Birmingham and Solihull Mental Health NHS Foundation Trust. Formulary. March 2013
|
|
|
- Morgan Freeman
- 6 years ago
- Views:
Transcription
1 Birmingham and Solihull Mental Health NHS Foundation Trust Formulary March
2 Table of contents Antipsychotics Introduction p3 1. Antipsychotics available p4 2. Mood stabilisers available p5 3. Prescribing guidance for the treatment of schizophrenia in adults p Monitoring of specific drugs p8 5. Pharmacological management of bipolar affective disorder p Management of a depressive episode p Pharmacological Aspects of long term treatment (relapse prevention) p Guidelines for the use of Paliperidone Long-Acting Injection p Guidance for the initiation of Clozapine for inpatients and patients p23-24 within home treatment services. 10. The prescribing of high dose and combination antipsychotic medication p25-32 Antidepressants 11. Antidepressants available p Pharmacological management of depression p Pharmacological management of generalised anxiety disorder p Hypnotics available p Managing insomnia p42-46 Dementia 16. Dementia p Prescribing guidance for dementia in BSMHFT p Guidance for the management of challenging behavioural p52-59 and psychological symptoms in dementia (BPSD) Treatments of ADHD 19. Treatments available p Treatment of ADHD p61-67 Treatment of addictions 21. Replacement therapies available p68 2
3 Introduction This is the first publication of the Birmingham and Solihull Mental Health Trust formulary document. We have compiled a list of the available mental health medicines within the Trust, along with the associated prescribing guidance developed by the Pharmacological Therapies Committee for a number of different mental health conditions. This should be seen as progress to date and will be extended in future and be included in future editions of the formulary. Whilst the document does not reference NICE technology appraisals specifically, all technology appraisals published by NICE that refer to mental health medicines are included in the formulary. The Pharmacological Therapies Committee will consider any further technology appraisals published by NICE for mental health medicines and these will be incorporated into the formulary within 3 months of the publication date of the guidance. This formulary does not specifically consider medicines for physical health conditions. Generally prescribers within BSMHFT will continue those physical health medicines that patients come into the trust on for inpatients. For patients in community services, physical health medicines will be prescribed by the GP. Physical health medicines may be prescribed by mental health prescribers but this will often follow initial prescription by general practitioners or specialists from other relevant health services. BSMHFT therefore follows the formularies of other local providers within the Birmingham and Solihull health community. These formularies can be accessed at University Hospitals Birmingham Heart of England Foundation Trust, Solihull CCG &Itemid=435 Sandwell and West Birmingham NHS Trust Birmingham Cross City CCG All mental health prescribing guidelines have been developed by pharmacy, medical and nursing staff. Primary care is often involved in development of guidance and is always offered the opportunity to comment prior to agreement by the Pharmacological Therapies Committee, ratification by Trust Clinical Governance Committee and publication. This formulary will be kept under regular review by the Pharmacological Therapies Committee and prescribing will be monitored by Pharmacy against the published formulary at least every 6 months. 3
4 Antipsychotics Antipsychotics available: Risperidone, Olanzapine, Quetiapine IR, Amisulpride, Haloperidol, Perphenazine, Sulpiride, Trifluoperazine, Zuclopenthixol, Flupentixol, Clozapine, Zotepine, Chlorpromazine, Pericyazine, Levomepromazine (for RT/PRN use only). Antipsychotics with additional requirements for prescribing - require consultant documentation of reasons for prescribing, (including why first tier drugs are not appropriate and why Clozapine is not an option if treatment-resistant) as well as the agreement of the long term prescribe Quetiapine XL, Aripiprazole, Pimozide, Penfluridol Asenapine Restricted antipsychotics require completion of specific form or application to pharmacy Risperidone LAI Paliperidone LAI Olanzapine LAI Associated guidance Pharmacological management of schizophrenia Pharmacological management of bipolar disorder Prescribing of risperidone or paliperidone long acting injections Initiation of Clozapine Prescribing of high dose antipsychotic medication 4
5 Mood stabilisers Mood stabilisers available: Valproate preparations Carbamazepine Lamotrigine Lithium Priadel is the preferred brand Preparations to manage antipsychotic side effects Procyclidine Trihexyphenidyl Orphenadrine Hyoscine Pirenzipine (unlicensed) 5
6 Prescribing guidance for the treatment of schizophrenia in adults Primary care make a referral to specialist mental health services Newly diagnosed Ongoing Treatment resistant Should be seen by appropriate service as soon as possible regardless of age. Make full assessment and diagnosis. Treat with a single oral antipsychotic, chosen from the list of available antipsychotics, at normal licensed doses or within the BNF maximum limit. (Some exceptions may be necessary for under 18s in FCAMHS and EIS. Consult individual product SPCs for further information). There is no good evidence for a difference in efficacy or outcomes between first and second generation antipsychotics. Both groups can be considered first choices. Facilitate the choice of medication by service user/carer by providing suitable information eg CMHP leaflets or Choice and Medication website. Ensure physical monitoring carried out as per trust guidelines, physical assessment and examination of service users. Monitor mental state objectively e.g. using recognised rating scale such as BPRS, PANNS, to assess response to treatment. If non-responsive despite increasing dose to maximum dose and checking for side effects and adherence then re-assess diagnosis and consider alternative medication Check medication adherence, using plasma assays if necessary. If problematic consider support for adherence before considering depot or other long acting preparation Assess side effects using rating scale eg GASS or LUNSERS. If problematic review medication with service user/carer and consider alternative medication Where maximum BNF doses are exceeded, follow Trust guidance on high dose antipsychotics. Ensure consent to treatment paperwork covers high dose antipsychotics. Assess co-morbid substance misuse and if appropriate refer to substance misuse services following dual diagnosis pathway Help service user to create advance statement Continue with physical health monitoring Once the patient is stable, there are no significant risks and prescribing is considered suitable for primary care then consider with the patient s GP the transfer of prescribing to primary care (see below). Offer Clozapine if there is an inadequate response to the sequential use of two different antipsychotics, prescribed at adequate doses for a reasonable length of time, at least one of which is a non-clozapine second generation antipsychotic Consider Clozapine augmentation if a partial response has been seen and serum levels are within therapeutic range. Agents for which there is evidence include Sulpiride, Amisulpride, Risperidone or Lamotrigine If Clozapine is not appropriate and high dose antipsychotics are considered, follow Trust high dose antipsychotics treatment guidance. Ensure consent to treatment paperwork covers high dose antipsychotics. Follow RCPsych guidance on prescribing medicines off-label 6
7 When service users mental state has responded to treatment and they are stable on the minimum effective dose consider return to primary care who will then take on responsibility for physical monitoring (see Appendix 1). The definition of stability is: No significant change in the prescription for a minimum of one month. No increases of doses of any treatment and no new treatment starts. No significant acute risks. Any compliance issues are manageable in primary care. Liaise with primary care with regard to any issues of risk Be prepared to retain prescribing if GP is uncomfortable or unwilling to take on complex prescribing. High dose antipsychotic prescribing should normally be retained within specialist services. Violence and Aggression: For guidance on the treatment of violence and aggression with medication refer to the trust Rapid Tranquilisation Policy References 1. NICE Schizophrenia March An update of NICE clinical guideline 1 2. List Choice of Approved and Medication Medicines accessed (Tier 1) via Trust intranet 3. UKPPG patient information leaflets available on trust intranet risperidone, olanzapine, quetiapine, amisulpride, haloperidol, perphenazine, sulpiride, trifluoperazine, zuclopenthixol, flupentixol, clozapine, zotepine, 4. chlorpromazine, Bazire S. Psychotropic pericyazine, Drug levomepromazine Directory 2010 (for RT/PRN use only). 5. Parker C: Antipsychotics in the treatment of schizophrenia. Progress in neurology and psychiatry. 2009;13(2): flupentixol Royal Coll. decanoate, of Psychiatrists. fluphenazine College decanoate, Report CR142. haloperidol January decanoate, Use pipotiazine of licensed palmitate, medicines zuclopentixol for unlicensed decanoate applications in psychiatric practice. Medicines with additional requirements for prescribing (Tier 2) require consultant documentation of reasons for prescribing, (including why first tier drugs are not appropriate and why clozapine is not an option if treatment-resistant) as well as the agreement of the long term prescriber Quetiapine XL (See PTC guidance), aripiprazole, pimozide, penfluridol Restricted Medicines (Tier 3) follow procedure for restricted medicines Paliperidone (oral), Risperidone LAI, Olanzapine LAI, Paliperidone LAI 7
8 Appendix 1 Monitoring of specific drugs According to product summary of characteristics and NICE guidance, patients receiving the following medications should receive additional specific monitoring. Further advice is available from pharmacy. Time Period Prior to treatment During treatment initiation Lithium Thyroid function tests Renal function U & E s Weight/BMI ECG if risk factors for CV disease Serum Lithium levels regularly until stable Sodium Valproate / Semisodium Valproate Liver function tests Full blood count BMI Weight/BMI Carbamazepine Venlafaxine Antipsychotics LFT s Renal function U&E s FBC Blood pressure Pulse rate Monitor blood pressure and pulse rate regularly until stable and after dose increases U+Es Renal function FBC Blood Lipids Weight/BMI Plasma glucose ECG Blood pressure Liver function tests Blood pressure Weight/BMI Three monthly Serum Lithium levels Blood Lipids Weight/BMI Blood pressure Plasma glucose 6 monthly In addition to three monthly monitoring: Annually Renal function U & E s Thyroid function test In addition to three monthly and six monthly checks: Weight/BMI LFTs FBC In addition to six monthly monitoring: Weight/BMI LFT Renal function U+Es FBC Blood pressure Pulse rate (at high doses) U+Es Renal function FBC Blood Lipids Weight/BMI Plasma glucose ECG (for Haloperidol, Pimozide, Sertindole and Clozapine) Liver function test 8
9 Pharmacological management of bipolar affective disorder Management of an acute manic / mixed episode Valproate, antipsychotics, Lithium and Carbamazepine all have evidence as monotherapy in mania. Valproate or an antipsychotic are recommended first line, because of their rapid effect. (Note valproate should not normally be prescribed for women of child-bearing potential) Care should be taken in using Carbamazepine due to risks of interaction. For patients who suffer a manic or mixed episode while on long term treatment, ensure that the highest well-tolerated dose of the current treatment is offered. For Lithium, check serum levels are within the therapeutic range (0.5 1 mmol/l); consider establishing a higher serum level within the therapeutic range. Valproate Should be titrated quickly for rapid effect (e.g. Semi-sodium valproate 750mg on day 1, increase to 20mg/kg day 2). Semi-sodium Valproate (Depakote) is licensed for manic episodes associated with bipolar disorder but not long term preventative treatment. Antipsychotics There is little evidence to inform choice of antipsychotic. Many of the typical antipsychotics have evidence as monotherapy in mania. It should be noted that there is evidence that bipolar patients may be at higher risk of motor side effects than schizophrenic patients. Using high doses (such as greater than 30mg haloperidol per day) is not recommended. Of the Atypicals, Risperidone, Olanzapine, Quetiapine*, Aripiprazole* and Asenapine have evidence as monotherapy in mania and are all licensed. When choosing an antipsychotic, consider whether it may form part of longer-term treatment after the resolution of the acute episode. If so, consider using an antipsychotic with good evidence in long term treatment. * Quetiapine XL and Aripiprazole should only be used in cases where there is a clear additional benefit over other antipsychotics for an individual patient, and this should be documented both in the patient s record and an appropriate form completed on RiO. These drugs should only be prescribed by a consultant, and in the case acute teams in functionalised services, also require the approval of the community consultant. Use of Asenapine Asenapine is available in BSMHFT for the acute treatment of bipolar mania, where other treatments are not appropriate due to lack of tolerability or lack of efficacy, but where Clozapine is not indicated. The use of Asenapine should be intensively monitored to ensure judicious use and permit an evaluation of the clinical effectiveness of the medicine. All requests for Asenapine should be made by consultant psychiatrists to central pharmacy using the existing paperwork used for approval of prescriptions for other branded atypical antipsychotics. Approval will be made where: Use is within the terms of the product license, and A baseline YMRS score is included, and Evidence that first tier antipsychotic options have been precluded, and 9
