Concepts for a personalized neurosurgical oncology. XXIV Annual Conference Pietro Paoletti 27. November 2015
|
|
|
- Godwin Sanders
- 5 years ago
- Views:
Transcription



1 Concepts for a personalized neurosurgical oncology Jörg-Christian Tonn Dept. of Neurosurgery Ludwig-Maximilian University München Großhadern Germany XXIV Annual Conference Pietro Paoletti 27. November 2015
 German Cancer Research Foundation (Deutsche")
2 Disclosures Consultant MerckSerono, Roche, medac, Celldex BrainLab, Siemens Grants Deutsche Forschungsgemmeinschaft (DFG) German Cancer Research Foundation (Deutsche Krebshilfe)
3 You can only offer personalized glioma surgery if you obtain a maximum of patient-specific information Microsurgical Resection Stereotactic Biopsy
4 Which glioma? The upcoming WHO classification Molecular marker Diffuse Glioma IDH mut with 1p/19q codel Diffuse Glioma IDH mut no 1p/19q codel Diffuse Glioma no IDH mut + 1p/19q codel IDH 1/2 mutant mutant wildtype 1p/19q codeleted intact intact Histology olidendroglial astrocytic astrocytic WHO grade II or III II or III (rarely IV) IV (rarely II or III) Median OS > 15 years 8-12 years < 2-3 years Weller, Reifenberger, Tonn, Wick, in press 2015
5 Which glioma? The upcoming WHO classification Molecular marker Diffuse Glioma IDH mut with 1p/19q codel Diffuse Glioma IDH mut no 1p/19q codel Diffuse Glioma no IDH mut + 1p/19q codel IDH 1/2 mutant mutant wildtype 1p/19q codeleted intact intact Histology olidendroglial astrocytic astrocytic WHO grade II or III II or III (rarely IV) IV (rarely II or III) Median OS > 15 years 8-12 years < 2-3 years Weller, Reifenberger, Tonn, Wick, in press 2015
6 Which glioma? The upcoming WHO classification Molecular marker Diffuse Glioma IDH mut with 1p/19q codel Diffuse Glioma IDH mut no 1p/19q codel Diffuse Glioma no IDH mut + 1p/19q codel IDH 1/2 mutant mutant wildtype 1p/19q codeleted intact intact Histology olidendroglial astrocytic astrocytic WHO grade II or III II or III (rarely IV) IV (rarely II or III) Median OS > 15 years 8-12 years < 2-3 years Weller, Reifenberger, Tonn, Wick, in press 2015
7 Which glioma? The upcoming WHO classification Molecular marker Diffuse Glioma IDH mut with 1p/19q codel Diffuse Glioma IDH mut no 1p/19q codel Diffuse Glioma no IDH mut + 1p/19q codel IDH 1/2 mutant mutant wildtype 1p/19q codeleted intact intact Histology olidendroglial astrocytic astrocytic WHO grade II or III II or III (rarely IV) IV (rarely II or III) Median OS > 15 years 8-12 years < 2-3 years Weller, Reifenberger, Tonn, Wick, in press 2015
8 Which glioma? The upcoming WHO classification Molecular marker Diffuse Glioma IDH mut with 1p/19q codel Diffuse Glioma IDH mut no 1p/19q codel Diffuse Glioma no IDH mut + 1p/19q codel IDH 1/2 mutant mutant wildtype 1p/19q codeleted intact intact Histology olidendroglial astrocytic astrocytic WHO grade II or III II or III (rarely IV) IV (rarely II or III) Median OS > 15 years 8-12 years < 2-3 years No decision about therapy without molecular marker! Weller, Reifenberger, Tonn, Wick, in press 2015
9 Where is it / extent and borders? Size and localize Is it all the same? Heterogeneity Molecular marker

10 WYSIWYG? T1/T2 +/- CE Perfusion-MRI DSC - CBV DWI PET

11 Outcome prediction in patients with glioblastoma by using imaging, clinical, and genomic biomarkers: focus on the nonenhancing component of the tumor. Jain R et al, Radiology Aug;272(2): rcbv of the non enhancing tumor as the top predictor; also important were KPS, age at diagnosis, and NER crossing the midline not CE-MRI Prospective glioma grading using single-dose dynamic contrast-enhanced perfusion MRI. Jain KK et al, Clin Radiol Jul 4
 Fusion Fusion")

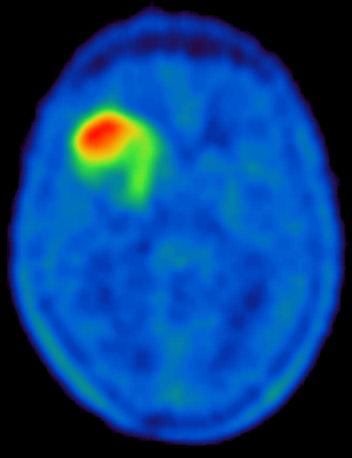
12 18 FET PET High Grade Gliomas T 2 18 FET-PET T 1 (Gd) Fusion Fusion Tumorvolume: T 2 > 18 FET-PET > T 1 -GD La Fougère et al., NeuroOncology 2011


13 Quantitative volumetric analysis of gliomas with sequential MRI and ¹¹C-methionine PET assessment: patterns of integration in therapy planning. Arbizu J, Tejada S, Marti-Climent JM, Diez-Valle R, Prieto E, Quincoces G, Vigil C, Idoate MA, Zubieta JL, Peñuelas I, Richter JA. Eur J Nucl Med Mol Imaging. 2012;39:771-81
14











15 Prognostic value of 18 FET-PET BTV for the clinical course in newly diagnosed glioblastoma Suchorska et al, Neurology, 2015 A 70% of GB were larger in 18 FET-PET than in CE-MRI BTV B R R R L L L R L Multivariate Analysis OS Factor MGMT methylation p < KPS p < TAC p < BTV ( 18 FET-PET) p < 0.001
16 Where is it / extent and borders? Size and localize extent and resection / extent of resection Is it all the same?
17 Volume 14 ml 113 ml (87,5% no CE)
18 Volume 14 ml 113 ml (87,5% no CE)
19

20 Microsurgery Improved results due to fluorescence guided resection (Stummer et al., Lancet Oncol 2006) /139 p < white light 25 47/131 ALA WL Parameter overall survival multivariate p value ALA UV-light Residual tumor no / yes p < KPS 80 / > no residual tumor residual tumor Age 55 / > Eloquent areas no / yes
 Fluorescence Guided Resection (5-ALA): Overall survival stratified by residual tumor volume 1.0 0.9 0.8 0.7 0.")
21 overall survival (Stummer et al., Lancet Oncol 2006) Fluorescence Guided Resection (5-ALA): Overall survival stratified by residual tumor volume p=0.34 Time [months] 0 ccm > ccm > 1.5 ccm p=
22 OS 16, 13.8, 12.8, 12.5 months
23 Whereas the 78% threshold represents the minimum value at which a survival benefit is seen, RPA selected 95% as the most significant predictor of survival in patients with GBM, emphasizing the added value of a complete resection Neverthless, the usual limitations of a retrospective analysis still apply, particularly with respect to the risk of selection bias.



24 Ann Oncol Dec;24(12):
:2057-64 MGMT+/- MGMT+/- Comparison of two different TMZ re-challenge regimens: Arm A: 1 week on/1 week off vs.")
25 Complete resection of contrast enhancing tumor volume is associated with improved survival in recurrent GB Arm A Arm B DIRECTOR trial Weller M et al: Clin Cancer Res. 2015; 21(9): MGMT+/- MGMT+/- Comparison of two different TMZ re-challenge regimens: Arm A: 1 week on/1 week off vs. Arm B: 3 weeks on/1 week off 25


 regimens at recurrence of glioblastoma GBM")

26 Complete resection of contrast enhancing tumour volume is associated with improved survival in recurrent GB Does surgery pe se matter or only complete resection? current analysis based on the DIRECTOR trial, a prospective randomized multicenter trial comparing two dose-intensified temozolomide (TMZ) regimens at recurrence of glioblastoma GBM Primary therapy Recurrence Analysis EOR for PFS/OS Surgery/No surgery TMZ 1week on/1week off TMZ 3 weeks on/1week off 26 Suchorska et al, ASCO 2015 KLINIKUM DER UNIVERSITÄT MÜNCHEN NEUROSURGICAL DEPARTMENT
27 Complete resection of contrast enhancing tumor volume is associated with improved survival in recurrent GB 27 Results: Surgery for recurrence Yes 71 No 34 p Age at diagnosis Median (years) Range (years) Gender: N (%) Male 48 (67.6) 21 (61.8) Female 23 (32.4) 13 (38.2) MGMT promoter: N (%) Methylated 31 (43.7) 15 (44.1) Unmethylated 40 (56.3) 19 (55.9) First-line therapy: Number of maintenance TMZ cycles Median Range Time to first progression (months) Median Range Tumor volume at recurrence (cm 3 ) Median Range Tumor volume at study entry (cm 3 ) Median <0.001 Range KPS at study entry: N (%) (56.3) 20 (58.8) (31.0) 9 (26.5) <70 9 (12.7) 5 (14.7) Steroids at study entry: N (%) Yes KLINIKUM 20 (31.3) DER UNIVERSITÄT 8 (28.6) MÜNCHEN NEUROSURGICAL DEPARTMENT No 44 (68.7) 20 (71.4)
28 Complete resection of contrast enhancing tumour volume is associated with improved survival in recurrent GB Results: Re-operation: yes/no yes (n=71) no (n=34) yes (n=71) no (n=34) p = 0.63 p = 0.36 p = 0.63 Progression Free Survival2 (months) Post Recurrence Survival (months) 28 Suchorska et al, ASCO 2015 KLINIKUM DER UNIVERSITÄT MÜNCHEN NEUROSURGICAL DEPARTMENT
29 Complete resection of contrast enhancing tumour volume is associated with improved survival in recurrent GB Results: Extent of resection GTR (n=40) incomplete (n=19) GTR (n=40) incomplete (n=19) p = 0.02 p <0.001 Progression Free Survival2 (months) Post Recurrence Survival (months) Suchorska et al, ASCO 2015 KLINIKUM DER UNIVERSITÄT MÜNCHEN NEUROSURGICAL DEPARTMENT
30 Complete resection of contrast enhancing tumour volume is associated with improved survival in recurrent GB Results: Extent of resection GTR (n=40) incomplete (n=19) no surgery (n=34) GTR (n=40) incomplete (n=19) no surgery (n=34) p = p = Progression Free Survival2 (months) Post Recurrence Survival (months) 30 Suchorska et al, ASCO 2015 KLINIKUM DER UNIVERSITÄT MÜNCHEN NEUROSURGICAL DEPARTMENT
31 Complete resection of contrast enhancing tumour volume is associated with improved survival in recurrent GB Results: Multivariate analysis Hazard ratio and p 95% CI Extent of resection: GTR versus incomplete 0.42 ( ) Age at study entry: versus 55+ years 1.25 ( ) MGMT promoter: methylated versus unmethylated 0.58 ( ) KPS at study entry: % versus KPS 50-80% 0.82 ( ) Steroids at study entry: no versus yes 0.82 ( ) Results: QoL analysis Patients receiving surgery had higher cognitive functioning values after 8 weeks (p=0.046) 31 Patients who received an incomplete resection were more likely to suffer from general motor dysfunction (p=0.04) and to have a worse global health status (p=0.008) compared to those who received GTR Suchorska et al, ASCO 2015 KLINIKUM DER UNIVERSITÄT MÜNCHEN NEUROSURGICAL DEPARTMENT


