Citation Pediatrics international (2015), 57.
|
|
|
- Norah Richards
- 5 years ago
- Views:
Transcription
 Hiramatsu, Hidefumi; Arakawa, Yoshi Nishiuchi, Ritsuo; Adachi, Souichi; Ken-Ichiro Citation Pediatrics international (2015), 57 Issue Date 2015-02-25 URL")

1 Title Long-term efficacy of bevacizumab a pediatric glioblastoma. Umeda, Katsutsugu; Shibata, Hirofum Author(s) Hiramatsu, Hidefumi; Arakawa, Yoshi Nishiuchi, Ritsuo; Adachi, Souichi; Ken-Ichiro Citation Pediatrics international (2015), 57 Issue Date URL A 5-year-old boy with glioblastoma postoperative irradiation in combin Second-line chemotherapy was also i bevacizumab and irinotecan were giv resection of the tumor. Treatment w due to development of posterior rev syndrome, but was re-initiated at a Rightwith prolonged intervals between tr alive and disease free 2 years afte Bevacizumab and irinotecan are a pr pediatric cases of recurrent gliobl resection, although the optimal tre determined on a patient-by-patient be made open to the public on 25 FE publisher's 'Terms and Conditions f Type Journal Article Textversion author Kyoto University
2 Patients Report Long-term efficacy of bevacizumab and irinotecan in recurrent pediatric glioblastoma KATSUTSUGU UMEDA, MD 1, HIROFUMI SHIBATA, MD 1, SATOSHI SAIDA, MD 1, HIDEFUMI HIRAMATSU, MD 1, YOSHIKI ARAKAWA, MD 2, TAKASHI MIZOWAKI, MD 3, RITSUO NISHIUCHI, MD 4, SOUICHI ADACHI, MD 5, TOSHIO HEIKE, MD 1 and KEN-ICHIRO WATANABE, MD 1. Department of Pediatrics 1, Neurosurgery 2, and Radiation Oncology and Image-Applied Therapy 3, Graduate School of Medicine, Kyoto University. 54 Kawahara-cho, Shogoin, Sakyo-ku, Kyoto , Japan 4 Department of Pediatrics, Kochi Health Sciences Center Ike, Kochi , Japan 5 Department of Human Health Science, Graduate School of Medicine, Kyoto University. 53 Kawahara-cho, Shogoin, Sakyo-ku, Kyoto , Japan Corresponding author: Katsutsugu Umeda Department of Pediatrics, Graduate School of Medicine, Kyoto University, 54 Kawahara-cho, Shogoin, Sakyo-ku, Kyoto, , Japan Phone: ; Fax: address: umeume@kuhp.kyoto-u.ac.jp 1
3 Abstract word count: 101 words Number of text pages: 6 pages Text word count: 953 words Number of tables and figures: 2 figures, 0 table Number of reference pages: 2 pages Number of legends to figures: 1 page Running head: Bevacizumab and irinotecan for glioblastoma Key words: bevacizumab, irinotecan, glioblastoma, posterior reversible encephalopathy syndrome 2
4 Abstract A 5-year-old boy with glioblastoma relapsed soon after postoperative irradiation in combination with temozolomide. Second-line chemotherapy was also ineffective; therefore, the bevacizumab and irinotecan were administered after a third gross-total resection of the tumor. Treatment was interrupted for 1 month due to development of posterior reversible encephalopathy syndrome, but was re-initiated at a lower dose of bevacizumab with prolonged intervals between administrations. The patient is alive and disease-free 2 years after initial diagnosis. Bevacizumab and irinotecan are a promising regimen for pediatric cases of recurrent glioblastoma after gross-total resection, although the optimal treatment schedule must be determined on a patient basis. 3
5 Introduction Glioblastoma is the most aggressive form of primary malignant brain tumors. Local radiation therapy in combination with 6 month administration of temozolomide (TMZ) is the standard therapy for newly diagnosed glioblastoma. However, most patients discontinue adjuvant therapy due to disease progression or recurrence. The prognosis of patients with relapsed or refractory glioblastoma is extremely poor with a median survival of 3 to 6 months 1. Furthermore, any effective second- or third-line chemotherapy has not established for such resistant cases. Glioblastoma express high levels of vascular endothelial growth factor (VEGF), and the expression level of VEGF correlates well with prognosis 2. Recently, bevacizumab (BV), a recombinant humanized monoclonal antibody against VEGF, was reported to be effective for recurrent or refractory glioblastoma in adults, especially in combination with irinotecan (CPT11) 3. However, these promising results were not reproduced in a clinical study in children 4, partly because of marked differences in the molecular features of pediatric versus adult glioblastoma 5. Moreover, given that few pediatric cases are treated by BV, there are limited data on its appropriate administration schedule and adverse effects. Here we present a pediatric patient with recurrent glioblastoma who continuously received BV and CPT11 despite the development of severe adverse effects and who is alive without disease progression 2 years after 4
6 initial diagnosis. 5
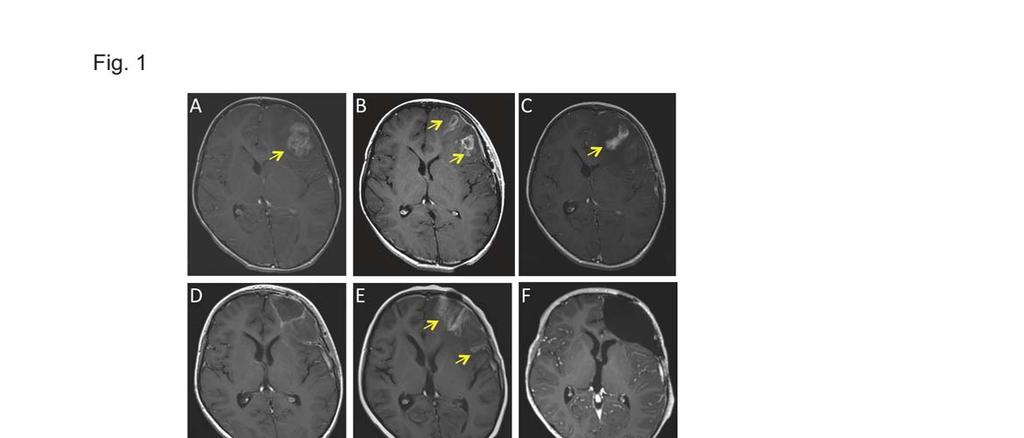
7 Case Report A 5-year-old boy presented with a 1 month history of persistent headache and emesis. Magnetic resonance imaging (MRI) revealed a huge tumor at the left frontal lobe (Figure 1A). Partial resection of the tumor was performed (Figure 1B), and the patient was diagnosed with glioblastoma based on histological findings of the biopsied tumor tissue. The patient first received local irradiation at a dose of 59.8 Gy in 26 fractions in combination with TMZ. However, the tumor regrew locally one month after the start of irradiation (Figure 1C), and the patient underwent a second gross-total resection (Figure 1D), followed by the remaining irradiation and two courses of chemotherapy using ifosfamide, carboplatin, and etoposide. However, 2 months later, the patient developed a second local recurrence (Figure 1E) and a third gross-total resection was performed after transfer to our hospital. The first and second recurrences were confirmed by histological findings of the resected tumor tissues. The patient had a normal neurological examination before chemotherapy. Following the third resection, the patient received BV (10 mg/kg) and CPT11 (125 mg/m 2 ) every 2 weeks. Grade II hypertension and grade III proteinuria occurred after the tenth cycle of chemotherapy, and the dose of BV was reduced to 8 mg/kg and enalapril was started to control hypertension. Eight days after the thirteenth cycle of chemotherapy, the patient developed grade IV hypertension (190 mm Hg systolic and 130 mm Hg diastolic pressure) with 6
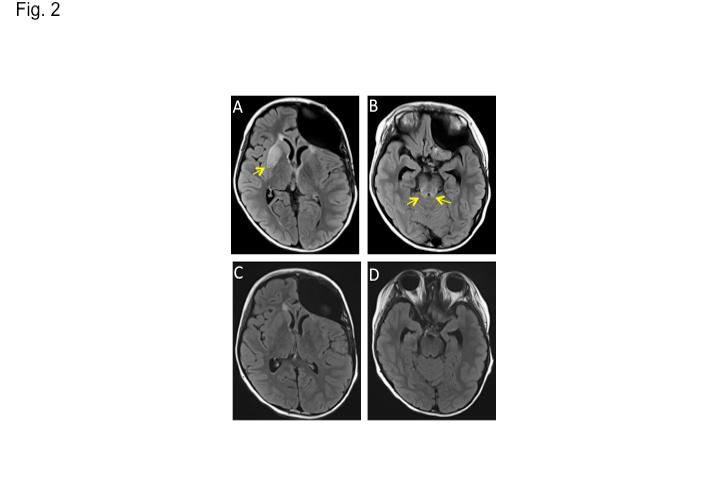
8 headache and emesis. FLAIR T2-weighted images of cranial MRI at symptom onset showed multiple areas of high-intensity intensities at the putamen, thalamus, cerebellum, and brainstem (Figure 2A, B). Therefore, the patient was diagnosed with posterior reversible encephalopathy syndrome (PRES). Chemotherapy was stopped and aggressive antihypertension treatment with nifedipine and enalapril was commenced, resulting in rapid improvement of all symptoms and normalization of blood pressure 3 weeks later; however, grade I proteinuria persisted. Three weeks after the onset of PRES, cranial MRI showed complete disappearance of high-intensity areas (Figure 2C, D). Due to the lack of appropriate alternative compounds for more effective treatment, chemotherapy was restarted 1 month after the onset of PRES with a reduction in BV dose to 7 mg/kg and extension of the treatment interval to once every 3 weeks, in combination with nifedipine and enalapril. Currently, the patient receives BV and CPT11 with no serious adverse effects or neurologic sequelae and is disease-free more than 2 years after initial diagnosis (Figure 1F). 7
