John D. Schaeffer, DO PMG Neurology Missoula, MT
|
|
|
- Meryl Golden
- 6 years ago
- Views:
Transcription

1 John D. Schaeffer, DO PMG Neurology Missoula, MT

 NFTs: Intracellular accumulation of")
2 Alzheimer s Disease First described by Alois Alzheimer, a German neuropathologist, in 1907 Observed in a 51-year-old female patient with memory loss, disorientation, and hallucinations Postmortem studies characterized senile plaques and neurofibrillary tangles (NFTs) in the cerebral cortex Senile plaques: Extracellular accumulation of insoluble fragments of beta-amyloid (Aβ 1-42 ) NFTs: Intracellular accumulation of hyperphosphorylated tau strands
3
4
5
6
7 In Office Evaluation A. History B. General exam C. Neuro exam D. Formal cognitive assessment tool 1. MMSE 2. MoCA
8 Differential Diagnosis Vascular: vascular dementia Inflammatory: CNS vasculitis, autoimmune Toxic: medication, psychoactive and endocrine Metabolic: hypothyroid, DM, hypercalcemia Infectious: fungal, TB, meningitis Nutritional: B12 deficiency Degenerative: AD, FTLD, etc. Epileptic: nonconvulsive complex partial status Trauma: dementia pugilistica (CTE) Psychiatric: conversion disorder Neoplastic: meningeal carcinomatous, paraneoplastic, etc Normal Pressure Hydrocephalus

9 Common Causes of Dementia Alzheimer s Disease Amnestic multidomain dementia syndrome Posterior Cortical Atrophy/visual variant Logopenic Aphasic Variant Dementia with Lewy Bodies Vascular Cognitive Impairment Frontotemporal Lobar Degeneration Progressive Nonfluent/Agrammatic Aphasia Semantic Dementia Frontotemporal Dementia Behavioral Variant ALS Dementia Mixed Chronic Traumatic Encephalopathy
10
11
12
13
14 Clinical Features DLB Cognitive Dementia Fluctuations Neuropsychiatric Visual hallucinations Delusions Depression Anxiety Motor Parkinsonism Sensory Anosmia Color vision changes Sleep REM Behavioral Disorder Hypersomnolence Insomnia Autonomic Orthostatic hypotension Urinary incontinence Constipation Erectile dysfunction
15 CHRONIC TRAUMATIC ENCEPHALOPATHY
16 CHRONIC TRAUMATIC ENCEPHALOPATHY
17 CHRONIC TRAUMATIC ENCEPHALOPATHY
18 CHRONIC TRAUMATIC ENCEPHALOPATHY
19 CHRONIC TRAUMATIC ENCEPHALOPATHY
20 CHRONIC TRAUMATIC ENCEPHALOPATHY
21
22
23
24
25
26

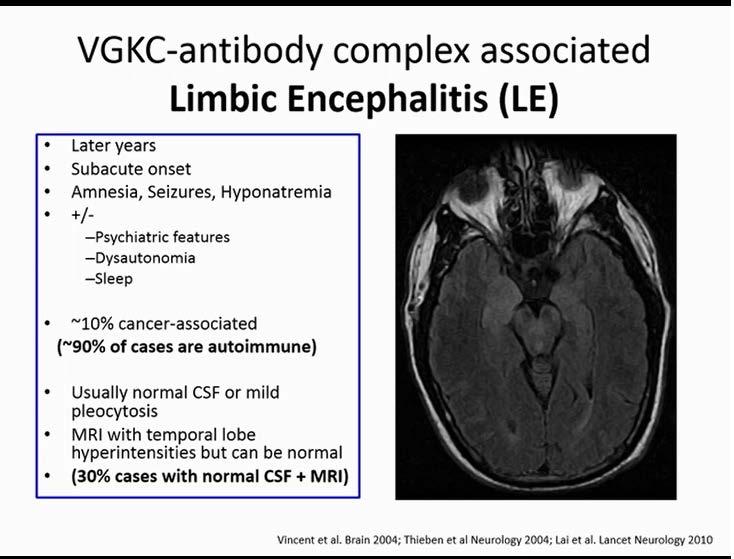
27 To Evaluate Further, A. Lab tests B. Conventional imaging C. Neuropsychological testing -Paraneoplastic panel -Antibodies - NMDAR - VGKC

28 To Evaluate Further, A. Lab tests B. Conventional imaging C. Neuropsychological testing D. Genetic testing? E. Functional Imaging (PET)?

29 CHRONIC TRAUMATIC ENCEPHALOPATHY
30
31
32
?")
33 To Evaluate Further, A. Lab tests B. Conventional imaging C. Neuropsychological testing D. Genetic testing? E. Functional Imaging (PET)? - Normal vs MCI vs dementia - Domains involved - Type of PPA - Dementia patterns
34 To Evaluate Further, A. Lab tests B. Conventional imaging C. Neuropsychological testing D. Genetic testing? E. Functional Imaging (PET)?
35 Risk factors for AD Age - Risk doubles every 5 years from If could delay onset by 5 yrs = 50% reduction in cases Family History x baseline risk if an affected first degree relative - 38% by age 85 Genes Dementia - If multiple family members affected before age 60 - Consider mutations of PS1, PS2, APP - If present, risk approaches - Accounts for about 5% of all AD - Genetic counseling - About 40% in this group will have an identifiable mutation
36 Dementia APOE (Distribution and clearance of Aβ?, synaptic plasticity?) Homozygous for E4 85% chance of AD by age x baseline risk Heterozygous for E4 No E % chance of AD by age x baseline risk 5-15% chance of AD by age 85 E2 appears protective Not specific for AD E2 (7%), E3 (79%), E4 (14%)
37 Summary The risk of AD increases with age, but younger onset is more likely to have a genetic basis Autosomal dominant mutations should be suspected in the right setting; genetic counseling and testing should be offered All other forms of possible inheritance are not clinically recommended at this time, but that may change if an effective therapy is discovered AD specifically, and dementia generally, is usually a polygenic entity, as well as a pathologically heterogenous disorder, especially in older patients
38 To Evaluate Further, A. Lab tests B. Conventional imaging C. Neuropsychological testing D. Genetic testing? E. Functional Imaging? FDG-PET Amyloid-PET Tau-PET SPECT (β CIT)

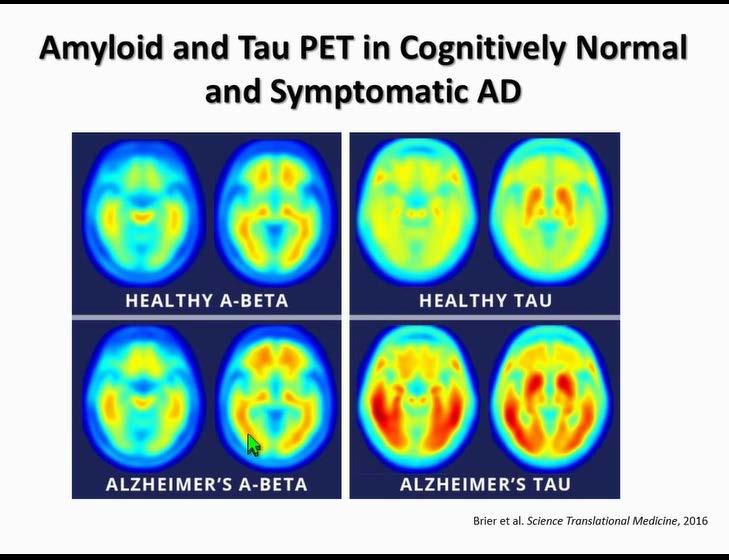
39 Functional Imaging Position Emission Tomography (PET) Labeled glucose Metabolism decreases in areas specific for AD Characteristic pattern can be present early in AD Adds marginally to existing diagnostic criteria - more sensitive than specific Can be helpful for distinguishing AD from other dementias Different dementias have different patterns Only approved neuro use is for distinguishing AD from Frontotemporal dementia
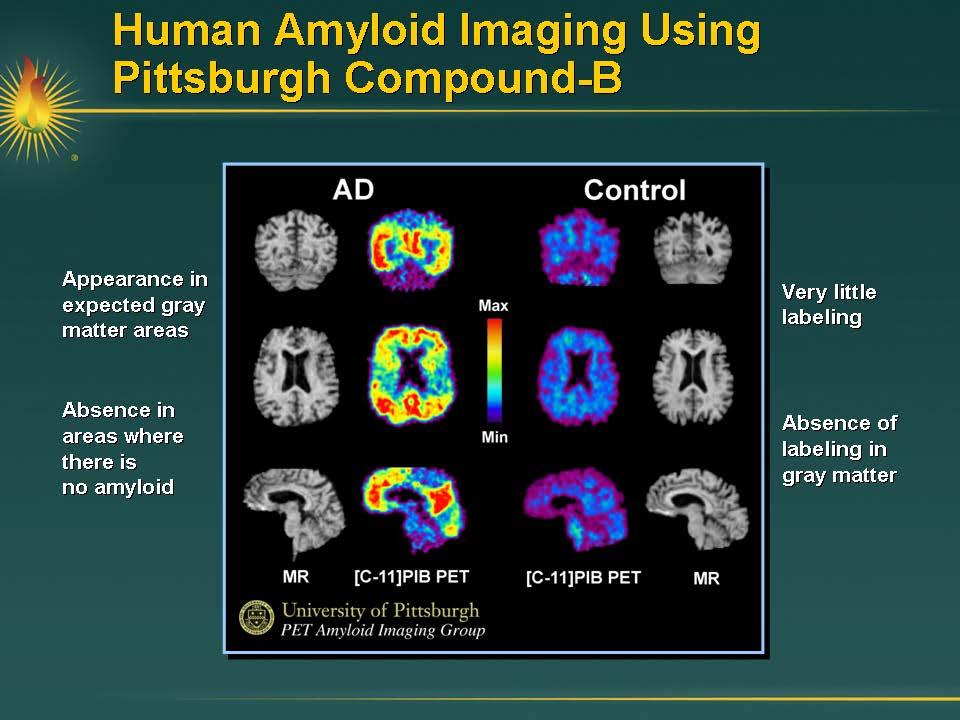
40
41
![TAU IMAGING [ 11 C]PBB3 preferentially interacts with](/docs-images/76/74087649/images/42-11.jpg "high-affinity for components formed by tau assemblies.")
