ERJ Express. Published on October 24, 2007 as doi: / Biomedical and Health Sciences, London, United Kingdom.
|
|
|
- Madison Magdalen Banks
- 5 years ago
- Views:
Transcription
1 ERJ Express. Published on October 24, 2007 as doi: / Elevated expression of adenosine A 1 receptor in bronchial biopsies from asthmatic subjects R.A. Brown *, G.W. Clarke #, C.L. Ledbetter #, M.J. Hurle, J.C. Denyer, D.E. Simcock #, J.E. Coote, T.J. Savage, R.D. Murdoch, C.P. Page *, D. Spina *, B.J. O Connor #. * King s College London, Sackler Institute of Pulmonary Pharmacology, Division of Biomedical and Health Sciences, London, United Kingdom. # King s College London, Department of Asthma and Allergy, Division of Medicine, London, United Kingdom. GlaxoSmithKline, Stevenage, United Kingdom. Corresponding Author: Clive P. Page, Ph.D King s College London Sackler Institute of Pulmonary Pharmacology 5 th floor, Hodgkin Building, Guy s Campus, London, U.K., SE1 1UL Tel: +44 (0) Fax: +44 (0) clive.page@kcl.ac.uk Funded by a grant from GlaxoSmithKline, Stevenage, United Kingdom. Word count: Copyright 2007 by the European Respiratory Society.
2 ABSTRACT Asthmatics, unlike healthy subjects, bronchoconstrict in response to inhaled adenosine and extracellular adenosine concentrations are elevated in bronchoalveolar lavage fluid and exhaled breath condensate of asthmatic subjects. However, little is understood about the location and expression of adenosine receptors in asthmatic airways. Our aim was to first investigate the distribution of adenosine A 1 receptors in bronchial biopsies from mild asthmatic steroid-naïve subjects and then compare the degree of expression with healthy subjects. Biopsy sections were immunostained with an adenosine A 1 receptor antibody, the selectivity of which was validated in specific experiments. Image analysis was then performed to determine differences in immunostaining intensity. Immunostaining of biopsies from the asthmatic subjects revealed strong expression of the A 1 receptor located predominantly to the bronchial epithelium and bronchial smooth muscle. In comparison, very weak immunostaining was observed in biopsies obtained from healthy subjects. Image analysis revealed that the intensity of positive staining on the asthmatic bronchial epithelium and smooth muscle regions was significantly greater than that observed with the healthy epithelium and smooth muscle (P < 0.01). In conclusion, the sensitivity of asthmatics to inhaled adenosine coupled with increased adenosine A 1 receptor expression implicates a role for these receptors in the pathophysiology of this disease. Key Words-Adenosine, asthma, adenosine A 1 receptor, adenosine A 1 receptor expression 2
3 INTRODUCTION Adenosine is a purine nucleoside that is expressed in all cells of the body and involved in a wide range of physiological processes. The effects of adenosine are mediated predominantly through specific cell surface receptors of which four subtypes (A 1, A 2A, A 2B and A 3 ) have been described. It is now well recognised that extracellular levels of adenosine markedly increase under metabolically stressful conditions, such as hypoxia and inflammation, and whilst an acutely elevated level of extracellular adenosine is considered to mediate anti-inflammatory and protective effects, a chronic accumulation has been associated with pathological consequences [1]. In asthmatic subjects, it has been demonstrated that adenosine levels in bronchoalveolar lavage fluid and exhaled breath condensate are significantly higher than those present in healthy subjects [2, 3], and current evidence strongly suggests that it may contribute to the pathophysiology of asthma. For example, it has been recognised for many years that inhalation of adenosine 5 -monophophate (AMP) (5 - nucleotidase in the lung rapidly hydrolyses AMP to adenosine) in asthmatic but not healthy subjects results in dose-related bronchoconstriction [4], which is considered to be mediated predominantly, but not exclusively by, mast cell degranulation via A 2B receptor activation (reviewed in 5). Furthermore, inhalation of AMP has been shown to increase airway eosinophilia [6]. A role for adenosine in asthma is further supported by the observation that plasma adenosine levels rapidly increase following allergen challenge in asthmatic subjects [7], suggesting a possible involvement of endogenous adenosine in the early-phase 3
4 airway response to allergen. This possibility is supported in allergic rabbits where allergen-induced bronchoconstriction was blocked through the use of an anti-sense oligonucleotide directed against the A 1 receptor [8] and very recently with a selective adenosine A 1 receptor antagonist [9]. Furthermore, it has been demonstrated that the concentrations of adenosine are increased in both plasma and exhaled breath condensate during exercise-induced bronchoconstriction in subjects with asthma [10, 11], and finally, it has also been shown that isolated human asthmatic bronchial tissue contracts in response to adenosine via an A 1 receptor dependent mechanism [12]. In order to further investigate the role of endogenous adenosine in asthma, it is crucial that we extend our knowledge concerning the distribution and specific functions of adenosine receptors in asthmatic airways. To date, binding studies in healthy peripheral lung tissue have suggested that A 2 receptor subtypes are more abundant than the A 1 and A 3 receptor subtypes [13], and expression of the A 3 receptor was observed to be upregulated in asthmatic lung tissue, where it was located predominantly to eosinophils [14]. Therefore, our aim was to extend these observations. Although we ultimately intend to profile the expression of all four adenosine receptor subtypes and identify the subtype specific cellular functions, we hypothesized that characterising the distribution and expression of the A 1 receptor would particularly further our understanding of the role of adenosine in asthma given the observations detailed above. Thus, the distribution of the adenosine A 1 receptor in bronchial biopsies from asthmatic subjects was investigated and then compared to the distribution and level of expression with biopsies obtained from healthy subjects in order to provide further insight into the role of adenosine in asthma. 4
5 METHODS Further details of all methods and procedures can be found in the online depository. Subjects All of the asthmatic volunteers gave a clinical history consistent with intermittent, reversible airflow obstruction, and atopy to common aeroallergens. Thus, all of the asthmatic subjects (non-smoking) were characterised on the basis of a previous history of wheeze, a forced expiratory volume in 1 second (FEV 1 ) greater than 70% predicted, atopy as defined by a positive cutaneous response to intradermal allergen, and airways hyperresponsiveness to both methacholine and AMP. In addition, all asthmatic subjects demonstrated an increase in baseline FEV 1 of at least 15-20% in response to inhaled salbutamol (data not shown). Sixteen mild asthmatic subjects were screened for this study and twelve went on to complete bronchial provocation challenge with AMP and bronchoscopy (four subjects withdrew their consent to undergo bronchoscopy). Each subject had infrequent symptoms, controlled with occasional inhaled short-acting ß 2 -agonists alone. No subject was taking any regular anti-asthma therapy and none had taken inhaled corticosteroids for at least 3 months prior to entry. None of the subjects had an exacerbation of asthma or respiratory infection in the preceding 6 weeks and all subjects were non-smokers. Patient demographics are summarised in Table I. For comparison, biopsies from eight healthy age-matched non-smoking subjects obtained in a separate but recent previous study under the same conditions were also analysed. The demographics from these subjects are described in Table 1. Written informed consent was obtained from each subject and the study was approved by the Ethics Committee of King's College Hospital. 5
6 Study design Procedures at Visit 1 for all subjects included medical history and physical examination, an asthma characterisation questionaire, intradermal skin prick tests, spirometry and methacholine challenge to determine provocative concentration (PC) 20 values. After approximately 1 week, asthmatic subjects returned for Visit 2 where they underwent AMP challenge to determine the PC 20 to AMP. All subjects refrained from using rescue medication and caffeinated beverages for at least 8 hours before each visit. After a period of 3-4 weeks, all subjects returned for Visit 3 at which bronchoscopy was performed. Immunohistochemistry Using the methods described below to validate the adenosine receptor subtype specificity of an antibody, we found that the specificity of commercially available antibodies against all adenosine receptor subtypes was unsatisfactory, hence an antibody against the adenosine A 1 receptor was created specifically for the present study (the costs involved in obtaining a custom-made antibody was also a contributing factor when deciding not to concurrently profile expression of the other adenosine receptor subtypes). Thus, the custom-made affinity purified A 1 receptor polyclonal antibody was raised in the rabbit against a synthetic peptide corresponding to the amino acid sequence (CQPAPPIDEDLPEERPDD) of the COOH-terminus of the human A 1 receptor (Cambridge Research Biochemicals, Cleveland, U.K.). Brain cortex and cardiac tissue sections from 3 subjects were co-analysed as a positive control, as it is well established that these tissues highly express A 1 receptors. 6
7 Cadaveric brain cortex and cardiac tissue samples were obtained from the Institute of Psychiatry Brain Bank and Peterborough Tissue Bank respectively, following GlaxoSmithKline and United Kingdom guidelines for the acquisition and use of human tissues, including ethical approval and the use of appropriate consent forms. Frozen biopsies of brain cortex, cardiac tissue and bronchial tissue were sectioned at 6 µm. Sections were placed on Vectabond coated slides and the brain cortex and cardiac tissue sections fixed in ice-cold 4% w/v paraformaldehyde for 5 min (bronchial biopsies were fixed with 4% w/v paraformaldehyde prior to cryopreservation). Sections were then immunostained for the A 1 receptor using an Optimax automatic immunostaining machine (Biogenex, San Ramon, CA, USA). Positive staining was detected with diaminobenzidine in addition to counterstaining with Mayer s haematoxylin. Image analysis Fully automated densitometry of A 1 receptor expression was developed with the Zeisss Vision KS400 system (Carl Zeiss, Gottingen, Germany). Stain intensity is described in arbitrary units (A.U.). All image analysis and measurements were performed blind by one observer. Antibody validation with adenosine receptor transfected cells Further antibody validation experiments were performed through flow cytometric analysis of the A 1 receptor antibody binding to each adenosine receptor subtype 7