32

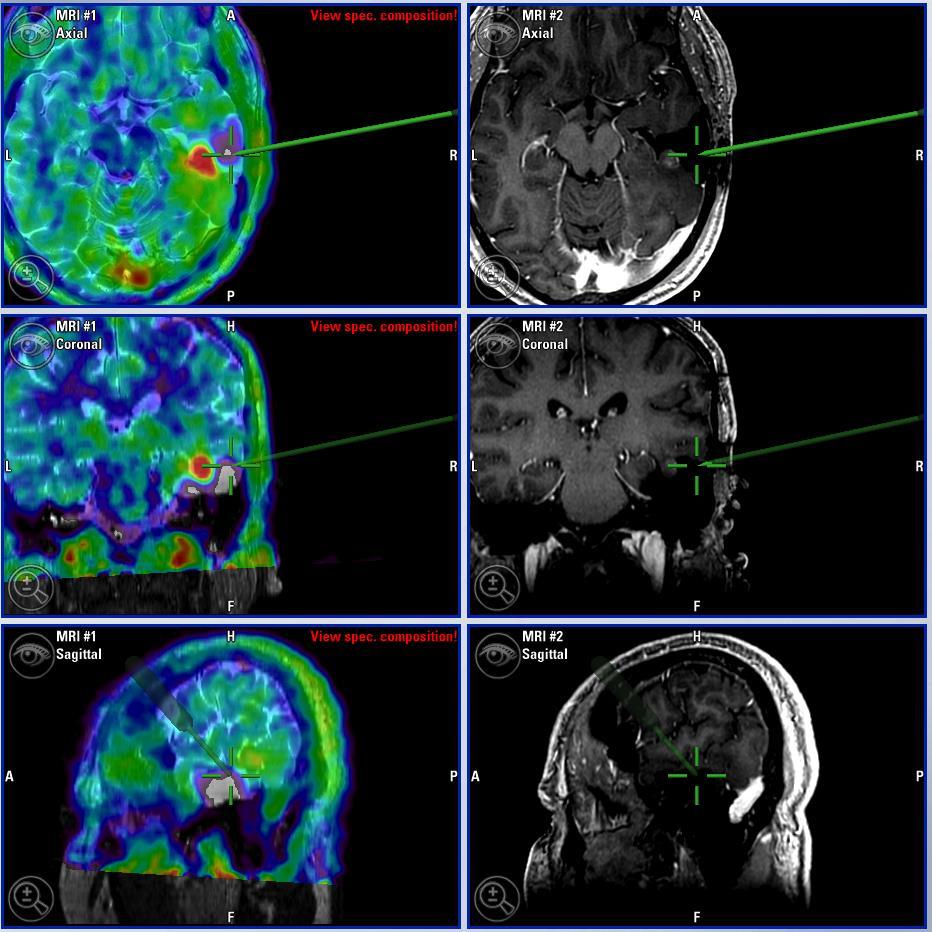
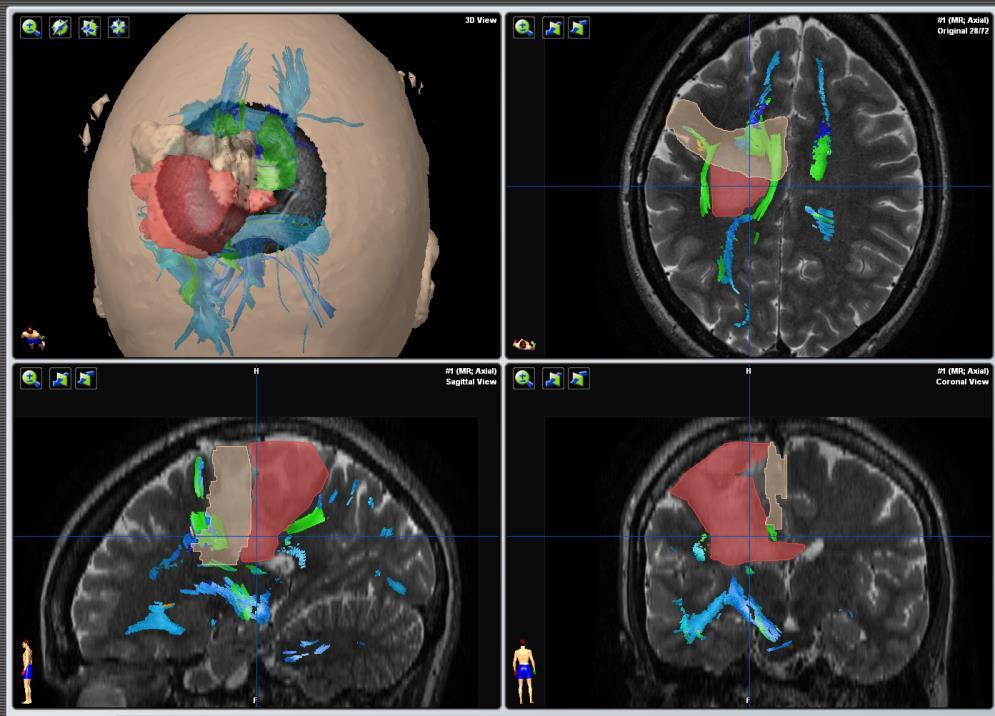
33 Intraoperative Neuronavigation Multiparametric Imaging

34 Intraoperative Neuronavigation Intraoperative Imaging update via ius

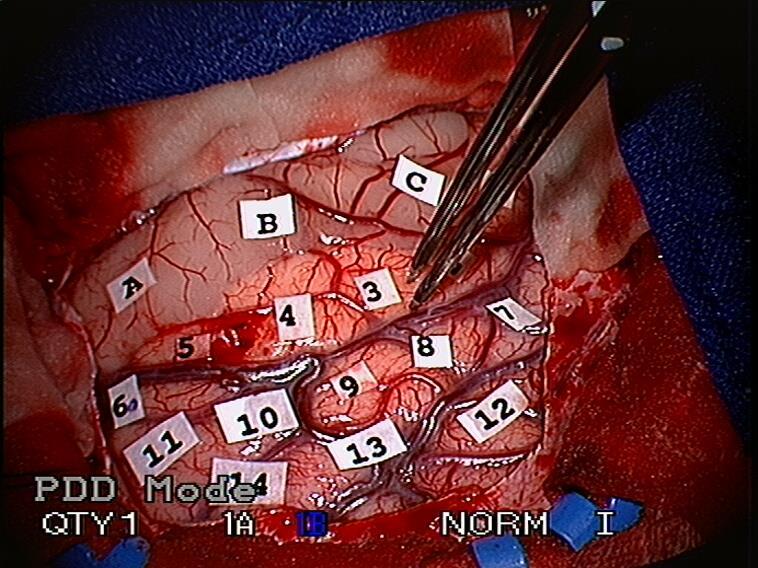
35 Gold-Standard for preservation of function?
36 Impact of intraoperative stimulation brain mapping on glioma surgery outcome: a meta-analysis. De Witt Hamer PC et al, J Clin Oncol Jul 10;30(20): Permanent severe neurological deficit: 3.4% with mapping 8.2% without mapping gross total resection (as by post-op MRI): 75% with mapping 58% without mapping
37 Where is it / extent and borders? Size and localize Is it all the same? Heterogeneity Molecular marker
:12550-5 samples from CE regions resembled the proneural, classical, or mesenchymal subtypes of GBM - samples from the NE regions predominantly resembled the neural")
38 MRI-localized biopsies reveal subtype-specific differences in molecular and cellular composition at the margins of glioblastoma Gill BJ et al, Proc Natl Acad Sci U S A. 2014;111(34): samples from CE regions resembled the proneural, classical, or mesenchymal subtypes of GBM - samples from the NE regions predominantly resembled the neural subtype









