Evaluation and Management of Refractory Asthma
|
|
|
- Basil Brooks
- 6 years ago
- Views:
Transcription

1 Evaluation and Management of Refractory Asthma Non-Pharmacological Treatments: Comorbidities & Bronchial Thermoplasty Diego J Maselli, MD, FCCP Assistant Professor of Medicine Division of Pulmonary Diseases & Cri<cal Care University of Texas Health Science Center at San Antonio
2 Disclosures Nothing to disclose
3 Objec<ve Devise a nonpharmacologic management strategy for a pa<ent with refractory asthma, including bronchial thermoplasty


4 Frustra<on/chronic illness Difficulty checking for adherence Social aspects COMPLIANCE Poor Asthma Control Incomplete training ENVIRONMENTAL FACTORS INHALER TECHNIQUE MSK problems Neurological problems Side effects Cost
 azer a heavy meal TesBng: PFTs: FEV1/FVC 65%, FEV1 69%, posi<ve BDR, posi<ve hyperinfla<on CXR: normal MedicaBons: Medium dose ICS/LABA")
5 Case # 1 48 y/o woman with asthma, allergic rhini<s and arthri<s, consults for frequent exacerba<ons (once a month x 3 ) Wheezing daily despite good compliance and technique Symptoms of allergic rhini<s are controlled Minimal GERD symptoms (once a month) azer a heavy meal TesBng: PFTs: FEV1/FVC 65%, FEV1 69%, posi<ve BDR, posi<ve hyperinfla<on CXR: normal MedicaBons: Medium dose ICS/LABA Rescue SABA Nasal steroids Ibuprofen
6 QuesBon # 1 In addi<on to increasing her ICS dose, what is the next step in management?? A. A trial of a proton pump inhibitor (PPI) once a day dosing for 8 weeks B. A trial of a PPI twice a day dosing for 8 weeks C. Refer the pa<ent for ph monitoring (24 hour tes<ng) D. Refer the pa<ent for an endoscopy to evaluate for GERD E. Obtain an IgE level and tesbng for perennial allergens



7 Allergic Rhini<s Vocal cord dysfunc<on OSA Obesity Anxiety ASTHMA Depression GERD Smoking Medica<ons β blockers ASA ACE inhibitors NSAIDS COPD


8 GERD Esophageal Syndromes Extra- Esophageal Syndromes SymptomaBc Syndromes Syndromes with Esophageal Injury Established AssociaBon Proposed AssociaBon Typical reflux syndrome Reflux chest pain syndrome Reflux esophagi<s Reflux stricture Barrei s esophagus Adenocarcinoma Reflux cough Reflux laryngi<s Reflux asthma Reflux dental erosions Sinusi<s Pulmonary fibrosis Pharyngi<s Recurrent o<<s media






9 ASTHMA Vagal response é abdominal Hyperinfla<on pressure / é nega<ve thoracic pressure Micro aspira<on Asthma medica<ons GERD Lower esophageal sphincter
10 GERD and Asthma 55% of difficult to control asthma<cs may have GERD 35% of asthma<c pa<ents with documented GERD by ph monitoring did not have typical symptoms Clinical suspicion Worsening of asthma symptoms azer a meal Heartburn or regurgita<on before the onset of asthma symptoms
 Daily asthma symptoms, albuterol use, and PFTs did not improve. Liiner MR, et al. Chest.")
11 GERD and Asthma LiQner et al. 24 weeks of lanzoprazole BID in moderate to severe asthma<cs and posi<ve GERD symptoms. (n=173) Daily asthma symptoms, albuterol use, and PFTs did not improve. Liiner MR, et al. Chest Sep;128(3):
12 GERD and Asthma Kiljander et al. 16 weeks of esomeprazole BID in moderate to severe asthma<cs (n=624). 1. (- ) GERD and (+) nocturnal symptoms Classified in 3 strata: 2. (+) GERD and (- ) nocturnal symptoms 3. (+) GERD and (+) nocturnal symptoms PPI was associated with benefits in PEF only in the group that had: (+) GERD and (+) nocturnal symptoms. Only 40% of the pa<ents were using LABA. These subgroup had the greatest é in PEF. No difference in exacerba<ons. Kiljander TO, et al. Am J Respir Crit Care Med May 15;173(10):
. Kiljander TO, et al.")
13 GERD and Asthma Kiljander et al. 26 weeks of esomeprazole once day vs. BID vs. placebo in asthma<cs using ICS/LABA + GERD symptoms (n=828). No difference in asthma control or symptom scores. Modest improvement in quality of life and FEV1 in the PPI groups (more significant with BID dosing). Kiljander TO, et al. Am J Respir Crit Care Med May 15;181(10):1042-8
14 GERD and Asthma Mastronarde JG, et al. (Study of Acid Reflux and Asthma) 24 weeks of esomeprazole BID in inadequately controlled asthma<cs despite ICS and minimal or no GERD symptoms (n=393). ~ 80% were using ICS + LABA No difference in asthma control, PFTs, symptom scores, nocturnal awakenings or quality of life. No subgroup had benefits with a PPI. Mastronarde JG et al.n Engl J Med Apr 9;360(15):
15 GERD and Asthma DiMango E, et al. Evaluated the baseline characteris<cs of the Study of Acid Reflux and Asthma (pa<ents with ph recordings) 53% of the pa<ents had reflux 38% had proximal reflux There was no difference in need for SABA, nocturnal awakenings, dose of ICS, use of LABA, PFTs, or methacholine reac<vity between individuals with and without proximal or distal GERD DiMango E, et al. Am J Respir Crit Care Med Nov 1;180(9):
16 GERD and Asthma TAKE HOME POINTS: 1. Asthma<cs with GERD symptoms should be treated with a PPI, especially if they nocturnal asthma symptoms. 2. Severe asthma<cs with GERD symptoms appear to have greater benefits with PPI treatment. 3. PPIs have no benefit in pa<ents with poorly controlled asthma with minimal or no symptoms of GERD. 4. Ambulatory ph monitoring is not usually warranted unless there are atypical symptoms.
17 Allergic RhiniBs and Asthma AR increases the risk of asthma 3- fold AR is present 75-80% in pa<ents with severe asthma AR may substan<al costs to asthma pa<ents p = p = Bousquet J, et al. Clin Exp Allergy Jun;35(6):723-7.
18 Allergic Rhini<s Ac<va<on of systemic inflammatory pathways Post nasal drip into the airways Nasobronchial reflex Asthma ê filtra<on ê humidifica<on ê warming
19 Impact of TreaBng AR in Asthma STUDY Adam RJ 2002 ASTHMATIC PATIENTS 1610 Crystal- Peters J Corren J 2004 OBSERVATIONS / CONCLUSIONS Retrospec<ve Nasal steroids and an<histamines were associated with reduced ED visits Asthma ED visits/hospitaliza<ons Retrospec<ve occurred less ozen in the treated group 6.6 vs 1.3%, p = cases Nested case controls control DESIGN Treatment with nasal steroids or an<histamines showed a reduc<on in the risk of hospitaliza<on for asthma Corren J, et al. J Allergy Clin Immunol Mar;113(3): Adams RJ, et al. J Allergy Clin Immunol Apr;109(4): Crystal- Peters J, et al. J Allergy Clin Immunol Jan;109(1):57-62.

