Role of Surgery in Management of Non Small Cell Lung Cancer. Dr. Ahmed Bamousa Consultant thoracic surgery Prince Sultan Military Medical City
|
|
|
- Aileen Bryan
- 5 years ago
- Views:
Transcription

1 Role of Surgery in Management of Non Small Cell Lung Cancer Dr. Ahmed Bamousa Consultant thoracic surgery Prince Sultan Military Medical City
2 Introduction Surgical approach Principle and type of surgery Surgery according to stage of the disease Pleural effusion Advance stages Follow up
3 Lung cancer The second most common cancer among both men and women Worldwide, lung cancer occurred in approximately 1.8 million patients in 2012 and caused an estimated 1.6 million deaths 1. In the United States, there will be an estimated 224,000 new cases of lung cancer and 159,000 deaths in Nearly 60% of people diagnosed with lung cancer die within 2 years. This had not improved in 10 years. 1- Brambilla E, Travis WD. Lung cancer. World Cancer Report, World Health Organization, Lyon Cancer statistics. Siegel R, ET AL, Cancer J Clin. 2014;64(1):9
4 2009 Estimated US Cancer Deaths* 30% 9% 9% 6% 4% 4% bile duct 4% Lung & bronchus Prostate Colon & rectum Pancreas Leukemia Liver & intrahepatic Esophagus Men 292,540 Women 269,800 Lung & bronchus 26% Breast 15% Colon & rectum Pancreas Ovary 5% 6% Non-Hodgkin lymphoma 4% 9% 3% Urinary bladder Leukemia 3% Non-Hodgkin 3% lymphoma 3% Kidney & renal pelvis All other sites 25% Uterine corpus 3% Liver & intrahepatic bile duct Brain/ONS 2% 2% 25% All other sites ONS=Other nervous system. Source: American Cancer Society, 2009.
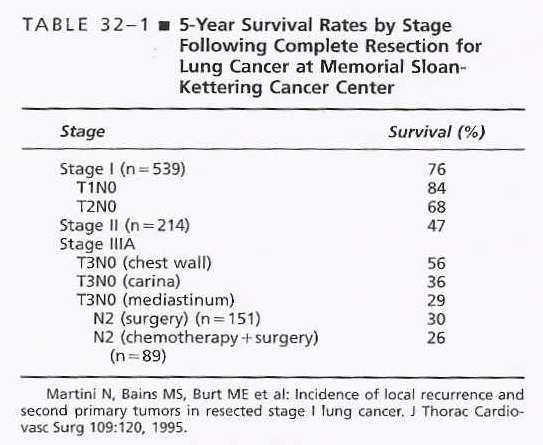
5 INTRODUCTION Surgical resection for lung cancer is still regarded as the most effective method of controlling the primary tumor The median survival is stage dependent - Stage IA ; 95 months - Stage IIIA ; 19 month
6
7

8
9 Surgical Approach Diagnosis: Is this cancer? STAGE : Is there spread? What is the best treatment option? Suitability: can the patient receive such therapy?
10 Diagnosis History and physical Chest X-ray CT scan Percutaneous biopsy Bronchoscopy Bone scan and CT head PET scan Mediastinoscopy
11 Treatment Option
12 Fitness for Surgery Age Pulmonary function Cardiovascular function Medical conditions Nutritional Status Performance status
13 ROLE OF SURGERY DIAGNOSTIC THERAPUTIC - CURABLE - PALLATIVE

