Antiangiogenic drugs in unresectable glioblastoma. Dra. Carmen Balañá. /
|
|
|
- Kristopher Burns
- 5 years ago
- Views:
Transcription


1 Antiangiogenic drugs in unresectable glioblastoma Dra. Carmen Balañá. /
2 Outcome for unresectable GBM Overall survival for unresectable GBM without further treatment is: 3 months at most. Radiotherapy increases OS to 6.6 months. Radiotherapy and temozolomide increases survival for patients with KPS 70% to 9.4months. Median survival for recurrent GBM treated with second line therapy is months. Median survival for patients with only a biopsy is then similar to those GBM treated at recurrence. Prestwitch RJ 2005, Hart MG, et al. Cochrane Database Syst Rev. 2005; Stupp R, ; Laws ER 2003; Mirimanoff RO 2006; Lacroix M, 2001, Wick 2012, Malström 2012
3 Patients with biopsy only included in clinical trials Trial Phase N (total) Only biospy % Standard EORTC (Stupp) III NABTT (historical) RT+No TMZ III Talampanel +/-standard (Grossman ) II RTOG histórical II-III severa NABTT+TMZ+ new agent II-III several III AVAGLIO 17
4 Incidence of only biopsy pts in the clinical setting Author/country N Source Period Biopsy Partial resection Complete resection Bauchet/France 952 French Brain Tumor DataBase Scoccianti/italy* RDT UNIT % Graus/Spain 833 Neurologist Chang/USA 418 Glioma outcomes project % resection first or second surgery *only patients who are sent for treatment, underestimation of patients who are even not biopsied 78.5% craneotomies
5 Biopsy patients and standard treatment No previous decompressive effect of surgery Clinically unstable: big tumours /eloquent areas/multifocality Large radiotherapy fields for big tumours Difficulty in completing treament Edema/pseudoprogression on eloquent areas Corticoid dependence Cushing QoL of a pal.liative treatment?. Balana 2007, Nieder 2005
6 Pre-radiation treatment/ Neo-adjuvant therapy? Objective: To obtain an objective response ( tumour burden) Improve or stabilize the patient-- better tolerance to radiation therapy Test of Therapeutic Efficaccy: Fewer confusion factors in interpreting MRI (no pseudoprogression) Better setting to apply RANO criteria Test of bioavailibity if administered previous to surgery (tipifarnib/imatinib) Does radiotherapy delay worsens survival? Yes (resected patients). Valduvieco, Irwin No: (experience of the Old NABTT CNS Consortium who rejected the activity of 4 agents (Taxol, 9-AC, CI-980, PZA, and oxaliplatin) with only 149 patients exposed), Class A studies. ASCO 2002 if 6 weeks RTOG 2855p. Blumenthal Hochberg et al., 2000, Fetell et al 1997, Balana et al 2014, Lustig 2008 et al, Razis et al 2009.
7 Pre-radiation treatments before 2005 No TMZ
8 Pre-radiation treatments before 2005 TMZ
9 TMZ alone upfront Autor Study Nº TRAT RT + TMZ % RT RESP OS m 1y S % Chinot 2007 Single Inst Phase II 29 TMZ 150mg/m2 /15d & TMZ x 4 post RT NO 76% / 55% 24% PR Brada 2005 Multicente Phase II 139 TMZ 200MG/m 2: 1-5/28 X2 NO?? 20% PR+MR 9 37
10 Neo-adjuvant treatment has never been compared to standard treatment in a randomized study
11 Unresectable GBM: neo-adjuvant treatment vs standard treatment. Retrospective study Cohort 1: p CDDP+TMZ x 2 cycles Cohort 2: p STUPP REGIMEN RDT or STUPP REGIMEN Capdevila et al J Neuro-oncology
12 Patient Characteristics Age < Histology Anaplastic Ast Glioblastoma PS Barthel index >70 70 Neurological impairment No Yes Dexamethasone No Yes Convulsions No Yes Second-line bev No Yes MGMT Unmethylated Methylated Neoadjuvant Cohort N (%) 3 (13.0) 20 (87.0) 5 (21.7) 18 (78.3) 15 (65.2) 8 (34.8) 15 (65.2) 8 (34.8) 6 (26.1) 17 (73.9) 1 (4.3) 22 (95.7) 13 (56.5) 10 (43.5) 19 (82.6) 4 (17.4) 12 (54.5) 10 (45.5) Adjuvant Cohort N (%) 2 (8.7) 21 (91.3) 7 (30.4) 16 (69.6) 14 (60.9) 9 (39.1) 18 (78.3) 5 (21.7) 11 (47.8) 12 (52.2) 3 (13.0) 20 (87.0) 17 (73.9) 6 (26.1) 15 (65.2) 8 (34.8) 14 (70.0) 7 (30.0) P /12 AA were IDH1 wild type Capdevila et al J Neuro-oncology

13 Results retrospective study PFS OS P=0.9 1 YEAR SURVIVAL 38.5% Cohort 1 and 45% Cohort 2 P=0.9
14 Fig. 2: Progression-free survival according to MGMT methylation status Cohort 1: Neo-Adj A Cohort 2: Stupp B MGMT MGMT - MGMT + MGMT + P=0.09 P=0.04 Un-Methylated pts don t get benefit of a Neoadjuvant TMZ based treatment
15 Achievements of Neo-adjuvant trials No randomized/prospective trials comparing neoadjuvant versus standard. Al least 6 agents have been rejected for further study in neo-adjuvant trials. (Taxol, 9AC, CI-980, PZA, oxaliplatin, sunitinib) The availability and pharmacokinetics of some agents have been studied administering them before surgery: tipifarnib, imatinib Hochberg et al., 2000, Fetell et al 1997, Balana et al 2014, Lustig 2008 et al, Razis et al 2009.

16 HOW TO REJECT AND AGENT FOR FURTHER STUDY WITH ONLY 12 PATIENTS
17 Statistical assumptions Main objective: to determine activity in inducing tumor response, in accordance with the RANO criteria. The Simon 2-phase design was used, with an alpha error of 0.05 and a beta error of Based on responses achieved in previous studies, in which the treatment was considered inactive if the response rate obtained was <10%, and with a maximum calculated objective response of 40%. the initial number of patients planned for recruitment in the first phase was 12. If one response was observed in the first 12 patients, the sample size was to be increased by 20 patients in the second phase (a total of 32 patients). The treatment would be considered effective if a minimum of four responses were observed.