:")
20 Bousquet J, et al. J Allergy Clin Immunol Nov;130(5):
21 Case # 2 42 y/o woman with asthma referred uncontrolled asthma. She has had several exacerba<ons in the past 6 months including a ICU stay/intuba<on. Compliant with medica<ons. Treated for omalizumab for 6 months 300mg q 2 weeks. TesBng: PFTs: FEV1/FVC 60%, FEV1 63%, posi<ve BDR. CXR: normal CT chest: bronchial thickening MedicaBons: High dose ICS/LABA Rescue SABA Montelukast Omalizumab
22 QuesBon # 2 Regarding treatment with bronchial thermoplasty (BT) in this pa<ent, you would recommend which of the following? A. BT is not recommended because of the severity of her asthma B. BT can be considered only azer omalizumab therapy has been tried for at least 12 months C. BT is could be considered, but long term safety is not yet known D. BT is indicated should be performed in this pabent E. BT is considered experimental and should be only done in referral centers

23 Bronchial Thermoplasty (BT) w Ra<onale: Airway remodeling: smooth muscle hyperplasia/ hypertrophy. BT, using radiofrequency energy, can decrease significantly the smooth muscle mass Airway remodeling
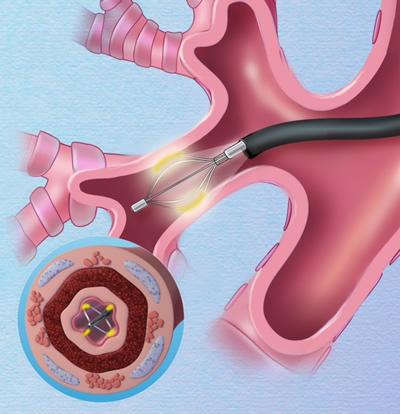
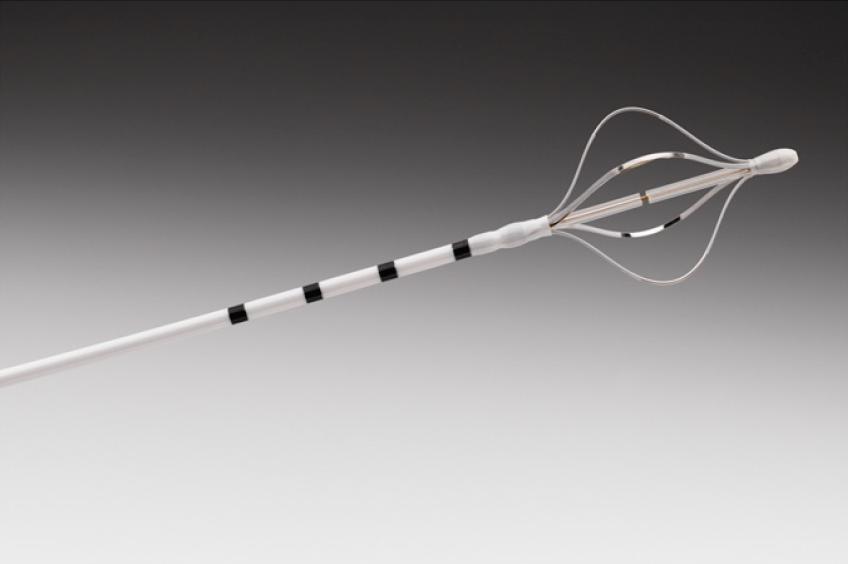

24 Bronchial Thermoplasty
 u u u u Severe asthma<cs received either BT or sham Excluded pts with > 3 exacerba<ons in the previous year or > 4 pulses of steroids 79% vs.")
25 Bronchial Thermoplasty: Efficacy Castro M, et al. Am J Respir Crit Care Med (n = 288) u u u u Severe asthma<cs received either BT or sham Excluded pts with > 3 exacerba<ons in the previous year or > 4 pulses of steroids 79% vs. 64% achieved changes in ADLQ scores (0.5 or >) 8.4% were hospitalized azer BT * 32% ê in severe exacerba<on + 84% reduc<on in ER visits
26 Bronchial Thermoplasty: Safety Thomson NC, et al. BMC Pulm Med (n = 45) u u u 5 year follow up study from the AIR trail Absence of clinical complica<ons Stable lung func<on over 5 years
 u u 5 year follow up study from the AIR2 trail Sustainable effect")
27 Bronchial Thermoplasty: Safety Wechsler ME, et al. J Allergy Clin Immunol (n = 162) u u 5 year follow up study from the AIR2 trail Sustainable effect azer 5 years
 u u 5 year follow up study from the AIR2 trail Sustainable effect")
28 Bronchial Thermoplasty: Safety Wechsler ME, et al. J Allergy Clin Immunol (n = 162) u u 5 year follow up study from the AIR2 trail Sustainable effect azer 5 years
29 Bronchial Thermoplasty Pros: Evidence of reduc<on of symptoms u Las<ng effects (5 years) u Cons: High cost u Early exacerba<on rate despite pre treatment with oral steroids u Need for 3 bronchoscopies u
30 Summary w In severe/refractory asthma the following should be always assessed: Compliance Inhaler technique Comorbidi<es (GERD, AR, obesity, OSA, smoking) w BT appears to be effec<ve and safe in pa<ents with uncontrolled asthma despite high dose ICS and has las<ng effects
5/1/18. Emerging Challenges in Primary Care: The Role of Type 2 Inflammation in Severe Asthma: Integrating Biologic Therapy to Optimize Outcomes
 Emerging Challenges in Primary Care: 2018 The Role of Type 2 Inflammation in Severe Asthma: Integrating Biologic Therapy to Optimize Outcomes 1 Faculty Diego J. Maselli, MD FCCP Assistant Professor of
Emerging Challenges in Primary Care: 2018 The Role of Type 2 Inflammation in Severe Asthma: Integrating Biologic Therapy to Optimize Outcomes 1 Faculty Diego J. Maselli, MD FCCP Assistant Professor of
Emerging Challenges in Primary Care: 2018 The Role of Type 2 Inflammation in Severe Asthma: Integrating Biologic Therapy to Optimize Outcomes
 Emerging Challenges in Primary Care: 2018 The Role of Type 2 Inflammation in Severe Asthma: Integrating Biologic Therapy to Optimize Outcomes 1 Faculty Diego J. Maselli, MD FCCP Assistant Professor of
Emerging Challenges in Primary Care: 2018 The Role of Type 2 Inflammation in Severe Asthma: Integrating Biologic Therapy to Optimize Outcomes 1 Faculty Diego J. Maselli, MD FCCP Assistant Professor of
Emerging Challenges in Primary Care: The Role of Type 2 Inflammation in Severe Asthma: Integrating Biologic Therapy to Optimize Outcomes
 Emerging Challenges in Primary Care: 2018 The Role of Type 2 Inflammation in Severe Asthma: Integrating Biologic Therapy to Optimize Outcomes 1 Faculty Diego J. Maselli, MD FCCP Assistant Professor of
Emerging Challenges in Primary Care: 2018 The Role of Type 2 Inflammation in Severe Asthma: Integrating Biologic Therapy to Optimize Outcomes 1 Faculty Diego J. Maselli, MD FCCP Assistant Professor of
Emerging Challenges in Primary Care: 2018 The Role of Type 2 Inflammation in Severe Asthma: Integrating Biologic Therapy to Optimize Outcomes
 Emerging Challenges in Primary Care: 2018 The Role of Type 2 Inflammation in Severe Asthma: Integrating Biologic Therapy to Optimize Outcomes 1 Faculty Diego J. Maselli, MD FCCP Assistant Professor of
Emerging Challenges in Primary Care: 2018 The Role of Type 2 Inflammation in Severe Asthma: Integrating Biologic Therapy to Optimize Outcomes 1 Faculty Diego J. Maselli, MD FCCP Assistant Professor of
Somkiat Wongtim Professor of Medicine Division of Respiratory Disease and Critical Care Chulalongkorn University
 Somkiat Wongtim Professor of Medicine Division of Respiratory Disease and Critical Care Chulalongkorn University Asthma-related Comorbidities Comorbid conditions of the upper airways Rhinitis and Sinusitis
Somkiat Wongtim Professor of Medicine Division of Respiratory Disease and Critical Care Chulalongkorn University Asthma-related Comorbidities Comorbid conditions of the upper airways Rhinitis and Sinusitis
HCT Medical Policy. Bronchial Thermoplasty. Policy # HCT113 Current Effective Date: 05/24/2016. Policy Statement. Overview
 HCT Medical Policy Bronchial Thermoplasty Policy # HCT113 Current Effective Date: 05/24/2016 Medical Policies are developed by HealthyCT to assist in administering plan benefits and constitute neither
HCT Medical Policy Bronchial Thermoplasty Policy # HCT113 Current Effective Date: 05/24/2016 Medical Policies are developed by HealthyCT to assist in administering plan benefits and constitute neither
Learning the Asthma Guidelines by Case Studies
 Learning the Asthma Guidelines by Case Studies Timothy Craig, DO Professor of Medicine and Pediatrics Distinguished Educator Penn State University Hershey Medical Center Objectives 1. Learn the Asthma
Learning the Asthma Guidelines by Case Studies Timothy Craig, DO Professor of Medicine and Pediatrics Distinguished Educator Penn State University Hershey Medical Center Objectives 1. Learn the Asthma
Asthma in Day to Day Practice
 Asthma in Day to Day Practice VIJAY.K.VANAM Financial relationships: Disclosures Employed at Mercy Medical Center, Mason City. Nonfinancial relationships: I receive no financial gain from any pharmaceutical
Asthma in Day to Day Practice VIJAY.K.VANAM Financial relationships: Disclosures Employed at Mercy Medical Center, Mason City. Nonfinancial relationships: I receive no financial gain from any pharmaceutical
Complements asthma therapy NOT a CURE for Severe. Non pharmacologic treatment of asthma. limits the ability of the airways to constrict.
