Tumors of the Central Nervous System
|
|
|
- Veronica Harrison
- 5 years ago
- Views:
Transcription
1 Tumors of the Central Nervous System 1
2 Financial Disclosures I have NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT
3 Introduction General: Brain tumors are lesions that have mass effect distorting the normal tissue and often result in increased intracranial pressure. 3
4 Introduction Primary neoplasms may develop from any cell type normally residing in or over the brain. Their neoplastic proliferation often is a bizarre mimic of normal morphology. Meninges Astrocytes Oligodendroglia Ependyma Neurons 4
5 Intracranial tumors Primary Axial: anywhere within the brain parenchyma Extra-axial: outside the brain parenchyma Metastatic usually at the gray/white junction (Axial location). May be extra-axial (dural). Patient may have a known primary. 5
6 Metastatic Carcinoma Most common intracranial adult tumor. Primary sources: Lung, Breast, Kidney, GI tract, Skin (Melanoma) Sarcomas are uncommon Predominance of location relates to volume of blood flow to area: Cerebrum>Cerebellum>Spinal cord 6


7 Metastatic Carcinoma Gross/Radiology: Tumor emboli most commonly found at the grey/white junction. May be more than one lesion. Often marked edema surrounding tumor. Microscopic: Tumor typically looks like the primary. 7
8 Primary Extra-axial Intracranial Tumors 8
9 Meningioma Neoplasm derived from the brain coverings ( meninges ). Incidence: 20% of primary CNS tumors Age: adult; yrs. Gender Predominance: Female (2:1) symptomatic tumors 9
10 Meningioma Clinical: slow progression clinical symptoms depend on location of tumor Sites: Parasagittal, sphenoid ridge, spinal cord Treatment: Surgical excision Prognosis: Good; 25% recurrence 10


11 Meningioma Surgical excision is the usual treatment. Some may be asymptomatic and found at autopsy. 11


12 MENINGIOMA While meningiomas are benign neoplasms, they can be locally aggressive, invading bone as in this case 12



13 Meningioma Brain & Normal Meninges Arachnoid Meningioma PIA Brain General slow growing, benign arises from cells forming surface coverings of brain compresses rather than invades brain well-circumscribed may be focally mineralized 13


14 Meningioma Microscopic arachnoid-like cells with vacuolated nucleus. sheets of cells without distinct borders (syncytium) spindle-shaped cells cellular whorls of arachnoid cells concentric laminated calcifications (psammoma bodies) 14
15 CNS Nerve Sheath Tumors Schwannoma 15
16 Schwannoma Benign tumor of schwann cells Incidence: 10% of primary CNS tumors Age: years; younger age and multiple if part of Neurofibromatosis complex Sites: cranial nerves (especially CNVIII), sensory spinal roots, peripheral nerves Prognosis: favorable; benign, slow growing tumors Rx: surgical excision 16
")
17 Schwannoma Bilateral schwannomas located at the cerebello-pontine angle (CPA tumor) 17


18 Schwannoma Gross: nerve focally enlarged and rubbery. The tumor grows by expansion and is encased within the nerve. It can usually be shelled out sparing remaining nerve. 18
 admixed with loose, less cellular areas (Antoni B).")
19 SCHWANNOMA Micro: spindle-cell proliferation with wavy appearance; Biphasic architecture: cellular with palisading nuclei (Antoni A) admixed with loose, less cellular areas (Antoni B). Antoni B Antoni A 19


20 Schwannoma Antoni B Verocay Body Antoni A Schwannomas may show a peculiar palisading of nuclei in parallel rows with intervening anuclear zone known as the VEROCAY BODY 20

21 Tumors of the CNS Parenchyma Astrocytoma Oligodendroglioma Ependymoma Medulloblastoma 21
22 Classification of Astrocytomas Circumscribed astrocytoma Diffuse Astrocytoma Relatively well-circumscribed or cystic. Usually low grade (WHO Grade I). Low tendency to have anaplastic progression. Favorable prognosis Infiltrative margin. Three histologic grades II-IV. Tendency to progress to more anaplastic forms. Unfavorable prognosis 22
23 Circumscribed Astrocytoma Incidence: 10% of primary CNS tumors Age: childhood tumor Clinical: slowly progressive. Site: Midline (esp. cerebellum, optic nerve) 23


24 Circumscribed Gliomas- Juvenile Pilocytic Astrocytoma Rx: surgical Gross: well-demarcated, effacing adjacent structures; grey-white, rubbery to gelatinous; may be cystic (esp. cerebellar tumors) 24


25 Juvenile Pilocytic Astrocytoma Microscopic elongated spindle-shaped astrocytes (piloid) biphasic pattern of hyper and hypodense areas with microcysts 25
.")
26 Circumscribed Astrocytoma Rosenthal fibers are common (pink beaded arrangement of astrocytic glial filaments). 26

27 Diffuse Astrocytomas Infiltrative tumor with ill-defined margins 27



28 Grade II Grade III Grade IV Astrocytic tumors show a histologic continuum from nearly normal looking neuropil in low grade tumors (Grade II/IV) to highly cellular proliferations with necrosis in high grade tumors (Grade IV/IV). Usually stain positively for the presence of the intermediate cytoskeletal filaments, GFAP (Glial Fibrillary Acidic Protein). 28
 High cellularity,")

29 Grade IV Astrocytoma- Glioblastoma Multiforme (GBM) High cellularity, pleomorphism, hyperplastic vascularity, mitoses and necrosis are features of glioblastoma. 29

30 Astrocytoma- Clinical Behavior Transformation of a low grade tumor to high grade is wellknown and can be traced by cumulative gene abnormalities including p53 mutations and LOH of chromosome
31 Diffuse Astrocytoma- Treatment Surgical debulking when possible. Radiation Chemotherapy- poor response Prognosis: Low Grade tumors: Good, years. High Grade tumors: Poor; usually 6-12 months 31
32 Tumors of the CNS Parenchyma (Gliomas) Astrocytoma Oligodendroglioma Ependymoma Medulloblastoma 32
33 Oligodendroglioma Incidence: 5% of CNS tumors Age: years Clinical: progressive course over several years Site: Cerebral hemispheres Prognosis: 40%, 5 year survival Treatment: Surgical Gross: poor circumscription, infiltrative, hemorrhage, focal calcification 33
34 Oligodendroglioma Immunohistochemistry: No good positive marker; GFAP- Negative. Often mutated IDH-1. Molecular marker: 1p 19q co-deletion 34


35 Oligodendroglioma Microscopic: Uniform, cellular pattern of oligodendrocytes with fried egg perinuclear halo appearance and calcifications. 35


36 Oligodendroglioma The chicken-wire vascular pattern is an important clue to histogenesis and can be identified with Factor VIII antibody against endothelial cells. Oligodendroglia with halos are negative for GFAP. 36
37 Tumors of the CNS Parenchyma (Gliomas) Astrocytoma Oligodendroglioma Ependymoma Medulloblastoma 37
38 Ependymoma Incidence: 5% of CNS tumors Age: 5-25 yrs (brain); years (spinal cord) Clinical: Present with symptoms of CSF obstruction. Site: fourth ventricle, cerebrum; distal spinal cord Prognosis: 40% 5 yr (brain); 60% 5 yr (spinal cord) Rx: Surgery; radiation 38
39 Ependymoma Gross: Many are intraventricular; granular and friable. These factors give this tumor a greater tendency to seed the CSF pathways. 39


