MANAGEMENT OF WILMS TUMOUR- ROLE OF RADIOTHERAPY
|
|
|
- Dylan Williamson
- 5 years ago
- Views:
Transcription

1 MANAGEMENT OF WILMS TUMOUR- ROLE OF RADIOTHERAPY DR. AHITAGNI BISWAS MD, DNB, ECMO ASSISTANT PROFESSOR DEPARTMENT OF RADIOTHERAPY & ONCOLOGY ALL INDIA INSTITUTE OF MEDICAL SCIENCES, NEW DELHI 20 th ICRO PG TEACHING COURSE, HYDERABAD, TH JULY 2015
2 EPIDEMIOLOGY Wilms tumour (nephroblastoma)-embryonic kidney tumor Most common abdominal tumour in children- 6% of childhood cancer Incidence rate in children younger than 15 years is 7 per million population -Birch et al. Hematol Oncol Clin North Am 1995;9: to 500 new cases in the US per year >75% patients present before 5 years of age Children present with more advanced disease in less developed nations
3 MOLECULAR BIOLOGY Function Locus Syndromic association Frequency of gene aberration Tumour suppressor gene Role in glomerular & gonadal development Effect on IGF2, the H19 tumorsuppressor gene, and the P57 cell cycle regulator 11p13 WAGR (WT, aniridia, genito-urinary malformation, mental retardation) Denys-Drashsyndrome (pseudohermaphroditism, mesangial sclerosis, renal failure, WT) 11p15.5 Beckwith- Wiedemannsyndrome (somatic gigantism, omphalocele, macroglossia, genitourinary abnormalities, ear creases, hypoglycemia, hemihypertrophy) Germline mutation: 82% in pts with rena failure/ GU anomali 10-20% of sporadic 4% offamilial WT LOH 11p15.5 in 30% Loss of imprinting o IGF2 in 40% of spo WT Tumour suppressor gene Xq WTX inactivation in of sporadic WT 1 Encodes β-catenin Role in WNT pathway muta on in 10% o 3p21 - Gain of function sporadic WT
4 CLINICAL PRESENTATION Abdominal mass (80-90%) Abdominal pain (30-40%) Haematuria (20-25%) Fever (20-25%) Hypertension Varicocele Metastatic symptoms-rare



5 DIAGNOSTIC WORK-UP




6 STAGING


7 PATHOLOGY Soft, homogeneous, tan to grey in colour with occasional foci of haemorrhage & necrosis Well circumscribed margin Enclosed by renal capsule/fibrous pseudo-capsule Bilateral-7% & multifocal -12% of cases Tumor can contain a mixture of cells: blastemal cells stromal cells epithelial cells High degree of anaplasia associated with poor outcomes



8 (A) WT with tightly packed blue cells consistent with blastemal component & interspersed primitive tubules, representing the epithelial component. Although multiple mitotic figures are seen, none are atypical in this field; (B) Focal anaplasia present in other areas characterised by cells with hyperchromatic, pleomorphic nuclei & abnormal mitoses
9 TREATMENT OPTIONS: NWTS VERSUS SIOP WTS Treatment principle: Nephrectomy adjuvant chemo ±RT Advantages: Avoidance of Administration of chemo to a patient with benign disease Administration of chemo to a patient with a different histological type of malignant tumour Modification of tumour histology Loss of staging information SIOP Treatment Principle: Pre-op chemo Nephrectomy adjuvant chemo ±RT Advantages: Tumour downsizing thereby making surgery simpler and ing intra-op tumor rupture & intraabd recurrence Makes nephron sparing surgery possible




10 1 Intra-op tumour spillage in NWTS protocol Tumour downsizing with pre-op chemo in SIOP protocol
11 1 NWTS 1-4 SCHEMA
12 NWTS-1 ( ) Is post-op RT necessary in group I disease? Is single agent chemo with vincristine (VCR) or actinomycind (AMD) equivalent to combining these drugs for group II and III disease? Is preoperative VCR of value in group IV disease? Radiation doses adjusted for age Birth 18 mo: 18 to 24 Gy mo: 24 to 30 Gy mo: 30 to 35 Gy 41 moor older: Gy -D Angio et al. Cancer 1976;38:
13 1 NWTS-1 RESULTS Post-op RT not needed for group I <2 yrs VA better than either agent alone for group II and III Pre-op VCR not useful in group IV 4 yrrfs for group I pts >2 yrstreated with AMD +RT-76% 4 yrrfs for group II/III pts treated with VA + RT-79%
14 1 NWTS-1 RESULTS 2-year RFS: Favorable histology- 89% Unfavorable histology- 29% Poor prognostic factors Large tumor size Lymph node involvement Age >2 years No RT dose response between Gy Delays of 10 days for post-op RT found acceptable WAI not necessary for tumor spills confined to the flank
15 1 NWTS-2 ( ) 79) Can VA substitute for RT in older children with Group I disease? Is protracted period of adjuvant VA helpful for Groups II IV disease? Is addition of Doxoto VA of value in Groups II IV disease? -D Angio et al. Cancer 1981;47:
16 1 NWTS-2 RESULTS VA can substitute for RT in Group I disease VA x 6 months = VA x 15 months for Group I disease Addition of Doxo to VA+RT for Group II-IV disease provided benefit Worse 2-year survival for LN + disease (54% vs 82%) and patients with unfavorable histology (54% vs 90%)
17 NWTS-3 ( ) Patients stratified by stage instead of group FH & UH incorporated in the treatment algorithm Five questions Can duration of chemotherapy be shortened for Stage I FH? Can RT be eliminated for Stage II FH? What is the minimum effective RT dose for Stage III FH? Is Doxoclearly beneficial and necessary for Stage II & III FH? Will addition of CTX improve survival in Stage I IV UH and Stage IV FH? -Green et al. Pediatr Clin North Am 1991;38:
18 1 NWTS-3 Stage I FH: VA (no RT) 24 vs 10 weeks Stage II FH: 3 vs. 2 drugs (VA±D) ± RT 20 Gy Stage III FH: 3 vs. 2 drugs (VA±D) + RT 10 vs. 20 Gy Stage IV FH and all UH: RT + 3 drugs ±CTX
19 1 NWTS-3 RESULTS Stage I: VA x 10 wksvs. VA x 24 wksequivalent 4-year RFS 89% & OS 96% Stage II: no difference between 2 or 3 drugs with or without RT 4-year RFS 87% & OS 91% Stage III: No stat sig difference in abdominal relapse between 10 and 20 Gyof RT; trend favored use of Doxoor 20 Gyof RT 4-year RFS 82% & OS 91%
20 2 NWTS-3 RESULTS Stage IV FH: 4 drugs equal to 3 drugs (both included flank RT/WAI + WLI) 4-year RFS 79% & OS 80% Anaplasia 4 drugs better than 3 drugs for stage II-IV Trend toward improved outcome with 4 drug regimen for CCSK 4 yros -25% for RTK in both arms
21 2 NWTS-4 ( ) Addressed issues of minimization of therapy and customization by stage & histology Evaluate the role of pulse dosed intensive chemotherapy -Green et al. J Clin Oncol 1998;16:


22 2 NWTS-4 SCHEMA
23 2 NWTS-4 RESULTS Pulse intensive chemotherapy feasible, produce less hematologic toxicity and allow for increased drug dose-intensity Cost analysis showed savings of $790,000 a year in the US if all Wilms patients were treated on pulse-intensive regimens


