L impatto dell imaging sulla definizione della strategia terapeutica
|
|
|
- Madison Todd
- 6 years ago
- Views:
Transcription


1 GISCoR L impatto dell imaging sulla definizione della strategia terapeutica M. Galeandro U.C. Radioterapia Oncologica ASMN-IRCCS Reggio Emilia 14 Novembre 2014


2 Rectal Cancer TNM AJCC-7 th edition 2010
3 Rectal cancer staging is based on 2 principles: To define the pertinent anatomy, allowing for surgical planning To allow prognostic stage grouping To select a tailored therapeutic approach in relation to the risk of local or distant recurrence To reduce overall morbidity from potential overtreatment, while allowing aggressive treatment of high-risk patients Therefore, the aim of preoperative staging is to accurately differentiate between good and poor prognosis tumors

4 IL BUONO ct1-2 AND cn0 No preop RT IL BRUTTO IL CATTIVO ct3, expected CRM or any suspicious node not threatening the surgical margin expected close (<1mm) or CRM+ rectal cancer or tumor encroaching onto sphincterial plane or elevator involvement Short course RT Combined-modality therapy consisting of surgery, radiation therapy, and chemotherapy is recommended for the majority of patients with stage II or stage III Long course CRT BRUTTO/CATTIVO borderline rectal cancer appearing unresectable or borderline resectable Long course CRT
5 Compared to postop (C)RT, the preop (C)RT is associated with a superior overall compliance rate, an improved rate of local control, reduced toxicity, an increased rate of sphincter preservation (?) Do not offer preop (C)RT solely to facilitate sphincter-saving surgery Main disadvantage: possibility of overtreating early-stage tumors Even with improvements in preoperative staging techniques, the risk of over or under-staging disease has not been eliminated Post-op CRT is recommended when stage I rectal cancer is upstaged to stage II or III after pathologic review of the surgical specimen
 2. circumferential resection margin (CRM) 3. extramural vascular invasion (EMVi) 4. nodal status 5.")
6 Selection of Patients for Preop Treatment Based on Prognostic Features The assessment of morphologic features by histopathologists in the resected rectal specimen remains the most robust method of prognostic stratification These features include assessment of 1. depth of spread (> o 5mm) 2. circumferential resection margin (CRM) 3. extramural vascular invasion (EMVi) 4. nodal status 5. peritoneal perforation
7 Modalities of Local Staging Intraluminal Endoscopic Ultrasound (EUS) Very accurate for early-stage low tumors (T1 and T2), with a sensitivity of 94% and specificity of 86% but performs less well in cases of advanced rectal cancer (Garcia-Aguilar 2000) EUS can detect lymph nodes >5 mm in size; but an estimated 50% of metastatic lymph node associated with rectal cancer is smaller than 5 mm, so the sensitivity of EUS is limited The mesorectum and the peritoneum cannot be visualized by EUS, so the CRM status and degree of peritoneal involevment cannot be determined None information about extramural venous invasion

8 CT Scanning for M MRI



9
 2. circumferential resection margin (CRM) 3. extramural vascular invasion (EMVi) 4. nodal status 1.")
10 Selection of Patients for Preop Treatment Based on Prognostic Features The assessment of morphologic features by histopathologists in the resected rectal specimen remains the most robust method of prognostic stratification These features include assessment of 1. depth of spread (> o 5mm) 2. circumferential resection margin (CRM) 3. extramural vascular invasion (EMVi) 4. nodal status 1. Location and sphinteric infiltration

11 Extramural tumor depth study # pts stage treatments results MERCURY Radiology any stage various approaches MR is accurate to measure Extramural depth MRI is equivalent to histology in measurement of extramural depth This is independent of lymph node involvement T with extension into the mesorectum >5 mm have lower 5 y survival Sensitivities 71-91% Specificities of % MRI imaging can enable accurate preoperative prognostication


12 Extramural tumor depth Since the maximal extramural depth of spread, from the outer edge of muscularis propria to the outermost edge of the tumour, correlates with cancer specific survival, clinical stage T3 rectal cancers should be subclassified as depicted in table


13 Circumferential resection margin If the MRF is involved or if the tumour extends to a point within 1 mm from the MRF, there is a clear risk that CRM will be involved after surgery if only a TME is performed



14 Circumferential resection margin Since Patients pre-op with RT-CRT a CRM clearance is more of efficient less than and 1 and less 5 mm toxic have than a worse post-op 5- therapy, y survival it has than become patients increasingly with a larger important margin to evaluate the risk of MRF+ before the surgery For preoperative staging of rectal cancer, the best cut-off distance Of for the predicting preoperative MRF involvement features, using the relationship MRI is 1 mm of the tumour to the MRF has emerged as one of the most powerful predictors of outcome in terms of local recurrence, development of DM, survival
15 Extramural venous invasion(emvi) Presence of malignant cells within the endothelial blood vessels beyond the muscularis propria It can occur in up to 50% of rectal cancer patients EMVI can be identified pre-operatively on MRI with reasonable accuracy EMVI is a poor prognostic factor for overall survival and local recurrence The poor prognostic value on overall survival and local recurrence of EMVI is independent of tumour stage
16 Lymph node status 15-42% of pts have small <5 mm mesorectal patologic lymph nodes Identifying nodal disease is still a diagnostic problem Although lymph node size is not accurate for defining N metastases, nodes of >8 mm are suspicious for nodal involvement on CT, MRI and EUS The most reliable method of positively identifying nodal metastases is based on morphological features such as the presence of a round shape, heterogeneity within the lymph node and/or irregularity of the borders of the lymph node due to capsular penetration by malignancy
17 Lymph node status The overall accuracy of N-staging is low but the preferred examination for nodal staging MRI is FNA is not recommended for nodal staging FDG/PET has shown disappointing results for N- staging in rectal cancer, especially in the mesorectum in the presence of a bulky tumour
18 Two more relavant information. Tumor location MRI is accurate in measuring the distance between the ano-rectal junction and the distal part of the tumor; is accurate for the tumor length Sphinteric infiltration MRI is reliable in assessing sphinteric infiltration, is the preferred method

