Advanced Airway Management
|
|
|
- Evangeline Edwards
- 5 years ago
- Views:
Transcription
1 CHAPTER 37 Advanced Airway Management
2 Airway Anatomy and Physiology Review
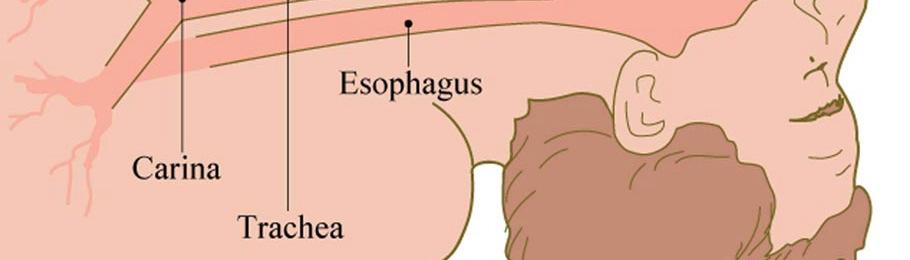
3 Respiratory System: The Airway
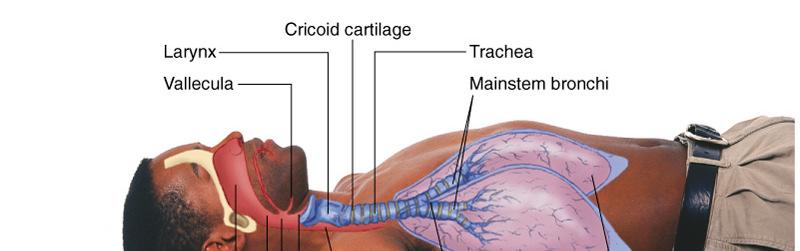
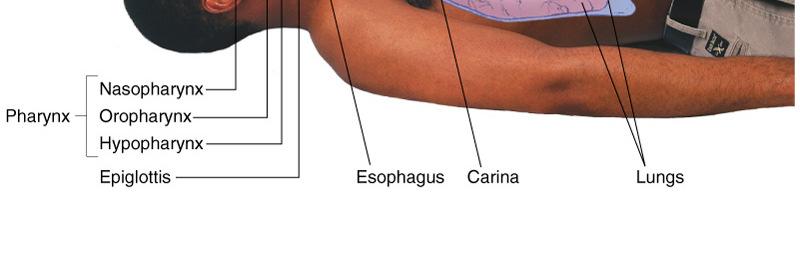
4 Respiratory System (Supine)
5 Physiology: Factors of Adequate Breathing Functioning brainstem Open airway Intact chest wall Alveolar gas exchange Changes in any of these may result in inadequate breathing!
6 Adequate Breathing: Normal Breath Rates Adults 12-20/min Children 15-30/min Infants 25-50/min
7 Adequate Breathing Rhythm Quality Depth Usually regular Breath sounds audible with stethoscope Minimal effort Chest expands normally
8 Signs of Inadequate Breathing Rate Rhythm Depth Outside normal range (too fast or slow) Irregular pattern Chest expansion shallow
9 Signs of Inadequate Breathing Quality Abnormal breath sounds (unequal, diminished, or absent) Chest expansion unequal Increased breathing effort Use of accessory muscles Inability to speak full sentences
10 Signs of Inadequate Breathing Skin Retractions Agonal Respirations Pale, cyanotic, cool, or clammy Above clavicles, between/below ribs Just before respiratory arrest
11 Airway Differences between Adults and Children
12 Differences between the Airways of Children & Adults Mouth and nose smaller Tongue is proportionally larger Trachea is softer & narrow Cricoid cartilage is narrowest opening Diaphragm performs most work
13 Signs of Inadequate Breathing In Infants and Children Slow heart rates Weak/absent peripheral pulse Retractions Nasal flaring Seesaw breathing
14 Suctioning Always be prepared for the need to suction the patient s airway as needed. Have suction equipment ready for use!
15 Advanced Airway Management
16 Orotracheal Intubation Advantages Complete control of the airway Allows direct ventilation of the lungs Minimizes risk of aspiration Better oxygen delivery Allows deep suctioning
17 Orotracheal Intubation Complications Stimulation of airway can cause bradycardia Trauma to lips, teeth, tongue, gums, airway structures Continued
18 Orotracheal Intubation Complications Hypoxia from prolonged attempts Right mainstem intubation Continued
19 Orotracheal Intubation Complications Esophageal intubation Vomiting Self-extubation Movement of tube out of trachea when patient moves


20 Equipment: Body Substance Isolation
21 Orotracheal Intubation Equipment Laryngoscope handle Laryngoscope blades Assorted sizes (0-4) Curved or straight Straight preferred for infants/children


22 Laryngoscope Blades

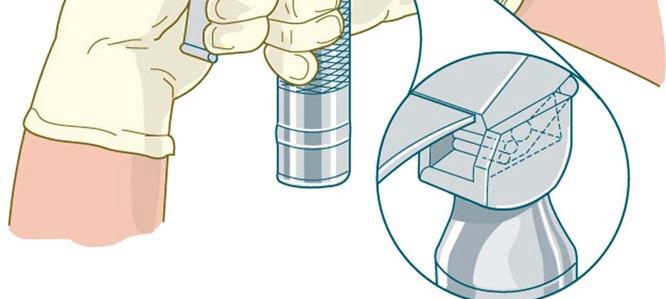
23 Assembly of Laryngoscope Handle and Blade
24 Assembly of Laryngoscope Handle and Blade
25 Straight blade brings vocal cords into view by lifting the epiglottis.
26 Curved blade brings vocal cords into view by lifting vallecula and indirectly lifting epiglottis.
27 Endotracheal Tubes Range in size (inner diameter) from 2.0 (smallest) to 10.0 (largest) Have a standard 15mm bag valve connection
28 Endotracheal Tubes Average Sizes (inner diameter) Adult Female: Adult Male: mm mm
29 Endotracheal Tube
30 Endotracheal Tubes Emergency Rule: 7.5 fits most adults. Have available one size larger and one size smaller.
31 Endotracheal Intubation Useful Dimensions Teeth to vocal cords: Teeth to suprasternal notch: Teeth to carina: Teeth to tip: 15 cm 20 cm 25 cm 22 cm
32 Endotracheal Intubation Stylet Provides stiffness/shape. Lubricant may ease removal. Use to shape tube like hockey stick. Do not let stylet go past the proximal end of the Murphy eye.


33 Stylet Stylet in Place
34 Endotracheal Intubation Other Equipment Water-soluble lubricant 10 cc syringe Securing devices Suction unit Towels
35 Endotracheal Intubation Indications Inability to ventilate apneic patient Protect airway when no cough or gag reflex Protect airway of patient unresponsive to painful stimuli Cardiac arrest


36 Ensure proper ventilation of the patient.


37 Assemble, prepare, and test equipment.


38 Position patient s head. If trauma is suspected, have a rescuer hold the head in a neutral position.


39 Insert laryngoscope blade into mouth, avoiding contact with teeth.


40 Lift tongue up and sweep to the left.


41 Lift mandible; do not use a fulcrum motion.
42 Have rescuer apply Sellick s maneuver (bring vocal cords into view).
43 Visualize glottic opening between vocal cords.


44 Gently insert ET tube (with stylet in place) until cuff passes between vocal cords.

45 Make sure airway structures are aligned.


46 Remove laryngoscope and stylet without moving tube. Inflate cuff with 5-10 cc of air.


47 Attach bag-valve resuscitator and ventilate. Observe rise of chest.


48 Confirm placement by auscultating epigastrium and lungs.
49 Confirm Correct Tube Placement Visualize tube passing through vocal cords. Observe chest rise and fall.
50 Confirm Correct Tube Placement Observe for signs of deterioration, such as cyanosis. As protocols direct, use pulse oximeter or CO 2 detector.