42 TAU IMAGING [ 11 C]PBB3 preferentially interacts with high-affinity for components formed by tau assemblies.
43
44
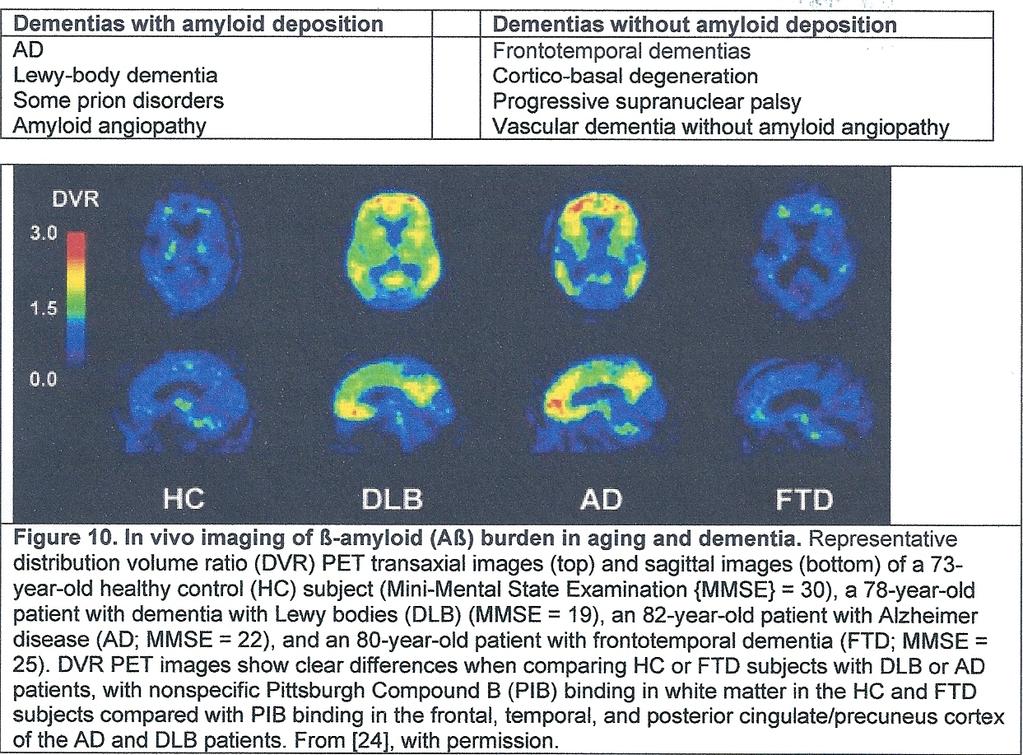
45 Additional Testing Comments Amyloid PET imaging can be used to predict conversion from normal cognition to MCI/dementia CSF ratio of total-tau (t-tau) or phosphorylated-tau (p-tau) to β-amyloid can predict conversion from normal cognition to MCI/dementia APOE genotype predictive of finding abnormal amyloid PET scan in cognitively normal individuals p-tau/t-tau ratio may be helpful for diagnosis of CTE The various imaging/csf studies can be used to more accurately diagnose dementia types (will be clinically useful when we have more specific treatments)
46


47 MILD COGNITIVE IMPAIRMENT - PHYSICAL ACTIVITY - COGNITIVE ACTIVITY - SOCIAL ACTIVITY - CARDIOVASCULAR RISK FACTORS - DIET
48 Approved Drugs for AD Dementia in the USA Drug Donepezil (Aricept) Rivastigmine (Exelon) Galantamine (Razadyne) Memantine (Namenda) Mechanism of Action Cholinesterase Inhibitor Cholinesterase Inhibitor Cholinesterase Inhibitor Glutamate Modulator As of September 2017, no other drugs near approval
49 Practical Issues in the Use of Cholinesterase Inhibitors When to start treatment with cholinesterase inhibitors? When dementia is diagnosed What are contraindications? Gastritis, chronic diarrhea, urinary urgency Second degree AV block

50 Practical Issues in the use of Cholinesterase Inhibitors Who to treat? Clinically diagnosed Alzheimer dementia Dementia with Lewy Bodies Consider treating when cerebrovascular disease dementia is diagnosed Unlikely to be of value in bvftd or non-ad PPA s Unlikely to be of value in MCI Unlikely to be of value in severe dementia
51 Practical Issues in the use of Cholinesterase Inhibitors How to adjust dosing Use standard doses of : Donepezil 10 mg daily Galantamine mg daily Rivastigmine 6 12 mg orally or 9.4 mg transdermal Higher doses are commonly associated with gastrointestinal side effects No compelling evidence that higher doses have greater efficacy Consider switching drugs when Toxicity occurs that could be idiosyncratic and might not be classspecific
52 Practical Issues in the use of Memantine Who to treat? Moderately severe AD dementia When to start treatment? After starting a cholinesterase inhibitor Contraindications None really How to adjust dose Use standard dose When to stop? Same as cholinesterase inhibitors
53 Practical Issues in the use of Cholinesterase Inhibitors When to stop cholinesterase Inhibitors? When patients reach a stage of severe dementia where delay of symptom progression is no longer of value to them.