18 GENOM-008: Sunitinib NA

19 OS /PFS sunitinb before standard treatment
20 Bevacizumab induces fast responses Neo-adjuvant trials with Bevacizumab
 PR 28 (68,3%) SD")
21 41 GBM 4 cycles: TMZ 200mg/m2/dx5/28+BEV 10MG/Kg/15d. if no progression keep on If progression standard treatment Responses 10 (24,4%) PR 28 (68,3%) SD 1 (2,4%) P OS median 11,7m 12m survival 48,8%
22 BEV &IRI vs BEV& TMZ BEV+IRI x 8 weeks RDT +BEV+IRI BEV+IRI x 8 weeks 32p R BEV+TMZx 8 weeks RDT +BEV+TMZ BEV+TMZx 8 weeks 31p No unresectable patients Primary endpoint : objective Response after 8 weeks BEV+ IRI: ORR 32%; CI 95%: 17-51%, PFS: 7.7m better than BEV+IRI : ORR 23%; CI 95%: 9-44%, PFS: 7.3m Holland 2014
 120p")

23 TEMAVIR TRIAL (ANOCEF) 120p No central review of images/ histology
24 TEMAVIR results Pre-defined main objective a PFS6m of 66% in the experimental arm (37/60 p without progression at 6 months, only 30/60 were without progression- negative study
25 TEMAVIR Toxicity GIII-V
26 GENOM 009
27 GENOM 009 GBM Biopsy of minimal Surgery PS 0-2 TMZ 85 mg/m2/21d/ 28d, 2 cycles RT 60 Gy / 2 Gy / 6 w TMZ 75 mg/m2/d TMZ mg/m2 d1-d5 q 28d, 6 cycles RT 60 Gy / 2 Gy / 6 w TMZ 75 mg/m2/d Bev 10 mg/kg q2w TMZ mg/m2 d1-d5 q 28d, 6 cycles (N=45) R 4w rest (N=48 TMZ 85 mg/m2/21d q 28d Bev 10 mg/kg /2w 2 cycles w9 MRI RANO Central pathology review Tissue MGMT (tmgmt) Serum MGMT (smgmt) Neoadjuvant phase w21 Concomitant phase w25 Adjuvant phase
28 Methods Endpoints: Primary: ORR (RANO) after 2 pre-rt cycles powered to detect a 30% difference between arms (α and β errors of 0.05 and 0.20). Secondary: 1. Toxicity 2. % neurological deterioration before RT 3. PFS 4. OS 5. 1y OS 6. MGMT Serum vs Tissue as predictive biomarkers CENTRAL RADIOLOGICAL REVIEW-CENTRAL PATHOLOGY REVIEW
29
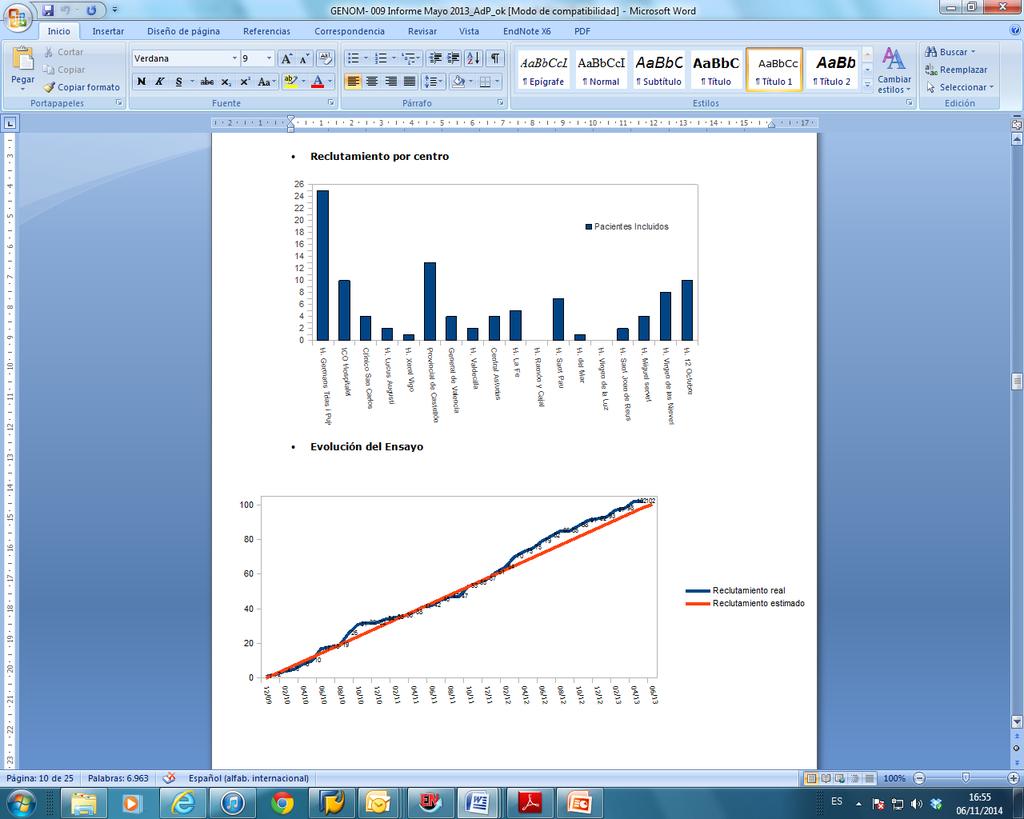
30 102 patients registered 2 GBM not confirmed 1 hemorrhage on MRI 51 allocated to TMZ arm 3 withdrawal Centralized Randomization (1: 1) IC 2 P before inclusion 1 did not meet inclusion criteria 48 started BEV & TMZ 3 progression 37 completed 2 8 toxicity c 45 started TMZ 30 received 2 c 9 progression 5 toxicity 1 refusal TMZ /RDT per protocol 22 (48.9%) Adjuvant TMZ completed 6 c: 6.7% completed 3 c: 15.6% 48 allocated to BEV arm Other treatment off-protocol 12 (26.7%) Palliative Care 5 (10.4%) 2 (4.4%) RDT 1 (2.1%) 8 (17.8%) RDT&TMZ 6 (12.5%) 1 *(2.2%) Other 4 (8.3%) *MORE THAN 1 TREATMENT BEV & TMZ & RDT per protocol 32 (66.7%) Adjuvant TMZ completed 6 c: 10.4% completed 3 c: 20.8%
31 Patient characteristics Characteristic TMZ Arm (n) BEV Arm (n) p Age median±range < ± ± Gender (M/F) 25/20 31/ ECOG PS MMS < Neurological deficit Surgery Biopsy Craneotomy DXM at inclusion (yes) % 56.3% 0.16 MGMT analyzed in tissue




32 HUGTIP Pathology Service Tissue revision & t MGMT Molecular Lab smgmt
33 Response Criteria by RANO/ centralized response revision CR PR SD PROGRESSION 0 50% >50% <25 % 25 % * =, =, =, =, * NEW LESIONS * DXM 0 =, =, =, * =, =, =, =, * T1-GD T2/FLAIR NEURO STATUS ALL ASCO 2009 ALL ALL ANY*


34 303 MRI images revised
35 Algorithm for central radiological review A Worsening of neurological status Disease progression Increase of dexametasone dose P by MRI with clinics and DXM stable B All responses (SD/PR/CR) by MRI CENTRALIZED RANO RESPONSE C D MRI revision mandatory Any change PI communication: revise and accept or no accept Eventual change of response and also data of progression Search the real data of progression
36 MRI review Review OK 72 No MRI to review (neurological deterioration or toxicity) 14 (15.1%) MRI sub-optimal 7 (7.5%) 20 discussed with the IP 17 IP accept review 1 IP didn t accept the review 2 no answer
37 Change of MRI response criteria MRI CENTRALIZED ASSESSMENT RMN IP CHANGE OF RESPONSE % CHANGE RESPONSE NO CHANGE % NO CHANGE RP 6 (to SD) SD 7 (to PR) 4 (to P) P 7 (to SD) % CHANGE 33.3 OVER CASES WITH MRI EVALUABLE:
38 FINAL RANO criteria change CHANGE % CHANGE = %= RP 6 to SD EE 7 to PR 4 to P P 3 to SD 3.2% % CHANGES 21.5% CHANGE 70.9% NO CHANGE OVER ALL PATIENTS INCLUDED IN THE TRIAL=93
39 Response by IP or centralized: final results By IP (evaluable) TMZ Arm N (%) BEV Arm N (%) CR - - PR 3 (7.0) 11 (25.0) SD 8 (18.6) 18 (40.9) PR & SD 11 (25.5) 29 (65.9) PD 32 (74.4) 15 (34,1) NE* 2 4 Centralized (evaluable) p TMZ Arm N (%) (95%CI) BEV Arm N (%) (95%CI) ( 9.3) p 11 (25.6) 6 (14.0) 17 (39.5) 10 (23.3) 28 (65.1) 33 (76.7) 15 (34.9)
40 SLP by IP and centralized -BEV Arm -TMZ Arm ARM BY IP TMZ 2.2 BEV 4.8 CENTRALIZED P=0.09 HR 95% CI 0.70 ( ) P=0.05 HR 95% CI 0.66 ( )
41 Overall survival -BEV Arm -TMZ Arm Arm mos 95%CI TMZ 7.7 (5.4-10) P 10.6 ( ) 1 y Suv 33% BEV HR; 95% CI 0.78 ( ) 48%
42 Results by MGMT status - MET - UnMET MGMT STATUS NOT METHYLATED METHYLATED PFS (mo) 2.2 ( ) 5.7 ( ) HR (95% CI) 0.31 ( ) P OS (mo) 5.3 ( ) ( ) HR (95% CI) P 0.40 ( ) 0.001
43 Conclusions A signal of higher efficacy is seen with the addition of Bevacizumab in this randomized neo-adjuvant trial. More responses and almost a significant tendency to better PFS and OS for patients treated with bevacizumab. Results seem to be reproduced in the BELOP trial with recurrent patients. Neo-adjuvant trials can be useful to identify signs of activity of new agents. Unmethylated patients should not be treated with neo-adjuvant therapy based on TMZ

44

45
Contemporary Management of Glioblastoma
 Contemporary Management of Glioblastoma Incidence Rates of Primary Brain Tumors Central Brain Tumor Registry of the United States, 1992-1997 100 Number of Cases per 100,000 Population 10 1 0.1 x I x I
