TABLE OF CONTENTS (Click on a link below to view the section.)
|
|
|
- Jeremy Simmons
- 6 years ago
- Views:
Transcription
1 Follow the links below to access the complete formularies for Plans: Buckeye Health Plan Acne Allergy Allergic Anaphylactic Reaction Allergic Conjunctivitis Allergic Rhinitis Asthma Atopic Dermatitis Behavioral Health TABLE OF CONTENTS (Click on a link below to view the section.) Anxiety Disorders & Depression Attention Deficit Hyperactivity Disorder Diabetes Gastroesophageal Reflux Head Lice Oral Antibiotics Otic Antibiotics
2 Benzoyl Peroxide (BPO ) Clindamycin Phosphate (Cleocin-T ) Erythromycin Adapalene (Differin ) Tretinoin (Retin-A ) Benzoyl Peroxide/ Erythromycin (Benzamycin ) Clindamycin/ Benzoyl Peroxide ACNE Topical Anti-bacterials 2.5%, 5%, 10% Gel or Liquid $21 1% Gel, 1% Lotion $110 1% Solution $49 2% Gel $171 PA 2% Solution $50 0.3% Gel, 0.1% Cream, 0.1% Lotion (Rx) $171 PA cream & gel PA PA PA 0.1% Gel (OTC) $106 PA PA 0.025%, 0.05% 0.1% Cream; 0.01%, 0.025% Gel Topical Retinoids Topical Combinations $188 PA PA 5-3% Gel $227 PA PA PA 1-5% Gel (Benzaclin ) $240 PA PA PA PA 1.2-5% Gel (Duac ) $123 PA PA PA PA
3 Doxycycline monohydrate Minocycline Isotretinoin (Claravis, Myorisan, Zenatane ) ACNE (CONTINUED) Oral Antibiotics 50 mg, 100 mg (capsule preferred) 50 mg, 75 mg, 100 mg (capsule preferred) Oral Retinoids $33 PA PA PA PA $37 10mg-40mg $648 PA PA PA PA PA PA
4 Adrenaclick 0.3mg/0.3mL, 0.15mg/0.15mL $170 PA PA PA Auvi-Q 0.3mg/0.3mL, 0.15mg/0.15mL $5,400 PA PA PA PA PA PA EpiPen 0.3mg/0.3mL, 0.15mg/0.15mL $156 EpiPen Jr. 0.15mg/0.3ml Azelastine 0.05% $31 PA PA Cromolyn 4% $19 Ketotifen (Alaway, Zatidor ) ALLERGIC ANAPHYLACTIC REACTION Epinephrine Auto-injector ALLERGIC CONJUNCTIVITIS Ophthalmic Antihistamines 0.025% $22 PA
5 Cetirizine (Zyrtec ) Fexofenadine (Allegra ) Loratadine (Claritin ) 5, 10 mg $48 1 mg/ml $18 < 6 yo 30 mg/5 ml $30 PA PA PA 60 mg, 180 mg $30 PA PA 180 mg 10 mg $20 1 mg/ml $27 5 mg Chew $26 PA Azelastine 0.15%, 0.1% $49 PA Budesonide (Rhinocort Allergy) 32 mcg/act $28 PA PA PA PA Flunisolide 25 mcg/act $65 PA Fluticasone (Flonase ) Triamcinolone (Nasacort ) ALLERGIC RHINITIS Oral Antihistamines Nasal Antihistamines Nasal Steroids 50 mcg/act $27 55 mcg/act $27 PA PA PA
6 Albuterol Solution 2.5 mg/3 ml $28 Albuterol (Preferred: Ventolin HFA) Beclomethasone dipropionate (Qvar HFA) Budesonide (Pulmicort Flexhaler ) Budesonide (Pulmicort Respules ) Flunisolide (Aerospan HFA) No dose counter Fluticasone furoate (Arnuity Ellipta ) Fluticasone propionate (Flovent Diskus ) Fluticasone propionate (Flovent HFA) ASTHMA Beta-2 Adrenergic Agonists 90 mcg/act $63 Inhaled Corticosteroids 40 mcg/act, 80 mcg/act $220 PA PA PA PA 90 mcg, 180 mcg DPI $227 PA PA PA PA 0.25 mg/2 ml, 0.5 mg/2ml, 1 mg/2ml $ yo < 4 yo 80 mcg/act $245 PA PA PA PA 100 mcg DPI, 200 mcg DPI 50 mcg DPI, 100 mcg DPI, 250 mcg DPI 44 mcg/act, 110 mcg/act, 220 mcg/act $223 PA PA PA PA $206 PA PA PA $275 PA PA PA
7 Mometasone furoate (Asmanex HFA) Mometasone furoate (Asmanex Twisthaler ) Budesonide/formoterol (Symbicort ) Fluticasone/salmeterol (Advair Diskus ) Fluticasone/salmeterol (Advair HFA ) Fluticasone/salmeterol (AirDuo RespiClick ) Mometasone/formoterol (Dulera HFA) Montelukast (Singulair ) ASTHMA (CONTINUED) Inhaled Corticosteroids (Continued) 100 mcg/act, 200 mcg/act $250 PA PA PA 110 mcg, 220 mcg DPI $270 PA PA PA Inhaled Beta-2 Adrenergic Agonist/Corticosteroid mcg/act, mcg/act mcg, mcg, mcg DPI mcg/act, mcg/act, 45-21mcg/act mcg, mcg, mcg mcg/act,200-5 mcg/act 4 mg (Oral packet), 4, 5 mg (Chew), 10 mg (Tablet) $235 PA PA PA $434 PA PA PA PA $272 PA PA PA PA PA $113 PA PA PA PA $236 Leukotriene Receptor Antagonists < 12 yo $41
8 Escitalopram (Lexapro ) Fluoxetine (Prozac ) Sertraline (Zoloft ) Duloxetine (Cymbalta ) Dexmethylphenidate Immediate Release (Focalin ) Dexmethylphenidate Long-Acting (Focalin XR ) Dextroamphetamine- Amphetamine Immediate Release (Adderall ) Dextroamphetamine- Amphetamine Long- Acting (Adderall XR ) ANXIETY DISORDERS/DEPRESSION Selective Serotonin Reuptake Inhibitors 5, 10, 20 mg $17 10, 20, 40, 60 mg (capsules preferred) $16 25, 50, 100 mg $16 Serotonin-Norepinephrine Reuptake Inhibitors 20, 30, 60 mg (capsules preferred) $22 PA ATTENTION DEFICIT/HYPERACTIVITY DISORDER (ADHD) Stimulants 2.5, 5, 10 mg $53 5, 10, 15, 20, 25, 30, 35, 40 mg 5, 7.5, 10, 12.5, 15, 20, 30 mg $155 PA PA $47 5, 10, 15, 20, 25, 30 mg $86 PA
9 ATTENTION DEFICIT/HYPERACTIVITY DISORDER (ADHD) (CONTINUED) Stimulants (Continued) Lisdexamfetamine (Vyvanse ) Methylphenidate Immediate Release (Ritalin ) Methylphenidate Long-Acting (Concerta ) Methylphenidate Long- Acting (Metadate CD ) Methylphenidate Long-Acting (Ritalin LA ) Atomoxetine (Strattera ) Clonidine (Catapres ) Clonidine Extended Release (Kapvay ) Guanfacine (Tenex ) Guanfacine ER (Intuniv ) 10, 20, 30, 40, 50, 60, 70 mg $325 PA PA PA 5, 10, 20 mg $45 18, 27, 36, 54 mg $246 PA 10, 20, 30, 40, 50, 60 mg $132 PA PA 10, 60 mg $342 PA PA PA PA 20, 30, 40 mg $129 PA PA 10, 18, 25, 40, 60, 80, 100 mg Non-Stimulants $216 PA 0.1 mg, 0.2 mg, 0.3 mg $ mg $180 PA PA PA PA PA 1, 2 mg $17 1, 2, 3, 4 mg $32 PA
10 Hydrocortisone External Alclometasone (Aclovate ) Betamethasone valerate (Diprolene External) Fluocinolone acetate (Synalar ) Triamcinolone acetonide (Kenalog ) Betamethasone valerate (Diprolene External) Fluocinolone acetate (Synalar ) Fluticasone propionate (Cutivate External) Mometasone furoate (Elocon External) Triamcinolone acetonide (Kenalog ) ATOPIC DERMATITIS Class 7 Topical Corticosteroids-Least Potent 0.5%, 0.1%, 2.5% Cream and Ointment; 1% Lotion $19 Class 6 Topical Corticosteroids-Mild Potency 0.05% Cream, Ointment $92 PA PA 0.1% Lotion $ % Cream $127 PA PA PA PA PA 0.025% Cream; 0.025% Lotion $32 Class 5 Topical Corticosteroids-Lower Mid Potency 0.1% Cream, Ointment $ % Cream, Ointment 0.005% Ointment; 0.05% Cream $104 PA $40 0.1% Cream, Lotion $ % Ointment $25 Classes 1-4 topical corticosteroids are not listed since most patients are treated with classes 5-7 topical corticosteroids.