54 The Future of Therapeutics in AD Promising leads but still lacking a definitive therapy that alters the natural history, economics and outlook of the disease Many questions remain about best targets
55 Management of DLB and PDD Pharmacologic Options Acetylcholinesterase inhibitors Donepezil * Rivastigmine * Galantamine * Glutamate antagonist Memantine * Atypical Neuroleptics Quetiapine ** Olanzapine ** Clozapine ** Antidepressants Sertraline Citalopram Venlafaxine Dopaminergics Levodopa ** Pramipexole Ropinirole Sedative/hypnotics Clonazepam ** Melatonin ** Psychostimulants/Wake-promoting agents Methylphenidate Armodafinil ** * Efficacy demonstrated in large RCT ** Efficacy suggested in small RCT
56 Treatment in FTD SSRI Loss of dorsal raphe 5HT neurons Low 5HT found on autopsy/csf/pet May underlie irritability, depression, compulsions Avoid cholinesterase inhibitors, memantine Cholinesterase inhibitors: mixed effects on cognition, may worsen behavior Memantine: no effect on behavior, may worsen cognition
57
58
59
60
61
62

63
64
65
66
67 General Principles of Behavioral Management Try behavioral modification techniques Avoid anticholinergic medications Avoid benzodiazepines Eliminate hazardous environments Provide adequate supervision Correct sensory deprivation Control over-stimulation Educate caregivers
68 Things to Consider with Sudden Changes in Behavior Check for infection and dehydration Evaluate for changes in medical conditions Watch for adverse medication effects: Stop or adjust any new medication added Assist with pain management In hospital setting: get a sitter to reassure, calm, redirect Try behavioral modification techniques Environmental modification for reactive aggression Endeavor to avoid hospital admission
69 General Principles of Behavior Pharmacotherapy Behavioral drug use in dementia is off-label Treat specific underlying behaviors Patients may have several behaviors that are best treated with different medications Individualize Polypharmacy is typical Use very low doses: 1/2 to 1/3 dose Review ongoing need
70 Treatment of Depression in Dementia SSRIs: effective and good tolerability Paroxetine and Fluvoxamine: slightly more sedating Fluoxetine: more energizing Sertraline and (Es)citalopram: in between SNRIs: Very few specific studies in dementia; may have beneficial side effects
71 Preferred Approaches for Depression in Dementia First line preferred treatments Sertraline *, Citalopram *, Escitalopram Paroxetine *, Fluvoxamine *, Fluoxetine * Second line preferred treatments Venlafaxine, Bupropion, Mirtazapine Trazodone * Lamotrigine Clomipramine*, Nortryptiline AVOID: tertiary tricyclic anti-depressants *positive double blind studies
72 Anxiety Worry, nervousness, phobias, fear of being left alone and somatic complaints Godot syndrome: anxiety regarding upcoming events Common early in dementia Can lead to irritability and aggression
73 Preferred Approaches for Anxiety in Dementia First line preferred treatments SSRI s *, Trazodone Second line preferred treatments Valproate * Gabapentin/Lamotrigine Buspirone Donepezil *, Galantamine *, Rivastigmine AVOID: Benzodiazepines *positive double blind studies
74 Behavior Modification Techniques Non-verbal Communication Always smile Use an open posture Positive gestures Nod yes Wave hello Shrug shoulders Pat on the back Hand them objects they like for distraction
75 Disinhibition / Intrusiveness Caused by impulsivity and poor judgement Often leads to intrusiveness Not typically severe in AD Very common in frontal lobe dementias
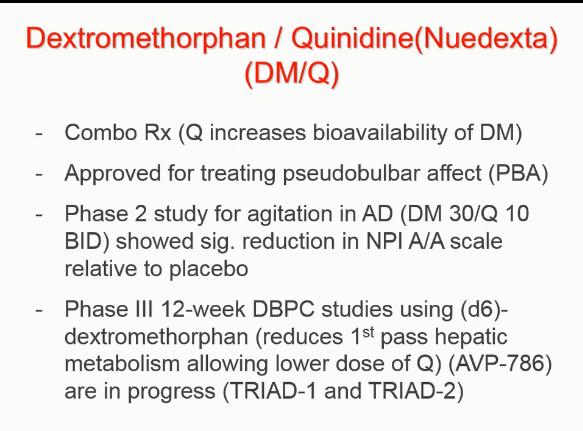
76 Treatment of Mood Lability, Disinhibition, Intrusiveness, Euphoria and Mania in Dementia Dextromethorphan/quinidine: Pseudobulbar affect Anticonvulsants: Good mood stabilizing properties but studies are lacking in dementia; Divalproex 250 to 1000 in divided doses and sprinkle formulation easy to give SSRIs: Studies show help with lability, social dysdecorum, disinhibition: watch for mania Cholinesterase inhibitions: Reduce disinhibition Olanzapine: decreases disinhibition and euphoria
77 Preferred Approaches for Mood Liability, Disinhibition, Intrusiveness, Euphoria and Mania in Dementia First line preferred treatments Valproate Dextromethorphan/quinidine for PBA Second line preferred treatments Citalopram *, SSRIs Gabapentin, Lamotrigine, Carbamazepine other anticonvulsants Galantamine *, Memantine *, Rivastigmine Olanzapine * and other atypicals *positive double blind studies
78 Behavior and Modification Techniques Distraction and Redirection Verbal redirection Object distraction Food distraction Can you help me?
79 Sleep Disturbances Diurnal rhythm disruption, repetitive wakenings, insomnia Disorientation and confusion in the evening or night (sundowning) often due to loss of sensory stimuli and fatigue; can lead to agitation and wandering
80 Treatment of Sleep Disturbances in Dementia Trazodone Helpful for insomnia and sleep/wake cycle disturbances in doses from mg qhs with minimal anticholinergic effects Zolpidem In 2 AD patients showed less insomnia Gabapentin Helped sleep in 20 AD subjects Melatonin Mixed results in dementia but largest study showed no benefit
81 Preferred Approaches for Sleep Disturbances in Dementia First line preferred treatments: Trazodone* Zolpidem Melatonin* Second line preferred treatments: Mirtazepine, Nortryptiline if depressed Quetiapine, Risperidone, Olanzapine if psychotic Valproate if restless, intrusive or manic Gabapentin Avoid: Barbiturates, benzodiazepines, hydroxyzine, diphenhydramine *positive double blind studies
82 Behavior Modification Techniques for Sleep/Wake Cycle Disturbances Regular sleep habits Avoid naps Increase daytime activities Avoid late meals, caffeine, alcohol
83 Aberrant Motor Behaviors Wandering occurs in 3-26% of AD patients Psychomotor activity disturbances include: Motor restlessness - hyperkinesis Purposeless activities - pacing Hoarding and hiding items - packing/unpacking Dressing/undressing - hyperverbalness Intrusive touching - pounding/tapping Insistent verbal repetition - singing
84 Treatment of Aberrant Motor Behaviors in Dementia Divalproex Reduces restlessness in dementia Citalopram mg daily decreased aberrant motor behaviors in open trial Sertraline Trend toward reducing aberrant motor behaviors in DBPC study Cholinesterase inhibitors Most will lessen wanting to go behaviors in AD Risperidone, Quetiapine Helped with wandering and restlessness
85 Preferred Approaches for Aberrant Motor Behaviors in Dementia First line preferred treatments Valproate* Citalopram Galantamine*, Rivastigmine, Memantine Second line preferred treatments Sertraline, Paroxetine, Trazodone Risperidone*, Quetiapine Gabapentin *positive double blind studies
86 Behavior Modification Techniques for Aberrant Motor Behaviors Obsessive-Compulsive traits Provide activities (fold clothes, ) Adequate supervision Psychomotor activity disturbance Allow wandering in a safe, contained environment Planned regular exercise, walking
87 Psychosis Delusions fixed false beliefs Theft Jealousy Phantom boarder Spouse as imposter (Capgras) House not home Hallucinations spurious sensory experience Visual, auditory, tactile, gustatory Content (simple complex) Belief/insight
88 Phenomenology vs Etiology Psychosis Idiopathic thought disorder? Specific disease-related pathophysiology? General medical condition (i.e. delirium)? Iatrogenic (meds)? Agitation Psychomotor dysregulation? Altered sleep-wake cycle? Pain or discomfort? Response to perceived threat? Search for trigger
89
90
91
92
93 NPS in Frontotemporal Dementia Cholinesterase inhibitors not effective, may worsen symptoms Memantine demonstrated not to be helpful in DBPC study Mood/anxiety/OCD sx SSRIs often helpful Repetitive motor behaviors/agitation Trazodone mg/day. (University of N. Carolina reports all of their FTD patients on combination of Sertraline and Trazodone) Insomnia Melatonin 3-10 mg qhs Hyperphagia Topamax?
