Happy Wheezer/Happy Parent/ Happy Doctor (?)
|
|
|
- Alyson Goodwin
- 5 years ago
- Views:
Transcription






1 Happy Wheezer/Happy Parent/ Happy Doctor (?) Andrew Bush MD FRCP FRCPCH FERS Imperial College & Royal Brompton Hospital
2 Conflict of Interest AB has no financial or other COI There will be discussion of off-label and unlicensed use of asthma medications
3 Aims of the Presentation Discuss the clinical approach to the pre-school child with wheeze Show how recent advances in understanding preschool wheeze impact on treatment Suggest approaches to the unhappy child, the unhappy parent, and the unhappy Dr I will NOT discuss epidemiology many scientific insights, but does not help me decide on treatment
4 Everyone happy? No treatment without a diagnosis What are the possibilities lessons from pathology Cui bono? (or for the classically challenged, who s it all for?) Summary and conclusions
5 Is it true wheeze? < 50% agreement between parents and clinicians on whether child wheezed; only 11% parents mentioned whistling Arch Dis Child 2000; 82: Only 32% agreement between parents and physicians Objective recording correlated with physician report Nurses and parents were not reliable J Asthma 2004; 41: Video-questionnaire: 30% parents used words other than wheeze to describe wheeze, or wheeze to describe non-wheeze sounds Arch Dis Child 2001; 84: 31-4 Video-questionnaire helps identify UA abnormalities Arch Dis Child 2005; 90: 961-4
6 All that wheezes is not asthma! Take a good history, detailed physical examination Targeted investigations Many need none Selective approach THEN, consider phenotypes and what treatment should be given (if any)
7 Isolated chronic cough is rarely if ever due to asthma Cough variant asthma is overdiagnosed and over-treated, to the detriment of children!
8 Coughs and Wheezes... Fall into one of five categories! Normal child (hardest diagnosis) Serious illness - eg CF, TB (rare, but essential to get right) An asthma syndrome Minor problems (rhinitis, reflux) which may mimic or exacerbate wheezing syndromes Overanxious, psychological
9 Normal Childhood Respiratory Symptoms Normal Cough Post-viral/bronchiolitic cough Viral colds: 10% children have >10/year, may have symptoms >2 weeks Acute otitis media: many children have >3/year Pertussis and its relatives Nursery School Syndrome Usually 1 st Child Early placement in child care facility Repeated viral infections, one viral cold merging into another No response to antibiotics, bronchodilators, ICS, etc.
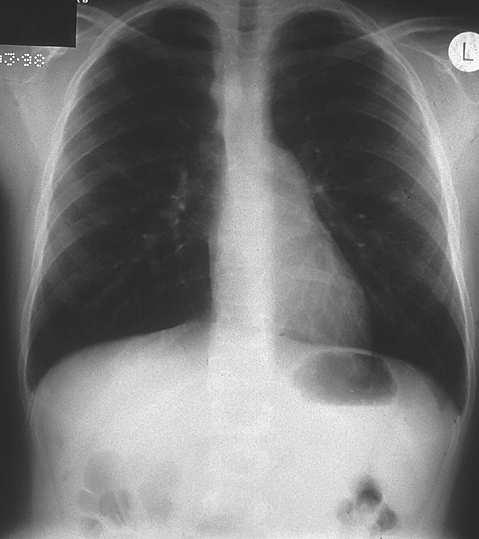
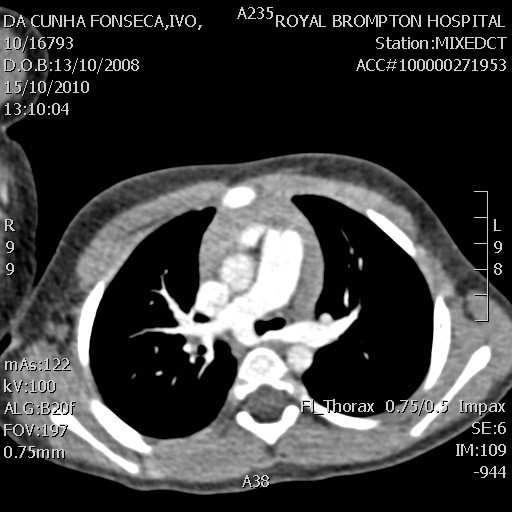
10
 Anomalous left subclavian")
11 Right sided aortic arch Diverticulum of Kommerel (arrow) Anomalous left subclavian artery
12
13 Points in the History - 1 Is it really wheeze? Upper airway symptoms prominent? Symptoms from first day of life Sudden onset symptoms Chronic moist cough/sputum reliable!

14 Points in the History - 2 Worse after meals, irritable feeder, arches back, vomits Systemic illness or immunodeficiency Continuous, unremitting symptoms


15 Physical Examination Clubbing, weight loss, failure to thrive Upper airway disease tonsils, rhinitis, NASAL POLYPS Unusually severe chest deformity Fixed monophonic wheeze, stridor, asymmetrical signs Signs of cardiac or systemic disease
16 Everyone happy? No treatment without a diagnosis What are the possibilities lessons from pathology Cui bono? (or for the classically challenged, who s it all for?) Summary and conclusions
17 Symptom Patterns Episodic (viral) wheeze Wheeze in association with (usually) clinically diagnosed viral URTI NOT the same as transient wheeze (Colt Ashford) Multi-trigger wheeze Wheeze both with viral URTI and with other triggers between URTIs Not the same as multiple trigger wheeze BUT PLEASE NOTE Phenotypes may not be stable (nor is any form of childhood asthma) There may be overlaps Parents may not appreciate interval symptoms



18
19 What about Pathology Helsinki Cohort Infants 3-26 months sgaw and BDR Clinically indicated rigid bronchoscopy A (reduced sgaw, BDR, n=16); B (reduced sgaw, no BDR, n=22); C (normal sgaw, n=15) RBH Cohort Children age 7-58 months Video-questionnaire (confirmed vs. reported vs. none) Clinically indicated FOB Confirmed wheeze (n=16), reported (unconfirmed) wheeze (n=14), control (n=10)