11 Insulin degludec (Tresiba ) Insulin detemir (Levemir ) Insulin glargine (Basaglar ) Insulin glargine (Lantus ) Insulin aspart protamine/insulin aspart (Novolog ) Insulin NPH/insulin regular (Humulin 70/30 ) Insulin NPH/insulin regular (Novolin 70/30 ) Diabetes Long Acting Insulin 100, 200 units/ml Flextouch pen (3mL/pen) $639 PA PA PA PA PA 100 units/ml vial $323 PA PA PA PA PA 100 units/ml Flextouch pen (3mL/pen) 100 units/ml Kwikpen (3mL/pen) $484 PA PA PA PA PA $380 PA 100 units/ml vial $307 PA PA PA PA PA 100 units/ml Solostar pen (3mL/pen) $461 PA PA PA PA PA 100 units/ml vial $ units/ml Flexpen (3mL/pen) $639 PA PA 100 units/ml vial $178 PA 100 units/ml Kwikpen (3mL/pen) Mixed Insulin $566 PA PA PA 100 units/ml vial $165 PA
12 Insulin NPH (Humulin N) Insulin NPH (Novolin N) Insulin aspart (Novolog ) Insulin glulisine (Apidra ) Insulin lispro (Humalog ) Insulin regular (Humulin R ) Insulin regular (Novolin R ) Diabetes Intermediate Acting Insulin 100 units/ml vial $178 PA 100 units/ml Kwikpen (3mL/pen) $566 PA PA PA 100 units/ml vial $165 PA Short Acting Insulin 100 units/ml vials $ units/ml Flexpen (3mL/pen) $639 PA 100 units/ml vial $306 PA PA PA 100 units/ml Solostar pen (3mL/pen) $591 PA PA PA 100 units/ml vial $ units/ml Kwikpen (3mL/pen) $636 PA 100 units/ml vial $178 PA 100 units/ml vial $165 PA
13 Famotidine (Pepcid ) Ranitidine (Zantac ) Esomeprazole (Nexium ) Lansoprazole (Prevacid ) Omeprazole (Prilosec ) GASTROESOPHAGEAL REFLUX H2 Antihistamines 10, 20, 40 mg $19 40 mg/5ml $58 75, 150, 300 mg $ mg 15 mg/ml $28 Proton Pump Inhibitors 20 mg, 40 mg $33 20 mg OTC (Nexium 24HR) PA PA PA PA PA 20 mg $20 PA PA 15 mg, 30 mg Capsules $25 PA PA 15 mg OTC (Prevacid 24HR) $22 PA PA PA 15, 30 mg Solutabs $498 PA PA PA PA PA 3 mg/ml First Lansoprazole $83 PA PA PA PA PA 10, 20, 40 mg Capsules $18 PA 2 mg/ml First Omeprazole $72 PA PA PA PA
14 Benzyl alcohol (Ulesfia ) Ivermectin lotion (Sklice ) Malathion lotion (Ovide ) Permethrin (Nix ) Pyrethrins/piperonyl butoxide (LiceMD /RID ) Spinosad suspension (Natroba ) HEAD LICE Topical Pediculocides 5% $237 PA PA PA PA PA PA 0.5% $412 PA PA PA PA 0.5% $225 PA PA 1% $ %-4% $7 PA PA 0.9% $266 PA
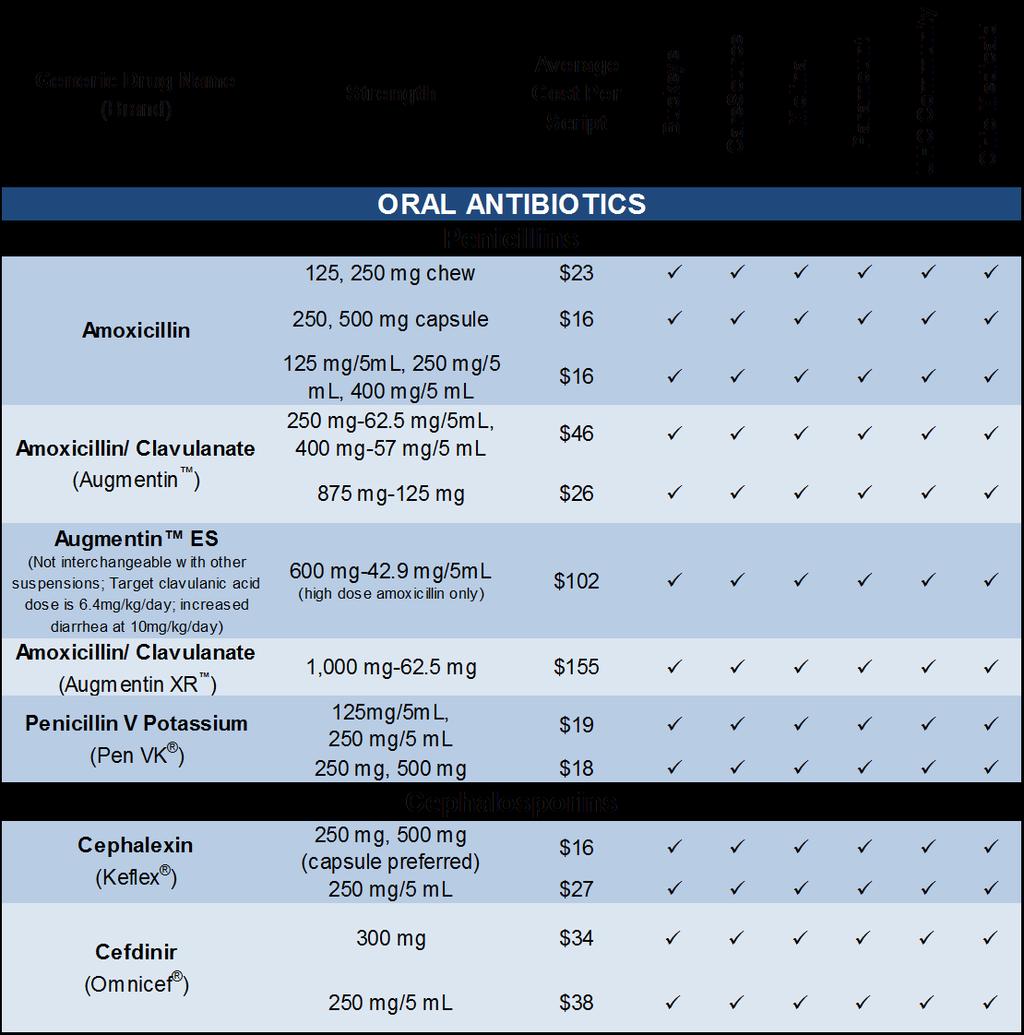
15
16 ORAL ANTIBIOTICS (CONTINUED) Fluoroquinolones Ciprofloxacin (Cipro ) Levofloxacin (Levaquin ) Azithromycin (Zithromax ) Clarithromycin (Biaxin ) Erythromycin (E.E.S., Ery-Tab ) Erythromycin Ethylsuccinate (EryPed ) Sulfamethoxazole/ Trimethoprim (Bactrim ) 250 mg, 500 mg 250 mg/5 ml, 500 mg/5ml $174 PA 250 mg, 500 mg $20 25mg/mL $105 PA PA 250 mg, 500 mg $ mg/5ml, 200 mg/5 ml 125 mg/5 ml, 250 mg/5ml $36 $ mg, 500 mg $ mg, 333 mg, 400 mg, 500 mg $303 PA 400 mg/5 ml $794 PA 400 mg-80 mg, 800 mg-160 mg $18 Macrolides Sulfonamides $ mg-40 mg/5 ml $30
17 Clindamycin (Cleocin ) Metronidazole (Flagyl ) Nitrofurantoin monohydrate Nitrofurantoin (Furadantin ) ORAL ANTIBIOTICS (CONTINUED) Miscellaneous 75 mg, 150 mg $ mg 150 mg 75 mg/5 ml $41 250, 500 mg $ mg $27 25 mg/5 ml $289
18 Ofloxacin Ciprofloxacin/ dexamethasone (Ciprodex ) Ciprofloxacin (Cetraxal ) OTIC ANTIBIOTICS Otic Anti-infectives 0.3% Floxin Otic $ % Ocuflox Opthl. $ /0.1% suspension $241 PA PA PA 0.2% solution $102 PA PA PA PA
TABLE OF CONTENTS (Click on a link below to view the section.)