 Bronchial Thermoplasty Karla Provost Pulmonary and Critical Care Medicine 2015 What is Bronchial Thermoplasty Non pharmacologic treatment of asthma Outpatient procedure performed over 3 treatment sessions
Bronchial Thermoplasty Karla Provost Pulmonary and Critical Care Medicine 2015 What is Bronchial Thermoplasty Non pharmacologic treatment of asthma Outpatient procedure performed over 3 treatment sessions
What is Severe Persistent Asthma? What is Bronchial Thermoplasty Non pharmacologic treatment of asthma
 Objectives BT defined What is Severe Persistent Asthma Case Study introduction How is BT performed Pre-op, PACU and Discharge care Who does it work for the criteria for BT Brief overview of BT results
Objectives BT defined What is Severe Persistent Asthma Case Study introduction How is BT performed Pre-op, PACU and Discharge care Who does it work for the criteria for BT Brief overview of BT results
Update on management of respiratory symptoms. Dr Farid Bazari Consultant Respiratory Physician Kingston Hospital NHS FT
 Update on management of respiratory symptoms Dr Farid Bazari Consultant Respiratory Physician Kingston Hospital NHS FT Topics The common respiratory symptoms Cough: causes, diagnosis and therapy Update
Update on management of respiratory symptoms Dr Farid Bazari Consultant Respiratory Physician Kingston Hospital NHS FT Topics The common respiratory symptoms Cough: causes, diagnosis and therapy Update
Biologic Agents in the treatment of Severe Asthma
 Biologic Agents in the treatment of Severe Asthma Daniel L Maxwell, D.O., FACOI, FAASM Clinical Assistant Professor of Medicine Michigan State University College of Osteopathic Medicine College of Human
Biologic Agents in the treatment of Severe Asthma Daniel L Maxwell, D.O., FACOI, FAASM Clinical Assistant Professor of Medicine Michigan State University College of Osteopathic Medicine College of Human
Endobronchial Thermoplasty
 Endobronchial Thermoplasty Asthma Education Day Thursday, October 30, 2014 Cynthia Ray, MD, FCCP Senior Staff Physician Interventional Pulmonology Pulmonary and Critical Care Medicine Henry Ford Hospital
Endobronchial Thermoplasty Asthma Education Day Thursday, October 30, 2014 Cynthia Ray, MD, FCCP Senior Staff Physician Interventional Pulmonology Pulmonary and Critical Care Medicine Henry Ford Hospital
Endobronchial Thermoplasty
 Endobronchial Thermoplasty Michigan Society for Respiratory Care Monday, October 5, 2015 Cynthia Ray, MD, FCCP Senior Staff Physician Interventional Pulmonology Pulmonary and Critical Care Medicine Henry
Endobronchial Thermoplasty Michigan Society for Respiratory Care Monday, October 5, 2015 Cynthia Ray, MD, FCCP Senior Staff Physician Interventional Pulmonology Pulmonary and Critical Care Medicine Henry
Improving Outcomes in the Management & Treatment of Asthma. April 21, Spring Managed Care Forum
 Improving Outcomes in the Management & Treatment of Asthma April 21, 2016 2016 Spring Managed Care Forum David M. Mannino, M.D. Professor Department of Preventive Medicine and Environmental Health University
Improving Outcomes in the Management & Treatment of Asthma April 21, 2016 2016 Spring Managed Care Forum David M. Mannino, M.D. Professor Department of Preventive Medicine and Environmental Health University
Bronchial Thermoplasty For Severe Persistent Asthma
 Bronchial Thermoplasty For Severe Persistent Asthma Faisal Khan MD Center For Respiratory and Sleep Medicine Indiana Internal Medicine Consultants Franciscan Saint Francis hospital Agenda Burden of Severe
Bronchial Thermoplasty For Severe Persistent Asthma Faisal Khan MD Center For Respiratory and Sleep Medicine Indiana Internal Medicine Consultants Franciscan Saint Francis hospital Agenda Burden of Severe
Searching for Targets to Control Asthma
 Searching for Targets to Control Asthma Timothy Craig Distinguished Educator Professor Medicine and Pediatrics Penn State University Hershey, PA, USA Inflammation and Remodeling in Asthma The most important
Searching for Targets to Control Asthma Timothy Craig Distinguished Educator Professor Medicine and Pediatrics Penn State University Hershey, PA, USA Inflammation and Remodeling in Asthma The most important
Difficult Asthma Assessment: A systematic approach
 Difficult Asthma Assessment: A systematic approach Dr Naghmeh Radhakrishna Respiratory, Sleep & Allergy Physician Allergy, Asthma & Clinical Immunology Service The Alfred Hospital Melbourne, Australia
Difficult Asthma Assessment: A systematic approach Dr Naghmeh Radhakrishna Respiratory, Sleep & Allergy Physician Allergy, Asthma & Clinical Immunology Service The Alfred Hospital Melbourne, Australia
THE PROMISE OF NEW AND NOVEL DRUGS. Pyng Lee Respiratory & Critical Care Medicine National University Hospital
 THE PROMISE OF NEW AND NOVEL DRUGS Pyng Lee Respiratory & Critical Care Medicine National University Hospital Pyng_lee@nuhs.edu.sg Asthma Prevalence, Morbidity, Mortality 235 million suffer from asthma
THE PROMISE OF NEW AND NOVEL DRUGS Pyng Lee Respiratory & Critical Care Medicine National University Hospital Pyng_lee@nuhs.edu.sg Asthma Prevalence, Morbidity, Mortality 235 million suffer from asthma
Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ
 Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ Financial Disclosures Advanced Practiced Advisory Board for Circassia Learning Objectives 1. Briefly
Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ Financial Disclosures Advanced Practiced Advisory Board for Circassia Learning Objectives 1. Briefly
Clinical Implications of Asthma Phenotypes. Michael Schatz, MD, MS Department of Allergy
 Clinical Implications of Asthma Phenotypes Michael Schatz, MD, MS Department of Allergy Definition of Phenotype The observable properties of an organism that are produced by the interaction of the genotype
Clinical Implications of Asthma Phenotypes Michael Schatz, MD, MS Department of Allergy Definition of Phenotype The observable properties of an organism that are produced by the interaction of the genotype
Current Approaches to Asthma & COPD
 10/11/18 Current Approaches to Asthma & COPD Lekshmi Santhosh, M.D. Assistant Professor, Pulm/Critical Care & Hosp Med Primary Care Medicine: Principles & Practice 10.11.2018 Revisiting the Dutch Hypothesis:
10/11/18 Current Approaches to Asthma & COPD Lekshmi Santhosh, M.D. Assistant Professor, Pulm/Critical Care & Hosp Med Primary Care Medicine: Principles & Practice 10.11.2018 Revisiting the Dutch Hypothesis:
Asthma Update I have no professional or personal financial conflicts of interest to disclose.
