Re-re-irradiation What do we know about it?
|
|
|
- Dylan Eaton
- 5 years ago
- Views:
Transcription

1 Re-re-irradiation What do we know about it? Carsten Nieder Dept. of Clinical Medicine Faculty of Health Sciences University of Tromsø and Dept. of Oncology Nordland Hospital Trust Bodø, Norway
2 Hoffman WJ, Carver LF. Chronic myelogenous leukemia. JAMA 1931;97: Remarkable symptomatic improvement lasting up to one year after repeated cycles of low doses of radiation to the spleen or spleen plus long bones

3 Published in Strahlentherapie 1941 Fatal complications after 3, 5 and 6 series for head and neck cancer Soft tissue and chondronecrosis; soft tissue & chondronecrosis plus osteomyelitis; aspiration pneumonia due to laryngeal dysfunction
4 WBRT, 81 patients with different primary tumors 12 were retreated twice and 3 received a total of 4 series 10-Gy single dose or 2-5 fractions (one week) No details reported Clinical benefit was reported after the first, second and third course in 69, 68 and 50% of the patients, respectively Mean duration of improvement was 1.8, 2.6 and 1.5 months, respectively
5 From bench to beside? Preclinical research Phase I clinical trial Phase II clinical trial Phase III clinical trial Evidence-based re-irradiation regimens Different EBRT fractionation concepts HDR brachytherapy, protons, carbon ions Combination with cytotoxic chemotherapy, immunotherapy, hyperthermia
6 Preclinical data repair/recovery Extent and kinetics of recovery of occult spinal cord injury K.Kian Ang, M.D., Guo-Liang Jiang, M.D., Yan Feng, M.D., L.Clifton Stephens, Susan L Tucker, Ph.D. and Roger E Price International Journal of Radiation Oncology * Biology * Physics Volume 50, Issue 4, Pages (July 2001) Rhesus monkeys: 2.2 Gy per fraction, total 44 Gy, cervicothoracic cord, interval 1-3 years, cumulative dose Gy, approximately 60% of the initial dose «disappears» within 1 year, up to 75% within 2 years
 a b c d Clinical side effect Time Modified from Dörr &")
7 Relative tissue integrity % Repair and recovery Experimental animal data: certain organs forget previous irradiation if this did not result in severe damage ( recovery from occult damage ) a b c d Clinical side effect Time Modified from Dörr & Herrmann

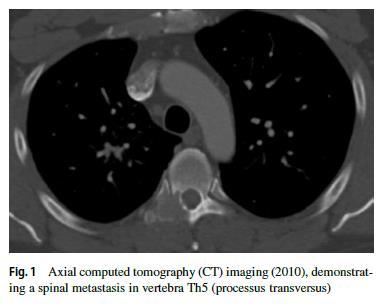
8 Female patient with painful sacral bone metastases from breast cancer June 2011: single posterior field (no 3-D plan) 30 Gy in 10 fractions of 3 Gy February 2012: 3-D conformal plan, same regimen January 2015: 3-D conformal plan, 20 Gy in 8 fractions of 2.5 Gy
9 Course Dose EQD2 (3 Gy) Recovery EQD2 re 1 30 (3) 36 25% after 6-12 mo (3) 36 50% after >12 mo (2.5) Sum EQD2 for all 3 courses (alpha/beta 3 Gy) = 94 Gy Residual EQD2 taking into account recovery = 67 Gy More than 2.5 years of follow-up without clinically evident toxicity
10 Pelvic reirradiation case (1) 79-year-old gentleman treated with abdominoperineal resection 4 years earlier, rectal cancer T3 N0 with lymphovascular invasion and 1mm margin to the peritoneal surface June 2008, 60 Gy in 2-Gy fractions, capecitabine Good clinical and CEA response, opted against surgery July 2009, 50.4 Gy in 1.8-Gy fractions, capecitabine Lung metastases, limited prognosis January 2012, 30 Gy in 2.5-Gy fractions



11 Pelvic reirradiation case (2) Maximum dose for sacral nerves was EQD2 142 Gy (residual EQD2 87 Gy)
12 Evidence based re-irradiation regimes All published randomized clinical studies Bone metastases fractionation (8 Gy vs. 20 Gy) Postoperative RCT vs. observation (H&N) Palliative RCT vs. CT (H&N), failed to accrue Nasopharynx ca fractionation (convent. vs. hypofr.) Nasopharynx ca RCT vs. RT Nasopharynx ca dose escalation ( Gy) Breast cancer skin met. fractionation (conv. vs. hypofr.) Brachytherapy vs. EBRT (H&N), 2014 (64 pat. only) Glioblastoma RT vs. RT + APG-101

13
14 Course Dose EQD2 (2 Gy) Recovery EQD2 re 1 30 (3) % after >12 mo (3) % after >12 mo ?? Sum EQD2 for 2 previous courses (alpha/beta 2 Gy) = 75 Gy Residual EQD2 taking into account recovery = 37.5 Gy
15 Sahgal A, Ma L, Weinberg V, et al. Reirradiation human spinal cord tolerance for stereotactic body radiotherapy. Int J Radiat Oncol Biol Phys 2012;82: SBRT given at least 5 months after conventional palliative radiotherapy with a reirradiation thecal sac P(max) EQD2 of Gy appears to be safe provided the total P(max) EQD2 does not exceed approximately 70 Gy, and the SBRT thecal sac P(max) EQD2 comprises no more than approximately 50% of the total nbed
16
17 Spinal cord EQD2: <10 Gy, 12.5 Gy, 12.5 Gy, 14 Gy, 19 Gy (maximum point dose) Sum EQD2: 94 Gy, residual EQD2: 56.5 Gy Compromise target volume coverage, however follow spine SBRT guidelines as closely as possible Different approaches to define the spinal cord PRV (cord +1 mm, cord +1.5 mm, cord +3 mm, spinal canal) With 3 courses, interfraction motion and body weight changes will probably prevent us from delivering the Dmax to the spinal cord to the exact same small volume each time Other toxicity: compression fracture, esophageal?, lung?, trachea?, skin?