51 If correct placement is confirmed, secure tube and continue to ventilate.
52 Incorrect Tube Placement If breath sounds present only on right: Deflate cuff. Ventilate, and while auscultating over lungs, Withdraw tube slightly until breath sounds are equal. Secure tube and ventilate.
53 Incorrect Tube Placement If sounds present only in epigastrium: Deflate cuff. Remove tube. Ventilate for at least 1 minute. Reattempt intubation.
54 Tube Placement Reassess breath sounds after every major move: From scene to ambulance From ambulance to hospital
55 Sellick s Maneuver (Cricoid Pressure)
56 Sellick s Maneuver Purpose To help prevent regurgitation and aspiration during endotracheal intubation
57 Key Term Cricoid Cartilage Surrounds entire trachea; it is inferior to cricothyroid membrane (depression below thyroid cartilage or Adam s apple).

58 Location of Cricoid Cartilage


59 Perform Sellick s maneuver by exerting posterior pressure on cricoid cartilage.
60 Sellick s Maneuver Verify correct position to avoid damaging other structures. Cricoid more difficult to find in infants/children.
61 Infant and Child Intubation
62 Anatomic and Physiologic Considerations Smaller mouth and nose Tongue larger proportionally Floppier epiglottis Smaller glottic opening
63 Anatomic and Physiologic Considerations Harder to see vocal cords Narrower trachea Less rigid cricoid cartilage Increased reliance on diaphragm for breathing




64 Child and Adult Airways Cricoid Cartilage
65 Infant and Child Intubation Special Considerations Since cricoid ring narrowest part of child s airway: Pediatric tube has no cuff Tube size depends on size of cricoid ring
66 Infant and Child Intubation Purpose Most effective means of controlling airway. In apneic patients, it also allows deeper suctioning.
67 Infant and Child Intubation Indications Prolonged artificial ventilation required Inability to ventilate by other means
68 Infant and Child Intubation Indications Apnea Cardiac arrest Unresponsive with no cough or gag reflex
69 Infant and Child Intubation Advantages Prevents gastric distention Minimizes risk of aspiration Permits suctioning of airway secretions
70 Infant and Child Intubation Equipment Bag-valve mask with mask of correct size Laryngoscope handle & blades
71 Infant and Child Intubation Equipment Laryngoscope Blades Straight blade allows: Greater displacement of tongue Better visualization of glottis (preferred in infants)
72 Infant and Child Intubation Equipment Laryngoscope Blades Curved blade Inserted into vallecula to allow visualization of glottis, cords Preferred in older children
73 Infant and Child Intubation Tube Size Consult chart or tape. In general, use: for newborns, small infants 4.0 up to 1 year old
74 Infant and Child Intubation TUBE SIZE FORMULA 16 + Age (years) 4 = Tube Size (mm)
75 Infant and Child Intubation Alternative tube size selection Use tube same size as little finger or that will fit nostril. Have tubes one size larger and smaller available.
76 Infant and Child Intubation ET Tubes Use UNCUFFED tubes for children up to 8 years old (narrowing of cricoid acts as a cuff).


77 Uncuffed ET Tube for Child Under 8 Years Old
78 Infant and Child Intubation ET Tubes Use CUFFED tubes for children older than 8 years. Tube should have marker for vocal cords, to assure proper insertion depth.
79 Pediatric ET Tube Distances Age Depth year 12 cm 2 years 14 cm 4-6 years 16 cm 6-10 years 18 cm years 20 cm Measured from teeth to mid-trachea
80 Endotracheal Intubation Equipment Pediatric stylet Water-soluble lubricant 10 cc syringe Securing devices Suction unit Towels
81 Infant and Child Intubation Techniques Ventilate appropriately. Assemble and test equipment. Take BSI precautions.
82 Infant and Child Intubation Techniques Monitor heart rate throughout. Stimulating airway may slow heart rate. If this happens, stop and ventilate.


83 Place head in sniffing position. If trauma is suspected, have rescuer hold head in neutral position.
84 Infant and Child Intubation Techniques Insert laryngoscope blade into right corner of mouth. Sweep tongue out of way.
85 Infant and Child Intubation Techniques Insert end of blade into position. Lift mandible.
86 Infant and Child Intubation Techniques Consider using Sellick s maneuver. Visualize glottic opening and vocal cords.
87 Infant and Child Intubation Techniques Gently insert tube until glottic marker (if present) is at level of vocal cords. If using cuffed tube, insert cuff beyond vocal cords.
88 Infant and Child Intubation Techniques Holding tube, remove laryngoscope blade and stylet. Attach bag-valve and ventilate. Confirm correct placement.
89 Infant and Child Intubation Confirming Placement Observe chest rise and fall. Auscultate lung sounds. Auscultate epigastrium for absence of sounds. Assess for improving skin color & heart rate.
90 Infant and Child Intubation Confirming Placement If correct placement confirmed, secure tube and continue to ventilate.
91 Infant and Child Intubation Techniques Ventilate patient at a rate appropriate for age. Note tube's depth of insertion. May insert oral airway as a bite block.
92 Incorrect Tube Placement If breath sounds present only on right: Deflate cuff (if used). Ventilate, and while auscultating over lung, withdraw tube slightly until breath sounds are equal. Secure tube and ventilate.
93 Incorrect Tube Placement If sounds present only in epigastrium: Deflate cuff (if used). Remove tube. Ventilate for at least 1 minute. Reattempt intubation.
94 Infant and Child Intubation Techniques Once tube is secured, secure head to prevent movement that can dislodge tube.
95 Infant and Child Intubation Techniques Reassess breath sounds after every major move: Scene to ambulance Ambulance to hospital
96 Infant and Child Intubation Complications If tube in proper place, but inadequate lung expansion: Tube may be too small. Auscultate neck. Replace with larger tube. Consider cuffed tube if child is older than 8 years old.
97 Infant and Child Intubation Complications If tube is in proper place, but inadequate lung expansion: Check if pop-off valve on bag-valve device is activated. Check for a leak in bag-valve device.
98 Infant and Child Intubation Complications If tube in proper place, but inadequate lung expansion: Possible inadequate compression of bag. Check for tube blocked with secretions. Continued
99 Infant and Child Intubation Complications Suction endotracheally; Replace tube.
100 Nasogastric Tubes
101 Nasogastric Tubes Indications Inability to ventilate infant/child because of gastric distention Unresponsive infant/ child with gastric distention
102 Nasogastric Tubes Reasons for Use: Decompress stomach Gastric lavage Administration of medications/nutrition
103 Nasogastric Tubes Contraindications Presence of major face, head, or spine trauma. Use orogastric technique instead.
104 Nasogastric Tubes Complications Tracheal intubation Nasal trauma Emesis Passage into cranium through basilar skull fracture
105 Nasogastric Tubes Tube Sizes Newborn/Infant Toddler/Preschool School-age Adolescent 8.0 French 10.0 French 12.0 French French
106 Nasogastric Tubes Equipment 20 cc syringe Water-soluble lubricant Emesis basin Tape, stethoscope Suction unit and catheters


107 Nasogastric Intubation Infant/Child: Use BSI; oxygenate patient; prepare and assemble equipment.


108 Measure tube from tip of nose, around ear, to below xiphoid process.


109 Pass lubricated tube downward along nasal floor into stomach.


110 Confirm placement as you inject cc air. Listen for bubbling.


111 Aspirate stomach contents.


112 Secure tube in place.
113 Orotracheal Suctioning Deep Tracheal Suctioning
114 Orotracheal Suctioning Indications: Obvious secretions in endotracheal tube Poor compliance with bag valve
115 Orotracheal Suctioning Complications Hypoxia Cardiac dysrhythmias Trauma to airway Bronchospasm Laryngospasm Coughing


116 Preoxygenate and hyperventilate patient.


117 Carefully check equipment. Use BSI.
118 Approximate depth of insertion by measuring the suction catheter from lips, to the ear, to the nipple line.