") Follow the links below to access the complete formularies for Plans: Health Plan Acne Allergy Allergic Anaphylactic Reaction Allergic Conjunctivitis Allergic Rhinitis Asthma Atopic Dermatitis Behavioral
Follow the links below to access the complete formularies for Plans: Health Plan Acne Allergy Allergic Anaphylactic Reaction Allergic Conjunctivitis Allergic Rhinitis Asthma Atopic Dermatitis Behavioral
TABLE OF CONTENTS (Click on a link below to view the section.)
") Follow the links below to access the complete formularies for Plans: Health Plan Acne Allergy Allergic Anaphylactic Reaction Allergic Conjunctivitis Allergic Rhinitis Asthma Atopic Dermatitis Behavioral
Follow the links below to access the complete formularies for Plans: Health Plan Acne Allergy Allergic Anaphylactic Reaction Allergic Conjunctivitis Allergic Rhinitis Asthma Atopic Dermatitis Behavioral
TABLE OF CONTENTS (Click on a link below to view the section.)
") Follow the links below to access the complete formularies for Plans: Health Plan Acne Allergy Allergic Anaphylactic Reaction Allergic Conjunctivitis Allergic Rhinitis Asthma Atopic Dermatitis Behavioral
Follow the links below to access the complete formularies for Plans: Health Plan Acne Allergy Allergic Anaphylactic Reaction Allergic Conjunctivitis Allergic Rhinitis Asthma Atopic Dermatitis Behavioral
OHIO MEDICAID PHARMACY COVERAGE
 OHIO MEDICAID PHARMACY COVERAGE This information is intended for use by providers to help select the most appropriate cost-effective medication and formulation for their patients. Prescribers should utilize
OHIO MEDICAID PHARMACY COVERAGE This information is intended for use by providers to help select the most appropriate cost-effective medication and formulation for their patients. Prescribers should utilize
Relative Cost/Month. Less than $10. Loratadine Liquid* $10-$15 Cetirizine liquid 1mg/mL*
 Allergy Chlorpheniramine Tablet* Diphenhydramine Tablet* Diphenhydramine Liquid* Loratadine Tablet* Cetirizine Tablet* Loratadine 10mg ODT* Less than $10 Loratadine Liquid* $10-$15 Cetirizine liquid 1mg/mL*
Allergy Chlorpheniramine Tablet* Diphenhydramine Tablet* Diphenhydramine Liquid* Loratadine Tablet* Cetirizine Tablet* Loratadine 10mg ODT* Less than $10 Loratadine Liquid* $10-$15 Cetirizine liquid 1mg/mL*
Mercy Care Plan. Acyclovir Ointment. Products Affected. acyclovir ointment 5 % external Details. Criteria. Requires use of oral Acyclovir
 Acyclovir Ointment Mercy Care Plan acyclovir ointment 5 % external Requires use of oral Acyclovir 1 Adcirca ADCIRCA TABLET 20 MG ORAL Requires use of Sildenafil 2 Albenza ALBENZA TABLET 200 MG ORAL Requires
Acyclovir Ointment Mercy Care Plan acyclovir ointment 5 % external Requires use of oral Acyclovir 1 Adcirca ADCIRCA TABLET 20 MG ORAL Requires use of Sildenafil 2 Albenza ALBENZA TABLET 200 MG ORAL Requires
Aetna Better Health of Illinois Medicaid Formulary Updates
 October 2017 o DOXYLAMINE SUCCINATE 25mg-QL o DULOXETINE CAP 40MG DR-QL o GUANFACIN ER TABS (all strengths)-ql o TOBRAMYCIN NEBU SOLUTION- PA August 2017 Aetna Better Health of Illinois Medicaid 2017 Formulary
October 2017 o DOXYLAMINE SUCCINATE 25mg-QL o DULOXETINE CAP 40MG DR-QL o GUANFACIN ER TABS (all strengths)-ql o TOBRAMYCIN NEBU SOLUTION- PA August 2017 Aetna Better Health of Illinois Medicaid 2017 Formulary
Oregon Health Plan prescription benefit updates
 Oregon Health Plan prescription benefit updates EOCCO s prescription program is a pharmacy benefit that offers members a choice of safe and effective medication treatments. The program also helps you save
Oregon Health Plan prescription benefit updates EOCCO s prescription program is a pharmacy benefit that offers members a choice of safe and effective medication treatments. The program also helps you save
Alameda Alliance for Health Pharmacy & Therapeutics (P&T) Committee Decisions
 Committee Decisions") Alameda Alliance for Health FORMULARY UPDATE Effective: October 27, 2017. Drugs notated with an * have an undetermined implementation date Alameda Alliance for Health Pharmacy & Therapeutics (P&T) Committee
Alameda Alliance for Health FORMULARY UPDATE Effective: October 27, 2017. Drugs notated with an * have an undetermined implementation date Alameda Alliance for Health Pharmacy & Therapeutics (P&T) Committee
Mercy Care ALBENDAZOLE. Products Affected. ALBENZA TABLET 200 MG ORAL Details. Criteria. Refer to PA Guideline for approval criteria
 ALBENDAZOLE Mercy Care ALBENZA TABLET 200 MG ORAL Refer to PA Guideline for approval criteria 1 BRIMONIDINE-TIMOLOL COMBIGAN SOLUTION 0.2-0.5 % OPHTHALMIC Requires use of separate ingredients for at least
ALBENDAZOLE Mercy Care ALBENZA TABLET 200 MG ORAL Refer to PA Guideline for approval criteria 1 BRIMONIDINE-TIMOLOL COMBIGAN SOLUTION 0.2-0.5 % OPHTHALMIC Requires use of separate ingredients for at least
ANTINEOPLASTIC DRUGS CHAPTER 21. Antineoplastic drugs - designed to treat malignancies, now also used to treat diseases with inflammatory component
 ANTINEOPLASTIC DRUGS CHAPTER 21 Antineoplastic drugs - designed to treat malignancies, now also used to treat diseases with inflammatory component Tx of malignancies Antineoplastic drugs: methotrexate
ANTINEOPLASTIC DRUGS CHAPTER 21 Antineoplastic drugs - designed to treat malignancies, now also used to treat diseases with inflammatory component Tx of malignancies Antineoplastic drugs: methotrexate
AETNA BETTER HEALTH January 2017 Formulary Change(s)
") AETNA BETTER HEALTH January 2017 Formulary Change(s) The following updates will be made to the Aetna Better Health of MI formulary on February 1, 2017 Drug Name, Strength, Dosage Form IVERMECTIN 3 MG TABLET
AETNA BETTER HEALTH January 2017 Formulary Change(s) The following updates will be made to the Aetna Better Health of MI formulary on February 1, 2017 Drug Name, Strength, Dosage Form IVERMECTIN 3 MG TABLET
Step Therapy Medications
 Step Therapy Medications Step Therapy (ST PA ) is an automated form of prior authorization. It encourages the use of therapies that should be tried first, before other treatments are covered, based on
Step Therapy Medications Step Therapy (ST PA ) is an automated form of prior authorization. It encourages the use of therapies that should be tried first, before other treatments are covered, based on
AETNA BETTER HEALTH January 2017 Formulary Change(s)
") AETNA BETTER HEALTH January 2017 Formulary Change(s) The following updates will be made to the Aetna Better Health of MI formulary on March 1, 2017 Drug Name, Strength, Dosage Form ALFUZOSIN HCL ER 10
AETNA BETTER HEALTH January 2017 Formulary Change(s) The following updates will be made to the Aetna Better Health of MI formulary on March 1, 2017 Drug Name, Strength, Dosage Form ALFUZOSIN HCL ER 10
CLINICAL MEDICAL POLICY
 CLINICAL MEDICAL POLICY Policy Name: Xolair (omalizumab) Policy Number: MP-051-MD-DE Responsible Department(s): Medical Management; Clinical Pharmacy Provider Notice Date: 10/01/2017 Original Effective
CLINICAL MEDICAL POLICY Policy Name: Xolair (omalizumab) Policy Number: MP-051-MD-DE Responsible Department(s): Medical Management; Clinical Pharmacy Provider Notice Date: 10/01/2017 Original Effective
Step Therapy Requirements
 An Independent Licensee of the Blue Cross and Blue Shield Association Step Therapy Requirements Effective: 05/01/2018 Updated 4/2018 H0302_2_2014 CMS Accepted 05/05/2014 1 BETA-BLOCKERS BYSTOLIC 10 MG
An Independent Licensee of the Blue Cross and Blue Shield Association Step Therapy Requirements Effective: 05/01/2018 Updated 4/2018 H0302_2_2014 CMS Accepted 05/05/2014 1 BETA-BLOCKERS BYSTOLIC 10 MG
CAMPER APPLICATION PACKET