24 NWTS-5 SCHEMA -Grundy et al. J Clin Oncol 2005;23:
25 NWTS-5 RESULTS-LOH LOH 1p / 16q LOH 1p associated with significantly worse RFS in Stage II but not Stage III/IV Suggests that adverse effects of LOH 1p can be overcome by more aggressive chemotherapy -Grundy et al. J Clin Oncol 2005;23:
26 2 NWTS-5 SELECTED RESULTS -FH Stage I FH: 4 y RFS 92% & OS 98% Stage II FH: 4 y RFS 83% & OS 92% Stage III FH: 4 y RFS 85.3% & OS 93.9% Stage IV FH: 4 y EFS 74.6% (most of these patients WLI)
27 2 NWTS-5 SELECTED RESULTS UH Diffuse Anaplasia:2 yr EFS- Stage I-64.3 % Stage II- 79.5% Stage III- 62.7% Stage IV- 33.6% CCSK:4 yr RFS- Stage I IV- 77.6% 6/9 Stage IV pts relapsed RTK Stage I- 50% Stage II- 33.3% Stage III- 33.3% Stage IV-21.4 % Stage V-0%
28 2 NWTS TREATMENT GUIDELINES Stage Stage I FH/UH Stage II FH Stage III + IV FH Stage II-IV UH Treatment VA x18 wks VA x 18 wks VAD x24 wks; RT to tumour bed ±metastatic site V,A,CTX,VP-16 x 24 wks; RT to tumour bed ±metastatic site
29 2 CURRENT PROTOCOLS AREN 0532 FH Stage I through FH Stage III Standard Risk
30 3 AREN 0533 & AREN 0321 AREN 0533 FH Stage III High Risk FH Stage IV AREN 0321 UH Wilms CCSK RTK RCC


31 3 AREN 0533
32 3 COG RISK STRATIFICATION


33 3 COG-RADIOTHERAPY GUIDELINES


34 COG-TREATMENT GUIDELINES EE4A-VA; DD4A-VAD; M-VAD/CyE; I-VDCy/CyE; UH1-VDCy/CyC(Carboplatin)E 3



35 3 SIOP TREATMENT GUIDELINES

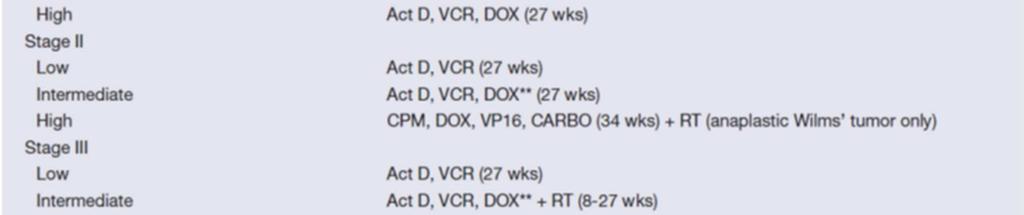

36 3 SIOP TREATMENT GUIDELINES

37 3 FLANK RT RT volto encompass the entire pre-op tumour bed Upper border-upper margin of tumour+1cm margin Lower border-lower margin of tumour+1cm margin Medial border-across the midline to include the entire width of the vertebral body & para-aortic LN chain Lateral border-abdominal wall

38 3 WHOLE ABDOMINAL IRRADIATION Upper border- dome of diaphragm Lower border-lower border of obturator foramen Lateral border-abdominal wall Femoral head & acetabulum to be shielded Hepatic dose <15 Gy Renal dose< Gy Appropriate shielding
39 CONFORMAL PLANNING GTV Pre-op tumour volume using co-registered MR-CT scans CTV GTV+1 cm isotropic expansion PTV CTV+SM+IM AP-PA beam arrangement with MLC shaping Aim Adequate target coverage with symmetrical irradiation of vertebrae, avoidance of contralateral kidney & minimisation of whole body dose IMRT rarely needed & conformal treatment adequate 3



40 4 CONFORMAL PLANNING


41 4 WHOLE LUNG IRRADIATION Upper border-to include both the lung apices Lower border-to include the pleural reflection infero-laterally Lat border-chest-wall Humerus& shoulder joint to be shielded bilaterally


42 4 CONFORMAL WLI oronal DRR AP-PA beam arrangement


43 4 WLI + FLANK RT



44 4
 -In Perez & Brady")