119 Insert catheter without suction. Use sterile technique.


120 Advance catheter no farther than carina.
 and")

121 Apply suction (no more than 15 seconds) and withdraw catheter in a twisting motion. Resume ventilations.
122 Combitubes

123 A Dual Lumen Airway
124 Combitubes Indication Unconscious patient in need of airway management
125 Combitubes Contraindications: Conscious patient Patient with gag reflex Under 5 feet tall Under 16 years old Ingestion of caustic substance Known esophageal disease
126 Combitubes Insertion Techniques Take BSI precautions. Ventilate with bag-valve mask. Prepare and check equipment. Have suction readily available. If patient becomes conscious, at any time, remove the tube!


127 Lubricate the Combitube
128 Combitube Insertion Techniques Insert device blindly along center of the mouth. Advance device until the teeth are centered between the black rings on the Combitube.


129 Insert the Combitube.
130 Combitubes Insertion Techniques Inflate valve #1 cuff with 100 cc of air. Inflate valve #2 cuff with 15 cc of air.

131 Combitube in place with cuffs inflated.


132 Ventilate through tube #1 (blue tube).
133 Combitubes Insertion Techniques Auscultate for lung sounds and the absence of epigastric sounds. If lung sounds are present and no epigastric sounds are heard, continue ventilating through the blue tube (tube #1).


134 If no lung sounds are present and epigastric sounds are heard, ventilate through the shorter tube (tube #2).
135 Laryngeal Mask Airway (LMA)

136 A Laryngeal Mask Airway
137 Laryngeal Mask Airway Insertion Techniques Take BSI precautions. Ventilate with bag-valve mask. Prepare and check equipment. Have suction readily available. Place patient in a sniffing position.
138 Laryngeal Mask Airway Insertion Techniques Lubricate the posterior side of cuff. Insert tube with open side facing anteriorly. Stop when resistance is felt.


139 Inserting the LMA
140 Laryngeal Mask Airway Insertion Techniques Inflate cuff with air based on size of LMA. Ventilate through the tube. Auscultate for lung sounds and the absence of epigastric sounds. Insert an oral airway as a bite block.
141 Automatic Transport Ventilators (ATVs)

142 An Automatic Transport Ventilator
143 Automatic Transport Ventilators Protocols may allow use in place of bag-valve mask. Controls set rate of ventilations and weight-based tidal volume.
144 Review Questions 1. Explain the differences between orotracheal and oropharyngeal suctioning. 2. Explain why nasogastric tubes are used in an infant or child. 3. Explain the purpose of Sellick s maneuver.
145 Review Questions 4. Explain the purpose of orotracheal intubation and the complications that can arise during intubation. 5. Explain the procedures for assuring correct placement of an endotracheal tube. 6. Describe the differences between child and adult airways.