19 122 of 374 patients followed up in the MERCURY study were defined as good prognosis stage III or less on MRI The routine policy was primary surgery alone in MRI-predicted stage I, II and in MRI good prognosis stage III Results: 5y-OS: 68% 5y-DFS: 85% LR: 3%
20 Scenario of ongoing research supported by the multimodal imaging Radiotherapy intensification Dose escalation Treatment de-intensification No surgery for complete clinical response?

21 Radiotherapy intensification Dose escalation
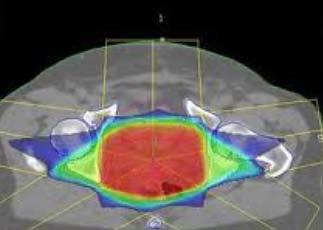
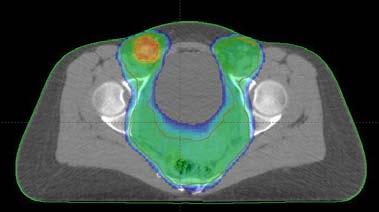
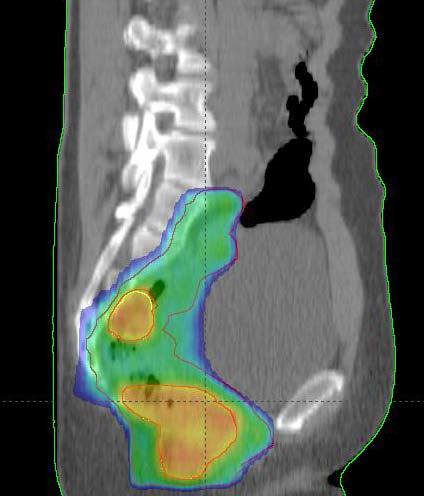
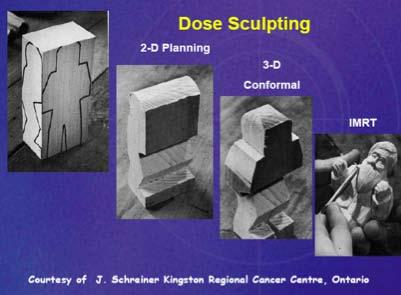
22 Radiotherapy intensification Dose escalation 3D CRT IMRT



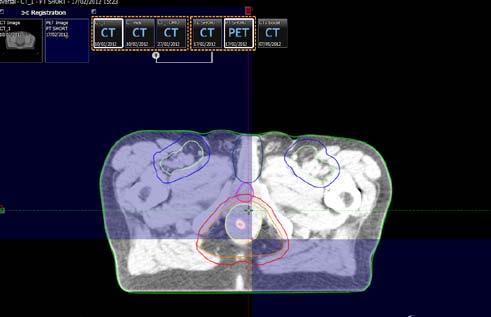

23 Registration images Multimodality Imaging


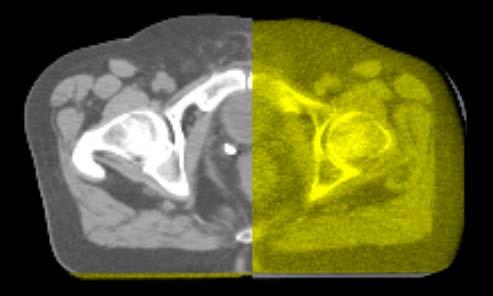
24 Radiotherapy intensification Dose escalation Set-up control before delivery

25 Treatment de-intensification No surgery for complete clinical response? Neoadjuvant therapy and surgery contributes markedly to poorer functional outcomes and secondary complications The impressive incidence of pcr in recent trials raises the possibility of selecting pts with a ccr atfer preopertive treatment to avoid surgery WATCH AND WAIT POLICY

26 Treatment de-intensification No surgery for complete clinical response? Collected data show a high recurrence in the first 12 months, patients following the watch and wait approach should be monitored intensively in the first year At present, the evidence supporting this treatment is limited Results from prospective studies and trials using modern imaging techniques will be essential to guide oncologists in the selection of appropriate patients for nonoperative management of rectal cancer after CRT

