성균관대학교삼성창원병원신경외과학교실신경종양학 김영준. KNS-MT-03 (April 15, 2015)
|
|
|
- Dwayne Waters
- 5 years ago
- Views:
Transcription

1 성균관대학교삼성창원병원신경외과학교실신경종양학 김영준
2 INTRODUCTIONS Low grade gliomas (LGG) - heterogeneous group of tumors with astrocytic, oligodendroglial, ependymal, or mixed cellular histology - In adults diffuse, infiltrating variety of tumors classified as WHO grade II lesions slow and continuous growth preceding anaplastic transformation 1) low grade astrocytomas : fibrillary, protoplasmic, and gemistocytic variants 2) oligodendrogliomas 3) mixed oligoastrocytomas - longstanding standard treatment includes 1) surgical resection of tumors when feasible, 2) followed by radiotherapy in incomplete resection, and 3) followed by chemotherapy at recurrence. but, historically considered to be poorly response to chemotherapy
3 Management of LGG patients has been a matter of debate 1. poorly studied natural course of LGG for a long time - the vast majority of investigators considered LGG as a stable and benign brain tumor and wait and see approach was advocated for many years - LGG usually affects young adults enjoying a normal life without or with only mild deficit on a standard neurologic examination - even AED can control the seizure in 80-90% of LGG patients 2. traditional thought that this infiltrative tumor cannot be removed without generating neurological and functional sequences - in particular when LGG is located in or close to eloquent area 3. deep argument that surgical removal had no impact on the natural history of LGG in the classic literatures - only biopsy for histopathological diagnosis - single follow-up or radiotherapy according to the morphological criteria - recently, prolonged OS from 61.1 to 90.5 month with GTR in meta-analysis
4 Recent conceptual advances of LGGs management : due to technical and knowledge advances in genetics, cognitive neurosciences, imaging, and treatment revolutionized of LGGs 1. Advanced knowledge of LGG biology 1) these aggressive tumors not are stable but grow continuously 2) these tumors migrate along the white matter pathways 3) inevitably progress to a higher grade of malignancy leading to neurologic disability and ultimately to death 2. Mechanism of neuroplasticity : cerebral processing of interaction between the disease and the host - development in brain-mapping techniques makes the benefit-risk ratio of surgery increase 3. Integration of onco-functional balances of surgical resection in an individualized multimodal therapeutic strategies : improving QOL
5 New insights into the natural course of LGGs 1. LGG is not stable disease at all - objective calculation of growth rate : linear increase of about 4mm/year (based on at least 2 MRIs spaced 3 months apart before any treatment) - the concept of PFS is meaningless in LGG before any treatment or incomplete surgical resection - inverse correlation between growth rate and survival in LGG 2. Migration of tumor cells along the white matter tracts - LGG is not a tumor mass but is an infiltrating chronic disease progressively invading CNS, especially the subcortical connectivity 3. LGG inescapably become malignant leading to death - OS of LGG patients by EORTC data (J Clin Oncol 2002;20: ) patients with favorable prognostic score : 7.7 years poor prognostic score : 3.2 years - LGG is not a benign tumor, but cancerous disease
6 Spontaneous worse prognostic factors of LGGs Pignatti F et al. J Clin Oncol 2002; 20: Soffieti R et al. Eur J Neurol 2010; 17: Clinical Age > 40 years Presence of neurological deficit Absence of seizure at onset KPS < 70 MMSE score < 25/30 Radiological Large tumors (>5~6cm) Tumors crossing midline Rapid growth rate Presence of contrast enhancement High CBV and high uptake of 11 C-MET Lipid & lactate on MRS STR >> GTR Molecular Absence of 1p19q codeletion Absence of IDH1 mutation Histological better outcome in oligodendroglioma than astrocytoma MIB index 8%
7 - Association between LGG tumor burden and patients outcome (JCO 2008;26:1338)
8 Individualized multi-stage therapeutic strategies in LGGs 1. Role of only one specific treatment without global view in the traditional literatures and studies 2. Switching goal to more holistic view - based on the anticipation of personalized and long-term multi-stage therapeutic approach - different points from traditional attitude 1) proposing earlier and maximal surgical resection 2) repeating treatment : 2 to 4 surgical resection spaced by several years 3) reversing the traditional order of therapies : neoadjuvant chemotherapy followed by surgery after tumor shrinkage (initially TMZ and followed by PCV) : no early radiotherapy 4) ultimate goal of increasing both OS and QOL
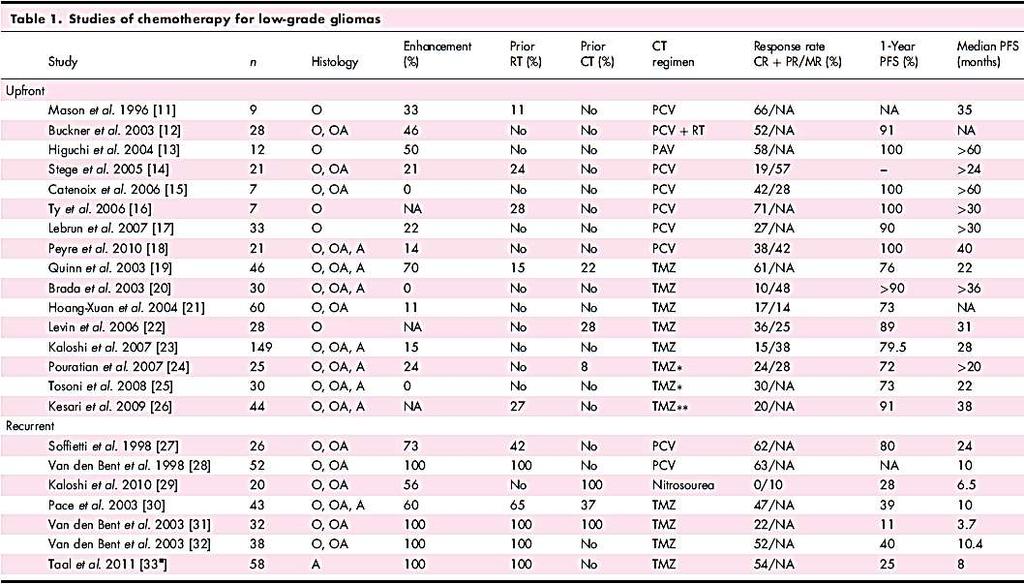
9 UPFRONT CHEMOTHERAPY The rationale for upfront chemotherapy of LGGs to radiotherapy : to avoid radiotherapy and thus to avoid potential radiation-induced cognitive effects, especially in large unresectable LGGs 1. a recent study clearly showed that LGGs patients who receive radiotherapy have a progressive cognitive decline (Lancet Neurol 2009; 8: ) : LGG patients who received radiotherapy showed a progressive decline in attentional functioning, even those who received fraction doses that are regarded as safe ( 2 Gy) 2. upfront chemotherapy as an effective treatment in LGGs through several phase II studies 1) a 50 75% response rate (including minor response) 2) a months median duration of response
10
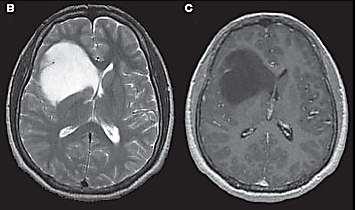
11 The response of upfront chemotherapy for LGGs : more frequent of minor response than partial response (Peyre et al. Neuro Oncol 2010; 12: / Richard et al. Ann Neurol 2007; 61: ) 1. slow, progressive and delayed response : median time to maximum response of approximately 12 months 2. response rate and duration of response 1) higher in patients with 1p/19q codeletion 2) also commonly observed in non-1p/19q codeleted LGG 3. commonly observed clinical improvement : even when there is no clear radiological response, more than half of the patients with epilepsy demonstrating a significant reduction of seizure frequency
MRI before TMZ (B)after 12 cycles of TMZ (C)after 24 cycles of")
12 - Slow and progressive response to TMZ of a patient with a low-grade oligodendroglioma of 1p19q codeletion (A)MRI before TMZ (B)after 12 cycles of TMZ (C)after 24 cycles of TMZ
 Oligodendrogliomas Astrocytoma baseline and post-tmz")
13 - Minimal response of TMZ for LGGs (Brada M, et al. Ann Oncol 2003; 14: ) Oligodendrogliomas Astrocytoma baseline and post-tmz cycle 12 baseline and post-tmz cycle 12

14 - Delayed response to TMZ in WHO grade II oligodendroglioma (FLAIR image) : TMZ as initial treatment for adults with low-grade oligodendrogliomas or oligoastrocytomas and correlation with chromosome 1p deletions (Hoang-Xuan K, et al. J Clin Oncol 2004; 22: ) (A) Before TMZ (B) after six cycles of TMZ (C) partial response after 17 cycles
15 ADJUVANT CHEMOTHERAPY The objective of adjuvant chemotherapy after radiotherapy : to increase survival in LGGs with poor prognostic factors 1. Phase III randomized trial of radiotherapy plus PCV chemotherapy for supratentorial adult LGG : RTOG 9802 (Shaw EG et al. JCO 2012; 30: ) P=0.020 P<0.001
16 2. Phase 2 study of TMZ-based concurrent chemoradiation therapy for high-risk LGG patients : RTOG 0424 (Fisher BJ et al, Int J Radiat Oncol Biol Phys 2015; 91: ) - High risk group 3 following factors 1)age 40 years 2)astrocytoma histology 3)bi-hemispherical tumor 4)preoperative tumor diameter 6 cm 5)preoperative neurological function status of >1-3-year OS : 73.1% 3-year PFS : 59.2% - longer OS compared to historical control
17 SALVAGE CHEMOTHERAPY Second-line chemotherapy with TMZ in recurrent oligodendroglioma after PCV chemotherapy: EORTC (den Bent MJ et al. Ann Oncol 2003; 14: ) - In a prospective non-randomized multicenter phase II trial patients were treated with TMZ 150 mg/m 2 on days 1 5 in cycles of 28 days for 12 cycles - 12 of 24 patients (50%) evaluable for response to first-line PCV chemotherapy had responded to TMZ 1) median TTP for responding patients : 8.0 months 2) 6-month PFS : 29% 12-month PFS : 11% - TMZ may be regarded as the preferred second-line treatment in OD after failure of PCV chemotherapy