40 Ependyma Ependymomas arise as neoplastic proliferations of ependymal cells which normally line ventricular spaces. Ependymal cells line the ventricles 40



41 Ependymal rosette Ependymoma GFAP Perivascular pseudorosette Vascular tumor with uniform sheets of cells with small dark round nuclei in a glial fibrillary background. Perivascular pseudorosettes are key diagnostic feature 41
42 Tumors of the CNS Parenchyma Astrocytoma Oligodendroglioma Ependymoma Medulloblastoma 42
43 Medulloblastoma 5% of primary tumors 5-20 yrs rapid progressive cerebellar symptoms Site: Cerebellar vermis (young); lateral hemisphere (older) Prognosis: 75% 5 year; CSF seeding is common Rx: Surgery and radiation Micro: Small, round blue cell tumor comprising Primitive neuroectodermal cell precursors of glia and neurons (PNET); Homer Wright rosettes 43
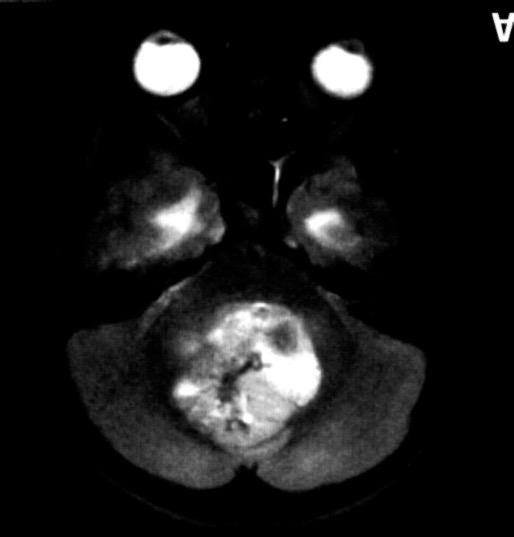
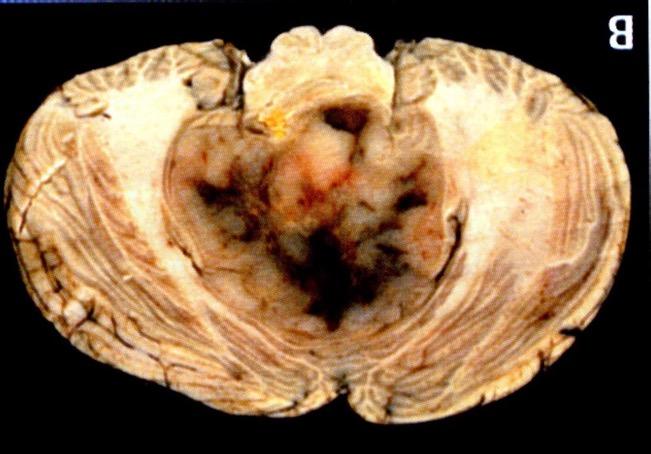