8 expressed on CHO-K1 cells (which lack any known subtype of adenosine receptor) transfected with the human recombinant A 1, A 2A, A 2B or A 3 receptor. Comparative expression levels of the adenosine receptor subtype in each cell line were first investigated using real-time RT-PCR. Data are expressed as gene copy number per 50 ng cdna. For flow cytometric analysis, cell lines were analyzed following antibody labelling by appropriate gating for immunofluorescence using a FACS Calibur flow cytometer (Beckton Dickinson, Oxford, U.K.) after excitation at 488 nm. At least 3,000 events were collected and mean fluorescence intensity values recorded. Statistics Data were analysed by unpaired Student s t-test, and unless stated otherwise, are expressed as mean ± SEM. 8
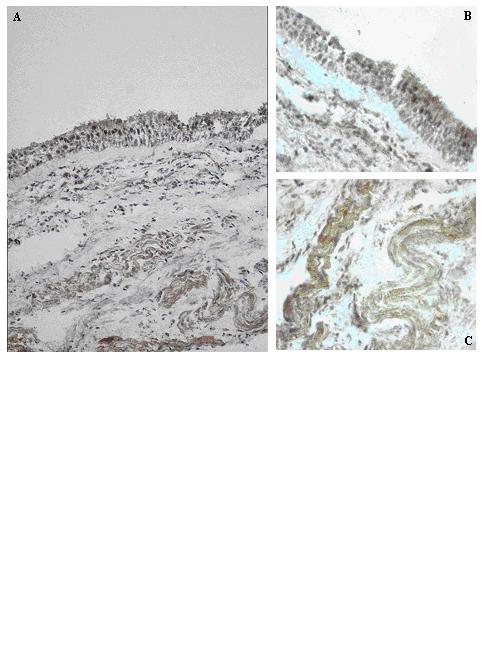
9 RESULTS Subjects Patient demographics are described in Table I. All asthmatic subjects who completed the study were hyperresponsive to AMP and methacholine (Table I). PC 20 values to methacholine in the eight non-atopic healthy subjects were all greater than 16 mg ml - 1. All asthmatic subjects exhibited a positive skin response to at least one allergen, whilst none of the healthy subjects responded to any of the allergens tested. Immunohistochemistry Positive immunostaining appeared brown against a blue background resulting from Mayer s haematoxylin counterstain. Immunostaining of bronchial biopsies obtained from asthmatic subjects with the A 1 receptor antibody consistently revealed strong positive staining on the bronchial epithelium and moderate to strong positive staining on the bronchial smooth muscle, these distinctive regions being identified morphologically (Figure 1, panels A-C). The immunostaining appeared to be distributed uniformly throughout the whole of these regions, rather than localised to specific areas or structures within these regions. By comparison, immunostaining of bronchial biopsies obtained from healthy subjects with the A 1 receptor antibody was strikingly less intense, with weak positive staining of the epithelium and very weak or sometimes undetectable positive staining of the smooth muscle (Figure 2, panels A- C). In all asthmatic and healthy bronchial biopsy sections, a negligible level of nonspecific staining was consistently observed with the isotype control antibody (data not shown). 9
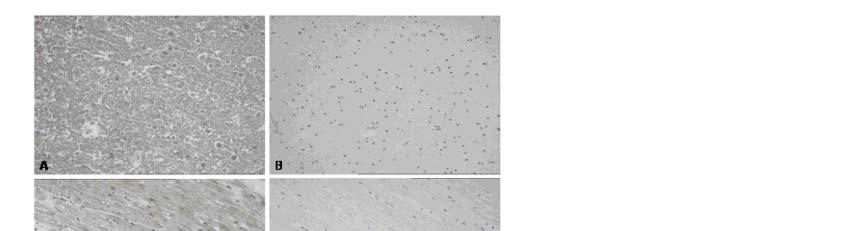
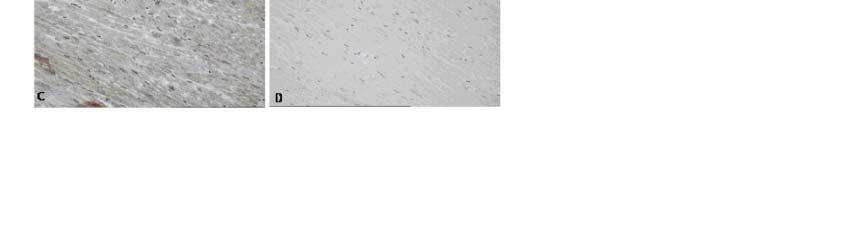
10 Sections obtained from 11 asthmatic subjects and 7 healthy subjects only were deemed of a suitable quality for image analysis as sections obtained from one subject in each study group lacked sufficient epithelial and smooth muscle areas required for the analysis. Quantification of the staining intensity of the epithelium revealed that the level of positive staining of the asthmatic epithelium was significantly more intense than that observed with the healthy epithelium (175.2 ± 5.3 A.U. vs 78.9 ± 30.9 A.U., P < 0.01). Similarly, the intensity of the immunostaining of the asthmatic bronchial smooth muscle was significantly greater than the immunostaining observed with the healthy bronchial smooth muscle (132.3 ± 9.9 A.U. vs 58.1 ± 24.4 A.U., P < 0.01) (Figure 3). Submucosal glands were identified on sections from two asthmatic bronchial biopsies and one healthy biopsy. Again, A 1 receptor expression appeared to be greater in the asthmatic biopsies (Figure 4, panel A), in comparison to the healthy biopsy (Figure 4, panel B). Both the brain cortex and cardiac tissue samples from all three subjects immunostained very strongly for the A 1 receptor (illustrated in Figure 5, panels A and C respectively), with no detectable staining observed with the isotype control antibody (Figure 4, panels B and D). A small degree of brown colouration observed in the cardiac tissue (panel D) was considered to be due to the presence of lipofuscin pigments. 10
11 A 1 receptor antibody validation In order to provide additional support to the observations resulting from the immunohistochemical analysis described above, antibody validation experiments were also performed to analyse the affinity and selectivity of the A 1 receptor antibody for the A 1 receptor. Quantitative RT-PCR of the CHO-K1 cell lines transfected with one of the four adenosine receptor subtypes revealed that each cell line expressed very high transcript levels of the transfected receptor and that the gene expression levels of each receptor were generally of a similar magnitude (Figure 6), although the level was slightly lower in the A 3 cell line. Subsequent flow cytometric analysis of the CHO-K1 cell lines using the A 1 receptor antibody resulted in a significant increase in the mean fluorescence intensity when compared to wild type CHO-K1 cells only in the A 1 cell line (478 A.U. ± 84 vs 35 A.U. ± 8; P < 0.01). There were no significant differences between any of the other cell lines and the wild type cells (Figure 6). 11
12 DISCUSSION Although the expression and functions of adenosine receptors have been studied in individual cell types, usually obtained from healthy subjects, there is very little information describing the distribution and relative expression of the four adenosine receptor subtypes in healthy or asthmatic airways. The aim of the present study therefore, was to investigate the distribution of A 1 receptors in bronchial biopsies obtained from mild asthmatic subjects and then compare the level of expression with biopsies taken from healthy subjects. Our data reveal that there is a low level of A 1 receptor expression present in healthy bronchial tissue, which appears to be predominantly located to the bronchial epithelium, whilst A 1 receptor expression is markedly elevated in asthmatic bronchial tissue, particularly on the bronchial epithelium and bronchial smooth muscle. Whilst the precise location of this receptor was not determined it is possible that this receptor is expressed on ciliated epithelial cells [15], goblet cells [16], sensory nerves [17], and smooth muscle cells [18]. Future studies using double labelling and confocal microscopy will discern the cell types involved. In an attempt to quantify the increased expression in asthmatic tissue, we performed image analysis on epithelial and smooth muscle areas on one tissue section from each biopsy. Image analysis thus revealed that the mean intensity of the staining in these regions of asthmatic tissue was significantly greater than that observed with healthy tissue, which therefore confirmed higher A 1 receptor expression. The A 1 receptor antibody used in this study was raised against a C-terminal portion of the A 1 receptor and was designed in order to limit the recognition of the other adenosine receptor subtypes by the antibody. To validate this antibody, experiments 12
13 were performed to provide evidence that the A 1 receptor antibody was able to selectively bind A 1 receptors. Flow cytometric analysis of CHO-K1 cells transfected with human recombinant adenosine receptors showed a significant increase in fluorescence only with the cell line expressing A 1 receptors when compared to wild type cells following incubation with the A 1 receptor antibody. The caveat to this is the assumption that there is similar adenosine receptor protein expression in each cell line. Although a formal comparison of protein expression was not attempted in the present study, an analysis of the mrna transcript levels revealed similar levels of gene expression in each cell line used in our experiments and though the A 3 receptor transcript level was slightly lower than the other subtypes, the level was still of a magnitude to expect a very high degree of actual receptor protein expression. Further confirmation that our antibody recognises and binds to the A 1 receptor was demonstrated by a high level of positive immunostaining on the brain cortex and cardiac tissue samples, tissues which are recognised to have a high expression of the A 1 receptor. Therefore, having validated the selectivity of the A 1 receptor antibody, we conclusively then demonstrated for the first time that the A 1 receptor is markedly upregulated in bronchial tissue from subjects with asthma who are responsive to AMP challenge, and confirmed that the difference was a consistent observation with image analysis. Given the limitations of immunohistochemistry and image analysis, we would expect that the image analysis data are certainly not proportionally representative of total A 1 receptor number but simply indicate that there is a difference in the pattern of A 1 receptor expression between the mild asthmatic and healthy phenotypes. 13
14 Our observations support a number of studies investigating adenosine receptor expression in animal models of allergic lung inflammation, which also identified an increase in airway A 1 receptor expression when compared to healthy naïve animals [8, 19-22]. In a rabbit model of allergic lung inflammation, it was demonstrated that the A 1 receptor was upregulated on the airway smooth muscle and a functional consequence of this increase was that it mediated bronchoconstriction following inhalation of adenosine [8, 23]. Given our observations, we could therefore speculate that an increase in A 1 receptors on bronchial smooth muscle in atopic mild asthmatic subjects may contribute to the bronchoconstrictor response to AMP observed in these subjects. In support of this possibility, an investigation into the spasmogenic effect of adenosine on isolated human bronchial strips showed a variable but overall small contractile response in tissue from healthy subjects and that the magnitude of this was significantly increased in tissue from asthmatic subjects [12]. The adenosine-induced contraction in isolated tissue from asthmatic subjects was significantly inhibited by the A 1 receptor antagonist 2-thio-[(1,3-dipropyl)-8-cyclopentyl]-xanthine (DPCPX). The same study also showed that the response could be blocked by preincubation with an H 1 antagonist and leukotriene synthesis inhibitor, suggesting that the response was mast cell mediated. However, a subsequent investigation demonstrated that isolated human bronchial tissue has a high degree of intrinsic tone and that histamine and leukotrienes constitute a major part of this basal tone [24]. Thus, it is difficult to ascertain to what degree the inhibition of adenosine-induced contractile responses by the H 1 receptor antagonist and leukotriene synthesis inhibitor in the former study can be attributed to the inhibition of mast cell products released by adenosine, or simply a reduction in basal tone. Hence, further studies investigating the effects of selective adenosine receptor agonists and antagonists on isolated asthmatic bronchial tissue are 14