 Asthma Update 2018 Disclosures Jennifer W. McCallister, MD, FACP, FCCP Associate Professor Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical Center I have
Asthma Update 2018 Disclosures Jennifer W. McCallister, MD, FACP, FCCP Associate Professor Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical Center I have
Asthma Update Jennifer W. McCallister, MD, FACP, FCCP
 Asthma Update 2018 Jennifer W. McCallister, MD, FACP, FCCP Associate Professor Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical Center Disclosures I have
Asthma Update 2018 Jennifer W. McCallister, MD, FACP, FCCP Associate Professor Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical Center Disclosures I have
BRONCHIAL THERMOPLASTY
 Review Article 155 BRONCHIAL THERMOPLASTY Prince James* and Richa Gupta* (Received on 4.5.2010; Accepted after revision on 5.9.2011) Summary: Even with the use of maximum pharmacological treatment, asthma
Review Article 155 BRONCHIAL THERMOPLASTY Prince James* and Richa Gupta* (Received on 4.5.2010; Accepted after revision on 5.9.2011) Summary: Even with the use of maximum pharmacological treatment, asthma
Asthma and Vocal Cord Dysfunction
 Asthma and Vocal Cord Dysfunction Amy L. Marks DO, FACOP Pediatric Allergy and Immunology Assistant Professor of Pediatrics Oakland University William Beaumont School of Medicine Objectives: Understanding
Asthma and Vocal Cord Dysfunction Amy L. Marks DO, FACOP Pediatric Allergy and Immunology Assistant Professor of Pediatrics Oakland University William Beaumont School of Medicine Objectives: Understanding
Asthma Pathophysiology and Treatment. John R. Holcomb, M.D.
 Asthma Pathophysiology and Treatment John R. Holcomb, M.D. Objectives Definition of Asthma Epidemiology and risk factors of Asthma Pathophysiology of Asthma Diagnostics test of Asthma Management of Asthma
Asthma Pathophysiology and Treatment John R. Holcomb, M.D. Objectives Definition of Asthma Epidemiology and risk factors of Asthma Pathophysiology of Asthma Diagnostics test of Asthma Management of Asthma
Cynthia S. Kelly, M.D. Professor of Pediatrics Eastern Virginia Medical School Division Director Allergy Children s Hospital of The King s Daughters
 Cynthia S. Kelly, M.D. Professor of Pediatrics Eastern Virginia Medical School Division Director Allergy Children s Hospital of The King s Daughters Disclosures Speakers bureau of Novartis and Genentech
Cynthia S. Kelly, M.D. Professor of Pediatrics Eastern Virginia Medical School Division Director Allergy Children s Hospital of The King s Daughters Disclosures Speakers bureau of Novartis and Genentech
Xolair (Omalizumab) Drug Prior Authorization Protocol (Medical Benefit & Part B Benefit)
 Drug Prior Authorization Protocol (Medical Benefit & Part B Benefit)") Line of Business: All Lines of Business Effective Date: August 16, 2017 Xolair (Omalizumab) Drug Prior Authorization Protocol (Medical Benefit & Part B Benefit) This policy has been developed through review
Line of Business: All Lines of Business Effective Date: August 16, 2017 Xolair (Omalizumab) Drug Prior Authorization Protocol (Medical Benefit & Part B Benefit) This policy has been developed through review
Asthma Update A/Prof. John Abisheganaden. Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital
 Asthma Update - 2013 A/Prof. John Abisheganaden Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital Asthma A complex syndrome Multifaceted disease Heterogeneous Genetic and
Asthma Update - 2013 A/Prof. John Abisheganaden Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital Asthma A complex syndrome Multifaceted disease Heterogeneous Genetic and
TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS
 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Recommendation PULMONARY FUNCTION TESTING (SPIROMETRY) Conditional: The Expert Panel that spirometry measurements FEV1,
TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Recommendation PULMONARY FUNCTION TESTING (SPIROMETRY) Conditional: The Expert Panel that spirometry measurements FEV1,
Do We Need Biologics in Pediatric Asthma Management?
 Do We Need Biologics in Pediatric Asthma Management? Ting Fan LEUNG, MBChB, MD, FRCPCH, FAAAAI Professor and Chairman Department of Paediatrics The Chinese University of Hong Kong Asthma and Allergy by
Do We Need Biologics in Pediatric Asthma Management? Ting Fan LEUNG, MBChB, MD, FRCPCH, FAAAAI Professor and Chairman Department of Paediatrics The Chinese University of Hong Kong Asthma and Allergy by
West of Scotland Difficult Asthma Group Statement of Practice
 West of Scotland Difficult Asthma Group Statement of Practice Member Health Boards: Ayrshire and Arran Dumfries and Galloway Forth Valley Lanarkshire Glasgow INFORMATION ON THE USE OF BRONCHIAL THERMOPLASTY
West of Scotland Difficult Asthma Group Statement of Practice Member Health Boards: Ayrshire and Arran Dumfries and Galloway Forth Valley Lanarkshire Glasgow INFORMATION ON THE USE OF BRONCHIAL THERMOPLASTY
Asthma Management for the Athlete
 Asthma Management for the Athlete Khanh Lai, MD Assistant Professor Division of Pediatric Pulmonary and Sleep Medicine University of Utah School of Medicine 2 nd Annual Sports Medicine Symposium: The Pediatric
Asthma Management for the Athlete Khanh Lai, MD Assistant Professor Division of Pediatric Pulmonary and Sleep Medicine University of Utah School of Medicine 2 nd Annual Sports Medicine Symposium: The Pediatric
Robert Kruklitis, MD, PhD Chief, Pulmonary Medicine Lehigh Valley Health Network
 Robert Kruklitis, MD, PhD Chief, Pulmonary Medicine Lehigh Valley Health Network Robert.kruklitis@lvh.com Correlation of a Asthma pathophyisology with basic science Asthma (Physiology) Bronchodilators
Robert Kruklitis, MD, PhD Chief, Pulmonary Medicine Lehigh Valley Health Network Robert.kruklitis@lvh.com Correlation of a Asthma pathophyisology with basic science Asthma (Physiology) Bronchodilators
Meeting the Challenges of Asthma
 Presenter Disclosure Information 11:05 11:45am Meeting the Challenge of Asthma SPEAKER Christopher Fanta, MD The following relationships exist related to this presentation: Christopher Fanta, MD: No financial
Presenter Disclosure Information 11:05 11:45am Meeting the Challenge of Asthma SPEAKER Christopher Fanta, MD The following relationships exist related to this presentation: Christopher Fanta, MD: No financial
Lung Cancer Screening Computed Tomography Screening in Pa6ents at Risk for Lung Cancer
 Lung Cancer Screening Computed Tomography Screening in Pa6ents at Risk for Lung Cancer Doug Arenberg, M.D. University of Michigan Disclosures Objec6ve Define patients who will benefit from screening for
Lung Cancer Screening Computed Tomography Screening in Pa6ents at Risk for Lung Cancer Doug Arenberg, M.D. University of Michigan Disclosures Objec6ve Define patients who will benefit from screening for
I have no perceived conflicts of interest or commercial relationships to disclose.