44 Medulloblastoma 44




45 Medulloblastoma Normal cerebellum Fetal cerebellum Rosette formation is a classic feature of Medulloblastoma and tend to be of the Homer Wright type. Other rosette formations are seen in primitive neuroectodermal tumors found elsewhere 45
46 Lecture Objectives Know the histologic features of meningioma, schwannoma, oligodendroglioma, astrocytomas (pilocytic and diffuse Grades II-IV), ependymoma, medulloblastoma Know the differences in behavior of the tumor types noted above. Be aware of age distribution of the tumor types discussed. 46
47 THE END 47
General: Brain tumors are lesions that have mass effect distorting the normal tissue and often result in increased intracranial pressure.
 1 Lecture Objectives Know the histologic features of the most common tumors of the CNS. Know the differences in behavior of the different tumor types. Be aware of the treatment modalities in the various
1 Lecture Objectives Know the histologic features of the most common tumors of the CNS. Know the differences in behavior of the different tumor types. Be aware of the treatment modalities in the various
Tumors of the Nervous System
 Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they present? What do they look like? How do they behave? 1
Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they present? What do they look like? How do they behave? 1
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 12: CNS tumours 2/3
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 12: CNS tumours 2/3 Pilocytic astrocytoma Relatively benign ( WHO grade 1) Occurs in children and young adults Mostly: in the cerebellum
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 12: CNS tumours 2/3 Pilocytic astrocytoma Relatively benign ( WHO grade 1) Occurs in children and young adults Mostly: in the cerebellum
Peter Canoll MD. PhD.
 Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they ypresent? What do they look like? How do they behave?
Tumors of the Nervous System Peter Canoll MD. PhD. What I want to cover What are the most common types of brain tumors? Who gets them? How do they ypresent? What do they look like? How do they behave?
CNS TUMORS. D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria)
. M. Path (U. of Alexandria)") CNS TUMORS D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) CNS TUMORS The annual incidence of intracranial tumors of the CNS ISmore than intraspinal tumors May be Primary or Secondary
CNS TUMORS D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) CNS TUMORS The annual incidence of intracranial tumors of the CNS ISmore than intraspinal tumors May be Primary or Secondary
Brain Tumors. Medulloblastoma. Pilocytic astrocytoma: Ahmed Koriesh, MD. Pathological finding
 NeuroPathology Page 8 Brain Tumors Pathological finding Pseudorosette Rosenthal fibers Rosettes Wet Keratin Psammoma bodies Fried egg Tumor Ependymoma, SEGA Pilocytic astrocytoma Medulloblastoma Craniopharyngioma
NeuroPathology Page 8 Brain Tumors Pathological finding Pseudorosette Rosenthal fibers Rosettes Wet Keratin Psammoma bodies Fried egg Tumor Ependymoma, SEGA Pilocytic astrocytoma Medulloblastoma Craniopharyngioma
TUMORS of nervous system
 TUMORS of nervous system By: Shifaa Alqa qa Done By : Ola Hijjawi CNS tumors : The annual incidence of CNS tumors ranges from 10 to 17 per 100,000 persons for intracranial tumors and 1 to 2 per 100,000
TUMORS of nervous system By: Shifaa Alqa qa Done By : Ola Hijjawi CNS tumors : The annual incidence of CNS tumors ranges from 10 to 17 per 100,000 persons for intracranial tumors and 1 to 2 per 100,000
SPECIAL SLIDE SEMINAR CASE 3
 SPECIAL SLIDE SEMINAR CASE 3 Tihana Džombeta, MD Leo Pažanin, MD, PhD Department of Pathology, School of Medicine, University of Zagreb Department of Pathology, Clinical Hospital Centre Sestre milosrdnice
SPECIAL SLIDE SEMINAR CASE 3 Tihana Džombeta, MD Leo Pažanin, MD, PhD Department of Pathology, School of Medicine, University of Zagreb Department of Pathology, Clinical Hospital Centre Sestre milosrdnice
Understanding general brain tumor pathology, Part I: The basics. Craig Horbinski, M.D., Ph.D. Department of Pathology University of Kentucky
 Understanding general brain tumor pathology, Part I: The basics Craig Horbinski, M.D., Ph.D. Department of Pathology University of Kentucky plan of attack what IS a pathologist, anyway? what s so special
Understanding general brain tumor pathology, Part I: The basics Craig Horbinski, M.D., Ph.D. Department of Pathology University of Kentucky plan of attack what IS a pathologist, anyway? what s so special
Brain tumors: tumor types
 Brain tumors: tumor types Tumor types There are more than 120 types of brain tumors. Today, most medical institutions use the World Health Organization (WHO) classification system to identify brain tumors.
Brain tumors: tumor types Tumor types There are more than 120 types of brain tumors. Today, most medical institutions use the World Health Organization (WHO) classification system to identify brain tumors.
SUPPLEMENTARY INFORMATION
 VOLUME: 1 ARTICLE NUMBER: 0027 In the format provided by the authors and unedited. Rapid intraoperative histology of unprocessed surgical specimens via fibre-laser-based stimulated Raman scattering microscopy
VOLUME: 1 ARTICLE NUMBER: 0027 In the format provided by the authors and unedited. Rapid intraoperative histology of unprocessed surgical specimens via fibre-laser-based stimulated Raman scattering microscopy
2. Subependymal giant cell astrocytoma:
 I. Astrocytomas: A. Diffusely infiltrating ( astrocytoma, anaplastic astrocytoma, GBM) B. Localised (pilocytic astrocytoma, pleomorphic xanthoastrocytoma, SGCA) *Grading: Diffuse: 1. Astrocytoma WHO grade
I. Astrocytomas: A. Diffusely infiltrating ( astrocytoma, anaplastic astrocytoma, GBM) B. Localised (pilocytic astrocytoma, pleomorphic xanthoastrocytoma, SGCA) *Grading: Diffuse: 1. Astrocytoma WHO grade
INFECTIONS OF THE NERVOUS SYSTEM
 NEUROPATHOLOGY INFECTIONS OF THE NERVOUS SYSTEM An infectious agent must use one of several routes of entry to reach the CNS & cause a disease. 1. Hematogenous spread via the arterial blood supply is the
NEUROPATHOLOGY INFECTIONS OF THE NERVOUS SYSTEM An infectious agent must use one of several routes of entry to reach the CNS & cause a disease. 1. Hematogenous spread via the arterial blood supply is the
Q&A. Fabulous Prizes. Collecting Cancer Data:CNS 2/7/12. NAACCR Webinar Series Collecting Cancer Data Central Nervous System
 Collecting Cancer Data Central Nervous System NAACCR 2012 2013 Webinar Series 2/7/2013 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Collecting Cancer Data Central Nervous System NAACCR 2012 2013 Webinar Series 2/7/2013 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Pleomorphic Xanthoastrocytoma
 Pleomorphic Xanthoastrocytoma Christine E. Fuller Keywords Pleomorphic xanthoastrocytoma; Pleomorphic xanthoastrocytoma with anaplastic features 2.1 OVERVIEW Pleomorphic xanthoastrocytoma (PXA) is an uncommon
Pleomorphic Xanthoastrocytoma Christine E. Fuller Keywords Pleomorphic xanthoastrocytoma; Pleomorphic xanthoastrocytoma with anaplastic features 2.1 OVERVIEW Pleomorphic xanthoastrocytoma (PXA) is an uncommon
Nonepithelial Tumors
 Nonepithelial Tumors General Definitions Mesenchymal Tumors These tumors consist of tissues that originate in the middle germ layer or mesoderm, primarily from the pluripotential supporting tissue of the
