PSYCHIATRIC MANAGEMENT IN PRIMARY CARE. Dr Fayyaz Khan MBBS, MRCPsych, MSc Consultant Psychiatrist (Locum) Mersey Care NHS Trust
|
|
|
- Octavia Lucas
- 5 years ago
- Views:
Transcription
1 PSYCHIATRIC MANAGEMENT IN PRIMARY CARE Dr Fayyaz Khan MBBS, MRCPsych, MSc Consultant Psychiatrist (Locum) Mersey Care NHS Trust
2 Areas to cover Mood Disorders Anxiety Disorders Miscellaneous Conditions
3 Objectives 1. Practical tips in managing them in Primary Care. 2. When to refer. 3. Overview of National Guidelines.
4 MOOD DISORDERS
5 Diagnosis-ICD 10-Depression Key Symptoms (must have at least 2 of these) Low mood Anhedonia Fatigue Other Symptoms Disturbed sleep Poor appetite Poor concentration Reduced self esteem and self confidence Ideas of guilt, worthless Ideas of self harm or suicide Psychomotor agitation or retardation
6 Duration 2 weeks Degree- Number, Severity Mild= 4 symptoms Mod= 5-6 Sev= 7+ (with or without psychosis)
7 Treatment Approach Bio Psycho Social
8 Stepped-care model -NICE Focus of the intervention STEP 4: Severe and complex [a] depression; risk to life; severe selfneglect STEP 3: Persistent subthreshold depressive symptoms or mild to moderate depression with inadequate response to initial interventions; moderate and severe depression STEP 2: Persistent subthreshold depressive symptoms; mild to moderate depression STEP 1: All known and suspected presentations of depression Nature of the intervention Medication, high-intensity psychological interventions, ECT, crisis service, combined treatments, multiprofessional and inpatient care Medication, high-intensity Figure 1 The stepped-care mode psychological interventions, combined treatments, collaborative care and referral for further assessment and interventions Low-intensity psychosocial interventions, psychological interventions, medication and referral for further assessment and interventions Assessment, support, psychoeducation, active monitoring and referral for further assessment and interventions [a] Complex depression includes depression that shows an inadequate response to multiple treatments, is complicated by psychotic symptoms, and/or is associated with significant psychiatric comorbidity or psychosocial factors.

9 How do AD work? Increase levels of Serotonin & Noradrenaline
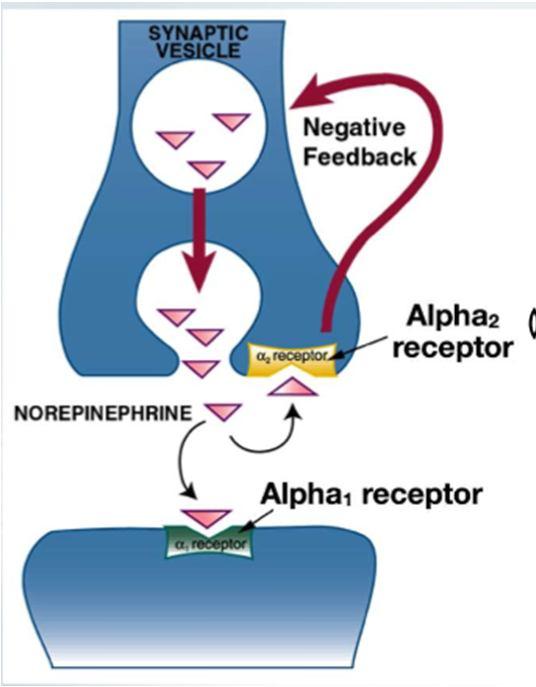
10
11 Types of AD SSRI- Fluoxetine, Citalopram, Sertraline SNRI- Duloxetine, Venlafaxine NRI- Roboxetine TCA- Amitriptyline, Dosulepin Other-Mirtazapine
12 Anti Depressants Do not use antidepressants routinely to treat persistent subthreshold depressive symptoms or mild depression because the risk benefit ratio is poor. NICE 1st Line: SSRI No effect/poorly tolerated: Another SSRI or different Class
13 AD-Swapping & Stopping 5,6 When changing from one antidepressant to another, abrupt withdrawal should usually be avoided. Cross-tapering is preferred, in which the dose of the ineffective or poorly tolerated drug is slowly reduced while the new drug is slowly introduced. In some cases cross-tapering may not be considered necessary. An example is when switching from one SSRI to another. Potential dangers of simultaneously administering two antidepressants include pharmacodynamic interactions (serotonin syndrome, hypotension, drowsiness) and pharmacokinetic interactions (e.g. elevation of tricyclic plasma levels by some SSRIs).
14 changing from tricyclics (TCA) citalopram/esc italopram fluoxetine paroxetine to tricyclics cross taper cautiously cross taper cautiously stop fluoxetine. Start tricyclic at very low dose and increase very slowly cross taper cautiously with very low dose of tricyclic to citalopram/esc to fluoxetine to paroxetine to sertraline to venlafaxine to mirtazapine italopram halve dose and add citalopram (or escitalopram) then slow withdrawal stop fluoxetine. Wait 4-7 days; start citalopram at 10mg per day (or escitalopram 5mg per day) and increase slowly withdraw paroxetine then start citalopram 10mg per day (or escitalopram 5mg per day) halve dose and add fluoxetine then slow withdrawal withdraw citalopram (escitalopram) then start fluoxetine withdraw paroxetine then start fluoxetine halve dose and add paroxetine then slow withdrawal halve dose and add sertraline then slow withdrawal withdraw withdraw citalopram citalopram (escitalopram) (escitalopram) and then start and then start paroxetine at 10 sertraline at 25 mg per day mg per day stop fluoxetine. Wait 4-7 days; start paroxetine at 10mg per day and increase slowly stop fluoxetine. Wait 4-7 days; start sertraline at 25 mg per day and increase slowly withdraw paroxetine then start sertraline at 25 mg per day cross taper cautiously starting with 37.5 mg per day cautious crosstapering recommended (4) withdraw and then start cautious crosstapering venlafaxine at 37.5 mg per day. recommended Increase very (4) slowly stop fluoxetine. cautious crosstapering Wait 4-7 days; start recommended, venlafaxine at start 37.5 mg per day. mirtazapine at Increase very 15mg daily (4) slowly withdraw paroxetine. Start venlafaxine at 37.5 mg per day. Increase very slowly cautious crosstapering recommended (4)
15 sertraline venlafaxine mirtazapine cross taper cautiously with very low dose of tricyclic cross taper cautiously with very low dose of tricycli cautious crosstapering recommended, using very low starting dose for tricyclic (4) withdraw sertraline then start citalopram 10mg per day (or escitalopram 5mg per day) cross taper cautiously. Start with citalopram 10 mg per day (or escitalopram 5mg per day) cautious crosstapering recommended (4) withdraw sertraline then start fluoxetine crosss taper cautiously. Start with 20 mg every other day cautious crosstapering recommended (4) withdraw sertraline then start paroxetine 10mg per day cross taper cautiously. Start with 10 mg per day. cautious crosstapering recommended (4) cross taper cautiously. Start with 25 mg per day cautious crosstapering recommended (4) withdraw sertraline then start venlafaxine at 37.5 mg per day cautious crosstapering recommended (4) cautious crosstapering recommended (4) cautious crosstapering recommended (4) stopping/with drawing of ticyclics particular reduce over antidepressant four weeks (4) s citalopram/esc italopram reduce over one to four weeks (4) fluoxetine at 20mg per day - just stop at 40 mg per day, reduce over four weeks paroxetine reduce over four weeks, or longer if necessary * sertraline reduce dose gradually over one to four weeks (4) venlafaxine reduce over four weeks or longer if necessary (2,4) mirtazapine reduce dose gradually over 4 weeks (4)
16 Clinical Scenarios 32 years old male with moderate depression has tried fluoxetine 20mg od as first anti depressant for 4 weeks and there has been no improvement. What is the next best step? 1) Wait for another 2-4 weeks for response. 2) Increase the dose. 3) Try a different AD.