 ASTHMA BASICS Michelle Dickens RN FNP-C AE-C Nurse Practitioner/Certified Asthma Educator Ferrell Duncan Allergy/Asthma/Immunology Coordinator, CoxHealth Asthma Center DISCLOSURES I have no perceived conflicts
ASTHMA BASICS Michelle Dickens RN FNP-C AE-C Nurse Practitioner/Certified Asthma Educator Ferrell Duncan Allergy/Asthma/Immunology Coordinator, CoxHealth Asthma Center DISCLOSURES I have no perceived conflicts
Outline. Outline. Definition. Asthma, GERD and Laryngeal Pharyngeal Reflux (LPR) Definitions
 Definitions") Asthma, GERD and Laryngeal Pharyngeal Reflux (LPR) Richard F. Lockey, M.D. Division of Allergy and Immunology Department of Internal Medicine University of South Florida College of Medicine and James A.
Asthma, GERD and Laryngeal Pharyngeal Reflux (LPR) Richard F. Lockey, M.D. Division of Allergy and Immunology Department of Internal Medicine University of South Florida College of Medicine and James A.
Current Asthma Therapy: Little Need to Phenotype. Phenotypes of Severe Asthma. Cellular Phenotypes 12/7/2012
 Subbasement Membrane Thickness(µm) 12/7/212 Current Asthma Therapy: Little Need to Phenotype Phenotypes of Severe Asthma Most mild and to some degree moderate asthmatics respond well to currently available
Subbasement Membrane Thickness(µm) 12/7/212 Current Asthma Therapy: Little Need to Phenotype Phenotypes of Severe Asthma Most mild and to some degree moderate asthmatics respond well to currently available
LONG-ACTING BETA AGONISTS
 LONG-ACTING BETA AGONISTS AND ICS/LABA COMBINATIONS DISCLOSURE Dr. Francisco has no financial interest in any commercial entity discussed in this presentation Dr. Francisco will not discuss experimental
LONG-ACTING BETA AGONISTS AND ICS/LABA COMBINATIONS DISCLOSURE Dr. Francisco has no financial interest in any commercial entity discussed in this presentation Dr. Francisco will not discuss experimental
Asthma - Chronic. Presentations of asthma Cough Wheeze Breathlessness Chest tightness
 Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Subject: Bronchial Thermoplasty
 Subject: Bronchial Thermoplasty Guidance Number: MCG-171 Revision Date(s): Original Effective Date: 6/12/14 Medical Coverage Guidance Approval Date: 6/12/14 PREFACE This Medical Guidance is intended to
Subject: Bronchial Thermoplasty Guidance Number: MCG-171 Revision Date(s): Original Effective Date: 6/12/14 Medical Coverage Guidance Approval Date: 6/12/14 PREFACE This Medical Guidance is intended to
New TLD Indication: Asthma RELIEF-1 Study. Nick ten Hacken, MD Study Co-Principal Investigator
 New TLD Indication: Asthma RELIEF-1 Study Nick ten Hacken, MD Study Co-Principal Investigator The Burden of Asthma WW Adult Asthma Prevalence 230.5 Million Mild/Intermittent 161.9 Million (70%) Moderate
New TLD Indication: Asthma RELIEF-1 Study Nick ten Hacken, MD Study Co-Principal Investigator The Burden of Asthma WW Adult Asthma Prevalence 230.5 Million Mild/Intermittent 161.9 Million (70%) Moderate
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing
 Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Update on Biologicals for ABPA and Asthma
 Update on Biologicals for ABPA and Asthma 5 th Advances Against Aspergillosis Istanbul 27 Jan 2012 Richard B. Moss MD Professor of Pediatrics Stanford University Palo Alto CA USA Disease of chronic airway
Update on Biologicals for ABPA and Asthma 5 th Advances Against Aspergillosis Istanbul 27 Jan 2012 Richard B. Moss MD Professor of Pediatrics Stanford University Palo Alto CA USA Disease of chronic airway
Treatment Options for Complicated/Severe Asthma. Henry J. Kanarek, MD Kanarek Allergy Asthma Immunology
 Treatment Options for Complicated/Severe Asthma Henry J. Kanarek, MD Kanarek Allergy Asthma Immunology www.kallergy.com 913-451-8555 Asthma Epidemiology World Health Organization, Asthma is one of the
Treatment Options for Complicated/Severe Asthma Henry J. Kanarek, MD Kanarek Allergy Asthma Immunology www.kallergy.com 913-451-8555 Asthma Epidemiology World Health Organization, Asthma is one of the
Asthma for Primary Care: Assessment, Control, and Long-Term Management
 Asthma for Primary Care: Assessment, Control, and Long-Term Management Learning Objectives After participating in this educational activity, participants should be better able to: 1. Choose the optimal
Asthma for Primary Care: Assessment, Control, and Long-Term Management Learning Objectives After participating in this educational activity, participants should be better able to: 1. Choose the optimal
Asthma Therapy 2017 JOSHUA S. JACOBS, M.D.
 Asthma Therapy 2017 JOSHUA S. JACOBS, M.D. BACKGROUND-PREVALENCE Asthma is one of the most common chronic diseases worldwide with an estimated 300 million affected individuals Prevalence is increasing
Asthma Therapy 2017 JOSHUA S. JACOBS, M.D. BACKGROUND-PREVALENCE Asthma is one of the most common chronic diseases worldwide with an estimated 300 million affected individuals Prevalence is increasing
New Therapies for Asthma
 New Therapies for Asthma Tracy Bridges, MD Speaker Disclosure: Dr. Bridges participates in speaker bureaus for Teva, Genetech & Astra Zeneca. Objectives: Discuss the use of LAMA s for Asthma Detail the
New Therapies for Asthma Tracy Bridges, MD Speaker Disclosure: Dr. Bridges participates in speaker bureaus for Teva, Genetech & Astra Zeneca. Objectives: Discuss the use of LAMA s for Asthma Detail the
Diagnosis and Differen-al Diagnosis of Asthma
 Diagnosis and Differen-al Diagnosis of Asthma Jay Peters MD Professor and Chief Pulmonary/Cri7cal Care Medicine University of Texas Health Science Center San Antonio Disclosures: None Disclosures Nothing
Diagnosis and Differen-al Diagnosis of Asthma Jay Peters MD Professor and Chief Pulmonary/Cri7cal Care Medicine University of Texas Health Science Center San Antonio Disclosures: None Disclosures Nothing
7/7/2015. Somboon Chansakulporn, MD. History of variable respiratory symptoms. 1. Documented excessive variability in PFT ( 1 test)
") Definition of Asthma GINA 2010: Chronic inflammatory disorder of the airways Airway hyper-responsiveness Recurrent wheezing, breathlessness, chest tightness, coughing Variable, reversible airflow obstruction
Definition of Asthma GINA 2010: Chronic inflammatory disorder of the airways Airway hyper-responsiveness Recurrent wheezing, breathlessness, chest tightness, coughing Variable, reversible airflow obstruction
Improving the Management of Asthma to Improve Patient Adherence and Outcomes
 Improving the Management of Asthma to Improve Patient Adherence and Outcomes Robert Sussman, MD Atlantic Health System Overlook Medical Center Asthma Remains a Serious Health Risk in the US Every day in