10 Evidence of failed trial of valproate (where appropriate*), and Evidence that Clozapine has been considered and is not indicated *consider carefully in females of child-bearing potential to facilitate this process, a temporary approval form has been prepared (see appendix 2) Applications for Asenapine will be considered where there is evidence of a clear physical health issue conferring the need for administration by the sublingual route. Evaluation of the effectiveness of use of asenapine will be made by: Comparing baseline YMRS score with YMRS score on day 21 of treatment Completion of a suitable assessment of tolerability on day 21 of treatment Prescribing may be initiated and continued by any clinical team providing that this remains within the terms of the product license. In all cases, a plan should be in place to withdraw asenapine once the acute phase of illness is over, instituting a maintenance treatment if necessary. Currently Sycrest (asenapine) is a black triangle status medicine, and as such is subject to intensive monitoring. All suspected adverse effects should be reported using a yellow card. Asenapine should not be prescribed on FP10 prescriptions or by primary care physicians; it is to be considered hospital only until further notice. Lithium In view of the risks of withdrawal mania, Lithium should only be prescribed in cases where long term Lithium treatment for relapse-prevention is planned, and where the patient is predicted to be compliant with the medication. Those initiated on Lithium will require monitoring in accordance with the NICE guidance, and this needs to be recorded in a Lithium record book as per recent NPSA guidance. Benzodiazepines and rapid tranquillisation For the treatment of agitated behaviour refer to the BSMHFT rapid tranquillisation policy, and consider the use of Lorazepam or Diazepam. To promote sleep for agitated, overactive patients in the short term, follow the BSMHFT insomnia guideline, including considering adjunctive treatment with hypnotic medication, such as Temazepam or Zopiclone. It is better to use Benzodiazepines for sedation than high dose antipsychotic. Antidepressants Antidepressants should be tapered and discontinued at a rate determined by the likelihood of withdrawal symptoms and by the patient's previous history. Inadequate response to first line treatment If symptoms are inadequately controlled with optimized doses of the first-line medicine and/or mania is very severe, add another medicine. Consider the combination of Lithium or Valproate with an antipsychotic Consider Clozapine in more refractory illness Electro-convulsive therapy (ECT) may be considered for manic patients who are severely ill and/or whose mania is treatment resistant, those patients who express a preference for ECT and patients with severe mania during pregnancy. 10
11 Initial treatment scheme mania episode (from BAP Guidelines, 2009) Diagnosis Bipolar disorder Manic episode Assessment Communication Safety, patient and family preferences and consider need for admission Explain treatment plan incl. need for medicines Severity Severe Mild i.m Rx if required Oral Rx Oral Rx antipsychotic or Benzodiazepine antipsychotic or Valproate antipsychotic or Valproate or Lithium (or Carbamazepine) On Antidepressant? Taper and discontinue Sleep deprived? Consider Benzodiazepine short term Already on long term treatment? Optimise and continue Review response Good response Poor response Consider maintenance Rx Combination Rx or ECT 11
12 Management of a depressive episode For patients becoming depressed on long term treatment, first consider optimising this treatment. If the patient fails to respond, initiate further treatment. Antipsychotics Quetiapine has good RCT evidence for the management of bipolar depression and is also licensed for mania and bipolar depression. The majority of the trials have been conducted using standard release Quetiapine at doses of 300mg or 600mg. There is one trial involving quetiapine XL*. Olanzapine has limited evidence as monotherapy, but good evidence in combination with Fluoxetine. It is licensed for mania but not bipolar depression. Aripiprazole* is only licensed for mania. It has failed to separate from placebo in monotherapy trials for bipolar depression, but has some evidence that it augments SSRIs in treatment-resistant depression. Consider adding an antipsychotic to other treatments for individuals with psychotic symptoms. * Quetiapine XL and Aripiprazole should only be used in cases where there is a clear additional benefit over other antipsychotics for an individual patient, and this should be documented both in the patient s record and an appropriate form completed on RiO. These drugs should only be prescribed by a consultant, and in the case acute teams in functionalised services, also require the approval of the community consultant. Lamotrigine There have been some positive trials, and meta-analysis indicates moderate benefit. It requires slow titration, and may take six weeks to achieve the likely effective dose (200mg / day). Antidepressants Most trials of antidepressants are in unipolar disease, and specifically exclude bipolar patients. Pooled data of the small trials in bipolar depression indicates antidepressants are superior to placebo. Antidepressant monotherapy is not recommended because of the possible risk of switch to mania or induction of rapid cycling. Tricyclic antidepressants and probably other dual action drugs like Venlafaxine (and possibly Duloxetine) carry a greater risk of precipitating a switch to mania than other antidepressants and are not recommended, except for patients who fail to respond to an initial treatment. Antidepressants appear less likely to induce mania when added to Lithium, Valproate or an antipsychotic. Tapered discontinuation of antidepressants may be considered after full remission of symptoms. In the absence of convincing evidence in favour of long term treatment with antidepressants, the usual policy should be discontinuation, although a small minority of patients appears to do well on combination treatment that includes an antidepressant. 12
13 Lithium Has been previously recommended in treating bipolar depression. Evidence for acute efficacy is poor. It failed to separate from placebo in the EMBOLDEN study. ECT Trials of ECT in depression have not tended to exclude bipolar patients, and evidence for its efficacy is good. Consider ECT for patients with high suicidal risk, psychosis, or severe depression during pregnancy. Treatment-resistant bipolar depression There is little evidence to inform the management of patients with treatment resistant bipolar depression. Therefore in such cases, consider treatments used in resistant unipolar depression (see guidelines for the pharmacological management of depression). 13
14 Initial treatment scheme depression (from BAP Guidelines 2009) Diagnosis Bipolar disorder Depressive episode Assessment Communication Suicide risk, patient and family preference and treatment setting Severity of risks, treatment options, eliminate stressors Severity of depression Severe Moderate Mild and or previous mood instability Consider ECT Quetiapine or Lamotrigine Consider SSRI or other antidepressant (not TCA) in combination with above Quetiapine or Lamotrigine On maintenance Rx? NO Bipolar-1? Add anti-manic agent if Bipolar 1 14
15 Pharmacological aspects of long term treatment (relapse prevention) Principles Consider long-term treatment following a single severe manic episode When a patient has accepted treatment for several years and remains very well, they should be strongly advised to continue indefinitely, because the risks of relapse remain high. If a long term medication is to be discontinued, it should be tapered over at least a two week period, and preferably longer. Clinical monitoring should be undertaken during the withdrawal period. Early relapse to mania is particularly a risk of abrupt lithium discontinuation. Choice of long term medicines An ideal mood stabilizer would prevent relapse to either pole of the illness, but the available medicines are probably more often effective against one pole than the other. Consider Lithium as initial monotherapy, which is probably effective against both manic and depressive relapse, although it is more effective in preventing mania. Long term treatment with lithium is associated with a reduced risk of suicide in bipolar patients. If Lithium is ineffective or poorly tolerated, consider: Where the burden of disease is depression: - Quetiapine* (prevents depressive and manic relapse) Lamotrigine (prevents more depressive relapse than manic) Where the burden of disease is mania: - Olanzapine (prevents more manic relapse than depressive, evidence of slight superiority over Llithium, and may be effective in preventing lithium withdrawal mania) Valproate (probably better at preventing manic than depressive relapses, although only 1 good RCT demonstrates effectiveness, and has no UK licence) Quetiapine* (prevents depressive and manic relapse) Aripiprazole* (prevents manic relapse) Carbamazepine is less effective than Lithium but may be employed especially in patients who do not show the classical pattern of episodic euphoric mania. Pharmacokinetic interactions may be problematic, and Oxcarbazine may be considered by extrapolation because of its lower potential for such interactions In an individual patient, if one of the above medicines led to prompt remission from the most recent depressive or manic episode, this may be considered evidence in favour of its long term use as monotherapy. There is little data for the older antipsychotics, including long acting injections, although some trials indicate a reduction in manic relapses. Topiramate and Gabapentin have failed to separate from placebo. * Quetiapine XL and Aripiprazole should only be used in cases where there is a clear additional benefit over other antipsychotics for an individual patient, and this should be documented both in the patient s record and an appropriate form completed on RiO. These drugs should only be prescribed 15
16 by a consultant, and in the case acute teams in functionalised services, also require the approval of the community consultant. Long term combination treatments Should be considered if the patient fails to respond to monotherapy and continues to experience sub-threshold symptoms or relapses. When the burden of disease is mania, it may be logical to combine predominantly anti-manic agents (e.g. Lithium, Valproate, an Antipsychotic) When the burden is depressive, Lamotrigine or Quetiapine may be more appropriate. In bipolar-i disorder, lamotrigine may usually require combination with an anti-manic long term agent. Lamotrigine and Quetiapine* may be effective as monotherapy in bipolar-ii disorder and both are licensed for this indication. The role of antidepressants in long term treatment is not established by controlled trials, but they appear to be used effectively, in combination with other preventative treatments, in a small minority of patients in the long term. Consider Clozapine in treatment refractory patients. It also has evidence in combination with Llithium or an anti convulsant. Pharmacological management of rapid cycling (4+ episodes per year) Identify and treat conditions such as Hypothyroidism or substance misuse that may contribute to cycling. Taper and discontinue antidepressants that may contribute to cycling. There is little data on which to base initial treatment beyond extrapolation or secondary analysis of acute and long term efficacy data for bipolar-i patients in general. For many patients, combinations of medicines are required. Evaluate anti-cycling effects over periods of six months or more by tracking mood states longitudinally. Discontinue ineffective treatments. Pharmacological management of early warning signs or high risk situations The preferred strategy is for continuous rather than intermittent treatment with oral medicines to prevent new mood episodes. However, the use of additional short term medication (e.g. Benzodiazepines or antipsychotics) is necessary when an acute stressor is imminent or present, early symptoms of relapse (especially insomnia) occur or anxiety becomes prominent. The Trust's mood on track programme encourages patients to identify early warning signs of relapse, and to plan actions to be taken in the event that they occur. This includes advice to ask their treating team to discuss short-term changes to medications. Consider supplying short-term medicines prospectively to patients to use with clear advice (e.g. suggest taking for four days, but if not settling or getting worse to seek medical attention). Higher doses of the long-term treatments may also be effective, thus avoiding the need for additional medications. 16
17 Long term treatment scheme maintenance therapy (from BAP Guidelines 2009) Diagnosis Acute episode resolved Euthymia Bipolar I disorder Communication Treatment Ensure education, information, and adherence Consider maintenance therapy If Mania predominates Protect against manic pole If Depression predominates Protect against depressive pole Consider Lithium or Aripiprazole or Quetiapine or Valproate or Olanzapine Consider Quetiapine or Lamotrigine 2 nd line Rx 2 nd line Rx Carbamazepine Lithium Rx Failure / Rapid Cycling Rx Failure / Rapid Cycling Combination therapy Optimise and continue 17
18 Key recent guidelines 1. NICE (2006). Bipolar Disorder. The management of bipolar disorder in adults, children and adolescents, in primary and secondary care. 2. Consensus group of the British Association for Psychopharmacology (2009). Evidence based guidelines for treating bipolar disorder: revised second edition recommendations from the British Association of Psychopharmacology. 3. World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for biological treatment of bipolar disorders, part I: Treatment of bipolar depression. The World Journal of Biological Psychiatry 3: World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for biological treatment of bipolar disorders, part II: Treatment of mania. The World Journal of Biological Psychiatry 4: World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for the biological treatment of bipolar disorders, part III: Maintenance treatment. The World Journal of Biological Psychiatry 5: The World Federation of Societies of Biological Psychiatry (WFSBP) Guidelines for the Biological Treatment of Bipolar Disorders: Update 2009 on the Treatment of Acute Mania. The World Journal of Biological Psychiatry 10: The World Federation of Societies of Biological Psychiatry (WFSBP) Guidelines for the Biological Treatment of Bipolar Disorders: Update 2010 on the Treatment of Acute Bipolar Depression. The World Journal of Biological Psychiatry 11:
19 Guidelines for the use of Paliperidone long acting injection Indications Paliperidone Long Acting Injection (PLAI) is indicated for maintenance treatment of schizophrenia in adult patients stabilised with Paliperidone or Risperidone. PLAI may be an effective treatment option in patients who have shown an initial treatment response to Paliperidone or Risperidone but for whom concordance with oral medication is a problem. Reflecting the 2009 NICE guidance, PLAI should be offered as a treatment option alongside other long acting antipsychotic injections (depots). Considering the costs of PLAI compared to other long acting injections, the pharmacological therapies committee have approved PLAI as an alternative to Risperidone long acting injection in new patients where at least one traditional long acting injections (depot) has led to unacceptable side effects, proved ineffective or is contra-indicated. PTC has not approved PLAI for the routine substitution of RLAI in patients who are stable on RLAI. This will only be considered on an individual case basis submitted in the first instance to the director of pharmacy and medicines management. The following table outlines actions that should be followed in different situations where paliperidone long acting injection may be considered. Status 1. Concordant with oral antipsychotics 2. Patient stabilised on an oral antipsychotic for at least two weeks but there are compliance issues 3. Patient stabilised on an older long acting antipsychotic injection but experiencing unacceptable side effects or it has not been sufficiently effective 4. Initial dose, when transferring from oral antipsychotic therapy Action Continue oral antipsychotics. Consider an older long acting injection as a first choice unless there are clear reasons to suggest these are unlikely to be effective, tolerated or are contra-indicated. Provided the patients has shown a previous responsiveness to either oral risperidone or paliperidone commence paliperidone on the day that the next depot injection is due (Day one) in deltoid muscle but do not administer the second initiation dose on Day eight. Administer subsequent doses on a monthly basis based on clinical assessment see point six for dose regimens. Recommended initiation is with a dose of 150mg on treatment day one and 100mg one week later (i.e. day 8) both administered in a deltoid muscle. The recommended monthly maintenance dose is 75mg in either deltoid or gluteal muscle; with individual patients doses tailored within the range of 25mg to 150mg based on tolerability and/or efficacy. Previous oral paliperidone or oral risperidone regardless of the previous dose can be discontinued at the time of first administration of paliperidone. 5. Elderly (>65 years). Not recommended Off Label 19
20 Status 6. Maintenance Treatment and Dose Changes 7. Switching from Risperidone Long Acting Injection Action Following the second dose monthly maintenance doses can be administered in either the deltoid or gluteal muscle. Dose changes can be made on a monthly basis, after the second dose, based on tolerability and efficacy with the maintenance dose range being between 25mg to 150mg Initiate paliperidone LAI in place of the next scheduled injection of risperidone LAI (deltoid or gluteal). For equivalent doses please see Table 1 below. Paliperidone LAI should then be administered at monthly intervals. The one week initiation regimen (Day one and Day eight respectively) is not required. Table 1 Previous Risperidone LAI dose 25mg every two weeks 37.5mg every two weeks 50mg every two weeks Paliperidone LAI 50mg monthly 75mg monthly 100mg monthly Storage conditions Paliperidone LAI Should be stored in a locked medicines cupboard. Refrigerated storage is not required. Training Nurses should familiarise themselves with the summary of product characteristics before administering including injection sites and needle size. Training is available for deltoid and gluteal administration. Please contact Frances Byrne to organise training. Administration The initial two doses (Day one and Day eight) when transferring from oral antipsychotic therapy are to be administered into the deltoid muscle; the following monthly doses can be administered in either the deltoid or gluteal muscle. When switching from risperidone LAI Paliperidone LAI can be administered into either the deltoid or gluteal muscles. When switching from a typical depot the first injection of Paliperidone LAI is into the deltoid muscle but subsequent injections can be into the deltoid or gluteal muscle. A switch from deltoid to gluteal and visa versa should be considered in the event of injection site pain, and it is also recommended to alternate between left and right sides. 20
21 Paliperidone LAI is intended for intramuscular use only. It should be injected slowly deep into the muscle. Deltoid muscle administration The recommended needle size for initial and maintenance administration is determined by the patients weight: > 90 kg - 1½ inch needle, 22 gauge < 90 kg 1 inch, 23 gauge Deltoid injection should be alternated between the two deltoid muscles Gluteal muscle administration The recommended needle size for maintenance administration is the 1½ inch, 22 gauge needle. Administration can be made into the upper-outer quadrant of the gluteal area. Gluteal injection should be alternated between the two gluteal muscles. Monitoring The pharmacological therapies committee requires referral paperwork to be completed and sent to pharmacy before an initial supply of PLAI can be made. If a patient discontinues treatment with PLAI and then restarts, new referral paperwork must be completed. An audit questionnaire on the use of PLAI must also be completed for each patient six months after initiation of PLAI. With this in mind you should use a recognized tool to assess the patient s mental state before initiating treatment which can be repeated after six months, e.g. BPRS or PANNS. Side effect monitoring using an accepted tool, e.g. LUNSERS or GASS should also be carried out on initiation of PLAI and repeated after six months of PLAI to assess tolerability of treatment. Responsibilities of the clinical team prescribing PLAI. It is the responsibility of the medical team to complete the referral paperwork and the audit questionnaire for each of their patients on PLAI. If necessary, if the initiating team is an inpatient of home treatment team then discussion should have taken place with the expected long term prescriber and agreement reached on the use of paliperidone long acting injection for that patient. 21
22 An objective assessment (such as BPRS or PANNS) should be undertaken before treatment is commenced and at six months after initiation. The initial assessment should be shared with the long term prescriber and the long term prescriber will normally be expected to repeat and review after six months. To objectively assess side effects experienced by the patient e.g. using the LUNSERS or GASS rating scale before treatment with PLAI is commenced and then six months after initiation. The initial assessment should be shared with the long term prescriber and the long term prescriber will normally be expected to repeat and review after six months. Responsibilities of pharmacy. All new requests for PLAI will be screened by a senior pharmacist. Where there are gaps in the information, for example, no signature of the long term prescriber or no prior use of traditional long acting injections, supply will be withheld and prescribers contacted. Only when all information is complete will initiating supply of PLAI be made. Pharmacy will contact each patient s long term prescriber after six months to audit the use of PLAI in each new patient. 22
23 Guidance for the initiation of Clozapine for inpatients and patients within home treatment services Pre-initiation The attached Clozapine pre-initiation schedule will prompt and support the necessary tasks prior to initiation of Clozapine including registration of the patient with ZTAS, baseline checks, the initial clozapine prescription and other logistical issues. The undertaking of these tasks will need to be agreed between the patient s long term clinical team and the team taking responsibility for initiation of clozapine. Further detail is included on the schedule itself. Inpatient initiation In addition to the pre-initiation schedule, all inpatient units will be provided a folder that includes A Clozapine initiation prescription chart for as Monday start A Clozapine initiation prescription chart for as Monday start A custom Clozapine initiation prescription chart for initiation on other days of the week A chart for recording physical observations necessary for safe clozapine initiation. Clozapine initiation prescription charts can be attached through double sided tape to Trust prescription charts. Most patients should start their Clozapine on a Monday with clozapine having been supplied on the previous Friday. Staff undertaking daily observations for service users initiating Clozapine must discuss the results with the responsible clinician the same day as they are taken or with the on-call doctor at weekends. Any concerns in daily observations must be raised with the responsible clinician immediately. Home treatment initiation Similar to inpatient units, home treatment teams will be provided with a folder that contains the following: A Clozapine initiation prescription chart for as Monday start A Clozapine initiation prescription chart for as Monday start A custom clozapine initiation prescription chart for initiation on other days of the week A chart for recording physical observations necessary for safe Clozapine initiation. Clozapine initiation prescription charts can be attached through double sided tape to Trust prescription charts. Most patients should start their Clozapine on a Monday with Clozapine having been supplied on the previous Friday. Staff undertaking daily observations for service users initiating Clozapine must discuss the results with the responsible clinician the same day as they are taken or with the on-call doctor at weekends. Any concerns in daily observations must be raised with the responsible clinician immediately. Transfer to community teams Inpatient or home treatment teams should continue to prescribe clozapine for such service users and continue observations until the service user s Clozapine dose and observations are stable. The service user may then be transferred back to the community consultant unless there are other reasons to keep the service user in acute services. 23
24 References 1. D Taylor et al. The Maudsley 2009 Prescribing Guidelines. 10 th Edition. Informa Healthcare. London 2. Zaponex Summary of Product Characteristics, January Available at 3. Out Patient Initiation of Zaponex. Available at 4. Ronaldson KJ et al. A new monitoring protocol for clozapine-induced myocarditis based on 75 cases and 94 controls. Aust & NZ J Psych 2011 DOI: /
25 Clinical guidance No: Item: Report Date: September 2010 Agreed by: The prescribing of high dose and combination antipsychotic medication Pharmacological therapies committee Clinical governance committee Aim of guidance The aim of this guideline is to highlight the consensus statement from the Royal College of Psychiatrists on high dose antipsychotics to clinical staff and to offer recommendations for using high dose antipsychotic therapy including the monitoring that should be in place. The guidance protects the right to treatment of patients who do require high doses for affective treatment. For this, each patient should be assessed carefully by a consultant psychiatrist and the reasons for this treatment documented in the patients care record. Developed by Nigel Barnes, Director of Pharmacy and Medicines Management Erica Young, Programme lead pharmacists, AWA acute inpatients Sheena Mitchell, Reaside Pharmacy Manager Dr. Imran Waheed, Consultant Psychiatrist Caroline Faulconbridge Senior Clinical Pharmacist Who it applies to This is prescribing guidance Process for review / feedback Prescribing high dose and combination antipsychotic medication is the subject of audit and will be reported to the pharmacological therapies committee for adherence to this guidance. This guidance will be updated annually in the light of any changes to national or local prescribing practice, NICE guidance or other evidence based comments from local clinicians. The next review date will be January
26 Introduction The Royal College of Psychiatrists published a consensus statement on high dose antipsychotic medication in October 1993 and updated this in May Since then, the Prescribing Observatory for Mental Health in the UK (POMH-UK) show that high dose antipsychotics are prescribed on average in around 40% of patients through the UK. This prescribing includes all regular and when required prescriptions per patient. Excluding the when required prescriptions still leaves between 10% and 20% of patients are still prescribed high dose antipsychotics regularly across the UK. In recent years this has fallen slightly so that in February 2010, the national average for the number of patients receiving high dose antipsychotics was 37%. For Birmingham and Solihulll Mental Health NHS Foundation Trust, this currently stands at 38%. Excluding when required prescriptions, this falls to 10%. Of the high dose prescribing, the majority is due to combination of antipsychotics which is often unnecessary. The National Patients Safety Agency report on patient safety incidents in mental health states that high dose prescribing should be reviewed within Trusts because of the increased potential for adverse effects including the unclear contribution towards ventricular tachycardia and sudden death. Unless otherwise stated, doses in the BNF are licensed doses. Any higher dose is therefore off license. The prescribing of licensed medicines outside the recommendations of the marketing authorisation alters (and probably increases) the doctors professional responsibility. The aim of this guideline is to highlight this guidance to clinical staff and to offer recommendations for using high dose antipsychotic therapy including the monitoring that should be in place. The guidance protects the right to treatment of patients who do require high doses for affective treatment. For this, each patient should be assessed carefully by a consultant psychiatrist. Definition of high dose antipsychotic therapy (HDAT) The 2006 Royal College of Psychiatrists Consensus Working Group recommends the following definition for high dose: A total daily dose of a single antipsychotic which exceeds the upper limit stated in the British National Formulary (BNF; published by the British Medical Association & Royal Pharmaceutical Society of Great Britain) or a total daily dose of two or more antipsychotics which exceeds the BNF maximum using the percentage method. For example:- Zuclopenthixol depot 300mg weekly (50%) and Olanzapine 15mg daily (75%). Total daily dose = 50% + 75% = 125% Anything above 100% is considered high dose antipsychotic therapy. Responsibilities Consultant psychiatrist responsibilities: Use of high dose antipsychotic therapy is solely the responsibility of the consultant. Responsibility for prescribing and monitoring of HDAT will always remain with the consultant psychiatrist and not be transferred to primary care. Ensure guidance is followed for HDAT 26