18 Phase II study of first-line chemotherapy with TMZ in recurrent oligodendroglial tumors after surgery and radiotherapy : the EORTC Study (van den Bent MJ et al. J Clin Oncol 2003; 21: ) - In a prospective, nonrandomized, multicenter, phase II trial : patients who had a recurrence after prior surgery and radiotherapy : 200 mg/m 2 of TMZ on days 1 through 5 in 28-day cycles for 12 cycles - TMZ provides an excellent response rate with good tolerability in chemotherapy-naive patients with recurrent oligodendroglioma 1) a complete (n = 10) or partial response to TMZ in 20 (52.6%) of 38 patients 2) median TTP of 10.4 months for all patients 13.2 months for responding patients 3) 12-months PFS from the start of treatment : 40% of patients
19 CHEMOTHERAPY REGIMEN The most common chemotherapy regimen of TMZ and PCV : no direct comparison study evaluating the efficacy of PCV and TMZ in LGGs - TMZ versus PCV in recurrent high grade gliomas in phase III trials (Brada M, et al. J Clin Oncol 2010; 28: ) P=0.350 P=0.229

20 - upfront TMZ versus PCV followed by radiotherapy in anaplastic gliomas in phase III trials (Wick W et al. J Clin Oncol 2009; 27: )
21 - upfront PCV chemotherapy might be more effective in terms of PFS (but not of OS) than upfront TMZ in 1p/19q codeleted AO (Lassman AB et al. Neuro-Oncol 2011; 13: ) : International retrospective study of over 1000 adults with AO
22 Temozolomide in LGGs : currently the preferred drug to treat LGGs either upfront or at recurrence because usually better tolerated than PCV chemotherapy also easier to administrate 1. upfront TMZ does not alter the QOL of LGG patients but improves : no change in scores of Box plots at each TMZ chemotherapy cycle compared to baseline for five realms of QOL and Functional Assessment of Cancer Therapy General (FACT-G). (Liu R et al. Neuro-Oncol 2009; 11: 59 68)
23 2. upfront chemotherapy with a protracted TMZ schedule in LGG : 75mg/m 2 /day in 11-week cycles of 7 weeks on/4 weeks off or 75mg/m 2 /day in 4-week cycles 3 weeks on/1 week off 1) rationale for the protracted dose-dense TMZ regimens : it can theoretically overcome MGMT resistance 2) apparently similar to those obtained with the classical TMZ regimen (Pouratian N, et al. J Neurooncol 2007; 82: ) (Tosoni A, et al. J Neurooncol 2008; 89: ) (Kesari S, et al. Clin Cancer Res 2009; 15: ) 3) reversely, even the 3 weeks on/1 week off regimen appeared to be less effective than the classical regimen in a phase III trial in recurrent HGGs (Brada M, et al. J Clin Oncol 2010; 28: )
24 DURATION OF CHEMOTHERAPY TMZ treatment in LGG - a prolonged duration of treatment might be important to achieve a prolonged response Kaloshi G, et al. Neurology 2007; 68: Hoang-Xuan K, et al. J Clin Oncol 2004; 22: : to treat LGGs with TMZ rather than PCV chemotherapy (its cumulative toxicity) - discontinued TMZ in the absence of progression in a dynamic volumetric study (after a median period of 18 cycles) : occurrence of their regrowth within 1 year in 60% of LGGs Ricard D, et al. Ann Neurol 2007; 61: in continuously responding patients, many neurooncologists give TMZ for up to 24 or more cycles Viaccoz A et al. Curr Opin Oncol 2012; 24:

25 PCV chemotherapy for LGGs - commonly a prolonged (>2 years) and ongoing response after chemotherapy termination in dynamic volumetric study, despite the shorter duration of PCV chemotherapy than the duration of TMZ chemotherapy Peyre M, et al. Neuro Oncol 2010; 12:
 during PCV chemotherapy persistent decrease in the MTD (red curves)")
26 - Evolution of the mean tumor diameter (MTD) before, during, and after PCV chemotherapy Peyre M, et al. Neuro Oncol 2010; 12: decrease in the MTD (green curves) during PCV chemotherapy persistent decrease in the MTD (red curves) after PCV chemotherapy discontinuation
27 RADIOLOGICAL RESPONSE Limited role of McDonald criteria on estimating the chemotherapeutic response of LGGs without enhancement Complete response Partial response Stable disease Progressive disease McDonald criteria - Disappearance of all enhancing measurable and non-measurable disease (sustained for 4 weeks) - No new lesions / No corticosteroids - Clinically stable or Improved - 50% decrease of all measurable enhancing lesions (sustained for 4 weeks) - No new lesions - Clinically stable or Improved - Clinically stable - Does not qualify for CR, PR, or progression - 25% increase in enhancing lesions - Any new lesion Modified McDonald criteria - Disappearance of all index lesions (sustained for 4 weeks) / No new lesions - No worsening of all non-index lesions (sustained for 4 weeks), with no evidence of PD - Improved or stable neurological symptoms - 50% decrease (sum of lesion diameters) of all index lesions (sustained for 4 weeks) - No progression of non-index lesions nor new lesion - Improved or stable neurological symptoms - Improved or stable neurologic symptoms - Does not qualify for CR, PR, or progression - 25% increase in enhancing lesions - Unequivocal progression of existing non-index lesions Olivier L, et al. Curr Neurol Neurosci Rep 2013; 13: 347
28 Response assessment in neurooncology (the RANO group) Van den Bent M, et al. Lancet Oncol 2011; 12: Complete response Partial response Stable disease Progressive disease Imaging feature - disappearance of all enhancing disease (measurable and nonmeasurable) - sustained for at least 4 weeks - stable or improved non enhancing FLAIR/T2 lesions - no new lesions - 50% or more decrease of all measurable enhancing lesions - sustained for at least 4 weeks - no progression of nonmeasurable disease - stable or improved non enhancing FLAIR/T2 lesions - no new lesions - does not qualify for complete response, partial response or progression - stable non-enhancing FLAIR/T2 lesions - 25% of more increase in enhancing lesions despite stable or increasing steroid dose - increase (significant) in non-enhancing T2/FLAIR lesions, not attributable to other non-tumor causes - any new lesions Clinical feature - no corticosteroids (physiological replacement doses allowed) - clinically stable or improved - stable or reduced corticosteroids (compared to baseline) - clinically stable or improved - stable or reduced corticosteroids (compared to baseline) - clinically stable - clinical deterioration (not attributable to other non-tumor causes and not due to steroid decrease)
29 Limitation of RANO criteria on assessment of chemotherapeutic response at LGGs 1. LGGs are never stable after chemotherapy nor before chemotherapy 2. mean tumor diameter (MTD) in LGGs decreases to minimum before recurrence : LGGs typically present a progressive and ongoing decrease in MTD that can last many months after chemotherapy disruption 3. mean tumor diameter (MTD) in LGGs treated with upfront chemotherapy increase in almost all LGG patients : the rate of partial response of 5% at the end of PCV chemotherapy, but maximal response of 35% at 3.4 years after PCV discontinuation 4. similar response to first-line radiotherapy 5. to precisely assess the impact of chemotherapy, both the duration and the magnitude of the MTD decrease should be measured
30 PREDICT THE RESPONSE Candidate for favorable factors of response : this needs to be confirmed in prospective clinical trials 1. 1p/19q codeletion 2. possibly methylation of the MGMT promoter 3. the IDH1 mutation upfront chemotherapy with 1p19q codeletion in LGGs 1. TMZ with 1p19q codeletion (Kaloshi G, et al. Neurology 2007; 68: ) : total of 149 consecutive patients in the retrospective, single center observational study 1) higher response rate to chemotherapy : 72% vs 46% (p=0.02) 2) longer duration of objective response : >40 months vs 20 months (p=0.017) 3) longer PFS (p= ) and OS (p=0.04)
31 - Conclusion : 1) LGGs respond to TMZ 2) loss of chromosome 1p/19q predicts both a durable chemosensitivity and a favorable outcome Progression-free survival Overall survival according to the 1p/19q loss of heterozygosity status