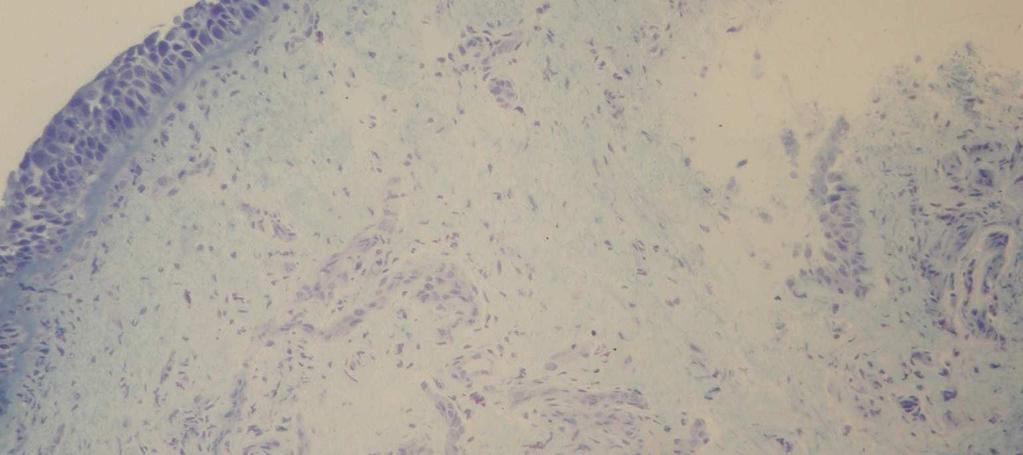
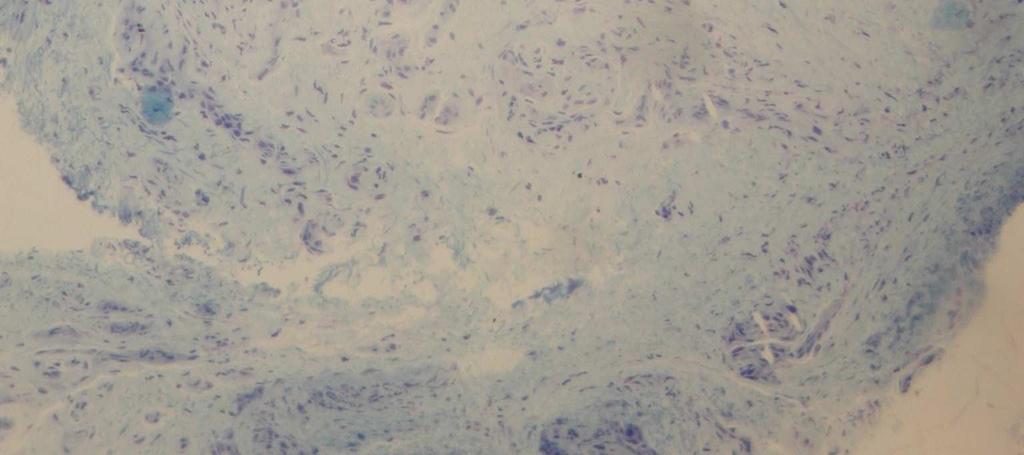
20
21 Infants (median age 1 year) Preschool children (median age 3 years) Eosinophils (%) Reversible airflow obstruction NS Normal lung function EG2 volume density (%) Confirmed wheeze p < 0.05 Controls 10.0 NS 10.0 p < 0.01 RBM (µm) RBM (µm) Reversible airflow obstruction Normal lung function 0.0 Confirmed wheeze Controls Saglani et al AJRCCM 2005 Saglani et al AJRCCM 2007
22 EVW & MTW: Different Pathology Severe pre-school wheezers divided on history into: Episodic viral wheeze (EVW) Multiple trigger wheeze (MTW) Controls EG2+ volume density (%) 4 * VW IW Ctrl EVW MTW Controls RBM thickness (µm) VW IW Ctrl EVW MTW Controls *
23 Symptom Patterns Episodic (viral) wheeze Wheeze in association with (usually) clinically diagnosed viral URTI NOT the same as transient wheeze! NO eosinophilic inflammation ICS???? Multi-trigger wheeze Wheeze both with viral URTI and with other triggers between URTIs NOT the same as persistent wheeze! Eosinophilia and remodelling ICS!
24 Everyone happy? No treatment without a diagnosis What are the possibilities lessons from pathology Cui bono? (or for the classically challenged, who s it all for?) Summary and conclusions



25 Wheeze Treatment For All: More than just medications What else is inhaled? Where is medicine going?
26 Indications for Treatment Prevention of disease progression Cannot intervene SO, treat ONLY if symptoms mandate treatment Treatment of symptoms: what CAN be given Nothing Bronchodilators (β-2 agonist, anticholinergics) LTRAs (3 studies, conflicting results) Inhaled corticosteroids Oral Corticosteroids
27 Intermittent ICS 129 children age 1-6 years FP 750 mcg bd vs. placebo with acute episodic (viral) wheeze In 40 weeks, 8% FP vs. 18% placebo were given prednisolone (43 vs. 93; OR 0.49, ) BUT: SAFETY 10% children have > 10 colds/year There was a growth effect (-0.24 Z score) Adrenal function only crudely assessed NEJM 2009; 360:
28 Intermittent vs. Continuous ICS 278 children aged months randomised +ve modified API Nebulised budesonide (only FDA approved ICS in preschoolers!) Regimens: I mg neb BUD for 7 days with URTI (n=139) 0.5 mg BUD neb regularly (n=139) NO PLACEBO LIMB! N Engl J Med 2011; 365:

29
30 What have we learned? Continuous BUD does Not prevent exacerbations Not make them any less severe Not lead to any less acute treatment Does increase the steroid dose taken BUT, this does not tell us whether intermittent BUD was at all helpful!
31 Episodic Treatment for Episodic problems (if needed) FIRST CHOICE: Nothing SECOND CHOICE: Intermittent bronchodilators THIRD CHOICE: Intermittent LTRA Potentially safer than ICS Fourth: Intermittent high dose ICS Dose and duration unknown, MONITOR carefully COUNCIL OF DESPAIR: Cmbination therapy Evidence base = zero
32 Oral Prednisolone Parent-initiated 217 children, already one admission Hospital-initiated 687 children (atopy NOT an exclusion) Parent initiated treatment at next exacerbation No benefit seen Clinically diagnosed acute viral wheeze Time to hospital discharge Lancet 2003; 362: NEJM 2009; 360:
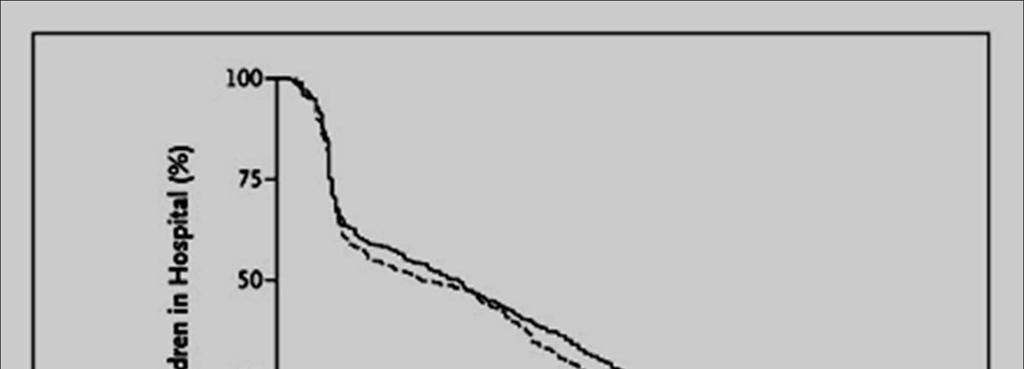
33 Prednisolone: Ineffective
34 Episodic (viral) Wheeze: The role of Prednisolone NOT a community medication NOT a routine 2 ry care medication (Possibly) multi-trigger wheeze with a severe exacerbation (Possibly) any severe episodic (viral) wheeze heading for PICU
35 Preschool Wheeze 3 steps USUALLY ONLY IN MULTIPLE - TRIGGER WHEEZE Step 1 Inhaled BUD 400 mcg bd OR, montelukast 4 mg od Step 2 Stop treatment after c. 8 weeks Step 3 (Only if response to Step 1) Restart BUD, titrate to lowest dose OR, restart montelukast
36 Everyone happy? No treatment without a diagnosis What are the possibilities lessons from pathology Cui bono? (or for the classically challenged, who s it all for?) Summary and conclusions
37 What OUGHT to be done? Unhappy child, unhappy parent Treat child along standard lines Happy child, unhappy parent: Find out WHY! Fear of a diagnosis? Overanxious? Disruptive symptoms? Is it right to give medications which may be ineffective to a child when the parent has the problem? 2nd opinion? Unhappy Dr Phone a friend!