9 Discussion Previous clinical studies showed encouraging results with BV and CPT11 therapy in adults with measurable disease of recurrent glioblastoma in terms of objective response rate and progression-free survival 3. However, few patients survived progression-free for more than 1 year. Furthermore, a recent study failed to show long-term survival in children with recurrent glioblastoma with measurable disease treated with BV and CPT11 4. By contrast, a previous study showed that two of three pediatric patients survived more than 3 years after near- or gross-total resection with treatment consisting of conformal radiation and upfront therapy using TMZ and BV 6. Thus, gross-total resection appears to be essential to prevent further relapses by BV-combined chemotherapy, as was reported in clinical studies on multi-drug chemotherapy 7. PRES is a clinical-radiological entity that includes clinical symptoms such as headache, nausea, emesis, visual loss and seizures, all of which are generally reversible. Cranial MRI typically shows white matter abnormalities predominantly in the parietooccipital posterior regions, but involvement of white matter of the anterior and posterior regions as well as of the cerebellum and brain stem has also been reported 8. In our case, interruption of therapy was inevitable due to development of PRES, although no risk factors for this disorder, such as renal dysfunction and hypertension were initially identified prior to commencement of BV and CPT11.BV occasionally causes PRES in both adult and pediatric patients, especially when 8
10 hypertension and proteinuria are poorly controlled, which was seen in the clinical course of the present case 8, 9. Re-initiation of BV-combined therapy is feasible under close blood pressure monitoring and aggressive management of hypertension 8. In our case, we decided to reduce the dose of BV and extend the treatment interval in combination with aggressive antihypertension treatment, because of persistent proteinuria after interruption; as a result, re-initiation of therapy was possible without exacerbation of adverse effects. In conclusion, BV and CPT11 exerted beneficial effects for recurrent pediatric glioblastoma after gross-total resection, although no definite conclusions can be drawn from the small number of cases with relatively short periods of follow-up periods currently in the literature. 9
11 Figure legends Figure 1. (A-F) Radiographic findings of our case. Gadolinium-enhanced T1-weighted images of cranial magnetic resonance imaging (MRI) reveal a huge tumor at the left frontal lobe at initial diagnosis (A). After a first partial resection (B), first recurrence occurred during local irradiation in combination with temozolomide (C). Despite a second gross-total resection (D), the patient developed a second local recurrence (E). After chemotherapy with bevacizumab and irinotecan, the patient is alive and disease-free more than 2 years after initial diagnosis (F). Arrows show tumors at the left frontal lobe. Figure 2. (A-D) Radiographic findings after development of posterior reversible encephalopathy syndrome. FLAIR T2-weighted images of cranial MRI demonstrate multiple high-intensity areas at the putamen, thalamus, cerebellum, and brainstem at symptom onset (arrows) (A, B). Three weeks later, all high-intensity areas completely disappeared (C, D). 10
12 References 1. Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Enlg. J. Med. 2005; 352: Stefanik DF, Fellows WK, Rizkalla LR, et al. Monoclonal antibodies to vascular endothelial growth factor (VEGF) and the VEGF receptor, Flt-1, inhibit the growth of C6 glioma in a mouse xenograft. J. Neurooncol. 2001; 55: Friedman HS, Prados MD, Wen PY, et al. Bevacizumab alone and in combination with irinotecan in recurrent glioblastoma. J. Clin. Oncol. 2009; 27: Gururangan S, Chi SN, Young Poussaint T, et al. Lack of efficacy of bevacizumab plus irinotecan in children with recurrent malignant glioma and diffuse brainstem glioma: a Pediatric Brain Consortium Study. J. Clin. Oncol. 2010; 28: Paugh BS, Qu C, Jones C, et al. Integrated molecular genetic profiling of pediatric high-grade gliomas reveals key differences with the adult disease. J. Clin. Oncol. 2010; 28: Friedman GK, Spiller SE, Harrison DK, et al. Treatment of children with glioblastoma with conformal radiation, temozolomide, and bevacizumab as adjuncts to surgical resection. J. Pediatr. Hematol. Oncol. 2013; 35: e
13 7. Wolff JE, Driever PH, Redldenbruch B, et al. Intensive chemotherapy improves survival in pediatric high-grade glioma after gross total resection: results of the HIT-GBM-C protocol. Cancer 2010; 116: Tlemsani C, Mir O, Boudou-Rouquette P, et al. Posterior encephalopathy syndrome induced by anti-vegf agents. Target Oncol. 2011; 6: Levy CF, Oo KZ, Fireman F, et al. Reversible posterior leukoencephalopathy syndrome in a child treated with bevacizumab. Pediatr Blood Cancer. 2009; 52:
14
15
Title remission for Burkitt's lymphoma. Itaru; Hiramatsu, Hidefumi; Yamada, Citation Pediatrics international (2015), 57
, 57") Title Rituximab-combination chemotherapy remission for Burkitt's lymphoma. Umeda, Katsutsugu; Fujino, Hisanori Author(s) Itaru; Hiramatsu, Hidefumi; Yamada, Toshinori; Adachi, Souichi; Heike, ichiro Citation
Title Rituximab-combination chemotherapy remission for Burkitt's lymphoma. Umeda, Katsutsugu; Fujino, Hisanori Author(s) Itaru; Hiramatsu, Hidefumi; Yamada, Toshinori; Adachi, Souichi; Heike, ichiro Citation
Treatment with Tumor-Treating Fields therapy and pulse dose bevacizumab in patients with bevacizumab-refractory recurrent glioblastoma: A case series.
 School of Medicine Digital Commons@Becker Open Access Publications 2016 Treatment with Tumor-Treating Fields therapy and pulse dose bevacizumab in patients with bevacizumab-refractory recurrent glioblastoma:
School of Medicine Digital Commons@Becker Open Access Publications 2016 Treatment with Tumor-Treating Fields therapy and pulse dose bevacizumab in patients with bevacizumab-refractory recurrent glioblastoma:
Bevacizumab rescue therapy extends the survival in patients with recurrent malignant glioma
 Original Article Bevacizumab rescue therapy extends the survival in patients with recurrent malignant glioma Lin-Bo Cai, Juan Li, Ming-Yao Lai, Chang-Guo Shan, Zong-De Lian, Wei-Ping Hong, Jun-Jie Zhen,
Original Article Bevacizumab rescue therapy extends the survival in patients with recurrent malignant glioma Lin-Bo Cai, Juan Li, Ming-Yao Lai, Chang-Guo Shan, Zong-De Lian, Wei-Ping Hong, Jun-Jie Zhen,
Concomitant (without adjuvant) temozolomide and radiation to treat glioblastoma: A retrospective study
 temozolomide and radiation to treat glioblastoma: A retrospective study") Concomitant (without adjuvant) temozolomide and radiation to treat glioblastoma: A retrospective study T Sridhar 1, A Gore 1, I Boiangiu 1, D Machin 2, R P Symonds 3 1. Department of Oncology, Leicester
Concomitant (without adjuvant) temozolomide and radiation to treat glioblastoma: A retrospective study T Sridhar 1, A Gore 1, I Boiangiu 1, D Machin 2, R P Symonds 3 1. Department of Oncology, Leicester
National Horizon Scanning Centre. Bevacizumab (Avastin) for glioblastoma multiforme - relapsed. August 2008
 for glioblastoma multiforme - relapsed. August 2008") Bevacizumab (Avastin) for glioblastoma multiforme - relapsed August 2008 This technology summary is based on information available at the time of research and a limited literature search. It is not intended
Bevacizumab (Avastin) for glioblastoma multiforme - relapsed August 2008 This technology summary is based on information available at the time of research and a limited literature search. It is not intended
CNS Tumors: The Med Onc Perspective. Ronald J. Scheff, MD Associate Clinical Professor Weill Medical College of Cornell U.