32 2. TMZ with 1p19q codeletion (Levin N, et al. Cancer 2006; 106: ) : total of LGGs patients in the retrospective, single center observational study 1) objective responses in 17 patients (61%) 2) the median TTP of 31 months 3) PFS rate of 70% at 24 months 4) Loss of chromosome 1p were associated with objective response (p=0.003) 3. PCV with 1p19q codeletion (Stege EM, et al. Cancer 2005; 103: ) : total of 16 newly diagnosed ODs and OA patients in the retrospective, single center observational study 1) objective response in 13 patients (81.3%) 2) progression in only 1 patient (6.3%) 3) newly diagnosed patients with OD tumors, with or without loss of 1p/19q, well responded to PCV chemotherapy
33 MGMT gene promoter methylation in LGGs 1. TMZ chemotherapy with methylated MGMT gene promoter in LGGs (Levin N, et al. Cancer 2006; 106: ) : MGMT protein expression was analyzed by immunohistochemistry staining 1) The highest MGMT protein expression level in LGGs from patients with intact 1p (positive nuclear staining of > 50%) - maximal radiographic response of SD 2) tumors with 1p LOH and lower MGMT protein expression - also demonstrated an objective radiographic response - significant association between loss of chromosome 1p and MGMT protein expression
34 2. MGMT methylation: a marker of response to TMZ in LGGs (Everhard S et al. Ann Neurol 2006; 60: ) : evaluation of methylation status of MGMT gene promoter in 68 LGGs patients treated by neoadjuvant TMZ - methylated MGMT gene promoter in 63 of 68 (92.6%) patients characteristics responsive nonresponsive p-value PFS (mo) p-value MGMT gene promoter <0.001 unmethylated methylated p19q intact lost Histology of LGGs oligodendroglioma oligoastrocytoma astrocytoma
35 IDH1 mutation in LGGs (Houillier C, et al. Neurology 2010; 75: ) : case study of 271 LGGs to evaluate the correlation with of upfront TMZ and OS 1. IDH mutations in 132/189 patients (70%) 2. association of IDH mutation with outcome 1) prolonged overall survival in univariate (p=0.002) and multivariate analysis (p=0.003) 2) a higher rate of response to TMZ (p=0.01) 1p19q codeletion + IDH mutation None of these alteration Only IDH mutation PFS according to IDH status in the untreated group
36 Summaries of clinical relevant molecular markers in LGGs Biological significance Method of assessment Clinical relevance 1p19q codeletion - Biological role unclear : codeletion of chromosomal arms 1p and 19q linked to oligodendroglial morphology : candidate genes CIC and FUBP1 are under evaluation PCR, FISH Controversial, probably prognostically favorable MGMT gene promoter methylation DNA repair Methylation-specific PCR Controversial IDH1/2 mutation Link to DNA and histone methylation, energy metabolism, and pro-angiogenic pathways Immunohistochemistry (IDH1R132H) or sequencing Prognostically favorable Weller M et al, Neuro-Oncol 2012; 14:
37 SUMMARIES Chemotherapy is an interesting treatment option, especially as an upfront treatment in large unresectable LGGs with a 1p/19q codeletion Dynamic volumetric studies have recently provided a better description of the evolution of LGGs after chemotherapy, and new response criteria have been defined by the RANO group Ongoing phase III studies that compare the efficacy of TMZ alone or in association with radiotherapy to radiotherapy alone will allow a better delineation of the role of chemotherapy in LGGs (EORTC /CE5). These studies will also help to determine the potential predictive value of a 1p/19q codeletion, a MGMT promoter methylation and an IDH1 mutation

38
Radioterapia no Tratamento dos Gliomas de Baixo Grau
 Radioterapia no Tratamento dos Gliomas de Baixo Grau Dr. Luis Souhami University Montreal - Canada Low Grade Gliomas Relatively rare Heterogeneous, slow growing tumors WHO Classification Grade I Pilocytic
Radioterapia no Tratamento dos Gliomas de Baixo Grau Dr. Luis Souhami University Montreal - Canada Low Grade Gliomas Relatively rare Heterogeneous, slow growing tumors WHO Classification Grade I Pilocytic
Systemic Treatment. Third International Neuro-Oncology Course. 23 May 2014
 Low-Grade Astrocytoma of the CNS: Systemic Treatment Third International Neuro-Oncology Course São Paulo, Brazil 23 May 2014 John de Groot, MD Associate Professor, Neuro-Oncology UT MD Anderson Cancer
Low-Grade Astrocytoma of the CNS: Systemic Treatment Third International Neuro-Oncology Course São Paulo, Brazil 23 May 2014 John de Groot, MD Associate Professor, Neuro-Oncology UT MD Anderson Cancer
UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS
 UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS Antonio M. Omuro Department of Neurology Memorial Sloan-Kettering Cancer Center II International Neuro-Oncology Congress Sao Paulo, 08/17/12 CHALLENGES IN
UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS Antonio M. Omuro Department of Neurology Memorial Sloan-Kettering Cancer Center II International Neuro-Oncology Congress Sao Paulo, 08/17/12 CHALLENGES IN
21/03/2017. Disclosure. Practice Changing Articles in Neuro Oncology for 2016/17. Gliomas. Objectives. Gliomas. No conflicts to declare
 Practice Changing Articles in Neuro Oncology for 2016/17 Disclosure No conflicts to declare Frances Cusano, BScPharm, ACPR April 21, 2017 Objectives Gliomas To describe the patient selection, methodology
Practice Changing Articles in Neuro Oncology for 2016/17 Disclosure No conflicts to declare Frances Cusano, BScPharm, ACPR April 21, 2017 Objectives Gliomas To describe the patient selection, methodology
Clinical Trials for Adult Brain Tumors - the Imaging Perspective
 Clinical Trials for Adult Brain Tumors - the Imaging Perspective Whitney B. Pope, M.D., Ph.D. Department of Radiology David Geffen School of Medicine at UCLA August 22, 2015 1 Disclosure of Financial Relationships
Clinical Trials for Adult Brain Tumors - the Imaging Perspective Whitney B. Pope, M.D., Ph.D. Department of Radiology David Geffen School of Medicine at UCLA August 22, 2015 1 Disclosure of Financial Relationships
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM ANAPLASTIC GLIOMAS CNS Site Group Anaplastic Gliomas Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM ANAPLASTIC GLIOMAS CNS Site Group Anaplastic Gliomas Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
Precision medicine for gliomas
 Precision medicine for YAZMIN ODIA, MD MS LEAD PHYSICIAN OF MEDICAL NEURO-ONCOLOGY DISCLOSURES Novocure: Advisory Board for Optune in No other financial conflicts of interest Glioma OVERVIEW INFILTRATIVE,
Precision medicine for YAZMIN ODIA, MD MS LEAD PHYSICIAN OF MEDICAL NEURO-ONCOLOGY DISCLOSURES Novocure: Advisory Board for Optune in No other financial conflicts of interest Glioma OVERVIEW INFILTRATIVE,
Concepts for a personalized neurosurgical oncology. XXIV Annual Conference Pietro Paoletti 27. November 2015
 Concepts for a personalized neurosurgical oncology Jörg-Christian Tonn Dept. of Neurosurgery Ludwig-Maximilian University München Großhadern Germany XXIV Annual Conference Pietro Paoletti 27. November
Concepts for a personalized neurosurgical oncology Jörg-Christian Tonn Dept. of Neurosurgery Ludwig-Maximilian University München Großhadern Germany XXIV Annual Conference Pietro Paoletti 27. November
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM LOW GRADE GLIOMAS CNS Site Group Low Grade Gliomas Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM LOW GRADE GLIOMAS CNS Site Group Low Grade Gliomas Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING
Low grade glioma: a journey towards a cure
 Editorial Page 1 of 5 Low grade glioma: a journey towards a cure Ali K. Choucair SIU School of Medicine, Springfield, IL, USA Correspondence to: Ali K. Choucair, MD. Professor of Neurology, Director of
Editorial Page 1 of 5 Low grade glioma: a journey towards a cure Ali K. Choucair SIU School of Medicine, Springfield, IL, USA Correspondence to: Ali K. Choucair, MD. Professor of Neurology, Director of
Response to postoperative radiotherapy as a prognostic factor for patients with low-grade gliomas
 ONCOLOGY LETTERS 4: 455-460, 2012 Response to postoperative radiotherapy as a prognostic factor for patients with low-grade gliomas MICHAL SPYCH 1,2, LESZEK GOTTWALD 3, EMILIA JESIEŃ LEWANDOWICZ 1,2, SŁAWOMIR