15 required to provide further insight into A 1 -mediated contraction of bronchial smooth muscle obtained from subjects with asthma. On a cellular level, however, an investigation into adenosine receptor signalling pathways in isolated airway smooth muscle cells from healthy donors identified A 2B receptors as the predominant adenosine receptor subtype [25]. The A 1 receptor is the subtype with the highest affinity for adenosine (reviewed in 26), so we could speculate that on asthmatic bronchial smooth muscle cells, adenosine may preferentially activate the upregulated A 1 receptor. Since the A 1 receptor is G i -protein coupled, stimulation of this receptor would result in a decrease in camp, leading to smooth muscle contraction. In support of this, it has recently been demonstrated that activation of the A 1 receptor with a selective A 1 receptor agonist on healthy human airway smooth muscle cells in vitro induces calcium mobilisation [18]. Thus, given that H 1 receptor antagonists do not completely block AMP-induced bronchoconstriction in asthmatic subjects and co-administration of inhibitors of other mast cell products are not additive (reviewed in 4), it is likely that other mechanisms besides mast cell degranulation are involved in the response to AMP. Further studies are thus required to investigate these other mechanisms, including the potential direct spasmogenic effects of adenosine in asthmatic subjects. The functional significance of the increased expression of the A 1 receptor on the asthmatic bronchial epithelium remains to be established. However, a recent study demonstrated that activation of the A 1 receptor on tracheal epithelial cells resulted in an increase in mucin gene expression [16]. Our observation of an increase in A 1 receptor expression on the bronchial epithelium in asthmatic subjects thus further 15
16 implicates adenosine in promoting mucus hyperscretion via activation of the A 1 receptor. Furthermore, in tissue sections from three subjects, submucosal glands were identified. Two were from asthmatic subjects and high A 1 receptor expression was observed yet was not apparent in sections from the healthy subject, but these are only preliminary observations and further investigations are required before definitive conclusions can be made. However, adenosine has been shown to induce canine tracheal mucus secretion in vivo through an A 1 receptor dependent mechanism [27], supporting the notion of adenosine as a secretagogue. Interestingly, it has very recently been demonstrated that subjects with chronic obstructive pulmonary disease (COPD), who also have an increased extracellular level of adenosine in the airways, have an increased density of A 1, A 2A and A 3 receptors in the lung parenchyma when compared to age-matched smoking controls [28]. However, in order to investigate the role of adenosine in asthma further, our future studies will aim to characterise the expression of the other adenosine receptor subtypes in asthmatic subjects, in addition to investigating the effects of glucocorticosteroid treatment on adenosine receptor expression, since clinically glucocorticosteroids decrease hyperresponsiveness to AMP in subjects with asthma [29]. Our evidence of an increased adenosine A 1 receptor expression in asthmatic subjects reflects studies characterising adenosine receptor expression in mice partially lacking adenosine deaminase [30]. These mice accumulate high levels of adenosine extracellularly and exhibit severe pulmonary inflammation. Some of the pathological features reported in this model were consistent with those observed in asthma such as 16
17 mucus hypersecretion, but the pulmonary inflammatory cell profile differed considerably and consisted mainly of macrophages, with no increase in eosinophil numbers. However, transcript levels for the A 1, A 2B and A 3 receptors were found to be significantly increased, suggesting that an increase in extracellular adenosine promotes adenosine receptor signalling. The pulmonary inflammation in mice totally deficient in adenosine deaminase was even more severe and the mice died at three weeks of age from respiratory distress [31]. Interestingly, concurrent knockout of the adenosine A 1 receptor was reported to exacerbate the inflammation further, suggesting a protective role of the A 1 receptor in this model [32]. However, the levels of eosinophils in this model were of a magnitude unlikely to result in alterations in airways responsiveness and therefore the relevance of these findings to asthma should be interpreted with caution (less than 2% of total cells, compared with approximately 40% of total in a murine model of allergic inflammation [33]). In conclusion therefore, we have demonstrated for the first time that adenosine A 1 receptor expression is markedly upregulated in bronchial tissue obtained from subjects with asthma who are responsive to AMP challenge, particularly on bronchial smooth muscle and the airway epithelium. Acknowledgements We thank David Hall and Ken Saunders for technical assistance with flow cytometry. 17
18 References 1. Hasko G, Cronstein BN. Adenosine: an endogenous regulator of innate immunity. Trends Immunol 2004: 25: Driver AG, Kukoly CA, Ali S, Mustafa, S.J. Adenosine in bronchoalveolar lavage fluid in asthma. Am Rev Respir Dis 1993: 148: Huszar E, Vass G, Vizi E, Csoma Z, Barat E, Molnar Vilagos G, Herjavecz I. Horvath, I. Adenosine in exhaled breath condensate in healthy volunteers and in patients with asthma. Eur Respir J 2002: 20: Meade CJ, Dumont I, Worrall L. Why do asthmatic subjects respond so strongly to inhaled adenosine? Life Sci 2001: 69: Forsythe P, Ennis M. Adenosine, mast cells and asthma. Inflamm Res 1999: 48: van den Berge M, Kerstjens HA, de Reus DM, Koeter GH, Kauffman HF, Postma DS. Provocation with adenosine 5'-monophosphate, but not methacholine, induces sputum eosinophilia. Clin Exp Allergy 2004: 34: Mann JS, Holgate ST, Renwick AG, Cushley MJ. Airway effects of purine nucleosides and nucleotides and release with bronchial provocation in asthma. J Appl Physiol 1986: 61:
19 8. Nyce JW, Metzger WJ. DNA antisense therapy for asthma in an animal model. Nature 1997: 385: Obiefuna PC, Batra VK, Nadeem A, Borron P, Wilson CN, Mustafa SJ. A Novel A 1 Adenosine Receptor Antagonist (L-97-1) Reduces Allergic Responses to House Dust Mite in an Allergic Rabbit Model of Asthma. J Pharmacol Exp Ther 2005: 315: Vizi E, Huszar E, Csoma Z, Boszormenyi-Nagy G, Barat E, Horvath I, Herjavecz I, Kollai M. Plasma adenosine concentration increases during exercise: a possible contributing factor in exercise-induced bronchoconstriction in asthma. J Allergy Clin Immunol 2002: 109: Csoma Z, Huszar E, Vizi E, Vass G, Szabo Z, Herjavecz I, Kollai M, Horvath I. Adenosine level in exhaled breath increases during exercise-induced bronchoconstriction. Eur Respir J 2005: 25: Bjorck T, Gustafsson LE, Dahlen SE. Isolated bronchi from asthmatics are hyperresponsive to adenosine, which apparently acts indirectly by liberation of leukotrienes and histamine. Am Rev Respir Dis 1992: 145: Joad JP. Characterization of the human peripheral lung adenosine receptor. Am J Respir Cell Mol Biol 1990: 2:
20 14. Walker BA, Jacobson MA, Knight DA, Salvatore CA, Weir T, Zhou D, Bai TR. Adenosine A 3 receptor expression and function in eosinophils. Am J Respir Cell Mol Biol 1997: 16: McCoy DE, Schwiebert EM, Karlson KH, Spielman WS, Stanton BA. Identification and function of A 1 adenosine receptors in normal and cystic fibrosis human airway epithelial cells. Am J Physiol 1995: 268(6 Pt 1): C McNamara N, Gallup M, Khong A, Sucher A, Maltseva I, Fahy J, Basbaum C. Adenosine up-regulation of the mucin gene, MUC2, in asthma. FASEB J 2004: 18: Chuaychoo B, Lee MG, Kollarik M, Pullmann R, Undem BJ. Evidence for both adenosine A 1 and A 2A receptors activating single vagal sensory C-fibres in guinea pig lungs. J Physiol 2006: 575(Pt 2): Ethier MF, Madison JM. Adenosine A 1 receptors mediate mobilization of calcium in human bronchial smooth muscle cells. Am J Respir Cell Mol Biol 2006: 35: Ali S, Mustafa SJ, Metzger WJ. Adenosine receptor-mediated bronchoconstriction and bronchial hyperresponsiveness in allergic rabbit model. Am J Physiol 1994: 266: L
21 20. Ali S, Mustafa SJ, Metzger WJ. Adenosine-induced bronchoconstriction and contraction of airway smooth muscle from allergic rabbits with late-phase airway obstruction: evidence for an inducible adenosine A 1 receptor. J Pharmacol Exp Ther 1994: 268: el-hashim A, D'Agostino B, Matera MG, Page C. Characterization of adenosine receptors involved in adenosine-induced bronchoconstriction in allergic rabbits. Br J Pharmacol 1996: 119: Pauwels RA, Joos GF. Characterization of the adenosine receptors in the airways. Arch Int Pharmacodyn Ther 1995: 329: Abebe W, Mustafa SJ. A 1 adenosine receptor-mediated Ins(1,4,5)P3 generation in allergic rabbit airway smooth muscle. Am J Physiol 1998: 275: L Ellis JL, Undem BJ. Role of cysteinyl-leukotrienes and histamine in mediating intrinsic tone in isolated human bronchi. Am J Respir Crit Care Med 1994: 149: Mundell SJ, Olah ME, Panettieri RA, Benovic JL, Penn RB. Regulation of G protein-coupled receptor-adenylyl cyclase responsiveness in human airway smooth muscle by exogenous and autocrine adenosine. Am J Respir Cell Mol Biol 2001: 24:
22 26. Marx D, Ezeamuzie CI, Nieber K, Szelenyi I. Therapy of bronchial asthma with adenosine receptor agonists and antagonists. Drug News Perspect 2001: 14: Johnson HG, McNee ML. Adenosine-induced secretion in the canine trachea: modification by methylxanthines and adenosine derivatives. Br J Pharmacol 1985: 86: Varani K, Caramori G, Vincenzi F, Adcock I, Casolari P, Leung E, Maclennan S, Gessi S, Morello S, Barnes PJ, Ito K, Chung KF, Cavallesco G, Azzena G, Papi A, Borea PA. Alteration of adenosine receptors in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2006: 173: Spicuzza L, Bonfiglio C, Polosa R. Research applications and implications of adenosine in diseased airways. Trends Pharmacol Sci 2003: 24: Chunn JL, Young HWJ, Banerjee SK, Colasurdo GN, Blackburn MR. Adenosinedependent airway inflammation and hyperresponsiveness in partially adenosine deaminase-deficient mice. J Immunol 2001: 167: Blackburn MR, Volmer JB, Thrasher JL, Zhong H, Crosby JR, Lee JJ, Kellems RE. Metabolic consequences of adenosine deaminase deficiency in mice are associated with defects in alveogenesis, pulmonary inflammation, and airway obstruction. J Exp Med 2000: 192:
