Gastric: 16% 18% 27% Esophageal: 5% 10% 19%
|
|
|
- Barbara Melton
- 5 years ago
- Views:
Transcription
1 2.5% of all cancers Median age 68 years Decline in gastric cancer incidence Increase in esophageal, GEJ, cardia adenocarcinoma OS improvement, , , Gastric: 16% 18% 27% Esophageal: 5% 10% 19%
2 Localised disease
3 Case study-1 WG 71 yrs male. HT, gout, Impaired Glucose tolerance Reflux- 8 cm ulcer on greater curvature- gastric adenoca (>T2, Nx, Mx) CT- GOJ thickening Laparoscopy- no peritoneal/ liver mets ECHO and PFT- normal PET

4
5 (Neo)Adjuvant Therapy in Gastric Cancer ( T2) Improves OS Postoperative RT + chemotherapy (US) [1] Treatment: 5-FU/LV + RT (INT-0116 study) 10% 5-yr OS; HR: 0.76 Postop chemo (Asia): 2 trials, 2000 pts, D2 resection, no RT Treatment: S-1 (oral 5-FU) (ACTS-GC study) [3] 10% 5-yr OS; HR: 0.67 Treatment: postop capecitabine/oxaliplatin (CLASSIC trial) [4] 9% 5-yr OS; HR: 0.66 Preop and postop chemo (UK and French) without RT [2] Treatment: ECF (MAGIC study) or CF 13% 5-yr OS; HR: 0.75 Survival improvements with all approaches similar, modest 1. Smalley SR, et al. J Clin Oncol. 2012;30: Cunningham D, et al. N Engl J Med. 2006;355: Sasako M, et al. J Clin Oncol. 2011;29: Noh SH, et al. Lancet Oncol. 2014;15:
6 Current standard of care
7 36 23
8 Randomised 250 Started 237 Completed 3 cycles 215 Surgery 209/ 83% Post- op 137

9 Surgery Post-op complications similar Evidence of down staging


10

11


12
13


14
15 MAGIC vs Macdonald (CRT) vs Chemo Atlantic divide Advantages of post-op- accurate pathological staging and offering definitive treatment first Advantage of neoadjuvant chemo- testing the biology of tumor and avoiding unnecessary surgery
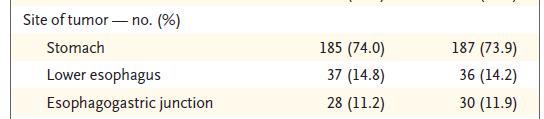
16 Case-2 AP 70 yrs- 5 cm tumor in gastric cardia- type III Laparoscopy and PET- normal ECHO and PFT- normal Hematemesis Total gastrectomy- T3, N2 adenoca Offered post op Macdonald approach? Chemo alone (XELOX)

17 GE junction tumors
18 Esophageal and GEJ Adenocarcinoma: Neoadjuvant chemotherapy alone Preop and postop chemo (UK and French) without RT MAGIC (perioperative ECF): 13% OS at 5 yrs; HR: 0.75 (esophageal, 120 pts), no increase in R0 resection [1] FFCD/FNLC (preop CF): 14% OS at 5 yrs; HR: 0.69 (esophageal cancer, 180 pts) same as MAGIC, no epirubicin, increase in R0 resection [2] 1. Cunningham D, et al. N Engl J Med. 2006;355: Ychou M, et al. J Clin Oncol. 2011;29:
19 Esophageal Adenoca: Neoadjuvant chemo Preop chemotherapy MRC OEO-2 (CF): N = 802 [1] 5-yr update: 6% OS increase vs resection alone US INT-113 (CF): N = 440 [2] No impact on OS or any endpoint, including R0 rate MRC OEO5 (CF vs ECX): N = 900, EUS staged [3] CF x 2 vs ECX x 4: equivalent No survival benefit with additional cycles of ECX Poor rates of R0 resection: 60% to 66% Demonstrates no role for anthracyclines in this setting 1. Allum WH, et al. J Clin Oncol. 2009;27: Kelsen DP, et al. N Engl J Med. 1998;339: Cunningham D, et al. ASCO Abstract 4002.

20 Standard of care- Neoadjuvant CRT


21
22 Preop CRT + Surgery vs Surgery Alone for Esophageal or Junctional Cancer Chemoradiotherapy followed by surgery compared with surgery alone (N = 368) M T W T F S S M T W T F S S M T W T F S S M T W T F S S M T W T F S S Wk 1 Wk 2 Wk 3 Wk 4 Wk 5 XRT CTX Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7 Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7 Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7 Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7 Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7 Paclitaxel 50 mg/m 2 + carboplatin AUC 2 on Days 1, 8, 15, 22, and 29 Concurrent radiotherapy: 41.4 Gy in 23 fractions of 1.8 Gy Surgery within 6 wks after completion of chemoradiotherapy van Hagen P, et al. N Engl J Med. 2012;366:
23 Proportion Surviving Proportion Surviving Preop CRT + Surgery vs Surgery Alone for Esophageal or Junctional Cancer: OS P =.003 OS by Treatment CRT + surgery Surgery alone Mos OS by Tumor Type and Treatment SCC, CRT + surgery AC, CRT + surgery AC, surgery alone SCC, surgery alone 0.2 AC, P =.049 SCC, P = Mos van Hagen P, et al. N Engl J Med. 2012;366: R0 resection increased from 69% w/surgery alone to 92% 5-yr OS: 47% vs 34% with surgery alone Squamous HR: Adeno HR: Pathologic CR with CRT + surgery Squamous: 49% Adenocarcinoma: 23% Considered a new standard of care
24 Case-3 63 yrs with long term reflux Endoscopy- lesion at cm, GOJ at 40 cm CT- distal esophageal tumor, enlarged nodes, liver cyst PET-

25
26 Pre-op chemo vs chemo RT Chemo RT is standard of care Chemo alone approach only when contraindication to RT or hiatus hernia
27 Carbo Paclitaxel (CROSS) vs Cis-FU RT dose different 41.4 vs Gy Toxicity profile
28 DOCTOR trial AdenoCa oesophagus or OG junction Based on PET response i.e. >35% using standard CF chemo Non-responders CF plus Docetaxel OR CF plus Docetaxel plus 45Gy in 25Fr
29 Localised disease but not surgical candidate: Case-4 JW 81 yrs- geriatric assessment- FIT THR, APR for colorectal tumor, HT, AF, T2DM, CAD Endoscopy- lesion at 30 cm- adenoca CT- distal esophageal tumor PET

30


31
32
33 Case-4 JW 81 yrs- geriatric assessment- FIT THR, APR for colorectal tumor, HT, AF, T2DM, CAD Endoscopy- lesion at 30 cm- adenoca CT/ PET- distal esophageal tumor Good lung functions and ECHO treated with definitive Chemo (carbo taxol) RT
34 Role of post op (adjuvant) treatment in Esophageal or GE cancers None Trials with post op chemo or immune therapies
35 Advanced stage disease
36 First-line Therapy Recommendations Preferred regimens* Fluoropyrimidine + cisplatin (category 1) or oxaliplatin (2A) ECF (category 1) Fluorouracil + irinotecan (category 1) HER2-positive disease Trastuzumab + cisplatin/ fluoropyrimidine (category 1) Trastuzumab + other agents (2B) 1. NCCN. Guidelines: gastric cancer. v Other regimens Paclitaxel + cis- or carboplatin (category 2A) Docetaxel with cisplatin (category 2A) Docetaxel + irinotecan (category 2B) Fluoropyrimidine Docetaxel Paclitaxel *2-drug regimens preferred due to lower toxicity, reserving triplet therapy for younger, medically fit pts. Trastuzumab should not be combined with anthracyclines.
