Asthma 2015: Establishing and Maintaining Control
|
|
|
- Shonda Jones
- 5 years ago
- Views:
Transcription
 Karen Meyerson, MSN, APRN, NP-C, AE-C June 16,")
1 Asthma 2015: Establishing and Maintaining Control Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) Karen Meyerson, MSN, APRN, NP-C, AE-C June 16, 2015
2 Asthma Prevalence Approx. 26 million Americans have asthma (2012) Most common chronic disorder in children about 9 million children and adolescents Children with asthma are 3 times more likely to miss school than children without the disease 10.5 million days/year Asthma is the 3rd leading cause of hospitalization in children < 15 years of age Each year asthma in children accounts for >500,000 ED visits Annual economic cost is $56 billion Direct costs; indirect costs (lost productivity); Rx single largest expenditure of >$6 billion
3 Asthma Prevalence Currently, prevalence rate is 8.4% in the U.S. (CDC) An average of one out of 10 school-aged children has asthma Higher prevalence among the poor and minority populations Prevalence is increasing Number of people with asthma in U.S. grew by 15% in the last decade Greatest rise in asthma rates among black children (almost a 50% increase) from 2001 through 2009 It is estimated that the number of people (worldwide) with asthma will grow by more than 100 million by ,388 deaths annually in U.S. due to asthma (2009) 9 people die from asthma each day in the U.S. In Michigan, approx deaths/year (10-15 are children)
4 Asthma in Michigan 213,600 children and 654,100 adults currently have asthma in Michigan. >50% of Michigan adults with asthma had an asthma attack in the last year. 20% of Michigan adults with asthma are experiencing asthma symptoms every day. Asthma hospitalization rates are highest in very young children, age 0 to 4 years. Hospitalization rates for blacks are 4 times the rate for whites.
5 State/National Response Asthma Initiative of Michigan (AIM) includes 10 local asthma coalitions who have formed the Michigan Consortium of Asthma Coalitions: visit U.S. Environmental Protection Agency (EPA) hosts annual National Asthma Forum and has created a website of asthma programs nationwide: visit National Asthma Educator Certification Board (NAECB) includes ~150 certified asthma educators in Michigan (~4,000 in the nation): visit to find an AE-C in your area
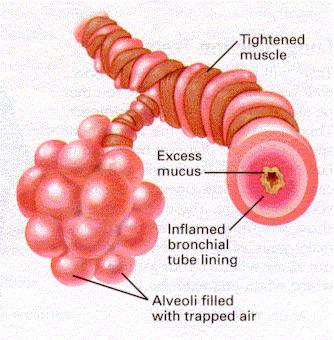
6 Definition of Asthma Chronic inflammatory disease of the airways characterized by: Recurrent episodes of wheezing Shortness of breath Chest tightness/pain Coughing Airflow limitation is at least partially reversible Airways are hyperresponsive (supersensitive) and react to a variety of stimuli or triggers
7 Asthma Pathophysiology In response to a trigger: Airway inflammation Bronchial smooth muscles constriction (bronchospasm) Increased mucus production The airways become narrow and breathing becomes difficult
 Airflow Limitation")
8 Mechanisms Underlying the Definition of Asthma Risk Factors (for development of asthma) INFLAMMATION Airway Hyperresponsiveness Risk Factors (triggers) Airflow Limitation Symptoms

9 Normal vs. Asthma Airways


10 Asthma Airways Before 10 Minutes After Allergen Challenge

11 The Tip of the Iceberg ASTHMA Symptoms Airflow obstruction Bronchial hyperresponsiveness Airway inflammation National Asthma Education and Prevention Program. Highlights of the Expert Panel Report 2: Guidelines for the Diagnosis and Management of Asthma. Bethesda, MD., May NIH Publication No A.
12 Factors Predicting Persistent Asthma Family history of asthma (maternal > paternal) Atopy (IgE/positive skin tests, eczema, rhinitis) Allergen exposure (dust mites / animals) Viral (RSV) infection Gender (males > females) Smoking (passive or active) The strongest predictor for wheezing that develops into asthma is ATOPY
13 Challenges in Treating Asthma Assessing Symptoms Cough Wheeze Dyspnea Nocturnal symptoms Activity affected? Recurrent episodes of cough (+ wheeze) are frequently due to asthma Coughing may be the only symptom present
14 Asthma Diagnosis Medical history Physical exam Measurements of lung function Diurnal variation in peak flow Evaluation of allergic status Exclude alternative diagnoses Bronchiolitis, cystic fibrosis, GERD, foreign body aspiration
15 Asthma Diagnosis Medical History Repeated cough, wheeze, chest tightness Repeated diagnoses of reactive airway disease, allergic bronchitis or wheezy bronchitis Symptoms worsened by viral infection, smoke, allergens, exercise, weather Symptoms occur/worsen at night Reversible airflow limitation Wheezing may or may not be present
16 Asthma Diagnosis Cough especially if: after exertion breathing cold air at night after colds paroxysmal Wheezing tightness noisy breathing? Dyspnea (Breathlessness) especially if: intermittent or variable after exertion at night
17 Asthma Diagnosis Cough especially if: after exertion breathing cold air at night after colds paroxysmal Wheezing tightness noisy breathing? Dyspnea (Breathlessness) especially if: intermittent or variable after exertion at night
18 Asthma Diagnosis Cough especially if: after exertion breathing cold air at night after colds paroxysmal Wheezing tightness noisy breathing? Dyspnea (Breathlessness) especially if: intermittent or variable after exertion at night
19 Asthma Diagnosis Cough especially if: after exertion breathing cold air at night after colds paroxysmal Wheezing tightness noisy breathing? Dyspnea (Breathlessness) especially if: intermittent or variable after exertion at night
 especially if: intermittent or variable after exertion at")
20 Asthma Diagnosis Cough especially if: after exertion breathing cold air at night after colds paroxysmal Wheezing tightness noisy breathing Dyspnea (Breathlessness) especially if: intermittent or variable after exertion at night
21 Coughing, wheezing Prolonged forced expiration Use of accessory muscles Retractions Hyperexpansion of the chest Signs of other allergic diseases: Atopic dermatitis Allergic rhinitis Asthma Diagnosis Physical Exam Physical examination of the chest may be normal
22 Spirometry Measurements of Lung Function FEV 1 volume forcefully exhaled in 1 sec. assesses large airways FVC forced vital capacity total amount forcefully exhaled FEV1 / FVC Ratio helps differentiate obstruction vs. restriction FEF 25-75% assesses small airways
23 Asthma Diagnosis Measurements of Lung Function Spirometry / Pulmonary Function Testing Obstruction - FEV 1 < 80% - FEV 1 / FVC ratio < 80% Reversibility - FEV 1 change of > 12 % or 200mL - FEF change of > 25%
24 Spirometry: Flow-Volume Loop Obstruction
25 Spirometry Results Classic finding is baseline spirometry reveals obstruction Post-bronchodilator spirometry may reveal reversibility Diagnosis Can still pursue post-bronchodilator spirometry even if baseline spirometry is normal Usually recommend 4 puffs of albuterol with spacer for post-bronchodilator trial Even if these values are all normal that does not completely exclude asthma
26 Flow-Volume Loops Side by Side Comparison Exhalation Loops Spirometric Results Obstructive - similar width to normal - scooped appearance - concave appearance Restrictive - narrowed width - similar shape
27 Spirometry Patient Positioning Critical to achieving acceptable spirometry Stand or sit upright no bending at the waist Trunk upright Chin slightly elevated Neck in extension Nose clips (+/-) Be consistent
28 Spirometry: Bronchodilator Studies A normal baseline lung function test does NOT rule out asthma, nor does it negate the need for a post-bronchodilator study It is quite possible that your patient s flow-volume loops could still improve after 2-4 puffs of a bronchodilator!