38 Everyone happy? No treatment without a diagnosis What are the possibilities lessons from pathology Cui bono? (or for the classically challenged, who s it all for?) Summary and conclusions
39 Take Home Messages Make sure it is wheeze; make sure you are not missing a diagnosis (history and examination) Classify pre-school wheeze as episodic (viral) and multi-trigger There are no disease-modifying therapies, so treat episodic symptoms episodically (if they need treatment!) Do NOT use oral corticosteroids for pre-school episodic (viral) wheeze Only treat the child if the CHILD needs treatment If the parents need treatment, find out why and what And if YOU are unhappy, GET A SECOND OPINION

40 Thank you for listening!
Recent advances in the management of pre-school wheeze
 Recent advances in the management of pre-school wheeze A Bush Abstract Pre-school wheeze is very common and often difficult to treat. Most children do not require any investigations, only a detailed history
Recent advances in the management of pre-school wheeze A Bush Abstract Pre-school wheeze is very common and often difficult to treat. Most children do not require any investigations, only a detailed history
Management of wheeze in pre-school children. Prof Colin Robertson, Respiratory Medicine, Royal Children s Hospital, Melbourne
 Management of wheeze in pre-school children Prof Colin Robertson, Respiratory Medicine, Royal Children s Hospital, Melbourne General Practitioner encounters for asthma Asthma in Australia, 2003 Emergency
Management of wheeze in pre-school children Prof Colin Robertson, Respiratory Medicine, Royal Children s Hospital, Melbourne General Practitioner encounters for asthma Asthma in Australia, 2003 Emergency
Outcome, classification and management of wheezing in preschool children Paul L.P. Brand
 Outcome, classification and management of wheezing in preschool children Paul L.P. Brand Princess Amalia Children s Clinic Isala klinieken, Zwolle the Netherlands p.l.p.brand@isala.nl Valle de la Luna,
Outcome, classification and management of wheezing in preschool children Paul L.P. Brand Princess Amalia Children s Clinic Isala klinieken, Zwolle the Netherlands p.l.p.brand@isala.nl Valle de la Luna,
Practical Approach to Managing Paediatric Asthma
 Practical Approach to Managing Paediatric Asthma Dr Andrew Tai FRACP, PhD Paediatric Respiratory and Sleep Specialist Women's and Children's Hospital, Adelaide Approaching the patient Check the diagnosis
Practical Approach to Managing Paediatric Asthma Dr Andrew Tai FRACP, PhD Paediatric Respiratory and Sleep Specialist Women's and Children's Hospital, Adelaide Approaching the patient Check the diagnosis
Recurrent Wheezing in Preschool Children. William Sheehan, MD Associate Professor of Pediatrics Division of Allergy and Immunology
 Recurrent Wheezing in Preschool Children William Sheehan, MD Associate Professor of Pediatrics Division of Allergy and Immunology Disclosure I have nothing to disclose related to this talk. Background
Recurrent Wheezing in Preschool Children William Sheehan, MD Associate Professor of Pediatrics Division of Allergy and Immunology Disclosure I have nothing to disclose related to this talk. Background
WHEEZING IN INFANCY: IS IT ASTHMA?
 WHEEZING IN INFANCY: IS IT ASTHMA? Jittlada Deerojanawong Department of Pediatrics, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand Wheezing is common symptoms throughout infancy and childhood
WHEEZING IN INFANCY: IS IT ASTHMA? Jittlada Deerojanawong Department of Pediatrics, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand Wheezing is common symptoms throughout infancy and childhood
Preschool Wheeze. AC Jeevarathnum 04/03/16. Paediatric Pulmonologist Steve Biko Academic Hospital
 Preschool Wheeze AC Jeevarathnum Paediatric Pulmonologist Steve Biko Academic Hospital MBBCh FcPaed(SA) MMED Dip Allergy(SA) Cert Pulm(Paed)(SA) European Respiratory Diploma 04/03/16 Overview Introduction
Preschool Wheeze AC Jeevarathnum Paediatric Pulmonologist Steve Biko Academic Hospital MBBCh FcPaed(SA) MMED Dip Allergy(SA) Cert Pulm(Paed)(SA) European Respiratory Diploma 04/03/16 Overview Introduction
Tips on managing asthma in children
 Tips on managing asthma in children Dr Ranjan Suri Consultant in Respiratory Paediatrics Bupa Cromwell Hospital Clinics: Friday (pm) Asthma in Children Making the diagnosis Patterns of childhood asthma
Tips on managing asthma in children Dr Ranjan Suri Consultant in Respiratory Paediatrics Bupa Cromwell Hospital Clinics: Friday (pm) Asthma in Children Making the diagnosis Patterns of childhood asthma
Prof Neil Barnes. Respiratory and General Medicine London Chest Hospital and The Royal London Hospital
 Prof Neil Barnes Respiratory and General Medicine London Chest Hospital and The Royal London Hospital ASTHMA: WHEN EVERYTHING FAILS WHAT DO YOU DO? South GP CME 2013, Dunedin Saturday 17 th August 2013
Prof Neil Barnes Respiratory and General Medicine London Chest Hospital and The Royal London Hospital ASTHMA: WHEN EVERYTHING FAILS WHAT DO YOU DO? South GP CME 2013, Dunedin Saturday 17 th August 2013
Alberta Childhood Asthma Pathway for Primary Care
 Asthma Diagnosis Box 1 Diagnosis: Based on symptom pattern, careful and thorough history of symptoms (wheeze, cough, night waking and activity limitations), and assessment of family history of asthma and
Asthma Diagnosis Box 1 Diagnosis: Based on symptom pattern, careful and thorough history of symptoms (wheeze, cough, night waking and activity limitations), and assessment of family history of asthma and
COPD and Asthma: Similarities and differences Prof. Peter Barnes
 and Asthma: Similarities and Differences and Asthma: 1 Imperial College Peter Barnes FRS, FMedSci, National Heart & Lung Institute Imperial College, London, UK p.j.barnes@imperial.ac.uk Royal Brompton
and Asthma: Similarities and Differences and Asthma: 1 Imperial College Peter Barnes FRS, FMedSci, National Heart & Lung Institute Imperial College, London, UK p.j.barnes@imperial.ac.uk Royal Brompton
Bronchial Provocation Results: What Does It Mean?