27 Document reasons for high dose antipsychotic therapy in integrated care record and EPEX/RiO Check high dose antipsychotic therapy (HDAT) is covered by consent to treatment, T2, T3 or CT011 Ensure all necessary physical health checks are carried out at appropriate frequencies including ordering of ECGs, checking of U & Es, LFTs Inform patients and document consent in integrated care record If an acute care consultant wishes to prescribe HDAT which is likely to extend beyond the period of IP/HTT care, then they should seek the agreement of the CMHT consultant. At transfer the prescribing consultant is responsible for ensuring that the receiving consultant is aware of the HDAT status, rationale for use of HDAT and the proposed length of treatment. Pharmacists responsibilities: Identify that a patient is on high dose antipsychotics Ensure clinical staff are aware of high dose status Endorse prescription chart with % of maximum antipsychotic dose being prescribed if approaching or above 100% Check for any interacting medicines and advise prescribers accordingly Nursing staff responsibilities for inpatients: Check observations including temperature and blood pressure Document high dose status in the integrated care record Ensure that high dose status is discussed at review Non-medical prescribers Use of high dose antipsychotic therapy is solely the responsibility of the consultant and the decision to proceed to high doses should not be made by non medical prescribers. Non-medical prescribers may participate in decisions to prescribe HDAT and may prescribe within the context of supplementary prescribing and where it is clearly stated within clinical management plans Guidelines for the use of high dose antipsychotic medication 1. Current evidence does not justify the routine use of high dose antipsychotic medication in general adult mental health services, either with a single agent or a combined antipsychotics. 2. If high doses are to be used in an individual case, this should only be after evidence based strategies have failed and as a carefully monitored therapeutic trial. 3. The decision to prescribe high dose (of either an individual agent or through combination) should be taken explicitly and should involve an individual risk benefit assessment by a consultant psychiatrist. This should be undertaken in consultation with the wider clinical team and the patient and a patient advocate, if available and if the patient wishes their presence. 4. The decision to prescribe high dose should be documented in the integrated care record and EPEX/RiO, including the risks and benefits of the strategy, the aims and when and how the outcome will be assessed. 5. Dose escalation should be made in relatively small increments with adequate time allowed for response. This includes prescribing beyond the high dose threshold. 6. Careful observation should be kept on the dosage in terms of the total % arising from drug combinations including the use of when required (as required) medication. Local systems, including pharmacist monitoring, should be developed to alert the responsible clinicians and clinical teams to patients currently being administered or at risk of receiving high doses. 27
28 7. The use of when required medication should be kept under regular review. Where possibly alternative ways of dealing with acute patient agitation should be followed. Staff administering when required medication should be aware of it s potential to raise the total daily dose of an antipsychotic above the high dose threshold. 8. When prescribing high dose antipsychotic medication consider the following risk factors: Cardiac history (particularly MI, Arrythmias or abnormal ECG) Hepatic / renal impairment Alcoholism / smoking Age Obesity 9. Consider possible drug interactions when prescribing high dose antipsychotic medication. Potential drug interactions, which should be avoided where possible include: Diuretics Anti-arrythmics Anti-hypertensives Tricyclic antidepressants Any drugs which might prolong the QT interval, or increase blood antipsychotic levels. 10. Before prescribing high dose antipsychotic medication, carry out an ECG to establish a baseline and exclude cardiac contraindications, including long QT syndromes. An ECG should be repeated after a few days and then every 1 to 3 months in the early stages of high dose treatment. The ECG should be repeated as clinically indicated. If the QT interval is recorded as greater than 440ms treatment should be reviewed. Consider cardiology assessment. If it is decided to continue treatment then record reasons for doing so in the patient s integrated care record. If treatment is continued then repeat an ECG more frequently than before. 11. Serum urea, electrolytes and liver function should be checked before prescribing, after one month and then three monthly to ensure liver or renal problems are not developing. Pulse, supine and standing blood pressure, temperature and clinical signs of dehydration should be checked for one week after dose changes, at one month and then three monthly. 12. Patients should be carefully monitored to ensure improvement in psychotic symptoms can be measured using scales such as the BPRS (Brief Psychiatric Rating Scale) or PANSS (Positive and Negative Symptom Score). Side effects should also be monitored carefully using either LUNSERS (Liverpool University Neuroleptic Side Effect Rating Scale) or GASS (Glasgow Antipsychotic Side Effect Scale). These should be performed at baseline, 6 and 12 weeks and then three monthly thereafter. 13. Each programme should establish an audit of antipsychotic doses using e.g. the POMH-UK audit methodology. Pharmacy can be contacted for more information on audit methodology. Alternative strategies to high dose antipsychotics Emergencies In emergency follow the trust rapid tranquilisation policy. Acute treatment In acute treatment, it is recommended that the dose of medication should be increased gradually, e.g. weekly, so as not to exceed the dose needed to treat psychotic symptoms. Any antipsychotic effects may take one to two weeks to become evident. Increasing the dose slowly is also thought to reduce the risk of neuroleptic malignant syndrome. If the patient is responding slowly and there is some urgency in the clinical situation, other methods of inducing a remission should also be considered. 28
29 When required medication The use of when required medication should be reviewed regularly. Staff should be aware of the potential for when required medication to raise the total daily dose of antipsychotic above the high dose threshold. There is further guidance in the medicines code on the prescribing and administration of when required medication. Treatment failure and consideration of Clozapine For patients who have failed to respond to two antipsychotics at full dose, consider the following: Review the diagnosis, consider organic causes and illicit drug use Measure therapeutic drug levels to ensure that they are within the recommended range for therapeutic effect Carefully review compliance with medication Consider whether sufficient time has been allowed for response to take place. Allow six to eight weeks at the maximum tolerable dose for each antipsychotic tried. Consider reducing the antipsychotic dose slowly for a trial period. Some studies suggest a curvilinear dose response relationship, possibly because of inducing iatrogenic negative symptoms at very high dose. Rarely the anticholinergic effects of the antipsychotics may induce a toxic psychosis which will improve with dose reduction. Consider adverse social and psychological factors which may be perpetuating the psychosis, including family factors environmental and other potential disturbances. Consider specific psychological interventions aimed at target symptoms such as hallucinations or at improving the level of social function and rehabilitation. Consider other treatments such as mood stabilisers or antidepressants if there are severe mood symptoms, agitation or overexcitement. For service users with treatment resistant schizophrenia (defined as a lack of significant clinical improvement despite the sequential use of the recommended doses for six to eight weeks of at least two antipsychotics, one of which is a second generation antipsychotic) then NICE guidance recommend treatment with clozapine. For those with treatment resistant schizophrenia who show a poor or only a partial response to clozapine, or where dose increases are limited due to side effects, the addition of another antipsychotic, e.g. Amisulpiride or Sulpiride, to Clozapine is a common clinical strategy, although the evidence is limited. Combination of antipsychotics Before combination antipsychotics are used, specific actions should be taken to ensure: The diagnosis is correct Treatment dose and duration have been adequate Plasma levels (if appropriate) are therapeutic Concordance with treatments ensured Alternative adjunctive therapies have been considered Appropriate indications for use of more than one antipsychotic: These may include: Rapid tranquilisation Failed or partial response to clozapine Neutropenia or agranulocytosis with Clozapine Switching from one antipsychotic to another (Six weeks maximum crossover if needed) 29
 Where clinical improvement occurred before a")
30 As a temporary measure as an adjunct to depot medication during an acute exacerbation of illness Inappropriate indications would include: Failure to wait an adequate length of time for the first treatment to have a full antipsychotic effect (Six months for clozapine, Six weeks for all other oral antipsychotics and eight weeks for depot medication) Where clinical improvement occurred before a switch of antipsychotics is completed Where patient is possibly treatment resistant and Clozapine has not been tried Where benefit (as assessed by rating scales) does not outweigh the risk Antipsychotics - maximum recommended doses 30

31 Audit of high dose antipsychotic therapy The trust subscribes to the POMH-UK audit programme. There is a regular audit of high dose antipsychotic medication and combinations. This will be continued and extended out to other programmes not currently participating so that there is regular and sustained monitoring of high dose antipsychotic therapy across the trust. Below are the listed audit criteria for the POMH-UK ausit on high dose and combination antipsychotics audit. 1: The total dose of antipsychotic drug prescribed should be within SPC/BNF limits. A high dose of antipsychotic is defined here as a total daily dose (whether of a single antipsychotic or more than one prescribed in combination) greater than 100% of the maximum recommended daily dose. 2: Individuals should receive only one antipsychotic at a time. This standard applies to 100% of individuals with schizophrenia. Exceptions: Individuals with schizophrenia who are receiving C lozapine but who have not responded sufficiently; and individuals who are changing from one antipsychotic to another (NICE schizophrenia guideline, 2009). 31
32 References 1. Royal College of Psychiatrists (2006) Consensus statement on High Dose Antipsychotic Medication (Council Report CR138) London: Royal College of Psychiatrists ( 2. Prescribing Observatory for Mental Health UK. The Royal College of Psychiatrists 2010 POMH-UK Topic1E Supplimentary Report. The prescribing of High Dose and Combination Antipsychotics on Adults Acute and Intensive Care Wards. 3. National Patients Safety Agency. With Safety In Mind: Mental Health Services and Patient Safety. July National Institute for Clinical Excellence (2009). Schizophrenia: Core Interventions in the Treatment and Management of Schizophrenia in Adults in Primary and Secondary Care. Clinical Guideline 82 ( 32
33 Anti-depressants Anti-depressants available: Fluoxetine Sertraline Citalopram Paroxetine Venlafaxine Mirtazepine Amitriptyline Trazodone Moclobemide Amitryptiline Lofepramine Trimipramine Nortriptyline Other treatments for anxiety disorders Pregabalin Buspirone Anti-depressants with additional requirements for prescribing - require consultant documentation of reasons for prescribing, (including why first tier drugs are not appropriate as well as the agreement of the long term prescriber. GPs may decline to accept prescribing of these antidepressants Escitalopram Duloxetine Agomelatine Bupropion (unlicensed) Associated guidance Pharmacological management of depression Pharmacological management of generalised anxiety disorder Lithium shared care agreement 33