94 Management of DLB and PDD Pharmacologic Options Acetylcholinesterase inhibitors Donepezil * Rivastigmine * Galantamine * Glutamate antagonist Memantine * Atypical Neuroleptics Quetiapine ** Olanzapine ** Clozapine ** Antidepressants Sertraline Citalopram Venlafaxine Dopaminergics Levodopa ** Pramipexole Ropinirole Sedative/hypnotics Clonazepam ** Melatonin ** Psychostimulants/Wake-promoting agents Methylphenidate Armodafinil ** * Efficacy demonstrated in large RCT ** Efficacy suggested in small RCT
95
96
97
98 THAT S A LOT OF INFORMATION The history still matters. Diagnostic tools for dementia are, and are continuing to, improve. Research remains extremely active but has shifted to underlying causes of dementia rather than symptomatic treatments. For mild cognitive impairment: 1. No expectation that ACHEI s or memantine will be helpful. 2. Consider recommending physical, cognitive, social activity, cardiovascular risk factor modification, Mediterranean-like diet. For Alzheimer disease: 1. Start ACHEI when dementia diagnosed. 2. Start memantine when dementia moderate.
99 THAT S A LOT OF INFORMATION For FTLD: 1. Most will benefit from SSRIs 2. Don t use cholinesterase inhibitors and avoid memantine. 3. Expect neuropsychiatric problems and expect polypharmacy may be necessary. For Lewy body dementias (DLB and PDD): 1. Use cholinesterase inhibitors. 2. Memantine may or may not be helpful. 3. Expect neuropsychiatric problems and polypharmacy. For neuropsychiatric symptoms of dementia: 1. Maximize use of behavioral techniques, which means educating caregivers. 2. There are guidelines for pharmacological treatment although data can be thin. Use when benefits > risks. 3. Research in this area of symptoms is increasing.

100
101
Diagnosis and Treatment of Alzhiemer s Disease
 Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
BEHAVIORAL PROBLEMS IN DEMENTIA
 BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
Medications and Non-Pharma Approaches to Treatment. David J. Irwin, MD Penn Frontotemporal Degeneration Center
 Medications and Non-Pharma Approaches to Treatment David J. Irwin, MD Penn Frontotemporal Degeneration Center Outline Non-Pharmacological Treatment Strategies Behavior Language Motor Supportive Care Check-points
Medications and Non-Pharma Approaches to Treatment David J. Irwin, MD Penn Frontotemporal Degeneration Center Outline Non-Pharmacological Treatment Strategies Behavior Language Motor Supportive Care Check-points
OLD AGE PSYCHIATRY. Dementia definition TYPES OF DEMENTIA. Other causes. Psychiatric disorders of the elderly. Dementia.
 Psychiatric disorders of the elderly OLD AGE PSYCHIATRY Dementia Depression Delusional disorder/late onset schizophrenia Delirium Dementia definition LOCALISATION OF CEREBRAL FUNCTION Impairment of multiple
Psychiatric disorders of the elderly OLD AGE PSYCHIATRY Dementia Depression Delusional disorder/late onset schizophrenia Delirium Dementia definition LOCALISATION OF CEREBRAL FUNCTION Impairment of multiple
Management of Behavioral Problems in Dementia
 Management of Behavioral Problems in Dementia Ghulam M. Surti, MD Clinical Assistant Professor Department of Psychiatry and Human Behavior Warren Alpert Medical School of Brown University Definition of
Management of Behavioral Problems in Dementia Ghulam M. Surti, MD Clinical Assistant Professor Department of Psychiatry and Human Behavior Warren Alpert Medical School of Brown University Definition of
GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences GERIATRIC MENTAL HEALTH AND MEDICATION TREATMENT RUTH KOHEN ASSOCIATE PROFESSOR UW DEPARTMENT OF PSYCHIATRY 5-4-2017
Psychotropic Medication Use in Dementia
 Psychotropic Medication Use in Dementia Marie A DeWitt, MD Diplomate of the American Board of Psychiatry and Neurology, Specialization in Psychiatry & Subspecialization in Geriatric Psychiatry Staff Physician,
Psychotropic Medication Use in Dementia Marie A DeWitt, MD Diplomate of the American Board of Psychiatry and Neurology, Specialization in Psychiatry & Subspecialization in Geriatric Psychiatry Staff Physician,
Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias. Aaron H. Kaufman, MD
 Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, MD Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, M.D. Health Sciences
Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, MD Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, M.D. Health Sciences
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia.
, also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia.") CHAPTER 3 Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia. This incurable, degenerative, terminal disease
CHAPTER 3 Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia. This incurable, degenerative, terminal disease
Form D1: Clinician Diagnosis
 Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
Initial Visit Packet Form D: Clinician Diagnosis NACC Uniform Data Set (UDS) ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to be completed by the clinician.
Dementia Update. Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota
 Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Nothing to disclose Dementia Progressive deterioration in mental function
Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Nothing to disclose Dementia Progressive deterioration in mental function
Recognition and Management of Behavioral Disturbances in Dementia
 Recognition and Management of Behavioral Disturbances in Dementia Danielle Hansen, DO, MS (Med Ed), MHSA INTRODUCTION 80% 90% of patients with dementia develop at least one behavioral disturbances or psychotic
Recognition and Management of Behavioral Disturbances in Dementia Danielle Hansen, DO, MS (Med Ed), MHSA INTRODUCTION 80% 90% of patients with dementia develop at least one behavioral disturbances or psychotic
Behavioral Issues in Dementia. March 27, 2014 Dylan Wint, M.D.
 Behavioral Issues in Dementia March 27, 2014 Dylan Wint, M.D. OVERVIEW Key points Depression Definitions and detection Treatment Psychosis Definitions and detection Treatment Agitation SOME KEY POINTS
Behavioral Issues in Dementia March 27, 2014 Dylan Wint, M.D. OVERVIEW Key points Depression Definitions and detection Treatment Psychosis Definitions and detection Treatment Agitation SOME KEY POINTS
Use of Psychotropic Medications in Older Adults with Dementia!
 Use of Psychotropic Medications in Older Adults with Dementia! Deepa Pattani, PharmD, RPh Owner: PrevInteract Health Deepa.Pattani@PrevInteract.com 972-372-9775 About Me Deepa Pattani, PharmD, RPh with
Use of Psychotropic Medications in Older Adults with Dementia! Deepa Pattani, PharmD, RPh Owner: PrevInteract Health Deepa.Pattani@PrevInteract.com 972-372-9775 About Me Deepa Pattani, PharmD, RPh with
Alzheimer s Disease. Pathophysiology: Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior,
 is a progressive dementia affecting cognition, behavior,") 2 Alzheimer s Disease Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior, and functional status with no known cause or cure. Patients eventually lose cognitive, analytical,
2 Alzheimer s Disease Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior, and functional status with no known cause or cure. Patients eventually lose cognitive, analytical,
Pharmacological Treatments for Neuropsychiatric Symptoms in Dementia 3/22/2018
 Pharmacological Treatments for Neuropsychiatric Symptoms in Dementia 3/22/2018 Mary Ellen Quiceno, MD, FAAN Associate Professor of Neurology UNTHSC Center for Geriatrics 855 Montgomery Street, PCC 4, Ft.
Pharmacological Treatments for Neuropsychiatric Symptoms in Dementia 3/22/2018 Mary Ellen Quiceno, MD, FAAN Associate Professor of Neurology UNTHSC Center for Geriatrics 855 Montgomery Street, PCC 4, Ft.