 Bronchial Provocation Results: What Does It Mean? Greg King 1 Department of Respiratory Medicine, Royal North Shore Hospital, St Leonards 2065 2 Woolcock Institute of Medical Research and Sydney Medical
Bronchial Provocation Results: What Does It Mean? Greg King 1 Department of Respiratory Medicine, Royal North Shore Hospital, St Leonards 2065 2 Woolcock Institute of Medical Research and Sydney Medical
Predicting, Preventing and Managing Asthma Exacerbations. Heather Zar Department of Paediatrics & Child Health University of Cape Town South Africa
 Predicting, Preventing and Managing Asthma Exacerbations Heather Zar Department of Paediatrics & Child Health University of Cape Town South Africa Asthma exacerbations Predicting exacerbation recognising
Predicting, Preventing and Managing Asthma Exacerbations Heather Zar Department of Paediatrics & Child Health University of Cape Town South Africa Asthma exacerbations Predicting exacerbation recognising
Paediatric Update. Pre-School Wheeze: Decrees and pleas for the under three s. Julian Vyas Respiratory Paediatrician STARSHIP HOSPITAL
 Pre-School Wheeze: Decrees and pleas for the under three s Julian Vyas Respiratory Paediatrician STARSHIP HOSPITAL 8th July 2015 No Conflicts of Interest to Declare what is wheeze? Definition: A wheeze
Pre-School Wheeze: Decrees and pleas for the under three s Julian Vyas Respiratory Paediatrician STARSHIP HOSPITAL 8th July 2015 No Conflicts of Interest to Declare what is wheeze? Definition: A wheeze
RESPIRATORY CARE IN GENERAL PRACTICE
 RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
WEBINAR. Difficult-to-treat and severe asthma: changing the paradigm
 WEBINAR Difficult-to-treat and severe asthma: changing the paradigm A multidisciplinary discussion on new therapies, and how to identify and manage difficult-to-treat and severe asthma DIFFICULT-TO-TREAT
WEBINAR Difficult-to-treat and severe asthma: changing the paradigm A multidisciplinary discussion on new therapies, and how to identify and manage difficult-to-treat and severe asthma DIFFICULT-TO-TREAT
Allwin Mercer Dr Andrew Zurek
 Allwin Mercer Dr Andrew Zurek 1 in 11 people are currently receiving treatment for asthma (5.4 million people in the UK) Every 10 seconds, someone is having a potentially life-threatening asthma attack
Allwin Mercer Dr Andrew Zurek 1 in 11 people are currently receiving treatment for asthma (5.4 million people in the UK) Every 10 seconds, someone is having a potentially life-threatening asthma attack
Chronic Cough. Dr Peter George Consultant Respiratory Physician Royal Brompton and Harefield Hospitals
 Chronic Cough Dr Peter George Consultant Respiratory Physician Royal Brompton and Harefield Hospitals Overview Common causes of chronic cough Important diagnoses not to miss How to investigate a cough
Chronic Cough Dr Peter George Consultant Respiratory Physician Royal Brompton and Harefield Hospitals Overview Common causes of chronic cough Important diagnoses not to miss How to investigate a cough
Preschool Asthma What you need to know in 10 minutes
 Preschool Asthma What you need to know in 10 minutes Alan Kaplan MD CCFP(EM) FCFP Family Physician Airways Group of Canada Respiratory Medicine section CFPC Faculty/Presenter Disclosure Faculty: Alan Kaplan
Preschool Asthma What you need to know in 10 minutes Alan Kaplan MD CCFP(EM) FCFP Family Physician Airways Group of Canada Respiratory Medicine section CFPC Faculty/Presenter Disclosure Faculty: Alan Kaplan
Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma
 Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma Magnitude of Asthma - India Delhi Childhood asthma: 10.9% Adults: 8% Other Cities 3 to 18% Chhabra SK et al Ann Allergy Asthma
Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma Magnitude of Asthma - India Delhi Childhood asthma: 10.9% Adults: 8% Other Cities 3 to 18% Chhabra SK et al Ann Allergy Asthma
Wheeze. Dr Jo Harrison
 Wheeze Dr Jo Harrison 9.9.14 Wheeze - Physiology a continuous musical sound that lasts longer than 250 msec. can be high-pitched or low-pitched, consist of single or multiple notes, and occur during inspiration
Wheeze Dr Jo Harrison 9.9.14 Wheeze - Physiology a continuous musical sound that lasts longer than 250 msec. can be high-pitched or low-pitched, consist of single or multiple notes, and occur during inspiration
11/15/2017. Highgate Private Hospital (Royal Free London NHS Foundation Trust) Causes of chronic cough
 Causes of chronic cough") A whistle stop of Chronic Cough For 10min consultations.. Dr Dean Creer Consultant Chest Physician (MBChB, FRCP) Highgate Private Hospital (Royal Free London NHS Foundation Trust) E: drcreer.pa@gmail.com(secretary)
A whistle stop of Chronic Cough For 10min consultations.. Dr Dean Creer Consultant Chest Physician (MBChB, FRCP) Highgate Private Hospital (Royal Free London NHS Foundation Trust) E: drcreer.pa@gmail.com(secretary)
Update on management of respiratory symptoms. Dr Farid Bazari Consultant Respiratory Physician Kingston Hospital NHS FT
 Update on management of respiratory symptoms Dr Farid Bazari Consultant Respiratory Physician Kingston Hospital NHS FT Topics The common respiratory symptoms Cough: causes, diagnosis and therapy Update
Update on management of respiratory symptoms Dr Farid Bazari Consultant Respiratory Physician Kingston Hospital NHS FT Topics The common respiratory symptoms Cough: causes, diagnosis and therapy Update
TREAMENT OF RECURRENT VIRUS-INDUCED WHEEZING IN YOUNG CHILDREN. Dr Lại Lê Hưng Respiratory Department
 TREAMENT OF RECURRENT VIRUS-INDUCED WHEEZING IN YOUNG CHILDREN Dr Lại Lê Hưng Respiratory Department Literature review current through: Feb 2013. This topic last updated: Aug 14, 2012 INTRODUCTION Wheezing
TREAMENT OF RECURRENT VIRUS-INDUCED WHEEZING IN YOUNG CHILDREN Dr Lại Lê Hưng Respiratory Department Literature review current through: Feb 2013. This topic last updated: Aug 14, 2012 INTRODUCTION Wheezing
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss?
 ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
Distinction and Overlap. Allergy Dpt, 2 nd Pediatric Clinic, University of Athens
 Asthma Phenotypes: Distinction and Overlap Nikos Papadopoulos Allergy Dpt, 2 nd Pediatric Clinic, University of Athens Asthma as a syndrome From the Iliad to ADAM 33 and back again Bronchoconstriction,
Asthma Phenotypes: Distinction and Overlap Nikos Papadopoulos Allergy Dpt, 2 nd Pediatric Clinic, University of Athens Asthma as a syndrome From the Iliad to ADAM 33 and back again Bronchoconstriction,
Wheeze. Respiratory Tract Symptoms. Prof RJ Green Department of Paediatrics. Cough. Wheeze/noisy breathing. Acute. Tight chest. Shortness of breath
 Wheeze Prof RJ Green Department of Paediatrics Respiratory Tract Symptoms Cough Tight chest Wheeze/noisy breathing Shortness of breath Acute Chronic Respiratory rate Most important sign of respiratory
Wheeze Prof RJ Green Department of Paediatrics Respiratory Tract Symptoms Cough Tight chest Wheeze/noisy breathing Shortness of breath Acute Chronic Respiratory rate Most important sign of respiratory
Asthma COPD Overlap (ACO)
") Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
ADULT ASTHMA GUIDE SUMMARY. This summary provides busy health professionals with key guidance for assessing and treating adult asthma.
 ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
Understanding Cough, Wheezing and Noisy Breathing in Children. Introduction
 Understanding Cough, Wheezing and Noisy Breathing in Children Introduction Symptoms such as cough, wheezing or noisy breathing can be caused by a number of conditions. When these occur, it is natural for
Understanding Cough, Wheezing and Noisy Breathing in Children Introduction Symptoms such as cough, wheezing or noisy breathing can be caused by a number of conditions. When these occur, it is natural for
Paediatric Wheeze and pneumonia. RCH Asthma RCH bronchiolitis RCH pneumonia Dr S Rajapaksa
 Paediatric Wheeze and pneumonia RCH Asthma RCH bronchiolitis RCH pneumonia Dr S Rajapaksa Case Charlotte is a 2 ½ year old who presents to ED with shortness of breath and wheeze. She had been picked up
Paediatric Wheeze and pneumonia RCH Asthma RCH bronchiolitis RCH pneumonia Dr S Rajapaksa Case Charlotte is a 2 ½ year old who presents to ED with shortness of breath and wheeze. She had been picked up
Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007
 Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Selecting Initial Therapy
Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Selecting Initial Therapy
ASTHMA. Epidemiology. Pathophysiology. Diagnosis. IAP UG Teaching slides
 BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
NG80. Asthma: diagnosis, monitoring and chronic asthma management (NG80)
") Asthma: diagnosis, monitoring and chronic asthma management (NG80) NG80 NICE has checked the use of its content in this product and the sponsor has had no influence on the content of this booklet. NICE
Asthma: diagnosis, monitoring and chronic asthma management (NG80) NG80 NICE has checked the use of its content in this product and the sponsor has had no influence on the content of this booklet. NICE
Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016
 Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016 Diagnosis: There is no lower limit to the age at which
Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016 Diagnosis: There is no lower limit to the age at which
Acute Wheezing Emergencies: From Young to Old! Little Wheezers in the ED: Managing Acute Pediatric Asthma
 Acute Wheezing Emergencies: From Young to Old! Little Wheezers in the ED: Managing Acute Pediatric Asthma Talk Outline Case Delivery of bronchodilators Meter-dose inhalers and spacers Continuous nebulization
Acute Wheezing Emergencies: From Young to Old! Little Wheezers in the ED: Managing Acute Pediatric Asthma Talk Outline Case Delivery of bronchodilators Meter-dose inhalers and spacers Continuous nebulization
Scegliere con cura per... l Asma bronchiale
 Scegliere con cura per... l Asma bronchiale Salvatore Cazzato Pneumologia Pediatrica UO Pediatria-Dir. A Pession Azienda Ospedaliero-Universitaria Policlinico S. Orsola-Malpighi Bologna Recurrent episodes
Scegliere con cura per... l Asma bronchiale Salvatore Cazzato Pneumologia Pediatrica UO Pediatria-Dir. A Pession Azienda Ospedaliero-Universitaria Policlinico S. Orsola-Malpighi Bologna Recurrent episodes
I have no perceived conflicts of interest or commercial relationships to disclose.