34 Pharmacological management of depression 1) General principles Where medication is prescribed, ensure that patients have adequate information about the options for treatment, the purpose of the treatment, and possible side effects. Provide written information (eg. UKPPG leaflet, available from Trust Intranet). Where appropriate, ensure that physical health monitoring is undertaken. 2) Treatment of sub threshold depressive symptoms and mild depression Only use antidepressants if: - there is a past history of moderate or severe depression Sub threshold depressive symptoms have been present more than two years Sub threshold symptoms or mild depression persists after other interventions 3) Choice of first line antidepressant Consider tolerability and efficacy of antidepressants previously taken. Should usually be an SSRI in generic form, eg Citalopram, Fluoxetine or Sertraline (as equally effective as other antidepressants in first-line treatment, favourable risk-benefit ratio and are cost-effective). (Please see section 11) 4) Choice of antidepressant in depression with a chronic physical health problem Use SSRIs with caution in patients taking aspirin and do not normally offer SSRIs to patients taking other non steroidal inflammatory drugs, because of the risk of gastrointestinal bleeding. Consider offering an antidepressant with a lower propensity for, or a different range of interactions, such as Mirtazapine or Trazodone. If no suitable alternative antidepressant can be identified, SSRIs may be prescribed at the same time as aspirin or non steroidals if gastro protective medicines (for example, proton-pump inhibitors most cost effective are Omeprazole or Lansoprazole), are also offered. Do not offer SSRIs to patients receiving triptan drugs for migraine. Offer a safer alternative such as mirtazapine or trazodone Do not normally offer SSRIs at the same time as Monoamine Oxidase B (MAO-B) inhibitors such as Selegiline and Rasagiline. Offer a safer alternative such as Mirtazapine or Trazodone, Do not normally offer Fluvoxamine to patients taking Theophylline, Clozapine, Methadone or Tizamidine. Offer a safer alternative such as Sertraline or Citalopram. Offer Sertraline as the preferred antidepressant for patients taking Flecainide or Propafenone, although Mirtazapine and Moclobemide may also be used. Do not offer Fluoxetine or Paroxetine to patients taking Atomoxetine. Offer a different SSRI. 34
35 5) Monitoring in initial phase of treatment If under 30 or at increased risk of suicide should be seen after one week and frequently thereafter until the risk is no longer significant. Otherwise, should be seen after two weeks, then regularly (e.g. two four weekly) for the first three months, then at longer intervals if response is good. If side effects, consider reassurance (if mild), reduction in dose or switch to another antidepressant, or addition of short-term (up to two weeks) benzodiazepine if problematic anxiety, agitation or insomnia. 6) Assessment and initial management of inadequate response to first line treatment If no response after 3-4 weeks: - check compliance and then consider the following: increasing support (eg to weekly contact) increasing dose within BNF limits, if no significant side effects. There is indirect evidence for a dose-response in TCAs and venlafaxine, but, there is poor evidence for the effectiveness of dose-escalation in SSRIs) switching antidepressant or combination medication or augmentation If at 6-8 weeks there is inadequate response,: - review diagnosis and check compliance increase the frequency of appointments use a validated outcome measure consider increasing dose within BNF limits (if no significant side effects) consider switching antidepressant or combination medication or augmentation (Please see section 11) 7) Switching anti-depressants Consider especially if there are troublesome side effects and / or no improvement with first-line treatment. Can generally be achieved quickly, but consider the potential for interactions Little evidence for advantage of between-class over within-class switching Choice of second line antidepressant Generally a second generic SSRI or Mirtazapine Choice of third line antidepressant Mirtazapine Venlafaxine Tricyclic antidepressant (avoid dosulepin due to cardiac risk and toxicity in overdose) 35
36 8) Combining and augmenting medications Consider especially if there has been a partial response to the first line treatment, there is good tolerability of the existing treatment, or if switching has already proved unsuccessful. There are several combination and augmentation strategies with evidence. Before using, the prescriber should ensure that they are familiar with the evidence for the tolerability and efficacy, and document the rationale for using this strategy in the ICR. The service user should be made aware of the increased side effect burden combination and augmentation strategies usually involve. If off-label medication is used, GMC guidance should be followed, and this recorded in the ICR. Strategies specifically mentioned in the NICE guidelines include: - Antidepressant plus Lithium Antidepressant plus an antipsychotic such as Aripiprazole, Olanzapine, Quetiapine or Risperidone. Typical doses for augmentation of depression are: Aripiprazole mg; Olanzapine 5-10mg; Quetiapine mg; Risperidone 0.5-3mg. If antipsychotics are used, appropriate monitoring of BMI, glucose and lipids must be undertaken. In the UK, of the antipsychotics, only quetiapine XL has a licence for augmentation of antidepressants in non-psychotic depression. SSRI or Venlafaxine plus Mirtazapine. Other combinations with evidence from STAR-D trial: - Antidepressant (such as SSRI) plus Bupriopion (Bupriopion does not have a licence for depression in UK). Antidepressant plus Buspirone Antidepressant plus thyroid hormones It may be that GPs are not confident in prescribing combinations of medications in depression, or prescribing outside of UK licence. In these cases, prescribing should continue in secondary care until this has been addressed. 9) Severe depression with psychotic symptoms Should be managed by a combination of antidepressant and antipsychotic medication. there is insufficient evidence to indicate an advantage of one antipsychotic over another, or to indicate ideal dosing strategies. 10) Antidepressants for continuation and relapse prevention Advise patients who have responded to antidepressants to continue (at the dose that was effective in acute treatment) for at least six months Advise patients to continue (at the dose that was effective in acute treatment) for at least two years (and consider even longer term treatment) if : - Two or more previous episodes with significant functional impairment in the recent past presence of residual symptoms multiple previous episodes history of severe or prolonged episodes history of inadequate response to treatment the consequences of relapsing are likely to be severe 36
37 Patients who have had multiple episodes of depression, and who have had a good response to treatment with an antidepressant and an augmenting agent should remain on this combination if they find the side effects tolerable and acceptable. If one medication is to be stopped, it should generally be the augmenting agent. Lithium should not be used as a sole agent to prevent recurrence. If a patient is discharged back to primary care while still taking medication, written advice should be given to the GP regarding: - Whether this is to be lifelong treatment If not, when and how the medication should be discontinued Details of any required monitoring (during treatment and during discontinuation 11 Stopping or reducing antidepressants Advise patients that discontinuation symptoms may occur in the short-term Gradually reduce the dose, generally over a four-week period (not required for Fluoxetine) 12 Antidepressants not for routine use in BSMHFT Due to the lack of evidence for additional benefit, and the much higher cost, the following antidepressants should NOT be routinely used in BSMHFT: - Escitalopram Duloxetine Agomelatine If consultant psychiatrists wish to use these medications for individual patients, trials of other antidepressants should have been made or considered, taking into account effectiveness, tolerability and contra-indications. The procedure for the request of restricted medicines should be followed. This involves the completion of a standard form to detail treatment received to date, explain why other treatments are not appropriate, tolerated or effective, and outline the rationale for the chosen treatment strategy. There will be a requirement that the patient's response to any one of these drugs is monitored using standard outcome measures. This procedure must be followed whether the drug is to be prescribed through a Trust pharmacy or on FP10. Local PCTs have indicated that they will not support the transfer of prescribing of these branded antidepressants from the Trust to primary care, and so prescribing of these drugs will usually remain the responsibility of the Trust. For this reason, should an acute care consultant wish to prescribe one of these branded antidepressants, they must obtain the agreement of the longterm prescriber (community consultant), and this should be indicated by the counter-signature of the long-term prescriber on the initial request form. 37
38 38
39 39
40 40
MERSEY CARE NHS TRUST HOW WE MANAGE MEDICINES. MM11 - High-Dose Antipsychotic Use Guidelines (local guideline) KEY ISSUES
 KEY ISSUES") MERSEY CARE NHS TRUST HOW WE MANAGE MEDICINES MM11 - High-Dose Antipsychotic Use Guidelines (local guideline) Medicines Management Services aim to ensure that (i) Service users receive their medicines
MERSEY CARE NHS TRUST HOW WE MANAGE MEDICINES MM11 - High-Dose Antipsychotic Use Guidelines (local guideline) Medicines Management Services aim to ensure that (i) Service users receive their medicines
High Dose Antipsychotic Therapy (HDAT) guideline
 guideline") Document level: Trustwide (TW) Code: MP18 Issue number: 2 High Dose Antipsychotic Therapy (HDAT) guideline Lead executive Medical Director Author and contact number Lead Clinical Pharmacist 01625 663 857
Document level: Trustwide (TW) Code: MP18 Issue number: 2 High Dose Antipsychotic Therapy (HDAT) guideline Lead executive Medical Director Author and contact number Lead Clinical Pharmacist 01625 663 857
Clinical. High Dose Antipsychotic Prescribing Procedures. Document Control Summary. Contents
 Clinical High Dose Antipsychotic Prescribing Procedures Document Control Summary Status: Version: Author/Owner/Title: Approved by: Ratified: Related Trust Strategy and/or Strategic Aims Implementation
Clinical High Dose Antipsychotic Prescribing Procedures Document Control Summary Status: Version: Author/Owner/Title: Approved by: Ratified: Related Trust Strategy and/or Strategic Aims Implementation
Formulary and Prescribing Guidelines
 Formulary and Prescribing Guidelines SECTION 3: TREATMENT OF BIPOLAR AFFECTIVE DISORDER This section provides information regarding the pharmacological management of Bipolar affective disorder in secondary
Formulary and Prescribing Guidelines SECTION 3: TREATMENT OF BIPOLAR AFFECTIVE DISORDER This section provides information regarding the pharmacological management of Bipolar affective disorder in secondary
SiGMA/ MMHSCT GUIDELINES FOR ANTIPSYCHOTIC DRUG TREATMENT OF SCHIZOPHRENIA. [compatible with NICE guidance]
![SiGMA/ MMHSCT GUIDELINES FOR ANTIPSYCHOTIC DRUG TREATMENT OF SCHIZOPHRENIA. [compatible with NICE guidance]](/thumbs/80/80440271.jpg "SiGMA/ MMHSCT GUIDELINES FOR ANTIPSYCHOTIC DRUG TREATMENT OF SCHIZOPHRENIA. [compatible with NICE guidance]") SiGMA/ MMHSCT GUIDELINES FOR ANTIPSYCHOTIC DRUG TREATMENT OF SCHIZOPHRENIA [compatible with NICE guidance] Medicines Management Committee August 2002 For review August 2003 Rationale The SiGMA algorithm
SiGMA/ MMHSCT GUIDELINES FOR ANTIPSYCHOTIC DRUG TREATMENT OF SCHIZOPHRENIA [compatible with NICE guidance] Medicines Management Committee August 2002 For review August 2003 Rationale The SiGMA algorithm
Prescription of High Dose Antipsychotic Medication
 Subject (M1) Title Medicine Prescription of High Dose Antipsychotic Medication Manual Mental Health Procedure No M1-P-2-MH Department Pharmacy Distribution All Author Rae McKnight Review 4 Reviewer Jonathan
Subject (M1) Title Medicine Prescription of High Dose Antipsychotic Medication Manual Mental Health Procedure No M1-P-2-MH Department Pharmacy Distribution All Author Rae McKnight Review 4 Reviewer Jonathan
Mental Health Medicines Management Pilot. Community Pharmacy. High Dose Antipsychotic Screening, Education & Advice Service
 Mental Health Medicines Management Pilot Community Pharmacy High Dose Antipsychotic Screening, Education & Advice Service Approved Version 1 Date of First Issue Review Date Date of Issue Author / Contact
Mental Health Medicines Management Pilot Community Pharmacy High Dose Antipsychotic Screening, Education & Advice Service Approved Version 1 Date of First Issue Review Date Date of Issue Author / Contact
High Dose Antipsychotic Therapy (HDAT) guideline
 guideline") Document level: Trustwide (TW) Code: MP18 Issue number: 4 High Dose Antipsychotic Therapy (HDAT) guideline Lead executive Medical Director Authors details Michael Slater (Clinical Pharmacist, tel. 01625
Document level: Trustwide (TW) Code: MP18 Issue number: 4 High Dose Antipsychotic Therapy (HDAT) guideline Lead executive Medical Director Authors details Michael Slater (Clinical Pharmacist, tel. 01625
Aripiprazole Long-Acting Injection (Abilify Maintena ) Guidelines for Prescribing and Administration (Version 3 August 2014)
 Guidelines for Prescribing and Administration (Version 3 August 2014)") 1. Key Points. Aripiprazole Long-Acting Injection (Abilify Maintena ) Guidelines for Prescribing and Administration (Version 3 August 2014) 1.1 Aripiprazole long acting injection (LAI) is licensed / indicated
1. Key Points. Aripiprazole Long-Acting Injection (Abilify Maintena ) Guidelines for Prescribing and Administration (Version 3 August 2014) 1.1 Aripiprazole long acting injection (LAI) is licensed / indicated
HIGH DOSE ANTIPSYCHOTIC GUIDELINES (HDAT)
") HIGH DOSE ANTIPSYCHOTIC GUIDELINES (HDAT) Document Reference Version Number 2.00 High Dose Antipsychotic Guidelines (HDAT) G376 Author/Lead Job Title Jackie Stark Principal Pharmacist Clinical Services
HIGH DOSE ANTIPSYCHOTIC GUIDELINES (HDAT) Document Reference Version Number 2.00 High Dose Antipsychotic Guidelines (HDAT) G376 Author/Lead Job Title Jackie Stark Principal Pharmacist Clinical Services
NHS Grampian Guidance For Staff Working In The Mental Health Service For The Use Of High-Dose Antipsychotic Medication
 NHS Grampian Westholme Woodend Hospital Queens Road ABERDEEN AB15 6LS Date 20 th November 2014 Our Ref HDAT_MGPG/Nov14 Enquiries to Caroline Hind Extension 56088 Direct Line 01224 556088 Email caroline.hind2@nhs.net
NHS Grampian Westholme Woodend Hospital Queens Road ABERDEEN AB15 6LS Date 20 th November 2014 Our Ref HDAT_MGPG/Nov14 Enquiries to Caroline Hind Extension 56088 Direct Line 01224 556088 Email caroline.hind2@nhs.net
Paliperidone Palmitate 3-monthly Long-Acting Injection (Trevicta ) Guidelines for Prescribing and Administration (Version 1 October 2016)
 Guidelines for Prescribing and Administration (Version 1 October 2016)") Paliperidone Palmitate 3-monthly Long-Acting Injection (Trevicta ) Guidelines for Prescribing and Administration (Version 1 October 2016) 1. Key Points 1.1 Paliperidone palmitate 3-monthly long-acting