Contemporary Management of Glioblastoma Incidence Rates of Primary Brain Tumors Central Brain Tumor Registry of the United States, 1992-1997 100 Number of Cases per 100,000 Population 10 1 0.1 x I x I
UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS
 UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS Antonio M. Omuro Department of Neurology Memorial Sloan-Kettering Cancer Center II International Neuro-Oncology Congress Sao Paulo, 08/17/12 CHALLENGES IN
UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS Antonio M. Omuro Department of Neurology Memorial Sloan-Kettering Cancer Center II International Neuro-Oncology Congress Sao Paulo, 08/17/12 CHALLENGES IN
Marizomib (MRZ): Brain Penetrant Irreversible Pan-Proteasome Inhibitor
: Brain Penetrant Irreversible Pan-Proteasome Inhibitor") MARIZOMIB (MRZ) WITH BEVACIZUMAB (BEV) IN WHO GRADE IV MALIGNANT GLIOMA (G4 MG): FULL ENROLLMENT RESULTS FROM THE PHASE 1, MULTICENTER, OPEN-LABEL STUDY Daniela Bota, MD, PhD 1, Annick Desjardins, MD,
MARIZOMIB (MRZ) WITH BEVACIZUMAB (BEV) IN WHO GRADE IV MALIGNANT GLIOMA (G4 MG): FULL ENROLLMENT RESULTS FROM THE PHASE 1, MULTICENTER, OPEN-LABEL STUDY Daniela Bota, MD, PhD 1, Annick Desjardins, MD,
Clinical Trials for Adult Brain Tumors - the Imaging Perspective
 Clinical Trials for Adult Brain Tumors - the Imaging Perspective Whitney B. Pope, M.D., Ph.D. Department of Radiology David Geffen School of Medicine at UCLA August 22, 2015 1 Disclosure of Financial Relationships
Clinical Trials for Adult Brain Tumors - the Imaging Perspective Whitney B. Pope, M.D., Ph.D. Department of Radiology David Geffen School of Medicine at UCLA August 22, 2015 1 Disclosure of Financial Relationships
성균관대학교삼성창원병원신경외과학교실신경종양학 김영준. KNS-MT-03 (April 15, 2015)
") 성균관대학교삼성창원병원신경외과학교실신경종양학 김영준 INTRODUCTIONS Low grade gliomas (LGG) - heterogeneous group of tumors with astrocytic, oligodendroglial, ependymal, or mixed cellular histology - In adults diffuse, infiltrating
성균관대학교삼성창원병원신경외과학교실신경종양학 김영준 INTRODUCTIONS Low grade gliomas (LGG) - heterogeneous group of tumors with astrocytic, oligodendroglial, ependymal, or mixed cellular histology - In adults diffuse, infiltrating
21/03/2017. Disclosure. Practice Changing Articles in Neuro Oncology for 2016/17. Gliomas. Objectives. Gliomas. No conflicts to declare
 Practice Changing Articles in Neuro Oncology for 2016/17 Disclosure No conflicts to declare Frances Cusano, BScPharm, ACPR April 21, 2017 Objectives Gliomas To describe the patient selection, methodology
Practice Changing Articles in Neuro Oncology for 2016/17 Disclosure No conflicts to declare Frances Cusano, BScPharm, ACPR April 21, 2017 Objectives Gliomas To describe the patient selection, methodology
CNS Tumors: The Med Onc Perspective. Ronald J. Scheff, MD Associate Clinical Professor Weill Medical College of Cornell U.
 CNS Tumors: The Med Onc Perspective Ronald J. Scheff, MD Associate Clinical Professor Weill Medical College of Cornell U. Disclosure Speakers Bureau, Merck Basic Oncology Concepts Tissue Diagnosis Stage
CNS Tumors: The Med Onc Perspective Ronald J. Scheff, MD Associate Clinical Professor Weill Medical College of Cornell U. Disclosure Speakers Bureau, Merck Basic Oncology Concepts Tissue Diagnosis Stage
Management of Glioma: The Basics Glioma Update The clinical challenge. Glioma a malignant disease of the CNS
 Management of Glioma: The Basics Glioma Update 3 oger Stupp, MD Department of Oncology & Cancer Center University Hospital Zurich, Switzerland (roger.stupp@usz.ch) Bern, 3. August 3 The clinical challenge
Management of Glioma: The Basics Glioma Update 3 oger Stupp, MD Department of Oncology & Cancer Center University Hospital Zurich, Switzerland (roger.stupp@usz.ch) Bern, 3. August 3 The clinical challenge
Systemic Treatment. Third International Neuro-Oncology Course. 23 May 2014
 Low-Grade Astrocytoma of the CNS: Systemic Treatment Third International Neuro-Oncology Course São Paulo, Brazil 23 May 2014 John de Groot, MD Associate Professor, Neuro-Oncology UT MD Anderson Cancer
Low-Grade Astrocytoma of the CNS: Systemic Treatment Third International Neuro-Oncology Course São Paulo, Brazil 23 May 2014 John de Groot, MD Associate Professor, Neuro-Oncology UT MD Anderson Cancer
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM ANAPLASTIC GLIOMAS CNS Site Group Anaplastic Gliomas Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM ANAPLASTIC GLIOMAS CNS Site Group Anaplastic Gliomas Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
Dr Roopinder Gillmore July 2017
 Dr Roopinder Gillmore July 2017 Resectable Borderline / locally advanced Metastatic 15-20% 15-20% 60-70% 22-28 months 9-15 months 6-12 months Does the patient have resectable disease?? Definitely not
Dr Roopinder Gillmore July 2017 Resectable Borderline / locally advanced Metastatic 15-20% 15-20% 60-70% 22-28 months 9-15 months 6-12 months Does the patient have resectable disease?? Definitely not
A Phase II Study on Efficacy, Safety and Intratumoral Pharmacokinetics of Oral Selinexor (KPT-330) in Patients with Recurrent Glioblastoma (GBM)
 in Patients with Recurrent Glioblastoma (GBM)") A Phase II Study on Efficacy, Safety and Intratumoral Pharmacokinetics of Oral Selinexor (KPT-330) in Patients with Recurrent Glioblastoma (GBM) Morten Mau-Sorensen 1, Scott Plotkin 2, Patrick Wen 3, Andrew
A Phase II Study on Efficacy, Safety and Intratumoral Pharmacokinetics of Oral Selinexor (KPT-330) in Patients with Recurrent Glioblastoma (GBM) Morten Mau-Sorensen 1, Scott Plotkin 2, Patrick Wen 3, Andrew
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr.
 Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
RINDOPEPIMUT (CDX-110) IN GLIOBLASTOMA
 IN GLIOBLASTOMA") RINDOPEPIMUT (CDX-110) IN GLIOBLASTOMA MULTIFORM GEINO 2014 Dra Estela Pineda Madrid Hospital Clínic Barcelona EGFRvIII in glioblastoma multiform The most common mutation of EGFR in GBM Expressed in 30%
RINDOPEPIMUT (CDX-110) IN GLIOBLASTOMA MULTIFORM GEINO 2014 Dra Estela Pineda Madrid Hospital Clínic Barcelona EGFRvIII in glioblastoma multiform The most common mutation of EGFR in GBM Expressed in 30%
Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First?
 Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First? Marc Peeters, MD, PhD Head of the Oncology Department Antwerp University Hospital Antwerp, Belgium marc.peeters@uza.be 71-year-old
Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First? Marc Peeters, MD, PhD Head of the Oncology Department Antwerp University Hospital Antwerp, Belgium marc.peeters@uza.be 71-year-old
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
VAL-083: Validated DNA-targeting Agent for Underserved Cancer Patients. September 2018
 VAL-083: Validated DNA-targeting Agent for Underserved Cancer Patients September 2018 Forward-Looking Statements Any statements contained in this presentation that do not describe historical facts may
VAL-083: Validated DNA-targeting Agent for Underserved Cancer Patients September 2018 Forward-Looking Statements Any statements contained in this presentation that do not describe historical facts may
Incidence of Early Pseudo-progression in a Cohort of Malignant Glioma Patients Treated With Chemoirradiation With Temozolomide
 405 Incidence of Early Pseudo-progression in a Cohort of Malignant Glioma Patients Treated With Chemoirradiation With Temozolomide Walter Taal, MD 1 Dieta Brandsma, MD, PhD 1 Hein G. de Bruin, MD, PhD
405 Incidence of Early Pseudo-progression in a Cohort of Malignant Glioma Patients Treated With Chemoirradiation With Temozolomide Walter Taal, MD 1 Dieta Brandsma, MD, PhD 1 Hein G. de Bruin, MD, PhD
Cilengitide (Impetreve) for glioblastoma multiforme. February 2012
 for glioblastoma multiforme. February 2012") Cilengitide (Impetreve) for glioblastoma multiforme February 2012 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to
Cilengitide (Impetreve) for glioblastoma multiforme February 2012 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to
MEETING SUMMARY ESMO 2018, Munich, Germany. Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER
 MEETING SUMMARY ESMO 2018, Munich, Germany Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER DISCLAIMER Please note: The views expressed within this presentation are the personal
MEETING SUMMARY ESMO 2018, Munich, Germany Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER DISCLAIMER Please note: The views expressed within this presentation are the personal
Radioterapia no Tratamento dos Gliomas de Baixo Grau
 Radioterapia no Tratamento dos Gliomas de Baixo Grau Dr. Luis Souhami University Montreal - Canada Low Grade Gliomas Relatively rare Heterogeneous, slow growing tumors WHO Classification Grade I Pilocytic
Radioterapia no Tratamento dos Gliomas de Baixo Grau Dr. Luis Souhami University Montreal - Canada Low Grade Gliomas Relatively rare Heterogeneous, slow growing tumors WHO Classification Grade I Pilocytic
Neuro-Oncology Program
 Neuro-Oncology Program The goals of the Neuro-oncology Committee are: 1) to improve duration and quality of life of brain tumor patients; 2) to assess disease and treatment-related effects on neurocognitive
Neuro-Oncology Program The goals of the Neuro-oncology Committee are: 1) to improve duration and quality of life of brain tumor patients; 2) to assess disease and treatment-related effects on neurocognitive
Scottish Medicines Consortium
 Scottish Medicines Consortium temozolomide 5, 20, 100 and 250mg capsules (Temodal ) Schering Plough UK Ltd No. (244/06) New indication: for the treatment of newly diagnosed glioblastoma multiforme concomitantly
Scottish Medicines Consortium temozolomide 5, 20, 100 and 250mg capsules (Temodal ) Schering Plough UK Ltd No. (244/06) New indication: for the treatment of newly diagnosed glioblastoma multiforme concomitantly
Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer
 Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of California
Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of California
IAN CROCKER = TIM HOWARD
 Winship Cancer Institute of Emory University Radiation as Consolidation in the Treatment of Newly Diagnosed CNS Lymphoma versus After Failure of Chemotherapy Pro: Upfront Radiation Ian Crocker MD, FACR,
Winship Cancer Institute of Emory University Radiation as Consolidation in the Treatment of Newly Diagnosed CNS Lymphoma versus After Failure of Chemotherapy Pro: Upfront Radiation Ian Crocker MD, FACR,
Concomitant (without adjuvant) temozolomide and radiation to treat glioblastoma: A retrospective study
 temozolomide and radiation to treat glioblastoma: A retrospective study") Concomitant (without adjuvant) temozolomide and radiation to treat glioblastoma: A retrospective study T Sridhar 1, A Gore 1, I Boiangiu 1, D Machin 2, R P Symonds 3 1. Department of Oncology, Leicester
Concomitant (without adjuvant) temozolomide and radiation to treat glioblastoma: A retrospective study T Sridhar 1, A Gore 1, I Boiangiu 1, D Machin 2, R P Symonds 3 1. Department of Oncology, Leicester
Glioblastoma: Current Treatment Approach 8/20/2018
 Glioblastoma: Current Treatment Approach 8/20/2018 Overview What is Glioblastoma? How is it diagnosed How is it treated? Principles of Treatment Surgery, Radiation, Chemotherapy Current Standard of care
Glioblastoma: Current Treatment Approach 8/20/2018 Overview What is Glioblastoma? How is it diagnosed How is it treated? Principles of Treatment Surgery, Radiation, Chemotherapy Current Standard of care
University of Zurich. Temozolomide and MGMT forever? Zurich Open Repository and Archive. Weller, M. Year: 2010
 University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich Year: 2010 Temozolomide and MGMT forever? Weller, M Weller, M (2010). Temozolomide and MGMT forever? Neuro-Oncology,
University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich Year: 2010 Temozolomide and MGMT forever? Weller, M Weller, M (2010). Temozolomide and MGMT forever? Neuro-Oncology,
2011 Oncology Highlights News from ASCO 2011:
 2011 Oncology Highlights News from ASCO 2011: Malignant Glioma David A. Reardon, M.D. Clinical Director Center for Neuro-Oncology Dana-Farber Cancer Institute 450 Brookline Avenue SW-430 Boston, MA 02215
2011 Oncology Highlights News from ASCO 2011: Malignant Glioma David A. Reardon, M.D. Clinical Director Center for Neuro-Oncology Dana-Farber Cancer Institute 450 Brookline Avenue SW-430 Boston, MA 02215
Clinical Management Protocol Chemotherapy [Glioblastoma Multiforme (CNS)] Protocol for Planning and Treatment
![Clinical Management Protocol Chemotherapy [Glioblastoma Multiforme (CNS)] Protocol for Planning and Treatment](/thumbs/87/96032554.jpg "Clinical Management Protocol Chemotherapy [Glioblastoma Multiforme (CNS)] Protocol for Planning and Treatment") Protocol for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: GLIOBLASTOMA MULTIFORME (CNS) Patient information given at each stage following agreed
Protocol for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: GLIOBLASTOMA MULTIFORME (CNS) Patient information given at each stage following agreed
Bevacizumab in combination with temozolomide and regional radiation therapy for up-front treatment of patients with newly-diagnosed glioblastoma
