Management of Retroperitoneal Sarcomas
|
|
|
- Prudence Wood
- 5 years ago
- Views:
Transcription
1 Management of Retroperitoneal Sarcomas Giorgos C. Karakousis, M.D. Division of Endocrine and Oncologic Surgery Department of Surgery University of Pennsylvania School of Medicine
2 Sarcomas General Background Rare tumors accounting for approximately 1% of malignancies in adults; 15% pediatric population Over 50 different histologic subtypes Approximately 50% occur in extremities Most common histologic subtype in adults in liposarcoma Staging is TNGM Stage I: localized low grade tumors; Stage II: localized intermediate grade tumors or high grade tumors small and superficial; Stage III: high grade > 5 cm; Stage IV metastatic disease
3 Sarcomas General Background Core biopsies are reasonable for extremity sarcomas over 2 cm Larger extremity sarcomas can be biopsied with incisional biopsy (longitudinal) Pre-operative evaluation includes cross-sectional imaging and chest imaging (CT scan for higher risk lesions) Most common histologic subtype in adults in liposarcoma Mainstay of treatment is surgical
4 Background Rare tumors accounting for <1% of solid malignancies ( %/100,000 incidence in population) Peak incidence in the 5 th decade of life Account for about 10-20% of sarcomas by location Most common histologic subtypes historically have been liposarcoma, MFH*, and leiomyosarcomas, although many MFH histologies are being reclassified Frequently, these tumors present late or are discovered incidentally Francis, Sondak et al. Cancer Imaging 2005; 5 (1): Mullinax et al. Cancer Control 2011; 18(3):
5 Presentation and diagnosis Often asymptomatic Patients may present with vague abdominal symptoms or abdominal and/or back pain Occasionally, patients may present with GI or ureteral obstructive symptoms, muscle wasting with increasing abdominal girth or palpable abdominal mass Cross-sectional imaging (CT/MRI) can identify the lesion and its anatomic relationship to other structures High resolution, thin-cut CT can usually differentiate between primary a primary visceral retroperitoneal tumor, metastatic lymphadenopathy and a suspected sarcoma
6 Differential Diagnosis Lymphoma Primary tumor of retroperitoneal organ (eg pancreas, renal, adrenal) Metastatic lymphadenopathy (including testicular origin) Clinical symptoms/signs may sometimes be helpful in distinguishing etiology
7 Role of Biopsy Generally, percutaneous pre-operative biopsy is not recommended in patients with suspected retroperitoneal sarcomas (concern for peritoneal seeding) Indications for biopsy would include 1) patients with radiologic findings more suspicious for lymphoma 2) patients in which consideration is given to for pre-op systemic therapy or radiotherapy

8 Contraindications to biopsy Paragangliomas may look like lymphadenopathy and can release catecholamines with biopsy, and therefore biopsy should be avoided if suspected paraganglioma Courtesy of Dr. D.L. Fraker
9 Prognostic factors for RP sarcomas: Nomogram N=343 patients with resectable non-metastatic RP sarcomas (MD Anderson) Median f/u: 50 months Median survival: 59 mo Anaya, Pollock et al. Ann Oncology 2010; 21:
 Median f/u 55 months Ardoino, Gronchi et al.")
10 Prognostic factors: Nomogram N=192 patients with resectable non-metastatic RP sarcomas (Milan, Italy) Median f/u 55 months Ardoino, Gronchi et al. Cancer 2010; 116:
11 Prognostic factors for RP Liposarcomas N=801 patients with resectable non-metastatic liposarcomas (MSKCC) Median f/u 45 months Dalal, Singer et al. Ann Surg 2006; 244:
12 Prognosis: Impact of focality in RP sarcomas N=393 Unifocality associated with significantly improved survival compared to multifocality (31% versus 60% 5 yr survival) Well-differentiated histology (ALT) associated with improved survival > 7 lesions associated with poor prognosis Anaya, Pollock et al. Ann Surg 2009; 249 (1):
13 Treatment Surgery Radiation Therapy Systemic Therapy/Chemotherapy
 is recommended Most common organs resected en bloc with specimen (kidney, colon, distal pancreas/spleen) Less commonly resected organs/structures (aorta/iliac")
14 Surgery Surgery when feasible remains the mainstay of curative treatment in patients with retroperitoneal sarcomas Gross resection of the tumor with negative margins (with resection of adjacent involved structures when feasible) is recommended Most common organs resected en bloc with specimen (kidney, colon, distal pancreas/spleen) Less commonly resected organs/structures (aorta/iliac arteries; IVC for primary IVC sarcomas)
15 Surgery N=200 patients with retroperitoneal sarcomas ( ) from Royal Marsden Complete resection in 170 patients (85%) Adjacent organ resection in N=126 patients (63%) or 75% with complete resection (36% kidney, 22% colon, 14% spleen) Post-operative mortality 3% Strauss, Thomas et al. Br J Surg 2010; 97 (5):
16 Surgery- Royal Marsden Study Strauss, Thomas et al. Br J Surg 2010; 97 (5):


17 Surgery: Role of compartment resection N=382 patients from the French sarcoma group 3 and 5-year survival was 66% and 57% respectively Median survival 6 years 120 patient underwent compartment resection beyond standard resection of gross tumor with adjacent organs Bonvalot et al. JCO 2009; 27 (1): 31-7.

18 Surgery: Role of compartment resection 3 year recurrence rate of 10% versus 50% with standard procedures; no difference in overall survival Bonvalot et al. JCO 2009; 27 (1): 31-7.
19 Compartment resection for RP sarcoma-controversy Value of compartment resection questioned because: Inherent selection bias in which patients can undergo a compartment resection (anatomic limitations eg sarcomas near the aorta or spine) No overall survival benefit observed although compartment resection associated with decreased local recurrence rate Surgeries performed over a long time period introducing potential other confounding variables in different technique methodologies Morbidity/mortality not insignificant: 16% surgical morbidity (50% of those requiring re-operation; mortality 4%) in Bonvalot study
20 Surgery-Impact of High Volume Centers on Outcome N=4205 cases Florida Cancer Data System ( ) Included soft tissue sarcomas from various locations Guitierrez et al. Ann Surg 2007; 245:
21 Surgery-Impact of High Volume Centers on Outcome Low volume center found to be negative independent prognostic factor for survival in patients undergoing surgery for soft tissue sarcomas Guitierrez et al. Ann Surg 2007; 245:

22 Case presentation 55 year male with increasing abdominal girth for 2 years Advised by primary care physician to go on diet; continued to lose muscle mass despite increasing abdominal girth Admitted urgently from clinic with dyspnea from diaphragmatic compression
 Massive retroperitoneal")
23 Case presentation: Retroperitoneal liposarcoma Large retroperitoneal sarcoma extending from the liver to the pelvis displacing right sided structures to the midline R kidney (not visualized in nearly midline location with right renal artery nearly vertical (from posterior to anterior) Massive retroperitoneal sarcoma


24 Case presentation Removed with en bloc with right nephrectomy Specimen weighed 18.2 kg Final Pathology: 48 cm dedifferentiated liposarcoma 3 months post-op

25 Case presentation # 2 75 M presented with urinary retention Cross-sectional imaging revealed a large pelvic mass (17 cm) involving the prostate and seminal vesicles Compression of the distal R ureter with R hydronephrosis Invasion of the bladder base