Improving the Management of Asthma to Improve Patient Adherence and Outcomes Robert Sussman, MD Atlantic Health System Overlook Medical Center Asthma Remains a Serious Health Risk in the US Every day in
COPD and Asthma Update. April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute
 COPD and Asthma Update April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute What we ll be talking about COPD: diagnosis, management of stable COPD, COPD exacerbations Asthma: diagnosis,
COPD and Asthma Update April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute What we ll be talking about COPD: diagnosis, management of stable COPD, COPD exacerbations Asthma: diagnosis,
ASTHMA. Dr Liz Gamble BRI
 ASTHMA Dr Liz Gamble BRI Diagnosis Clinical: wheeze, breathlessness, chest tightness, cough Variable airflow obstruction: peak flow chart, spirometry with reversibility to bronchodilators Airways hyper-responsiveness
ASTHMA Dr Liz Gamble BRI Diagnosis Clinical: wheeze, breathlessness, chest tightness, cough Variable airflow obstruction: peak flow chart, spirometry with reversibility to bronchodilators Airways hyper-responsiveness
Prof Neil Barnes. Respiratory and General Medicine London Chest Hospital and The Royal London Hospital
 Prof Neil Barnes Respiratory and General Medicine London Chest Hospital and The Royal London Hospital ASTHMA: WHEN EVERYTHING FAILS WHAT DO YOU DO? South GP CME 2013, Dunedin Saturday 17 th August 2013
Prof Neil Barnes Respiratory and General Medicine London Chest Hospital and The Royal London Hospital ASTHMA: WHEN EVERYTHING FAILS WHAT DO YOU DO? South GP CME 2013, Dunedin Saturday 17 th August 2013
GERD DIAGNOSIS & TREATMENT DISCLOSURES 4/18/2018
 GERD DIAGNOSIS & TREATMENT Subhash Chandra MBBS Assistant Professor CHI Health Clinic Gastroenterology Creighton University, School of Medicine April 28, 2018 DISCLOSURES None 1 OBJECTIVES Review update
GERD DIAGNOSIS & TREATMENT Subhash Chandra MBBS Assistant Professor CHI Health Clinic Gastroenterology Creighton University, School of Medicine April 28, 2018 DISCLOSURES None 1 OBJECTIVES Review update
Adult asthma management: focus on control
 Adult asthma management: focus on control Jennifer W. McCallister, MD Associate Professor Pulmonary, Allergy, Critical Care & Sleep Medicine The Ohio State University Wexner Medical Center Objectives Apply
Adult asthma management: focus on control Jennifer W. McCallister, MD Associate Professor Pulmonary, Allergy, Critical Care & Sleep Medicine The Ohio State University Wexner Medical Center Objectives Apply
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: bronchial_thermoplasty 10/2010 3/2018 3/2019 3/2018 Description of Procedure or Service Bronchial thermoplasty
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: bronchial_thermoplasty 10/2010 3/2018 3/2019 3/2018 Description of Procedure or Service Bronchial thermoplasty
Eosinophilic esophagitis. Kathleen Boynton MD University of Utah Gastroenterology Division
 Eosinophilic esophagitis Kathleen Boynton MD University of Utah Gastroenterology Division Financial disclosures: Janssen Genetech UCB All for research support Learning Objectives To identify the clinical
Eosinophilic esophagitis Kathleen Boynton MD University of Utah Gastroenterology Division Financial disclosures: Janssen Genetech UCB All for research support Learning Objectives To identify the clinical
Smooth Muscle & Asthma: Bronchial Thermoplasty - A Smooth Muscle Modifier
 Smooth Muscle & Asthma: Bronchial Thermoplasty - A Smooth Muscle Modifier Mario Castro, MD, MPH Professor of Medicine and Pediatrics Director, The Asthma and Airway Translational Research Unit, Washington
Smooth Muscle & Asthma: Bronchial Thermoplasty - A Smooth Muscle Modifier Mario Castro, MD, MPH Professor of Medicine and Pediatrics Director, The Asthma and Airway Translational Research Unit, Washington
Exercise-Induced Bronchospasm. Michael A Lucia, MD, FCCP Asst Clinical Professor, UNR School of Medicine Sierra Pulmonary & Sleep Institute
 Exercise-Induced Bronchospasm Michael A Lucia, MD, FCCP Asst Clinical Professor, UNR School of Medicine Sierra Pulmonary & Sleep Institute EIB Episodic bronchoconstriction with exercise May be an exacerbation
Exercise-Induced Bronchospasm Michael A Lucia, MD, FCCP Asst Clinical Professor, UNR School of Medicine Sierra Pulmonary & Sleep Institute EIB Episodic bronchoconstriction with exercise May be an exacerbation
Clinical efficacy of montelukast in anti-inflammatory treatment of asthma and allergic rhinitis
 Clinical efficacy of montelukast in anti-inflammatory treatment of asthma and allergic rhinitis Kim Hyun Hee, MD, PhD. Dept. of Pediatrics The Catholic University of Korea College of Medicine Achieving
Clinical efficacy of montelukast in anti-inflammatory treatment of asthma and allergic rhinitis Kim Hyun Hee, MD, PhD. Dept. of Pediatrics The Catholic University of Korea College of Medicine Achieving
Asthma Update Eric S. Papierniak, DO Malcom Randall VAMC Assistant Professor of Medicine UF Div. of Pulmonary, Critical Care, and Sleep Medicine
 Asthma Update 2014 Eric S. Papierniak, DO Malcom Randall VAMC Assistant Professor of Medicine UF Div. of Pulmonary, Critical Care, and Sleep Medicine Goals/Objectives Review of 2014 GINA guidelines Significant
Asthma Update 2014 Eric S. Papierniak, DO Malcom Randall VAMC Assistant Professor of Medicine UF Div. of Pulmonary, Critical Care, and Sleep Medicine Goals/Objectives Review of 2014 GINA guidelines Significant
Breakfast Session Prof Neil Barnes Professor of Respiratory Medicine London Chest Hospital & The Royal London Hospital United Kingdom
 Breakfast Session Prof Neil Barnes Professor of Respiratory Medicine London Chest Hospital & The Royal London Hospital United Kingdom 2 BEYOND SYMPTOMS ADDRESSING FUTURE RISK IN ASTHMA South GP CME 2013,
Breakfast Session Prof Neil Barnes Professor of Respiratory Medicine London Chest Hospital & The Royal London Hospital United Kingdom 2 BEYOND SYMPTOMS ADDRESSING FUTURE RISK IN ASTHMA South GP CME 2013,
Global Initiative for Asthma (GINA) What s new in GINA 2016?
 What s new in GINA 2016?") Global Initiative for Asthma (GINA) What s new in GINA 2016? GINA Global Strategy for Asthma Management and Prevention GINA: A Brief History Established in 1993 Collaboration between NHLBI and WHO Multiple
Global Initiative for Asthma (GINA) What s new in GINA 2016? GINA Global Strategy for Asthma Management and Prevention GINA: A Brief History Established in 1993 Collaboration between NHLBI and WHO Multiple
Pulmonary Function Testing: Concepts and Clinical Applications. Potential Conflict Of Interest. Objectives. Rationale: Why Test?
 Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Asthma and Its Many Unmet Needs: Directions for Novel Therapeutic Approaches
 Asthma and Its Many Unmet Needs: Directions for Novel Therapeutic Approaches William W. Busse,, M.D. University of Wisconsin School of Medicine and Public Health Madison, WI, USA Disclosure Slide Employment
Asthma and Its Many Unmet Needs: Directions for Novel Therapeutic Approaches William W. Busse,, M.D. University of Wisconsin School of Medicine and Public Health Madison, WI, USA Disclosure Slide Employment
EFFECTIVE ASTHMA MANAGEMENT IN PRIMARY CARE Severity Assessment, Guidelines, and New Therapeutic Options
 Educational Objectives EFFECTIVE ASTHMA MANAGEMENT IN PRIMARY CARE Bradley E. Chipps, MD, FAAP, FACAAI, FAAAAI, FCCP President-Elect, American College of Allergy, Asthma & Immunology Medical Director,
Educational Objectives EFFECTIVE ASTHMA MANAGEMENT IN PRIMARY CARE Bradley E. Chipps, MD, FAAP, FACAAI, FAAAAI, FCCP President-Elect, American College of Allergy, Asthma & Immunology Medical Director,
Dual-Controller Asthma Therapy: Rationale and Clinical Benefits
 B/1 Dual-Controller Asthma Therapy: Rationale and Clinical Benefits MODULE B The 1997 National Heart, Lung, and Blood Institute (NHLBI) Expert Panel guidelines on asthma management recommend a 4-step approach
B/1 Dual-Controller Asthma Therapy: Rationale and Clinical Benefits MODULE B The 1997 National Heart, Lung, and Blood Institute (NHLBI) Expert Panel guidelines on asthma management recommend a 4-step approach
Five Consecutive cases of Bronchial Thermoplasty
 Five Consecutive cases of Bronchial Thermoplasty -Hiren J. Mehta MD Assistant Professor of Medicine Interventional Pulmonology University of Florida Hiren.Mehta@medicine.ufl.edu none Disclosures Asthma
Five Consecutive cases of Bronchial Thermoplasty -Hiren J. Mehta MD Assistant Professor of Medicine Interventional Pulmonology University of Florida Hiren.Mehta@medicine.ufl.edu none Disclosures Asthma
Common Confounding Consults In Pulmonary & Critical Care
 Common Confounding Consults In Pulmonary & Critical Care Lekshmi Santhosh, M.D. Assistant Professor, Pulm/Critical Care & Hosp Med Management of the Hospitalized Patient 10.20.2018 Disclosures None. 1
Common Confounding Consults In Pulmonary & Critical Care Lekshmi Santhosh, M.D. Assistant Professor, Pulm/Critical Care & Hosp Med Management of the Hospitalized Patient 10.20.2018 Disclosures None. 1
Pediatric and Adult. Disclosure. Asthma. Learning Objectives. EPR-3: What s Changed? Asthma: Pediatric and Adult
 Asthma: Pediatric and Adult Americo D. Fraboni, MD, FAAFP Assistant Clinical Professor Department of Family Practice & Community Health University of Minnesota Medical School Minneapolis, Minnesota Disclosure
Asthma: Pediatric and Adult Americo D. Fraboni, MD, FAAFP Assistant Clinical Professor Department of Family Practice & Community Health University of Minnesota Medical School Minneapolis, Minnesota Disclosure
12/18/2017. Disclosures. Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing
 Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Bronchial Thermoplasty
 Medical Policy Manual Surgery, Policy No. 178 Bronchial Thermoplasty Next Review: September 2018 Last Review: October 2017 Effective: November 1, 2017 IMPORTANT REMINDER Medical Policies are developed
Medical Policy Manual Surgery, Policy No. 178 Bronchial Thermoplasty Next Review: September 2018 Last Review: October 2017 Effective: November 1, 2017 IMPORTANT REMINDER Medical Policies are developed
Severe Asthma(s): Can THEY be prevented or reversed?
: Can THEY be prevented or reversed?") Severe Asthma(s): Can THEY be prevented or reversed? Sally Wenzel, MD Professor of Medicine UPMC Chair in Translational Airway Biology Disclosures Sally Wenzel, M.D. Grant/Research Support: Boehringer-Ingelheim,
Severe Asthma(s): Can THEY be prevented or reversed? Sally Wenzel, MD Professor of Medicine UPMC Chair in Translational Airway Biology Disclosures Sally Wenzel, M.D. Grant/Research Support: Boehringer-Ingelheim,
Bronchial Thermoplasty
 Bronchial Thermoplasty Policy Number: 7.01.127 Last Review: 9/2014 Origination: 11/2010 Next Review: 3/2015 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will not provide coverage for bronchial
Bronchial Thermoplasty Policy Number: 7.01.127 Last Review: 9/2014 Origination: 11/2010 Next Review: 3/2015 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will not provide coverage for bronchial
WEBINAR. Difficult-to-treat and severe asthma: changing the paradigm
 WEBINAR Difficult-to-treat and severe asthma: changing the paradigm A multidisciplinary discussion on new therapies, and how to identify and manage difficult-to-treat and severe asthma DIFFICULT-TO-TREAT
WEBINAR Difficult-to-treat and severe asthma: changing the paradigm A multidisciplinary discussion on new therapies, and how to identify and manage difficult-to-treat and severe asthma DIFFICULT-TO-TREAT
Asthma in the college health setting: diagnosis, treatment, pitfalls
 Asthma in the college health setting: diagnosis, treatment, pitfalls A 20-year-old college student with a history of asthma and allergic rhinitis, which were diagnosed in childhood, presents with cough
Asthma in the college health setting: diagnosis, treatment, pitfalls A 20-year-old college student with a history of asthma and allergic rhinitis, which were diagnosed in childhood, presents with cough
An Insight into Allergy and Allergen Immunotherapy Co-morbidities of allergic disease
 An Insight into Allergy and Allergen Immunotherapy Co-morbidities of allergic disease Carmen Vidal Athens, September 11, 2014 Pucci S & Incorvaia C, 2008; 153:1-2 1. The major player in driving the immune
An Insight into Allergy and Allergen Immunotherapy Co-morbidities of allergic disease Carmen Vidal Athens, September 11, 2014 Pucci S & Incorvaia C, 2008; 153:1-2 1. The major player in driving the immune
Interven'ons that Improve Outcomes of COPD
 Interven'ons that Improve Outcomes of COPD Sidney S. Braman MD FCCP Professor of Medicine The Ichan School of Medicine at Mount Sinai New York, NY Disclosures Consultant Sunovion, BI, Forest, Meda Reference
Interven'ons that Improve Outcomes of COPD Sidney S. Braman MD FCCP Professor of Medicine The Ichan School of Medicine at Mount Sinai New York, NY Disclosures Consultant Sunovion, BI, Forest, Meda Reference
BRONCHIAL THERMOPLASTY
 BRONCHIAL THERMOPLASTY UnitedHealthcare Community Plan Medical Policy Policy Number: CS014.E Effective Date: July 1, 2017 Table of Contents Page INSTRUCTIONS FOR USE... 1 BENEFIT CONSIDERATIONS... 1 COVERAGE
BRONCHIAL THERMOPLASTY UnitedHealthcare Community Plan Medical Policy Policy Number: CS014.E Effective Date: July 1, 2017 Table of Contents Page INSTRUCTIONS FOR USE... 1 BENEFIT CONSIDERATIONS... 1 COVERAGE
Biologics in asthma Are we turning the corner? Roland Buhl Pulmonary Department Mainz University Hospital
 Biologics in asthma Are we turning the corner? Roland Buhl Pulmonary Department Mainz University Hospital Biologics in asthma - are we turning the corner? Allergic asthma anti - IgE Allergic airway inflammation
Biologics in asthma Are we turning the corner? Roland Buhl Pulmonary Department Mainz University Hospital Biologics in asthma - are we turning the corner? Allergic asthma anti - IgE Allergic airway inflammation
Asthma COPD Overlap (ACO)
") Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
Asthma in Older Adults