27 Grazie per l Attenzione
Disclosure. Acknowledgement. What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Rectal cancer imaging. None
 What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
RECTAL CARCINOMA: A DISTANCE APPROACH. Stephanie Nougaret
 RECTAL CARCINOMA: A DISTANCE APPROACH Stephanie Nougaret stephanienougaret@free.fr Despite the major improvements that have been made due to total mesorectal excision (TME) management of rectal cancer
RECTAL CARCINOMA: A DISTANCE APPROACH Stephanie Nougaret stephanienougaret@free.fr Despite the major improvements that have been made due to total mesorectal excision (TME) management of rectal cancer
Carcinoma del retto: Highlights
 Carcinoma del retto: Highlights Stefano Cordio Struttura Complessa di Oncologia Medica ARNAS Garibaldi Catania Roma 17 Febbraio 2018 Disclosures Advisory Committee, research funding and speakers bureau
Carcinoma del retto: Highlights Stefano Cordio Struttura Complessa di Oncologia Medica ARNAS Garibaldi Catania Roma 17 Febbraio 2018 Disclosures Advisory Committee, research funding and speakers bureau
Radiotherapy for rectal cancer. Karin Haustermans Department of Radiation Oncology
 Radiotherapy for rectal cancer Karin Haustermans Department of Radiation Oncology O U T L I N E RT with TME surgery? Neoadjuvant or adjuvant RT? 5 x 5 Gy or long-course CRT? RT with new drugs? Selection
Radiotherapy for rectal cancer Karin Haustermans Department of Radiation Oncology O U T L I N E RT with TME surgery? Neoadjuvant or adjuvant RT? 5 x 5 Gy or long-course CRT? RT with new drugs? Selection
RECTAL CANCER CLINICAL CASE PRESENTATION
 RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Rectal cancer management: a team sport The role of radiology and the multidisciplinary conference
 Rectal cancer management: a team sport The role of radiology and the multidisciplinary conference W. Donald Buie MD MSc FRCSC Professor of Surgery and Oncology Department of Surgery University of Calgary
Rectal cancer management: a team sport The role of radiology and the multidisciplinary conference W. Donald Buie MD MSc FRCSC Professor of Surgery and Oncology Department of Surgery University of Calgary
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress?
 Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
IMAGING GUIDELINES - COLORECTAL CANCER
 IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016. Background
 Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Rectal Cancer: Classic Hits
 Rectal Cancer: Classic Hits Charles M. Friel, MD Associate Professor of Surgery Section of Colon and Rectal Surgery University of Virginia September 28, 2016 None Disclosures 1 Objectives Review the Classic
Rectal Cancer: Classic Hits Charles M. Friel, MD Associate Professor of Surgery Section of Colon and Rectal Surgery University of Virginia September 28, 2016 None Disclosures 1 Objectives Review the Classic
COLORECTAL CARCINOMA
 QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
Role of MRI for Staging Rectal Cancer
 Role of MRI for Staging Rectal Cancer High-resolution MRI has supplanted endoscopic ultrasound for staging rectal cancer. High-resolution MR images closely match histology and can show details such as
Role of MRI for Staging Rectal Cancer High-resolution MRI has supplanted endoscopic ultrasound for staging rectal cancer. High-resolution MR images closely match histology and can show details such as
COLORECTAL CANCER STAGING in 2010
 COLORECTAL CANCER STAGING in 2010 Robert A. Halvorsen, MD, FACR MCV Hospitals / VCU Medical Center Richmond, Virginia I do not have any relevant financial relationships with any commercial interests COLON
COLORECTAL CANCER STAGING in 2010 Robert A. Halvorsen, MD, FACR MCV Hospitals / VCU Medical Center Richmond, Virginia I do not have any relevant financial relationships with any commercial interests COLON
Rob Glynne-Jones Mount Vernon Cancer Centre
 ESMO Preceptorship Programme Colorectal Cancer Valencia May 2018 State of the art: Standards of care in preoperative treatment for rectal cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures:
ESMO Preceptorship Programme Colorectal Cancer Valencia May 2018 State of the art: Standards of care in preoperative treatment for rectal cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures:
Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015
: Imaging Guidelines September 2015") Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015 1 Contents Page No. 1. Objective 3 2. Imaging Techniques 3 3. Staging of Colorectal Cancer 5 4. Radiological Reporting 6
Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015 1 Contents Page No. 1. Objective 3 2. Imaging Techniques 3 3. Staging of Colorectal Cancer 5 4. Radiological Reporting 6
Rectal Cancer : Curative treatment without surgery
 Rectal Cancer : Curative treatment without surgery Dieter Hahnloser dieter.hahnloser@chuv.ch CHUV University Hospital Lausanne Switzerland Reasons for intervention (surgery) Cure Live longer Feel better
Rectal Cancer : Curative treatment without surgery Dieter Hahnloser dieter.hahnloser@chuv.ch CHUV University Hospital Lausanne Switzerland Reasons for intervention (surgery) Cure Live longer Feel better
UCL. Rectum Adenocarcinoma. Quality of conformal radiotherapy Impact for the surgeon P. Scalliet & K. Haustermans
 Rectum Adenocarcinoma Quality of conformal radiotherapy Impact for the surgeon P. Scalliet & K. Haustermans Fifth Belgian Surgical Week May 6th, 2004, Oostende SOR rectum adenocarcinoma Indication of radiotherapy