26 Case presentation # 2 Removed en bloc with prostate and bladder Ileal conduit diversion performed Malignant SFT 23.4 cm (resection margins negative)
27 Treatment Surgery Radiation Therapy Systemic Therapy/Chemotherapy
28 Radiotherapy No Level I data on value of radiation therapy in retroperitoneal sarcomas so data largely extrapolated from studies with extremity sarcomas The benefit of XRT on survival in sarcomas has not been shown Decision for pre-operative versus post-operative therapy should consider resectability of tumor keeping in mind however no benefit of survival shown in studies with neo-adjuvant versus adjuvant XRT in patients with sarcoma, but higher incidence of wound complications in the neo-adjuvant group Special consideration must be given to radiotherapy (lower doses) compared to extremity soft-tissue sarcomas because of potential toxicity to adjacent organs (bowel) Mullinax et al. Cancer Control 2011; 18(3):
29 Radiotherapy-Rationale for pre-operative therapy Smaller radiation field when tumor is in situ Tumor serves as a tissue expander thereby displacing viscera and minimizing toxicity to the bowel Tumor periphery is better oxygenated and therefore more radiosensitive
:")
30 Radiotherapy Mullinax et al. Cancer Control 2011; 18(3):
 IORT Post-op Median Survival (mo) 45 52")
31 Radiotherapy-RCT of intra vs. post-op XRT N=15 Intra-op XRT 20 Gy Post-op Gy N=35 patients with resected RP sarcomas N=20 No Intra-op XRT Post-op high dose XRT (50-55 GY) IORT Post-op Median Survival (mo) Loco-regional relapse 40% (6/15) 80% (16/20) Radiation enteritis 13% (2/15) 50% (10/20) Peripheral/femoral neuropathy 60% (9/15) 5% (1/20) Sindelar,Glatstein et al. Arch Surg 1993; 128 (4):
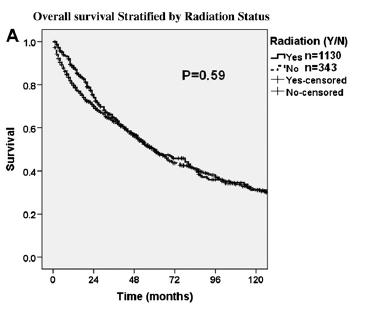
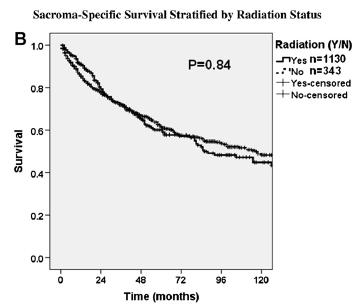
32 Radiotherapy-SEER analysis N=1535 patients from (SEER database) 373 patients (23.3%) received XRT Median survival 60 months for both patients receiving and not receiving XRT Tseng et al. Jour Surg Res 2011; 168:
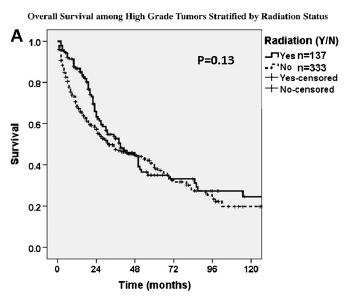
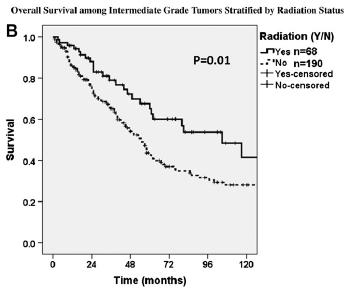
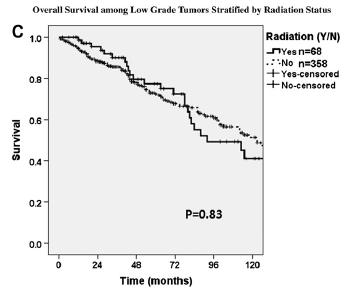
33 Radiotherapy-SEER analysis Overall Stratified by Grade High Low Intermediate Tseng et al. Jour Surg Res 2011; 168:


34 Radiotherapy-SEER analysis MFH Histology Tseng et al. Jour Surg Res 2011; 168:

35 Radiotherapy with Proton Beam Use of protons to deliver ionizing radiation Principal advantage is to provide more targeted treatment with less collateral toxicity Due to relatively large particle mass, protons have little lateral scatter and therefore can be used for more focused radiation; tissues also deeper to the planned treatment field also receive little radiation
: 1515-29")
36 Radiotherapy with Proton Beam N=28 patients treated with IMRT or proton therapy at Massachusetts General Hospital Yoon et al. Ann Surg Onc 2010; 17(6):

37 Radiotherapy with Proton Beam Roberts Proton Therapy at Penn Largest facility of its kind affiliated with academic center 5 treatment rooms Clinical protocol open for patients with RP sarcomas
38 Radiotherapy with Proton Beam Potential advantages of Proton therapy: Less radiation to normal tissue Treating tumors near critical organs (eg spinal cord) Ability to retreat tumors that have already been irradiated Clinical trial at University of Pennsylvania: First Phase: Safety and feasibility of the approach with protons Second phase: Use of proton therapy in the neoadjuvant and adjuvant setting
39 Treatment Surgery Radiation Therapy Systemic Therapy/Chemotherapy
40 Chemotherapy Response rates of approximately 25-25% for STS Most series report on use of doxorubicin based regimen (with or without ifosfamide) or with other combinations Meta-analysis of randomized trials comparing doxorubicin to doxorubicin with other chemotherapeutics show no statistically significant survival benefit but with increased adverse effect to the combination 1 More and more, there is increasing awareness of differential responsiveness of different histologic subtypes of sarcoma to various chemotherapeutics Bramwell et al. Sarcoma 2000; 4:
41 Systemic therapy by histologic subtype Histologic Subtype GIST Dermatofibrosarcoma Protuberans (DFSP) Angiosarcoma Leiomyosarcomas Alveolar soft part Systemic Agent Imatinib Imatinib Paclitaxel, sorafenib, pazopanib Gemcitabine VEGF inhibitors (cediranib or sunitinib)
 Blay et al.")
42 Adjuvant chemotherapy: Randomized controlled trials A few trials demonstrated improved overall survival (OS) with adjuvant chemotherapy HOWEVER, Meta-analysis of these trials showed significantly lower local or metastatic relapse rates but no significant difference in OS with adjuvant chemotherapy (4% at 10 years) Blay et al. Oncologist 2009; 14:

43 Chemotherapy Data include patients with extremity soft tissue sarcomas Little data in subgroup of patients with RP sarcomas Frustaci trial showed initially showed improved OS, with adjuvant chemotherapy for high risk extremity sarcomas but difference was lost with longer follow-up Mullinax et al. Cancer Control 2011; 18(3):
44 Adjuvant chemotherapy: EORTC trial European Organization for Research and Treatment of Cancer (EORTC 62931) Soft Tissue and Bone Sarcoma Group (STBSG) reported on largest adjuvant trial of chemotherapy (Dox+Ifos) for sarcoma at ASCO meeting in 2007 N=351 patients with localized (primary or local recurrence) with grade II (43%) or III Adjuvant XRT for microscopic residual disease, inadequate margins and local recurrence Patients randomized within 4 weeks of surgery This trial failed to demonstrate any significant difference in relapse-free or overall survival (69% OS control arm versus 64% in treatment arm) Woll et al. Proc A, Soc Clin Oncol 2007; 25 (3): 546s
45 Adjuvant chemotherapy: Pooled EORTC trials N=819 patients pooled from the two EORTC trials Median follow-up 8.2 years Large tumor size, histologic grade and R1 resection were independent negative prognostic factors for progression-free and overall survival Adjuvant chemotherapy was an independent prognostic factor for progression-free (PFS) but not overall survival (OS) Patients> 40 years had better PFS in adjuvant chemotherapy arm; adjuvant chemotherapy associated with marginally worse OS in patients <40 years Patients with R1 resection had better PFS and OS in adjuvant chemotherapy arm
46 Adjuvant Chemotherapy: Reasons for Failure Soft tissue sarcomas, because of their rarity, are frequently grouped together in clinical trials despite varying histology and tumor biology Surgical resection is variable depending upon the experience for the surgeons in various participating centers Patient factors (eg advanced age, gender) may influence responsiveness to chemotherapy; therefore sub-groups of patients who may benefit from systemic therapy may not be appreciated in unselected populations in clinical trials
47 New Therapies Olaratumab Trabectedin Eribulin Immune checkpoint inhibitors

48 Sarcomatosis Condition characterized by the presence of multiple sarcomas in the peritoneal cavity Frequently not amenable to surgical resection Poor overall prognosis with median survival of approximately 12 months

49 Sarcomatosis and HIPEC/IPEC Mullinax et al. Cancer Control 2011; 18(3):

50 Intraperitoneal chemotherapy for sarcomatosis-rct No difference in overall survival, local relapse free and metastasis free survival between IPEC+ and IPEC- groups No difference between visceral and RP sarcoma groups Morbidity 21% Bonvalot et al. Eur J Surg Onc 2005; 31:
51 IP chemotherapy for sarcomatosis: systematic review Median DFS 2.3 to 22 months Median survival 5.5 to 39.6 months Morbidity 9% to 44% Mortality 0% to 11% Data at present does not support the use of intraperitoneal chemo for sarcomatosis Munene, Temple et al. AnnSurg Onc 2011; 18:
52 Metastatectomy for RP sarcomas Extrapolating from extremity soft tissue sarcomas, metastatectomy is associated with improved outcomes with reported 5 year survival rates of 25-40% in selected patients from pulmonary metastatectomy Disease free interval, number of metastase, complete resection, and grade of primary tumor are all factors associated with better prognosis in metastatectomy Resection of liver metastases historically was associated with poor outcomes
53 Resection of hepatic metastases for sarcoma Recent literature reporting 5 year survival rates as high as 27-32% following resection of liver metastases Disease free interval, and size of metastases, histologic subtype have been shown to be negative prognostic factors Study results confounded by the inclusion of GIST tumors for which imatinib therapy has significantly impacted on outcomes Marudanayagam et al. Eur J Surg Onc 2011; 37: Zacherl et al. Langenbecks Arch Surg 2011; 396:

54 Primary Tumors of the IVC (Leiomyosarcomas) Arise from the smooth muscle cells of the vena cava Frequently slow growing Frequently limited to the vena cava and can grow intra-or extraluminally :


55 Case Presentation #3: IVC tumor 75 M presented with leg swelling after a boating accident Initially felt to have thrombus in IVC MRI showed enhancement of the lesion suggesting primary IVC sarcoma
56 Case Presentation #3: IVC tumor Patient placed on veno-veno bypass Vena cava resected with R nephrectomy (tumor was invading into right renal vein) Homograft was used to reconstruct the IVC (vascular surgery) Final pathology: 4.3 cm high grade leiomyosarcoma
57 IVC tumors: extent of local resection 120 patients were analyzed in the International Registry of IVC leiomyosarcomas 44% went caval rim resection and 56% underwent segmental caval resection No difference in local or distant metastases or overall survival between the two groups with varying degree of resection 57.3% patients recurred at a median follow-up of 32 months Mortality 2.5% and morbidity 5.8% Mingoli et al. Anticancer research 2011; 17:
58 IVC (Leiomyosarcomas) Recent study suggest IVC caval resection may frequently not be necessary; transient lower extremity edema observed (50%) with no long term sequelae Role of preoperative XRT? Daylami et al. JACS 2011; 210:
59 IVC (Leiomyosarcomas) These tumors should be resected with margin negative resection More extensive caval resections do not appear necessary and may increase the morbidity Caval reconstruction may frequently be avoided with few long-term sequelae
60 Final conclusions Diagnosis of retroperitoneal sarcomas should generally be made on radiographic findings and biopsy should be avoided Complete surgical resection with gross negative margins remains the mainstay of treatment Data for neoadjuvant systemic therapy (chemotherapy) are limited No substantial data to support the routine use of adjuvant doxorubicin based chemotherapy after resection Future systemic therapy trials should acknowledge the tremendous variability among different histologic subtypes
61 Conclusions No level I evidence for the use of radiotherapy for RP sarcomas extrapolation can be made from extremity sarcoma studies Recurrent disease should be managed surgically when feasible with intent of negative margin resection or palliation (when complete resection not feasible), taking into account factors such as location and number of recurrences, disease free interval, tumor grade and patient factors
62 Conclusions Sarcomatosis carries a poor prognosis; cytoreductive surgery may be indicated in selected patients; Intraperitoneal/Chemotherapy/HIPEC does not appear to improve outcomes Sarcoma surgery should be managed at high volume centers by experienced surgeons Primary IVC caval tumors present unique challenges; limited caval resection with negative margin is recommended reconstruction may often be avoided