37 Advanced Esophagogastric Cancer Chemotherapy: Which Regimen to Use? Oxali: EOX or EOF [1] 3-Drug Regimens Cape: 2-Drug Regimens EOX [1] DCF [2] FOLFIRI [6] [3] XP [4] FLO [5] [7] S-1 ECX or ECF Cis N ORR, % TTP, mo OS, mo Cunningham D, et al. N Engl J Med. 2008;358: Van Cutsem E, et al. J Clin Oncol. 2006;24: Webb A, et al. J Clin Oncol. 1997;15: Kang YK, et al. Ann Oncol. 2009;20: Al-Batran SE, et al. J Clin Oncol. 2008;26: Guimbaud R, et al. J Clin Oncol. 2014;32: Koizumi W, et al. Lancet Oncol. 2008;9:
38
39 REAL-2 Trial: Capecitabine vs 5-FU, Oxaliplatin vs Cisplatin ECF (n = 249) Epirubicin Cisplatin 5-FU EOF (n = 235) Epirubicin Oxaliplatin 5-FU 50 mg/m 2 IV q3w 60 mg/m 2 IV q3w 200 mg/m 2 /d IV given continuously 50 mg/m 2 IV q3w 130 mg/m 2 IV q3w 200 mg/m 2 /d IV given continuously ECX (n = 241) Epirubicin Cisplatin Capecitabine EOX (n = 239) Epirubicin Oxaliplatin Capecitabine 50 mg/m 2 IV q3w 60 mg/m 2 IV q3w 625 mg/m 2 PO BID continuously 50 mg/m 2 IV q3w 130 mg/m 2 IV q3w 625 mg/m 2 PO BID continuously 2 x 2 randomization, 8 cycles Noninferiority of X over F and O over C with 1-yr survival of 35% (1-side α of 5%) Cunningham D, et al. N Engl J Med. 2008;358:36-46.

40
41

42
43 Does Epirubicin Add Anything in Advanced GE Cancer? FOLFIRI vs ECX 1.0 Time to Treatment Failure N = 416 1/3 GEJ, 2/3 gastric TTF (Proportion) Pts at Risk, n ECX FOLFIRI Mos ECX FOLFIRI HR: 0.77 (95% CI: ; P =.008) ORR: 39% vs 38% Median PFS: 5.3 vs 5.8 mos Median OS: 9.5 vs 9.7 mos TTF, toxicity favored first-line FOLFIRI over ECX Guimbaud R, et al. J Clin Oncol. 2014;32:
44 Second-line Therapy Recommendations Depends on prior therapy and PS Preferred regimens (all category 1) Ramucirumab + paclitaxel Docetaxel Paclitaxel Irinotecan Ramucirumab Other regimens Irinotecan and cisplatin (category 2A) Irinotecan and fluoropyrimidine (category 2B) Docetaxel and irinotecan (category 2B) Alternative regimens (category 2B) Mitomycin and irinotecan Mitomycin and fluorouracil NCCN Guidelines: gastric cancer. v
45 Improved OS in Phase III Trials of Second-line Chemo for Gastric Cancer Survival Probability SLC BSC OS (%) Docetaxel Active symptom control HR: 0.67 (95% CI: ; P =.01) Mos Mos From Randomization Docetaxel or Irinotecan vs BSC [1] Docetaxel vs BSC [2] 1. Kang JH, et al. J Clin Oncol. 2012;30: Ford HE, et al. Lancet Oncol. 2014;15:78-86.
46 Genome Atlas Project: Gene Amplification in Esophagogastric Cancer 296 Esophageal/Gastric Cancers; 190 CRCs Focal Events per Sample (n) Number of Focal Events per Sample Amplified genes in 37% of gastroesophageal tumors EGFR MET FGFR1-2 KRAS Targetable receptors and receptor tyrosine kinases Dulak AM, et al. Can Res. 2012;72: *** *** n.s. *** *** Colorectal Gastric Esophageal Multilevel Events per Sample (n) HER2 80 *** 0 3 Amplifications Deletions Multicopy Alterations *** *** * n.s. ** 2 ** 1 0 Multicopy Amplifications Multicopy Deletions
47 Gastric Adenocarcinoma: 4 Genomic Subsets Genomically unstable (50%) Intestinal, present in most GEJ tumors High rate of p53 mutation, amplification of RTKs MSI-high (22%): High rate of microsatellite instability, gene mutation, and promoter hypermethylation Genomically stable (20%) Associated with diffuse histology, CHD-1 and RHOA mutation High Epstein-Barr virus burden (9%) High rate of PIK3CA mutation, PD-L1 and PD-L2 amplification, strong IL-12 signaling indicating an immune presence The Cancer Genome Atlas Research Network. Nature. 2014;513:
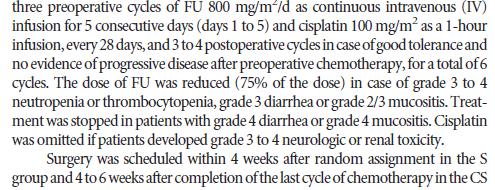
48 Phase III ToGA: Trastuzumab + Chemo in Advanced HER2+ Gastric Cancer Rationale: a subpopulation of gastric cancers overexpress HER2 Stratified by ECOG PS, advanced vs metastatic, gastric vs GEJ, measurable disease, capecitabine vs 5-FU Pts with advanced gastric cancer screened for HER2 status (N = 3803) Pts with HER2+ advanced gastric cancer (n = 810; 22% of successful screenings) R (n = 584) 5-FU or Capecitabine* + Cisplatin 80 mg/m 2 q3w x 6 + Trastuzumab 6 mg/kg q3w until PD (8 mg/kg loading dose) (n = 294) 5-FU or Capecitabine* + Cisplatin 80 mg/m 2 q3w x 6 (n = 290) Primary endpoint: OS *Selected at investigator s discretion: 5-FU 800 mg/m 2 /day infusional on Days 1-5 q3w x 6; capecitabine 1000 mg/m 2 BID on Days 1-14 q3w x 6. Bang YJ, et al. Lancet. 2010;376:
49 Phase III ToGA: OS Survival Probability Pts at Risk, n FC + T FC Mos Median Events, OS, n mos HR % CI P Value.0046 Bang YJ, et al. Lancet. 2010;376:
50 Phase III ToGA: OS in Pts With IHC 3+ or FISH+ and IHC 2+ Survival Probability Pts at Risk, n Exploratory analysis Mos FC + T FC Median Events, OS, n mos HR % CI Bang YJ, et al. Lancet. 2010;376:
51 Phase III LOGiC: CapeOx ± Lapatinib in HER2+ Advanced Gastric Cancer Stratified by prior neo/adjuvant therapy, region (Asia vs North America vs rest of the world) Pts with HER2-amplified locally advanced, unresectable, or metastatic gastric, esophageal, or GEJ cancer (N = 545) CapeOx* + Lapatinib 1250 mg QD 21-day cycles CapeOx* + Placebo *Day 1: oxaliplatin 130 mg/m 2, Days 2-14: capecitabine 850 mg/m 2 BID. Primary endpoint: OS Secondary endpoints: PFS, ORR, DoR, CBR, safety/toxicity, QoL, molecular and pharmacogenetics analyses Hecht J, et al. J Clin Oncol. 2015;[Epub ahead of print].
52 CapeOx ± Lapatinib in HER2+ Advanced Gastric Cancer (LOGiC): OS Cumulative Survival Probability Pts at Risk, n CapeOx + L CapeOx + P CapeOx + L CapeOx + P Mos Since Randomization CapeOx + L (n = 249) CapeOx + P (n = 238) Median OS, Mos (95% CI) 12.2 ( ) 10.5 ( ) HR (95% CI) 0.91 ( ) P = ITT analysis HR: Hecht J, et al. J Clin Oncol. 2015;[Epub ahead of print].
53 Phase III Clinical Trials of HER2-Directed Therapy in Gastric Cancer First line JACOB: capecitabine/cisplatin/trastuzumab ± pertuzumab (planned N = 780) [1] HELOISE: capecitabine/cisplatin + 2 dose levels of trastuzumab (planned N = 400) [2] Second line GATSBY: paclitaxel vs T-DM1 (planned N = 412) [3] T-DM1 was no better than paclitaxel 1. ClinicalTrials.gov. NCT ClinicalTrials.gov. NCT ClinicalTrials.gov. NCT
54 VEGF Revisited?: Second and Later Line of Therapy AVAGAST: capecitabine/cisplatin ± bevacizumab [1] No OS benefit for addition of bevacizumab in first-line setting Small-molecule multitargeted TKI with activity against VEGFR Apatinib- Phase III trial at ASCO 2014: median OS significantly longer with 850 mg QD vs placebo (195 vs 140 days, respectively; HR: 0.71) [2] Regorafenib- Ph II Integrate Study- single agent activity 1. Ohtsu A, et al. J Clin Oncol. 2011;29: Qin S, et al. ASCO Abstract 4003.
55 Phase III REGARD Trial: BSC ± Ramucirumab in Met Gastric or GEJ Cancer Stratified by geographic region, weight loss (> vs < 10% over 3 mos), location of primary tumor (gastric vs GEJ) Pts with metastatic gastric or GEJ adenocarcinoma progressing on first-line platinum- and/or fluoropyrimidinecontaining combination therapy, ECOG PS 0-1 (N = 355) Primary objective: OS Ramucirumab 8 mg/kg IV q2w + BSC (n = 238) BSC + Placebo (n = 117) Treatment until PD, unacceptable toxicity, or death Secondary endpoints: PFS, 12-wk PFS, ORR, DoR, QoL, safety Fuchs CS, et al. Lancet. 2014;383:31-39.