39 3,0 2,0 1,0 0, ,0 6,0 5,0 4,0 PFS (2 yrs): 78%, 35%, 26% fraction hotspot 2% - 90% Size of hotspot: no prognostic relevance 3, ,0 2,0 1,0 0, ,0 45 % of suspected LGG were anaplastic WHO III or GBM! 6,0 5,0 4,0 Kunz et al, NeuroOncol. 2011; 13:307 3, homogeneous increasing TAC heterogeneous TAC homogeneous decreasing TAC p=0.002 Thon N et al, Int J Cancer 2015 n=98 censored
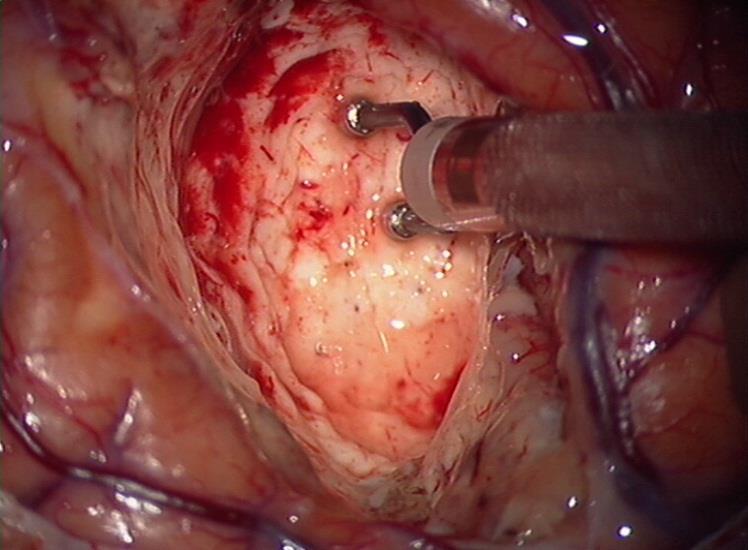
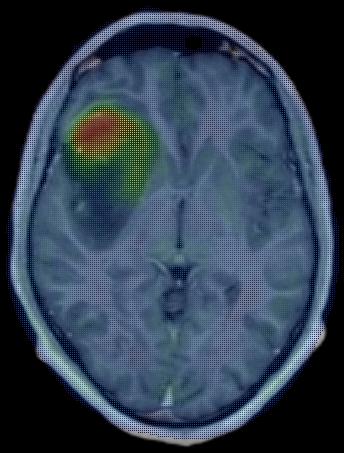
40 PET- guided microsurgical resection

41 PET- guided microsurgical resection Focus adjusted resection

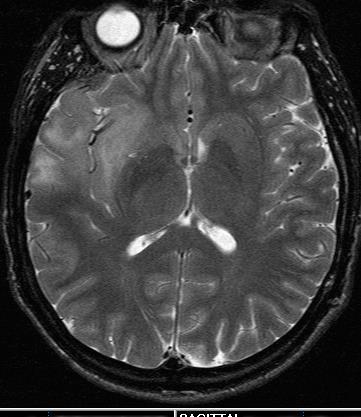
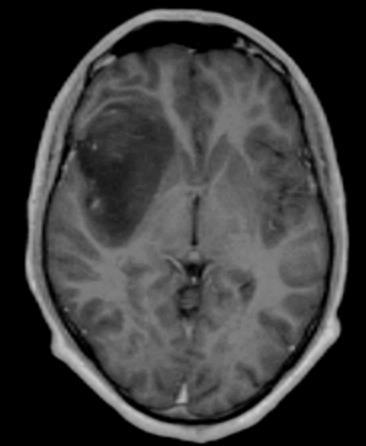
42 Preoperative MRI/FET-PET (36y/o female w suspected LGG WHO II)

43 Postoperative MRI/FET-PET after focus-adjusted resection ( WHO III)


44
45
 Thon et al: J Neuropathol Exp Neurol,")
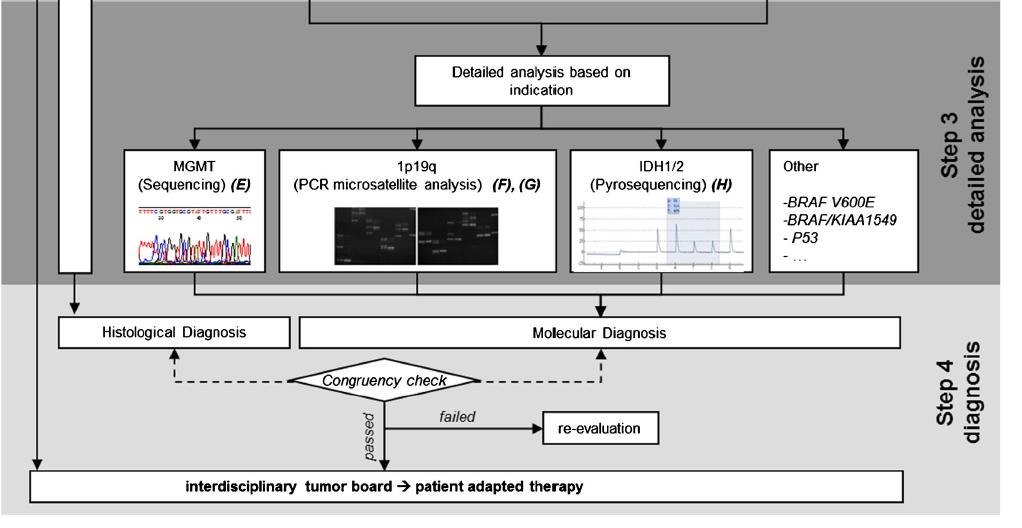
46 Homogeneous distribution of biomarker (Tp53, MGMT, LOH1p/19q, IDH1) solid tumor Risk of false negative results infiltrative zone Success rate of molecular-genetic analyses: > 98% Morbidity rate: < 1% (> 900 biopsy procedures ) Thon et al: J Neuropathol Exp Neurol, 09
47 Where is it / extent and borders? Size and localize Is it all the same? Heterogeneity Molecular marker
48 unmethylated MGMT promotor MGMT promotor region MGMT gene active Transcription/Translation TMZresistent MGMT promotor methylation CH CH CH CH CH 3 3 MGMT promotor region MGMT gene inactive Transcription/Translation TMZsensitive
49 unmethylated MGMT promotor MGMT promotor region MGMT gene active Transcription/Translation TMZresistent MGMT promotor methylation CH CH CH CH CH 3 3 MGMT promotor region MGMT gene inactive Transcription/Translation TMZsensitive Hegi et al 2008

50 Thon et al 2010 Hegi et al 2008
51 Temozolomide chemotherapy alone versus radiotherapy alone for malignant astrocytoma in the elderly: the NOA-08 randomised phase 3 trial. Wick W et al, Lancet Oncol :707 MGMT pos + TMZ MGMT neg + TMZ OS 373 pts, age > 65 ys, KPS > 60
52 Phase III Trial of Chemoradiotherapy for Anaplastic Oligodendroglioma: Long-Term Results of RTOG Cairncross G et al, J Clin Oncol :337 Epub 2012 LOH 1p/19q PCV+RT vs RT only 14.7 vs 7.3 yrs; p = 0.03 no codeletion PCV+RT vs RT only 2.6 vs 2.7 yrs; p = 0.39
 Weller, Reifenberger, Tonn, Wick, in press 2015 Biomarker")
53 WHO-Grad-II/III/IV-Glioma IDH-1/2 wildtype mutant Histology WHO-Grade IV WHO-Grade II/III WHO-Grade II/III/(IV) Age > 65 MGMT - RT MGMT + TMZ or TMZ/RT TMZ Age 65 MGMT - MGMT + RT TMZ/RT TMZ 1p/19q intact TMZ or PCV or RT 1p/19q codeletet RT/PCV (TMZ/RT TMZ) Weller, Reifenberger, Tonn, Wick, in press 2015 Biomarker Therapy