 Bevacizumab in combination with temozolomide and regional radiation therapy for up-front treatment of patients with newly-diagnosed glioblastoma Design and analysis of single-arm Phase II clinical trial
Bevacizumab in combination with temozolomide and regional radiation therapy for up-front treatment of patients with newly-diagnosed glioblastoma Design and analysis of single-arm Phase II clinical trial
EORTC (RTOG 0834 Endorsed) Opened: July 22, 2009
 Opened: July 22, 2009") January 2011 0834-1 EORTC 26053 22054 (RTOG 0834 Endorsed) Protocol Status: Opened: July 22, 2009 Title: Phase III Trial on Concurrent and Adjuvant Temozolomide Chemotherapy in Non-1P/19Q Deleted Anaplastic
January 2011 0834-1 EORTC 26053 22054 (RTOG 0834 Endorsed) Protocol Status: Opened: July 22, 2009 Title: Phase III Trial on Concurrent and Adjuvant Temozolomide Chemotherapy in Non-1P/19Q Deleted Anaplastic
NON-SURGICAL STRATEGY FOR ADULT EPENDYMOMA
 NON-SURGICAL STRATEGY FOR ADULT EPENDYMOMA Roberta Rudà Department of Neuro-Oncology University and City of Health and Science Hospital of Turin, Italy EORTC EANO ESMO Conference 2015 Istanbul, March 27-28
NON-SURGICAL STRATEGY FOR ADULT EPENDYMOMA Roberta Rudà Department of Neuro-Oncology University and City of Health and Science Hospital of Turin, Italy EORTC EANO ESMO Conference 2015 Istanbul, March 27-28
Hypofractionated radiation therapy for glioblastoma
 Hypofractionated radiation therapy for glioblastoma Luis Souhami, MD, FASTRO Professor McGill University Department of Oncology, Division of Radiation Oncology Montreal Canada McGill University Health
Hypofractionated radiation therapy for glioblastoma Luis Souhami, MD, FASTRO Professor McGill University Department of Oncology, Division of Radiation Oncology Montreal Canada McGill University Health
Concepts for a personalized neurosurgical oncology. XXIV Annual Conference Pietro Paoletti 27. November 2015
 Concepts for a personalized neurosurgical oncology Jörg-Christian Tonn Dept. of Neurosurgery Ludwig-Maximilian University München Großhadern Germany XXIV Annual Conference Pietro Paoletti 27. November
Concepts for a personalized neurosurgical oncology Jörg-Christian Tonn Dept. of Neurosurgery Ludwig-Maximilian University München Großhadern Germany XXIV Annual Conference Pietro Paoletti 27. November
DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID
 DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID RESUMEN DE ARTICULOS THERESA BOLERO 3 NOAH UP-DATE GEPAR SIXTO RADIOTHERAPY EBCTCG CTCs MISCELANEAS Lancet Oncol 2014;
DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID RESUMEN DE ARTICULOS THERESA BOLERO 3 NOAH UP-DATE GEPAR SIXTO RADIOTHERAPY EBCTCG CTCs MISCELANEAS Lancet Oncol 2014;
Management of Brain Metastases Sanjiv S. Agarwala, MD
 Management of Brain Metastases Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA, USA Incidence (US):
Management of Brain Metastases Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA, USA Incidence (US):
Newcastle Neuro-oncology Team Audit of Outcome of Glioblastoma Multiforme Chemoradiotherapy Treatment
 Newcastle Neuro-oncology Team Audit of Outcome of Glioblastoma Multiforme Chemoradiotherapy Treatment Jennifer Wright Neurosurgery SSC Audit Team Jennifer Wright, Rachel Tresman, Cyril Dubois, Surash Surash,
Newcastle Neuro-oncology Team Audit of Outcome of Glioblastoma Multiforme Chemoradiotherapy Treatment Jennifer Wright Neurosurgery SSC Audit Team Jennifer Wright, Rachel Tresman, Cyril Dubois, Surash Surash,
Glioblastoma and CNS tumors
 Glioblastoma and CNS tumors PRECEPTORSHIP PROGRAMME IMMUNO-ONCOLOGY Amsterdam, 27 May 2017 Patrick Roth Department of Neurology and Brain Tumor Center University Hospital Zurich Challenges in immunooncology
Glioblastoma and CNS tumors PRECEPTORSHIP PROGRAMME IMMUNO-ONCOLOGY Amsterdam, 27 May 2017 Patrick Roth Department of Neurology and Brain Tumor Center University Hospital Zurich Challenges in immunooncology
Crizotinib in addition to Radiotherapy and TMZ in newly diagnosed GBM
 Crizotinib in addition to Radiotherapy and TMZ in newly diagnosed GBM Juan M Sepúlveda Sánchez Unidad Multidisciplinar de Neurooncología Hospital 12 de Octubre Madrid GEINO 1402. Phase Ib, open-label,
Crizotinib in addition to Radiotherapy and TMZ in newly diagnosed GBM Juan M Sepúlveda Sánchez Unidad Multidisciplinar de Neurooncología Hospital 12 de Octubre Madrid GEINO 1402. Phase Ib, open-label,
CHMP Type II variation assessment report
 26 January 2017 EMA/CHMP/59238/2017 Invented name: Avastin International non-proprietary name: bevacizumab Procedure No. EMEA/H/C/000582/II/0093 Marketing authorisation holder (MAH): Roche Registration
26 January 2017 EMA/CHMP/59238/2017 Invented name: Avastin International non-proprietary name: bevacizumab Procedure No. EMEA/H/C/000582/II/0093 Marketing authorisation holder (MAH): Roche Registration
Bevacizumab rescue therapy extends the survival in patients with recurrent malignant glioma
 Original Article Bevacizumab rescue therapy extends the survival in patients with recurrent malignant glioma Lin-Bo Cai, Juan Li, Ming-Yao Lai, Chang-Guo Shan, Zong-De Lian, Wei-Ping Hong, Jun-Jie Zhen,
Original Article Bevacizumab rescue therapy extends the survival in patients with recurrent malignant glioma Lin-Bo Cai, Juan Li, Ming-Yao Lai, Chang-Guo Shan, Zong-De Lian, Wei-Ping Hong, Jun-Jie Zhen,
CILENT P Leblond, DIPG Meeting, Barcelone 2012
 CILENT-0902 Cilengitide (EMD121974) in combination with irradiation in children and adolescents with newly diagnosed diffuse intrinsic brainstem glioma : Phase I Study P Leblond, DIPG Meeting, Barcelone
CILENT-0902 Cilengitide (EMD121974) in combination with irradiation in children and adolescents with newly diagnosed diffuse intrinsic brainstem glioma : Phase I Study P Leblond, DIPG Meeting, Barcelone
Zurich Open Repository and Archive. Long-term survival of glioblastoma patients treated with radiotherapy and lomustine plus temozolomide
 University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich http://www.zora.uzh.ch Year: 2009 Long-term survival of glioblastoma patients treated with radiotherapy and lomustine
University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich http://www.zora.uzh.ch Year: 2009 Long-term survival of glioblastoma patients treated with radiotherapy and lomustine
Immunotherapy for Breast Cancer. Aurelio B. Castrellon Medical Oncology Memorial Healthcare System
 Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
CONSIDERATIONS IN DEVELOPMENT OF PEMBROLIZUMAB IN MSI-H CANCERS
 CONSIDERATIONS IN DEVELOPMENT OF PEMBROLIZUMAB IN MSI-H CANCERS December 2017 Christine K. Gause, Ph.D Executive Director, Biostatistics. 2 Microsatellite Instability-High Cancer - USPI KEYTRUDA is indicated
CONSIDERATIONS IN DEVELOPMENT OF PEMBROLIZUMAB IN MSI-H CANCERS December 2017 Christine K. Gause, Ph.D Executive Director, Biostatistics. 2 Microsatellite Instability-High Cancer - USPI KEYTRUDA is indicated
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents
 Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Chemotherapy for resectable liver mets: Options and Issues. Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA
 Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Immuno-Oncology. Glioblastoma and CNS tumors 5 July 2016 Siena, Italy
 ESMO Preceptorship Programme Immuno-Oncology From the essentials of tumour immunology to clinical application Glioblastoma and CNS tumors 5 July 2016 Siena, Italy Michael Weller Department of Neurology
ESMO Preceptorship Programme Immuno-Oncology From the essentials of tumour immunology to clinical application Glioblastoma and CNS tumors 5 July 2016 Siena, Italy Michael Weller Department of Neurology
Maintenance Therapy for Advanced NSCLC: When, What, Why & What s Left After Post-Maintenance Relapse?