56 BSC ± Ramucirumab in Metastatic Gastric or GEJ Cancer (REGARD): PFS, Response Proportion Without Progression Pts at Risk, n Ramucirumab Placebo Ramucirumab Placebo Censored Ramucirumab Placebo Pts/events 238/ /108 Median, mos 2.1 ( ) 1.3 ( ) (95% CI) 12-wk PFS, % ORR, % 3 3 DCR, % HR: (95% CI: ; P <.0001) Mos Fuchs CS, et al. Lancet. 2014;383:31-39.
57 BSC ± Ramucirumab in Metastatic Gastric or GEJ Cancer (REGARD): OS Proportion Remaining Alive Pts at Risk, n Ramucirumab Placebo Ramucirumab Placebo Pts/events 238/ /99 Median, mos 5.2 ( ) 3.8 ( ) (95% CI) 6-mo OS, % mo OS, % HR: (95% CI: ; P =.0473) Ramucirumab Placebo Censored Mos Fuchs CS, et al. Lancet. 2014;383:31-39.
58 BSC ± Ramucirumab in Metastatic Gastric or GEJ Cancer (REGARD): AEs of Interest AE, % Ramucirumab (n = 236) Placebo (n = 115) Any Grade Grade 3 Any Grade Grade 3 Hypertension* Bleeding/hemorrhage Arteriothromboembolic Venous thromboembolic Proteinuria 3 < 1 < 3 < 0 GI perforation < 1 < 1 < 1 < 1 Fistula (GI and non-gi) < 1 < 1 < 1 < 1 Infusion-related reaction < Cardiac failure < *Includes increased blood pressure. No grade 4 hypertension observed among ramucirumab-treated pts. Fuchs CS, et al. Lancet. 2014;383:31-39.
59 Randomized Second-line Gastric Cancer Studies ( ): Median OS Median OS by Study Arm, Mos Ramucirumab vs BSC [1] (n = 355) Docetaxel vs ASC [2] (n = 131) Chemo (docetaxel or irinotecan) vs BSC [3] (n = 202) Irinotecan vs BSC [4] (n = 40) Fuchs CS, et al. Lancet. 2014;383: Ford H, et al. ASCO GI Abstract LBA4. 3. Kang JH, et al. J Clin Oncol. 2012;30: Thuss-Patience PC, et al. Eur J Cancer. 2011;47: Active treatment BSC/ASC
60 RAINBOW: Second-line Paclitaxel ± Ramucirumab in Advanced Gastric Cancer Randomized, double-blind phase III trial Stratified by geographic region, measurable vs nonmeasurable disease, TTP on first-line therapy (< 6 vs 6 mos) 4-wk cycle Pts with metastatic or locally adv unresectable gastric or GEJ cancer and progression on first-line chemo* (N = 665) *Platinum agent plus fluoropyrimidine ± anthracycline. Ramucirumab 8 mg/kg Days 1, 15 + Paclitaxel 80 mg/m 2 Days 1, 8, 15 (n = 330) Placebo Days 1, 15 + Paclitaxel 80 mg/m 2 Days 1, 8, 15 (n = 335) Treat until PD or intolerable toxicity Primary endpoint: OS Secondary endpoints: PFS, ORR, TTP Wilke H, et al. Lancet Oncol. 2014;15:
61 2 nd -Line Ramucirumab in Advanced Gastric Cancer (RAINBOW): OS 1.0 RAINBOW [1] REGARD [2] Ram/Pac Placebo/Pac Ram Probability of OS Δ mos = 2.3 mos Pts/events, n 330/ / /199 Median, mos 9.63 ( ) 7.38 ( ) 5.2 ( ) (95% CI) 6-mo OS, % mo OS, % HR: (95% CI: ; P =.0169) 0.2 Ram + Pac Placebo + Pac Censored Mos 1. Wilke H, et al. Lancet Oncol. 2014;15: Fuchs CS, et al. Lancet. 2014;383:31-39.
62 Second-line Ramucirumab in Adv Gastric Cancer (RAINBOW): PFS, Responses Probability of PFS Ram + Pac Placebo + Pac Censored RAINBOW [1] REGARD [2] Ram/Pac Placebo/Pac Ram Pts/events, n 330/ / /199 Median, mos 4.40 ( ) 2.86 ( ) 2.1 ( ) (95% CI) 6-mo PFS, % mo PFS, % ORR, % P = DCR, % P < HR: (95% CI: ; P <.0001) Mos 1. Wilke H, et al. Lancet Oncol. 2014;15: Fuchs CS, et al. Lancet. 2014;383:31-39.
63 RAINFALL: Capecitabine/5-FU + Cisplatin ± Ramucirumab in Metastatic Gastric CA Randomized, double-blind, phase III trial Pts with metastatic gastric/gej CA with no prior first-line therapy (N = 616, planned) Ramucirumab 8 mg/kg IV Days 1, 8 Capecitabine* 1000 mg/m 2 PO Days 1-14 Cisplatin 80 mg/m 2 IV Day 1 Placebo IV Days 1, 8 Capecitabine* 1000 mg/m 2 PO Days 1-14 Cisplatin 80 mg/m 2 IV Day 1 21-day cycles Primary endpoint: PFS *Pts unable to take capecitabine receive 5-FU 800 mg/m 2 /day Days 1-5. Secondary endpoints: OS, PFS2, ORR, DCR, TTP, DoR, QoL, PK ClinicalTrials.gov. NCT
64 Phase III Trials in Gastric Cancer: EGFR-Targeted Agents REAL3: ECX ± panitumumab (UK) [1] Negative: panitumumab had inferior outcomes EXPAND: capecitabine/cisplatin ± cetuximab (EU) [2] Negative: cetuximab trended inferior COG: BSC vs gefitinib (UK): negative [3] Trials conducted with no biomarker selection of pts No biomarker identified in esophagogastric cancer 1. Waddell T, et al. Lancet Oncol. 2013;14: Lordick F, et al. Lancet Oncol. 2013;14: Dutton SJ, et al. Lancet Oncol. 2014;15:
65 cmet Antibodies in Gastric Cancer: Phase III Trials RILOMET-1 [1] Locally advanced or metastatic gastric and AEG Cancer, METpositive by immunohistochemistry (IHC) HER2 negative Primary endpoint: OS MetGastric [2] Locally advanced or metastatic gastric and AEG Cancer, METpositive by immunohistochemistry (IHC) HER2 negative R N = 450 R N = 800 ECX + Rilotumumab 1:1 ECX alone ECX + Rilotumumab 1:1 ECX alone Primary endpoint: OS in the Met IHC 2+/3+ pt subgroup 1. ClinicalTrials.gov. NCT ClinicalTrials.gov. NCT
66 CTLA-4 and PD-1/L1 Checkpoint Blockade Priming phase (lymph node) Effector phase (peripheral tissue) Dendritic cell T cell T-cell migration T cell Cancer cell MHC TCR TCR MHC Dendritic cell B7 CD28 CTLA-4 T cell T cell PD-1 PD-L1 Cancer cell Ribas A. N Engl J Med. 2012;366:
67 Immune Checkpoint Inhibitors in Esophagogastric Carcinoma CTLA-4 Tremelimumab: phase II study (N = 18) showed 1 PR > 30 mos [1] PD-L1 Atezolizumab: 1 gastric cancer pt in expansion study had TTP of 9.8 mos [2] Durvalumab: dose-expansion study (N = 28) showed 2 PRs and 12- wk DCR of 25% [3] PD-1 Pembrolizumab: KEYNOTE-012: ORR 22% to 33%; 53% of pts had reduction in size of target lesions [4] 1. Ralph C, et al. Clin Cancer Res. 2010;16: Tabernero J, et al. ASCO Abstract Segal D, et al. ESMO Abstract 1058PD. 4. Bang YJ, et al. ASCO Abstract 4001.
68 KEYNOTE-012: Pembrolizumab in Gastric Cancer Cohort Multicenter, multicohort open-label phase Ib trial Pts with PD-L1 positive recurrent or metastatic adenocarcinoma of the stomach or gastroesophageal junction; ECOG PS 0-1; no active brain metastases (N = 39) Pembrolizumab 10 mg/kg IV q2w CR Confirmed PD PR, SD Discontinue treatment Pembrolizumab 10 mg/kg IV q2w for 24 mos or until progression or intolerable toxicity Discontinue treatment Endpoints: association of clinical response with PD-L1 expression Assessment of response every 8 wks by RECIST v1.1 Assessment of PD-L1 expression by IHC Bang YJ, et al. ASCO Abstract 4001.