 CAMPER APPLICATION PACKET Monday- Friday June 12-16, 2017 Rockport, Texas DEADLINE FOR SUBMITTING ALL FORMS: THE IMPORTANCE OF COMPLETING ALL CAMP FORMS Although it may seem like a lot of paperwork, the
CAMPER APPLICATION PACKET Monday- Friday June 12-16, 2017 Rockport, Texas DEADLINE FOR SUBMITTING ALL FORMS: THE IMPORTANCE OF COMPLETING ALL CAMP FORMS Although it may seem like a lot of paperwork, the
Quarterly pharmacy formulary change notice
 Provider Bulletin June 2017 The formulary changes listed in the table below apply to all Anthem HealthKeepers Plus patients. These changes were reviewed and approved at the first quarter Pharmacy and Therapeutics
Provider Bulletin June 2017 The formulary changes listed in the table below apply to all Anthem HealthKeepers Plus patients. These changes were reviewed and approved at the first quarter Pharmacy and Therapeutics
Acyclovir Ointment. Aetna Better Health Pennsylvania. Products Affected. acyclovir ointment 5 % external Details. Criteria
 Medications that require Step Therapy (ST) require trial and failure of preferred formulary agents prior to their authorization. If the prerequisite medications have been filled within the specified time
Medications that require Step Therapy (ST) require trial and failure of preferred formulary agents prior to their authorization. If the prerequisite medications have been filled within the specified time
Drug Class Monograph
 Drug Class Monograph Class: Inhaled Corticosteroids Drugs: Aerospan (flunisolide), Advair Diskus, Advair HFA (fluticasone/salmeterol), Alvesco (ciclesonide), Arnuity Ellipta (fluticasone furoate), Asmanex
Drug Class Monograph Class: Inhaled Corticosteroids Drugs: Aerospan (flunisolide), Advair Diskus, Advair HFA (fluticasone/salmeterol), Alvesco (ciclesonide), Arnuity Ellipta (fluticasone furoate), Asmanex
Diagnosis and Management of Asthma
 Supporting Evidence: Diagnosis and Management of Asthma The subdivision of this section is: Appendix B Tables Copyright 2016 by 1 Eleventh Edition/December 2016 Appendix B Asthma Summary Tables Class:
Supporting Evidence: Diagnosis and Management of Asthma The subdivision of this section is: Appendix B Tables Copyright 2016 by 1 Eleventh Edition/December 2016 Appendix B Asthma Summary Tables Class:
Inhaled bronchodilators relax constricted airways and treat the noisy part of asthma: coughing, wheezing, choking and shortness of breath.
 Inhaled bronchodilators relax constricted airways and treat the noisy part of asthma: coughing, wheezing, choking and shortness of breath. AccuNeb inhalation 0.021% solution: 0.63mg/3mL 3-4 times solution
Inhaled bronchodilators relax constricted airways and treat the noisy part of asthma: coughing, wheezing, choking and shortness of breath. AccuNeb inhalation 0.021% solution: 0.63mg/3mL 3-4 times solution
Pharmacy Updates Summary
 All of the following changes were reviewed and approved by the SFHP Pharmacy & Therapeutics (P&T) Committee on 01/21/2015 Effective date: 02/21/2015 Therapeutic Classes reviewed: Allergen-Specific Immunotherapy
All of the following changes were reviewed and approved by the SFHP Pharmacy & Therapeutics (P&T) Committee on 01/21/2015 Effective date: 02/21/2015 Therapeutic Classes reviewed: Allergen-Specific Immunotherapy
Oral Agents. Formulary Limits. Available Strengths. IR: 4mg ER: 12mg Syrup: 2mg/5ml
 MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Seasonal Allergy Medications LAST REVIEW: 9/20/2016 THERAPEUTIC CLASS: Rheumatologic/Immunologic REVIEW HISTORY: 5/16, 5/15,
MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Seasonal Allergy Medications LAST REVIEW: 9/20/2016 THERAPEUTIC CLASS: Rheumatologic/Immunologic REVIEW HISTORY: 5/16, 5/15,
Clinical Policy: Dupilumab (Dupixent) Reference Number: ERX.SPA.49 Effective Date:
 Reference Number: ERX.SPA.49 Effective Date:") Clinical Policy: (Dupixent) Reference Number: ERX.SPA.49 Effective Date: 06.01.17 Last Review Date: 02.19 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Dupixent) Reference Number: ERX.SPA.49 Effective Date: 06.01.17 Last Review Date: 02.19 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Commissioner for the Department for Medicaid Services Selections for Preferred Products
 Commissioner for the Department for Medicaid Services Selections for Preferred Products This is a summary of the final Preferred Drug List (PDL) selections made by the Commissioner for the Department for
Commissioner for the Department for Medicaid Services Selections for Preferred Products This is a summary of the final Preferred Drug List (PDL) selections made by the Commissioner for the Department for
FORMULARY Revised January 2019
 MEDICATION STRENGTH NOTES ANTIMICROBIALS-ANTIBIOTICS AMOXICILLIN CAPS 500 MG AMOXICILLIN SUSP 125 MG/5 ML 250 MG/5 ML 400 MG/5 ML AMOXICILLIN CHEW 250 MG AMOXICILLIN AND CLAVULANIC ACID CAPS (AUGMENTIN)
MEDICATION STRENGTH NOTES ANTIMICROBIALS-ANTIBIOTICS AMOXICILLIN CAPS 500 MG AMOXICILLIN SUSP 125 MG/5 ML 250 MG/5 ML 400 MG/5 ML AMOXICILLIN CHEW 250 MG AMOXICILLIN AND CLAVULANIC ACID CAPS (AUGMENTIN)
Step Therapy Criteria 2019
 Step Therapy 2019 For information on obtaining an updated coverage determination or an exception to a coverage determination please call Freedom Health Member Services at 1-800-401-2740 or, for TTY/TDD
Step Therapy 2019 For information on obtaining an updated coverage determination or an exception to a coverage determination please call Freedom Health Member Services at 1-800-401-2740 or, for TTY/TDD
FORMULARY NOTES ABOUT FORMULARY AND PHARMACY
 FORMULARY NOTES ABOUT FORMULARY AND PHARMACY 1. Purposes: Assist team leaders in preparing for trips Limit the number of interchangeable drugs Limit pharmacy errors Improve efficiency and organization
FORMULARY NOTES ABOUT FORMULARY AND PHARMACY 1. Purposes: Assist team leaders in preparing for trips Limit the number of interchangeable drugs Limit pharmacy errors Improve efficiency and organization
Oral Agents. Fml Limits. Available Strengths NF NF
 MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Allergy Medications LAST REVIEW: 9/12/2017 THERAPEUTIC CLASS: Rheumatologic/Immunologic REVIEW HISTORY: 9/16, 5/15, 9/14
MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Allergy Medications LAST REVIEW: 9/12/2017 THERAPEUTIC CLASS: Rheumatologic/Immunologic REVIEW HISTORY: 9/16, 5/15, 9/14
Inhaled Corticosteroids Drug Class Prior Authorization Protocol
 Inhaled Corticosteroids Drug Class Prior Authorization Protocol Line of Business: Medi-Cal P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
Inhaled Corticosteroids Drug Class Prior Authorization Protocol Line of Business: Medi-Cal P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
MEDICAL ASSISTANCE BULLETIN
 ISSUE DATE SUBJECT EFFECTIVE DATE January 20, 2016 MEDICAL ASSISTANCE BULLETIN NUMBER *See Below BY Drug List (PDL) Update January 20, 2016 Pharmacy Services Leesa M. Allen, Deputy Secretary Office of
ISSUE DATE SUBJECT EFFECTIVE DATE January 20, 2016 MEDICAL ASSISTANCE BULLETIN NUMBER *See Below BY Drug List (PDL) Update January 20, 2016 Pharmacy Services Leesa M. Allen, Deputy Secretary Office of
Inhaled Corticosteroids Drug Class Prior Authorization Protocol
 Inhaled Corticosteroids Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
Inhaled Corticosteroids Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
WellCare s South Carolina Preferred Drug List Update
 WellCare s South Carolina Preferred Drug List Update This is a list of changes to our preferred drug list. These are a result of the latest WellCare Pharmacy & Therapeutics meeting held on 09/03/2015.