Rectum Adenocarcinoma Quality of conformal radiotherapy Impact for the surgeon P. Scalliet & K. Haustermans Fifth Belgian Surgical Week May 6th, 2004, Oostende SOR rectum adenocarcinoma Indication of radiotherapy
Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh
 Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh What is Early rectal cancer? pt1t2n0m0 Predictors for LN involvement Size Depth Intramural
Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh What is Early rectal cancer? pt1t2n0m0 Predictors for LN involvement Size Depth Intramural
Rectal Cancer Update 2008 The Last 5 cm. Consensus Building
 Rectal Cancer Update 2008 The Last 5 cm Consensus Building Case Distal Rectal Cancer 65 male physician Rectal mass: 5cm from anal verge, 1cm above sphincter? Imaging choice: CT vs MR vs ERUS? Adjuvant
Rectal Cancer Update 2008 The Last 5 cm Consensus Building Case Distal Rectal Cancer 65 male physician Rectal mass: 5cm from anal verge, 1cm above sphincter? Imaging choice: CT vs MR vs ERUS? Adjuvant
Radiotherapy for Rectal Cancer. Kevin Palumbo Adelaide Radiotherapy Centre
 Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Local staging of colon cancer: the current role of CT
 Local staging of colon cancer: the current role of CT Poster No.: C-2699 Congress: ECR 2018 Type: Authors: Keywords: DOI: Educational Exhibit A. P. Pissarra, R. R. Domingues Madaleno, C. Sanches, L. Curvo-
Local staging of colon cancer: the current role of CT Poster No.: C-2699 Congress: ECR 2018 Type: Authors: Keywords: DOI: Educational Exhibit A. P. Pissarra, R. R. Domingues Madaleno, C. Sanches, L. Curvo-
MRI in staging of rectal carcinoma
 MRI in staging of rectal carcinoma Poster No.: C-0152 Congress: ECR 2015 Type: Scientific Exhibit Authors: J. R. Ramos Rodriguez, M. Atencia Ballesteros, M. D. M. Muñoz Ruiz, A. J. Márquez Moreno, M. D.
MRI in staging of rectal carcinoma Poster No.: C-0152 Congress: ECR 2015 Type: Scientific Exhibit Authors: J. R. Ramos Rodriguez, M. Atencia Ballesteros, M. D. M. Muñoz Ruiz, A. J. Márquez Moreno, M. D.
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/887/22038 holds various files of this Leiden University dissertation. Author: Swellengrebel, H.A.M. Title: Challenges in the multimodality treatment of rectal
Cover Page The handle http://hdl.handle.net/887/22038 holds various files of this Leiden University dissertation. Author: Swellengrebel, H.A.M. Title: Challenges in the multimodality treatment of rectal
Case Scenario 1. The patient has now completed his neoadjuvant chemoradiation and has been cleared for surgery.
 Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Handling & Grossing of Colo-rectal Specimens for Tumours. for Medical Officers in Pathology
 Handling & Grossing of Colo-rectal Specimens for Tumours for Medical Officers in Pathology Dr Gayana Mahendra Department of Pathology Faculty of Medicine University of Kelaniya Your Role in handling colorectal
Handling & Grossing of Colo-rectal Specimens for Tumours for Medical Officers in Pathology Dr Gayana Mahendra Department of Pathology Faculty of Medicine University of Kelaniya Your Role in handling colorectal
ADJUVANT CHEMOTHERAPY...
 Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
CT PET SCANNING for GIT Malignancies A clinician s perspective
 CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
Staging Colorectal Cancer
 Staging Colorectal Cancer CT is recommended as the initial staging scan for colorectal cancer to assess local extent of the disease and to look for metastases to the liver and/or lung Further imaging for
Staging Colorectal Cancer CT is recommended as the initial staging scan for colorectal cancer to assess local extent of the disease and to look for metastases to the liver and/or lung Further imaging for
Pathohistological Assessment of the Circular Margin of Resection During Total Mesorectal Excision, Conducted on The Malignant Formations of the Rectum
 International Journal of Research Studies in Science, Engineering and Technology Volume 4, Issue 5, 2017, PP 17-22 ISSN : 2349-476X http://dx.doi.org/10.22259/ijrsset.0405004 Pathohistological Assessment
International Journal of Research Studies in Science, Engineering and Technology Volume 4, Issue 5, 2017, PP 17-22 ISSN : 2349-476X http://dx.doi.org/10.22259/ijrsset.0405004 Pathohistological Assessment
COLON AND RECTAL CANCER
 COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
is time consuming and expensive. An intra-operative assessment is not going to be helpful if there is no more tissue that can be taken to improve the
 My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
CHAPTER 7 Concluding remarks and implications for further research
 CONCLUDING REMARKS AND IMPLICATIONS FOR FURTHER RESEARCH CHAPTER 7 Concluding remarks and implications for further research 111 CHAPTER 7 Molecular staging of large sessile rectal tumors In this thesis,
CONCLUDING REMARKS AND IMPLICATIONS FOR FURTHER RESEARCH CHAPTER 7 Concluding remarks and implications for further research 111 CHAPTER 7 Molecular staging of large sessile rectal tumors In this thesis,
State of the art: Standard(s) of radio/chemotherapy for rectal cancer
 of radio/chemotherapy for rectal cancer") State of the art: Standard(s) of radio/chemotherapy for rectal cancer Dr Ian Chau Consultant Medical Oncologist The Royal Marsden Hospital London & Surrey Disclosure Advisory Board: Sanofi Oncology, Eli-