BEHAVIOURAL AND PSYCHOLOGICAL SYMPTOMS IN DEMENTIA
 BEHAVIOURAL AND PSYCHOLOGICAL SYMPTOMS IN DEMENTIA Unmet needs What might be your behavioural response to this experience? Content Definition What are BPSD? Prevalence How common are they? Aetiological
BEHAVIOURAL AND PSYCHOLOGICAL SYMPTOMS IN DEMENTIA Unmet needs What might be your behavioural response to this experience? Content Definition What are BPSD? Prevalence How common are they? Aetiological
WHEN THE GOING GETS TOUGH: Working Through the Challenges of Dementia Together. Presented by
 WHEN THE GOING GETS TOUGH: Working Through the Challenges of Dementia Together Presented by Our agenda for today Understanding behavioral symptoms in people living with dementia Briefly review key strategies
WHEN THE GOING GETS TOUGH: Working Through the Challenges of Dementia Together Presented by Our agenda for today Understanding behavioral symptoms in people living with dementia Briefly review key strategies
Comprehensive Approach to DLB Management
 Comprehensive Approach to DLB Management Bradley F. Boeve, MD Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Comprehensive Approach to DLB Management Disclosures
Comprehensive Approach to DLB Management Bradley F. Boeve, MD Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Comprehensive Approach to DLB Management Disclosures
Behavioral and Psychological Symptoms of dementia (BPSD)
") Behavioral and Psychological Symptoms of dementia (BPSD) Chris Collins - Old Age Psychiatrist, Christchurch chris.collins@cdhb.health.nz Approaching BPSD: the right mindset Assessment Non-drug management
Behavioral and Psychological Symptoms of dementia (BPSD) Chris Collins - Old Age Psychiatrist, Christchurch chris.collins@cdhb.health.nz Approaching BPSD: the right mindset Assessment Non-drug management
Lewy Body Disease. Dementia Education for the First Responder July 27, 2017
 Lewy Body Disease Dementia Education for the First Responder July 27, 2017 Dylan Wint, M.D. NV Energy Chair for Brain Health Education Cleveland Clinic Lou Ruvo Center for Brain Health OUTLINE Lewy body
Lewy Body Disease Dementia Education for the First Responder July 27, 2017 Dylan Wint, M.D. NV Energy Chair for Brain Health Education Cleveland Clinic Lou Ruvo Center for Brain Health OUTLINE Lewy body
Overview. Overview. Parkinson s disease. Secondary Parkinsonism. Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits
 Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Parkinson s Disease Psychosis Treatment in Long-Term Care: Clinical and Operational Considerations
 Parkinson s Disease Psychosis Treatment in Long-Term Care: Clinical and Operational Considerations Pari Deshmukh MD Triple board-certified psychiatrist (Boards of psychiatry, addiction medicine, integrative
Parkinson s Disease Psychosis Treatment in Long-Term Care: Clinical and Operational Considerations Pari Deshmukh MD Triple board-certified psychiatrist (Boards of psychiatry, addiction medicine, integrative
Cognitive enhancers PINCH ME. Anticholinergic burden BPSD. Agitation, Aggression and antipsychotics
 Cognitive enhancers PINCH ME Anticholinergic burden BPSD Agitation, Aggression and antipsychotics 2 types Cholinesterase inhibitors licensed for mild to moderate AD Donepezil Galantamine Rivastigmine also
Cognitive enhancers PINCH ME Anticholinergic burden BPSD Agitation, Aggression and antipsychotics 2 types Cholinesterase inhibitors licensed for mild to moderate AD Donepezil Galantamine Rivastigmine also
Updates in Geriatric Psychiatry
 Updates in Geriatric Psychiatry Feyza Marouf M.D. Assistant Psychiatrist, MGH Program Director, Partners Healthcare Geriatric Psychiatry Fellowship Disclosures I have no significant financial relationships
Updates in Geriatric Psychiatry Feyza Marouf M.D. Assistant Psychiatrist, MGH Program Director, Partners Healthcare Geriatric Psychiatry Fellowship Disclosures I have no significant financial relationships
A BRIEF LOOK AT DEMENTIA
 Dementia A BRIEF LOOK AT DEMENTIA David Kaufman, MD Neurology Consultants of Bellin Health November 2, 2017 Defined as a progressive decline in cognitive function that impairs daily activities. Always
Dementia A BRIEF LOOK AT DEMENTIA David Kaufman, MD Neurology Consultants of Bellin Health November 2, 2017 Defined as a progressive decline in cognitive function that impairs daily activities. Always
Greg Jicha, M.D., Ph.D. Associate Professor of Neurology The Robert T. & Nyles Y. McCowan Chair in Alzheimer s Research University of Kentucky
 Greg Jicha, M.D., Ph.D. Associate Professor of Neurology The Robert T. & Nyles Y. McCowan Chair in Alzheimer s Research University of Kentucky Alzheimer s Disease Center and the Sanders-Brown Center on
Greg Jicha, M.D., Ph.D. Associate Professor of Neurology The Robert T. & Nyles Y. McCowan Chair in Alzheimer s Research University of Kentucky Alzheimer s Disease Center and the Sanders-Brown Center on
ALZHEIMER S DISEASE. Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey
 ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
MOVEMENT DISORDERS AND DEMENTIA
 MOVEMENT DISORDERS AND DEMENTIA FOCUS ON DEMENTIA WITH LEWY BODIES MADHAVI THOMAS MD NORTH TEXAS MOVEMENT DISORDERS INSTITUTE, INC DEMENTIA de men tia dəˈmen(t)sh(ē)ə/ nounmedicine noun: dementia a chronic
MOVEMENT DISORDERS AND DEMENTIA FOCUS ON DEMENTIA WITH LEWY BODIES MADHAVI THOMAS MD NORTH TEXAS MOVEMENT DISORDERS INSTITUTE, INC DEMENTIA de men tia dəˈmen(t)sh(ē)ə/ nounmedicine noun: dementia a chronic
Delirium & Dementia. Nicholas J. Silvestri, MD
 Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Index. Note: Page numbers of article titles are in boldface type. A ADHD. See Attention-deficit/hyperactivity disorder (ADHD) b-adrenergic blockers
 b-adrenergic blockers") Note: Page numbers of article titles are in boldface type. A ADHD. See Attention-deficit/hyperactivity disorder (ADHD) a-adrenergic blockers for PTSD, 798 b-adrenergic blockers for PTSD, 798 Adrenergic
Note: Page numbers of article titles are in boldface type. A ADHD. See Attention-deficit/hyperactivity disorder (ADHD) a-adrenergic blockers for PTSD, 798 b-adrenergic blockers for PTSD, 798 Adrenergic
Appendix N: Research recommendations
 Appendix N: recommendations N.1 First-line treatment of motor symptoms recommendation 1 Interventions What is the effectiveness of initial levodopa monotherapy versus initial levodopa-dopamine agonist
Appendix N: recommendations N.1 First-line treatment of motor symptoms recommendation 1 Interventions What is the effectiveness of initial levodopa monotherapy versus initial levodopa-dopamine agonist
Objectives. Objectives continued: 3/24/2012. Copyright Do not distribute or replicate without permission 1
 Frontotemporal Degeneration and Primary Progressive Aphasia Caregiver and Professional Education Conference Diana R. Kerwin, MD Assistant Professor of Medicine-Geriatrics Cognitive Neurology and Alzheimer
Frontotemporal Degeneration and Primary Progressive Aphasia Caregiver and Professional Education Conference Diana R. Kerwin, MD Assistant Professor of Medicine-Geriatrics Cognitive Neurology and Alzheimer
Understanding Alzheimer s Disease
 Understanding Alzheimer s Disease Alzheimer s disease is an irreversible, progressive brain disorder that slowly impacts memory, thinking, skills and, eventually, the ability to carry out the simplest
Understanding Alzheimer s Disease Alzheimer s disease is an irreversible, progressive brain disorder that slowly impacts memory, thinking, skills and, eventually, the ability to carry out the simplest
The Person: Dementia Basics
 The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
Cognitive disorders. Dr S. Mashaphu Department of Psychiatry
 Cognitive disorders Dr S. Mashaphu Department of Psychiatry Delirium Syndrome characterised by: Disturbance of consciousness Impaired attention Change in cognition Develops over hours-days Fluctuates during
Cognitive disorders Dr S. Mashaphu Department of Psychiatry Delirium Syndrome characterised by: Disturbance of consciousness Impaired attention Change in cognition Develops over hours-days Fluctuates during
Pharmacological Treatment of Aggression in the Elderly
 Pharmacological Treatment of Aggression in the Elderly Howard Fenn, MD Adjunct Clinical Associate Professor Department of Psychiatry and Behavioral Sciences Stanford University Self-Assessment Question
Pharmacological Treatment of Aggression in the Elderly Howard Fenn, MD Adjunct Clinical Associate Professor Department of Psychiatry and Behavioral Sciences Stanford University Self-Assessment Question
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE
 Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Dementia ALI ABBAS ASGHAR-ALI, MD STAFF PSYCHIATRIST MICHAEL E. DEBAKEY VA MEDICAL CENTER ASSOCIATE PROFESSOR BAYLOR COLLEGE OF MEDICINE Objectives At the conclusion of the session, participants will be
Diagnosis and management of non-alzheimer dementias. Melissa Yu, M.D. Department of Neurology
 Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
Dementia Basics. Welcome! What to expect and how to handle a dementia diagnosis. In partnership with Scripps Health.