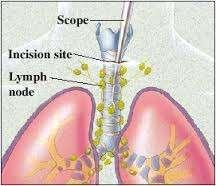
14 CERVICAL MEDIASTOTOSCOPY
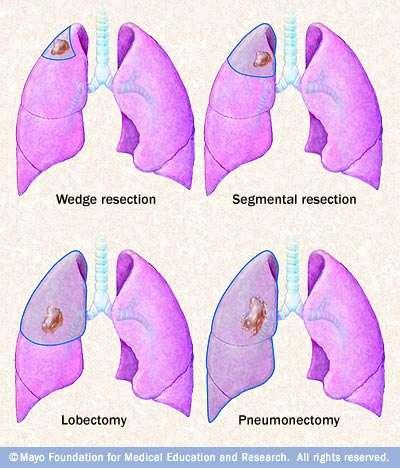
15 Surgical Principles and Management The tumor and all intrapulmonary lymphatic drainage should be removed completely. En bloc resection of closely adjacent or invaded structures. Avoid tumor spillage during surgery. Assesses the resection margins by frozen-section analysis. Positive resection margins should be Reresected whenever is possible. Complete the staging by removing All accessible Mediastinal lymph node stations for accurate staging.
16
17 Standard of Care For Peripheral Nodules 1940 s Pneumonectomy 1960 s Lobectomy 1990 s?segmentectomy/wedge (and adjuvant local/systemic Rx) 2005 VATS LOBECTOMY
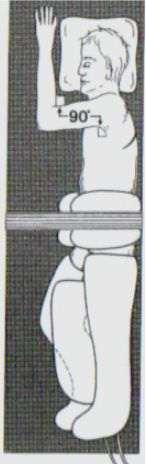
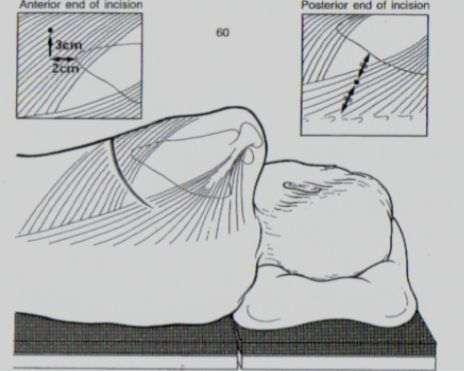
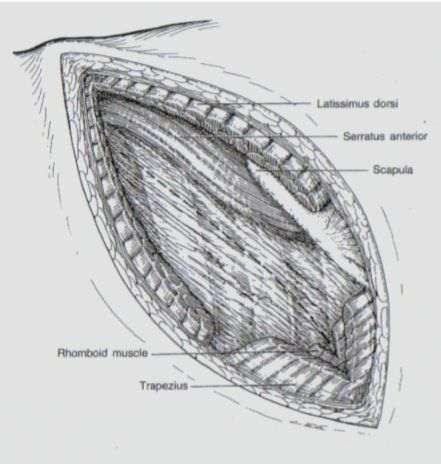
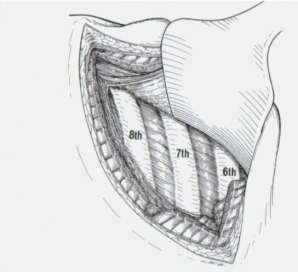