State of the art: Standard(s) of radio/chemotherapy for rectal cancer Dr Ian Chau Consultant Medical Oncologist The Royal Marsden Hospital London & Surrey Disclosure Advisory Board: Sanofi Oncology, Eli-
Preoperative adjuvant radiotherapy
 Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Staging of rectal cancer on MRI: What the surgeons want to know.
 Staging of rectal cancer on MRI: What the surgeons want to know. Poster No.: C-1108 Congress: ECR 2014 Type: Educational Exhibit Authors: G. Ayub, R. Chittal, A. Lowe, A. S. Punekar ; Leeds/, 1 2 1 2 2
Staging of rectal cancer on MRI: What the surgeons want to know. Poster No.: C-1108 Congress: ECR 2014 Type: Educational Exhibit Authors: G. Ayub, R. Chittal, A. Lowe, A. S. Punekar ; Leeds/, 1 2 1 2 2
PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS
 PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS Produced by: Address: Yorkshire Cancer Network Pathology Group Arthington House, Cookridge Hospital, Hospital
PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS Produced by: Address: Yorkshire Cancer Network Pathology Group Arthington House, Cookridge Hospital, Hospital
LOINC. Clinical information. RCPA code. Record if different to report header Operating surgeon name and contact details. Absent.
 Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Case Conference. Craig Morgenthal Department of Surgery Long Island College Hospital
 Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Disclosures. Outline. What IS tumor budding?? Tumor Budding in Colorectal Carcinoma: What, Why, and How. I have nothing to disclose
 Tumor Budding in Colorectal Carcinoma: What, Why, and How Disclosures I have nothing to disclose Soo-Jin Cho, MD, PhD Assistant Professor UCSF Dept of Pathology Current Issues in Anatomic Pathology 2017
Tumor Budding in Colorectal Carcinoma: What, Why, and How Disclosures I have nothing to disclose Soo-Jin Cho, MD, PhD Assistant Professor UCSF Dept of Pathology Current Issues in Anatomic Pathology 2017
Colorectal Cancer Structured Pathology Reporting Proforma DD MM YYYY
 Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Meta analysis in Rectal Cancer
 Meta analysis in Rectal Cancer Dr. Monica Irukulla Professor and Head Department of Radiation Oncology Nizam s Institute of Medical Sciences hyderabad Areas of meta analysis in rectal cancers Epidemiology
Meta analysis in Rectal Cancer Dr. Monica Irukulla Professor and Head Department of Radiation Oncology Nizam s Institute of Medical Sciences hyderabad Areas of meta analysis in rectal cancers Epidemiology
Treatment of Locally Advanced Rectal Cancer: Current Concepts
 Treatment of Locally Advanced Rectal Cancer: Current Concepts James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Treatment of Locally Advanced Rectal Cancer: Current Concepts James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Dr. Anat Ravid Surgical Oncology Lead Erie St. Clair Regional Cancer Program May 1, 2014
 Preoperative Staging MRI in Rectal Cancer: Where Are We Going in the Pelvis? Dr. Anat Ravid Surgical Oncology Lead Erie St. Clair Regional Cancer Program May 1, 2014 Objectives: How are we looking? Who
Preoperative Staging MRI in Rectal Cancer: Where Are We Going in the Pelvis? Dr. Anat Ravid Surgical Oncology Lead Erie St. Clair Regional Cancer Program May 1, 2014 Objectives: How are we looking? Who
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
MRI Rectal Staging Template Revision Summary
 MRI Rectal Staging Template 2015 Revision Summary The following changes have been made since the June 2012 release. Formatting Standardized headings were added to the template. These headings are: Clinical
MRI Rectal Staging Template 2015 Revision Summary The following changes have been made since the June 2012 release. Formatting Standardized headings were added to the template. These headings are: Clinical
Colorectal Cancer and FDG PET/CT
 Hybrid imaging in colorectal & esophageal cancer Emmanuel Deshayes IAEA WorkShop, November 2017 Colorectal Cancer and FDG PET/CT 1 Clinical background Cancer of the colon and rectum is one of the most
Hybrid imaging in colorectal & esophageal cancer Emmanuel Deshayes IAEA WorkShop, November 2017 Colorectal Cancer and FDG PET/CT 1 Clinical background Cancer of the colon and rectum is one of the most
Current Issues and Controversies in the Management of Rectal Cancer
 Current Issues and Controversies in the Management of Rectal Cancer Ghazi M. Nsouli MD 11 th Annual Congress of the Lebanese Society of Gastroenterology November 16, 2012 GMN 20121116 1 Staging of rectal
Current Issues and Controversies in the Management of Rectal Cancer Ghazi M. Nsouli MD 11 th Annual Congress of the Lebanese Society of Gastroenterology November 16, 2012 GMN 20121116 1 Staging of rectal
COLON AND RECTAL CANCER
 No disclosures COLON AND RECTAL CANCER Mark Sun, MD Clinical Assistant Professor of Surgery University of Minnesota Colon and Rectal Cancer Statistics Overall Incidence 2016 134,490 new cases 8.0% of all
No disclosures COLON AND RECTAL CANCER Mark Sun, MD Clinical Assistant Professor of Surgery University of Minnesota Colon and Rectal Cancer Statistics Overall Incidence 2016 134,490 new cases 8.0% of all
Dr Sneha Shah Tata Memorial Hospital, Mumbai.
 Dr Sneha Shah Tata Memorial Hospital, Mumbai. Topics covered Lymphomas including Burkitts Pediatric solid tumors (non CNS) Musculoskeletal Ewings & osteosarcoma. Neuroblastomas Nasopharyngeal carcinomas