 ASTHMA BASICS Michelle Dickens RN FNP-C AE-C Nurse Practitioner/Certified Asthma Educator Ferrell Duncan Allergy/Asthma/Immunology Coordinator, CoxHealth Asthma Center DISCLOSURES I have no perceived conflicts
ASTHMA BASICS Michelle Dickens RN FNP-C AE-C Nurse Practitioner/Certified Asthma Educator Ferrell Duncan Allergy/Asthma/Immunology Coordinator, CoxHealth Asthma Center DISCLOSURES I have no perceived conflicts
COUGH. Jim Reid University of Otago Medical School Dunedin, New Zealand
 COUGH Jim Reid University of Otago Medical School Dunedin, New Zealand COUGH One of five most common presentations in general practice Remember the law of probability Common things occur commonly But
COUGH Jim Reid University of Otago Medical School Dunedin, New Zealand COUGH One of five most common presentations in general practice Remember the law of probability Common things occur commonly But
Chronic Cough An Unusual Presentation. Dr Sourabh Jain Department of Respiratory Medicine
 Chronic Cough An Unusual Presentation Dr Sourabh Jain Department of Respiratory Medicine A 72 years old male from Pune, non smoker, with no co-morbidities Chief Complaints : Chronic cough with scanty mucoid
Chronic Cough An Unusual Presentation Dr Sourabh Jain Department of Respiratory Medicine A 72 years old male from Pune, non smoker, with no co-morbidities Chief Complaints : Chronic cough with scanty mucoid
Management of the Symptomatic PCD
 Management of the Symptomatic PCD Andrew Bush MD FRCP FRCPCH FERS Imperial College & Royal Brompton Hospital a.bush@imperial.ac.uk Conflict of Interest AB has no financial or other COI There will be discussion
Management of the Symptomatic PCD Andrew Bush MD FRCP FRCPCH FERS Imperial College & Royal Brompton Hospital a.bush@imperial.ac.uk Conflict of Interest AB has no financial or other COI There will be discussion
(Asthma) Diagnosis, monitoring and chronic asthma management
 Diagnosis, monitoring and chronic asthma management") Dubai Standards of Care 2018 (Asthma) Diagnosis, monitoring and chronic asthma management Preface Asthma is one of the most common problem dealt with in daily practice. In Dubai, the management of chronic
Dubai Standards of Care 2018 (Asthma) Diagnosis, monitoring and chronic asthma management Preface Asthma is one of the most common problem dealt with in daily practice. In Dubai, the management of chronic
Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007
 Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Selecting Initial Therapy
Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Selecting Initial Therapy
Improving Outcomes in the Management & Treatment of Asthma. April 21, Spring Managed Care Forum
 Improving Outcomes in the Management & Treatment of Asthma April 21, 2016 2016 Spring Managed Care Forum David M. Mannino, M.D. Professor Department of Preventive Medicine and Environmental Health University
Improving Outcomes in the Management & Treatment of Asthma April 21, 2016 2016 Spring Managed Care Forum David M. Mannino, M.D. Professor Department of Preventive Medicine and Environmental Health University
Air Flow Limitation. In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation.
 Asthma Air Flow Limitation In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation. True whether reversible, asthma and exercise-induced bronchospasm,
Asthma Air Flow Limitation In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation. True whether reversible, asthma and exercise-induced bronchospasm,
On completion of this chapter you should be able to: discuss the stepwise approach to the pharmacological management of asthma in children
 7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
UNUSUAL CAUSE OF ADRENAL INSUFFICIENCY. Dr.Khushboo Dr.S.Balasubramanian s unit
 UNUSUAL CAUSE OF ADRENAL INSUFFICIENCY Dr.Khushboo Dr.S.Balasubramanian s unit BRIEF HISTORY 7 year old male child presented with Fever : 3 days Vomiting : 3 days h/0 Acute encephalopathy with fever O/E
UNUSUAL CAUSE OF ADRENAL INSUFFICIENCY Dr.Khushboo Dr.S.Balasubramanian s unit BRIEF HISTORY 7 year old male child presented with Fever : 3 days Vomiting : 3 days h/0 Acute encephalopathy with fever O/E
The child with a troublesome cough. Dr Marco Zampoli Paediatric Pulmonology Red Cross War Memorial Children s Hospital GP Refresher Course 2012
 The child with a troublesome cough Dr Marco Zampoli Paediatric Pulmonology Red Cross War Memorial Children s Hospital GP Refresher Course 2012 Cough is the most common symptom in children Inability to
The child with a troublesome cough Dr Marco Zampoli Paediatric Pulmonology Red Cross War Memorial Children s Hospital GP Refresher Course 2012 Cough is the most common symptom in children Inability to
Using Patient Characteristics to Individualize and Improve Asthma Care
 Using Patient Characteristics to Individualize and Improve Asthma Care Leonard B. Bacharier, M.D. Associate Professor of Pediatrics Clinical Director, Division of Allergy, Immunology, & Pulmonary Medicine
Using Patient Characteristics to Individualize and Improve Asthma Care Leonard B. Bacharier, M.D. Associate Professor of Pediatrics Clinical Director, Division of Allergy, Immunology, & Pulmonary Medicine
Assessing wheeze in pre-school children
 Assessing wheeze in pre-school children 8 Wheeze in children aged less than five years has many potential causes. Often it is regarded as the first sign of asthma, however, a substantial proportion of
Assessing wheeze in pre-school children 8 Wheeze in children aged less than five years has many potential causes. Often it is regarded as the first sign of asthma, however, a substantial proportion of
Asthma - Chronic. Presentations of asthma Cough Wheeze Breathlessness Chest tightness
 Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
GINA. At-A-Glance Asthma Management Reference. for adults, adolescents and children 6 11 years. Updated 2017
 GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
Asthma and COPD in older people lumping or splitting? Christine Jenkins Concord Hospital Woolcock Institute of Medical Research
 Asthma and COPD in older people lumping or splitting? Christine Jenkins Concord Hospital Woolcock Institute of Medical Research Concord Hospital Woolcock Institute of Medical Research Joe has asthma What
Asthma and COPD in older people lumping or splitting? Christine Jenkins Concord Hospital Woolcock Institute of Medical Research Concord Hospital Woolcock Institute of Medical Research Joe has asthma What
Asthma Update A/Prof. John Abisheganaden. Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital
 Asthma Update - 2013 A/Prof. John Abisheganaden Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital Asthma A complex syndrome Multifaceted disease Heterogeneous Genetic and
Asthma Update - 2013 A/Prof. John Abisheganaden Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital Asthma A complex syndrome Multifaceted disease Heterogeneous Genetic and
Pathway diagrams Annex F
 Pathway diagrams Annex F Fig 1 Asthma: The patient journey Asthma is diagnosed Making the diagnosis of asthma Confirming the diagnosis may depend on history, response to treatment, measurement of airflow