 Dementia Basics What to expect and how to handle a dementia diagnosis March 18, 2017 In partnership with Scripps Health Welcome! 1 Welcome Kristin Gaspar San Diego County Supervisor District 3 2 Our Mission:
Dementia Basics What to expect and how to handle a dementia diagnosis March 18, 2017 In partnership with Scripps Health Welcome! 1 Welcome Kristin Gaspar San Diego County Supervisor District 3 2 Our Mission:
WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient
 DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
Assessing and Managing the Patient with Cognitive Decline
 Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist
 and Glutamate (NMDA) Receptor Antagonist") Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist Medication Dosage Indication for Use Aricept (donepezil) Exelon (rivastigmine) 5mg 23mg* ODT 5mg Solution
Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist Medication Dosage Indication for Use Aricept (donepezil) Exelon (rivastigmine) 5mg 23mg* ODT 5mg Solution
Dementia: Managing Difficult Behaviors. No conflicts of interest. Off-label medication use will be discussed during this talk.
 Dementia: Managing Difficult Behaviors No conflicts of interest. Off-label medication use will be discussed during this talk. 1 Types of Neurocognitive Disorder Alzheimer s Disease Vascular Frontotemporal
Dementia: Managing Difficult Behaviors No conflicts of interest. Off-label medication use will be discussed during this talk. 1 Types of Neurocognitive Disorder Alzheimer s Disease Vascular Frontotemporal
Dementia: It s Not Always Alzheimer s
 Dementia: It s Not Always Alzheimer s A Caregiver s Perspective Diane E. Vance, Ph.D. Mid-America Institute on Aging and Wellness 2017 My Background Caregiver for my husband who had Lewy Body Dementia
Dementia: It s Not Always Alzheimer s A Caregiver s Perspective Diane E. Vance, Ph.D. Mid-America Institute on Aging and Wellness 2017 My Background Caregiver for my husband who had Lewy Body Dementia
Drugs used to relieve behavioural and psychological symptoms in dementia
 alzheimers.org.uk Drugs used to relieve behavioural and psychological symptoms in dementia People with dementia may develop behavioural and psychological symptoms including restlessness, aggression, delusions,
alzheimers.org.uk Drugs used to relieve behavioural and psychological symptoms in dementia People with dementia may develop behavioural and psychological symptoms including restlessness, aggression, delusions,
Dementia Past, Present and Future
 Dementia Past, Present and Future Morris Freedman MD, FRCPC Division of Neurology Baycrest and University of Toronto Rotman Research Institute, Baycrest CNSF 2015 Objectives By the end of this presentation,
Dementia Past, Present and Future Morris Freedman MD, FRCPC Division of Neurology Baycrest and University of Toronto Rotman Research Institute, Baycrest CNSF 2015 Objectives By the end of this presentation,
Psychiatric aspects of Parkinson s disease an update
 Psychiatric aspects of Parkinson s disease an update Dr Chris Collins 027 2787593 chris.collins@cdhb.health.nz Disclosures: none Non-motor aspects physical Sensory anosmia, visual symptoms Speech and
Psychiatric aspects of Parkinson s disease an update Dr Chris Collins 027 2787593 chris.collins@cdhb.health.nz Disclosures: none Non-motor aspects physical Sensory anosmia, visual symptoms Speech and
Non Alzheimer Dementias
 Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
Dementia NICE Guidelines Update. Key points for primary care - NICE guideline (June 2018 update ) 26 September 2018
 26 September 2018") Dementia NICE Guidelines Update Key points for primary care - NICE guideline (June 2018 update ) 26 September 2018 How NICE guidelines are reviewed Multidisciplinary guideline committee established Review
Dementia NICE Guidelines Update Key points for primary care - NICE guideline (June 2018 update ) 26 September 2018 How NICE guidelines are reviewed Multidisciplinary guideline committee established Review
Addressing Difficult Behaviors in Dementia
 Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
CHILD & ADOLESCENT PSYCHIATRY ALERTS, VOLUME XIV, 2012 INDEX
 A Adderall Counterfeit, 31 addiction, internet CBT, 55 ADHD Adjunctive Guanfacine, 11 Counterfeit Adderall, 31 Developmental Trajectory and Risk Factors, 5 Dopamine Transporter Alterations, 14 Extended-Release
A Adderall Counterfeit, 31 addiction, internet CBT, 55 ADHD Adjunctive Guanfacine, 11 Counterfeit Adderall, 31 Developmental Trajectory and Risk Factors, 5 Dopamine Transporter Alterations, 14 Extended-Release
A Basic Approach to Mood and Anxiety Disorders in the Elderly
 A Basic Approach to Mood and Anxiety Disorders in the Elderly November 1 2013 Sarah Colman MD FRCPC Clinical Fellow, Geriatric Psychiatry Mount Sinai Hospital, University of Toronto Disclosure No conflict
A Basic Approach to Mood and Anxiety Disorders in the Elderly November 1 2013 Sarah Colman MD FRCPC Clinical Fellow, Geriatric Psychiatry Mount Sinai Hospital, University of Toronto Disclosure No conflict
DEMENTIA AND MEDICATION
 DEMENTIA AND MEDICATION Dr. Siobhan Ni Bhriain, MRCP, MRCPsych. Clinical Director, Tallaght and SJH MHS, Consultant Old Age Psychiatrist, Chair, DSIDC Steering Committee. SUMMARY OF TODAY S TALK Dementia-definition,
DEMENTIA AND MEDICATION Dr. Siobhan Ni Bhriain, MRCP, MRCPsych. Clinical Director, Tallaght and SJH MHS, Consultant Old Age Psychiatrist, Chair, DSIDC Steering Committee. SUMMARY OF TODAY S TALK Dementia-definition,
Any interventions, where RCTs in PD are not available, are not included in the tables.
 Tables Interventions where new studies have been published are indicated in bold italics. Changes in conclusions are indicated in italics and are highlighted in yellow. Any interventions, where RCTs in
Tables Interventions where new studies have been published are indicated in bold italics. Changes in conclusions are indicated in italics and are highlighted in yellow. Any interventions, where RCTs in
40% of mild cognitive impairment 60% of patients in early stage of dementia
 BPSD Vague and under-researched although described clearly by Alois Alzheimer Term ratified by 1996 IPA consensus conference Not fully recognised in current diagnostic systems Bypassed by dementia strategy
BPSD Vague and under-researched although described clearly by Alois Alzheimer Term ratified by 1996 IPA consensus conference Not fully recognised in current diagnostic systems Bypassed by dementia strategy
Medications for Anxiety & Behavior in Williams Syndrome. Disclosure of Potential Conflicts. None 9/22/2016. Evaluation
 Medications for Anxiety & Behavior in Williams Syndrome Christopher J. McDougle, M.D. Director, Lurie Center for Autism Professor of Psychiatry and Pediatrics Massachusetts General Hospital and MassGeneral
Medications for Anxiety & Behavior in Williams Syndrome Christopher J. McDougle, M.D. Director, Lurie Center for Autism Professor of Psychiatry and Pediatrics Massachusetts General Hospital and MassGeneral
Depression in Late Life
 Depression in Late Life Robert Madan MD FRCPC Geriatric Psychiatrist Key Learnings Robert Madan MD FRCPC Key Learnings By the end of the session, participants will be able to List the symptoms of depression
Depression in Late Life Robert Madan MD FRCPC Geriatric Psychiatrist Key Learnings Robert Madan MD FRCPC Key Learnings By the end of the session, participants will be able to List the symptoms of depression
New life Collage of nursing Karachi
 New life Collage of nursing Karachi Presenter: Zafar ali shah Faculty: Raja khatri Subject: Pathophysiology Topic :Alzheimer s Disease Post RN BScN semester 2 nd Objective Define Alzheimer s Describe pathophysiology
New life Collage of nursing Karachi Presenter: Zafar ali shah Faculty: Raja khatri Subject: Pathophysiology Topic :Alzheimer s Disease Post RN BScN semester 2 nd Objective Define Alzheimer s Describe pathophysiology
10th Medicine Review Course st July Prakash Kumar
 10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD
 DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
Reducing the Anxiety of Pediatric Anxiety Part 2: Treatment
 Reducing the Anxiety of Pediatric Anxiety Part 2: Treatment Lisa Lloyd Giles, MD Medical Director, Behavioral Consultation, Crisis, and Community Services Primary Children s Hospital Associate Professor,
Reducing the Anxiety of Pediatric Anxiety Part 2: Treatment Lisa Lloyd Giles, MD Medical Director, Behavioral Consultation, Crisis, and Community Services Primary Children s Hospital Associate Professor,
Disclosure. Speaker Bureaus. Grant Support. Pfizer Forest Norvartis. Pan American Health Organization/WHO NIA HRSA
 Disclosure Speaker Bureaus Pfizer Forest Norvartis Grant Support Pan American Health Organization/WHO NIA HRSA How Common is Psychosis in Alzheimer s Disease? Review of 55 studies 41% of those with Alzheimer
Disclosure Speaker Bureaus Pfizer Forest Norvartis Grant Support Pan American Health Organization/WHO NIA HRSA How Common is Psychosis in Alzheimer s Disease? Review of 55 studies 41% of those with Alzheimer
The Basics of Alzheimer s Disease
 2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
2017 Memory Loss Conference The Basics of Alzheimer s Disease Tom Ala, MD Center for Alzheimer s Disease and Related Disorders Southern Illinois University School of Medicine Springfield, Illinois SIU
Psychotropic Strategies Handout Package
 Psychotropic Strategies Handout Package Psychotropic Strategies Learning Objectives Utilize all clinical information available Assess the patient s overall condition this is essential Basic Principles
Psychotropic Strategies Handout Package Psychotropic Strategies Learning Objectives Utilize all clinical information available Assess the patient s overall condition this is essential Basic Principles
Antipsychotics for Dementia Under Control or Over-Prescribed?
