MTF Quarterly Webcast September 9, CDR Joe Lawrence Director, DoD Pharmacoeconomic Center
|
|
|
- Oscar Lane
- 5 years ago
- Views:
Transcription
1 MTF Quarterly Webcast September 9, 2011 CDR Joe Lawrence Director, DoD Pharmacoeconomic Center

2 Greetings from the PEC Purpose of the Quarterly MTF Webcast DCO Ground Rules Type questions into the DCO system Put on mute, not on hold Contingency plan if DCO system quits working 2
")
 Overview of August 2011 P&T")
3 Introduction MTF Corner: Tallman Lettering in CHCS (LTC Carrillo) Review of May 2011 P&T Meeting (Dr Meade) Overview of August 2011 P&T Meeting (Dr Meade) 3

4 LTC Jorge D. Carrillo, PharmD, MS, BCPS Manager, Army Patient Safety Center
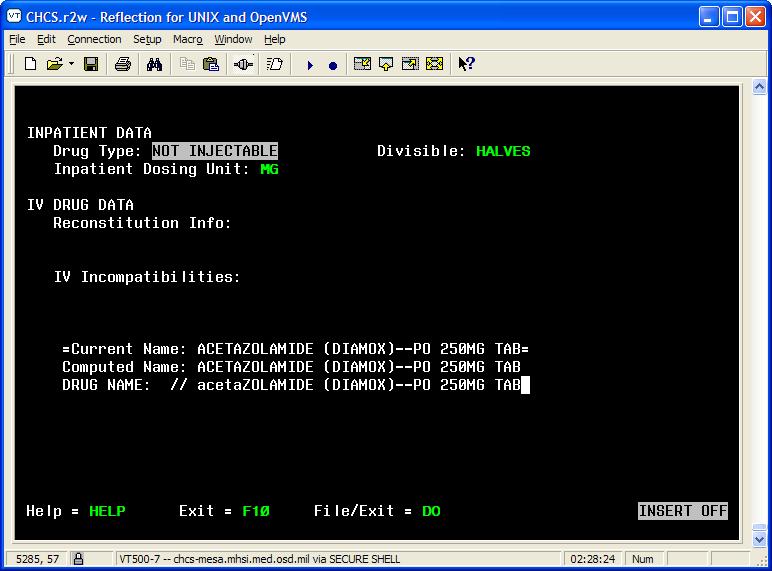
5 PURPOSE: To provide an overview of how to implement Tall Man Lettering in the CHCS Drug File. 1. Review The Joint Commission Look- Alike/Sounds-Alike (LASA) medication requirements 2. Change Drug Name to Tall Man Lettering in the CHCS Drug File 3. Run report to produce list of LASA medications with Tall Man Letting 4. Future Tall Man Lettering strategies

6 TJC Requirements MM develop LASA medication list, take actions to prevent errors and review list annually MM precautions for ordering LASA medications FDA-approved Tall Man Lettering list ISMP Tall Man Lettering Recommendations
7
8
9
10
11
12
13
14
15
16

17 Tallman lettering appears in AHLTA to mirror the CHCS changes.
18 ISMP Medication Safety Alert Newsletter, 14 Jul 2011 RxNorm will incorporate the ISMP list of drug names using Tall Man Letters A system of normalized names for clinical drugs links the names to many of the drug vocabularies commonly used in pharmacy management and drug interaction software, including those of First DataBank, Micromedex, Medi-Span, Gold Standard Alchemy, and Multum


19 The Army s Home for Health Saving Lives and Fostering Healthy and Resilient People ~ Partnerships Built on Trust
20 LTC Jorge D. Carrillo, PharmD, MS, BCPS Manager, Army Patient Safety Center HQ, U.S. Army Medical Command Quality Management Division Fort Sam Houston, TX Phone:
21 Dave Meade, PharmD, BCPS Clinical Pharmacist
22 Uniform Formulary Class Reviews Atypical Antipsychotics Agents Nasal Allergy Drugs New Drugs in Previously Reviewed Classes Bromfenac (Bromday ophthalmic soln) Dutasteride/tamsulosin (Jalyn) Saxagliptin /metformin extended-release (Kombiglyze XR)
23 Utilization Management Buprenorphine Transdermal System (Butrans) - Quantity Limits Alsuma (Sumatriptan Inj) - Quantity Limits
24 24
25 Generic Clozapine Risperidone Olanzapine Quetiapine Ziprasidone Aripiprazole Olanzapine/ Fluoxetine Paliperidone Iloperidone Brand Clozaril, Fazaclo (Novartis, multiple generics) Risperdal, Risperdal Consta (Ortho McNeil Janssen, multiple generics) Zyprexa, Zyprexa Zydis (Eli Lilly & Co) Seroquel, Seroquel XR (Astra Zeneca) Geodon (Pfizer) Abilify (Bristol-Myers Squibb) Symbyax (Eli Lilly & Co) Invega (Ortho McNeil Janssen) Fanapt (Vanda Pharmaceuticals) Strengths/ Formulations 12.5, 25, 50, 100, 200 mg tabs; 12.5, 25, 50, 100, 150, 200 mg ODT tabs 0.25, 0.5, 1, 2, 3, 4 mg tabs; 0.25, 0.5, 1, 2, 3, 4 mg ODT tabs; 1mg/mL oral solution 2.5, 5, 7.5, 10, 15, 20mg tabs; Zydis: 5, 10, 15, 20 mg ODT tabs 25, 50, 100, 150, 200, 300, 400 mg tabs 50, 150, 200, 300, 400 mg XR tabs 20, 40, 60, 80 mg caps; 10 mg/ml oral solution 2, 5, 10, 15, 20, 30 mg tabs; 10, 15 mg ODT tabs; 1mg/mL oral soln FDA Approval Date Patent Expiration 9/26/89 02/12/ /29/93 05/19/2014 9/30/96 4/06/00 9/26/97 5/17/07 10/23/ /26/2012 2/5/01 03/02/ /15/02 04/20/ , 6-25, 6-50, 12-25, mg caps 12/24/03 10/23/ , 3, 6, 9, 12 mg XR tabs 12/19/06 10/09/2012 1, 2, 4, 6, 8, 10, 12 mg tabs 5/6/09 11/15/2011 Asenapine Saphris (Merck) 5, 10 mg SL tabs 8/13/09 06/09/2015 Lurasidone Latuda (Sunovion) 40, 80 mg tabs 10/28/10 07/02/2013
26 Drug QD Dosing Approved Indications Other Than Schizophrenia MTF Market- Share > 5% Pediatric Indication Generic/ Upcoming Patent exp Low Metabolic Risk Profile Aripiprazole X X X X X Asenapine Iloperidone Lurasidone X X Olanzapine X X X X Evidence for Off-Label Use PTSD; Dementia PTSD; Dementia Olan/Fluox X X Paliperidone X X X Quetiapine X X X X PTSD; Dementia Quetiapine XR X X X Risperidone X X X X PTSD; Dementia Ziprasidone X X X
27 AAPs are efficacious for the treatment of schizophrenia and have some utility in treating other conditions Utilization patterns indicate a rise in off-label prescribing of AAPs Available evidence supports the use of AAPs as adjunctive therapy to CBT and SSRIs in the treatment of PTSD The small benefit seen in psychosis and behavioral disturbances associated with dementia is offset by a significant risk of increased mortality in elderly patients
28 In the absence of other psychiatric comorbidities, the use of low-dose AAPs for insomnia should be discouraged Strongly recommend education of providers and revision of MOD-10 Benefits conferred by AAPs are offset by limiting adverse effects Choice of treatment should be influenced by the relationship between the efficacy, tolerability and individual patient characteristics
29 BCF/ECF Medications MTFs must have BCF meds on formulary UF Medications MTFs may have on formulary Nonformulary Medications MTFs may not have on formulary PA and QL Issues Comments Risperidone (Risperdal, generics) Quetiapine (Seroquel, Seroquel XR) Aripiprazole (Abilify, Abilify discmelt) Clozapine (Clozaril, Fazaclo, generics) Olanzapine (Zyprexa, Zydis) Paliperidone ER (Invega) Olanzapine/fluoxetine (Symbyax) Ziprasidone (Geodon) Asenapine (Saphris) Iloperidone (Fanapt) Lurasidone (Latuda) None Risperidone (all oral formulations except ODT) remains on the BCF along with quetiapine IR and ER UF status of Risperidone ODT will be clarified at the Nov 2011 P&T meeting
30 30
31 Generic name Trade Name Manufacturer Patent expiration Nasal Corticosteroids Fluticasone propionate Flonase Glaxo SmithKline, generics Mometasone Nasonex Merck & Co Flunisolide -- Generics -- Beclomethasone Beconase AQ GlaxoSmithKline -- Budesonide Rhinocort Aqua AstraZeneca 2017 Ciclesonide Omnaris Sunovion Fluticasone furoate Veramyst GlaxoSmithKline 2021 Triamcinolone Nasacort AQ Sanofi-Aventis 2016 Nasal Anticholinergic & Antihistamines Azelastine 0.1% Astelin MEDA Pharma, generic -- Azelastine 0.15% with sucrose Astepro MEDA Pharma Excl to Aug 2012 Ipratropium bromide Atrovent nasal spray Boehringer-Ingelheim, generics Olopatadine HCL Patanase Alcon Jun 2011, Excl to
32 For treatment of allergic rhinitis, all of the Nasal Allergy agents appear to be safe and clinically effective There is no new evidence which substantively changes the conclusions of the DoD P&T Committee class review completed in 2008
33 Nasal saline is a viable therapeutic option and should be actively considered in most patients Vehicle effect is 2-4 times the magnitude of any active drug treatment effect Nasal steroids are first-line treatment for patients requiring medication No agent, within its subclass, is clearly better than another Non-sedating oral antihistamines should be considered before nasal antihistamines 33
34 BCF/ECF Medications MTFs must have BCF meds on formulary UF Medications MTFs may have on formulary Nonformulary Medications MTFs may not have on formulary Comments Fluticasone propionate (Flonase, generics) Nasal Corticosteroids Flunisolide (generics) Mometasone (Nasonex) Nasal Antihistamines Azelastine 0.1% (Astelin, generic) Olopatadine (Patanase) Anticholinergic Ipratropium (Atrovent, generics) Nasal Corticosteroids Beclomethasone (Beconase AQ) Budesonide (Rhinocort Aqua) Ciclesonide (Omnaris) Fluticasone furoate (Veramyst) Triamcinolone (Nasacort AQ) Antihistamine Azelastine 0.15% (Astepro) Azelastine 0.1% (Astelin, generic) no longer BCF Brand name at MTF is currently less expensive than the generic Olopatadine (Patanase) now UF