29 Spirometry: Bronchodilator Studies Test Restriction Obstruction Reversibility FEV 1 < 80% < 80% >12% FVC decreased decreased / normal >12% FEV 1 /FVC normal decreased FEF25-75% decreased decreased >25%
30 Diagnosis Response to Medications If still suspect asthma can pursue medication trial Can consider a 2 to 4 week trial of inhaled steroid Could also consider 2 week trial of oral steroids Assess for spirometry changes at follow up Significant improvement in symptoms and spirometry is consistent with asthma
31 CLASSIFYING ASTHMA SEVERITY AND INITIATING TREATMENT IN CHILDREN 0-4 YEARS OF AGE EPR-3, p72, 307 Components of Severity Symptoms Classification of Asthma Severity Intermittent Persistent Mild Moderate Severe <2 days/week >2 days/week not daily Daily Continuous Nighttime Awakenings 0 1-2x/month 3-4x/month >1x/week Impairment SABA use for sx control Interference with normal activity <2 days/week >2 days/week not daily Daily Several times daily none Minor limitation Some limitation Extremely limited Risk Exacerbations (consider frequency and severity) Recommended Step for Initiating Treatment 0-1/year >2 exacerbations in 6 months requiring oral steroids, or >4 wheezing episodes/ year lasting >1 day AND risk factors for persistent asthma Frequency and severity of may fluctuate over time Exacerbations of any severity may occur in patients in any category Step 1 Step 2 Step 3 Consider short course of oral steroids In 2-6 weeks, evaluate asthma control that is achieved and adjust therapy accordingly
32 STEPWISE APPROACH FOR MANAGING ASTHMA IN CHILDREN 0-4 YEARS OF AGE EPR-3, p Intermittent Asthma Persistent Asthma: Daily Medication Consult with asthma specialist if step 3 or higher care is required Consider consultation at step 2 Step 5 Step 6 Preferred: High dose ICS Step up if needed (check adherence, environmental control ) Step 1 Preferred: SABA prn Step 2 Preferred: Low-dose ICS Alternative: LTRA Cromolyn Step 3 Preferred: Medium-dose ICS Step 4 Preferred: Medium-dose ICS AND either LTRA Or LABA Preferred: High dose ICS AND either LTRA Or LABA AND either LTRA Or LABA AND Oral Corticosteroid Assess Control Step down if possible (asthma well controlled for 3 months) Patient Education and Environmental Control at Each Step
33 ASSESSING ASTHMA CONTROL AND ADJUSTING THERAPY IN CHILDREN 0-4 YEARS OF AGE Components of Control Symptoms Nighttime awakenings Classification of Asthma Control Well Controlled Not Well Controlled EPR-3, p75, 309 Very Poorly Controlled < 2 days/week > 2 days/week Throughout the day < 1/month > 2 x/month >2x/week IMPAIRMENT Interference with normal activity SABA use none Some limitation Extremely limited < 2 days/week > 2 days/week Several times/day Exacerbations 0-1 per year 2-3 per year > 3 per year RISK Recommended Action For Treatment Progressive loss of lung function Rx-related adverse effects Evaluation requires long-term follow up care Consider in overall assessment of risk Consider oral Maintain current step Step up 1 step steroids REGULAR FOLLOW UP EVERY 3-6 MONTHS Consider step down if well controlled at least 3 months Reevaluate in 2-6 weeks If no clear benefit in 4-6 weeks, consider alternative dx or adjust therapy Step up (1-2 steps) and reevaluate in 2 weeks If no clear benefit in 4-6 weeks, consider alternative dx or adjust therapy
34 CLASSIFYING ASTHMA SEVERITY AND INITIATING TREATMENT IN CHILDREN 5-11 YEARS OF AGE EPR-3, p73, 308 Components of Severity Impairment Risk Symptoms Nighttime Awakenings SABA use for sx control Interference with normal activity Lung Function Exacerbations (consider frequency and severity) Recommended Step for Initiating Treatment Classification of Asthma Severity Intermittent 0-2/year Persistent Mild Moderate Severe <2 days/week >2 days/week not daily Daily Continuous <2x/month 3-4x/month > 2 /year >1x/week not nightly Frequency and severity may vary over time for patients in any category Relative annual risk of exacerbations may be related to FEV Step 2 Step3 mediumdose ICS option Step 3 or 4 Consider short course of oral steroids In 2-6 weeks, evaluate asthma control that is achieved and adjust therapy Often nightly <2 days/week >2 days/week not daily Daily Several times daily none Minor limitation Some limitation Extremely limited Normal FEV 1 between exacerbations FEV 1 > 80% FEV 1 /FVC> 85% Step 1 FEV 1 >80% FEV 1 /FVC> 80% FEV 1 =60% - 80% FEV 1 /FVC=75% -80% FEV 1 <60% FEV 1 /FVC < 75%
35 STEPWISE APPROACH FOR MANAGING ASTHMA IN CHILDREN 5-11 YEARS OF AGE EPR-3, p Intermittent Asthma Step 1 Preferred: SABA prn Persistent Asthma: Daily Medication Consult with asthma specialist if step 4 or higher care is required Consider consultation at step 3 Step 2 Preferred: Low-dose ICS Alternative: LTRA Cromolyn Theophylline Step 3 Preferred: Medium-dose ICS OR Low-dose ICS + either LABA, LTRA, or Theophylline Step 4 Preferred: Medium-dose ICS+LABA Alternative: Medium-dose ICS + either LTRA, or Theophylline Step 5 Preferred: High dose ICS + LABA Step 6 Preferred: High-dose ICS + LABA + oral Corticosteroid Alternative: Alternative: High-dose ICS High-dose ICS + either LTRA or + either LTRA Theophylline or + oral Theophylline corticosteroid Step up if needed (check adherence, environmental control and comorbidities) Assess Control Step down if possible (asthma well controlled for 3 months) Patient Education and Environmental Control at Each Step
36 ASSESSING ASTHMA CONTROL AND ADJUSTING THERAPY IN CHILDREN 5-11 YEARS OF AGE Components of Control Symptoms Nighttime awakenings Classification of Asthma Control Well Controlled Not Well Controlled EPR-3, p76, 310 Very Poorly Controlled < 2 days/week > 2 days/week Throughout the day < 1/month > 2 x/month >2x/week IMPAIRMENT Interference with normal activity SABA use none Some limitation Extremely limited < 2 days/week > 2 days/week Several times/day FEV 1 or peak flow > 80% predicted/ personal best 60-80% predicted/ personal best <60% predicted/ personal best RISK FEV 1 /FVC Exacerbations Progressive loss of lung function Rx-related adverse effects > 80% predicted 75-80% predicted <75% predicted 0-1 per year 2-3 per year > 3 per year Evaluation requires long-term follow up care Consider in overall assessment of risk Recommended Action For Treatment Maintain current step Consider step down if well controlled at least 3 months Step up 1 step Reevaluate in 2-6 weeks Consider oral steroids Step up 1-2 weeks and reevaluate in 2 weeks
37 CLASSIFYING ASTHMA SEVERITY AND INITIATING TREATMENT IN YOUTHS > 12 YEARS AND ADULTS EPR-3, p74, 344 Components of Severity Impairment Normal FEV 1 /FVC 8-19 yr 85% yr 80% yr 75% yr 70% Risk Symptoms Nighttime Awakenings SABA use for sx control Interference with normal activity Lung Function Exacerbations (consider frequency and severity) Recommended Step for Initiating Treatment Intermittent Classification of Asthma Severity 0-2/year Persistent Mild Moderate Severe <2 days/week >2 days/week not daily Daily Continuous <2x/month 3-4x/month > 2 /year >1x/week not nightly Frequency and severity may vary over time for patients in any category Relative annual risk of exacerbations may be related to FEV 1 Often nightly <2 days/week >2 days/week not daily Daily Several times daily none Minor limitation Some limitation Extremely limited Normal FEV 1 between exacerbations FEV 1 > 80% FEV 1 /FVC normal FEV 1 >80% FEV 1 /FVC normal FEV 1 >60% but< 80% FEV 1 /FVC reduced 5% FEV 1 <60% FEV 1 /FVC reduced >5% Step 1 Step 2 Step 3 Step 4 or 5 Consider short course of oral steroids In 2-6 weeks, evaluate asthma control that is achieved and adjust therapy accordingly
38 STEPWISE APPROACH FOR MANAGING ASTHMA IN YOUTHS > 12 YEARS AND ADULTS EPR-3, p Intermittent Asthma Step 1 Preferred: SABA prn Persistent Asthma: Daily Medication Consult with asthma specialist if step 4 or higher care is required Consider consultation at step 3 Step 2 Preferred: Low-dose ICS Alternative: LTRA Cromolyn Theophylline Step 3 Preferred: Medium-dose ICS OR Low-dose ICS + either LABA, LTRA, Theophylline Or Zileutin Step 4 Preferred: Medium-dose ICS+LABA Alternative: Medium-dose ICS+either LTRA, Theophlline Or Zileutin Step 5 Preferred: High dose ICS + LABA AND Consider omalizumab for patients with allergies Step 6 Preferred: High-dose ICS + LABA + oral Corticosteroid AND Consider omalizumab for patients with allergies Step up if needed (check adherence, environmental control and comorbidities) Assess Control Step down if possible (asthma well controlled for 3 months) Patient Education and Environmental Control at Each Step