 Maintenance Therapy for Advanced NSCLC: When, What, Why & What s Left After Post-Maintenance Relapse? Mark A. Socinski, MD Professor of Medicine Multidisciplinary Thoracic Oncology Program Lineberger Comprehensive
Maintenance Therapy for Advanced NSCLC: When, What, Why & What s Left After Post-Maintenance Relapse? Mark A. Socinski, MD Professor of Medicine Multidisciplinary Thoracic Oncology Program Lineberger Comprehensive
Neoplasie del laringe Diagnosi e trattamento
 Neoplasie del laringe Diagnosi e trattamento Venerdì 22 maggio 2015 Alessandria Trattamenti non chirurgici: Preservazione d organo, malattia localmente avanzata Marco C Merlano A.O. S.Croce e Carle, Ospedale
Neoplasie del laringe Diagnosi e trattamento Venerdì 22 maggio 2015 Alessandria Trattamenti non chirurgici: Preservazione d organo, malattia localmente avanzata Marco C Merlano A.O. S.Croce e Carle, Ospedale
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón
 Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
Temozolomide with Radiotherapy for the Treatment of Malignant Gliomas, Center Experience
 Temozolomide with Radiotherapy for the Treatment of Malignant Gliomas, Center Experience *Ehab Abdou and **Mohamed Gaafar *Department of Radiation Oncology, Faculty of Medicine, Al-Azhar University, Cairo,
Temozolomide with Radiotherapy for the Treatment of Malignant Gliomas, Center Experience *Ehab Abdou and **Mohamed Gaafar *Department of Radiation Oncology, Faculty of Medicine, Al-Azhar University, Cairo,
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist
 Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
Targeted/Immunotherapy & Molecular Profiling State-of-the-art in Cancer Care
 Targeted/Immunotherapy & Molecular Profiling State-of-the-art in Cancer Care Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland
Targeted/Immunotherapy & Molecular Profiling State-of-the-art in Cancer Care Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland
Oncological Management of Brain Tumours. Anna Maria Shiarli SpR in Clinical Oncology 15 th July 2013
 Oncological Management of Brain Tumours Anna Maria Shiarli SpR in Clinical Oncology 15 th July 2013 Outline General considerations of Primary Brain Tumours: epidemiology, pathology, presentation. Diagnosis
Oncological Management of Brain Tumours Anna Maria Shiarli SpR in Clinical Oncology 15 th July 2013 Outline General considerations of Primary Brain Tumours: epidemiology, pathology, presentation. Diagnosis
ESMO 2017, Madrid, Spain Dr. Loredana Vecchione Charite Comprehensive Cancer Center, Berlin HIGHLIGHTS ON CANCERS OF THE UPPER GI TRACT
 ESMO 2017, Madrid, Spain Dr. Loredana Vecchione Charite Comprehensive Cancer Center, Berlin HIGHLIGHTS ON CANCERS OF THE UPPER GI TRACT DOCETAXEL, OXALIPLATIN AND FLUOROURACIL/LEUCOVORIN (FLOT) FOR RESECTABLE
ESMO 2017, Madrid, Spain Dr. Loredana Vecchione Charite Comprehensive Cancer Center, Berlin HIGHLIGHTS ON CANCERS OF THE UPPER GI TRACT DOCETAXEL, OXALIPLATIN AND FLUOROURACIL/LEUCOVORIN (FLOT) FOR RESECTABLE
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES
 DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES Marco Krengli Radiotherapy, Department of Translational Medicine, University of Piemonte Orientale A. Avogadro THE STANDARD OF CARE
DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES Marco Krengli Radiotherapy, Department of Translational Medicine, University of Piemonte Orientale A. Avogadro THE STANDARD OF CARE
National Horizon Scanning Centre. Bevacizumab (Avastin) for glioblastoma multiforme - relapsed. August 2008
 for glioblastoma multiforme - relapsed. August 2008") Bevacizumab (Avastin) for glioblastoma multiforme - relapsed August 2008 This technology summary is based on information available at the time of research and a limited literature search. It is not intended
Bevacizumab (Avastin) for glioblastoma multiforme - relapsed August 2008 This technology summary is based on information available at the time of research and a limited literature search. It is not intended
Precision medicine for gliomas
 Precision medicine for YAZMIN ODIA, MD MS LEAD PHYSICIAN OF MEDICAL NEURO-ONCOLOGY DISCLOSURES Novocure: Advisory Board for Optune in No other financial conflicts of interest Glioma OVERVIEW INFILTRATIVE,
Precision medicine for YAZMIN ODIA, MD MS LEAD PHYSICIAN OF MEDICAL NEURO-ONCOLOGY DISCLOSURES Novocure: Advisory Board for Optune in No other financial conflicts of interest Glioma OVERVIEW INFILTRATIVE,
Lung Cancer Non-small Cell Local, Regional, Small Cell, Other Thoracic Cancers: The Question Isn t Can We, but Should We
 Lung Cancer Non-small Cell Local, Regional, Small Cell, Other Thoracic Cancers: The Question Isn t Can We, but Should We Edward Garon, MD, MS Associate Professor Director- Thoracic Oncology Program David
Lung Cancer Non-small Cell Local, Regional, Small Cell, Other Thoracic Cancers: The Question Isn t Can We, but Should We Edward Garon, MD, MS Associate Professor Director- Thoracic Oncology Program David
UPDATE FROM ASCO GU FEBRUARY 2018, SAN FRANCISCO, USA. Prof. David Pfister University Hospital of Cologne Germany RENAL CELL CARCINOMA
 UPDATE FROM ASCO GU FEBRUARY 2018, SAN FRANCISCO, USA Prof. David Pfister University Hospital of Cologne Germany RENAL CELL CARCINOMA DISCLAIMER Please note: The views expressed within this presentation
UPDATE FROM ASCO GU FEBRUARY 2018, SAN FRANCISCO, USA Prof. David Pfister University Hospital of Cologne Germany RENAL CELL CARCINOMA DISCLAIMER Please note: The views expressed within this presentation
PRESURGICAL PLANNING. Strongly consider neuropsychological evaluation before functional imaging study Strongly consider functional imaging study
 NOTE: Consider Clinical Trials as treatment options for eligible patients. Page 1 of 6 RADIOLOGICAL PRESENTATION PRESURGICAL PLANNING TREATMENT Imaging study suggestive of glioma 1 Left hemisphere speech/motor
NOTE: Consider Clinical Trials as treatment options for eligible patients. Page 1 of 6 RADIOLOGICAL PRESENTATION PRESURGICAL PLANNING TREATMENT Imaging study suggestive of glioma 1 Left hemisphere speech/motor
FACT SHEET. About Optune
 About Optune Optune is the Tumor Treating Fields (TTFields) delivery system that is approved by the United States (US) Food and Drug Administration (FDA) for the treatment of adult patients with glioblastoma.
About Optune Optune is the Tumor Treating Fields (TTFields) delivery system that is approved by the United States (US) Food and Drug Administration (FDA) for the treatment of adult patients with glioblastoma.