146 STREET SCENES What priority would you assign the patient? What definitive treatment do pulseless patients require? What alternatives for managing the airway might you consider?
147 STREET SCENES What assessment procedures should be performed at this time? How often should this patient be reassessed?
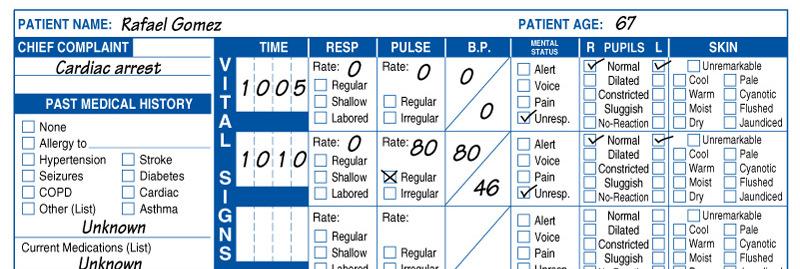
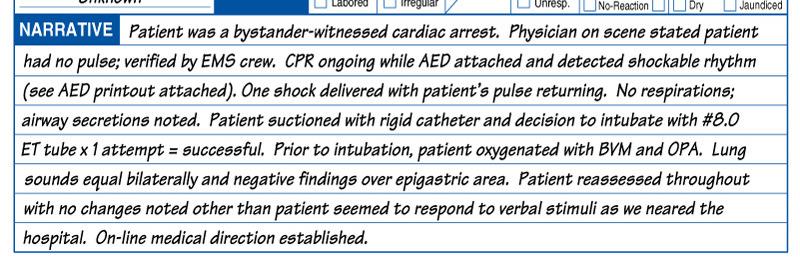
148 Sample Documentation
Overview. Chapter 37. Advanced Airway Techniques. Sellick Maneuver 9/11/2012
 Chapter 37 Advanced Airway Techniques Slide 1 Sellick Maneuver Purpose Anatomic Location Technique Special Considerations Overview Advanced Airway Management of Adults Esophageal Tracheal Combitubes Tracheal
Chapter 37 Advanced Airway Techniques Slide 1 Sellick Maneuver Purpose Anatomic Location Technique Special Considerations Overview Advanced Airway Management of Adults Esophageal Tracheal Combitubes Tracheal
Airway/Breathing. Chapter 5
 Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to
 1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only. In
1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only. In
Chapter 40 Advanced Airway Management
 1 2 3 4 5 Chapter 40 Advanced Airway Management Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only.
1 2 3 4 5 Chapter 40 Advanced Airway Management Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only.
Waitin In The Wings. Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider
 Indications and Use for the Pre-Hospital Provider") Waitin In The Wings Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider 1 CombiTube Kit General Description The CombiTube is A double-lumen tube with
Waitin In The Wings Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider 1 CombiTube Kit General Description The CombiTube is A double-lumen tube with
Pediatric Patients. BCFPD Paramedic Education Program. EMS Education Paramedic Level
 Pediatric Patients BCFPD Program Basic Considerations Much of the initial patient assessment can be done during visual examination of the scene. Involve the caregiver or parent as much as possible. Allow
Pediatric Patients BCFPD Program Basic Considerations Much of the initial patient assessment can be done during visual examination of the scene. Involve the caregiver or parent as much as possible. Allow
Airway/Breathing. Chapter 5
 Airway/Breathing Chapter 5 Airway/Breathing Introduction Rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur rapidly
Airway/Breathing Chapter 5 Airway/Breathing Introduction Rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur rapidly
Advanced Airway Management. University of Colorado Medical School Rural Track
 Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
General Medical Procedure. Emergency Airway Techniques (General Airway Protocol)
") General Medical Procedure Appropriate airway management is often the most important intervention a prehospital care provider makes, as ensuring adequate oxygenation and ventilation is crucial to the survival
General Medical Procedure Appropriate airway management is often the most important intervention a prehospital care provider makes, as ensuring adequate oxygenation and ventilation is crucial to the survival
Equipment: NRP algorithm, MRSOPA table, medication chart, SpO 2 table Warm
 NRP Skills Stations Performance Skills Station OR Integrated Skills Station STATION: Assisting with and insertion of endotracheal tube (ETT) Equipment: NRP algorithm, MRSOPA table, medication chart, SpO
NRP Skills Stations Performance Skills Station OR Integrated Skills Station STATION: Assisting with and insertion of endotracheal tube (ETT) Equipment: NRP algorithm, MRSOPA table, medication chart, SpO
Orotracheal Intubation
 T h e n e w e ng l a nd j o u r na l o f m e dic i n e videos in clinical medicine Orotracheal Intubation Christopher Kabrhel, M.D., Todd W. Thomsen, M.D., Gary S. Setnik, M.D., and Ron M. Walls, M.D.
T h e n e w e ng l a nd j o u r na l o f m e dic i n e videos in clinical medicine Orotracheal Intubation Christopher Kabrhel, M.D., Todd W. Thomsen, M.D., Gary S. Setnik, M.D., and Ron M. Walls, M.D.
Airway/Breathing. Chapter 5
 Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid, assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid, assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
Adult Intubation Skill Sheet
 Adult Intubation 2. Opens the airway manually and inserts an oral airway *** 3. Ventilates the patient with BVM attached to oxygen at 15 lpm *** 4. Directs assistant to oxygenate the patient 5. Selects
Adult Intubation 2. Opens the airway manually and inserts an oral airway *** 3. Ventilates the patient with BVM attached to oxygen at 15 lpm *** 4. Directs assistant to oxygenate the patient 5. Selects
Introducing the Fastrach-LMA. Prepared by Jim Medeiros, NREMT-P Regional Field Coordinator Lord Fairfax EMS Council
 Introducing the Fastrach-LMA Prepared by Jim Medeiros, NREMT-P Regional Field Coordinator Lord Fairfax EMS Council Objectives Review Anatomy of the Upper Airway Review LFEMSC LMA Protocol Discuss Indications
Introducing the Fastrach-LMA Prepared by Jim Medeiros, NREMT-P Regional Field Coordinator Lord Fairfax EMS Council Objectives Review Anatomy of the Upper Airway Review LFEMSC LMA Protocol Discuss Indications
Anatomy and Physiology. The airways can be divided in to parts namely: The upper airway. The lower airway.
 Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
Michigan General Procedures EMERGENCY AIRWAY. Date: November 15, 2012 Page 1 of 16
 Date: November 15, 2012 Page 1 of 16 Emergency Airway Effective airway management and ventilation are important lifesaving interventions that all EMS providers must be able to perform. The approach to
Date: November 15, 2012 Page 1 of 16 Emergency Airway Effective airway management and ventilation are important lifesaving interventions that all EMS providers must be able to perform. The approach to
PEMSS PROTOCOLS INVASIVE PROCEDURES
 PEMSS PROTOCOLS INVASIVE PROCEDURES Panhandle Emergency Medical Services System SURGICAL AND NEEDLE CRICOTHYROTOMY Inability to intubate is the primary indication for creating an artificial airway. Care
PEMSS PROTOCOLS INVASIVE PROCEDURES Panhandle Emergency Medical Services System SURGICAL AND NEEDLE CRICOTHYROTOMY Inability to intubate is the primary indication for creating an artificial airway. Care
ADVANCED AIRWAY PROCEDURES
 ADVANCED AIRWAY PROCEDURES This procedure includes the following: Endotracheal intubation (plus use of Supraglottic Airway Laryngopharyngeal Tube (S.A.L.T. device), gum elastic bougie assisted tracheal
ADVANCED AIRWAY PROCEDURES This procedure includes the following: Endotracheal intubation (plus use of Supraglottic Airway Laryngopharyngeal Tube (S.A.L.T. device), gum elastic bougie assisted tracheal
Other methods for maintaining the airway (not definitive airway as still unprotected):
:") Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
The Pediatric Patient. Morgen Bernius, MD NCEMS Conference February 24, 2007
 The Pediatric Patient Morgen Bernius, MD NCEMS Conference February 24, 2007 Rule #1: Everyone Loves the Pediatric Patient Pediatrics in EMS Approximately 10% of all EMS treatment is for children younger
The Pediatric Patient Morgen Bernius, MD NCEMS Conference February 24, 2007 Rule #1: Everyone Loves the Pediatric Patient Pediatrics in EMS Approximately 10% of all EMS treatment is for children younger
PRODUCTS FOR THE DIFFICULT AIRWAY. Courtesy of Cook Critical Care
 PRODUCTS FOR THE DIFFICULT AIRWAY Courtesy of Cook Critical Care EMERGENCY CRICOTHYROTOMY Thyroid Cartilage Access Site Cricoid Cartilage Identify the cricothyroid membrane between the cricoid and thyroid
PRODUCTS FOR THE DIFFICULT AIRWAY Courtesy of Cook Critical Care EMERGENCY CRICOTHYROTOMY Thyroid Cartilage Access Site Cricoid Cartilage Identify the cricothyroid membrane between the cricoid and thyroid
Airway Anatomy. Soft palate. Hard palate. Nasopharynx. Tongue. Oropharynx. Hypopharynx. Thyroid cartilage
 Airway Anatomy Hard palate Soft palate Tongue Nasopharynx Oropharynx Hypopharynx Thyroid cartilage Airway Anatomy Hyoid bone Thyroid cartilage Cricoid cartilage Trachea Cricothyroid membrane Airway Anatomy
Airway Anatomy Hard palate Soft palate Tongue Nasopharynx Oropharynx Hypopharynx Thyroid cartilage Airway Anatomy Hyoid bone Thyroid cartilage Cricoid cartilage Trachea Cricothyroid membrane Airway Anatomy
Airway Workshop Lecture. University of Ottawa
 Airway Workshop Lecture Department of Anesthesiology University of Ottawa Overview Ventilation Airway assessment Difficult airways Airway management equipment aids Intubation/Improving Intubation Success