35 35
36
37 Type of Drug Non-steroidal anti-inflammatory drug (NSAID) Background Supplemental New Drug Application (snda) o Changed to once-a-day dosing from BID FDA discontinued Xibrom o Feb 28, 2011-shipments to wholesalers end o Generics to Xibrom (BID dosing) approved after May 2011 P&T meeting 37
38 Generic Name Brand Mfg Generic Strength FDA Approval Patent Expiration NSAIDs Bromfenac Bromday Ista No 0.09% 2005 No expired patents Bromfenac Xibrom Ista D/C 0.09% ; generics approved 06/11 Acular - Yes 0.5% Ketorolac Acular PF - D/C 0.5% - - Acular LS - Yes 0.4% Acuvail Allergan No 0.45% Diclofenac Voltaren - Yes 0.1% Flurbiprofen Ocufen - Yes 0.03% Nepafenac Nevanac Alcon No 0.1% D/C: Discontinued Acular PF: Preservative-free Acular LS: Lower strength
39 Bromday was approved using a snda In the 2 Phase III trials used to obtain FDA approval, bromfenac demonstrated superiority over placebo for the primary endpoint of cleared ocular inflammation when dosed QD There are no head-to-head studies of Bromday vs. other ophthalmic 1 drugs Based on the available safety data, there are no clinically relevant differences between bromfenac and other ophthalmic NSAID formulations In regards to other factors, bromfenac in the only ophthalmic NSAID that has QD dosing Whether the lower concentration of benzalkonium chloride in bromfenac is associated with lower risk of long-term effects is yet to be determined 40
40
41 Class: BPH Agents Subclass: Alpha-1 Blockers (A1Bs) Subclass: 5-Alpha Reductase Inhibitors (5-ARIs) Jalyn is a combination product containing an A1B and 5-ARI Prior Authorization for Alpha-1 blocker subclass must try tamsulosin or Uroxatral first 42
 in men with an enlarged prostate Generic Strength Dosing Tamsulosin available as generic Dutasteride (Avodart) not available as generic (patent expiration September 17,")
42 Parameter Type of Drug Comments Combination of 5-ARI (dutasteride) and A1B (tamsulosin) FDA Indications Approved June 14, 2010 Patent Expiration September 17, 2013 Treatment of symptomatic benign prostatic hyperplasia (BPH) in men with an enlarged prostate Generic Strength Dosing Tamsulosin available as generic Dutasteride (Avodart) not available as generic (patent expiration September 17, 2013) Capsule contains dutasteride 0.5mg and tamsulosin 0.4mg One capsule taken 30 minutes after same meal each day
43 Generic Brand (manufacturer) Generic Availability Strengths & Formulations FDA Approval Earliest Patent Expiration Terazosin Hytrin (Abbott) Yes 1, 2, 5 mg tablets / capsules 8/7/1987 tab 12/14/1995 cap (-) Doxazosin Cardura (Pfizer) Yes 1, 2, 4, 8 mg tablets 4, 8 mg XL tablets 11/2/1990 2/22/2005 XL (-) (-) Tamsulosin Flomax (Boehringer Ingelheim) Yes 0.4 mg capsule 4/15/1997 (-) Alfuzosin* Uroxatral (Sanofi-Aventis) No 10 mg ER capsule 6/12/2003 July 2011-Aug 2017 Silodosin Rapaflo (Watson Labs) No 4, 8 mg capsules 8/8/2008 Oct 2013 *generics to Uroxatral approved July 2011
44 Generic Name Brand (Manufacturer) Strength & Formulation FDA approval date (earliest patent expiration) Finasteride Proscar (Merck), generics (Ivax, Teva, Dr Reddys, Mylan, Gedeon, Actavis) 5 mg tablet 6/19/1992 (-) Dutasteride Avodart (GSK) 0.5 mg capsule 11/20/2001 (Sep 2013) 45
45 Based on the best available evidence, the combination of dutasteride and tamsulosin is not superior to dutasteride monotherapy for males with BPH with an enlarged prostate (>30ml) over a 4-year period, in terms of objective clinical progression, such as AUR and BPH-related surgery Combination therapy is superior to both tamsulosin and dutasteride monotherapy, in terms of delaying progression of IPSS symptom score There are no clinically relevant differences between the combination of dutasteride and tamsulosin versus monotherapy with either agent in terms of safety and tolerability AUR : Acute Urinary Retention IPSS: International Prostate Symptom Score
46 47
47 Active Ingredient Brand Strengths FDA Approval Date Patent Expiration Date Sitagliptin Januvia (Merck) 25mg, 50mg, 100mg 10/16/ /24/2017 Sitagliptin/ Metformin Janumet (Merck) 50mg/500mg, 50mg/1000mg 03/30/ /24/2017 Saxagliptin Onglyza (BMS) 2.5mg, 5mg 07/31/ /16/2021 Saxagliptin/ Metformin XR Linagliptin Kombiglyze XR (BMS) Tradjenta (Lilly/BI) 2.5mg/1000mg 5mg/500mg 5mg/1000mg 11/05/ /16/2021 5mg 5/2/2011 -
48 Sitagliptin and saxagliptin have similar A1c lowering effect when used as monotherapy ~ % Saxagliptin/metformin FDC provides a 2.5% decrease in A1c from baseline Sitagliptin/metformin FDC provides a 1.9% decrease in A1c from baseline One head-to-head trial, using metformin IR, did not show clinically significant differences in efficacy or safety between sitagliptin/met and saxagliptin/met One 4-week study with metformin XR and saxagliptin showed an improvement in average daily glucose compared to placebo 49
49 DPP-4 inhibitor FDC s are weight neutral, lipid neutral, and have minimal impact on blood pressure DPP-4 inhibitor FDC s are generally well-tolerated, have few side effects and few drug interactions Initiating 2-drug regimens is not currently recommended by the ADA, however, a FDC agent may improve compliance by decreasing pill burden An additional metformin dose is required in addition to Kombiglyze XR to achieve target metformin doses FDC: fixed dose combination
50 Drug BCF UF NF Comments- PA issues BPH Agents Alpha 1 Blockers None Tamsulosin/dutasteride (Jalyn) None Step Therapy (automated PA) with tamsulosin or alfuzosin as the preferred agents; pt must have an inadequate response to preferred agent and require tx with both an A1B and 5-ARI (Note: Step Therapy does not apply to terazosin, doxazosin, or doxazosin ER) Ophthalmic-1s Non-Insulin Diabetes Drugs DPP-4 Inhibitors Bromfenac QD (Bromday) Saxagliptin/metformin ER (Kombiglyze XR) None Step Therapy (automated PA) with metformin and sulfonylureas as step- preferred drugs
51 52
52 Type of Drug QL recommendation Mu opioid partial agonist, Maximum quantity Schedule III controlled o Retail: 4 patches /28 days substance o Mail: 12 patches/ 84 days Transdermal buprenorphine FDA Approved Indication Justification Management of moderate to severe chronic pain in patients requiring a continuous, aroundthe-clock opioid analgesic for an extended period of time Consistent with recommended dosing Prevent inadvertent misuse Dosing 5 mcg/hour, 10 mcg/hour, and 20 mcg/hour Each patch intended for 7 days 53
53 Type of Drug Injectable sumatriptan NDA (auto-injector) QL recommendation Maximum quantity o o Retail: 8 syringes /30 days Mail: 24 syringes/ 90 days FDA Approved Indication Acute treatment of migraine with or without aura Acute treatment of cluster headache episodes NOT intended for migraine prophylaxis Justification Collective QL exists for injectable sumatriptan Consistent with recommended dosing Dosing 6mg/0.5 ml subq injection Maximum of 2 doses in 24 hours separated by at least 1 hour 54

54 Dave Meade, PharmD, BCPS Clinical Pharmacist
55 Uniform Formulary Class Reviews Contraceptive Agents Oral Non-Steroidal Anti-Inflammatory (NSAID) Phosphodiesterase-5 Inhibitor (PDE-5) 56
 Bromocriptine quick release tablets (Cycloset) Buprenorphine - (Butrans")
56 New Drugs in Previously Reviewed Classes Azilsartan (Edarbi) Aliskiren/amlodipine/HCTZ (Amturnide) Bromocriptine quick release tablets (Cycloset) Buprenorphine - (Butrans transdermal patch)
57 Utilization Management Singulair Prior Authorization Lovaza PA update Avandia REMS (info) Simvastatin 80 and Simcor BCF status 58
58 Please assist us in improving the webcast presentations by completing an anonymous, 5-question survey Link: Thank you!