63 Thank you for your attention
Multidisciplinary management of retroperitoneal sarcomas
 Multidisciplinary management of retroperitoneal sarcomas Eric K. Nakakura, MD UCSF Department of Surgery UCSF Comprehensive Cancer Center San Francisco, CA 7 th Annual Clinical Cancer Update North Lake
Multidisciplinary management of retroperitoneal sarcomas Eric K. Nakakura, MD UCSF Department of Surgery UCSF Comprehensive Cancer Center San Francisco, CA 7 th Annual Clinical Cancer Update North Lake
INTRAOPERATIVE RADIATION THERAPY FOR RETROPERITONEAL SARCOMA
 INTRAOPERATIVE RADIATION THERAPY FOR RETROPERITONEAL SARCOMA ISIORT 2014 Ivy A Petersen, MD Mayo Clinic Rochester, MN NOTHING TO DISCLOSE SOFT TISSUE SARCOMAS 2014 Estimated cases in the USA 12,020 diagnosed
INTRAOPERATIVE RADIATION THERAPY FOR RETROPERITONEAL SARCOMA ISIORT 2014 Ivy A Petersen, MD Mayo Clinic Rochester, MN NOTHING TO DISCLOSE SOFT TISSUE SARCOMAS 2014 Estimated cases in the USA 12,020 diagnosed
Update on Sarcomas of the Head and Neck. Kevin Harrington
 Update on Sarcomas of the Head and Neck Kevin Harrington Overview Classification and incidence of sarcomas Clinical presentation Challenges to treatment Management approaches Prognostic factors Radiation-induced
Update on Sarcomas of the Head and Neck Kevin Harrington Overview Classification and incidence of sarcomas Clinical presentation Challenges to treatment Management approaches Prognostic factors Radiation-induced
Surgical strategies to improve results in retroperitoneal sarcoma. Christoph Kettelhack University Hospital Basel
 Surgical strategies to improve results in retroperitoneal sarcoma Christoph Kettelhack University Hospital Basel Retroperitoneal Sarcoma General considerations Advanced tumor stage Complex anatomy Absence
Surgical strategies to improve results in retroperitoneal sarcoma Christoph Kettelhack University Hospital Basel Retroperitoneal Sarcoma General considerations Advanced tumor stage Complex anatomy Absence
Diagnosis and management of retroperitoneal sarcoma
 SON Update 2017 Diagnosis and management of retroperitoneal sarcoma Andrea J MacNeill, MD MSc FRCSC Surgical Oncologist, BC Cancer Agency Vancouver 2 Histologic Subtypes of STS 3 RP Subtypes (n=684) Extremity
SON Update 2017 Diagnosis and management of retroperitoneal sarcoma Andrea J MacNeill, MD MSc FRCSC Surgical Oncologist, BC Cancer Agency Vancouver 2 Histologic Subtypes of STS 3 RP Subtypes (n=684) Extremity
Leiomyosarcoma of the inferior vena cava: 1 case. B. Bancel, A. Rode, C. Ducerf. Hôpital CROIX ROUSSE LYON. Case report
 Leiomyosarcoma of the inferior vena cava: 1 case B. Bancel, A. Rode, C. Ducerf Hôpital CROIX ROUSSE LYON Bucharest Nov 2011 Case report 34 yr-old woman, no antecedent Sept 2004: Abdominal upper right quadrant
Leiomyosarcoma of the inferior vena cava: 1 case B. Bancel, A. Rode, C. Ducerf Hôpital CROIX ROUSSE LYON Bucharest Nov 2011 Case report 34 yr-old woman, no antecedent Sept 2004: Abdominal upper right quadrant
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Ablative therapy, nonsurgical, for pulmonary metastases of soft tissue sarcoma, 279 280 Adipocytic tumors, atypical lipomatous tumor vs. well-differentiated
Note: Page numbers of article titles are in boldface type. A Ablative therapy, nonsurgical, for pulmonary metastases of soft tissue sarcoma, 279 280 Adipocytic tumors, atypical lipomatous tumor vs. well-differentiated
MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER
 10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
Wilms Tumor and Neuroblastoma
 Wilms Tumor and Neuroblastoma Wilm s Tumor AKA: Nephroblastoma the most common intra-abdominal cancer in children. peak incidence is 2 to 3 years of age Biology somatic mutations restricted to tumor tissue
Wilms Tumor and Neuroblastoma Wilm s Tumor AKA: Nephroblastoma the most common intra-abdominal cancer in children. peak incidence is 2 to 3 years of age Biology somatic mutations restricted to tumor tissue
Soft Tissue Sarcoma. Presley Regional Trauma Center Department of Surgery University of Tennessee Health Science Center Memphis, Tennessee
 Soft Tissue Sarcoma Presley Regional Trauma Center Department of Surgery University of Tennessee Health Science Center Memphis, Tennessee Soft Tissue Sarcoma Collective term for an unusual and diverse
Soft Tissue Sarcoma Presley Regional Trauma Center Department of Surgery University of Tennessee Health Science Center Memphis, Tennessee Soft Tissue Sarcoma Collective term for an unusual and diverse
Radiation Therapy for Soft Tissue Sarcomas
 Radiation Therapy for Soft Tissue Sarcomas Alexander R. Gottschalk, MD, PhD Assistant Professor, Radiation Oncology University of California, San Francisco 1/25/08 NCI: limb salvage vs. amputation 43 patients
Radiation Therapy for Soft Tissue Sarcomas Alexander R. Gottschalk, MD, PhD Assistant Professor, Radiation Oncology University of California, San Francisco 1/25/08 NCI: limb salvage vs. amputation 43 patients
Case Presentation. Gordon Callender M.D. Surgical Resident
 Case Presentation Gordon Callender M.D. Surgical Resident Retroperitoneal Sarcomas Sarcomas Heterogeneous group of rare tumors that arise predominantly from the embryonic mesoderm. Expected incidence for
Case Presentation Gordon Callender M.D. Surgical Resident Retroperitoneal Sarcomas Sarcomas Heterogeneous group of rare tumors that arise predominantly from the embryonic mesoderm. Expected incidence for
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R
 Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
Sacral Chordoma: The Loma Linda University Radiation Medicine Experience. Kevin Yiee MD, MPH Resident Physician
 Sacral Chordoma: The Loma Linda University Radiation Medicine Experience Kevin Yiee MD, MPH Resident Physician What is a chordoma? 1 st chordoma discovered in clivus by Virchow and Luschka 1856 Rare tumor
Sacral Chordoma: The Loma Linda University Radiation Medicine Experience Kevin Yiee MD, MPH Resident Physician What is a chordoma? 1 st chordoma discovered in clivus by Virchow and Luschka 1856 Rare tumor
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
When to Integrate Surgery for Metatstatic Urothelial Cancers
 When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
is time consuming and expensive. An intra-operative assessment is not going to be helpful if there is no more tissue that can be taken to improve the
 My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
Trimodality Therapy for Muscle Invasive Bladder Cancer
 Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Patient Selection for Surgery in RCC with Thrombus. E. Jason Abel, M.D.
 Patient Selection for Surgery in RCC with Thrombus E. Jason Abel, M.D. RCC with venous invasion Venous invasion occurs in ~10% of RCC Surgery more complex Increased risk for morbidity Thrombus may be confined
Patient Selection for Surgery in RCC with Thrombus E. Jason Abel, M.D. RCC with venous invasion Venous invasion occurs in ~10% of RCC Surgery more complex Increased risk for morbidity Thrombus may be confined
Surgical outcome and patterns of recurrence for retroperitoneal sarcoma at a single centre
 ONCOLOGY Ann R Coll Surg Engl 2016; 98: 192 197 doi 10.1308/rcsann.2016.0057 Surgical outcome and patterns of recurrence for retroperitoneal sarcoma at a single centre HDJ Hogg 1, DM Manas 1, D Lee 1,
ONCOLOGY Ann R Coll Surg Engl 2016; 98: 192 197 doi 10.1308/rcsann.2016.0057 Surgical outcome and patterns of recurrence for retroperitoneal sarcoma at a single centre HDJ Hogg 1, DM Manas 1, D Lee 1,