ONCOLOGY LETTERS 4: 455-460, 2012 Response to postoperative radiotherapy as a prognostic factor for patients with low-grade gliomas MICHAL SPYCH 1,2, LESZEK GOTTWALD 3, EMILIA JESIEŃ LEWANDOWICZ 1,2, SŁAWOMIR
Oligodendroglial Tumors: A Review
 Oligodendroglial Tumors: A Review Sajeel Chowdhary, MD H Lee Moffitt Cancer Center and Research Institute Marc C Chamberlain, MD H Lee Moffitt Cancer Center and Research Institute Corresponding author:
Oligodendroglial Tumors: A Review Sajeel Chowdhary, MD H Lee Moffitt Cancer Center and Research Institute Marc C Chamberlain, MD H Lee Moffitt Cancer Center and Research Institute Corresponding author:
Antiangiogenic drugs in unresectable glioblastoma. Dra. Carmen Balañá. /
 Antiangiogenic drugs in unresectable glioblastoma Dra. Carmen Balañá. / Outcome for unresectable GBM Overall survival for unresectable GBM without further treatment is: 3 months at most. Radiotherapy increases
Antiangiogenic drugs in unresectable glioblastoma Dra. Carmen Balañá. / Outcome for unresectable GBM Overall survival for unresectable GBM without further treatment is: 3 months at most. Radiotherapy increases
University of Zurich. Temozolomide and MGMT forever? Zurich Open Repository and Archive. Weller, M. Year: 2010
 University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich Year: 2010 Temozolomide and MGMT forever? Weller, M Weller, M (2010). Temozolomide and MGMT forever? Neuro-Oncology,
University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich Year: 2010 Temozolomide and MGMT forever? Weller, M Weller, M (2010). Temozolomide and MGMT forever? Neuro-Oncology,
A clinical perspective on neuropathology and molecular genetics in brain tumors
 A clinical perspective on neuropathology and molecular genetics in brain tumors M.J. van den Bent Erasmus MC Cancer Institute Rotterdam, the Netherlands Disclosures Member speakersbureau: MSD Consultancy:
A clinical perspective on neuropathology and molecular genetics in brain tumors M.J. van den Bent Erasmus MC Cancer Institute Rotterdam, the Netherlands Disclosures Member speakersbureau: MSD Consultancy:
Prior to 1993, the only data available in the medical
 Neuro-Oncology Prospective clinical trials of intracranial low-grade glioma in adults and children Edward G. Shaw 1 and Jeffrey H. Wisoff Department of Radiation Oncology, Wake Forest University School
Neuro-Oncology Prospective clinical trials of intracranial low-grade glioma in adults and children Edward G. Shaw 1 and Jeffrey H. Wisoff Department of Radiation Oncology, Wake Forest University School
Temozolomide as Treatment in Low-grade Glioma: A Systematic Review
 Research Article imedpub Journals http://www.imedpub.com Neuro-Oncology: Open Access ISSN 2572-0376 DOI: 10.21767/2572-0376.100015 Abstract Temozolomide as Treatment in Low-grade Glioma: A Systematic Review
Research Article imedpub Journals http://www.imedpub.com Neuro-Oncology: Open Access ISSN 2572-0376 DOI: 10.21767/2572-0376.100015 Abstract Temozolomide as Treatment in Low-grade Glioma: A Systematic Review
Contemporary Management of Glioblastoma
 Contemporary Management of Glioblastoma Incidence Rates of Primary Brain Tumors Central Brain Tumor Registry of the United States, 1992-1997 100 Number of Cases per 100,000 Population 10 1 0.1 x I x I
Contemporary Management of Glioblastoma Incidence Rates of Primary Brain Tumors Central Brain Tumor Registry of the United States, 1992-1997 100 Number of Cases per 100,000 Population 10 1 0.1 x I x I
Neuro-Oncology. Martin J. van den Bent. Department of Neuro-oncology/Neurology, Erasmus M.C. Cancer Institute, Rotterdam, Netherlands
 Neuro-Oncology Neuro-Oncology 16(12), 1570 1574, 2014 doi:10.1093/neuonc/nou297 Advance Access date 29 October 2014 Practice changing mature results of RTOG study 9802: another positive PCV trial makes
Neuro-Oncology Neuro-Oncology 16(12), 1570 1574, 2014 doi:10.1093/neuonc/nou297 Advance Access date 29 October 2014 Practice changing mature results of RTOG study 9802: another positive PCV trial makes
Examining large groups of cancer patients to identify ways of predicting which therapies cancers might respond to.
 Stratified Medicine Examining large groups of cancer patients to identify ways of predicting which therapies cancers might respond to. Looking in detail at cancer cells and their genetic make up. Permit
Stratified Medicine Examining large groups of cancer patients to identify ways of predicting which therapies cancers might respond to. Looking in detail at cancer cells and their genetic make up. Permit
MOLECULAR DIAGNOSTICS OF GLIOMAS
 MOLECULAR DIAGNOSTICS OF GLIOMAS Arie Perry, M.D. Director, Neuropathology Division DIFFUSE GLIOMAS Cell types Astrocytomas (A) Oligodendrogliomas (O) Mixed oligoastrocytoma (MOA) Three WHO grades: II,
MOLECULAR DIAGNOSTICS OF GLIOMAS Arie Perry, M.D. Director, Neuropathology Division DIFFUSE GLIOMAS Cell types Astrocytomas (A) Oligodendrogliomas (O) Mixed oligoastrocytoma (MOA) Three WHO grades: II,
The New WHO Classification and the Role of Integrated Molecular Profiling in the Diagnosis of Malignant Gliomas
 The New WHO Classification and the Role of Integrated Molecular Profiling in the Diagnosis of Malignant Gliomas Stefan Prokop, MD Neuropathology Fellow Hospital of the University of Pennsylvania Background
The New WHO Classification and the Role of Integrated Molecular Profiling in the Diagnosis of Malignant Gliomas Stefan Prokop, MD Neuropathology Fellow Hospital of the University of Pennsylvania Background
Management of Glioma: The Basics Glioma Update The clinical challenge. Glioma a malignant disease of the CNS
 Management of Glioma: The Basics Glioma Update 3 oger Stupp, MD Department of Oncology & Cancer Center University Hospital Zurich, Switzerland (roger.stupp@usz.ch) Bern, 3. August 3 The clinical challenge
Management of Glioma: The Basics Glioma Update 3 oger Stupp, MD Department of Oncology & Cancer Center University Hospital Zurich, Switzerland (roger.stupp@usz.ch) Bern, 3. August 3 The clinical challenge
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
CNS SESSION 3/8/ th Multidisciplinary Management of Cancers: A Case based Approach
 CNS SESSION Chair: Ruben Fragoso, MD/PhD UC Davis Fellow: Michael Cardenas, MD UC Davis Panel: Gordon Li, MD Stanford Seema Nagpal, MD Stanford Jennie Taylor, MD UCSF HPI: 46 yo right handed woman who
CNS SESSION Chair: Ruben Fragoso, MD/PhD UC Davis Fellow: Michael Cardenas, MD UC Davis Panel: Gordon Li, MD Stanford Seema Nagpal, MD Stanford Jennie Taylor, MD UCSF HPI: 46 yo right handed woman who
EORTC (RTOG 0834 Endorsed) Opened: July 22, 2009
 Opened: July 22, 2009") January 2011 0834-1 EORTC 26053 22054 (RTOG 0834 Endorsed) Protocol Status: Opened: July 22, 2009 Title: Phase III Trial on Concurrent and Adjuvant Temozolomide Chemotherapy in Non-1P/19Q Deleted Anaplastic
January 2011 0834-1 EORTC 26053 22054 (RTOG 0834 Endorsed) Protocol Status: Opened: July 22, 2009 Title: Phase III Trial on Concurrent and Adjuvant Temozolomide Chemotherapy in Non-1P/19Q Deleted Anaplastic
Corporate Medical Policy
 Corporate Medical Policy Analysis of MGMT Promoter Methylation in Malignant Gliomas File Name: Origination: Last CAP Review: Next CAP Review: Last Review: analysis_of_mgmt_promoter_methylation_in_malignant_gliomas
Corporate Medical Policy Analysis of MGMT Promoter Methylation in Malignant Gliomas File Name: Origination: Last CAP Review: Next CAP Review: Last Review: analysis_of_mgmt_promoter_methylation_in_malignant_gliomas
Glioblastoma: Current Treatment Approach 8/20/2018
 Glioblastoma: Current Treatment Approach 8/20/2018 Overview What is Glioblastoma? How is it diagnosed How is it treated? Principles of Treatment Surgery, Radiation, Chemotherapy Current Standard of care
Glioblastoma: Current Treatment Approach 8/20/2018 Overview What is Glioblastoma? How is it diagnosed How is it treated? Principles of Treatment Surgery, Radiation, Chemotherapy Current Standard of care
Primary Brain Tumors: Characteristics, Practical Diagnostic and Treatment Approaches
 Primary Brain Tumors: Characteristics, Practical Diagnostic and Treatment Approaches Kraig Moore and Lyndon Kim Abstract Primary brain tumors are classified according to the tissue of phylogenic origin.