39 ASSESSING ASTHMA CONTROL AND ADJUSTING THERAPY IN YOUTHS > 12 YEARS OF AGE AND ADULTS EPR-3, p77, 345 Components of Control Symptoms Nighttime awakenings Classification of Asthma Control Well Controlled Not Well Controlled Very Poorly Controlled < 2 days/week > 2 days/week Throughout the day < 2/month 1-3/week > 4/week IMPAIRMENT RISK Interference with normal activity SABA use FEV 1 or peak flow Validated questionnaires ATAQ/ACT Exacerbations Progressive loss of lung function Rx-related adverse effects none Some limitation Extremely limited < 2 days/week > 2 days/week Several times/day > 80% predicted/ personal best 60-80% predicted/ personal best 0-1 per year 2-3 per year > 3 per year Evaluation requires long-term follow up care Consider in overall assessment of risk <60% predicted/ personal best 0/> / /<15 Recommended Action For Treatment Maintain current step Consider step down if well controlled at least 3 months Step up 1 step Reevaluate in 2-6 weeks Consider oral steroids Step up 1-2 weeks and reevaluate in 2 weeks
40 Childhood Asthma Control Test (ACT): Questions Completed by Child 1. How is your asthma today? SCORE Very bad Bad Good Very Good 2. How much of a problem is your asthma when you run, exercise or play sports? It s a big problem, I can t do what I want to do. It s a problem and I don t like it. It s a little problem but it s okay. It s not a problem 3. Do you cough because of your asthma? Yes, all of the time. Yes, most of the time. Yes, some of the time. No, none of the time 4. Do you wake up during the night because of your asthma? Yes, all of the time. Yes, most of the time. Yes, some of the time. No, none of the time
41 Childhood Asthma Control Test (ACT): Questions Completed by Parent/Caregiver 5. During the last 4 weeks, on average, how many days per month did your child have any daytime asthma symptoms? Not at all 1-3 days/mo 4-10 days/mo days/mo days/mo Everyday 6. During the last 4 weeks, on average, how many days per month did your child wheeze during the day because of asthma? Not at all 1-3 days/mo 4-10 days/mo days/mo days/mo Everyday 7. During the last 4 weeks, on average, how many days per month did your child wake up during the night because of asthma? Not at all 1-3 days/mo 4-10 days/mo days/mo days/mo Everyday TOTAL

")
? 5.")
42 Asthma Control Test (ACT) for Patients 12 Years and Older 1. In the past 4 weeks, how much of the time did your asthma keep you from getting as much done at work, school or at home? Score 2. During the past 4 weeks, how often have you had shortness of breath? 3. During the past 4 weeks, how often did your asthma symptoms (wheezing, coughing, shortness of breath, chest tightness or pain) wake you up at night, or earlier than usual in the morning? 4. During the past 4 weeks, how often have you used your rescue inhaler or nebulizer medication (such as albuterol)? 5. How would you rate your asthma control during the past 4 weeks? Copyright 2002, QualityMetric Incorporated. Asthma Control Test Is a Trademark of QualityMetric Incorporated. Patient Total Score
43 Treatment Strategies Gain Control! Aggressive, intensive initial therapy to suppress airway inflammation and gain prompt control Maintain Control Frequent follow-up clinically and physiologically Therapeutic modifications depending on severity and clinical course Step down long-term control medications to maintain control with minimal side effects
44 Recommended Action for Treatment Well Controlled Maintain current step Consider step down if well controlled for at least 3 months Based on Assessment of Control Not Well Controlled Step up 1 step and reevaluate in 2-6 weeks For side effects, consider alternative treatment options Very Poorly Controlled Consider short course of oral corticosteroids Step up 1-2 steps and reevaluate in 2 weeks For side effects, consider alternative treatment options Before stepping up check adherence and environmental control
45 Monitoring Asthma Control Ask the patient Has your asthma awakened you at night or early morning? Have you needed more rescue inhaler than usual? Have you needed urgent care for asthma? (office, ED, etc) Are you participating in your usual or desired activities? What are your triggers? (and how can we manage them?) Actions to consider Assess whether medications are being taken as prescribed Assess whether inhalation technique is correct Assess spirometry and compare to previous measurements Adjust medications, as needed to achieve best control with the lowest dose needed to maintain control Environmental mitigation strategy EPR-3, Page 78
46 Questions? Karen Meyerson, MSN, APRN, NP-C, AE-C: Phone: (616) websites:
Improving the Management of Asthma to Improve Patient Adherence and Outcomes
 Improving the Management of Asthma to Improve Patient Adherence and Outcomes Robert Sussman, MD Atlantic Health System Overlook Medical Center Asthma Remains a Serious Health Risk in the US Every day in
Improving the Management of Asthma to Improve Patient Adherence and Outcomes Robert Sussman, MD Atlantic Health System Overlook Medical Center Asthma Remains a Serious Health Risk in the US Every day in
Inhaler Confusion. Today s Speaker Dr. Randall Brown. Director of Asthma Programs 6/7/2016. Dr. Randall Brown March 31, 2016
 + Inhaler Confusion Dr. Randall Brown March 31, 2016 + Today s Speaker Dr. Randall Brown Director of Asthma Programs Center for Managing Chronic Disease University of Michigan 1 ASTHMA ESSENTIALS IN PRIMARY
+ Inhaler Confusion Dr. Randall Brown March 31, 2016 + Today s Speaker Dr. Randall Brown Director of Asthma Programs Center for Managing Chronic Disease University of Michigan 1 ASTHMA ESSENTIALS IN PRIMARY
Learning the Asthma Guidelines by Case Studies
 Learning the Asthma Guidelines by Case Studies Timothy Craig, DO Professor of Medicine and Pediatrics Distinguished Educator Penn State University Hershey Medical Center Objectives 1. Learn the Asthma
Learning the Asthma Guidelines by Case Studies Timothy Craig, DO Professor of Medicine and Pediatrics Distinguished Educator Penn State University Hershey Medical Center Objectives 1. Learn the Asthma
Asthma Management for the Athlete
 Asthma Management for the Athlete Khanh Lai, MD Assistant Professor Division of Pediatric Pulmonary and Sleep Medicine University of Utah School of Medicine 2 nd Annual Sports Medicine Symposium: The Pediatric
Asthma Management for the Athlete Khanh Lai, MD Assistant Professor Division of Pediatric Pulmonary and Sleep Medicine University of Utah School of Medicine 2 nd Annual Sports Medicine Symposium: The Pediatric
The Asthma Guidelines: Diagnosis and Assessment of Asthma
 The Asthma Guidelines: Diagnosis and Assessment of Asthma Christopher H. Fanta, M.D. Partners Asthma Center Brigham and Women s Hospital Harvard Medical School Objectives Know how the diagnosis of asthma
The Asthma Guidelines: Diagnosis and Assessment of Asthma Christopher H. Fanta, M.D. Partners Asthma Center Brigham and Women s Hospital Harvard Medical School Objectives Know how the diagnosis of asthma
Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma
 Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma Magnitude of Asthma - India Delhi Childhood asthma: 10.9% Adults: 8% Other Cities 3 to 18% Chhabra SK et al Ann Allergy Asthma
Diagnosis, Assessment, Monitoring and Pharmacological Treatment of Asthma Magnitude of Asthma - India Delhi Childhood asthma: 10.9% Adults: 8% Other Cities 3 to 18% Chhabra SK et al Ann Allergy Asthma
RESPIRATORY CARE IN GENERAL PRACTICE
 RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
National Institutes of Health (NIH) NAEPP 2007 Asthma Guideline UPDATE. Susan K. Ross RN, AE-C MDH Asthma Program.