45 4 LONG TERM TREATMENT OUTCOME (NWTS 3 & 4) -In Perez & Brady s Principles & Practice of Radiation Oncology, 6 th edition, 20
46 4 TREATMENT OF RELAPSE Children with relapsed FH WT can have favorable outcome based on Initial stage Time from initial diagnosis Site of relapse Adverse factors for relapsed WT Prior use of Doxorubicin Relapse < 12 months from initial diagnosis Intra-abdominal relapse after previous abdominal RT Previous therapy
47 4 RESTAGING Stage 1R Localized disease, completely excised Stage 2R Gross total resection with evidence of regional spread Stage 3R Residual non-haematogenoustumor present and confined to abdomen Stage 4R Haematogenous mets present Stage 5R Bilateral renal involvement
48 4 RADIOTHERAPY GUIDELINES FOR RELAPSE RT is administered at site of relapse Dose to infradiaphragmatic sites CR after surgery (1R/2R) who have either received no previous RT or have received 10.8 Gy Birth 12 months Gy 13 months or older 21.6 Gy Gross residual disease after Sx Should get an additional boost (9Gy) Total dose including boost should not exceed 30.6 Gy Dose to infradiaphragmatic sites Total nominal dose (including previous RT) <36 months should not exceed 30.6 Gy >36 months should not exceed 39.6 Gy Total spine dose < 41.4 Gy Total liver dose <30.6 Gy Total remaining kidney dose < 19.8 Gy
49 4 RADIOTHERAPY GUIDELINES FOR RELAPSE Lung Irradiation Complete remission & no previous RT 18 months: 9 Gy; 1.5 Gy/fraction > 18 months: 12 Gy, 1.5 Gy/fraction Gross residual disease after surgical resection & no previous RT Can boost gross disease with additional 7.5 Gy Liver, Brain, Bone mets Follow guidelines from NWTS 5
50 5 CLEAR CELL SARCOMA OF KIDNEY (CCSK) Primitive mesenchymal neoplasm of kidney Constitutes 4% of childhood renal tumours Cell of origin unknown Propensity for bone mets(in NWTS 4 study incidence of bone mets23% in CCSK versus 0.3% in other tumours) In NWTS 1-4 study, 351 pts of CCSK included OS rate-69% On MVA, independent prognostic factors: Age Tumour stage Tumour necrosis Use of Doxorubicin -ArganiP et al. Am J SurgPathol2000;24:4-18.
51 5 RHABDOID TUMOUR OF KIDNEY (RTK) Highly malignant renal tumour Unrelated to WT or RMS Probably of neural crest origin Usually detected in first 2 yrsof life Associated with CNS lesion NWTS 1-5 study,142 pts of RTK included 4 yros-23% Prognostic factors: Age Tumour stage Higher dose of RT (>25 Gy) -Tomlinson et al. J Clin Oncol2005;23:
52 5 LATE EFFECTS OF TREATMENT Scoliosis-54% in patients treated with a median dose of 30Gy - Thomas et al. IJROBP 1983;9: CHF-4.4% at 20 years (NWTS1-4) - Green et al. JCO 2001;19: End stage renal disease (ESRD)-20 year cumulative incidence 74% in children with Denys-Drash syndrome 36% in children with WAGR syndrome 7% in children with GU abnormalities 0.6% in children without any syndrome/ abnormality - Breslow NE et al. J Urol 2005;174:
53 5 LATE EFFECTS OF TREATMENT Second malignant neoplasm (SMN)-15 year cumulative incidence 1.6% Leukaemia/ lymphoma incidence 0.4% at 8 years with no case thereafter Solid malignancy incidence continued to rise sharply with time 73% of the solid malignancies arose in previous RT field Associated factors: higher dose of RT, use of Doxorubicin & Rx of relapse - Breslow et al. JCO 1995;13: Adverse pregnancy outcome- Foetal malposition Premature labour LBW baby Congenital malformation - Green et al. JCO 2010;28:
54 5 FUTURE DIRECTION Deintensificationof Rx in LR pts & intensification of Rx in HR pts Refinement of tumour risk stratification using molecular signature IMRT- cardiac & renal sparing in whole lung & liver RT respectively Re-evaluation of the necessity of RT in all pts receiving pre-op chemo Re-evaluation of the current recommendation of WAI in localised preop tumour rupture limited to the flank Biochemotherapyin pts of RTK & WT with DA
55 5 CONCLUSION WT- highly curable childhood neoplasm The prognosis of children with WT has dramatically improved from a very high mortality rate at the beginning of the 20th century to the current cure rate of >90% The management of WT-paradigm for successful interdisciplinary treatment of solid tumours of childhood to maximize cure rates and minimize treatment-related complications
56 5
Goals and Objectives. Historical Background. Historical Background. Incidence. Epidemiology 7/1/2015 ROLE OF RADIOTHERAPY IN WILMS TUMOR
 Goals and Objectives ROLE OF RADIOTHERAPY IN WILMS TUMOR Arnold C. Paulino, M.D. Professor of Radiation Oncology MD Anderson Cancer Center To gain an understanding of presentation and work-up of Wilms
Goals and Objectives ROLE OF RADIOTHERAPY IN WILMS TUMOR Arnold C. Paulino, M.D. Professor of Radiation Oncology MD Anderson Cancer Center To gain an understanding of presentation and work-up of Wilms
Intrarenal Extension. sinus
 Intrarenal Extension into sinus Document Capsular Penetration sinus 16 Pediatric Renal Tumor Staging Stage I Limited to Kidney & Completely Resected Intact Renal Capsule No Previous Rupture or Biopsy Renal
Intrarenal Extension into sinus Document Capsular Penetration sinus 16 Pediatric Renal Tumor Staging Stage I Limited to Kidney & Completely Resected Intact Renal Capsule No Previous Rupture or Biopsy Renal
Wilms Tumor and Neuroblastoma
 Wilms Tumor and Neuroblastoma Wilm s Tumor AKA: Nephroblastoma the most common intra-abdominal cancer in children. peak incidence is 2 to 3 years of age Biology somatic mutations restricted to tumor tissue
Wilms Tumor and Neuroblastoma Wilm s Tumor AKA: Nephroblastoma the most common intra-abdominal cancer in children. peak incidence is 2 to 3 years of age Biology somatic mutations restricted to tumor tissue
SIOP PODC WILMS TUMOUR-1 Protocol
 SIOP PODC WILMS TUMOUR-1 Protocol A SIOP PODC Level 1 protocol and guideline for the treatment of Wilms Tumour in Children Adapted for Papua New Guinea A/Professor MICHAEL SULLIVAN FRACP PhD Head Solid
SIOP PODC WILMS TUMOUR-1 Protocol A SIOP PODC Level 1 protocol and guideline for the treatment of Wilms Tumour in Children Adapted for Papua New Guinea A/Professor MICHAEL SULLIVAN FRACP PhD Head Solid
All India Institute of Medical Sciences, New Delhi, INDIA. Department of Pediatric Surgery, Medical Oncology, and Radiology
 All India Institute of Medical Sciences, New Delhi, INDIA Department of Pediatric Surgery, Medical Oncology, and Radiology Clear cell sarcoma of the kidney- rare renal neoplasm second most common renal
All India Institute of Medical Sciences, New Delhi, INDIA Department of Pediatric Surgery, Medical Oncology, and Radiology Clear cell sarcoma of the kidney- rare renal neoplasm second most common renal
WILMS TUMOR. Click to edit Master subtitle style. Dr.S.G.RAMANAN M.D,D.M MCCF, CRRT
 WILMS TUMOR Click to edit Master subtitle style Dr.S.G.RAMANAN M.D,D.M MCCF, CRRT HISTORY German Surgeon Childhood renal tumors Burns. tuberculosis Radiation Co-author of Surgical text book Died taking
WILMS TUMOR Click to edit Master subtitle style Dr.S.G.RAMANAN M.D,D.M MCCF, CRRT HISTORY German Surgeon Childhood renal tumors Burns. tuberculosis Radiation Co-author of Surgical text book Died taking
Wilms Tumor Outcomes at a Single Institution and Review of Current Management Recommendations
 Wilms Tumor Outcomes at a Single Institution and Review of Current Management Recommendations Background: The Duval County Medical Society (DCMS) is proud to provide its members with free continuing medical
Wilms Tumor Outcomes at a Single Institution and Review of Current Management Recommendations Background: The Duval County Medical Society (DCMS) is proud to provide its members with free continuing medical
PDF created with pdffactory Pro trial version