 CNS Tumors: The Med Onc Perspective Ronald J. Scheff, MD Associate Clinical Professor Weill Medical College of Cornell U. Disclosure Speakers Bureau, Merck Basic Oncology Concepts Tissue Diagnosis Stage
CNS Tumors: The Med Onc Perspective Ronald J. Scheff, MD Associate Clinical Professor Weill Medical College of Cornell U. Disclosure Speakers Bureau, Merck Basic Oncology Concepts Tissue Diagnosis Stage
BC Cancer Protocol Summary for Palliative Therapy for Recurrent Malignant Gliomas Using Bevacizumab With or Without Concurrent Etoposide or Lomustine
 BC Cancer Protocol Summary for Palliative Therapy for Recurrent Malignant Gliomas Using Bevacizumab With or Without Concurrent Etoposide or Lomustine Protocol Code Tumour Group Contact Physician CNBEV
BC Cancer Protocol Summary for Palliative Therapy for Recurrent Malignant Gliomas Using Bevacizumab With or Without Concurrent Etoposide or Lomustine Protocol Code Tumour Group Contact Physician CNBEV
Hypofractionated radiation therapy for glioblastoma
 Hypofractionated radiation therapy for glioblastoma Luis Souhami, MD, FASTRO Professor McGill University Department of Oncology, Division of Radiation Oncology Montreal Canada McGill University Health
Hypofractionated radiation therapy for glioblastoma Luis Souhami, MD, FASTRO Professor McGill University Department of Oncology, Division of Radiation Oncology Montreal Canada McGill University Health
Bevacizumab: A Controversial Agent Against High-Grade Gliomas
 Tumor Bevacizumab: A Controversial Agent Against High-Grade Gliomas Sussan Salas, MD 1, Miguel Guzman, MD 2, Kevin Judy, MD 1 1 Department of Neurological Surgery, Thomas Jefferson University, Philadelphia,
Tumor Bevacizumab: A Controversial Agent Against High-Grade Gliomas Sussan Salas, MD 1, Miguel Guzman, MD 2, Kevin Judy, MD 1 1 Department of Neurological Surgery, Thomas Jefferson University, Philadelphia,
Incidence of Early Pseudo-progression in a Cohort of Malignant Glioma Patients Treated With Chemoirradiation With Temozolomide
 405 Incidence of Early Pseudo-progression in a Cohort of Malignant Glioma Patients Treated With Chemoirradiation With Temozolomide Walter Taal, MD 1 Dieta Brandsma, MD, PhD 1 Hein G. de Bruin, MD, PhD
405 Incidence of Early Pseudo-progression in a Cohort of Malignant Glioma Patients Treated With Chemoirradiation With Temozolomide Walter Taal, MD 1 Dieta Brandsma, MD, PhD 1 Hein G. de Bruin, MD, PhD
Scottish Medicines Consortium
 Scottish Medicines Consortium temozolomide 5, 20, 100 and 250mg capsules (Temodal ) Schering Plough UK Ltd No. (244/06) New indication: for the treatment of newly diagnosed glioblastoma multiforme concomitantly
Scottish Medicines Consortium temozolomide 5, 20, 100 and 250mg capsules (Temodal ) Schering Plough UK Ltd No. (244/06) New indication: for the treatment of newly diagnosed glioblastoma multiforme concomitantly
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM ANAPLASTIC GLIOMAS CNS Site Group Anaplastic Gliomas Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM ANAPLASTIC GLIOMAS CNS Site Group Anaplastic Gliomas Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
University of Zurich. Temozolomide and MGMT forever? Zurich Open Repository and Archive. Weller, M. Year: 2010
 University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich Year: 2010 Temozolomide and MGMT forever? Weller, M Weller, M (2010). Temozolomide and MGMT forever? Neuro-Oncology,
University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich Year: 2010 Temozolomide and MGMT forever? Weller, M Weller, M (2010). Temozolomide and MGMT forever? Neuro-Oncology,
Glioblastoma: Current Treatment Approach 8/20/2018
 Glioblastoma: Current Treatment Approach 8/20/2018 Overview What is Glioblastoma? How is it diagnosed How is it treated? Principles of Treatment Surgery, Radiation, Chemotherapy Current Standard of care
Glioblastoma: Current Treatment Approach 8/20/2018 Overview What is Glioblastoma? How is it diagnosed How is it treated? Principles of Treatment Surgery, Radiation, Chemotherapy Current Standard of care
Clinical Trials for Adult Brain Tumors - the Imaging Perspective
 Clinical Trials for Adult Brain Tumors - the Imaging Perspective Whitney B. Pope, M.D., Ph.D. Department of Radiology David Geffen School of Medicine at UCLA August 22, 2015 1 Disclosure of Financial Relationships
Clinical Trials for Adult Brain Tumors - the Imaging Perspective Whitney B. Pope, M.D., Ph.D. Department of Radiology David Geffen School of Medicine at UCLA August 22, 2015 1 Disclosure of Financial Relationships
Contemporary Management of Glioblastoma
 Contemporary Management of Glioblastoma Incidence Rates of Primary Brain Tumors Central Brain Tumor Registry of the United States, 1992-1997 100 Number of Cases per 100,000 Population 10 1 0.1 x I x I
Contemporary Management of Glioblastoma Incidence Rates of Primary Brain Tumors Central Brain Tumor Registry of the United States, 1992-1997 100 Number of Cases per 100,000 Population 10 1 0.1 x I x I
Glioblastoma multiforme has been described as. Bevacizumab and irinotecan therapy in glioblastoma multiforme: a series of 13 cases
 » This article has been updated from its originally published version to correct units of measure. See the corresponding erratum notice, DOI: 10.3171/2017.8.JNS08268a. «J Neurosurg 108:000 000, 109:268
» This article has been updated from its originally published version to correct units of measure. See the corresponding erratum notice, DOI: 10.3171/2017.8.JNS08268a. «J Neurosurg 108:000 000, 109:268
Glioblastoma: Adjuvant Treatment Abdulrazag Ajlan, MD, MSc, FRCSC, UCNS(D)
") Glioblastoma: Adjuvant Treatment Abdulrazag Ajlan, MD, MSc, FRCSC, UCNS(D) *Neurosurgery Consultant, King Saud University, Riyadh, KSA *Adjunct Teaching Faculty, Neurosurgery, Stanford School Of Medicine,
Glioblastoma: Adjuvant Treatment Abdulrazag Ajlan, MD, MSc, FRCSC, UCNS(D) *Neurosurgery Consultant, King Saud University, Riyadh, KSA *Adjunct Teaching Faculty, Neurosurgery, Stanford School Of Medicine,
Survival of High Grade Glioma Patients Treated by Three Radiation Schedules with Chemotherapy: A Retrospective Comparative Study
 Original Article Research in Oncology June 2017; Vol. 13, No. 1: 18-22. DOI: 10.21608/resoncol.2017.552.1022 Survival of High Grade Glioma Patients Treated by Three Radiation Schedules with Chemotherapy:
Original Article Research in Oncology June 2017; Vol. 13, No. 1: 18-22. DOI: 10.21608/resoncol.2017.552.1022 Survival of High Grade Glioma Patients Treated by Three Radiation Schedules with Chemotherapy:
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM LOW GRADE GLIOMAS CNS Site Group Low Grade Gliomas Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM LOW GRADE GLIOMAS CNS Site Group Low Grade Gliomas Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING
Carmustine implants and Temozolomide for the treatment of newly diagnosed high grade glioma
 National Institute for Health and Clinical Excellence Health Technology Appraisal Carmustine implants and Temozolomide for the treatment of newly diagnosed high grade glioma Personal statement Conventional
National Institute for Health and Clinical Excellence Health Technology Appraisal Carmustine implants and Temozolomide for the treatment of newly diagnosed high grade glioma Personal statement Conventional
Bevacizumab and dose-intense temozolomide in recurrent high-grade glioma
 Annals of Oncology 21: 1723 1727, 2010 doi:10.1093/annonc/mdp591 Published online 11 January 2010 Bevacizumab and dose-intense temozolomide in recurrent high-grade glioma J. J. C. Verhoeff 1, C. Lavini
Annals of Oncology 21: 1723 1727, 2010 doi:10.1093/annonc/mdp591 Published online 11 January 2010 Bevacizumab and dose-intense temozolomide in recurrent high-grade glioma J. J. C. Verhoeff 1, C. Lavini
PRESURGICAL PLANNING. Strongly consider neuropsychological evaluation before functional imaging study Strongly consider functional imaging study