18 Second re-irradiation: spine Thibault I. et al. Int J Radiat Oncol Biol Phys 2015 Toronto group: 24 spinal segments Conventional RT Gy in 5-40 fractions Than 2 series of SBRT and Gy in 2-5 fractions Individual sum doses and time intervals not reported Median spinal cord PRV EQD2: 30, 20.8, 21.9 Gy maximum point dose Median cumulative EQD2: 73.9 Gy Median EQD2 to 0.1 cc: 30, 17.2, 18.1 Gy (cum Gy) Regarding thecal sac (repr. cauda equina PRV), median cumulative EQD2 was higher: 80.4 Gy (max), 71.5 Gy (0.1 cc)
19 Second re-irradiation: spine Thibault I. et al. Int J Radiat Oncol Biol Phys 2015 Median follow-up from 2 nd SBRT: 6.8 months No compression fracture in patients who were surgery-naϊve (not stabilized before) No radiation myelopathy No toxicity grade 3+ Crude local control 77% Most often prescribed 30 Gy in 4 fractions of 7.5 Gy (identical to the recommendation in the previously presented case scenario)
20 Second re-irradiation: spine Katsoulakis E. et al. J Neurosurg Spine 2013 MSKCC group: 10 patients, IG-IMRT Initial course: 9 different dose/fractionation regimes Median time interval 1: 18.5 mo (3-6 in 2 cases) Second course: 30 Gy in 5 fractions (n=6), 25/5 (n=2) Median time interval 2: 11.5 mo (minimum 2, in the 2 cases with short interval 1 minimum 9 mo) Third course: often 30 Gy or 25 Gy in 5 fractions
21 Second re-irradiation: spine Katsoulakis E. et al. J Neurosurg Spine 2013 Median follow-up from 2 nd Re-RT: 12 months Crude rate of local control: 80% Median true spinal cord (CT myelogram) maximum EQD2: 70.7 Gy Three patients had >75 Gy (2/3 to the lumbar spine) No high-grade toxicity, however one grade 2 neuropathy after Gy EQD2 to segment L3
22 Second re-irradiation: bone mets Jeremic B. et al. J Pain Symptom Manage patients, first RT: 4, 6 or 8 Gy single fraction Second & third RT: 4 Gy each Median time interval to third RT: 20 weeks 80% overall response rate, 64% palliated until death Median OS 7 weeks As expected with low dose RT, no serious toxicity
23 Peulen H, Karlsson K, Lindberg K, Tullgren O, Baumann P, Lax I, Lewensohn R, Wersäll P. Toxicity after reirradiation of pulmonary tumours with stereotactic body radiotherapy. Radiother Oncol 2011;101: All patients re-irradiated with SBRT in the period , for stage II III lung tumors or lung metastases, at Karolinska University Hospital, Sweden n=29, 4 had 3 courses (1 even 4), mean EQD2 for each course was 109 Gy, 10 Gy x3 and 8 Gy x5 were common regimens Higher risk in central tumors (tracheal fistula, stenosis of superior vena cava), larger clinical target volumes; no grade 4 or 5 toxicity in peripheral tumors
24 Second re-irradiation: pelvis Feddock J. et al. Int J Radiat Oncol Biol Phys 2017 Permanent interstitial brachytherapy, mostly uterine cancer after previous pelvic RT 9 patients with re-implant to vaginal lesions Median cumulative EQD2 was 152 Gy Only 3/9 tumors controlled at last follow-up or death Median time to failure was 7.7 months All patients developed soft tissue necrosis (symptomatic in 2/9)
25 Second re-irradiation: pelvis Abusaris H. et al. Radiother Oncol 2011 Rotterdam group: 23 patients with dose summation after 2 nd re-irradiation, 14 treated to pelvic target volumes (often rectal cancer), 6 to thoracic wall target volumes For re-irradiation of the organs at risk, the maximum dose was set as 50% more than the normal constraint if the interval was >=12 mo (maximum allowed dose for spinal cord, sacral nerves (cauda equine) was EQD2 75 Gy, 105 Gy (alpha/beta 3 Gy) ) A dose adjustment of 25% was allowed for re-irradiation after 6 12 months. No recovery was used when reirradiation was done within 6 months
26 Second re-irradiation: pelvis Abusaris H. et al. Radiother Oncol 2011 Individualized technique and fractionation 32 Gy/4, 20 Gy/4, 30 Gy/2 Median interval 15 and 7 mo (f/u 7 mo, OS 7 mo) 71% experienced pain reduction No grade 4 acute or late toxity <10% each acute grade 3 dysuria or pain 1 grade 3 late skin toxicity
27 Second re-irradiation: brain mets Six small datasets WBRT + SRS + SRS (and 2 studies WBRT x2 + SRS) Balermpas et al., n=5 (1 radiation necrosis) Koffer et al., n=8, compared to SRS + SRS higher rate of local failure (37.5 vs. 12.5%, p=0.15) and of radiation necrosis (37.5% vs. 6.3%, p=0.05). 75% experienced failure or necrosis
28 Second re-irradiation: brain mets Rana N. et al. Frontiers in Oncology patients: WBRT + SRS + SRS Median 10.7 mo between WBRT and SRS1, 9.7 mo between SRS1 and 2 (all 28 patients with SRS x2) Includes SRS to surgical cavities and SFRT Prior WBRT not sign. associated with local failure, no further details reported The same is true for radionecrosis Overall rate of radionecrosis: 19% (1 patient needed surgery)
29 Second re-irradiation: brain mets Moreau J. et al. PLOS One patients: WBRT + SRS + SRS All without neurological deficit and with KPS 70+ Minimum 10 mo between SRS 1 and 2 >5 mm to brain stem/optic nerve/chiasm Outside motor area Another 2 patients had SRS + SRS + WBRT WBRT standard regimen was 30 Gy in 10 fr. SRS 2 was Gy (median 18) at the isocenter
30 Second re-irradiation: brain mets Moreau J. et al. PLOS One 2018 Results unfortunately reported in 30 patients (some had SRS + SRS without any WBRT) LC after SRS 2: 68% at 12 months 1-year OS: 65.5% If previous WBRT, better LC (similar OS) All adverse effects were RTOG grade 1 or 2 and did not cause neurologic deficit All were observed in patients with WBRT + SRS x2 5 local edema, 5 hemorrhage, 4 radionecrosis (18%) Less adverse effects if BM was <7 ccm
31 Conclusions (1) Some centers offer re-re-irradiation, resulting in increasing numbers of publications Due to small retrospective datasets, the level of evidence is limited and the number of open questions is high Highly selected patients who tolerated prior RT and were willing to provide informed consent Typically, individually tailored approaches, which might result in clinical benefit and acceptable risk of complications in bone metastases and pelvic targets Tissue necrosis and fatal outcomes have been reported
 and 50% (12 mo)?")

32 Conclusions (2) Research into recovery processes Starting point for clinicians 25% (6 mo) and 50% (12 mo)? No established dose constraints Image registration, assessment of true cumulative life time dose The impact of different fractionation regimens is not clear Emerging strategy in palliative scenarios

33 Discussion


34 Disclaimer
 Source: Radiotherapy and Oncology")
35 Fig. 2 Evans JD et al. Thorakale Aorta: <120 Gy (1 cm 3 ) Source: Radiotherapy and Oncology 2013; 106: (DOI: /j.radonc )

36 Tolerance of the Brachial Plexus to High-Dose Reirradiation Allen M. Chen, Taeko Yoshizaki, Maria A. Velez, Argin G. Mikaeilian, Sophia Hsu, Minsong Cao International Journal of Radiation Oncology Biology Physics Volume 98, Issue 1, Pages (May 2017) DOI: /j.ijrobp patients with head and neck cancer deformable dose registration screened for symptoms of neuropathy (pain, motor weakness etc.), any grade 12 patients had self-reported symptoms Copyright 2017 Elsevier Inc.
37 Low risk of neuropathy if >2 years between courses and Dmax <95 Gy (EQD2) High risk if <2 years and Dmax >95 Gy Even with 120 Gy or more 8/13 patients (62%) remained free from symptoms Copyright 2017 Elsevier Inc.
38 Key questions How radiosensitive is the tumor? Relapse within the previous target volume shortly after correctly administered accurate treatment? Relapse in a low-dose or adjuvant region? Second primary tumor, e.g., in the head & neck region? Curative vs. palliative treatment, other options? Tolerance of normal tissues/organs at risk at the site of reirradiation? (volume, dose/fractionation, interval, toxicity of the previous treatment)
39 Future trends More data about QoL NTCP models, risk scores Reliable data about total accumulated dose (IGRT, 4-D imaging, deformable image registration) MR Linac Protons and Carbon ions Multimodal concepts Diseases such as pancreatic, esophageal, HC cancer Three courses of radiation treatment
40 Published re-irradiation concepts Head & neck, lung and brain tumors
Disclosure. Paul Medin teaches radiosurgery courses sponsored by BrainLAB Many animals (and humans) were harmed to make this presentation possible!