Primary Brain Tumors: Characteristics, Practical Diagnostic and Treatment Approaches Kraig Moore and Lyndon Kim Abstract Primary brain tumors are classified according to the tissue of phylogenic origin.
Oncological Management of Brain Tumours. Anna Maria Shiarli SpR in Clinical Oncology 15 th July 2013
 Oncological Management of Brain Tumours Anna Maria Shiarli SpR in Clinical Oncology 15 th July 2013 Outline General considerations of Primary Brain Tumours: epidemiology, pathology, presentation. Diagnosis
Oncological Management of Brain Tumours Anna Maria Shiarli SpR in Clinical Oncology 15 th July 2013 Outline General considerations of Primary Brain Tumours: epidemiology, pathology, presentation. Diagnosis
MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES
 MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES DISCLOSURE No conflicts of interest to disclose Patricia Bruns APRN, CNS Givens Brain Tumor Center Abbott Northwestern Hospital October 12, 2018 OBJECTIVES THEN
MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES DISCLOSURE No conflicts of interest to disclose Patricia Bruns APRN, CNS Givens Brain Tumor Center Abbott Northwestern Hospital October 12, 2018 OBJECTIVES THEN
NON-SURGICAL STRATEGY FOR ADULT EPENDYMOMA
 NON-SURGICAL STRATEGY FOR ADULT EPENDYMOMA Roberta Rudà Department of Neuro-Oncology University and City of Health and Science Hospital of Turin, Italy EORTC EANO ESMO Conference 2015 Istanbul, March 27-28
NON-SURGICAL STRATEGY FOR ADULT EPENDYMOMA Roberta Rudà Department of Neuro-Oncology University and City of Health and Science Hospital of Turin, Italy EORTC EANO ESMO Conference 2015 Istanbul, March 27-28
Hypofractionated radiation therapy for glioblastoma
 Hypofractionated radiation therapy for glioblastoma Luis Souhami, MD, FASTRO Professor McGill University Department of Oncology, Division of Radiation Oncology Montreal Canada McGill University Health
Hypofractionated radiation therapy for glioblastoma Luis Souhami, MD, FASTRO Professor McGill University Department of Oncology, Division of Radiation Oncology Montreal Canada McGill University Health
Incidence of Early Pseudo-progression in a Cohort of Malignant Glioma Patients Treated With Chemoirradiation With Temozolomide
 405 Incidence of Early Pseudo-progression in a Cohort of Malignant Glioma Patients Treated With Chemoirradiation With Temozolomide Walter Taal, MD 1 Dieta Brandsma, MD, PhD 1 Hein G. de Bruin, MD, PhD
405 Incidence of Early Pseudo-progression in a Cohort of Malignant Glioma Patients Treated With Chemoirradiation With Temozolomide Walter Taal, MD 1 Dieta Brandsma, MD, PhD 1 Hein G. de Bruin, MD, PhD
Marizomib (MRZ): Brain Penetrant Irreversible Pan-Proteasome Inhibitor
: Brain Penetrant Irreversible Pan-Proteasome Inhibitor") MARIZOMIB (MRZ) WITH BEVACIZUMAB (BEV) IN WHO GRADE IV MALIGNANT GLIOMA (G4 MG): FULL ENROLLMENT RESULTS FROM THE PHASE 1, MULTICENTER, OPEN-LABEL STUDY Daniela Bota, MD, PhD 1, Annick Desjardins, MD,
MARIZOMIB (MRZ) WITH BEVACIZUMAB (BEV) IN WHO GRADE IV MALIGNANT GLIOMA (G4 MG): FULL ENROLLMENT RESULTS FROM THE PHASE 1, MULTICENTER, OPEN-LABEL STUDY Daniela Bota, MD, PhD 1, Annick Desjardins, MD,
Scottish Medicines Consortium
 Scottish Medicines Consortium temozolomide 5, 20, 100 and 250mg capsules (Temodal ) Schering Plough UK Ltd No. (244/06) New indication: for the treatment of newly diagnosed glioblastoma multiforme concomitantly
Scottish Medicines Consortium temozolomide 5, 20, 100 and 250mg capsules (Temodal ) Schering Plough UK Ltd No. (244/06) New indication: for the treatment of newly diagnosed glioblastoma multiforme concomitantly
LOW GRADE ASTROCYTOMAS
 LOW GRADE ASTROCYTOMAS This article was provided to us by David Schiff, MD, Associate Professor of Neurology, Neurosurgery, and Medicine at University of Virginia, Charlottesville. We appreciate his generous
LOW GRADE ASTROCYTOMAS This article was provided to us by David Schiff, MD, Associate Professor of Neurology, Neurosurgery, and Medicine at University of Virginia, Charlottesville. We appreciate his generous
PROCARBAZINE, lomustine, and vincristine (PCV) is
 is") RAPID PUBLICATION Procarbazine, Lomustine, and Vincristine () Chemotherapy for Anaplastic Astrocytoma: A Retrospective Review of Radiation Therapy Oncology Group Protocols Comparing Survival With Carmustine
RAPID PUBLICATION Procarbazine, Lomustine, and Vincristine () Chemotherapy for Anaplastic Astrocytoma: A Retrospective Review of Radiation Therapy Oncology Group Protocols Comparing Survival With Carmustine
Asma Bashir, MD, 1 Jannick Brennum, MD, DMSc, 2 Helle Broholm, MD, 3 and Ian Law, MD, PhD, DMSc 1
 CLINICAL ARTICLE The diagnostic accuracy of detecting malignant transformation of low-grade glioma using O-(2-[ 18 F]fluoroethyl)-l-tyrosine positron emission tomography: a retrospective study Asma Bashir,
CLINICAL ARTICLE The diagnostic accuracy of detecting malignant transformation of low-grade glioma using O-(2-[ 18 F]fluoroethyl)-l-tyrosine positron emission tomography: a retrospective study Asma Bashir,
PI3-Kinase Signaling. Rational Incorporation of Novel Agents into Multimodality Therapy. PI3-kinase. PI3-kinase 5/2/2010
 Rational Incorporation of Novel Agents into Multimodality Therapy I3-Kinase Signaling EGF IRS1 I3K EGFR I2 I3 TEN Rictor GßL AKT RAS40 Survival Raptor GßL Daphne Haas-Kogan UCSF Annual Course April 30-May
Rational Incorporation of Novel Agents into Multimodality Therapy I3-Kinase Signaling EGF IRS1 I3K EGFR I2 I3 TEN Rictor GßL AKT RAS40 Survival Raptor GßL Daphne Haas-Kogan UCSF Annual Course April 30-May
Concomitant (without adjuvant) temozolomide and radiation to treat glioblastoma: A retrospective study
 temozolomide and radiation to treat glioblastoma: A retrospective study") Concomitant (without adjuvant) temozolomide and radiation to treat glioblastoma: A retrospective study T Sridhar 1, A Gore 1, I Boiangiu 1, D Machin 2, R P Symonds 3 1. Department of Oncology, Leicester
Concomitant (without adjuvant) temozolomide and radiation to treat glioblastoma: A retrospective study T Sridhar 1, A Gore 1, I Boiangiu 1, D Machin 2, R P Symonds 3 1. Department of Oncology, Leicester
Gliomas in the 2016 WHO Classification of CNS Tumors
 Gliomas in the 2016 WHO Classification of CNS Tumors Hindi N Al-Hindi, MD, FCAP Consultant Neuropathologist and Head Section of Anatomic Pathology Department of Pathology and Laboratory Medicine King Faisal
Gliomas in the 2016 WHO Classification of CNS Tumors Hindi N Al-Hindi, MD, FCAP Consultant Neuropathologist and Head Section of Anatomic Pathology Department of Pathology and Laboratory Medicine King Faisal
Imaging for suspected glioma
 Imaging for suspected glioma 1.1.1 Offer standard structural MRI (defined as T2 weighted, FLAIR, DWI series and T1 pre- and post-contrast volume) as the initial diagnostic test for suspected glioma, unless
Imaging for suspected glioma 1.1.1 Offer standard structural MRI (defined as T2 weighted, FLAIR, DWI series and T1 pre- and post-contrast volume) as the initial diagnostic test for suspected glioma, unless
Dose dense 1 week on/1 week off temozolomide in recurrent glioma: a retrospective study
 J Neurooncol (2012) 108:195 200 DOI 10.1007/s11060-012-0832-5 CLINICAL STUDY Dose dense 1 week on/1 week off temozolomide in recurrent glioma: a retrospective study Walter Taal Joyce M. W. Segers-van Rijn
J Neurooncol (2012) 108:195 200 DOI 10.1007/s11060-012-0832-5 CLINICAL STUDY Dose dense 1 week on/1 week off temozolomide in recurrent glioma: a retrospective study Walter Taal Joyce M. W. Segers-van Rijn
MolDX: Chromosome 1p/19q deletion analysis
 MolDX: Chromosome 1p/19q deletion analysis CGS Administrators, LLC Jump to Section... Please Note: This is a Proposed LCD. Proposed LCDs are works in progress and not necessarily a reflection of the current
MolDX: Chromosome 1p/19q deletion analysis CGS Administrators, LLC Jump to Section... Please Note: This is a Proposed LCD. Proposed LCDs are works in progress and not necessarily a reflection of the current
Bevacizumab rescue therapy extends the survival in patients with recurrent malignant glioma
 Original Article Bevacizumab rescue therapy extends the survival in patients with recurrent malignant glioma Lin-Bo Cai, Juan Li, Ming-Yao Lai, Chang-Guo Shan, Zong-De Lian, Wei-Ping Hong, Jun-Jie Zhen,
Original Article Bevacizumab rescue therapy extends the survival in patients with recurrent malignant glioma Lin-Bo Cai, Juan Li, Ming-Yao Lai, Chang-Guo Shan, Zong-De Lian, Wei-Ping Hong, Jun-Jie Zhen,
Neuro-Oncology Program
 Neuro-Oncology Program The goals of the Neuro-oncology Committee are: 1) to improve duration and quality of life of brain tumor patients; 2) to assess disease and treatment-related effects on neurocognitive
Neuro-Oncology Program The goals of the Neuro-oncology Committee are: 1) to improve duration and quality of life of brain tumor patients; 2) to assess disease and treatment-related effects on neurocognitive
Zurich Open Repository and Archive. Procarbazine and CCNU as initial treatment in gliomatosis cerebri
 University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich http://www.zora.uzh.ch Year: 2008 Procarbazine and CCNU as initial treatment in gliomatosis cerebri Glas, M;
University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich http://www.zora.uzh.ch Year: 2008 Procarbazine and CCNU as initial treatment in gliomatosis cerebri Glas, M;
The Role of Radiation Therapy in the Treatment of Brain Metastases. Matthew Cavey, M.D.