 Neuroblastoma Tumor derived from neural crest cell that form the sympathetic ganglia&adrenal medulla. Causes *unknown. *familial neuroblastoma has been reported but is rare. * The incidence is 1:100,000
Neuroblastoma Tumor derived from neural crest cell that form the sympathetic ganglia&adrenal medulla. Causes *unknown. *familial neuroblastoma has been reported but is rare. * The incidence is 1:100,000
PITFALLS AND TRAPS IN THE DIAGNOSIS AND STAGING OF RENAL TUMOURS OF CHILDHOOD. Gordan M. Vujanić Cardiff, U.K.
 PITFALLS AND TRAPS IN THE DIAGNOSIS AND STAGING OF RENAL TUMOURS OF CHILDHOOD Gordan M. Vujanić Cardiff, U.K. RENAL TUMOURS OF CHILDHOOD - CLASSIFICATION (2016) Nephroblastic tumours Mesenchymal tumours
PITFALLS AND TRAPS IN THE DIAGNOSIS AND STAGING OF RENAL TUMOURS OF CHILDHOOD Gordan M. Vujanić Cardiff, U.K. RENAL TUMOURS OF CHILDHOOD - CLASSIFICATION (2016) Nephroblastic tumours Mesenchymal tumours
doi: /j.ijrobp
 doi:10.1016/j.ijrobp.2009.01.046 Int. J. Radiation Oncology Biol. Phys., Vol. 76, No. 1, pp. 201 206, 2010 Copyright Ó 2010 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/10/$ see front
doi:10.1016/j.ijrobp.2009.01.046 Int. J. Radiation Oncology Biol. Phys., Vol. 76, No. 1, pp. 201 206, 2010 Copyright Ó 2010 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/10/$ see front
Case 1. Clinical history
 Case 1 Case 1 Clinical history 17-month-old boy with a kidney tumor found during routine childhood care program. CT scan showed a solid mass. Chemotherapy was given for 4 weeks using actinomycin D and
Case 1 Case 1 Clinical history 17-month-old boy with a kidney tumor found during routine childhood care program. CT scan showed a solid mass. Chemotherapy was given for 4 weeks using actinomycin D and
Effective local and systemic therapy is necessary for the cure of Ewing tumor Most chemotherapy regimens are a combination of cyclophosphamide,
 Ewing Tumor Perez Ewing tumor is the second most common primary tumor of bone in childhood, and also occurs in soft tissues Ewing tumor is uncommon before 8 years of age and after 25 years of age In the
Ewing Tumor Perez Ewing tumor is the second most common primary tumor of bone in childhood, and also occurs in soft tissues Ewing tumor is uncommon before 8 years of age and after 25 years of age In the
Dr Marty Campbell Paediatric Oncologist Royal Children's Hospital, Melbourne. FRACP lecture series Oct 2014
 Dr Marty Campbell Paediatric Oncologist Royal Children's Hospital, Melbourne FRACP lecture series Oct 2014 Background Neuroblastoma (NB) is the most common solid tumour outside the CNS in children 6-10%
Dr Marty Campbell Paediatric Oncologist Royal Children's Hospital, Melbourne FRACP lecture series Oct 2014 Background Neuroblastoma (NB) is the most common solid tumour outside the CNS in children 6-10%
Pediatric Retroperitoneal Masses Radiologic-Pathologic Correlation
 Acta Radiológica Portuguesa, Vol.XVIII, nº 70, pág. 61-70, Abr.-Jun., 2006 Pediatric Retroperitoneal Masses Radiologic-Pathologic Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
Acta Radiológica Portuguesa, Vol.XVIII, nº 70, pág. 61-70, Abr.-Jun., 2006 Pediatric Retroperitoneal Masses Radiologic-Pathologic Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
Tumors of kidney and urinary bladder
 Tumors of kidney and urinary bladder Overview of kidney tumors Benign and malignant Of the benign: papillary adenoma -cortical -small (0.5cm) -in 40% of population -clinically insignificant The most common
Tumors of kidney and urinary bladder Overview of kidney tumors Benign and malignant Of the benign: papillary adenoma -cortical -small (0.5cm) -in 40% of population -clinically insignificant The most common
1 Department of Epidemiology and Cancer Control, St. Jude Children s. 4 Midwest Children s Cancer Center at Children s Hospital of
 Pediatr Blood Cancer 2014;61:134 139 Outcome of Patients With Stage II/Favorable Histology Wilms Tumor With and Without Local Tumor Spill: A Report From the National Wilms Tumor Study Group Daniel M. Green,
Pediatr Blood Cancer 2014;61:134 139 Outcome of Patients With Stage II/Favorable Histology Wilms Tumor With and Without Local Tumor Spill: A Report From the National Wilms Tumor Study Group Daniel M. Green,
MR Tumor Staging for Treatment Decision in Case of Wilms Tumor
 MR Tumor Staging for Treatment Decision in Case of Wilms Tumor G. Schneider, M.D., Ph.D.; P. Fries, M.D. Dept. of Diagnostic and Interventional Radiology, Saarland University Hospital, Homburg/Saar, Germany
MR Tumor Staging for Treatment Decision in Case of Wilms Tumor G. Schneider, M.D., Ph.D.; P. Fries, M.D. Dept. of Diagnostic and Interventional Radiology, Saarland University Hospital, Homburg/Saar, Germany
Wilms Tumour A brief note for the parents
 Wilms Tumour A brief note for the parents By Dr. Abid Qazi!1 PARENT S GUIDE FACTSHEET Cancer is not an incurable disease any more in many circumstances. The key for cure is early diagnosis. However, it
Wilms Tumour A brief note for the parents By Dr. Abid Qazi!1 PARENT S GUIDE FACTSHEET Cancer is not an incurable disease any more in many circumstances. The key for cure is early diagnosis. However, it
Radiation and Hodgkin s Disease: A Changing Field. Sravana Chennupati Radiation Oncology PGY-2
 Radiation and Hodgkin s Disease: A Changing Field Sravana Chennupati Radiation Oncology PGY-2 History of Present Illness 19 yo previously healthy male college student began having pain in his R shoulder
Radiation and Hodgkin s Disease: A Changing Field Sravana Chennupati Radiation Oncology PGY-2 History of Present Illness 19 yo previously healthy male college student began having pain in his R shoulder
Dr.Dafalla Ahmed Babiker Jazan University
 Dr.Dafalla Ahmed Babiker Jazan University Brain tumors are the second commonest malignancy in children Infratentorial tumors are more common As a general rule they do not metastasize out of the CNS, but
Dr.Dafalla Ahmed Babiker Jazan University Brain tumors are the second commonest malignancy in children Infratentorial tumors are more common As a general rule they do not metastasize out of the CNS, but
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM MENINGIOMA CNS Site Group Meningioma Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION 3 2. PREVENTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM MENINGIOMA CNS Site Group Meningioma Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION 3 2. PREVENTION
PEDIATRIC ORBITAL TUMORS RADIOTHERAPY PLANNING
 PEDIATRIC ORBITAL TUMORS RADIOTHERAPY PLANNING ANATOMY ANATOMY CONT ANATOMY CONT. ANATOMY CONT. EYE OF A CHILD Normal tissue tolerance doses (in conventional #) TD 5/5 TD 50/5 Endpoint Gy Gy Optic nerve
PEDIATRIC ORBITAL TUMORS RADIOTHERAPY PLANNING ANATOMY ANATOMY CONT ANATOMY CONT. ANATOMY CONT. EYE OF A CHILD Normal tissue tolerance doses (in conventional #) TD 5/5 TD 50/5 Endpoint Gy Gy Optic nerve
Corporate Medical Policy
 Corporate Medical Policy Hematopoietic Stem-Cell Transplantation for Solid Tumors of File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_stem-cell_transplantation_for_solid_tumors_childhood
Corporate Medical Policy Hematopoietic Stem-Cell Transplantation for Solid Tumors of File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_stem-cell_transplantation_for_solid_tumors_childhood
UPDATE ON WILMS TUMOR IN CHILDREN
 UROLOGY FOR THE PRACTITIONER UPDATE ON WILMS TUMOR IN CHILDREN Anthony COOK, Walid FARHAT, Antoine KHOURY Cook A, Farhat W, Khoury A. Update on Wilms tumor in children. Leb Med J 2005 ; 53 (2) : 85-90.
UROLOGY FOR THE PRACTITIONER UPDATE ON WILMS TUMOR IN CHILDREN Anthony COOK, Walid FARHAT, Antoine KHOURY Cook A, Farhat W, Khoury A. Update on Wilms tumor in children. Leb Med J 2005 ; 53 (2) : 85-90.
A 20-Year Prospective Study of Wilms Tumor and Other Kidney Tumors: A Report From Hong Kong Pediatric Hematology and Oncology Study Group