59 Questions?
60 (DSN ) For PEC Clinical Staff ASK 4 PEC ( ) Pharmacy Operation Center PECWEB@amedd.army.mil o Website issues pdts.ameddcs@amedd.army.mil o Questions, assistance with PDTS, Business Objects PECUF@amedd.army.mil o Clinical, formulary questions
Beneficiary Advisory Panel Handout Uniform Formulary Decisions 23 June 2011
 Beneficiary Advisory Panel Handout Uniform Formulary Decisions 23 June 211 PURPOSE: The purpose of this handout is to provide BAP Committee members with a reference document for the relative clinical effectiveness
Beneficiary Advisory Panel Handout Uniform Formulary Decisions 23 June 211 PURPOSE: The purpose of this handout is to provide BAP Committee members with a reference document for the relative clinical effectiveness
DEPARTMENT OF DEFENSE PHARMACY AND THERAPEUTICS COMMITTEE RECOMMENDATIONS. May 2011
 DEPARTMENT OF DEFENSE PHARMACY AND THERAPEUTICS COMMITTEE RECOMMENDATIONS I. CONVENING May 2011 The Department of Defense (DoD) Pharmacy and Therapeutics (P&T) Committee convened at 0800 hours on May 11
DEPARTMENT OF DEFENSE PHARMACY AND THERAPEUTICS COMMITTEE RECOMMENDATIONS I. CONVENING May 2011 The Department of Defense (DoD) Pharmacy and Therapeutics (P&T) Committee convened at 0800 hours on May 11
Comparison of Atypical Antipsychotics
 PL Detail-Document #281006 This PL Detail-Document gives subscribers additional insight related to the Recommendations published in PHARMACIST S LETTER / PRESCRIBER S LETTER October 2012 Comparison of
PL Detail-Document #281006 This PL Detail-Document gives subscribers additional insight related to the Recommendations published in PHARMACIST S LETTER / PRESCRIBER S LETTER October 2012 Comparison of
The Medical Letter. on Drugs and Therapeutics. Drug Some Formulations OTC/Rx Usual Dosage Comments Class Comments Cost 1
 The Medical Letter publications are protected by US and international copyright laws. Forwarding, copying or any other distribution of this material is strictly prohibited. For further information call:
The Medical Letter publications are protected by US and international copyright laws. Forwarding, copying or any other distribution of this material is strictly prohibited. For further information call:
Pharmacy Medical Necessity Guidelines: Antipsychotic Medications
 Pharmacy Medical Necessity Guidelines: Antipsychotic Medications Effective: July. 1, 2016 Prior Authorization Required Type of Review Care Management Not Covered Type of Review Clinical Review Pharmacy
Pharmacy Medical Necessity Guidelines: Antipsychotic Medications Effective: July. 1, 2016 Prior Authorization Required Type of Review Care Management Not Covered Type of Review Clinical Review Pharmacy
MTF Quarterly Webcast
 TMA Fort Sam Houston, TX MTF Quarterly Webcast LTC Stacia Spridgen Director, 1 Introduction Greetings from the PEC Purpose of the Quarterly MTF Webcast DCO Ground Rules Type questions into DCO system Put
TMA Fort Sam Houston, TX MTF Quarterly Webcast LTC Stacia Spridgen Director, 1 Introduction Greetings from the PEC Purpose of the Quarterly MTF Webcast DCO Ground Rules Type questions into DCO system Put
Triage Information: 1. Duration of HPSJ Membership 2. Age 3. Fill history of Seasonal Allergy Medications
 MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Seasonal Allergy Medications LAST REVIEW: 5/28/2015 THERAPEUTIC CLASS: Rheumatologic/Immunologic REVIEW HISTORY: 5/15, 9/14
MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Seasonal Allergy Medications LAST REVIEW: 5/28/2015 THERAPEUTIC CLASS: Rheumatologic/Immunologic REVIEW HISTORY: 5/15, 9/14
Oral Agents. Fml Limits. Available Strengths NF NF
 MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Allergy Medications LAST REVIEW: 9/12/2017 THERAPEUTIC CLASS: Rheumatologic/Immunologic REVIEW HISTORY: 9/16, 5/15, 9/14
MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Allergy Medications LAST REVIEW: 9/12/2017 THERAPEUTIC CLASS: Rheumatologic/Immunologic REVIEW HISTORY: 9/16, 5/15, 9/14
Pharmacy Medical Necessity Guidelines: Antipsychotic Medications
 Pharmacy Medical Necessity Guidelines: Effective: October 1, 2016 Prior Authorization Required Type of Review Care Management Not Covered Type of Review Clinical Review Pharmacy (RX) or Medical (MED) Benefit
Pharmacy Medical Necessity Guidelines: Effective: October 1, 2016 Prior Authorization Required Type of Review Care Management Not Covered Type of Review Clinical Review Pharmacy (RX) or Medical (MED) Benefit
Pharmacy Medical Necessity Guidelines: Atypical Antipsychotic Medications. Effective: December 12, 2017
 Pharmacy Medical Necessity Guidelines: Effective: December 12, 2017 Prior Authorization Required Type of Review Care Management Not Covered Type of Review Clinical Review Pharmacy (RX) or Medical (MED)
Pharmacy Medical Necessity Guidelines: Effective: December 12, 2017 Prior Authorization Required Type of Review Care Management Not Covered Type of Review Clinical Review Pharmacy (RX) or Medical (MED)
Pharmacy Medical Necessity Guidelines: Atypical Antipsychotic Medications. Effective: February 20, 2017
 Pharmacy Medical Necessity Guidelines: Effective: February 20, 2017 Prior Authorization Required Type of Review Care Management Not Covered Type of Review Clinical Review Pharmacy (RX) or Medical (MED)
Pharmacy Medical Necessity Guidelines: Effective: February 20, 2017 Prior Authorization Required Type of Review Care Management Not Covered Type of Review Clinical Review Pharmacy (RX) or Medical (MED)
DOD PHARMACY AND THERAPEUTICS COMMITTEE RECOMMENDATIONS INFORMATION FOR THE UNIFORM FORMULARY BENEFICIARY ADVISORY PANEL
 DOD PHARMACY AND THERAPEUTICS COMMITTEE RECOMMENDATIONS INFORMATION FOR THE UNIFORM FORMULARY BENEFICIARY ADVISORY PANEL I. Uniform Formulary Review Process Under 10 U.S.C. 1074g, as implemented by 32
DOD PHARMACY AND THERAPEUTICS COMMITTEE RECOMMENDATIONS INFORMATION FOR THE UNIFORM FORMULARY BENEFICIARY ADVISORY PANEL I. Uniform Formulary Review Process Under 10 U.S.C. 1074g, as implemented by 32
Pharmacy Benefit Management (PBM) Program FORMULARY/PRODUCT RESTRICTIONS
 Program FORMULARY/PRODUCT RESTRICTIONS") Workforce Safety & Insurance Revised Document Date: 07/21/2015 1600 E Century Ave Ste 1 PO Box 5585 Bismarck, ND 58506-5585 701.328.3800 1.800.777.5033 www.workforcesafety.com Pharmacy Benefit Management
Workforce Safety & Insurance Revised Document Date: 07/21/2015 1600 E Century Ave Ste 1 PO Box 5585 Bismarck, ND 58506-5585 701.328.3800 1.800.777.5033 www.workforcesafety.com Pharmacy Benefit Management
Oral Agents. Formulary Limits. Available Strengths. IR: 4mg ER: 12mg Syrup: 2mg/5ml
 MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Seasonal Allergy Medications LAST REVIEW: 9/20/2016 THERAPEUTIC CLASS: Rheumatologic/Immunologic REVIEW HISTORY: 5/16, 5/15,
MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Seasonal Allergy Medications LAST REVIEW: 9/20/2016 THERAPEUTIC CLASS: Rheumatologic/Immunologic REVIEW HISTORY: 5/16, 5/15,
Pharmacy Medical Necessity Guidelines: Antipsychotic Medications
 Pharmacy Medical Necessity Guidelines: Effective: April 1, 2018 Prior Authorization Required Type of Review Care Management Not Covered Type of Review Clinical Review Pharmacy (RX) or Medical (MED) Benefit
Pharmacy Medical Necessity Guidelines: Effective: April 1, 2018 Prior Authorization Required Type of Review Care Management Not Covered Type of Review Clinical Review Pharmacy (RX) or Medical (MED) Benefit
Antipsychotics Prior Authorization Criteria for Louisiana Fee for Service and MCO Medicaid Recipients
 Antipsychotics Prior Authorization Criteria for Louisiana Fee for Service and MCO Medicaid Recipients Preferred Agents (Oral) a Amitriptyline/Perphenazine (Generic) Aripiprazole Tablet (Generic) b Chlorpromazine
Antipsychotics Prior Authorization Criteria for Louisiana Fee for Service and MCO Medicaid Recipients Preferred Agents (Oral) a Amitriptyline/Perphenazine (Generic) Aripiprazole Tablet (Generic) b Chlorpromazine
Antipsychotic Medications Age and Step Therapy
 Market DC *- Florida Healthy Kids Antipsychotic Medications Age and Step Therapy Override(s) Approval Duration Prior Authorization 1 year Quantity Limit *Virginia Medicaid See State Specific Mandates *Indiana
Market DC *- Florida Healthy Kids Antipsychotic Medications Age and Step Therapy Override(s) Approval Duration Prior Authorization 1 year Quantity Limit *Virginia Medicaid See State Specific Mandates *Indiana
PL CE LIVE February 2011 Forum
 February 2011 PL CE LIVE Kristin W. Weitzel, Pharm.D., CDE, FAPhA Associate Editor and Director of Editorial Projects Pharmacist s Letter/Prescriber s Letter Atypical Antipsychotics Atypical Antipsychotics
February 2011 PL CE LIVE Kristin W. Weitzel, Pharm.D., CDE, FAPhA Associate Editor and Director of Editorial Projects Pharmacist s Letter/Prescriber s Letter Atypical Antipsychotics Atypical Antipsychotics
Step Therapy Group. Atypical Antipsychotic Agents
 Atypical Antipsychotic Agents Any beneficiary newly enrolled into Community Care, Inc. currently receiving aripiprazole, aripiprazole ODT, risperidone, risperidone ODT, olanzapine, olanzapine ODT, quetiapine,
Atypical Antipsychotic Agents Any beneficiary newly enrolled into Community Care, Inc. currently receiving aripiprazole, aripiprazole ODT, risperidone, risperidone ODT, olanzapine, olanzapine ODT, quetiapine,
Drugs requiring prior authorization: the list of drugs requiring prior authorization for this clinical criteria
 Drug/Drug Class Antipsychotics Clinical Criteria Information Included in this Document Drugs requiring prior authorization: the list of drugs requiring prior authorization for this clinical criteria Prior
Drug/Drug Class Antipsychotics Clinical Criteria Information Included in this Document Drugs requiring prior authorization: the list of drugs requiring prior authorization for this clinical criteria Prior
Antipsychotics in Bipolar
 Use of Second-Generation Antipsychotics in Bipolar Disorder: A Practical Guide Flavio Guzman, MD Editor Psychopharmacology Institute This practical guide is an update on the use of second-generation antipsychotics
Use of Second-Generation Antipsychotics in Bipolar Disorder: A Practical Guide Flavio Guzman, MD Editor Psychopharmacology Institute This practical guide is an update on the use of second-generation antipsychotics
Lonasen (Blonanserin) Lullan (Perospirone) Saphris/Sycrest (Asenapine, ORG 5222, SCH ) Saphris/Sycrest (Continued)...
 Lullan (Perospirone) Saphris/Sycrest (Asenapine, ORG 5222, SCH ) Saphris/Sycrest (Continued)...") CHAPTER ONE: INTRODUCTION... 1 STUDY GOALS AND OBJECTIVES... 1 REASONS FOR DOING THIS STUDY... 2 INTENDED AUDIENCE... 2 SCOPE OF REPORT... 3 METHODOLOGY... 3 INFORMATION SOURCES... 4 AUTHOR S CREDENTIALS...
CHAPTER ONE: INTRODUCTION... 1 STUDY GOALS AND OBJECTIVES... 1 REASONS FOR DOING THIS STUDY... 2 INTENDED AUDIENCE... 2 SCOPE OF REPORT... 3 METHODOLOGY... 3 INFORMATION SOURCES... 4 AUTHOR S CREDENTIALS...
CRITERIA Trial of two generic formulary products from the following: atomoxetine or ADHD stimulant medication.
 ADHD STIMULANTS ATOMOXETINE HCL, DEXEDRINE 10 MG TABLET, DEXEDRINE 5 MG TABLET, DEXMETHYLPHENIDATE HCL, DEXMETHYLPHENIDATE HCL ER, DEXTROAMPHETAMINE 10 MG TAB, DEXTROAMPHETAMINE 5 MG TAB, DEXTROAMPHETAMINE
ADHD STIMULANTS ATOMOXETINE HCL, DEXEDRINE 10 MG TABLET, DEXEDRINE 5 MG TABLET, DEXMETHYLPHENIDATE HCL, DEXMETHYLPHENIDATE HCL ER, DEXTROAMPHETAMINE 10 MG TAB, DEXTROAMPHETAMINE 5 MG TAB, DEXTROAMPHETAMINE
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Invega Sustenna, Invega Trinza) Reference Number: CP.PHAR.291 Effective Date: 12.01.16 Last Review Date: 08.18 Line of Business: Medicaid See Important Reminder at the end of this policy
Clinical Policy: (Invega Sustenna, Invega Trinza) Reference Number: CP.PHAR.291 Effective Date: 12.01.16 Last Review Date: 08.18 Line of Business: Medicaid See Important Reminder at the end of this policy
MTF Quarterly Webcast June 13, 2013
 MTF Quarterly Webcast June 13, 2013 Greetings from the PEC Purpose of the Quarterly MTF Webcast DCO Ground Rules Type questions into the DCO system Put on mute, not on hold Contingency plan if DCO system
MTF Quarterly Webcast June 13, 2013 Greetings from the PEC Purpose of the Quarterly MTF Webcast DCO Ground Rules Type questions into the DCO system Put on mute, not on hold Contingency plan if DCO system
2018 PDP Premier Step Therapy Document September 2018 Y0114_18_33144_I_009
 2018 PDP Premier Step Therapy Document September 2018 Aggrenox Y0114_18_33144_I_009 aspirin 25 mg-dipyridamole 200 mg capsule,ext.release 12 hr multiphase drug may be given. Step 1 Drug(s): clopidigrel.
2018 PDP Premier Step Therapy Document September 2018 Aggrenox Y0114_18_33144_I_009 aspirin 25 mg-dipyridamole 200 mg capsule,ext.release 12 hr multiphase drug may be given. Step 1 Drug(s): clopidigrel.
HOSPITAL BASED INPATIENT PSYCHIATRIC SERVICES (HBIPS) MEASURE SET
 MEASURE SET") HOSPITAL BASED INPATIENT PSYCHIATRIC SERVICES (HBIPS) MEASURE SET Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: February, 2013 Most recently revised: December 2018 The Psychiatric Measure Set CMS
HOSPITAL BASED INPATIENT PSYCHIATRIC SERVICES (HBIPS) MEASURE SET Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: February, 2013 Most recently revised: December 2018 The Psychiatric Measure Set CMS
Clinical Policy: Olanzapine Long-Acting Injection (Zyprexa Relprevv) Reference Number: CP.PHAR.292 Effective Date: Last Review Date: 08.