Pathway diagrams Annex F Fig 1 Asthma: The patient journey Asthma is diagnosed Making the diagnosis of asthma Confirming the diagnosis may depend on history, response to treatment, measurement of airflow
What s new in COPD? Apichart Khanichap MD. Department of Medicine, Faculty of Medicine, Thammasat university
 What s new in COPD? Apichart Khanichap MD. Department of Medicine, Faculty of Medicine, Thammasat university Management stable COPD Relieve symptoms Improve exercise tolerance Improve health status Prevent
What s new in COPD? Apichart Khanichap MD. Department of Medicine, Faculty of Medicine, Thammasat university Management stable COPD Relieve symptoms Improve exercise tolerance Improve health status Prevent
Clinical Implications of Asthma Phenotypes. Michael Schatz, MD, MS Department of Allergy
 Clinical Implications of Asthma Phenotypes Michael Schatz, MD, MS Department of Allergy Definition of Phenotype The observable properties of an organism that are produced by the interaction of the genotype
Clinical Implications of Asthma Phenotypes Michael Schatz, MD, MS Department of Allergy Definition of Phenotype The observable properties of an organism that are produced by the interaction of the genotype
Optimising the management of wheeze in preschool children
 Optimising the management of wheeze in preschool children McVea S, Bourke T. Optimising the management of wheeze in preschool children. Practitioner 2016;260(1794):11-14 Dr Steven McVea MB BCh BAO MRCPCH
Optimising the management of wheeze in preschool children McVea S, Bourke T. Optimising the management of wheeze in preschool children. Practitioner 2016;260(1794):11-14 Dr Steven McVea MB BCh BAO MRCPCH
ASTHMA RESOURCE PACK Section 3. Chronic Cough Guidelines
 ASTHMA RESOURCE PACK Section 3 Chronic Cough Guidelines NHS Fife Guidelines for the Management of Chronic Cough in Adults In this section: 1. Introduction 2. Scope Guidelines for Management of Chronic
ASTHMA RESOURCE PACK Section 3 Chronic Cough Guidelines NHS Fife Guidelines for the Management of Chronic Cough in Adults In this section: 1. Introduction 2. Scope Guidelines for Management of Chronic
Greater Manchester Asthma Management Plan 2018 Inhaler therapy options for adult patients (18 and over) with asthma
 with asthma") Greater Manchester Asthma Management Plan 2018 Inhaler therapy options for adult patients (18 and over) with asthma Non-pharmacological options for ALL patients, consider at ALL stages Make sure diagnosis
Greater Manchester Asthma Management Plan 2018 Inhaler therapy options for adult patients (18 and over) with asthma Non-pharmacological options for ALL patients, consider at ALL stages Make sure diagnosis
Respiratory Subcommittee of PTAC meeting held 5 February (minutes for web publishing)
") Respiratory Subcommittee of PTAC meeting held 5 February 2010 (minutes for web publishing) Respiratory Subcommittee minutes are published in accordance with the Terms of Reference for the Pharmacology
Respiratory Subcommittee of PTAC meeting held 5 February 2010 (minutes for web publishing) Respiratory Subcommittee minutes are published in accordance with the Terms of Reference for the Pharmacology
Asthma: diagnosis and monitoring
 Asthma: diagnosis and monitoring NICE guideline: short version Draft for second consultation, July 01 This guideline covers assessing, diagnosing and monitoring suspected or confirmed asthma in adults,
Asthma: diagnosis and monitoring NICE guideline: short version Draft for second consultation, July 01 This guideline covers assessing, diagnosing and monitoring suspected or confirmed asthma in adults,
Cynthia S. Kelly, M.D. Professor of Pediatrics Eastern Virginia Medical School Division Director Allergy Children s Hospital of The King s Daughters
 Cynthia S. Kelly, M.D. Professor of Pediatrics Eastern Virginia Medical School Division Director Allergy Children s Hospital of The King s Daughters Disclosures Speakers bureau of Novartis and Genentech
Cynthia S. Kelly, M.D. Professor of Pediatrics Eastern Virginia Medical School Division Director Allergy Children s Hospital of The King s Daughters Disclosures Speakers bureau of Novartis and Genentech
Asthma and Vocal Cord Dysfunction
 Asthma and Vocal Cord Dysfunction Amy L. Marks DO, FACOP Pediatric Allergy and Immunology Assistant Professor of Pediatrics Oakland University William Beaumont School of Medicine Objectives: Understanding
Asthma and Vocal Cord Dysfunction Amy L. Marks DO, FACOP Pediatric Allergy and Immunology Assistant Professor of Pediatrics Oakland University William Beaumont School of Medicine Objectives: Understanding
Get Healthy Stay Healthy
 Asthma Management WHAT IS ASTHMA? Asthma causes swelling and inflammation in the breathing passages that lead to your lungs. When asthma flares up, the airways tighten and become narrower. This keeps the
Asthma Management WHAT IS ASTHMA? Asthma causes swelling and inflammation in the breathing passages that lead to your lungs. When asthma flares up, the airways tighten and become narrower. This keeps the
ASTHMA. Dr Liz Gamble BRI
 ASTHMA Dr Liz Gamble BRI Diagnosis Clinical: wheeze, breathlessness, chest tightness, cough Variable airflow obstruction: peak flow chart, spirometry with reversibility to bronchodilators Airways hyper-responsiveness
ASTHMA Dr Liz Gamble BRI Diagnosis Clinical: wheeze, breathlessness, chest tightness, cough Variable airflow obstruction: peak flow chart, spirometry with reversibility to bronchodilators Airways hyper-responsiveness
Interventions to improve adherence to inhaled steroids for asthma. Respiratory department
 Interventions to improve adherence to inhaled steroids for asthma Respiratory department Content Overview Research References Overview Asthma is a chronic breathing condition that affects more than 300
Interventions to improve adherence to inhaled steroids for asthma Respiratory department Content Overview Research References Overview Asthma is a chronic breathing condition that affects more than 300
Allergy and Immunology Review Corner: Chapter 75 of Middleton s Allergy Principles and Practice, 7 th Edition, edited by N. Franklin Adkinson, et al.
 Allergy and Immunology Review Corner: Chapter 75 of Middleton s Allergy Principles and Practice, 7 th Edition, edited by N. Franklin Adkinson, et al. Chapter 75: Approach to Infants and Children with Asthma
Allergy and Immunology Review Corner: Chapter 75 of Middleton s Allergy Principles and Practice, 7 th Edition, edited by N. Franklin Adkinson, et al. Chapter 75: Approach to Infants and Children with Asthma
The Acute & Maintenance Treatment of Asthma via Aerosolized Medications
 The Acute & Maintenance Treatment of Asthma via Aerosolized Medications Douglas S. Gardenhire, EdD, RRT-NPS, FAARC Associate Professor and Chairman Department of Respiratory Therapy Objectives Define Asthma.
The Acute & Maintenance Treatment of Asthma via Aerosolized Medications Douglas S. Gardenhire, EdD, RRT-NPS, FAARC Associate Professor and Chairman Department of Respiratory Therapy Objectives Define Asthma.
