 1. The other AEs showed no consistent trend between the 18 years or 6 to 11 years of age subgroups, and any differences may have been due to the small number of patients in the subgroups. Table 43 Study 110: Adverse Events Occurring in At Least 15% of Patients in Either Treatment Group by System Organ Class, Preferred Term, and Age Subgroups, Safety Set Placebo (N = 26) n (%) Age 18 Years Ivacaftor (N = 24) n (%) Placebo (N = 8) n (%) Age 6 to 11 Years Ivacaftor (N = 9) n (%) System Organ Class Preferred Term Patients with any AEs 26 (100.0) 23 (95.8) 8 (100.0) 9 (100.0) Patients with any SAEs 6 (23.1) 2 (8.3) 0 2 (22.2) Infections and infestations 19 (73.1) 16 (66.7) 5 (62.5) 5 (55.6) Infective pulmonary 13 (50.0) 11 (45.8) 1 (12.5) 2 (22.2) exacerbation of CF Bacterial disease carrier 1 (3.8) 1 (4.2) 0 2 (22.2) Upper respiratory tract infection 5 (19.2) 2 (8.3) 0 1 (11.1) Sinusitis 3 (11.5) 1 (4.2) 2 (25.0) 1 (11.1) Respiratory, thoracic, and 14 (53.8) 16 (66.7) 4 (50.0) 2 (22.2) mediastinal disorders Cough 7 (26.9) 9 (37.5) 1 (12.5) 1 (11.1) Sputum increased 4 (15.4) 5 (20.8) 0 0 Hemoptysis 6 (23.1) Nasal congestion 1 (3.8) 5 (20.8) 1 (12.5) 0 Oropharyngeal pain 0 4 (16.7) 2 (25.0) 1 (11.1) Wheezing 1 (3.8) 4 (16.7) 0 0
112 FDA Advisory Committee Briefing Materials Page 112 of 157 Table 43 Study 110: Adverse Events Occurring in At Least 15% of Patients in Either Treatment Group by System Organ Class, Preferred Term, and Age Subgroups, Safety Set Placebo (N = 26) n (%) Age 18 Years Ivacaftor (N = 24) n (%) Placebo (N = 8) n (%) Age 6 to 11 Years Ivacaftor (N = 9) n (%) System Organ Class Preferred Term Gastrointestinal disorders 10 (38.5) 9 (37.5) 3 (37.5) 4 (44.4) Abdominal pain 0 2 (8.3) 0 2 (22.2) Diarrhea 3 (11.5) 4 (16.7) 1 (12.5) 1 (11.1) Abdominal pain upper 0 1 (4.2) 2 (25.0) 1 (11.1) General disorders and 8 (30.8) 5 (20.8) 2 (25.0) 2 (22.2) administration site conditions Pyrexia 3 (11.5) 1 (4.2) 2 (25.0) 1 (11.1) Nervous system disorders 7 (26.9) 4 (16.7) 1 (12.5) 2 (22.2) Headache 3 (11.5) 4 (16.7) 1 (12.5) 2 (22.2) Psychiatric disorders 1 (3.8) 0 2 (25.0) 0 Attention deficit/hyperactivity disorder (25.0) 0 Notes: A patient with multiple events within an SOC or within a PT was counted only once within an SOC or PT, respectively. Adverse events were coded from MedDRA, Version A review of AEs in patients 6 to 11 years of age was conducted to further investigate the observed changes in percent predicted FEV 1 (see Section for FEV 1 results). No AEs suggested the presence of bronchospasm, and no AEs suggested the presence of a clinically significant adverse effect due to ivacaftor. Table 44 Preferred Term, n (%) Study 110: Adverse Events Reviewed for Association with FEV 1 Changes in Patients Age 6 to 11 Years Age 6 to 11 years Placebo N = 8 Ivacaftor N = 9 Placebo N = 26 Age 18 years Ivacaftor N = 24 Infective pulmonary exacerbation of CF 1 (12.5) 2 (22.2) 13 (50.0) 11 (45.8) Forced expiratory volume decreased 0 1 (11.1) 2 (7.7) 2 (8.3) Hemoptysis (23.1) 0 Wheezing (3.8) 4 (16.7) Adverse Events by Severity In both treatment groups, the majority of patients had AEs that were mild or moderate in severity. Compared with placebo, ivacaftor was associated with a lower incidence of severe AEs (2.9% [1 patient] in the ivacaftor group versus 14.3% [5 patients] in the placebo group). There were no life-threatening AEs. Consistent with their greater baseline disease severity, the incidence of severe AEs was greater for patients in the 18 years of age subgroup than for patients <18 years of age. In the
113 FDA Advisory Committee Briefing Materials Page 113 of years of age subgroup, severe AEs occurred in 4 (15.4%) patients in the placebo group (3 patients had severe infective pulmonary exacerbation of CF, 1 patient had severe hypokalemia) and 1 (4.2%) patient in the ivacaftor group (severe infective pulmonary exacerbation of CF). One patient in the 12 to 17 years of age subgroup of the placebo group had a severe AE of increased ALT (maximum ALT value >3 ULN to 5 ULN; resolved without treatment). No severe AEs occurred in the 12 to 17 years of age subgroup of the ivacaftor group or the 6 to 11 years of age subgroup of either treatment group Deaths, Other Serious Adverse Events, and Adverse Events Leading to Discontinuation of Study Drug There were no deaths or AEs that led to discontinuation of study drug. The most common SAE in both treatment groups was infective pulmonary exacerbation of CF; the incidence was higher in the placebo group than in the ivacaftor group (Table 45). All SAEs of infective pulmonary exacerbation of CF resolved without study drug discontinuation. None of the SAEs were considered related to study drug. Table 45 Study 110: Serious Adverse Events; Safety Set and Age Subgroups Placebo (N = 35) n (%) All Ages 18 Years 6 to 11 Years Ivacaftor (N = 34) n (%) Placebo (N = 26) n (%) Ivacaftor (N = 24) n (%) Placebo (N = 8) n (%) Ivacaftor (N = 9) n (%) System Organ Class Preferred Term Any Serious Adverse 6 (17.1) 4 (11.8) 6 (23.1) 2 (8.3) 0 2 (22.2) Event Infective pulmonary 6 (17.1) 3 (8.8) 6 (23.1) 2 (8.3) 0 1 (11.1) exacerbation of CF Cellulitis 0 1 (2.9) 0 1 (4.2) 0 0 Constipation 0 1 (2.9) (11.1) CF: cystic fibrosis; N: total number of patients; n: number of patients with an observation Adverse events were coded from Medical Dictionary for Regulatory Activities (MedDRA) Version Laboratory Evaluations, Vital Signs, and Other Safety Evaluations Overall, the descriptive statistics, mean results over time, and the incidence in categorical shifts from baseline for the clinical laboratory parameters (serum chemistry, hematology, and coagulation studies), vital signs, physical examinations, and ECGs showed minor differences between the ivacaftor and placebo groups that were not considered to be clinically meaningful. Patients with CF are chronically ill, have frequent infections, take numerous medications, and have disease-related metabolic abnormalities. Thus, fluctuations in laboratory parameters are common. 85 AEs associated with abnormal chemistry and hematology values occurred infrequently and none resulted in the permanent discontinuation of study drug. AEs associated with abnormal LFTs occurred in 3 patients in the placebo group and 1 patient in the ivacaftor group (see Section ).
114 FDA Advisory Committee Briefing Materials Page 114 of Liver-Related Parameters Liver function test changes appeared similar to prior studies and the ivacaftor post-marketing experience. Table 46 shows the maximum on-treatment LFT results. Most patients had maximum on-treatment alanine aminotransferase (ALT), aspartate aminotransferase (AST), and total bilirubin results 2 upper limit of normal (ULN), and no differences >5% occurred between the placebo and ivacaftor treatments for any category. No patients in either group had a maximum ALT or AST value >5 ULN or a maximum total bilirubin value >2 ULN. As with previous studies with ivacaftor, no patients met Hy s Law criteria. Table 46 Maximum On-Treatment Result 2 ULN Study 110: Maximum On-Treatment Liver Function Test Results, Safety Set Placebo N = 35 n (%) Ivacaftor N = 34 n (%) Liver Function Test ALT (U/L) 33 (94.3) 31 (91.2) AST (U/L) 35 (100.0) 33 (97.1) Total bilirubin (μmol/l) 35 (100.0) 34 (100.0) ALT (U/L) 1 (2.9) 2 (5.9) >2 ULN to 3 ULN AST (U/L) 0 1 (2.9) Total bilirubin (μmol/l) 0 0 ALT (U/L) 1 (2.9) 1 (2.9) >3 ULN to 5 ULN AST (U/L) 0 0 Total bilirubin (μmol/l) 0 0 ALT (U/L) 0 0 >5 ULN AST (U/L) 0 0 Total bilirubin (μmol/l) 0 0 ALT: alanine transaminase; AST: aspartate transaminase; LFT: liver function test; N: total number of patients; n: number of patients with an observation; ULN: upper limit of normal. Notes: Baseline is defined as the most recent measurement before intake of the first dose of study drug. The result categorized is the maximum of all post baseline LFT results occurring on or before the Week 24 Visit Electrocardiogram Data An assessment of the standard 12-lead ECG data did not alter the interpretation of results from the pooled Phase 2b/3 studies. No patients had ECG-related AEs, and there were no clinically meaningful differences noted between ivacaftor and placebo treatments Safety in Special Populations and Situations The incidence of AEs was summarized for subgroups based on sex (female and male), percent predicted FEV 1 severity at baseline (<70%, 70% to 90%, and >90% predicted), and geographic region (North America and Europe). While small sample sizes in the subgroups preclude definitive conclusions, subgroup analyses did not suggest any notable treatment-related differences in safety based on sex, baseline FEV 1 severity, or geographic region.
115 FDA Advisory Committee Briefing Materials Page 115 of Study 112 A review of SAEs from the pharmacovigilance database was performed after all patients had been treated for at least 12 weeks in Study 112. No new safety concerns were apparent. Table 47 shows the incidence of SAEs. Eight patients in the ivacaftor treatment arm had a total of 12 SAEs (2 patients 6 to 11 years of age; 6 patients 18 years of age). Nine of the SAEs were infective pulmonary exacerbation of CF, 8 of which were considered by the investigators to be not related to study drug. One SAE of infective pulmonary exacerbation of CF was considered by the investigator to be possibly related to study drug. The remaining 3 SAEs (influenza in 1 patient; angioedema and urticaria in 1 patient who had a history of environmental allergies) were considered by the investigators as not related to study drug. Neither of the 2 patients in the observational arm had SAEs. There were no deaths. Table 47 SAE Study 112: Serious Adverse Events 6 to 11 years N=15 18 years N=49 Any SAE 2 (13.3) 6 (12.2) Infective pulmonary exacerbation of CF 2 (13.3) 6 (12.2) Angioedema 0 1 (2.0) a Urticaria 0 1 (2.0) a Influenza 0 1 (2.0) a Angioedema and urticarial occurred in the same patient Post-Marketing Pharmacovigilance Activities The long-term safety of ivacaftor is being assessed in a Post-authorization Safety Study that is a 5-year retrospective observational study using US and UK CF patient registries. The US CF Registry includes more than 90% of CF patients in the US, and the UK registry includes about 100% of CF patients in the UK. This study captures data on ivacaftor-treated patients and untreated patients matched by age, gender, and genotype class. The study is in its second year, and will include data from R117H patients where ivacaftor is approved for this population. The objectives of the study include assessments of safety (hospitalizations, pulmonary exacerbations, deaths, microbiology, complications). Analyses are stratified by age, percent predicted FEV 1, genotype, and exposure duration. It would therefore be possible to provide safety data specific to the R117H mutation in a very substantial proportion of R117H patients in whom ivacaftor may be used.
116 FDA Advisory Committee Briefing Materials Page 116 of BENEFITS AND RISKS The totality of the evidence provides a positive benefit/risk assessment for patients with the R117H mutation and supports approval of ivacaftor for the treatment of CF in patients age 6 years and older who have an R117H mutation in the CFTR gene The R117H mutation is present in about 700 people with CF in the US, including 500 people age 6 years and older. 1 No currently approved treatments are available to treat the underlying cause of disease in this patient population, in whom disease progresses with advancing age The R117H patient population is challenging to study, given the rarity of the mutation and heterogeneity in clinical presentation and progression. The patients enrolled in Study 110 represented a substantial proportion of the R117H patient population in the US. Ivacaftor treatment increased CFTR chloride transport in patients with the R117H mutation, including all patient subgroups, as evidenced by substantial reductions in sweat chloride concentrations. This is consistent with ivacaftor s unique mechanism of action, which targets CFTR dysfunction the underlying cause of CF. This mechanism of action has been proven to be effective in people with other CFTR mutations that cause a defect in channel gating. Despite the failed primary endpoint in Study 110, a biologically understandable and clinically consistent pattern of results demonstrates that ivacaftor provided clinical benefit for patients 18 years of age and had a favorable safety profile for all patients studied. In patients 18 years of age with the R117H mutation, ivacaftor demonstrated consistent, clinically meaningful benefit: Ivacaftor treatment resulted in sustained, clinically relevant increases in lung function (FEV 1 ) and the CFQ-R respiratory domain score in Study 110. Measures of pulmonary exacerbations, including markers for more clinically severe events, favored ivacaftor in Study 110. Improvements in FEV 1 were reduced when ivacaftor treatment was withdrawn during a blinded washout period at the end of Study 110, and then were restored in Study 112 after reintroduction of ivacaftor treatment. Percent predicted FEV 1 results in Study 112 for patients 18 years of age were closely comparable to results in Study 110 for patients 18 years of age. The totality of data in this subgroup, which comprised 72.5% of the patients in Study 110, supports the efficacy of ivacaftor in patients with the R117H mutation. Given the small size of the R117H patient population and the difference in baseline FEV 1 between patients 6 to 11 years of age and patients 18 years of age, it is clinically and scientifically appropriate for results in the adult population in Study 110 to be evaluated separately and to be judged in their own right. The safety experience in the R117H population was favorable and consistent with the well-established safety profile that is based on more than 1100 patients treated with ivacaftor in clinical trials and post-marketing exposure for more than 2000 patients. In R117H patients, no unique safety concerns were apparent, no adverse events resulted in discontinuation of ivacaftor, and adverse events that were severe and/or serious were infrequent. Similar to the
117 FDA Advisory Committee Briefing Materials Page 117 of 157 safety profile observed in placebo-controlled studies for the currently approved mutations, the incidence of SAEs in Study 110 was lower for ivacaftor treatment group than the placebo treatment group. Across all sources, the most common adverse events involve the respiratory, infectious, gastrointestinal, or nervous systems. Ivacaftor for the treatment of CF in patients age 6 years and older with the R117H mutation meets the regulatory criteria for extrapolation of efficacy from adult patients to pediatric patients. Therefore, extrapolation of efficacy to children is appropriate. The disease process is similar, and there were comparable exposures and safety profiles in pediatric and adult patients. Ivacaftor was pharmacodynamically active in pediatric patients, as evidenced by decreases in sweat chloride concentrations during ivacaftor treatment. Ivacaftor was well-tolerated in pediatric patients. Despite the lung function as measured by FEV 1 being in the normal range in the small number of pediatric patients in Study 110, some children and adolescents have lung disease that is not evident based on FEV 1 measurements, and some patients with the R117H mutation have more rapidly progressing disease. These patients have the potential to benefit from ivacaftor treatment. This is a small group of patients that could best be identified based on the individual assessment of clinicians. In summary, the totality of data provides substantial evidence of effectiveness, and the benefit:risk profile supports approval of ivacaftor in patients age 6 years and older who have an R117H mutation in the CFTR gene.