NSCLC: immunotherapy as a first-line treatment. Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To)
") NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
Colon cancer: Highlights. Filippo Pietrantonio Istituto Nazionale dei Tumori di Milano
 Colon cancer: Highlights Filippo Pietrantonio Istituto Nazionale dei Tumori di Milano Agenda 1) Metastatic colorectal cancer First-line treatment molecularly unselected: FOLFOXIRI-bev (CHARTA trial) Later-line
Colon cancer: Highlights Filippo Pietrantonio Istituto Nazionale dei Tumori di Milano Agenda 1) Metastatic colorectal cancer First-line treatment molecularly unselected: FOLFOXIRI-bev (CHARTA trial) Later-line
Karcinom dojke. PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski
 Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
HER2-Targeted Rx. An Historical Perspective
 HER2-Targeted Rx An Historical Perspective Trastuzumab: Front Line Rx for MBC Median 20.3 v. 25.1 mo P = 0.046 HR 0.8 65% of control patients crossed over Slamon D, et al. N Engl J Med, 2001; 344:783 Trastuzumab:Front-line
HER2-Targeted Rx An Historical Perspective Trastuzumab: Front Line Rx for MBC Median 20.3 v. 25.1 mo P = 0.046 HR 0.8 65% of control patients crossed over Slamon D, et al. N Engl J Med, 2001; 344:783 Trastuzumab:Front-line
Glioblastoma and CNS tumors
 Glioblastoma and CNS tumors PRECEPTORSHIP PROGRAMME IMMUNO-ONCOLOGY Amsterdam, 1 October 2016 Patrick Roth Department of Neurology and Brain Tumor Center University Hospital Zurich Immunology in the CNS
Glioblastoma and CNS tumors PRECEPTORSHIP PROGRAMME IMMUNO-ONCOLOGY Amsterdam, 1 October 2016 Patrick Roth Department of Neurology and Brain Tumor Center University Hospital Zurich Immunology in the CNS
Non-methylated MGMT as Predictive Factor in Newly Diagnosed Glioblastoma. Multiforme Treated with Bevacizumab
 Research Article imedpub Journals www.imedpub.com Archives in Cancer Research DOI: 10.21767/2254-6081.100177 Non-methylated MGMT as Predictive Factor in Newly Diagnosed Glioblastoma Multiforme Treated
Research Article imedpub Journals www.imedpub.com Archives in Cancer Research DOI: 10.21767/2254-6081.100177 Non-methylated MGMT as Predictive Factor in Newly Diagnosed Glioblastoma Multiforme Treated
MÁS ALLA DE LA PRIMERA LÍNEA: SECUENCIA DE TRATAMIENTO. Dra. Ruth Vera Complejo Hospitalario de Navarra
 MÁS ALLA DE LA PRIMERA LÍNEA: SECUENCIA DE TRATAMIENTO Dra. Ruth Vera Complejo Hospitalario de Navarra GOALS Prolongation of survival Cure Improving tumour-related symptoms Stopping tumour progression
MÁS ALLA DE LA PRIMERA LÍNEA: SECUENCIA DE TRATAMIENTO Dra. Ruth Vera Complejo Hospitalario de Navarra GOALS Prolongation of survival Cure Improving tumour-related symptoms Stopping tumour progression
TRIALs of CDK4/6 inhibitor in women with hormone-receptor-positive metastatic breast cancer
 TRIALs of CDK4/6 inhibitor in women with hormone-receptor-positive metastatic breast cancer Marta Bonotto Department of Oncology University Hospital of Udine TRIALs of CDK4/6 inhibitor in women with hormone-receptor-positive
TRIALs of CDK4/6 inhibitor in women with hormone-receptor-positive metastatic breast cancer Marta Bonotto Department of Oncology University Hospital of Udine TRIALs of CDK4/6 inhibitor in women with hormone-receptor-positive
Brain Schema March 2018
 Breast Cancer w/brain Mets 14 2283 / Lilly Abemaciclib PO Breast Ca or Melanoma mets allowed Leptomeningeal mets excluded Want brain met tissue Melanoma w/brain Mets 14 2209 / Bristol Myers Squibb Nivolumab
Breast Cancer w/brain Mets 14 2283 / Lilly Abemaciclib PO Breast Ca or Melanoma mets allowed Leptomeningeal mets excluded Want brain met tissue Melanoma w/brain Mets 14 2209 / Bristol Myers Squibb Nivolumab
Presentation Number: LBA18_PR. Lecture Time: 09:15-09:27. Speakers: Heinz-Josef J. Lenz (Los Angeles, US) Background
 Background") LBA18_PR - Durable Clinical Benefit With Nivolumab (NIVO) Plus Low-Dose Ipilimumab (IPI) as First-Line Therapy in Microsatellite Instability-High/Mismatch Repair Deficient (MSI-H/dMMR) Metastatic Colorectal
LBA18_PR - Durable Clinical Benefit With Nivolumab (NIVO) Plus Low-Dose Ipilimumab (IPI) as First-Line Therapy in Microsatellite Instability-High/Mismatch Repair Deficient (MSI-H/dMMR) Metastatic Colorectal
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
University of Colorado Cancer Center Brain Disease Site Schema
 GBM FIRST LINE 18 0376/Kazia Phase 2a study (Part 1): A phase 2a study to evaluate the safety, pharmacokinetics and clinical activity of the PI3K/mTOR inhibitor GDC 0084 administered to patients with glioblastoma
GBM FIRST LINE 18 0376/Kazia Phase 2a study (Part 1): A phase 2a study to evaluate the safety, pharmacokinetics and clinical activity of the PI3K/mTOR inhibitor GDC 0084 administered to patients with glioblastoma
Roche announces final phase III study results of Avastin plus radiotherapy and chemotherapy in people with an aggressive form of brain cancer
 Media Release Basel, 1 June 2013 Roche announces final phase III study results of Avastin plus radiotherapy and chemotherapy in people with an aggressive form of brain cancer Roche (SIX: RO, ROG; OTCQX:
Media Release Basel, 1 June 2013 Roche announces final phase III study results of Avastin plus radiotherapy and chemotherapy in people with an aggressive form of brain cancer Roche (SIX: RO, ROG; OTCQX:
Evidenze cliniche nel trattamento del RCC
 Criteri di scelta nel trattamento sistemico del carcinoma renale Evidenze cliniche nel trattamento del RCC Alessandro Morabito Unità Sperimentazioni Cliniche Istituto Nazionale Tumori di Napoli Napoli,
Criteri di scelta nel trattamento sistemico del carcinoma renale Evidenze cliniche nel trattamento del RCC Alessandro Morabito Unità Sperimentazioni Cliniche Istituto Nazionale Tumori di Napoli Napoli,
The Role of Radiation Therapy in the Treatment of Brain Metastases. Matthew Cavey, M.D.
 The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
The next wave of successful drug therapy strategies in HER2-positive breast cancer. Hans Wildiers University Hospitals Leuven Belgium
 The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
INMUNOTERAPIA I. Dra. Virginia Calvo
 INMUNOTERAPIA I Dra. Virginia Calvo LBA62. Health-related quality of life (HRQoL) for Pembrolizumab or placebo plus Carboplatin and Paclitaxel or nab-paclitaxel in patients with metastatic squamous NSCLC:
INMUNOTERAPIA I Dra. Virginia Calvo LBA62. Health-related quality of life (HRQoL) for Pembrolizumab or placebo plus Carboplatin and Paclitaxel or nab-paclitaxel in patients with metastatic squamous NSCLC:
Overview. What s New in the Treatment of Pancreatic Cancer? Lots! Steven J. Cohen, M.D. Fox Chase Cancer Center September 17, 2013
 What s New in the Treatment of Pancreatic Cancer? Lots! Steven J. Cohen, M.D. Fox Chase Cancer Center September 17, 2013 Overview Staging and Workup Resectable Disease Surgery Adjuvant therapy Locally
What s New in the Treatment of Pancreatic Cancer? Lots! Steven J. Cohen, M.D. Fox Chase Cancer Center September 17, 2013 Overview Staging and Workup Resectable Disease Surgery Adjuvant therapy Locally
Optimal Management of Isolated HER2+ve Brain Metastases
 Optimal Management of Isolated HER2+ve Brain Metastases Eliot Sims November 2013 Background Her2+ve patients 15% of all breast cancer Even with adjuvant trastuzumab 10-15% relapse Trastuzumab does not
Optimal Management of Isolated HER2+ve Brain Metastases Eliot Sims November 2013 Background Her2+ve patients 15% of all breast cancer Even with adjuvant trastuzumab 10-15% relapse Trastuzumab does not
Overview: Immunotherapy in CNS Metastases
 Overview: Immunotherapy in CNS Metastases Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland Clinic Disclosures Consultant- Monteris
Overview: Immunotherapy in CNS Metastases Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland Clinic Disclosures Consultant- Monteris
Rationale for Multimodality Therapy for High Risk Localized Prostate Cancer
 Rationale for Multimodality Therapy for High Risk Localized Prostate Cancer 100 80 60 Cancer Death Rates for Men, US 1930-2002 Rate Per 100,000 Lung William K. Oh, M.D. 40 Stomach Colon & rectum Prostate
Rationale for Multimodality Therapy for High Risk Localized Prostate Cancer 100 80 60 Cancer Death Rates for Men, US 1930-2002 Rate Per 100,000 Lung William K. Oh, M.D. 40 Stomach Colon & rectum Prostate
Maintenance paradigm in non-squamous NSCLC
 Maintenance paradigm in non-squamous NSCLC L. Paz-Ares Hospital Universitario Virgen del Rocío Sevilla Agenda Theoretical basis The data The comparisons Agenda Theoretical basis The data The comparisons
Maintenance paradigm in non-squamous NSCLC L. Paz-Ares Hospital Universitario Virgen del Rocío Sevilla Agenda Theoretical basis The data The comparisons Agenda Theoretical basis The data The comparisons
Brain mets under I.O.