 Reference Number: CP.PHAR.292 Effective Date: Last Review Date: 08.") Clinical Policy: (Zyprexa Relprevv) Reference Number: CP.PHAR.292 Effective Date: 12.01.16 Last Review Date: 08.18 Line of Business: Medicaid See Important Reminder at the end of this policy for important
Clinical Policy: (Zyprexa Relprevv) Reference Number: CP.PHAR.292 Effective Date: 12.01.16 Last Review Date: 08.18 Line of Business: Medicaid See Important Reminder at the end of this policy for important
Michael J. Bailey, M.D. OptumHealth Public Sector
 Michael J. Bailey, M.D. OptumHealth Public Sector LIHP Quality Charter To ensure the quality of care delivered to enrollees in San Diego County Assistance Programs, such as County Medical Services (CMS)
Michael J. Bailey, M.D. OptumHealth Public Sector LIHP Quality Charter To ensure the quality of care delivered to enrollees in San Diego County Assistance Programs, such as County Medical Services (CMS)
Literature Scan: Drugs for BPH
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
IOWA MEDICAID DRUG UTILIZATION REVIEW COMMISSION 100 Army Post Road (515)
") IOWA MEDICAID DRUG UTILIZATION REVIEW COMMISSION 100 Army Post Road (515) 974-3131 -866-626-0216 Brett Faine, Pharm.D. Larry Ambroson, R.Ph. Casey Clor, M.D. Professional Staff: Mark Graber, M.D., FACEP
IOWA MEDICAID DRUG UTILIZATION REVIEW COMMISSION 100 Army Post Road (515) 974-3131 -866-626-0216 Brett Faine, Pharm.D. Larry Ambroson, R.Ph. Casey Clor, M.D. Professional Staff: Mark Graber, M.D., FACEP
New Exception Status Benefits
 AUGUST 2017 Nova Scotia Formulary Updates New Exception Status Benefits Forxiga (dapagliflozin) Xigduo (dapagliflozin and metformin hydrochloride) Criteria Update: Antipsychotic Medications Abilify (aripiprazole)
AUGUST 2017 Nova Scotia Formulary Updates New Exception Status Benefits Forxiga (dapagliflozin) Xigduo (dapagliflozin and metformin hydrochloride) Criteria Update: Antipsychotic Medications Abilify (aripiprazole)
Quarterly Pharmacy Formulary Change Notice
 MEDICAID PROVIDER BULLETIN February 26, 2015 Quarterly Pharmacy Formulary Change Notice Summary of Change: The formulary changes listed in the table below were reviewed and approved at our September 24,
MEDICAID PROVIDER BULLETIN February 26, 2015 Quarterly Pharmacy Formulary Change Notice Summary of Change: The formulary changes listed in the table below were reviewed and approved at our September 24,
Drug Use Criteria: Atypical Antipsychotics (oral)
") Texas Vendor Drug Program Drug Use Criteria: Atypical Antipsychotics (oral) Publication History 1. Developed: February 1997 2. Revised: September 2017; September 2015; December 2013; February 2012; June
Texas Vendor Drug Program Drug Use Criteria: Atypical Antipsychotics (oral) Publication History 1. Developed: February 1997 2. Revised: September 2017; September 2015; December 2013; February 2012; June
STEP THERAPY CRITERIA
 DRUG CLASS PRODUCTS) BRAND NAME (BRAND ONLY) (generic) STEP THERAPY CRITERIA ATYPICAL ANTIPSYCHOTICS (BRAND ONLY ABILIFY (AL TABLET & AL SOLUTION ONLY) (aripiprazole) FANAPT (BRAND ONLY) (iloperidone)
DRUG CLASS PRODUCTS) BRAND NAME (BRAND ONLY) (generic) STEP THERAPY CRITERIA ATYPICAL ANTIPSYCHOTICS (BRAND ONLY ABILIFY (AL TABLET & AL SOLUTION ONLY) (aripiprazole) FANAPT (BRAND ONLY) (iloperidone)
A Brief Overview of Psychiatric Pharmacotherapy. Joel V. Oberstar, M.D. Chief Executive Officer
 A Brief Overview of Psychiatric Pharmacotherapy Joel V. Oberstar, M.D. Chief Executive Officer Disclosures Some medications discussed are not approved by the FDA for use in the population discussed/described.
A Brief Overview of Psychiatric Pharmacotherapy Joel V. Oberstar, M.D. Chief Executive Officer Disclosures Some medications discussed are not approved by the FDA for use in the population discussed/described.
II. UF CLASS REVIEWS NASAL ALLERGY DRUGS
 DEPARTMENT OF DEFENSE PHARMACY AND THERAPEUTICS COMMITTEE RECOMMENDATIONS INFORMATION FOR THE UNIFORM FORMULARY BENEFICIARY ADVISORY PANEL I. UNIFORM FORMULARY REVIEW PROCESS Under 10 United States Code
DEPARTMENT OF DEFENSE PHARMACY AND THERAPEUTICS COMMITTEE RECOMMENDATIONS INFORMATION FOR THE UNIFORM FORMULARY BENEFICIARY ADVISORY PANEL I. UNIFORM FORMULARY REVIEW PROCESS Under 10 United States Code
Script Notes. Treatment of Mild to Moderate Asthma. In This Issue: Script Notes Has a New Look!
 Script Notes Third Quarter 2006 The Pharmacy and Therapeutics Newsletter for Keystone Mercy Health Plan Participating Providers In This Issue: Treatment of Mild to Moderate Asthma........... 1 Formulary
Script Notes Third Quarter 2006 The Pharmacy and Therapeutics Newsletter for Keystone Mercy Health Plan Participating Providers In This Issue: Treatment of Mild to Moderate Asthma........... 1 Formulary
Drug Class Review Second Generation Antipsychotic Drugs
 Drug Class Review Second Generation Antipsychotic Drugs Final Update 4 Report November 2013 The purpose of reports is to make available information regarding the comparative clinical effectiveness and
Drug Class Review Second Generation Antipsychotic Drugs Final Update 4 Report November 2013 The purpose of reports is to make available information regarding the comparative clinical effectiveness and
Judges Reference Table for the March 2016 Psychotropic Medication Utilization Parameters for Foster Children
 Judges Reference Table for the Psychotropic Medication Utilization Parameters for Foster Children Stimulants for treatment of ADHD Preschool (Ages 3-5 years) Child (Ages 6-12 years) Adolescent (Ages 13-17
Judges Reference Table for the Psychotropic Medication Utilization Parameters for Foster Children Stimulants for treatment of ADHD Preschool (Ages 3-5 years) Child (Ages 6-12 years) Adolescent (Ages 13-17
Slide 1. Slide 2. Slide 3. About this module. About this module. Antipsychotics: The Essentials Module 5 A Primer on Selected Antipsychotics
 Slide 1 Antipsychotics: The Essentials Module 5 A Primer on Selected Antipsychotics Flavio Guzmán, MD Slide 2 About this module 13 antipsychotics will be studied 3 first generation antipsychotics 10 second
Slide 1 Antipsychotics: The Essentials Module 5 A Primer on Selected Antipsychotics Flavio Guzmán, MD Slide 2 About this module 13 antipsychotics will be studied 3 first generation antipsychotics 10 second
ADHD STIMULANTS-S(SHC)
") Step Therapy Simply Health Care 2014 Formulary ID: 14406 Version: 14 Last Updated: 08/01/2014 ADHD STIMULANTS-S(SHC) Daytrana Focalin Xr Strattera Patient needs to have a paid claim for one Step 1 drug
Step Therapy Simply Health Care 2014 Formulary ID: 14406 Version: 14 Last Updated: 08/01/2014 ADHD STIMULANTS-S(SHC) Daytrana Focalin Xr Strattera Patient needs to have a paid claim for one Step 1 drug
Step Therapy Criteria 2019
 Step Therapy 2019 For information on obtaining an updated coverage determination or an exception to a coverage determination please call Freedom Health Member Services at 1-800-401-2740 or, for TTY/TDD
Step Therapy 2019 For information on obtaining an updated coverage determination or an exception to a coverage determination please call Freedom Health Member Services at 1-800-401-2740 or, for TTY/TDD
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Abilify Maintena, Aristada, Aristada Initio) Reference Number: CP.PHAR.290 Effective Date: 12.01.16 Last Review Date: 08.18 Line of Business: Medicaid Coding Implications Revision Log
Clinical Policy: (Abilify Maintena, Aristada, Aristada Initio) Reference Number: CP.PHAR.290 Effective Date: 12.01.16 Last Review Date: 08.18 Line of Business: Medicaid Coding Implications Revision Log