118 FDA Advisory Committee Briefing Materials Page 118 of REFERENCES 1 Cystic Fibrosis Foundation. Cystic Fibrosis Foundation patient registry: 2012 annual data report. Bethesda, Maryland; O Sullivan BP, Freedman SD. Cystic fibrosis. Lancet. 2009;373: Sheppard DN, Rich DP, Ostedgaard LS, Gregory RJ, Smith AE, Welsh MJ. Mutations in CFTR associated with mild-disease-form Cl- channels with altered pore properties. Nature. 1993;362(6416): Zielinski J. Genotype and phenotype in cystic fibrosis. Respiration 2000; 67: Ward CL, Kopito. Intracellular Turnover of cystic fibrosis transmembrane conductance regulator. J Biol Chem 1994; 269(41): Cystic Fibrosis Foundation. Cystic Fibrosis Foundation patient registry: 2011 annual data report. Bethesda, Maryland; 2012; Vertex Pharmaceuticals data request. 7 Kiesewetter S, Macek Jr. M, Davis C, Curristin SM, Chu C-S, Graham C, et al. A mutation in CFTR produces different phenotypes depending on chromosomal background. Nat Genet. 1993;5: Massie RJH, Poplawski N, Wilcken B, Goldblatt J, Byrnes C, Robertson C. Intron-8 polythymidine sequence in Australasian individuals with CF mutations R117H and R117C. Eur Respir J. 2001;17: The Clinical and Functional Translation of CFTR (CFTR2) [Internet]. Available at: [Accessed 28 May 2014]. (Sosnay PR, Siklosi KR, Van Goor F, Kaniecki K, Yu H, Sharma N et al. Defining the disease liability of variants in the cystic fibrosis transmembrane conductance regulator gene. Nature Gen 2013; published online 25 August 2013; doi: /ng.2745.) 10 Castellani C, Cuppens H, Macek M Jr, Cassiman J, Kerem E, Durie P, et al. Consensus on the use and interpretation of cystic fibrosis mutation analysis in clinical practice. Cyst Fibros 2008;7(3): Chu C-S, Trapnell BC, Curristin S, Cutting GR, Crystal RG. Genetic basis of variable exon 9 skipping in cystic fibrosis transmembrane conductance regulator mrna. Nat Genet. 1993;3: Rave-Harel N, Kerem E, Nissim-Rafinia M, Madjar I, Goshen R, Augarten A, et al. The molecular basis of partial penetrance of splicing mutations in cystic fibrosis. Am J Hum Genet 1997;60: Nissim-Rafinia M, Kerem B. Splicing modulation as a modifier of the CFTR function. Progress in Molecular and Subcellular Biology. Philippe Jeantuer (Ed.). Springer-Verlag Berlin Heidelberg; 2006; Peckham D, Conway SP, Morton A, Jones A, Webb K. Delayed diagnosis of cystic fibrosis associated with R117H on a background of 7T polythymidine tract at intron 8. J Cys Fibros. 2006;5: KALYDECO United States Prescribing Information (provided in Appendix 13.1). 16 McKone E, Borowitz D, Drevinek P, et al. Long-term safety and efficacy of ivacaftor in patients with cystic fibrosis who have the G551D-CFTR mutation: response through 144 weeks of treatment (96 weeks of PERSIST) [Poster 227]. Presented at the 27th Annual North American Cystic Fibrosis Conference. Salt Lake City, UT, USA; October 17-19, Sawicki G, McKone E, Pasta D, et al. The Effect of Ivacaftor on the Rate of Lung Function Decline in CF Patients With a G551D-CFTR Mutation. Presented at the 37th Meeting of the European Cystic Fibrosis Society at Gothenburg, Sweden, June 12, 2014
119 FDA Advisory Committee Briefing Materials Page 119 of Rowe SM, Heltshe SL, Gonska T, et al. Clinical mechanism of the cystic fibrosis transmembrane conductance regulator potentiator ivacaftor in G551D-mediated cystic fibrosis. Am J Respir Crit Care Med. 2014;190(2): Farrell PM. The prevalence of cystic fibrosis in the European Union. J Cyst Fibros. 2008;7(5): Cystic Fibrosis Canada. The Canadian cystic fibrosis registry: 2011 annual report. Toronto, Canada; Cystic Fibrosis Australia. Cystic fibrosis in Australia 2012: 15th annual report Australian cystic fibrosis data registry. Baulkham Hills, Australia; Rommens JM, Iannuzzi MC, Kerem B, Drumm ML, Melmer G, Dean M, et al. Identification of the cystic fibrosis gene: chromosome walking and jumping. Science. 1989;245: Boucher RC. Airway surface dehydration in cystic fibrosis: pathogenesis and therapy. Ann Rev Med. 2007;58: Knowles M, Gatzy J, Boucher R. Relative ion permeability of normal and cystic fibrosis nasal epithelium. J Clin Invest. 1983;71(5): Quinton PM. Chloride impermeability in cystic fibrosis. Nature. 1983;301(5899): Riordan JR, Rommens JM, Kerem B, Alon N, Rozmahel R, Grzelczak Z, et al. Identification of the cystic fibrosis gene: cloning and characterization of complementary DNA. Science. 1989;245(4922): Cystic Fibrosis Mutation Database (CFTR1). Cystic Fibrosis Centre at the Hospital for Sick Children in Toronto Web site. Available at: Accessed 21 May De Boeck K, Wilschanski M, Castellani C, Taylor C, Cuppens H, Dodge J, et al. Cystic fibrosis: terminology and diagnostic algorithms. Thorax. 2006;61(7): Farrell PM, Rosenstein BJ, White TB, Accurso FJ, Castellani C, Cutting GR, et al. Guidelines for diagnosis of cystic fibrosis in newborns through older adults: Cystic Fibrosis Foundation consensus report. J Pediatr. 2008;153:S Konstan MW, Morgan WJ, Butler SM, Pasta DJ, Craib ML, Silva SJ, Stokes DC, Wohl ME, Wagener JS, et al.; Scientific Advisory Group and the Investigators and Coordinators of the Epidemiologic Study of Cystic Fibrosis. Risk factors for rate of decline in forced expiratory volume in one second in children and adolescents with cystic fibrosis. J Pediatr 2007;151: Emerson J, Rosenfeld M, McNamara S, Ramsey B, Gibson RL. Pseudomonas aeruginosa and other predictors of mortality and morbidity in young children with cystic fibrosis. Pediatr Pulmonol 2002;34: Kerem E, Reisman J, Corey M, Canny GJ, Levison H. Prediction of mortality in patients with cystic fibrosis. N Engl J Med. 1992;326: Corey M. Power considerations for studies of lung function in cystic fibrosis. Proc Am Thorac Soc Vol 2007; 4:pp European Medicines Agency Committee for Medicinal Products for Human Use; Guideline on the clinical development of medicinal products for the treatment of cystic fibrosis; October U.S. Department of Health and Human Services, Food and Drug Administration, Center for Drug Evaluation and Research. Guidance for Industry: Chronic Obstructive Pulmonary Disease: Developing Drugs for Treatment; Draft Guidance; November Tiddens AWM. Detecting early structural lung damage in cystic fibrosis. Pediatr Pulmonal. 2002;34: Macklem PT. The physiology of small airways. Am J Respir Crit Care Med. 1998;157:S
120 FDA Advisory Committee Briefing Materials Page 120 of de Jong PA, Nakano Y, Lequin MH, Mayo JR, Woods R, Paré PD, and Tiddens HAWM. Progressive damage on high resolution computed tomorgraphy despite stable lung function in cystic fibrosis. Eur Respir J. 2004;23: de Jong PA, Lindblad A, Rubin L, Hop WC, de Jongste JC, Brink M, Tiddens HA. Progression of lung disease on computed tomography and pulmonary function tests in children and adults with cystic fibrosis. Thorax. 2006;61: Ellemunter H, Fuchs SI, Unsinn KM, Freund MC, Waltner-Romen M, Steinkamp G, Gappa M. Sensitivity of lung clearance index and chest computed tomography in early cf lung disease. Respir Med. 2010;104: Owens CM, Aurora P, Stanojevic S, Bush A, Wade A, Oliver C, et al. Lung clearance index and HRCT are complementary markers of lung abnormalities in young children with CF. Thorax. 2011;66: Long FR, Williams RS, Castile RG. Structural airway abnormalities in infants and young children with cystic fibrosis. J Pediatr. 2004;144: Stick SM, Brennan S, Murray C, Douglas T, von Ungern-Sternberg BS, Garratt LW, et al. Bronchiectasis in infants and preschool children diagnosed with cystic fibrosis after newborn screening. J Pediatr. 2009;155: Martinez TM, Llapur CJ, Williams TH, Coates C, Gunderman R, Cohen MD, et al. High-resolution computed tomography imaging of airway disease in infants with cystic fibrosis. Am J Respir Crit Care Med. 2005;172: Sly P, Gangell CL, Chen L, Ware RS, Ranganathan S, Mott LS, et al. Risk Factors for Bronchiectasis in Children with Cystic Fibrosis New Eng J Med 2013; 368: Khan TZ, Wagener JS, Bost T, Martinez J, Accurso FJ, Riches DWH. Early pulmonary inflammation in infants with cystic fibrosis. Am J Respir Crit Care Med. 1995;151: Sly PD, Brennan S, Gangell C, de Klerk N, Murray C, Mott L, et al. Lung disease at diagnosis in infants with cystic fibrosis detected by newborn screening. Am J Respir Crit Care Med. 2009;180: Pillarisetti N, Williamson E, Linnane B, Skoric B, Robertson CF, Robinson P, et al. Infection, inflammation, and lung function decline in infants with cystic fibrosis. Am J Respir Crit Care Med. 2011; 184: Starner TD, McCray PB. Pathogenesis of early lung disease in cystic fibrosis: a window of opportunity to eradicate bacteria. Ann Intern Med. 2005;143: Li Z, Kosorok MR, Farrell PM, Laxova A, West SEH, Green CG, et al. Longitudinal development of mucoid Pseudomonas aeruginosa infection and lung disease progression in children with cystic fibrosis. JAMA. 2005;293: Koch C. Early infection and progression of cystic fibrosis lung disease. Pediatr Pulmonol. 2002;34: Du K, Sharma M, Lukacs GL. The ΔF508 cystic fibrosis mutation impairs domain-domain interactions and arrests post-translational folding of CFTR. Nat Struct Mol Biol. 2005;12: Thibodeau PH, Brautigam CA, Machius M, Thomas PJ. Side chain and backbone contributions of Phe508 to CFTR folding. Nat Struct Mol Biol. 2005;12: Lukacs GL, Chang X-B, Bear C, Kartner N, Mohamed A, Riordan JR, Grinstein S. The ΔF508 mutation decreases the stability of cystic fibrosis transmembrane conductance regulator in the plasma membrane. Determination of functional half-lives on transfected cells. J Biol Chem 1993;268:
121 FDA Advisory Committee Briefing Materials Page 121 of Denning GM, Anderson MP, Amara JF, Marshall J, Smith AE, Welsh MJ. Processing of mutant cystic fibrosis transmembrane conductance regulator is temperature-sensitive. Nature 1992;358: Welsh MJ, Smith AE: Molecular mechanisms of CFTR chloride channel dysfunction in cystic fibrosis. Cell 1993;73: Nooijer RA, Nobel JM, Arets HGM, Bot AG, van Berkhout FT, de Rijke YB, et al. Assessment of CFTR function in homozygous R117H-7T subjects. J Cystic Fibros. 2011;10: McCoy KS, Quittner AL, Oermann CM, Gibson RL, Retsch-Bogart GZ, Montgomery AB. Inhaled aztreonam lysine for chronic airway Pseudomonas aeruginosa in cystic fibrosis. Am J Respir Crit Care Med. 2008;178(9): Retsch-Bogart GZ, Quittner AL, Gibson RL, Oermann CM, McCoy KS, Montgomery AB, et al. Efficacy and safety of inhaled aztreonam lysine for airway Pseudomonas in cystic fibrosis. Chest. 2009;135: Cystic Fibrosis Trust. UK cystic fibrosis registry: annual data Report Bromley Kent, UK; Castellani C, Bonizzato A, Cabrini G, Mastella G. Newborn screening strategy for cystic fibrosis: a field study in an area with high allelic heterogeneity. Acta Paediatr. 1997;86(5): Cystic Fibrosis Registry of Ireland. Cystic Fibrosis registry of Ireland: 2012 annual report. Dublin, Ireland; Vaincre la Mucoviscidose and Institut National d Études Démographiques. The French cystic fibrosis data registry: annual data report Paris, France; The Clinical and Functional Translation of CFTR (CFTR2) [Internet]. Available at: [Accessed 28 May 2014]. (Sosnay PR, Siklosi KR, Van Goor F, Kaniecki K, Yu H, Sharma N et al. Defining the disease liability of variants in the cystic fibrosis transmembrane conductance regulator gene. Nature Gen 2013; published online 25 August 2013; doi: /ng.2745.) 65 McKone EF, Goss CH, Aitken ML. CFTR genotype as a predictor of prognosis in cystic fibrosis. Chest. 2006;130: Lording A, McGaw J, Dalton A, Beal G, Everard M, Taylor CJ. Pulmonary infection in mild variant cystic fibrosis: implications for care. J Cystic Fibrosis 2006;5: O Sullivan B, Zwerdling RG, Dorkin HL, Comeau AM, Parad R. Early pulmonary manifestation of cystic fibrosis in children with the ΔF508/R117H-7T genotype. Pediatrics 2006;118(3): Moskowitz SM, Chmiel JF, Sternen DL, Cheng E, Gibson RL, Marshall SG, et al. Clinical practice and genetic counseling for cystic fibrosis and CFTR-related disorders. Genet Med. 2008:10(12): Thauvin-Robinet C, Munck A, Huet F, Génin E, Bellis G, Gautier E, et al. The very low penetrance of cystic fibrosis for the R117H mutation: a reappraisal for genetic counselling and newborn screening. J Med Genet. 2009;46: McCloskey M, Redmond AO, Elborn JS. Clinical features associated with a delayed diagnosis of cystic fibrosis. Respiration. 2000;67: Van Goor F, Hadida S, Grootenhuis PD, Burton B, Cao D, Neuberger T, et al. Rescue of CF airway epithelial cell function in vitro by a CFTR potentiator, VX-770. Proc Natl Acad Sci U S A 2009 Nov 3;106(44): Yu H, Burton B, Huang CJ, Worley J, Cao D, Johnson JP Jr, et al. Ivacaftor potentiation of multiple CFTR channel with gating mutations. J Cyst Fibros. 2012;11: Hankinson JL, Odencrantz RJ, Fedan KB. Spirometric reference values from a sample of the general U.S. population. Am J Respir Crit Care Med. 1999;159:
122 FDA Advisory Committee Briefing Materials Page 122 of Wang X, Dockery DW, Wyupij D, Fay ME, Ferris BG Jr. Pulmonary function between 6 and 18 years of age. Pediatr Pulmonol. 1993;15: Rosenstein BJ, Cutting GR. The diagnosis of cystic fibrosis: a consensus statement. Cystic Fibrosis Foundation Consensus Panel. J Pediatr. 1998;132(4): Ramsey BW, Davies J, McElvaney NG, Tullis E, Bell SC, Dřevínek P, et al. A CFTR potentiator in patients with cystic fibrosis and the G551D mutation. N Engl J Med. 2011;365(18): Davies JC, Wainwright CE, Canny GJ, Chilvers MA, Howenstine MS, Munck A, et al. Efficacy and safety of ivacaftor in patients aged 6 to 11 years with cystic fibrosis with a G551D mutation. Am J Respir Crit Care Med. 2013;187(11): Quittner AL, Modi A, Cruz I. Systematic review of health-related quality of life measure for children with respiratory conditions. Pediatr Respir Rev. 2008;9: Goss C, Quittner AL. Patient-reported outcomes in cystic fibrosis. Proc Am Thorac Soc. 2007;4: Modi AC, Quittner AL. Validation of a disease-specific measure of health-related quality of life for children with cystic fibrosis. J Pediatr Psychol. 2003;28: Quittner AL, Modi AC, Wainwright C, Otto K, Kirihara J,Montgomery AB. Determination of the minimal clinically important difference scores for the Cystic Fibrosis Questionnaire-Revised Respiratory Symptom scale in two populations of patients with CF and chronic Pseudomonas aeruginosa airway infection. Chest. 2009;135: Siddiqui O, Hung HM, O Neill R. MMRM vs. LOCF: a comprehensive comparison based on simulation study and 25 NDA datasets. J Biopharm Stat. 2009;19(2): Kenward MG, Roger JH. Small sample inference for fixed effects from restricted maximum likelihood. Biometrics. 1997;53(3): Cazzole M, MacNee W, Martinex FJ, Rabe KF, Franciosi LG, Barnes PJ, et al. Outcomes for COPD pharmacological trials: from lung function to biomarkers. Eur Respir J. 2008;31: Goss CH, Mayer-Hamblett N, Kronmal RA, Williams J, Ramsey BW. Laboratory parameter profiles among patients with cystic fibrosis. J Cyst Fibros. 2007;6(2):
123 FDA Advisory Committee: Briefing Materials Page 123 of APPENDICES 13.1 Kalydeco USPI