Dr Sneha Shah Tata Memorial Hospital, Mumbai. Topics covered Lymphomas including Burkitts Pediatric solid tumors (non CNS) Musculoskeletal Ewings & osteosarcoma. Neuroblastomas Nasopharyngeal carcinomas
Surgical Margins in Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma
 Surgical Margins in Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma Consensus update and recommendations, 2018 Head and Neck Steering Committee P. Gorphe *, F. Nguyen, Y. Tao, P. Blanchard,
Surgical Margins in Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma Consensus update and recommendations, 2018 Head and Neck Steering Committee P. Gorphe *, F. Nguyen, Y. Tao, P. Blanchard,
Local Excision of Rectal Cancer Techniques and Outcomes
 Local Excision of Rectal Cancer Techniques and Outcomes Manoj J. Raval, MD, MSc, FRCSC Clinical Assistant Professor, UBC Rectal Cancer Update 2008 October 25, 2008 Overview Techniques & Description Patient
Local Excision of Rectal Cancer Techniques and Outcomes Manoj J. Raval, MD, MSc, FRCSC Clinical Assistant Professor, UBC Rectal Cancer Update 2008 October 25, 2008 Overview Techniques & Description Patient
Locally advanced head and neck cancer
 Locally advanced head and neck cancer Radiation Oncology Perspective Petek Erpolat, MD Gazi University, Turkey Definition and Management of LAHNC Stage III or IV cancers generally include larger primary
Locally advanced head and neck cancer Radiation Oncology Perspective Petek Erpolat, MD Gazi University, Turkey Definition and Management of LAHNC Stage III or IV cancers generally include larger primary
Opportunity for palliative care Research
 Opportunity for palliative care Research Role of Radiotherapy in Multidisciplinary Management of Rectal Cancers Dr Sushmita Pathy Associate Professor Department of Radiation Oncology Dr BRA Institute Rotary
Opportunity for palliative care Research Role of Radiotherapy in Multidisciplinary Management of Rectal Cancers Dr Sushmita Pathy Associate Professor Department of Radiation Oncology Dr BRA Institute Rotary
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic
 Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Pancreatic Cancer and Radiation Therapy
 Pancreatic Cancer and Radiation Therapy Why? Is there a role for local therapy with radiation in a disease with such a high rate of distant metastases? When? Resectable Disease Is there a role for post-op
Pancreatic Cancer and Radiation Therapy Why? Is there a role for local therapy with radiation in a disease with such a high rate of distant metastases? When? Resectable Disease Is there a role for post-op
Case Scenario year-old white male presented to personal physician with dyspepsia with reflux.
 Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors
 Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors Frédéric Bibeau, MD, PhD Pathology department Biopathology unit Institut du Cancer de Montpellier France Quality
Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors Frédéric Bibeau, MD, PhD Pathology department Biopathology unit Institut du Cancer de Montpellier France Quality
Alison Douglass Gillian Lieberman, MD. November. Colon Cancer. Alison Douglass, Harvard Medical School Year III Gillian Lieberman, MD
 November Colon Cancer Alison Douglass, Harvard Medical School Year III Our Patient Mr. K. is a 67 year old man with no prior medical problems other than hemorrhoids which have caused occasional rectal
November Colon Cancer Alison Douglass, Harvard Medical School Year III Our Patient Mr. K. is a 67 year old man with no prior medical problems other than hemorrhoids which have caused occasional rectal
Rob Glynne-Jones Mount Vernon Cancer Centre
 ESMO Preceptorship Programme Colorectal Cancer Barcelona October 2017 State of the art: Radio- /chemotherapy for rectal cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures: last 5 years Speaker:
ESMO Preceptorship Programme Colorectal Cancer Barcelona October 2017 State of the art: Radio- /chemotherapy for rectal cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures: last 5 years Speaker:
Rectal Cancer Cookbook Update. A. JOURET-MOURIN with the collaboration of A Hoorens,P Demetter, G De Hertogh,C Cuvelier and C Sempoux
 Rectal Cancer Cookbook Update A. JOURET-MOURIN with the collaboration of A Hoorens,P Demetter, G De Hertogh,C Cuvelier and C Sempoux Prof Dr A Jouret-Mourin, Department of Pathology, UCL, St Luc, Brussels
Rectal Cancer Cookbook Update A. JOURET-MOURIN with the collaboration of A Hoorens,P Demetter, G De Hertogh,C Cuvelier and C Sempoux Prof Dr A Jouret-Mourin, Department of Pathology, UCL, St Luc, Brussels
CREATE Trial Proposal: Survey of current practice and potential trial participation
 CREATE Trial Proposal: Survey of current practice and potential trial participation Approximately a quarter of newly diagnosed rectal cancer patients have features on pre-treatment pelvic MRI indicating
CREATE Trial Proposal: Survey of current practice and potential trial participation Approximately a quarter of newly diagnosed rectal cancer patients have features on pre-treatment pelvic MRI indicating
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer
 Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer
 Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Advances in Imaging Technology In The Management of Colorectal Cancer