54 Personalized tumor therapy
Radioterapia no Tratamento dos Gliomas de Baixo Grau
 Radioterapia no Tratamento dos Gliomas de Baixo Grau Dr. Luis Souhami University Montreal - Canada Low Grade Gliomas Relatively rare Heterogeneous, slow growing tumors WHO Classification Grade I Pilocytic
Radioterapia no Tratamento dos Gliomas de Baixo Grau Dr. Luis Souhami University Montreal - Canada Low Grade Gliomas Relatively rare Heterogeneous, slow growing tumors WHO Classification Grade I Pilocytic
Systemic Treatment. Third International Neuro-Oncology Course. 23 May 2014
 Low-Grade Astrocytoma of the CNS: Systemic Treatment Third International Neuro-Oncology Course São Paulo, Brazil 23 May 2014 John de Groot, MD Associate Professor, Neuro-Oncology UT MD Anderson Cancer
Low-Grade Astrocytoma of the CNS: Systemic Treatment Third International Neuro-Oncology Course São Paulo, Brazil 23 May 2014 John de Groot, MD Associate Professor, Neuro-Oncology UT MD Anderson Cancer
성균관대학교삼성창원병원신경외과학교실신경종양학 김영준. KNS-MT-03 (April 15, 2015)
") 성균관대학교삼성창원병원신경외과학교실신경종양학 김영준 INTRODUCTIONS Low grade gliomas (LGG) - heterogeneous group of tumors with astrocytic, oligodendroglial, ependymal, or mixed cellular histology - In adults diffuse, infiltrating
성균관대학교삼성창원병원신경외과학교실신경종양학 김영준 INTRODUCTIONS Low grade gliomas (LGG) - heterogeneous group of tumors with astrocytic, oligodendroglial, ependymal, or mixed cellular histology - In adults diffuse, infiltrating
A clinical perspective on neuropathology and molecular genetics in brain tumors
 A clinical perspective on neuropathology and molecular genetics in brain tumors M.J. van den Bent Erasmus MC Cancer Institute Rotterdam, the Netherlands Disclosures Member speakersbureau: MSD Consultancy:
A clinical perspective on neuropathology and molecular genetics in brain tumors M.J. van den Bent Erasmus MC Cancer Institute Rotterdam, the Netherlands Disclosures Member speakersbureau: MSD Consultancy:
Contemporary Management of Glioblastoma
 Contemporary Management of Glioblastoma Incidence Rates of Primary Brain Tumors Central Brain Tumor Registry of the United States, 1992-1997 100 Number of Cases per 100,000 Population 10 1 0.1 x I x I
Contemporary Management of Glioblastoma Incidence Rates of Primary Brain Tumors Central Brain Tumor Registry of the United States, 1992-1997 100 Number of Cases per 100,000 Population 10 1 0.1 x I x I
21/03/2017. Disclosure. Practice Changing Articles in Neuro Oncology for 2016/17. Gliomas. Objectives. Gliomas. No conflicts to declare
 Practice Changing Articles in Neuro Oncology for 2016/17 Disclosure No conflicts to declare Frances Cusano, BScPharm, ACPR April 21, 2017 Objectives Gliomas To describe the patient selection, methodology
Practice Changing Articles in Neuro Oncology for 2016/17 Disclosure No conflicts to declare Frances Cusano, BScPharm, ACPR April 21, 2017 Objectives Gliomas To describe the patient selection, methodology
UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS
 UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS Antonio M. Omuro Department of Neurology Memorial Sloan-Kettering Cancer Center II International Neuro-Oncology Congress Sao Paulo, 08/17/12 CHALLENGES IN
UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS Antonio M. Omuro Department of Neurology Memorial Sloan-Kettering Cancer Center II International Neuro-Oncology Congress Sao Paulo, 08/17/12 CHALLENGES IN
Clinical Trials for Adult Brain Tumors - the Imaging Perspective
 Clinical Trials for Adult Brain Tumors - the Imaging Perspective Whitney B. Pope, M.D., Ph.D. Department of Radiology David Geffen School of Medicine at UCLA August 22, 2015 1 Disclosure of Financial Relationships
Clinical Trials for Adult Brain Tumors - the Imaging Perspective Whitney B. Pope, M.D., Ph.D. Department of Radiology David Geffen School of Medicine at UCLA August 22, 2015 1 Disclosure of Financial Relationships
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
Low grade glioma: a journey towards a cure
 Editorial Page 1 of 5 Low grade glioma: a journey towards a cure Ali K. Choucair SIU School of Medicine, Springfield, IL, USA Correspondence to: Ali K. Choucair, MD. Professor of Neurology, Director of
Editorial Page 1 of 5 Low grade glioma: a journey towards a cure Ali K. Choucair SIU School of Medicine, Springfield, IL, USA Correspondence to: Ali K. Choucair, MD. Professor of Neurology, Director of
Precision medicine for gliomas
 Precision medicine for YAZMIN ODIA, MD MS LEAD PHYSICIAN OF MEDICAL NEURO-ONCOLOGY DISCLOSURES Novocure: Advisory Board for Optune in No other financial conflicts of interest Glioma OVERVIEW INFILTRATIVE,
Precision medicine for YAZMIN ODIA, MD MS LEAD PHYSICIAN OF MEDICAL NEURO-ONCOLOGY DISCLOSURES Novocure: Advisory Board for Optune in No other financial conflicts of interest Glioma OVERVIEW INFILTRATIVE,
Imaging for suspected glioma
 Imaging for suspected glioma 1.1.1 Offer standard structural MRI (defined as T2 weighted, FLAIR, DWI series and T1 pre- and post-contrast volume) as the initial diagnostic test for suspected glioma, unless
Imaging for suspected glioma 1.1.1 Offer standard structural MRI (defined as T2 weighted, FLAIR, DWI series and T1 pre- and post-contrast volume) as the initial diagnostic test for suspected glioma, unless
Examining large groups of cancer patients to identify ways of predicting which therapies cancers might respond to.
 Stratified Medicine Examining large groups of cancer patients to identify ways of predicting which therapies cancers might respond to. Looking in detail at cancer cells and their genetic make up. Permit
Stratified Medicine Examining large groups of cancer patients to identify ways of predicting which therapies cancers might respond to. Looking in detail at cancer cells and their genetic make up. Permit
Concomitant (without adjuvant) temozolomide and radiation to treat glioblastoma: A retrospective study
 temozolomide and radiation to treat glioblastoma: A retrospective study") Concomitant (without adjuvant) temozolomide and radiation to treat glioblastoma: A retrospective study T Sridhar 1, A Gore 1, I Boiangiu 1, D Machin 2, R P Symonds 3 1. Department of Oncology, Leicester
Concomitant (without adjuvant) temozolomide and radiation to treat glioblastoma: A retrospective study T Sridhar 1, A Gore 1, I Boiangiu 1, D Machin 2, R P Symonds 3 1. Department of Oncology, Leicester
Antiangiogenic drugs in unresectable glioblastoma. Dra. Carmen Balañá. /
 Antiangiogenic drugs in unresectable glioblastoma Dra. Carmen Balañá. / Outcome for unresectable GBM Overall survival for unresectable GBM without further treatment is: 3 months at most. Radiotherapy increases
Antiangiogenic drugs in unresectable glioblastoma Dra. Carmen Balañá. / Outcome for unresectable GBM Overall survival for unresectable GBM without further treatment is: 3 months at most. Radiotherapy increases
Prognostic value of ADC in glioblastoma multiforme and its correlation with survival and MGMT promoter methylation status.
 Prognostic value of ADC in glioblastoma multiforme and its correlation with survival and MGMT promoter methylation status. R. Zalazar, M.D. Hernández, M. Páramo, P. Slon, M. Millor Muruzabal, J. Solorzano
Prognostic value of ADC in glioblastoma multiforme and its correlation with survival and MGMT promoter methylation status. R. Zalazar, M.D. Hernández, M. Páramo, P. Slon, M. Millor Muruzabal, J. Solorzano
Limited role for extended maintenance temozolomide for newly diagnosed glioblastoma
 Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 2017 Limited role for extended maintenance temozolomide for newly diagnosed
Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 2017 Limited role for extended maintenance temozolomide for newly diagnosed
Classification of Diffuse Gliomas: Progress, Pearls and Pitfalls. Rob Macaulay Neuropathologist, MCC October 21, 2017
 Classification of Diffuse Gliomas: Progress, Pearls and Pitfalls Rob Macaulay Neuropathologist, MCC October 21, 2017 Objectives Explain why the designation high grade glioma is preferable to GBM for intraoperative
Classification of Diffuse Gliomas: Progress, Pearls and Pitfalls Rob Macaulay Neuropathologist, MCC October 21, 2017 Objectives Explain why the designation high grade glioma is preferable to GBM for intraoperative
Zurich Open Repository and Archive. Long-term survival of glioblastoma patients treated with radiotherapy and lomustine plus temozolomide
 University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich http://www.zora.uzh.ch Year: 2009 Long-term survival of glioblastoma patients treated with radiotherapy and lomustine
University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich http://www.zora.uzh.ch Year: 2009 Long-term survival of glioblastoma patients treated with radiotherapy and lomustine
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM ANAPLASTIC GLIOMAS CNS Site Group Anaplastic Gliomas Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM ANAPLASTIC GLIOMAS CNS Site Group Anaplastic Gliomas Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
Management of Glioma: The Basics Glioma Update The clinical challenge. Glioma a malignant disease of the CNS
 Management of Glioma: The Basics Glioma Update 3 oger Stupp, MD Department of Oncology & Cancer Center University Hospital Zurich, Switzerland (roger.stupp@usz.ch) Bern, 3. August 3 The clinical challenge