 NOTE: Consider Clinical Trials as treatment options for eligible patients. Page 1 of 6 RADIOLOGICAL PRESENTATION PRESURGICAL PLANNING TREATMENT Imaging study suggestive of glioma 1 Left hemisphere speech/motor
NOTE: Consider Clinical Trials as treatment options for eligible patients. Page 1 of 6 RADIOLOGICAL PRESENTATION PRESURGICAL PLANNING TREATMENT Imaging study suggestive of glioma 1 Left hemisphere speech/motor
Clinical Management Protocol Chemotherapy [Glioblastoma Multiforme (CNS)] Protocol for Planning and Treatment
![Clinical Management Protocol Chemotherapy [Glioblastoma Multiforme (CNS)] Protocol for Planning and Treatment](/thumbs/87/96032554.jpg "Clinical Management Protocol Chemotherapy [Glioblastoma Multiforme (CNS)] Protocol for Planning and Treatment") Protocol for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: GLIOBLASTOMA MULTIFORME (CNS) Patient information given at each stage following agreed
Protocol for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: GLIOBLASTOMA MULTIFORME (CNS) Patient information given at each stage following agreed
Case Report Antiangiogenic Therapy in the Treatment of Recurrent Medulloblastoma in the Adult: Case Report and Review of the Literature
 Oncology Volume 2009, Article ID 247873, 4 pages doi:10.1155/2009/247873 Case Report Antiangiogenic Therapy in the Treatment of Recurrent Medulloblastoma in the Adult: Case Report and Review of the Literature
Oncology Volume 2009, Article ID 247873, 4 pages doi:10.1155/2009/247873 Case Report Antiangiogenic Therapy in the Treatment of Recurrent Medulloblastoma in the Adult: Case Report and Review of the Literature
Effective local and systemic therapy is necessary for the cure of Ewing tumor Most chemotherapy regimens are a combination of cyclophosphamide,
 Ewing Tumor Perez Ewing tumor is the second most common primary tumor of bone in childhood, and also occurs in soft tissues Ewing tumor is uncommon before 8 years of age and after 25 years of age In the
Ewing Tumor Perez Ewing tumor is the second most common primary tumor of bone in childhood, and also occurs in soft tissues Ewing tumor is uncommon before 8 years of age and after 25 years of age In the
J Clin Oncol 25: by American Society of Clinical Oncology INTRODUCTION
 VOLUME 25 NUMBER 30 OCTOBER 20 2007 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Bevacizumab Plus Irinotecan in Recurrent Glioblastoma Multiforme James J. Vredenburgh, Annick Desjardins, James
VOLUME 25 NUMBER 30 OCTOBER 20 2007 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Bevacizumab Plus Irinotecan in Recurrent Glioblastoma Multiforme James J. Vredenburgh, Annick Desjardins, James
UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS
 UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS Antonio M. Omuro Department of Neurology Memorial Sloan-Kettering Cancer Center II International Neuro-Oncology Congress Sao Paulo, 08/17/12 CHALLENGES IN
UPDATES ON CHEMOTHERAPY FOR LOW GRADE GLIOMAS Antonio M. Omuro Department of Neurology Memorial Sloan-Kettering Cancer Center II International Neuro-Oncology Congress Sao Paulo, 08/17/12 CHALLENGES IN
21/03/2017. Disclosure. Practice Changing Articles in Neuro Oncology for 2016/17. Gliomas. Objectives. Gliomas. No conflicts to declare
 Practice Changing Articles in Neuro Oncology for 2016/17 Disclosure No conflicts to declare Frances Cusano, BScPharm, ACPR April 21, 2017 Objectives Gliomas To describe the patient selection, methodology
Practice Changing Articles in Neuro Oncology for 2016/17 Disclosure No conflicts to declare Frances Cusano, BScPharm, ACPR April 21, 2017 Objectives Gliomas To describe the patient selection, methodology
Going Past the Data for Temozolomide. J. Lee Villano, M.D., Ph.D., Nathalie Letarte, B.Pharm, M.Sc, Linda R. Bressler, Pharm. D.
 Going Past the Data for Temozolomide J. Lee Villano, M.D., Ph.D., Nathalie Letarte, B.Pharm, M.Sc, Linda R. Bressler, Pharm. D. Departments of Medicine (JLV), Neurosurgery (JLV) and Pharmacy Practice (LRB)
Going Past the Data for Temozolomide J. Lee Villano, M.D., Ph.D., Nathalie Letarte, B.Pharm, M.Sc, Linda R. Bressler, Pharm. D. Departments of Medicine (JLV), Neurosurgery (JLV) and Pharmacy Practice (LRB)
PROCARBAZINE, lomustine, and vincristine (PCV) is
 is") RAPID PUBLICATION Procarbazine, Lomustine, and Vincristine () Chemotherapy for Anaplastic Astrocytoma: A Retrospective Review of Radiation Therapy Oncology Group Protocols Comparing Survival With Carmustine
RAPID PUBLICATION Procarbazine, Lomustine, and Vincristine () Chemotherapy for Anaplastic Astrocytoma: A Retrospective Review of Radiation Therapy Oncology Group Protocols Comparing Survival With Carmustine
Bevacizumab in combination with temozolomide and regional radiation therapy for up-front treatment of patients with newly-diagnosed glioblastoma
 Bevacizumab in combination with temozolomide and regional radiation therapy for up-front treatment of patients with newly-diagnosed glioblastoma Design and analysis of single-arm Phase II clinical trial
Bevacizumab in combination with temozolomide and regional radiation therapy for up-front treatment of patients with newly-diagnosed glioblastoma Design and analysis of single-arm Phase II clinical trial
Systemic Treatment. Third International Neuro-Oncology Course. 23 May 2014
 Low-Grade Astrocytoma of the CNS: Systemic Treatment Third International Neuro-Oncology Course São Paulo, Brazil 23 May 2014 John de Groot, MD Associate Professor, Neuro-Oncology UT MD Anderson Cancer
Low-Grade Astrocytoma of the CNS: Systemic Treatment Third International Neuro-Oncology Course São Paulo, Brazil 23 May 2014 John de Groot, MD Associate Professor, Neuro-Oncology UT MD Anderson Cancer
Treatment With Bevacizumab and Irinotecan for Recurrent High-Grade Glial Tumors
 2267 Treatment With Bevacizumab and Irinotecan for Recurrent High-Grade Glial Tumors Felix Bokstein, MD 1 Shulim Shpigel, MD 2 Deborah T. Blumenthal, MD 1 1 Neuro-Oncology Service, Tel Aviv Sourasky Medical
2267 Treatment With Bevacizumab and Irinotecan for Recurrent High-Grade Glial Tumors Felix Bokstein, MD 1 Shulim Shpigel, MD 2 Deborah T. Blumenthal, MD 1 1 Neuro-Oncology Service, Tel Aviv Sourasky Medical
Theodore S. Johnson, MD, PhD
 Front-line Therapy of DIPG Using IDO Pathway Inhibitor Indoximod in Combination with Radiation and Chemotherapy American Association of Cancer Research (AACR) 2018 Theodore S. Johnson, MD, PhD Georgia
Front-line Therapy of DIPG Using IDO Pathway Inhibitor Indoximod in Combination with Radiation and Chemotherapy American Association of Cancer Research (AACR) 2018 Theodore S. Johnson, MD, PhD Georgia
Protocol Abstract and Schema
 Protocol Abstract and Schema Phase II study of Bevacizumab plus Irinotecan (Camptosar ) in Children with Recurrent, Progressive, or Refractory Malignant Gliomas, Diffuse/Intrinsic Brain Stem Gliomas, Medulloblastomas,
Protocol Abstract and Schema Phase II study of Bevacizumab plus Irinotecan (Camptosar ) in Children with Recurrent, Progressive, or Refractory Malignant Gliomas, Diffuse/Intrinsic Brain Stem Gliomas, Medulloblastomas,
Interferon β and temozolomide combination therapy for temozolomide monotherapy refractory malignant gliomas
 MOLECULAR AND CLINICAL ONCOLOGY 3: 909-913, 2015 Interferon β and temozolomide combination therapy for temozolomide monotherapy refractory malignant gliomas HIROSHI KAWAJI, TSUTOMU TOKUYAMA, TOMOHIRO YAMASAKI,
MOLECULAR AND CLINICAL ONCOLOGY 3: 909-913, 2015 Interferon β and temozolomide combination therapy for temozolomide monotherapy refractory malignant gliomas HIROSHI KAWAJI, TSUTOMU TOKUYAMA, TOMOHIRO YAMASAKI,
FACT SHEET. About Optune
 About Optune Optune is the Tumor Treating Fields (TTFields) delivery system that is approved by the United States (US) Food and Drug Administration (FDA) for the treatment of adult patients with glioblastoma.