124 Page 124 of 157 HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use KALYDECO safely and effectively. See full prescribing information for KALYDECO. KALYDECO (ivacaftor) Tablets, for oral use Initial U.S. Approval: RECENT MAJOR CHANGES Indications and Usage (1) 02/ INDICATIONS AND USAGE KALYDECO is a cystic fibrosis transmembrane conductance regulator (CFTR) potentiator indicated for the treatment of cystic fibrosis (CF) in patients age 6 years and older who have one of the following mutations in the CFTR gene: G551D, G1244E, G1349D, G178R, G551S, S1251N, S1255P, S549N, or S549R. If the patient s genotype is unknown, an FDA-cleared CF mutation test should be used to detect the presence of a CFTR mutation followed by verification with bi-directional sequencing when recommended by the mutation test instructions for use. (1) Limitations of Use Not effective in patients with CF who are homozygous for the F508del mutation in the CFTR gene. (1, 14) DOSAGE AND ADMINISTRATION Adults and pediatric patients age 6 years and older: one 150 mg tablet taken orally every 12 hours with fat-containing food. (2.1, 12.3) Reduce dose in patients with moderate and severe hepatic impairment. (2.2, 8.6, 12.3) Reduce dose when co-administered with drugs that are moderate or strong CYP3A inhibitors. (2.3, 7.1, 12.3) DOSAGE FORMS AND STRENGTHS Tablets: 150 mg (3) CONTRAINDICATIONS None (4) WARNINGS AND PRECAUTIONS Elevated transaminases (ALT or AST): Transaminases (ALT and AST) should be assessed prior to initiating KALYDECO, every 3 months during the first year of treatment, and annually thereafter. Patients who develop increased transaminase levels should be closely monitored until the abnormalities resolve. Dosing should be interrupted in patients with ALT or AST of greater than 5 times the upper limit of normal (ULN). Following resolution of transaminase elevations, consider the benefits and risks of resuming KALYDECO dosing. (5.1, 6) Use with CYP3A inducers: Concomitant use with strong CYP3A inducers (e.g., rifampin, St. John s Wort) substantially decreases exposure of ivacaftor, which may diminish effectiveness. Therefore, coadministration is not recommended. (5.2, 7.2, 12.3) ADVERSE REACTIONS The most common adverse drug reactions to KALYDECO (occurring in 8% of patients with CF who have a G551D mutation in the CFTR gene) were headache, oropharyngeal pain, upper respiratory tract infection, nasal congestion, abdominal pain, nasopharyngitis, diarrhea, rash, nausea, and dizziness. (6.1) DRUG INTERACTIONS CYP3A inhibitors: Reduce KALYDECO dose to 150 mg twice a week when co-administered with strong CYP3A inhibitors (e.g., ketoconazole). Reduce KALYDECO dose to 150 mg once daily when co-administered with moderate CYP3A inhibitors (e.g., fluconazole). Avoid food containing grapefruit or Seville oranges. (7.1, 12.3) To report SUSPECTED ADVERSE REACTIONS, contact Vertex Pharmaceuticals Incorporated at or FDA at FDA or See 17 for PATIENT COUNSELING INFORMATION and FDAapproved patient labeling. Revised: 02/2014 FULL PRESCRIBING INFORMATION: CONTENTS* 1 INDICATIONS AND USAGE 2 DOSAGE AND ADMINISTRATION 2.1 Dosing Information in Adults and Children Ages 6 Years and Older 2.2 Dosage Adjustment for Patients with Hepatic Impairment 2.3 Dosage Adjustment for Patients Taking Drugs that are CYP3A Inhibitors 3 DOSAGE FORMS AND STRENGTHS 4 CONTRAINDICATIONS 5 WARNINGS AND PRECAUTIONS 5.1 Transaminase (ALT or AST) Elevations 5.2 Concomitant Use with CYP3A Inducers 6 ADVERSE REACTIONS 6.1 Clinical Trials Experience 7 DRUG INTERACTIONS 7.1 Inhibitors of CYP3A 7.2 Inducers of CYP3A 7.3 CYP3A and/or P-gp Substrates 8 USE IN SPECIFIC POPULATIONS 8.1 Pregnancy 8.3 Nursing Mothers 8.4 Pediatric Use 8.5 Geriatric Use 8.6 Hepatic Impairment 8.7 Renal Impairment 8.8 Patients with CF who are Homozygous for the F508del Mutation in the CFTR Gene 10 OVERDOSAGE 11 DESCRIPTION 12 CLINICAL PHARMACOLOGY 12.1 Mechanism of Action 12.2 Pharmacodynamics 12 3 Pharmacokinetics 13 NONCLINICAL TOXICOLOGY 13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility 13 2 Animal Toxicology and/or Pharmacology 14 CLINICAL STUDIES 14.1 Trials in Patients with CF who have a G551D Mutation in the CFTR Gene 14.2 Trial in Patients with a G1244E, G1349D, G178R, G551S, G970R, S1251N, S1255P, S549N, or S549R Mutation in the CFTR Gene 14.3 Trial in Patients Homozygous for the F508del Mutation in the CFTR Gene 16 HOW SUPPLIED/STORAGE AND HANDLING 17 PATIENT COUNSELING INFORMATION 17.1 Transaminase (ALT or AST) Elevations and Monitoring 17.2 Drug Interactions with CYP3A Inducers and Inhibitors 17.3 Use in Patients with Hepatic Impairment 17.4 Take with Fat-Containing Food *Sections or subsections omitted from the full prescribing information are not listed. 1 of 14
125 Page 125 of 157 KALYDECO (ivacaftor) Tablets FULL PRESCRIBING INFORMATION 1 INDICATIONS AND USAGE KALYDECO is a cystic fibrosis transmembrane conductance regulator (CFTR) potentiator indicated for the treatment of cystic fibrosis (CF) in patients age 6 years and older who have one of the following mutations in the CFTR gene: G551D, G1244E, G1349D, G178R, G551S, S1251N, S1255P, S549N, or S549R. If the patient s genotype is unknown, an FDA-cleared CF mutation test should be used to detect the presence of a CFTR mutation followed by verification with bidirectional sequencing when recommended by the mutation test instructions for use. Limitations of Use KALYDECO is not effective in patients with CF who are homozygous for the F508del mutation in the CFTR gene. 2 DOSAGE AND ADMINISTRATION 2.1 Dosing Information in Adults and Children Ages 6 Years and Older The recommended dose of KALYDECO for both adults and pediatric patients age 6 years and older is one 150 mg tablet taken orally every 12 hours (300 mg total daily dose) with fat-containing food. Examples of appropriate fat-containing foods include eggs, butter, peanut butter, cheese pizza, etc. [see Clinical Pharmacology (12.3) and Patient Counseling Information (17.4)]. 2.2 Dosage Adjustment for Patients with Hepatic Impairment The dose of KALYDECO should be reduced to 150 mg once daily for patients with moderate hepatic impairment (Child-Pugh Class B). KALYDECO should be used with caution in patients with severe hepatic impairment (Child-Pugh Class C) at a dose of 150 mg once daily or less frequently [see Use in Specific Populations (8.6), Clinical Pharmacology (12.3), and Patient Counseling Information (17.3)]. 2.3 Dosage Adjustment for Patients Taking Drugs that are CYP3A Inhibitors When KALYDECO is being co-administered with strong CYP3A inhibitors (e.g., ketoconazole), the dose should be reduced to 150 mg twice a week. The dose of KALYDECO should be reduced to 150 mg once daily when co-administered with moderate CYP3A inhibitors (e.g., fluconazole). Food containing grapefruit or Seville oranges should be avoided [see Drug Interactions (7.1), Clinical Pharmacology (12.3), and Patient Counseling Information (17.2)]. 3 DOSAGE FORMS AND STRENGTHS 150 mg tablets. 4 CONTRAINDICATIONS None 5 WARNINGS AND PRECAUTIONS 5.1 Transaminase (ALT or AST) Elevations Elevated transaminases have been reported in patients with CF receiving KALYDECO. It is recommended that ALT and AST be assessed prior to initiating KALYDECO, every 3 months during the first year of treatment, and annually thereafter. Patients who develop increased transaminase levels should be closely monitored until the abnormalities resolve. Dosing should be interrupted in patients with ALT or AST of greater than 5 times the upper limit of normal (ULN). Following resolution of transaminase elevations, consider the benefits and risks of resuming KALYDECO dosing [see Adverse Reactions (6)]. 5.2 Concomitant Use with CYP3A Inducers Use of KALYDECO with strong CYP3A inducers, such as rifampin, substantially decreases the exposure of ivacaftor, which may reduce the therapeutic effectiveness of KALYDECO. Therefore, co-administration of KALYDECO with strong CYP3A inducers (e.g., rifampin, St. John s Wort) is not recommended [see Drug Interactions (7.2) and Clinical Pharmacology (12.3)]. 6 ADVERSE REACTIONS The following adverse reaction is discussed in greater detail in other sections of the label: Transaminase Elevations [see Warnings and Precautions (5.1)] 6.1 Clinical Trials Experience Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice. The overall safety profile of KALYDECO is based on pooled data from three placebo-controlled clinical trials conducted in 353 patients with CF who had a G551D mutation in the CFTR gene (Trials 1 and 2) or were homozygous for the F508del mutation (Trial 3). In addition, an 8-week crossover design trial (Trial 4) involving 39 patients with a G1244E, G1349D, G178R, G551S, G970R, S1251N, S1255P, S549N, or S549R mutation in the CFTR gene was conducted. Patients treated with KALYDECO in these trials were between the ages of 6 and 57 years. Of the 353 patients included in the pooled analyses of patients with CF who had either a G551D mutation or were homozygous for the F508del mutation in the CFTR gene, 50% of patients were female and 97% were Caucasian; 221 received KALYDECO and 132 received placebo from 16 to 48 weeks. The proportion of patients who prematurely discontinued study drug due to adverse reactions was 2% for KALYDECO-treated patients and 5% for placebotreated patients. Serious adverse reactions, whether considered drug-related or not by the investigators, that occurred more frequently in KALYDECOtreated patients included abdominal pain, increased hepatic enzymes, and hypoglycemia. The most common adverse reactions in the 221 patients treated with KALYDECO were headache (17%), upper respiratory tract infection (16%), nasal congestion (16%), nausea (10%), rash (10%), rhinitis (6%), dizziness (5%), arthralgia (5%), and bacteria in sputum (5%). The incidence of adverse reactions below is based upon two double-blind, placebo-controlled, 48-week clinical trials (Trials 1 and 2) in a total of 213 patients with CF ages 6 to 53 who have a G551D mutation in the CFTR gene and who were treated with KALYDECO 150 mg orally or placebo twice daily. 2 of 14
126 Page 126 of 157 KALYDECO (ivacaftor) Tablets Table 1 shows adverse reactions occurring in 8% of KALYDECO-treated patients with CF who have a G551D mutation in the CFTR gene that also occurred at a higher rate than in the placebo-treated patients in the two double-blind, placebo-controlled trials. Table 1: Incidence of Adverse Drug Reactions in 8% of KALYDECO-Treated Patients with a G551D Mutation in the CFTR Gene and Greater than Placebo in 2 Placebo-Controlled Phase 3 Clinical Trials of 48 Weeks Duration Incidence: Pooled 48-week Trials Adverse Reaction (Preferred Term) KALYDECO N=109 n (%) Placebo N=104 n (%) Headache 26 (24) 17 (16) Oropharyngeal pain 24 (22) 19 (18) Upper respiratory tract infection 24 (22) 14 (14) Nasal congestion 22 (20) 16 (15) Abdominal pain 17 (16) 13 (13) Nasopharyngitis 16 (15) 12 (12) Diarrhea 14 (13) 10 (10) Rash 14 (13) 7 (7) Nausea 13 (12) 11 (11) Dizziness 10 (9) 1 (1) Adverse reactions in the 48-week clinical trials that occurred in the KALYDECO group at a frequency of 4 to 7% where rates exceeded that in the placebo group include: Infections and infestations: rhinitis Investigations: aspartate aminotransferase increased, bacteria in sputum, blood glucose increased, hepatic enzyme increased Musculoskeletal and connective tissue disorders: arthralgia, musculoskeletal chest pain, myalgia Nervous system disorders: sinus headache Respiratory, thoracic and mediastinal disorders: pharyngeal erythema, pleuritic pain, sinus congestion, wheezing Skin and subcutaneous tissue disorders: acne Laboratory Abnormalities Transaminase Elevations During 48-week placebo-controlled clinical studies, the incidence of maximum transaminase (ALT or AST) >8, >5 or >3 x ULN was 2%, 3% and 6% in KALYDECO-treated patients and 2%, 2% and 8% in placebo-treated patients, respectively. Two patients (2%) on placebo and 1 patient (0.5 %) on KALYDECO permanently discontinued treatment for elevated transaminases, all >8 x ULN. Two patients treated with KALYDECO were reported to have serious adverse reactions of elevated liver transaminases compared to none on placebo [see Warnings and Precautions (5.1)]. The safety profile for the 39 patients with CF with a G1244E, G1349D, G178R, G551S, G970R, S1251N, S1255P, S549N, or S549R mutation enrolled in the 8-week crossover trial (Trial 4) was similar to that observed in the 48-week placebo-controlled trials (Trials 1 and 2). 7 DRUG INTERACTIONS Potential for other drugs to affect ivacaftor 7.1 Inhibitors of CYP3A Ivacaftor is a sensitive CYP3A substrate. Co-administration with ketoconazole, a strong CYP3A inhibitor, significantly increased ivacaftor exposure [measured as area under the curve (AUC)] by 8.5-fold. Based on simulations of these results, a reduction of the KALYDECO dose to 150 mg twice a week is recommended for co-administration with strong CYP3A inhibitors, such as ketoconazole, itraconazole, posaconazole, voriconazole, telithromycin, and clarithromycin. Co-administration with fluconazole, a moderate inhibitor of CYP3A, increased ivacaftor exposure by 3-fold. Therefore, a reduction of the KALYDECO dose to 150 mg once daily is recommended for patients taking concomitant moderate CYP3A inhibitors, such as fluconazole and erythromycin. Co-administration of KALYDECO with grapefruit juice, which contains one or more components that moderately inhibit CYP3A, may increase exposure of ivacaftor. Therefore, food containing grapefruit or Seville oranges should be avoided during treatment with KALYDECO [see Clinical Pharmacology (12.3)]. 7.2 Inducers of CYP3A Co-administration with rifampin, a strong CYP3A inducer, significantly decreased ivacaftor exposure (AUC) by approximately 9-fold. Therefore, coadministration with strong CYP3A inducers, such as rifampin, rifabutin, phenobarbital, carbamazepine, phenytoin, and St. John s Wort is not recommended [see Warnings and Precautions (5.2) and Clinical Pharmacology (12.3)]. Potential for ivacaftor to affect other drugs 7.3 CYP3A and/or P-gp Substrates Ivacaftor and its M1 metabolite have the potential to inhibit CYP3A and P-gp. Co-administration with midazolam, a sensitive CYP3A substrate, increased midazolam exposure 1.5-fold, consistent with weak inhibition of CYP3A by ivacaftor. Co-administration with digoxin, a sensitive P-gp substrate, increased digoxin exposure by 1.3-fold, consistent with weak inhibition of P-gp by ivacaftor. Administration of KALYDECO may increase systemic exposure of drugs 3 of 14
127
128 Page 128 of 157 KALYDECO (ivacaftor) Tablets 12 CLINICAL PHARMACOLOGY 12.1 Mechanism of Action Ivacaftor is a potentiator of the CFTR protein. The CFTR protein is a chloride channel present at the surface of epithelial cells in multiple organs. Ivacaftor facilitates increased chloride transport by potentiating the channel-open probability (or gating) of the CFTR protein. In vitro, ivacaftor increased CFTR-mediated transepithelial current (I T ) in rodent cells expressing the G551D-CFTR protein following addition of a cyclic adenosine monophosphate (camp) agonist with an EC 50 of 100 ± 47 nm; however, ivacaftor did not increase I T in the absence of camp agonist. Ivacaftor also increased I T in human bronchial epithelial cells expressing G551D-CFTR protein following addition of a camp agonist by 10-fold with an EC 50 of 236 ± 200 nm. Ivacaftor increased the open probability of G551D-CFTR protein in single channel patch clamp experiments using membrane patches from rodent cells expressing G551D-CFTR protein by 6-fold versus untreated cells after addition of PKA and ATP. In addition to G551D-CFTR, ivacaftor increased the channel-open probability of other mutant CFTR forms expressed in rodent cells, resulting in enhanced CFTR-mediated I T. These mutant CFTR forms included G178R-, S549N-, S549R-, G551S-, G970R-, G1244E-, S1251N-, S1255P-, and G1349D-CFTR. In vitro responses do not necessarily correspond to in vivo pharmacodynamic response or clinical benefit Pharmacodynamics Sweat Chloride Evaluation Changes in sweat chloride response to KALYDECO were evaluated in four clinical trials. In two randomized, double-blind, placebo-controlled clinical trials in patients with a G551D mutation in the CFTR gene, one in patients 12 and older (Trial 1) and the other in patients 6-11 years of age (Trial 2), the treatment difference (between KALYDECO and placebo) in mean change in sweat chloride from baseline through Week 24 was -48 mmol/l (95% CI -51, -45) and - 54 mmol/l (95% CI -62, -47), respectively. These changes persisted through 48 weeks. In a 16-week randomized, double-blind, placebo-controlled, parallelgroup clinical trial in patients with CF age 12-years and older who were homozygous for the F508del mutation in the CFTR gene (Trial 3), the treatment difference in mean change in sweat chloride from baseline through 8 weeks of treatment was -3 mmol/l (95% CI -6, -0.2). In a two-part, randomized, double-blind, placebo-controlled, crossover clinical trial in patients with CF who had a G1244E, G1349D, G178R, G551S, G970R, S1251N, S1255P, S549N, or S549R mutation in the CFTR gene (Trial 4), the treatment difference in mean change in sweat chloride from baseline through 8 weeks of treatment was -49 mmol/l (95% CI -57, -41). In Trial 4, mean changes in sweat chloride for the