Airway Workshop Lecture Department of Anesthesiology University of Ottawa Overview Ventilation Airway assessment Difficult airways Airway management equipment aids Intubation/Improving Intubation Success
1. Review the anatomy and physiology of the respiratory system.
 By Mike Stricker 1. Review the anatomy and physiology of the respiratory system. 2. Review the assessment process. 3. Review the management of airway and ventilation status. 4. Review the advanced management
By Mike Stricker 1. Review the anatomy and physiology of the respiratory system. 2. Review the assessment process. 3. Review the management of airway and ventilation status. 4. Review the advanced management
ADVANCED AIRWAY MANAGEMENT
 The Advanced Airway Management protocol should be used on all patients requiring advanced airway management procedures. This protocol is divided into three sections the Crash Airway Algorithm, the Rapid
The Advanced Airway Management protocol should be used on all patients requiring advanced airway management procedures. This protocol is divided into three sections the Crash Airway Algorithm, the Rapid
This interdisciplinary clinical support document provides guidelines for the safe establishment of an artificial airway.
 PURPOSE This interdisciplinary clinical support document provides guidelines for the safe establishment of an artificial airway. POLICY STATEMENTS Endotracheal intubation will be performed by the Most
PURPOSE This interdisciplinary clinical support document provides guidelines for the safe establishment of an artificial airway. POLICY STATEMENTS Endotracheal intubation will be performed by the Most
Angkana Lurngnateetape,, MD. Department of Anesthesiology Siriraj Hospital
 AIRWAY MANAGEMENT Angkana Lurngnateetape,, MD. Department of Anesthesiology Siriraj Hospital Perhaps the most important responsibility of the anesthesiologist is management of the patient s airway Miller
AIRWAY MANAGEMENT Angkana Lurngnateetape,, MD. Department of Anesthesiology Siriraj Hospital Perhaps the most important responsibility of the anesthesiologist is management of the patient s airway Miller
AIRWAY MANAGEMENT AND VENTILATION
 AIRWAY MANAGEMENT AND VENTILATION D1 AIRWAY MANAGEMENT AND VENTILATION Basic airway management and ventilation The laryngeal mask airway and Combitube Advanced techniques of airway management D2 Basic
AIRWAY MANAGEMENT AND VENTILATION D1 AIRWAY MANAGEMENT AND VENTILATION Basic airway management and ventilation The laryngeal mask airway and Combitube Advanced techniques of airway management D2 Basic
We will not be using the King LTS-D in our system!
 King LT-D The King LT is a superior, disposable supraglottic airway tool that utilizes the latest technological advances in materials and design to provide the best nonintubating airway possible. The King
King LT-D The King LT is a superior, disposable supraglottic airway tool that utilizes the latest technological advances in materials and design to provide the best nonintubating airway possible. The King
AIRWAY MANAGEMENT SUZANNE BROWN, CRNA
 AIRWAY MANAGEMENT SUZANNE BROWN, CRNA OBJECTIVE OF LECTURE Non Anesthesia Sedation Providers Review for CRNA s Informal Questions encouraged 2 AIRWAY MANAGEMENT AWARENESS BASICS OF ANATOMY EQUIPMENT 3
AIRWAY MANAGEMENT SUZANNE BROWN, CRNA OBJECTIVE OF LECTURE Non Anesthesia Sedation Providers Review for CRNA s Informal Questions encouraged 2 AIRWAY MANAGEMENT AWARENESS BASICS OF ANATOMY EQUIPMENT 3
Chapter 10. Objectives. Objectives 01/09/2013. Airway Management, Artificial Ventilation, and Oxygenation
 Chapter 10 Airway Management, Artificial Ventilation, and Oxygenation Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights
Chapter 10 Airway Management, Artificial Ventilation, and Oxygenation Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights
Airway and Ventilation. Emergency Medical Response
 Airway and Ventilation Lesson 14: Airway and Ventilation You Are the Emergency Medical Responder Your medical emergency response team has been called to the fitness center by building security on a report
Airway and Ventilation Lesson 14: Airway and Ventilation You Are the Emergency Medical Responder Your medical emergency response team has been called to the fitness center by building security on a report
CARDIAC EMERGENCIES Other Cardiac Dysrhythmias C9
 CARDIAC EMERGENCIES Other Cardiac Dysrhythmias C9 ATRIAL FLUTTER Variable rate depending on block. Atrial rate between 250-350, saw-tooth pattern. (see Appendix B for energy settings for bi-phasic low
CARDIAC EMERGENCIES Other Cardiac Dysrhythmias C9 ATRIAL FLUTTER Variable rate depending on block. Atrial rate between 250-350, saw-tooth pattern. (see Appendix B for energy settings for bi-phasic low
Blind Insertion Airway Devices (BIAD)
") P03 Procedures 2017-05-12 All ages Office of the Medical Director Blind Insertion Airway Devices (BIAD) Primary Intermediate Advanced Critical From AIRWAY & BREATHING MANAGEMENT or AIRWAY OBSTRUCTION Yes
P03 Procedures 2017-05-12 All ages Office of the Medical Director Blind Insertion Airway Devices (BIAD) Primary Intermediate Advanced Critical From AIRWAY & BREATHING MANAGEMENT or AIRWAY OBSTRUCTION Yes
Introduction to Emergency Medical Care 1
 Introduction to Emergency Medical Care 1 OBJECTIVES 8.1 Define key terms introduced in this chapter. Slides 12 15, 21, 24, 31-34, 39, 40, 54 8.2 Describe the anatomy and physiology of the upper and lower
Introduction to Emergency Medical Care 1 OBJECTIVES 8.1 Define key terms introduced in this chapter. Slides 12 15, 21, 24, 31-34, 39, 40, 54 8.2 Describe the anatomy and physiology of the upper and lower
Educational Session: Evaluation and Management of the Difficult Airway
 Educational Session: Evaluation and Management of the Difficult Airway Diane M. Birnbaumer, MD, FACEP 3/24/2010 7:30 AM - 8:30 AM The Difficult Airway What s Up YOUR Sleeve? Diane M. Birnbaumer, M.D.,
Educational Session: Evaluation and Management of the Difficult Airway Diane M. Birnbaumer, MD, FACEP 3/24/2010 7:30 AM - 8:30 AM The Difficult Airway What s Up YOUR Sleeve? Diane M. Birnbaumer, M.D.,
Airway Management Adult
 Airway Management Adult Goals: Provide effective oxygenation and ventilation; recognize and alleviate respiratory distress or failure; provide necessary interventions quickly and safely to patients who
Airway Management Adult Goals: Provide effective oxygenation and ventilation; recognize and alleviate respiratory distress or failure; provide necessary interventions quickly and safely to patients who
Airway Management and Ventilation. Eric V. Ernest, M.D., EMT-P Department of Emergency Medicine University of Nebraska Medical Center
 Airway Management and Ventilation Eric V. Ernest, M.D., EMT-P Department of Emergency Medicine University of Nebraska Medical Center Airway/Ventilation Overview Respiratory Assessment Supplemental Oxygen
Airway Management and Ventilation Eric V. Ernest, M.D., EMT-P Department of Emergency Medicine University of Nebraska Medical Center Airway/Ventilation Overview Respiratory Assessment Supplemental Oxygen
and most critical steps in the initial assessment of every patient you will encounter.
 1 Chapter 8 Airway Management and Ventilation 2 Airway management and ventilation are the and most critical steps in the initial assessment of every patient you will encounter. 3 Respiratory Problems 4
1 Chapter 8 Airway Management and Ventilation 2 Airway management and ventilation are the and most critical steps in the initial assessment of every patient you will encounter. 3 Respiratory Problems 4
Airway Management From Brady s First Responder (8th Edition) 82 Questions
 82 Questions") Airway Management From Brady s First Responder (8th Edition) 82 Questions 1. What color will cyanotic skin be? p. 119 *A.) Blue B.) Red C.) Yellow D.) Green 2. Which is the primary path for air to enter
Airway Management From Brady s First Responder (8th Edition) 82 Questions 1. What color will cyanotic skin be? p. 119 *A.) Blue B.) Red C.) Yellow D.) Green 2. Which is the primary path for air to enter
Overview. The Team Concept. Chapter 7. Assisting the ALS Provider 9/11/2012. The Team Concept ALS Procedures and Equipment
 Chapter 7 Assisting the ALS Provider Slide 1 Overview The Team Concept ALS Procedures and Equipment Electrocardiogram (ECG) Monitoring Slide 2 The Team Concept Prehospital care involves many individuals
Chapter 7 Assisting the ALS Provider Slide 1 Overview The Team Concept ALS Procedures and Equipment Electrocardiogram (ECG) Monitoring Slide 2 The Team Concept Prehospital care involves many individuals
1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be
 1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be difficult to determine. Even for physician in hospital