DOD PHARMACY AND THERAPEUTICS COMMITTEE RECOMMENDATIONS INFORMATION FOR THE UNIFORM FORMULARY BENEFICIARY ADVISORY PANEL
 DOD PHARMACY AND THERAPEUTICS COMMITTEE RECOMMENDATIONS INFORMATION FOR THE UNIFORM FORMULARY BENEFICIARY ADVISORY PANEL I. Uniform Formulary Review Process Under 10 U.S.C. 1074g, as implemented by 32
DOD PHARMACY AND THERAPEUTICS COMMITTEE RECOMMENDATIONS INFORMATION FOR THE UNIFORM FORMULARY BENEFICIARY ADVISORY PANEL I. Uniform Formulary Review Process Under 10 U.S.C. 1074g, as implemented by 32
Uniform Formulary Decisions 9 January 2014
 Beneficiary Advisory Panel Handout Uniform Formulary Decisions 9 January 2014 Purpose: The purpose of this handout is to provide the BAP members with a reference document for the clinical effective presentation
Beneficiary Advisory Panel Handout Uniform Formulary Decisions 9 January 2014 Purpose: The purpose of this handout is to provide the BAP members with a reference document for the clinical effective presentation
REXULTI (brexpiprazole) oral tablet
 oral tablet") REXULTI (brexpiprazole) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
REXULTI (brexpiprazole) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
ALLERGIC RHINITIS-NASAL
 ALLERGIC RHINITIS-NASAL FLUNISOLIDE Patient needs to have paid claims for any one of the following Step 1 drugs: NasaCort OTC, fluticasone Rx, fluticasone OTC, Budesonide OTC. Prior to filling the Step
ALLERGIC RHINITIS-NASAL FLUNISOLIDE Patient needs to have paid claims for any one of the following Step 1 drugs: NasaCort OTC, fluticasone Rx, fluticasone OTC, Budesonide OTC. Prior to filling the Step
Relative Cost/Month. Less than $10. Loratadine Liquid* $10-$15 Cetirizine liquid 1mg/mL*
 Allergy Chlorpheniramine Tablet* Diphenhydramine Tablet* Diphenhydramine Liquid* Loratadine Tablet* Cetirizine Tablet* Loratadine 10mg ODT* Less than $10 Loratadine Liquid* $10-$15 Cetirizine liquid 1mg/mL*
Allergy Chlorpheniramine Tablet* Diphenhydramine Tablet* Diphenhydramine Liquid* Loratadine Tablet* Cetirizine Tablet* Loratadine 10mg ODT* Less than $10 Loratadine Liquid* $10-$15 Cetirizine liquid 1mg/mL*
Introduction. Objectives. Psychotropic Medications & Cardiometabolic Risk
 Psychotropic Medications & Cardiometabolic Risk Sam Ellis, PharmD, BCPS, CDE Associate Professor University of Colorado School of Pharmacy Introduction Second GenerationAntipsychotics (SGA) first FDA approved
Psychotropic Medications & Cardiometabolic Risk Sam Ellis, PharmD, BCPS, CDE Associate Professor University of Colorado School of Pharmacy Introduction Second GenerationAntipsychotics (SGA) first FDA approved
Investor Presentation December The vision to see past tomorrow
 Investor Presentation December 2011 The vision to see past tomorrow Safe Harbor Statement Certain statements contained herein are forward-looking statements (as such term is defined in the Private Securities
Investor Presentation December 2011 The vision to see past tomorrow Safe Harbor Statement Certain statements contained herein are forward-looking statements (as such term is defined in the Private Securities
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Reference Number: HIM.PA.59 Effective Date: 12/14 Last Review Date: 08/17 Line of Business: Health Insurance Marketplace Coding Implications Revision Log See Important Reminder at the
Clinical Policy: Reference Number: HIM.PA.59 Effective Date: 12/14 Last Review Date: 08/17 Line of Business: Health Insurance Marketplace Coding Implications Revision Log See Important Reminder at the
Ophthalmic-1s: Antihistamine and Dual Acting Antihistamine/Mast Cell Stabilizers DHA Formulary Management Branch
 May 2017 Antihistamine and Dual Acting Antihistamine/Mast Cell Stabilizers Executive Summary Page 1 of 5 Ophthalmic-1s: Antihistamine and Dual Acting Antihistamine/Mast Cell Stabilizers DHA Formulary Management
May 2017 Antihistamine and Dual Acting Antihistamine/Mast Cell Stabilizers Executive Summary Page 1 of 5 Ophthalmic-1s: Antihistamine and Dual Acting Antihistamine/Mast Cell Stabilizers DHA Formulary Management
South Carolina Department of Health and Human Services Post Office Box 8206 Columbia, South Carolina
 South Carolina Department of Health and Human Services Post Office Box 8206 Columbia, South Carolina 29202-8206 Pharmacy and Therapeutics (P&T) Committee Meeting MINUTES 1. Call to Order A meeting of the
South Carolina Department of Health and Human Services Post Office Box 8206 Columbia, South Carolina 29202-8206 Pharmacy and Therapeutics (P&T) Committee Meeting MINUTES 1. Call to Order A meeting of the
CONTRAINDICATIONS TABLE
 CONTRAINDICATIONS TABLE Generic Name Brand Name Contraindications Amphetamine Salts Adderall, Adderall XR Hypersensitivity to amphetamine, dextroamphetamine, or other sympathomimetic amines Advanced arteriosclerosis
CONTRAINDICATIONS TABLE Generic Name Brand Name Contraindications Amphetamine Salts Adderall, Adderall XR Hypersensitivity to amphetamine, dextroamphetamine, or other sympathomimetic amines Advanced arteriosclerosis
Antipsychotics. Something Old, Something New, Something Used to Treat the Blues
 Antipsychotics Something Old, Something New, Something Used to Treat the Blues Objectives To provide an overview of the key differences between first and second generation agents To an overview the newer
Antipsychotics Something Old, Something New, Something Used to Treat the Blues Objectives To provide an overview of the key differences between first and second generation agents To an overview the newer
Iowa Medicaid Drug Utilization Review (DUR) Commission Meeting March 4, 2009
 Commission Meeting March 4, 2009") CHESTER J. CULVER, GOVERNOR PATTY JUDGE, LT. GOVERNOR DEPARTMENT OF HUMAN SERVICES EUGENE I. GESSOW, DIRECTOR Iowa Medicaid Drug Utilization Review (DUR) Commission Meeting March 4, 2009 Location: Learning
CHESTER J. CULVER, GOVERNOR PATTY JUDGE, LT. GOVERNOR DEPARTMENT OF HUMAN SERVICES EUGENE I. GESSOW, DIRECTOR Iowa Medicaid Drug Utilization Review (DUR) Commission Meeting March 4, 2009 Location: Learning
II. UF CLASS REVIEWS SHORT-ACTING BETA AGONISTS (SABAs)
") DEPARTMENT OF DEFENSE PHARMACY AND THERAPEUTICS COMMITTEE RECOMMENDATIONS INFORMATION FOR THE UNIFORM FORMULARY BENEFICIARY ADVISORY PANEL I. UNIFORM FORMULARY REVIEW PROCESS Under 10 United States Code
DEPARTMENT OF DEFENSE PHARMACY AND THERAPEUTICS COMMITTEE RECOMMENDATIONS INFORMATION FOR THE UNIFORM FORMULARY BENEFICIARY ADVISORY PANEL I. UNIFORM FORMULARY REVIEW PROCESS Under 10 United States Code
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Reference Number: CP.HNCA.01 Effective Date: 11.16.16 Last Review Date: 04.18 Line of Business: Commercial - HNCA Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: Reference Number: CP.HNCA.01 Effective Date: 11.16.16 Last Review Date: 04.18 Line of Business: Commercial - HNCA Revision Log See Important Reminder at the end of this policy for important
BLUE SHIELD OF CALIFORNIA MARCH 2016 STANDARD DRUG FORMULARY CHANGES
 BLUE SHIELD OF CALIFORNIA MARCH 2016 STANDARD DRUG FORMULARY CHANGES Blue Shield is committed to covering safe, effective and affordable medications, so we regularly review and update our drug formularies.
BLUE SHIELD OF CALIFORNIA MARCH 2016 STANDARD DRUG FORMULARY CHANGES Blue Shield is committed to covering safe, effective and affordable medications, so we regularly review and update our drug formularies.