Multidisciplinary approach for renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute
 Multidisciplinary approach for renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute 20 April, Antalya, Turkey RCC European Union 60.000 new diagnoses/year 26.000 Cancer related deaths
Multidisciplinary approach for renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute 20 April, Antalya, Turkey RCC European Union 60.000 new diagnoses/year 26.000 Cancer related deaths
Pancreatic Cancer and Radiation Therapy
 Pancreatic Cancer and Radiation Therapy Why? Is there a role for local therapy with radiation in a disease with such a high rate of distant metastases? When? Resectable Disease Is there a role for post-op
Pancreatic Cancer and Radiation Therapy Why? Is there a role for local therapy with radiation in a disease with such a high rate of distant metastases? When? Resectable Disease Is there a role for post-op
1/25/13 Right partial nephrectomy followed by completion right radical nephrectomy.
 History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease
 Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
Effective local and systemic therapy is necessary for the cure of Ewing tumor Most chemotherapy regimens are a combination of cyclophosphamide,
 Ewing Tumor Perez Ewing tumor is the second most common primary tumor of bone in childhood, and also occurs in soft tissues Ewing tumor is uncommon before 8 years of age and after 25 years of age In the
Ewing Tumor Perez Ewing tumor is the second most common primary tumor of bone in childhood, and also occurs in soft tissues Ewing tumor is uncommon before 8 years of age and after 25 years of age In the
RETROPERITONEAL SARCOMA
 Basrah Journal Of Surgery Bas J Surg, March, 17, 2011 RETROPERITONEAL SARCOMA Review Article with Case Report MBChB, FRCSEd, FRACS, FACS, Gastrointestinal and General Surgeon, Tauranga Hospital, Tauranga,
Basrah Journal Of Surgery Bas J Surg, March, 17, 2011 RETROPERITONEAL SARCOMA Review Article with Case Report MBChB, FRCSEd, FRACS, FACS, Gastrointestinal and General Surgeon, Tauranga Hospital, Tauranga,
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER
 MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
Case Conference. Craig Morgenthal Department of Surgery Long Island College Hospital
 Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Prof. Dr. Aydın ÖZSARAN
 Prof. Dr. Aydın ÖZSARAN Adenocarcinomas of the endometrium Most common gynecologic malignancy in developed countries Second most common in developing countries. Adenocarcinomas, grade 1 and 2 endometrioid
Prof. Dr. Aydın ÖZSARAN Adenocarcinomas of the endometrium Most common gynecologic malignancy in developed countries Second most common in developing countries. Adenocarcinomas, grade 1 and 2 endometrioid
Index. Surg Oncol Clin N Am 14 (2005) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress?
 Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Managing adult soft tissue sarcomas and gastrointestinal stromal tumours
 Managing adult soft tissue sarcomas and gastrointestinal stromal tumours Sarcomas and gastrointestinal stromal tumours include a wide variety of biologically diverse cancers, many of them very rare. Paolo
Managing adult soft tissue sarcomas and gastrointestinal stromal tumours Sarcomas and gastrointestinal stromal tumours include a wide variety of biologically diverse cancers, many of them very rare. Paolo
Adjuvant Therapies in Endometrial Cancer. Emma Hudson
 Adjuvant Therapies in Endometrial Cancer Emma Hudson Endometrial Cancer Most common gynaecological cancer Incidence increasing in Western world 1-2% cancer deaths 75% patients postmenopausal 97% epithelial
Adjuvant Therapies in Endometrial Cancer Emma Hudson Endometrial Cancer Most common gynaecological cancer Incidence increasing in Western world 1-2% cancer deaths 75% patients postmenopausal 97% epithelial
Advances in radiation oncology in the management of soft tissue sarcoma 放疗于治疗肉瘤的最新发展
 Advances in radiation oncology in the management of soft tissue sarcoma 放疗于治疗肉瘤的最新发展 Brian O Sullivan Bartley-Smith / Wharton Chair Professor, Department of Radiation Oncology The Princess Margaret / University
Advances in radiation oncology in the management of soft tissue sarcoma 放疗于治疗肉瘤的最新发展 Brian O Sullivan Bartley-Smith / Wharton Chair Professor, Department of Radiation Oncology The Princess Margaret / University
Bladder Cancer Guidelines
 Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Cancer is a group of more than 100 different diseases that are characterized by uncontrolled cellular growth,
BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Cancer is a group of more than 100 different diseases that are characterized by uncontrolled cellular growth,
Pan Arab Journal of Oncology
 Pan Arab Journal of Oncology Original Article Retrospective Analysis of Clinicopathologic and Management Aspects of Soft Tissue Sarcoma Tarek Hussein Kamel, Azza Mohamed Adel, Reham Mohamed Faheim, Rana
Pan Arab Journal of Oncology Original Article Retrospective Analysis of Clinicopathologic and Management Aspects of Soft Tissue Sarcoma Tarek Hussein Kamel, Azza Mohamed Adel, Reham Mohamed Faheim, Rana
Winship Cancer Institute of Emory University Optimizing First Line Treatment of Advanced Ovarian Cancer
 Winship Cancer Institute of Emory University Optimizing First Line Treatment of Advanced Ovarian Cancer Ira R. Horowitz, MD, SM, FACOG, FACS John D. Thompson Professor and Chairman Department of Gynecology
Winship Cancer Institute of Emory University Optimizing First Line Treatment of Advanced Ovarian Cancer Ira R. Horowitz, MD, SM, FACOG, FACS John D. Thompson Professor and Chairman Department of Gynecology
Gastrointestinal Stromal Tumor Case Presentations
 Gastrointestinal Stromal Tumor Case Presentations Ricardo J. Gonzalez, MD Professor of Surgery Chair, Sarcoma Department Chief of Surgery Moffitt Cancer Center Patient number 1 64 yo male with upper abdominal
Gastrointestinal Stromal Tumor Case Presentations Ricardo J. Gonzalez, MD Professor of Surgery Chair, Sarcoma Department Chief of Surgery Moffitt Cancer Center Patient number 1 64 yo male with upper abdominal
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic
 Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Surgical Management of Pancreatic Cancer
 I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
Printed by Maria Chen on 3/11/2012 5:46:52 AM. For personal use only. Not approved for distribution. Copyright 2012 National Comprehensive Cancer
 , Table of Contents NCCN Categories of Evidence and Consensus Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate. Category 2A: Based upon lower-level
, Table of Contents NCCN Categories of Evidence and Consensus Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate. Category 2A: Based upon lower-level
HIPEC Controversies in the Indications and Application of Regional Chemotherapy for Peritoneal Surface Malignancies
 HIPEC Controversies in the Indications and Application of Regional Chemotherapy for Peritoneal Surface Malignancies Crescent City Cancer Update: GI and HPB Saturday September 24, 2016 George M. Fuhrman,
HIPEC Controversies in the Indications and Application of Regional Chemotherapy for Peritoneal Surface Malignancies Crescent City Cancer Update: GI and HPB Saturday September 24, 2016 George M. Fuhrman,
Partial Nephrectomy Techniques for Renal Preservation: Historical and Modern Approaches