1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be difficult to determine. Even for physician in hospital
Basic Airway Management
 Basic Airway Management Dr. Madhurita Singh, Assoc. Professor, Dept. of Critical Care, CMC Vellore. This is the first module in a series on management of airway and ventilation in critically ill patients.
Basic Airway Management Dr. Madhurita Singh, Assoc. Professor, Dept. of Critical Care, CMC Vellore. This is the first module in a series on management of airway and ventilation in critically ill patients.
Anatomy Review. Anatomy Review. Respiratory Emergencies CHAPTER 16
 CHAPTER 16 Respiratory Emergencies Anatomy Review Anatomy Review 1 Pediatric Anatomy Airway structure differences Proportionally larger tongue Smaller, more flexible trachea Abdominal breathers Reasons
CHAPTER 16 Respiratory Emergencies Anatomy Review Anatomy Review 1 Pediatric Anatomy Airway structure differences Proportionally larger tongue Smaller, more flexible trachea Abdominal breathers Reasons
CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS
 CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS PRACTICAL STATIONS CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS 1. CARDIAC ARREST MANAGEMENT 2. AIRWAY & RESPIRATORY MANAGEMENT 3. SPINAL IMMOBILIZATION
CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS PRACTICAL STATIONS CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS 1. CARDIAC ARREST MANAGEMENT 2. AIRWAY & RESPIRATORY MANAGEMENT 3. SPINAL IMMOBILIZATION
Respiratory Emergencies
 CHAPTER 16 Respiratory Emergencies Anatomy Review Anatomy Review Pediatric Anatomy Airway structure differences Proportionally larger tongue Smaller, more flexible trachea Abdominal breathers Reasons for
CHAPTER 16 Respiratory Emergencies Anatomy Review Anatomy Review Pediatric Anatomy Airway structure differences Proportionally larger tongue Smaller, more flexible trachea Abdominal breathers Reasons for
student handbook BARS handbook September 2012.indd Front Cover 27/11/12 12:08 PM
 student handbook BARS handbook September 2012.indd Front Cover 27/11/12 12:08 PM All materials regarding the Basic Airway Resuscitation Strategy Course were written and developed by Dr. Richard Morris
student handbook BARS handbook September 2012.indd Front Cover 27/11/12 12:08 PM All materials regarding the Basic Airway Resuscitation Strategy Course were written and developed by Dr. Richard Morris
Module 2: Facilitator instructions for Airway & Breathing Skills Station
 Module 2: Facilitator instructions for Airway & Breathing Skills Station 1. Preparation a. Assemble equipment beforehand. b. Make sure that you have what you need and that it is functioning properly. 2.
Module 2: Facilitator instructions for Airway & Breathing Skills Station 1. Preparation a. Assemble equipment beforehand. b. Make sure that you have what you need and that it is functioning properly. 2.
Prior to applying a nonrebreathing mask on a patient with difficulty breathing, you should:!
 An elderly woman with COPD presents with a decreased level of consciousness, cyanosis to her face and neck, and labored respirations. Her pulse is rapid and weak and her oxygen saturation is 76%. You should:
An elderly woman with COPD presents with a decreased level of consciousness, cyanosis to her face and neck, and labored respirations. Her pulse is rapid and weak and her oxygen saturation is 76%. You should:
ITLS Pediatric Provider Course Advanced Pre-Test
 ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ACLS Provider Manual Supplementary Material
 ACLS Provider Manual Supplementary Material 2011 American Heart Association 1 Contents Airway Management... 4 Part 1: Basic Airway Management... 4 Devices to Provide Supplementary Oxygen... 4 Overview...
ACLS Provider Manual Supplementary Material 2011 American Heart Association 1 Contents Airway Management... 4 Part 1: Basic Airway Management... 4 Devices to Provide Supplementary Oxygen... 4 Overview...
RSPT Tracheal Aspiration. Tracheal Aspiration. RSPT 1410 Tracheal Aspiration
 1 RSPT 1410 2 is the use of to facilitate the removal of secretions from the respiratory tract. Under normal circumstances, patients with normal coughing do not have difficulty in removing secretions.
1 RSPT 1410 2 is the use of to facilitate the removal of secretions from the respiratory tract. Under normal circumstances, patients with normal coughing do not have difficulty in removing secretions.
Adult Advanced Cardiovascular Life Support. Emergency Procedures in PT
 Adult Advanced Cardiovascular Life Support Emergency Procedures in PT BLS Can be learned & practiced by the general public Includes: CPR First Aid (e.g. choking relief) Use of AED ACLS Used by healthcare
Adult Advanced Cardiovascular Life Support Emergency Procedures in PT BLS Can be learned & practiced by the general public Includes: CPR First Aid (e.g. choking relief) Use of AED ACLS Used by healthcare
Airway Management Essentials Self-Study Guide
 Airway Management Essentials Self-Study Guide Fourth Quarter 2010 Self-Study Guide Learning Objectives Cognitive Domain 1. Describe the various conditions that cause concern during treatment in the field
Airway Management Essentials Self-Study Guide Fourth Quarter 2010 Self-Study Guide Learning Objectives Cognitive Domain 1. Describe the various conditions that cause concern during treatment in the field
Airway Management. DFMRT Casualty Care Examination Course. Revision notes for. January Les Gordon
 Airway Management Revision notes for DFMRT Casualty Care Examination Course January 2013 Les Gordon Indicating special information in Revision Notes presentations New information since Casualty Care in
Airway Management Revision notes for DFMRT Casualty Care Examination Course January 2013 Les Gordon Indicating special information in Revision Notes presentations New information since Casualty Care in
Pediatrics 1 Neonatal Resuscitation Pediatric Assessment Airway Management. Neonatology. Topics. EMT Paramedic / Critical Refresher Session # 22
 EMT Paramedic / Critical Refresher Session # 22 Pediatrics 1 Neonatal Resuscitation Pediatric Assessment Airway Management 1 Neonatology 2 Topics Newborns & Neonates High Risk Newborn Patients APGAR Scoring
EMT Paramedic / Critical Refresher Session # 22 Pediatrics 1 Neonatal Resuscitation Pediatric Assessment Airway Management 1 Neonatology 2 Topics Newborns & Neonates High Risk Newborn Patients APGAR Scoring
Introduction. Topics. Seattle/King County EMT-B Class. EMS Online. Class schedule Message board Lecture presentations
 Seattle/King County EMT-B Class Introduction EMS Online http://www.emsonline.net/emtb Class schedule Message board Lecture presentations Topics Airway Management: Chapter 7 Patient Assessment: Chapter
Seattle/King County EMT-B Class Introduction EMS Online http://www.emsonline.net/emtb Class schedule Message board Lecture presentations Topics Airway Management: Chapter 7 Patient Assessment: Chapter
INTUBATION APPENDIX II. INDICATIONS AND CONTRAINDICATIONS II. COMPLICATIONS: APPENDIX: 2 TITLE: INTUBATION PROCEDURES. REVISED: May 1, 2016
 APPENDIX: TITLE: PROCEDURES REVISED: May 1, 016 I. BACKGROUND Advanced Airway Procedures and competency are the cornerstones of Paramedicine. True competency involves knowing not only how to control the
APPENDIX: TITLE: PROCEDURES REVISED: May 1, 016 I. BACKGROUND Advanced Airway Procedures and competency are the cornerstones of Paramedicine. True competency involves knowing not only how to control the
How to use the Control-Cric to perform a surgical cricothyrotomy
 TRAININGGROUNDS How to use the Control-Cric to perform a surgical cricothyrotomy Product Description The Control-Cric is a System which verifies tracheal location during a surgical airway procedure, without
TRAININGGROUNDS How to use the Control-Cric to perform a surgical cricothyrotomy Product Description The Control-Cric is a System which verifies tracheal location during a surgical airway procedure, without
Paediatric Resuscitation. EMS Rounds Gurinder Sangha MD Paediatric Emergency Fellow June 18, 2009
 Paediatric Resuscitation EMS Rounds Gurinder Sangha MD Paediatric Emergency Fellow June 18, 2009 Essentials of Resuscitation Airway Breathing Circulation AIRWAY Differences in Paediatric Airway Shorter
Paediatric Resuscitation EMS Rounds Gurinder Sangha MD Paediatric Emergency Fellow June 18, 2009 Essentials of Resuscitation Airway Breathing Circulation AIRWAY Differences in Paediatric Airway Shorter
Portage County EMS Annual Skills Labs
 Portage County EMS Annual Skills Labs Scope: Provide skills labs for all Emergency Medical Responders and First Response EMTs to assure proficiency of skills and satisfy the Wisconsin State approved Operational