 NAEPP 2007 Asthma Guideline UPDATE. Susan K. Ross RN, AE-C MDH Asthma Program.") National Institutes of Health (NIH) NAEPP 2007 Asthma Guideline UPDATE Susan K. Ross RN, AE-C MDH Asthma Program 651-201 201-5629 Susan.Ross@health.state.mn.us 1 National Institutes of Health National
National Institutes of Health (NIH) NAEPP 2007 Asthma Guideline UPDATE Susan K. Ross RN, AE-C MDH Asthma Program 651-201 201-5629 Susan.Ross@health.state.mn.us 1 National Institutes of Health National
Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016
 Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016 Diagnosis: There is no lower limit to the age at which
Diagnosis and Management of Asthma in Children based on the British Thoracic Society and Scottish Intercollegiate Guidelines Network September 2016 Diagnosis: There is no lower limit to the age at which
National Institutes of Health (NIH) NAEPP 2007 Asthma Guideline Expert Panel Report (EPR) 3
 NAEPP 2007 Asthma Guideline Expert Panel Report (EPR) 3") National Institutes of Health (NIH) NAEPP 2007 Asthma Guideline Expert Panel Report (EPR) 3 Susan K. Ross RN, AE C MDH Asthma Program 651 201 201 5629 Susan.Ross@state.mn.us 1 National Institutes of Health
National Institutes of Health (NIH) NAEPP 2007 Asthma Guideline Expert Panel Report (EPR) 3 Susan K. Ross RN, AE C MDH Asthma Program 651 201 201 5629 Susan.Ross@state.mn.us 1 National Institutes of Health
Presented by the California Academy of Family Physicians 2013/California Academy of Family Physicians
 Family Medicine and Patient-Centered Asthma Care Presented by the California Academy of Family Physicians Faculty: Hobart Lee, MD Disclosures: Jeffrey Luther, MD, Program Director, Memorial Family Medicine
Family Medicine and Patient-Centered Asthma Care Presented by the California Academy of Family Physicians Faculty: Hobart Lee, MD Disclosures: Jeffrey Luther, MD, Program Director, Memorial Family Medicine
Asthma in the Athlete
 Asthma in the Athlete Jorge E. Gomez, MD Associate Professor Texas Children s Hospital Baylor College of Medicine Assist Team Physician UH Understand how we diagnose asthma Objectives Be familiar with
Asthma in the Athlete Jorge E. Gomez, MD Associate Professor Texas Children s Hospital Baylor College of Medicine Assist Team Physician UH Understand how we diagnose asthma Objectives Be familiar with
Asthma in Pediatric Patients. DanThuy Dao, D.O., FAAP. Disclosures. None
 Asthma in Pediatric Patients DanThuy Dao, D.O., FAAP Disclosures None Objectives 1. Discuss the evaluation and management of asthma in a pediatric patient 2. Accurately assess asthma severity and level
Asthma in Pediatric Patients DanThuy Dao, D.O., FAAP Disclosures None Objectives 1. Discuss the evaluation and management of asthma in a pediatric patient 2. Accurately assess asthma severity and level
Diagnosis, Treatment and Management of Asthma
 Diagnosis, Treatment and Management of Asthma Asthma is a complex disorder characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation.
Diagnosis, Treatment and Management of Asthma Asthma is a complex disorder characterized by variable and recurring symptoms, airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation.
Asthma. UVM. University of Vermont. Alicia Jacobs MD Fletcher Allen Health Care and the University of Vermont
 University of Vermont ScholarWorks @ UVM Family Medicine Scholarly Works 6-14-2013 Asthma Alicia Jacobs MD Fletcher Allen Health Care and the University of Vermont Follow this and additional works at:
University of Vermont ScholarWorks @ UVM Family Medicine Scholarly Works 6-14-2013 Asthma Alicia Jacobs MD Fletcher Allen Health Care and the University of Vermont Follow this and additional works at:
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss?
 ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
HealthPartners Care Coordination Clinical Care Planning and Resource Guide ASTHMA
 The following evidence based guideline was used in developing this clinical care guide: National Institute of Health (NIH National Heart, Lung, and Blood Institute (NHLBI) and American Academy of Allergy,
The following evidence based guideline was used in developing this clinical care guide: National Institute of Health (NIH National Heart, Lung, and Blood Institute (NHLBI) and American Academy of Allergy,
Asthma for Primary Care: Assessment, Control, and Long-Term Management
 Asthma for Primary Care: Assessment, Control, and Long-Term Management Learning Objectives After participating in this educational activity, participants should be better able to: 1. Choose the optimal
Asthma for Primary Care: Assessment, Control, and Long-Term Management Learning Objectives After participating in this educational activity, participants should be better able to: 1. Choose the optimal
Air Flow Limitation. In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation.
 Asthma Air Flow Limitation In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation. True whether reversible, asthma and exercise-induced bronchospasm,
Asthma Air Flow Limitation In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation. True whether reversible, asthma and exercise-induced bronchospasm,
Pediatric Asthma Management
 Pediatric Asthma Management APRN Conference February 2016 Cheryl Kerrigan, MSN, CPNP Aimee Tiller RN, AE-C The Plan Definition Pathophysiology review Triggers & Risk Factors Incidence and Prevalence Making
Pediatric Asthma Management APRN Conference February 2016 Cheryl Kerrigan, MSN, CPNP Aimee Tiller RN, AE-C The Plan Definition Pathophysiology review Triggers & Risk Factors Incidence and Prevalence Making
Improving asthma outcomes though education
 Improving asthma outcomes though education Segment 1 Clinical Aspects of Asthma and Long term Plan Primary Care and Asthma Most common chronic disease of childhood. Primary care providers are expected
Improving asthma outcomes though education Segment 1 Clinical Aspects of Asthma and Long term Plan Primary Care and Asthma Most common chronic disease of childhood. Primary care providers are expected
I have no perceived conflicts of interest or commercial relationships to disclose.
 ASTHMA BASICS Michelle Dickens RN FNP-C AE-C Nurse Practitioner/Certified Asthma Educator Ferrell Duncan Allergy/Asthma/Immunology Coordinator, CoxHealth Asthma Center DISCLOSURES I have no perceived conflicts
ASTHMA BASICS Michelle Dickens RN FNP-C AE-C Nurse Practitioner/Certified Asthma Educator Ferrell Duncan Allergy/Asthma/Immunology Coordinator, CoxHealth Asthma Center DISCLOSURES I have no perceived conflicts
MSRC AIR Course Karla Stoermer Grossman, MSA, BSN, RN, AE-C
 MSRC AIR Course Karla Stoermer Grossman, MSA, BSN, RN, AE-C Explain the importance of objective measures in the management of asthma Explain the different types of objective measures used in the management
MSRC AIR Course Karla Stoermer Grossman, MSA, BSN, RN, AE-C Explain the importance of objective measures in the management of asthma Explain the different types of objective measures used in the management
Asthma ASTHMA. Current Strategies for Asthma and COPD
 Current Strategies for Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor of Medicine Chair, Department of Medicine University of California San Francisco (UCSF) San Francisco,
Current Strategies for Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor of Medicine Chair, Department of Medicine University of California San Francisco (UCSF) San Francisco,
Primary Care Medicine: Concepts and Controversies Wed., February 17, 2010 Fiesta Americana Puerto Vallarta, Mexico Update on Asthma and COPD
 Primary Care Medicine: Concepts and Controversies Wed., February 17, 2010 Fiesta Americana Puerto Vallarta, Mexico Update on Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor
Primary Care Medicine: Concepts and Controversies Wed., February 17, 2010 Fiesta Americana Puerto Vallarta, Mexico Update on Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor
GINA. At-A-Glance Asthma Management Reference. for adults, adolescents and children 6 11 years. Updated 2017
 GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
Adult asthma management: focus on control
 Adult asthma management: focus on control Jennifer W. McCallister, MD Associate Professor Pulmonary, Allergy, Critical Care & Sleep Medicine The Ohio State University Wexner Medical Center Objectives Apply
Adult asthma management: focus on control Jennifer W. McCallister, MD Associate Professor Pulmonary, Allergy, Critical Care & Sleep Medicine The Ohio State University Wexner Medical Center Objectives Apply
Because the more you know, the better you ll feel.