mutations for which KALYDECO is indicated ranged from -51 to -78, whereas the range for individual subjects with the G970R mutations was -1 to -11 mmol/l. There was no direct correlation between decrease in sweat chloride levels and improvement in lung function (FEV 1 ). ECG Evaluation The effect of multiple doses of ivacaftor 150 mg and 450 mg twice daily on QTc interval was evaluated in a randomized, placebo- and active-controlled (moxifloxacin 400 mg) four-period crossover thorough QT study in 72 healthy subjects. In a study with demonstrated ability to detect small effects, the upper bound of the one-sided 95% confidence interval for the largest placebo adjusted, baseline-corrected QTc based on Fridericia s correction method (QTcF) was below 10 ms, the threshold for regulatory concern Pharmacokinetics The pharmacokinetics of ivacaftor is similar between healthy adult volunteers and patients with CF. After oral administration of a single 150 mg dose to healthy volunteers in a fed state, peak plasma concentrations (T max ) occurred at approximately 4 hours, and the mean (±SD) for AUC and C max were (5260) ng*hr/ml and 768 (233) ng/ml, respectively. After every 12-hour dosing, steady-state plasma concentrations of ivacaftor were reached by days 3 to 5, with an accumulation ratio ranging from 2.2 to 2.9. Absorption The exposure of ivacaftor increased approximately 2- to 4-fold when given with food containing fat. Therefore, KALYDECO should be administered with fat-containing food. Examples of fat-containing foods include eggs, butter, peanut butter, and cheese pizza. The median (range) T max is approximately 4.0 (3.0; 6.0) hours in the fed state. Distribution Ivacaftor is approximately 99% bound to plasma proteins, primarily to alpha 1-acid glycoprotein and albumin. Ivacaftor does not bind to human red blood cells. The mean apparent volume of distribution (Vz/F) of ivacaftor after a single dose of 275 mg of KALYDECO in the fed state was similar for healthy subjects and patients with CF. After oral administration of 150 mg every 12 hours for 7 days to healthy volunteers in a fed state, the mean (±SD) for apparent volume of distribution was 353 (122) L. Metabolism Ivacaftor is extensively metabolized in humans. In vitro and clinical studies indicate that ivacaftor is primarily metabolized by CYP3A. M1 and M6 are the two major metabolites of ivacaftor in humans. M1 has approximately one-sixth the potency of ivacaftor and is considered pharmacologically active. M6 has less than one-fiftieth the potency of ivacaftor and is not considered pharmacologically active. Elimination Following oral administration, the majority of ivacaftor (87.8%) is eliminated in the feces after metabolic conversion. The major metabolites M1 and M6 accounted for approximately 65% of the total dose eliminated with 22% as M1 and 43% as M6. There was negligible urinary excretion of ivacaftor as unchanged parent. The apparent terminal half-life was approximately 12 hours following a single dose. The mean apparent clearance (CL/F) of ivacaftor was similar for healthy subjects and patients with CF. The CL/F (SD) for the 150 mg dose was 17.3 (8.4) L/hr in healthy subjects. Special populations Hepatic impairment Patients with moderately impaired hepatic function (Child-Pugh Class B, score 7 to 9) had similar ivacaftor C max, but an approximately two-fold increase in ivacaftor AUC 0- compared with healthy subjects matched for demographics. Based on simulations of these results, a reduced KALYDECO dose of 150 mg once daily is recommended for patients with moderate hepatic impairment. The impact of mild hepatic impairment (Child-Pugh Class A) on pharmacokinetics of ivacaftor has not been studied, but the increase in ivacaftor AUC 0- is expected to be less than two-fold. Therefore, no dose adjustment 5 of 14
129 Page 129 of 157 KALYDECO (ivacaftor) Tablets is necessary for patients with mild hepatic impairment. The impact of severe hepatic impairment (Child-Pugh Class C, score 10-15) on pharmacokinetics of ivacaftor has not been studied. The magnitude of increase in exposure in these patients is unknown but is expected to be substantially higher than that observed in patients with moderate hepatic impairment. When benefits are expected to outweigh the risks, KALYDECO should be used with caution in patients with severe hepatic impairment at a dose of 150 mg given once daily or less frequently. Renal impairment KALYDECO has not been studied in patients with mild, moderate or severe renal impairment (creatinine clearance less than or equal to 30 ml/min) or in patients with end-stage renal disease. No dose adjustments are recommended for mild and moderate renal impairment patients because of minimal elimination of ivacaftor and its metabolites in urine (only 6.6% of total radioactivity was recovered in the urine in a human PK study); however, caution is recommended when administering KALYDECO to patients with severe renal impairment or end-stage renal disease. Gender The effect of gender on KALYDECO pharmacokinetics was evaluated using population pharmacokinetics of data from clinical studies of KALYDECO. No dose adjustments are necessary based on gender. Drug Interactions Drug interaction studies were performed with KALYDECO and other drugs likely to be co-administered or drugs commonly used as probes for pharmacokinetic interaction studies [see Drug Interactions (7)]. Dosing recommendations based on clinical studies or potential drug interactions with KALYDECO are presented below. Potential for Ivacaftor to Affect Other Drugs Based on in vitro results, ivacaftor and metabolite M1 have the potential to inhibit CYP3A and P-gp. Clinical studies showed that KALYDECO is a weak inhibitor of CYP3A and P-gp, but not an inhibitor of CYP2C8. In vitro studies suggest that ivacaftor and M1 may inhibit CYP2C9. In vitro, ivacaftor, M1, and M6 were not inducers of CYP isozymes. Dosing recommendations for co-administered drugs with KALYDECO are shown in Figure 1. Figure 1: Impact of KALYDECO on Other Drugs Note The data obtained with substrates but without co-administration of KALYDECO are used as reference. *NE: Norethindrone; **EE: Ethinyl Estradiol The vertical lines are at 0.8, 1.0 and 1.25, respectively. Potential for Other Drugs to Affect Ivacaftor In vitro studies showed that ivacaftor and metabolite M1 were substrates of CYP3A enzymes (i.e., CYP3A4 and CYP3A5). Exposure to ivacaftor is reduced by concomitant CYP3A inducers and increased by concomitant CYP3A inhibitors [see Dosage and Administration (2.3) and Drug Interactions (7)]. KALYDECO dosing recommendations for co-administration with CYP3A inhibitors or inducers are shown in Figure 2. 6 of 14
130 Page 130 of 157 KALYDECO (ivacaftor) Tablets Figure 2: Impact of Other Drugs on KALYDECO Note The data obtained for KALYDECO without co-administration of inducers or inhibitors are used as reference. The vertical lines are at 0.8, 1.0 and 1.25, respectively. 13 NONCLINICAL TOXICOLOGY 13 1 Carcinogenesis, Mutagenesis, Impairment of Fertility Two-year studies were conducted in mice and rats to assess carcinogenic potential of KALYDECO. No evidence of tumorigenicity was observed in mice or rats at ivacaftor oral doses up to 200 mg/kg/day and 50 mg/kg/day, respectively (approximately equivalent to and 3 to 5 times the MRHD, respectively, based on summed AUCs of ivacaftor and its metabolites). Ivacaftor was negative for genotoxicity in the following assays: Ames test for bacterial gene mutation, in vitro chromosomal aberration assay in Chinese hamster ovary cells, and in vivo mouse micronucleus test. Ivacaftor impaired fertility and reproductive performance indices in male and female rats at 200 mg/kg/day (approximately 5 and 6 times, respectively, the MRHD based on summed AUCs of ivacaftor and its metabolites). Increases in prolonged diestrus were observed in females at 200 mg/kg/day. Ivacaftor also increased the number of females with all nonviable embryos and decreased corpora lutea, implantations, and viable embryos in rats at 200 mg/kg/day (approximately 6 times the MRHD based on summed AUCs of ivacaftor and its metabolites) when dams were dosed prior to and during early pregnancy. These impairments of fertility and reproductive performance in male and female rats at 200 mg/kg/day were attributed to severe toxicity. No effects on male or female fertility and reproductive performance indices were observed at 100 mg/kg/day (approximately 3 times the MRHD based on summed AUCs of ivacaftor and its metabolites) Animal Toxicology and/or Pharmacology Cataracts were seen in juvenile rats dosed with ivacaftor from postnatal day 7-35 at dose levels of 10 mg/kg/day and higher (approximately 0.12 times the MRHD based on summed AUCs of ivacaftor and its metabolites). This finding has not been observed in older animals. 14 CLINICAL STUDIES 14.1 Trials in Patients with CF who have a G551D Mutation in the CFTR Gene Dose Ranging Dose ranging for the clinical program consisted primarily of one double-blind, placebo-controlled, crossover trial in 39 adult (mean age 31 years) Caucasian patients with CF who had FEV 1 40% predicted. Twenty patients with median predicted FEV 1 at baseline of 56% (range: 42% to 109%) received KALYDECO 25, 75, 150 mg or placebo every 12 hours for 14 days and 19 patients with median predicted FEV 1 at baseline of 69% (range: 40% to 122%) received KALYDECO 150, 250 mg or placebo every 12 hours for 28 days. The selection of the 150 mg every 12 hours dose was primarily based on nominal improvements in lung function (pre-dose FEV 1 ) and changes in pharmacodynamic parameters (sweat chloride and nasal potential difference). The twicedaily dosing regimen was primarily based on an apparent terminal plasma half-life of approximately 12 hours. Selection of the 150 mg dose of KALYDECO for children 6 to 11 years of age was based on achievement of comparable pharmacokinetics as those observed for adult patients. Efficacy The efficacy of KALYDECO in patients with CF who have a G551D mutation in the CFTR gene was evaluated in two randomized, double-blind, placebocontrolled clinical trials in 213 clinically stable patients with CF (109 receiving KALYDECO 150 mg twice daily). All eligible patients from these trials were rolled over into an open-label extension study. Trial 1 evaluated 161 patients with CF who were 12 years of age or older (mean age 26 years) with FEV 1 at screening between 40-90% predicted [mean FEV 1 64% predicted at baseline (range: 32% to 98%)]. Trial 2 evaluated 52 patients who were 6 to 11 years of age (mean age 9 years) with FEV 1 at screening between % predicted [mean FEV 1 84% predicted at baseline (range: 44% to 134%)]. Patients who had persistent Burkholderia cenocepacia, Burkholderia dolosa, or Mycobacterium abscessus isolated from sputum at screening and those with abnormal liver function defined as 3 or more liver function tests (ALT, AST, AP, GGT, total bilirubin) 3 times the upper limit of normal were excluded. Patients in both trials were randomized 1:1 to receive either 150 mg of KALYDECO or placebo every 12 hours with food containing fat for 48 weeks in addition to their prescribed CF therapies (e.g., tobramycin, dornase alfa). The use of inhaled hypertonic saline was not permitted. 7 of 14
131
132 Page 132 of 157 KALYDECO (ivacaftor) Tablets The primary efficacy endpoint was improvement in lung function as determined by the mean absolute change from baseline in percent predicted FEV 1 through 8 weeks of treatment. Other efficacy variables included absolute change from baseline in sweat chloride through 8 weeks of treatment [see Clinical Pharmacology (12.2)], absolute change from baseline in body mass index (BMI) at 8 weeks of treatment (including body weight at 8 weeks), and improvement in cystic fibrosis symptoms (including relevant respiratory symptoms such as cough, sputum production, and difficulty breathing) through 8 weeks of treatment. For the overall population of the 9 mutations studied, treatment with KALYDECO compared to placebo resulted in significant improvement in percent predicted FEV 1 [10.7 through Week 8 (P < )], BMI [0.66 kg/m 2 at Week 8 (P < )], and cystic fibrosis respiratory symptom score [9.6 through Week 8 (P = )]; however, there was a high degree of variability of efficacy responses among the 9 mutations (Table 3). Based on clinical and pharmacodynamic (sweat chloride) responses to ivacaftor, efficacy in patients with the G970R mutation could not be established [see Clinical Pharmacology (12.2)]. Table 3: Effect of KALYDECO for Efficacy Variables in the Overall Populations and for Specific CFTR Mutations Mutation (n) Absolute change in percent predicted FEV 1 BMI (kg/m 2 ) CF Respiratory Symptom Score (points) At Week 2 At Week 4 At Week 8 At Week 8 At Week 8 All patients (n=39) Results shown as mean (95% CI) change from baseline KALYDECO vs placebo-treated patients: 8.3 (4.5, 12.1) 10.0 (6.2, 13.8) 13.8 (9.9, 17.6) 0.66 (0.34, 0.99) 12.8 (6.7, 18.9) Patients grouped under mutation types (n) Results shown as mean (minimum, maximum) for change from baseline for KALYDECO-treated patients*: G1244E (5) G1349D (2) G178R (5) G551S (2) G970R (4) S1251N (8) S1255P (2) S549N (6) S549R (4) 11 (-5, 25) 6 (-5, 13) 8 (-1, 18) 0.63 (0.34, 1.32) 3.3 (-27.8, 22.2) 19 (5, 33) 18 (2, 35) 20 (3, 36) 1.15 (1.07, 1.22) 16.7 (-11.1, 44.4) 7 (1, 17) 10 (-2, 21) 8 (-1, 18) 0.85 (0.33, 1.46) 20.0 (5.6, 50.0) 0 (-5, 5) 0.3 (-5, 6) (1, 13) 7 (1, 14) 3 (-1, 5) 0.48 (-0.38, 1.75) 1.4 (-16.7, 16.7) 2 (-23, 20) 8 (-13, 26) 9 (-20, 21) 0.73 (0.08, 1.83) 23.3 (5.6, 50.0) 11 (8, 14) 9 (5, 13) 3 (-1, 8) 1.62 (1.39, 1.84) 8.3 (5.6, 11.1) 11 (5, 16) 8 (-9, 19) 11 (-2, 20) 0.79 (0.00, 1.91) 8.8 (-8.3, 27.8) 3 (-4, 8) 4 (-4, 10) 5 (-3, 13) 0.53 (0.33, 0.80) 6.9 (0.0, 11.1) * Statistical testing was not performed due to small numbers for individual mutations. Result for weight gain as a component of body mass index was consistent with BMI. Reflects results from the one patient with the G551S mutation with data at the 8-week time point Trial in Patients Homozygous for the F508del Mutation in the CFTR Gene Trial 3 was a 16-week randomized, double-blind, placebo-controlled, parallel-group trial in 140 patients with CF age 12 years and older who were homozygous for the F508del mutation in the CFTR gene and who had FEV 1 40% predicted. Patients were randomized 4:1 to receive KALYDECO 150 mg (n=112) every twelve hours or placebo (n=28) in addition to their prescribed CF therapies. The mean age of patients enrolled was 23 years and the mean baseline FEV 1 was 79% predicted (range 40% to 129%). As in Trials 1 and 2, patients who had persistent Burkholderia cenocepacia, Burkholderia dolosa, or Mycobacterium abscessus isolated from sputum at screening and those with abnormal liver function defined as 3 or more liver function tests (ALT, AST, AP, GGT, total bilirubin) 3 times the upper limit of normal were excluded. The use of inhaled hypertonic saline was not permitted. The primary endpoint was improvement in lung function as determined by the mean absolute change from baseline through Week 16 in percent predicted FEV 1. Treatment with KALYDECO resulted in no improvement in FEV 1 relative to placebo in patients with CF homozygous for the F508del mutation in the CFTR gene [mean absolute change from baseline through Week 16 in percent predicted FEV 1 was 1.5% and -0.2% for patients in the KALYDECO and placebo-treated groups, respectively (P = 0.15)]. There were no meaningful differences between patients treated with KALYDECO compared to placebo for secondary endpoints (change in CF symptoms, change in weight, or change in sweat chloride concentration). 16 HOW SUPPLIED/STORAGE AND HANDLING KALYDECO (ivacaftor) is supplied as light blue, film-coated, capsule-shaped tablets containing 150 mg of ivacaftor. Each tablet is printed with the characters V 150 on one side and plain on the other, and is packaged as follows: 56-count carton (contains 4 individual blister cards of 14 tablets per card) NDC count bottle NDC Store at C (68-77 F); excursions permitted to C (59-86 F) [see USP Controlled Room Temperature]. 17 PATIENT COUNSELING INFORMATION Advise the patient to read the FDA-approved patient labeling (Patient Information) Transaminase (ALT or AST) Elevations and Monitoring Inform patients that elevation in liver tests have occurred in patients treated with KALYDECO. Liver function tests will be performed prior to initiating KALYDECO, every 3 months during the first year of treatment and annually thereafter [see Warnings and Precautions (5.1)] Drug Interactions with CYP3A Inducers and Inhibitors Ask patients to tell you all the medications they are taking including any herbal supplements or vitamins. Co-administration of KALYDECO with strong CYP3A inducers (e.g., rifampin, St. John s Wort) is not recommended as they may reduce the therapeutic effectiveness of KALYDECO. Reduction of the dose of KALYDECO to 150 mg twice a week is recommended when co-administered with strong CYP3A inhibitors, such as ketoconazole. Dose reduction to 150 mg once daily is recommended when co-administered with moderate CYP3A inhibitors, such as fluconazole. Food containing grapefruit or Seville oranges should be avoided [see Drug Interactions (7.1, 7.2) and Clinical Pharmacology (12.3)]. 9 of 14