 Advances in Imaging Technology In The Management of Colorectal Cancer Dushyant Sahani, M.D Director of CT Associate Professor Department of Radiology Massachusetts General Hospital Harvard Medical School
Advances in Imaging Technology In The Management of Colorectal Cancer Dushyant Sahani, M.D Director of CT Associate Professor Department of Radiology Massachusetts General Hospital Harvard Medical School
4/22/2010. Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey.
 Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
16/09/2015. ACOSOG Z011 changing practice. Presentation outline. Nodal mets #1 prognostic tool. Less surgery no change in oncologic outcomes
 ACOSOG Z011 changing practice The end of axillary US/FNA? Preoperative staging of the axilla in the era of Z011 Adena S Scheer MD MSc FRCSC Surgical Oncologist, St. Michael s Hospital Assistant Professor,
ACOSOG Z011 changing practice The end of axillary US/FNA? Preoperative staging of the axilla in the era of Z011 Adena S Scheer MD MSc FRCSC Surgical Oncologist, St. Michael s Hospital Assistant Professor,
The role of chemoradiotherapy in GE junction and gastric cancer. Karin Haustermans
 The role of chemoradiotherapy in GE junction and gastric cancer Karin Haustermans Overview Postoperative chemoradiotherapy Preoperative chemoradiotherapy Palliative radiation Technical aspects Overview
The role of chemoradiotherapy in GE junction and gastric cancer Karin Haustermans Overview Postoperative chemoradiotherapy Preoperative chemoradiotherapy Palliative radiation Technical aspects Overview
MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER
 10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
SMALL BOWEL ADENOCARCINOMA. Dr. C. Jeske
 SMALL BOWEL ADENOCARCINOMA Dr. C. Jeske Case presentation 54 year old female. Presents with OJ and weight loss. Abdominal examination only reveals a palpable gallbladder. ERCP reveals a circumferential
SMALL BOWEL ADENOCARCINOMA Dr. C. Jeske Case presentation 54 year old female. Presents with OJ and weight loss. Abdominal examination only reveals a palpable gallbladder. ERCP reveals a circumferential
Controversies in Breast Pathology ELENA PROVENZANO ADDENBROOKES HOSPITAL, CAMBRIDGE
 Controversies in Breast Pathology ELENA PROVENZANO ADDENBROOKES HOSPITAL, CAMBRIDGE Neoadjuvant Chemotherapy Indications: Management of locally advanced invasive breast cancers including inflammatory breast
Controversies in Breast Pathology ELENA PROVENZANO ADDENBROOKES HOSPITAL, CAMBRIDGE Neoadjuvant Chemotherapy Indications: Management of locally advanced invasive breast cancers including inflammatory breast
Breast Surgery When Less is More and More is Less. E MacIntosh, MD June 6, 2015
 Breast Surgery When Less is More and More is Less E MacIntosh, MD June 6, 2015 Presenter Disclosure Faculty: E. MacIntosh Relationships with commercial interests: None Mitigating Potential Bias Not applicable
Breast Surgery When Less is More and More is Less E MacIntosh, MD June 6, 2015 Presenter Disclosure Faculty: E. MacIntosh Relationships with commercial interests: None Mitigating Potential Bias Not applicable
11/09/2014. Update Management of Rectal Cancer. Outline. I have no disclosures
 Update Management of Rectal Cancer June 7, 2014 W. Donald Buie MD,MSc, FRCSC Associate Professor of Surgery University of Calgary I have no disclosures Outline Pre-operative staging Who needs neoadjuvant
Update Management of Rectal Cancer June 7, 2014 W. Donald Buie MD,MSc, FRCSC Associate Professor of Surgery University of Calgary I have no disclosures Outline Pre-operative staging Who needs neoadjuvant
Gastric Cancer Staging AJCC eighth edition. Duncan McLeod Westmead Hospital, NSW
 Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
Oral cavity cancer Post-operative treatment
 Oral cavity cancer Post-operative treatment Dr. Christos CHRISTOPOULOS Radiation Oncologist Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Important issues RT -techniques Patient selection
Oral cavity cancer Post-operative treatment Dr. Christos CHRISTOPOULOS Radiation Oncologist Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Important issues RT -techniques Patient selection
Innovations in Rectal Cancer Surgery
 Innovations in Rectal Cancer Surgery A. D Hoore MD PhD, EBSQ-CR, (hon)fascrs A. Wolthuis MD PhD, EBSQ-CR, FACS G. Bislenghi MD Departement of Abdominal Surgery University Hospitals Leuven, Belgium invasiveness
Innovations in Rectal Cancer Surgery A. D Hoore MD PhD, EBSQ-CR, (hon)fascrs A. Wolthuis MD PhD, EBSQ-CR, FACS G. Bislenghi MD Departement of Abdominal Surgery University Hospitals Leuven, Belgium invasiveness
Loco-Regional Management After Neoadjuvant Chemotherapy
 1 Loco-Regional Management After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
1 Loco-Regional Management After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
Prostate Case Scenario 1
 Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
Pre- Versus Post-operative Radiotherapy
 Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Introduction. Approximately 40,000 patients are diagnosed with rectal. Original Article
 Original Article Does a fine line exist between regional and metastatic pelvic lymph nodes in rectal cancer striking discordance between national guidelines and treatment recommendations by US radiation
Original Article Does a fine line exist between regional and metastatic pelvic lymph nodes in rectal cancer striking discordance between national guidelines and treatment recommendations by US radiation