Nonepithelial Tumors General Definitions Mesenchymal Tumors These tumors consist of tissues that originate in the middle germ layer or mesoderm, primarily from the pluripotential supporting tissue of the
Supra- and infratentorial brain tumors from childhood to maternity
 Supra- and infratentorial brain tumors from childhood to maternity What to expect? I am going to show you the characteristic imaging findings of following tumors: Thierry A.G.M. Huisman, MD, FICIS, EQNR
Supra- and infratentorial brain tumors from childhood to maternity What to expect? I am going to show you the characteristic imaging findings of following tumors: Thierry A.G.M. Huisman, MD, FICIS, EQNR
Intraoperative Cytology of CNS Lesions
 1 Intraoperative Cytology of CNS Lesions Matthew A Zarka, M.D. Director of Cytopathology Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Scottsdale, Arizona Gregory S. Moes, M.D. Department
1 Intraoperative Cytology of CNS Lesions Matthew A Zarka, M.D. Director of Cytopathology Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Scottsdale, Arizona Gregory S. Moes, M.D. Department
Pathologic Analysis of CNS Surgical Specimens
 2015 Kenneth M. Earle Memorial Neuropathology Review Pathologic Analysis of CNS Surgical Specimens Peter C. Burger, MD Interdisciplinary Quality Control Familiarity with entities Use of diagnostic algorithm
2015 Kenneth M. Earle Memorial Neuropathology Review Pathologic Analysis of CNS Surgical Specimens Peter C. Burger, MD Interdisciplinary Quality Control Familiarity with entities Use of diagnostic algorithm
Anaplastic Pilocytic Astrocytoma: The fusion of good and bad
 Anaplastic Pilocytic Astrocytoma: The fusion of good and bad Alexandrina Nikova 1, Charalampos-Chrysovalantis Chytoudis-Peroudis 2, Penelope Korkolopoulou 3 and Dimitrios Kanakis 4 Abstract 5 Pilocytic
Anaplastic Pilocytic Astrocytoma: The fusion of good and bad Alexandrina Nikova 1, Charalampos-Chrysovalantis Chytoudis-Peroudis 2, Penelope Korkolopoulou 3 and Dimitrios Kanakis 4 Abstract 5 Pilocytic
Cerebral Parenchymal Lesions: I. Metastatic Neoplasms
 Chapter 4 Cerebral Parenchymal Lesions: I. Metastatic Neoplasms After one has reasonably ruled out the possibility of a nonneoplastic diagnosis (see Chap. 3), one is left with considering a diagnosis of
Chapter 4 Cerebral Parenchymal Lesions: I. Metastatic Neoplasms After one has reasonably ruled out the possibility of a nonneoplastic diagnosis (see Chap. 3), one is left with considering a diagnosis of
Classification of Diffuse Gliomas: Progress, Pearls and Pitfalls. Rob Macaulay Neuropathologist, MCC October 21, 2017
 Classification of Diffuse Gliomas: Progress, Pearls and Pitfalls Rob Macaulay Neuropathologist, MCC October 21, 2017 Objectives Explain why the designation high grade glioma is preferable to GBM for intraoperative
Classification of Diffuse Gliomas: Progress, Pearls and Pitfalls Rob Macaulay Neuropathologist, MCC October 21, 2017 Objectives Explain why the designation high grade glioma is preferable to GBM for intraoperative
Imaging the Spinal Cord & Intradural Disease
 Department of Radiology University of California San Diego Imaging the Spinal Cord & Intradural Disease John R. Hesselink, M.D. Spinal Cord Diseases Tumors Syringohydromyelia Trauma Ischemia / Infarction
Department of Radiology University of California San Diego Imaging the Spinal Cord & Intradural Disease John R. Hesselink, M.D. Spinal Cord Diseases Tumors Syringohydromyelia Trauma Ischemia / Infarction
Accuracy of intra-operative rapid diagnosis by Squash smear in CNS lesions An early institutional experience. KK Bansal,
 Accuracy of intra-operative rapid diagnosis by Squash smear in CNS lesions An early institutional experience. KK Bansal, Monika Bansal, Sanjeev Kishore, Anuradha K, Meena H, Dushyant G. Department of Neurosurgery
Accuracy of intra-operative rapid diagnosis by Squash smear in CNS lesions An early institutional experience. KK Bansal, Monika Bansal, Sanjeev Kishore, Anuradha K, Meena H, Dushyant G. Department of Neurosurgery
Malignant Peripheral Nerve Sheath Tumor
 C H A P T E R 120 Malignant Peripheral Nerve Sheath Tumor Currently, malignant peripheral nerve sheath tumor (MPNST) is the most commonly used generic name for the neoplasms known in the past as neurosarcoma,
C H A P T E R 120 Malignant Peripheral Nerve Sheath Tumor Currently, malignant peripheral nerve sheath tumor (MPNST) is the most commonly used generic name for the neoplasms known in the past as neurosarcoma,
Five Most Common Problems in Surgical Neuropathology
 Five Most Common Problems in Surgical Neuropathology If the brain were so simple that we could understand it, we would be so simple that we couldn t Emerson Pugh What is your greatest difficulty in neuropathology?
Five Most Common Problems in Surgical Neuropathology If the brain were so simple that we could understand it, we would be so simple that we couldn t Emerson Pugh What is your greatest difficulty in neuropathology?
Classification of spontaneous brain tumors in rats
 Classification of spontaneous brain tumors in rats Central Nervous System Neoplasms in the Rat (Solleveld HA, et al., 1991) 1. Tumors of Neuroepithelial Tissue A. Astrocytic and oligodendroglial tumors
Classification of spontaneous brain tumors in rats Central Nervous System Neoplasms in the Rat (Solleveld HA, et al., 1991) 1. Tumors of Neuroepithelial Tissue A. Astrocytic and oligodendroglial tumors
H Haloes cautions, 57 neurocytomas, perinuclear, 56 Headache blue cell tumors, 147 cautions, 135, 147, 152 clinical history, 132, 144, 148
 Index A ADC. See Apparent diffusion coefficient Adult. See also Supratentorial mass, adult cerebral tumor, 1 headache and ataxia cysts, mural nodules, 118 sporadic tumors, 118 headaches and visual changes,
Index A ADC. See Apparent diffusion coefficient Adult. See also Supratentorial mass, adult cerebral tumor, 1 headache and ataxia cysts, mural nodules, 118 sporadic tumors, 118 headaches and visual changes,
Infections. Meningitis- leptomenings (usually bakterial)
") Neuropathology Neuropathology Cerebral Edema, raised intracranial pressure, Herniatio Malformations, Developmental Diseases Perinatal Brain Injury Trauma Cerebrovascular Diseases Infections Transmissible
Neuropathology Neuropathology Cerebral Edema, raised intracranial pressure, Herniatio Malformations, Developmental Diseases Perinatal Brain Injury Trauma Cerebrovascular Diseases Infections Transmissible
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM MEDULLOBLASTOMA AND PNET CNS Site Group Medulloblastoma and PNET Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM MEDULLOBLASTOMA AND PNET CNS Site Group Medulloblastoma and PNET Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION
Histopathological Study and Categorisation of Brain Tumors
 Histopathological Study and Categorisation of Brain Tumors Ruchira Wadhwa 1*, Purvi Patel 2, Hansa Goswami 3 1 Third Year Resident, 2 Assistant Professor, 3 Professor and Head, Department of Pathology,
Histopathological Study and Categorisation of Brain Tumors Ruchira Wadhwa 1*, Purvi Patel 2, Hansa Goswami 3 1 Third Year Resident, 2 Assistant Professor, 3 Professor and Head, Department of Pathology,
Astroblastoma: Radiologic-Pathologic Correlation and Distinction from Ependymoma
 AJNR Am J Neuroradiol 23:243 247, February 2002 Case Report Astroblastoma: Radiologic-Pathologic Correlation and Distinction from Ependymoma John D. Port, Daniel J. Brat, Peter C. Burger, and Martin G.
AJNR Am J Neuroradiol 23:243 247, February 2002 Case Report Astroblastoma: Radiologic-Pathologic Correlation and Distinction from Ependymoma John D. Port, Daniel J. Brat, Peter C. Burger, and Martin G.