17 Response time for AD? It is widely held that AD do not exert their effect for 2-4 weeks. This is a myth. All AD show a pattern of response where the rate of improvement is highest during weeks 1-2 and lowest during weeks 4-6. The Maudsley Prescribing Guidelines, 12 th edition-page-233
18 British Assoc Psychopharmacology Lack of significant improvement after 2-4 weeks treatment reduces the probability of eventual sustained response. After 4 weeks adequate treatment: if there is at least some improvement continue treatment with the same AD for another 2-4 weeks. if there is no trajectory of improvement undertake a next step (higher dose or different AD) After 6-8 weeks adequate treatment: if there is moderate or greater improvement continue same treatment. if there is minimal improvement undertake a next step (higher dose or different AD)
19 Clinical Scenario 40 years old female with moderate depression did not respond to citalopram. Has been now treated with fluoxetine 40mg for 4 weeks and there is no response. What is the next best step? Increase dose of fluoxetine to 60mg. Change to different class of AD.
20 Evidence of high dose SSRI in Major Depression High dose AD treatment for patients refractory to medium dose is not recommended for SSRI. 2
21 Clinical Scenario 35 years old lady, has been feeling low for 8 wks, following change of role at work. She took this change as a failure and developed feeling of worthlessness. She started making mistakes at work and was experiencing occasional thoughts of life is not worth living, but did not made any attempts to end her life and continued to work. She is able still to complete her household chores, but does get easily tired and is struggling to look after her 6 years old son. She was prescribed fluoxetine 20mg od, which she stopped after 1 week due to side effects of nausea. What is your diagnosis and management plan?
22 Clinical Scenario 60 years old female patient, on Haloperidol for Schizophrenia, presents with major depression. Which AD s are contraindicated?
23 Clinical Scenario 60 years old female, with history of IHD, is currently on erythromycin, presents with major depression. Which AD s are contraindicated?
24 Clinical Scenario 50 years old female patient, on ritonavir (anti retroviral), presents with major depression. Which AD s are contraindicated?
25 Clinical scenario 25 years old female presents to you with low mood, suicidal thoughts and intense feeling of worthlessness after splitting up with her boyfriend of 3 months. During consultation she was very emotional and hopeless. She reports to you that she has tried several anti depressants in the past without much benefit. What is your management plan?
26 DM & Depression 55 years old diabetic, female with history of major depression and poor response to x2 SSRI. Which AD should be avoided?
27 HTN & Depression 55 years old male with Hypertension, history of major depression and poor response to x2 SSRI. Which AD should be avoided?
28 Average duration between onset and diagnosis of BPAD? 6 years: UNSW Australia and Italian study published in the Canadian Journal of Psychiatry, July 2016.The meta-analysis of 9,415 patients from 27 studies, the largest of its kind. Some studies have quoted up to 10 years.
29 When to refer to Mental Health Services NICE: Referral to specialist mental health services should normally be for people with depression: who are at significant risk of self-harm, have psychotic symptoms, require complex multi-professional care, or where an expert opinion on treatment and management is needed. With history of mania and hyopmania
30 Anxiety Disorders GAD Panic Disorder PTSD OCD Social Phobia
31 GAD, PD, OCD (NICE): Psychological therapy is more effective than pharmacological therapy and should be used as first line where possible. SSRI s & Venlafaxine across the range of Anxiety Disorders.
32 GAD 4 Reassurance Anxiety Mx including relaxation training, exposure therapy CBT Exercise
33 GAD 4 Emergency Mx: BZD (2-4 weeks) First Line SSRIs Venlafaxine Duloxetine Mirtazapine Pregabalin Other: Buspirone (negligible sedative, 4 wks of 10mg TDS) B- Blockers (somatic sx) Quetiapine
34 PD 4 CBT Anxiety Mx including relaxation training Combination- not consistently better than pharmacological alone
35 Panic Disorders 4 Emergency Mx: BZD (rapid effect, NICE does not recommend) First Line SSRIs Other: Venlafaxine Mirtazapine TCA (imipramine, clomipramine)
36 PTSD 4 Debriefing Counselling Anxiety Mx CBT EMDR
37 PTSD 4 Emergency Mx: Not usually appropiate First Line SSRIs Other: Mirtazapine Venlafaxine Duloxetine Clomipramine Anti psychotic (as augmentation)
38 OCD 4 Exposure therapy Behavioural therapy CBT Combination- Most effective
39 OCD 4 Emergency Mx: BZD (Not usually appropriate) First Line SSRIs Clomipramine Other: Citalopram with Clomipramine Anti Psychotic with AD Mirtazapine with AD (NICE)
40 Clinical scenario A 45 years old lady with a OCD of moderate severity, not keen on psychological therapy was prescribed fluoxetine 20mg od. She was followed up in 4 weeks time and there was no improvement. What will you do? Increase the dose or Change medication
41 Continue The dose was increased to 40mg OD, she was followed up after 4 weeks and still reports no improvement. What will you do now? Increase the dose or Change medication
42 Continue She was trialled on Sertraline 50mg od for 4 weeks and still no improvement. What will you do now? Increase the dose or Change medication
43 Continue Sertraline was gradually increased to 200mg od over 10 week period and there was not any significant improvement. What will you do now? Change medication. Wait longer Refer to Secondary Mental Health Services.
44 Dose response of SSRI in OCD Compared with low or medium doses, high doses of SSRI were associated with improved treatment efficacy.1
45 The American Psychiatric Association Practice Guidelines recommend higher target doses of SSRIs in the treatment of OCD than they do for depression. 3 High doses usually needed, at least 12wks for treatment response. 5
46 Social Phobia 4 CBT Exposure therapy Combination- More effective
47 Social Phobia 4 Emergency Mx: BZD (PRN) First Line SSRIs Pregabalin Gabapentin Other: BZD with SSRI Propranolol (performance anxiety) Venlafaxine Olanzapine
48 Insomnia Difficulty in initiating and maintaining sleep. Symptom of underlying problem. Identify and Treat the cause. Emphasis on sleep hygiene
49 Sleep Hygiene Avoid: Excessive caffeine, alcohol, nicotine 3-6 hrs before bed. Daytime nap. TV/Ipad/Phones 1 hr before bed. Strenuous exercise or mental activity near bed time. Prolonged periods in bed if not asleep. Promote: Bedtime routine, comfortable environment, warm bath, light exercise.