About Optune Optune is the Tumor Treating Fields (TTFields) delivery system that is approved by the United States (US) Food and Drug Administration (FDA) for the treatment of adult patients with glioblastoma.
Pediatric Brain Tumors: Updates in Treatment and Care
 Pediatric Brain Tumors: Updates in Treatment and Care Writer Classroom Rishi R. Lulla, MD MS Objectives Introduce the common pediatric brain tumors Discuss current treatment strategies for pediatric brain
Pediatric Brain Tumors: Updates in Treatment and Care Writer Classroom Rishi R. Lulla, MD MS Objectives Introduce the common pediatric brain tumors Discuss current treatment strategies for pediatric brain
Management of Glioma: The Basics Glioma Update The clinical challenge. Glioma a malignant disease of the CNS
 Management of Glioma: The Basics Glioma Update 3 oger Stupp, MD Department of Oncology & Cancer Center University Hospital Zurich, Switzerland (roger.stupp@usz.ch) Bern, 3. August 3 The clinical challenge
Management of Glioma: The Basics Glioma Update 3 oger Stupp, MD Department of Oncology & Cancer Center University Hospital Zurich, Switzerland (roger.stupp@usz.ch) Bern, 3. August 3 The clinical challenge
Newcastle Neuro-oncology Team Audit of Outcome of Glioblastoma Multiforme Chemoradiotherapy Treatment
 Newcastle Neuro-oncology Team Audit of Outcome of Glioblastoma Multiforme Chemoradiotherapy Treatment Jennifer Wright Neurosurgery SSC Audit Team Jennifer Wright, Rachel Tresman, Cyril Dubois, Surash Surash,
Newcastle Neuro-oncology Team Audit of Outcome of Glioblastoma Multiforme Chemoradiotherapy Treatment Jennifer Wright Neurosurgery SSC Audit Team Jennifer Wright, Rachel Tresman, Cyril Dubois, Surash Surash,
Case Report Tackling a Recurrent Pinealoblastoma
 Case Reports in Oncological Medicine, Article ID 135435, 4 pages http://dx.doi.org/10.1155/2014/135435 Case Report Tackling a Recurrent Pinealoblastoma Siddanna Palled, 1 Sruthi Kalavagunta, 1 Jaipal Beerappa
Case Reports in Oncological Medicine, Article ID 135435, 4 pages http://dx.doi.org/10.1155/2014/135435 Case Report Tackling a Recurrent Pinealoblastoma Siddanna Palled, 1 Sruthi Kalavagunta, 1 Jaipal Beerappa
Citation Cancer Management and Research, 2(1
 NAOSITE: Nagasaki University's Ac Title Author(s) Efficacy and safety of amrubicin hy small cell lung cancer Ogawara, Daiki; Fukuda, Minoru; Nak Citation Cancer Management and Research, 2(1 Issue Date
NAOSITE: Nagasaki University's Ac Title Author(s) Efficacy and safety of amrubicin hy small cell lung cancer Ogawara, Daiki; Fukuda, Minoru; Nak Citation Cancer Management and Research, 2(1 Issue Date
ORIGINAL PAPERS. The Impact of Surgery on the Efficacy of Adjuvant Therapy in Glioblastoma Multiforme
 ORIGINAL PAPERS Adv Clin Exp Med 2015, 24, 2, 279 287 DOI: 10.17219/acem/40456 Copyright by Wroclaw Medical University ISSN 1899 5276 Anna Brzozowska 1, 2, A D, Anna Toruń 3, G, Maria Mazurkiewicz1, 2,
ORIGINAL PAPERS Adv Clin Exp Med 2015, 24, 2, 279 287 DOI: 10.17219/acem/40456 Copyright by Wroclaw Medical University ISSN 1899 5276 Anna Brzozowska 1, 2, A D, Anna Toruń 3, G, Maria Mazurkiewicz1, 2,
National Institute for Health and Clinical Excellence. Single Technology Appraisal (STA)
") National Institute for Health and Clinical Excellence Appendix C Comment 1: the draft scope Single Technology Appraisal (STA) Carmustine implants for the treatment of recurrent glioblastoma multiforme
National Institute for Health and Clinical Excellence Appendix C Comment 1: the draft scope Single Technology Appraisal (STA) Carmustine implants for the treatment of recurrent glioblastoma multiforme
MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES
 MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES DISCLOSURE No conflicts of interest to disclose Patricia Bruns APRN, CNS Givens Brain Tumor Center Abbott Northwestern Hospital October 12, 2018 OBJECTIVES THEN
MALIGNANT GLIOMAS: TREATMENT AND CHALLENGES DISCLOSURE No conflicts of interest to disclose Patricia Bruns APRN, CNS Givens Brain Tumor Center Abbott Northwestern Hospital October 12, 2018 OBJECTIVES THEN
It s s Always Something!
 It s s Always Something! New Approaches in Brain Tumor Treatment Virginia Stark-Vance, M.D. When Something Is a Brain Tumor Brain tumors aren t rare: there are over 100,000/yr Most originate as other cancers
It s s Always Something! New Approaches in Brain Tumor Treatment Virginia Stark-Vance, M.D. When Something Is a Brain Tumor Brain tumors aren t rare: there are over 100,000/yr Most originate as other cancers
성균관대학교삼성창원병원신경외과학교실신경종양학 김영준. KNS-MT-03 (April 15, 2015)
") 성균관대학교삼성창원병원신경외과학교실신경종양학 김영준 INTRODUCTIONS Low grade gliomas (LGG) - heterogeneous group of tumors with astrocytic, oligodendroglial, ependymal, or mixed cellular histology - In adults diffuse, infiltrating
성균관대학교삼성창원병원신경외과학교실신경종양학 김영준 INTRODUCTIONS Low grade gliomas (LGG) - heterogeneous group of tumors with astrocytic, oligodendroglial, ependymal, or mixed cellular histology - In adults diffuse, infiltrating
Zurich Open Repository and Archive. Procarbazine and CCNU as initial treatment in gliomatosis cerebri
 University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich http://www.zora.uzh.ch Year: 2008 Procarbazine and CCNU as initial treatment in gliomatosis cerebri Glas, M;
University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich http://www.zora.uzh.ch Year: 2008 Procarbazine and CCNU as initial treatment in gliomatosis cerebri Glas, M;
Temozolomide with Radiotherapy for the Treatment of Malignant Gliomas, Center Experience
 Temozolomide with Radiotherapy for the Treatment of Malignant Gliomas, Center Experience *Ehab Abdou and **Mohamed Gaafar *Department of Radiation Oncology, Faculty of Medicine, Al-Azhar University, Cairo,
Temozolomide with Radiotherapy for the Treatment of Malignant Gliomas, Center Experience *Ehab Abdou and **Mohamed Gaafar *Department of Radiation Oncology, Faculty of Medicine, Al-Azhar University, Cairo,
Selecting the Optimal Treatment for Brain Metastases
 Selecting the Optimal Treatment for Brain Metastases Clinical Practice Today CME Co-provided by Learning Objectives Upon completion, participants should be able to: Understand the benefits, limitations,
Selecting the Optimal Treatment for Brain Metastases Clinical Practice Today CME Co-provided by Learning Objectives Upon completion, participants should be able to: Understand the benefits, limitations,
ADSS Case 1. A 31-year-old male with a seizure. Se-Hoon Kim
 ADSS Case 1 A 31-year-old male with a seizure Se-Hoon Kim Department of Pathology, Yonsei University College of Medicine, Severance Hospital, Seoul, Korea A 31-year-old male patient without specific medical
ADSS Case 1 A 31-year-old male with a seizure Se-Hoon Kim Department of Pathology, Yonsei University College of Medicine, Severance Hospital, Seoul, Korea A 31-year-old male patient without specific medical
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
Department of Medical Oncology, National Cancer Institute of Aviano, Aviano (PN) Italy 3
 Italy 3") WCRJ 2014; 1 (4): e401 RADIOCHEMOTHERAPY FOR UNRESECTABLE GLIOBLASTOMA MULTIFORME: A MONO- INSTITUTIONAL EXPERIENCE M. COLELLA 1, F. FIORICA 1, P. API 1, A. STEFANELLI 1, B. URBINI 2, A. SGUALDO 1, D.
WCRJ 2014; 1 (4): e401 RADIOCHEMOTHERAPY FOR UNRESECTABLE GLIOBLASTOMA MULTIFORME: A MONO- INSTITUTIONAL EXPERIENCE M. COLELLA 1, F. FIORICA 1, P. API 1, A. STEFANELLI 1, B. URBINI 2, A. SGUALDO 1, D.