 ORIGINAL ARTICLE A 20-Year Prospective Study of Wilms Tumor and Other Kidney Tumors: A Report From Hong Kong Pediatric Hematology and Oncology Study Group Ching Ching Chan, MRCP,* Ka Fai To, FHKAM,w Hui
ORIGINAL ARTICLE A 20-Year Prospective Study of Wilms Tumor and Other Kidney Tumors: A Report From Hong Kong Pediatric Hematology and Oncology Study Group Ching Ching Chan, MRCP,* Ka Fai To, FHKAM,w Hui
Surgery for Wilms Tumour in Children in a Tertiary Centre in Hong Kong: A 15-year Retrospective Review
 HK J Paediatr (new series) 2012;17:103-108 Surgery for Wilms Tumour in Children in a Tertiary Centre in Hong Kong: A 15-year Retrospective Review KW CHAN, KH LEE, JW MOU, YH TAM Abstract Key words Objective:
HK J Paediatr (new series) 2012;17:103-108 Surgery for Wilms Tumour in Children in a Tertiary Centre in Hong Kong: A 15-year Retrospective Review KW CHAN, KH LEE, JW MOU, YH TAM Abstract Key words Objective:
State of the Art Radiotherapy for Pediatric Tumors. Suzanne L. Wolden, MD Memorial Sloan-Kettering Cancer Center
 State of the Art Radiotherapy for Pediatric Tumors Suzanne L. Wolden, MD Memorial Sloan-Kettering Cancer Center Introduction Progress and success in pediatric oncology Examples of low-tech and high-tech
State of the Art Radiotherapy for Pediatric Tumors Suzanne L. Wolden, MD Memorial Sloan-Kettering Cancer Center Introduction Progress and success in pediatric oncology Examples of low-tech and high-tech
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
SOLID TUMOURS IN CHILDHOOD
 SOLID TUMOURS IN CHILDHOOD Fareed Omar Paediatric Oncology Steve Biko Academic hospital Introduction 1 Introduction Lymphomas and Leukemias make up about 40% of all childhood Cancers (Systemic cancers)
SOLID TUMOURS IN CHILDHOOD Fareed Omar Paediatric Oncology Steve Biko Academic hospital Introduction 1 Introduction Lymphomas and Leukemias make up about 40% of all childhood Cancers (Systemic cancers)
Late recurrence in children with Wilms tumor
 The Turkish Journal of Pediatrics 2007; 49: 226-230 Case Late recurrence in children with Wilms tumor Münevver Büyükpamukçu 1, Yavuz Köksal 1, Ali Varan 1, Lale Atahan 2, Melda Çağlar 3 Canan Akyüz 1,
The Turkish Journal of Pediatrics 2007; 49: 226-230 Case Late recurrence in children with Wilms tumor Münevver Büyükpamukçu 1, Yavuz Köksal 1, Ali Varan 1, Lale Atahan 2, Melda Çağlar 3 Canan Akyüz 1,
Leukaemia 35% Lymphoma 14%
 Distribution ib ti of Cancers in Children under 15 years Leukaemia 35% Lymphoma 14% Neuroblastoma 9% Other 5% Liver 1% Retinoblastoma 3% Bone and STS 15% CNS 20% Wilms' 8% 30-40% Mortality Germ Cell Tumours
Distribution ib ti of Cancers in Children under 15 years Leukaemia 35% Lymphoma 14% Neuroblastoma 9% Other 5% Liver 1% Retinoblastoma 3% Bone and STS 15% CNS 20% Wilms' 8% 30-40% Mortality Germ Cell Tumours
Università di Roma La Sapienza
 Università di Roma La Sapienza U.O.C. Chirurgia Pediatrica - Policlinico Umberto I Direttore: Prof Francesco Cozzi Chirurgia nephron-sparing per tumori renali primitivi in età pediatrica. Prof. Denis A.
Università di Roma La Sapienza U.O.C. Chirurgia Pediatrica - Policlinico Umberto I Direttore: Prof Francesco Cozzi Chirurgia nephron-sparing per tumori renali primitivi in età pediatrica. Prof. Denis A.
Radiotherapy in DLCL is often worthwhile. Dr. Joachim Yahalom Memorial Sloan-Kettering, New York
 Radiotherapy in DLCL is often worthwhile Dr. Joachim Yahalom Memorial Sloan-Kettering, New York The case for radiotherapy Past: Pre-Rituximab randomized trials Present: R-CHOP as backbone, retrospective
Radiotherapy in DLCL is often worthwhile Dr. Joachim Yahalom Memorial Sloan-Kettering, New York The case for radiotherapy Past: Pre-Rituximab randomized trials Present: R-CHOP as backbone, retrospective
THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA. TIMUR MITIN, MD, PhD
 THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA TIMUR MITIN, MD, PhD RESECTABLE DISEASE MANAGEMENT: RESECTABLE DISEASE Resection offers the only possibility of long term survival
THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA TIMUR MITIN, MD, PhD RESECTABLE DISEASE MANAGEMENT: RESECTABLE DISEASE Resection offers the only possibility of long term survival
Radiation Oncology MOC Study Guide
 Radiation Oncology MOC Study Guide The following study guide is intended to give a general overview of the type of material that will be covered on the Radiation Oncology Maintenance of Certification (MOC)
Radiation Oncology MOC Study Guide The following study guide is intended to give a general overview of the type of material that will be covered on the Radiation Oncology Maintenance of Certification (MOC)
Wilms' tumor most often occurs in just one kidney, though it can sometimes be found in both kidneys at the same time.
 Wilms' Tumor Wilms' tumor is a rare kidney cancer that primarily affects children. Also known as nephroblastoma, Wilms' tumor is the most common cancer of the kidneys in children. Wilms' tumor most often
Wilms' Tumor Wilms' tumor is a rare kidney cancer that primarily affects children. Also known as nephroblastoma, Wilms' tumor is the most common cancer of the kidneys in children. Wilms' tumor most often
Clinical Trials and Epidemiology
 Clinical Trials and Epidemiology Reflections of the Statistician for the National Wilms Tumor Study Professor Norman Breslow Department of Biostatistics University of Washington, Seattle Fields Institute,
Clinical Trials and Epidemiology Reflections of the Statistician for the National Wilms Tumor Study Professor Norman Breslow Department of Biostatistics University of Washington, Seattle Fields Institute,
Etiopathological and management profile of Wilms tumour A single centre experience
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 10 Ver. 10 (October. 2018), PP 48-53 www.iosrjournals.org Etiopathological and management profile
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 10 Ver. 10 (October. 2018), PP 48-53 www.iosrjournals.org Etiopathological and management profile
The role of chemoradiotherapy in GE junction and gastric cancer. Karin Haustermans
 The role of chemoradiotherapy in GE junction and gastric cancer Karin Haustermans Overview Postoperative chemoradiotherapy Preoperative chemoradiotherapy Palliative radiation Technical aspects Overview
The role of chemoradiotherapy in GE junction and gastric cancer Karin Haustermans Overview Postoperative chemoradiotherapy Preoperative chemoradiotherapy Palliative radiation Technical aspects Overview
2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow, Necrotic Mass with a Pseudocapsule
 GENITOURINARY PATHOLOGY Kathleen M. O Toole, M.D. Renal Cell Carcinoma 2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow Necrotic Mass Grossly is a Bright
GENITOURINARY PATHOLOGY Kathleen M. O Toole, M.D. Renal Cell Carcinoma 2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow Necrotic Mass Grossly is a Bright
Opportunity for palliative care Research
 Opportunity for palliative care Research Role of Radiotherapy in Multidisciplinary Management of Rectal Cancers Dr Sushmita Pathy Associate Professor Department of Radiation Oncology Dr BRA Institute Rotary
Opportunity for palliative care Research Role of Radiotherapy in Multidisciplinary Management of Rectal Cancers Dr Sushmita Pathy Associate Professor Department of Radiation Oncology Dr BRA Institute Rotary
The management of bilateral Wilms tumor
 Wilms Tumor The management of bilateral Wilms tumor Derya Özyörük 1, Suna Emir 2 1 Pediatric Oncologist, Department of Pediatric Hematology Oncology, 2 Associate Professor of Pediatrics, Department of