Site Specific Coding Rules MALIGNANT CENTRAL NERVOUS SYSTEM TUMORS
 Multiple Primary and Histology Site Specific Coding Rules MALIGNANT CENTRAL NERVOUS SYSTEM TUMORS 1 Prerequisites 2 Completion of Multiple Primary and Histology General Coding Rules 3 There are many ways
Multiple Primary and Histology Site Specific Coding Rules MALIGNANT CENTRAL NERVOUS SYSTEM TUMORS 1 Prerequisites 2 Completion of Multiple Primary and Histology General Coding Rules 3 There are many ways
MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES
 MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES DISCLOSURE No conflicts of interest to disclose Patricia Bruns APRN, CNS Givens Brain Tumor Center Abbott Northwestern Hospital October 12, 2018 OBJECTIVES THEN
MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES DISCLOSURE No conflicts of interest to disclose Patricia Bruns APRN, CNS Givens Brain Tumor Center Abbott Northwestern Hospital October 12, 2018 OBJECTIVES THEN
What is Brain Cancer? What is the brain?
 What is Brain Cancer? The brain and spinal column make up the central nervous system (CNS), where all vital functions of the body are controlled. When tumors arise in the central nervous system, they are
What is Brain Cancer? The brain and spinal column make up the central nervous system (CNS), where all vital functions of the body are controlled. When tumors arise in the central nervous system, they are
Pediatric Brain Tumors: Updates in Treatment and Care
 Pediatric Brain Tumors: Updates in Treatment and Care Writer Classroom Rishi R. Lulla, MD MS Objectives Introduce the common pediatric brain tumors Discuss current treatment strategies for pediatric brain
Pediatric Brain Tumors: Updates in Treatment and Care Writer Classroom Rishi R. Lulla, MD MS Objectives Introduce the common pediatric brain tumors Discuss current treatment strategies for pediatric brain
Oligodendrogliomas & Oligoastrocytomas
 Oligodendrogliomas & Oligoastrocytomas ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the first national nonprofit organization dedicated solely
Oligodendrogliomas & Oligoastrocytomas ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the first national nonprofit organization dedicated solely
CHAPTER 11 Tumors Originating in the Brain Medulloblastomas, PNETs and Ependymomas
 Tumors Originating in the Brain Medulloblastomas, PNETs and Ependymomas Foolishly, I waited 7 months before I joined this (or any) group. By that time, my son had radiation, chemo, and a recurrence of
Tumors Originating in the Brain Medulloblastomas, PNETs and Ependymomas Foolishly, I waited 7 months before I joined this (or any) group. By that time, my son had radiation, chemo, and a recurrence of
Year 2003 Paper two: Questions supplied by Tricia
 question 43 A 42-year-old man presents with a two-year history of increasing right facial numbness. He has a history of intermittent unsteadiness, mild hearing loss and vertigo but has otherwise been well.
question 43 A 42-year-old man presents with a two-year history of increasing right facial numbness. He has a history of intermittent unsteadiness, mild hearing loss and vertigo but has otherwise been well.
Advances In Orbital Neuropathology
 Advances In Orbital Neuropathology Charles G. Eberhart, MD PhD Associate Professor of Pathology, Ophthalmology and Oncology Johns Hopkins University School of Medicine Overview Non-neoplastic lesions Microphthalmos/pseudoglioma
Advances In Orbital Neuropathology Charles G. Eberhart, MD PhD Associate Professor of Pathology, Ophthalmology and Oncology Johns Hopkins University School of Medicine Overview Non-neoplastic lesions Microphthalmos/pseudoglioma
What are brain and spinal cord tumours? Contents
 13 11 20 Information and support What are brain and spinal cord tumours? Contents The brain and spinal cord Brain function What is a brain or spinal cord tumour? What types of tumours are there? How common
13 11 20 Information and support What are brain and spinal cord tumours? Contents The brain and spinal cord Brain function What is a brain or spinal cord tumour? What types of tumours are there? How common
MOLECULAR DIAGNOSTICS OF GLIOMAS
 MOLECULAR DIAGNOSTICS OF GLIOMAS Arie Perry, M.D. Director, Neuropathology Division DIFFUSE GLIOMAS Cell types Astrocytomas (A) Oligodendrogliomas (O) Mixed oligoastrocytoma (MOA) Three WHO grades: II,
MOLECULAR DIAGNOSTICS OF GLIOMAS Arie Perry, M.D. Director, Neuropathology Division DIFFUSE GLIOMAS Cell types Astrocytomas (A) Oligodendrogliomas (O) Mixed oligoastrocytoma (MOA) Three WHO grades: II,
Nervous system. Dr. Rawaa Salim Hameed
 Nervous system Dr. Rawaa Salim Hameed Central nervous system (CNS) CNS consists of the brain (cerebrum, cerebellum, and brainstem) and spinal cord CNS is covered by connective tissue layers, the meninges
Nervous system Dr. Rawaa Salim Hameed Central nervous system (CNS) CNS consists of the brain (cerebrum, cerebellum, and brainstem) and spinal cord CNS is covered by connective tissue layers, the meninges
CT & MRI Evaluation of Brain Tumour & Tumour like Conditions
 CT & MRI Evaluation of Brain Tumour & Tumour like Conditions Dr. Anjana Trivedi 1, Dr. Jay Thakkar 2, Dr. Maulik Jethva 3, Dr. Ishita Virda 4 1 M.D. Radiology, Professor and Head, P.D.U. Medical College
CT & MRI Evaluation of Brain Tumour & Tumour like Conditions Dr. Anjana Trivedi 1, Dr. Jay Thakkar 2, Dr. Maulik Jethva 3, Dr. Ishita Virda 4 1 M.D. Radiology, Professor and Head, P.D.U. Medical College
BAH1 - Primary Glioblastoma
 BAH1 - Primary Glioblastoma R frontal tumour for frozen section. No known primary. Contrast enhancing lesion. Cholecystectomy. FROZEN SECTION REPORT Right frontal tumour: The specimen consists of multiple
BAH1 - Primary Glioblastoma R frontal tumour for frozen section. No known primary. Contrast enhancing lesion. Cholecystectomy. FROZEN SECTION REPORT Right frontal tumour: The specimen consists of multiple
USCAP Neuropathology night panel CASE 4
 USCAP Neuropathology night panel CASE 4 B.K. Kleinschmidt-DeMasters MD University of Colorado Denver Denver, Colorado Sheep Mountain, Telluride, Colorado Clinical History The patient is a 46 year old male
USCAP Neuropathology night panel CASE 4 B.K. Kleinschmidt-DeMasters MD University of Colorado Denver Denver, Colorado Sheep Mountain, Telluride, Colorado Clinical History The patient is a 46 year old male
Neuropathology Specialty Conference
 Neuropathology Specialty Conference March 22, 2010 Case 2 Rebecca Folkerth, MD Brigham and Women s Hospital Children s Hospital Harvard Medical School Clinical History 18-gestational-week fetus found on
Neuropathology Specialty Conference March 22, 2010 Case 2 Rebecca Folkerth, MD Brigham and Women s Hospital Children s Hospital Harvard Medical School Clinical History 18-gestational-week fetus found on
AMERICAN BRAIN TUMOR ASSOCIATION. Oligodendroglioma and Oligoastrocytoma
 AMERICAN BRAIN TUMOR ASSOCIATION Oligodendroglioma and Oligoastrocytoma ACKNOWLEDGEMENTS ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the
AMERICAN BRAIN TUMOR ASSOCIATION Oligodendroglioma and Oligoastrocytoma ACKNOWLEDGEMENTS ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the
Note: The cause of testicular neoplasms remains unknown
 - In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
- In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
Dr. T. Venkat Kishan Asst. Prof Department of Radiodiagnosis