50 BNF Listed Z : Zopiclone, Zolpidem BZD: Nitrazepam, Temazepam Anti Histamines: Promethazine (low abuse potential) Melatonin ( Circadin 2mg, 55 and above, up to 13 wks)
51 Minimise Polypharamacy Stress Incontinence & Depression Duloxetine Diabetic Neuropathy & Depression Duloxetine Peripheral & Central Neuropathic Pain and GAD Pregabalin Seizures and GAD Pregabalin
52 Insomnia and Depression Mirtazapine, TCA, Trazadone
53 Thank you
54 References 1. Meta analysis of dose response of SSRI in OCD. J F Leckman & C Pitteger. Molecular Psychiatry 15, (2010) 2.Is dose escalation of antidepressants a rational strategy after a medium dose treatment has failed? European Archives of Psychiatry and Clinical Neuroscience, December 2005, Volume 255, issue 6, pp American_Psychiatric_Association. Practice guideline for the treatment of patients with obsessive-compulsive disorder. American Psychiatric Association: Arlington, VA, The Maudsley Prescribing Guidelines, 12 th Edition. 5. Oxford Handbook of Psychiatry, 3 rd edition. 6. GP Notebook
Pregnancy. General Principles of Prescribing in Pregnancy (The Maudsley, 12 th Edition)
") Pregnancy General Principles of Prescribing in Pregnancy (The Maudsley, 12 th Edition) In all women of child bearing potential Always discuss the possibility of pregnancy; half of all pregnancies are unplanned
Pregnancy General Principles of Prescribing in Pregnancy (The Maudsley, 12 th Edition) In all women of child bearing potential Always discuss the possibility of pregnancy; half of all pregnancies are unplanned
Reducing the Anxiety of Pediatric Anxiety Part 2: Treatment
 Reducing the Anxiety of Pediatric Anxiety Part 2: Treatment Lisa Lloyd Giles, MD Medical Director, Behavioral Consultation, Crisis, and Community Services Primary Children s Hospital Associate Professor,
Reducing the Anxiety of Pediatric Anxiety Part 2: Treatment Lisa Lloyd Giles, MD Medical Director, Behavioral Consultation, Crisis, and Community Services Primary Children s Hospital Associate Professor,
Document Title Pharmacological Management of Generalised Anxiety Disorder
 Document Title Pharmacological Management of Generalised Anxiety Disorder Document Description Document Type Policy Service Application Trust Wide Version 1.1 Policy Reference no. POL 201 Lead Author(s)
Document Title Pharmacological Management of Generalised Anxiety Disorder Document Description Document Type Policy Service Application Trust Wide Version 1.1 Policy Reference no. POL 201 Lead Author(s)
Pharmacological Treatment of Anxiety & Depressive Disorders
 Pharmacological Treatment of Anxiety & Depressive Disorders Dr Gary Jackson (MB BCh FRCPsych) Consultant Psychiatrist The Priory Hospital Chelmsford Wellesley Hospital Southend-on-Sea Medical Secretary:
Pharmacological Treatment of Anxiety & Depressive Disorders Dr Gary Jackson (MB BCh FRCPsych) Consultant Psychiatrist The Priory Hospital Chelmsford Wellesley Hospital Southend-on-Sea Medical Secretary:
Guidelines MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD)
") MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD) Guidelines CH Lim, B Baizury, on behalf of Development Group Clinical Practice Guidelines Management of Major Depressive Disorder A. Introduction Major depressive
MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD) Guidelines CH Lim, B Baizury, on behalf of Development Group Clinical Practice Guidelines Management of Major Depressive Disorder A. Introduction Major depressive
Anxiety Disorders: First aid and when to refer on
 Anxiety Disorders: First aid and when to refer on Presenter: Dr Roger Singh, Consultant Psychiatrist, ABT service, Hillingdon Educational resources from NICE, 2011 NICE clinical guideline 113 What is anxiety?
Anxiety Disorders: First aid and when to refer on Presenter: Dr Roger Singh, Consultant Psychiatrist, ABT service, Hillingdon Educational resources from NICE, 2011 NICE clinical guideline 113 What is anxiety?
Mental illness A Broad Overview. Dr H Pathmanandam March 2017
 Mental illness A Broad Overview Dr H Pathmanandam March 2017 Introduction Mental disorders are common in primary and secondary care Many are not recognised and not treated Some receive unnecessary or inappropriate
Mental illness A Broad Overview Dr H Pathmanandam March 2017 Introduction Mental disorders are common in primary and secondary care Many are not recognised and not treated Some receive unnecessary or inappropriate
Volume 4; Number 5 May 2010
 Volume 4; Number 5 May 2010 CLINICAL GUIDELINES FOR ANTIDEPRESSANT USE IN PRIMARY AND SECONDARY CARE Lincolnshire Partnership Foundation Trust in conjunction with Lincolnshire PACEF have recently updated
Volume 4; Number 5 May 2010 CLINICAL GUIDELINES FOR ANTIDEPRESSANT USE IN PRIMARY AND SECONDARY CARE Lincolnshire Partnership Foundation Trust in conjunction with Lincolnshire PACEF have recently updated
Anxiety Disorders.
 Anxiety Disorders Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@swedish.org Disclosures Neither I nor my spouse/partner
Anxiety Disorders Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@swedish.org Disclosures Neither I nor my spouse/partner
MEDICATION ALGORITHM FOR ANXIETY DISORDERS
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences MEDICATION ALGORITHM FOR ANXIETY DISORDERS RYAN KIMMEL, MD MEDICAL DIRECTOR HOSPITAL PSYCHIATRY UNIVERSITY OF WASHINGTON
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences MEDICATION ALGORITHM FOR ANXIETY DISORDERS RYAN KIMMEL, MD MEDICAL DIRECTOR HOSPITAL PSYCHIATRY UNIVERSITY OF WASHINGTON
Treatment of Anxiety (without benzos)
") Treatment of Anxiety (without benzos) Alison C. Lynch MD MS Clinical Professor Departments of Psychiatry and Family Medicine University of Iowa Health Care None Disclosures Overview/objectives Review common
Treatment of Anxiety (without benzos) Alison C. Lynch MD MS Clinical Professor Departments of Psychiatry and Family Medicine University of Iowa Health Care None Disclosures Overview/objectives Review common
KEY MESSAGES. It is often under-recognised and 30-50% of MDD cases in primary care and medical settings are not detected.
 KEY MESSAGES Major depressive disorder (MDD) is a significant mental health problem that disrupts a person s mood and affects his psychosocial and occupational functioning. It is often under-recognised
KEY MESSAGES Major depressive disorder (MDD) is a significant mental health problem that disrupts a person s mood and affects his psychosocial and occupational functioning. It is often under-recognised
PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS. Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA
 CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
Psychiatric Treatment of the Concussed Athlete
 Psychiatric Treatment of the Concussed Athlete Eastern Athletic Trainers Association January 11 th, 2015 Alexander S. Strauss, MD Centra, P.C. E-MAIL: DRSTRAUSS@ALEXSTRAUSSMD.COM Evidence Mounts Linking
Psychiatric Treatment of the Concussed Athlete Eastern Athletic Trainers Association January 11 th, 2015 Alexander S. Strauss, MD Centra, P.C. E-MAIL: DRSTRAUSS@ALEXSTRAUSSMD.COM Evidence Mounts Linking
Guidance on the use of Antidepressants for the Treatment of Unipolar Depression and Anxiety Spectrum Disorders in adults (Version 3 October 2014)
") Guidance on the use of Antidepressants for the Treatment of Unipolar Depression and Anxiety Spectrum Disorders in adults (Version 3 October 2014) Date of Preparation: September 2014 Date for next full
Guidance on the use of Antidepressants for the Treatment of Unipolar Depression and Anxiety Spectrum Disorders in adults (Version 3 October 2014) Date of Preparation: September 2014 Date for next full
Clinical Guideline / Formulary Document Pharmacy Department Medicines Management Services
 Clinical Guideline / Formulary Document Pharmacy Department Medicines Management Services ANXIETY DISORDERS This guideline covers a range of anxiety disorders, including generalised anxiety disorder, social
Clinical Guideline / Formulary Document Pharmacy Department Medicines Management Services ANXIETY DISORDERS This guideline covers a range of anxiety disorders, including generalised anxiety disorder, social
For: NEON Primary Healthcare Providers By: Michelle Romero, DO June 2013