Wilms Tumor The management of bilateral Wilms tumor Derya Özyörük 1, Suna Emir 2 1 Pediatric Oncologist, Department of Pediatric Hematology Oncology, 2 Associate Professor of Pediatrics, Department of
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
JAMES EWING, Endothelial origin. 14 yr Girl
 JAMES EWING, 1921 Endothelial origin 14 yr Girl SPECTRUM OF ESFT NEURAL DIFFERENTIATION Least Well EWING S SARCOMA ATYPICAL EWING S SARCOMA PNET Peripheral Neuroepithelioma ASKIN TUMOR (thoraco-pulmonary)
JAMES EWING, 1921 Endothelial origin 14 yr Girl SPECTRUM OF ESFT NEURAL DIFFERENTIATION Least Well EWING S SARCOMA ATYPICAL EWING S SARCOMA PNET Peripheral Neuroepithelioma ASKIN TUMOR (thoraco-pulmonary)
Multidisciplinary Approach to Wilms Tumor: A Retrospective Analytical Study of 53 Patients
 Journal of the Egyptian Nat. Cancer Inst., Vol. 20, No. 4, December: 410-423, 2008 Multidisciplinary Approach to Wilms Tumor: A Retrospective Analytical Study of 53 Patients SHERIF F. NAGUIB, M.D.*; ALAA
Journal of the Egyptian Nat. Cancer Inst., Vol. 20, No. 4, December: 410-423, 2008 Multidisciplinary Approach to Wilms Tumor: A Retrospective Analytical Study of 53 Patients SHERIF F. NAGUIB, M.D.*; ALAA
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM LOW GRADE GLIOMAS CNS Site Group Low Grade Gliomas Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM LOW GRADE GLIOMAS CNS Site Group Low Grade Gliomas Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING
Insights into Thymic Epithelial Tumors: Radiation Therapy
 Insights into Thymic Epithelial Tumors: Radiation Therapy Charles R. Thomas, MD Professor and Chairman, Department of Radiation Medicine Professor, Department of Medicine, Division of Hematology/Medical
Insights into Thymic Epithelial Tumors: Radiation Therapy Charles R. Thomas, MD Professor and Chairman, Department of Radiation Medicine Professor, Department of Medicine, Division of Hematology/Medical
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Protocol applies to specimens from patients with Wilms tumor (nephroblastoma) or other renal tumors of childhood.
 or other renal tumors of childhood.") Wilms Tumor Protocol applies to specimens from patients with Wilms tumor (nephroblastoma) or other renal tumors of childhood. Procedures Cytology (No Accompanying Checklist) Incisional Biopsy (Needle or
Wilms Tumor Protocol applies to specimens from patients with Wilms tumor (nephroblastoma) or other renal tumors of childhood. Procedures Cytology (No Accompanying Checklist) Incisional Biopsy (Needle or
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM MEDULLOBLASTOMA AND PNET CNS Site Group Medulloblastoma and PNET Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM MEDULLOBLASTOMA AND PNET CNS Site Group Medulloblastoma and PNET Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION
Update on Limited Small Cell Lung Cancer. Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver
 Update on Limited Small Cell Lung Cancer Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver Objectives - Limited Radiation Dose Radiation Timing Radiation Volume PCI Neurotoxicity
Update on Limited Small Cell Lung Cancer Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver Objectives - Limited Radiation Dose Radiation Timing Radiation Volume PCI Neurotoxicity
Hodgkin Lymphoma: Umberto Ricardi
 Hodgkin Lymphoma: Radiation Volumes Umberto Ricardi Università di Torino The changing role of RT in the cure of HL From Maximal use as a single agent To Combination of chemotherapy and full dose-full volume
Hodgkin Lymphoma: Radiation Volumes Umberto Ricardi Università di Torino The changing role of RT in the cure of HL From Maximal use as a single agent To Combination of chemotherapy and full dose-full volume
RCC in Adolescents and Young Adults (AYAs): Diagnosis and Management
: Diagnosis and Management") RCC in Adolescents and Young Adults (AYAs): Diagnosis and Management Nicholas G. Cost, M.D. Assistant Professor, Department of Surgery, Division of Urology University of Colorado Cancer Center Fifteenth
RCC in Adolescents and Young Adults (AYAs): Diagnosis and Management Nicholas G. Cost, M.D. Assistant Professor, Department of Surgery, Division of Urology University of Colorado Cancer Center Fifteenth
IAEA Pediatric Radiation Oncology Training Dr Laskar Version 1 June SOFT TISSUE SARCOMA (Non Rhabdomyosarcoma)
") SOFT TISSUE SARCOMA (Non Rhabdomyosarcoma) Soft Tissue structures Fat, Muscles, Fibrous tissue, Blood vessels, Supporting cells of peripheral nervous system Soft Tissue Sarcomas:- embryologically arise
SOFT TISSUE SARCOMA (Non Rhabdomyosarcoma) Soft Tissue structures Fat, Muscles, Fibrous tissue, Blood vessels, Supporting cells of peripheral nervous system Soft Tissue Sarcomas:- embryologically arise
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Approach to Abdominal Mass Part 2. These podcasts are designed to give medical students an overview of key topics in
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Approach to Abdominal Mass Part 2. These podcasts are designed to give medical students an overview of key topics in
Dr Sneha Shah Tata Memorial Hospital, Mumbai.
 Dr Sneha Shah Tata Memorial Hospital, Mumbai. Topics covered Lymphomas including Burkitts Pediatric solid tumors (non CNS) Musculoskeletal Ewings & osteosarcoma. Neuroblastomas Nasopharyngeal carcinomas
Dr Sneha Shah Tata Memorial Hospital, Mumbai. Topics covered Lymphomas including Burkitts Pediatric solid tumors (non CNS) Musculoskeletal Ewings & osteosarcoma. Neuroblastomas Nasopharyngeal carcinomas
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016. Background
 Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Pediatric Oncology. Vlad Radulescu, MD
 Pediatric Oncology Vlad Radulescu, MD Objectives Review the epidemiology of childhood cancer Discuss the presenting signs and symptoms, general treatment principles and overall prognosis of the most common
Pediatric Oncology Vlad Radulescu, MD Objectives Review the epidemiology of childhood cancer Discuss the presenting signs and symptoms, general treatment principles and overall prognosis of the most common
INTRAOPERATIVE RADIATION THERAPY FOR RETROPERITONEAL SARCOMA
 INTRAOPERATIVE RADIATION THERAPY FOR RETROPERITONEAL SARCOMA ISIORT 2014 Ivy A Petersen, MD Mayo Clinic Rochester, MN NOTHING TO DISCLOSE SOFT TISSUE SARCOMAS 2014 Estimated cases in the USA 12,020 diagnosed
INTRAOPERATIVE RADIATION THERAPY FOR RETROPERITONEAL SARCOMA ISIORT 2014 Ivy A Petersen, MD Mayo Clinic Rochester, MN NOTHING TO DISCLOSE SOFT TISSUE SARCOMAS 2014 Estimated cases in the USA 12,020 diagnosed
Renal tumors are among the most common
 Renal tumor in developing countries: 142 cases from a single institution at Shanghai, China Ci Pan, Jiao-Yang Cai, Min Xu, Qi-Dong Ye, Min Zhou, Min-Zhi Yin, Yu-Min Zhong, Jing Chen, Shu-Hong Shen, Jing-Yan
Renal tumor in developing countries: 142 cases from a single institution at Shanghai, China Ci Pan, Jiao-Yang Cai, Min Xu, Qi-Dong Ye, Min Zhou, Min-Zhi Yin, Yu-Min Zhong, Jing Chen, Shu-Hong Shen, Jing-Yan
When to Integrate Surgery for Metatstatic Urothelial Cancers
 When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
Tecniche Radioterapiche U. Ricardi
 Tecniche Radioterapiche U. Ricardi UNIVERSITA DEGLI STUDI DI TORINO Should we always rely on stage? T4N0M0 Stage IIIB T2N3M0 Early stage NSCLC The treatment of choice for early-stage NSCLC is anatomic
Tecniche Radioterapiche U. Ricardi UNIVERSITA DEGLI STUDI DI TORINO Should we always rely on stage? T4N0M0 Stage IIIB T2N3M0 Early stage NSCLC The treatment of choice for early-stage NSCLC is anatomic
Wilms' tumour and renal dysplasia: an hypothesis
 J Clin Pathol 1982;35:1069-1073 Wilms' tumour and renal dysplasia: an hypothesis HB MARSDEN, W LAWLER* From the Royal Manchester Children's Hospital, Manchester M27 I HA and the *Department of Pathology,