 Dr. T. Venkat Kishan Asst. Prof Department of Radiodiagnosis Schwannomas (also called neurinomas or neurilemmomas) constitute the most common primary cranial nerve tumors. They are benign slow-growing
Dr. T. Venkat Kishan Asst. Prof Department of Radiodiagnosis Schwannomas (also called neurinomas or neurilemmomas) constitute the most common primary cranial nerve tumors. They are benign slow-growing
Posterior fossa tumors: clues to differential diagnosis with case-based review
 Posterior fossa tumors: clues to differential diagnosis with case-based review Poster No.: C-0323 Congress: ECR 2017 Type: Educational Exhibit Authors: H. A. Aboughalia, M. Abdelhady; Doha/QA Keywords:
Posterior fossa tumors: clues to differential diagnosis with case-based review Poster No.: C-0323 Congress: ECR 2017 Type: Educational Exhibit Authors: H. A. Aboughalia, M. Abdelhady; Doha/QA Keywords:
Gliomas in the 2016 WHO Classification of CNS Tumors
 Gliomas in the 2016 WHO Classification of CNS Tumors Hindi N Al-Hindi, MD, FCAP Consultant Neuropathologist and Head Section of Anatomic Pathology Department of Pathology and Laboratory Medicine King Faisal
Gliomas in the 2016 WHO Classification of CNS Tumors Hindi N Al-Hindi, MD, FCAP Consultant Neuropathologist and Head Section of Anatomic Pathology Department of Pathology and Laboratory Medicine King Faisal
Morphological features and genetic alterations
 Morphological features and genetic alterations Tutor : Audrey Rousseau Caget Lise: Université d Angers Iorio Vittoria: Seconda Università degli studi di Napoli Manaila Roxana: Iuliu Hatieganu University
Morphological features and genetic alterations Tutor : Audrey Rousseau Caget Lise: Université d Angers Iorio Vittoria: Seconda Università degli studi di Napoli Manaila Roxana: Iuliu Hatieganu University
Financial disclosures
 Mesenchymal Neoplasms with Melanocytic Differentiation By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel
Mesenchymal Neoplasms with Melanocytic Differentiation By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel
Childhood brain tumours
 Childhood brain tumours Our bodies are made up of billions of cells. Normally, these cells reproduce and repair themselves in a controlled way and do not cause us any problems. If for some reason this
Childhood brain tumours Our bodies are made up of billions of cells. Normally, these cells reproduce and repair themselves in a controlled way and do not cause us any problems. If for some reason this
I have no conflicts of interest in relation to this presentation. Vogel FS & Burger PC 3/28/2016
 IF THIS IS NOT GLIOBLASTOMA, THEN WHAT IS IT? Murat Gokden, MD Department of Pathology/Neuropathology University of Arkansas for Medical Sciences Little Rock, AR mgokden@uams.edu I have no conflicts of
IF THIS IS NOT GLIOBLASTOMA, THEN WHAT IS IT? Murat Gokden, MD Department of Pathology/Neuropathology University of Arkansas for Medical Sciences Little Rock, AR mgokden@uams.edu I have no conflicts of
USCAP Neuropathology. Case No. 3 Elisabeth J. Rushing, MD Armed Forces Institute of Pathology Washington, DC
 USCAP Neuropathology Case No. 3 Elisabeth J. Rushing, MD Armed Forces Institute of Pathology Washington, DC Clinical history The patient is a 9 year-old boy who has had seizures since age 2, at which time
USCAP Neuropathology Case No. 3 Elisabeth J. Rushing, MD Armed Forces Institute of Pathology Washington, DC Clinical history The patient is a 9 year-old boy who has had seizures since age 2, at which time
LOW GRADE ASTROCYTOMAS
 LOW GRADE ASTROCYTOMAS This article was provided to us by David Schiff, MD, Associate Professor of Neurology, Neurosurgery, and Medicine at University of Virginia, Charlottesville. We appreciate his generous
LOW GRADE ASTROCYTOMAS This article was provided to us by David Schiff, MD, Associate Professor of Neurology, Neurosurgery, and Medicine at University of Virginia, Charlottesville. We appreciate his generous
Characteristic features of CNS pathology. By: Shifaa AlQa qa
 Characteristic features of CNS pathology By: Shifaa AlQa qa Normal brain: - The neocortex (gray matter): six layers: outer plexiform, outer granular, outer pyramidal, inner granular, inner pyramidal, polymorphous
Characteristic features of CNS pathology By: Shifaa AlQa qa Normal brain: - The neocortex (gray matter): six layers: outer plexiform, outer granular, outer pyramidal, inner granular, inner pyramidal, polymorphous
Pediatric Spine Tumors (and other masses)
") Pediatric Spine Tumors (and other masses) Francisco A Perez, MD, PhD Assistant Professor Neuroradiology and Pediatric Radiology Seattle Children s Hospital University of Washington, Seattle Commercial
Pediatric Spine Tumors (and other masses) Francisco A Perez, MD, PhD Assistant Professor Neuroradiology and Pediatric Radiology Seattle Children s Hospital University of Washington, Seattle Commercial
Neoplasms of the BRAIN and CNS
 Neoplasms of the BRAIN and CNS 2015-21016 FCDS Educational Webcast Series Steven Peace, BS, CTR October 15, 2015 2015 Focus Anatomy SSS 2000 MPH Rules AJCC TNM Presentation Outline Overview Reportable
Neoplasms of the BRAIN and CNS 2015-21016 FCDS Educational Webcast Series Steven Peace, BS, CTR October 15, 2015 2015 Focus Anatomy SSS 2000 MPH Rules AJCC TNM Presentation Outline Overview Reportable
monotonous, stippled, round, smoothcontoured nuclei and scanty acidophilic or
 monotonous, stippled, round, smoothcontoured nuclei and scanty acidophilic or vacuolated cytoplasm. The cells are surrounded by a loose fibrillary stroma that is traversed by delicate capillaries. Ill
monotonous, stippled, round, smoothcontoured nuclei and scanty acidophilic or vacuolated cytoplasm. The cells are surrounded by a loose fibrillary stroma that is traversed by delicate capillaries. Ill
Adult Brain and Spinal Cord Tumors
 Adult Brain and Spinal Cord Tumors An adult central nervous system (CNS) tumor is a disease in which abnormal cells form in the tissues of the brain and or the spinal cord. Major Parts of the Brain Anatomy
Adult Brain and Spinal Cord Tumors An adult central nervous system (CNS) tumor is a disease in which abnormal cells form in the tissues of the brain and or the spinal cord. Major Parts of the Brain Anatomy
2018 Diagnostic Slide Session Case #8
 2018 Diagnostic Slide Session Case #8 Angela N. Viaene, MacLean P. Nasrallah, and Zissimos Mourelatos Hospital of the University of Pennsylvania AANP June 9, 2018 Disclosures: none Clinical History Healthy,
2018 Diagnostic Slide Session Case #8 Angela N. Viaene, MacLean P. Nasrallah, and Zissimos Mourelatos Hospital of the University of Pennsylvania AANP June 9, 2018 Disclosures: none Clinical History Healthy,
AMERICAN BRAIN TUMOR ASSOCIATION. Oligodendroglioma and Oligoastrocytoma
 AMERICAN BRAIN TUMOR ASSOCIATION Oligodendroglioma and Oligoastrocytoma ACKNOWLEDGEMENTS ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the
AMERICAN BRAIN TUMOR ASSOCIATION Oligodendroglioma and Oligoastrocytoma ACKNOWLEDGEMENTS ABOUT THE AMERICAN BRAIN TUMOR ASSOCIATION Founded in 1973, the American Brain Tumor Association (ABTA) was the
Anna Maria Buccoliero Department of Biomedicine, Careggi Hospital Florence
 PEDIATRIC RHABDOID MENINGIOMA Anna Maria Buccoliero Department of Biomedicine, Careggi Hospital Florence CLINICAL HISTORY A 3-year-old boy, with a recent history of seizures, was admitted to the Neurosurgery
PEDIATRIC RHABDOID MENINGIOMA Anna Maria Buccoliero Department of Biomedicine, Careggi Hospital Florence CLINICAL HISTORY A 3-year-old boy, with a recent history of seizures, was admitted to the Neurosurgery