 The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
Case Presentation: USCAP Jason T. Huse, MD, PhD Assistant Member Department of Pathology Memorial Sloan Kettering Cancer Center
 Case Presentation: USCAP 2016 Jason T. Huse, MD, PhD Assistant Member Department of Pathology Memorial Sloan Kettering Cancer Center Case History 53 year old female with a long standing history of migraines
Case Presentation: USCAP 2016 Jason T. Huse, MD, PhD Assistant Member Department of Pathology Memorial Sloan Kettering Cancer Center Case History 53 year old female with a long standing history of migraines
Neurocognitive Assessment in Patients with Brain Metastases. Martin Klein VU University Medical Center Amsterdam, The Netherlands
 Neurocognitive Assessment in Patients with Brain Metastases Martin Klein VU University Medical Center Amsterdam, The Netherlands Treatment Outcomes I Traditional/primary endpoints of efficacy:! Physician
Neurocognitive Assessment in Patients with Brain Metastases Martin Klein VU University Medical Center Amsterdam, The Netherlands Treatment Outcomes I Traditional/primary endpoints of efficacy:! Physician
Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease
 Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease Jennifer E. Tseng, MD UFHealth Cancer Center-Orlando Health Sep 12, 2014 Background Approximately
Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease Jennifer E. Tseng, MD UFHealth Cancer Center-Orlando Health Sep 12, 2014 Background Approximately
Zurich Open Repository and Archive. Long-term survival of glioblastoma patients treated with radiotherapy and lomustine plus temozolomide
 University of Zurich Zurich Open Repository and Archive Winterthurerstr. 19 CH-857 Zurich http://www.zora.uzh.ch Year: 29 Long-term survival of glioblastoma patients treated with radiotherapy and lomustine
University of Zurich Zurich Open Repository and Archive Winterthurerstr. 19 CH-857 Zurich http://www.zora.uzh.ch Year: 29 Long-term survival of glioblastoma patients treated with radiotherapy and lomustine
Modeling origin and natural evolution of low-grade gliomas
 Modeling origin and natural evolution of low-grade gliomas Mathilde Badoual Paris Diderot University, IMNC lab 2nd HTE workshop: Mathematical & Computer Modeling to study tumors heterogeneity in its ecosystem,
Modeling origin and natural evolution of low-grade gliomas Mathilde Badoual Paris Diderot University, IMNC lab 2nd HTE workshop: Mathematical & Computer Modeling to study tumors heterogeneity in its ecosystem,
Chika Nwachukwu, Ph.D. MS IV Radiation Oncology Rotation
 Chika Nwachukwu, Ph.D. MS IV Radiation Oncology Rotation Background Histology/Tumor Characteristics Presenting Symptoms/diagnosis Treatment/outcome Patient cohort Research on HRQOL Slow growing indolent
Chika Nwachukwu, Ph.D. MS IV Radiation Oncology Rotation Background Histology/Tumor Characteristics Presenting Symptoms/diagnosis Treatment/outcome Patient cohort Research on HRQOL Slow growing indolent
PRESURGICAL PLANNING. Strongly consider neuropsychological evaluation before functional imaging study Strongly consider functional imaging study
 NOTE: Consider Clinical Trials as treatment options for eligible patients. Page 1 of 6 RADIOLOGICAL PRESENTATION PRESURGICAL PLANNING TREATMENT Imaging study suggestive of glioma 1 Left hemisphere speech/motor
NOTE: Consider Clinical Trials as treatment options for eligible patients. Page 1 of 6 RADIOLOGICAL PRESENTATION PRESURGICAL PLANNING TREATMENT Imaging study suggestive of glioma 1 Left hemisphere speech/motor
CURRENT CONTROVERSIES IN THE MANAGEMENT OF HIGH GRADE GLIOMAS: AN INTERACTIVE CASE DISCUSSION *
 CURRENT CONTROVERSIES IN THE MANAGEMENT OF HIGH GRADE GLIOMAS: AN INTERACTIVE CASE DISCUSSION * Alessandro Olivi, MD, Jaishri Blakeley, MD, and Allen K. Sills, MD, FACS ABSTRACT The management of glioma
CURRENT CONTROVERSIES IN THE MANAGEMENT OF HIGH GRADE GLIOMAS: AN INTERACTIVE CASE DISCUSSION * Alessandro Olivi, MD, Jaishri Blakeley, MD, and Allen K. Sills, MD, FACS ABSTRACT The management of glioma
Zurich Open Repository and Archive. Long-term survival of glioblastoma patients treated with radiotherapy and lomustine plus temozolomide
 University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich http://www.zora.uzh.ch Year: 2009 Long-term survival of glioblastoma patients treated with radiotherapy and lomustine
University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich http://www.zora.uzh.ch Year: 2009 Long-term survival of glioblastoma patients treated with radiotherapy and lomustine
Chemotherapy in malignant brain tumors
 Chemotherapy in malignant brain tumors Frank Zimmermann Institut für Radioonkologie Universitätsspital Basel Petersgraben 4 CH 4031 Basel zimmermannf@uhbs.ch Tumor types Neuro-epithelial tumors - Glioblastoma
Chemotherapy in malignant brain tumors Frank Zimmermann Institut für Radioonkologie Universitätsspital Basel Petersgraben 4 CH 4031 Basel zimmermannf@uhbs.ch Tumor types Neuro-epithelial tumors - Glioblastoma
PROPOSED/DRAFT Local Coverage Determination (LCD): MolDX: Chromosome 1p/19q deletion analysis (DL36483)
: MolDX: Chromosome 1p/19q deletion analysis (DL36483)") moldx: Chromosome 1p/19q deletion analysis (DL36483) Page 1 of 8 PROPOSED/DRAFT Local Coverage Determination (LCD): MolDX: Chromosome 1p/19q deletion analysis (DL36483) Close Section Navigation
moldx: Chromosome 1p/19q deletion analysis (DL36483) Page 1 of 8 PROPOSED/DRAFT Local Coverage Determination (LCD): MolDX: Chromosome 1p/19q deletion analysis (DL36483) Close Section Navigation
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 12: CNS tumours 2/3
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 12: CNS tumours 2/3 Pilocytic astrocytoma Relatively benign ( WHO grade 1) Occurs in children and young adults Mostly: in the cerebellum
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 12: CNS tumours 2/3 Pilocytic astrocytoma Relatively benign ( WHO grade 1) Occurs in children and young adults Mostly: in the cerebellum
Survival of High Grade Glioma Patients Treated by Three Radiation Schedules with Chemotherapy: A Retrospective Comparative Study
 Original Article Research in Oncology June 2017; Vol. 13, No. 1: 18-22. DOI: 10.21608/resoncol.2017.552.1022 Survival of High Grade Glioma Patients Treated by Three Radiation Schedules with Chemotherapy:
Original Article Research in Oncology June 2017; Vol. 13, No. 1: 18-22. DOI: 10.21608/resoncol.2017.552.1022 Survival of High Grade Glioma Patients Treated by Three Radiation Schedules with Chemotherapy:
DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES
 DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES Marco Krengli Radiotherapy, Department of Translational Medicine, University of Piemonte Orientale A. Avogadro THE STANDARD OF CARE
DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES Marco Krengli Radiotherapy, Department of Translational Medicine, University of Piemonte Orientale A. Avogadro THE STANDARD OF CARE
Nature Genetics: doi: /ng.2995
 Supplementary Figure 1 Kaplan-Meier survival curves of patients with brainstem tumors. (a) Comparison of patients with PPM1D mutation versus wild-type PPM1D. (b) Comparison of patients with PPM1D mutation