WellCare s South Carolina Preferred Drug List Update This is a list of changes to our preferred drug list. These are a result of the latest WellCare Pharmacy & Therapeutics meeting held on 09/03/2015.
Allergies and Asthma 5/21/2013. Objectives. Allergic Rhinitis (AR): Risk Factor for ASTHMA. Rhinitis and Asthma
: Risk Factor for ASTHMA. Rhinitis and Asthma") Allergies and Asthma Presented By: Dr. Fadwa Gillanders, Pharm.D Clinical Pharmacy Specialist May 2013 Objectives Understand the relationship between asthma and allergic rhinitis Understand what is going
Allergies and Asthma Presented By: Dr. Fadwa Gillanders, Pharm.D Clinical Pharmacy Specialist May 2013 Objectives Understand the relationship between asthma and allergic rhinitis Understand what is going
UWSP Student Health Service Pharmacy Formulary 1/22/2015
 UWSP Student Health Service Pharmacy Formulary 1/22/2015 UWSP Student Health Service Pharmacy Formulary 1/22/2015 Medication Name Strength DosageForm Route Acetaminophen 325 MG Tablet Oral Acetaminophen-Codeine
UWSP Student Health Service Pharmacy Formulary 1/22/2015 UWSP Student Health Service Pharmacy Formulary 1/22/2015 Medication Name Strength DosageForm Route Acetaminophen 325 MG Tablet Oral Acetaminophen-Codeine
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Dupixent) Reference Number: CP.PHAR.336 Effective Date: 05.01.17 Last Review Date: 02.19 Line of Business: Commercial, HIM, Medicaid Coding Implications Revision Log See Important Reminder
Clinical Policy: (Dupixent) Reference Number: CP.PHAR.336 Effective Date: 05.01.17 Last Review Date: 02.19 Line of Business: Commercial, HIM, Medicaid Coding Implications Revision Log See Important Reminder
FORMULARY Revised January 2018 NOTES ABOUT FORMULARY AND PHARMACY
 FORMULARY Revised NOTES ABOUT FORMULARY AND PHARMACY 1. Purposes: Assist team leaders in preparing for trips Limit the number of interchangeable drugs Limit pharmacy errors Improve efficiency and organization
FORMULARY Revised NOTES ABOUT FORMULARY AND PHARMACY 1. Purposes: Assist team leaders in preparing for trips Limit the number of interchangeable drugs Limit pharmacy errors Improve efficiency and organization
SmithRx Standard Formulary Step Therapy List
 SmithRx Standard Formulary Step Therapy List Revised: January 27, 2017 The following medications require prior use of at least one other medication for coverage. Please note that any plan-specific customizations
SmithRx Standard Formulary Step Therapy List Revised: January 27, 2017 The following medications require prior use of at least one other medication for coverage. Please note that any plan-specific customizations
Quarterly pharmacy formulary change notice
 Quarterly pharmacy formulary change notice The formulary changes listed in the table below were reviewed and approved at our second quarter 2018 Pharmacy and Therapeutics Committee meeting. Effective October
Quarterly pharmacy formulary change notice The formulary changes listed in the table below were reviewed and approved at our second quarter 2018 Pharmacy and Therapeutics Committee meeting. Effective October
Key features and changes to these four components of asthma care include:
 Guidelines for the Diagnosis and Management of Asthma in Adults Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions regarding
Guidelines for the Diagnosis and Management of Asthma in Adults Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions regarding
Inhaled Corticosteroid Dose Comparison in Asthma
 This Clinical Resource gives subscribers additional insight related to the Recommendations published in April 2017 ~ Resource #330402 Inhaled Corticosteroid Dose Comparison in Asthma The chart below provides
This Clinical Resource gives subscribers additional insight related to the Recommendations published in April 2017 ~ Resource #330402 Inhaled Corticosteroid Dose Comparison in Asthma The chart below provides
Pharmacy Updates Summary
 All of the following changes were reviewed and approved by the SFHP Pharmacy & Therapeutics (P&T) Committee on 4/16/2014 Effective date: 5/15/2014 Therapeutic Classes reviewed: ADHD Ophthalmic antihistamines
All of the following changes were reviewed and approved by the SFHP Pharmacy & Therapeutics (P&T) Committee on 4/16/2014 Effective date: 5/15/2014 Therapeutic Classes reviewed: ADHD Ophthalmic antihistamines
Drug List exclusions for Blue Cross commercial plans
 Drug List exclusions for Blue Cross commercial plans The drugs shown below aren t covered on the commercial Blue Cross Blue Shield of Michigan drug lists. In most cases, if you fill a prescription for
Drug List exclusions for Blue Cross commercial plans The drugs shown below aren t covered on the commercial Blue Cross Blue Shield of Michigan drug lists. In most cases, if you fill a prescription for
Quarterly pharmacy formulary change notice
 Provider Bulletin October 2018 Quarterly pharmacy formulary change notice The formulary changes listed in the table below apply to all Anthem HealthKeepers Plus patients. The changes listed in the table
Provider Bulletin October 2018 Quarterly pharmacy formulary change notice The formulary changes listed in the table below apply to all Anthem HealthKeepers Plus patients. The changes listed in the table
Triage Information: 1. Duration of HPSJ Membership 2. Age 3. Fill history of Seasonal Allergy Medications
 MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Seasonal Allergy Medications LAST REVIEW: 5/28/2015 THERAPEUTIC CLASS: Rheumatologic/Immunologic REVIEW HISTORY: 5/15, 9/14
MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Seasonal Allergy Medications LAST REVIEW: 5/28/2015 THERAPEUTIC CLASS: Rheumatologic/Immunologic REVIEW HISTORY: 5/15, 9/14
Clinical Policy: Omalizumab (Xolair) Reference Number: ERX.SPA.141 Effective Date: Last Review Date: 08.17
 Reference Number: ERX.SPA.141 Effective Date: Last Review Date: 08.17") Clinical Policy: (Xolair) Reference Number: ERX.SPA.141 Effective Date: 03.01.14 Last Review Date: 08.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Xolair) Reference Number: ERX.SPA.141 Effective Date: 03.01.14 Last Review Date: 08.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
ALLERGIC RHINITIS-NASAL
 ALLERGIC RHINITIS-NASAL FLUNISOLIDE Patient needs to have paid claims for any one of the following Step 1 drugs: NasaCort OTC, fluticasone Rx, fluticasone OTC, Budesonide OTC. Prior to filling the Step
ALLERGIC RHINITIS-NASAL FLUNISOLIDE Patient needs to have paid claims for any one of the following Step 1 drugs: NasaCort OTC, fluticasone Rx, fluticasone OTC, Budesonide OTC. Prior to filling the Step
Step Therapy Requirements
 An Independent Licensee of the Blue Cross and Blue Shield Association Step Therapy Requirements Effective: 12/01/2017 Updated 11/2017 H0302_2_2014 CMS Accepted 05/05/2014 1 ABILIFY Abilify 10 mg tablet
An Independent Licensee of the Blue Cross and Blue Shield Association Step Therapy Requirements Effective: 12/01/2017 Updated 11/2017 H0302_2_2014 CMS Accepted 05/05/2014 1 ABILIFY Abilify 10 mg tablet
Quarterly pharmacy formulary change notice
 MEDICAID PROVIDER BULLETIN October 2018 The formulary changes listed in the table below were reviewed and approved at the second-quarter 2018 Pharmacy and Therapeutics Committee meeting. Effective October
MEDICAID PROVIDER BULLETIN October 2018 The formulary changes listed in the table below were reviewed and approved at the second-quarter 2018 Pharmacy and Therapeutics Committee meeting. Effective October