Portage County EMS Annual Skills Labs Scope: Provide skills labs for all Emergency Medical Responders and First Response EMTs to assure proficiency of skills and satisfy the Wisconsin State approved Operational
Respiratory Emergencies. Chapter 11
 Respiratory Emergencies Chapter 11 Respiratory System Anatomy and Function of the Lung Characteristics of Adequate Breathing Normal rate and depth Regular breathing pattern Good breath sounds on both sides
Respiratory Emergencies Chapter 11 Respiratory System Anatomy and Function of the Lung Characteristics of Adequate Breathing Normal rate and depth Regular breathing pattern Good breath sounds on both sides
ENDOTRACHEAL INTUBATION POLICY
 POLICY Indications: Ineffective ventilation with mask and t-piece, or mask and bag technique Inability to maintain a patent airway Need or anticipation of need for prolonged ventilation Need for endotracheal
POLICY Indications: Ineffective ventilation with mask and t-piece, or mask and bag technique Inability to maintain a patent airway Need or anticipation of need for prolonged ventilation Need for endotracheal
RAPID SEQUENCE INTUBATION FOR THE RURAL DOC
 Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Braam de Klerk VICTORIA BC 240 RAPID SEQUENCE INTUBATION FOR
Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Braam de Klerk VICTORIA BC 240 RAPID SEQUENCE INTUBATION FOR
Airway Management. Teeradej Kuptanon, MD
 Airway Management Teeradej Kuptanon, MD Outline Anatomy Detect difficult airway Rapid sequence intubation Difficult ventilation Difficult intubation Surgical airway access ICU setting Intubation Difficult
Airway Management Teeradej Kuptanon, MD Outline Anatomy Detect difficult airway Rapid sequence intubation Difficult ventilation Difficult intubation Surgical airway access ICU setting Intubation Difficult
Dr.Bharghavi.M 2 nd year post graduate Dept of Anaesthesia
 DIFFICULT AIRWAY CANNOT VENTILATE, CANNOT INTUBATE. Dr.Bharghavi.M 2 nd year post graduate Dept of Anaesthesia Difficult airway According to AMERICAN SOCIETY OF ANAESTHESIOLOGISTS Difficult Airway is defined
DIFFICULT AIRWAY CANNOT VENTILATE, CANNOT INTUBATE. Dr.Bharghavi.M 2 nd year post graduate Dept of Anaesthesia Difficult airway According to AMERICAN SOCIETY OF ANAESTHESIOLOGISTS Difficult Airway is defined
BASIC LIFE SUPPORT (BLS)
") ADULT Suspected Foreign Body Airway Obstruction (FBAO) 1 If conscious, ask, "Are you choking?" 2 If patient is unable to speak and/or shakes head yes, give abdominal thrusts, (chest thrusts if pregnant
ADULT Suspected Foreign Body Airway Obstruction (FBAO) 1 If conscious, ask, "Are you choking?" 2 If patient is unable to speak and/or shakes head yes, give abdominal thrusts, (chest thrusts if pregnant
INTUBATION/RSI. PURPOSE: A. To facilitate secure, definitive control of the airway by endotracheal intubation in an expeditious and safe manner
 Manual: LifeLine Patient Care Protocols Section: Adult/Pediatrics Protocol #: AP1-009 Approval Date: 03/01/2018 Effective Date: 03/05/2018 Revision Due Date: 12/01/2018 INTUBATION/RSI PURPOSE: A. To facilitate
Manual: LifeLine Patient Care Protocols Section: Adult/Pediatrics Protocol #: AP1-009 Approval Date: 03/01/2018 Effective Date: 03/05/2018 Revision Due Date: 12/01/2018 INTUBATION/RSI PURPOSE: A. To facilitate
HeartCode PALS. PALS Actions Overview > Legend. Contents
 HeartCode PALS PALS Actions Overview > Legend Action buttons (round buttons) Clicking a round button initiates an action. Clicking this button, for example, checks the child s carotid pulse. Menu buttons
HeartCode PALS PALS Actions Overview > Legend Action buttons (round buttons) Clicking a round button initiates an action. Clicking this button, for example, checks the child s carotid pulse. Menu buttons
Rapid Sequence Induction
 Rapid Sequence Induction Virtual simultaneous administration, after preoxygenation, of a potent sedative agent and a rapidly acting neuromuscular blocking agent to facilitate rapid tracheal intubation
Rapid Sequence Induction Virtual simultaneous administration, after preoxygenation, of a potent sedative agent and a rapidly acting neuromuscular blocking agent to facilitate rapid tracheal intubation
ITLS Pediatric Provider Course Basic Pre-Test
 ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Respiratory Emergencies. Lesson Goal. Lesson Objectives 9/10/2012
 Respiratory Emergencies Lesson Goal Assess and provide timely treatment & transport to patients experiencing respiratory emergencies Lesson Objectives List parts of respiratory system and how they work
Respiratory Emergencies Lesson Goal Assess and provide timely treatment & transport to patients experiencing respiratory emergencies Lesson Objectives List parts of respiratory system and how they work
LESSON ASSIGNMENT. After completing this lesson, you should be able to:
 LESSON ASSIGNMENT LESSON 3 Cricothyroidotomy LESSON ASSIGNMENT Paragraphs 3-1 through 3-7. LESSON OBJECTIVES After completing this lesson, you should be able to: 3-1. Define cricothyroidotomy. 3-2. Identify
LESSON ASSIGNMENT LESSON 3 Cricothyroidotomy LESSON ASSIGNMENT Paragraphs 3-1 through 3-7. LESSON OBJECTIVES After completing this lesson, you should be able to: 3-1. Define cricothyroidotomy. 3-2. Identify
Sanders: Mosby's Paramedic Textbook, Revised 3 rd Edition PowerPoint Lecture Notes Chapter 19: Airway Management and Ventilation
 Sanders: Mosby's Paramedic Textbook, Revised 3 rd Edition PowerPoint Lecture Notes Chapter 19: Airway Management and Ventilation Chapter 19 Airway Management and Ventilation Objectives Distinguish between
Sanders: Mosby's Paramedic Textbook, Revised 3 rd Edition PowerPoint Lecture Notes Chapter 19: Airway Management and Ventilation Chapter 19 Airway Management and Ventilation Objectives Distinguish between
Respiratory Management in Pediatrics
 Respiratory Management in Pediatrics Children s Hospital Omaha Critical Care Transport Sue Holmer RN, C-NPT Objectives Examine the differences between the pediatric and adults airways. Recognize respiratory
Respiratory Management in Pediatrics Children s Hospital Omaha Critical Care Transport Sue Holmer RN, C-NPT Objectives Examine the differences between the pediatric and adults airways. Recognize respiratory
October Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE
 October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
DIFFICULT AIRWAY MANAGMENT. Dr.N.SANTHOSH KUMAR MD ANESTHESIA (2 nd Yr)
") DIFFICULT AIRWAY MANAGMENT Dr.N.SANTHOSH KUMAR MD ANESTHESIA (2 nd Yr) AIRWAY MANAGEMENT AND MAINTAINING OXYGENATION ARE THE FUNDAMENTAL RESPONSIBILITIES OF ANY BASIC DOCTOR. TO MANAGE A DIFFICULT AIRWAY,
DIFFICULT AIRWAY MANAGMENT Dr.N.SANTHOSH KUMAR MD ANESTHESIA (2 nd Yr) AIRWAY MANAGEMENT AND MAINTAINING OXYGENATION ARE THE FUNDAMENTAL RESPONSIBILITIES OF ANY BASIC DOCTOR. TO MANAGE A DIFFICULT AIRWAY,
Airway Management and The Difficult Airway
 Airway Management and The Difficult Airway Gary McCalla, MD, FACEP Medical Director REACH Air Medical Services Services 1 It is not enough to do your best, unless you have prepared to be the best. -John
Airway Management and The Difficult Airway Gary McCalla, MD, FACEP Medical Director REACH Air Medical Services Services 1 It is not enough to do your best, unless you have prepared to be the best. -John
12-Lead ECG. Cardioversion. Evaluator: Evaluator: Identifies indications and contraindication for 12-Lead. Identifies indications for cardioversion
 12-Lead ECG Cardioversion Identifies indications and contraindication for 12-Lead Identifies indications for cardioversion Assembles equipment Turns monitor on, applies pads and cables appropriately Prepares
12-Lead ECG Cardioversion Identifies indications and contraindication for 12-Lead Identifies indications for cardioversion Assembles equipment Turns monitor on, applies pads and cables appropriately Prepares
Chapter 2: Airway Management and Ventilation
 Chapter 2: Airway Management and Ventilation Objectives: Upon completion of this topic, the physician will be able to explain and demonstrate the principles of airway management. Specifically, the physician
Chapter 2: Airway Management and Ventilation Objectives: Upon completion of this topic, the physician will be able to explain and demonstrate the principles of airway management. Specifically, the physician
12/15/2010. Presented by: Jim Fox EMT-PS EMS-I EMS Assistant Coordinator Des Moines Fire Department
 Presented by: Jim Fox EMT-PS EMS-I EMS Assistant Coordinator Des Moines Fire Department History Controversies Airway Management King Combi-Tube Easy Tube ETI Instructions for use Anatomy of King airway