Paliperidone Palmitate 3-monthly Long-Acting Injection (Trevicta ) Guidelines for Prescribing and Administration (Version 1 October 2016) 1. Key Points 1.1 Paliperidone palmitate 3-monthly long-acting
Document Title Antipsychotics Prescribing Guidelines for Schizophrenia
 Document Title Antipsychotics Prescribing Guidelines for Schizophrenia Document Description Document Type Prescribing Guidance Service Application Medicines Management Version 1.0 Policy Reference no.
Document Title Antipsychotics Prescribing Guidelines for Schizophrenia Document Description Document Type Prescribing Guidance Service Application Medicines Management Version 1.0 Policy Reference no.
MMG012 GUIDELINES FOR THE USE OF HIGH DOSE ANTIPSYCHOTIC MEDICATION
 MMG012 GUIDELINES FOR THE USE OF HIGH DOSE ANTIPSYCHOTIC MEDICATION Page 1 of 16 Table of Contents Why we need this Policy... 3 What the Policy is trying to do... 3 Which stakeholders have been involved
MMG012 GUIDELINES FOR THE USE OF HIGH DOSE ANTIPSYCHOTIC MEDICATION Page 1 of 16 Table of Contents Why we need this Policy... 3 What the Policy is trying to do... 3 Which stakeholders have been involved
GUIDELINES FOR THE USE OF ARIPIPRAZOLE LONG-ACTING INJECTION (ABILIFY MAINTENA)
") GUIDELINES FOR THE USE OF ARIPIPRAZOLE LONG-ACTING INJECTION (ABILIFY MAINTENA) Introduction Aripiprazole long-acting injection (LAI)is licensed for the maintenance treatment of adult patients with schizophrenia
GUIDELINES FOR THE USE OF ARIPIPRAZOLE LONG-ACTING INJECTION (ABILIFY MAINTENA) Introduction Aripiprazole long-acting injection (LAI)is licensed for the maintenance treatment of adult patients with schizophrenia
POLICY DOCUMENT. Pharmacy MMG/MPG. Approved By and Date Medicines Management roup March March 2016
 POLICY DOCUMENT Document Title High dose and combination antipsychotic guidance Reference Number n/a Policy Type Prescribing and Treatment Guideline Electronic File/Location Clinical Resources/Pharmacy/Prescribing
POLICY DOCUMENT Document Title High dose and combination antipsychotic guidance Reference Number n/a Policy Type Prescribing and Treatment Guideline Electronic File/Location Clinical Resources/Pharmacy/Prescribing
SHARED CARE GUIDELINE
 SHARED CARE GUIDELINE Title: Prescribing and/ or Monitoring of Antipsychotics Scope: Pennine Care NHS Foundation Trust NHS Bury NHS Oldham NHS Heywood, Middleton and Rochdale NHS Stockport NHS Tameside
SHARED CARE GUIDELINE Title: Prescribing and/ or Monitoring of Antipsychotics Scope: Pennine Care NHS Foundation Trust NHS Bury NHS Oldham NHS Heywood, Middleton and Rochdale NHS Stockport NHS Tameside
High Dose Antipsychotic Medication Policy
 High Dose Antipsychotic Medication Policy Policy Title State previous title where relevant State if Policy New or Revised Policy Strand Org, HR, Clinical, H&S, Infection Control, Finance For clinical policies
High Dose Antipsychotic Medication Policy Policy Title State previous title where relevant State if Policy New or Revised Policy Strand Org, HR, Clinical, H&S, Infection Control, Finance For clinical policies
Treatment of Schizophrenia Appendix Three Page 1 of 8
 Prescribing Guidelines Treatment of Schizophrenia Scope of this guidance This guidance aims to describe the pharmacological management of schizophrenia at a simple and intermediate level, with a brief
Prescribing Guidelines Treatment of Schizophrenia Scope of this guidance This guidance aims to describe the pharmacological management of schizophrenia at a simple and intermediate level, with a brief
ESSENTIAL SHARED CARE AGREEMENT FOR Risperidone, Olanzapine, Quetiapine, Aripiprazole, Amisulpride (South Staffordshire Only)
") E099 ESSENTIAL SHARED CARE AGREEMENT FOR Risperidone, Olanzapine, Quetiapine, Aripiprazole, Amisulpride (South Staffordshire Only) NOTE: Please complete details on P1 &3 Send one copy to GP, Patient and
E099 ESSENTIAL SHARED CARE AGREEMENT FOR Risperidone, Olanzapine, Quetiapine, Aripiprazole, Amisulpride (South Staffordshire Only) NOTE: Please complete details on P1 &3 Send one copy to GP, Patient and
ESSENTIAL SHARED CARE AGREEMENT FOR Risperidone, Olanzapine, Quetiapine, Aripiprazole, Amisulpride or Asenapine
 Ref No: E053 ESSENTIAL SHARED CARE AGREEMENT FOR Risperidone, Olanzapine, Quetiapine, Aripiprazole, Amisulpride or Asenapine NOTE: Please complete details on P1 &3 Send one copy to GP, Patient and file
Ref No: E053 ESSENTIAL SHARED CARE AGREEMENT FOR Risperidone, Olanzapine, Quetiapine, Aripiprazole, Amisulpride or Asenapine NOTE: Please complete details on P1 &3 Send one copy to GP, Patient and file
Pregnancy. General Principles of Prescribing in Pregnancy (The Maudsley, 12 th Edition)
") Pregnancy General Principles of Prescribing in Pregnancy (The Maudsley, 12 th Edition) In all women of child bearing potential Always discuss the possibility of pregnancy; half of all pregnancies are unplanned
Pregnancy General Principles of Prescribing in Pregnancy (The Maudsley, 12 th Edition) In all women of child bearing potential Always discuss the possibility of pregnancy; half of all pregnancies are unplanned
Olanzapine Long-Acting Injection (Zypadhera ) - Guidelines for Prescribing and Administration (Version 3 May 2015)
 - Guidelines for Prescribing and Administration (Version 3 May 2015)") 1. Key Points Olanzapine Long-Acting Injection (Zypadhera ) - Guidelines for Prescribing and Administration (Version 3 May 2015) 1.1 Olanzapine long acting injection (LAI) is indicated for the maintenance
1. Key Points Olanzapine Long-Acting Injection (Zypadhera ) - Guidelines for Prescribing and Administration (Version 3 May 2015) 1.1 Olanzapine long acting injection (LAI) is indicated for the maintenance
PALIPERIDONE LONG ACTING INJECTION PRESCRIBING GUIDELINE. Chief Pharmacist. Chief Pharmacist
 REFERENCE NUMBER: PALIPERIDONE LONG ACTING INJECTION PRESCRIBING GUIDELINE AREA: NAME OF RESPONSIBLE COMMITTEE / INDIVIDUAL NAME OF ORIGINATOR / AUTHOR Trust-wide Chief Pharmacist Chief Pharmacist DATE
REFERENCE NUMBER: PALIPERIDONE LONG ACTING INJECTION PRESCRIBING GUIDELINE AREA: NAME OF RESPONSIBLE COMMITTEE / INDIVIDUAL NAME OF ORIGINATOR / AUTHOR Trust-wide Chief Pharmacist Chief Pharmacist DATE
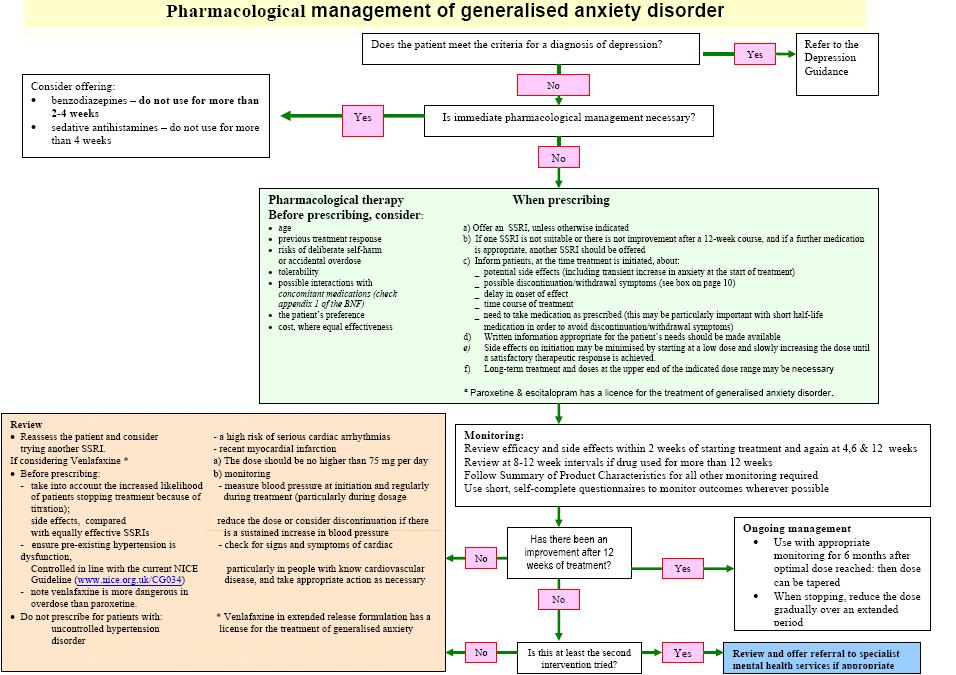
Document Title Pharmacological Management of Generalised Anxiety Disorder
 Document Title Pharmacological Management of Generalised Anxiety Disorder Document Description Document Type Policy Service Application Trust Wide Version 1.1 Policy Reference no. POL 201 Lead Author(s)
Document Title Pharmacological Management of Generalised Anxiety Disorder Document Description Document Type Policy Service Application Trust Wide Version 1.1 Policy Reference no. POL 201 Lead Author(s)
PRESCRIBING GUIDELINES
 The Maudsley The South London and Maudsley NHS Foundation Trust & Oxleas NHS Foundation Trust PRESCRIBING GUIDELINES 10th Edition David Taylor Carol Paton Shitij Kapur informa healthcare Contents Authors
The Maudsley The South London and Maudsley NHS Foundation Trust & Oxleas NHS Foundation Trust PRESCRIBING GUIDELINES 10th Edition David Taylor Carol Paton Shitij Kapur informa healthcare Contents Authors
Drug Name: Lithium Clinical Indications: Treatment and prophylaxis of mania; bipolar disorder; augmentation therapy in treatment resistant depression
 SHARED CARE PROTOCOL AND INFORMATION FOR GPS Drug Name: Lithium Clinical Indications: Treatment and prophylaxis of mania; bipolar disorder; augmentation therapy in treatment resistant depression Version:
SHARED CARE PROTOCOL AND INFORMATION FOR GPS Drug Name: Lithium Clinical Indications: Treatment and prophylaxis of mania; bipolar disorder; augmentation therapy in treatment resistant depression Version:
Resubmission. Scottish Medicines Consortium
 Scottish Medicines Consortium Resubmission aripiprazole 5mg, 10mg, 15mg, 0mg tablets; 10mg, 15mg orodispersible tablets; 1mg/mL oral solution (Abilify ) No. (498/08) Bristol-Myers Squibb Pharmaceuticals
Scottish Medicines Consortium Resubmission aripiprazole 5mg, 10mg, 15mg, 0mg tablets; 10mg, 15mg orodispersible tablets; 1mg/mL oral solution (Abilify ) No. (498/08) Bristol-Myers Squibb Pharmaceuticals
SHARED CARE GUIDELINE
 SHARED CARE GUIDELINE Title: Shared Care Guideline for the prescribing and monitoring of Antipsychotics for the treatment of Schizophrenia and psychotic symptoms in children and adolescents Scope: Pennine
SHARED CARE GUIDELINE Title: Shared Care Guideline for the prescribing and monitoring of Antipsychotics for the treatment of Schizophrenia and psychotic symptoms in children and adolescents Scope: Pennine
Formulary and Clinical Guideline Document Pharmacy Department Medicines Management Services
 Formulary and Clinical Guideline Document Pharmacy Department Medicines Management Services VIOLENCE, AGGRESSION OR SEVERE BEHAVIOURAL DISTURBANCE Introduction During an acute episode or illness, some
Formulary and Clinical Guideline Document Pharmacy Department Medicines Management Services VIOLENCE, AGGRESSION OR SEVERE BEHAVIOURAL DISTURBANCE Introduction During an acute episode or illness, some
Datix Ref:
 Title Document Details Shared Care Agreement: Antipsychotics (Risperidone, Olanzapine, Quetiapine, Aripiprazole, Amisulpride or Asenapine) Trust Ref No 2081-38933 Local Ref (optional) Main points the document
Title Document Details Shared Care Agreement: Antipsychotics (Risperidone, Olanzapine, Quetiapine, Aripiprazole, Amisulpride or Asenapine) Trust Ref No 2081-38933 Local Ref (optional) Main points the document
ESSENTIAL SHARED CAR E AGREEMENT FOR
 E093 ESSENTIAL SHARED CARE AGREEMENT FOR Risperidone, Olanzapine, Quetiapine, Aripiprazole, or Amisulpride for Behavioural indications in People with Learning Disability (LD) Referral Criteria In some
E093 ESSENTIAL SHARED CARE AGREEMENT FOR Risperidone, Olanzapine, Quetiapine, Aripiprazole, or Amisulpride for Behavioural indications in People with Learning Disability (LD) Referral Criteria In some
Methylphenidate Shared Care Agreement For attention deficit hyperactivity disorder (ADHD) in adults Effective Shared Care Agreement
 in adults Effective Shared Care Agreement") Methylphenidate Shared Care Agreement For attention deficit hyperactivity disorder (ADHD) in adults Effective Shared Care Agreement Section 1: Shared Care arrangements and responsibilities Section 1.1
Methylphenidate Shared Care Agreement For attention deficit hyperactivity disorder (ADHD) in adults Effective Shared Care Agreement Section 1: Shared Care arrangements and responsibilities Section 1.1
PORT, 2009 Spain, 2009 Malaysia, 2009 Singapore, 2009 BAP, 2011 WFSBP, 2012 SIGN, 2013 Harvard NICE RANZCP, 2016
 Appendix 3. Comparison of recommendations from clinical practice guidelines. Data extracted in relation to key health questions that are relevant to a clinician adopting an algorithmic approach to the
Appendix 3. Comparison of recommendations from clinical practice guidelines. Data extracted in relation to key health questions that are relevant to a clinician adopting an algorithmic approach to the
Hearts and Minds An ECG Update. Tuesday 18 th November The Met Hotel, Leeds
 Hearts and Minds An ECG Update Tuesday 18 th November The Met Hotel, Leeds Ashleigh Bradley Specialist Clinical Pharmacist for Mental Health and Lithium Clinic Airedale NHS Foundation Trust Introduction
Hearts and Minds An ECG Update Tuesday 18 th November The Met Hotel, Leeds Ashleigh Bradley Specialist Clinical Pharmacist for Mental Health and Lithium Clinic Airedale NHS Foundation Trust Introduction
asenapine 5mg, 10mg sublingual tablet (Sycrest ) SMC No. (762/12) Lundbeck Ltd
 SMC No. (762/12) Lundbeck Ltd") asenapine 5mg, 10mg sublingual tablet (Sycrest ) SMC No. (762/12) Lundbeck Ltd 10 February 2012 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and advises NHS
asenapine 5mg, 10mg sublingual tablet (Sycrest ) SMC No. (762/12) Lundbeck Ltd 10 February 2012 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and advises NHS
ESSENTIAL SHARED CARE AGREEMENT FOR Risperidone, Olanzapine, Quetiapine, Aripiprazole, or Amisulpride for Behavioural indications in DNLD
 Ref No: E050 ESSENTIAL SHARED CARE AGREEMENT FOR Risperidone, Olanzapine, Quetiapine, Aripiprazole, or Amisulpride for Behavioural indications in DNLD Please complete the following details: Patient s name,
Ref No: E050 ESSENTIAL SHARED CARE AGREEMENT FOR Risperidone, Olanzapine, Quetiapine, Aripiprazole, or Amisulpride for Behavioural indications in DNLD Please complete the following details: Patient s name,
Preferred Prescribing Choices of Antipsychotic Drugs (APD) in Adults for Schizophrenia and Other Psychoses
 in Adults for Schizophrenia and Other Psychoses") Preferred Prescribing Choices of Antipsychotic Drugs (APD) in Adults for Schizophrenia and Other Psychoses HPFT Medicines Formulary lists the APDs that have been approved for use, however, it does not
Preferred Prescribing Choices of Antipsychotic Drugs (APD) in Adults for Schizophrenia and Other Psychoses HPFT Medicines Formulary lists the APDs that have been approved for use, however, it does not
Bournemouth, Dorset and Poole Prescribing Forum
 SHARED CARE GUIDELINE FOR THE USE OF ATOMOXETINE IN ADULTS WITH ATTENTION DEFICIT HYPERACTIVITY DISORDER INDICATION Atomoxetine is a non-stimulant non-amphetamine inhibitor of noradrenaline reuptake. It
SHARED CARE GUIDELINE FOR THE USE OF ATOMOXETINE IN ADULTS WITH ATTENTION DEFICIT HYPERACTIVITY DISORDER INDICATION Atomoxetine is a non-stimulant non-amphetamine inhibitor of noradrenaline reuptake. It
Formulary Item Restrictions and/or Advice Site availability
 Formulary Item Restrictions and/or Advice Site availability C&W CNWL Typical Antipsychotic drugs Chlorpromazine 25mg Chlorpromazine 50mg Chlorpromazine 100mg Chlorpromazine 25mg/5ml syrup Chlorpromazine
Formulary Item Restrictions and/or Advice Site availability C&W CNWL Typical Antipsychotic drugs Chlorpromazine 25mg Chlorpromazine 50mg Chlorpromazine 100mg Chlorpromazine 25mg/5ml syrup Chlorpromazine
What s new in the treatment of bipolar disorder?
 What s new in the treatment of bipolar disorder? Dr. David Cousins MRC Clinician Scientist Institute of Neuroscience Newcastle University NCMD 2017 What s new in the treatment of bipolar disorder? Dr.
What s new in the treatment of bipolar disorder? Dr. David Cousins MRC Clinician Scientist Institute of Neuroscience Newcastle University NCMD 2017 What s new in the treatment of bipolar disorder? Dr.