23 32. Sun CX, Young HW, Molina JG, Volmer JB, Schnermann J, Blackburn MR. A protective role for the A 1 adenosine receptor in adenosine-dependent pulmonary injury. J Clin Invest 2005: 115: Riffo-Vasquez Y, Spina D, Page C, Tormay P, Singh M, Henderson B, Coates A. Effect of Mycobacterium tuberculosis chaperonins on bronchial eosinophilia and hyper-responsiveness in a murine model of allergic inflammation. Clin Exp Allergy 2004: 34:
24 Tables Table I Patient demographics Asthmatic Healthy Number 16 8 Sex (male:female) 11:5 4:4 Age (yr) 26.6 (20-36)* 25.6 (20-37)* Baseline FEV 1 (%predicted) 92.7 (74-120)* (89-127)* Height (cm) ( )* 179 ( )* Weight (Kg) 74 (56-95)* 79.2 (52-106)* AMP PC 20 (mg ml -1 ) 28.1 ( )* N/A Methacholine PC 20 (mg ml -1 ) 1.13 ( ) >16 mg ml -1 *Geometric mean (range) 24
25 Figure legends Figure 1 Photomicrographs representative of positive immunostaining of asthmatic bronchial biopsy sections with an A 1 receptor antibody. Positive immunostaining has a brown appearance against a blue background resulting from Mayer s haematoxylin counterstain. Panel A (X 200) shows high expression of the A 1 receptor on the epithelium and smooth muscle, the same section is also shown in panels B and C respectively at 400 X magnification, in order to see the epithelium (B) and smooth muscle (C) more clearly. 25
26 26
27 27

 shows weak expression of the A 1 receptor on the epithelium and virtually no positive immunostaining of")
28 Figure 2 Photomicrographs representative of positive immunostaining of healthy bronchial biopsy sections with an A 1 receptor antibody. Positive immunostaining has a brown appearance against a blue background resulting from Mayer s haematoxylin counterstain. Panel A (X 200) shows weak expression of the A 1 receptor on the epithelium and virtually no positive immunostaining of smooth muscle. Panels B and C show the epithelium and smooth muscle respectively at 400 X magnification for clarity. 28
29 Figure 3 Image analysis of asthmatic and healthy bronchial biopsies immunostained with an A 1 receptor antibody. The intensity of positive staining specifically on the epithelium and smooth muscle on bronchial biopsy sections from 11 asthmatic subjects and 7 healthy subjects (1 section per subject) was quantified using Zeiss Vision KS400 software, from 4 different views of both epithelium and smooth muscle at 1000X magnification. Data are expressed as the mean of intensity staining ± SEM, **P < 0.01 and ## P <
30 30
31 31

32 Figure 4 Photomicrographs representative of immunostaining of asthmatic and healthy bronchial biopsy sections with an A 1 receptor antibody. Positive immunostaining has a brown appearance against a blue background resulting from Mayer s haematoxylin counterstain. Panel A (X 400) shows high expression of the A 1 receptor on the submucosal glands, panel B (X 400) shows no apparent positive immunostaining of healthy submucosal glands. 32
33 Figure 5 Photomicrographs (X 200) illustrating positive staining of brain cortex and cardiac tissue with the A 1 antibody (panels A and C respectively). Positive immunostaining is identified by a brown appearance against a blue background resulting from Mayer s haematoxylin counterstain. Panels B and D respectively show the negligible staining of brain cortex and cardiac sections from the same samples following staining with an isotype control antibody. 33
34 34
35 Figure 6 Quantitative real-time RT-PCR (A) and flow cytometric analysis (B) of CHO-K1 cells transfected with the human recombinant adenosine A 1, A 2A, A 2B or A 3 receptor. Expression of each transfected receptor was analysed using the appropriate primer pair and probe described in Table II in the online supplementary material. PE-labelled cells were analyzed by appropriate gating for immunofluorescence after excitation at 488 nm. At least 3,000 events were collected and mean fluorescence intensity values recorded. Results are from 3 separate experiments and data are expressed as mean copy number per 50 ng cdna ± SEM (A) and mean fluorescence intensity (A.U. ± SEM) (B) respectively. An increase in fluorescence is observed only in the A 1 transfected cell line (**P < 0.01 when compared to wild type cells). 35
36 36
37 37
Immunology of Asthma. Kenneth J. Goodrum,Ph. Ph.D. Ohio University College of Osteopathic Medicine
 Immunology of Asthma Kenneth J. Goodrum,Ph Ph.D. Ohio University College of Osteopathic Medicine Outline! Consensus characteristics! Allergens:role in asthma! Immune/inflammatory basis! Genetic basis!
Immunology of Asthma Kenneth J. Goodrum,Ph Ph.D. Ohio University College of Osteopathic Medicine Outline! Consensus characteristics! Allergens:role in asthma! Immune/inflammatory basis! Genetic basis!
Soluble ADAM33 initiates airway remodeling to promote susceptibility for. Elizabeth R. Davies, Joanne F.C. Kelly, Peter H. Howarth, David I Wilson,
 Revised Suppl. Data: Soluble ADAM33 1 Soluble ADAM33 initiates airway remodeling to promote susceptibility for allergic asthma in early life Elizabeth R. Davies, Joanne F.C. Kelly, Peter H. Howarth, David
Revised Suppl. Data: Soluble ADAM33 1 Soluble ADAM33 initiates airway remodeling to promote susceptibility for allergic asthma in early life Elizabeth R. Davies, Joanne F.C. Kelly, Peter H. Howarth, David
Systems Pharmacology Respiratory Pharmacology. Lecture series : General outline
 Systems Pharmacology 3320 2017 Respiratory Pharmacology Associate Professor Peter Henry (Rm 1.34) Peter.Henry@uwa.edu.au Division of Pharmacology, School of Biomedical Sciences Lecture series : General
Systems Pharmacology 3320 2017 Respiratory Pharmacology Associate Professor Peter Henry (Rm 1.34) Peter.Henry@uwa.edu.au Division of Pharmacology, School of Biomedical Sciences Lecture series : General
Differential Effect of Formoterol on Adenosine Monophosphate and Histamine Reactivity in Asthma
 Differential Effect of Formoterol on Adenosine Monophosphate and Histamine Reactivity in Asthma JULIA A. NIGHTINGALE, DUNCAN F. ROGERS, and PETER J. BARNES Thoracic Medicine, National Heart and Lung Institute,
Differential Effect of Formoterol on Adenosine Monophosphate and Histamine Reactivity in Asthma JULIA A. NIGHTINGALE, DUNCAN F. ROGERS, and PETER J. BARNES Thoracic Medicine, National Heart and Lung Institute,
COPD and Asthma: Similarities and differences Prof. Peter Barnes
 and Asthma: Similarities and Differences and Asthma: 1 Imperial College Peter Barnes FRS, FMedSci, National Heart & Lung Institute Imperial College, London, UK p.j.barnes@imperial.ac.uk Royal Brompton
and Asthma: Similarities and Differences and Asthma: 1 Imperial College Peter Barnes FRS, FMedSci, National Heart & Lung Institute Imperial College, London, UK p.j.barnes@imperial.ac.uk Royal Brompton
Adenosine 5 0 -monophosphate increases levels of leukotrienes in breath condensate in asthma
 Respiratory Medicine (2004) 98, 651 655 Adenosine 5 0 -monophosphate increases levels of leukotrienes in breath condensate in asthma E. Bucchioni, Z. Csoma, L. Allegra, K.F. Chung, P.J. Barnes, S.A. Kharitonov*
Respiratory Medicine (2004) 98, 651 655 Adenosine 5 0 -monophosphate increases levels of leukotrienes in breath condensate in asthma E. Bucchioni, Z. Csoma, L. Allegra, K.F. Chung, P.J. Barnes, S.A. Kharitonov*
Exhaled Nitric Oxide: An Adjunctive Tool in the Diagnosis and Management of Asthma
 Exhaled Nitric Oxide: An Adjunctive Tool in the Diagnosis and Management of Asthma Jason Debley, MD, MPH Assistant Professor, Pediatrics Division of Pulmonary Medicine University of Washington School of
Exhaled Nitric Oxide: An Adjunctive Tool in the Diagnosis and Management of Asthma Jason Debley, MD, MPH Assistant Professor, Pediatrics Division of Pulmonary Medicine University of Washington School of
Respiratory Pharmacology PCTH 400 Asthma and β-agonists
 Respiratory Pharmacology PCTH 400 Asthma and β-agonists Dr. Tillie-Louise Hackett Department of Anesthesiology, Pharmacology and Therapeutics University of British Columbia Associate Director, Centre of
Respiratory Pharmacology PCTH 400 Asthma and β-agonists Dr. Tillie-Louise Hackett Department of Anesthesiology, Pharmacology and Therapeutics University of British Columbia Associate Director, Centre of
Mechanisms of action of bronchial provocation testing
 Mechanisms of action of bronchial provocation testing TSANZ / ANZSRS Masterclass: April 3rd, 2016 13:00 13:30 John D. Brannan PhD Scientific Director - Dept. Respiratory & Sleep Medicine John Hunter Hospital,
Mechanisms of action of bronchial provocation testing TSANZ / ANZSRS Masterclass: April 3rd, 2016 13:00 13:30 John D. Brannan PhD Scientific Director - Dept. Respiratory & Sleep Medicine John Hunter Hospital,
Searching for Targets to Control Asthma
 Searching for Targets to Control Asthma Timothy Craig Distinguished Educator Professor Medicine and Pediatrics Penn State University Hershey, PA, USA Inflammation and Remodeling in Asthma The most important
Searching for Targets to Control Asthma Timothy Craig Distinguished Educator Professor Medicine and Pediatrics Penn State University Hershey, PA, USA Inflammation and Remodeling in Asthma The most important
Dual-Controller Asthma Therapy: Rationale and Clinical Benefits
 B/1 Dual-Controller Asthma Therapy: Rationale and Clinical Benefits MODULE B The 1997 National Heart, Lung, and Blood Institute (NHLBI) Expert Panel guidelines on asthma management recommend a 4-step approach
B/1 Dual-Controller Asthma Therapy: Rationale and Clinical Benefits MODULE B The 1997 National Heart, Lung, and Blood Institute (NHLBI) Expert Panel guidelines on asthma management recommend a 4-step approach
Medicine Dr. Kawa Lecture 1 Asthma Obstructive & Restrictive Pulmonary Diseases Obstructive Pulmonary Disease Indicate obstruction to flow of air
 Medicine Dr. Kawa Lecture 1 Asthma Obstructive & Restrictive Pulmonary Diseases Obstructive Pulmonary Disease Indicate obstruction to flow of air through the airways. As asthma, COPD ( chronic bronchitis
Medicine Dr. Kawa Lecture 1 Asthma Obstructive & Restrictive Pulmonary Diseases Obstructive Pulmonary Disease Indicate obstruction to flow of air through the airways. As asthma, COPD ( chronic bronchitis
Impact of Asthma in the U.S. per Year. Asthma Epidemiology and Pathophysiology. Risk Factors for Asthma. Childhood Asthma Costs of Asthma
 American Association for Respiratory Care Asthma Educator Certification Prep Course Asthma Epidemiology and Pathophysiology Robert C. Cohn, MD, FAARC MetroHealth Medical Center Cleveland, OH Impact of
American Association for Respiratory Care Asthma Educator Certification Prep Course Asthma Epidemiology and Pathophysiology Robert C. Cohn, MD, FAARC MetroHealth Medical Center Cleveland, OH Impact of
Do current treatment protocols adequately prevent airway remodeling in children with mild intermittent asthma?