[A RESEARCH COORDINATOR S GUIDE]
![[A RESEARCH COORDINATOR S GUIDE]](/thumbs/88/117127924.jpg "[A RESEARCH COORDINATOR S GUIDE]") 2013 COLORECTAL SURGERY GROUP Dr. Carl J. Brown Dr. Ahmer A. Karimuddin Dr. P. Terry Phang Dr. Manoj J. Raval Authored by Jennifer Lee A cartoon about colonoscopies. 1 [A RESEARCH COORDINATOR S GUIDE]
2013 COLORECTAL SURGERY GROUP Dr. Carl J. Brown Dr. Ahmer A. Karimuddin Dr. P. Terry Phang Dr. Manoj J. Raval Authored by Jennifer Lee A cartoon about colonoscopies. 1 [A RESEARCH COORDINATOR S GUIDE]
Laparoscopic Resection Of Colon & Rectal Cancers. R Sim Centre for Advanced Laparoscopic Surgery, TTSH
 Laparoscopic Resection Of Colon & Rectal Cancers R Sim Centre for Advanced Laparoscopic Surgery, TTSH Feasibility and safety Adequacy - same radical surgery as open op. Efficacy short term benefits and
Laparoscopic Resection Of Colon & Rectal Cancers R Sim Centre for Advanced Laparoscopic Surgery, TTSH Feasibility and safety Adequacy - same radical surgery as open op. Efficacy short term benefits and
Diagnosis and management of retroperitoneal sarcoma
 SON Update 2017 Diagnosis and management of retroperitoneal sarcoma Andrea J MacNeill, MD MSc FRCSC Surgical Oncologist, BC Cancer Agency Vancouver 2 Histologic Subtypes of STS 3 RP Subtypes (n=684) Extremity
SON Update 2017 Diagnosis and management of retroperitoneal sarcoma Andrea J MacNeill, MD MSc FRCSC Surgical Oncologist, BC Cancer Agency Vancouver 2 Histologic Subtypes of STS 3 RP Subtypes (n=684) Extremity
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
Modalities of Radiation
 Modalities of Radiation Superficial radiotherapy Orthovoltage Megavoltage Photons Electrons Brachytherapy Interstitial Moulds When to refer? The vast majority of skin cancers will be managed without any
Modalities of Radiation Superficial radiotherapy Orthovoltage Megavoltage Photons Electrons Brachytherapy Interstitial Moulds When to refer? The vast majority of skin cancers will be managed without any
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma
 Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
malignant polyp Daily Challenges in Digestive Endoscopy for Endoscopists and Endoscopy Nurses BSGIE Annual Meeting 18/09/2014 Mechelen
 Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Neoadjuvant treatment Evolution and Current Status
 Neoadjuvant treatment Evolution and Current Status Dr Andrew See Radiation Oncologist 2017 Rectal Cancer Symposium Friday 10 th November 2017 2 1 Major Randomised Trials Supporting Neoadjuvant CRT Trial
Neoadjuvant treatment Evolution and Current Status Dr Andrew See Radiation Oncologist 2017 Rectal Cancer Symposium Friday 10 th November 2017 2 1 Major Randomised Trials Supporting Neoadjuvant CRT Trial
EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013
 EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013 Head and Neck Coding and Staging Head and Neck Coding and Staging Anatomy & Primary Site Sequencing and MPH
EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013 Head and Neck Coding and Staging Head and Neck Coding and Staging Anatomy & Primary Site Sequencing and MPH
Surgical Management of Pancreatic Cancer
 I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
The Role Of The Post-CRT MRI In Assessing Response
 Low Rectal Cancer: Is It Safe To Change The Plane Of Surgery? The Role Of The Post-CRT MRI In Assessing Response Nick Battersby, Mit Dattani, Nick West, Graham Branagan, Mark Gudgeon, Phil Quirke, Paris
Low Rectal Cancer: Is It Safe To Change The Plane Of Surgery? The Role Of The Post-CRT MRI In Assessing Response Nick Battersby, Mit Dattani, Nick West, Graham Branagan, Mark Gudgeon, Phil Quirke, Paris
Loco-Regional Management After Neoadjuvant Chemotherapy
 1 Loco-Regional Management After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
1 Loco-Regional Management After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
Esophageal cancer: Biology, natural history, staging and therapeutic options
 EGEUS 2nd Meeting Esophageal cancer: Biology, natural history, staging and therapeutic options Michael Bau Mortensen MD, Ph.D. Associate Professor of Surgery Centre for Surgical Ultrasound, Upper GI Section,
EGEUS 2nd Meeting Esophageal cancer: Biology, natural history, staging and therapeutic options Michael Bau Mortensen MD, Ph.D. Associate Professor of Surgery Centre for Surgical Ultrasound, Upper GI Section,
State-of-the-art of surgery for resectable primary tumors
 Early colorectal cancer State-of-the-art of surgery for resectable primary tumors (Special focus on rectal cancer surgery) Stefan Heinrich & Hauke Lang Department of General, Visceral and University Hospital
Early colorectal cancer State-of-the-art of surgery for resectable primary tumors (Special focus on rectal cancer surgery) Stefan Heinrich & Hauke Lang Department of General, Visceral and University Hospital
Index. Surg Oncol Clin N Am 16 (2007) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Index. Surg Oncol Clin N Am 14 (2005) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease
 Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease Jennifer E. Tseng, MD UFHealth Cancer Center-Orlando Health Sep 12, 2014 Background Approximately
Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease Jennifer E. Tseng, MD UFHealth Cancer Center-Orlando Health Sep 12, 2014 Background Approximately