Amitriptyline Hydrochloride Heart Health & BP Amlodipine Besylate 5mg Norvasc Antibiotics Amoxicillin 500 mg Amoxil
 School Corp Formulary Antiviral Acyclovir 400mg Zovirax Asthma Advair Diskus Diskus 250/50 Fluticasone/Salmeterol Asthma Albuterol Sulfate 2.5 mg/3 ml Proventil Arthritis and Pain Allendronate Sodium 70
School Corp Formulary Antiviral Acyclovir 400mg Zovirax Asthma Advair Diskus Diskus 250/50 Fluticasone/Salmeterol Asthma Albuterol Sulfate 2.5 mg/3 ml Proventil Arthritis and Pain Allendronate Sodium 70
Amitriptyline Hydrochloride Heart Health & BP Amlodipine Besylate 5mg Norvasc Antibiotics Amoxicillin 500 mg Amoxil
 Antiviral Acyclovir 400mg Zovirax Asthma Advair Diskus Diskus 250/50 Fluticasone/Salmeterol Asthma Albuterol Sulfate 2.5 mg/3 ml Proventil Arthritis and Pain Allendronate Sodium 70 mg Fosamax Arthritis
Antiviral Acyclovir 400mg Zovirax Asthma Advair Diskus Diskus 250/50 Fluticasone/Salmeterol Asthma Albuterol Sulfate 2.5 mg/3 ml Proventil Arthritis and Pain Allendronate Sodium 70 mg Fosamax Arthritis
Step Therapy Criteria (Criteria for Step Therapy-2 [ST-2] Drugs)
![Step Therapy Criteria (Criteria for Step Therapy-2 [ST-2] Drugs)](/thumbs/85/91743011.jpg "Step Therapy Criteria (Criteria for Step Therapy-2 [ST-2] Drugs)") CareAdvantage CMC 2018 Formulary Supplement II (List of Covered Drugs) Step Therapy Criteria (Criteria for Step Therapy-2 [ST-2] Drugs) Formulary ID: 00018157 Formulary Version:11 19 CMS Approved: 08/21/2018
CareAdvantage CMC 2018 Formulary Supplement II (List of Covered Drugs) Step Therapy Criteria (Criteria for Step Therapy-2 [ST-2] Drugs) Formulary ID: 00018157 Formulary Version:11 19 CMS Approved: 08/21/2018
ARBS MEDICATION(S) SUBJECT TO STEP THERAPY DIOVAN HCT MG TAB, DIOVAN HCT MG TABLET
 SUBJECT TO STEP THERAPY DIOVAN HCT MG TAB, DIOVAN HCT MG TABLET") ARBS DIOVAN HCT 160-12.5 MG TAB, DIOVAN HCT 80-12.5 MG TABLET 30-day trial of a Step 1 drug in the previous 120 days is required. Step 1 Drugs: Losartan, Losartan/HCTZ PAGE 1 LAST UPDATED 05/2016 BILE
ARBS DIOVAN HCT 160-12.5 MG TAB, DIOVAN HCT 80-12.5 MG TABLET 30-day trial of a Step 1 drug in the previous 120 days is required. Step 1 Drugs: Losartan, Losartan/HCTZ PAGE 1 LAST UPDATED 05/2016 BILE
Kentucky Medicaid will incorporate the following changes to its PDL on June 11, 2014:
 Fee-For-Service Pharmacy Provider Notice #179 April Pharmacy Updates May 22, 2014 11013 W. Broad Street Glen Allen, VA 23060 Dear Kentucky Medicaid Provider: Please be advised that the Department for Medicaid
Fee-For-Service Pharmacy Provider Notice #179 April Pharmacy Updates May 22, 2014 11013 W. Broad Street Glen Allen, VA 23060 Dear Kentucky Medicaid Provider: Please be advised that the Department for Medicaid
Behavioral Health. Behavioral Health. Prescribing Guidelines
 Behavioral Health Behavioral Health Prescribing Guidelines Attention Deficit/Hyperactivity Disorder (ADHD) Start with a first line medication, either from the methylphenidate or dextroamphetamine-amphetamine
Behavioral Health Behavioral Health Prescribing Guidelines Attention Deficit/Hyperactivity Disorder (ADHD) Start with a first line medication, either from the methylphenidate or dextroamphetamine-amphetamine
PHARMA-MEDIC SERVICES INC. POLICY MANUAL
 PHARMA-MEDIC SERVICES INC. POLICY MANUAL SUBJECT: INDEX: P.5.a.iii Automatic-Therapeutic Substitution DATE: June 1/2011 REVISED: March 2, 2015., Feb 2017. PROCEDURE: 1. Long term care homes use the Manitoba
PHARMA-MEDIC SERVICES INC. POLICY MANUAL SUBJECT: INDEX: P.5.a.iii Automatic-Therapeutic Substitution DATE: June 1/2011 REVISED: March 2, 2015., Feb 2017. PROCEDURE: 1. Long term care homes use the Manitoba
Adapted from: Best Practices for Medication Management for Children & Adolescents in Foster Care. October 2015
 Adapted from: Best Practices for Medication Management for Children & Adolescents in Foster Care October 2015 Psychotropic Medications Key Information Purpose: This document is designed for any reader
Adapted from: Best Practices for Medication Management for Children & Adolescents in Foster Care October 2015 Psychotropic Medications Key Information Purpose: This document is designed for any reader
Calgary Long Term Care Formulary
 Page 1 of 14 Calgary Long Term Care Formulary Pharmacy & Therapeutics Highlights https://www.albertahealthservices.ca/info/page4071.aspx Page 2 of 14 Contents... 3 Formulary Changes (Additions, Changes,
Page 1 of 14 Calgary Long Term Care Formulary Pharmacy & Therapeutics Highlights https://www.albertahealthservices.ca/info/page4071.aspx Page 2 of 14 Contents... 3 Formulary Changes (Additions, Changes,
Big Lots Behavioral Health. Prescribing Guidelines for Behavioral Health
 Big Lots Behavioral Health Prescribing Guidelines for Behavioral Health Prescribing for Behavioral Health This document was developed by Nationwide Children s Hospital in conjunction with Partners For
Big Lots Behavioral Health Prescribing Guidelines for Behavioral Health Prescribing for Behavioral Health This document was developed by Nationwide Children s Hospital in conjunction with Partners For
APPENDIX 1 Printable point-of-care tables Asthma Action Plan Yellow Zone Formulation Table Region: Europe
 APPENDIX 1 Printable point-of-care tables Asthma Action Plan Yellow Zone Formulation Table Region: Europe Instructions: Print on 8.5 x14 (216 x 279 mm) paper (Legal size) Medication in Green Zone Change
APPENDIX 1 Printable point-of-care tables Asthma Action Plan Yellow Zone Formulation Table Region: Europe Instructions: Print on 8.5 x14 (216 x 279 mm) paper (Legal size) Medication in Green Zone Change
UPDATE WellCare s South Carolina
 September 3, 2015 UPDATE WellCare s South Carolina Preferred Drug List Dear Provider: At the September 3, 2015 WellCare Pharmacy & Therapeutics Committee meeting, it was decided that the following changes
September 3, 2015 UPDATE WellCare s South Carolina Preferred Drug List Dear Provider: At the September 3, 2015 WellCare Pharmacy & Therapeutics Committee meeting, it was decided that the following changes
Updates to your prescription benefits
 Updates to your prescription benefits Effective Jan. 1, 2018 Update Summary Within the Prescription Drug List (PDL), medications are grouped by tier. The tier indicates the amount you pay when you fill
Updates to your prescription benefits Effective Jan. 1, 2018 Update Summary Within the Prescription Drug List (PDL), medications are grouped by tier. The tier indicates the amount you pay when you fill
JULY 2017 ADDITIONS. NP Thyroid 120mg NP Thyroid 15mg JUNE 2017 CHANGES
 APRIL 2017 Ivermectin, Pin-X and Reeses (Pyrantel Pamoate) Selzentry 25mg and 75mg tablets Linzess 72 mcg capsule-with QLL Levalbuterol Tartrate Inhal Aerosol (Generic Xopenex HFA) with ST & QLL Jentadueto
APRIL 2017 Ivermectin, Pin-X and Reeses (Pyrantel Pamoate) Selzentry 25mg and 75mg tablets Linzess 72 mcg capsule-with QLL Levalbuterol Tartrate Inhal Aerosol (Generic Xopenex HFA) with ST & QLL Jentadueto
Secretary for Health and Family Services Selections for Preferred Products
 Secretary for Health and Family Services Selections for Preferred Products This is a summary of the final Preferred Drug List (PDL) selections made by the Secretary for Health and Family Services based
Secretary for Health and Family Services Selections for Preferred Products This is a summary of the final Preferred Drug List (PDL) selections made by the Secretary for Health and Family Services based
Berkshire Allergy & Asthma Center 2210 Ridgewood Road, Suite 100 Wyomissing, PA (610)