Supplementary Figure 1 Kaplan-Meier survival curves of patients with brainstem tumors. (a) Comparison of patients with PPM1D mutation versus wild-type PPM1D. (b) Comparison of patients with PPM1D mutation
2015 EUROPEAN CANCER CONGRESS
 2015 EUROPEAN CANCER CONGRESS 25-29 September 2015 Vienna, Austria SUMMARY The European Cancer Congress (ECC 2015) combined the 40th European Society for Medical Oncology (ESMO) congress with the 18th
2015 EUROPEAN CANCER CONGRESS 25-29 September 2015 Vienna, Austria SUMMARY The European Cancer Congress (ECC 2015) combined the 40th European Society for Medical Oncology (ESMO) congress with the 18th
Brain tumours (primary) and brain metastases in adults
 and brain metastases in adults") Brain tumours (primary) and brain metastases in adults NICE guideline Draft for consultation, January 0 This guideline covers diagnosing, monitoring and managing any type of primary brain tumour or brain
Brain tumours (primary) and brain metastases in adults NICE guideline Draft for consultation, January 0 This guideline covers diagnosing, monitoring and managing any type of primary brain tumour or brain
Epidemiology and outcome research of glioma patients in Southern Switzerland: A population based analysis
 Epidemiology and outcome research of glioma patients in Southern Switzerland: A population based analysis G. Pesce 1, A. Bordoni, F. Montanaro, R. Renella 3, A. Richetti 1, D. Boscherini 3, S. Mauri 4,
Epidemiology and outcome research of glioma patients in Southern Switzerland: A population based analysis G. Pesce 1, A. Bordoni, F. Montanaro, R. Renella 3, A. Richetti 1, D. Boscherini 3, S. Mauri 4,
Jennie W Taylor, MD 02/15/2019. Patient 1 Presentation
 Patient 1 Presentation Jennie W Taylor, MD 02/15/2019 A 34 year old right handed woman presents in 07/2015 with 9 years of stereotyped spells of olfactory change, nausea, and altered awareness. Imaging
Patient 1 Presentation Jennie W Taylor, MD 02/15/2019 A 34 year old right handed woman presents in 07/2015 with 9 years of stereotyped spells of olfactory change, nausea, and altered awareness. Imaging
Classification of Diffuse Gliomas: Progress, Pearls and Pitfalls. Rob Macaulay Neuropathologist, MCC October 21, 2017
 Classification of Diffuse Gliomas: Progress, Pearls and Pitfalls Rob Macaulay Neuropathologist, MCC October 21, 2017 Objectives Explain why the designation high grade glioma is preferable to GBM for intraoperative
Classification of Diffuse Gliomas: Progress, Pearls and Pitfalls Rob Macaulay Neuropathologist, MCC October 21, 2017 Objectives Explain why the designation high grade glioma is preferable to GBM for intraoperative
NICE guideline Published: 11 July 2018 nice.org.uk/guidance/ng99
 Brain tumours (primary) and brain metastases in adults NICE guideline Published: 11 July 2018 nice.org.uk/guidance/ng99 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Brain tumours (primary) and brain metastases in adults NICE guideline Published: 11 July 2018 nice.org.uk/guidance/ng99 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Chemotherapy in Adults with Gliomas
 364 Chemotherapy in Adults with Gliomas Siew-Ju See and Mark R Gilbert Review Article Chemotherapy in Adults with Gliomas Siew-Ju See, 1 MBBS (S pore), MRCP (UK), Mark R Gilbert, 2 MD Abstract Treating
364 Chemotherapy in Adults with Gliomas Siew-Ju See and Mark R Gilbert Review Article Chemotherapy in Adults with Gliomas Siew-Ju See, 1 MBBS (S pore), MRCP (UK), Mark R Gilbert, 2 MD Abstract Treating
Treatment with Tumor-Treating Fields therapy and pulse dose bevacizumab in patients with bevacizumab-refractory recurrent glioblastoma: A case series.
 School of Medicine Digital Commons@Becker Open Access Publications 2016 Treatment with Tumor-Treating Fields therapy and pulse dose bevacizumab in patients with bevacizumab-refractory recurrent glioblastoma:
School of Medicine Digital Commons@Becker Open Access Publications 2016 Treatment with Tumor-Treating Fields therapy and pulse dose bevacizumab in patients with bevacizumab-refractory recurrent glioblastoma:
Carmustine implants and Temozolomide for the treatment of newly diagnosed high grade glioma
 National Institute for Health and Clinical Excellence Health Technology Appraisal Carmustine implants and Temozolomide for the treatment of newly diagnosed high grade glioma Personal statement Conventional
National Institute for Health and Clinical Excellence Health Technology Appraisal Carmustine implants and Temozolomide for the treatment of newly diagnosed high grade glioma Personal statement Conventional
IAN CROCKER = TIM HOWARD
 Winship Cancer Institute of Emory University Radiation as Consolidation in the Treatment of Newly Diagnosed CNS Lymphoma versus After Failure of Chemotherapy Pro: Upfront Radiation Ian Crocker MD, FACR,
Winship Cancer Institute of Emory University Radiation as Consolidation in the Treatment of Newly Diagnosed CNS Lymphoma versus After Failure of Chemotherapy Pro: Upfront Radiation Ian Crocker MD, FACR,
Brain Tumors: Radiologic Perspective
 Brain Tumors: Radiologic Perspective Alberto Bizzi, M.D. Neuroradiology Humanitas Research Hospital Milan, Italy The job of the neuroradiologist in the work-up of brain tumors has quite changed in the
Brain Tumors: Radiologic Perspective Alberto Bizzi, M.D. Neuroradiology Humanitas Research Hospital Milan, Italy The job of the neuroradiologist in the work-up of brain tumors has quite changed in the
Oral Communications & Posters
 Carcinoma uroteliale: Current and future directions of treatment of Muscle-Invasive Bladder cancer/ Multimodality approach of bladder cancer Oral Communications & Posters CRISTINA MASINI Oncologia Medica
Carcinoma uroteliale: Current and future directions of treatment of Muscle-Invasive Bladder cancer/ Multimodality approach of bladder cancer Oral Communications & Posters CRISTINA MASINI Oncologia Medica
Optimal Management of Isolated HER2+ve Brain Metastases
 Optimal Management of Isolated HER2+ve Brain Metastases Eliot Sims November 2013 Background Her2+ve patients 15% of all breast cancer Even with adjuvant trastuzumab 10-15% relapse Trastuzumab does not
Optimal Management of Isolated HER2+ve Brain Metastases Eliot Sims November 2013 Background Her2+ve patients 15% of all breast cancer Even with adjuvant trastuzumab 10-15% relapse Trastuzumab does not
Protocol Abstract and Schema
 Protocol Abstract and Schema This is a phase I/II study to determine: 1) the maximum tolerated dose (MTD) or recommended phase II dose of ABT-888 in combination with radiation therapy, and 2) the efficacy
Protocol Abstract and Schema This is a phase I/II study to determine: 1) the maximum tolerated dose (MTD) or recommended phase II dose of ABT-888 in combination with radiation therapy, and 2) the efficacy
Virtual Journal Club: Front-Line Therapy and Beyond Recent Perspectives on ALK-Positive Non-Small Cell Lung Cancer.
 Virtual Journal Club: Front-Line Therapy and Beyond Recent Perspectives on ALK-Positive Non-Small Cell Lung Cancer Reference Slides ALK Rearrangement in NSCLC ALK (anaplastic lymphoma kinase) is a receptor
Virtual Journal Club: Front-Line Therapy and Beyond Recent Perspectives on ALK-Positive Non-Small Cell Lung Cancer Reference Slides ALK Rearrangement in NSCLC ALK (anaplastic lymphoma kinase) is a receptor
Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen?