J Clin Pathol 1982;35:1069-1073 Wilms' tumour and renal dysplasia: an hypothesis HB MARSDEN, W LAWLER* From the Royal Manchester Children's Hospital, Manchester M27 I HA and the *Department of Pathology,
Nephroblastoma: Does The Decrease In Tumour Volume Under Preoperative Chemotherapy Predict The Lymph Nodes Status At Surgery?
 Nephroblastoma: Does The Decrease In Tumour Volume Under Preoperative Chemotherapy Predict The Lymph Nodes Status At Surgery? Jan Godzinski,, Harm van Tinteren,, Jan de Kraker,, Norbert Graf, Christophe
Nephroblastoma: Does The Decrease In Tumour Volume Under Preoperative Chemotherapy Predict The Lymph Nodes Status At Surgery? Jan Godzinski,, Harm van Tinteren,, Jan de Kraker,, Norbert Graf, Christophe
Refresher Course EAR TUMOR. Sasikarn Chamchod, MD Chulabhorn Hospital
 Refresher Course EAR TUMOR Sasikarn Chamchod, MD Chulabhorn Hospital Reference: Perez and Brady s Principles and Practice of radiation oncology sixth edition Outlines Anatomy Epidemiology Clinical presentations
Refresher Course EAR TUMOR Sasikarn Chamchod, MD Chulabhorn Hospital Reference: Perez and Brady s Principles and Practice of radiation oncology sixth edition Outlines Anatomy Epidemiology Clinical presentations
Journal of Pediatric Sciences
 Journal of Pediatric Sciences Role of post-operative radiation therapy in single brain metastasis from clear cell sarcoma in children: a case report with systemic review Fadoua Rais, Naoual Benhmidou,
Journal of Pediatric Sciences Role of post-operative radiation therapy in single brain metastasis from clear cell sarcoma in children: a case report with systemic review Fadoua Rais, Naoual Benhmidou,
Ruolo dell imaging nella pianificazione del trattamento
 Simposio AIRO-SIRM: Diagnostica per immagini morfologica e funzionale nella stadiazione, terapia e follow-up dei sarcomi delle parti molli Ruolo dell imaging nella pianificazione del trattamento Marco
Simposio AIRO-SIRM: Diagnostica per immagini morfologica e funzionale nella stadiazione, terapia e follow-up dei sarcomi delle parti molli Ruolo dell imaging nella pianificazione del trattamento Marco
Pre- Versus Post-operative Radiotherapy
 Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
RENAL CELL CARCINOMA 2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow, Necrotic Mass with a Pseud
 GENITOURINARY PATHOLOGY Kathleen M. O Toole Toole, M.D. RENAL CELL CARCINOMA 2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow, Necrotic Mass with a
GENITOURINARY PATHOLOGY Kathleen M. O Toole Toole, M.D. RENAL CELL CARCINOMA 2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow, Necrotic Mass with a
GUIDELINES ON RENAL CELL CANCER
 20 G. Mickisch (chairman), J. Carballido, S. Hellsten, H. Schulze, H. Mensink Eur Urol 2001;40(3):252-255 Introduction is characterised by a constant rise in incidence over the last 50 years, with a predominance
20 G. Mickisch (chairman), J. Carballido, S. Hellsten, H. Schulze, H. Mensink Eur Urol 2001;40(3):252-255 Introduction is characterised by a constant rise in incidence over the last 50 years, with a predominance
Update on Sarcomas of the Head and Neck. Kevin Harrington
 Update on Sarcomas of the Head and Neck Kevin Harrington Overview Classification and incidence of sarcomas Clinical presentation Challenges to treatment Management approaches Prognostic factors Radiation-induced
Update on Sarcomas of the Head and Neck Kevin Harrington Overview Classification and incidence of sarcomas Clinical presentation Challenges to treatment Management approaches Prognostic factors Radiation-induced
the urinary system pathology Dr. Fairoz A Eltorgman
 the urinary system pathology Dr. Fairoz A Eltorgman Tumors of the renal pelvis & kidney Benign tumors of the renal pelvis: Hemangioma Leiomyoma Malignant tumors: Transitional cell carcinoma Squamous cell
the urinary system pathology Dr. Fairoz A Eltorgman Tumors of the renal pelvis & kidney Benign tumors of the renal pelvis: Hemangioma Leiomyoma Malignant tumors: Transitional cell carcinoma Squamous cell
Clinical Trials of Proton Therapy for Breast Cancer. Andrew L. Chang, MD 張維安 Study Chair
 Clinical Trials of Proton Therapy for Breast Cancer Andrew L. Chang, MD 張維安 Study Chair AndrewLChangMD@gmail.com Disclosure Proton Center Development Corporation Scripps San Diego Proton Therapy Center
Clinical Trials of Proton Therapy for Breast Cancer Andrew L. Chang, MD 張維安 Study Chair AndrewLChangMD@gmail.com Disclosure Proton Center Development Corporation Scripps San Diego Proton Therapy Center
Optimal Management of Isolated HER2+ve Brain Metastases
 Optimal Management of Isolated HER2+ve Brain Metastases Eliot Sims November 2013 Background Her2+ve patients 15% of all breast cancer Even with adjuvant trastuzumab 10-15% relapse Trastuzumab does not
Optimal Management of Isolated HER2+ve Brain Metastases Eliot Sims November 2013 Background Her2+ve patients 15% of all breast cancer Even with adjuvant trastuzumab 10-15% relapse Trastuzumab does not
A Dosimetric Comparison of Whole-Lung Treatment Techniques. in the Pediatric Population
 A Dosimetric Comparison of Whole-Lung Treatment Techniques in the Pediatric Population Corresponding Author: Christina L. Bosarge, B.S., R.T. (R) (T) Indiana University School of Medicine Department of
A Dosimetric Comparison of Whole-Lung Treatment Techniques in the Pediatric Population Corresponding Author: Christina L. Bosarge, B.S., R.T. (R) (T) Indiana University School of Medicine Department of
PORTEC-4. Patient seqnr. Age at inclusion (years) Hospital:
 Hospital:") May 2016 Randomisation Checklist Form 1, page 1 of 2 Patient seqnr. Age at inclusion (years) Hospital: Eligible patients should be registered and randomised via the Internet at : https://prod.tenalea.net/fs4/dm/delogin.aspx?refererpath=dehome.aspx
May 2016 Randomisation Checklist Form 1, page 1 of 2 Patient seqnr. Age at inclusion (years) Hospital: Eligible patients should be registered and randomised via the Internet at : https://prod.tenalea.net/fs4/dm/delogin.aspx?refererpath=dehome.aspx
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
2007 ANNUAL SITE STUDY HODGKIN S LYMPHOMA
 2007 ANNUAL SITE STUDY HODGKIN S LYMPHOMA SUSQUEHANNA HEALTH David B. Nagel, M.D. April 11, 2008 Hodgkin s lymphoma was first described by Thomas Hodgkin in 1832. It remained an incurable malignancy until
2007 ANNUAL SITE STUDY HODGKIN S LYMPHOMA SUSQUEHANNA HEALTH David B. Nagel, M.D. April 11, 2008 Hodgkin s lymphoma was first described by Thomas Hodgkin in 1832. It remained an incurable malignancy until
Pancreatic Cancer and Radiation Therapy
 Pancreatic Cancer and Radiation Therapy Why? Is there a role for local therapy with radiation in a disease with such a high rate of distant metastases? When? Resectable Disease Is there a role for post-op
Pancreatic Cancer and Radiation Therapy Why? Is there a role for local therapy with radiation in a disease with such a high rate of distant metastases? When? Resectable Disease Is there a role for post-op
REVISITING ICRU VOLUME DEFINITIONS. Eduardo Rosenblatt Vienna, Austria
 REVISITING ICRU VOLUME DEFINITIONS Eduardo Rosenblatt Vienna, Austria Objective: To introduce target volumes and organ at risk concepts as defined by ICRU. 3D-CRT is the standard There was a need for a
REVISITING ICRU VOLUME DEFINITIONS Eduardo Rosenblatt Vienna, Austria Objective: To introduce target volumes and organ at risk concepts as defined by ICRU. 3D-CRT is the standard There was a need for a
Renal Parenchymal Neoplasms
 Renal Parenchymal Neoplasms د. BENIGN TUMORS : Benign renal tumors include adenoma, oncocytoma, angiomyolipoma, leiomyoma, lipoma, hemangioma, and juxtaglomerular tumors. Renal Adenomas : The adenoma is