") Berkshire Allergy & Asthma Center 2210 Ridgewood Road, Suite 100 Wyomissing, PA 19610 (610) 372-0502 It is with pleasure that we welcome you as a new patient to Berkshire Allergy & Asthma Center, a division
Berkshire Allergy & Asthma Center 2210 Ridgewood Road, Suite 100 Wyomissing, PA 19610 (610) 372-0502 It is with pleasure that we welcome you as a new patient to Berkshire Allergy & Asthma Center, a division
TRELEGY ELLIPTA (fluticasone-umeclidinium-vilanterol) aerosol powder
 aerosol powder") TRELEGY ELLIPTA (fluticasone-umeclidinium-vilanterol) aerosol powder Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
TRELEGY ELLIPTA (fluticasone-umeclidinium-vilanterol) aerosol powder Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
Calgary Long Term Care Formulary
 Page 1 of 10 Calgary Long Term Care Formulary Pharmacy & Therapeutics November 2018 Highlights https://www.albertahealthservices.ca/info/page4071.aspx Page 2 of 10 Contents November 2018... 3 Formulary
Page 1 of 10 Calgary Long Term Care Formulary Pharmacy & Therapeutics November 2018 Highlights https://www.albertahealthservices.ca/info/page4071.aspx Page 2 of 10 Contents November 2018... 3 Formulary
Clinical Policy: Omalizumab (Xolair) Reference Number: ERX.SPA.141 Effective Date:
 Reference Number: ERX.SPA.141 Effective Date:") Clinical Policy: (Xolair) Reference Number: ERX.SPA.141 Effective Date: 03.01.14 Last Review Date: 02.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Xolair) Reference Number: ERX.SPA.141 Effective Date: 03.01.14 Last Review Date: 02.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Big Lots Behavioral Health. Prescribing Guidelines for Behavioral Health
 Big Lots Behavioral Health Prescribing Guidelines for Behavioral Health Prescribing for Behavioral Health This document was developed by Nationwide Children s Hospital in conjunction with Partners For
Big Lots Behavioral Health Prescribing Guidelines for Behavioral Health Prescribing for Behavioral Health This document was developed by Nationwide Children s Hospital in conjunction with Partners For
Removed from formulary. Removed from formulary. Added to formulary. Quanitity limit changed. Removed from formulary. Removed from formulary
 AETNA BETTER HEALTH October 2017 Formulary Change(s) The following updates will be made to the Aetna Better Health of MI formulary on October 1, 2017 MIDAZOLAM HCL 5MG/ML VIAL MIDAZOLAM HCL 10 MG/2 ML
AETNA BETTER HEALTH October 2017 Formulary Change(s) The following updates will be made to the Aetna Better Health of MI formulary on October 1, 2017 MIDAZOLAM HCL 5MG/ML VIAL MIDAZOLAM HCL 10 MG/2 ML
Date: October 3, 2017 To: Participating Providers From: YourCare Health Plan Provider Relations Subject: 2018 Formulary Changes
 Date: October 3, 2017 To: Participating Providers From: YourCare Health Plan Provider Relations Subject: 2018 Formulary Changes 2018 Formulary-UM Changes What does this mean now, and for 2018? A number
Date: October 3, 2017 To: Participating Providers From: YourCare Health Plan Provider Relations Subject: 2018 Formulary Changes 2018 Formulary-UM Changes What does this mean now, and for 2018? A number
A Brief Overview of Psychiatric Pharmacotherapy. Joel V. Oberstar, M.D. Chief Executive Officer
 A Brief Overview of Psychiatric Pharmacotherapy Joel V. Oberstar, M.D. Chief Executive Officer Disclosures Some medications discussed are not approved by the FDA for use in the population discussed/described.
A Brief Overview of Psychiatric Pharmacotherapy Joel V. Oberstar, M.D. Chief Executive Officer Disclosures Some medications discussed are not approved by the FDA for use in the population discussed/described.
UWSP Student Health Service Pharmacy Formulary updated: 1/2017
 UWSP Student Health Service Pharmacy Formulary updated: 1/2017 Medication Name Strength DosageForm Route Acetaminophen 325 MG Tablet Oral Acetaminophen-Codeine #2 300-15 MG Tablet Oral Acetaminophen-Codeine
UWSP Student Health Service Pharmacy Formulary updated: 1/2017 Medication Name Strength DosageForm Route Acetaminophen 325 MG Tablet Oral Acetaminophen-Codeine #2 300-15 MG Tablet Oral Acetaminophen-Codeine
Data Class: Internal. 1 inhaler (30 blisters OR 14 blisters institutional pack) per presciption
 per presciption") To help make the use of prescription drugs safer and more affordable, our plan is now using a Drug Quantity Management program. That is, for certain medications, you can receive an amount to last you a
To help make the use of prescription drugs safer and more affordable, our plan is now using a Drug Quantity Management program. That is, for certain medications, you can receive an amount to last you a
Alprazolam 0.25mg, 0.5mg, 1mg tablets
 Presbyterian Senior Care (HMO) / Presbyterian MediCare PPO Quantity Limits Effective November 1, 2014 For the most recent list of drugs or other questions, please contact the Presbyterian Customer Service
Presbyterian Senior Care (HMO) / Presbyterian MediCare PPO Quantity Limits Effective November 1, 2014 For the most recent list of drugs or other questions, please contact the Presbyterian Customer Service
Step Therapy Requirements. Effective: 12/01/2016
 Effective: 12/01/2016 H2986_PD_049 Updated 11/2016 ALPHA 1-PROTEINASE INHIBITOR GLASSIA PRIOR CLAIM FOR ARALAST NP OR ZEMAIRA WITHIN THE PAST 120 DAYS. ANALGESICS, NARCOTICS KADIAN MORPHINE SULFATE ER
Effective: 12/01/2016 H2986_PD_049 Updated 11/2016 ALPHA 1-PROTEINASE INHIBITOR GLASSIA PRIOR CLAIM FOR ARALAST NP OR ZEMAIRA WITHIN THE PAST 120 DAYS. ANALGESICS, NARCOTICS KADIAN MORPHINE SULFATE ER
Quarterly pharmacy formulary change notice
 Quarterly pharmacy formulary change notice Summary of change: The Pharmacy and Therapeutics Committee (P&T) reviewed and approved the formulary changes listed in the table below on March 29, 2016. What
Quarterly pharmacy formulary change notice Summary of change: The Pharmacy and Therapeutics Committee (P&T) reviewed and approved the formulary changes listed in the table below on March 29, 2016. What
Step Therapy Requirements. Effective: 05/01/2018
 Step Therapy Requirements Effective: 05/01/2018 ANTIDEPRESSANTS TRINTELLIX 10 MG TABLET TRINTELLIX 20 MG TABLET TRINTELLIX 5 MG TABLET VIIBRYD 10 MG (7)-20 MG (23) TABLETS IN A DOSE PACK VIIBRYD 10 MG
Step Therapy Requirements Effective: 05/01/2018 ANTIDEPRESSANTS TRINTELLIX 10 MG TABLET TRINTELLIX 20 MG TABLET TRINTELLIX 5 MG TABLET VIIBRYD 10 MG (7)-20 MG (23) TABLETS IN A DOSE PACK VIIBRYD 10 MG
Effective for all members on August 1, 2017
 August 2017 Pharmacy Formulary Change Notice BlueChoice HealthPlan Medicaid is here to help you stay on top of your health care. We want to tell you about some upcoming changes to your Preferred Drug List
August 2017 Pharmacy Formulary Change Notice BlueChoice HealthPlan Medicaid is here to help you stay on top of your health care. We want to tell you about some upcoming changes to your Preferred Drug List
ADHD Medications Table
 Stimulants are the first line treatment of choice for ADHD followed by Non-Stimulants, then off-label medications. We are providing this list of medications so that you can be familiar with the common
Stimulants are the first line treatment of choice for ADHD followed by Non-Stimulants, then off-label medications. We are providing this list of medications so that you can be familiar with the common
University System of Georgia Prior Authorization, Step Therapy and Quantity Limit List (Updated 1/1/2016)
") University System of Georgia, Step Therapy and Quantity Limit List (Updated 1/1/2016) (PA) Your doctor will need to obtain a prior authorization for the drugs listed below, before your prescription drug