 For: NEON Primary Healthcare Providers By: Michelle Romero, DO June 2013 This power point is only a guideline for recommendations in the treatment of psychiatric disorders. This is not comprehensive. Please
For: NEON Primary Healthcare Providers By: Michelle Romero, DO June 2013 This power point is only a guideline for recommendations in the treatment of psychiatric disorders. This is not comprehensive. Please
Depression & Anxiety in Adolescents
 Depression & Anxiety in Adolescents Objectives 1) Review diagnosis of anxiety and depression in adolescents 2) Provide overview of evidence-based treatment options 3) Increase provider comfort level with
Depression & Anxiety in Adolescents Objectives 1) Review diagnosis of anxiety and depression in adolescents 2) Provide overview of evidence-based treatment options 3) Increase provider comfort level with
Index. Note: Page numbers of article titles are in boldface type. A ADHD. See Attention-deficit/hyperactivity disorder (ADHD) b-adrenergic blockers
 b-adrenergic blockers") Note: Page numbers of article titles are in boldface type. A ADHD. See Attention-deficit/hyperactivity disorder (ADHD) a-adrenergic blockers for PTSD, 798 b-adrenergic blockers for PTSD, 798 Adrenergic
Note: Page numbers of article titles are in boldface type. A ADHD. See Attention-deficit/hyperactivity disorder (ADHD) a-adrenergic blockers for PTSD, 798 b-adrenergic blockers for PTSD, 798 Adrenergic
A Basic Approach to Mood and Anxiety Disorders in the Elderly
 A Basic Approach to Mood and Anxiety Disorders in the Elderly November 1 2013 Sarah Colman MD FRCPC Clinical Fellow, Geriatric Psychiatry Mount Sinai Hospital, University of Toronto Disclosure No conflict
A Basic Approach to Mood and Anxiety Disorders in the Elderly November 1 2013 Sarah Colman MD FRCPC Clinical Fellow, Geriatric Psychiatry Mount Sinai Hospital, University of Toronto Disclosure No conflict
Depression in adults: treatment and management
 1 2 3 4 Depression in adults: treatment and management 5 6 7 8 Appendix V3: recommendations that have been deleted of changed from 2009 guideline Depression in adults: Appendix V3 1 of 22 1 Recommendations
1 2 3 4 Depression in adults: treatment and management 5 6 7 8 Appendix V3: recommendations that have been deleted of changed from 2009 guideline Depression in adults: Appendix V3 1 of 22 1 Recommendations
Medication management of anxiety & depression. Dr Katie Simpson GP Mental health lead East Berks CCG
 Medication management of anxiety & depression Dr Katie impson GP Mental health lead East Berks CCG NICE guidelines for Anxiety tepped Care RIs and NRIs in Anxiety disorders RI ertraline Citalopram Fluoxetine
Medication management of anxiety & depression Dr Katie impson GP Mental health lead East Berks CCG NICE guidelines for Anxiety tepped Care RIs and NRIs in Anxiety disorders RI ertraline Citalopram Fluoxetine
Depression: selective serotonin reuptake inhibitors
 Depression: selective serotonin reuptake inhibitors Selective serotonin reuptake inhibitors (SSRIs) are considered first-line treatment for the majority of patients with depression. citalopram and fluoxetine
Depression: selective serotonin reuptake inhibitors Selective serotonin reuptake inhibitors (SSRIs) are considered first-line treatment for the majority of patients with depression. citalopram and fluoxetine
Mental Health Pathway
 Mental Health Pathway Triggers for Mental Health Pathway Information for professionals Consider mainstream Mental Health Services (Green light Toolkit) Clinical Interface Protocol Clinical Assessment Information
Mental Health Pathway Triggers for Mental Health Pathway Information for professionals Consider mainstream Mental Health Services (Green light Toolkit) Clinical Interface Protocol Clinical Assessment Information
Treating Anxiety Disorders. Adil Virani, BSc (Pharm), Pharm D, FCSHP
, Pharm D, FCSHP") Treating Anxiety Disorders Adil Virani, BSc (Pharm), Pharm D, FCSHP Outline! Michelle s Case! Types of anxiety disorders! Goals of therapy! Treatment options and guidelines! Pharmacological options! Benzodiazepines
Treating Anxiety Disorders Adil Virani, BSc (Pharm), Pharm D, FCSHP Outline! Michelle s Case! Types of anxiety disorders! Goals of therapy! Treatment options and guidelines! Pharmacological options! Benzodiazepines
Medication for Anxiety and Depression. PJ Cowen Department of Psychiatry, University of Oxford
 Medication for Anxiety and Depression PJ Cowen Department of Psychiatry, University of Oxford Topics Medication for anxiety disorders Medication for first line depression treatment Medication for resistant
Medication for Anxiety and Depression PJ Cowen Department of Psychiatry, University of Oxford Topics Medication for anxiety disorders Medication for first line depression treatment Medication for resistant
Major Depressive Disorder (MDD) in Children under Age 6
 in Children under Age 6") in Children under Age 6 Level 0 Comprehensive assessment. Refer to Principles of Practice on page 6. Level 1 Psychotherapeutic intervention (e.g., dyadic therapy) for 6 to 9 months; assessment of parent/guardian
in Children under Age 6 Level 0 Comprehensive assessment. Refer to Principles of Practice on page 6. Level 1 Psychotherapeutic intervention (e.g., dyadic therapy) for 6 to 9 months; assessment of parent/guardian
Guidance on the use of Antidepressants for the Treatment of Unipolar Depression and Anxiety Spectrum Disorders in adults (Version 4.
 Guidance on the use of Antidepressants for the Treatment of Unipolar Depression and Anxiety Spectrum Disorders in adults (Version 4.1 December 2018) Date of Preparation: January 2018 (with addition of
Guidance on the use of Antidepressants for the Treatment of Unipolar Depression and Anxiety Spectrum Disorders in adults (Version 4.1 December 2018) Date of Preparation: January 2018 (with addition of
Clinical Guideline / Formulary Document Pharmacy Department Medicines Management Services
 Clinical Guideline / Formulary Document Pharmacy Department Medicines Management Services DEPRESSION Pharmacological Treatment of Depression NICE guidelines suggest the following stepped care model also
Clinical Guideline / Formulary Document Pharmacy Department Medicines Management Services DEPRESSION Pharmacological Treatment of Depression NICE guidelines suggest the following stepped care model also
Diagnosis & Management of Major Depression: A Review of What s Old and New. Cerrone Cohen, MD
 Diagnosis & Management of Major Depression: A Review of What s Old and New Cerrone Cohen, MD Why You re Treating So Much Mental Health 59% of Psychiatrists Are Over the Age of 55 AAMC 2014 Physician specialty
Diagnosis & Management of Major Depression: A Review of What s Old and New Cerrone Cohen, MD Why You re Treating So Much Mental Health 59% of Psychiatrists Are Over the Age of 55 AAMC 2014 Physician specialty
Medication Management. Dr Ajith Weeraman MBBS, MD (Psychiatry), FRANZCP Consultant Psychiatrist Epworth Clinic Camberwell 14 th March 2015
, FRANZCP Consultant Psychiatrist Epworth Clinic Camberwell 14 th March 2015") Medication Management Dr Ajith Weeraman MBBS, MD (Psychiatry), FRANZCP Consultant Psychiatrist Epworth Clinic Camberwell 14 th March 2015 1 Medication Management Objectives: 1. Principles of psycho-pharmacology
Medication Management Dr Ajith Weeraman MBBS, MD (Psychiatry), FRANZCP Consultant Psychiatrist Epworth Clinic Camberwell 14 th March 2015 1 Medication Management Objectives: 1. Principles of psycho-pharmacology
Depression in Late Life
 Depression in Late Life Robert Madan MD FRCPC Geriatric Psychiatrist Key Learnings Robert Madan MD FRCPC Key Learnings By the end of the session, participants will be able to List the symptoms of depression
Depression in Late Life Robert Madan MD FRCPC Geriatric Psychiatrist Key Learnings Robert Madan MD FRCPC Key Learnings By the end of the session, participants will be able to List the symptoms of depression
Introduction to Drug Treatment
 Introduction to Drug Treatment LPT Gondar Mental Health Group www.le.ac.uk Introduction to Psychiatric Drugs Drugs and Neurotransmitters 5 Classes of Psychotropic medications Mechanism of action Clinical
Introduction to Drug Treatment LPT Gondar Mental Health Group www.le.ac.uk Introduction to Psychiatric Drugs Drugs and Neurotransmitters 5 Classes of Psychotropic medications Mechanism of action Clinical
How to Manage Anxiety