18 Thoracotomy - Posterolateral


19 Video Assisted Thoracic Surgery
20


21 T cm adenocarcinoma cm adenocarcinoma 2 cm T1a > 2 cm to 3 T1b
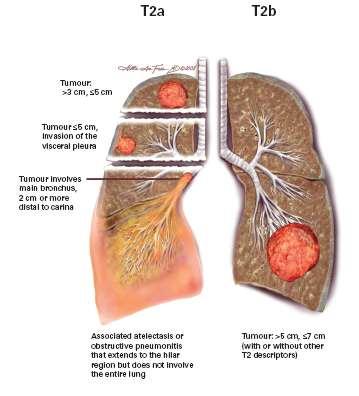
22 Stage I Disease - IA ( T1a ( 2cm), T1b(>2-3cm), N0,M0 - IB T2a( 5cm),N0,MO Surgery is the treatment of choice, usually in form of lobectomy & systematic lymph node dissection or sampling. Lesser resection therapy should be used only for patient with limited lung reserve. Curative radiotherapy : - surgical resection is not possible - patient with positive surgical margins in whom surgical re-resection can not be performed.
23 Randomized Trial of Lobectomy Versus Limited Resection for T1 N0 Non-Small Cell Lung Cancer (125 Lobectomy, 122 Limited Resection) RJ Ginsberg, LV Rubinstein and Lung Cancer Study Group Ann Thorac Surg 1995;60:615-23
24 % Survival Lobectomy vs Limited Resection Time to death (from any cause) by treatment Lobectomy Limited Resection logrank p=0.088 (one-tailed) Ginsberg and Rubinstein Ann Thorac Surg
25
26 Stage IIA Disease - T1a,b or T2a, N1 M0 T2b (>5-7cm) N0 M0 Accounts <5% of lung cancer and < 10% for all resected lung cancer. Lobectomy is the procedure of choice in most patients. Complete lymph node sampling or dissection should be added for better control. Pneumonectomy or even Sleeve resection can be used if needed to achieve complete resection (R0). Postoperative radiation therapy (no impact on survival).
27 Size of Tumor The survival rate following resection depends upon: Number of Lymph Nodes Involved With 5 year survival is 45% for single lymph node compared with 31% in-patient with multiple lymph nodes. Histological Type Local or regional recurrences are more prevalent in patients with Squamous carcinoma & Distant meta occurred more with Adenocarcinoma.
28 Role of adjuvant Chemotherapy in early stage lung cancer No adjuvant treatment is recommended for patients with stage I disease following resection. Except for lesions 4 cm with highrisk features (poorly differentiated, wedge resection, minimal margins, and vascular invasions). With new introduction of the 7th TNM staging system recently the size of tumor had major role in chemotherapy for even early stage.
29 Impact of 7 th TNM TUMOR SIZE Tumors < 3 no chemotherapy 3-5 the chemotherapy is optional 5-7 chemotherapy is preferred, >7cm they consider as T3 and chemotherapy is indicated.
30 Impact of 7 th TNM NODAL STATUS - They found that multiple involvement N1 disease needs chemotherapy while single station of N1 disease doesn't. - Patient with N2 disease that present as single disease has better survival than multiple LN although this did not reach statistically significant and wasn't included in 7th TNM staging.
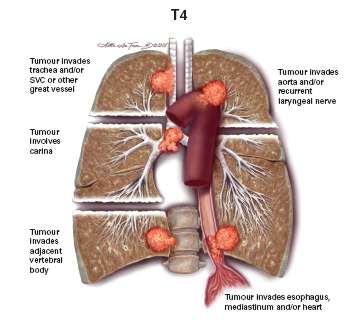
31 T 3
32 Stage IIB Disease -T2b(>5-7cm) N1 M0 -T3 (>7 cm or invasion or two nodules on same lobe) N0 m0 Tumors Invading Chest wall T3 : Factors that appear to influence survival in this group of patients include (1) Completeness of resection of the tumor (2) The extent of invasion of the chest wall (3) The presence or absence of regional lymph node metastases. The 5 years survival rate fort3n0 up to 40-50%. In patient with macroscopic or microscopic incomplete resection is zero.


33 Option for Chest wall reconstruction Nothing for one or two small rib segment especially if located posteriorly beneath large muscle or scapula Taut Marlex mesh or Gore-tex patch for bigger defect to achieve acceptable cosmetic results and chest wall instability if 2 3 rib removal or to prevent trapping of tip of scapula. Marlex mesh methyl methacnylaste sandwich technique for big defect in sternum or when chest wall instability is anticipated.

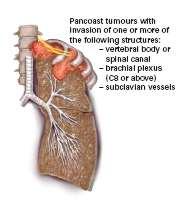
34 Superior Sulcus Tumors T3 Majority are squamous cell or adeno carcinomas, but 3% to 5% are small cell carcinomas. Mediastinoscopy is important N2 disease patient have poor survivals not longer than 1 year if they are treated with combined chemotherapy treatment or radiation therapy Unresectability The involvement of subclavian artery or vertebral body with or without cord compression, and wide spread involvement of major division of brachial plexus.
35 Superior Sulcus Tumors T3 The current standard therapy pre-operative induction chemoradiotherapy, followed-up with surgery then post-op chemotherapy with 3-year survival up to 44% for all patients and 54% after complete resection.
36 Superior Sulcus Tumors T3 Surgery involves En bloc removal of the affected lobe and chest wall, including the entire first rib and the posterior segments of ribs two, three, and often four; the transverse processes of the contiguous thoracic vertebrae; the nerve roots C8 and T1 to T3; the lower trunk of the brachial plexus; and the dorsal sympathetic chain with mediastinal node dissection.