The New WHO Classification and the Role of Integrated Molecular Profiling in the Diagnosis of Malignant Gliomas
 The New WHO Classification and the Role of Integrated Molecular Profiling in the Diagnosis of Malignant Gliomas Stefan Prokop, MD Neuropathology Fellow Hospital of the University of Pennsylvania Background
The New WHO Classification and the Role of Integrated Molecular Profiling in the Diagnosis of Malignant Gliomas Stefan Prokop, MD Neuropathology Fellow Hospital of the University of Pennsylvania Background
NEURORADIOLOGY DIL part 5
 NEURORADIOLOGY DIL part 5 Masses and tumors K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL part
NEURORADIOLOGY DIL part 5 Masses and tumors K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL part
Histology of the CNS
 Histology of the CNS Lecture Objectives Describe the histology of the cerebral cortex layers. Describe the histological features of the cerebellum; layers and cells of cerebellar cortex. Describe the elements
Histology of the CNS Lecture Objectives Describe the histology of the cerebral cortex layers. Describe the histological features of the cerebellum; layers and cells of cerebellar cortex. Describe the elements
THE NEUROBIOLOGY OF THE NEURON AND THE NEUROGLIA
 THE NEUROBIOLOGY OF THE NEURON AND THE NEUROGLIA DEFINITION OF A NEURON Neuron is the name given to the nerve cell and all its processes. Neurons are excitable cells that are specialized for the reception
THE NEUROBIOLOGY OF THE NEURON AND THE NEUROGLIA DEFINITION OF A NEURON Neuron is the name given to the nerve cell and all its processes. Neurons are excitable cells that are specialized for the reception
Adult Central Nervous System Tumors Treatment (PDQ )
") 1 di 20 28/06/2016 11.18 NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health. PDQ Cancer Information Summaries [Internet]. Bethesda (MD): National Cancer Institute
1 di 20 28/06/2016 11.18 NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health. PDQ Cancer Information Summaries [Internet]. Bethesda (MD): National Cancer Institute
Case 1. Maysa Al-Hussaini MD FRCPath
 Case 1 Maysa Al-Hussaini MD FRCPath MAYSA King AL-HUSSAINI Hussein Cancer MD Center MRCPATH KING HUSSEIN Amman CANCER Jordan CENTER Clinical history 4 year old boy History of frontal headache, sleepiness.
Case 1 Maysa Al-Hussaini MD FRCPath MAYSA King AL-HUSSAINI Hussein Cancer MD Center MRCPATH KING HUSSEIN Amman CANCER Jordan CENTER Clinical history 4 year old boy History of frontal headache, sleepiness.
Brain Tumors. Andrew J. Fabiano, MD FAANS. Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine
 Brain Tumors Andrew J. Fabiano, MD FAANS Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine Brain Tumors Brain Tumor Basics Types of Tumors Cases Brain
Brain Tumors Andrew J. Fabiano, MD FAANS Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine Brain Tumors Brain Tumor Basics Types of Tumors Cases Brain
Essentials of Clinical MR, 2 nd edition. 51. Primary Neoplasms
 51. Primary Neoplasms As with spinal central canal neoplasms in other regions, those of the lumbar spine may be classified as extradural, intradural extramedullary, and medullary. If an extradural lesion
51. Primary Neoplasms As with spinal central canal neoplasms in other regions, those of the lumbar spine may be classified as extradural, intradural extramedullary, and medullary. If an extradural lesion
Pediatric CNS Tumors. Disclosures. Acknowledgements. Introduction. Introduction. Posterior Fossa Tumors. Whitney Finke, MD
 Pediatric CNS Tumors Disclosures Whitney Finke, MD Neuroradiology Fellow PGY-6 University of Utah Health Sciences Center Salt Lake City, Utah None Acknowledgements Introduction Nicholas A. Koontz, MD Luke
Pediatric CNS Tumors Disclosures Whitney Finke, MD Neuroradiology Fellow PGY-6 University of Utah Health Sciences Center Salt Lake City, Utah None Acknowledgements Introduction Nicholas A. Koontz, MD Luke
SOME BASIC TERMINOLOGY CNS: Central Nervous System: Brain + Spinal Cord
 SOME BASIC TERMINOLOGY CNS: Central Nervous System: Brain + Spinal Cord CEREBROSPINAL FLUID (CSF): The fluid filling the ventricles, cerebral aqueduct, central canal, and subarachnoid space. It is a filtrate
SOME BASIC TERMINOLOGY CNS: Central Nervous System: Brain + Spinal Cord CEREBROSPINAL FLUID (CSF): The fluid filling the ventricles, cerebral aqueduct, central canal, and subarachnoid space. It is a filtrate
RINGS N THINGS: Imaging Patterns in Differential Diagnosis. Anne G. Osborn, M.D.
 RINGS N THINGS: Imaging Patterns in Differential Diagnosis Anne G. Osborn, M.D. ExpDDxs: Intra-axial (Parenchymal) Lesions Ring-enhancing lesions, solitary 1 Ring-enhancing lesion crossing corpus callosum
RINGS N THINGS: Imaging Patterns in Differential Diagnosis Anne G. Osborn, M.D. ExpDDxs: Intra-axial (Parenchymal) Lesions Ring-enhancing lesions, solitary 1 Ring-enhancing lesion crossing corpus callosum
-The cause of testicular neoplasms remains unknown
 - In the 15- to 34-year-old age group, they are the most common tumors of men. - include: I. Germ cell tumors : (95%); all are malignant. II. Sex cord-stromal tumors: from Sertoli or Leydig cells; usually
- In the 15- to 34-year-old age group, they are the most common tumors of men. - include: I. Germ cell tumors : (95%); all are malignant. II. Sex cord-stromal tumors: from Sertoli or Leydig cells; usually
Pathology Mystery and Surprise
 Pathology Mystery and Surprise Tim Smith, MD Director Anatomic Pathology Medical University of South Carolina Disclosures No conflicts to declare Some problem cases Kidney tumor Scalp tumor Bladder tumor
Pathology Mystery and Surprise Tim Smith, MD Director Anatomic Pathology Medical University of South Carolina Disclosures No conflicts to declare Some problem cases Kidney tumor Scalp tumor Bladder tumor
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM MENINGIOMA CNS Site Group Meningioma Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION 3 2. PREVENTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM MENINGIOMA CNS Site Group Meningioma Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION 3 2. PREVENTION
Diagnostic implications of IDH1-R132H and OLIG2 expression patterns in rare and challenging glioblastoma variants
 & 2012 USCAP, Inc. All rights reserved 0893-3952/12 $32.00 1 Diagnostic implications of IDH1-R132H and OLIG2 expression patterns in rare and challenging glioblastoma variants Nancy M Joseph 1, Joanna Phillips
& 2012 USCAP, Inc. All rights reserved 0893-3952/12 $32.00 1 Diagnostic implications of IDH1-R132H and OLIG2 expression patterns in rare and challenging glioblastoma variants Nancy M Joseph 1, Joanna Phillips
A Journey Down The Canal
 A Journey Down The Canal Radiological Assessment of Spinal Cord Masses John Berry-Candelario HMS III Gillian Lieberman, MD BIDMC Objectives Patient review Anatomy of the spine Imaging techniques Classification
A Journey Down The Canal Radiological Assessment of Spinal Cord Masses John Berry-Candelario HMS III Gillian Lieberman, MD BIDMC Objectives Patient review Anatomy of the spine Imaging techniques Classification
STUDY OFPAEDIATRIC CNS TUMORS IN TERTIARY CARE CENTER
 IJCRR Section: Healthcare Sci. Journal Impact Factor 4.016 Original Article STUDY OFPAEDIATRIC CNS TUMORS IN TERTIARY CARE CENTER Grishma P. Jobanputra Tutor, Department of Pathology, B.J. Medical College,
IJCRR Section: Healthcare Sci. Journal Impact Factor 4.016 Original Article STUDY OFPAEDIATRIC CNS TUMORS IN TERTIARY CARE CENTER Grishma P. Jobanputra Tutor, Department of Pathology, B.J. Medical College,