Asthma: Classification, Management, Prevention and New Treatments
 Asthma: Classification, Management, Prevention and New Treatments Cori Daines, MD, Professor Pediatric Pulmonary Medicine University of Arizona April 28, 2018 I have no relevant financial relationships
Asthma: Classification, Management, Prevention and New Treatments Cori Daines, MD, Professor Pediatric Pulmonary Medicine University of Arizona April 28, 2018 I have no relevant financial relationships
Asthma in Pediatric Patients. DanThuy Dao, D.O., FAAP. Disclosures. None
 Asthma in Pediatric Patients DanThuy Dao, D.O., FAAP Disclosures None Objectives 1. Discuss the evaluation and management of asthma in a pediatric patient 2. Accurately assess asthma severity and level
Asthma in Pediatric Patients DanThuy Dao, D.O., FAAP Disclosures None Objectives 1. Discuss the evaluation and management of asthma in a pediatric patient 2. Accurately assess asthma severity and level
Asthma Care in the Emergency Department Clinical Practice Guideline
 Asthma Care in the Emergency Department Clinical Practice Guideline Inclusion: 1) Children 2 years of age or older with a prior history of wheezing, and 2) Children less than 2 years of age with likely
Asthma Care in the Emergency Department Clinical Practice Guideline Inclusion: 1) Children 2 years of age or older with a prior history of wheezing, and 2) Children less than 2 years of age with likely
Significance. Asthma Definition. Focus on Asthma
 Focus on Asthma (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Asthma Definition Chronic inflammatory disorder of airways Causes airway hyperresponsiveness
Focus on Asthma (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Asthma Definition Chronic inflammatory disorder of airways Causes airway hyperresponsiveness
Global Initiative for Asthma (GINA) What s new in GINA 2017?
 What s new in GINA 2017?") Global Initiative for Asthma (GINA) GINA Global Strategy for Asthma Management and Prevention Asthma-COPD overlap The word syndrome has been removed from the previous term asthma-copd overlap syndrome
Global Initiative for Asthma (GINA) GINA Global Strategy for Asthma Management and Prevention Asthma-COPD overlap The word syndrome has been removed from the previous term asthma-copd overlap syndrome
Breakfast Session Prof Neil Barnes Professor of Respiratory Medicine London Chest Hospital & The Royal London Hospital United Kingdom
 Breakfast Session Prof Neil Barnes Professor of Respiratory Medicine London Chest Hospital & The Royal London Hospital United Kingdom 2 BEYOND SYMPTOMS ADDRESSING FUTURE RISK IN ASTHMA South GP CME 2013,
Breakfast Session Prof Neil Barnes Professor of Respiratory Medicine London Chest Hospital & The Royal London Hospital United Kingdom 2 BEYOND SYMPTOMS ADDRESSING FUTURE RISK IN ASTHMA South GP CME 2013,
Evaluating a child with recurrent cough and nighttime symptoms
 Evaluating a child with recurrent cough and nighttime symptoms CATHERINE KIER, MD Professor of Clinical Pediatrics Division Chief, Pediatric Pulmonary, and Cystic Fibrosis Center Director, Pediatric Sleep
Evaluating a child with recurrent cough and nighttime symptoms CATHERINE KIER, MD Professor of Clinical Pediatrics Division Chief, Pediatric Pulmonary, and Cystic Fibrosis Center Director, Pediatric Sleep
in children Diagnosing and managing Asthma is chronically common amongst New Zealand children Diagnosing asthma in children
 Diagnosing and managing in children New Zealand has one of the highest rates of childhood asthma in the developed world. 1 It is the leading cause of sleep disturbance, missed school days and hospital
Diagnosing and managing in children New Zealand has one of the highest rates of childhood asthma in the developed world. 1 It is the leading cause of sleep disturbance, missed school days and hospital
Asthma. & Older Adults. A guide to living with asthma for people aged 65 years and over FOR PATIENTS & CARERS
 Asthma & Older Adults A guide to living with asthma for people aged 65 years and over FOR PATIENTS & CARERS what is Asthma? Asthma is a disease of the airways, the small tubes which carry air in and out
Asthma & Older Adults A guide to living with asthma for people aged 65 years and over FOR PATIENTS & CARERS what is Asthma? Asthma is a disease of the airways, the small tubes which carry air in and out
Asthma training. Mike Levin Division of Asthma and Allergy Red Cross Hospital
 Asthma training Mike Levin Division of Asthma and Allergy Red Cross Hospital Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
Asthma training Mike Levin Division of Asthma and Allergy Red Cross Hospital Introduction Physiology Diagnosis Severity Treatment Control Stage 3 of guidelines Acute asthma Drug delivery Conclusion Overview
Changing Landscapes in COPD New Zealand Respiratory Conference
 Changing Landscapes in COPD New Zealand Respiratory Conference Dr Robert Young BMedSc MBChB DPhil (Oxon) FRACP FRCP Associate Professor Consultant Physician Changing Landscapes in COPD: Summary 1. Overview
Changing Landscapes in COPD New Zealand Respiratory Conference Dr Robert Young BMedSc MBChB DPhil (Oxon) FRACP FRCP Associate Professor Consultant Physician Changing Landscapes in COPD: Summary 1. Overview
Treatment Responses. Ronald Dahl, Aarhus University Hospital, Denmark
 Asthma and COPD: Are They a Spectrum Treatment Responses Ronald Dahl, Aarhus University Hospital, Denmark Pharmacological Treatments Bronchodilators Inhaled short-acting β -Agonist (rescue) Inhaled short-acting
Asthma and COPD: Are They a Spectrum Treatment Responses Ronald Dahl, Aarhus University Hospital, Denmark Pharmacological Treatments Bronchodilators Inhaled short-acting β -Agonist (rescue) Inhaled short-acting
Life-long asthma and its relationship to COPD. Stephen T Holgate School of Medicine University of Southampton
 Life-long asthma and its relationship to COPD Stephen T Holgate School of Medicine University of Southampton Definitions COPD is a preventable and treatable disease with some significant extrapulmonary
Life-long asthma and its relationship to COPD Stephen T Holgate School of Medicine University of Southampton Definitions COPD is a preventable and treatable disease with some significant extrapulmonary
Current guidelines for the management of asthma in young children
 Review pissn 2092-7355 eissn 2092-7363 Current guidelines for the management of asthma in young children Paul C Potter* Allergy Diagnostic & Clinical Research Unit, University of Cape Town Lung Institute,
Review pissn 2092-7355 eissn 2092-7363 Current guidelines for the management of asthma in young children Paul C Potter* Allergy Diagnostic & Clinical Research Unit, University of Cape Town Lung Institute,
Recurrent wheezing illnesses 24.9% Similar to Australia Above global averages
 Prof Mike South Department of General Medicine Royal Children s Hospital Melbourne Australia www.mikesouth.org.au Asthma is very common in Australia Approx 25% children have recurrent wheezing illnesses
Prof Mike South Department of General Medicine Royal Children s Hospital Melbourne Australia www.mikesouth.org.au Asthma is very common in Australia Approx 25% children have recurrent wheezing illnesses
A Guide to Monitoring and Achieving Asthma Control in Children Younger Than 5 Years
 CPSS_09012009_000C1.ps 8/24/09 8:54 AM Page 3 SUPPLEMENT TO A P E E R - R E V I E W E D J O U R N A L SEPTEMBER 2009 VOL.8 NO.9 FOR PEDIATRICIANS A Guide to Monitoring and Achieving Asthma Control in Children
CPSS_09012009_000C1.ps 8/24/09 8:54 AM Page 3 SUPPLEMENT TO A P E E R - R E V I E W E D J O U R N A L SEPTEMBER 2009 VOL.8 NO.9 FOR PEDIATRICIANS A Guide to Monitoring and Achieving Asthma Control in Children
Most common chronic disease in childhood Different phenotypes:
 Dr. W. Wijnant Paediatric Pulmonology Steve Biko Academic Hospital Most common chronic disease in childhood Different phenotypes: Viral wheezer Multiple trigger wheezer Transient wheezer Persistent early
Dr. W. Wijnant Paediatric Pulmonology Steve Biko Academic Hospital Most common chronic disease in childhood Different phenotypes: Viral wheezer Multiple trigger wheezer Transient wheezer Persistent early
Asthma in the Athlete
 Asthma in the Athlete Jorge E. Gomez, MD Associate Professor Texas Children s Hospital Baylor College of Medicine Assist Team Physician UH Understand how we diagnose asthma Objectives Be familiar with
Asthma in the Athlete Jorge E. Gomez, MD Associate Professor Texas Children s Hospital Baylor College of Medicine Assist Team Physician UH Understand how we diagnose asthma Objectives Be familiar with
AT TRIAGE. Alberta Acute Childhood Asthma Pathway: Evidence based* recommendations For Emergency / Urgent Care
 1 1 Should the child be placed into the Pathway? Asthma Clinical Score (PRAM) Inclusion Children 1 year and 18 years of age who present with wheezing and respiratory distress, and have been diagnosed by
1 1 Should the child be placed into the Pathway? Asthma Clinical Score (PRAM) Inclusion Children 1 year and 18 years of age who present with wheezing and respiratory distress, and have been diagnosed by
Asthma Update I have no professional or personal financial conflicts of interest to disclose.