 ABOUT ASTHMA Because the more you know, the better you ll feel. This booklet is designed to help you understand asthma and the things you can do every day to help control symptoms. As always, talk to your
ABOUT ASTHMA Because the more you know, the better you ll feel. This booklet is designed to help you understand asthma and the things you can do every day to help control symptoms. As always, talk to your
MANAGING ASTHMA. Nancy Davis, RRT, AE-C
 MANAGING ASTHMA Nancy Davis, RRT, AE-C What is asthma? Asthma is a chronic respiratory disease characterized by episodes or attacks of inflammation and narrowing of small airways in response to asthma
MANAGING ASTHMA Nancy Davis, RRT, AE-C What is asthma? Asthma is a chronic respiratory disease characterized by episodes or attacks of inflammation and narrowing of small airways in response to asthma
Because the more you know, the better you ll feel.
 ABOUT ASTHMA Because the more you know, the better you ll feel. What You ll Find Attitudes and Beliefs Asthma What Is It? Where You ll Find It Page 4-5 This booklet is designed to help you understand asthma
ABOUT ASTHMA Because the more you know, the better you ll feel. What You ll Find Attitudes and Beliefs Asthma What Is It? Where You ll Find It Page 4-5 This booklet is designed to help you understand asthma
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing
 Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Function of the Respiratory System. Exchange CO2 (on expiration) for O2 (on inspiration)
 for O2 (on inspiration)") Function of the Respiratory System Exchange CO2 (on expiration) for O2 (on inspiration) Upper Respiratory Tract Includes: Nose Mouth Pharynx Larynx Function: Warms and humidifies the inspired air Filters
Function of the Respiratory System Exchange CO2 (on expiration) for O2 (on inspiration) Upper Respiratory Tract Includes: Nose Mouth Pharynx Larynx Function: Warms and humidifies the inspired air Filters
Outpatient Guideline for the Diagnosis and Management of Asthma
 Outpatient Guideline for the Diagnosis and Management of Asthma Initial Visit Follow-Up Visits See page 2 Asthma Diagnosis See page 3 Classifying Asthma Severity and Initiating Treatment See pages 2 and
Outpatient Guideline for the Diagnosis and Management of Asthma Initial Visit Follow-Up Visits See page 2 Asthma Diagnosis See page 3 Classifying Asthma Severity and Initiating Treatment See pages 2 and
ASTHMA BEST PRACTICES FOR SCHOOL NURSES. School Nurses November 2015
 ASTHMA BEST PRACTICES FOR SCHOOL NURSES School Nurses November 2015 1 BACKGROUND AND CURRENT STATS General definitions and explanations 2 Incidence of Asthma Centers for Disease Control (CDC) - 1 in 12
ASTHMA BEST PRACTICES FOR SCHOOL NURSES School Nurses November 2015 1 BACKGROUND AND CURRENT STATS General definitions and explanations 2 Incidence of Asthma Centers for Disease Control (CDC) - 1 in 12
On completion of this chapter you should be able to: discuss the stepwise approach to the pharmacological management of asthma in children
 7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
7 Asthma Asthma is a common disease in children and its incidence has been increasing in recent years. Between 10-15% of children have been diagnosed with asthma. It is therefore a condition that pharmacists
Bronchial asthma. E. Cserháti 1 st Department of Paediatrics. Lecture for english speaking students 5 February 2013
 Bronchial asthma E. Cserháti 1 st Department of Paediatrics Lecture for english speaking students 5 February 2013 Epidemiology of childhood bronchial asthma Worldwide prevalence of 7-8 and 13-14 years
Bronchial asthma E. Cserháti 1 st Department of Paediatrics Lecture for english speaking students 5 February 2013 Epidemiology of childhood bronchial asthma Worldwide prevalence of 7-8 and 13-14 years
7/7/2015. Somboon Chansakulporn, MD. History of variable respiratory symptoms. 1. Documented excessive variability in PFT ( 1 test)
") Definition of Asthma GINA 2010: Chronic inflammatory disorder of the airways Airway hyper-responsiveness Recurrent wheezing, breathlessness, chest tightness, coughing Variable, reversible airflow obstruction
Definition of Asthma GINA 2010: Chronic inflammatory disorder of the airways Airway hyper-responsiveness Recurrent wheezing, breathlessness, chest tightness, coughing Variable, reversible airflow obstruction
Clinical Practice Guideline: Asthma
 Clinical Practice Guideline: Asthma INTRODUCTION A critical aspect of the diagnosis and management of asthma is the precise and periodic measurement of lung function both before and after bronchodilator
Clinical Practice Guideline: Asthma INTRODUCTION A critical aspect of the diagnosis and management of asthma is the precise and periodic measurement of lung function both before and after bronchodilator
Pathology of Asthma Epidemiology
 Asthma A Presentation on Asthma Management and Prevention What Is Asthma? A chronic disease of the airways that may cause Wheezing Breathlessness Chest tightness Nighttime or early morning coughing Pathology
Asthma A Presentation on Asthma Management and Prevention What Is Asthma? A chronic disease of the airways that may cause Wheezing Breathlessness Chest tightness Nighttime or early morning coughing Pathology
Asthma and Vocal Cord Dysfunction
 Asthma and Vocal Cord Dysfunction Amy L. Marks DO, FACOP Pediatric Allergy and Immunology Assistant Professor of Pediatrics Oakland University William Beaumont School of Medicine Objectives: Understanding
Asthma and Vocal Cord Dysfunction Amy L. Marks DO, FACOP Pediatric Allergy and Immunology Assistant Professor of Pediatrics Oakland University William Beaumont School of Medicine Objectives: Understanding
Improving Outcomes in the Management & Treatment of Asthma. April 21, Spring Managed Care Forum
 Improving Outcomes in the Management & Treatment of Asthma April 21, 2016 2016 Spring Managed Care Forum David M. Mannino, M.D. Professor Department of Preventive Medicine and Environmental Health University
Improving Outcomes in the Management & Treatment of Asthma April 21, 2016 2016 Spring Managed Care Forum David M. Mannino, M.D. Professor Department of Preventive Medicine and Environmental Health University
12/18/2017. Disclosures. Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing
 Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007
 Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Selecting Initial Therapy
Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma Full Report 2007 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Selecting Initial Therapy
Asthma Pathophysiology and Treatment. John R. Holcomb, M.D.