Bevacizumab 5mg/kg Therapy 14 days
 INDICATIONS FOR USE: Bevacizumab 5mg/kg Therapy 14 days Regimen Code 00211a *Reimbursement status Hospital INDICATION ICD10 In combination with fluoropyrimidine-based chemotherapy C18 for treatment of
INDICATIONS FOR USE: Bevacizumab 5mg/kg Therapy 14 days Regimen Code 00211a *Reimbursement status Hospital INDICATION ICD10 In combination with fluoropyrimidine-based chemotherapy C18 for treatment of
Imaging for suspected glioma
 Imaging for suspected glioma 1.1.1 Offer standard structural MRI (defined as T2 weighted, FLAIR, DWI series and T1 pre- and post-contrast volume) as the initial diagnostic test for suspected glioma, unless
Imaging for suspected glioma 1.1.1 Offer standard structural MRI (defined as T2 weighted, FLAIR, DWI series and T1 pre- and post-contrast volume) as the initial diagnostic test for suspected glioma, unless
HIF-1-mediated metabolic reprogramming reduces ROS levels and facilitates
 HIF-1-mediated metabolic reprogramming reduces ROS levels and facilitates the metastatic colonization of cancers in lungs Authors: Tao ZHAO 1,2,3, Yuxi ZHU 1,2,4, Akiyo MORINIBU 1,2, Minoru KOBAYASHI 1,2,
HIF-1-mediated metabolic reprogramming reduces ROS levels and facilitates the metastatic colonization of cancers in lungs Authors: Tao ZHAO 1,2,3, Yuxi ZHU 1,2,4, Akiyo MORINIBU 1,2, Minoru KOBAYASHI 1,2,
NON-SURGICAL STRATEGY FOR ADULT EPENDYMOMA
 NON-SURGICAL STRATEGY FOR ADULT EPENDYMOMA Roberta Rudà Department of Neuro-Oncology University and City of Health and Science Hospital of Turin, Italy EORTC EANO ESMO Conference 2015 Istanbul, March 27-28
NON-SURGICAL STRATEGY FOR ADULT EPENDYMOMA Roberta Rudà Department of Neuro-Oncology University and City of Health and Science Hospital of Turin, Italy EORTC EANO ESMO Conference 2015 Istanbul, March 27-28
CILENT P Leblond, DIPG Meeting, Barcelone 2012
 CILENT-0902 Cilengitide (EMD121974) in combination with irradiation in children and adolescents with newly diagnosed diffuse intrinsic brainstem glioma : Phase I Study P Leblond, DIPG Meeting, Barcelone
CILENT-0902 Cilengitide (EMD121974) in combination with irradiation in children and adolescents with newly diagnosed diffuse intrinsic brainstem glioma : Phase I Study P Leblond, DIPG Meeting, Barcelone
Bone HDR brachytherapy in a patient with recurrent Ewing s sarcoma of the acetabulum: Alternative to aggressive surgery
 Bone HDR brachytherapy in a patient with recurrent Ewing s sarcoma of the acetabulum: Alternative to aggressive surgery Rafael Martínez-Monge 1,* Agata Pérez-Ochoa 1, Mikel San Julián 2, Dámaso Aquerreta
Bone HDR brachytherapy in a patient with recurrent Ewing s sarcoma of the acetabulum: Alternative to aggressive surgery Rafael Martínez-Monge 1,* Agata Pérez-Ochoa 1, Mikel San Julián 2, Dámaso Aquerreta
Cilengitide (Impetreve) for glioblastoma multiforme. February 2012
 for glioblastoma multiforme. February 2012") Cilengitide (Impetreve) for glioblastoma multiforme February 2012 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to
Cilengitide (Impetreve) for glioblastoma multiforme February 2012 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to
Chika Nwachukwu, Ph.D. MS IV Radiation Oncology Rotation
 Chika Nwachukwu, Ph.D. MS IV Radiation Oncology Rotation Background Histology/Tumor Characteristics Presenting Symptoms/diagnosis Treatment/outcome Patient cohort Research on HRQOL Slow growing indolent
Chika Nwachukwu, Ph.D. MS IV Radiation Oncology Rotation Background Histology/Tumor Characteristics Presenting Symptoms/diagnosis Treatment/outcome Patient cohort Research on HRQOL Slow growing indolent
3-D conformal radiotherapy with concomitant and adjuvant temozolomide for patients with glioblastoma multiforme and evaluation of prognostic factors
 research article 213 3-D conformal radiotherapy with concomitant and adjuvant temozolomide for patients with glioblastoma multiforme and evaluation of prognostic factors Yilmaz Tezcan and Mehmet Koc Department
research article 213 3-D conformal radiotherapy with concomitant and adjuvant temozolomide for patients with glioblastoma multiforme and evaluation of prognostic factors Yilmaz Tezcan and Mehmet Koc Department
Antiangiogenic drugs in unresectable glioblastoma. Dra. Carmen Balañá. /
 Antiangiogenic drugs in unresectable glioblastoma Dra. Carmen Balañá. / Outcome for unresectable GBM Overall survival for unresectable GBM without further treatment is: 3 months at most. Radiotherapy increases
Antiangiogenic drugs in unresectable glioblastoma Dra. Carmen Balañá. / Outcome for unresectable GBM Overall survival for unresectable GBM without further treatment is: 3 months at most. Radiotherapy increases
Zurich Open Repository and Archive. Long-term survival of glioblastoma patients treated with radiotherapy and lomustine plus temozolomide
 University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich http://www.zora.uzh.ch Year: 2009 Long-term survival of glioblastoma patients treated with radiotherapy and lomustine
University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich http://www.zora.uzh.ch Year: 2009 Long-term survival of glioblastoma patients treated with radiotherapy and lomustine
John D. Hainsworth, MD, Kent C. Shih, MD, Gregg C. Shepard, MD, Guy W. Tillinghast, MD, Brett T. Brinker, MD, and David R. Spigel, MD.
 Phase II Study of Concurrent Radiation Therapy, Temozolomide, and Bevacizumab Followed by Bevacizumab/Everolimus as First- Line Treatment for Patients With Glioblastoma John D. Hainsworth, MD, Kent C.
Phase II Study of Concurrent Radiation Therapy, Temozolomide, and Bevacizumab Followed by Bevacizumab/Everolimus as First- Line Treatment for Patients With Glioblastoma John D. Hainsworth, MD, Kent C.