 Baystate Medical Center Grand Rounds Asthma in Older Adults Sucharita Kher, MD Medical Director, Pulmonary Clinic, Assistant Professor, TUSM Objectives Recognize the problem of asthma in older adults Review
Baystate Medical Center Grand Rounds Asthma in Older Adults Sucharita Kher, MD Medical Director, Pulmonary Clinic, Assistant Professor, TUSM Objectives Recognize the problem of asthma in older adults Review
DIFFICULT ASTHMA. Dr. Prathyusha Dr. S.Balasubramanian KKCTH
 DIFFICULT ASTHMA Dr. Prathyusha Dr. S.Balasubramanian KKCTH CASE SUMMARY 11 yr old girl, Neyveli Treated as moderate persistent asthma x 5 years On Seroflo [ LABA + steroid ] 250 2 puffs BD and intermittent
DIFFICULT ASTHMA Dr. Prathyusha Dr. S.Balasubramanian KKCTH CASE SUMMARY 11 yr old girl, Neyveli Treated as moderate persistent asthma x 5 years On Seroflo [ LABA + steroid ] 250 2 puffs BD and intermittent
Asthma. Rachel Miller, MD, FAAAAI Director Allergy and Immunology New York Presbyterian Hospital. Figure 1 Asthma Prevalence,
 Asthma Rachel Miller, MD, FAAAAI Director Allergy and Immunology New York Presbyterian Hospital Figure 1 Asthma Prevalence, 1980-2000 * Gap between 1995-1996 and 1997 indicates a break in trend due to
Asthma Rachel Miller, MD, FAAAAI Director Allergy and Immunology New York Presbyterian Hospital Figure 1 Asthma Prevalence, 1980-2000 * Gap between 1995-1996 and 1997 indicates a break in trend due to
B2. PHARMACISTS DIFFICULT TO TREAT ASTHMA/COPD EXACERBATIONS 12:45-1:45PM
 B2. PHARMACISTS DIFFICULT TO TREAT ASTHMA/COPD EXACERBATIONS 12:45-1:45PM ACPE UAN: 107-000-14-024-L01-P Activity Type: Application-Based 0.1 CEU/1.0 hr Learning Objectives for Pharmacists: Upon completion
B2. PHARMACISTS DIFFICULT TO TREAT ASTHMA/COPD EXACERBATIONS 12:45-1:45PM ACPE UAN: 107-000-14-024-L01-P Activity Type: Application-Based 0.1 CEU/1.0 hr Learning Objectives for Pharmacists: Upon completion
Clinical Practice Guideline: Asthma
 Clinical Practice Guideline: Asthma INTRODUCTION A critical aspect of the diagnosis and management of asthma is the precise and periodic measurement of lung function both before and after bronchodilator
Clinical Practice Guideline: Asthma INTRODUCTION A critical aspect of the diagnosis and management of asthma is the precise and periodic measurement of lung function both before and after bronchodilator
Symptoms are worse at night and in the morning and includes cough, whz, chest tightness.
 Asthma Review ETIOLOGY Airflow limitation is caused by the following: - bronchoconstriction - mucous pluggin - airway inflammation Sudden death - heavy mucous plugging is common - typically occurs between
Asthma Review ETIOLOGY Airflow limitation is caused by the following: - bronchoconstriction - mucous pluggin - airway inflammation Sudden death - heavy mucous plugging is common - typically occurs between
Step up if needed (first, check adherence, environmental control and comorbid conditions) Patients ASSESS CONTROL. Step down if possible
 Patients ASSESS CONTROL. Step down if possible") 12/9/212 Pharmacogenomics Treating the Individual Asthma Patient Elliot Israel, M.D. Professor of Medicine Harvard Medical School Brigham & Women s Hospital Partners Asthma Center Too much of a good thing?
12/9/212 Pharmacogenomics Treating the Individual Asthma Patient Elliot Israel, M.D. Professor of Medicine Harvard Medical School Brigham & Women s Hospital Partners Asthma Center Too much of a good thing?
Asthma Treatment Update: 2018
 Asthma Treatment Update: 2018 John B. Cox MD Clinical Professor Division of Pulmonary, Critical Care, Allergy and Sleep Medicine Medical University of South Carolina Disclosures I have no conflicts and
Asthma Treatment Update: 2018 John B. Cox MD Clinical Professor Division of Pulmonary, Critical Care, Allergy and Sleep Medicine Medical University of South Carolina Disclosures I have no conflicts and
Update in Pulmonology Update in Medicine and Primary Care November 11, 2017
 Update in Pulmonology Update in Medicine and Primary Care November 11, 2017 Denitza P. Blagev, MD Pulmonary & Critical Care Medicine Director, Schmidt Chest Clinic Director, Lung Cancer Screening Program
Update in Pulmonology Update in Medicine and Primary Care November 11, 2017 Denitza P. Blagev, MD Pulmonary & Critical Care Medicine Director, Schmidt Chest Clinic Director, Lung Cancer Screening Program
Outline FEF Reduced FEF25-75 in asthma. What does it mean and what are the clinical implications?
 Reduced FEF25-75 in asthma. What does it mean and what are the clinical implications? Fernando Holguin MD MPH Director, Asthma Clinical & Research Program Center for lungs and Breathing University of Colorado
Reduced FEF25-75 in asthma. What does it mean and what are the clinical implications? Fernando Holguin MD MPH Director, Asthma Clinical & Research Program Center for lungs and Breathing University of Colorado
Asthma Upate 2018: What s New Since the 2007 Asthma Guidelines of NAEPP?
 10:50-11:50am Asthma Update 2018: What s New Since the 2007 National Asthma Guidelines? SPEAKER Christopher H. Fanta, MD Disclosures The following relationships exist related to this presentation: Christopher
10:50-11:50am Asthma Update 2018: What s New Since the 2007 National Asthma Guidelines? SPEAKER Christopher H. Fanta, MD Disclosures The following relationships exist related to this presentation: Christopher
11/15/2017. Highgate Private Hospital (Royal Free London NHS Foundation Trust) Causes of chronic cough
 Causes of chronic cough") A whistle stop of Chronic Cough For 10min consultations.. Dr Dean Creer Consultant Chest Physician (MBChB, FRCP) Highgate Private Hospital (Royal Free London NHS Foundation Trust) E: drcreer.pa@gmail.com(secretary)
A whistle stop of Chronic Cough For 10min consultations.. Dr Dean Creer Consultant Chest Physician (MBChB, FRCP) Highgate Private Hospital (Royal Free London NHS Foundation Trust) E: drcreer.pa@gmail.com(secretary)
Week 23 Respirology. Other Asthma & COPD Medications Self Learning Module
 Week 23 Respirology Other Asthma & COPD Medications Self Learning Module DISCLOSURE Relevant relationships with commercial entities [None] Potential for conflicts of interest within this presentation [None]
Week 23 Respirology Other Asthma & COPD Medications Self Learning Module DISCLOSURE Relevant relationships with commercial entities [None] Potential for conflicts of interest within this presentation [None]
Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007
 Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Selecting Initial Therapy
Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Selecting Initial Therapy
Asthma Phenotypes, Heterogeneity and Severity: The Basis of Asthma Management
 Asthma Phenotypes, Heterogeneity and Severity: The Basis of Asthma Management Eugene R. Bleecker, MD Professor and Director, Center for Genomics & Personalized Medicine Research Professor, Translational
Asthma Phenotypes, Heterogeneity and Severity: The Basis of Asthma Management Eugene R. Bleecker, MD Professor and Director, Center for Genomics & Personalized Medicine Research Professor, Translational
Asthma Management in Pregnancy HEATHER HOWE, MD UNIVERSITY OF UTAH PULMONARY DIVISION
 Asthma Management in Pregnancy HEATHER HOWE, MD UNIVERSITY OF UTAH PULMONARY DIVISION Asthma Management in Pregnancy Effects of asthma on pregnancy outcomes Effects of pregnancy on asthma control Management
Asthma Management in Pregnancy HEATHER HOWE, MD UNIVERSITY OF UTAH PULMONARY DIVISION Asthma Management in Pregnancy Effects of asthma on pregnancy outcomes Effects of pregnancy on asthma control Management