 Asthma Pathophysiology and Treatment John R. Holcomb, M.D. Objectives Definition of Asthma Epidemiology and risk factors of Asthma Pathophysiology of Asthma Diagnostics test of Asthma Management of Asthma
Asthma Pathophysiology and Treatment John R. Holcomb, M.D. Objectives Definition of Asthma Epidemiology and risk factors of Asthma Pathophysiology of Asthma Diagnostics test of Asthma Management of Asthma
Spirometry Workshop for Primary Care Nurse Practitioners
 Spirometry Workshop for Primary Care Nurse Practitioners Catherine Casey S. Jones PhD, RN, AE-C, ANP-C Certified Adult Nurse Practitioner Texas Pulmonary & Critical Care Consultants P.A. and Adjunct Professor
Spirometry Workshop for Primary Care Nurse Practitioners Catherine Casey S. Jones PhD, RN, AE-C, ANP-C Certified Adult Nurse Practitioner Texas Pulmonary & Critical Care Consultants P.A. and Adjunct Professor
Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ
 Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ Financial Disclosures Advanced Practiced Advisory Board for Circassia Learning Objectives 1. Briefly
Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ Financial Disclosures Advanced Practiced Advisory Board for Circassia Learning Objectives 1. Briefly
Pediatric and Adult. Disclosure. Asthma. Learning Objectives. EPR-3: What s Changed? Asthma: Pediatric and Adult
 Asthma: Pediatric and Adult Americo D. Fraboni, MD, FAAFP Assistant Clinical Professor Department of Family Practice & Community Health University of Minnesota Medical School Minneapolis, Minnesota Disclosure
Asthma: Pediatric and Adult Americo D. Fraboni, MD, FAAFP Assistant Clinical Professor Department of Family Practice & Community Health University of Minnesota Medical School Minneapolis, Minnesota Disclosure
Asthma and Its Many Unmet Needs: Directions for Novel Therapeutic Approaches
 Asthma and Its Many Unmet Needs: Directions for Novel Therapeutic Approaches William W. Busse,, M.D. University of Wisconsin School of Medicine and Public Health Madison, WI, USA Disclosure Slide Employment
Asthma and Its Many Unmet Needs: Directions for Novel Therapeutic Approaches William W. Busse,, M.D. University of Wisconsin School of Medicine and Public Health Madison, WI, USA Disclosure Slide Employment
Clinical Implications of Asthma Phenotypes. Michael Schatz, MD, MS Department of Allergy
 Clinical Implications of Asthma Phenotypes Michael Schatz, MD, MS Department of Allergy Definition of Phenotype The observable properties of an organism that are produced by the interaction of the genotype
Clinical Implications of Asthma Phenotypes Michael Schatz, MD, MS Department of Allergy Definition of Phenotype The observable properties of an organism that are produced by the interaction of the genotype
Children First Medical Group Physicians. Steven Yedlin, MD, Chief Medical Officer Medical Director. DATE: January 3, 2008
 TO: FROM: Children First Medical Group Physicians Steven Yedlin, MD, Chief Medical Officer Medical Director DATE: January 3, 2008 RE: Asthma Clinical Practice Guideline Revision Children First Medical
TO: FROM: Children First Medical Group Physicians Steven Yedlin, MD, Chief Medical Officer Medical Director DATE: January 3, 2008 RE: Asthma Clinical Practice Guideline Revision Children First Medical
What is this patient s diagnosis?
 Asthma and COPD KANTA VELAMURI, MD ASSOCIATE PROFESSOR OF MEDICINE PULMONARY, CRITICAL CARE AND SLEEP MEDICINE SECTION MICHAEL E. DEBAKEY VA MEDICAL CENTER BAYLOR COLLEGE OF MEDICINE Disclosures None Case
Asthma and COPD KANTA VELAMURI, MD ASSOCIATE PROFESSOR OF MEDICINE PULMONARY, CRITICAL CARE AND SLEEP MEDICINE SECTION MICHAEL E. DEBAKEY VA MEDICAL CENTER BAYLOR COLLEGE OF MEDICINE Disclosures None Case
SCREENING AND PREVENTION
 These protocols are designed to implement standard guidelines, based on the best evidence, that provide a consistent clinical experience for AHC II Integrated Clinical Delivery Network patients and allow
These protocols are designed to implement standard guidelines, based on the best evidence, that provide a consistent clinical experience for AHC II Integrated Clinical Delivery Network patients and allow
ASTHMA IN THE PEDIATRIC POPULATION
 ASTHMA IN THE PEDIATRIC POPULATION SEARCH Rotation 2 August 23, 2010 Objectives Define asthma as a chronic disease Discuss the morbidity of asthma in pediatrics Discuss a few things that a health center
ASTHMA IN THE PEDIATRIC POPULATION SEARCH Rotation 2 August 23, 2010 Objectives Define asthma as a chronic disease Discuss the morbidity of asthma in pediatrics Discuss a few things that a health center
Asthma - Chronic. Presentations of asthma Cough Wheeze Breathlessness Chest tightness
 Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
HARRISON COUNTY SCHOOLS OFFICE OF HEALTH SERVICES 445 W. Main Street Clarksburg, WV (304) FAX (304)
 FAX (304)") HARRISON COUNTY SCHOOLS OFFICE OF HEALTH SERVICES 44 W. Main Street Clarksburg, WV 6 (4) 6-769 FAX (4) 6-769 Dear Parent, Date Please complete the enclosed forms and return them to your school nurse. This
HARRISON COUNTY SCHOOLS OFFICE OF HEALTH SERVICES 44 W. Main Street Clarksburg, WV 6 (4) 6-769 FAX (4) 6-769 Dear Parent, Date Please complete the enclosed forms and return them to your school nurse. This
ADULT ASTHMA GUIDE SUMMARY. This summary provides busy health professionals with key guidance for assessing and treating adult asthma.
 ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
COPD COPD. Update on COPD and Asthma
 Update on COPD and Asthma Talmadge E. King, Jr., M.D. Krevins Distinguished Professor of Medicine Chair, Department of Medicine University of California San Francisco (UCSF) San Francisco, CA COPD COPD
Update on COPD and Asthma Talmadge E. King, Jr., M.D. Krevins Distinguished Professor of Medicine Chair, Department of Medicine University of California San Francisco (UCSF) San Francisco, CA COPD COPD
Provider Respiratory Inservice
 Provider Respiratory Inservice 2 Welcome Opening Remarks We will cover: Definition of Asthma & COPD Evidence based guidelines for diagnosis, evaluation, and management of asthma Evidence based guidelines
Provider Respiratory Inservice 2 Welcome Opening Remarks We will cover: Definition of Asthma & COPD Evidence based guidelines for diagnosis, evaluation, and management of asthma Evidence based guidelines
Allergy and Immunology Review Corner: Chapter 75 of Middleton s Allergy Principles and Practice, 7 th Edition, edited by N. Franklin Adkinson, et al.
 Allergy and Immunology Review Corner: Chapter 75 of Middleton s Allergy Principles and Practice, 7 th Edition, edited by N. Franklin Adkinson, et al. Chapter 75: Approach to Infants and Children with Asthma
Allergy and Immunology Review Corner: Chapter 75 of Middleton s Allergy Principles and Practice, 7 th Edition, edited by N. Franklin Adkinson, et al. Chapter 75: Approach to Infants and Children with Asthma
Yellow Zone Practice Parameters for Management of Acute Loss of Asthma Control
 Yellow Zone Practice Parameters for Management of Acute Loss of Asthma Control Asthma Educator Sharing Day Lansing, MI October 28, 2016 Karen Meyerson, MSN, APRN, NP-C, AE-C Director, Commercial Care Management
Yellow Zone Practice Parameters for Management of Acute Loss of Asthma Control Asthma Educator Sharing Day Lansing, MI October 28, 2016 Karen Meyerson, MSN, APRN, NP-C, AE-C Director, Commercial Care Management
In 2002, it was reported that 72 of 1000
 REPORTS Aligning Patient Care and Asthma Treatment Guidelines Eric Cannon, PharmD Abstract This article describes how the National Asthma Education and Prevention Program Guidelines for the Diagnosis and
REPORTS Aligning Patient Care and Asthma Treatment Guidelines Eric Cannon, PharmD Abstract This article describes how the National Asthma Education and Prevention Program Guidelines for the Diagnosis and
Asthma COPD Overlap (ACO)
") Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
Adult Asthma Clinical Practice Guideline Summary
 Adult Asthma Clinical Practice Guideline Summary The following evidence-based guideline was developed to assist Primary Care physicians and other clinicians in the management of asthma in adults. It was
Adult Asthma Clinical Practice Guideline Summary The following evidence-based guideline was developed to assist Primary Care physicians and other clinicians in the management of asthma in adults. It was
Asthma: Chronic Management. Yung-Yang Liu, MD Attending physician, Chest Department Taipei Veterans General Hospital April 26, 2015
 Asthma: Chronic Management Yung-Yang Liu, MD Attending physician, Chest Department Taipei Veterans General Hospital April 26, 2015 Global Strategy for Asthma Management and Prevention Evidence-based Implementation
Asthma: Chronic Management Yung-Yang Liu, MD Attending physician, Chest Department Taipei Veterans General Hospital April 26, 2015 Global Strategy for Asthma Management and Prevention Evidence-based Implementation
Known Allergies: Shellfish. Symptoms: abdominal pain, nausea, diarrhea, or vomiting. congestion, trouble breathing, or wheezing.