Renal Parenchymal Neoplasms د. BENIGN TUMORS : Benign renal tumors include adenoma, oncocytoma, angiomyolipoma, leiomyoma, lipoma, hemangioma, and juxtaglomerular tumors. Renal Adenomas : The adenoma is
T of Wilms' tumor during the past 10
 WILMS' TUMOR-AN INTERDISCIPLINARY TREATMENT PROGRAM WITH AND WITHOUT DACTI N 0 MYCIN LAWRENCE W. MARGOLIS, MD,* W. BYRON SMITH, MD,+ WILLIAM M. WARA, MD,~ JOSEPH H. KUSHNER, MD,~ AND ALFRED A. DELORIMIER,
WILMS' TUMOR-AN INTERDISCIPLINARY TREATMENT PROGRAM WITH AND WITHOUT DACTI N 0 MYCIN LAWRENCE W. MARGOLIS, MD,* W. BYRON SMITH, MD,+ WILLIAM M. WARA, MD,~ JOSEPH H. KUSHNER, MD,~ AND ALFRED A. DELORIMIER,
Case 2. Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset
 Case 2 Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset History 24 year old male presented with a 3 day history of right flank pain, sharp in nature Denies fever, chills, hematuria or
Case 2 Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset History 24 year old male presented with a 3 day history of right flank pain, sharp in nature Denies fever, chills, hematuria or
PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma
 with classical Hodgkin lymphoma") PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma Ryan Lynch MD Assistant Professor, University of Washington Assistant Member, Fred Hutchinson Cancer
PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma Ryan Lynch MD Assistant Professor, University of Washington Assistant Member, Fred Hutchinson Cancer
RARE TUMORS OF INFANCY. RAJKUMAR VENKATRAMANI, MD, MS Director, Rare Tumors Program, Texas Children s Hospital
 RARE TUMORS OF INFANCY RAJKUMAR VENKATRAMANI, MD, MS Director, Rare Tumors Program, Texas Children s Hospital OBJECTIVES Review the epidemiology and clinical presentation of soft tissue sarcomas in infancy.
RARE TUMORS OF INFANCY RAJKUMAR VENKATRAMANI, MD, MS Director, Rare Tumors Program, Texas Children s Hospital OBJECTIVES Review the epidemiology and clinical presentation of soft tissue sarcomas in infancy.
Pediatric electron intraoperative radiotherapy: results and innovations
 Pediatric electron intraoperative radiotherapy: results and innovations Felipe A. Calvo ESTRO Hospital General Universitario Gregorio Marañon Madrid, Spain 2017 IOeRT in pediatric cancer: results and innovations
Pediatric electron intraoperative radiotherapy: results and innovations Felipe A. Calvo ESTRO Hospital General Universitario Gregorio Marañon Madrid, Spain 2017 IOeRT in pediatric cancer: results and innovations
San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy
 San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy Kathleen C. Horst, M.D. Assistant Professor Department of Radiation Oncology Stanford University The Optimal SEquencing of Adjuvant Chemotherapy
San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy Kathleen C. Horst, M.D. Assistant Professor Department of Radiation Oncology Stanford University The Optimal SEquencing of Adjuvant Chemotherapy
The Physics of Oesophageal Cancer Radiotherapy
 The Physics of Oesophageal Cancer Radiotherapy Dr. Philip Wai Radiotherapy Physics Royal Marsden Hospital 1 Contents Brief clinical introduction Imaging and Target definition Dose prescription & patient
The Physics of Oesophageal Cancer Radiotherapy Dr. Philip Wai Radiotherapy Physics Royal Marsden Hospital 1 Contents Brief clinical introduction Imaging and Target definition Dose prescription & patient
Radiation Therapy for Soft Tissue Sarcomas
 Radiation Therapy for Soft Tissue Sarcomas Alexander R. Gottschalk, MD, PhD Assistant Professor, Radiation Oncology University of California, San Francisco 1/25/08 NCI: limb salvage vs. amputation 43 patients
Radiation Therapy for Soft Tissue Sarcomas Alexander R. Gottschalk, MD, PhD Assistant Professor, Radiation Oncology University of California, San Francisco 1/25/08 NCI: limb salvage vs. amputation 43 patients
Adjuvant Therapies in Endometrial Cancer. Emma Hudson
 Adjuvant Therapies in Endometrial Cancer Emma Hudson Endometrial Cancer Most common gynaecological cancer Incidence increasing in Western world 1-2% cancer deaths 75% patients postmenopausal 97% epithelial
Adjuvant Therapies in Endometrial Cancer Emma Hudson Endometrial Cancer Most common gynaecological cancer Incidence increasing in Western world 1-2% cancer deaths 75% patients postmenopausal 97% epithelial
9.5. CONVENTIONAL RADIOTHERAPY TECHNIQUE FOR TREATING THYROID CANCER
 9.5. CONVENTIONAL RADIOTHERAPY TECHNIQUE FOR TREATING THYROID CANCER ROBERT J. AMDUR, MD, SIYONG KIM, PhD, JONATHAN GANG LI, PhD, CHIRAY LIU, PhD, WILLIAM M. MENDENHALL, MD, AND ERNEST L. MAZZAFERRI, MD,
9.5. CONVENTIONAL RADIOTHERAPY TECHNIQUE FOR TREATING THYROID CANCER ROBERT J. AMDUR, MD, SIYONG KIM, PhD, JONATHAN GANG LI, PhD, CHIRAY LIU, PhD, WILLIAM M. MENDENHALL, MD, AND ERNEST L. MAZZAFERRI, MD,
Melanoma Case Scenario 1
 Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
3/8/2014. Case Presentation. Primary Treatment of Anal Cancer. Anatomy. Overview. March 6, 2014
 Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
Systemic Treatment. Third International Neuro-Oncology Course. 23 May 2014
 Low-Grade Astrocytoma of the CNS: Systemic Treatment Third International Neuro-Oncology Course São Paulo, Brazil 23 May 2014 John de Groot, MD Associate Professor, Neuro-Oncology UT MD Anderson Cancer
Low-Grade Astrocytoma of the CNS: Systemic Treatment Third International Neuro-Oncology Course São Paulo, Brazil 23 May 2014 John de Groot, MD Associate Professor, Neuro-Oncology UT MD Anderson Cancer
Protocol for the Examination of Specimens From Patients With Wilms and Other Pediatric Renal Tumors
 Protocol for the Examination of Specimens From Patients With Wilms and Other Pediatric Renal Tumors Version: Protocol Posting Date: August 2016 Includes the Children s Oncology Group staging system For
Protocol for the Examination of Specimens From Patients With Wilms and Other Pediatric Renal Tumors Version: Protocol Posting Date: August 2016 Includes the Children s Oncology Group staging system For
1. Sorbonne Universités, UPMC Univ Paris 06, APHP Hôpital Armand Trousseau Pediatric. Surgery, Research Unit St Antoine Inserm UMRS.
 Wilms Tumor state-of-the-art update 2016 Sabine Irtan 1, MD, PhD, Peter F Ehrlich 2, MD, Kathy Pritchard-Jones 3, MD, PhD 1. Sorbonne Universités, UPMC Univ Paris 06, APHP Hôpital Armand Trousseau Pediatric
Wilms Tumor state-of-the-art update 2016 Sabine Irtan 1, MD, PhD, Peter F Ehrlich 2, MD, Kathy Pritchard-Jones 3, MD, PhD 1. Sorbonne Universités, UPMC Univ Paris 06, APHP Hôpital Armand Trousseau Pediatric
BLADDER RADIOTHERAPY PLANNING DOCUMENT
 A 2X2 FACTORIAL RANDOMISED PHASE III STUDY COMPARING STANDARD VERSUS REDUCED VOLUME RADIOTHERAPY WITH AND WITHOUT SYNCHRONOUS CHEMOTHERAPY IN MUSCLE INVASIVE BLADDER CANCER (ISRCTN 68324339) BLADDER RADIOTHERAPY
A 2X2 FACTORIAL RANDOMISED PHASE III STUDY COMPARING STANDARD VERSUS REDUCED VOLUME RADIOTHERAPY WITH AND WITHOUT SYNCHRONOUS CHEMOTHERAPY IN MUSCLE INVASIVE BLADDER CANCER (ISRCTN 68324339) BLADDER RADIOTHERAPY
RECURRENT ADRENAL DISEASE. Megan Applewhite Endorama 2/19/2015 SR , SC
 RECURRENT ADRENAL DISEASE Megan Applewhite Endorama 2/19/2015 SR 2412318, SC 3421561 Category: Adrenal Attendings: Angelos & Grogan PATIENT #1 36yo woman with a hx of Cushing s Syndrome and right adrenalectomy
RECURRENT ADRENAL DISEASE Megan Applewhite Endorama 2/19/2015 SR 2412318, SC 3421561 Category: Adrenal Attendings: Angelos & Grogan PATIENT #1 36yo woman with a hx of Cushing s Syndrome and right adrenalectomy
Radiation Therapy for Liver Malignancies
 Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Melanoma Case Scenario 1
 Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5