The treatment of bipolar disorder in adults, children and adolescents
 DRAFT FOR CONSULTATION The treatment of bipolar disorder in adults, children and adolescents The paragraphs in the draft are numbered for the purposes of consultation. The final version will not contain
DRAFT FOR CONSULTATION The treatment of bipolar disorder in adults, children and adolescents The paragraphs in the draft are numbered for the purposes of consultation. The final version will not contain
This shared care protocol covers when atypical antipsychotics are prescribed for the treatment of
 SHARED CARE PROTOCOL for ATYPICAL ANTIPSYCHOTICS SCOPE Greater Manchester West Mental health NHS Foundation Trust Bolton Primary Care Trust Salford Primary Care Trust Trafford Primary Care Trusts Issue
SHARED CARE PROTOCOL for ATYPICAL ANTIPSYCHOTICS SCOPE Greater Manchester West Mental health NHS Foundation Trust Bolton Primary Care Trust Salford Primary Care Trust Trafford Primary Care Trusts Issue
Dosing & Administration
 Dosing & Administration REAL LIFE. REAL RESULTS. INDICATION INVEGA SUSTENNA (paliperidone palmitate) is indicated for the treatment of: Schizophrenia. Schizoaffective disorder as monotherapy and as an
Dosing & Administration REAL LIFE. REAL RESULTS. INDICATION INVEGA SUSTENNA (paliperidone palmitate) is indicated for the treatment of: Schizophrenia. Schizoaffective disorder as monotherapy and as an
Clinical Guideline for the Management of Bipolar Disorder in Adults
 Clinical Guideline for the Management of Bipolar Disorder in Adults Goal: To improve the quality of life of adults with bipolar disorder Identification and Treatment of Bipolar Disorder Criteria for Diagnosis:
Clinical Guideline for the Management of Bipolar Disorder in Adults Goal: To improve the quality of life of adults with bipolar disorder Identification and Treatment of Bipolar Disorder Criteria for Diagnosis:
Prescribing of high-dose and combined antipsychotics for patients on forensic wards.
 POMH-UK Topic 3 baseline May 2007 Prescribing of high-dose and combined antipsychotics for patients on forensic wards. Prepared by the Prescribing Observatory for Mental Health (POMH-UK) for member Healthcare
POMH-UK Topic 3 baseline May 2007 Prescribing of high-dose and combined antipsychotics for patients on forensic wards. Prepared by the Prescribing Observatory for Mental Health (POMH-UK) for member Healthcare
Professor Tony Holland, Department of Psychiatry, University of Cambridge
 INFORMATION SHEET The Use of Medication for Challenging Behaviour Professor Tony Holland, Department of Psychiatry, University of Cambridge Introduction Challenging behaviours displayed by people with
INFORMATION SHEET The Use of Medication for Challenging Behaviour Professor Tony Holland, Department of Psychiatry, University of Cambridge Introduction Challenging behaviours displayed by people with
Initiation of Clozapine Treatment Community Patients
 Initiation of Clozapine Treatment Community Patients Who Should Read This Policy Target Audience All clinical staff working in the community N/A N/A Initiation of Clozapine Treatment for Patients in the
Initiation of Clozapine Treatment Community Patients Who Should Read This Policy Target Audience All clinical staff working in the community N/A N/A Initiation of Clozapine Treatment for Patients in the
Prescribing medications for people with a personality disorder A service evaluation of a community mental health team
 Prescribing medications for people with a personality disorder A service evaluation of a community mental health team Dr Umama Khan, Consultant Psychiatrist Dr Venkatesh Ballagere, Specialist Registrar
Prescribing medications for people with a personality disorder A service evaluation of a community mental health team Dr Umama Khan, Consultant Psychiatrist Dr Venkatesh Ballagere, Specialist Registrar
SHARED CARE GUIDELINE
 SHARED CARE GUIDELINE Title: Lithium Treatment in Adults aged 18-65 years Scope: Pennine Care NHS Foundation Trust NHS Bury NHS Oldham NHS Heywood, Middleton and Rochdale NHS Stockport NHS Tameside & Glossop
SHARED CARE GUIDELINE Title: Lithium Treatment in Adults aged 18-65 years Scope: Pennine Care NHS Foundation Trust NHS Bury NHS Oldham NHS Heywood, Middleton and Rochdale NHS Stockport NHS Tameside & Glossop
New Medicines Committee Briefing November 2011
 New Medicines Committee Briefing November 2011 Paliperidone long-acting injection (Xeplion ) for schizophrenia Paliperidone palmitate long-acting injection (Xeplion ) is to be reviewed for use within:
New Medicines Committee Briefing November 2011 Paliperidone long-acting injection (Xeplion ) for schizophrenia Paliperidone palmitate long-acting injection (Xeplion ) is to be reviewed for use within:
PALIPERIDONE (Trevicta ) 3 MONTHLY Long acting injection (LAI) Guidance for Prescribing and Administration
 3 MONTHLY Long acting injection (LAI) Guidance for Prescribing and Administration") PALIPERIDONE (Trevicta ) 3 MONTHLY Long acting injection (LAI) Guidance for Prescribing and Administration Paliperidone 1 monthly long acting injection (Xeplion ) This is included in the Trust medicines
PALIPERIDONE (Trevicta ) 3 MONTHLY Long acting injection (LAI) Guidance for Prescribing and Administration Paliperidone 1 monthly long acting injection (Xeplion ) This is included in the Trust medicines
The Deprescribing of Psychotropic Medication in Service Users (Patients) with Learning Disability
 with Learning Disability") The Deprescribing of Psychotropic Medication in Service Users (Patients) with Learning Disability Danielle Adams Principal Clinical Pharmacist Pharmacy and Medicines Optimisation Team HPFT July 2017 1
The Deprescribing of Psychotropic Medication in Service Users (Patients) with Learning Disability Danielle Adams Principal Clinical Pharmacist Pharmacy and Medicines Optimisation Team HPFT July 2017 1
Bipolar Disorder Clinical Practice Guideline Summary for Primary Care
 Bipolar Disorder Clinical Practice Guideline Summary for Primary Care DIAGNOSIS AND CLINICAL ASSESSMENT Bipolar Disorder is categorized by extreme mood cycling; manifested by periods of euphoria, grandiosity,
Bipolar Disorder Clinical Practice Guideline Summary for Primary Care DIAGNOSIS AND CLINICAL ASSESSMENT Bipolar Disorder is categorized by extreme mood cycling; manifested by periods of euphoria, grandiosity,
-Guidelines for the discontinuation of oral antipsychotics in patients with BPSD within the primary care setting Summary- Quetiapine
 -Guidelines for the discontinuation of oral antipsychotics in patients with BPSD within the primary care setting Summary- Quetiapine An independent report Time for action 1 by Professor Sube Banerjee looked
-Guidelines for the discontinuation of oral antipsychotics in patients with BPSD within the primary care setting Summary- Quetiapine An independent report Time for action 1 by Professor Sube Banerjee looked
Guidance on the Use of Antipsychotic Long-acting Injections in North of England
 Guidance on the Use of Antipsychotic Long-acting Injections in North of England This guidance aims to inform and support prescribers within the three mental health service providers in the north of England
Guidance on the Use of Antipsychotic Long-acting Injections in North of England This guidance aims to inform and support prescribers within the three mental health service providers in the north of England
Prescribing antipsychotics for children and adolescents
 POMH-UK Topic 10a baseline report Prescribing antipsychotics for children and adolescents September 2010 Prepared by the Prescribing Observatory for Mental Health-UK for Coventry and Warwickshire Partnership
POMH-UK Topic 10a baseline report Prescribing antipsychotics for children and adolescents September 2010 Prepared by the Prescribing Observatory for Mental Health-UK for Coventry and Warwickshire Partnership
Atomoxetine Effective Shared Care Agreement For Attention Deficit Hyperactivity Disorder (ADHD)
") Atomoxetine Effective Shared Care Agreement For Attention Deficit Hyperactivity Disorder (ADHD) Section 1: Shared Care arrangements and responsibilities Section 1.1 Agreement to transfer of prescribing
Atomoxetine Effective Shared Care Agreement For Attention Deficit Hyperactivity Disorder (ADHD) Section 1: Shared Care arrangements and responsibilities Section 1.1 Agreement to transfer of prescribing
Psychopharmacology. Psychopharmacology. Hamish McAllister-Williams Reader in Clinical. Department of Psychiatry, RVI
 Regional Affective Disorders Service Psychopharmacology Northumberland, Tyne and Wear NHS Trust Hamish McAllister-Williams Reader in Clinical Psychopharmacology Department of Psychiatry, RVI Intro NOT
Regional Affective Disorders Service Psychopharmacology Northumberland, Tyne and Wear NHS Trust Hamish McAllister-Williams Reader in Clinical Psychopharmacology Department of Psychiatry, RVI Intro NOT
Treatment Options for Bipolar Disorder Contents
 Keeping Your Balance Treatment Options for Bipolar Disorder Contents Medication Treatment for Bipolar Disorder 2 Page Medication Record 5 Psychosocial Treatments for Bipolar Disorder 6 Module Summary 8
Keeping Your Balance Treatment Options for Bipolar Disorder Contents Medication Treatment for Bipolar Disorder 2 Page Medication Record 5 Psychosocial Treatments for Bipolar Disorder 6 Module Summary 8
Volume 4; Number 5 May 2010
 Volume 4; Number 5 May 2010 CLINICAL GUIDELINES FOR ANTIDEPRESSANT USE IN PRIMARY AND SECONDARY CARE Lincolnshire Partnership Foundation Trust in conjunction with Lincolnshire PACEF have recently updated
Volume 4; Number 5 May 2010 CLINICAL GUIDELINES FOR ANTIDEPRESSANT USE IN PRIMARY AND SECONDARY CARE Lincolnshire Partnership Foundation Trust in conjunction with Lincolnshire PACEF have recently updated
Monitoring of patients prescribed lithium
 POMH-UK Topic 7 Monitoring of patients prescribed lithium Please use the following to cite this report: Prescribing Observatory for Mental Health (2009). Topic 7 baseline report. Monitoring of patients
POMH-UK Topic 7 Monitoring of patients prescribed lithium Please use the following to cite this report: Prescribing Observatory for Mental Health (2009). Topic 7 baseline report. Monitoring of patients
Guidance on the Use of Antipsychotic Long-acting Injections in North of England (TEWV version)
") Guidance on the Use of Antipsychotic Long-acting Injections in North of England (TEWV version) This guidance aims to inform and support prescribers within the three mental health service providers in the
Guidance on the Use of Antipsychotic Long-acting Injections in North of England (TEWV version) This guidance aims to inform and support prescribers within the three mental health service providers in the
Joint Formulary for Psychotropic Medication.
 Joint for Psychotropic Medication. This document has been produced in collaboration with the Lancashire Commissioning Support Unit Page 1 Table of Contents Section Page Number Page 2 Definition of categories
Joint for Psychotropic Medication. This document has been produced in collaboration with the Lancashire Commissioning Support Unit Page 1 Table of Contents Section Page Number Page 2 Definition of categories
Prescribing of high-dose and combination antipsychotics on adult acute and intensive care wards: Clinical introduction, methodology and glossary.