 CSTAR CASE STUDIES: BLOCK B Asthma or COPD? Setting: Walk in clinic. Dan: I havi g that cough thi g agai HPI: Dan is a 49-year-old male teacher who reports having had episodes of cough with mucus production
CSTAR CASE STUDIES: BLOCK B Asthma or COPD? Setting: Walk in clinic. Dan: I havi g that cough thi g agai HPI: Dan is a 49-year-old male teacher who reports having had episodes of cough with mucus production
Nancy Davis, RRT, AE-C
 Nancy Davis, RRT, AE-C Asthma Statistics 25.6 million Americans diagnosed with asthma 6.8 million are children 10.5 million missed school days per year 14.2 lost work days for adults Approximately 10%
Nancy Davis, RRT, AE-C Asthma Statistics 25.6 million Americans diagnosed with asthma 6.8 million are children 10.5 million missed school days per year 14.2 lost work days for adults Approximately 10%
ASTHMA CARE FOR CHILDREN BASKET OF CARE SUBCOMMITTEE Report to: Minnesota Department of Health. June 22, 2009
 This document is made available electronically by the Minnesota Legislative Reference Library as part of an ongoing digital archiving project. http://www.leg.state.mn.us/lrl/lrl.asp ASTHMA CARE FOR CHILDREN
This document is made available electronically by the Minnesota Legislative Reference Library as part of an ongoing digital archiving project. http://www.leg.state.mn.us/lrl/lrl.asp ASTHMA CARE FOR CHILDREN
Speaker Disclosure. Identification and Diagnosis of Asthma. Definition of Asthma. Objectives 11/9/2017
 Speaker Disclosure Identification and Diagnosis of Asthma Isabel L. Virella Lowell, MD, Associate Professor, Pulmonology and Sleep Medicine, University of Alabama at Birmingham Isabel Virella-Lowell, MD
Speaker Disclosure Identification and Diagnosis of Asthma Isabel L. Virella Lowell, MD, Associate Professor, Pulmonology and Sleep Medicine, University of Alabama at Birmingham Isabel Virella-Lowell, MD
Asthma and COPD. Health Net Provider Educational Webinar
 Asthma and COPD Health Net Provider Educational Webinar AstraZeneca 2015 Disclosures Presenters today are employed by Astra Zeneca and have nothing to disclose. This presentation is free from bias. 2 Objectives
Asthma and COPD Health Net Provider Educational Webinar AstraZeneca 2015 Disclosures Presenters today are employed by Astra Zeneca and have nothing to disclose. This presentation is free from bias. 2 Objectives
Your Guide to MANAGING ASTHMA
 Your Guide to MANAGING ASTHMA Asthma affects more than 24 MILLION AMERICANS. It is a chronic disease that causes your airways to become inflamed, making it hard to breathe. There is no cure for asthma.
Your Guide to MANAGING ASTHMA Asthma affects more than 24 MILLION AMERICANS. It is a chronic disease that causes your airways to become inflamed, making it hard to breathe. There is no cure for asthma.
COPD and Asthma Update. April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute
 COPD and Asthma Update April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute What we ll be talking about COPD: diagnosis, management of stable COPD, COPD exacerbations Asthma: diagnosis,
COPD and Asthma Update April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute What we ll be talking about COPD: diagnosis, management of stable COPD, COPD exacerbations Asthma: diagnosis,
The methodology behind GINA and EPR-3 medication recommendations: Stepwise treatment in asthma
 The methodology behind GINA and EPR-3 medication recommendations: Stepwise treatment in asthma Maureen George PhD RN AE-C FAAN Columbia University mg3656@cumc.columbia.edu Faculty Disclosures Maureen George
The methodology behind GINA and EPR-3 medication recommendations: Stepwise treatment in asthma Maureen George PhD RN AE-C FAAN Columbia University mg3656@cumc.columbia.edu Faculty Disclosures Maureen George
Current Approaches to Asthma & COPD
 10/11/18 Current Approaches to Asthma & COPD Lekshmi Santhosh, M.D. Assistant Professor, Pulm/Critical Care & Hosp Med Primary Care Medicine: Principles & Practice 10.11.2018 Revisiting the Dutch Hypothesis:
10/11/18 Current Approaches to Asthma & COPD Lekshmi Santhosh, M.D. Assistant Professor, Pulm/Critical Care & Hosp Med Primary Care Medicine: Principles & Practice 10.11.2018 Revisiting the Dutch Hypothesis:
Asthma Update A/Prof. John Abisheganaden. Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital
 Asthma Update - 2013 A/Prof. John Abisheganaden Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital Asthma A complex syndrome Multifaceted disease Heterogeneous Genetic and
Asthma Update - 2013 A/Prof. John Abisheganaden Senior Consultant, Dept Of Respiratory & Crit Care Medicine Tan Tock Seng Hospital Asthma A complex syndrome Multifaceted disease Heterogeneous Genetic and
(Asthma) Diagnosis, monitoring and chronic asthma management
 Diagnosis, monitoring and chronic asthma management") Dubai Standards of Care 2018 (Asthma) Diagnosis, monitoring and chronic asthma management Preface Asthma is one of the most common problem dealt with in daily practice. In Dubai, the management of chronic
Dubai Standards of Care 2018 (Asthma) Diagnosis, monitoring and chronic asthma management Preface Asthma is one of the most common problem dealt with in daily practice. In Dubai, the management of chronic
TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS
 TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Recommendation PULMONARY FUNCTION TESTING (SPIROMETRY) Conditional: The Expert Panel that spirometry measurements FEV1,
TARGET POPULATION Eligibility Inclusion Criterion Exclusion Criterion RECOMMENDATIONS Recommendation PULMONARY FUNCTION TESTING (SPIROMETRY) Conditional: The Expert Panel that spirometry measurements FEV1,
Glen Ellyn Pharmacy Complementary Asthma Management Program Initial Visit
 Asthma Project Goals: Decrease hospitalizations Decrease use of asthma medications Increase peak flow readings Improve quality of life Decrease doctor visits Page 1 of 10 Page 2 of 10 Patient Name: Patient
Asthma Project Goals: Decrease hospitalizations Decrease use of asthma medications Increase peak flow readings Improve quality of life Decrease doctor visits Page 1 of 10 Page 2 of 10 Patient Name: Patient
Life-long asthma and its relationship to COPD. Stephen T Holgate School of Medicine University of Southampton
 Life-long asthma and its relationship to COPD Stephen T Holgate School of Medicine University of Southampton Definitions COPD is a preventable and treatable disease with some significant extrapulmonary
Life-long asthma and its relationship to COPD Stephen T Holgate School of Medicine University of Southampton Definitions COPD is a preventable and treatable disease with some significant extrapulmonary
Differential diagnosis
 Differential diagnosis The onset of COPD is insidious. Pathological changes may begin years before symptoms appear. The major differential diagnosis is asthma, and in some cases, a clear distinction between
Differential diagnosis The onset of COPD is insidious. Pathological changes may begin years before symptoms appear. The major differential diagnosis is asthma, and in some cases, a clear distinction between
DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL
 DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL Definition Guidelines contact complicated definitions Central to this is Presence of symptoms Variable airflow obstruction Diagnosis
DR REBECCA THOMAS CONSULTANT RESPIRATORY PHYSICIAN YORK DISTRICT HOSPITAL Definition Guidelines contact complicated definitions Central to this is Presence of symptoms Variable airflow obstruction Diagnosis
ASTHMA. Epidemiology. Pathophysiology. Diagnosis. IAP UG Teaching slides
 BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
Asthma. Rachel Miller, MD, FAAAAI Director Allergy and Immunology New York Presbyterian Hospital. Figure 1 Asthma Prevalence,
 Asthma Rachel Miller, MD, FAAAAI Director Allergy and Immunology New York Presbyterian Hospital Figure 1 Asthma Prevalence, 1980-2000 * Gap between 1995-1996 and 1997 indicates a break in trend due to