69 Pembrolizumab in Gastric Cancer Cohort (KEYNOTE-012): Responses Pembrolizumab therapy associated with PR in 13 of 39 pts by investigator review and 8 of 36 pts by central review 53% of pts had decrease in lesion size Median time to response: 8 wks 4 of 8 responses ongoing at time of data cutoff Outcomes Investigator Review (n = 39) Central Review (n = 36) 33 (19-50) 22 (10-39) CR 0 0 PR 13 (33) 8 (22) SD 3 (8) 5 (14) PD 23 (59) 19 (53) No assessment 0 1 (3) Not determined 0 3 (8) Response ORR, % (95% CI) Best response, n (%) Median response duration: 40 wks (range: 20+ to 48+) Bang YJ, et al. ASCO Abstract 4001.
70 Pembrolizumab in Gastric Cancer Cohort (KEYNOTE-012): Change in Tumor Size Change From Baseline in Sum of Longest Diameter of Target Lesion (%) Maximum Percentage Change From Baseline in Tumor Size (RECIST v1.1, Central Review) % of pts experienced a decrease in target lesions Bang YJ, et al. ASCO Abstract 4001.
71 Immune Checkpoint Inhibitors in Adv. Gastric CA: Ongoing Clinical Trials Checkpoint Agent Trial Details NCT Number CTLA-4 Ipilimumab Ph II maintenance ipi NCT PD-1 PD-L1 Combo Pembrolizumab Pembrolizumab Pembrolizumab Avelumab KEYNOTE-061: Ph III 2nd-line pembro vs paclitaxel KEYNOTE-062: Ph III first-line pembro monotherapy KEYNOTE-059: Ph II pembro vs pembro+ cis/5-fu Ph III avelumab vs continuation of first-line chemo NCT NCT NCT NCT Avelumab Ph III avelumab vs chemo, 3rd-line NCT Tremelimumab + durvalumab Nivolumab + ipilimumab Ph Ib/II tremelimumab + durvalumab vs treme vs durvalumab Ph I/II nivolumab vs nivo/ipi NCT NCT
72 Advanced Esophageal cancer TROG 03.01/ NCI CTG ES2- Dr Penniment et al RT vs Chemo RT (1 cycle cisplatin and FU) No advantage for adding chemo for palliation of dysphagia
73 Take Home Messages Current adjuvant therapy achieves a limited survival improvement Both perioperative and postoperative chemotherapy improve survival Postoperative RT + chemotherapy needed for < D1 resection Preoperative chemotherapy + RT SOC for GEJ and esophageal cancer Metastatic disease Fluorinated pyrimidine + platinum agent (standard chemo): FOLFOX, CAPOX, capecitabine/cisplatin Positive trials for VEGFR2 inhibitors as second-line therapy Ramucirumab improves outcome alone and with paclitaxel Failed trials targeting EGFR, MET HER2+: trastuzumab added to first-line chemo Immunotherapy trials ongoing
74 Localised disease Gastric/GE Esophageal/GE ECF peri-op Neo adj CRT Post op CRT Pre-op Chemo
75 Metastatic disease Cis FU/ FOLFOX/ FOLFIRI/ XP/ XELOX/ ECF/ ECX/ EOX/ ±Herceptin Paclitaxel/ docetaxel/ irinotecan/ ramucirumab Irinotecan/ pembro
PCPA Advanced Trainee Program Upper GI Cancers. Dr N Singhal Medical Oncologist Royal Adelaide Hospital
 Upper GI Cancers Dr N Singhal Medical Oncologist Royal Adelaide Hospital Localised disease PCPA Advanced Trainee Program 2018 Submucosal PCPA Advanced Trainee Program 2018 Work up EUS- 90% sensitivity
Upper GI Cancers Dr N Singhal Medical Oncologist Royal Adelaide Hospital Localised disease PCPA Advanced Trainee Program 2018 Submucosal PCPA Advanced Trainee Program 2018 Work up EUS- 90% sensitivity
NOVITA IN TEMA DI CARCINOMA GASTRICO ROSA BERENATO
 NOVITA IN TEMA DI CARCINOMA GASTRICO ROSA BERENATO ONCOLOGIA MEDICA 1 FONDAZIONE IRCCS ISTITUTO NAZIONALE DEI TUMORI MILANO PROGRESS AGAINST METASTATIC GC OS in first-line palliative setting Little progress
NOVITA IN TEMA DI CARCINOMA GASTRICO ROSA BERENATO ONCOLOGIA MEDICA 1 FONDAZIONE IRCCS ISTITUTO NAZIONALE DEI TUMORI MILANO PROGRESS AGAINST METASTATIC GC OS in first-line palliative setting Little progress
Updated Apr 2017 by Dr. Ko (Medical Oncologist, Abbotsford Cancer Centre)
") Metastatic Esophagogastric Cancer Summary Updated Apr 2017 by Dr. Ko (Medical Oncologist, Abbotsford Cancer Centre) Reviewed by Dr. Yoo-Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer Centre, University
Metastatic Esophagogastric Cancer Summary Updated Apr 2017 by Dr. Ko (Medical Oncologist, Abbotsford Cancer Centre) Reviewed by Dr. Yoo-Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer Centre, University
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
Updates and best practices in the management of gastric cancer
 Updates and best practices in the management of gastric cancer Olatunji B. Alese, MD Gastrointestinal Oncology, Winship Cancer Institute of Emory University July 28, 2017 1 Incidence 3rd leading cause
Updates and best practices in the management of gastric cancer Olatunji B. Alese, MD Gastrointestinal Oncology, Winship Cancer Institute of Emory University July 28, 2017 1 Incidence 3rd leading cause
Current standards of care in gastric cancer
 Current standards of care in gastric cancer Prof Eric Van Cutsem, MD, PhD Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be Outline Resectable gastric cancer: the role of neoadjuvant and adjuvant
Current standards of care in gastric cancer Prof Eric Van Cutsem, MD, PhD Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be Outline Resectable gastric cancer: the role of neoadjuvant and adjuvant
Getting to the Bottom of Treatment: An Update in the Management of Esophagogastric Cancers
 Getting to the Bottom of Treatment: An Update in the Management of Esophagogastric Cancers Disclosures None Cindy L. O Bryant, PharmD, BCOP, FCCP, FHOPA Professor, University of Colorado Skaggs School
Getting to the Bottom of Treatment: An Update in the Management of Esophagogastric Cancers Disclosures None Cindy L. O Bryant, PharmD, BCOP, FCCP, FHOPA Professor, University of Colorado Skaggs School
Chemotherapy for Advanced Gastric Cancer
 Chemotherapy for Advanced Gastric Cancer Andrés Cervantes Professor of Medicine DISCLOSURE OF INTEREST Employment: None Consultant or Advisory Role: Merck Serono, Roche, Beigene, Bayer, Servier, Lilly,
Chemotherapy for Advanced Gastric Cancer Andrés Cervantes Professor of Medicine DISCLOSURE OF INTEREST Employment: None Consultant or Advisory Role: Merck Serono, Roche, Beigene, Bayer, Servier, Lilly,
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
Systemic treatment in early and advanced gastric cancer
 Systemic treatment in early and advanced gastric cancer Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer n Surgical resection n Pathology assessment and estimation
Systemic treatment in early and advanced gastric cancer Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer n Surgical resection n Pathology assessment and estimation
Medicinae Doctoris. One university. Many futures.
 Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Management of advanced Gastric Cancer in the era of targeted therapy
 Management of advanced Gastric Cancer in the era of targeted therapy Osman M.Mansour Prof. Medical Oncology, NCI, Cairo University BGO: 28-3 October 215 Gastric Cancer: A Significant Problem in Some Countries
Management of advanced Gastric Cancer in the era of targeted therapy Osman M.Mansour Prof. Medical Oncology, NCI, Cairo University BGO: 28-3 October 215 Gastric Cancer: A Significant Problem in Some Countries
Perioperative chemotherapy: individualized therapy or same treatment for all? Prof. Dr. med. Salah-Eddin Al-Batran
 Perioperative chemotherapy: individualized therapy or same treatment for all? Prof. Dr. med. Salah-Eddin Al-Batran Institute of Clinical Cancer Research Krankenhaus Nordwest UCT - University Cancer Center
Perioperative chemotherapy: individualized therapy or same treatment for all? Prof. Dr. med. Salah-Eddin Al-Batran Institute of Clinical Cancer Research Krankenhaus Nordwest UCT - University Cancer Center
Advances in gastric cancer: Biology and Treatment for advanced disease
 Advances in gastric cancer: Biology and Treatment for advanced disease Andrés Cervantes Professor of Medicine Outline Molecular classification Pathology Classification after gene expression The Cancer
Advances in gastric cancer: Biology and Treatment for advanced disease Andrés Cervantes Professor of Medicine Outline Molecular classification Pathology Classification after gene expression The Cancer
Which Treatment Approach is Most Appropriate for Primary Therapy of Gastric Cancer: Neoadjuvant Chemotherapy
 Which Treatment Approach is Most Appropriate for Primary Therapy of Gastric Cancer: Neoadjuvant Chemotherapy Joseph Chao, M.D. Assistant Clinical Professor Department of Medical Oncology & Therapeutics
Which Treatment Approach is Most Appropriate for Primary Therapy of Gastric Cancer: Neoadjuvant Chemotherapy Joseph Chao, M.D. Assistant Clinical Professor Department of Medical Oncology & Therapeutics
New experimental targets for gastric cancer Andrés Cervantes
 New experimental targets for gastric cancer Andrés Cervantes Professor of Medicine Outline Acquired capabilities of Cancer IGFR pathway PI3K-AKT-m-TOR pathway MET pathway FGFR pathway Check point inhibitors
New experimental targets for gastric cancer Andrés Cervantes Professor of Medicine Outline Acquired capabilities of Cancer IGFR pathway PI3K-AKT-m-TOR pathway MET pathway FGFR pathway Check point inhibitors
BIOLOGICAL TARGETED AGENTS
 BIOLOGICAL TARGETED AGENTS (INCLUDING HER2, EGFR, ANGIOGENESIS) Dr Elizabeth Smyth Royal Marsden Hospital ESMO GI Cancer Preceptorship Singapore 2017 DISCLOSURES Honoraria for advisory role Five Prime
BIOLOGICAL TARGETED AGENTS (INCLUDING HER2, EGFR, ANGIOGENESIS) Dr Elizabeth Smyth Royal Marsden Hospital ESMO GI Cancer Preceptorship Singapore 2017 DISCLOSURES Honoraria for advisory role Five Prime
Current Standard of Care of Gastric Cancer:
 Current Standard of Care of Gastric Cancer: Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer Surgical resection Pathology assessment and estimation of risk Treatment
Current Standard of Care of Gastric Cancer: Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer Surgical resection Pathology assessment and estimation of risk Treatment
Neo- and adjuvant treatment for gastric cancer: The role of chemotherapy
 Anna Dorothea Wagner, PD & MER Department of Oncology University of Lausanne Neo- and adjuvant treatment for gastric cancer: The role of chemotherapy Structure 1. Background and overview 2. Adjuvant chemotherapy:
Anna Dorothea Wagner, PD & MER Department of Oncology University of Lausanne Neo- and adjuvant treatment for gastric cancer: The role of chemotherapy Structure 1. Background and overview 2. Adjuvant chemotherapy:
Highlights STOMACH CANCER
 UPDATES and NEWS from the Gastrointestinal Cancers Symposium in San Francisco Roma, 10-11 Febbraio 2017 Highlights STOMACH CANCER Lorenzo Fornaro, MD Unit of Medical Oncology 2 Azienda Ospedaliero-Universitaria
UPDATES and NEWS from the Gastrointestinal Cancers Symposium in San Francisco Roma, 10-11 Febbraio 2017 Highlights STOMACH CANCER Lorenzo Fornaro, MD Unit of Medical Oncology 2 Azienda Ospedaliero-Universitaria
Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
 Efficacy Results from the ToGA Trial: A Phase III Study of Trastuzumab Added to Standard Chemotherapy in First-Line HER2- Positive Advanced Gastric Cancer Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
Efficacy Results from the ToGA Trial: A Phase III Study of Trastuzumab Added to Standard Chemotherapy in First-Line HER2- Positive Advanced Gastric Cancer Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS
 IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Cambridge University Hospitals NHS Foundation Trust ESMO Gastric Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Cambridge University Hospitals NHS Foundation Trust ESMO Gastric Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role
ESMO 2017, Madrid, Spain Dr. Loredana Vecchione Charite Comprehensive Cancer Center, Berlin HIGHLIGHTS ON CANCERS OF THE UPPER GI TRACT
 ESMO 2017, Madrid, Spain Dr. Loredana Vecchione Charite Comprehensive Cancer Center, Berlin HIGHLIGHTS ON CANCERS OF THE UPPER GI TRACT DOCETAXEL, OXALIPLATIN AND FLUOROURACIL/LEUCOVORIN (FLOT) FOR RESECTABLE
ESMO 2017, Madrid, Spain Dr. Loredana Vecchione Charite Comprehensive Cancer Center, Berlin HIGHLIGHTS ON CANCERS OF THE UPPER GI TRACT DOCETAXEL, OXALIPLATIN AND FLUOROURACIL/LEUCOVORIN (FLOT) FOR RESECTABLE
Current Standard of Care of Gastro- Esophageal Cancer
 Current Standard of Care of Gastro- Esophageal Cancer Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer Surgical resection Pathology assessment and estimation of risk
Current Standard of Care of Gastro- Esophageal Cancer Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer Surgical resection Pathology assessment and estimation of risk
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Esophageal and GEJ Cancers. Case Presentations
 Esophageal and GEJ Cancers Case Presentations Locally Advanced GEJ Cancer (Case 1) A 55 year old man with longstanding GERD presents with increasing solid food dysphagia. EGD reveals a 3 cm mass in the
Esophageal and GEJ Cancers Case Presentations Locally Advanced GEJ Cancer (Case 1) A 55 year old man with longstanding GERD presents with increasing solid food dysphagia. EGD reveals a 3 cm mass in the
Neo- and adjuvant treatment for gastric cancer: The role of chemotherapy
 Neo- and adjuvant treatment for gastric cancer: The role of chemotherapy Priv. Doz. Dr. Dr. med. T.O. Götze Institute of Clinical Cancer Research Director: Prof. Dr. S.-E. Al- Batran University Cancer
Neo- and adjuvant treatment for gastric cancer: The role of chemotherapy Priv. Doz. Dr. Dr. med. T.O. Götze Institute of Clinical Cancer Research Director: Prof. Dr. S.-E. Al- Batran University Cancer
ASCO 2017 updates in Colorectal and Gastric Cancers. May Cho, M.D.