 How to Manage Anxiety Dr Tony Fernando Psychological Medicine University of Auckland Auckland District Health Board www.insomniaspecialist.co.nz www.calm.auckland.ac.nz Topics How to diagnose How to manage
How to Manage Anxiety Dr Tony Fernando Psychological Medicine University of Auckland Auckland District Health Board www.insomniaspecialist.co.nz www.calm.auckland.ac.nz Topics How to diagnose How to manage
Disclosures. Overview of Workshop. Objectives. Medical Care of Vulnerable and Underserved Populations: Advanced Cases in Anxiety and Depression
 Medical Care of Vulnerable and Underserved Populations: Advanced Cases in Anxiety and Depression Disclosures The speakers have no disclosures. Lisa Ochoa-Frongia, MD Christina Mangurian, MD, MAS L. Elizabeth
Medical Care of Vulnerable and Underserved Populations: Advanced Cases in Anxiety and Depression Disclosures The speakers have no disclosures. Lisa Ochoa-Frongia, MD Christina Mangurian, MD, MAS L. Elizabeth
Psychopharmacology. Psychopharmacology. Hamish McAllister-Williams Reader in Clinical. Department of Psychiatry, RVI
 Regional Affective Disorders Service Psychopharmacology Northumberland, Tyne and Wear NHS Trust Hamish McAllister-Williams Reader in Clinical Psychopharmacology Department of Psychiatry, RVI Intro NOT
Regional Affective Disorders Service Psychopharmacology Northumberland, Tyne and Wear NHS Trust Hamish McAllister-Williams Reader in Clinical Psychopharmacology Department of Psychiatry, RVI Intro NOT
Appendix 4B - Guidance for the use of Pharmacological Agents for the Treatment of Depression in Adults (18 years and over)
") Appendix 4B - Guidance for the use of Pharmacological Agents for the Treatment of Depression in Adults (18 years and over) Introduction / Background Treatment comes after diagnosis Diagnosis is based on
Appendix 4B - Guidance for the use of Pharmacological Agents for the Treatment of Depression in Adults (18 years and over) Introduction / Background Treatment comes after diagnosis Diagnosis is based on
Antidepressant Treatment of Depression
 Antidepressant Treatment of Depression PLEASE REFER TO INTEGRATED CARE PATHWAY FOR INFORMATION RELATING TO THE OVERALL MANAGEMENT OF DEPRESSION SSRI s are first choice agents because they are as effective
Antidepressant Treatment of Depression PLEASE REFER TO INTEGRATED CARE PATHWAY FOR INFORMATION RELATING TO THE OVERALL MANAGEMENT OF DEPRESSION SSRI s are first choice agents because they are as effective
Antidepressant Selection in Primary Care
 Antidepressant Selection in Primary Care R E B E C C A D. L E W I S, D O O O A S U M M E R C M E B R A N S O N, M O 1 5 A U G U S T 2 0 1 5 Objectives Understand the epidemiology of depression. Recognize
Antidepressant Selection in Primary Care R E B E C C A D. L E W I S, D O O O A S U M M E R C M E B R A N S O N, M O 1 5 A U G U S T 2 0 1 5 Objectives Understand the epidemiology of depression. Recognize
Recommendation 1: Diagnosis of Generalized Anxiety Disorder (IΙΙ-2)
") Final GAD RECOMMENDATIONS & EVIDENCE Recommendation 1: Diagnosis of Generalized Anxiety Disorder (IΙΙ-2) It is recommended for general practitioners and other Primary Health Care doctors to consider the
Final GAD RECOMMENDATIONS & EVIDENCE Recommendation 1: Diagnosis of Generalized Anxiety Disorder (IΙΙ-2) It is recommended for general practitioners and other Primary Health Care doctors to consider the
Presentation is Being Recorded
 Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
Children s Hospital Of Wisconsin
 Children s Hospital Of Wisconsin Co-Management Guidelines To support collaborative care, we have developed guidelines for our community providers to utilize when referring to, and managing patients with,
Children s Hospital Of Wisconsin Co-Management Guidelines To support collaborative care, we have developed guidelines for our community providers to utilize when referring to, and managing patients with,
9/20/2011. Integrated Care for Depression & Anxiety: Psychotropic Medication Management for PCPs. Presentation is Being Recorded
 Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
Anti-Depressant Medications
 Anti-Depressant Medications A Introduction: This topic may be a little bit underestimated here in Jordan, while in western countries it has more significance. The function of anti-depressants is to change
Anti-Depressant Medications A Introduction: This topic may be a little bit underestimated here in Jordan, while in western countries it has more significance. The function of anti-depressants is to change
This initial discovery led to the creation of two classes of first generation antidepressants:
 Antidepressants - TCAs, MAOIs, SSRIs & SNRIs First generation antidepressants TCAs and MAOIs The discovery of antidepressants could be described as a lucky accident. During the 1950s, while carrying out
Antidepressants - TCAs, MAOIs, SSRIs & SNRIs First generation antidepressants TCAs and MAOIs The discovery of antidepressants could be described as a lucky accident. During the 1950s, while carrying out
Treatment Options for Bipolar Disorder Contents
 Keeping Your Balance Treatment Options for Bipolar Disorder Contents Medication Treatment for Bipolar Disorder 2 Page Medication Record 5 Psychosocial Treatments for Bipolar Disorder 6 Module Summary 8
Keeping Your Balance Treatment Options for Bipolar Disorder Contents Medication Treatment for Bipolar Disorder 2 Page Medication Record 5 Psychosocial Treatments for Bipolar Disorder 6 Module Summary 8
Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist
 and Glutamate (NMDA) Receptor Antagonist") Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist Medication Dosage Indication for Use Aricept (donepezil) Exelon (rivastigmine) 5mg 23mg* ODT 5mg Solution
Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist Medication Dosage Indication for Use Aricept (donepezil) Exelon (rivastigmine) 5mg 23mg* ODT 5mg Solution
Major Depressive Disorder (MDD) in Children under Age 6
 in Children under Age 6") in Children under Age 6 Level 0 Comprehensive assessment. Refer to Principles of Practice on page 5. Level 1 Psychotherapeutic intervention (e.g., dyadic therapy) for 6 to 9 months; assessment of parent/guardian
in Children under Age 6 Level 0 Comprehensive assessment. Refer to Principles of Practice on page 5. Level 1 Psychotherapeutic intervention (e.g., dyadic therapy) for 6 to 9 months; assessment of parent/guardian
Overview. Part II: Part I: Screening for Depression and Anxiety Risk Assessment Diagnosis of Depressive Disorders
 1 Learning Objectives 1. Providers will become familiar with methods of screening for depression and anxiety. 2. Providers will become more comfortable with diagnosis and management of these common pediatric
1 Learning Objectives 1. Providers will become familiar with methods of screening for depression and anxiety. 2. Providers will become more comfortable with diagnosis and management of these common pediatric
Pharmacological treatment of anxiety disorders where is
 Pharmacological treatment of anxiety disorders where is the room for improvement? David S Baldwin, Professor of Psychiatry BAP Masterclass, 15 th April 2011 dsb1@soton.ac.uk Declaration of interests (last
Pharmacological treatment of anxiety disorders where is the room for improvement? David S Baldwin, Professor of Psychiatry BAP Masterclass, 15 th April 2011 dsb1@soton.ac.uk Declaration of interests (last
DIAGNOSTIC CRITERIA (ICD 10)
") DEPRESSION Depression is a major public health problem around the world Affects 1:5 older people living in the community Affects 2:5 older people living in care homes Various treatment options available,
DEPRESSION Depression is a major public health problem around the world Affects 1:5 older people living in the community Affects 2:5 older people living in care homes Various treatment options available,
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 Step 3: GAD with marked functional impairment or that has not improved after step 2 interventionsentions bring together everything NICE says on a topic in an interactive flowchart. are interactive and
Step 3: GAD with marked functional impairment or that has not improved after step 2 interventionsentions bring together everything NICE says on a topic in an interactive flowchart. are interactive and
Anxiety Disorders.