 Antipsychotics for Dementia Under Control or Over-Prescribed? Nathaniel Hedrick, PharmD ProCare HospiceCare, Manager of Clinical Services Learning Objectives Summarize the disease progression and most
Antipsychotics for Dementia Under Control or Over-Prescribed? Nathaniel Hedrick, PharmD ProCare HospiceCare, Manager of Clinical Services Learning Objectives Summarize the disease progression and most
Treatment of Anxiety (without benzos)
") Treatment of Anxiety (without benzos) Alison C. Lynch MD MS Clinical Professor Departments of Psychiatry and Family Medicine University of Iowa Health Care None Disclosures Overview/objectives Review common
Treatment of Anxiety (without benzos) Alison C. Lynch MD MS Clinical Professor Departments of Psychiatry and Family Medicine University of Iowa Health Care None Disclosures Overview/objectives Review common
Dementia. Assessing Brain Damage. Mental Status Examination
 Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
7/3/2013 ABNORMAL PSYCHOLOGY SEVENTH EDITION CHAPTER FOURTEEN CHAPTER OUTLINE. Dementia, Delirium, and Amnestic Disorders. Oltmanns and Emery
 ABNORMAL PSYCHOLOGY SEVENTH EDITION Oltmanns and Emery PowerPoint Presentations Prepared by: Ashlea R. Smith, Ph.D. This multimedia and its contents are protected under copyright law. The following are
ABNORMAL PSYCHOLOGY SEVENTH EDITION Oltmanns and Emery PowerPoint Presentations Prepared by: Ashlea R. Smith, Ph.D. This multimedia and its contents are protected under copyright law. The following are
Michael A. Lobatz MD The Neurology Center Scripps Rehabilitation Center
 Michael A. Lobatz MD The Neurology Center Scripps Rehabilitation Center Dementia an acquired syndrome consisting of a decline in memory and other cognitive functions Alzheimer s Disease Fronto temporal
Michael A. Lobatz MD The Neurology Center Scripps Rehabilitation Center Dementia an acquired syndrome consisting of a decline in memory and other cognitive functions Alzheimer s Disease Fronto temporal
Alzheimer s Disease - Dementia
 - Dementia Neurocognitive disorder with dysfunction or loss of " Memory " Orientation " Attention " Language " Judgment " Reasoning Other characteristics that can manifest " Personality changes " Behavioral
- Dementia Neurocognitive disorder with dysfunction or loss of " Memory " Orientation " Attention " Language " Judgment " Reasoning Other characteristics that can manifest " Personality changes " Behavioral
Delirium. Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning.
 and fluctuating course of deterioration in mental functioning.") Delirium Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning. DELIRIUM IS A MEDICAL EMERGENCY! Delirium: Hallmark Features Inattention-
Delirium Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning. DELIRIUM IS A MEDICAL EMERGENCY! Delirium: Hallmark Features Inattention-
2/12/2016. Drugs and Dementia in the Hospice Patient. Jim Joyner, Pharm.D., C.G.P. Director of Clinical Operations Outcome Resources
 Drugs and Dementia in the Hospice Patient Jim Joyner, Pharm.D., C.G.P. Director of Clinical Operations Outcome Resources 1 Drug Therapy: Targeted at Symptoms Cognitive: Impaired abstract thinking Impaired
Drugs and Dementia in the Hospice Patient Jim Joyner, Pharm.D., C.G.P. Director of Clinical Operations Outcome Resources 1 Drug Therapy: Targeted at Symptoms Cognitive: Impaired abstract thinking Impaired
Psychobiology Handout
 Nsg 85A / Psychiatric Page 1 of 7 Psychobiology Handout STRUCTURE AND FUNCTION OF THE BRAIN Psychiatric illness and the treatment of psychiatric illness alter brain functioning. Some examples of this are
Nsg 85A / Psychiatric Page 1 of 7 Psychobiology Handout STRUCTURE AND FUNCTION OF THE BRAIN Psychiatric illness and the treatment of psychiatric illness alter brain functioning. Some examples of this are
Psychiatric Treatment of the Concussed Athlete
 Psychiatric Treatment of the Concussed Athlete Eastern Athletic Trainers Association January 11 th, 2015 Alexander S. Strauss, MD Centra, P.C. E-MAIL: DRSTRAUSS@ALEXSTRAUSSMD.COM Evidence Mounts Linking
Psychiatric Treatment of the Concussed Athlete Eastern Athletic Trainers Association January 11 th, 2015 Alexander S. Strauss, MD Centra, P.C. E-MAIL: DRSTRAUSS@ALEXSTRAUSSMD.COM Evidence Mounts Linking
Organic mental disorders
 Organic mental disorders F00-F09 Organic, including symptomatic, mental disorders This block comprises a range of mental disorders grouped together on the basis of their having in common a demonstrable
Organic mental disorders F00-F09 Organic, including symptomatic, mental disorders This block comprises a range of mental disorders grouped together on the basis of their having in common a demonstrable
Caring for a Patient or Family Member with Alzheimer s Disease or Related Dementia
 Caring for a Patient or Family Member with Alzheimer s Disease or Related Dementia Tiffany D. Long, MS4 UNC School of Medicine MD Candidate Class of 2018 Disclaimers A portion of this project is/was supported
Caring for a Patient or Family Member with Alzheimer s Disease or Related Dementia Tiffany D. Long, MS4 UNC School of Medicine MD Candidate Class of 2018 Disclaimers A portion of this project is/was supported
Caring Sheet #11: Alzheimer s Disease:
 CARING SHEETS: Caring Sheet #11: Alzheimer s Disease: A Summary of Information and Intervention Suggestions with an Emphasis on Cognition By Shelly E. Weaverdyck, PhD Introduction This caring sheet focuses
CARING SHEETS: Caring Sheet #11: Alzheimer s Disease: A Summary of Information and Intervention Suggestions with an Emphasis on Cognition By Shelly E. Weaverdyck, PhD Introduction This caring sheet focuses
Alzheimer s Dementia May 5, 2008
 Sharon Leigh, PharmD. BCPS Alzheimer s Dementia Page - 1 - I. Dementia vs. delirium Alzheimer s Dementia May 5, 2008 Dementia Gradual onset (insidious) Chronic illness progressing over years Irreversible
Sharon Leigh, PharmD. BCPS Alzheimer s Dementia Page - 1 - I. Dementia vs. delirium Alzheimer s Dementia May 5, 2008 Dementia Gradual onset (insidious) Chronic illness progressing over years Irreversible
Behavioural and Psychological Symptoms of Dementia (BPSD) in Primary Care
 in Primary Care") Behavioural and Psychological Symptoms of Dementia (BPSD) in Primary Care Dr. John Puxty Ontario s Ontario s Strategy Strategy for Alzheimer for Disease and Related Dementia: Initiative #2, #2, Physician
Behavioural and Psychological Symptoms of Dementia (BPSD) in Primary Care Dr. John Puxty Ontario s Ontario s Strategy Strategy for Alzheimer for Disease and Related Dementia: Initiative #2, #2, Physician
Treatment Options for Bipolar Disorder Contents
 Keeping Your Balance Treatment Options for Bipolar Disorder Contents Medication Treatment for Bipolar Disorder 2 Page Medication Record 5 Psychosocial Treatments for Bipolar Disorder 6 Module Summary 8
Keeping Your Balance Treatment Options for Bipolar Disorder Contents Medication Treatment for Bipolar Disorder 2 Page Medication Record 5 Psychosocial Treatments for Bipolar Disorder 6 Module Summary 8