Management of Glioma: The Basics Glioma Update 3 oger Stupp, MD Department of Oncology & Cancer Center University Hospital Zurich, Switzerland (roger.stupp@usz.ch) Bern, 3. August 3 The clinical challenge
Chemotherapy plus Radiotherapy versus Radiotherapy Alone for Patients with Anaplastic Oligodendroglioma: Long Term Results of RTOG 9402
 Chemotherapy plus Radiotherapy versus Radiotherapy Alone for Patients with Anaplastic Oligodendroglioma: Long Term Results of RTOG 9402 Gregory Cairncross, Meihua Wang, Edward Shaw, Berndt Scheithauer
Chemotherapy plus Radiotherapy versus Radiotherapy Alone for Patients with Anaplastic Oligodendroglioma: Long Term Results of RTOG 9402 Gregory Cairncross, Meihua Wang, Edward Shaw, Berndt Scheithauer
What s new in Management of Gliomas
 What s new in Management of Gliomas Allan James Consultant Clinical Oncologist Beatson West of Scotland Cancer Centre Glasgow In The Beginning (1978) All (High Grade) Gliomas Were The Same Background :
What s new in Management of Gliomas Allan James Consultant Clinical Oncologist Beatson West of Scotland Cancer Centre Glasgow In The Beginning (1978) All (High Grade) Gliomas Were The Same Background :
Zurich Open Repository and Archive. Long-term survival of glioblastoma patients treated with radiotherapy and lomustine plus temozolomide
 University of Zurich Zurich Open Repository and Archive Winterthurerstr. 19 CH-857 Zurich http://www.zora.uzh.ch Year: 29 Long-term survival of glioblastoma patients treated with radiotherapy and lomustine
University of Zurich Zurich Open Repository and Archive Winterthurerstr. 19 CH-857 Zurich http://www.zora.uzh.ch Year: 29 Long-term survival of glioblastoma patients treated with radiotherapy and lomustine
Related Policies None
 Medical Policy MP 2.04.113 BCBSA Ref. Policy: 2.04.113 Last Review: 05/30/2018 Effective Date: 05/30/2018 Section: Medicine Related Policies None DISCLAIMER Our medical policies are designed for informational
Medical Policy MP 2.04.113 BCBSA Ref. Policy: 2.04.113 Last Review: 05/30/2018 Effective Date: 05/30/2018 Section: Medicine Related Policies None DISCLAIMER Our medical policies are designed for informational
University of Zurich. Temozolomide and MGMT forever? Zurich Open Repository and Archive. Weller, M. Year: 2010
 University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich Year: 2010 Temozolomide and MGMT forever? Weller, M Weller, M (2010). Temozolomide and MGMT forever? Neuro-Oncology,
University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich Year: 2010 Temozolomide and MGMT forever? Weller, M Weller, M (2010). Temozolomide and MGMT forever? Neuro-Oncology,
The New WHO Classification and the Role of Integrated Molecular Profiling in the Diagnosis of Malignant Gliomas
 The New WHO Classification and the Role of Integrated Molecular Profiling in the Diagnosis of Malignant Gliomas Stefan Prokop, MD Neuropathology Fellow Hospital of the University of Pennsylvania Background
The New WHO Classification and the Role of Integrated Molecular Profiling in the Diagnosis of Malignant Gliomas Stefan Prokop, MD Neuropathology Fellow Hospital of the University of Pennsylvania Background
Oncological Management of Brain Tumours. Anna Maria Shiarli SpR in Clinical Oncology 15 th July 2013
 Oncological Management of Brain Tumours Anna Maria Shiarli SpR in Clinical Oncology 15 th July 2013 Outline General considerations of Primary Brain Tumours: epidemiology, pathology, presentation. Diagnosis
Oncological Management of Brain Tumours Anna Maria Shiarli SpR in Clinical Oncology 15 th July 2013 Outline General considerations of Primary Brain Tumours: epidemiology, pathology, presentation. Diagnosis
Neuro-Oncology. Martin J. van den Bent. Department of Neuro-oncology/Neurology, Erasmus M.C. Cancer Institute, Rotterdam, Netherlands
 Neuro-Oncology Neuro-Oncology 16(12), 1570 1574, 2014 doi:10.1093/neuonc/nou297 Advance Access date 29 October 2014 Practice changing mature results of RTOG study 9802: another positive PCV trial makes
Neuro-Oncology Neuro-Oncology 16(12), 1570 1574, 2014 doi:10.1093/neuonc/nou297 Advance Access date 29 October 2014 Practice changing mature results of RTOG study 9802: another positive PCV trial makes
Prognostic or predictive value of MGMT promoter methylation in gliomas depends on IDH1 mutation
 Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 2013 Prognostic or predictive value of MGMT promoter methylation in gliomas
Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 2013 Prognostic or predictive value of MGMT promoter methylation in gliomas
WHO 2016 CNS Tumor Classification Update. DISCLOSURES (Arie Perry, MD) PATTERN RECOGNITION. Arie Perry, M.D. Director, Neuropathology
 PATTERN RECOGNITION. Arie Perry, M.D. Director, Neuropathology") WHO 2016 CNS Tumor Classification Update Arie Perry, M.D. Director, Neuropathology DISCLOSURES (Arie Perry, MD) I have no financial relationships to disclose. - and - I will not discuss off label use or
WHO 2016 CNS Tumor Classification Update Arie Perry, M.D. Director, Neuropathology DISCLOSURES (Arie Perry, MD) I have no financial relationships to disclose. - and - I will not discuss off label use or
See the corresponding editorial in this issue, pp 1 2. J Neurosurg 115:3 8, An extent of resection threshold for newly diagnosed glioblastomas
 See the corresponding editorial in this issue, pp 1 2. J Neurosurg 115:3 8, 2011 An extent of resection threshold for newly diagnosed glioblastomas Clinical article Nader Sanai, M.D., 1 Mei-Yin Polley,
See the corresponding editorial in this issue, pp 1 2. J Neurosurg 115:3 8, 2011 An extent of resection threshold for newly diagnosed glioblastomas Clinical article Nader Sanai, M.D., 1 Mei-Yin Polley,
Hypofractionated radiation therapy for glioblastoma
 Hypofractionated radiation therapy for glioblastoma Luis Souhami, MD, FASTRO Professor McGill University Department of Oncology, Division of Radiation Oncology Montreal Canada McGill University Health
Hypofractionated radiation therapy for glioblastoma Luis Souhami, MD, FASTRO Professor McGill University Department of Oncology, Division of Radiation Oncology Montreal Canada McGill University Health
Carmustine implants and Temozolomide for the treatment of newly diagnosed high grade glioma
 National Institute for Health and Clinical Excellence Health Technology Appraisal Carmustine implants and Temozolomide for the treatment of newly diagnosed high grade glioma Personal statement Conventional
National Institute for Health and Clinical Excellence Health Technology Appraisal Carmustine implants and Temozolomide for the treatment of newly diagnosed high grade glioma Personal statement Conventional
Prior to 1993, the only data available in the medical
 Neuro-Oncology Prospective clinical trials of intracranial low-grade glioma in adults and children Edward G. Shaw 1 and Jeffrey H. Wisoff Department of Radiation Oncology, Wake Forest University School
Neuro-Oncology Prospective clinical trials of intracranial low-grade glioma in adults and children Edward G. Shaw 1 and Jeffrey H. Wisoff Department of Radiation Oncology, Wake Forest University School
Corporate Medical Policy
 Corporate Medical Policy Analysis of MGMT Promoter Methylation in Malignant Gliomas File Name: Origination: Last CAP Review: Next CAP Review: Last Review: analysis_of_mgmt_promoter_methylation_in_malignant_gliomas
Corporate Medical Policy Analysis of MGMT Promoter Methylation in Malignant Gliomas File Name: Origination: Last CAP Review: Next CAP Review: Last Review: analysis_of_mgmt_promoter_methylation_in_malignant_gliomas
Scottish Medicines Consortium
 Scottish Medicines Consortium temozolomide 5, 20, 100 and 250mg capsules (Temodal ) Schering Plough UK Ltd No. (244/06) New indication: for the treatment of newly diagnosed glioblastoma multiforme concomitantly
Scottish Medicines Consortium temozolomide 5, 20, 100 and 250mg capsules (Temodal ) Schering Plough UK Ltd No. (244/06) New indication: for the treatment of newly diagnosed glioblastoma multiforme concomitantly
NICE guideline Published: 11 July 2018 nice.org.uk/guidance/ng99
 Brain tumours (primary) and brain metastases in adults NICE guideline Published: 11 July 2018 nice.org.uk/guidance/ng99 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Brain tumours (primary) and brain metastases in adults NICE guideline Published: 11 July 2018 nice.org.uk/guidance/ng99 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
CNS SESSION 3/8/ th Multidisciplinary Management of Cancers: A Case based Approach
 CNS SESSION Chair: Ruben Fragoso, MD/PhD UC Davis Fellow: Michael Cardenas, MD UC Davis Panel: Gordon Li, MD Stanford Seema Nagpal, MD Stanford Jennie Taylor, MD UCSF HPI: 46 yo right handed woman who
CNS SESSION Chair: Ruben Fragoso, MD/PhD UC Davis Fellow: Michael Cardenas, MD UC Davis Panel: Gordon Li, MD Stanford Seema Nagpal, MD Stanford Jennie Taylor, MD UCSF HPI: 46 yo right handed woman who
MOLECULAR DIAGNOSTICS OF GLIOMAS
 MOLECULAR DIAGNOSTICS OF GLIOMAS Arie Perry, M.D. Director, Neuropathology Division DIFFUSE GLIOMAS Cell types Astrocytomas (A) Oligodendrogliomas (O) Mixed oligoastrocytoma (MOA) Three WHO grades: II,
MOLECULAR DIAGNOSTICS OF GLIOMAS Arie Perry, M.D. Director, Neuropathology Division DIFFUSE GLIOMAS Cell types Astrocytomas (A) Oligodendrogliomas (O) Mixed oligoastrocytoma (MOA) Three WHO grades: II,