 Anxiety Disorders Shamim Nejad, MD Medical Director, Division of Psychosocial Oncology Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@swedish.org Epidemiology Lifetime
Anxiety Disorders Shamim Nejad, MD Medical Director, Division of Psychosocial Oncology Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@swedish.org Epidemiology Lifetime
Some newer, investigational approaches to treating refractory major depression are being used.
 CREATED EXCLUSIVELY FOR FINANCIAL PROFESSIONALS Rx FOR SUCCESS Depression and Anxiety Disorders Mood and anxiety disorders are common, and the mortality risk is due primarily to suicide, cardiovascular
CREATED EXCLUSIVELY FOR FINANCIAL PROFESSIONALS Rx FOR SUCCESS Depression and Anxiety Disorders Mood and anxiety disorders are common, and the mortality risk is due primarily to suicide, cardiovascular
Antidepressant Selection in Primary Care
 Antidepressant Selection in Primary Care Rebecca D. Lewis, DO OOA Summer CME Oklahoma City, OK 6 August 2017 Objectives Understand the epidemiology of depression. Recognize factors to help choose antidepressants.
Antidepressant Selection in Primary Care Rebecca D. Lewis, DO OOA Summer CME Oklahoma City, OK 6 August 2017 Objectives Understand the epidemiology of depression. Recognize factors to help choose antidepressants.
Depression Workshop 26 January 2007
 Depression Workshop 26 January 2007 Leslie G Walker Professor of Cancer Rehabilitation Donald M Sharp Senior Lecturer in Behavioural Oncology Mary B Walker Senior Clinical and Research Nurse Specialist
Depression Workshop 26 January 2007 Leslie G Walker Professor of Cancer Rehabilitation Donald M Sharp Senior Lecturer in Behavioural Oncology Mary B Walker Senior Clinical and Research Nurse Specialist
Management Of Depression And Anxiety
 Management Of Depression And Anxiety CME Financial Disclosure Statement I, or an immediate family member including spouse/partner, have at present and/or have had within the last 12 months, or anticipate
Management Of Depression And Anxiety CME Financial Disclosure Statement I, or an immediate family member including spouse/partner, have at present and/or have had within the last 12 months, or anticipate
CHILD & ADOLESCENT PSYCHIATRY ALERTS, VOLUME XIV, 2012 INDEX
 A Adderall Counterfeit, 31 addiction, internet CBT, 55 ADHD Adjunctive Guanfacine, 11 Counterfeit Adderall, 31 Developmental Trajectory and Risk Factors, 5 Dopamine Transporter Alterations, 14 Extended-Release
A Adderall Counterfeit, 31 addiction, internet CBT, 55 ADHD Adjunctive Guanfacine, 11 Counterfeit Adderall, 31 Developmental Trajectory and Risk Factors, 5 Dopamine Transporter Alterations, 14 Extended-Release
Clinical guideline Published: 28 October 2009 nice.org.uk/guidance/cg90
 Depression in adults: recognition and management Clinical guideline Published: 28 October 2009 nice.org.uk/guidance/cg90 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Depression in adults: recognition and management Clinical guideline Published: 28 October 2009 nice.org.uk/guidance/cg90 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
How to treat depression with medication: Some rules of thumb
 How to treat depression with medication: Some rules of thumb R. Hamish McAllister-Williams, MD, PhD, FRCPsych Reader in Clinical Psychopharmacology Newcastle University Hon. Consultant Psychiatrist Regional
How to treat depression with medication: Some rules of thumb R. Hamish McAllister-Williams, MD, PhD, FRCPsych Reader in Clinical Psychopharmacology Newcastle University Hon. Consultant Psychiatrist Regional
Guilt Suicidality. Depression Co-Occurs with Medical Illness The rate of major depression among those with medical illness is significant.
 1-800-PSYCH If you are obsessive-compulsive, dial 1 repeatedly If you are paranoid-delusional, dial 2 and wait, your call is being traced If you are schizophrenic, a little voice will tell you what number
1-800-PSYCH If you are obsessive-compulsive, dial 1 repeatedly If you are paranoid-delusional, dial 2 and wait, your call is being traced If you are schizophrenic, a little voice will tell you what number
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Neuropathic pain pharmacological management: the pharmacological management of neuropathic pain in adults in non-specialist
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Neuropathic pain pharmacological management: the pharmacological management of neuropathic pain in adults in non-specialist
Partners in Care Quick Reference Cards
 Partners in Care Quick Reference Cards Supported by the Agency for Healthcare Research and Quality MR-1198/8-AHRQ R This project was funded by the Agency for Healthcare Research and Quality (AHRQ), formerly
Partners in Care Quick Reference Cards Supported by the Agency for Healthcare Research and Quality MR-1198/8-AHRQ R This project was funded by the Agency for Healthcare Research and Quality (AHRQ), formerly
Clinical Significance of Anxiety in Depressed Patients Selecting an Antidepressant
 The Clinical Significance of Anxiety Disorders and the DSM-5 Anxious Distress Specifier in Depressed Patients Clinical Significance of Anxiety in Depressed Patients Selecting an Antidepressant Rhode Island
The Clinical Significance of Anxiety Disorders and the DSM-5 Anxious Distress Specifier in Depressed Patients Clinical Significance of Anxiety in Depressed Patients Selecting an Antidepressant Rhode Island
Psychiatry in Primary Care: What is the Role of Pharmacist?
 Psychiatry in Primary Care: What is the Role of Pharmacist? Benjamin Chavez, PharmD, BCPP, BCACP Clinical Associate Professor Director of Behavioral Health Pharmacy Services January 12, 2019 Disclosure
Psychiatry in Primary Care: What is the Role of Pharmacist? Benjamin Chavez, PharmD, BCPP, BCACP Clinical Associate Professor Director of Behavioral Health Pharmacy Services January 12, 2019 Disclosure
BRIEF SUMMARY CONTENT
 Page 1 of 17 Brief Summary GUIDELINE TITLE Depression. The treatment and management of depression in adults. BIBLIOGRAPHIC SOURCE(S) National Collaborating Centre for Mental Health. Depression. The treatment
Page 1 of 17 Brief Summary GUIDELINE TITLE Depression. The treatment and management of depression in adults. BIBLIOGRAPHIC SOURCE(S) National Collaborating Centre for Mental Health. Depression. The treatment
Optimal Use of Antidepressants: Focusing on SNRI, NDRI and SSRE
 Optimal Use of Antidepressants: Focusing on SNRI, NDRI and SSRE Chan-Hyung Kim, MD Severance Mental Health Hospital Institute of Behavioral Science in Medicine Diagnostic Criteria Pyramid Etiologic Pathophysiologic
Optimal Use of Antidepressants: Focusing on SNRI, NDRI and SSRE Chan-Hyung Kim, MD Severance Mental Health Hospital Institute of Behavioral Science in Medicine Diagnostic Criteria Pyramid Etiologic Pathophysiologic
FROM MEDICATION TO MINDFULNESS: NEW INSIGHTS INTO THE WORLD OF ANXIETY
 13 th Pearl Leibovitch Clinical Day November 18th, 2014 Mounir H. Samy, MD, FRCP(C) Associate Professor of Psychiatry McGill University (ret.) FROM MEDICATION TO MINDFULNESS: NEW INSIGHTS INTO THE WORLD
13 th Pearl Leibovitch Clinical Day November 18th, 2014 Mounir H. Samy, MD, FRCP(C) Associate Professor of Psychiatry McGill University (ret.) FROM MEDICATION TO MINDFULNESS: NEW INSIGHTS INTO THE WORLD
Start Low, Go Slow but Treat to Target
 Start Low, Go Slow but Treat to Target Pharmacotherapy for Depression, Anxiety and At-Risk Alcohol Use in Late Life September 29, 2014 Audio and Control Panel instruction On the phone? Raise your hand
Start Low, Go Slow but Treat to Target Pharmacotherapy for Depression, Anxiety and At-Risk Alcohol Use in Late Life September 29, 2014 Audio and Control Panel instruction On the phone? Raise your hand
Depression: management of depression in primary and secondary care
 Issue date: December 2004, with amendments April 2007 Quick reference guide (amended) Depression: management of depression in primary and secondary care Amendment of recommendations concerning venlafaxine:
Issue date: December 2004, with amendments April 2007 Quick reference guide (amended) Depression: management of depression in primary and secondary care Amendment of recommendations concerning venlafaxine:
A guide to reducing or stopping mental health medication. Notes for prescribers
 A guide to reducing or stopping mental health medication Notes for prescribers 1 Prescribers notes for reducing or stopping mental health medication These notes are written to augment the information for
A guide to reducing or stopping mental health medication Notes for prescribers 1 Prescribers notes for reducing or stopping mental health medication These notes are written to augment the information for
Clinical guideline Published: 28 October 2009 nice.org.uk/guidance/cg91
 Depression in adults with a chronic physical health problem: recognition and management Clinical guideline Published: 28 October 2009 nice.org.uk/guidance/cg91 NICE 2018. All rights reserved. Subject to
Depression in adults with a chronic physical health problem: recognition and management Clinical guideline Published: 28 October 2009 nice.org.uk/guidance/cg91 NICE 2018. All rights reserved. Subject to
AN OVERVIEW OF ANXIETY
 AN OVERVIEW OF ANXIETY Fear and anxiety are a normal part of life. Normal anxiety keeps us alert. Intervention is required when fear and anxiety becomes overwhelming intruding on a persons quality of life.