133 Page 133 of 157 KALYDECO (ivacaftor) Tablets 17.3 Use in Patients with Hepatic Impairment Inquire and/or assess whether patients have liver impairment. Reduce the dose of KALYDECO in patients with moderately impaired hepatic function (Child-Pugh Class B, score 7 to 9) to 150 mg once daily. KALYDECO has not been studied in patients with severe hepatic impairment (Child-Pugh Class C, score 10-15); however, exposure is expected to be substantially higher than that observed in patients with moderate hepatic impairment. When benefits are expected to outweigh the risks, KALYDECO should be used with caution in patients with severe hepatic impairment at a dose of 150 mg given once daily or less frequently. No dose adjustment is recommended for patients with mild hepatic impairment (Child-Pugh Class A, score 5-6) [see Clinical Pharmacology (12.3)] Take with Fat-Containing Food Inform your patients that KALYDECO is best absorbed by the body when taken with fat-containing food. A typical CF diet will satisfy this requirement. Examples include eggs, butter, peanut butter, cheese pizza, etc. Manufactured for Boston, MA KALYDECO, VERTEX, and the VERTEX triangle logo are registered trademarks of. All other trademarks referenced herein are the property of their respective owners ALL RIGHTS RESERVED Revised February of 14
134 Page 134 of 157 KALYDECO (ivacaftor) Tablets Patient Information is perforated for dispensing to the patient. PATIENT INFORMATION KALYDECO (kuh-lye-deh-koh) (ivacaftor) Film-Coated Tablets Read this Patient Information before you start taking KALYDECO and each time you get a refill. There may be new information. This information does not take the place of talking to your doctor about your medical condition or your treatment. What is KALYDECO? KALYDECO is a prescription medicine used for the treatment of cystic fibrosis (CF) in patients age 6 years and older who have one of the following mutations in their CF gene: G551D, G1244E, G1349D, G178R, G551S, S1251N, S1255P, S549N, or S549R. KALYDECO is not for use in people with CF due to other mutations in the CF gene. KALYDECO is not effective in CF patients with two copies of the F508del mutation (F508del/F508del) in the CF gene. It is not known if KALYDECO is safe and effective in children under 6 years of age. Who should not take KALYDECO? Do not take KALYDECO if you take certain medicines or herbal supplements such as: the antibiotics rifampin (Rifamate, Rifater ) or rifabutin (Mycobutin ) seizure medications such as phenobarbital, carbamazepine (Tegretol, Carbatrol, Equetro ) or phenytoin (Dilantin, Phenytek ) St. John s Wort Talk to your doctor before taking KALYDECO if you take any of the medicines or supplements listed above. What should I tell my doctor before taking KALYDECO? Before you take KALYDECO, tell your doctor if you: have liver or kidney problems drink grapefruit juice, or eat grapefruit or Seville oranges are pregnant or plan to become pregnant. It is not known if KALYDECO will harm your unborn baby. You and your doctor should decide if you will take KALYDECO while you are pregnant. are breastfeeding or planning to breastfeed. It is not known if KALYDECO passes into your breast milk. You and your doctor should decide if you will take KALYDECO while you are breastfeeding. KALYDECO may affect the way other medicines work, and other medicines may affect how KALYDECO works. 11 of 14
135 Page 135 of 157 KALYDECO (ivacaftor) Tablets Tell your doctor about all the medicines you take, including prescription and nonprescription medicines, vitamins, and herbal supplements, as the dose of KALYDECO may need to be adjusted when taken with certain medications. Ask your doctor or pharmacist for a list of these medicines if you are not sure. Especially tell your doctor if you take: antifungal medications such as ketoconazole (e.g., Nizoral ), itraconazole (e.g., Sporanox ), posaconazole (e.g., Noxafil ), voriconazole (e.g., Vfend ), or fluconazole (e.g., Diflucan ) antibiotics such as telithromycin (e.g., Ketek ), clarithromycin (e.g., Biaxin ), or erythromycin (e.g., Ery-Tab ) Know the medicines you take. Keep a list of them to show your doctor and pharmacist when you get a new medicine. How should I take KALYDECO? Take KALYDECO exactly as your doctor tells you to take it. Always take KALYDECO with fat-containing food. Examples of fat-containing foods include eggs, butter, peanut butter, cheese pizza, etc. Your doses of KALYDECO should be taken 12 hours apart. What should I avoid while taking KALYDECO? KALYDECO can cause dizziness in some people who take it. Do not drive a car, use machinery or do anything that needs you to be alert until you know how KALYDECO affects you. You should avoid food containing grapefruit or Seville oranges while you are taking KALYDECO. What are the possible side effects of KALYDECO? KALYDECO can cause serious side effects. High liver enzymes in the blood have been reported in patients receiving KALYDECO. Your doctor will do blood tests to check your liver: before you start KALYDECO every 3 months during your first year of taking KALYDECO every year while you are taking KALYDECO Call your doctor right away if you have any of the following symptoms of liver problems: pain or discomfort in the upper right stomach (abdominal) area yellowing of your skin or the white part of your eyes loss of appetite nausea or vomiting dark, amber-colored urine The most common side effects of KALYDECO include: headache upper respiratory tract infection (common cold), including: sore throat 12 of 14
136 Page 136 of 157 KALYDECO (ivacaftor) Tablets nasal or sinus congestion runny nose stomach (abdominal) pain diarrhea rash nausea dizziness Tell your doctor if you have any side effect that bothers you or that does not go away. These are not all the possible side effects of KALYDECO. For more information, ask your doctor or pharmacist. Call your doctor for medical advice about side effects. You may report side effects to FDA at FDA How should I store KALYDECO? Store KALYDECO at room temperature between 68ºF to 77ºF (20ºC to 25ºC). Do not use KALYDECO after the expiration date on the package. Keep KALYDECO and all medicines out of the reach of children. General information about KALYDECO Medicines are sometimes prescribed for purposes other than those listed in a Patient Information leaflet. Do not use KALYDECO for a condition for which it was not prescribed. Do not give KALYDECO to other people, even if they have the same symptoms you have. It may harm them. This Patient Information summarizes the most important information about KALYDECO. If you would like more information, talk with your doctor. You can ask your pharmacist or doctor for information about KALYDECO that is written for health professionals. For more information, go to or call What are the ingredients in KALYDECO? Active ingredient: ivacaftor Inactive ingredients: colloidal silicon dioxide, croscarmellose sodium, hypromellose acetate succinate, lactose monohydrate, magnesium stearate, microcrystalline cellulose, and sodium lauryl sulfate. The tablet film coat contains: carnauba wax, FD&C Blue #2, PEG 3350, polyvinyl alcohol, talc, and titanium dioxide. The printing ink contains: ammonium hydroxide, iron oxide black, propylene glycol, and shellac. This Patient Information has been approved by the U.S. Food and Drug Administration. Manufactured for: 13 of 14
137 Page 137 of 157 KALYDECO (ivacaftor) Tablets 50 Northern Avenue Boston, MA Approved February 2014 KALYDECO, VERTEX, and the VERTEX triangle logo are registered trademarks of Vertex Pharmaceuticals Incorporated. All other trademarks referenced herein are the property of their respective owners ALL RIGHTS RESERVED of 14
138 FDA Advisory Committee: Briefing Materials Page 138 of CFQ-R Three versions of the CFQ-R instrument have been developed: one for adults and adolescents 14 years of age and older (CFQ-R Teen/Adult) and two for assessing children ages 6 to 13 years (one to be completed by the child [CFQ-R Child] and one to be completed by the parent [CFQ-R Parent]). The CFQ-R contains 3 modules: 1) Health-related quality of life (HRQoL): 9 domains (physical functioning, vitality, emotional state, social limitations, role limitations/school performance, embarrassment, body image, eating disturbances, treatment constraints) 2) Symptoms: 3 symptom scales (respiratory, digestive, weight) 3) Health perception scale: health status (present/evolution) Items are scaled using 4-point Likert scales (e.g., always/often/ sometime/never). To score the HRQoL domain, each item is summarized to generate a domain score and then standardized. Scores range from 0 to 100, with higher scores indicating better health.
139 Page 139 of 157
140 Page 140 of 157
141 Page 141 of 157
142 Page 142 of 157
143 FDA Advisory Committee: Briefing Materials Page 143 of Supplemental Tables and Figures Comparison of Entry Criteria: Studies 102, 103, 111, and 104 Table Principal Inclusion Criteria and Enrollment of Patients with Cystic Fibrosis in Phase 3 Placebo-controlled Studies of Ivacaftor Enrollment criteria at screening Confirmed diagnosis of CF 75 CFTR mutation Age Percent predicted FEV 1 (percentage points) Number of patients dosed (planned) Study 102 Study 103 Study 111 Study 104 sweat chloride value 60 mmol/l by quantitative pilocarpine iontophoresis or 2 CF-causing mutations (all as documented in the patient s medical record) AND chronic sinopulmonary disease a or gastrointestinal/nutritional abnormalities (Study 104 only) G551D on at G551D on at least non-g551d gating F508del homozygous least 1 allele 1 allele on at least 1 allele 12 years and 6 to 11 years 6 years and older 12 years and older older (inclusive) 40 to 90 (inclusive) 40 to 105 (inclusive) (30 minimum) 39 (20 minimum) 140 (80 minimum) (approximately 120) 1:1 1:1 1:1 b 4:1 Randomization (ivacaftor:placebo) Notes: Knudson equations (Knudson RJ, et al; Am Rev Respir Dis. 1983;127:725-34) were used to determine percent predicted FEV 1 values in Studies 102 and 103. Hankinson 73 or Wang 74 equations were used in Studies 111 and 110. For male patients, the Wang standard was applied for patients 6 to 17 years of age, and the Hankinson standard was applied for patients 18 years and older. For female patients, the Wang standard was applied for patients 6 to 15 years of age, and the Hankinson standard was applied for patients 16 years and older. a In Studies 102 and 103, the confirmed diagnosis of CF specified that patients must have had either chronic sinopulmonary disease OR gastrointestinal/nutritional abnormalities in addition to the other criteria specified. b Study 111 was a crossover study. Patients were randomized to receive both ivacaftor and placebo in 1 of 2 treatment sequences (ivacaftorplacebo and placeboivacaftor). 40
144 FDA Advisory Committee: Briefing Materials Page 144 of Demographic and Baseline Characteristics Table Study 112: Demographics and Baseline Characteristics, Full Analysis Set Variable Placebo/Ivacaftor N = 35 Ivacaftor/Ivacaftor N = 30 Overall N = 65 Sex, n (%) Male 15 (42.9) 13 (43.3) 28 (43.1) Female 20 (57.1) 17 (56.7) 37 (56.9) Race, n (%) White 35 (100.0) 30 (100.0) 65 (100.0) Ethnicity, n (%) Hispanic or Latino Not Hispanic or Latino 35 (100.0) 30 (100.0) 65 (100.0) Not Collected Per Local Regulations Age (Years at Study 110 Baseline) N Mean (SD) 32.7 (17.43) 31.0 (16.52) 31.9 (16.91) Age Group (Years at Study 110 Baseline), n (%) 6 to 11 8 (22.9) 7 (23.3) 15 (23.1) 12 to 17 1 (2.9) 0 1 (1.5) (74.3) 23 (76.7) 49 (75.4) Percent Predicted FEV 1 FAS N Mean (SD) 71.0 (21.5) 72.7 (19.5) 71.8 (20.4) 6 to 11 Years N Mean (SD) 97.5 (11.8) 85.8 (22.1) 92.1 (17.8) 18 Years N Mean (SD) 61.9 (15.8) 68.7 (17.2) 65.1 (16.6) Sweat Chloride (mmol/l) FAS N Mean (SD) (19.508) (18.141) (19.423) 6 to 11 Years N Mean (SD) (26.164) (25.732) (24.996) 18 Years N Mean (SD) (17.806) (15.750) (17.808) FEV 1 : forced expiratory volume in 1 second; SD: standard deviation Notes: All results displayed are baseline results in Study 112, except for patient age, which is the baseline age in Study 110. N is the number of patients with non-missing assessment at baseline. Baseline is defined as the most recent measurement before the first dose of study drug.
145 FDA Advisory Committee: Briefing Materials Page 145 of Concomitant Medications Table Study 110: Concomitant Medications Received by At Least 15% of Patients in Any Treatment Group, Full Analysis Set WHO Drug Dictionary Classification Placebo N = 35 n (%) Ivacaftor N = 34 n (%) Overall N = 69 n (%) Patients with Any Concomitant Medication 35 (100.0) 34 (100.0) 69 (100.0) Salbutamol 28 (80.0) 22 (64.7) 50 (72.5) Dornase Alfa 23 (65.7) 21 (61.8) 44 (63.8) Azithromycin 18 (51.4) 14 (41.2) 32 (46.4) Multivitamins, Combinations 10 (28.6) 13 (38.2) 23 (33.3) Fluticasone Propionate 10 (28.6) 9 (26.5) 19 (27.5) Paracetamol 13 (37.1) 4 (11.8) 17 (24.6) Tobramycin 9 (25.7) 7 (20.6) 16 (23.2) Colecalciferol 7 (20.0) 7 (20.6) 14 (20.3) Ibuprofen 5 (14.3) 9 (26.5) 14 (20.3) Seretide 7 (20.0) 7 (20.6) 14 (20.3) Omeprazole 9 (25.7) 4 (11.8) 13 (18.8) Cetirizine Hydrochloride 9 (25.7) 3 (8.8) 12 (17.4) Ciprofloxacin 5 (14.3) 7 (20.6) 12 (17.4) Aztreonam Lysine 6 (17.1) 4 (11.8) 10 (14.5) Budesonide w/formoterol Fumarate 6 (17.1) 4 (11.8) 10 (14.5) Colistin 6 (17.1) 1 (2.9) 7 (10.1) Doxycycline 6 (17.1) 2 (5.9) 8 (11.6) Levofloxacin 6 (17.1) 2 (5.9) 8 (11.6) Pancreatin 7 (20.0) 1 (2.9) 8 (11.6) Notes: Preferred Terms (PT) are sorted in descending order of frequency in the Overall column. A patient with multiple concomitant medications within Anatomical Therapeutic Chemical (ATC) level or PT is counted only once within the ATC level or PT. Concomitant medications were coded from the WHO Drug Dictionary Enhanced, March 2012.
146 FDA Advisory Committee: Briefing Materials Page 146 of Efficacy Results Study 110 Primary Endpoint: Sensitivity Analyses Table Study 110: Absolute Change From Baseline in Percent Predicted FEV 1, Sensitivity Analysis, Full Analysis Set Treatment Absolute Change From Baseline Treatment Difference (Ivacaftor vs Placebo) Sensitivity Analysis Group N LS Mean Difference (95% CI) P value Stratified Wilcoxon a Placebo Ivacaftor Dropout Reason-based Placebo Multiple Imputation (using Ivacaftor ANCOVA) b ( , ) Pattern Mixture Model c : Placebo Overall Ivacaftor ( , ) a Stratified (by age group and percent predicted FEV 1 severity at baseline) Wilcoxon rank-sum test on the endpoint of mean change from baseline. Medians are displayed in the LS Mean column. b ANCOVA model with drop-out reason based method. c Estimates from MMRM with the dependent variable absolute change from baseline; with fixed effects for visit, treatment, dropout pattern, interaction between dropout pattern and treatment, and interaction between dropout pattern and visit; and adjustment for continuous baseline value of percent predicted FEV 1 using compound symmetry covariance matrix. The overall treatment difference adjusting for dropout patterns was obtained from pattern-specific estimates by a weighted average.