 ASCO 2017 updates in Colorectal and Gastric Cancers May Cho, M.D. Relevant financial relationships in the past twelve months by presenter or spouse/partner: None The speaker will directly disclosure the
ASCO 2017 updates in Colorectal and Gastric Cancers May Cho, M.D. Relevant financial relationships in the past twelve months by presenter or spouse/partner: None The speaker will directly disclosure the
Concept to Practice: New Advances in the Treatment of GI Cancers
 Concept to Practice: New Advances in the Treatment of GI Cancers 2016 Community Oncology Alliance Conference Orlando, FL Thomas George, MD, FACP Director, GI Oncology Program Director, Experimental Therapeutics
Concept to Practice: New Advances in the Treatment of GI Cancers 2016 Community Oncology Alliance Conference Orlando, FL Thomas George, MD, FACP Director, GI Oncology Program Director, Experimental Therapeutics
CHEMOTHERAPY FOR METASTATIC GASTRIC CANCER
 CHEMOTHERAPY FOR METASTATIC GASTRIC CANCER Dr Elizabeth Smyth Royal Marsden, UK ESMO Gastric Cancer Preceptorship Valencia 2017 IMPORTANT CONSIDERATIONS WHEN TREATING ADVANCED GASTRIC CANCER Short OS Pain
CHEMOTHERAPY FOR METASTATIC GASTRIC CANCER Dr Elizabeth Smyth Royal Marsden, UK ESMO Gastric Cancer Preceptorship Valencia 2017 IMPORTANT CONSIDERATIONS WHEN TREATING ADVANCED GASTRIC CANCER Short OS Pain
Upper Gastrointestinal Cancers in the Elderly. Choo Su Pin Senior Consultant Medical Oncology National Cancer Centre Singapore
 Upper Gastrointestinal Cancers in the Elderly Choo Su Pin Senior Consultant Medical Oncology National Cancer Centre Singapore Gastric Cancer --High Global Burden Global Cancer Deaths % of all cancer (2008)
Upper Gastrointestinal Cancers in the Elderly Choo Su Pin Senior Consultant Medical Oncology National Cancer Centre Singapore Gastric Cancer --High Global Burden Global Cancer Deaths % of all cancer (2008)
Immunotherapy for the Treatment of Head and Neck Cancers. Barbara Burtness, MD Yale University
 Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Targeted Therapies in Gastric Cancer : Where Do We Stand Today. Yoon-Koo Kang Asan Medical Center, University of Ulsan Seoul, Korea
 Targeted Therapies in Gastric Cancer : Where Do We Stand Today Yoon-Koo Kang Asan Medical Center, University of Ulsan Seoul, Korea Chemotherapy is the standard of care in advanced gastric cancer Median
Targeted Therapies in Gastric Cancer : Where Do We Stand Today Yoon-Koo Kang Asan Medical Center, University of Ulsan Seoul, Korea Chemotherapy is the standard of care in advanced gastric cancer Median
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Immunotherapy for the Treatment of Head and Neck Cancers. Robert F. Taylor, MD Aurora Health Care
 Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Resectable locally advanced oesophagogastric cancer
 Resectable locally advanced oesophagogastric cancer Clinical Case Discussion Florian Lordick University Cancer Center Leipzig University Clinic Leipzig Leipzig, Germany esmo.org DISCLOSURES Honoraria for
Resectable locally advanced oesophagogastric cancer Clinical Case Discussion Florian Lordick University Cancer Center Leipzig University Clinic Leipzig Leipzig, Germany esmo.org DISCLOSURES Honoraria for
Conflicts of Interest GI Malignancies: An Update on Current Treatment Options
 Conflicts of Interest GI Malignancies: An Update on Current Treatment Options Nothing to disclose Trevor McKibbin, PharmD, MS, BCOP Clinical Specialist, Hematology/Oncology Winship Cancer Institute of
Conflicts of Interest GI Malignancies: An Update on Current Treatment Options Nothing to disclose Trevor McKibbin, PharmD, MS, BCOP Clinical Specialist, Hematology/Oncology Winship Cancer Institute of
The role of chemoradiotherapy in GE junction and gastric cancer. Karin Haustermans
 The role of chemoradiotherapy in GE junction and gastric cancer Karin Haustermans Overview Postoperative chemoradiotherapy Preoperative chemoradiotherapy Palliative radiation Technical aspects Overview
The role of chemoradiotherapy in GE junction and gastric cancer Karin Haustermans Overview Postoperative chemoradiotherapy Preoperative chemoradiotherapy Palliative radiation Technical aspects Overview
Chemotherapy for metastatic gastric cancer
 ESMO Asia GI Preceptorship 2018 Chemotherapy for metastatic gastric cancer Sun Young Rha, MD, PhD Yonsei Cancer Center, Institute for Cancer Research, Yonsei University College of Medicine Disclosures
ESMO Asia GI Preceptorship 2018 Chemotherapy for metastatic gastric cancer Sun Young Rha, MD, PhD Yonsei Cancer Center, Institute for Cancer Research, Yonsei University College of Medicine Disclosures
Jonathan Dickinson, LCL Xeloda
 Xeloda A blockbuster in the making Jonathan Dickinson, LCL Xeloda Xeloda unique tumor-activated mechanism Delivering more cancer-killing agent straight into cancer Highly effective comparable efficacy
Xeloda A blockbuster in the making Jonathan Dickinson, LCL Xeloda Xeloda unique tumor-activated mechanism Delivering more cancer-killing agent straight into cancer Highly effective comparable efficacy
Immunotherapy for Upper GI Cancers
 Immunotherapy for Upper GI Cancers Esophageal Adenocarcinoma GE Junction Adeno Gastric Carcinoma Ahmed Zakari MD Medical Director of GI Cancer Program, Florida Hospital Cancer Institute Associate Professor
Immunotherapy for Upper GI Cancers Esophageal Adenocarcinoma GE Junction Adeno Gastric Carcinoma Ahmed Zakari MD Medical Director of GI Cancer Program, Florida Hospital Cancer Institute Associate Professor
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist
 Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
ESMO Preceptorship Targeted Therapy for Gastric Cancer
 ESMO Preceptorship Targeted Therapy for Gastric Cancer Professor Dr. Florian Lordick Professor of Oncology Director University Cancer Center Leipzig (UCCL) Disclosure Florian Lordick declares honoraria
ESMO Preceptorship Targeted Therapy for Gastric Cancer Professor Dr. Florian Lordick Professor of Oncology Director University Cancer Center Leipzig (UCCL) Disclosure Florian Lordick declares honoraria
Immunotherapy for Breast Cancer. Aurelio B. Castrellon Medical Oncology Memorial Healthcare System
 Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Targeted Therapies in Metastatic Colorectal Cancer: An Update
 Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
(Neo-) adjuvant Treatment of Gastric Cancer. - The European View
 adjuvant Treatment of Gastric Cancer. - The European View") (Neo-) adjuvant Treatment of Gastric Cancer - The European View Florian Lordick, MD Professor of Oncology Director of the University Cancer Center Leipzig (UCCL) University of Leipzig, Germany My Conflict
(Neo-) adjuvant Treatment of Gastric Cancer - The European View Florian Lordick, MD Professor of Oncology Director of the University Cancer Center Leipzig (UCCL) University of Leipzig, Germany My Conflict
Ca Cardias e Stomaco: le diversita e le terapie
 XXII Riunione Nazionale I.T.M.O. Ca Cardias e Stomaco: le diversita e le terapie Maria Di Bartolomeo s.s. Oncologia Medica Gastroenterologica Fondazione IRCCS Istituto Nazionale Tumori Milano OUTLINE History
XXII Riunione Nazionale I.T.M.O. Ca Cardias e Stomaco: le diversita e le terapie Maria Di Bartolomeo s.s. Oncologia Medica Gastroenterologica Fondazione IRCCS Istituto Nazionale Tumori Milano OUTLINE History
Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute
 Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute e.smit@nki.nl Evolution of front line therapy in NSCLC unselected pts
Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute e.smit@nki.nl Evolution of front line therapy in NSCLC unselected pts
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr.
 Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
My name is Dr. David Ilson, Professor of Medicine at Memorial Sloan Kettering Cancer Center and Weill Cornell Medical Center in New York, New York.
 Welcome to this CME/CE-certified activity entitled, Integrating the Latest Advances Into Clinical Experience: Data and Expert Insights From the 2016 Meeting on Gastrointestinal Cancers in San Francisco.
Welcome to this CME/CE-certified activity entitled, Integrating the Latest Advances Into Clinical Experience: Data and Expert Insights From the 2016 Meeting on Gastrointestinal Cancers in San Francisco.
CONSIDERATIONS IN DEVELOPMENT OF PEMBROLIZUMAB IN MSI-H CANCERS
 CONSIDERATIONS IN DEVELOPMENT OF PEMBROLIZUMAB IN MSI-H CANCERS December 2017 Christine K. Gause, Ph.D Executive Director, Biostatistics. 2 Microsatellite Instability-High Cancer - USPI KEYTRUDA is indicated
CONSIDERATIONS IN DEVELOPMENT OF PEMBROLIZUMAB IN MSI-H CANCERS December 2017 Christine K. Gause, Ph.D Executive Director, Biostatistics. 2 Microsatellite Instability-High Cancer - USPI KEYTRUDA is indicated
Recent Therapeutic Advances for Thoracic Malignancies
 Recent Therapeutic Advances for Thoracic Malignancies Developed in collaboration Learning Objectives Upon completion, participants should be able to: Interpret new developments in the use of radiation
Recent Therapeutic Advances for Thoracic Malignancies Developed in collaboration Learning Objectives Upon completion, participants should be able to: Interpret new developments in the use of radiation
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Adaptive therapy, for locally advanced gastroesophageal cancers, 447 Adenocarcinoma, emerging novel therapeutic agents for gastroesophageal
Index Note: Page numbers of article titles are in boldface type. A Adaptive therapy, for locally advanced gastroesophageal cancers, 447 Adenocarcinoma, emerging novel therapeutic agents for gastroesophageal
Educational Objectives. Worldwide Incidence. Agenda. Gastric Adenocarcinoma: Risk Factors. Gastric Cancer Statistics
 Educational Objectives Evaluate the current evidence across multiple lines of therapy and appropriately sequence therapies for gastric and gastroesophageal (GEJ) cancers Mitigate toxicities associated
Educational Objectives Evaluate the current evidence across multiple lines of therapy and appropriately sequence therapies for gastric and gastroesophageal (GEJ) cancers Mitigate toxicities associated
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS
 IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Royal Marsden Hospital ESMO Colorectal Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role Servier, Celgene, BMS, Five
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Royal Marsden Hospital ESMO Colorectal Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role Servier, Celgene, BMS, Five
Conversations in Oncology. November Kerry Hotel Pudong, Shanghai China
 Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
GASTRIC & PANCREATIC CANCER
 GASTRIC & PANCREATIC CANCER ASCO HIGHLIGHTS 2005 Fadi Sami Farhat, MD Head of Hematology Oncology Division Hammoud Hospital University Medical Center Saida Lebanon Tel: +961 3 753 155 E-Mail: drfadi@drfadi.org
GASTRIC & PANCREATIC CANCER ASCO HIGHLIGHTS 2005 Fadi Sami Farhat, MD Head of Hematology Oncology Division Hammoud Hospital University Medical Center Saida Lebanon Tel: +961 3 753 155 E-Mail: drfadi@drfadi.org
Gastroesophag Gastroesopha eal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. G. H addock Haddock M.D.