3-D conformal radiotherapy with concomitant and adjuvant temozolomide for patients with glioblastoma multiforme and evaluation of prognostic factors
 research article 213 3-D conformal radiotherapy with concomitant and adjuvant temozolomide for patients with glioblastoma multiforme and evaluation of prognostic factors Yilmaz Tezcan and Mehmet Koc Department
research article 213 3-D conformal radiotherapy with concomitant and adjuvant temozolomide for patients with glioblastoma multiforme and evaluation of prognostic factors Yilmaz Tezcan and Mehmet Koc Department
Case Presentation: USCAP Jason T. Huse, MD, PhD Assistant Member Department of Pathology Memorial Sloan Kettering Cancer Center
 Case Presentation: USCAP 2016 Jason T. Huse, MD, PhD Assistant Member Department of Pathology Memorial Sloan Kettering Cancer Center Case History 53 year old female with a long standing history of migraines
Case Presentation: USCAP 2016 Jason T. Huse, MD, PhD Assistant Member Department of Pathology Memorial Sloan Kettering Cancer Center Case History 53 year old female with a long standing history of migraines
RINDOPEPIMUT (CDX-110) IN GLIOBLASTOMA
 IN GLIOBLASTOMA") RINDOPEPIMUT (CDX-110) IN GLIOBLASTOMA MULTIFORM GEINO 2014 Dra Estela Pineda Madrid Hospital Clínic Barcelona EGFRvIII in glioblastoma multiform The most common mutation of EGFR in GBM Expressed in 30%
RINDOPEPIMUT (CDX-110) IN GLIOBLASTOMA MULTIFORM GEINO 2014 Dra Estela Pineda Madrid Hospital Clínic Barcelona EGFRvIII in glioblastoma multiform The most common mutation of EGFR in GBM Expressed in 30%
What yield in the last decade about Molecular Diagnostics in Neuro
 What yield in the last decade about Molecular Diagnostics in Neuro Oncology? Raphael Salles S.Medeiros Neuropathologist at HC FMUSP Clinical Research Project Manager at Oncology department at Hospital
What yield in the last decade about Molecular Diagnostics in Neuro Oncology? Raphael Salles S.Medeiros Neuropathologist at HC FMUSP Clinical Research Project Manager at Oncology department at Hospital
Technology appraisal guidance Published: 27 June 2007 nice.org.uk/guidance/ta121
 Carmustine implants and temozolomide for the treatment of newly diagnosed high-grade glioma Technology appraisal guidance Published: 27 June 2007 nice.org.uk/guidance/ta121 NICE 2018. All rights reserved.
Carmustine implants and temozolomide for the treatment of newly diagnosed high-grade glioma Technology appraisal guidance Published: 27 June 2007 nice.org.uk/guidance/ta121 NICE 2018. All rights reserved.
Gliomas in the 2016 WHO Classification of CNS Tumors
 Gliomas in the 2016 WHO Classification of CNS Tumors Hindi N Al-Hindi, MD, FCAP Consultant Neuropathologist and Head Section of Anatomic Pathology Department of Pathology and Laboratory Medicine King Faisal
Gliomas in the 2016 WHO Classification of CNS Tumors Hindi N Al-Hindi, MD, FCAP Consultant Neuropathologist and Head Section of Anatomic Pathology Department of Pathology and Laboratory Medicine King Faisal
To analyse whether ADC values have a correlation with survival or EGFR amplification status in glioblastoma
 To analyse whether ADC values have a correlation with survival or EGFR amplification status in glioblastoma R. Zalazar, M. Páramo, M. Hernández, P. Domínguez, J.Etxano, P.García Barquín, H.Quiceno Arias,
To analyse whether ADC values have a correlation with survival or EGFR amplification status in glioblastoma R. Zalazar, M. Páramo, M. Hernández, P. Domínguez, J.Etxano, P.García Barquín, H.Quiceno Arias,
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM LOW GRADE GLIOMAS CNS Site Group Low Grade Gliomas Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM LOW GRADE GLIOMAS CNS Site Group Low Grade Gliomas Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING
Brain Tumors: Radiologic Perspective
 Brain Tumors: Radiologic Perspective Alberto Bizzi, M.D. Neuroradiology Humanitas Research Hospital Milan, Italy The job of the neuroradiologist in the work-up of brain tumors has quite changed in the
Brain Tumors: Radiologic Perspective Alberto Bizzi, M.D. Neuroradiology Humanitas Research Hospital Milan, Italy The job of the neuroradiologist in the work-up of brain tumors has quite changed in the
Glioblastoma: Current Treatment Approach 8/20/2018
 Glioblastoma: Current Treatment Approach 8/20/2018 Overview What is Glioblastoma? How is it diagnosed How is it treated? Principles of Treatment Surgery, Radiation, Chemotherapy Current Standard of care
Glioblastoma: Current Treatment Approach 8/20/2018 Overview What is Glioblastoma? How is it diagnosed How is it treated? Principles of Treatment Surgery, Radiation, Chemotherapy Current Standard of care
DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES
 DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES Marco Krengli Radiotherapy, Department of Translational Medicine, University of Piemonte Orientale A. Avogadro THE STANDARD OF CARE
DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES Marco Krengli Radiotherapy, Department of Translational Medicine, University of Piemonte Orientale A. Avogadro THE STANDARD OF CARE
Neuro-Oncology Program
 Neuro-Oncology Program The goals of the Neuro-oncology Committee are: 1) to improve duration and quality of life of brain tumor patients; 2) to assess disease and treatment-related effects on neurocognitive
Neuro-Oncology Program The goals of the Neuro-oncology Committee are: 1) to improve duration and quality of life of brain tumor patients; 2) to assess disease and treatment-related effects on neurocognitive
Diffuse infiltrative LGGs of the cerebral hemispheres
 J Neurosurg 117:1039 1052, 2012 Low-grade glioma surgery in eloquent areas: volumetric analysis of extent of resection and its impact on overall survival. A single-institution experience in 190 patients
J Neurosurg 117:1039 1052, 2012 Low-grade glioma surgery in eloquent areas: volumetric analysis of extent of resection and its impact on overall survival. A single-institution experience in 190 patients
Interferon β and temozolomide combination therapy for temozolomide monotherapy refractory malignant gliomas
 MOLECULAR AND CLINICAL ONCOLOGY 3: 909-913, 2015 Interferon β and temozolomide combination therapy for temozolomide monotherapy refractory malignant gliomas HIROSHI KAWAJI, TSUTOMU TOKUYAMA, TOMOHIRO YAMASAKI,
MOLECULAR AND CLINICAL ONCOLOGY 3: 909-913, 2015 Interferon β and temozolomide combination therapy for temozolomide monotherapy refractory malignant gliomas HIROSHI KAWAJI, TSUTOMU TOKUYAMA, TOMOHIRO YAMASAKI,
Asma Bashir, MD, 1 Jannick Brennum, MD, DMSc, 2 Helle Broholm, MD, 3 and Ian Law, MD, PhD, DMSc 1
 CLINICAL ARTICLE The diagnostic accuracy of detecting malignant transformation of low-grade glioma using O-(2-[ 18 F]fluoroethyl)-l-tyrosine positron emission tomography: a retrospective study Asma Bashir,
CLINICAL ARTICLE The diagnostic accuracy of detecting malignant transformation of low-grade glioma using O-(2-[ 18 F]fluoroethyl)-l-tyrosine positron emission tomography: a retrospective study Asma Bashir,
Early postoperative tumor progression predicts clinical outcome in glioblastoma implication for clinical trials
 J Neurooncol (2017) 132:249 254 DOI 10.1007/s11060-016-2362-z CLINICAL STUDY Early postoperative tumor progression predicts clinical outcome in glioblastoma implication for clinical trials Andreas Merkel
J Neurooncol (2017) 132:249 254 DOI 10.1007/s11060-016-2362-z CLINICAL STUDY Early postoperative tumor progression predicts clinical outcome in glioblastoma implication for clinical trials Andreas Merkel
Brain tumours (primary) and brain metastases in adults
 and brain metastases in adults") Brain tumours (primary) and brain metastases in adults NICE guideline Draft for consultation, January 0 This guideline covers diagnosing, monitoring and managing any type of primary brain tumour or brain
Brain tumours (primary) and brain metastases in adults NICE guideline Draft for consultation, January 0 This guideline covers diagnosing, monitoring and managing any type of primary brain tumour or brain
Response to postoperative radiotherapy as a prognostic factor for patients with low-grade gliomas
 ONCOLOGY LETTERS 4: 455-460, 2012 Response to postoperative radiotherapy as a prognostic factor for patients with low-grade gliomas MICHAL SPYCH 1,2, LESZEK GOTTWALD 3, EMILIA JESIEŃ LEWANDOWICZ 1,2, SŁAWOMIR
ONCOLOGY LETTERS 4: 455-460, 2012 Response to postoperative radiotherapy as a prognostic factor for patients with low-grade gliomas MICHAL SPYCH 1,2, LESZEK GOTTWALD 3, EMILIA JESIEŃ LEWANDOWICZ 1,2, SŁAWOMIR
CNS Tumors: The Med Onc Perspective. Ronald J. Scheff, MD Associate Clinical Professor Weill Medical College of Cornell U.
 CNS Tumors: The Med Onc Perspective Ronald J. Scheff, MD Associate Clinical Professor Weill Medical College of Cornell U. Disclosure Speakers Bureau, Merck Basic Oncology Concepts Tissue Diagnosis Stage
CNS Tumors: The Med Onc Perspective Ronald J. Scheff, MD Associate Clinical Professor Weill Medical College of Cornell U. Disclosure Speakers Bureau, Merck Basic Oncology Concepts Tissue Diagnosis Stage
PRESURGICAL PLANNING. Strongly consider neuropsychological evaluation before functional imaging study Strongly consider functional imaging study
 NOTE: Consider Clinical Trials as treatment options for eligible patients. Page 1 of 6 RADIOLOGICAL PRESENTATION PRESURGICAL PLANNING TREATMENT Imaging study suggestive of glioma 1 Left hemisphere speech/motor