147 FDA Advisory Committee: Briefing Materials Page 147 of Study 110: Figure of Time to First Pulmonary Exacerbation, FAS Figure 13-1 Study 110: Time to First Pulmonary Exacerbation, Full Analysis Set P r o p o r t i o n o f E x a c e r b a t i o n - F r e e S u b P la c e b o Iv a c a fto r S tu d y D a y
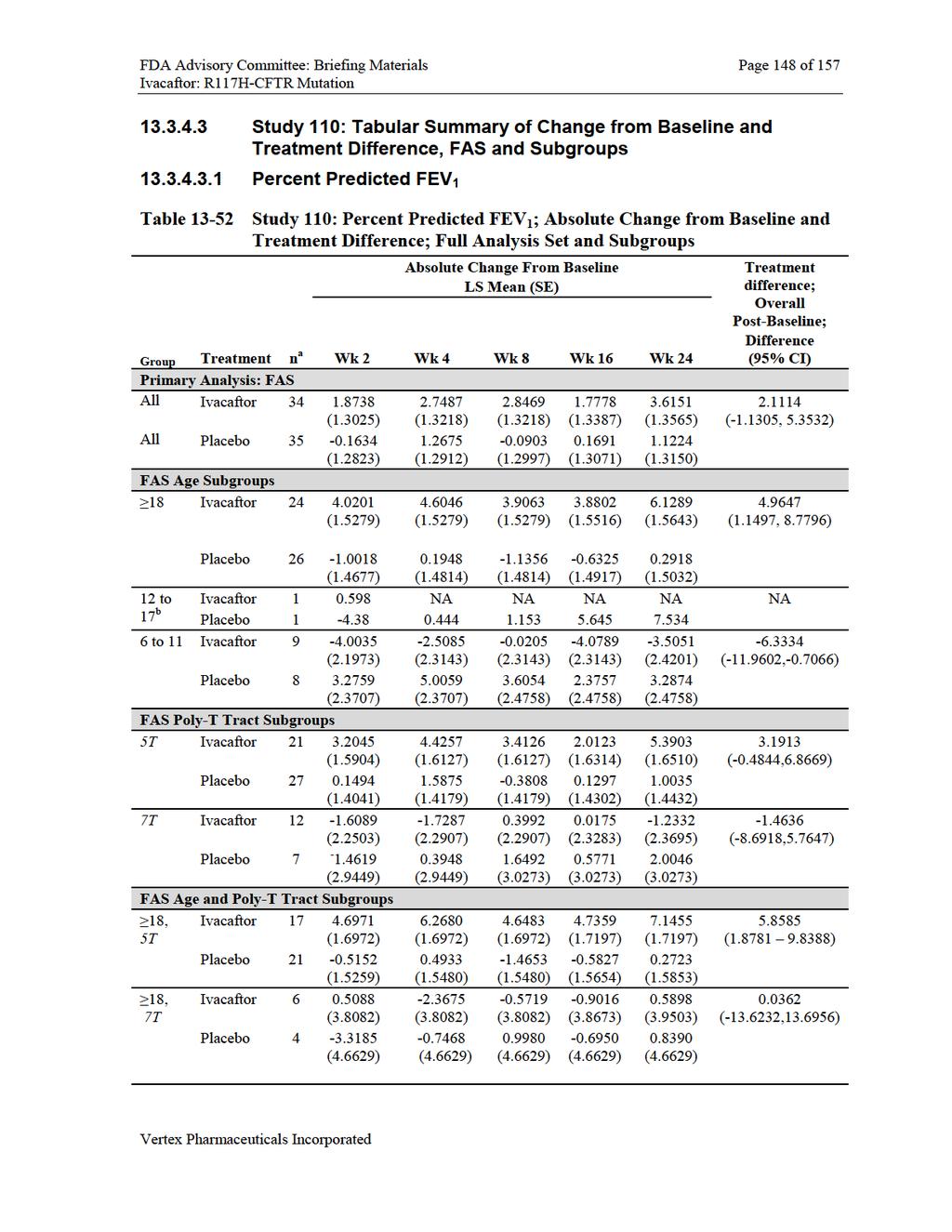
148
149
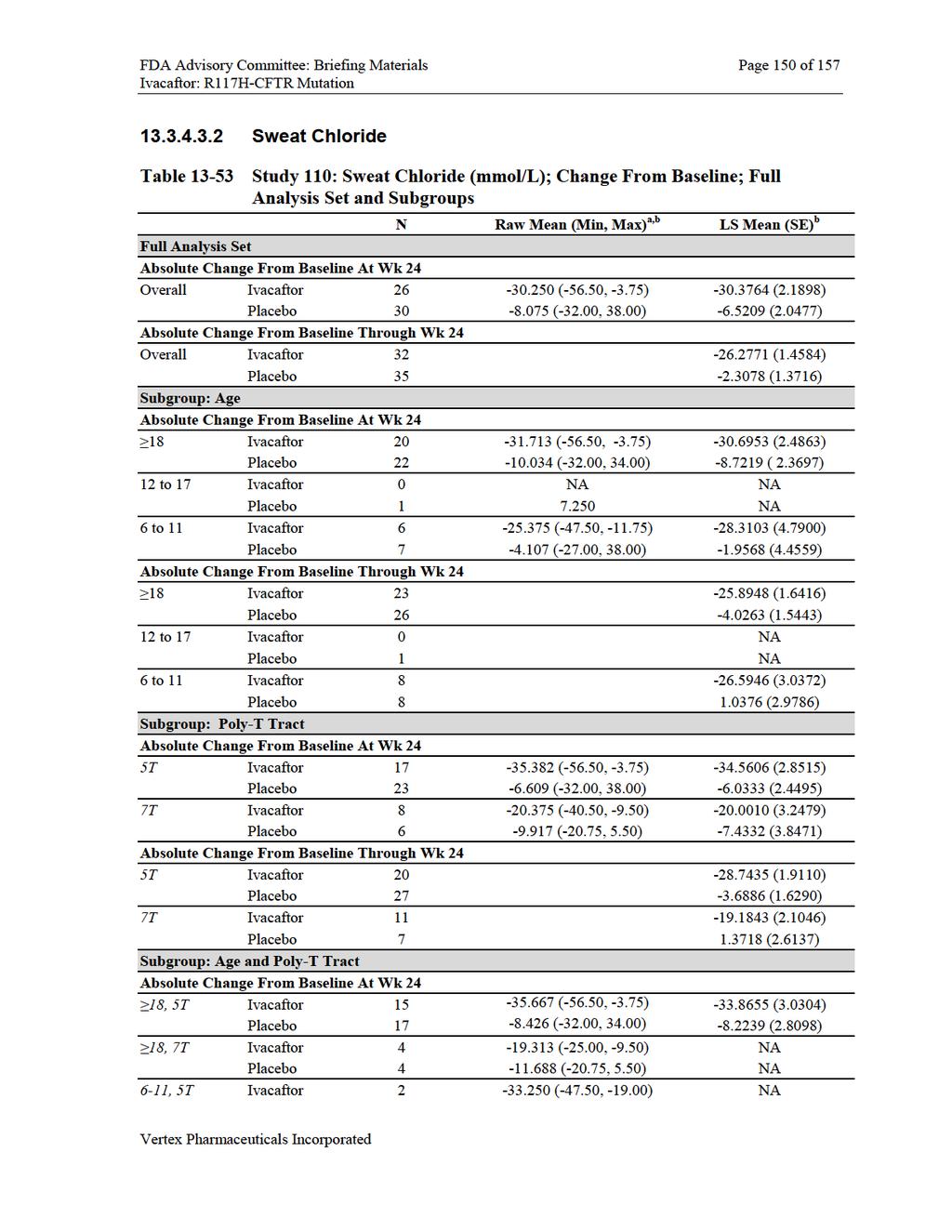
150
151

152
A Genetic Approach to the Treatment of Cystic Fibrosis
 A Genetic Approach to the Treatment of Cystic Fibrosis Peter Mueller, PhD Chief Scientific Officer and Executive Vice President Global Research and Development Vertex Pharmaceuticals, Incorporated March
A Genetic Approach to the Treatment of Cystic Fibrosis Peter Mueller, PhD Chief Scientific Officer and Executive Vice President Global Research and Development Vertex Pharmaceuticals, Incorporated March
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Moss RB, Flume PA, Elborn JS, et al, on behalf
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Moss RB, Flume PA, Elborn JS, et al, on behalf
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Cystic Fibrosis Transmembrane Page 1 of 13 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Cystic Fibrosis Transmembrane Conductance Regulator (CFTR) Prime Therapeutics
Cystic Fibrosis Transmembrane Page 1 of 13 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Cystic Fibrosis Transmembrane Conductance Regulator (CFTR) Prime Therapeutics
Transformational Treatments. PRESTON W. CAMPBELL, III, M.D. Executive Vice President for Medical Affairs
 Transformational Treatments PRESTON W. CAMPBELL, III, M.D. Executive Vice President for Medical Affairs Symptom-based CF Therapies 45 Median Predicted Survival Age of US Patients with Cystic Fibrosis 41
Transformational Treatments PRESTON W. CAMPBELL, III, M.D. Executive Vice President for Medical Affairs Symptom-based CF Therapies 45 Median Predicted Survival Age of US Patients with Cystic Fibrosis 41
Pharmacogenomics in Rare Diseases: Development Strategy for Ivacaftor as a Therapy for Cystic Fibrosis
 Pharmacogenomics in Rare Diseases: Development Strategy for Ivacaftor as a Therapy for Cystic Fibrosis Federico Goodsaid Vice President Strategic Regulatory Intelligence Vertex Pharmaceuticals Is there
Pharmacogenomics in Rare Diseases: Development Strategy for Ivacaftor as a Therapy for Cystic Fibrosis Federico Goodsaid Vice President Strategic Regulatory Intelligence Vertex Pharmaceuticals Is there
Brand Name: Kalydeco. Generic: ivacaftor. Manufacturer 1 : Vertex Pharmaceuticals Incorporated
 Brand Name: Kalydeco Generic: ivacaftor Manufacturer 1 : Vertex Pharmaceuticals Incorporated Drug Class 2,3 : Cystic Fibrosis Transmembrane Conductance Regulator (CFTR) Potentiator Uses: Labeled Uses 1,2,3,4,5
Brand Name: Kalydeco Generic: ivacaftor Manufacturer 1 : Vertex Pharmaceuticals Incorporated Drug Class 2,3 : Cystic Fibrosis Transmembrane Conductance Regulator (CFTR) Potentiator Uses: Labeled Uses 1,2,3,4,5
PA Update: Oral Cystic Fibrosis Modulators
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS
 ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals are asked
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals are asked
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Cystic Fibrosis Transmembrane Page 1 of 11 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Cystic Fibrosis Transmembrane Conductance Regulator (CFTR) Prime Therapeutics
Cystic Fibrosis Transmembrane Page 1 of 11 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Cystic Fibrosis Transmembrane Conductance Regulator (CFTR) Prime Therapeutics
Enabling CF Therapeutic Development
 Enabling CF Therapeutic Development PRESTON W. CAMPBELL, III, M.D. Executive Vice President for Medical Affairs No Disclosures Cystic Fibrosis In 1955 In 1955 most children with CF did not live long enough
Enabling CF Therapeutic Development PRESTON W. CAMPBELL, III, M.D. Executive Vice President for Medical Affairs No Disclosures Cystic Fibrosis In 1955 In 1955 most children with CF did not live long enough
Kalydeco. Kalydeco (ivacaftor) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.45.03 Subject: Kalydeco Page: 1 of 6 Last Review Date: November 30, 2018 Kalydeco Description Kalydeco
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.45.03 Subject: Kalydeco Page: 1 of 6 Last Review Date: November 30, 2018 Kalydeco Description Kalydeco
Cost-effectiveness of Ivacaftor (Kalydeco ) for the treatment of cystic fibrosis in patients age 6 years and older who have the G551D mutation
 for the treatment of cystic fibrosis in patients age 6 years and older who have the G551D mutation") Cost-effectiveness of Ivacaftor (Kalydeco ) for the treatment of cystic fibrosis in patients age 6 years and older who have the G551D mutation January 2013 1. A rapid review submission on the drug ivacaftor
Cost-effectiveness of Ivacaftor (Kalydeco ) for the treatment of cystic fibrosis in patients age 6 years and older who have the G551D mutation January 2013 1. A rapid review submission on the drug ivacaftor
TRANSPARENCY COMMITTEE
 The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 5 November 2014 KALYDECO 150 mg, film-coated tablet B/56 (CIP: 34009 266 060 5 3) Applicant: VERTEX INN ATC code Reason
The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 5 November 2014 KALYDECO 150 mg, film-coated tablet B/56 (CIP: 34009 266 060 5 3) Applicant: VERTEX INN ATC code Reason
Symdeko. Symdeko (tezacaftor and ivacaftor) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.45.10 Subject: Symdeko Page: 1 of 5 Last Review Date: June 22, 2018 Symdeko Description Symdeko (tezacaftor
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.45.10 Subject: Symdeko Page: 1 of 5 Last Review Date: June 22, 2018 Symdeko Description Symdeko (tezacaftor
Cystic Fibrosis Foundation Patient Registry 2013
 5/9/2015 Targeting CFTR to Treat Cystic Fibrosis: Small Molecule Therapy Mary Ellen Kleinhenz, MD Director, UCSF Adult Cystic Fibrosis Program Professor of Medicine UCSF Division of Pulmonary, Critical
5/9/2015 Targeting CFTR to Treat Cystic Fibrosis: Small Molecule Therapy Mary Ellen Kleinhenz, MD Director, UCSF Adult Cystic Fibrosis Program Professor of Medicine UCSF Division of Pulmonary, Critical
Opinion 7 November 2012
 The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 7 November 2012 KALYDECO 150 mg film-coated tablets B/56 (CIP code: 34009 266 060 5 3) Applicant: VERTEX INN ATC Code
The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 7 November 2012 KALYDECO 150 mg film-coated tablets B/56 (CIP code: 34009 266 060 5 3) Applicant: VERTEX INN ATC Code
THE ROLE OF CFTR MUTATIONS IN CAUSING CYSTIC FIBROSIS (CF)
") THE ROLE OF CFTR MUTATIONS IN CAUSING CYSTIC FIBROSIS (CF) Vertex Pharmaceuticals Incorporated, 50 Northern Avenue, Boston, MA 02210. Vertex and the Vertex triangle logo are registered trademarks for Vertex
THE ROLE OF CFTR MUTATIONS IN CAUSING CYSTIC FIBROSIS (CF) Vertex Pharmaceuticals Incorporated, 50 Northern Avenue, Boston, MA 02210. Vertex and the Vertex triangle logo are registered trademarks for Vertex
Scottish Paediatric Cystic Fibrosis MCN. Protocols / Guidelines. Ivacaftor: A guideline for use in paediatric CF patients in Scotland
 Scottish Paediatric Cystic Fibrosis MCN Protocols / Guidelines Ivacaftor: A guideline for use in paediatric CF patients in Scotland Authors: Dr Carol Dryden Dr Jane Wilkinson Miss Julie Crocker, Registered
Scottish Paediatric Cystic Fibrosis MCN Protocols / Guidelines Ivacaftor: A guideline for use in paediatric CF patients in Scotland Authors: Dr Carol Dryden Dr Jane Wilkinson Miss Julie Crocker, Registered
CADTH CANADIAN DRUG EXPERT COMMITTEE FINAL RECOMMENDATION
 CADTH CANADIAN DRUG EXPERT COMMITTEE FINAL RECOMMENDATION LUMACAFTOR / IVACAFTOR (Orkambi Vertex Pharmaceuticals [Canada] Inc.) Indication: Cystic Fibrosis, F508del-CFTR mutation Recommendation: The CADTH
CADTH CANADIAN DRUG EXPERT COMMITTEE FINAL RECOMMENDATION LUMACAFTOR / IVACAFTOR (Orkambi Vertex Pharmaceuticals [Canada] Inc.) Indication: Cystic Fibrosis, F508del-CFTR mutation Recommendation: The CADTH
The Future of CF Therapy
 The Future of CF Therapy Peter J. Mogayzel, Jr., M.D., Ph.D. Eudowood Division of Pediatric Respiratory Sciences The Johns Hopkins School of Medicine Overview The Future of CF Therapy Personalized therapy
The Future of CF Therapy Peter J. Mogayzel, Jr., M.D., Ph.D. Eudowood Division of Pediatric Respiratory Sciences The Johns Hopkins School of Medicine Overview The Future of CF Therapy Personalized therapy
Oral Cystic Fibrosis Modulators
 Oral Cystic Fibrosis Modulators Goals: To ensure appropriate drug use and limit to patient populations in which they have demonstrated to be effective and safe. To monitor for clinical response for appropriate
Oral Cystic Fibrosis Modulators Goals: To ensure appropriate drug use and limit to patient populations in which they have demonstrated to be effective and safe. To monitor for clinical response for appropriate
GLPG1837 in Subjects with Cystic Fibrosis (CF) and the G551D Mutation: results from a Phase II study (SAPHIRA1)
 and the G551D Mutation: results from a Phase II study (SAPHIRA1)") GLPG1837 in Subjects with Cystic Fibrosis (CF) and the G551D Mutation: results from a Phase II study (SAPHIRA1) ECFS, Sevilla, Spain 9 June 2017 Jane Davies on behalf of the SAPHIRA1 Study Team Copyright
GLPG1837 in Subjects with Cystic Fibrosis (CF) and the G551D Mutation: results from a Phase II study (SAPHIRA1) ECFS, Sevilla, Spain 9 June 2017 Jane Davies on behalf of the SAPHIRA1 Study Team Copyright
Pediatrics Grand Rounds 18 Sept University of Texas Health Science Center. + Disclosure. + Learning Objectives.
 Disclosure Dr Donna Willey Courand receives research support from Cystic Fibrosis Therapeutics The Cystic Fibrosis Foundation Children with Special Health Care Needs Cystic Fibrosis 05: Improving Survival
Disclosure Dr Donna Willey Courand receives research support from Cystic Fibrosis Therapeutics The Cystic Fibrosis Foundation Children with Special Health Care Needs Cystic Fibrosis 05: Improving Survival
Phase 3 EVOLVE & EXPAND Studies of Tezacaftor/Ivacaftor Combination Show Statistically Significant Improvements in Lung Function and Other Measures
 Phase 3 EVOLVE & EXPAND Studies of Tezacaftor/Ivacaftor Combination Show Statistically Significant Improvements in Lung Function and Other Measures in CF Patients March 29, 2017 Agenda Introduction Michael
Phase 3 EVOLVE & EXPAND Studies of Tezacaftor/Ivacaftor Combination Show Statistically Significant Improvements in Lung Function and Other Measures in CF Patients March 29, 2017 Agenda Introduction Michael
Orkambi. Orkambi (lumacaftor/ivacaftor) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.45.06 Subject: Orkambi Page: 1 of 6 Last Review Date: November 30, 2018 Orkambi Description Orkambi (lumacaftor/ivacaftor)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.45.06 Subject: Orkambi Page: 1 of 6 Last Review Date: November 30, 2018 Orkambi Description Orkambi (lumacaftor/ivacaftor)
ivacaftor 150mg film-coated tablets (Kalydeco ) SMC No. (1193/16) Vertex Pharmaceuticals (Europe) Ltd
 SMC No. (1193/16) Vertex Pharmaceuticals (Europe) Ltd") ivacaftor 150mg film-coated tablets (Kalydeco ) SMC No. (1193/16) Vertex Pharmaceuticals (Europe) Ltd 04 November 2016 The Scottish Medicines Consortium (SMC) has completed its assessment of the above
ivacaftor 150mg film-coated tablets (Kalydeco ) SMC No. (1193/16) Vertex Pharmaceuticals (Europe) Ltd 04 November 2016 The Scottish Medicines Consortium (SMC) has completed its assessment of the above
PRODUCT MONOGRAPH INCLUDING PATIENT MEDICATION INFORMATION KALYDECO. Ivacaftor tablets 150 mg Ivacaftor granules 50 mg per packet, 75 mg per packet
 PRODUCT MONOGRAPH INCLUDING PATIENT MEDICATION INFORMATION Pr KALYDECO Ivacaftor tablets 150 mg Ivacaftor granules 50 mg per packet, 75 mg per packet Cystic Fibrosis Transmembrane Conductance Regulator
PRODUCT MONOGRAPH INCLUDING PATIENT MEDICATION INFORMATION Pr KALYDECO Ivacaftor tablets 150 mg Ivacaftor granules 50 mg per packet, 75 mg per packet Cystic Fibrosis Transmembrane Conductance Regulator
Phase 1 and 2 Data for Triple Combination Regimens Demonstrate Improvements in Lung Function and Other Measures in CF Patients
 Phase 1 and 2 Data for Triple Combination Regimens Demonstrate Improvements in Lung Function and Other Measures in CF Patients July 18, 2017 Agenda Introduction Michael Partridge, VP Investor Relations
Phase 1 and 2 Data for Triple Combination Regimens Demonstrate Improvements in Lung Function and Other Measures in CF Patients July 18, 2017 Agenda Introduction Michael Partridge, VP Investor Relations
Cystic Fibrosis the future
 Cystic Fibrosis the future Pathophysiologic cascade Abnormal Gene Abnormal CFTR Therapy Gene replacement Protein replacement Gene read through therapy Abnormal sodium chloride & water movement through
Cystic Fibrosis the future Pathophysiologic cascade Abnormal Gene Abnormal CFTR Therapy Gene replacement Protein replacement Gene read through therapy Abnormal sodium chloride & water movement through
PFIZER INC. These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert.