 Respiratory Medicine (2006) 100, 458 462 Do current treatment protocols adequately prevent airway remodeling in children with mild intermittent asthma? Haim S. Bibi a,, David Feigenbaum a, Mariana Hessen
Respiratory Medicine (2006) 100, 458 462 Do current treatment protocols adequately prevent airway remodeling in children with mild intermittent asthma? Haim S. Bibi a,, David Feigenbaum a, Mariana Hessen
Defining Asthma: Clinical Criteria. Defining Asthma: Bronchial Hyperresponsiveness
 Defining Asthma: Clinical Criteria Atopy 34% Recent wheeze 20% Asthma 11% AHR 19% n = 807 From: Woolcock, AJ. Asthma in Textbook of Respiratory Medicine, 2nd ed. Murray, Nadel, eds.(saunders:philadelphia)
Defining Asthma: Clinical Criteria Atopy 34% Recent wheeze 20% Asthma 11% AHR 19% n = 807 From: Woolcock, AJ. Asthma in Textbook of Respiratory Medicine, 2nd ed. Murray, Nadel, eds.(saunders:philadelphia)
Life-long asthma and its relationship to COPD. Stephen T Holgate School of Medicine University of Southampton
 Life-long asthma and its relationship to COPD Stephen T Holgate School of Medicine University of Southampton Definitions COPD is a preventable and treatable disease with some significant extrapulmonary
Life-long asthma and its relationship to COPD Stephen T Holgate School of Medicine University of Southampton Definitions COPD is a preventable and treatable disease with some significant extrapulmonary
Increased peak expiratory flow variation in asthma: severe persistent increase but not nocturnal worsening of airway inflammation
 Eur Respir J 998; : 5655 DOI:.83/93936.98.356 Printed in UK - all rights reserved Copyright ERS Journals Ltd 998 European Respiratory Journal ISSN 93-936 Increased peak expiratory flow variation in asthma:
Eur Respir J 998; : 5655 DOI:.83/93936.98.356 Printed in UK - all rights reserved Copyright ERS Journals Ltd 998 European Respiratory Journal ISSN 93-936 Increased peak expiratory flow variation in asthma:
Allergy and Immunology Review Corner: Chapter 75 of Middleton s Allergy Principles and Practice, 7 th Edition, edited by N. Franklin Adkinson, et al.
 Allergy and Immunology Review Corner: Chapter 75 of Middleton s Allergy Principles and Practice, 7 th Edition, edited by N. Franklin Adkinson, et al. Chapter 75: Approach to Infants and Children with Asthma
Allergy and Immunology Review Corner: Chapter 75 of Middleton s Allergy Principles and Practice, 7 th Edition, edited by N. Franklin Adkinson, et al. Chapter 75: Approach to Infants and Children with Asthma
Respiratory Pharmacology
 Allergy Targets of allergies Type I Histamine Leukotrienes Prostaglandins Bradykinin Hypersensitivity reactions Asthma Characterised by Triggered by Intrinsic Extrinsic (allergic) Mediators Result Early
Allergy Targets of allergies Type I Histamine Leukotrienes Prostaglandins Bradykinin Hypersensitivity reactions Asthma Characterised by Triggered by Intrinsic Extrinsic (allergic) Mediators Result Early
COPYRIGHTED MATERIAL. Definition and Pathology CHAPTER 1. John Rees
 CHAPTER 1 Definition and Pathology John Rees Sherman Education Centre, Guy s Hospital, London, UK OVERVIEW Asthma is an overall descriptive term but there are a number of more or less distinct phenotypes
CHAPTER 1 Definition and Pathology John Rees Sherman Education Centre, Guy s Hospital, London, UK OVERVIEW Asthma is an overall descriptive term but there are a number of more or less distinct phenotypes
Asthma. - A chronic inflammatory disorder which causes recurrent episodes of wheezing, breathlessness, cough and chest tightness.
 Obstructive diseases Asthma - A chronic inflammatory disorder which causes recurrent episodes of wheezing, breathlessness, cough and chest tightness. - Characterized by Intermittent and reversible (the
Obstructive diseases Asthma - A chronic inflammatory disorder which causes recurrent episodes of wheezing, breathlessness, cough and chest tightness. - Characterized by Intermittent and reversible (the
Robert Kruklitis, MD, PhD Chief, Pulmonary Medicine Lehigh Valley Health Network
 Robert Kruklitis, MD, PhD Chief, Pulmonary Medicine Lehigh Valley Health Network Robert.kruklitis@lvh.com Correlation of a Asthma pathophyisology with basic science Asthma (Physiology) Bronchodilators
Robert Kruklitis, MD, PhD Chief, Pulmonary Medicine Lehigh Valley Health Network Robert.kruklitis@lvh.com Correlation of a Asthma pathophyisology with basic science Asthma (Physiology) Bronchodilators
Asthma Phenotypes, Heterogeneity and Severity: The Basis of Asthma Management
 Asthma Phenotypes, Heterogeneity and Severity: The Basis of Asthma Management Eugene R. Bleecker, MD Professor and Director, Center for Genomics & Personalized Medicine Research Professor, Translational
Asthma Phenotypes, Heterogeneity and Severity: The Basis of Asthma Management Eugene R. Bleecker, MD Professor and Director, Center for Genomics & Personalized Medicine Research Professor, Translational
Exhaled Biomarkers Asthma & COPD. AS Paul DM Seminar 30 March 07
 Exhaled Biomarkers Asthma & COPD AS Paul DM Seminar 30 March 07 Introduction Diagnosis and course of COPD/Asthma Clinical information Pulmonary function tests Arterial blood gases Chest X-raysX No direct
Exhaled Biomarkers Asthma & COPD AS Paul DM Seminar 30 March 07 Introduction Diagnosis and course of COPD/Asthma Clinical information Pulmonary function tests Arterial blood gases Chest X-raysX No direct
Identifying Biologic Targets to Attenuate or Eliminate Asthma Exacerbations
 Identifying Biologic Targets to Attenuate or Eliminate Exacerbations exacerbations are a major cause of disease morbidity and costs. For both children and adults, viral respiratory infections are the major
Identifying Biologic Targets to Attenuate or Eliminate Exacerbations exacerbations are a major cause of disease morbidity and costs. For both children and adults, viral respiratory infections are the major
Mast cell numbers in airway smooth muscle and PC 20 AMP in asthma and COPD
 Respiratory Medicine (2007) 101, 882 887 Mast cell numbers in airway smooth muscle and PC 20 AMP in asthma and COPD J.J.W. Liesker a, N.H.T. ten Hacken a,, S.R. Rutgers a, M. Zeinstra-Smith b, D.S. Postma
Respiratory Medicine (2007) 101, 882 887 Mast cell numbers in airway smooth muscle and PC 20 AMP in asthma and COPD J.J.W. Liesker a, N.H.T. ten Hacken a,, S.R. Rutgers a, M. Zeinstra-Smith b, D.S. Postma
Systems Pharmacology Respiratory Pharmacology. Lecture series : General outline
 Systems Pharmacology 3320 2017 Respiratory Pharmacology Associate Professor Peter Henry (Rm 1.34) Peter.Henry@uwa.edu.au Division of Pharmacology, School of Biomedical Sciences Lecture series : General
Systems Pharmacology 3320 2017 Respiratory Pharmacology Associate Professor Peter Henry (Rm 1.34) Peter.Henry@uwa.edu.au Division of Pharmacology, School of Biomedical Sciences Lecture series : General
Advanced Pharmaceutical Bulletin, 2014, x(x), xxx-xxx doi:
, xxx-xxx doi:") Advanced Pharmaceutical Bulletin, 2014, x(x), xxx-xxx doi: http://dx.doi.org/10.5681/apb.2014.013 http://apb.tbzmed.ac.ir/ The Effect of Adenosine A 2A and A 2B Antagonists on Tracheal Responsiveness,
Advanced Pharmaceutical Bulletin, 2014, x(x), xxx-xxx doi: http://dx.doi.org/10.5681/apb.2014.013 http://apb.tbzmed.ac.ir/ The Effect of Adenosine A 2A and A 2B Antagonists on Tracheal Responsiveness,
E-1 Role of IgE and IgE receptors in allergic airway inflammation and remodeling
 E-1 Role of IgE and IgE receptors in allergic airway inflammation and remodeling Ruby Pawankar, MD, Ph.D. FRCP, FAAAAI Prof. Div of Allergy, Dept of Pediatrics Nippon Medical School Tokyo, Japan pawankar.ruby@gmail.com
E-1 Role of IgE and IgE receptors in allergic airway inflammation and remodeling Ruby Pawankar, MD, Ph.D. FRCP, FAAAAI Prof. Div of Allergy, Dept of Pediatrics Nippon Medical School Tokyo, Japan pawankar.ruby@gmail.com
NG80. Asthma: diagnosis, monitoring and chronic asthma management (NG80)
") Asthma: diagnosis, monitoring and chronic asthma management (NG80) NG80 NICE has checked the use of its content in this product and the sponsor has had no influence on the content of this booklet. NICE
Asthma: diagnosis, monitoring and chronic asthma management (NG80) NG80 NICE has checked the use of its content in this product and the sponsor has had no influence on the content of this booklet. NICE
The Link Between Viruses and Asthma
 The Link Between Viruses and Asthma CATHERINE KIER, MD Professor of Clinical Pediatrics Division Chief, Pediatric Pulmonary, and Cystic Fibrosis Center Director, Pediatric Sleep Disorders Center SUNY Stony
The Link Between Viruses and Asthma CATHERINE KIER, MD Professor of Clinical Pediatrics Division Chief, Pediatric Pulmonary, and Cystic Fibrosis Center Director, Pediatric Sleep Disorders Center SUNY Stony
Defining Asthma: Clinical Criteria. Defining Asthma: Bronchial Hyperresponsiveness
 Defining Asthma: Clinical Criteria Atopy 34% Recent wheeze 20% Asthma 11% AHR 19% n = 807 From: Woolcock, AJ. Asthma in Textbook of Respiratory Medicine, 2nd ed. Murray, Nadel, eds.(saunders:philadelphia)
Defining Asthma: Clinical Criteria Atopy 34% Recent wheeze 20% Asthma 11% AHR 19% n = 807 From: Woolcock, AJ. Asthma in Textbook of Respiratory Medicine, 2nd ed. Murray, Nadel, eds.(saunders:philadelphia)
Defining Asthma: Bronchial Hyperresponsiveness. Defining Asthma: Clinical Criteria. Impaired Ventilation in Asthma. Dynamic Imaging of Asthma
 Defining Asthma: Clinical Criteria Defining Asthma: Bronchial Hyperresponsiveness Atopy 34% Recent wheeze 20% Asthma 11% AHR 19% n = 807 From: Woolcock, AJ. Asthma in Textbook of Respiratory Medicine,
Defining Asthma: Clinical Criteria Defining Asthma: Bronchial Hyperresponsiveness Atopy 34% Recent wheeze 20% Asthma 11% AHR 19% n = 807 From: Woolcock, AJ. Asthma in Textbook of Respiratory Medicine,
Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ
 Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ Financial Disclosures Advanced Practiced Advisory Board for Circassia Learning Objectives 1. Briefly
Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ Financial Disclosures Advanced Practiced Advisory Board for Circassia Learning Objectives 1. Briefly
Phenotypes of asthma; implications for treatment. Medical Grand Rounds Feb 2018 Jim Martin MD DSc
 Phenotypes of asthma; implications for treatment Medical Grand Rounds Feb 2018 Jim Martin MD DSc No conflicts to declare Objectives To understand the varied clinical forms of asthma To understand the pathobiologic
Phenotypes of asthma; implications for treatment Medical Grand Rounds Feb 2018 Jim Martin MD DSc No conflicts to declare Objectives To understand the varied clinical forms of asthma To understand the pathobiologic
Asthma Management for the Athlete
 Asthma Management for the Athlete Khanh Lai, MD Assistant Professor Division of Pediatric Pulmonary and Sleep Medicine University of Utah School of Medicine 2 nd Annual Sports Medicine Symposium: The Pediatric
Asthma Management for the Athlete Khanh Lai, MD Assistant Professor Division of Pediatric Pulmonary and Sleep Medicine University of Utah School of Medicine 2 nd Annual Sports Medicine Symposium: The Pediatric
10801 Sixth St, Rancho Cucamonga, CA Tel (909) Fax (909) Visit our web site at:
 Fax (909) Visit our web site at:") for the Diagnosis and Management of Asthma and Other Pulmonary Disorders IEHP Policy: Based on a review of the currently available literature, there is insufficient evidence to support the use of FE NO
for the Diagnosis and Management of Asthma and Other Pulmonary Disorders IEHP Policy: Based on a review of the currently available literature, there is insufficient evidence to support the use of FE NO
NON-SPECIFIC BRONCHIAL HYPERESPONSIVENESS. J. Sastre. Allergy Service
 NON-SPECIFIC BRONCHIAL HYPERESPONSIVENESS J. Sastre. Allergy Service Asthma: definition Asthma is a syndrome defined on basis of three main aspects: 1- Symptoms due to variable and reversible airway obstruction
NON-SPECIFIC BRONCHIAL HYPERESPONSIVENESS J. Sastre. Allergy Service Asthma: definition Asthma is a syndrome defined on basis of three main aspects: 1- Symptoms due to variable and reversible airway obstruction
On completion of this chapter you should be able to: discuss the stepwise approach to the pharmacological management of asthma in children
 7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
ASTHMA. Epidemiology. Pathophysiology. Diagnosis. IAP UG Teaching slides
 BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
Pulmonary Function Testing: Concepts and Clinical Applications. Potential Conflict Of Interest. Objectives. Rationale: Why Test?
 Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
RESPIRATORY BLOCK. Bronchial Asthma. Dr. Maha Arafah Department of Pathology KSU
 RESPIRATORY BLOCK Bronchial Asthma Dr. Maha Arafah Department of Pathology KSU marafah@ksu.edu.sa Jan 2018 Objectives Define asthma (BA) Know the two types of asthma 1. Extrinsic or atopic allergic 2.
RESPIRATORY BLOCK Bronchial Asthma Dr. Maha Arafah Department of Pathology KSU marafah@ksu.edu.sa Jan 2018 Objectives Define asthma (BA) Know the two types of asthma 1. Extrinsic or atopic allergic 2.
Asthma - Chronic. Presentations of asthma Cough Wheeze Breathlessness Chest tightness
 Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Property of Presenter
 Have We Missed A Role For Neutrophils In Asthma? In Steroid-Refractory Asthma? Erwin W. Gelfand, MD Chairman, Department of Pediatrics National Jewish Health Professor of Pediatrics and Immunology University
Have We Missed A Role For Neutrophils In Asthma? In Steroid-Refractory Asthma? Erwin W. Gelfand, MD Chairman, Department of Pediatrics National Jewish Health Professor of Pediatrics and Immunology University
Using Patient Characteristics to Individualize and Improve Asthma Care
 Using Patient Characteristics to Individualize and Improve Asthma Care Leonard B. Bacharier, M.D. Associate Professor of Pediatrics Clinical Director, Division of Allergy, Immunology, & Pulmonary Medicine
Using Patient Characteristics to Individualize and Improve Asthma Care Leonard B. Bacharier, M.D. Associate Professor of Pediatrics Clinical Director, Division of Allergy, Immunology, & Pulmonary Medicine
2010 Health Press Ltd.
 Fast Facts Fast Facts: Asthma Third edition Stephen T Holgate MD DSc FRCP FMedSci MRC Clinical Professor of Immunopharmacology School of Medicine Southampton General Hospital Southampton, UK Jo Douglass
Fast Facts Fast Facts: Asthma Third edition Stephen T Holgate MD DSc FRCP FMedSci MRC Clinical Professor of Immunopharmacology School of Medicine Southampton General Hospital Southampton, UK Jo Douglass
Abstract. IgE. IgE Th2. x x IL-4 IL-5 IgE CD4 +
 D. o ƒf 6,''!" # + % %$ '& ' '' & " k n k x k k k k k x k IgE k x IgE Ò1Ó k Ò2Ó v k x IgE Th2 x } x x IL-4 IL-5 IgE IgE j IFN-γ IgG j j CD4 + { k d «d j B7 w k k x IgE k 1 k Abstract Parental immunization
D. o ƒf 6,''!" # + % %$ '& ' '' & " k n k x k k k k k x k IgE k x IgE Ò1Ó k Ò2Ó v k x IgE Th2 x } x x IL-4 IL-5 IgE IgE j IFN-γ IgG j j CD4 + { k d «d j B7 w k k x IgE k 1 k Abstract Parental immunization
Inflammation in chronic obstructive pulmonary disease : its assessment and the effects of corticosteroids Boorsma, M.
 UvA-DARE (Digital Academic Repository) Inflammation in chronic obstructive pulmonary disease : its assessment and the effects of corticosteroids Boorsma, M. Link to publication Citation for published version
UvA-DARE (Digital Academic Repository) Inflammation in chronic obstructive pulmonary disease : its assessment and the effects of corticosteroids Boorsma, M. Link to publication Citation for published version
Borg scores before and after challenge with adenosine 5'-monophosphate and methacholine in subjects with COPD and asthma
 Eur Respir J 2000; 16: 486±490 Printed in UK ± all rights reserved Copyright #ERS Journals Ltd 2000 European Respiratory Journal ISSN 0903-1936 Borg scores before and after challenge with adenosine 5'-monophosphate
Eur Respir J 2000; 16: 486±490 Printed in UK ± all rights reserved Copyright #ERS Journals Ltd 2000 European Respiratory Journal ISSN 0903-1936 Borg scores before and after challenge with adenosine 5'-monophosphate
S. Jamal Mustafa, Ahmed Nadeem, Ming Fan, Hongyan Zhong, Luiz Belardinelli, and Dewan Zeng
 0022-3565/07/3203-1246 1251$20.00 THE JOURNAL OF PHARMACOLOGY AND EXPERIMENTAL THERAPEUTICS Vol. 320, No. 3 Copyright 2007 by The American Society for Pharmacology and Experimental Therapeutics 112250/3180790
0022-3565/07/3203-1246 1251$20.00 THE JOURNAL OF PHARMACOLOGY AND EXPERIMENTAL THERAPEUTICS Vol. 320, No. 3 Copyright 2007 by The American Society for Pharmacology and Experimental Therapeutics 112250/3180790
Safety, PK and PD of ARRY-502, a CRTh2 Antagonist, in Healthy Subjects with a History of Seasonal Allergies
 Safety, PK and PD of ARRY502, a CRTh2 Antagonist, in Healthy Subjects with a History of Seasonal Allergies L. Burgess*, L. Anderson, C. Nugent, N. Klopfenstein, C. Eberhardt, L. Carter, C. Kass, S. RojasCaro,
Safety, PK and PD of ARRY502, a CRTh2 Antagonist, in Healthy Subjects with a History of Seasonal Allergies L. Burgess*, L. Anderson, C. Nugent, N. Klopfenstein, C. Eberhardt, L. Carter, C. Kass, S. RojasCaro,
Outline FEF Reduced FEF25-75 in asthma. What does it mean and what are the clinical implications?
 Reduced FEF25-75 in asthma. What does it mean and what are the clinical implications? Fernando Holguin MD MPH Director, Asthma Clinical & Research Program Center for lungs and Breathing University of Colorado
Reduced FEF25-75 in asthma. What does it mean and what are the clinical implications? Fernando Holguin MD MPH Director, Asthma Clinical & Research Program Center for lungs and Breathing University of Colorado
Current Asthma Management: Opportunities for a Nutrition-Based Intervention
 Current Asthma Management: Opportunities for a Nutrition-Based Intervention Stanley J. Szefler, MD Approximately 22 million Americans, including 6 million children, have asthma. It is one of the most prevalent
Current Asthma Management: Opportunities for a Nutrition-Based Intervention Stanley J. Szefler, MD Approximately 22 million Americans, including 6 million children, have asthma. It is one of the most prevalent
ASTHMA ASTHMA DISEASE SUMMARY. Risk Factors
 ASTHMA Risk Factors Family history of asthma or other atopic diseases (eczema, hayfever) Having eczema or hayfever currently or as a child Living in an industrialised area more exposure to airborne pollutants,
ASTHMA Risk Factors Family history of asthma or other atopic diseases (eczema, hayfever) Having eczema or hayfever currently or as a child Living in an industrialised area more exposure to airborne pollutants,
Air Flow Limitation. In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation.
 Asthma Air Flow Limitation In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation. True whether reversible, asthma and exercise-induced bronchospasm,
Asthma Air Flow Limitation In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation. True whether reversible, asthma and exercise-induced bronchospasm,
Asthma Pathophysiology and Treatment. John R. Holcomb, M.D.