 were harmed to make this presentation possible!") Disclosure The tolerance of the nervous system to SBRT: dogma, data and recommendations Paul Medin, PhD Paul Medin teaches radiosurgery courses sponsored by BrainLAB Many animals (and humans) were harmed
Disclosure The tolerance of the nervous system to SBRT: dogma, data and recommendations Paul Medin, PhD Paul Medin teaches radiosurgery courses sponsored by BrainLAB Many animals (and humans) were harmed
Radiotherapy symptoms control in bone mets. Francesco Cellini GemelliART. Ernesto Maranzano,MD. Session 5: Symptoms management
 Session 5: Symptoms management Radiotherapy symptoms control in bone mets Francesco Cellini GemelliART Ernesto Maranzano,MD Director of Oncology Department Chief of Radiation Oncology Centre S. Maria Hospital
Session 5: Symptoms management Radiotherapy symptoms control in bone mets Francesco Cellini GemelliART Ernesto Maranzano,MD Director of Oncology Department Chief of Radiation Oncology Centre S. Maria Hospital
Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2
 Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2 Case 79 yo M with hx of T3N0 colon cancer diagnosed in 2008 metastatic liver disease s/p liver segmentectomy 2009
Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2 Case 79 yo M with hx of T3N0 colon cancer diagnosed in 2008 metastatic liver disease s/p liver segmentectomy 2009
Reirradiazione. La radioterapia stereotassica ablativa: torace. Pierluigi Bonomo Firenze
 Reirradiazione La radioterapia stereotassica ablativa: torace Pierluigi Bonomo Firenze Background Stage III NSCLC isolated locoregional recurrence in 25% of pts mostly unresectable; low RR with 2 nd line
Reirradiazione La radioterapia stereotassica ablativa: torace Pierluigi Bonomo Firenze Background Stage III NSCLC isolated locoregional recurrence in 25% of pts mostly unresectable; low RR with 2 nd line
Disclosure SBRT. SBRT for Spinal Metastases 5/2/2010. No conflicts of interest. Overview
 Stereotactic Body Radiotherapy (SBRT) for Recurrent Spine Tumors Arjun Sahgal M.D., F.R.C.P.C. Assistant Professor Princess Margaret Hospital Sunnybrook Health Sciences Center University of Toronto Department
Stereotactic Body Radiotherapy (SBRT) for Recurrent Spine Tumors Arjun Sahgal M.D., F.R.C.P.C. Assistant Professor Princess Margaret Hospital Sunnybrook Health Sciences Center University of Toronto Department
Re-irradiation with or without chemotherapy. Jozsef Lövey National Institute of Oncology, Budapest, Hungary
 Re-irradiation with or without chemotherapy Jozsef Lövey National Institute of Oncology, Budapest, Hungary Disclosures Occasional advisory board and educational activity to Merck, Roche, Nutricia, Takeda,
Re-irradiation with or without chemotherapy Jozsef Lövey National Institute of Oncology, Budapest, Hungary Disclosures Occasional advisory board and educational activity to Merck, Roche, Nutricia, Takeda,
NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) BONE (Version , 03/28/18)
 BONE (Version , 03/28/18)") BONE (Version 2.2018, 03/28/18) NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) Radiation Therapy Specialized techniques such as intensity-modulated RT (IMRT); particle beam RT with protons, carbon ions,
BONE (Version 2.2018, 03/28/18) NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) Radiation Therapy Specialized techniques such as intensity-modulated RT (IMRT); particle beam RT with protons, carbon ions,
Re-irradiation: clinical considerations, outcomes and patient selection
 Re-irradiation: clinical considerations, outcomes and patient selection Michael Gubanski MD, PhD Karolinska University Hospital New? Prospective Phase First reports 3 trials trials of in re-irradiation
Re-irradiation: clinical considerations, outcomes and patient selection Michael Gubanski MD, PhD Karolinska University Hospital New? Prospective Phase First reports 3 trials trials of in re-irradiation
Disclosures. Overview 8/3/2016. SRS: Cranial and Spine
 SRS: Cranial and Spine Brian Winey, Ph.D. Department of Radiation Oncology Massachusetts General Hospital Harvard Medical School Disclosures Travel and research funds from Elekta Travel funds from IBA
SRS: Cranial and Spine Brian Winey, Ph.D. Department of Radiation Oncology Massachusetts General Hospital Harvard Medical School Disclosures Travel and research funds from Elekta Travel funds from IBA
Pelvic palliative radiotherapy for gynecological cancers present state of knowledge and pending research questions to answer
 Pelvic palliative radiotherapy for gynecological cancers present state of knowledge and pending research questions to answer Esten S. Nakken MD PhD Division of Cancer Medicine Oslo University Hospital
Pelvic palliative radiotherapy for gynecological cancers present state of knowledge and pending research questions to answer Esten S. Nakken MD PhD Division of Cancer Medicine Oslo University Hospital
The Role of Radiation Therapy in the Treatment of Brain Metastases. Matthew Cavey, M.D.
 The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
Clinical Case Conference
 Clinical Case Conference Palliative radiation therapy for bone metastasis Jeff Burkeen, MD, PGY2 7/20/2015 1 Overview Epidemiology Pathophysiology Common presentations and symptoms Imaging Surgery Radiation
Clinical Case Conference Palliative radiation therapy for bone metastasis Jeff Burkeen, MD, PGY2 7/20/2015 1 Overview Epidemiology Pathophysiology Common presentations and symptoms Imaging Surgery Radiation
Stereotactic radiotherapy
 Stereotactic radiotherapy Influence of patient positioning and fixation on treatment planning - clinical results Frank Zimmermann Institut für Radioonkologie Universitätsspital Basel Petersgraben 4 CH
Stereotactic radiotherapy Influence of patient positioning and fixation on treatment planning - clinical results Frank Zimmermann Institut für Radioonkologie Universitätsspital Basel Petersgraben 4 CH
8/3/2017. Spine SBRT: A Clinician's Update On Techniques and Outcomes. Disclosures. Outline
 Spine SBRT: A Clinician's Update On Techniques and Outcomes Chia-Lin (Eric) Tseng, MD FRCPC Radiation Oncologist Sunnybrook Health Sciences Centre University of Toronto August 3, 2017 Disclosures I have
Spine SBRT: A Clinician's Update On Techniques and Outcomes Chia-Lin (Eric) Tseng, MD FRCPC Radiation Oncologist Sunnybrook Health Sciences Centre University of Toronto August 3, 2017 Disclosures I have
20. Background. Oligometastases. Oligometastases: bone (including spine) and lymph nodes
 and lymph nodes") 125 20. Oligometastases Background The oligometastatic state can be defined as 1 3 isolated metastatic sites, typically occurring more than six months after successful treatment of primary disease. 1 In
125 20. Oligometastases Background The oligometastatic state can be defined as 1 3 isolated metastatic sites, typically occurring more than six months after successful treatment of primary disease. 1 In
Radiotherapy physics & Equipments
 Radiotherapy physics & Equipments RAD 481 Lecture s Title: An Overview of Radiation Therapy for Health Care Professionals Dr. Mohammed Emam Vision :IMC aspires to be a leader in applied medical sciences,
Radiotherapy physics & Equipments RAD 481 Lecture s Title: An Overview of Radiation Therapy for Health Care Professionals Dr. Mohammed Emam Vision :IMC aspires to be a leader in applied medical sciences,
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
a Phase II Randomised Controlled Trial Matthias Guckenberger
 Dose-intensified Image-guided Fractionated Stereotactic Body Radiation Therapy for Painful Spinal Metastases (DOSIS) versus Conventional Radiation Therapy: a Phase II Randomised Controlled Matthias Guckenberger