 Partial Nephrectomy Techniques for Renal Preservation: Historical and Modern Approaches Cary N Robertson MD FACS Associate Professor Division of Urology Associate Director Urologic Oncology Duke Cancer
Partial Nephrectomy Techniques for Renal Preservation: Historical and Modern Approaches Cary N Robertson MD FACS Associate Professor Division of Urology Associate Director Urologic Oncology Duke Cancer
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016. Background
 Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
STAGING, BIOPSY AND NATURAL HISTORY OF TUMORS SCOTT D WEINER MD
 STAGING, BIOPSY AND NATURAL HISTORY OF TUMORS SCOTT D WEINER MD WHAT DO YOU DO WHEN THIS SHOWS UP IN YOUR OFFICE? besides panicking KEY PRINCIPLE!!! Reactive zone is the edema, neovascularity and inflammation
STAGING, BIOPSY AND NATURAL HISTORY OF TUMORS SCOTT D WEINER MD WHAT DO YOU DO WHEN THIS SHOWS UP IN YOUR OFFICE? besides panicking KEY PRINCIPLE!!! Reactive zone is the edema, neovascularity and inflammation
Palliative radiotherapy in lung cancer
 New concepts and insights regarding the role of radiation therapy in metastatic disease Umberto Ricardi University of Turin Department of Oncology Radiation Oncology Palliative radiotherapy in lung cancer
New concepts and insights regarding the role of radiation therapy in metastatic disease Umberto Ricardi University of Turin Department of Oncology Radiation Oncology Palliative radiotherapy in lung cancer
Radio-Pathologic Workup of a Retroperitoneal Abdominal Mass
 Radio-Pathologic Workup of a Retroperitoneal Abdominal Mass Joe Carlson Advanced Radiology Clerkship Harvard Medical School Year IV September 12, 2002 84 year old Male Presented to PCP With Abdominal Pain
Radio-Pathologic Workup of a Retroperitoneal Abdominal Mass Joe Carlson Advanced Radiology Clerkship Harvard Medical School Year IV September 12, 2002 84 year old Male Presented to PCP With Abdominal Pain
Brief History. Identification : Past History : HTN without regular treatment.
 Brief History Identification : Name : 陳 x - Admission : 94/10/06 Gender : male Age : 75 y/o Chief Complaint : Urinary difficulty for months. Past History : HTN without regular treatment. Brief History
Brief History Identification : Name : 陳 x - Admission : 94/10/06 Gender : male Age : 75 y/o Chief Complaint : Urinary difficulty for months. Past History : HTN without regular treatment. Brief History
Pathology Mystery and Surprise
 Pathology Mystery and Surprise Tim Smith, MD Director Anatomic Pathology Medical University of South Carolina Disclosures No conflicts to declare Some problem cases Kidney tumor Scalp tumor Bladder tumor
Pathology Mystery and Surprise Tim Smith, MD Director Anatomic Pathology Medical University of South Carolina Disclosures No conflicts to declare Some problem cases Kidney tumor Scalp tumor Bladder tumor
Oncologic Emergencies: When to call the Radiation Oncologist
 Oncologic Emergencies: When to call the Radiation Oncologist Dr. Shrinivas Rathod Radiation Oncologist Radiation Oncology Program CancerCare Manitoba and University of Manitoba Disclosures Speaker s name:
Oncologic Emergencies: When to call the Radiation Oncologist Dr. Shrinivas Rathod Radiation Oncologist Radiation Oncology Program CancerCare Manitoba and University of Manitoba Disclosures Speaker s name:
Treatment strategy of metastatic rectal cancer
 35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy. Julia White MD Professor, Radiation Oncology
 Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy Julia White MD Professor, Radiation Oncology Agenda Efficacy of radiotherapy in the management of breast cancer in the Adjuvant
Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy Julia White MD Professor, Radiation Oncology Agenda Efficacy of radiotherapy in the management of breast cancer in the Adjuvant
Case Scenario 1. Pathology report Specimen from mediastinoscopy Final Diagnosis : Metastatic small cell carcinoma with residual lymphatic tissue
 Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
Lymphadenectomy in RCC: Yes, No, Clinical Trial?
 Lymphadenectomy in RCC: Yes, No, Clinical Trial? Viraj Master MD PhD FACS Professor Associate Chair for Clinical Affairs and Quality Director of Clinical Research Unit Department of Urology Emory University
Lymphadenectomy in RCC: Yes, No, Clinical Trial? Viraj Master MD PhD FACS Professor Associate Chair for Clinical Affairs and Quality Director of Clinical Research Unit Department of Urology Emory University
Preoperative adjuvant radiotherapy
 Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
CHEMO-RADIOTHERAPY FOR BLADDER CANCER. Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre
 CHEMO-RADIOTHERAPY FOR BLADDER CANCER Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre AIMS Muscle invasive disease Current Gold-Standard Rationale behind Chemo-Radiotherapy
CHEMO-RADIOTHERAPY FOR BLADDER CANCER Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre AIMS Muscle invasive disease Current Gold-Standard Rationale behind Chemo-Radiotherapy
NEOADJUVANT THERAPY IN CARCINOMA STOMACH. Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah
 NEOADJUVANT THERAPY IN CARCINOMA STOMACH Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah NEOADJUVANT THERAPY?! Few believers Limited evidence Many surgeons
NEOADJUVANT THERAPY IN CARCINOMA STOMACH Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah NEOADJUVANT THERAPY?! Few believers Limited evidence Many surgeons
14. Background. Sarcoma. Resectable extremity soft tissue sarcomas
 96 14. Sarcoma Background Radiotherapy is widely used as an adjunct to surgery in the management of soft tissue sarcomas as the risk of failure in the surgical bed can be high. For bone sarcomas, radiotherapy
96 14. Sarcoma Background Radiotherapy is widely used as an adjunct to surgery in the management of soft tissue sarcomas as the risk of failure in the surgical bed can be high. For bone sarcomas, radiotherapy
Case 8 Soft tissue swelling
 Case 8 Soft tissue swelling 26-year-old female presented with a swelling on the back of the left knee joint since the last 6 months and chronic pain in the calf and foot since the last 2 months. Pain in
Case 8 Soft tissue swelling 26-year-old female presented with a swelling on the back of the left knee joint since the last 6 months and chronic pain in the calf and foot since the last 2 months. Pain in
Regional Therapy for Management of Peritoneal Carcinomatosis from Gastrointestinal Malignancies
 Regional Therapy for Management of Peritoneal Carcinomatosis from Gastrointestinal Malignancies Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service City of Hope Division of Surgical Oncology September
Regional Therapy for Management of Peritoneal Carcinomatosis from Gastrointestinal Malignancies Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service City of Hope Division of Surgical Oncology September
Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease
 Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease Jennifer E. Tseng, MD UFHealth Cancer Center-Orlando Health Sep 12, 2014 Background Approximately
Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease Jennifer E. Tseng, MD UFHealth Cancer Center-Orlando Health Sep 12, 2014 Background Approximately
Update on RECIST and Staging of Common Pediatric Tumors Ethan A. Smith, MD
 Update on RECIST and Staging of Common Pediatric Tumors Ethan A. Smith, MD Section of Pediatric Radiology C.S. Mott Children s Hospital University of Michigan ethans@med.umich.edu Disclosures No relevant