 Asthma Pathophysiology and Treatment John R. Holcomb, M.D. Objectives Definition of Asthma Epidemiology and risk factors of Asthma Pathophysiology of Asthma Diagnostics test of Asthma Management of Asthma
Asthma Pathophysiology and Treatment John R. Holcomb, M.D. Objectives Definition of Asthma Epidemiology and risk factors of Asthma Pathophysiology of Asthma Diagnostics test of Asthma Management of Asthma
Supplementary Information
 Supplementary Information TABLE S1. SUBJECT CHARACTERISTICS* Normal Control Subjects Subjects with Asthma p Value Number 23 48 Age (years) 35±10 35±10 0.75 Sex, M:F (% F) 9:12 (57) 17:26 (60) 0.76 FEV1
Supplementary Information TABLE S1. SUBJECT CHARACTERISTICS* Normal Control Subjects Subjects with Asthma p Value Number 23 48 Age (years) 35±10 35±10 0.75 Sex, M:F (% F) 9:12 (57) 17:26 (60) 0.76 FEV1
IgE-mediated allergy in elderly patients with asthma
 Allergology international (1997) 46: 237-241 Original Article IgE-mediated allergy in elderly patients with asthma Fumihiro Mitsunobu, Takashi Mifune, Yasuhiro Hosaki, Kouzou Ashida, Hirofumi Tsugeno,
Allergology international (1997) 46: 237-241 Original Article IgE-mediated allergy in elderly patients with asthma Fumihiro Mitsunobu, Takashi Mifune, Yasuhiro Hosaki, Kouzou Ashida, Hirofumi Tsugeno,
Learning Outcomes. Systems Pharmacology PHAR3320. Nerves of the Respiratory Tract. Dr Fernandes
 Systems Pharmacology PHAR3320 Nerves of the Respiratory Tract Dr Fernandes Learning Outcomes By the end of this lecture, students should be able to describe nerve pathways that innervate the airways discuss
Systems Pharmacology PHAR3320 Nerves of the Respiratory Tract Dr Fernandes Learning Outcomes By the end of this lecture, students should be able to describe nerve pathways that innervate the airways discuss
Asthma in Pediatric Patients. DanThuy Dao, D.O., FAAP. Disclosures. None
 Asthma in Pediatric Patients DanThuy Dao, D.O., FAAP Disclosures None Objectives 1. Discuss the evaluation and management of asthma in a pediatric patient 2. Accurately assess asthma severity and level
Asthma in Pediatric Patients DanThuy Dao, D.O., FAAP Disclosures None Objectives 1. Discuss the evaluation and management of asthma in a pediatric patient 2. Accurately assess asthma severity and level
Induced sputum to assess airway inflammation: a study of reproducibility
 Clinical and Experimental Allergy. 1997. Volume 27. pages 1138-1144 Induced sputum to assess airway inflammation: a study of reproducibility A. SPANEVELLO, G. B. MIGLIORI. A. SHARARA*, L. BALLARDlNIt,
Clinical and Experimental Allergy. 1997. Volume 27. pages 1138-1144 Induced sputum to assess airway inflammation: a study of reproducibility A. SPANEVELLO, G. B. MIGLIORI. A. SHARARA*, L. BALLARDlNIt,
Leukotriene C 4 synthase polymorphisms and responsiveness to leukotriene antagonists in asthma
 Blackwell Science, LtdOxford, UKBCPBritish Journal of Clinical Pharmacology0306-5251Blackwell Publishing 2003? 2003564422426Original ArticleLeukotriene C4 synthasej. J. Lima et al. Leukotriene C 4 synthase
Blackwell Science, LtdOxford, UKBCPBritish Journal of Clinical Pharmacology0306-5251Blackwell Publishing 2003? 2003564422426Original ArticleLeukotriene C4 synthasej. J. Lima et al. Leukotriene C 4 synthase
Evolution of asthma from childhood. Carlos Nunes Center of Allergy and Immunology of Algarve, PT
 Evolution of asthma from childhood Carlos Nunes Center of Allergy and Immunology of Algarve, PT allergy@mail.telepac.pt Questionnaire data Symptoms occurring once or several times at follow-up (wheeze,
Evolution of asthma from childhood Carlos Nunes Center of Allergy and Immunology of Algarve, PT allergy@mail.telepac.pt Questionnaire data Symptoms occurring once or several times at follow-up (wheeze,
COPD: From Phenotypes to Endotypes. MeiLan K Han, M.D., M.S. Associate Professor of Medicine University of Michigan, Ann Arbor, MI
 COPD: From Phenotypes to Endotypes MeiLan K Han, M.D., M.S. Associate Professor of Medicine University of Michigan, Ann Arbor, MI Presenter Disclosures MeiLan K. Han Consulting Research support Novartis
COPD: From Phenotypes to Endotypes MeiLan K Han, M.D., M.S. Associate Professor of Medicine University of Michigan, Ann Arbor, MI Presenter Disclosures MeiLan K. Han Consulting Research support Novartis
Dr Rodney Itaki Lecturer Division of Pathology Anatomical Pathology Discipline
 Pathology of Asthma Dr Rodney Itaki Lecturer Division of Pathology Anatomical Pathology Discipline Bronchial Asthma Definition: chronic, relapsing inflammatory lung disorder characterised by reversible
Pathology of Asthma Dr Rodney Itaki Lecturer Division of Pathology Anatomical Pathology Discipline Bronchial Asthma Definition: chronic, relapsing inflammatory lung disorder characterised by reversible
Biologic Therapy in the Management of Asthma. Nabeel Farooqui, MD
 Biologic Therapy in the Management of Asthma Nabeel Farooqui, MD None Disclosures Objectives Define severe asthma phenotypes and endotypes Describe the role of biologics in asthma management Review pivotal
Biologic Therapy in the Management of Asthma Nabeel Farooqui, MD None Disclosures Objectives Define severe asthma phenotypes and endotypes Describe the role of biologics in asthma management Review pivotal
THE PROMISE OF NEW AND NOVEL DRUGS. Pyng Lee Respiratory & Critical Care Medicine National University Hospital
 THE PROMISE OF NEW AND NOVEL DRUGS Pyng Lee Respiratory & Critical Care Medicine National University Hospital Pyng_lee@nuhs.edu.sg Asthma Prevalence, Morbidity, Mortality 235 million suffer from asthma
THE PROMISE OF NEW AND NOVEL DRUGS Pyng Lee Respiratory & Critical Care Medicine National University Hospital Pyng_lee@nuhs.edu.sg Asthma Prevalence, Morbidity, Mortality 235 million suffer from asthma
responsiveness in asthmatic patients and smokers
 63 Department of Pulmonology B Auffarth D S Postma G H Koeter Th W van der Mark Department of Allergology J G R de Monchy University Hospital, 973 EZ Groningen, The Netherlands Reprint requests to: Professor
63 Department of Pulmonology B Auffarth D S Postma G H Koeter Th W van der Mark Department of Allergology J G R de Monchy University Hospital, 973 EZ Groningen, The Netherlands Reprint requests to: Professor
Bronchial asthma. MUDr. Mojmír Račanský Odd. Alergologie a klinické imunologie FNOL Ústav Imunologie LF UPOL
 Bronchial asthma MUDr. Mojmír Račanský Odd. Alergologie a klinické imunologie FNOL Ústav Imunologie LF UPOL DEFINITION ASTHMA BRONCHIALE = Asthma is a chronic inflammatory disorder of the airways in which
Bronchial asthma MUDr. Mojmír Račanský Odd. Alergologie a klinické imunologie FNOL Ústav Imunologie LF UPOL DEFINITION ASTHMA BRONCHIALE = Asthma is a chronic inflammatory disorder of the airways in which
Airway Inflammation in Asthma Chih-Yung Chiu 1,2, Kin-Sun Wong 2 1 Department of Pediatrics, Chang Gung Memorial Hospital, Keelung, Taiwan.
 REVIEW ARTICLE Chih-Yung Chiu 1,2, Kin-Sun Wong 2 1 Department of Pediatrics, Chang Gung Memorial Hospital, Keelung, Taiwan. 2 Division of Pediatric Pulmonology, Department of Pediatrics, Chang Gung Memorial
REVIEW ARTICLE Chih-Yung Chiu 1,2, Kin-Sun Wong 2 1 Department of Pediatrics, Chang Gung Memorial Hospital, Keelung, Taiwan. 2 Division of Pediatric Pulmonology, Department of Pediatrics, Chang Gung Memorial
Grass pollen immunotherapy induces Foxp3 expressing CD4 + CD25 + cells. in the nasal mucosa. Suzana Radulovic MD, Mikila R Jacobson PhD,
 Radulovic 1 1 2 3 Grass pollen immunotherapy induces Foxp3 expressing CD4 + CD25 + cells in the nasal mucosa 4 5 6 7 Suzana Radulovic MD, Mikila R Jacobson PhD, Stephen R Durham MD, Kayhan T Nouri-Aria
Radulovic 1 1 2 3 Grass pollen immunotherapy induces Foxp3 expressing CD4 + CD25 + cells in the nasal mucosa 4 5 6 7 Suzana Radulovic MD, Mikila R Jacobson PhD, Stephen R Durham MD, Kayhan T Nouri-Aria
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: exhaled_nitric_oxide_measurement 2/2009 3/2018 3/2019 3/2018 Description of Procedure or Service Asthma is
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: exhaled_nitric_oxide_measurement 2/2009 3/2018 3/2019 3/2018 Description of Procedure or Service Asthma is
Defining COPD. Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist
 Defining COPD Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist Defining COPD Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease
Defining COPD Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist Defining COPD Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease
Function of the Respiratory System. Exchange CO2 (on expiration) for O2 (on inspiration)
 for O2 (on inspiration)") Function of the Respiratory System Exchange CO2 (on expiration) for O2 (on inspiration) Upper Respiratory Tract Includes: Nose Mouth Pharynx Larynx Function: Warms and humidifies the inspired air Filters
Function of the Respiratory System Exchange CO2 (on expiration) for O2 (on inspiration) Upper Respiratory Tract Includes: Nose Mouth Pharynx Larynx Function: Warms and humidifies the inspired air Filters
Respiratory Health L O O K, F E E L A N D L I V E B E T T E R
 LOOK, FEEL AND LIVE BET TER Respiratory health: hay-fever and asthma Airway obstruction and symptoms in asthma and hay-fever alike are the result of inappropriate responses of the body s immune system
LOOK, FEEL AND LIVE BET TER Respiratory health: hay-fever and asthma Airway obstruction and symptoms in asthma and hay-fever alike are the result of inappropriate responses of the body s immune system
Viral-Induced Asthma:
 Viral-Induced : Sorting through the Studies Malcolm R. Sears, MB, FRACP, FRCPC Presented at the Respirology Update Continuing Education Program, January 2005 Viral-associated wheezing is common and not
Viral-Induced : Sorting through the Studies Malcolm R. Sears, MB, FRACP, FRCPC Presented at the Respirology Update Continuing Education Program, January 2005 Viral-associated wheezing is common and not
Potent and Selective CRTh2 Antagonists are Efficacious in Models of Asthma, Allergic Rhinitis and Atopic Dermatitis
 Potent and Selective CRTh2 Antagonists are Efficacious in Models of Asthma, Allergic Rhinitis and Atopic Dermatitis Laura L. Carter, Yoshi Shiraishi, Yooseob Shin, Laurence Burgess, Christine Eberhardt,
Potent and Selective CRTh2 Antagonists are Efficacious in Models of Asthma, Allergic Rhinitis and Atopic Dermatitis Laura L. Carter, Yoshi Shiraishi, Yooseob Shin, Laurence Burgess, Christine Eberhardt,
Chronic Cough Due to Nonasthmatic Eosinophilic Bronchitis. ACCP Evidence-Based Clinical Practice Guidelines
 Chronic Cough Due to Nonasthmatic Eosinophilic Bronchitis ACCP Evidence-Based Clinical Practice Guidelines Christopher E. Brightling, MBBS, PhD, FCCP Objectives: Nonasthmatic eosinophilic bronchitis is
Chronic Cough Due to Nonasthmatic Eosinophilic Bronchitis ACCP Evidence-Based Clinical Practice Guidelines Christopher E. Brightling, MBBS, PhD, FCCP Objectives: Nonasthmatic eosinophilic bronchitis is
THE PHARMA INNOVATION - JOURNAL Clinical Characteristics of Chronic Obstructive Pulmonary Disease
 Received: 09012014 Accepted: 30032014 ISSN: 2277 7695 CODEN Code: PIHNBQ ZDBNumber: 26630382 IC Journal No: 7725 Vol. 3 No. 2. 2014 Online Available at www.thepharmajournal.com THE PHARMA INNOVATION JOURNAL
Received: 09012014 Accepted: 30032014 ISSN: 2277 7695 CODEN Code: PIHNBQ ZDBNumber: 26630382 IC Journal No: 7725 Vol. 3 No. 2. 2014 Online Available at www.thepharmajournal.com THE PHARMA INNOVATION JOURNAL
ASTHMA TREATMENT EFFICACY ASSESSMENT BY FeNO MEASUREMENT
 Bulletin of the Transilvania University of Braşov Series VI: Medical Sciences Vol. 5 (54) No. 2-2012 ASTHMA TREATMENT EFFICACY ASSESSMENT BY FeNO MEASUREMENT Dana ALEXANDRESCU 1 Abstract: The author of
Bulletin of the Transilvania University of Braşov Series VI: Medical Sciences Vol. 5 (54) No. 2-2012 ASTHMA TREATMENT EFFICACY ASSESSMENT BY FeNO MEASUREMENT Dana ALEXANDRESCU 1 Abstract: The author of
B Y L E S L I E K U M P F, R R T, C P F T, A E - C
 FeNO B Y L E S L I E K U M P F, R R T, C P F T, A E - C LESLIE KUMPF RRT, CPFT, AE-C Graduated from Henry Ford with a degree in Respiratory Therapy in 2006 Currently working on my BSRT Help start the RRT
FeNO B Y L E S L I E K U M P F, R R T, C P F T, A E - C LESLIE KUMPF RRT, CPFT, AE-C Graduated from Henry Ford with a degree in Respiratory Therapy in 2006 Currently working on my BSRT Help start the RRT
Comparison of the Effect of Short Course of Oral Prednisone in Patients with Acute Asthma
 ISPUB.COM The Internet Journal of Pulmonary Medicine Volume 7 Number 1 Comparison of the Effect of Short Course of Oral Prednisone in Patients with Acute Asthma E Razi, G Moosavi Citation E Razi, G Moosavi.