ABILIFY INJ. Products Affected Step 2: ABILIFY MAINTENA PREFILLED SYRINGE 300 MG INTRAMUSCULAR ABILIFY MAINTENA PREFILLED SYRINGE 400 MG INTRAMUSCULAR
 ABILIFY INJ ABILIFY MAINTENA PREFILLED SYRINGE 300 MG ABILIFY MAINTENA PREFILLED SYRINGE 400 MG ABILIFY MAINTENA SUSPENSION RECONSTITUTED ER 300 MG Claim will pay automatically for ABILIFY MAINTENA if
ABILIFY INJ ABILIFY MAINTENA PREFILLED SYRINGE 300 MG ABILIFY MAINTENA PREFILLED SYRINGE 400 MG ABILIFY MAINTENA SUSPENSION RECONSTITUTED ER 300 MG Claim will pay automatically for ABILIFY MAINTENA if
Scope and Methodology Size and Growth of the Market Issues and Trends Affecting the Rx-to-OTC Switches Market Leading Competitors
 TABLE OF CONTENTS CHAPTER ONE: EXECUTIVE SUMMARY Scope and Methodology Size and Growth of the Market Issues and Trends Affecting the Rx-to-OTC Switches Market Leading Competitors CHAPTER TWO: INTRODUCTION
TABLE OF CONTENTS CHAPTER ONE: EXECUTIVE SUMMARY Scope and Methodology Size and Growth of the Market Issues and Trends Affecting the Rx-to-OTC Switches Market Leading Competitors CHAPTER TWO: INTRODUCTION
Objectives. Antipsychotics 7/25/2016. LeadingAge Florida 53rd Annual Convention & Exposition
 Reducing the Use of Antipsychotics in Long Term Care Communities Alan W. Obringer RPh, CPh, CGP Executive Director Senior Care Pharmacy Objectives Recognize the clinical evidence for the need to change
Reducing the Use of Antipsychotics in Long Term Care Communities Alan W. Obringer RPh, CPh, CGP Executive Director Senior Care Pharmacy Objectives Recognize the clinical evidence for the need to change
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Saphris) Reference Number: CP.PMN.15 Effective Date: 12.01.14 Last Review Date: 02.18 Line of Business: Commercial, Health Insurance Marketplace, Medicaid Revision Log See Important Reminder
Clinical Policy: (Saphris) Reference Number: CP.PMN.15 Effective Date: 12.01.14 Last Review Date: 02.18 Line of Business: Commercial, Health Insurance Marketplace, Medicaid Revision Log See Important Reminder
Texas Prior Authorization Program Clinical Edit Criteria
 Texas Prior Authorization Program Clinical Edit Criteria Drug/Drug Class Clinical Edit Information Included in this Document Drugs requiring prior authorization: the list of drugs requiring prior authorization
Texas Prior Authorization Program Clinical Edit Criteria Drug/Drug Class Clinical Edit Information Included in this Document Drugs requiring prior authorization: the list of drugs requiring prior authorization
ADHD STIMULANTS - SCORE
 ADHD STIMULANTS - SCORE Step Therapy Strattera Patient needs to have a paid claim for two generic formulary ADHD stimulant medications. Formulary ID# 00017034 Last Updated: 08/01/2017 1 ALPHA GLUCOSIDASE
ADHD STIMULANTS - SCORE Step Therapy Strattera Patient needs to have a paid claim for two generic formulary ADHD stimulant medications. Formulary ID# 00017034 Last Updated: 08/01/2017 1 ALPHA GLUCOSIDASE
Debra Brown, PharmD, FASCP Pharmaceutical Consultant II Specialist. HMS Training Webinar January 27, 2017
 Debra Brown, PharmD, FASCP Pharmaceutical Consultant II Specialist HMS Training Webinar January 27, 2017 1 Describe nationwide prevalence and types of elderly dementia + define BPSD Define psychotropic
Debra Brown, PharmD, FASCP Pharmaceutical Consultant II Specialist HMS Training Webinar January 27, 2017 1 Describe nationwide prevalence and types of elderly dementia + define BPSD Define psychotropic
Rexulti (brexpiprazole)
") Market DC Rexulti (brexpiprazole) Override(s) Approval Duration Prior Authorization 1 year Quantity Limit *Indiana see State Specific Mandates below *Maryland see State Specific Mandates below *Virginia
Market DC Rexulti (brexpiprazole) Override(s) Approval Duration Prior Authorization 1 year Quantity Limit *Indiana see State Specific Mandates below *Maryland see State Specific Mandates below *Virginia
US pharmaceutical market: trends, issues, forecast. Doug Long Vice President Industry Relations IMS Health
 US pharmaceutical market: trends, issues, forecast Doug Long Vice President Industry Relations IMS Health 2006 Strategic management review The World Pharmaceutical Market All reproduction rights, quotations,
US pharmaceutical market: trends, issues, forecast Doug Long Vice President Industry Relations IMS Health 2006 Strategic management review The World Pharmaceutical Market All reproduction rights, quotations,
Allergies and Asthma 5/21/2013. Objectives. Allergic Rhinitis (AR): Risk Factor for ASTHMA. Rhinitis and Asthma
: Risk Factor for ASTHMA. Rhinitis and Asthma") Allergies and Asthma Presented By: Dr. Fadwa Gillanders, Pharm.D Clinical Pharmacy Specialist May 2013 Objectives Understand the relationship between asthma and allergic rhinitis Understand what is going
Allergies and Asthma Presented By: Dr. Fadwa Gillanders, Pharm.D Clinical Pharmacy Specialist May 2013 Objectives Understand the relationship between asthma and allergic rhinitis Understand what is going
TEST ANTICONVULSANT THERAPY. Products Affected. Step 2: Network Health Insurance Corporation NetworkCares Step Therapy Criteria Last Updated 11/2018
 TEST Network Health Insurance Corporation NetworkCares Step Therapy Last Updated 11/2018 ANTICONVULSANT THERAPY Aptiom Banzel Briviact Celontin Dilantin 30 Mg Capsule Equetro Fycompa 0.5 Mg/ml Oral Susp
TEST Network Health Insurance Corporation NetworkCares Step Therapy Last Updated 11/2018 ANTICONVULSANT THERAPY Aptiom Banzel Briviact Celontin Dilantin 30 Mg Capsule Equetro Fycompa 0.5 Mg/ml Oral Susp
Generics. Lead with. P r e s c r i p t i o n S t e p T h e r a p y P r o g r a m
 Lead with Generics P r e s c r i p t i o n S t e p T h e r a p y P r o g r a m WWW.BCBSLA.COM 04HQ3972 5/09 Blue Cross and Blue Shield of Louisiana incorporated as Louisiana Health Service & Indemnity
Lead with Generics P r e s c r i p t i o n S t e p T h e r a p y P r o g r a m WWW.BCBSLA.COM 04HQ3972 5/09 Blue Cross and Blue Shield of Louisiana incorporated as Louisiana Health Service & Indemnity
MTF Quarterly Webcast December 13, 2012
 MTF Quarterly Webcast December 13, 2012 Greetings from the PEC Purpose of the Quarterly MTF Webcast DCO Ground Rules Type questions into the DCO system Put on mute, not on hold Contingency plan if DCO
MTF Quarterly Webcast December 13, 2012 Greetings from the PEC Purpose of the Quarterly MTF Webcast DCO Ground Rules Type questions into the DCO system Put on mute, not on hold Contingency plan if DCO
ADHD STIMULANTS - SCORE
 Step Therapy Trillium 5 Tier Effective Date: 12/01/2017 Approval Date: 10/24/2017 ADHD STIMULANTS - SCORE Strattera Trial of two generic formulary products from the following: atomoxetine or ADHD stimulant
Step Therapy Trillium 5 Tier Effective Date: 12/01/2017 Approval Date: 10/24/2017 ADHD STIMULANTS - SCORE Strattera Trial of two generic formulary products from the following: atomoxetine or ADHD stimulant
STEP THERAPY PROGRAM
 STEP THERAPY PROGRAM Step Therapy Program Certain prescription drugs call for a more detailed assessment to help ensure that they represent reasonable treatment. For these drugs, Great-West s Special Authorization
STEP THERAPY PROGRAM Step Therapy Program Certain prescription drugs call for a more detailed assessment to help ensure that they represent reasonable treatment. For these drugs, Great-West s Special Authorization
Step Therapy Medications
 Step Therapy Medications Step Therapy Group APTIOM Step-2: APTIOM 200 MG TABLET or APTIOM 400 MG TABLET or APTIOM 600 MG TABLET or APTIOM 800 MG TABLET Step 1 Drug(s): Oxcarbazepine immediate-release,
Step Therapy Medications Step Therapy Group APTIOM Step-2: APTIOM 200 MG TABLET or APTIOM 400 MG TABLET or APTIOM 600 MG TABLET or APTIOM 800 MG TABLET Step 1 Drug(s): Oxcarbazepine immediate-release,
FirstCarolinaCare Insurance Company Step Therapy Requirements
 ANALGESICS, NARCOTICS KADIAN MORPHINE SULFATE ER PRIOR CLAIM FOR MORPHINE SULFATE SUSTAINED ACTION TABLET (MS CONTIN) WITHIN THE PAST 120 DAYS. ANTIBACTERIALS (EENT) BESIVANCE PRIOR CLAIM FOR CIPROFLOXACIN
ANALGESICS, NARCOTICS KADIAN MORPHINE SULFATE ER PRIOR CLAIM FOR MORPHINE SULFATE SUSTAINED ACTION TABLET (MS CONTIN) WITHIN THE PAST 120 DAYS. ANTIBACTERIALS (EENT) BESIVANCE PRIOR CLAIM FOR CIPROFLOXACIN
MTF Quarterly Webcast September 12, 2013
 MTF Quarterly Webcast September 12, 2013 Greetings from the PEC Purpose of the Quarterly MTF Webcast DCO Ground Rules Type questions into the DCO system Put on mute, not on hold Contingency plan if DCO
MTF Quarterly Webcast September 12, 2013 Greetings from the PEC Purpose of the Quarterly MTF Webcast DCO Ground Rules Type questions into the DCO system Put on mute, not on hold Contingency plan if DCO
Should flomax be taken at bedtime
 Should flomax be taken at bedtime Adults with radiopaque lower ureteral stones of 10 mm or smaller have received tamsulosin 0.4 mg PO at bedtime for 28 days or until definite stone passage (i.e. Prostate
Should flomax be taken at bedtime Adults with radiopaque lower ureteral stones of 10 mm or smaller have received tamsulosin 0.4 mg PO at bedtime for 28 days or until definite stone passage (i.e. Prostate
MEDICAL ASSISTANCE HANDBOOK PRIOR AUTHORIZATION OF PHARMACEUTICAL SERVICES. I. Requirements for Prior Authorization of Antipsychotics
 MEDICAL ASSISTANCE HBOOK PRI AUTHIZATION OF PHARMACEUTICAL SERVICES I. Requirements for Prior Authorization of Antipsychotics A. Prescriptions That Require Prior Authorization Prescriptions for Antipsychotics
MEDICAL ASSISTANCE HBOOK PRI AUTHIZATION OF PHARMACEUTICAL SERVICES I. Requirements for Prior Authorization of Antipsychotics A. Prescriptions That Require Prior Authorization Prescriptions for Antipsychotics
Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Criteria for Child Psychiatrist on the Use of Selected Psychotropic Medications in Children & Adolescents
 Criteria for Child Psychiatrist on the Use of Selected Psychotropic Medications in Children & Adolescents DRUG NAME INDICATIONS / ACCEPTABLE USES PRIOR STIMULANT/ADHD DRUGS Daytrana (methylphenidate) ADHD
Criteria for Child Psychiatrist on the Use of Selected Psychotropic Medications in Children & Adolescents DRUG NAME INDICATIONS / ACCEPTABLE USES PRIOR STIMULANT/ADHD DRUGS Daytrana (methylphenidate) ADHD
Psychotropics and Foster Care: Challenge or Opportunity?