 Brain mets under I.O. Bernard Escudier Gustave Roussy, Villejuif, France Disclosure Honorarium received from BMS, Novartis, Pfizer, Bayer, Roche, Exelixis, Ipsen, Eisai, Calithera Travel Grant from BMS,
Brain mets under I.O. Bernard Escudier Gustave Roussy, Villejuif, France Disclosure Honorarium received from BMS, Novartis, Pfizer, Bayer, Roche, Exelixis, Ipsen, Eisai, Calithera Travel Grant from BMS,
Targeted Therapies in Metastatic Colorectal Cancer: An Update
 Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
New Paradigms for Treatment of. Erminia Massarelli, MD, PHD, MS Clinical Associate Professor
 New Paradigms for Treatment of Head and Neck cancers Erminia Massarelli, MD, PHD, MS Clinical Associate Professor City of Hope Disclosure Statement Grant/Research Support frommerck Bristol Grant/Research
New Paradigms for Treatment of Head and Neck cancers Erminia Massarelli, MD, PHD, MS Clinical Associate Professor City of Hope Disclosure Statement Grant/Research Support frommerck Bristol Grant/Research
Media Release. Basel, 17 November 2012
 Media Release Basel, 17 November 2012 Roche study showed that Avastin helped people with newly diagnosed glioblastoma live longer without their disease worsening when added to radiation and chemotherapy
Media Release Basel, 17 November 2012 Roche study showed that Avastin helped people with newly diagnosed glioblastoma live longer without their disease worsening when added to radiation and chemotherapy
Douglas Jolly Executive VP R&D Tocagen Inc.
 REPLICATING RETROVIRUSES FOR MANIPULATION OF THE TUMOR IMMUNE ECOSYSTEM: PRECLINICAL AND CLINICAL OUTCOMES. Douglas Jolly Executive VP R&D Tocagen Inc. PEGS 2018 IT Track Boston May 1 2018 Outline Phase
REPLICATING RETROVIRUSES FOR MANIPULATION OF THE TUMOR IMMUNE ECOSYSTEM: PRECLINICAL AND CLINICAL OUTCOMES. Douglas Jolly Executive VP R&D Tocagen Inc. PEGS 2018 IT Track Boston May 1 2018 Outline Phase
Zurich Open Repository and Archive. Long-term survival of glioblastoma patients treated with radiotherapy and lomustine plus temozolomide
 University of Zurich Zurich Open Repository and Archive Winterthurerstr. 19 CH-857 Zurich http://www.zora.uzh.ch Year: 29 Long-term survival of glioblastoma patients treated with radiotherapy and lomustine
University of Zurich Zurich Open Repository and Archive Winterthurerstr. 19 CH-857 Zurich http://www.zora.uzh.ch Year: 29 Long-term survival of glioblastoma patients treated with radiotherapy and lomustine
Lynn S. Ashby 1*, Kris A. Smith 2 and Baldassarre Stea 3
 Ashby et al. World Journal of Surgical Oncology (2016) 14:225 DOI 10.1186/s12957-016-0975-5 REVIEW Gliadel wafer implantation combined with standard radiotherapy and concurrent followed by adjuvant temozolomide
Ashby et al. World Journal of Surgical Oncology (2016) 14:225 DOI 10.1186/s12957-016-0975-5 REVIEW Gliadel wafer implantation combined with standard radiotherapy and concurrent followed by adjuvant temozolomide
BEATcc Trial: ENGOT-Cx10 / GEICO 68-C / JGOG1084. GCIG Meeting
 BEATcc Trial: ENGOT-Cx10 / GEICO 68-C / JGOG1084 GCIG Meeting Ana Oaknin, MD PhD Head of Gynecologic Cancer Program. Vall d Hebron Institute of Oncology(VHIO). Vall d Hebron University Hospital. GEICO
BEATcc Trial: ENGOT-Cx10 / GEICO 68-C / JGOG1084 GCIG Meeting Ana Oaknin, MD PhD Head of Gynecologic Cancer Program. Vall d Hebron Institute of Oncology(VHIO). Vall d Hebron University Hospital. GEICO
Neurocognitive Assessment in Patients with Brain Metastases. Martin Klein VU University Medical Center Amsterdam, The Netherlands
 Neurocognitive Assessment in Patients with Brain Metastases Martin Klein VU University Medical Center Amsterdam, The Netherlands Treatment Outcomes I Traditional/primary endpoints of efficacy:! Physician
Neurocognitive Assessment in Patients with Brain Metastases Martin Klein VU University Medical Center Amsterdam, The Netherlands Treatment Outcomes I Traditional/primary endpoints of efficacy:! Physician
Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen?
 Department of Radiation Oncology Chairman: Prof. Dr. Matthias Guckenberger Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen? Matthias
Department of Radiation Oncology Chairman: Prof. Dr. Matthias Guckenberger Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen? Matthias
Nivolumab: esperienze italiane nel carcinoma polmonare avanzato
 NSCLC avanzato: quali novità nel 2018? Negrar, 30 Ottobre 2018 Nivolumab: esperienze italiane nel carcinoma polmonare avanzato Francesco Grossi UOC Oncologia Medica Fondazione IRCCS Ca Granda Ospedale
NSCLC avanzato: quali novità nel 2018? Negrar, 30 Ottobre 2018 Nivolumab: esperienze italiane nel carcinoma polmonare avanzato Francesco Grossi UOC Oncologia Medica Fondazione IRCCS Ca Granda Ospedale
Weitere Kombinationspartner der Immunotherapie
 1 Weitere Kombinationspartner der Immunotherapie Rolf Stahel University Hospital of Zürich Zürich, 9.12.216 2 Immunotherapy in a multimodality approach NSCLC Advanced disease Checkpoint inhibitors for
1 Weitere Kombinationspartner der Immunotherapie Rolf Stahel University Hospital of Zürich Zürich, 9.12.216 2 Immunotherapy in a multimodality approach NSCLC Advanced disease Checkpoint inhibitors for
GEINO TRIALS. RESULTS IN 2015
 VII Symposium Educacional GEINO Madrid, 3-4 diciembre 2015 GEINO TRIALS. RESULTS IN 2015 Juan M Sepúlveda Sánchez Unidad Multidisciplinar de Neurooncología Hospital 12 de Octubre GEINO-11: A Prospective
VII Symposium Educacional GEINO Madrid, 3-4 diciembre 2015 GEINO TRIALS. RESULTS IN 2015 Juan M Sepúlveda Sánchez Unidad Multidisciplinar de Neurooncología Hospital 12 de Octubre GEINO-11: A Prospective