Update on RECIST and Staging of Common Pediatric Tumors Ethan A. Smith, MD Section of Pediatric Radiology C.S. Mott Children s Hospital University of Michigan ethans@med.umich.edu Disclosures No relevant
How much colon should be resected?
 Colon Cancer Surgical Standard of Care and Operative Techniques Madhulika G. Varma MD Professor and Chief Section of Colorectal Surgery University of California, San Francisco How much colon should be
Colon Cancer Surgical Standard of Care and Operative Techniques Madhulika G. Varma MD Professor and Chief Section of Colorectal Surgery University of California, San Francisco How much colon should be
Patient Presentation. 32 y.o. female complains of lower abdominal mass CEA = 433, CA125 = 201
 Patient Presentation 32 y.o. female complains of lower abdominal mass CEA = 433, CA125 = 201 CT shows: Thickening of the right hemidiaphragm CT shows: Fluid in the right paracolic sulcus CT shows: Large
Patient Presentation 32 y.o. female complains of lower abdominal mass CEA = 433, CA125 = 201 CT shows: Thickening of the right hemidiaphragm CT shows: Fluid in the right paracolic sulcus CT shows: Large
Surgical Management of Advanced Stage Colon Cancer. Nathan Huber, MD 6/11/14
 Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Pre-operative assessment of patients for cytoreduction and HIPEC
 Pre-operative assessment of patients for cytoreduction and HIPEC Washington Hospital Center Washington, DC, USA Ovarian Cancer Surgery New Strategies Bergamo, Italy May 5, 2011 Background Cytoreductive
Pre-operative assessment of patients for cytoreduction and HIPEC Washington Hospital Center Washington, DC, USA Ovarian Cancer Surgery New Strategies Bergamo, Italy May 5, 2011 Background Cytoreductive
External Beam Radiation Therapy for Thyroid Cancer
 External Beam Radiation Therapy for Thyroid Cancer C. Jillian Tsai, M.D, PH.D. Assistant Attending Director of Head and Neck Cancer Research Department of Radiation Oncology Memorial Sloan Kettering Cancer
External Beam Radiation Therapy for Thyroid Cancer C. Jillian Tsai, M.D, PH.D. Assistant Attending Director of Head and Neck Cancer Research Department of Radiation Oncology Memorial Sloan Kettering Cancer
Leiomyosarcoma involving the inferior vena cava in an. elderly patient with reference to its operative modalities: a case report
 Leiomyosarcoma involving the inferior vena cava in an elderly patient with reference to its operative modalities: a case report Hiroshi Ushida 1, Ryosuke Murai 1, Mitsuhiro Narita 1, Fumiyoshi Kojima 2
Leiomyosarcoma involving the inferior vena cava in an elderly patient with reference to its operative modalities: a case report Hiroshi Ushida 1, Ryosuke Murai 1, Mitsuhiro Narita 1, Fumiyoshi Kojima 2
UPDATE IN THE MANAGEMENT OF INVASIVE CERVICAL CANCER
 UPDATE IN THE MANAGEMENT OF INVASIVE CERVICAL CANCER Susan Davidson, MD Professor Department of Obstetrics and Gynecology Division of Gynecologic Oncology University of Colorado- Denver Anatomy Review
UPDATE IN THE MANAGEMENT OF INVASIVE CERVICAL CANCER Susan Davidson, MD Professor Department of Obstetrics and Gynecology Division of Gynecologic Oncology University of Colorado- Denver Anatomy Review
Appendix 4 Urology Care Pathways
 Appendix 4 Urology Care Pathways Cancer Care Pathways outline the steps and stages in the patient journey from referral through to diagnostics, staging, treatment, follow up, rehabilitation and if applicable
Appendix 4 Urology Care Pathways Cancer Care Pathways outline the steps and stages in the patient journey from referral through to diagnostics, staging, treatment, follow up, rehabilitation and if applicable
GUIDELINES ON RENAL CELL CARCINOMA
 GUIDELINES ON RENAL CELL CARCINOMA B. Ljungberg (chairman), D.C. Hanbury, M.A. Kuczyk, A.S. Merseburger, P.F.A. Mulders, J-J. Patard, I.C. Sinescu Introduction This EAU guideline was prepared to help urologists
GUIDELINES ON RENAL CELL CARCINOMA B. Ljungberg (chairman), D.C. Hanbury, M.A. Kuczyk, A.S. Merseburger, P.F.A. Mulders, J-J. Patard, I.C. Sinescu Introduction This EAU guideline was prepared to help urologists
COLON AND RECTAL CANCER
 COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Thank you for agreeing to give us a statement on your organisation s view of the technology and the way it should be used in the NHS.
 Thank you for agreeing to give us a statement on your organisation s view of the technology and the way it should be used in the NHS. Healthcare professionals can provide a unique perspective on the technology
Thank you for agreeing to give us a statement on your organisation s view of the technology and the way it should be used in the NHS. Healthcare professionals can provide a unique perspective on the technology
Retroperitoneal Soft Tissue Sarcomas: Prognosis and Treatment of Primary and Recurrent Disease in 117 Patients
 Retroperitoneal Soft Tissue Sarcomas: Prognosis and Treatment of Primary and Recurrent Disease in 117 Patients INGO ALLDINGER 1,2, QIN YANG 3, CHRISTIAN PILARSKY 1, HANS-DETLEV SAEGER 1, WOLFRAM T. KNOEFEL
Retroperitoneal Soft Tissue Sarcomas: Prognosis and Treatment of Primary and Recurrent Disease in 117 Patients INGO ALLDINGER 1,2, QIN YANG 3, CHRISTIAN PILARSKY 1, HANS-DETLEV SAEGER 1, WOLFRAM T. KNOEFEL
Locally Advanced Colon Cancer. Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery
 Locally Advanced Colon Cancer Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery Case 34 yo man presented with severe RLQ abdominal pain X 24 hrs. No nausea/vomiting/fever. + flatus.
Locally Advanced Colon Cancer Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery Case 34 yo man presented with severe RLQ abdominal pain X 24 hrs. No nausea/vomiting/fever. + flatus.
Louisa Fleure. Advanced Prostate Cancer Clinical Nurse Specialist. Guys and St Thomas NHS Trust
 Louisa Fleure Advanced Prostate Cancer Clinical Nurse Specialist Guys and St Thomas NHS Trust The classification of advanced prostate cancer The incidence of patients presenting with, or developing advanced
Louisa Fleure Advanced Prostate Cancer Clinical Nurse Specialist Guys and St Thomas NHS Trust The classification of advanced prostate cancer The incidence of patients presenting with, or developing advanced
Guidelines for the management of soft tissue sarcomas. The British Sarcoma Group Authors:
 Guidelines for the management of soft tissue sarcomas. The British Sarcoma Group Authors: Mr Robert Grimer Consultant Orthopaedic Surgeon, Royal Orthopaedic Hospital, Birmingham Prof Ian Judson Consultant
Guidelines for the management of soft tissue sarcomas. The British Sarcoma Group Authors: Mr Robert Grimer Consultant Orthopaedic Surgeon, Royal Orthopaedic Hospital, Birmingham Prof Ian Judson Consultant
Regional Therapy for Management of Peritoneal Carcinomatosis from Gastrointestinal Malignancies
 Regional Therapy for Management of Peritoneal Carcinomatosis from Gastrointestinal Malignancies Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service City of Hope Division of Surgical Oncology September
Regional Therapy for Management of Peritoneal Carcinomatosis from Gastrointestinal Malignancies Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service City of Hope Division of Surgical Oncology September
Clinical/Surgical trials that will change my practice
 Clinical/Surgical trials that will change my practice Mr Jim M Adshead Herts and Beds Urological Cancer Centre, Lister Hospital What s changed and where do I feel we are clutching at straws? Regional Specialist