NOTE: Consider Clinical Trials as treatment options for eligible patients. Page 1 of 6 RADIOLOGICAL PRESENTATION PRESURGICAL PLANNING TREATMENT Imaging study suggestive of glioma 1 Left hemisphere speech/motor
PROCARBAZINE, lomustine, and vincristine (PCV) is
 is") RAPID PUBLICATION Procarbazine, Lomustine, and Vincristine () Chemotherapy for Anaplastic Astrocytoma: A Retrospective Review of Radiation Therapy Oncology Group Protocols Comparing Survival With Carmustine
RAPID PUBLICATION Procarbazine, Lomustine, and Vincristine () Chemotherapy for Anaplastic Astrocytoma: A Retrospective Review of Radiation Therapy Oncology Group Protocols Comparing Survival With Carmustine
Chemotherapy in malignant brain tumors
 Chemotherapy in malignant brain tumors Frank Zimmermann Institut für Radioonkologie Universitätsspital Basel Petersgraben 4 CH 4031 Basel zimmermannf@uhbs.ch Tumor types Neuro-epithelial tumors - Glioblastoma
Chemotherapy in malignant brain tumors Frank Zimmermann Institut für Radioonkologie Universitätsspital Basel Petersgraben 4 CH 4031 Basel zimmermannf@uhbs.ch Tumor types Neuro-epithelial tumors - Glioblastoma
The Role of Radiation Therapy in the Treatment of Brain Metastases. Matthew Cavey, M.D.
 The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
Zurich Open Repository and Archive. Procarbazine and CCNU as initial treatment in gliomatosis cerebri
 University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich http://www.zora.uzh.ch Year: 2008 Procarbazine and CCNU as initial treatment in gliomatosis cerebri Glas, M;
University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich http://www.zora.uzh.ch Year: 2008 Procarbazine and CCNU as initial treatment in gliomatosis cerebri Glas, M;
PI3-Kinase Signaling. Rational Incorporation of Novel Agents into Multimodality Therapy. PI3-kinase. PI3-kinase 5/2/2010
 Rational Incorporation of Novel Agents into Multimodality Therapy I3-Kinase Signaling EGF IRS1 I3K EGFR I2 I3 TEN Rictor GßL AKT RAS40 Survival Raptor GßL Daphne Haas-Kogan UCSF Annual Course April 30-May
Rational Incorporation of Novel Agents into Multimodality Therapy I3-Kinase Signaling EGF IRS1 I3K EGFR I2 I3 TEN Rictor GßL AKT RAS40 Survival Raptor GßL Daphne Haas-Kogan UCSF Annual Course April 30-May
Corporate Medical Policy
 Corporate Medical Policy Brachytherapy, Intracavitary Balloon Catheter for Brain Cancer File Name: Origination: Last CAP Review: Next CAP Review: Last Review: brachytherapy_intracavitary_balloon_catheter_for_brain_cancer
Corporate Medical Policy Brachytherapy, Intracavitary Balloon Catheter for Brain Cancer File Name: Origination: Last CAP Review: Next CAP Review: Last Review: brachytherapy_intracavitary_balloon_catheter_for_brain_cancer
5-hydroxymethylcytosine loss is associated with poor prognosis for
 5-hydroxymethylcytosine loss is associated with poor prognosis for patients with WHO grade II diffuse astrocytomas Feng Zhang 1,*, Yifan Liu 2, Zhiwen Zhang 1, Jie Li 1, Yi Wan 3, Liying Zhang 1, Yangmei
5-hydroxymethylcytosine loss is associated with poor prognosis for patients with WHO grade II diffuse astrocytomas Feng Zhang 1,*, Yifan Liu 2, Zhiwen Zhang 1, Jie Li 1, Yi Wan 3, Liying Zhang 1, Yangmei
Goals for this Lecture. Case 1. Key Points MRI TECHNIQUES FOR DIFFERENTIAL DIAGNOSIS OF RECURRENT BRAIN LESIONS
 MRI TECHNIQUES FOR DIFFERENTIAL DIAGNOSIS OF RECURRENT BRAIN LESIONS Goals for this Lecture 1. Review common appearances for recurrent tumor and treatment effects on conventional MRI 2. Discuss current
MRI TECHNIQUES FOR DIFFERENTIAL DIAGNOSIS OF RECURRENT BRAIN LESIONS Goals for this Lecture 1. Review common appearances for recurrent tumor and treatment effects on conventional MRI 2. Discuss current
WHO 2016 CNS TUMOR CLASSIFICATION UPDATE. Arie Perry, M.D. Director, Neuropathology
 WHO 2016 CNS TUMOR CLASSIFICATION UPDATE Arie Perry, M.D. Director, Neuropathology DISCLOSURES (Arie Perry, MD) I have no financial relationships to disclose. - and - I will not discuss off label use or
WHO 2016 CNS TUMOR CLASSIFICATION UPDATE Arie Perry, M.D. Director, Neuropathology DISCLOSURES (Arie Perry, MD) I have no financial relationships to disclose. - and - I will not discuss off label use or
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist
 Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
European Association for Neuro-Oncology (EANO) guideline on the diagnosis and treatment of adult astrocytic and oligodendroglial gliomas
 guideline on the diagnosis and treatment of adult astrocytic and oligodendroglial gliomas") European Association for Neuro-Oncology (EANO) guideline on the diagnosis and treatment of adult astrocytic and oligodendroglial gliomas Michael Weller, Martin van den Bent, Jörg C Tonn, Roger Stupp, Matthias
European Association for Neuro-Oncology (EANO) guideline on the diagnosis and treatment of adult astrocytic and oligodendroglial gliomas Michael Weller, Martin van den Bent, Jörg C Tonn, Roger Stupp, Matthias
Treatment and outcomes for glioblastoma in elderly compared with non-elderly patients: a population-based study
 ORIGINAL ARTICLE Treatment and outcomes for glioblastoma in elderly compared with non-elderly patients: a population-based study E.R. Morgan md,* A. Norman md, K. Laing md, and M.D. Seal md ABSTRACT Purpose
ORIGINAL ARTICLE Treatment and outcomes for glioblastoma in elderly compared with non-elderly patients: a population-based study E.R. Morgan md,* A. Norman md, K. Laing md, and M.D. Seal md ABSTRACT Purpose
MR-Radiomics in Neuro-Oncology
 Klinik für Stereotaxie und funktionelle Neurochirurgie Institut für Neurowissenschaften und Medizin MR-Radiomics in Neuro-Oncology M. Kocher Klinik für funktionelle Neurochirurgie und Stereotaxie Forschungszentrum
Klinik für Stereotaxie und funktionelle Neurochirurgie Institut für Neurowissenschaften und Medizin MR-Radiomics in Neuro-Oncology M. Kocher Klinik für funktionelle Neurochirurgie und Stereotaxie Forschungszentrum
MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES
 MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES DISCLOSURE No conflicts of interest to disclose Patricia Bruns APRN, CNS Givens Brain Tumor Center Abbott Northwestern Hospital October 12, 2018 OBJECTIVES THEN
MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES DISCLOSURE No conflicts of interest to disclose Patricia Bruns APRN, CNS Givens Brain Tumor Center Abbott Northwestern Hospital October 12, 2018 OBJECTIVES THEN
2011 Oncology Highlights News from ASCO 2011:
 2011 Oncology Highlights News from ASCO 2011: Malignant Glioma David A. Reardon, M.D. Clinical Director Center for Neuro-Oncology Dana-Farber Cancer Institute 450 Brookline Avenue SW-430 Boston, MA 02215
2011 Oncology Highlights News from ASCO 2011: Malignant Glioma David A. Reardon, M.D. Clinical Director Center for Neuro-Oncology Dana-Farber Cancer Institute 450 Brookline Avenue SW-430 Boston, MA 02215
Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey
 Updated Oncology 2015: State of the Art News & Challenging Topics CURRENT STATUS OF STEREOTACTIC RADIOSURGERY IN BRAIN METASTASES Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey Bucharest,
Updated Oncology 2015: State of the Art News & Challenging Topics CURRENT STATUS OF STEREOTACTIC RADIOSURGERY IN BRAIN METASTASES Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey Bucharest,
Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen?
 Department of Radiation Oncology Chairman: Prof. Dr. Matthias Guckenberger Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen? Matthias
Department of Radiation Oncology Chairman: Prof. Dr. Matthias Guckenberger Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen? Matthias
THE EFFECTIVE OF BRAIN CANCER AND XAY BETWEEN THEORY AND IMPLEMENTATION. Mustafa Rashid Issa
 THE EFFECTIVE OF BRAIN CANCER AND XAY BETWEEN THEORY AND IMPLEMENTATION Mustafa Rashid Issa ABSTRACT: Illustrate malignant tumors that form either in the brain or in the nerves originating in the brain.
THE EFFECTIVE OF BRAIN CANCER AND XAY BETWEEN THEORY AND IMPLEMENTATION Mustafa Rashid Issa ABSTRACT: Illustrate malignant tumors that form either in the brain or in the nerves originating in the brain.
Anticonvulsive therapy. Roberta Rudà Division of Neuro-Oncology, Dept. of Neuroscience City of Health and Science and University of Turin, Italy
 Anticonvulsive therapy Roberta Rudà Division of Neuro-Oncology, Dept. of Neuroscience City of Health and Science and University of Turin, Italy Symposium on Brain Metastases, Zurich, 19 Jan 2018 DISCLOSURE
Anticonvulsive therapy Roberta Rudà Division of Neuro-Oncology, Dept. of Neuroscience City of Health and Science and University of Turin, Italy Symposium on Brain Metastases, Zurich, 19 Jan 2018 DISCLOSURE
Elderly Patients with Glioblastoma Multiforme Treated with Concurrent Temozolomide and Standard- versus Abbreviated-Course Radiotherapy
 Elderly Patients with Glioblastoma Multiforme Treated with Concurrent Temozolomide and Standard- versus Abbreviated-Course Radiotherapy Christine N Chang-Halpenny, MD; Jekwon Yeh, MD; Winston W Lien, MD
Elderly Patients with Glioblastoma Multiforme Treated with Concurrent Temozolomide and Standard- versus Abbreviated-Course Radiotherapy Christine N Chang-Halpenny, MD; Jekwon Yeh, MD; Winston W Lien, MD
Jennie W Taylor, MD 02/15/2019. Patient 1 Presentation