 POMH-UK Topic 1 report 1b Prescribing of high-dose and combination antipsychotics on adult : Clinical introduction, methodology and glossary. March 2007 Prepared by the Prescribing Observatory for Mental
POMH-UK Topic 1 report 1b Prescribing of high-dose and combination antipsychotics on adult : Clinical introduction, methodology and glossary. March 2007 Prepared by the Prescribing Observatory for Mental
Integrated Care Pathway (ICP) for the. Management of clozapine INPATIENT INITIATION
 for the. Management of clozapine INPATIENT INITIATION") Document Reference MM 048 Integrated Care Pathway (ICP) for the Management of clozapine INPATIENT INITIATION Surname Title Address Forenames Date of Birth RT/NHS number Care Co-ordinator GP CS number Consultant
Document Reference MM 048 Integrated Care Pathway (ICP) for the Management of clozapine INPATIENT INITIATION Surname Title Address Forenames Date of Birth RT/NHS number Care Co-ordinator GP CS number Consultant
South London and the Maudsley NHS Foundation Trust Medicines Formulary
 South London and the Maudsley NHS Foundation Trust Medicines Formulary Medicine Formulations Restrictions Additional Information / Related NICE Technology Appraisal 4.1 Hypnotics and anxiolytics 4.1.1
South London and the Maudsley NHS Foundation Trust Medicines Formulary Medicine Formulations Restrictions Additional Information / Related NICE Technology Appraisal 4.1 Hypnotics and anxiolytics 4.1.1
Medicines Guideline: High-dose antipsychotic prescribing (MG01)
") Medicines Guideline: High-dose antipsychotic prescribing (MG01) Document author Assured by Review cycle Ben Browning, Locality Lead Pharmacist (Secure Services) MOG sub-group (04.05.16) Review every two
Medicines Guideline: High-dose antipsychotic prescribing (MG01) Document author Assured by Review cycle Ben Browning, Locality Lead Pharmacist (Secure Services) MOG sub-group (04.05.16) Review every two
Depression in adults: treatment and management
 1 2 3 4 Depression in adults: treatment and management 5 6 7 8 Appendix V3: recommendations that have been deleted of changed from 2009 guideline Depression in adults: Appendix V3 1 of 22 1 Recommendations
1 2 3 4 Depression in adults: treatment and management 5 6 7 8 Appendix V3: recommendations that have been deleted of changed from 2009 guideline Depression in adults: Appendix V3 1 of 22 1 Recommendations
SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR ALCOHOL DEPENDENCE INDICATION
 SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR ALCOHOL DEPENDENCE INDICATION Naltrexone is used as part of a comprehensive programme of treatment against alcoholism to reduce the
SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR ALCOHOL DEPENDENCE INDICATION Naltrexone is used as part of a comprehensive programme of treatment against alcoholism to reduce the
Class Update: Oral Antipsychotics
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
This document has been produced in collaboration with the Lancashire Commissioning Support Unit
 Joint for Psychotropic Medication. This document has been produced in collaboration with the Lancashire Commissioning Support Unit Date: December 2014. Reviewed August 2016. Next review Date April 2019
Joint for Psychotropic Medication. This document has been produced in collaboration with the Lancashire Commissioning Support Unit Date: December 2014. Reviewed August 2016. Next review Date April 2019
Safe transfer of prescribing guidance
 Safe transfer of prescribing guidance TEWV Prescriber Summary Application required before prescribing Products requiring an application, before prescribing, using the single application form Unlicensed
Safe transfer of prescribing guidance TEWV Prescriber Summary Application required before prescribing Products requiring an application, before prescribing, using the single application form Unlicensed
Guidance on Consent to Treatment Documentation for Medication Patient s Detained under the Mental Health Act
 Guidance on Consent to Treatment Documentation for Medication Patient s Detained under the Mental Health Act This guidance is intended for Coventry and Warwickshire Partnership Trust staff to use when
Guidance on Consent to Treatment Documentation for Medication Patient s Detained under the Mental Health Act This guidance is intended for Coventry and Warwickshire Partnership Trust staff to use when
SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR OPIOID DEPENDENCE
 SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR OPIOID DEPENDENCE INDICATION Naltrexone is a pure opiate antagonist licensed as an adjunctive prophylactic therapy in the maintenance
SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR OPIOID DEPENDENCE INDICATION Naltrexone is a pure opiate antagonist licensed as an adjunctive prophylactic therapy in the maintenance
Abbreviated Class Review: Long-Acting Injectable Antipsychotics
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Abbreviated Class Review: Long-Acting Injectable Antipsychotics
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
SHARED CARE PROTOCOL FOR THE PRESCRIBING AND MONITORING OF MEDICINES FOR ATTENTION-DEFICIT HYPERACTIVITY DISORDER (ADHD)
") SHARED CARE PROTOCOL FOR THE PRESCRIBING AND MONITORING OF MEDICINES FOR ATTENTION-DEFICIT HYPERACTIVITY DISORDER (ADHD) 1. Introduction This protocol describes how patients prescribed medicines for ADHD
SHARED CARE PROTOCOL FOR THE PRESCRIBING AND MONITORING OF MEDICINES FOR ATTENTION-DEFICIT HYPERACTIVITY DISORDER (ADHD) 1. Introduction This protocol describes how patients prescribed medicines for ADHD
Psychotropic Medication. Including Role of Gradual Dose Reductions
 Psychotropic Medication Including Role of Gradual Dose Reductions What are they? The phrase psychotropic drugs is a technical term for psychiatric medicines that alter chemical levels in the brain which
Psychotropic Medication Including Role of Gradual Dose Reductions What are they? The phrase psychotropic drugs is a technical term for psychiatric medicines that alter chemical levels in the brain which
SECTION 9 : MANAGEMENT OF MOVEMENT DISORDERS AND EXTRAPYRAMIDAL SIDE EFFECTS
 SECTION 9 : MANAGEMENT OF MOVEMENT DISORDERS AND EXTRAPYRAMIDAL SIDE EFFECTS Formulary and Prescribing Guidelines 9.1 Introduction Movement disorders and extrapyramidal side effects can manifest in the
SECTION 9 : MANAGEMENT OF MOVEMENT DISORDERS AND EXTRAPYRAMIDAL SIDE EFFECTS Formulary and Prescribing Guidelines 9.1 Introduction Movement disorders and extrapyramidal side effects can manifest in the
Procedure Reviewed By: Narinder Sangha Deputy Chief Pharmacist STANDARD OPERATING PROCEDURE
 Written By: Objective By: ed By: To ensure safe and consistent working practice throughout Black Country Partnership Foundation Trust (BCPFT) and to avoid unnecessary harm to patients on lithium therapy
Written By: Objective By: ed By: To ensure safe and consistent working practice throughout Black Country Partnership Foundation Trust (BCPFT) and to avoid unnecessary harm to patients on lithium therapy
Authorised by Greater Medicines Management Group
 SHARED CARE PROTOCOL for ATYPICAL ANTIPSYCHOTICS SCOPE Greater Manchester West Mental health NHS Foundation trust Bolton Primary Care Trust Salford Primary Care Trust Trafford Primary Care Trusts Issue
SHARED CARE PROTOCOL for ATYPICAL ANTIPSYCHOTICS SCOPE Greater Manchester West Mental health NHS Foundation trust Bolton Primary Care Trust Salford Primary Care Trust Trafford Primary Care Trusts Issue
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 Ongoing care for adults with psychosis or schizophrenia bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly
Ongoing care for adults with psychosis or schizophrenia bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly
Dear Colleagues, NATIONAL STANDARD FOR MONITORING THE PHYSICAL HEALTH OF PEOPLE BEING TREATED WITH LITHIUM
 Directorate of Chief Medical Officer T: 0131-244 6930 E: john.mitchell4@gov.scot Dear Colleagues, NATIONAL STANDARD FOR MONITORING THE PHYSICAL HEALTH OF PEOPLE BEING TREATED WITH LITHIUM Lithium is a
Directorate of Chief Medical Officer T: 0131-244 6930 E: john.mitchell4@gov.scot Dear Colleagues, NATIONAL STANDARD FOR MONITORING THE PHYSICAL HEALTH OF PEOPLE BEING TREATED WITH LITHIUM Lithium is a
Managing Behavioural Problems in Patients with Learning Disabilities
 Managing Behavioural Problems in Patients with Learning Disabilities Some people with a learning disability display behaviour that challenges. Although such behaviour is a challenge to services, family
Managing Behavioural Problems in Patients with Learning Disabilities Some people with a learning disability display behaviour that challenges. Although such behaviour is a challenge to services, family
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 Recognising and managing bipolar disorder in adults in primary care bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are
Recognising and managing bipolar disorder in adults in primary care bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are
Perinatal Mental Health: Prescribing Guidance for Trust Prescribers and GPs
 Perinatal Mental Health: Prescribing Guidance for Trust Prescribers and GPs (Version 3 January 2015) Principal Author: Dr Jenny Cooke Consultant Psychiatrist, Brighton & Hove Perinatal Mental Health Service
Perinatal Mental Health: Prescribing Guidance for Trust Prescribers and GPs (Version 3 January 2015) Principal Author: Dr Jenny Cooke Consultant Psychiatrist, Brighton & Hove Perinatal Mental Health Service
Essential Shared Care Agreement: Lithium
 Ref No. E042 Essential Shared Care Agreement: Lithium Please complete the following details: Patient s name, address, date of birth Treatment (indication, dose regimen, brand name) Monitoring (proposed
Ref No. E042 Essential Shared Care Agreement: Lithium Please complete the following details: Patient s name, address, date of birth Treatment (indication, dose regimen, brand name) Monitoring (proposed
Shared Care Guideline for Olanzapine (Zyprexa )
") Shared Care Guideline for Olanzapine (Zyprexa ) Development Process This guidance has been produced by Sarah Hudson Lead Pharmacist SWYPFT following an AMBER classification status of Olanzapine by the
Shared Care Guideline for Olanzapine (Zyprexa ) Development Process This guidance has been produced by Sarah Hudson Lead Pharmacist SWYPFT following an AMBER classification status of Olanzapine by the
S H A R E D P R E S C R I B I N G G U I D E L I N E
 S H A R E D P R E S C R I B I N G G U I D E L I N E Introduction This shared prescribing guideline for the second generation antipsychotic medications listed above has been developed with due consideration
S H A R E D P R E S C R I B I N G G U I D E L I N E Introduction This shared prescribing guideline for the second generation antipsychotic medications listed above has been developed with due consideration
Neuropathic Pain Treatment Guidelines
 Neuropathic Pain Treatment Guidelines Background Pain is an unpleasant sensory and emotional experience that can have a significant impact on a person s quality of life, general health, psychological health,
Neuropathic Pain Treatment Guidelines Background Pain is an unpleasant sensory and emotional experience that can have a significant impact on a person s quality of life, general health, psychological health,
GREATER MANCHESTER INTERFACE PRESCRIBING GROUP
 GREATER MANCHESTER INTERFACE PRESCRIBING GROUP On behalf of the GREATER MANCHESTER MEDICINES MANAGEMENT GROUP SHARED CARE GUIDELINE FOR THE PRESCRIBING OF SELECTIVE SEROTONIN REUPTAKE INHIBITORS (SSRIs)
GREATER MANCHESTER INTERFACE PRESCRIBING GROUP On behalf of the GREATER MANCHESTER MEDICINES MANAGEMENT GROUP SHARED CARE GUIDELINE FOR THE PRESCRIBING OF SELECTIVE SEROTONIN REUPTAKE INHIBITORS (SSRIs)
SHARED CARE GUIDELINE
 SHARED CARE GUIDELINE Shared Care Guideline for the prescribing and monitoring of antipsychotics for the treatment of Neurodevelopmental Disorders in children and adolescents. Scope: Version 1 Pennine
SHARED CARE GUIDELINE Shared Care Guideline for the prescribing and monitoring of antipsychotics for the treatment of Neurodevelopmental Disorders in children and adolescents. Scope: Version 1 Pennine
The Pharmacological Management of Bipolar Disorder: An Update
 Psychobiology Research Group The Pharmacological Management of Bipolar Disorder: An Update R. Hamish McAllister-Williams, MD, PhD, FRCPsych Reader in Clinical Psychopharmacology Newcastle University Hon.
Psychobiology Research Group The Pharmacological Management of Bipolar Disorder: An Update R. Hamish McAllister-Williams, MD, PhD, FRCPsych Reader in Clinical Psychopharmacology Newcastle University Hon.
Scottish Medicines Consortium
 Scottish Medicines Consortium olanzapine 210mg, 300mg, 405mg powder and solvent for prolonged release suspension for injection (ZypAdhera ) No. (624/10) Eli Lilly and Company Limited 09 July 2010 The Scottish
Scottish Medicines Consortium olanzapine 210mg, 300mg, 405mg powder and solvent for prolonged release suspension for injection (ZypAdhera ) No. (624/10) Eli Lilly and Company Limited 09 July 2010 The Scottish
Adult Neurodevelopmental Services. ADHD Shared Protocol
 Adult Neurodevelopmental Services ADHD Shared Protocol Issue 1: April 2016 1 2 Adult Neurodevelopmental Service Shared Care Protocol for Adult Attention Deficit Hyperactivity Disorder (ADHD) 1. BACKGROUND
Adult Neurodevelopmental Services ADHD Shared Protocol Issue 1: April 2016 1 2 Adult Neurodevelopmental Service Shared Care Protocol for Adult Attention Deficit Hyperactivity Disorder (ADHD) 1. BACKGROUND
Conduct Disorder in Children and Young People (CYP 5-18 years of age) RISPERIDONE Effective Shared Care Agreement (ESCA)
 RISPERIDONE Effective Shared Care Agreement (ESCA)") E102 Conduct Disorder in Children and Young People (CYP 5-18 years of age) RISPERIDONE Effective Shared Care Agreement (ESCA) Patient details Name: Date of birth: NHS number: Contact details Specialist:
E102 Conduct Disorder in Children and Young People (CYP 5-18 years of age) RISPERIDONE Effective Shared Care Agreement (ESCA) Patient details Name: Date of birth: NHS number: Contact details Specialist:
AT RISK MENTAL STATES IN PSYCHOSIS AND SCHIZOPHRENIA IN CHILDREN AND YOUNG PEOPLE
 AT RISK MENTAL STATES IN PSYCHOSIS AND SCHIZOPHRENIA IN CHILDREN AND YOUNG PEOPLE Topic AT RISK MENTAL STATES IN PSYCHOSIS AND SCHIZOPHRENIA IN CHILDREN AND YOUNG PEOPLE Scope 4.3.1 (a) Review question(s)
AT RISK MENTAL STATES IN PSYCHOSIS AND SCHIZOPHRENIA IN CHILDREN AND YOUNG PEOPLE Topic AT RISK MENTAL STATES IN PSYCHOSIS AND SCHIZOPHRENIA IN CHILDREN AND YOUNG PEOPLE Scope 4.3.1 (a) Review question(s)
for adults engaged with the Family Wellbeing Service Isle of Wight In Community Pharmacy for Isle of Wight Public Health Commissioned Services
 The supply of Champix (Varenicline) Tablets 500mcg and 1mg by registered community pharmacists for smoking cessation / management of nicotine withdrawal for adults engaged with the Family Wellbeing Service
The supply of Champix (Varenicline) Tablets 500mcg and 1mg by registered community pharmacists for smoking cessation / management of nicotine withdrawal for adults engaged with the Family Wellbeing Service
Pharmacy Medical Necessity Guidelines: Antipsychotic Medications
 Pharmacy Medical Necessity Guidelines: Antipsychotic Medications Effective: July. 1, 2016 Prior Authorization Required Type of Review Care Management Not Covered Type of Review Clinical Review Pharmacy
Pharmacy Medical Necessity Guidelines: Antipsychotic Medications Effective: July. 1, 2016 Prior Authorization Required Type of Review Care Management Not Covered Type of Review Clinical Review Pharmacy