ISPUB.COM The Internet Journal of Pulmonary Medicine Volume 7 Number 1 Comparison of the Effect of Short Course of Oral Prednisone in Patients with Acute Asthma E Razi, G Moosavi Citation E Razi, G Moosavi.
Clinical Benefits of FeNO Monitoring in Asthma RYAN BURTON, MS, RPFT
 Clinical Benefits of FeNO Monitoring in Asthma RYAN BURTON, MS, RPFT Disclosures I am an employee of Circassia Pharmaceuticals. Objectives Nitric Oxide Inflammation in Asthma Phenotyping Personalized Medicine
Clinical Benefits of FeNO Monitoring in Asthma RYAN BURTON, MS, RPFT Disclosures I am an employee of Circassia Pharmaceuticals. Objectives Nitric Oxide Inflammation in Asthma Phenotyping Personalized Medicine
RESPIRATORY PHARMACOLOGY - ASTHMA. Primary Exam Teaching - Westmead ED
 RESPIRATORY PHARMACOLOGY - ASTHMA Primary Exam Teaching - Westmead ED Sympathomimetic agents MOA: relax airway smooth muscle and inhibit broncho constricting mediators from mast cells May also inhibit
RESPIRATORY PHARMACOLOGY - ASTHMA Primary Exam Teaching - Westmead ED Sympathomimetic agents MOA: relax airway smooth muscle and inhibit broncho constricting mediators from mast cells May also inhibit
Increased Leukotriene E 4 in the Exhaled Breath Condensate of Children With Mild Asthma*
 CHEST Original Research Increased Leukotriene E 4 in the Exhaled Breath Condensate of Children With Mild Asthma* Atsushi Shibata, MD; Toshio Katsunuma, MD, PhD; Morimitsu Tomikawa, MD; Aiko Tan, MD; Keisuke
CHEST Original Research Increased Leukotriene E 4 in the Exhaled Breath Condensate of Children With Mild Asthma* Atsushi Shibata, MD; Toshio Katsunuma, MD, PhD; Morimitsu Tomikawa, MD; Aiko Tan, MD; Keisuke
Joint Session ACOFP and AOASM: Exercise Induced Asthma. Bruce Dubin, DO, JD, FCLM, FACOI
 Joint Session ACOFP and AOASM: Exercise Induced Asthma Bruce Dubin, DO, JD, FCLM, FACOI ACOFP FULL DISCLOSURE FOR CME ACTIVITIES Please check where applicable and sign below. Provide additional pages as
Joint Session ACOFP and AOASM: Exercise Induced Asthma Bruce Dubin, DO, JD, FCLM, FACOI ACOFP FULL DISCLOSURE FOR CME ACTIVITIES Please check where applicable and sign below. Provide additional pages as
Salmeterol, a new long acting inhaled,f2 adrenoceptor agonist: comparison with salbutamol in adult asthmatic patients
 Thorax 1988;43:674-678 Salmeterol, a new long acting inhaled,f2 adrenoceptor agonist: comparison with salbutamol in adult asthmatic patients ANDERS ULLMAN, NILS SVEDMYR From the Department of Clinical
Thorax 1988;43:674-678 Salmeterol, a new long acting inhaled,f2 adrenoceptor agonist: comparison with salbutamol in adult asthmatic patients ANDERS ULLMAN, NILS SVEDMYR From the Department of Clinical
Optimal Assessment of Asthma Control in Clinical Practice: Is there a role for biomarkers?
 Disclosures: Optimal Assessment of Asthma Control in Clinical Practice: Is there a role for biomarkers? Stanley Fineman, MD Past-President, American College of Allergy, Asthma & Immunology Adjunct Associate
Disclosures: Optimal Assessment of Asthma Control in Clinical Practice: Is there a role for biomarkers? Stanley Fineman, MD Past-President, American College of Allergy, Asthma & Immunology Adjunct Associate
COPD or not COPD, that is the question.
 COPD or not COPD, that is the question. Asthma-COPD Overlap Syndrome: ACOS Do we really need this? Michelle Harkins Disclosure Slide Slide help - William Busse, MD Organizational Interests ATS, ACCP, ACP
COPD or not COPD, that is the question. Asthma-COPD Overlap Syndrome: ACOS Do we really need this? Michelle Harkins Disclosure Slide Slide help - William Busse, MD Organizational Interests ATS, ACCP, ACP
I have no perceived conflicts of interest or commercial relationships to disclose.
 ASTHMA BASICS Michelle Dickens RN FNP-C AE-C Nurse Practitioner/Certified Asthma Educator Ferrell Duncan Allergy/Asthma/Immunology Coordinator, CoxHealth Asthma Center DISCLOSURES I have no perceived conflicts
ASTHMA BASICS Michelle Dickens RN FNP-C AE-C Nurse Practitioner/Certified Asthma Educator Ferrell Duncan Allergy/Asthma/Immunology Coordinator, CoxHealth Asthma Center DISCLOSURES I have no perceived conflicts
This is a cross-sectional analysis of the National Health and Nutrition Examination
 SUPPLEMENTAL METHODS Study Design and Setting This is a cross-sectional analysis of the National Health and Nutrition Examination Survey (NHANES) data 2007-2008, 2009-2010, and 2011-2012. The NHANES is
SUPPLEMENTAL METHODS Study Design and Setting This is a cross-sectional analysis of the National Health and Nutrition Examination Survey (NHANES) data 2007-2008, 2009-2010, and 2011-2012. The NHANES is
The natural history of asthma and early intervention
 The natural history of asthma and early intervention Stanley J. Szefler, MD Denver, Colo The understanding of the natural history of asthma has changed significantly during the last 4 decades, with the
The natural history of asthma and early intervention Stanley J. Szefler, MD Denver, Colo The understanding of the natural history of asthma has changed significantly during the last 4 decades, with the
Diagnosis, Treatment and Management of Asthma
 Diagnosis, Treatment and Management of Asthma Asthma is a complex disorder characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation.
Diagnosis, Treatment and Management of Asthma Asthma is a complex disorder characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation.
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Clinical trial efficacy: What does it really tell you?
 Clinical trial efficacy: What does it really tell you? Joseph Spahn, MD Denver, Colo The primary goal of most clinical trials is an evaluation of the efficacy of the drug being evaluated. Therefore, it
Clinical trial efficacy: What does it really tell you? Joseph Spahn, MD Denver, Colo The primary goal of most clinical trials is an evaluation of the efficacy of the drug being evaluated. Therefore, it
Bronchial hyperresponsiveness in type Ia (simple bronchoconstriction) asthma Relationship to patient age and the proportions of bronchoalveolar cells
 asthma Relationship to patient age and the proportions of bronchoalveolar cells") 28 Bronchial hyperresponsiveness in type I Bronchial hyperresponsiveness in type Ia (simple bronchoconstriction) Relationship to patient age and the proportions of bronchoalveolar cells Kouzou Ashida,
28 Bronchial hyperresponsiveness in type I Bronchial hyperresponsiveness in type Ia (simple bronchoconstriction) Relationship to patient age and the proportions of bronchoalveolar cells Kouzou Ashida,
British Journal of Clinical Pharmacology
 et al. et al. British Journal of Clinical Pharmacology DOI:10.1111/j.1365-2125.2004.02072.x Effects of single or combined histamine H 1 -receptor and leukotriene CysLT 1 -receptor antagonism on nasal adenosine
et al. et al. British Journal of Clinical Pharmacology DOI:10.1111/j.1365-2125.2004.02072.x Effects of single or combined histamine H 1 -receptor and leukotriene CysLT 1 -receptor antagonism on nasal adenosine
Asthma for Primary Care: Assessment, Control, and Long-Term Management
 Asthma for Primary Care: Assessment, Control, and Long-Term Management Learning Objectives After participating in this educational activity, participants should be better able to: 1. Choose the optimal
Asthma for Primary Care: Assessment, Control, and Long-Term Management Learning Objectives After participating in this educational activity, participants should be better able to: 1. Choose the optimal
LOOK, FEEL AND LIVE BETTER. Respiratory Health
 LOOK, FEEL AND LIVE BETTER Respiratory Health Respiratory health: hay fever and asthma Airway obstruction and symptoms in asthma and hay fever alike are the result of inappropriate responses of the body
LOOK, FEEL AND LIVE BETTER Respiratory Health Respiratory health: hay fever and asthma Airway obstruction and symptoms in asthma and hay fever alike are the result of inappropriate responses of the body