 Asthma Update 2018 Disclosures Jennifer W. McCallister, MD, FACP, FCCP Associate Professor Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical Center I have
Asthma Update 2018 Disclosures Jennifer W. McCallister, MD, FACP, FCCP Associate Professor Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical Center I have
Asthma Update Jennifer W. McCallister, MD, FACP, FCCP
 Asthma Update 2018 Jennifer W. McCallister, MD, FACP, FCCP Associate Professor Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical Center Disclosures I have
Asthma Update 2018 Jennifer W. McCallister, MD, FACP, FCCP Associate Professor Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical Center Disclosures I have
Managing the wheezing infant. Alessandro Fiocchi. Chair, WAO Special Committee on Food Allergy. Milano, Italy
 Managing the wheezing infant Alessandro Fiocchi Chair, WAO Special Committee on Food Allergy Milano, Italy Asthma and viral infections Dubai, December 8 th, 2010 Conflict of interest Speakers Bureau: none
Managing the wheezing infant Alessandro Fiocchi Chair, WAO Special Committee on Food Allergy Milano, Italy Asthma and viral infections Dubai, December 8 th, 2010 Conflict of interest Speakers Bureau: none
Evaluating a child with recurrent cough and night time symptoms
 Evaluating a child with recurrent cough and night time symptoms CATHERINE KIER, MD Professor of Clinical Pediatrics Division Chief, Pediatric Pulmonary, and Cystic Fibrosis Center Director, Pediatric Sleep
Evaluating a child with recurrent cough and night time symptoms CATHERINE KIER, MD Professor of Clinical Pediatrics Division Chief, Pediatric Pulmonary, and Cystic Fibrosis Center Director, Pediatric Sleep
Child and Adolescent Asthma Guidelines. Asthma and Respiratory Foundation NZ 2017
 Child and Adolescent Asthma Guidelines Asthma and Respiratory Foundation NZ 2017 Acknowledgements Innes Asher Cheryl Davies Teresa Demetriou Terry Fleming Matire Harwood Lorraine Hetaraka-Stevens Tristram
Child and Adolescent Asthma Guidelines Asthma and Respiratory Foundation NZ 2017 Acknowledgements Innes Asher Cheryl Davies Teresa Demetriou Terry Fleming Matire Harwood Lorraine Hetaraka-Stevens Tristram
Long-Term Management of Bronchial Asthma and Wheezy Chest in Children
 Long-Term Management of Bronchial Asthma and Wheezy Chest in Children Ali Al-Giurnazi,* Taher Ben-Ahameida**, Elham Al-Karewi,** Awatef Al-Bouacshi*** A. Dau Masaud,**** Abstract: This paper represents
Long-Term Management of Bronchial Asthma and Wheezy Chest in Children Ali Al-Giurnazi,* Taher Ben-Ahameida**, Elham Al-Karewi,** Awatef Al-Bouacshi*** A. Dau Masaud,**** Abstract: This paper represents
Asthma and Its Many Unmet Needs: Directions for Novel Therapeutic Approaches
 Asthma and Its Many Unmet Needs: Directions for Novel Therapeutic Approaches William W. Busse,, M.D. University of Wisconsin School of Medicine and Public Health Madison, WI, USA Disclosure Slide Employment
Asthma and Its Many Unmet Needs: Directions for Novel Therapeutic Approaches William W. Busse,, M.D. University of Wisconsin School of Medicine and Public Health Madison, WI, USA Disclosure Slide Employment
Reducing unnecessary antibiotic use in respiratory tract infections in children
 Reducing unnecessary antibiotic use in respiratory tract infections in children -a secondary care perspective Dr Conor Doherty (Consultant in paediatric infectious diseases and immunology GGC) Current
Reducing unnecessary antibiotic use in respiratory tract infections in children -a secondary care perspective Dr Conor Doherty (Consultant in paediatric infectious diseases and immunology GGC) Current
HealthPartners Care Coordination Clinical Care Planning and Resource Guide ASTHMA
 The following evidence based guideline was used in developing this clinical care guide: National Institute of Health (NIH National Heart, Lung, and Blood Institute (NHLBI) and American Academy of Allergy,
The following evidence based guideline was used in developing this clinical care guide: National Institute of Health (NIH National Heart, Lung, and Blood Institute (NHLBI) and American Academy of Allergy,
ASTHMA IN THE PEDIATRIC POPULATION
 ASTHMA IN THE PEDIATRIC POPULATION SEARCH Rotation 2 August 23, 2010 Objectives Define asthma as a chronic disease Discuss the morbidity of asthma in pediatrics Discuss a few things that a health center
ASTHMA IN THE PEDIATRIC POPULATION SEARCH Rotation 2 August 23, 2010 Objectives Define asthma as a chronic disease Discuss the morbidity of asthma in pediatrics Discuss a few things that a health center
Asthma Upate 2018: What s New Since the 2007 Asthma Guidelines of NAEPP?
 10:50-11:50am Asthma Update 2018: What s New Since the 2007 National Asthma Guidelines? SPEAKER Christopher H. Fanta, MD Disclosures The following relationships exist related to this presentation: Christopher
10:50-11:50am Asthma Update 2018: What s New Since the 2007 National Asthma Guidelines? SPEAKER Christopher H. Fanta, MD Disclosures The following relationships exist related to this presentation: Christopher
รศ. นพ. ว ชรา บ ญสว สด M.D., Ph.D. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร มหาว ทยาล ยขอนแก น
 รศ. นพ. ว ชรา บ ญสว สด M.D., Ph.D. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร มหาว ทยาล ยขอนแก น COPD Guideline Changing concept in COPD management Evidences that we can offer COPD patients better life COPD Guidelines
รศ. นพ. ว ชรา บ ญสว สด M.D., Ph.D. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร มหาว ทยาล ยขอนแก น COPD Guideline Changing concept in COPD management Evidences that we can offer COPD patients better life COPD Guidelines