Clinical/Surgical trials that will change my practice Mr Jim M Adshead Herts and Beds Urological Cancer Centre, Lister Hospital What s changed and where do I feel we are clutching at straws? Regional Specialist
UK Musculoskeletal Oncology: Something for All Ages. Lars Wagner, MD Pediatric Hematology/Oncology University of Kentucky
 UK Musculoskeletal Oncology: Something for All Ages Lars Wagner, MD Pediatric Hematology/Oncology University of Kentucky Pediatric-Type Sarcomas of Bone and Soft Tissue The incidence of sarcoma continues
UK Musculoskeletal Oncology: Something for All Ages Lars Wagner, MD Pediatric Hematology/Oncology University of Kentucky Pediatric-Type Sarcomas of Bone and Soft Tissue The incidence of sarcoma continues
Thymic Tumors. Feiran Lou MD. MS. Kings County Hospital Department of Surgery
 Thymic Tumors Feiran Lou MD. MS. Kings County Hospital Department of Surgery Case HPI 53 yo man referred from OSH for anterior mediastinal mass. Initially presented with leg weakness and back pain for
Thymic Tumors Feiran Lou MD. MS. Kings County Hospital Department of Surgery Case HPI 53 yo man referred from OSH for anterior mediastinal mass. Initially presented with leg weakness and back pain for
Afternoon Session Cases
 Afternoon Session Cases Case 1 19 year old woman Presented with abdominal pain to community hospital Mild incr WBC a14, 000, Hg normal, lipase 100 (normal to 75) US 5.2 x 3.7 x 4 cm mass in porta hepatis
Afternoon Session Cases Case 1 19 year old woman Presented with abdominal pain to community hospital Mild incr WBC a14, 000, Hg normal, lipase 100 (normal to 75) US 5.2 x 3.7 x 4 cm mass in porta hepatis
Cancer of Unknown Primary (CUP) Protocol
 Protocol") 1 Department of Oncology. Cancer of Unknown Primary (CUP) Protocol Version: Document type: Document sponsor Designation Document author [ s] Designation[s] Approving committee / Group Ratified by: Date
1 Department of Oncology. Cancer of Unknown Primary (CUP) Protocol Version: Document type: Document sponsor Designation Document author [ s] Designation[s] Approving committee / Group Ratified by: Date
All India Institute of Medical Sciences, New Delhi, INDIA. Department of Pediatric Surgery, Medical Oncology, and Radiology
 All India Institute of Medical Sciences, New Delhi, INDIA Department of Pediatric Surgery, Medical Oncology, and Radiology Clear cell sarcoma of the kidney- rare renal neoplasm second most common renal
All India Institute of Medical Sciences, New Delhi, INDIA Department of Pediatric Surgery, Medical Oncology, and Radiology Clear cell sarcoma of the kidney- rare renal neoplasm second most common renal
Hepatobiliary Malignancies Retrospective Study at Truman Medical Center
 Hepatobiliary Malignancies 206-207 Retrospective Study at Truman Medical Center Brandon Weckbaugh MD, Prarthana Patel & Sheshadri Madhusudhana MD Introduction: Hepatobiliary malignancies are cancers which
Hepatobiliary Malignancies 206-207 Retrospective Study at Truman Medical Center Brandon Weckbaugh MD, Prarthana Patel & Sheshadri Madhusudhana MD Introduction: Hepatobiliary malignancies are cancers which
CT PET SCANNING for GIT Malignancies A clinician s perspective
 CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
The evidence for and against neoadjuvant chemotherapy in localized STS
 The evidence for and against neoadjuvant chemotherapy in localized STS Axel Le Cesne Gustave Roussy, Villejuif French Sarcoma Group EORTC, CTOS Académie de Médecine Drugs Practice, 2 nd of December 2016
The evidence for and against neoadjuvant chemotherapy in localized STS Axel Le Cesne Gustave Roussy, Villejuif French Sarcoma Group EORTC, CTOS Académie de Médecine Drugs Practice, 2 nd of December 2016
Chemotherapy Treatment Algorithms for Urology Cancer
 Chemotherapy Treatment Algorithms for Urology Cancer Chemoradiation for bladder cancer; Chemotherapy algorithm for non TCC bladder cancer Squamous cell carcinoma; Chemotherapy Algorithm for Non Transitional
Chemotherapy Treatment Algorithms for Urology Cancer Chemoradiation for bladder cancer; Chemotherapy algorithm for non TCC bladder cancer Squamous cell carcinoma; Chemotherapy Algorithm for Non Transitional
Disclosures 5/13/2013. Principles and Practice of Radiation Oncology First Annual Cancer Rehabilitation Symposium May 31, 2013
 Principles and Practice of Radiation Oncology First Annual Cancer Rehabilitation Symposium May 31, 2013 Josh Yamada MD FRCPC Department of Radiation Oncology Memorial Sloan Kettering Cancer Center Disclosures
Principles and Practice of Radiation Oncology First Annual Cancer Rehabilitation Symposium May 31, 2013 Josh Yamada MD FRCPC Department of Radiation Oncology Memorial Sloan Kettering Cancer Center Disclosures
Dr. Tareq Salah Ahmed,MD,ESMO. Lecturer of clinical oncology, Assiut faculty of medicine ESMO accreditation certificate
 Dr. Tareq Salah Ahmed,MD,ESMO Lecturer of clinical oncology, Assiut faculty of medicine ESMO accreditation certificate 1 st Assiut Urology department conference,marsa Alam 3 rd February 2015 Bladder cancer
Dr. Tareq Salah Ahmed,MD,ESMO Lecturer of clinical oncology, Assiut faculty of medicine ESMO accreditation certificate 1 st Assiut Urology department conference,marsa Alam 3 rd February 2015 Bladder cancer
Q&A. Fabulous Prizes. Collecting Cancer Data: Bladder, Renal Pelvis, and Ureter 5/2/13. NAACCR Webinar Series
 Collecting Cancer Data Bladder & Renal Pelvis NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data Bladder & Renal Pelvis NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Boot Camp Case Scenarios
 Boot Camp Case Scenarios Case Scenario 1 Patient is a 69-year-old white female. She presents with dyspnea on exertion, cough, and right rib pain. Patient is a smoker. 9/21/12 CT Chest FINDINGS: There is
Boot Camp Case Scenarios Case Scenario 1 Patient is a 69-year-old white female. She presents with dyspnea on exertion, cough, and right rib pain. Patient is a smoker. 9/21/12 CT Chest FINDINGS: There is
MDCT signs differentiating retroperitoneal and intraperitoneal lesions- diagnostic pearls
 MDCT signs differentiating retroperitoneal and intraperitoneal lesions- diagnostic pearls Poster No.: C-0987 Congress: ECR 2015 Type: Educational Exhibit Authors: D. V. Bhargavi, R. Avantsa, P. Kala; Bangalore/IN
MDCT signs differentiating retroperitoneal and intraperitoneal lesions- diagnostic pearls Poster No.: C-0987 Congress: ECR 2015 Type: Educational Exhibit Authors: D. V. Bhargavi, R. Avantsa, P. Kala; Bangalore/IN
Radiation and DCIS. The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging
 Radiation and DCIS The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging Einsley-Marie Janowski, MD, PhD Assistant Professor Department of Radiation Oncology
Radiation and DCIS The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging Einsley-Marie Janowski, MD, PhD Assistant Professor Department of Radiation Oncology
Jose Ramos. Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma
 Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Evolution of liver resection Better understanding
Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Evolution of liver resection Better understanding
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: SURGICAL ONCOLOGY 5-May-2013 DEVELOPED BY: Bruce
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: SURGICAL ONCOLOGY 5-May-2013 DEVELOPED BY: Bruce