 Department of Radiation Oncology Chairman: Prof. Dr. Matthias Guckenberger Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen? Matthias
Department of Radiation Oncology Chairman: Prof. Dr. Matthias Guckenberger Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen? Matthias
CILENT P Leblond, DIPG Meeting, Barcelone 2012
 CILENT-0902 Cilengitide (EMD121974) in combination with irradiation in children and adolescents with newly diagnosed diffuse intrinsic brainstem glioma : Phase I Study P Leblond, DIPG Meeting, Barcelone
CILENT-0902 Cilengitide (EMD121974) in combination with irradiation in children and adolescents with newly diagnosed diffuse intrinsic brainstem glioma : Phase I Study P Leblond, DIPG Meeting, Barcelone
Long-term follow-up in adult patients with low-grade glioma (WHO II) postoperatively irradiated. Analysis of prognostic factors
 postoperatively irradiated. Analysis of prognostic factors") reports of practical oncology and radiotherapy 1 7 (2 0 1 2) 141 145 Available online at www.sciencedirect.com journal homepage: http://www.elsevier.com/locate/rpor Original research article Long-term
reports of practical oncology and radiotherapy 1 7 (2 0 1 2) 141 145 Available online at www.sciencedirect.com journal homepage: http://www.elsevier.com/locate/rpor Original research article Long-term
Management of Brain Metastases Sanjiv S. Agarwala, MD
 Management of Brain Metastases Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA, USA Incidence (US):
Management of Brain Metastases Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA, USA Incidence (US):
Cilengitide (Impetreve) for glioblastoma multiforme. February 2012
 for glioblastoma multiforme. February 2012") Cilengitide (Impetreve) for glioblastoma multiforme February 2012 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to
Cilengitide (Impetreve) for glioblastoma multiforme February 2012 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to
Minesh Mehta, Northwestern University. Chicago, IL
 * Minesh Mehta, Northwestern University Chicago, IL Consultant: Adnexus, Bayer, Merck, Tomotherapy Stock Options: Colby, Pharmacyclics, Procertus, Stemina, Tomotherapy Board of Directors: Pharmacyclics
* Minesh Mehta, Northwestern University Chicago, IL Consultant: Adnexus, Bayer, Merck, Tomotherapy Stock Options: Colby, Pharmacyclics, Procertus, Stemina, Tomotherapy Board of Directors: Pharmacyclics
Epidemiology and Semiology of Tumor-based Epilepsy December 2, 2012
 Epidemiology and Semiology of Tumor-based Epilepsy December 2, 2012 Charles J. Vecht, MD, PhD Medical Center The Hague SEIN Epilepsy Foundation, The Netherlands CHU Pitié-Salpêtrière, Paris, France American
Epidemiology and Semiology of Tumor-based Epilepsy December 2, 2012 Charles J. Vecht, MD, PhD Medical Center The Hague SEIN Epilepsy Foundation, The Netherlands CHU Pitié-Salpêtrière, Paris, France American
Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms. Overall Clinical Significance 8/3/13
 Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms Jason Sheehan, MD, PhD Departments of Neurosurgery and Radiation Oncology University of Virginia, Charlottesville, VA USA Overall
Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms Jason Sheehan, MD, PhD Departments of Neurosurgery and Radiation Oncology University of Virginia, Charlottesville, VA USA Overall
Corporate Medical Policy
 Corporate Medical Policy Brachytherapy, Intracavitary Balloon Catheter for Brain Cancer File Name: Origination: Last CAP Review: Next CAP Review: Last Review: brachytherapy_intracavitary_balloon_catheter_for_brain_cancer
Corporate Medical Policy Brachytherapy, Intracavitary Balloon Catheter for Brain Cancer File Name: Origination: Last CAP Review: Next CAP Review: Last Review: brachytherapy_intracavitary_balloon_catheter_for_brain_cancer
RINDOPEPIMUT (CDX-110) IN GLIOBLASTOMA
 IN GLIOBLASTOMA") RINDOPEPIMUT (CDX-110) IN GLIOBLASTOMA MULTIFORM GEINO 2014 Dra Estela Pineda Madrid Hospital Clínic Barcelona EGFRvIII in glioblastoma multiform The most common mutation of EGFR in GBM Expressed in 30%
RINDOPEPIMUT (CDX-110) IN GLIOBLASTOMA MULTIFORM GEINO 2014 Dra Estela Pineda Madrid Hospital Clínic Barcelona EGFRvIII in glioblastoma multiform The most common mutation of EGFR in GBM Expressed in 30%
Adjuvant treatment of high grade gliomas
 17 (Supplement 10): x186 x190, 2006 doi:10.1093/annonc/mdl258 Adjuvant treatment of high grade gliomas M. J. van den Bent Department of Neuro-Oncology, Erasmus University Hospital Rotterdam/Rotterdam Cancer
17 (Supplement 10): x186 x190, 2006 doi:10.1093/annonc/mdl258 Adjuvant treatment of high grade gliomas M. J. van den Bent Department of Neuro-Oncology, Erasmus University Hospital Rotterdam/Rotterdam Cancer
Neurosurgical Management of Brain Tumours. Nicholas Little Neurosurgeon RNSH
 Neurosurgical Management of Brain Tumours Nicholas Little Neurosurgeon RNSH General Most common tumours are metastatic 10x more common than primary Incidence of primary neoplasms is 20 per 100000 per year
Neurosurgical Management of Brain Tumours Nicholas Little Neurosurgeon RNSH General Most common tumours are metastatic 10x more common than primary Incidence of primary neoplasms is 20 per 100000 per year
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Management of Brain Metastases Dr. Luis Souhami Professor Department of Radiation Oncology University,
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Management of Brain Metastases Dr. Luis Souhami Professor Department of Radiation Oncology University,
Citation Pediatrics international (2015), 57.
, 57.") Title Long-term efficacy of bevacizumab a pediatric glioblastoma. Umeda, Katsutsugu; Shibata, Hirofum Author(s) Hiramatsu, Hidefumi; Arakawa, Yoshi Nishiuchi, Ritsuo; Adachi, Souichi; Ken-Ichiro Citation
Title Long-term efficacy of bevacizumab a pediatric glioblastoma. Umeda, Katsutsugu; Shibata, Hirofum Author(s) Hiramatsu, Hidefumi; Arakawa, Yoshi Nishiuchi, Ritsuo; Adachi, Souichi; Ken-Ichiro Citation
Long-term efficacy of early versus delayed radiotherapy for low-grade astrocytoma and oligodendroglioma in adults: the EORTC randomised trial
 Long-term efficacy of early versus delayed radiotherapy for low-grade astrocytoma and oligodendroglioma in adults: the EORTC 22845 randomised trial M J van den Bent, D Afra, O de Witte, M Ben Hassel, S
Long-term efficacy of early versus delayed radiotherapy for low-grade astrocytoma and oligodendroglioma in adults: the EORTC 22845 randomised trial M J van den Bent, D Afra, O de Witte, M Ben Hassel, S
Oligodendrogliomas & Oligoastrocytomas
 Oligodendrogliomas & Oligoastrocytomas ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the first national nonprofit organization dedicated solely
Oligodendrogliomas & Oligoastrocytomas ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the first national nonprofit organization dedicated solely
11/27/2017. Modern Treatment of Meningiomas. Disclosures. Modern is Better? No disclosures relevant to this presentation
 Modern Treatment of Meningiomas Michael A. Vogelbaum MD, PhD Professor of Neurosurgery Cleveland Clinic Disclosures No disclosures relevant to this presentation IP and royalties related to drug and device
Modern Treatment of Meningiomas Michael A. Vogelbaum MD, PhD Professor of Neurosurgery Cleveland Clinic Disclosures No disclosures relevant to this presentation IP and royalties related to drug and device
ORE Open Research Exeter
 ORE Open Research Exeter TITLE Temozolomide for high grade glioma AUTHORS Hart, MG; Garside, R; Rogers, G; et al. JOURNAL Cochrane Database Of Systematic Reviews DEPOSITED IN ORE 22 October 2013 This version
ORE Open Research Exeter TITLE Temozolomide for high grade glioma AUTHORS Hart, MG; Garside, R; Rogers, G; et al. JOURNAL Cochrane Database Of Systematic Reviews DEPOSITED IN ORE 22 October 2013 This version
Temozolomide Concomitant and Adjuvant to Radiotherapy in Elderly Patients With Glioblastoma
 Temozolomide Concomitant and Adjuvant to Radiotherapy in Elderly Patients With Glioblastoma Correlation With MGMT Promoter Methylation Status Alba A. Brandes, MD 1 ; Enrico Franceschi, MD 1 ; Alicia Tosoni,
Temozolomide Concomitant and Adjuvant to Radiotherapy in Elderly Patients With Glioblastoma Correlation With MGMT Promoter Methylation Status Alba A. Brandes, MD 1 ; Enrico Franceschi, MD 1 ; Alicia Tosoni,
Efficacy of Treatment for Glioblastoma Multiforme in Elderly Patients (65+): A Retrospective Analysis
: A Retrospective Analysis") Efficacy of Treatment for Glioblastoma Multiforme in Elderly Patients (65+): A Retrospective Analysis Igal Kushnir MD 1 * and Tzahala Tzuk-Shina MD 2 1 Oncology Insitute, Tel Aviv Sourasky Medical Center,
Efficacy of Treatment for Glioblastoma Multiforme in Elderly Patients (65+): A Retrospective Analysis Igal Kushnir MD 1 * and Tzahala Tzuk-Shina MD 2 1 Oncology Insitute, Tel Aviv Sourasky Medical Center,
2017 Diagnostic Slide Session Case 3
 2017 Diagnostic Slide Session Case 3 Andrew Gao, MD Lili-Naz Hazrati, MD, PhD Cynthia Hawkins, MD, PhD Hospital for Sick Children and University of Toronto, Toronto, Canada Disclosures: none Clinical History
2017 Diagnostic Slide Session Case 3 Andrew Gao, MD Lili-Naz Hazrati, MD, PhD Cynthia Hawkins, MD, PhD Hospital for Sick Children and University of Toronto, Toronto, Canada Disclosures: none Clinical History