Asthma Rachel Miller, MD, FAAAAI Director Allergy and Immunology New York Presbyterian Hospital Figure 1 Asthma Prevalence, 1980-2000 * Gap between 1995-1996 and 1997 indicates a break in trend due to
Sources. Taking Charge of Your Asthma. Asthma Action Plan (to be completed with your doctor) UnitedHealthcare Insurance Company
 UnitedHealthcare Insurance Company") Asthma Action Plan (to be completed with your doctor) Green Zone: (80 to 00% of my personal best) Peak Flow between and (00% = personal best) You can do all the things you usually do. Your asthma medicine
Asthma Action Plan (to be completed with your doctor) Green Zone: (80 to 00% of my personal best) Peak Flow between and (00% = personal best) You can do all the things you usually do. Your asthma medicine
ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1
 ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1 1. Richard Beasley, Bob Hancox, Matire Harwood, Kyle Perrin, Betty Poot, Janine Pilcher, Jim Reid, Api Talemaitoga,
ASTHMA & RESPIRATORY FOUNDATION NZ ADULT ASTHMA GUIDELINES: A QUICK REFERENCE GUIDE 1 1. Richard Beasley, Bob Hancox, Matire Harwood, Kyle Perrin, Betty Poot, Janine Pilcher, Jim Reid, Api Talemaitoga,
Management of wheeze in pre-school children. Prof Colin Robertson, Respiratory Medicine, Royal Children s Hospital, Melbourne
 Management of wheeze in pre-school children Prof Colin Robertson, Respiratory Medicine, Royal Children s Hospital, Melbourne General Practitioner encounters for asthma Asthma in Australia, 2003 Emergency
Management of wheeze in pre-school children Prof Colin Robertson, Respiratory Medicine, Royal Children s Hospital, Melbourne General Practitioner encounters for asthma Asthma in Australia, 2003 Emergency
Asthma By Mayo Clinic staff
 MayoClinic.com reprints This single copy is for your personal, noncommercial use only. For permission to reprint multiple copies or to order presentation-ready copies for distribution, use the reprints
MayoClinic.com reprints This single copy is for your personal, noncommercial use only. For permission to reprint multiple copies or to order presentation-ready copies for distribution, use the reprints
Significance. Asthma Definition. Focus on Asthma
 Focus on Asthma (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Asthma Definition Chronic inflammatory disorder of airways Causes airway hyperresponsiveness
Focus on Asthma (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Asthma Definition Chronic inflammatory disorder of airways Causes airway hyperresponsiveness
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series. Pediatric Asthma: Assessment & Control August 2, :00pm 1:00pm
 Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Pediatric Asthma: Assessment & Control August 2, 2017 12:00pm 1:00pm Allyson S. Larkin, MD Assistant Professor of Pediatrics
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Pediatric Asthma: Assessment & Control August 2, 2017 12:00pm 1:00pm Allyson S. Larkin, MD Assistant Professor of Pediatrics
Guideline for the Diagnosis and Management of Chronic Childhood Asthma
 Guideline for the Diagnosis and Management of Chronic Childhood Asthma Guideline developed by Larry A. Simmons, MD, FAAP, Associate Professor of Pediatrics, Department of Pediatrics, UAMS at Arkansas Children
Guideline for the Diagnosis and Management of Chronic Childhood Asthma Guideline developed by Larry A. Simmons, MD, FAAP, Associate Professor of Pediatrics, Department of Pediatrics, UAMS at Arkansas Children
Alberta Childhood Asthma Pathway for Primary Care
 Asthma Diagnosis Box 1 Diagnosis: Based on symptom pattern, careful and thorough history of symptoms (wheeze, cough, night waking and activity limitations), and assessment of family history of asthma and
Asthma Diagnosis Box 1 Diagnosis: Based on symptom pattern, careful and thorough history of symptoms (wheeze, cough, night waking and activity limitations), and assessment of family history of asthma and
Update on management of respiratory symptoms. Dr Farid Bazari Consultant Respiratory Physician Kingston Hospital NHS FT
 Update on management of respiratory symptoms Dr Farid Bazari Consultant Respiratory Physician Kingston Hospital NHS FT Topics The common respiratory symptoms Cough: causes, diagnosis and therapy Update
Update on management of respiratory symptoms Dr Farid Bazari Consultant Respiratory Physician Kingston Hospital NHS FT Topics The common respiratory symptoms Cough: causes, diagnosis and therapy Update
What is Asthma? Chronic disease of the airways that may cause Wheezing Breathlessness Chest tightness Night time or early morning coughing
 Asthma What is Asthma? Chronic disease of the airways that may cause Wheezing Breathlessness Chest tightness Night time or early morning coughing Episodes are usually associated with widespread, but
Asthma What is Asthma? Chronic disease of the airways that may cause Wheezing Breathlessness Chest tightness Night time or early morning coughing Episodes are usually associated with widespread, but
Asthma in Pregnancy. Asthma. Chronic Airway Inflammation. Objective Measures of Airflow. Peak exp. flow rate (PEFR)
") Chronic Airway Inflammation Asthma in Pregnancy Robin Field, MD Maternal Fetal Medicine Kaiser Permanente San Francisco Asthma Chronic airway inflammation increased airway responsiveness to a variety of
Chronic Airway Inflammation Asthma in Pregnancy Robin Field, MD Maternal Fetal Medicine Kaiser Permanente San Francisco Asthma Chronic airway inflammation increased airway responsiveness to a variety of
Connecting Health & Housing: Asthma and the Home. Presented by: The California-Nevada Public Health Training Center
 Connecting Health & Housing: Asthma and the Home Presented by: The California-Nevada Public Health Training Center Funded by Grant #UB6HP20202 from the Health Resources and Services Administration, U.S.
Connecting Health & Housing: Asthma and the Home Presented by: The California-Nevada Public Health Training Center Funded by Grant #UB6HP20202 from the Health Resources and Services Administration, U.S.
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER
 MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER 16 year old female with h/o moderate persistent asthma presents to the ED after 6 hours of difficulty breathing, cough, and wheezing
MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER 16 year old female with h/o moderate persistent asthma presents to the ED after 6 hours of difficulty breathing, cough, and wheezing
Medicine Dr. Kawa Lecture 1 Asthma Obstructive & Restrictive Pulmonary Diseases Obstructive Pulmonary Disease Indicate obstruction to flow of air
 Medicine Dr. Kawa Lecture 1 Asthma Obstructive & Restrictive Pulmonary Diseases Obstructive Pulmonary Disease Indicate obstruction to flow of air through the airways. As asthma, COPD ( chronic bronchitis
Medicine Dr. Kawa Lecture 1 Asthma Obstructive & Restrictive Pulmonary Diseases Obstructive Pulmonary Disease Indicate obstruction to flow of air through the airways. As asthma, COPD ( chronic bronchitis
CME/CE POSTTEST CME/CE QUESTIONS
 CME/CE POSTTEST CME/CE QUESTIONS Controlling Asthma Severity: Identifying Unmet Needs and Optimizing Therapeutic Options There are no fees for participating in and receiving continuing medical education
CME/CE POSTTEST CME/CE QUESTIONS Controlling Asthma Severity: Identifying Unmet Needs and Optimizing Therapeutic Options There are no fees for participating in and receiving continuing medical education
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Controversial Issues in the Management of Childhood Asthma: Insights from NIH Asthma Network Studies
 Controversial Issues in the Management of Childhood Asthma: Insights from NIH Asthma Network Studies Stanley J. Szefler, MD Helen Wohlberg and Herman Lambert Chair in Pharmacokinetics, Head, Pediatric
Controversial Issues in the Management of Childhood Asthma: Insights from NIH Asthma Network Studies Stanley J. Szefler, MD Helen Wohlberg and Herman Lambert Chair in Pharmacokinetics, Head, Pediatric