Presented by: Jim Fox EMT-PS EMS-I EMS Assistant Coordinator Des Moines Fire Department History Controversies Airway Management King Combi-Tube Easy Tube ETI Instructions for use Anatomy of King airway
All bedside percutaneously placed tracheostomies
 Page 1 of 5 Scope: All bedside percutaneously placed tracheostomies Population: All ICU personnel Outcomes: To standardize and outline the steps necessary to safely perform a percutaneous tracheostomy
Page 1 of 5 Scope: All bedside percutaneously placed tracheostomies Population: All ICU personnel Outcomes: To standardize and outline the steps necessary to safely perform a percutaneous tracheostomy
Airway management and ventilation are the and most critical steps in the initial assessment of every patient you will encounter.
 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Chapter 8 Airway Management and Ventilation Airway management and ventilation are the and most critical steps in the initial assessment of every patient you will encounter.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Chapter 8 Airway Management and Ventilation Airway management and ventilation are the and most critical steps in the initial assessment of every patient you will encounter.
promed Surgical Gowns Sterile Oropharyngeal Airway Guedels Solution
 promed Surgical Gowns Sterile Oropharyngeal Airway Guedels Solution What s behind the brand? promed is an established brand that has been in the Australian market for more than 40 years Product categories
promed Surgical Gowns Sterile Oropharyngeal Airway Guedels Solution What s behind the brand? promed is an established brand that has been in the Australian market for more than 40 years Product categories
Overview. The Respiratory System. Chapter 18. Respiratory Emergencies 9/11/2012
 Chapter 18 Respiratory Emergencies Slide 1 Overview Respiratory System Review Anatomy Physiology Breathing Assessment Adequate Breathing Breathing Difficulty Focused History and Physical Examination Emergency
Chapter 18 Respiratory Emergencies Slide 1 Overview Respiratory System Review Anatomy Physiology Breathing Assessment Adequate Breathing Breathing Difficulty Focused History and Physical Examination Emergency
Pediatric Emergencies. Lesson Goal. Lesson Objectives 9/10/2012
 Pediatric Emergencies Lesson Goal Explain special characteristics of infants and children to become both comfortable & efficient in treating pediatric emergencies Lesson Objectives Identify physical &
Pediatric Emergencies Lesson Goal Explain special characteristics of infants and children to become both comfortable & efficient in treating pediatric emergencies Lesson Objectives Identify physical &
Nursing General Essential ALS Classic SimMom* Anne Nursing Airway features Essential ALS Classic SimMom Anne
 General 3G Essential ALS Classic SimMom* Nursing Late free Simulated patient monitor Runs pre programmed LLEAP scenarios Adult Male Female genitalia Female breasts Pre recorded vocal sounds Live vocal
General 3G Essential ALS Classic SimMom* Nursing Late free Simulated patient monitor Runs pre programmed LLEAP scenarios Adult Male Female genitalia Female breasts Pre recorded vocal sounds Live vocal
DESIGNED FOR DIFFICULT TRACHEAL OR ESOPHAGEAL INTUBATION
 Airway Superglottic Kendall Combitube Esophageal/Tracheal Double Lumen Airway for Emergency or Difficult Intubation. Blind placement without laryngoscope Unique design provides patient airway with either
Airway Superglottic Kendall Combitube Esophageal/Tracheal Double Lumen Airway for Emergency or Difficult Intubation. Blind placement without laryngoscope Unique design provides patient airway with either
Pre-Hospital Laryngeal Mask Airway Insertion Program Overview
 Program Overview Program Title Student Eligibility Emergency Medical Technicians certified as Intermediates or Paramedics to perform endotracheal intubation in the Commonwealth of Massachusetts. Course
Program Overview Program Title Student Eligibility Emergency Medical Technicians certified as Intermediates or Paramedics to perform endotracheal intubation in the Commonwealth of Massachusetts. Course
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 14 Practical Anesthesia Key Points 2 14.1 General Anesthesia Have a clear plan before starting anesthesia Never use an unfamiliar anesthetic technique in an emergency
Surgical Care at the District Hospital 1 14 Practical Anesthesia Key Points 2 14.1 General Anesthesia Have a clear plan before starting anesthesia Never use an unfamiliar anesthetic technique in an emergency
LESSON ASSIGNMENT. Oral, Nasopharyngeal, and Nasotracheal Suctioning. After completing this lesson, you will be able to:
 LESSON ASSIGNMENT LESSON 4 Oral, Nasopharyngeal, and Nasotracheal Suctioning. LESSON ASSIGNMENT Paragraphs 4-1 through 4-4. LESSON OBJECTIVES After completing this lesson, you will be able to: 4-1. State/identify
LESSON ASSIGNMENT LESSON 4 Oral, Nasopharyngeal, and Nasotracheal Suctioning. LESSON ASSIGNMENT Paragraphs 4-1 through 4-4. LESSON OBJECTIVES After completing this lesson, you will be able to: 4-1. State/identify
Clearing the air.. How to assist and rescue neck breathing patients. Presented by: Don Hall MCD, CCC/SLP Sarah Markel RRT, MHA
 Clearing the air.. How to assist and rescue neck breathing patients Presented by: Don Hall MCD, CCC/SLP Sarah Markel RRT, MHA Learning Objectives Define common terms identified with total (laryngectomy)
Clearing the air.. How to assist and rescue neck breathing patients Presented by: Don Hall MCD, CCC/SLP Sarah Markel RRT, MHA Learning Objectives Define common terms identified with total (laryngectomy)
Emergency Department/Trauma Adult Airway Management Protocol
 Emergency Department/Trauma Adult Airway Management Protocol Purpose: A standardized protocol for management of the airway in the setting of trauma in an academic center, with the goal of maximizing successful
Emergency Department/Trauma Adult Airway Management Protocol Purpose: A standardized protocol for management of the airway in the setting of trauma in an academic center, with the goal of maximizing successful
They re not little adults, but they are little humans. Pearls for your next pediatric trauma patient. Children are little humans
 They re not little adults, but they are little humans Pearls for your next pediatric trauma patient Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen
They re not little adults, but they are little humans Pearls for your next pediatric trauma patient Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen
Pediatric CPR. Mustafa SERİNKEN MD Professor of Emergency Medicine, Pamukkale University, TURKEY
 Pediatric CPR Mustafa SERİNKEN MD Professor of Emergency Medicine, Pamukkale University, TURKEY What are the differences? Normal limits ADULT CARDIOPULMONARY ARREST CAUSES INFANTS AND CHILDREN İschemic
Pediatric CPR Mustafa SERİNKEN MD Professor of Emergency Medicine, Pamukkale University, TURKEY What are the differences? Normal limits ADULT CARDIOPULMONARY ARREST CAUSES INFANTS AND CHILDREN İschemic
H: Respiratory Care. Saskatchewan Association of Licensed Practical Nurses, Competency Profile for LPNs, 3rd Ed. 79
 H: Respiratory Care Saskatchewan Association of Licensed Practical Nurses, Competency Profile for LPNs, 3rd Ed. 79 Competency: H-1 Airway Management H-1-1 H-1-2 H-1-3 H-1-4 H-1-5 Demonstrate knowledge
H: Respiratory Care Saskatchewan Association of Licensed Practical Nurses, Competency Profile for LPNs, 3rd Ed. 79 Competency: H-1 Airway Management H-1-1 H-1-2 H-1-3 H-1-4 H-1-5 Demonstrate knowledge
EMERGENCY CARE. Advanced Patient Simulators 116 CALL US TOLL FREE AT
 EMERGENCY CARE Advanced Patient Simulators 116 CALL US TOLL FREE AT 800.882.6655 Our Code Blue III ALS training simulators allow you to teach high-performance, quality CPR by providing you with real-time
EMERGENCY CARE Advanced Patient Simulators 116 CALL US TOLL FREE AT 800.882.6655 Our Code Blue III ALS training simulators allow you to teach high-performance, quality CPR by providing you with real-time
Pediatric Shock. Hypovolemia. Sepsis. Most common cause of pediatric shock Small blood volumes (80cc/kg)
") Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Advanced Airways. An introduction to what, why, why not, and how.
 Advanced Airways An introduction to what, why, why not, and how. This presentation is about advanced airways. Not just what and how, but why and why not. The goal of all advanced airways is to protect
Advanced Airways An introduction to what, why, why not, and how. This presentation is about advanced airways. Not just what and how, but why and why not. The goal of all advanced airways is to protect
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials
 Preparatory Materials") Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and