 Public Disclosure Synopsis Protocol A7772 September 25 Final PFIZER INC. These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert.
Public Disclosure Synopsis Protocol A7772 September 25 Final PFIZER INC. These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert.
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS
 ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals are asked
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals are asked
Respiratory Pharmacology: Treatment of Cystic Fibrosis
 Respiratory Pharmacology: Treatment of Cystic Fibrosis Dr. Tillie-Louise Hackett Department of Anesthesiology, Pharmacology and Therapeutics University of British Columbia Associate Head, Centre of Heart
Respiratory Pharmacology: Treatment of Cystic Fibrosis Dr. Tillie-Louise Hackett Department of Anesthesiology, Pharmacology and Therapeutics University of British Columbia Associate Head, Centre of Heart
PFIZER INC. THERAPEUTIC AREA AND FDA APPROVED INDICATIONS: See United States Package Insert (USPI)
") PFIZER INC. These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert. For publications based on this study, see associated bibliography.
PFIZER INC. These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert. For publications based on this study, see associated bibliography.
Clinical Commissioning Policy: Ivacaftor for Cystic Fibrosis (named mutations)
") Clinical Commissioning Policy: Ivacaftor for Cystic Fibrosis (named mutations) Reference: NHS England: A01/P/c NHS England INFORMATION READER BOX Directorate Medical Commissioning Operations Patients and
Clinical Commissioning Policy: Ivacaftor for Cystic Fibrosis (named mutations) Reference: NHS England: A01/P/c NHS England INFORMATION READER BOX Directorate Medical Commissioning Operations Patients and
Synopsis Style Clinical Study Report SAR ACT sarilumab Version number : 1 (electronic 1.0)
") SYNOPSIS Title of the study: A randomized, double-blind, parallel-group, placebo- and active calibrator-controlled study assessing the clinical benefit of SAR153191 subcutaneous (SC) on top of methotrexate
SYNOPSIS Title of the study: A randomized, double-blind, parallel-group, placebo- and active calibrator-controlled study assessing the clinical benefit of SAR153191 subcutaneous (SC) on top of methotrexate
Class Update with New Drug Evaluation: Oral Cystic Fibrosis Modulators
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Cavosonstat Phase 2 Trial Results. November 28 th, 2016
 Phase 2 Trial Results November 28 th, 2016 Nivalis Therapeutics 2016 Agenda Introduction Mike Carruthers, Chief Financial Officer Initial Remarks Jon Congleton, President and CEO Data Highlights David
Phase 2 Trial Results November 28 th, 2016 Nivalis Therapeutics 2016 Agenda Introduction Mike Carruthers, Chief Financial Officer Initial Remarks Jon Congleton, President and CEO Data Highlights David
New Zealand Datasheet
 New Zealand Datasheet KALYDECO (ivacaftor) NAME OF THE MEDICINE Ivacaftor is N-(2,4-di-tert-butyl-5-hydroxyphenyl)-1,4-dihydro-4-oxoquinoline-3-carboxamide. The empirical formula of ivacaftor is C 24 H
New Zealand Datasheet KALYDECO (ivacaftor) NAME OF THE MEDICINE Ivacaftor is N-(2,4-di-tert-butyl-5-hydroxyphenyl)-1,4-dihydro-4-oxoquinoline-3-carboxamide. The empirical formula of ivacaftor is C 24 H
Drug Use Criteria: Ivacaftor (Kalydeco ) and Lumacaftor/Ivacaftor (Orkambi )
 and Lumacaftor/Ivacaftor (Orkambi )") Texas Vendor Program Use Criteria: (Kalydeco ) and Lumacaftor/ (Orkambi ) Publication History Developed: October 2012 Revised: December 2017; February 2016; June 2014. Notes: Information on indications
Texas Vendor Program Use Criteria: (Kalydeco ) and Lumacaftor/ (Orkambi ) Publication History Developed: October 2012 Revised: December 2017; February 2016; June 2014. Notes: Information on indications
ClinicalTrials.gov Protocol Registration and Results System (PRS) Receipt Release Date: October 3, ClinicalTrials.gov ID: NCT
 Receipt Release Date: October 3, ClinicalTrials.gov ID: NCT") ClinicalTrials.gov Protocol Registration and Results System (PRS) Receipt Release Date: October 3, 2012 ClinicalTrials.gov ID: NCT00457821 Study Identification Unique Protocol ID: VX06-770-101 Brief Title:
ClinicalTrials.gov Protocol Registration and Results System (PRS) Receipt Release Date: October 3, 2012 ClinicalTrials.gov ID: NCT00457821 Study Identification Unique Protocol ID: VX06-770-101 Brief Title:
We strive to develop innovative solutions that improve and extend the lives of people with cystic fibrosis
 Nivalis Therapeutics, Inc., October 2015 Analyst Breakfast at NACFC We strive to develop innovative solutions that improve and extend the lives of people with cystic fibrosis Disclaimer Regarding Forward
Nivalis Therapeutics, Inc., October 2015 Analyst Breakfast at NACFC We strive to develop innovative solutions that improve and extend the lives of people with cystic fibrosis Disclaimer Regarding Forward
IVACAFTOR THE ISRAELI EXPERIENCE ADI DAGAN MD THE ISRAELI CF CENTER SHEBA MEDICAL CENTER, TEL-HASHOMER
 IVACAFTOR THE ISRAELI EXPERIENCE ADI DAGAN MD THE ISRAELI CF CENTER SHEBA MEDICAL CENTER, TEL-HASHOMER February 21, 2014 U.S. Food and Drug Administration Approves KALYDECO (ivacaftor) for Use in Eight
IVACAFTOR THE ISRAELI EXPERIENCE ADI DAGAN MD THE ISRAELI CF CENTER SHEBA MEDICAL CENTER, TEL-HASHOMER February 21, 2014 U.S. Food and Drug Administration Approves KALYDECO (ivacaftor) for Use in Eight
What is the inheritance pattern (e.g., autosomal, sex-linked, dominant, recessive, etc.)?
?") Module I: Introduction to the disease Give a brief introduction to the disease, considering the following: the symptoms that define the syndrome, the range of phenotypes exhibited by individuals with the
Module I: Introduction to the disease Give a brief introduction to the disease, considering the following: the symptoms that define the syndrome, the range of phenotypes exhibited by individuals with the
North American Cystic Fibrosis Conference 27 October Noreen R Henig, MD Chief Development Officer ProQR Therapeutics
 Proof of Concept Study to Demonstrate the Effects of QR-010 on Nasal Potential Difference in Subjects With Cystic Fibrosis with the F508del CFTR Mutation Noreen R Henig, MD Chief Development Officer ProQR
Proof of Concept Study to Demonstrate the Effects of QR-010 on Nasal Potential Difference in Subjects With Cystic Fibrosis with the F508del CFTR Mutation Noreen R Henig, MD Chief Development Officer ProQR
12th Annual Meeting of the Oligonucleotide Therapeutics Society (OTS) 28 September 2016
 28 September 2016") A Randomized, Single-Blind, Placebo-Controlled, Phase /2 Study of ALN-AAT, an Investigational RNAi Therapeutic for the Treatment of Alpha- Antitrypsin Deficiency Associated Liver Disease: Interim Study
A Randomized, Single-Blind, Placebo-Controlled, Phase /2 Study of ALN-AAT, an Investigational RNAi Therapeutic for the Treatment of Alpha- Antitrypsin Deficiency Associated Liver Disease: Interim Study
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
SYNOPSIS. Study center(s) This study was conducted in the United States (128 centers).
 This study was conducted in the United States (128 centers).") Drug product: Drug substance(s): Document No.: Edition No.: Study code: Date: SYMBICORT pmdi 160/4.5 µg Budesonide/formoterol SD-039-0725 17 February 2005 SYNOPSIS A Twelve-Week, Randomized, Double-blind,
Drug product: Drug substance(s): Document No.: Edition No.: Study code: Date: SYMBICORT pmdi 160/4.5 µg Budesonide/formoterol SD-039-0725 17 February 2005 SYNOPSIS A Twelve-Week, Randomized, Double-blind,
The clinical trial information provided in this public disclosure synopsis is supplied for informational purposes only.
 The clinical trial information provided in this public disclosure synopsis is supplied for informational purposes only. Please note that the results reported in any single trial may not reflect the overall
The clinical trial information provided in this public disclosure synopsis is supplied for informational purposes only. Please note that the results reported in any single trial may not reflect the overall
The clinical trial information provided in this public disclosure synopsis is supplied for informational purposes only.
 The clinical trial information provided in this public disclosure synopsis is supplied for informational purposes only. Please note that the results reported in any single trial may not reflect the overall
The clinical trial information provided in this public disclosure synopsis is supplied for informational purposes only. Please note that the results reported in any single trial may not reflect the overall
The clinical trial information provided in this public disclosure synopsis is supplied for informational purposes only.
 The clinical trial information provided in this public disclosure synopsis is supplied for informational purposes only. Please note that the results reported in any single trial may not reflect the overall
The clinical trial information provided in this public disclosure synopsis is supplied for informational purposes only. Please note that the results reported in any single trial may not reflect the overall
Case Study What is the Relationship Between the Cell Membrane and Cystic Fibrosis?
 Names: Date: Case Study What is the Relationship Between the Cell Membrane and Cystic Fibrosis? Dr. Weyland examined a six month old infant that had been admitted to University Hospital earlier in the
Names: Date: Case Study What is the Relationship Between the Cell Membrane and Cystic Fibrosis? Dr. Weyland examined a six month old infant that had been admitted to University Hospital earlier in the
SYNOPSIS. First subject enrolled 15 August 2003 Therapeutic confirmatory (III) Last subject completed 03 February 2005
 Last subject completed 03 February 2005") Drug product: SYMBICORT pmdi 160/4.5 μg Drug substance(s): Budesonide/formoterol Study code: SD-039-0728 Edition No.: FINAL Date: 27 February 2006 SYNOPSIS A 52-week, randomized, double-blind, single-dummy,
Drug product: SYMBICORT pmdi 160/4.5 μg Drug substance(s): Budesonide/formoterol Study code: SD-039-0728 Edition No.: FINAL Date: 27 February 2006 SYNOPSIS A 52-week, randomized, double-blind, single-dummy,
"Management and Treatment of Patients with Cystic fibrosis (CF)
") "Management and Treatment of Patients with Cystic fibrosis (CF) Dr. Malena Cohen-Cymberknoh Pediatric Pulmonology and CF Center Hadassah Hebrew-University Medical Center Jerusalem, Israel Afula, March
"Management and Treatment of Patients with Cystic fibrosis (CF) Dr. Malena Cohen-Cymberknoh Pediatric Pulmonology and CF Center Hadassah Hebrew-University Medical Center Jerusalem, Israel Afula, March
North American Cystic Fibrosis Conference 27 October Noreen R Henig, MD Chief Development Officer ProQR Therapeutics
 Proof of Concept Study to Demonstrate the Effects of QR-010 on Nasal Potential Difference in Subjects With Cystic Fibrosis with the F508del CFTR Mutation Noreen R Henig, MD Chief Development Officer ProQR
Proof of Concept Study to Demonstrate the Effects of QR-010 on Nasal Potential Difference in Subjects With Cystic Fibrosis with the F508del CFTR Mutation Noreen R Henig, MD Chief Development Officer ProQR
CYSTIC FIBROSIS OBJECTIVES NO CONFLICT OF INTEREST TO DISCLOSE
 CYSTIC FIBROSIS Madhu Pendurthi MD MPH Staff Physician, Mercy Hospital Springfield, MO NO CONFLICT OF INTEREST TO DISCLOSE OBJECTIVES Epidemiology of Cystic Fibrosis (CF) Genetic basis and pathophysiology
CYSTIC FIBROSIS Madhu Pendurthi MD MPH Staff Physician, Mercy Hospital Springfield, MO NO CONFLICT OF INTEREST TO DISCLOSE OBJECTIVES Epidemiology of Cystic Fibrosis (CF) Genetic basis and pathophysiology
SYNOPSIS THIS IS A PRINTED COPY OF AN ELECTRONIC DOCUMENT. PLEASE CHECK ITS VALIDITY BEFORE USE.
 Drug product: Drug substance(s): Document No.: Edition No.: 1 Study code: Accolate Zafirlukast (ZD9188) 9188IL/0138 Date: 02 May 2007 SYNOPSIS A Multicenter, Randomized, Double-blind, -controlled, Parallel
Drug product: Drug substance(s): Document No.: Edition No.: 1 Study code: Accolate Zafirlukast (ZD9188) 9188IL/0138 Date: 02 May 2007 SYNOPSIS A Multicenter, Randomized, Double-blind, -controlled, Parallel
GSK Medicine: Study Number: Title: Rationale: Phase: Study Period: Study Design: Centers: Indication: Treatment: Objective:
 GSK Medicine: abacavir (ABC)/dolutegravir (DTG)/lamivudine (3TC) Study Number: 201147 Title: A IIIb, randomized, open-label study of the safety, efficacy, and tolerability of switching to a fixed-dose
GSK Medicine: abacavir (ABC)/dolutegravir (DTG)/lamivudine (3TC) Study Number: 201147 Title: A IIIb, randomized, open-label study of the safety, efficacy, and tolerability of switching to a fixed-dose
KALYDECO (ivacaftor) Tablets and Oral Granules
 Tablets and Oral Granules") HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use KALYDECO safely and effectively. See full prescribing information for KALYDECO. KALYDECO (ivacaftor)
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use KALYDECO safely and effectively. See full prescribing information for KALYDECO. KALYDECO (ivacaftor)
HIGHLIGHTS OF PRESCRIBING INFORMATION WARNINGS AND PRECAUTIONS
 HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use KALYDECO safely and effectively. See full prescribing information for KALYDECO. KALYDECO (ivacaftor)
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use KALYDECO safely and effectively. See full prescribing information for KALYDECO. KALYDECO (ivacaftor)
SYNOPSIS. Drug substance(s) Budesonide/formoterol Document No. Edition No. Study code SD Date 16 December 2004
 Budesonide/formoterol Document No. Edition No. Study code SD Date 16 December 2004") Drug product SYMBICORT pmdi 160/4.5 µg SYNOPSIS Drug substance(s) Budesonide/formoterol Document No. Edition No. Date 16 December 2004 A Twelve-Week, Randomized, Double-Blind, Double-Dummy, Placebo-Controlled
Drug product SYMBICORT pmdi 160/4.5 µg SYNOPSIS Drug substance(s) Budesonide/formoterol Document No. Edition No. Date 16 December 2004 A Twelve-Week, Randomized, Double-Blind, Double-Dummy, Placebo-Controlled
BRL /RSD-101RLL/1/CPMS-716. Report Synopsis
 Report Synopsis Study Title: A Multicenter, Open-label, Six-Month Extension Study to Assess the Long-term Safety of Paroxetine in Children and Adolescents with Major Depressive Disorder (MDD) or Obsessive-Compulsive
Report Synopsis Study Title: A Multicenter, Open-label, Six-Month Extension Study to Assess the Long-term Safety of Paroxetine in Children and Adolescents with Major Depressive Disorder (MDD) or Obsessive-Compulsive
A Case of Cystic Fibrosis
 Name(s) Date A Case of Cystic Fibrosis Dr. Weyland examined a six month old infant that had been admitted to University Hospital earlier in the day. The baby's parents had brought young Zoey to the emergency
Name(s) Date A Case of Cystic Fibrosis Dr. Weyland examined a six month old infant that had been admitted to University Hospital earlier in the day. The baby's parents had brought young Zoey to the emergency
Bristol-Myers Squibb
 A Study of the Safety and Efficacy of plus Tenofovir in Adults with Chronic Hepatitis B Virus Infection with Previous Nucleoside/Nucleotide Treatment Failure () FINAL CLINICAL STUDY REPORT EUDRACT Number:
A Study of the Safety and Efficacy of plus Tenofovir in Adults with Chronic Hepatitis B Virus Infection with Previous Nucleoside/Nucleotide Treatment Failure () FINAL CLINICAL STUDY REPORT EUDRACT Number:
SYNOPSIS A two-stage randomized, open-label, parallel group, phase III, multicenter, 7-month study to assess the efficacy and safety of SYMBICORT
 Drug product: Drug substance(s): Edition No.: Study code: SYMBICORT pmdi 160/4.5 g Budesonide/formoterol D5896C00005 Date: 8 May 2006 SYNOPSIS A two-stage randomized, open-label, parallel group, phase
Drug product: Drug substance(s): Edition No.: Study code: SYMBICORT pmdi 160/4.5 g Budesonide/formoterol D5896C00005 Date: 8 May 2006 SYNOPSIS A two-stage randomized, open-label, parallel group, phase
A Quick Guide to the. I507del. Mutation CFTR SCIENCE
 A Quick Guide to the I507del Mutation CFTR SCIENCE 2016 Vertex Pharmaceuticals Incorporated VXR-HQ-02-00045a(1) 03/2016 Loss of CFTR activity is the underlying cause of cystic fibrosis (CF) 1 Spectrum
A Quick Guide to the I507del Mutation CFTR SCIENCE 2016 Vertex Pharmaceuticals Incorporated VXR-HQ-02-00045a(1) 03/2016 Loss of CFTR activity is the underlying cause of cystic fibrosis (CF) 1 Spectrum
Clinical Study Report AI Final 28 Feb Volume: Page:
 Study Design, Continued Electrocardiogram (ECG) and vital sign assessments were done at select times during the study. Blood and urine samples for clinical laboratory evaluations were collected at specified
Study Design, Continued Electrocardiogram (ECG) and vital sign assessments were done at select times during the study. Blood and urine samples for clinical laboratory evaluations were collected at specified
The clinical trial information provided in this public disclosure synopsis is supplied for informational purposes only.