 Gastroesophageal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. Haddock M.D. Mayo Clinic Rochester, MN Locally Advanced GE Junction ACA CT S CT or CT S CT/RT Proposition Chemoradiation
Gastroesophageal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. Haddock M.D. Mayo Clinic Rochester, MN Locally Advanced GE Junction ACA CT S CT or CT S CT/RT Proposition Chemoradiation
Advances in gastric cancer: How to approach localised disease?
 Advances in gastric cancer: How to approach localised disease? Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer Surgical resection Pathology assessment and estimation
Advances in gastric cancer: How to approach localised disease? Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer Surgical resection Pathology assessment and estimation
pan-canadian Oncology Drug Review Final Clinical Guidance Report Ramucirumab (Cyramza) for Gastric Cancer October 29, 2015
 for Gastric Cancer October 29, 2015") pan-canadian Oncology Drug Review Final Clinical Guidance Report Ramucirumab (Cyramza) for Gastric Cancer October 29, 2015 DISCLAIMER Not a Substitute for Professional Advice This report is primarily intended
pan-canadian Oncology Drug Review Final Clinical Guidance Report Ramucirumab (Cyramza) for Gastric Cancer October 29, 2015 DISCLAIMER Not a Substitute for Professional Advice This report is primarily intended
Immunotherapy in Colorectal cancer
 Immunotherapy in Colorectal cancer Ahmed Zakari, MD Associate Professor University of Central Florida, College of Medicine Medical Director, Gastro Intestinal Cancer Program Florida Hospital Cancer Institute
Immunotherapy in Colorectal cancer Ahmed Zakari, MD Associate Professor University of Central Florida, College of Medicine Medical Director, Gastro Intestinal Cancer Program Florida Hospital Cancer Institute
Esophageal and GEJ Adenocarcinoma: Chemo + RT is the Preferred Treatment
 Esophageal and GEJ Adenocarcinoma: Chemo + RT is the Preferred Treatment David H. Ilson, MD, PhD Gastrointestinal Oncology Service Memorial Sloan-Kettering Cancer Center Preop Therapy in Esophageal and
Esophageal and GEJ Adenocarcinoma: Chemo + RT is the Preferred Treatment David H. Ilson, MD, PhD Gastrointestinal Oncology Service Memorial Sloan-Kettering Cancer Center Preop Therapy in Esophageal and
Are we making progress? Marked reduction in operative morbidity and mortality
 Are we making progress? Surgical Progress Marked reduction in operative morbidity and mortality Introduction of Minimal-Access approaches for complex esophageal cancer resections Significantly better functional
Are we making progress? Surgical Progress Marked reduction in operative morbidity and mortality Introduction of Minimal-Access approaches for complex esophageal cancer resections Significantly better functional
Immunotherapies for Advanced NSCLC: Current State of the Field. H. Jack West Swedish Cancer Institute Seattle, Washington
 Immunotherapies for Advanced NSCLC: Current State of the Field H. Jack West Swedish Cancer Institute Seattle, Washington Nivolumab in Squamous NSCLC Chemo-pretreated (1 st line) Adv squamous NSCLC N =
Immunotherapies for Advanced NSCLC: Current State of the Field H. Jack West Swedish Cancer Institute Seattle, Washington Nivolumab in Squamous NSCLC Chemo-pretreated (1 st line) Adv squamous NSCLC N =
Systemic Treatments for Esophagogastric and Pancreas Cancer in the Adjuvant and Metastatic Settings
 Systemic Treatments for Esophagogastric and Pancreas Cancer in the Adjuvant and Metastatic Settings Peter C. Enzinger, MD Dana-Farber Cancer Institute & Harvard Medical School 2017 Master Class Course
Systemic Treatments for Esophagogastric and Pancreas Cancer in the Adjuvant and Metastatic Settings Peter C. Enzinger, MD Dana-Farber Cancer Institute & Harvard Medical School 2017 Master Class Course
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective
 Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Third Line and Beyond: Management of Refractory Colorectal Cancer
 Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer
 Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Immunotherapy in the clinic. Lung Cancer. Marga Majem 20 octubre 2017
 Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents
 Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
EGFR inhibitors in NSCLC
 Suresh S. Ramalingam, MD Associate Professor Director of Medical Oncology Emory University i Winship Cancer Institute EGFR inhibitors in NSCLC Role in 2nd/3 rd line setting Role in first-line and maintenance
Suresh S. Ramalingam, MD Associate Professor Director of Medical Oncology Emory University i Winship Cancer Institute EGFR inhibitors in NSCLC Role in 2nd/3 rd line setting Role in first-line and maintenance
MEETING SUMMARY ESMO 2018, Munich, Germany. Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER
 MEETING SUMMARY ESMO 2018, Munich, Germany Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER DISCLAIMER Please note: The views expressed within this presentation are the personal
MEETING SUMMARY ESMO 2018, Munich, Germany Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER DISCLAIMER Please note: The views expressed within this presentation are the personal
Tumores esófago-gástricos, tiene algo que decir la inmunoterapia? Dr. Fernando Rivera Herrero Hospital Universitario Marqués de Valdecilla.
 Tumores esófago-gástricos, tiene algo que decir la inmunoterapia? Dr. Fernando Rivera Herrero Hospital Universitario Marqués de Valdecilla. Santander Finantial disclosure Consultor: CELGENE Research fundings:
Tumores esófago-gástricos, tiene algo que decir la inmunoterapia? Dr. Fernando Rivera Herrero Hospital Universitario Marqués de Valdecilla. Santander Finantial disclosure Consultor: CELGENE Research fundings:
Objectives. Briefly summarize the current state of colorectal cancer
 Disclaimer I do not have any financial conflicts to disclose. I will not be promoting any service or product. This presentation is not meant to offer medical advice and is not intended to establish a standard
Disclaimer I do not have any financial conflicts to disclose. I will not be promoting any service or product. This presentation is not meant to offer medical advice and is not intended to establish a standard
Karcinom dojke. PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski
 Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
Chemotherapy for resectable liver mets: Options and Issues. Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA
 Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Chemotherapy of colon cancers
 Chemotherapy of colon cancers Stage distribution Stage I : 15% T 1,2 NO Stage IV: 20 25% M+ Stage II : 20 30% T3,4 NO Stage III N+: 30 40% clinical stages I, II, or III colon cancer are at risk for having
Chemotherapy of colon cancers Stage distribution Stage I : 15% T 1,2 NO Stage IV: 20 25% M+ Stage II : 20 30% T3,4 NO Stage III N+: 30 40% clinical stages I, II, or III colon cancer are at risk for having
Colon Cancer Molecular Target Agents
 Colon Cancer Molecular Target Agents Ci Caio Max SR S. Rocha Lima, M.D. MD Professor of Medicine CDi CoDiretor Cl Colorectal tlheptobiliary, Pancreatic SDG, and Phase I Unit University of Miami & Silvester
Colon Cancer Molecular Target Agents Ci Caio Max SR S. Rocha Lima, M.D. MD Professor of Medicine CDi CoDiretor Cl Colorectal tlheptobiliary, Pancreatic SDG, and Phase I Unit University of Miami & Silvester
New Therapies in HCC Bruno Sangro Clínica Universidad de Navarra. IdISNA. CIBERehd. Pamplona, Spain
 New Therapies in HCC Bruno Sangro Clínica Universidad de Navarra. IdISNA. CIBERehd. Pamplona, Spain PHC 2018 - www.aphc.info EASL-EORTC Guidelines EASL EORTC Guidelines. J Hepatol. 2012;56:908-43. Systemic
New Therapies in HCC Bruno Sangro Clínica Universidad de Navarra. IdISNA. CIBERehd. Pamplona, Spain PHC 2018 - www.aphc.info EASL-EORTC Guidelines EASL EORTC Guidelines. J Hepatol. 2012;56:908-43. Systemic
Slide 1. Slide 2 Maintenance Therapy Options. Slide 3. Maintenance Therapy in the Management of Non-Small Cell Lung Cancer. Maintenance Chemotherapy
 Slide 1 Maintenance Therapy in the Management of Non-Small Cell Lung Cancer Frances A Shepherd, MD FRCPC Scott Taylor Chair in Lung Cancer Research Princess Margaret Hospital, Professor of Medicine, University
Slide 1 Maintenance Therapy in the Management of Non-Small Cell Lung Cancer Frances A Shepherd, MD FRCPC Scott Taylor Chair in Lung Cancer Research Princess Margaret Hospital, Professor of Medicine, University
2 nd line Therapy and Beyond NSCLC. Alan Sandler, M.D. Oregon Health & Science University
 2 nd line Therapy and Beyond NSCLC Alan Sandler, M.D. Oregon Health & Science University Treatment options for advanced or metastatic (stage IIIb/IV) NSCLC Suitable for chemotherapy Diagnosis Unsuitable/unwilling
2 nd line Therapy and Beyond NSCLC Alan Sandler, M.D. Oregon Health & Science University Treatment options for advanced or metastatic (stage IIIb/IV) NSCLC Suitable for chemotherapy Diagnosis Unsuitable/unwilling
Does it matter which chemotherapy regimen you partner with the biologic agents?