Parkinson s Disease: initial diagnosis, initial treatment & non-motor features. J. Timothy Greenamyre, MD, PhD
 Parkinson s Disease: initial diagnosis, initial treatment & non-motor features J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even
Parkinson s Disease: initial diagnosis, initial treatment & non-motor features J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even
Diagnosing & managing dementia & delirium
 Aging: Its complex management Dunedin School of Medicine Diagnosing & managing dementia & delirium Falling Confusion Incontinence A. John Campbell University of Otago Medical School New Zealand Impaired
Aging: Its complex management Dunedin School of Medicine Diagnosing & managing dementia & delirium Falling Confusion Incontinence A. John Campbell University of Otago Medical School New Zealand Impaired
Diagnosis before NIA AA The impact of FDG PET in. Diagnosis after NIA AA Neuropathology and PET image 2015/10/16
 The impact of FDG PET in degenerative dementia diagnosis Jung Lung, Hsu MD, Ph.D (Utrecht) Section of dementia and cognitive impairment Department of Neurology Chang Gung Memorial Hospital, Linkou, Taipei
The impact of FDG PET in degenerative dementia diagnosis Jung Lung, Hsu MD, Ph.D (Utrecht) Section of dementia and cognitive impairment Department of Neurology Chang Gung Memorial Hospital, Linkou, Taipei
Alison Charleston 1 st September 2016
 Alison Charleston 1 st September 2016 Clinical features of Parkinson s disease Differential diagnosis Management of the motor features Non-motor and neuropsychiatric aspects 100-200 per 100,000 prevalence
Alison Charleston 1 st September 2016 Clinical features of Parkinson s disease Differential diagnosis Management of the motor features Non-motor and neuropsychiatric aspects 100-200 per 100,000 prevalence
Reality, as perceived by the patient, constitutes the reality of the situation. My Mother s Doing What???!!
 My Mother s Doing What???!! Management & Treatment of Dementia Related Behaviors Objectives Describe the prevalence, etiology of dementia related behaviors that include physical outbursts & sexual hyperactivity.
My Mother s Doing What???!! Management & Treatment of Dementia Related Behaviors Objectives Describe the prevalence, etiology of dementia related behaviors that include physical outbursts & sexual hyperactivity.
For: NEON Primary Healthcare Providers By: Michelle Romero, DO June 2013
 For: NEON Primary Healthcare Providers By: Michelle Romero, DO June 2013 This power point is only a guideline for recommendations in the treatment of psychiatric disorders. This is not comprehensive. Please
For: NEON Primary Healthcare Providers By: Michelle Romero, DO June 2013 This power point is only a guideline for recommendations in the treatment of psychiatric disorders. This is not comprehensive. Please
Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O.
 Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O. Parkinson s Epidemiology AFFECTS 1% OF POPULATION OVER 65 MEAN AGE OF ONSET 65 MEN:WOMEN 1.5:1 IDIOPATHIC:HEREDITARY 90:10
Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O. Parkinson s Epidemiology AFFECTS 1% OF POPULATION OVER 65 MEAN AGE OF ONSET 65 MEN:WOMEN 1.5:1 IDIOPATHIC:HEREDITARY 90:10
Introduction to Drug Treatment
 Introduction to Drug Treatment LPT Gondar Mental Health Group www.le.ac.uk Introduction to Psychiatric Drugs Drugs and Neurotransmitters 5 Classes of Psychotropic medications Mechanism of action Clinical
Introduction to Drug Treatment LPT Gondar Mental Health Group www.le.ac.uk Introduction to Psychiatric Drugs Drugs and Neurotransmitters 5 Classes of Psychotropic medications Mechanism of action Clinical
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya
 DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
ANTIPSYCHOTICS IN LONG TERM CARE: Are We Doing More Harm than Good?
 ANTIPSYCHOTICS IN LONG TERM CARE: Are We Doing More Harm than Good? STEPHANIE M. OZALAS, PHARMD, BCPS, BCGP VA MARYLAND HEALTH CARE SYSTEM BALTIMORE, MD DISCLOSURES Off-label use of medications will be
ANTIPSYCHOTICS IN LONG TERM CARE: Are We Doing More Harm than Good? STEPHANIE M. OZALAS, PHARMD, BCPS, BCGP VA MARYLAND HEALTH CARE SYSTEM BALTIMORE, MD DISCLOSURES Off-label use of medications will be
DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future
 DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future Daniel S. Sitar Professor Emeritus University of Manitoba Email: Daniel.Sitar@umanitoba.ca March 6, 2018 INTRODUCTION EPIDEMIOLOGY
DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future Daniel S. Sitar Professor Emeritus University of Manitoba Email: Daniel.Sitar@umanitoba.ca March 6, 2018 INTRODUCTION EPIDEMIOLOGY
Dementia. Aetiology, pathophysiology and the role of neuropsychological testing. Dr Sheng Ling Low Geriatrician
 Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Alzheimer Disease and Related Dementias. Alzheimer Society of Manitoba Dr. David Strang
 Alzheimer Disease and Related Dementias Alzheimer Society of Manitoba Dr. David Strang What is Dementia? Dementia is a syndrome symptoms include loss of memory, judgment and reasoning, and changes in mood
Alzheimer Disease and Related Dementias Alzheimer Society of Manitoba Dr. David Strang What is Dementia? Dementia is a syndrome symptoms include loss of memory, judgment and reasoning, and changes in mood
The ABCs of Dementia Diagnosis
 The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS. Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA
 CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
10/5/2017. BEHAVIORAL and PSYCHOLOGICAL SYMPTOMS in DEMENTIA (BPSD) Dr. Shah MD, MPH Braodlawns Medical Center DISCLOSURE
 Dr. Shah MD, MPH Braodlawns Medical Center DISCLOSURE") 1 BEHAVIORAL and PSYCHOLOGICAL SYMPTOMS in DEMENTIA (BPSD) Dr. Shah MD, MPH Braodlawns Medical Center DISCLOSURE 2 Dr. Shah has no relevant conflicts with commercial interests to disclose. OBJECTIVES 3
1 BEHAVIORAL and PSYCHOLOGICAL SYMPTOMS in DEMENTIA (BPSD) Dr. Shah MD, MPH Braodlawns Medical Center DISCLOSURE 2 Dr. Shah has no relevant conflicts with commercial interests to disclose. OBJECTIVES 3
Medication Treatments for Dementia. Stephen Thielke
 Medication Treatments for Dementia Stephen Thielke Treatment is a MORAL decision. Facts can help you determine HOW to accomplish something. Facts cannot tell you WHAT YOU WANT to accomplish. Dementia Meds
Medication Treatments for Dementia Stephen Thielke Treatment is a MORAL decision. Facts can help you determine HOW to accomplish something. Facts cannot tell you WHAT YOU WANT to accomplish. Dementia Meds
Huntington s Disease Psychiatry. Christopher A. Ross MD PhD HDSA Convention June 6, Many slides adapted from Adam Rosenblatt, MD
 Huntington s Disease Psychiatry Christopher A. Ross MD PhD HDSA Convention June 6, 2008 --Many slides adapted from Adam Rosenblatt, MD Huntington s Disease Society of America The information provided by
Huntington s Disease Psychiatry Christopher A. Ross MD PhD HDSA Convention June 6, 2008 --Many slides adapted from Adam Rosenblatt, MD Huntington s Disease Society of America The information provided by