Dose-intensified Image-guided Fractionated Stereotactic Body Radiation Therapy for Painful Spinal Metastases (DOSIS) versus Conventional Radiation Therapy: a Phase II Randomised Controlled Matthias Guckenberger
Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer
 for Gynaecological Cancer") Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer Tan Chek Wee 15 06 2016 National University Cancer Institute, Singapore Clinical Care Education Research
Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer Tan Chek Wee 15 06 2016 National University Cancer Institute, Singapore Clinical Care Education Research
Benefits of Radiation Therapy in the Palliative Cancer Patient
 Benefits of Radiation Therapy in the Palliative Cancer Patient Dr Joshua Sappiatzer Radiation Oncologist Page 1 Overview Why we should aim for better palliative radiotherapy treatment Bone metastases Rapid
Benefits of Radiation Therapy in the Palliative Cancer Patient Dr Joshua Sappiatzer Radiation Oncologist Page 1 Overview Why we should aim for better palliative radiotherapy treatment Bone metastases Rapid
Therapeutic ratio - An Overview. Past Present Future Prof Ramesh S Bilimaga
 Therapeutic ratio - An Overview Past Present Future Prof Ramesh S Bilimaga Radiation Oncology Discipline of human medicine concerned with the generation, conservation and dissemination of knowledge concerning
Therapeutic ratio - An Overview Past Present Future Prof Ramesh S Bilimaga Radiation Oncology Discipline of human medicine concerned with the generation, conservation and dissemination of knowledge concerning
Re-Irradiation: Outcome, Cumulative Dose and Toxicity in Patients Retreated with Stereotactic Radiotherapy in the Abdominal or Pelvic Region
 Technology in Cancer Research and Treatment ISSN 1533-0346 Volume 11, Number 6, December 2012 Adenine Press (2012) Re-Irradiation: Outcome, Cumulative Dose and Toxicity in Patients Retreated with Stereotactic
Technology in Cancer Research and Treatment ISSN 1533-0346 Volume 11, Number 6, December 2012 Adenine Press (2012) Re-Irradiation: Outcome, Cumulative Dose and Toxicity in Patients Retreated with Stereotactic
8/2/2018. Acknowlegements: TCP SPINE. Disclosures
 A Presentation for the AAPM Annual meeting, Aug 2, 2018 Nashville, TN Stereotactic Radiosurgery for Spinal Metastases: Tumor Control Probability Analyses and Recommended Reporting Standards for Future
A Presentation for the AAPM Annual meeting, Aug 2, 2018 Nashville, TN Stereotactic Radiosurgery for Spinal Metastases: Tumor Control Probability Analyses and Recommended Reporting Standards for Future
Second Single 4 Gy Reirradiation for Painful Bone Metastasis
 26 Journal of Pain and Symptom Management Vol. 23 No. 1 January 2002 Original Article Second Single 4 Gy Reirradiation for Painful Bone Metastasis Branislav Jeremic, MD, PhD, Yuta Shibamoto, MD, DMSc,
26 Journal of Pain and Symptom Management Vol. 23 No. 1 January 2002 Original Article Second Single 4 Gy Reirradiation for Painful Bone Metastasis Branislav Jeremic, MD, PhD, Yuta Shibamoto, MD, DMSc,
CLINICAL APPLICATION OF LINEAR-QUADRATIC MODEL IN REIRRADIATION OF SYMPTOMATIC BONE METASTASES
 MEDICAL PHYSICS CLINICAL APPLICATION OF LINEAR-QUADRATIC MODEL IN REIRRADIATION OF SYMPTOMATIC BONE METASTASES L. REBEGEA 1,2, M. DUMITRU 1, D. FIRESCU 2,3 1 Sf. Ap. Andrei Emergency Clinical Hospital,
MEDICAL PHYSICS CLINICAL APPLICATION OF LINEAR-QUADRATIC MODEL IN REIRRADIATION OF SYMPTOMATIC BONE METASTASES L. REBEGEA 1,2, M. DUMITRU 1, D. FIRESCU 2,3 1 Sf. Ap. Andrei Emergency Clinical Hospital,
Where are we with radiotherapy for biliary tract cancers?
 Where are we with radiotherapy for biliary tract cancers? Professor Maria A. Hawkins Associate Professor in Clinical Oncology MRC Group Leader/Honorary Consultant Clinical Oncologist CRUK MRC Oxford Institute
Where are we with radiotherapy for biliary tract cancers? Professor Maria A. Hawkins Associate Professor in Clinical Oncology MRC Group Leader/Honorary Consultant Clinical Oncologist CRUK MRC Oxford Institute
Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey
 Updated Oncology 2015: State of the Art News & Challenging Topics CURRENT STATUS OF STEREOTACTIC RADIOSURGERY IN BRAIN METASTASES Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey Bucharest,
Updated Oncology 2015: State of the Art News & Challenging Topics CURRENT STATUS OF STEREOTACTIC RADIOSURGERY IN BRAIN METASTASES Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey Bucharest,
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS. Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1.
 RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
Palliative RT. Jiraporn Setakornnukul, M.D. Radiation Oncology Division Siriraj Hospital, Mahidol University
 Palliative RT Jiraporn Setakornnukul, M.D. Radiation Oncology Division Siriraj Hospital, Mahidol University Scope Brain metastasis Metastasis epidural spinal cord compression SVC obstruction Bone pain
Palliative RT Jiraporn Setakornnukul, M.D. Radiation Oncology Division Siriraj Hospital, Mahidol University Scope Brain metastasis Metastasis epidural spinal cord compression SVC obstruction Bone pain
External Beam Radiotherapy for Prostate Cancer
 External Beam Radiotherapy for Prostate Cancer Chomporn Sitathanee, Radiation Oncology Unit Ramathibodi Hospital, Mahidol University Roles of RT in prostate cancer Definitive RT; intact prostate Post radical
External Beam Radiotherapy for Prostate Cancer Chomporn Sitathanee, Radiation Oncology Unit Ramathibodi Hospital, Mahidol University Roles of RT in prostate cancer Definitive RT; intact prostate Post radical
SBRT in early stage NSCLC
 SBRT in early stage NSCLC Optimal technique and tumor dose Frank Zimmermann Clinic of Radiotherapy and Radiation Oncology University Hospital Basel Petersgraben 4 CH 4031 Basel radioonkologiebasel.ch Techniques
SBRT in early stage NSCLC Optimal technique and tumor dose Frank Zimmermann Clinic of Radiotherapy and Radiation Oncology University Hospital Basel Petersgraben 4 CH 4031 Basel radioonkologiebasel.ch Techniques
Rola brachyterapii w leczeniu wznów nowotworów języka i dna jamy ustnej. The role of brachytherapy in recurrent. oral cavity
 Rola brachyterapii w leczeniu wznów nowotworów języka i dna jamy ustnej The role of brachytherapy in recurrent tumours of the tongue and fundus of the oral cavity Janusz Skowronek, MD, PhD, Ass. Prof.
Rola brachyterapii w leczeniu wznów nowotworów języka i dna jamy ustnej The role of brachytherapy in recurrent tumours of the tongue and fundus of the oral cavity Janusz Skowronek, MD, PhD, Ass. Prof.
The role of Radiation Oncologist: Hi-tech treatments for liver metastases
 The role of Radiation Oncologist: Hi-tech treatments for liver metastases Icro Meattini, MD Radiotherapy-Oncology Unit AOU Careggi Hospital Florence University, Italy Liver Metastases - Background The
The role of Radiation Oncologist: Hi-tech treatments for liver metastases Icro Meattini, MD Radiotherapy-Oncology Unit AOU Careggi Hospital Florence University, Italy Liver Metastases - Background The
Linac or Non-Linac Demystifying And Decoding The Physics Of SBRT/SABR
 Linac or Non-Linac Demystifying And Decoding The Physics Of SBRT/SABR PhD, FAAPM, FACR, FASTRO Department of Radiation Oncology Indiana University School of Medicine Indianapolis, IN, USA Indra J. Das,
Linac or Non-Linac Demystifying And Decoding The Physics Of SBRT/SABR PhD, FAAPM, FACR, FASTRO Department of Radiation Oncology Indiana University School of Medicine Indianapolis, IN, USA Indra J. Das,
Questions may be submitted anytime during the presentation.