Journal of Pediatric Sciences
 Journal of Pediatric Sciences Role of post-operative radiation therapy in single brain metastasis from clear cell sarcoma in children: a case report with systemic review Fadoua Rais, Naoual Benhmidou,
Journal of Pediatric Sciences Role of post-operative radiation therapy in single brain metastasis from clear cell sarcoma in children: a case report with systemic review Fadoua Rais, Naoual Benhmidou,
Prior to 1993, the only data available in the medical
 Neuro-Oncology Prospective clinical trials of intracranial low-grade glioma in adults and children Edward G. Shaw 1 and Jeffrey H. Wisoff Department of Radiation Oncology, Wake Forest University School
Neuro-Oncology Prospective clinical trials of intracranial low-grade glioma in adults and children Edward G. Shaw 1 and Jeffrey H. Wisoff Department of Radiation Oncology, Wake Forest University School
Efficacy of Treatment for Glioblastoma Multiforme in Elderly Patients (65+): A Retrospective Analysis
: A Retrospective Analysis") Efficacy of Treatment for Glioblastoma Multiforme in Elderly Patients (65+): A Retrospective Analysis Igal Kushnir MD 1 * and Tzahala Tzuk-Shina MD 2 1 Oncology Insitute, Tel Aviv Sourasky Medical Center,
Efficacy of Treatment for Glioblastoma Multiforme in Elderly Patients (65+): A Retrospective Analysis Igal Kushnir MD 1 * and Tzahala Tzuk-Shina MD 2 1 Oncology Insitute, Tel Aviv Sourasky Medical Center,
High grade glioma + brainstem glioma
 + brainstem glioma Highly agressive tumours Median survival ca 9-12 months Curative or palliative treatments? Intensity of treatment Side effects Quality of life issues + brainstem glioma Aims of radiotherapy
+ brainstem glioma Highly agressive tumours Median survival ca 9-12 months Curative or palliative treatments? Intensity of treatment Side effects Quality of life issues + brainstem glioma Aims of radiotherapy
All India Institute of Medical Sciences, New Delhi, INDIA. Department of Pediatric Surgery, Medical Oncology, and Radiology
 All India Institute of Medical Sciences, New Delhi, INDIA Department of Pediatric Surgery, Medical Oncology, and Radiology Clear cell sarcoma of the kidney- rare renal neoplasm second most common renal
All India Institute of Medical Sciences, New Delhi, INDIA Department of Pediatric Surgery, Medical Oncology, and Radiology Clear cell sarcoma of the kidney- rare renal neoplasm second most common renal
Clinical Policy: Electric Tumor Treating Fields (Optune) Reference Number: PA.CP.MP.145
 Reference Number: PA.CP.MP.145") Clinical Policy: Electric Tumor Treating Fields (Optune) Reference Number: PA.CP.MP.145 Effective Date: 01/18 Last Review Date: 04/18 Coding Implications Revision Log Description Electric tumor treating
Clinical Policy: Electric Tumor Treating Fields (Optune) Reference Number: PA.CP.MP.145 Effective Date: 01/18 Last Review Date: 04/18 Coding Implications Revision Log Description Electric tumor treating
Temozolomide in the treatment of recurrent malignant glioma in Chinese patients!"#$%&'()*+,-./0,1234
*+,-./0,1234") Key words: Astrocytoma; Brain neoplasms; Disease-free survival; Glioblastoma; Neoplasm recurrence!!"!"!"#$ DTM Chan WS Poon YL Chan HK Ng Hong Kong Med J 2005;11:452-6 The Chinese University of Hong Kong,
Key words: Astrocytoma; Brain neoplasms; Disease-free survival; Glioblastoma; Neoplasm recurrence!!"!"!"#$ DTM Chan WS Poon YL Chan HK Ng Hong Kong Med J 2005;11:452-6 The Chinese University of Hong Kong,
BC Cancer Protocol Summary for Treatment of Elderly Newly Diagnosed Glioma Patient with Concurrent and Adjuvant Temozolomide and Radiation Therapy
 BC Cancer Protocol Summary for Treatment of Elderly Newly Diagnosed Glioma Patient with Concurrent Adjuvant Temozolomide Radiation Therapy Protocol Code Tumour Group Contact Physician CNELTZRT Neuro-Oncology
BC Cancer Protocol Summary for Treatment of Elderly Newly Diagnosed Glioma Patient with Concurrent Adjuvant Temozolomide Radiation Therapy Protocol Code Tumour Group Contact Physician CNELTZRT Neuro-Oncology
DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES
 DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES Marco Krengli Radiotherapy, Department of Translational Medicine, University of Piemonte Orientale A. Avogadro THE STANDARD OF CARE
DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES Marco Krengli Radiotherapy, Department of Translational Medicine, University of Piemonte Orientale A. Avogadro THE STANDARD OF CARE
1. Introduction. Correspondence should be addressed to Christopher M. Lee; Received 9 July 2013; Accepted 27 August 2013
 Case Reports in Oncological Medicine Volume 2013, Article ID 431857, 5 pages http://dx.doi.org/10.1155/2013/431857 Case Report Long-Term Survival and Improved Quality of Life following Multiple Repeat
Case Reports in Oncological Medicine Volume 2013, Article ID 431857, 5 pages http://dx.doi.org/10.1155/2013/431857 Case Report Long-Term Survival and Improved Quality of Life following Multiple Repeat
Proton beam therapy with concurrent chemotherapy for glioblastoma multiforme: comparison of nimustine hydrochloride and temozolomide
 J Neurooncol DOI 1.17/s11-1-2228-4 CLINIcAL STUDY Proton beam therapy with concurrent chemotherapy for glioblastoma multiforme: comparison of nimustine hydrochloride and temozolomide Masashi Mizumoto 1
J Neurooncol DOI 1.17/s11-1-2228-4 CLINIcAL STUDY Proton beam therapy with concurrent chemotherapy for glioblastoma multiforme: comparison of nimustine hydrochloride and temozolomide Masashi Mizumoto 1
Brain Tumors: Radiologic Perspective
 Brain Tumors: Radiologic Perspective Alberto Bizzi, M.D. Neuroradiology Humanitas Research Hospital Milan, Italy The job of the neuroradiologist in the work-up of brain tumors has quite changed in the
Brain Tumors: Radiologic Perspective Alberto Bizzi, M.D. Neuroradiology Humanitas Research Hospital Milan, Italy The job of the neuroradiologist in the work-up of brain tumors has quite changed in the
Radioterapia no Tratamento dos Gliomas de Baixo Grau
 Radioterapia no Tratamento dos Gliomas de Baixo Grau Dr. Luis Souhami University Montreal - Canada Low Grade Gliomas Relatively rare Heterogeneous, slow growing tumors WHO Classification Grade I Pilocytic
Radioterapia no Tratamento dos Gliomas de Baixo Grau Dr. Luis Souhami University Montreal - Canada Low Grade Gliomas Relatively rare Heterogeneous, slow growing tumors WHO Classification Grade I Pilocytic
Crizotinib in addition to Radiotherapy and TMZ in newly diagnosed GBM
 Crizotinib in addition to Radiotherapy and TMZ in newly diagnosed GBM Juan M Sepúlveda Sánchez Unidad Multidisciplinar de Neurooncología Hospital 12 de Octubre Madrid GEINO 1402. Phase Ib, open-label,
Crizotinib in addition to Radiotherapy and TMZ in newly diagnosed GBM Juan M Sepúlveda Sánchez Unidad Multidisciplinar de Neurooncología Hospital 12 de Octubre Madrid GEINO 1402. Phase Ib, open-label,
Practice of Interferon Therapy
 Interferon Therapy Practice of Interferon Therapy Brain tumor JMAJ 47(1): 18 23, 2004 Toshihiko WAKABAYASHI* and Jun YOSHIDA** *Associate Professor, Center for Genetic and Regenerative Medicine, Nagoya
Interferon Therapy Practice of Interferon Therapy Brain tumor JMAJ 47(1): 18 23, 2004 Toshihiko WAKABAYASHI* and Jun YOSHIDA** *Associate Professor, Center for Genetic and Regenerative Medicine, Nagoya
A Randomized Phase III study: Comparison between Intravenous and Intraarterial ACNU Administration in Newly Diagnosed Primary Glioblastomas
 A Randomized Phase III study: Comparison between Intravenous and Intraarterial ACNU Administration in Newly Diagnosed Primary Glioblastomas F. IMBESI 1, E. MARCHIONI 2, E. BENERICETTI 3, F. ZAPPOLI 4,
A Randomized Phase III study: Comparison between Intravenous and Intraarterial ACNU Administration in Newly Diagnosed Primary Glioblastomas F. IMBESI 1, E. MARCHIONI 2, E. BENERICETTI 3, F. ZAPPOLI 4,
 Title Late recurrence of nonseminomatous successfully treated with intensity Author(s) Kita, Yuki; Imamura, Masaaki; Mizow Yoshiki; Yoshimura, Koji; Hiraoka, Citation Japanese journal of clinical oncolo
Title Late recurrence of nonseminomatous successfully treated with intensity Author(s) Kita, Yuki; Imamura, Masaaki; Mizow Yoshiki; Yoshimura, Koji; Hiraoka, Citation Japanese journal of clinical oncolo