University System of Georgia, Step Therapy and Quantity Limit List (Updated 1/1/2016) (PA) Your doctor will need to obtain a prior authorization for the drugs listed below, before your prescription drug
Pain Oral-Intranasal Fentanyl (Abstral, Actiq, Fentora, Lazanda, Onsolis, Subsys)
") Pennsylvania Employees Benefit Trust Fund (PEBTF) and n- Medicare Eligible Retired Employees Health Program (REHP), Step Therapy and Quantity Limit List Your doctor needs to get prior authorization for
Pennsylvania Employees Benefit Trust Fund (PEBTF) and n- Medicare Eligible Retired Employees Health Program (REHP), Step Therapy and Quantity Limit List Your doctor needs to get prior authorization for
Upper Peninsula Health Plan Advantage (HMO) (List of Covered Drugs)
 (List of Covered Drugs)") Analgesics Opioid Analgesics, Long-acting fentanyl 100 mcg/hr patch td72 morphine sulfate 30 mg tablet er Opioid Analgesics, Short-acting fentanyl citrate 200 mcg lozenge hd hydrocodone/acetaminophen 5
Analgesics Opioid Analgesics, Long-acting fentanyl 100 mcg/hr patch td72 morphine sulfate 30 mg tablet er Opioid Analgesics, Short-acting fentanyl citrate 200 mcg lozenge hd hydrocodone/acetaminophen 5
Attention: Behavioral Health Providers, Pharmacists and Prescribers N.C. Medicaid and N.C. Health Choice Preferred Drug List Changes - UPDATE
 Attention: Behavioral Health Providers, Pharmacists and Prescribers N.C. Medicaid and N.C. Health Choice Drug List Changes - UPDATE Note: This article was previously published in the December 2014 Medicaid
Attention: Behavioral Health Providers, Pharmacists and Prescribers N.C. Medicaid and N.C. Health Choice Drug List Changes - UPDATE Note: This article was previously published in the December 2014 Medicaid
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Fasenra) Reference Number: CP.PHAR.## Effective Date: 01.16.18 Last Review Date: 05.18 Line of Business: Commercial, Medicaid Revision Log See Important Reminder at the end of this policy
Clinical Policy: (Fasenra) Reference Number: CP.PHAR.## Effective Date: 01.16.18 Last Review Date: 05.18 Line of Business: Commercial, Medicaid Revision Log See Important Reminder at the end of this policy
MEDICAL ASSISTANCE BULLETIN
 ISSUE DATE February 18, 2015 SUBJECT EFFECTIVE DATE January 21, 2015 MEDICAL ASSISTANCE BULLETIN NUMBER *See below BY Drug List (PDL) Update January 21, 2015 Pharmacy Services Vincent D. Gordon, Deputy
ISSUE DATE February 18, 2015 SUBJECT EFFECTIVE DATE January 21, 2015 MEDICAL ASSISTANCE BULLETIN NUMBER *See below BY Drug List (PDL) Update January 21, 2015 Pharmacy Services Vincent D. Gordon, Deputy
Aetna Better Health of Michigan 1333 Gratiot Avenue, Suite 400 Detroit, MI AETNA BETTER HEALTH January 2017 Formulary Change(s)
") AETNA BETTER HEALTH January 2017 Formulary Change(s) The following updates will be made to the Aetna Better Health of MI formulary on July 1, 2017 ADAPALENE 0.1% CREAM ADAPALENE 0.1% GEL ATORVASTATIN 10
AETNA BETTER HEALTH January 2017 Formulary Change(s) The following updates will be made to the Aetna Better Health of MI formulary on July 1, 2017 ADAPALENE 0.1% CREAM ADAPALENE 0.1% GEL ATORVASTATIN 10
CRITERIA Trial of two generic formulary products from the following: atomoxetine or ADHD stimulant medication.
 ADHD STIMULANTS ATOMOXETINE HCL, DEXEDRINE 10 MG TABLET, DEXEDRINE 5 MG TABLET, DEXMETHYLPHENIDATE HCL, DEXMETHYLPHENIDATE HCL ER, DEXTROAMPHETAMINE 10 MG TAB, DEXTROAMPHETAMINE 5 MG TAB, DEXTROAMPHETAMINE
ADHD STIMULANTS ATOMOXETINE HCL, DEXEDRINE 10 MG TABLET, DEXEDRINE 5 MG TABLET, DEXMETHYLPHENIDATE HCL, DEXMETHYLPHENIDATE HCL ER, DEXTROAMPHETAMINE 10 MG TAB, DEXTROAMPHETAMINE 5 MG TAB, DEXTROAMPHETAMINE
Amerigroup Washington, Inc. to conduct postservice reviews of certain modifiers and services
 Provider News Bulletin Amerigroup Washington, Inc. https://providers.amerigroup.com/ Medicaid providers: 1-800-454-3730 Medicare providers: 1-866-805-4589 December 2017 Table of Contents Special Announcement:
Provider News Bulletin Amerigroup Washington, Inc. https://providers.amerigroup.com/ Medicaid providers: 1-800-454-3730 Medicare providers: 1-866-805-4589 December 2017 Table of Contents Special Announcement:
Parents Guide to ADHD Medications. Copyright Child Mind Institute
 Copyright 2017. Child Mind Institute Children with attention-deficit hyperactivity disorder (ADHD) find it unusually difficult to concentrate on tasks, to pay attention, to sit still and to control impulsive
Copyright 2017. Child Mind Institute Children with attention-deficit hyperactivity disorder (ADHD) find it unusually difficult to concentrate on tasks, to pay attention, to sit still and to control impulsive
Medication Policy Manual. Topic: Dupixent, dupilumab Date of Origin: March 10, Committee Approval: March 10, 2017 Next Review Date: May 2018
 Independent licensees of the Blue Cross and Blue Shield Association Medication Policy Manual Policy No: dru493 Topic: Dupixent, dupilumab Date of Origin: March 10, 2017 Committee Approval: March 10, 2017
Independent licensees of the Blue Cross and Blue Shield Association Medication Policy Manual Policy No: dru493 Topic: Dupixent, dupilumab Date of Origin: March 10, 2017 Committee Approval: March 10, 2017
THERAPEUTIC AREA NAME STRENGTH DOSAGE FORM
 Value Based Tier Drugs are selected for the management of Asthma, Diabetes, Hypertension and Hyperlipidemia. These drugs are covered at no charge or at a reduced cost share. Medications are under continual
Value Based Tier Drugs are selected for the management of Asthma, Diabetes, Hypertension and Hyperlipidemia. These drugs are covered at no charge or at a reduced cost share. Medications are under continual
Clinical Policy: Dupilumab (Dupixent) Reference Number: ERX.SPA.49 Effective Date:
 Reference Number: ERX.SPA.49 Effective Date:") Clinical Policy: (Dupixent) Reference Number: ERX.SPA.49 Effective Date: 06.01.17 Last Review Date: 02.19 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Dupixent) Reference Number: ERX.SPA.49 Effective Date: 06.01.17 Last Review Date: 02.19 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
A Visual Approach to Simplifying Respiratory Drug Regimens
 A Visual Approach to Simplifying Respiratory Drug Regimens Stephanie Cheng, PharmD, MPH, BCGP 3 Main Categories Inhaled Respiratory Drugs Binds to beta-2 receptors Relaxation of smooth muscles in the lung
A Visual Approach to Simplifying Respiratory Drug Regimens Stephanie Cheng, PharmD, MPH, BCGP 3 Main Categories Inhaled Respiratory Drugs Binds to beta-2 receptors Relaxation of smooth muscles in the lung
2015 Step Therapy Prior Authorization Medical Necessity Guidelines
 Tufts Health Unify 2015 Step Therapy Prior Authorization Medical Necessity Guidelines Effective: 01/01/2015 Updated: 10/01/2015 Tufts Health Plan P.O. Box 9194 Watertown, MA 02471-9194 Phone: 855-393-3154
Tufts Health Unify 2015 Step Therapy Prior Authorization Medical Necessity Guidelines Effective: 01/01/2015 Updated: 10/01/2015 Tufts Health Plan P.O. Box 9194 Watertown, MA 02471-9194 Phone: 855-393-3154
THERAPEUTIC AREA NAME STRENGTH DOSAGE FORM
 Value Based Tier Drugs are selected for the management of Asthma, Diabetes, Hypertension and Hyperlipidemia. These drugs are covered at no charge or at a reduced cost share. Medications are under continual
Value Based Tier Drugs are selected for the management of Asthma, Diabetes, Hypertension and Hyperlipidemia. These drugs are covered at no charge or at a reduced cost share. Medications are under continual