 Understanding Radiation Therapy and its Role in Treating Patients with Pancreatic Cancer Presented by Pancreatic Cancer Action Network www.pancan.org August 18, 2014 If you experience technical difficulty
Understanding Radiation Therapy and its Role in Treating Patients with Pancreatic Cancer Presented by Pancreatic Cancer Action Network www.pancan.org August 18, 2014 If you experience technical difficulty
Optimal Management of Isolated HER2+ve Brain Metastases
 Optimal Management of Isolated HER2+ve Brain Metastases Eliot Sims November 2013 Background Her2+ve patients 15% of all breast cancer Even with adjuvant trastuzumab 10-15% relapse Trastuzumab does not
Optimal Management of Isolated HER2+ve Brain Metastases Eliot Sims November 2013 Background Her2+ve patients 15% of all breast cancer Even with adjuvant trastuzumab 10-15% relapse Trastuzumab does not
Treatment of Recurrent Brain Metastases
 Treatment of Recurrent Brain Metastases Penny K. Sneed, M.D. Dept. of Radiation Oncology University of California San Francisco Background Brain metastases occur in 8.5-15% of cancer pts in population-
Treatment of Recurrent Brain Metastases Penny K. Sneed, M.D. Dept. of Radiation Oncology University of California San Francisco Background Brain metastases occur in 8.5-15% of cancer pts in population-
Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms. Overall Clinical Significance 8/3/13
 Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms Jason Sheehan, MD, PhD Departments of Neurosurgery and Radiation Oncology University of Virginia, Charlottesville, VA USA Overall
Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms Jason Sheehan, MD, PhD Departments of Neurosurgery and Radiation Oncology University of Virginia, Charlottesville, VA USA Overall
Introduction to clinical Radiotherapy
 Introduction to clinical Radiotherapy Sarah Brothwood Radiotherapy Practice Educator Rosemere Cancer Centre Sarah.brothwood@lthtr.nhs.uk 01772 522694 Radiotherapy We have been able to see and document
Introduction to clinical Radiotherapy Sarah Brothwood Radiotherapy Practice Educator Rosemere Cancer Centre Sarah.brothwood@lthtr.nhs.uk 01772 522694 Radiotherapy We have been able to see and document
Hypofractionated RT in Cervix Cancer. Anuja Jhingran, MD
 Hypofractionated RT in Cervix Cancer Anuja Jhingran, MD Hypofractionated RT in Cervix Cancer: Clinicaltrials.gov 919 cervix trials 134 hypofractionated RT trials Prostate, breast, NSCLC, GBM 0 cervix trials
Hypofractionated RT in Cervix Cancer Anuja Jhingran, MD Hypofractionated RT in Cervix Cancer: Clinicaltrials.gov 919 cervix trials 134 hypofractionated RT trials Prostate, breast, NSCLC, GBM 0 cervix trials
Palliative radiotherapy in lung cancer
 New concepts and insights regarding the role of radiation therapy in metastatic disease Umberto Ricardi University of Turin Department of Oncology Radiation Oncology Palliative radiotherapy in lung cancer
New concepts and insights regarding the role of radiation therapy in metastatic disease Umberto Ricardi University of Turin Department of Oncology Radiation Oncology Palliative radiotherapy in lung cancer
New modalities in the salvage of recurrent nasopharyngeal carcinoma
 New modalities in the salvage of recurrent nasopharyngeal carcinoma Dr Jeeve Kanagalingam FRCS Eng (ORL-HNS) Department of Otorhinolaryngology Tan Tock Seng Hospital SINGAPORE Nasopharyngeal carcinoma
New modalities in the salvage of recurrent nasopharyngeal carcinoma Dr Jeeve Kanagalingam FRCS Eng (ORL-HNS) Department of Otorhinolaryngology Tan Tock Seng Hospital SINGAPORE Nasopharyngeal carcinoma
Advances in radiation oncology in the management of soft tissue sarcoma 放疗于治疗肉瘤的最新发展
 Advances in radiation oncology in the management of soft tissue sarcoma 放疗于治疗肉瘤的最新发展 Brian O Sullivan Bartley-Smith / Wharton Chair Professor, Department of Radiation Oncology The Princess Margaret / University
Advances in radiation oncology in the management of soft tissue sarcoma 放疗于治疗肉瘤的最新发展 Brian O Sullivan Bartley-Smith / Wharton Chair Professor, Department of Radiation Oncology The Princess Margaret / University
Stereotactic Body Radiation Therapy and Radiofrequency Ablation 2014 Masters of Minimally Invasive Surgery
 Stereotactic Body Radiation Therapy and Radiofrequency Ablation 2014 Masters of Minimally Invasive Surgery Matthew Hartwig, M.D. Duke Cancer Institute Case Presentation I: Patient ER 74 y/o male with A1A
Stereotactic Body Radiation Therapy and Radiofrequency Ablation 2014 Masters of Minimally Invasive Surgery Matthew Hartwig, M.D. Duke Cancer Institute Case Presentation I: Patient ER 74 y/o male with A1A
Rob Glynne-Jones Mount Vernon Cancer Centre
 ESMO Preceptorship Programme Colorectal Cancer Barcelona October 2017 Interventional radiology and stereotactic radiotherapy Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures: last 5 years Speaker:
ESMO Preceptorship Programme Colorectal Cancer Barcelona October 2017 Interventional radiology and stereotactic radiotherapy Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures: last 5 years Speaker:
Clinically Proven Metabolically-Guided TomoTherapy SM Treatments Advancing Cancer Care
 Clinically Proven Metabolically-Guided TomoTherapy SM Treatments Advancing Cancer Care Institution: San Raffaele Hospital Milan, Italy By Nadia Di Muzio, M.D., Radiotherapy Department (collaborators: Berardi
Clinically Proven Metabolically-Guided TomoTherapy SM Treatments Advancing Cancer Care Institution: San Raffaele Hospital Milan, Italy By Nadia Di Muzio, M.D., Radiotherapy Department (collaborators: Berardi
State of the Art Radiotherapy for Pediatric Tumors. Suzanne L. Wolden, MD Memorial Sloan-Kettering Cancer Center
 State of the Art Radiotherapy for Pediatric Tumors Suzanne L. Wolden, MD Memorial Sloan-Kettering Cancer Center Introduction Progress and success in pediatric oncology Examples of low-tech and high-tech
State of the Art Radiotherapy for Pediatric Tumors Suzanne L. Wolden, MD Memorial Sloan-Kettering Cancer Center Introduction Progress and success in pediatric oncology Examples of low-tech and high-tech
Helical Tomotherapy Experience. TomoTherapy Whole Brain Head & Neck Prostate Lung Summary. HI-ART TomoTherapy System. HI-ART TomoTherapy System
 The Challenges Associated with Differential Dose Delivery using IMRT Chester Ramsey, Ph.D. Director of Medical Physics Thompson Cancer Center Knoxville, Tennessee, U.S.A Collaborators Chester Ramsey, Ph.D.
The Challenges Associated with Differential Dose Delivery using IMRT Chester Ramsey, Ph.D. Director of Medical Physics Thompson Cancer Center Knoxville, Tennessee, U.S.A Collaborators Chester Ramsey, Ph.D.
Citation Key for more information see:
 Citation Key for more information see: http://open.umich.edu/wiki/citationpolicy Use + Share + Adapt { Content the copyright holder, author, or law permits you to use, share and adapt. } Public Domain
Citation Key for more information see: http://open.umich.edu/wiki/citationpolicy Use + Share + Adapt { Content the copyright holder, author, or law permits you to use, share and adapt. } Public Domain
Would SBRT Hypofractionated Approach Be as Good? Then Why Bother With Brachytherapy?