AN OVERVIEW OF ANXIETY Fear and anxiety are a normal part of life. Normal anxiety keeps us alert. Intervention is required when fear and anxiety becomes overwhelming intruding on a persons quality of life.
Clinical guideline Published: 28 October 2009 nice.org.uk/guidance/cg90
 Depression in adults: recognition and management Clinical guideline Published: 28 October 2009 nice.org.uk/guidance/cg90 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Depression in adults: recognition and management Clinical guideline Published: 28 October 2009 nice.org.uk/guidance/cg90 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Pharmaceutical Interventions. Collaborative Model of Mental Health Care for Older Iowans Des Moines May 18, 2007
 Pharmaceutical Interventions Collaborative Model of Mental Health Care for Older Iowans Des Moines May 18, 2007 Outline Overview Overview of initial workup and decisions in elderly depressed individual
Pharmaceutical Interventions Collaborative Model of Mental Health Care for Older Iowans Des Moines May 18, 2007 Outline Overview Overview of initial workup and decisions in elderly depressed individual
Short Clinical Guidelines: General Anxiety Disorder (GAD)
") Definition is one of the most prevalent psychiatric disorders seen in the primary care office and is characterized by excessive anxiety and worry about a number of events that cause clinically significant
Definition is one of the most prevalent psychiatric disorders seen in the primary care office and is characterized by excessive anxiety and worry about a number of events that cause clinically significant
Depression in Older Adults. Paul Boulware, MD Arizona Neurological Institute April 22, 2012
 Depression in Older Adults Paul Boulware, MD Arizona Neurological Institute April 22, 2012 What is it? Major depressive disorder is a syndrome, a collection of symptoms Presentation is variable among individuals
Depression in Older Adults Paul Boulware, MD Arizona Neurological Institute April 22, 2012 What is it? Major depressive disorder is a syndrome, a collection of symptoms Presentation is variable among individuals
Mixing and Matching: Layering Medications as Family Physicians
 Mixing and Matching: Layering Medications as Family Physicians Family Medicine Forum Vancouver, B.C. November 9-12, 2016. Jon Davine, CCFP, FRCP(C) McMaster University Objectives Discuss different examples
Mixing and Matching: Layering Medications as Family Physicians Family Medicine Forum Vancouver, B.C. November 9-12, 2016. Jon Davine, CCFP, FRCP(C) McMaster University Objectives Discuss different examples
Psychotropic Medication Use in Dementia
 Psychotropic Medication Use in Dementia Marie A DeWitt, MD Diplomate of the American Board of Psychiatry and Neurology, Specialization in Psychiatry & Subspecialization in Geriatric Psychiatry Staff Physician,
Psychotropic Medication Use in Dementia Marie A DeWitt, MD Diplomate of the American Board of Psychiatry and Neurology, Specialization in Psychiatry & Subspecialization in Geriatric Psychiatry Staff Physician,
Intro to Concurrent Disorders
 CSAM-SCAM Fundamentals Intro to Concurrent Disorders Presentation provided by Jennifer Brasch, MD, FRCPC Psychiatrist, Concurrent Disorders Program, St. Joseph s Healthcare There are all kinds of addicts,
CSAM-SCAM Fundamentals Intro to Concurrent Disorders Presentation provided by Jennifer Brasch, MD, FRCPC Psychiatrist, Concurrent Disorders Program, St. Joseph s Healthcare There are all kinds of addicts,
Common Antidepressant Medications for Adults
 (and Citalopram (Celexa) Escitalopram (Lexapro) Fluoxetine (Prozac) Fluoxetine Weekly (Prozac Weekly) 20 in AM w/ food (10 mg in elderly or those w/ panic disorder) 20 40 40 (If age >60yo, max 20) 10 10
(and Citalopram (Celexa) Escitalopram (Lexapro) Fluoxetine (Prozac) Fluoxetine Weekly (Prozac Weekly) 20 in AM w/ food (10 mg in elderly or those w/ panic disorder) 20 40 40 (If age >60yo, max 20) 10 10
Antidepressants Choosing the Right One
 Antidepressants Choosing the Right One Dr Lim Boon Leng Consultant Psychiatrist Dr BL Lim Centre For Psychological Wellness #09-09, Gleneagles Medical Centre, 6 Napier Rd, S258499 www.psywellness.com.sg
Antidepressants Choosing the Right One Dr Lim Boon Leng Consultant Psychiatrist Dr BL Lim Centre For Psychological Wellness #09-09, Gleneagles Medical Centre, 6 Napier Rd, S258499 www.psywellness.com.sg
 DEPRESSION Depression is a major public health problem around the world Affects 1:5 older people living in the community Affects 2:5 older people living in care homes Various treatment options available,
DEPRESSION Depression is a major public health problem around the world Affects 1:5 older people living in the community Affects 2:5 older people living in care homes Various treatment options available,
Psychiatry curbside: Answers to a primary care doctor s top mental health questions
 Psychiatry curbside: Answers to a primary care doctor s top mental health questions April 27, 2018 Laurel Ralston, DO Psychiatrist, Taussig Cancer Institute Objectives Review current diagnostic and prescribing
Psychiatry curbside: Answers to a primary care doctor s top mental health questions April 27, 2018 Laurel Ralston, DO Psychiatrist, Taussig Cancer Institute Objectives Review current diagnostic and prescribing
Prepared by: Elizabeth Vicens-Fernandez, LMHC, Ph.D.