 Patient 1 Presentation Jennie W Taylor, MD 02/15/2019 A 34 year old right handed woman presents in 07/2015 with 9 years of stereotyped spells of olfactory change, nausea, and altered awareness. Imaging
Patient 1 Presentation Jennie W Taylor, MD 02/15/2019 A 34 year old right handed woman presents in 07/2015 with 9 years of stereotyped spells of olfactory change, nausea, and altered awareness. Imaging
Immuno-Oncology. Glioblastoma and CNS tumors 5 July 2016 Siena, Italy
 ESMO Preceptorship Programme Immuno-Oncology From the essentials of tumour immunology to clinical application Glioblastoma and CNS tumors 5 July 2016 Siena, Italy Michael Weller Department of Neurology
ESMO Preceptorship Programme Immuno-Oncology From the essentials of tumour immunology to clinical application Glioblastoma and CNS tumors 5 July 2016 Siena, Italy Michael Weller Department of Neurology
SURGICAL MANAGEMENT OF BRAIN TUMORS
 SURGICAL MANAGEMENT OF BRAIN TUMORS LIGIA TATARANU, MD, Ph D NEUROSURGICAL CLINIC, BAGDASAR ARSENI CLINICAL HOSPITAL BUCHAREST, ROMANIA SURGICAL INDICATIONS CONFIRMING HISTOLOGIC DIAGNOSIS REDUCING TUMOR
SURGICAL MANAGEMENT OF BRAIN TUMORS LIGIA TATARANU, MD, Ph D NEUROSURGICAL CLINIC, BAGDASAR ARSENI CLINICAL HOSPITAL BUCHAREST, ROMANIA SURGICAL INDICATIONS CONFIRMING HISTOLOGIC DIAGNOSIS REDUCING TUMOR
Clinical significance of genetic analysis in glioblastoma treatment
 Clinical significance of genetic analysis in glioblastoma treatment Department of Neurosurgery, Graduate School of Medical Sciences, Kyushu University, Fukuoka, Japan Koji Yoshimoto Can we get prognostic
Clinical significance of genetic analysis in glioblastoma treatment Department of Neurosurgery, Graduate School of Medical Sciences, Kyushu University, Fukuoka, Japan Koji Yoshimoto Can we get prognostic
MRI represents the diagnostic gold standard in neurooncology,
 Serial F-FET PET Imaging of Primarily F-FET Negative Glioma: Does It Make Sense? Marcus Unterrainer 1, Florian Schweisthal 1, Bogdana Suchorska 2, Vera Wenter 1, Christine Schmid-Tannwald 3, Wolfgang P.
Serial F-FET PET Imaging of Primarily F-FET Negative Glioma: Does It Make Sense? Marcus Unterrainer 1, Florian Schweisthal 1, Bogdana Suchorska 2, Vera Wenter 1, Christine Schmid-Tannwald 3, Wolfgang P.
Clinical Policy: Electric Tumor Treating Fields (Optune) Reference Number: PA.CP.MP.145
 Reference Number: PA.CP.MP.145") Clinical Policy: Electric Tumor Treating Fields (Optune) Reference Number: PA.CP.MP.145 Effective Date: 01/18 Last Review Date: 04/18 Coding Implications Revision Log Description Electric tumor treating
Clinical Policy: Electric Tumor Treating Fields (Optune) Reference Number: PA.CP.MP.145 Effective Date: 01/18 Last Review Date: 04/18 Coding Implications Revision Log Description Electric tumor treating
The prognostic value of MGMT promoter status by pyrosequencing assay for glioblastoma patients survival: a metaanalysis
 Zhao et al. World Journal of Surgical Oncology (2016) 14:261 DOI 10.1186/s12957-016-1012-4 REVIEW The prognostic value of MGMT promoter status by pyrosequencing assay for glioblastoma patients survival:
Zhao et al. World Journal of Surgical Oncology (2016) 14:261 DOI 10.1186/s12957-016-1012-4 REVIEW The prognostic value of MGMT promoter status by pyrosequencing assay for glioblastoma patients survival:
Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms. Overall Clinical Significance 8/3/13
 Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms Jason Sheehan, MD, PhD Departments of Neurosurgery and Radiation Oncology University of Virginia, Charlottesville, VA USA Overall
Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms Jason Sheehan, MD, PhD Departments of Neurosurgery and Radiation Oncology University of Virginia, Charlottesville, VA USA Overall
High-Grade Gliomas. Andrew B. Lassman, Diana Matceyevsky, and Benjamin W. Corn ETIOLOGY AND EPIDEMIOLOGY PREVENTION AND EARLY DETECTION
 C H A P T E R 27 High-Grade Gliomas Andrew B. Lassman, Diana Matceyevsky, and Benjamin W. Corn INCIDENCE There are approximately 68,000 new cases of brain tumors diagnosed in the United States each year.
C H A P T E R 27 High-Grade Gliomas Andrew B. Lassman, Diana Matceyevsky, and Benjamin W. Corn INCIDENCE There are approximately 68,000 new cases of brain tumors diagnosed in the United States each year.
CURRENT CONTROVERSIES IN THE MANAGEMENT OF HIGH GRADE GLIOMAS: AN INTERACTIVE CASE DISCUSSION *
 CURRENT CONTROVERSIES IN THE MANAGEMENT OF HIGH GRADE GLIOMAS: AN INTERACTIVE CASE DISCUSSION * Alessandro Olivi, MD, Jaishri Blakeley, MD, and Allen K. Sills, MD, FACS ABSTRACT The management of glioma
CURRENT CONTROVERSIES IN THE MANAGEMENT OF HIGH GRADE GLIOMAS: AN INTERACTIVE CASE DISCUSSION * Alessandro Olivi, MD, Jaishri Blakeley, MD, and Allen K. Sills, MD, FACS ABSTRACT The management of glioma
Optimal Management of Isolated HER2+ve Brain Metastases
 Optimal Management of Isolated HER2+ve Brain Metastases Eliot Sims November 2013 Background Her2+ve patients 15% of all breast cancer Even with adjuvant trastuzumab 10-15% relapse Trastuzumab does not
Optimal Management of Isolated HER2+ve Brain Metastases Eliot Sims November 2013 Background Her2+ve patients 15% of all breast cancer Even with adjuvant trastuzumab 10-15% relapse Trastuzumab does not
NON-SURGICAL STRATEGY FOR ADULT EPENDYMOMA
 NON-SURGICAL STRATEGY FOR ADULT EPENDYMOMA Roberta Rudà Department of Neuro-Oncology University and City of Health and Science Hospital of Turin, Italy EORTC EANO ESMO Conference 2015 Istanbul, March 27-28
NON-SURGICAL STRATEGY FOR ADULT EPENDYMOMA Roberta Rudà Department of Neuro-Oncology University and City of Health and Science Hospital of Turin, Italy EORTC EANO ESMO Conference 2015 Istanbul, March 27-28
2015 EUROPEAN CANCER CONGRESS
 2015 EUROPEAN CANCER CONGRESS 25-29 September 2015 Vienna, Austria SUMMARY The European Cancer Congress (ECC 2015) combined the 40th European Society for Medical Oncology (ESMO) congress with the 18th
2015 EUROPEAN CANCER CONGRESS 25-29 September 2015 Vienna, Austria SUMMARY The European Cancer Congress (ECC 2015) combined the 40th European Society for Medical Oncology (ESMO) congress with the 18th
journals/eano/index.html Homepage: Online Database Featuring Author, Key Word and Full-Text Search
 Volume 3 (2013) // Issue 2 // e-issn 2224-3453 Neurology Neurosurgery Medical Oncology Radiotherapy Paediatric Neurooncology Neuropathology Neuroradiology Neuroimaging Nursing Patient Issues Journey of
Volume 3 (2013) // Issue 2 // e-issn 2224-3453 Neurology Neurosurgery Medical Oncology Radiotherapy Paediatric Neurooncology Neuropathology Neuroradiology Neuroimaging Nursing Patient Issues Journey of
EORTC (RTOG 0834 Endorsed) Opened: July 22, 2009
 Opened: July 22, 2009") January 2011 0834-1 EORTC 26053 22054 (RTOG 0834 Endorsed) Protocol Status: Opened: July 22, 2009 Title: Phase III Trial on Concurrent and Adjuvant Temozolomide Chemotherapy in Non-1P/19Q Deleted Anaplastic
January 2011 0834-1 EORTC 26053 22054 (RTOG 0834 Endorsed) Protocol Status: Opened: July 22, 2009 Title: Phase III Trial on Concurrent and Adjuvant Temozolomide Chemotherapy in Non-1P/19Q Deleted Anaplastic
Advances in gastric cancer: How to approach localised disease?
 Advances in gastric cancer: How to approach localised disease? Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer Surgical resection Pathology assessment and estimation
Advances in gastric cancer: How to approach localised disease? Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer Surgical resection Pathology assessment and estimation
ORE Open Research Exeter
 ORE Open Research Exeter TITLE Temozolomide for high grade glioma AUTHORS Hart, MG; Garside, R; Rogers, G; et al. JOURNAL Cochrane Database Of Systematic Reviews DEPOSITED IN ORE 22 October 2013 This version
ORE Open Research Exeter TITLE Temozolomide for high grade glioma AUTHORS Hart, MG; Garside, R; Rogers, G; et al. JOURNAL Cochrane Database Of Systematic Reviews DEPOSITED IN ORE 22 October 2013 This version
IDH1 R132H/ATRX Immunohistochemical validation
 IDH1 R132H/ATRX Immunohistochemical validation CIQC/DSM 2016 12 June 2016 0835-0905 Stephen Yip, M.D., Ph.D., FRCPC University of British Columbia Disclosure Statement I have nothing to disclose I will
IDH1 R132H/ATRX Immunohistochemical validation CIQC/DSM 2016 12 June 2016 0835-0905 Stephen Yip, M.D., Ph.D., FRCPC University of British Columbia Disclosure Statement I have nothing to disclose I will
VAL-083: Validated DNA-targeting Agent for Underserved Cancer Patients. September 2018
 VAL-083: Validated DNA-targeting Agent for Underserved Cancer Patients September 2018 Forward-Looking Statements Any statements contained in this presentation that do not describe historical facts may
VAL-083: Validated DNA-targeting Agent for Underserved Cancer Patients September 2018 Forward-Looking Statements Any statements contained in this presentation that do not describe historical facts may
European Association for Neuro-Oncology (EANO) guideline on the diagnosis and treatment of adult astrocytic and oligodendroglial gliomas
 guideline on the diagnosis and treatment of adult astrocytic and oligodendroglial gliomas") Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 2017 European Association for Neuro-Oncology (EANO) guideline on the diagnosis
Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 2017 European Association for Neuro-Oncology (EANO) guideline on the diagnosis