 Psychotropics and Foster Care: Challenge or Opportunity? Raymond C. Love, PharmD, BCPP, FASHP Professor and Director, Mental Health Program University of Maryland School of Pharmacy Objectives At the conclusion
Psychotropics and Foster Care: Challenge or Opportunity? Raymond C. Love, PharmD, BCPP, FASHP Professor and Director, Mental Health Program University of Maryland School of Pharmacy Objectives At the conclusion
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Invega) Reference Number: CP. PMA.10.11.19 Effective Date: 10.06.16 Last Review Date: 04.18 Line of Business: CenpaticoMedicaid Revision Log See Important Reminder at the end of this
Clinical Policy: (Invega) Reference Number: CP. PMA.10.11.19 Effective Date: 10.06.16 Last Review Date: 04.18 Line of Business: CenpaticoMedicaid Revision Log See Important Reminder at the end of this
Indiana Medicaid Drug Utilization Review Board Newsletter
 Indiana Medicaid Drug Utilization Review Board Newsletter Volume 15 Issue 1 April 2012 Indiana Medicaid DUR Board Room W382 Indiana State Government Center, South 402 West Washington Street Indianapolis,
Indiana Medicaid Drug Utilization Review Board Newsletter Volume 15 Issue 1 April 2012 Indiana Medicaid DUR Board Room W382 Indiana State Government Center, South 402 West Washington Street Indianapolis,
Step Therapy Criteria
 Tier 5 Formulary Step Therapy 2016 Updated: 05/24/2016 Effective: 06/01/2016 What is Step Therapy? Some prescription drugs require step therapy (ST). In some cases, the plan requires you to first try certain
Tier 5 Formulary Step Therapy 2016 Updated: 05/24/2016 Effective: 06/01/2016 What is Step Therapy? Some prescription drugs require step therapy (ST). In some cases, the plan requires you to first try certain
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Reference Number: AZ.CP.PHAR.10.11.10 Effective Date: 07.16 Last Review Date: 09.12.18 Line of Business: Medicaid Arizona Revision Log See Important Reminder at the end of this policy
Clinical Policy: Reference Number: AZ.CP.PHAR.10.11.10 Effective Date: 07.16 Last Review Date: 09.12.18 Line of Business: Medicaid Arizona Revision Log See Important Reminder at the end of this policy
NEWER ATYPICAL ANTIPSYCHOTICS: NOVEL IDEAS OR
 NEWER ATYPICAL ANTIPSYCHOTICS: NOVEL IDEAS OR METOOS? Sanaz Farhadian, Pharm.D., BCPP Clinical Psychiatric Pharmacist Veterans Affairs Healthcare System, San Diego, CA OBJECTIVES Discuss new antipsychotics
NEWER ATYPICAL ANTIPSYCHOTICS: NOVEL IDEAS OR METOOS? Sanaz Farhadian, Pharm.D., BCPP Clinical Psychiatric Pharmacist Veterans Affairs Healthcare System, San Diego, CA OBJECTIVES Discuss new antipsychotics
AETNA BETTER HEALTH OF TEXAS Provider Relations newsletter
 AETNA BETTER HEALTH OF TEXAS Provider Relations newsletter Summer 2017 Table of contents Chief Medical Officer Comments and New Guideline Application...1 Chief Medical Officer Comments and Pharmacy Corner...2
AETNA BETTER HEALTH OF TEXAS Provider Relations newsletter Summer 2017 Table of contents Chief Medical Officer Comments and New Guideline Application...1 Chief Medical Officer Comments and Pharmacy Corner...2
Commissioner for the Department for Medicaid Services Selections for Preferred Products
 Commissioner for the Department for Medicaid Services Selections for Preferred Products This is a summary of the final Preferred Drug List (PDL) selections made by the Commissioner for the Department for
Commissioner for the Department for Medicaid Services Selections for Preferred Products This is a summary of the final Preferred Drug List (PDL) selections made by the Commissioner for the Department for
South Carolina Department of Health and Human Services Post Office Box 8206 Columbia, South Carolina
 South Carolina Department of Health and Human Services Post Office Box 8206 Columbia, South Carolina 29202-8206 Pharmacy and Therapeutics (P&T) Committee Meeting MINUTES 1. Call to Order A meeting of the
South Carolina Department of Health and Human Services Post Office Box 8206 Columbia, South Carolina 29202-8206 Pharmacy and Therapeutics (P&T) Committee Meeting MINUTES 1. Call to Order A meeting of the
ALLERGIC CONJUNCTIVITIS AGENTS
 2018 5 Tier Standard- Keystone First VIP Choice Document: 2018 Step Therapy Formulary ID: 18390 Last Updated: 04/2018 Effective Date: 05-01-2018 ALLERGIC CONJUNCTIVITIS AGENTS epinastine 0.05 % eye drops
2018 5 Tier Standard- Keystone First VIP Choice Document: 2018 Step Therapy Formulary ID: 18390 Last Updated: 04/2018 Effective Date: 05-01-2018 ALLERGIC CONJUNCTIVITIS AGENTS epinastine 0.05 % eye drops
ABILIFY ABILIFY DISCMELT ACTONEL ACTOPLUS MET ACTOPLUS MET XR ACTOS ADCIRCA ADVAIR DISKUS ADVAIR HFA
 Quantity Limits Paramount Medicare Formulary 2012 Formulary ID 12112, Version 22. CMS Approved 10-23-2012. ABILIFY Abilify TABS ABILIFY DISCMELT Abilify Discmelt ACTONEL Actonel TABS 150MG Actonel TABS
Quantity Limits Paramount Medicare Formulary 2012 Formulary ID 12112, Version 22. CMS Approved 10-23-2012. ABILIFY Abilify TABS ABILIFY DISCMELT Abilify Discmelt ACTONEL Actonel TABS 150MG Actonel TABS
Antipsychotic Prior Authorization Request
 Antipsychotic Prior Authorization Request Commonwealth of Massachusetts MassHealth Drug Utilization Review Program P.O. Box 2586, Worcester, MA 01613-2586 Fax: 1-877-208-7428 Phone: 1-800-745-7318 MassHealth
Antipsychotic Prior Authorization Request Commonwealth of Massachusetts MassHealth Drug Utilization Review Program P.O. Box 2586, Worcester, MA 01613-2586 Fax: 1-877-208-7428 Phone: 1-800-745-7318 MassHealth