Zurich Open Repository and Archive. Long-term survival of glioblastoma patients treated with radiotherapy and lomustine plus temozolomide
 University of Zurich Zurich Open Repository and Archive Winterthurerstr. 19 CH-857 Zurich http://www.zora.uzh.ch Year: 29 Long-term survival of glioblastoma patients treated with radiotherapy and lomustine
University of Zurich Zurich Open Repository and Archive Winterthurerstr. 19 CH-857 Zurich http://www.zora.uzh.ch Year: 29 Long-term survival of glioblastoma patients treated with radiotherapy and lomustine
Appraisal of carmustine. implants and temozolomide. for newly diagnosed high. Brain and Spine Foundation
 Appraisal of carmustine implants and temozolomide for newly diagnosed high grade glioma Brain and Spine Foundation June 2005 Submission to the National Institute for Health and Clinical Excellence Brain
Appraisal of carmustine implants and temozolomide for newly diagnosed high grade glioma Brain and Spine Foundation June 2005 Submission to the National Institute for Health and Clinical Excellence Brain
CNS SESSION 3/8/ th Multidisciplinary Management of Cancers: A Case based Approach
 CNS SESSION Chair: Ruben Fragoso, MD/PhD UC Davis Fellow: Michael Cardenas, MD UC Davis Panel: Gordon Li, MD Stanford Seema Nagpal, MD Stanford Jennie Taylor, MD UCSF HPI: 46 yo right handed woman who
CNS SESSION Chair: Ruben Fragoso, MD/PhD UC Davis Fellow: Michael Cardenas, MD UC Davis Panel: Gordon Li, MD Stanford Seema Nagpal, MD Stanford Jennie Taylor, MD UCSF HPI: 46 yo right handed woman who
The Radiologic Evaluation of Glioblastoma (GBM) and Differentiation from Pseudoprogression
 and Differentiation from Pseudoprogression") The Radiologic Evaluation of Glioblastoma (GBM) and Differentiation from Pseudoprogression Alexis Roy, Harvard Medical School, Year III Our Patient AB: Clinical Presentation 53 year old female with a past
The Radiologic Evaluation of Glioblastoma (GBM) and Differentiation from Pseudoprogression Alexis Roy, Harvard Medical School, Year III Our Patient AB: Clinical Presentation 53 year old female with a past
Bevacizumab 10mg/kg 14 days
 INDICATIONS FOR USE: Bevacizumab 10mg/kg 14 days Regimen Code 00212a *Reimbursement status Hospital INDICATION ICD10 In combination with fluoropyrimidine-based chemotherapy C18 for treatment of adult patients
INDICATIONS FOR USE: Bevacizumab 10mg/kg 14 days Regimen Code 00212a *Reimbursement status Hospital INDICATION ICD10 In combination with fluoropyrimidine-based chemotherapy C18 for treatment of adult patients
Marizomib (MRZ): Brain Penetrant Irreversible Pan-Proteasome Inhibitor
: Brain Penetrant Irreversible Pan-Proteasome Inhibitor") MARIZOMIB (MRZ) WITH BEVACIZUMAB (BEV) IN WHO GRADE IV MALIGNANT GLIOMA (G4 MG): FULL ENROLLMENT RESULTS FROM THE PHASE 1, MULTICENTER, OPEN-LABEL STUDY Daniela Bota, MD, PhD 1, Annick Desjardins, MD,
MARIZOMIB (MRZ) WITH BEVACIZUMAB (BEV) IN WHO GRADE IV MALIGNANT GLIOMA (G4 MG): FULL ENROLLMENT RESULTS FROM THE PHASE 1, MULTICENTER, OPEN-LABEL STUDY Daniela Bota, MD, PhD 1, Annick Desjardins, MD,
Characteristics of childhood glial tumors, management approaches and life expectancy of the patients
 JBUON 2014; 19(3): 724-732 ISSN: 1107-0625, online ISSN: 2241-6293 www.jbuon.com E-mail: editorial_office@jbuon.com ORIGINAL ARTICLE Characteristics of childhood glial tumors, management approaches and
JBUON 2014; 19(3): 724-732 ISSN: 1107-0625, online ISSN: 2241-6293 www.jbuon.com E-mail: editorial_office@jbuon.com ORIGINAL ARTICLE Characteristics of childhood glial tumors, management approaches and
CURRENT CONTROVERSIES IN THE MANAGEMENT OF HIGH GRADE GLIOMAS: AN INTERACTIVE CASE DISCUSSION *
 CURRENT CONTROVERSIES IN THE MANAGEMENT OF HIGH GRADE GLIOMAS: AN INTERACTIVE CASE DISCUSSION * Alessandro Olivi, MD, Jaishri Blakeley, MD, and Allen K. Sills, MD, FACS ABSTRACT The management of glioma
CURRENT CONTROVERSIES IN THE MANAGEMENT OF HIGH GRADE GLIOMAS: AN INTERACTIVE CASE DISCUSSION * Alessandro Olivi, MD, Jaishri Blakeley, MD, and Allen K. Sills, MD, FACS ABSTRACT The management of glioma
Committee to Evaluate Drugs (CED)
") Committee to Evaluate Drugs (CED) Recommendations and Reasons Document Posted: January 2014 Bevacizumab for recurrent glioblastoma multiforme Product: BEVACIZUMAB (Avastin ) Class of Drugs: vascular endothelial
Committee to Evaluate Drugs (CED) Recommendations and Reasons Document Posted: January 2014 Bevacizumab for recurrent glioblastoma multiforme Product: BEVACIZUMAB (Avastin ) Class of Drugs: vascular endothelial
NICaN Testicular Germ Cell Tumours SACT protocols
 Reference No: Title: Author(s) Ownership: Approval by: Systemic Anti-Cancer Therapy (SACT) Guidelines for Germ Cell Tumours Dr Audrey Fenton Consultant Medical Oncologist, Dr Vicky Coyle Consultant Medical
Reference No: Title: Author(s) Ownership: Approval by: Systemic Anti-Cancer Therapy (SACT) Guidelines for Germ Cell Tumours Dr Audrey Fenton Consultant Medical Oncologist, Dr Vicky Coyle Consultant Medical
J Clin Oncol 27: by American Society of Clinical Oncology INTRODUCTION
 VOLUME 27 NUMBER 28 OCTOBER 1 29 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T From the Brain Tumor Center, Duke University, Durham, NC; Department of Neurosurgery, University of California,
VOLUME 27 NUMBER 28 OCTOBER 1 29 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T From the Brain Tumor Center, Duke University, Durham, NC; Department of Neurosurgery, University of California,
Jennie W Taylor, MD 02/15/2019. Patient 1 Presentation
 Patient 1 Presentation Jennie W Taylor, MD 02/15/2019 A 34 year old right handed woman presents in 07/2015 with 9 years of stereotyped spells of olfactory change, nausea, and altered awareness. Imaging
Patient 1 Presentation Jennie W Taylor, MD 02/15/2019 A 34 year old right handed woman presents in 07/2015 with 9 years of stereotyped spells of olfactory change, nausea, and altered awareness. Imaging
Central Poorly Differentiated Adenocarcinoma of the Maxilla: Report of a Case
 Kobe J. Med. Sci., Vol. 49, No. 2, pp. 45-49, 2003 Central Poorly Differentiated Adenocarcinoma of the Maxilla: Report of a Case MASAHIRO UMEDA 1), SATOSHI YOKOO 1), YASUYUKI SHIBUYA 1), TAKAHIDE KOMORI
Kobe J. Med. Sci., Vol. 49, No. 2, pp. 45-49, 2003 Central Poorly Differentiated Adenocarcinoma of the Maxilla: Report of a Case MASAHIRO UMEDA 1), SATOSHI YOKOO 1), YASUYUKI SHIBUYA 1), TAKAHIDE KOMORI
Survival Analysis of Glioblastoma Multiforme
 DOI:10.22034/APJCP.2018.19.9.2613 RESEARCH ARTICLE Editorial Process: Submission:04/24/2018 Acceptance:08/19/2018 Supapan Witthayanuwat, Montien Pesee*, Chunsri Supaadirek, Narudom Supakalin, Komsan Thamronganantasakul,
DOI:10.22034/APJCP.2018.19.9.2613 RESEARCH ARTICLE Editorial Process: Submission:04/24/2018 Acceptance:08/19/2018 Supapan Witthayanuwat, Montien Pesee*, Chunsri Supaadirek, Narudom Supakalin, Komsan Thamronganantasakul,
An international study under the guidance of the European Organization
 2617 COMMENTARY Chemotherapy for Glioblastoma Is Costly Better? Ute Linz, MD, PhD Juelich Research Center, IKP/INB, Juelich, Germany. Address for reprints: Ute Linz, MD, PhD, Forschungszentrum J ulich
2617 COMMENTARY Chemotherapy for Glioblastoma Is Costly Better? Ute Linz, MD, PhD Juelich Research Center, IKP/INB, Juelich, Germany. Address for reprints: Ute Linz, MD, PhD, Forschungszentrum J ulich
Efficacy of carbon-ion radiotherapy and high-dose chemotherapy for patients with unresectable Ewing s sarcoma family of tumors
 DOI 10.1007/s10147-012-0480-y ORIGINAL ARTICLE Efficacy of carbon-ion radiotherapy and high-dose chemotherapy for patients with unresectable Ewing s sarcoma family of tumors Shintaro Iwata Tsukasa Yonemoto
DOI 10.1007/s10147-012-0480-y ORIGINAL ARTICLE Efficacy of carbon-ion radiotherapy and high-dose chemotherapy for patients with unresectable Ewing s sarcoma family of tumors Shintaro Iwata Tsukasa Yonemoto
Defining pseudoprogression in glioblastoma multiforme
 European Journal of Neurology 2013, 20: 1335 1341 CME ARTICLE doi:10.1111/ene.12192 Defining pseudoprogression in glioblastoma multiforme E. Van Mieghem a, A. Wozniak b, Y. Geussens c, J. Menten c, S.
European Journal of Neurology 2013, 20: 1335 1341 CME ARTICLE doi:10.1111/ene.12192 Defining pseudoprogression in glioblastoma multiforme E. Van Mieghem a, A. Wozniak b, Y. Geussens c, J. Menten c, S.