 Would SBRT Hypofractionated Approach Be as Good? Then Why Bother With Brachytherapy? Yasuo Yoshioka, MD Department of Radiation Oncology Osaka University Graduate School of Medicine Osaka, Japan Disclosure
Would SBRT Hypofractionated Approach Be as Good? Then Why Bother With Brachytherapy? Yasuo Yoshioka, MD Department of Radiation Oncology Osaka University Graduate School of Medicine Osaka, Japan Disclosure
Conflict of interest disclosure
 Stereotactic Body Radiation Therapy (SBRT) I: Radiobiology and Clinical Experience Brian Kavanagh, M.D., MPH University of Colorado Eric Chang, M.D. UT MD Anderson Conflict of interest disclosure I have
Stereotactic Body Radiation Therapy (SBRT) I: Radiobiology and Clinical Experience Brian Kavanagh, M.D., MPH University of Colorado Eric Chang, M.D. UT MD Anderson Conflict of interest disclosure I have
Outline. WBRT field. Brain Metastases. Whole Brain RT Prophylactic WBRT Stereotactic radiosurgery (SRS) 1 fraction Stereotactic frame
 1 fraction Stereotactic frame") Radiation Therapy for Advanced NSC Lung Ca Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of California San Francisco
Radiation Therapy for Advanced NSC Lung Ca Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of California San Francisco
Radiotherapy Planning (Contouring Lung Cancer for Radiotherapy dose prescription) Dr Raj K Shrimali
 Dr Raj K Shrimali") Radiotherapy Planning (Contouring Lung Cancer for Radiotherapy dose prescription) Dr Raj K Shrimali Let us keep this simple and stick to some basic rules Patient positioning Must be reproducible Must be
Radiotherapy Planning (Contouring Lung Cancer for Radiotherapy dose prescription) Dr Raj K Shrimali Let us keep this simple and stick to some basic rules Patient positioning Must be reproducible Must be
DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES
 DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES Marco Krengli Radiotherapy, Department of Translational Medicine, University of Piemonte Orientale A. Avogadro THE STANDARD OF CARE
DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES Marco Krengli Radiotherapy, Department of Translational Medicine, University of Piemonte Orientale A. Avogadro THE STANDARD OF CARE
What s New in Radiotherapy For STS of The Extremity? Kaled M. Alektiar, MD, FASTRO Dept of Rad Onc Memorial Sloan Kettering Cancer Center
 What s New in Radiotherapy For STS of The Extremity? Kaled M. Alektiar, MD, FASTRO Dept of Rad Onc Memorial Sloan Kettering Cancer Center Topics Predictive tools for risk assessment Reassessment of dose/volume
What s New in Radiotherapy For STS of The Extremity? Kaled M. Alektiar, MD, FASTRO Dept of Rad Onc Memorial Sloan Kettering Cancer Center Topics Predictive tools for risk assessment Reassessment of dose/volume
Vaginal Sparing with Volumetric Modulated Arc Therapy (VMAT) for Rectal Cancer. Scott Boulet BSc, RT(T)
 for Rectal Cancer. Scott Boulet BSc, RT(T)") Vaginal Sparing with Volumetric Modulated Arc Therapy (VMAT) for Rectal Cancer Scott Boulet BSc, RT(T) Outline Background Objectives Design Results Discussion Conclusion Acknowledgements Questions Background
Vaginal Sparing with Volumetric Modulated Arc Therapy (VMAT) for Rectal Cancer Scott Boulet BSc, RT(T) Outline Background Objectives Design Results Discussion Conclusion Acknowledgements Questions Background
and Strength of Recommendations
 ASTRO with ASCO Qualifying Statements in Bold Italics s patients with T1-2, N0 non-small cell lung cancer who are medically operable? 1A: Patients with stage I NSCLC should be evaluated by a thoracic surgeon,
ASTRO with ASCO Qualifying Statements in Bold Italics s patients with T1-2, N0 non-small cell lung cancer who are medically operable? 1A: Patients with stage I NSCLC should be evaluated by a thoracic surgeon,
FROM ICARO1 TO ICARO2: THE MEDICAL PHYSICS PERSPECTIVE. Geoffrey S. Ibbott, Ph.D. June 20, 2017
 FROM ICARO1 TO ICARO2: THE MEDICAL PHYSICS PERSPECTIVE Geoffrey S. Ibbott, Ph.D. June 20, 2017 1 DISCLOSURES My institution holds Strategic Partnership Research Agreements with Varian, Elekta, and Philips
FROM ICARO1 TO ICARO2: THE MEDICAL PHYSICS PERSPECTIVE Geoffrey S. Ibbott, Ph.D. June 20, 2017 1 DISCLOSURES My institution holds Strategic Partnership Research Agreements with Varian, Elekta, and Philips
Pancreatic Cancer and Radiation Therapy
 Pancreatic Cancer and Radiation Therapy Why? Is there a role for local therapy with radiation in a disease with such a high rate of distant metastases? When? Resectable Disease Is there a role for post-op
Pancreatic Cancer and Radiation Therapy Why? Is there a role for local therapy with radiation in a disease with such a high rate of distant metastases? When? Resectable Disease Is there a role for post-op
Protocol of Radiotherapy for Small Cell Lung Cancer
 107 年 12 月修訂 Protocol of Radiotherapy for Small Cell Lung Cancer Indication of radiotherapy Limited stage: AJCC (8th edition) stage I-III (T any, N any, M0) that can be safely treated with definitive RT
107 年 12 月修訂 Protocol of Radiotherapy for Small Cell Lung Cancer Indication of radiotherapy Limited stage: AJCC (8th edition) stage I-III (T any, N any, M0) that can be safely treated with definitive RT
Principles of radiotherapy and radiochemotherapy. Polgár Cs. 1,2 National Institute of Oncology 1, Chair of Oncology, Semmelweis University 2
 Principles of radiotherapy and radiochemotherapy of malignant tumours Polgár Cs. 1,2 National Institute of Oncology 1, Chair of Oncology, Semmelweis University 2 Multidisciplinary treatment of malignant
Principles of radiotherapy and radiochemotherapy of malignant tumours Polgár Cs. 1,2 National Institute of Oncology 1, Chair of Oncology, Semmelweis University 2 Multidisciplinary treatment of malignant
Evaluation of Monaco treatment planning system for hypofractionated stereotactic volumetric arc radiotherapy of multiple brain metastases
 Evaluation of Monaco treatment planning system for hypofractionated stereotactic volumetric arc radiotherapy of multiple brain metastases CASE STUDY Institution: Odette Cancer Centre Location: Sunnybrook
Evaluation of Monaco treatment planning system for hypofractionated stereotactic volumetric arc radiotherapy of multiple brain metastases CASE STUDY Institution: Odette Cancer Centre Location: Sunnybrook
Protons for Head and Neck Cancer. William M Mendenhall, M.D.
 Protons for Head and Neck Cancer William M Mendenhall, M.D. Protons for Head and Neck Cancer Potential Advantages: Reduce late complications via more conformal dose distributions Likely to be the major
Protons for Head and Neck Cancer William M Mendenhall, M.D. Protons for Head and Neck Cancer Potential Advantages: Reduce late complications via more conformal dose distributions Likely to be the major
Radiation Therapy: From Fallacy to Science
 27 th Annual Management of Colon and Rectal Diseases 2.23.2019 Radiation Therapy: From Fallacy to Science Hadi Zahra, MD, DABR Radiation Oncologist CHI Health Henry Lynch Cancer Center Assistant Clinical
27 th Annual Management of Colon and Rectal Diseases 2.23.2019 Radiation Therapy: From Fallacy to Science Hadi Zahra, MD, DABR Radiation Oncologist CHI Health Henry Lynch Cancer Center Assistant Clinical
Hong Kong Hospital Authority Convention 2018
 Hong Kong Hospital Authority Convention 2018 Stereotactic Radiosurgery in Brain Metastases - Development of the New Treatment Paradigm in HA, Patients Profiles and Their Clinical Outcomes 8 May 2018 Dr
Hong Kong Hospital Authority Convention 2018 Stereotactic Radiosurgery in Brain Metastases - Development of the New Treatment Paradigm in HA, Patients Profiles and Their Clinical Outcomes 8 May 2018 Dr