 Prepared by: Elizabeth Vicens-Fernandez, LMHC, Ph.D. Sources: National Institute of Mental Health (NIMH), the National Alliance on Mental Illness (NAMI), and from the American Psychological Association
Prepared by: Elizabeth Vicens-Fernandez, LMHC, Ph.D. Sources: National Institute of Mental Health (NIMH), the National Alliance on Mental Illness (NAMI), and from the American Psychological Association
Anxiolytics. What s new? Lindsey Sinclair
 Anxiolytics Lindsey Sinclair David Nutt What s new? pregabalin has gained a licence for the treatment of generalized anxiety disorder new data support the use of escitalopram in several anxiety disorders
Anxiolytics Lindsey Sinclair David Nutt What s new? pregabalin has gained a licence for the treatment of generalized anxiety disorder new data support the use of escitalopram in several anxiety disorders
Quick Guide to Common Antidepressants-Adults
 Quick Guide to Common Antidepressants-Adults Medication Therapeutic Range (mg/day) Initial Suggested Serotonin Reuptake Inhibitors (SSRIs) All available as generic FLUOXETINE (Prozac) CITALOPRAM (Celexa
Quick Guide to Common Antidepressants-Adults Medication Therapeutic Range (mg/day) Initial Suggested Serotonin Reuptake Inhibitors (SSRIs) All available as generic FLUOXETINE (Prozac) CITALOPRAM (Celexa
GREATER MANCHESTER INTERFACE PRESCRIBING GROUP
 GREATER MANCHESTER INTERFACE PRESCRIBING GROUP On behalf of the GREATER MANCHESTER MEDICINES MANAGEMENT GROUP SHARED CARE GUIDELINE FOR THE PRESCRIBING OF SELECTIVE SEROTONIN REUPTAKE INHIBITORS (SSRIs)
GREATER MANCHESTER INTERFACE PRESCRIBING GROUP On behalf of the GREATER MANCHESTER MEDICINES MANAGEMENT GROUP SHARED CARE GUIDELINE FOR THE PRESCRIBING OF SELECTIVE SEROTONIN REUPTAKE INHIBITORS (SSRIs)
Objectives. Objectives. A practice review. 02-Nov-16 MAJOR DEPRESSIVE DISORDER: NEW DEVELOPMENTS AND PRACTICAL IMPLICATIONS
 MAJOR DEPRESSIVE DISORDER: NEW DEVELOPMENTS AND PRACTICAL IMPLICATIONS Jon-Paul Khoo What is treatment resistance really? Database review 328 consecutive non-remitted MDD patients referred for private
MAJOR DEPRESSIVE DISORDER: NEW DEVELOPMENTS AND PRACTICAL IMPLICATIONS Jon-Paul Khoo What is treatment resistance really? Database review 328 consecutive non-remitted MDD patients referred for private
Depression major depressive disorder. Some terms: Major Depressive Disorder: Major Depressive Disorder:
 Depression major depressive disorder Oldest recognized disorder: melancholia It is a positive and active anguish, a sort of psychical neuralgia wholly unknown to normal life. - William James "I am now
Depression major depressive disorder Oldest recognized disorder: melancholia It is a positive and active anguish, a sort of psychical neuralgia wholly unknown to normal life. - William James "I am now
Adult Depression - Clinical Practice Guideline
 1 Adult Depression - Clinical Practice Guideline 05/2018 Diagnosis and Screening Diagnostic criteria o Please refer to Attachment A Screening o The United States Preventative Services Task Force (USPSTF)
1 Adult Depression - Clinical Practice Guideline 05/2018 Diagnosis and Screening Diagnostic criteria o Please refer to Attachment A Screening o The United States Preventative Services Task Force (USPSTF)
VA/DOD CLINICAL PRACTICE GUIDELINE
 VA/DOD CLIICAL PRACTICE GUIDELIE Management of Major Depressive Disorder (MDD) KE ELEMETS OF THE MDD GUIDELIE Screen annually for Depression (PHQ-2) Assess for Suicide Risk Obtain Standardized Symptom
VA/DOD CLIICAL PRACTICE GUIDELIE Management of Major Depressive Disorder (MDD) KE ELEMETS OF THE MDD GUIDELIE Screen annually for Depression (PHQ-2) Assess for Suicide Risk Obtain Standardized Symptom
MOOD (AFFECTIVE) DISORDERS and ANXIETY DISORDERS
 DISORDERS and ANXIETY DISORDERS") MOOD (AFFECTIVE) DISORDERS and ANXIETY DISORDERS Shelley Klipp AS91 Spring 2010 TIP 42 Pages 226-231 and 369-379 DSM IV-TR APA 2000 Co-Occurring Substance Abuse and Mental Disorders by John Smith Types
MOOD (AFFECTIVE) DISORDERS and ANXIETY DISORDERS Shelley Klipp AS91 Spring 2010 TIP 42 Pages 226-231 and 369-379 DSM IV-TR APA 2000 Co-Occurring Substance Abuse and Mental Disorders by John Smith Types
Diabetes and Depression. Roshini Pinto-Powell, MD Stephen Noyes, LICSW, LADC William Gunn, PhD Beverly Bean, RN, C
 Diabetes and Depression Roshini Pinto-Powell, MD Stephen Noyes, LICSW, LADC William Gunn, PhD Beverly Bean, RN, C 2008 Learning Objectives State the risk factors for depression Identify the vulnerability
Diabetes and Depression Roshini Pinto-Powell, MD Stephen Noyes, LICSW, LADC William Gunn, PhD Beverly Bean, RN, C 2008 Learning Objectives State the risk factors for depression Identify the vulnerability
Effective Date: 5/28/2014 Version: 2.0 (Revised: 10/12/2015) Approval By: CCC Clinical Delivery Steering Planned Review Date: (04/47/2017)
 Approval By: CCC Clinical Delivery Steering Planned Review Date: (04/47/2017)") Protocol Title: Depression & Generalized Anxiety Disorder Effective Date: 5/28/2014 Version: 2.0 (Revised: 10/12/2015) Approval By: CCC Clinical Delivery Steering Planned Review Date: (04/47/2017) Group
Protocol Title: Depression & Generalized Anxiety Disorder Effective Date: 5/28/2014 Version: 2.0 (Revised: 10/12/2015) Approval By: CCC Clinical Delivery Steering Planned Review Date: (04/47/2017) Group
Affective Disorders.
 Affective Disorders http://www.bristol.ac.uk/medicalschool/hippocrates/psychethics/ Affective Disorders Depression Mania / Hypomania Bipolar mood disorder Recurrent depression Persistent mood disorders
Affective Disorders http://www.bristol.ac.uk/medicalschool/hippocrates/psychethics/ Affective Disorders Depression Mania / Hypomania Bipolar mood disorder Recurrent depression Persistent mood disorders
DEMENTIA AND MEDICATION
 DEMENTIA AND MEDICATION Dr. Siobhan Ni Bhriain, MRCP, MRCPsych. Clinical Director, Tallaght and SJH MHS, Consultant Old Age Psychiatrist, Chair, DSIDC Steering Committee. SUMMARY OF TODAY S TALK Dementia-definition,
DEMENTIA AND MEDICATION Dr. Siobhan Ni Bhriain, MRCP, MRCPsych. Clinical Director, Tallaght and SJH MHS, Consultant Old Age Psychiatrist, Chair, DSIDC Steering Committee. SUMMARY OF TODAY S TALK Dementia-definition,
Mood Disorders.
 Mood Disorders Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@swedish.org Disclosures Neither I nor my spouse/partner
Mood Disorders Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@swedish.org Disclosures Neither I nor my spouse/partner
Mentoring Session: Participant Cases
 Handout for the Neuroscience Education Institute (NEI) online activity: Mentoring Session: Participant Cases The Case: 55-year-old patient with depression and anxiety The Question: What to do when antidepressants
Handout for the Neuroscience Education Institute (NEI) online activity: Mentoring Session: Participant Cases The Case: 55-year-old patient with depression and anxiety The Question: What to do when antidepressants
POLYPHARMACY : FOR AND AGAINST NZMA GP CONFERENCE 2012 PSYCHOPHARMACOLOGY SERIES. Guna Kanniah Waikato Hospital
 POLYPHARMACY : FOR AND AGAINST NZMA GP CONFERENCE 212 PSYCHOPHARMACOLOGY SERIES Guna Kanniah Waikato Hospital POLYPHARMACY FIVE REASONS FOR POLYPHARMACY 1. To treat a concomitant disorder 2. To treat an
POLYPHARMACY : FOR AND AGAINST NZMA GP CONFERENCE 212 PSYCHOPHARMACOLOGY SERIES Guna Kanniah Waikato Hospital POLYPHARMACY FIVE REASONS FOR POLYPHARMACY 1. To treat a concomitant disorder 2. To treat an