 The clinical trial information provided in this public disclosure synopsis is supplied for informational purposes only. Please note that the results reported in any single trial may not reflect the overall
The clinical trial information provided in this public disclosure synopsis is supplied for informational purposes only. Please note that the results reported in any single trial may not reflect the overall
A treatment option for patients with CF who have responsive mutations
 A treatment option for patients with CF who have responsive mutations INDICATIONS AND USAGE SYMDEKO is indicated for the treatment of patients with cystic fibrosis (CF) aged 12 years and older who are
A treatment option for patients with CF who have responsive mutations INDICATIONS AND USAGE SYMDEKO is indicated for the treatment of patients with cystic fibrosis (CF) aged 12 years and older who are
Sponsor. Novartis Pharmaceuticals Corporation Generic Drug Name. Agomelatine Therapeutic Area of Trial. Major depressive disorder Approved Indication
 Clinical Trial Results Database Page 1 Sponsor Novartis Pharmaceuticals Corporation Generic Drug Name Therapeutic Area of Trial Major depressive disorder Approved Indication Investigational drug Study
Clinical Trial Results Database Page 1 Sponsor Novartis Pharmaceuticals Corporation Generic Drug Name Therapeutic Area of Trial Major depressive disorder Approved Indication Investigational drug Study
PFIZER INC. THERAPEUTIC AREA AND FDA APPROVED INDICATIONS: See USPI.
 PFIZER INC. These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert. For publications based on this study, see associated bibliography.
PFIZER INC. These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert. For publications based on this study, see associated bibliography.
(For National Authority Use Only) Name of Study Drug: to Part of Dossier:
 Name of Study Drug: to Part of Dossier:") 2.0 Synopsis Abbott Laboratories Individual Study Table Referring to Part of Dossier: (For National Authority Use Only) Name of Study Drug: Volume: ABT-335 Name of Active Ingredient: Page: ABT-335, A-7770335.115
2.0 Synopsis Abbott Laboratories Individual Study Table Referring to Part of Dossier: (For National Authority Use Only) Name of Study Drug: Volume: ABT-335 Name of Active Ingredient: Page: ABT-335, A-7770335.115
Clinical Study Synopsis
 Clinical Study Synopsis This Clinical Study Synopsis is provided for patients and healthcare professionals to increase the transparency of Bayer's clinical research. This document is not intended to replace
Clinical Study Synopsis This Clinical Study Synopsis is provided for patients and healthcare professionals to increase the transparency of Bayer's clinical research. This document is not intended to replace
Evaluation of Patients with Diffuse Bronchiectasis
 Evaluation of Patients with Diffuse Bronchiectasis Dr. Patricia Eshaghian, MD Assistant Clinical Professor of Medicine Director, UCLA Adult Cystic Fibrosis Affiliate Program UCLA Division of Pulmonary
Evaluation of Patients with Diffuse Bronchiectasis Dr. Patricia Eshaghian, MD Assistant Clinical Professor of Medicine Director, UCLA Adult Cystic Fibrosis Affiliate Program UCLA Division of Pulmonary
PFIZER INC. THERAPEUTIC AREA AND FDA APPROVED INDICATIONS: See USPI.
 PFIZER INC. These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert. For publications based on this study, see associated bibliography.
PFIZER INC. These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert. For publications based on this study, see associated bibliography.
SYNOPSIS. Date 15 June 2004
 Drug product Drug substance(s) Document No. Edition No. Study code SYMBICORT pmdi 160/4.5 mg per actuation Budesonide/formoterol SD-039-0719 Date 15 June 2004 SYNOPSIS A Six-Month, Randomized, Open-Label
Drug product Drug substance(s) Document No. Edition No. Study code SYMBICORT pmdi 160/4.5 mg per actuation Budesonide/formoterol SD-039-0719 Date 15 June 2004 SYNOPSIS A Six-Month, Randomized, Open-Label
BRL /RSD-101C0F/1/CPMS-716. Report Synopsis
 Report Synopsis Study Title: A Multicenter, Open-label, Six-Month Extension Study to Assess the Long-Term Safety of Paroxetine in Children and Adolescents with Major Depressive Disorder (MDD) or Obsessive-Compulsive
Report Synopsis Study Title: A Multicenter, Open-label, Six-Month Extension Study to Assess the Long-Term Safety of Paroxetine in Children and Adolescents with Major Depressive Disorder (MDD) or Obsessive-Compulsive
Targeted therapies to improve CFTR function in cystic fibrosis
 Brodlie et al. Genome Medicine (2015) 7:101 DOI 10.1186/s13073-015-0223-6 REVIEW Targeted therapies to improve CFTR function in cystic fibrosis Malcolm Brodlie 1*, Iram J. Haq 2, Katie Roberts 2 and J.
Brodlie et al. Genome Medicine (2015) 7:101 DOI 10.1186/s13073-015-0223-6 REVIEW Targeted therapies to improve CFTR function in cystic fibrosis Malcolm Brodlie 1*, Iram J. Haq 2, Katie Roberts 2 and J.
2.0 Synopsis. Adalimumab M Clinical Study Report R&D/04/900. (For National Authority Use Only) Referring to Part of Dossier: Volume:
 Referring to Part of Dossier: Volume:") 2. Synopsis Abbott Laboratories Name of Study Drug: Name of Active Ingredient: Title of Study: Individual Study Table Referring to Part of Dossier: Volume: Page: (For National Authority Use Only) Phase
2. Synopsis Abbott Laboratories Name of Study Drug: Name of Active Ingredient: Title of Study: Individual Study Table Referring to Part of Dossier: Volume: Page: (For National Authority Use Only) Phase
Clinical Trial Synopsis
 Clinical Trial Synopsis Title of Study: A Phase III, Open-Label, Fixed-Dose Study to Determine the Safety of Long-Term Administration of TAK-375 in Subjects With Chronic Insomnia Protocol Number: Name
Clinical Trial Synopsis Title of Study: A Phase III, Open-Label, Fixed-Dose Study to Determine the Safety of Long-Term Administration of TAK-375 in Subjects With Chronic Insomnia Protocol Number: Name
SYNOPSIS Final Clinical Study Report for Study AI444031
 Name of Sponsor/Company: Bristol-Myers Squibb Name of Finished Product: Name of Active Ingredient: () Individual Study Table Referring to the Dossier (For National Authority Use Only) SYNOPSIS for Study
Name of Sponsor/Company: Bristol-Myers Squibb Name of Finished Product: Name of Active Ingredient: () Individual Study Table Referring to the Dossier (For National Authority Use Only) SYNOPSIS for Study
Clinical Trials for Rare Diseases in CDER
 Clinical Trials for Rare Diseases in CDER CDER Antibacterial Task Force/CTTI Think Tank October 11, 2012 Kathryn O Connell, MD PhD Medical Officer, Rare Diseases Program Office of New Drugs, CDER, FDA
Clinical Trials for Rare Diseases in CDER CDER Antibacterial Task Force/CTTI Think Tank October 11, 2012 Kathryn O Connell, MD PhD Medical Officer, Rare Diseases Program Office of New Drugs, CDER, FDA
The clinical trial information provided in this public disclosure synopsis is supplied for informational purposes only.
 The clinical trial information provided in this public disclosure synopsis is supplied for informational purposes only. Please note that the results reported in any single trial may not reflect the overall
The clinical trial information provided in this public disclosure synopsis is supplied for informational purposes only. Please note that the results reported in any single trial may not reflect the overall
2.0 Synopsis. ABT-333 M Clinical Study Report R&D/09/956
 2.0 Synopsis Abbott Laboratories Individual Study Table Referring to Part of Dossier: (For National Authority Use Only) Name of Study Drug: ABT-333 Volume: Name of Active Ingredient: Page: Sodium N-{6-[3-tert-butyl-5-(2,4-
2.0 Synopsis Abbott Laboratories Individual Study Table Referring to Part of Dossier: (For National Authority Use Only) Name of Study Drug: ABT-333 Volume: Name of Active Ingredient: Page: Sodium N-{6-[3-tert-butyl-5-(2,4-
Cystic Fibrosis: Progress in Treatment Management. Patrick A. Flume, M.D. Medical University of South Carolina
 Cystic Fibrosis: Progress in Treatment Management Patrick A. Flume, M.D. Medical University of South Carolina Disclosures Grant support Mpex Pharmaceuticals, Inc Gilead Sciences, Inc Bayer Healthcare AG
Cystic Fibrosis: Progress in Treatment Management Patrick A. Flume, M.D. Medical University of South Carolina Disclosures Grant support Mpex Pharmaceuticals, Inc Gilead Sciences, Inc Bayer Healthcare AG
SYNOPSIS. Clinical Study Report IM Double-blind Period
 Name of Sponsor/Company: Bristol-Myers Squibb Name of Finished Product: Abatacept () Name of Active Ingredient: Abatacept () Individual Study Table Referring to the Dossier SYNOPSIS (For National Authority
Name of Sponsor/Company: Bristol-Myers Squibb Name of Finished Product: Abatacept () Name of Active Ingredient: Abatacept () Individual Study Table Referring to the Dossier SYNOPSIS (For National Authority
Principal Investigator and Study Center: F. Nobuoka, MD Ageo Medical Clinic, 3133 Haraichi, Ageo City, Saitama , Japan
 Page 1 APPENDIX 9: ZRHM-PK-05-JP CLINICAL STUDY SUMMARY The study was conducted in Japan from August to November 2013. Principles as defined in International Conference on Harmonization (ICH) Good Clinical
Page 1 APPENDIX 9: ZRHM-PK-05-JP CLINICAL STUDY SUMMARY The study was conducted in Japan from August to November 2013. Principles as defined in International Conference on Harmonization (ICH) Good Clinical
ASSESSMENT REPORT FOR HEPSERA. International Nonproprietary Name: Adefovir Dipivoxil. Procedure No. EMEA/H/C/485/II/30
 London, 4 January 8 Product Name: Hepsera Procedure Number: EMEA/H/C/485/II/3 ASSESSMENT REPORT FOR HEPSERA International Nonproprietary Name: Adefovir Dipivoxil Procedure No. EMEA/H/C/485/II/3 7 Westferry
London, 4 January 8 Product Name: Hepsera Procedure Number: EMEA/H/C/485/II/3 ASSESSMENT REPORT FOR HEPSERA International Nonproprietary Name: Adefovir Dipivoxil Procedure No. EMEA/H/C/485/II/3 7 Westferry
Summary ID# Clinical Study Summary: Study B4Z-JE-LYBC
 CT Registry ID# 5285 Page 1 Summary ID# 5285 Clinical Study Summary: Study B4Z-JE-LYBC A Randomized, Double-Blind, Placebo-Controlled Efficacy and Safety Comparison of Fixed-Dose Ranges of Hydrochloride
CT Registry ID# 5285 Page 1 Summary ID# 5285 Clinical Study Summary: Study B4Z-JE-LYBC A Randomized, Double-Blind, Placebo-Controlled Efficacy and Safety Comparison of Fixed-Dose Ranges of Hydrochloride
Disclosures. Advances in the Management of Cystic Fibrosis: A Closer Look at the Roles of CFTR Modulation Therapy 10/28/2016
 Advances in the Management of Cystic Fibrosis: A Closer Look at the Roles of CFTR Modulation Therapy Susanna A McColley, MD Associate Chief Research Officer Stanley Manne Children s Research Institute
Advances in the Management of Cystic Fibrosis: A Closer Look at the Roles of CFTR Modulation Therapy Susanna A McColley, MD Associate Chief Research Officer Stanley Manne Children s Research Institute
Cystic Fibrosis. Jennifer McDaniel, BS, RRT-NPS
 Cystic Fibrosis Jennifer McDaniel, BS, RRT-NPS Overview Cystic fibrosis is the most common fatal, inherited disease in the U. S. CF results from a defective autosomal recessive gene One copy of gene =
Cystic Fibrosis Jennifer McDaniel, BS, RRT-NPS Overview Cystic fibrosis is the most common fatal, inherited disease in the U. S. CF results from a defective autosomal recessive gene One copy of gene =
Class Update: Oral Cystic Fibrosis Modulators
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
Cystic fibrosis (CF) is the most frequent. Ivacaftor treatment in patients with cystic REVIEW. Isabelle Sermet-Gaudelus
 is the most frequent. Ivacaftor treatment in patients with cystic REVIEW. Isabelle Sermet-Gaudelus") Eur Respir Rev 2013; 22: 127, 66 71 DOI: 10.1183/09059180.00008512 CopyrightßERS 2013 REVIEW Ivacaftor treatment in patients with cystic fibrosis and the G551D-CFTR mutation Isabelle Sermet-Gaudelus ABSTRACT:
Eur Respir Rev 2013; 22: 127, 66 71 DOI: 10.1183/09059180.00008512 CopyrightßERS 2013 REVIEW Ivacaftor treatment in patients with cystic fibrosis and the G551D-CFTR mutation Isabelle Sermet-Gaudelus ABSTRACT:
mg 25 mg mg 25 mg mg 100 mg 1
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
This clinical study synopsis is provided in line with Boehringer Ingelheim s Policy on Transparency and Publication of Clinical Study Data.
 abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the
abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the
Summary ID#7029. Clinical Study Summary: Study F1D-MC-HGKQ
 CT Registry ID# 7029 Page 1 Summary ID#7029 Clinical Study Summary: Study F1D-MC-HGKQ Clinical Study Report: Versus Divalproex and Placebo in the Treatment of Mild to Moderate Mania Associated with Bipolar
CT Registry ID# 7029 Page 1 Summary ID#7029 Clinical Study Summary: Study F1D-MC-HGKQ Clinical Study Report: Versus Divalproex and Placebo in the Treatment of Mild to Moderate Mania Associated with Bipolar
Mipomersen (ISIS ) Page 2 of 1979 Clinical Study Report ISIS CS3
 Page 2 of 1979 Clinical Study Report ISIS CS3") (ISIS 301012) Page 2 of 1979 2 SYNOPSIS ISIS 301012-CS3 synopsis Page 1 Title of Study: A Phase 2, Randomized, Double-Blind, Placebo-Controlled Study to Assess the Safety, Tolerability, Pharmacokinetics,
(ISIS 301012) Page 2 of 1979 2 SYNOPSIS ISIS 301012-CS3 synopsis Page 1 Title of Study: A Phase 2, Randomized, Double-Blind, Placebo-Controlled Study to Assess the Safety, Tolerability, Pharmacokinetics,
PFIZER INC. These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert.
 PFIZER INC. These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert. PROPRIETARY DRUG NAME / GENERIC DRUG NAME: Lyrica / Pregabalin
PFIZER INC. These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert. PROPRIETARY DRUG NAME / GENERIC DRUG NAME: Lyrica / Pregabalin
Clinical Study Synopsis
 Clinical Study Synopsis This Clinical Study Synopsis is provided for patients and healthcare professionals to increase the transparency of Bayer's clinical research. This document is not intended to replace
Clinical Study Synopsis This Clinical Study Synopsis is provided for patients and healthcare professionals to increase the transparency of Bayer's clinical research. This document is not intended to replace