What we will talk about
 Surgical Neuropathology: Avoiding pitfalls at frozen section and Immunochemistry that really helps Arizona Society of Pathologists Fall 2013 Stephen W. Coons MD Barrow Neurological Institute Beauregard
Surgical Neuropathology: Avoiding pitfalls at frozen section and Immunochemistry that really helps Arizona Society of Pathologists Fall 2013 Stephen W. Coons MD Barrow Neurological Institute Beauregard
A case of multinodular high-grade neuroepithelial tumor
 Brain Tumor Pathol (2011) 28:253 257 DOI 10.1007/s10014-011-0032-6 CASE REPORT A case of multinodular high-grade neuroepithelial tumor with ependymal differentiation Kensaku Kamada Yuko Tanaka Takayuki
Brain Tumor Pathol (2011) 28:253 257 DOI 10.1007/s10014-011-0032-6 CASE REPORT A case of multinodular high-grade neuroepithelial tumor with ependymal differentiation Kensaku Kamada Yuko Tanaka Takayuki
Spinal Neoplasms. First Things First!! Localize the Lesion!! Ependymomas. Common Intramedullary Lesions
 Acta Radiológica Portuguesa, Vol.XXIII, nº 90, pág. 101-114, Abr.-Jun., 2011 Spinal Neoplasms Bruno A Policeni University of Iowa Hospitals and Clinics Assistant Professor of Radiology Disclosure of Commercial
Acta Radiológica Portuguesa, Vol.XXIII, nº 90, pág. 101-114, Abr.-Jun., 2011 Spinal Neoplasms Bruno A Policeni University of Iowa Hospitals and Clinics Assistant Professor of Radiology Disclosure of Commercial
What Are We Going to Do? Fourth Year Meds Clinical Neuroanatomy. Hydrocephalus and Effects of Interruption of CSF Flow. Tube Blockage Doctrine
 Fourth Year Meds Clinical Neuroanatomy Ventricles, CSF, Brain Swelling etc. David A. Ramsay, Neuropathologist, LHSC What Are We Going to Do? Hydrocephalus and some effects of the interruption of CSF flow
Fourth Year Meds Clinical Neuroanatomy Ventricles, CSF, Brain Swelling etc. David A. Ramsay, Neuropathologist, LHSC What Are We Going to Do? Hydrocephalus and some effects of the interruption of CSF flow
Epidemiology and Outcome of Brain Disorders & Damage Across the Life Span: Some Notes. Vincent W. Hevern, SJ, Ph.D. 2018
 Epidemiology and Outcome of Brain Disorders & Damage Across the Life Span: Some Notes Cerebrovascular Disease or Stroke Vincent W. Hevern, SJ, Ph.D. 2018 A. Epidemiology of Brain Disorders & Damage Number
Epidemiology and Outcome of Brain Disorders & Damage Across the Life Span: Some Notes Cerebrovascular Disease or Stroke Vincent W. Hevern, SJ, Ph.D. 2018 A. Epidemiology of Brain Disorders & Damage Number
Supplementary Information
 Rise in Glioblastoma Multiforme incidence in England 1995 2015 suggests an adverse environmental or lifestyle factor Alasdair Philips, Denis L Henshaw, Graham Lamburn, Michael J O Carroll Supplementary
Rise in Glioblastoma Multiforme incidence in England 1995 2015 suggests an adverse environmental or lifestyle factor Alasdair Philips, Denis L Henshaw, Graham Lamburn, Michael J O Carroll Supplementary
Brain and Spine Tumors
 Brain and Spine Tumors Andrew J. Fabiano, MD FAANS Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine Brain Tumors Brain Tumor Basics Types of Tumors Cases
Brain and Spine Tumors Andrew J. Fabiano, MD FAANS Associate Professor of Neurosurgery Roswell Park Cancer Institute SUNY at Buffalo School of Medicine Brain Tumors Brain Tumor Basics Types of Tumors Cases
Nervous system. 1. Neurons :
 Nervous system nervous system is composed of billions of cells, the most essential being the nerve cells or neurons. There are estimated to be as many as 100 billion neurons in our nervous system. Two
Nervous system nervous system is composed of billions of cells, the most essential being the nerve cells or neurons. There are estimated to be as many as 100 billion neurons in our nervous system. Two
Normal thyroid tissue
 Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
Pediatric Retroperitoneal Masses Radiologic-Pathologic Correlation
 Acta Radiológica Portuguesa, Vol.XVIII, nº 70, pág. 61-70, Abr.-Jun., 2006 Pediatric Retroperitoneal Masses Radiologic-Pathologic Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
Acta Radiológica Portuguesa, Vol.XVIII, nº 70, pág. 61-70, Abr.-Jun., 2006 Pediatric Retroperitoneal Masses Radiologic-Pathologic Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM EPENDYMOMA Last Revision Date July 2015 1 CNS Site Group Ependymoma Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2.
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM EPENDYMOMA Last Revision Date July 2015 1 CNS Site Group Ependymoma Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2.
Oligodendroglioma: imaging findings, radio-pathological correlation and evolution
 Oligodendroglioma: imaging findings, radio-pathological correlation and evolution Poster No.: C-2104 Congress: ECR 2013 Type: Authors: Keywords: DOI: Scientific Exhibit A. Hernandez Castro, M. D. Monedero
Oligodendroglioma: imaging findings, radio-pathological correlation and evolution Poster No.: C-2104 Congress: ECR 2013 Type: Authors: Keywords: DOI: Scientific Exhibit A. Hernandez Castro, M. D. Monedero
1 NORMAL ANATOMY AND HISTOLOGY
 1 NORMAL ANATOMY AND HISTOLOGY OF THE CNS Anatomy 1 Histology 4 ANATOMY Knowledge of nervous system anatomy is essential for success in surgical neuropathology. Familiarity with native cellular elements
1 NORMAL ANATOMY AND HISTOLOGY OF THE CNS Anatomy 1 Histology 4 ANATOMY Knowledge of nervous system anatomy is essential for success in surgical neuropathology. Familiarity with native cellular elements
Symtomatic Subependymoma Of The Lateral Ventricle: A Rare Entity A Case report and review of literature
 ISPUB.COM The Internet Journal of Neurosurgery Volume 7 Number 1 Symtomatic Subependymoma Of The Lateral Ventricle: A Rare Entity A Case report and review of M Sharma, V Velho, P Ghodgaonkar, D Palande
ISPUB.COM The Internet Journal of Neurosurgery Volume 7 Number 1 Symtomatic Subependymoma Of The Lateral Ventricle: A Rare Entity A Case report and review of M Sharma, V Velho, P Ghodgaonkar, D Palande
NON MALIGNANT BRAIN TUMOURS Facilitator. Ros Taylor Advanced Neurosurgical Nurse Practitioner Southmead Hospital Bristol
 NON MALIGNANT BRAIN TUMOURS Facilitator Ros Taylor Advanced Neurosurgical Nurse Practitioner Southmead Hospital Bristol Neurosurgery What will be covered? Meningioma Vestibular schwannoma (acoustic neuroma)
NON MALIGNANT BRAIN TUMOURS Facilitator Ros Taylor Advanced Neurosurgical Nurse Practitioner Southmead Hospital Bristol Neurosurgery What will be covered? Meningioma Vestibular schwannoma (acoustic neuroma)
Cross sectional imaging of Intracranial cystic lesions Abdel Razek A
 Cross sectional imaging of Intracranial cystic lesions Abdel Razek A Department of Radiology. Mansoura Faculty of Medicine, Mansoura. Egypt. arazek@mans.edu.eg Introduction Intracranial cystic lesions
Cross sectional imaging of Intracranial cystic lesions Abdel Razek A Department of Radiology. Mansoura Faculty of Medicine, Mansoura. Egypt. arazek@mans.edu.eg Introduction Intracranial cystic lesions
Fourth Ventricular Lesions in Metastatic Gliomas: A Rare Predilection?
 CASE REPORT Brain Tumor Res Treat 2017;5(1):24-29 / pissn 2288-2405 / eissn 2288-2413 https://doi.org/10.14791/btrt.2017.5.1.24 Fourth Ventricular Lesions in Metastatic Gliomas: A Rare Predilection? Mohammed
CASE REPORT Brain Tumor Res Treat 2017;5(1):24-29 / pissn 2288-2405 / eissn 2288-2413 https://doi.org/10.14791/btrt.2017.5.1.24 Fourth Ventricular Lesions in Metastatic Gliomas: A Rare Predilection? Mohammed