Clinical outcome of patients treated with re-irradiation for spine or pelvic bone metastasis: A multi-institutional analysis of 98 patients
 MOLECULAR AND CLINICAL ONCOLOGY 6: 871-875, 2017 Clinical outcome of patients treated with re-irradiation for spine or pelvic bone metastasis: A multi-institutional analysis of 98 patients GEN SUZUKI 1,
MOLECULAR AND CLINICAL ONCOLOGY 6: 871-875, 2017 Clinical outcome of patients treated with re-irradiation for spine or pelvic bone metastasis: A multi-institutional analysis of 98 patients GEN SUZUKI 1,
Treatment Planning & IGRT Credentialing for NRG SBRT Trials
 Treatment Planning & IGRT Credentialing for NRG SBRT Trials Hania Al Hallaq, Ph.D. Department of Radiation & Cellular Oncology The University of Chicago Learning Objectives Explain rationale behind credentialing
Treatment Planning & IGRT Credentialing for NRG SBRT Trials Hania Al Hallaq, Ph.D. Department of Radiation & Cellular Oncology The University of Chicago Learning Objectives Explain rationale behind credentialing
The Physics of Oesophageal Cancer Radiotherapy
 The Physics of Oesophageal Cancer Radiotherapy Dr. Philip Wai Radiotherapy Physics Royal Marsden Hospital 1 Contents Brief clinical introduction Imaging and Target definition Dose prescription & patient
The Physics of Oesophageal Cancer Radiotherapy Dr. Philip Wai Radiotherapy Physics Royal Marsden Hospital 1 Contents Brief clinical introduction Imaging and Target definition Dose prescription & patient
Therapy of Non-Operable early stage NSCLC
 SBRT Stage I NSCLC Therapy of Non-Operable early stage NSCLC Dr. Adnan Al-Hebshi MD, FRCR(UK), FRCP(C), ABR King Faisal Specialist Hospital & Research Centre This is our territory Early Stages NSCLC Surgical
SBRT Stage I NSCLC Therapy of Non-Operable early stage NSCLC Dr. Adnan Al-Hebshi MD, FRCR(UK), FRCP(C), ABR King Faisal Specialist Hospital & Research Centre This is our territory Early Stages NSCLC Surgical
ACR Appropriateness Criteria Metastatic Epidural Spinal Cord Compression and Recurrent Spinal Metastasis EVIDENCE TABLE
 . Cole JS, Patchell RA. Metastatic epidural spinal cord compression. Lancet Neurol. 2008;7(5):59-66. 2. Loblaw DA, Mitera G, Ford M, Laperriere NJ. A 20 updated systematic review and clinical practice
. Cole JS, Patchell RA. Metastatic epidural spinal cord compression. Lancet Neurol. 2008;7(5):59-66. 2. Loblaw DA, Mitera G, Ford M, Laperriere NJ. A 20 updated systematic review and clinical practice
Hypofractionated radiation therapy for glioblastoma
 Hypofractionated radiation therapy for glioblastoma Luis Souhami, MD, FASTRO Professor McGill University Department of Oncology, Division of Radiation Oncology Montreal Canada McGill University Health
Hypofractionated radiation therapy for glioblastoma Luis Souhami, MD, FASTRO Professor McGill University Department of Oncology, Division of Radiation Oncology Montreal Canada McGill University Health
Palliative radiotherapy near the end of life for brain metastases from lung cancer: a populationbased
 Palliative radiotherapy near the end of life for brain metastases from lung cancer: a populationbased analysis Roel Schlijper Fellow Radiation Oncology BC Cancer, Prince George Disclosures No conflicts
Palliative radiotherapy near the end of life for brain metastases from lung cancer: a populationbased analysis Roel Schlijper Fellow Radiation Oncology BC Cancer, Prince George Disclosures No conflicts
External Beam Radiation Therapy for Thyroid Cancer
 External Beam Radiation Therapy for Thyroid Cancer C. Jillian Tsai, M.D, PH.D. Assistant Attending Director of Head and Neck Cancer Research Department of Radiation Oncology Memorial Sloan Kettering Cancer
External Beam Radiation Therapy for Thyroid Cancer C. Jillian Tsai, M.D, PH.D. Assistant Attending Director of Head and Neck Cancer Research Department of Radiation Oncology Memorial Sloan Kettering Cancer
Conflicts of Interest
 Dose Constraints to Prevent Radiation-Induced Brachial Plexopathy for Unresectable Lung Cancer Amini A*, Yang J, Williamson R, McBurney ML, Erasmus J, Allen PK, Karhade M, Komaki R, Liao Z, Gomez D, Cox
Dose Constraints to Prevent Radiation-Induced Brachial Plexopathy for Unresectable Lung Cancer Amini A*, Yang J, Williamson R, McBurney ML, Erasmus J, Allen PK, Karhade M, Komaki R, Liao Z, Gomez D, Cox
JMSCR Vol 06 Issue 12 Page December 2018
 www.jmscr.igmpublication.org Impact Factor (SJIF): 6.379 Index Copernicus Value: 79.54 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v6i12.15 Single Institutional Comparative
www.jmscr.igmpublication.org Impact Factor (SJIF): 6.379 Index Copernicus Value: 79.54 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v6i12.15 Single Institutional Comparative
Protocol of Radiotherapy for Head and Neck Cancer
 106 年 12 月修訂 Protocol of Radiotherapy for Head and Neck Cancer Indication of radiotherapy Indication of definitive radiotherapy with or without chemotherapy (1) Resectable, but medically unfit, or high
106 年 12 月修訂 Protocol of Radiotherapy for Head and Neck Cancer Indication of radiotherapy Indication of definitive radiotherapy with or without chemotherapy (1) Resectable, but medically unfit, or high
Carbon Ion Radiotherapy for Skull Base and Paracervical Chordomas
 Carbon Ion Radiotherapy for Skull Base and Paracervical Chordomas Azusa Hasegawa, Jun-etsu Mizoe and Hirohiko Tsujii Research Center Hospital for Charged Particle Therapy National Institute of Radiological
Carbon Ion Radiotherapy for Skull Base and Paracervical Chordomas Azusa Hasegawa, Jun-etsu Mizoe and Hirohiko Tsujii Research Center Hospital for Charged Particle Therapy National Institute of Radiological
Modern Dose Fractionation and Treatment Techniques for Definitive Prostate RT
 Modern Dose Fractionation and Treatment Techniques for Definitive Prostate RT Daniel J Bourgeois, III MD, MPH Board Certified Radiation Oncologist Southeast Louisiana Radiation Oncology Group (SLROG) Disclosures
Modern Dose Fractionation and Treatment Techniques for Definitive Prostate RT Daniel J Bourgeois, III MD, MPH Board Certified Radiation Oncologist Southeast Louisiana Radiation Oncology Group (SLROG) Disclosures
Sacral Chordoma: The Loma Linda University Radiation Medicine Experience. Kevin Yiee MD, MPH Resident Physician
 Sacral Chordoma: The Loma Linda University Radiation Medicine Experience Kevin Yiee MD, MPH Resident Physician What is a chordoma? 1 st chordoma discovered in clivus by Virchow and Luschka 1856 Rare tumor
Sacral Chordoma: The Loma Linda University Radiation Medicine Experience Kevin Yiee MD, MPH Resident Physician What is a chordoma? 1 st chordoma discovered in clivus by Virchow and Luschka 1856 Rare tumor
Impact of pre-treatment symptoms on survival after palliative radiotherapy An improved model to predict prognosis?
 Impact of pre-treatment symptoms on survival after palliative radiotherapy An improved model to predict prognosis? Thomas André Ankill Kämpe 30.05.2016 MED 3950,-5 year thesis Profesjonsstudiet i medisin
Impact of pre-treatment symptoms on survival after palliative radiotherapy An improved model to predict prognosis? Thomas André Ankill Kämpe 30.05.2016 MED 3950,-5 year thesis Profesjonsstudiet i medisin
The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology
 The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology (specifically, lung cancer) 2/10/18 Jeffrey Kittel, MD Radiation Oncology, Aurora St. Luke s Medical Center Outline The history
The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology (specifically, lung cancer) 2/10/18 Jeffrey Kittel, MD Radiation Oncology, Aurora St. Luke s Medical Center Outline The history
Radiation Therapy for Liver Malignancies
 Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
ADJUVANT CHEMOTHERAPY...
 Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
CASE REPORT. Department of Radiology and Radiation Oncology, Nagoya City University Graduate School of Medical Sciences, Nagoya, Japan
 Nagoya J. Med. Sci. 75. 263 ~ 271, 2013 CASE REPORT STEREOTACTIC RADIOTHERAPY FOR SPINAL INTRADURAL METASTASES DEVELOPING WITHIN OR ADJACENT TO THE PREVIOUS IRRADIATION FIELD REPORT OF THREE CASES Yoshimasa
Nagoya J. Med. Sci. 75. 263 ~ 271, 2013 CASE REPORT STEREOTACTIC RADIOTHERAPY FOR SPINAL INTRADURAL METASTASES DEVELOPING WITHIN OR ADJACENT TO THE PREVIOUS IRRADIATION FIELD REPORT OF THREE CASES Yoshimasa
Radiation Therapy in SCLC. What is New? Prof. Dr. Hoda Abdel Baky El Bakry Cairo Cancer Institute Radiation Oncology Department
 Radiation Therapy in SCLC What is New? Prof. Dr. Hoda Abdel Baky El Bakry Cairo Cancer Institute Radiation Oncology Department Background Overview Small Cell Lung cancer constitute about 15 % of all newly
Radiation Therapy in SCLC What is New? Prof. Dr. Hoda Abdel Baky El Bakry Cairo Cancer Institute Radiation Oncology Department Background Overview Small Cell Lung cancer constitute about 15 % of all newly
Old and New Radiation for Bladder and Upper Tract Cancers. Bridget Koontz Radiation Oncology Duke Cancer Institute
 Old and New Radiation for Bladder and Upper Tract Cancers Bridget Koontz Radiation Oncology Duke Cancer Institute Disclosures Janssen funded clinical research BlueEarth Diagnostics advisory board member
Old and New Radiation for Bladder and Upper Tract Cancers Bridget Koontz Radiation Oncology Duke Cancer Institute Disclosures Janssen funded clinical research BlueEarth Diagnostics advisory board member
Accuracy Requirements and Uncertainty Considerations in Radiation Therapy
 Departments of Oncology and Medical Biophysics Accuracy Requirements and Uncertainty Considerations in Radiation Therapy Introduction and Overview 6 August 2013 Jacob (Jake) Van Dyk Conformality 18 16
Departments of Oncology and Medical Biophysics Accuracy Requirements and Uncertainty Considerations in Radiation Therapy Introduction and Overview 6 August 2013 Jacob (Jake) Van Dyk Conformality 18 16
Advances in external beam radiotherapy
 International Conference on Modern Radiotherapy: Advances and Challenges in Radiation Protection of Patients Advances in external beam radiotherapy New techniques, new benefits and new risks Michael Brada
International Conference on Modern Radiotherapy: Advances and Challenges in Radiation Protection of Patients Advances in external beam radiotherapy New techniques, new benefits and new risks Michael Brada
Tecniche Radioterapiche U. Ricardi
 Tecniche Radioterapiche U. Ricardi UNIVERSITA DEGLI STUDI DI TORINO Should we always rely on stage? T4N0M0 Stage IIIB T2N3M0 Early stage NSCLC The treatment of choice for early-stage NSCLC is anatomic
Tecniche Radioterapiche U. Ricardi UNIVERSITA DEGLI STUDI DI TORINO Should we always rely on stage? T4N0M0 Stage IIIB T2N3M0 Early stage NSCLC The treatment of choice for early-stage NSCLC is anatomic
IGRT Solution for the Living Patient and the Dynamic Treatment Problem
 IGRT Solution for the Living Patient and the Dynamic Treatment Problem Lei Dong, Ph.D. Associate Professor Dept. of Radiation Physics University of Texas M. D. Anderson Cancer Center Houston, Texas Learning
IGRT Solution for the Living Patient and the Dynamic Treatment Problem Lei Dong, Ph.D. Associate Professor Dept. of Radiation Physics University of Texas M. D. Anderson Cancer Center Houston, Texas Learning
University of Washington, Radiation Oncology Physics Residency Program. Medical Physics Site Specific Clinical Rotation
 Physics Faculty Mentor: Start date: End Date: Duration: Medical Physics Site Specific Clinical Rotation Meet with mentor(s) every week on?? to review work including readings, journal entries, project development,
Physics Faculty Mentor: Start date: End Date: Duration: Medical Physics Site Specific Clinical Rotation Meet with mentor(s) every week on?? to review work including readings, journal entries, project development,
Hypofractionated Radiotherapy for breast cancer: Updated evidence
 2 rd Bangladesh Breast Cancer Conference, Dhaka, December 2017 Hypofractionated Radiotherapy for breast cancer: Updated evidence Tabassum Wadasadawala Associate Professor of Radiation Oncology Tata Memorial
2 rd Bangladesh Breast Cancer Conference, Dhaka, December 2017 Hypofractionated Radiotherapy for breast cancer: Updated evidence Tabassum Wadasadawala Associate Professor of Radiation Oncology Tata Memorial
Linking DVH-parameters to clinical outcome. Richard Pötter, Medical University of Vienna, General Hospital of Vienna, Austria
 Linking DVH-parameters to clinical outcome Richard Pötter, Medical University of Vienna, General Hospital of Vienna, Austria Outline DVH parameters for HR CTV (D90) and OAR (2 ccm) simple integration of
Linking DVH-parameters to clinical outcome Richard Pötter, Medical University of Vienna, General Hospital of Vienna, Austria Outline DVH parameters for HR CTV (D90) and OAR (2 ccm) simple integration of
Overview of MLC-based Linac Radiosurgery
 SRT I: Comparison of SRT Techniques 1 Overview of MLC-based Linac Radiosurgery Grace Gwe-Ya Kim, Ph.D. DABR 2 MLC based Linac SRS Better conformity for irregular target Improved dose homogeneity inside
SRT I: Comparison of SRT Techniques 1 Overview of MLC-based Linac Radiosurgery Grace Gwe-Ya Kim, Ph.D. DABR 2 MLC based Linac SRS Better conformity for irregular target Improved dose homogeneity inside
A Dosimetric Comparison of Whole-Lung Treatment Techniques. in the Pediatric Population
 A Dosimetric Comparison of Whole-Lung Treatment Techniques in the Pediatric Population Corresponding Author: Christina L. Bosarge, B.S., R.T. (R) (T) Indiana University School of Medicine Department of
A Dosimetric Comparison of Whole-Lung Treatment Techniques in the Pediatric Population Corresponding Author: Christina L. Bosarge, B.S., R.T. (R) (T) Indiana University School of Medicine Department of
HYPERTHERMIA in CERVIX and VAGINA CANCER. J. van der Zee
 HYPERTHERMIA in CERVIX and VAGINA CANCER J. van der Zee ESTRO 2006 Deep hyperthermia in Rotterdam HYPERTHERMIA in CERVIX and VAGINA CANCER ESTRO 2006 Hyperthermia and radiotherapy in primary advanced cervix
HYPERTHERMIA in CERVIX and VAGINA CANCER J. van der Zee ESTRO 2006 Deep hyperthermia in Rotterdam HYPERTHERMIA in CERVIX and VAGINA CANCER ESTRO 2006 Hyperthermia and radiotherapy in primary advanced cervix
Malignant epidural spinal cord compression: the role of external beam radiotherapy
 REVIEW C URRENT OPINION Malignant epidural spinal cord compression: the role of external beam radiotherapy Tanya Holt a, Peter Hoskin b, Ernesto Maranzano c, Arjun Sahgal d, Steven E. Schild e, Samuel
REVIEW C URRENT OPINION Malignant epidural spinal cord compression: the role of external beam radiotherapy Tanya Holt a, Peter Hoskin b, Ernesto Maranzano c, Arjun Sahgal d, Steven E. Schild e, Samuel
It s All About Margins. Maaike Milder, Ph.D. Accuray Symposium April 21 st 2018
 It s All About Margins Maaike Milder, Ph.D. Accuray Symposium April 21 st 2018 Why margins? The smaller the better! Short Introduction Erasmus MC has been using the CyberKnife Robotic Radiosurgery System
It s All About Margins Maaike Milder, Ph.D. Accuray Symposium April 21 st 2018 Why margins? The smaller the better! Short Introduction Erasmus MC has been using the CyberKnife Robotic Radiosurgery System
Radiotherapy for Rectal Cancer. Kevin Palumbo Adelaide Radiotherapy Centre
 Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Corporate Medical Policy
 Corporate Medical Policy Intensity Modulated Radiation Therapy (IMRT) of Head and Neck File Name: Origination: Last CAP Review: Next CAP Review: Last Review: intensity_modulated_radiation_therapy_imrt_of_head_and_neck
Corporate Medical Policy Intensity Modulated Radiation Therapy (IMRT) of Head and Neck File Name: Origination: Last CAP Review: Next CAP Review: Last Review: intensity_modulated_radiation_therapy_imrt_of_head_and_neck