 Does it matter which chemotherapy regimen you partner with the biologic agents? Yes, it does matter! Axel Grothey Disclosures Research Funding to MAYO Clinic Genentech Bayer Eisai Pfizer Imclone Potential
Does it matter which chemotherapy regimen you partner with the biologic agents? Yes, it does matter! Axel Grothey Disclosures Research Funding to MAYO Clinic Genentech Bayer Eisai Pfizer Imclone Potential
The next wave of successful drug therapy strategies in HER2-positive breast cancer. Hans Wildiers University Hospitals Leuven Belgium
 The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
Addressing Tumor Molecular Heterogeneity using A Novel Clinical Trial Design - PANGEA
 Addressing Tumor Molecular Heterogeneity using A Novel Clinical Trial Design - PANGEA Daniel Catenacci, MD Assistant Professor of Medicine Associate Director GI Oncology Program May 12, 2017 Addressing
Addressing Tumor Molecular Heterogeneity using A Novel Clinical Trial Design - PANGEA Daniel Catenacci, MD Assistant Professor of Medicine Associate Director GI Oncology Program May 12, 2017 Addressing
Incorporating biologics in the management of older patients with metastatic colorectal cancer
 Incorporating biologics in the management of older patients with metastatic colorectal cancer D Papamichael MB BS MD FRCP Cyprus Oncology Centre GSK Satellite Symposium SIOG APAC Singapore 12-13 July 2014
Incorporating biologics in the management of older patients with metastatic colorectal cancer D Papamichael MB BS MD FRCP Cyprus Oncology Centre GSK Satellite Symposium SIOG APAC Singapore 12-13 July 2014
Advances in Systemic Therapy Hepatocellular Carcinoma (HCC) Dr ZEE Ying Kiat HASLD Conference Ho Chi Minh City, 18 December 2016
 Dr ZEE Ying Kiat HASLD Conference Ho Chi Minh City, 18 December 2016") Advances in Systemic Therapy for Hepatocellular Carcinoma (HCC) Dr ZEE Ying Kiat HASLD Conference Ho Chi Minh City, 18 December 2016 Scope Background Staging and treatment strategies Current systemic therapy
Advances in Systemic Therapy for Hepatocellular Carcinoma (HCC) Dr ZEE Ying Kiat HASLD Conference Ho Chi Minh City, 18 December 2016 Scope Background Staging and treatment strategies Current systemic therapy
Weitere Kombinationspartner der Immunotherapie
 1 Weitere Kombinationspartner der Immunotherapie Rolf Stahel University Hospital of Zürich Zürich, 9.12.216 2 Immunotherapy in a multimodality approach NSCLC Advanced disease Checkpoint inhibitors for
1 Weitere Kombinationspartner der Immunotherapie Rolf Stahel University Hospital of Zürich Zürich, 9.12.216 2 Immunotherapy in a multimodality approach NSCLC Advanced disease Checkpoint inhibitors for
2015 EUROPEAN CANCER CONGRESS
 2015 EUROPEAN CANCER CONGRESS 25-29 September 2015 Vienna, Austria SUMMARY The European Cancer Congress (ECC 2015) combined the 40th European Society for Medical Oncology (ESMO) congress with the 18th
2015 EUROPEAN CANCER CONGRESS 25-29 September 2015 Vienna, Austria SUMMARY The European Cancer Congress (ECC 2015) combined the 40th European Society for Medical Oncology (ESMO) congress with the 18th
Immunotherapy for NSCLC: Current State of the Art and Future Directions. H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States
 Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
ADVANCED COLORECTAL CANCER: UNRESECTABLE OR BORDERLINE RESECTABLE (GROUP 1) CHEMOTHERAPY +/- TARGETED AGENTS. Andrés Cervantes. Professor of Medicine
 CHEMOTHERAPY +/- TARGETED AGENTS. Andrés Cervantes. Professor of Medicine") ADVANCED COLORECTAL CANCER: UNRESECTABLE OR BORDERLINE RESECTABLE (GROUP 1) CHEMOTHERAPY +/- TARGETED AGENTS Andrés Cervantes Professor of Medicine 1995 One option Advances in the treatment of mcrc 2000
ADVANCED COLORECTAL CANCER: UNRESECTABLE OR BORDERLINE RESECTABLE (GROUP 1) CHEMOTHERAPY +/- TARGETED AGENTS Andrés Cervantes Professor of Medicine 1995 One option Advances in the treatment of mcrc 2000
Developping the next generation of studies in RCC
 Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
A Giant Leap in the Treatment Options for Advanced Bladder Cancer
 A Giant Leap in the Treatment Options for Advanced Bladder Cancer Yohann Loriot, MD, PhD Department of Cancer Medicine & INSERM U981 Gustave Roussy Villejuif, France Clinical Features of Bladder Cancer
A Giant Leap in the Treatment Options for Advanced Bladder Cancer Yohann Loriot, MD, PhD Department of Cancer Medicine & INSERM U981 Gustave Roussy Villejuif, France Clinical Features of Bladder Cancer
NSCLC: immunotherapy as a first-line treatment. Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To)
") NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer
 Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of California
Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of California
PERIOPERATIVE TREATMENT OF NON SMALL CELL LUNG CANCER. Virginie Westeel Chest Disease Department University Hospital Besançon, France
 PERIOPERATIVE TREATMENT OF NON SMALL CELL LUNG CANCER Virginie Westeel Chest Disease Department University Hospital Besançon, France LEARNING OBJECTIVES 1. To understand the potential of perioperative
PERIOPERATIVE TREATMENT OF NON SMALL CELL LUNG CANCER Virginie Westeel Chest Disease Department University Hospital Besançon, France LEARNING OBJECTIVES 1. To understand the potential of perioperative
Incorporating Immunotherapy into the treatment of NSCLC
 Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
Where Are We with Check-Point Inhibitors in Gastric Cancer?
 21 June 2018, Barcelona Session VII: Metastatic Gastric Cancer Where Are We with Check-Point Inhibitors in Gastric Cancer? Kei Muro, MD. kmuro@aichi-cc.jp Department of Clinical Oncology Aichi Cancer Center
21 June 2018, Barcelona Session VII: Metastatic Gastric Cancer Where Are We with Check-Point Inhibitors in Gastric Cancer? Kei Muro, MD. kmuro@aichi-cc.jp Department of Clinical Oncology Aichi Cancer Center
Out of 129 patients with NSCLC treated with Nivolumab in a phase I trial, the OS rate at 5-y was about 16 %, clearly higher than historical rates.
 6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
Fabienne Warmerdam Zuyderland
 GE Fabienne Warmerdam Zuyderland Disclosure ASCO 2017 travelgrant Pfizer CRC ADJUVANT Less is more? More is More! 1 Less is more? Perspectief INT-0035 stadium III (niets vs 5-FU) 6.5-jaars OS 46% vs. 60%
GE Fabienne Warmerdam Zuyderland Disclosure ASCO 2017 travelgrant Pfizer CRC ADJUVANT Less is more? More is More! 1 Less is more? Perspectief INT-0035 stadium III (niets vs 5-FU) 6.5-jaars OS 46% vs. 60%
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC)
") Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program