37 Tumor into main stem bronchus < 2cm from carina but does not involve carina that associated with complete collapse of lung T 3
38 Stage IIB Disease ( cont) Tumors in Proximity to Carina T3: - Central tumors that extend within 2 cm of the carina without carinal involvement. -The nodal involvement severely affect prognosis. The 5 year survival rate can reach up to 30% to 40% - Pneumonectomy is most common resection but sleeve lobectomy can be used as this will provide lower morbidity, mortality and preserve pulmonary function.

39 Stage IIB Disease ( cont) Tumors presented with two lung nodules in same lung lobe T3: - Patient usually will be treated with adjuvant chemotherapy followed by surgery.

40
41 Stage IIIA Disease Tumors that present with lymphatic metastasis to the mediastinum as N2 disease, or tumors that invade adjacent organ (T4) or tumors presented with two nodule in ipsilateral lung. Distant metastases should be ruled out by CT scan or whole body PET scan/ct scan. Preoperative mediastinoscopy
42 T3N1-2 The survival rate following complete resection in the presence of nodal disease is less than 20% at 5 years. pre operative adjuvant chemotherapy with re-evaluation for response. There is no evidence that preoperative radiation therapy alone for clinical N1 or N2 disease benefits patients with tumors invading the chest wall. Postoperative radiation therapy in patients who have evidence of mediastinal lymph node metastases or residual disease is usually advised in an attempt to decrease the incidence of local recurrence but does not impact overall survival.
43 The role of primary surgery in N2 Unsuspected N2 disease at thoracotomy, surgery should be continued unless pneumonectomy is needed. Mediastinal lymph node dissection is strongly advisable and postoperative adjuvant chemotherapy is indicated. Preoperative radiotherapy alone for clinically N2 disease will not improve survival because most of patients die of distant metastasis.
44 N2 disease at Mediastinoscopy * Neoadjuvant concurrent chemoradiotherapy or induction chemotherapy followed by assessment of response. * For responders, surgery can be offered with mediastinal lymph node dissection. * Non-responder should be treated with chemotherapy or concurrent chemoradiotherapy if not given before as sole treatment.
45 T4 NO.N1 M0 T4 (two lesion in ipsilateral lung lobes). * Neo adjuvant chemotherapy. * Curative Pneumonectomy can be offered. * Adjuvant preoperative radiotherapy should be avoided as it carries high risk morbidity, and mortality in post Pneumonectomy patients epically in the right side. * Patient with tumors invading mediastinal structures or mian airway involvement surgery should be consider only if curative attention is approach. ( R0).
46 Stage IIIB Disease -T4 N2 MO - Any T N3M0 These patients present with -Invasion of the spine, trachea, carina, esophagus, aorta or heart (T4) with N2 Disease - Supraclavicular or contralateral mediastinal lymph node metastases (N3); * These patients are considered inoperable. Most of these patients are treated by combined concurrent chemoradiation.

47 T4 Disease, Carinal Involvement Pneumonectomy with tracheal sleeve resection and direct re-anastomosis of the trachea to the contralateral mainstem bronchus has been offered to patients with good surgical risks with up to 20-40% 5-year survival rare, often in the face of 13% to 30% operative mortality rates. This should be reserved for young healthy patient with clinically no disease determined by mediastinoscopy.
48 T4 Disease, Carinal Involvement All other patients should be treated primarily with chemoradiation without resection. local therapy in form of -Transbronchoscopic brachytherapy - photodynamic therapy.
49 N3 Disease Absolute contraindication to surgery M1 Distant metastasis * M1a Separate tumor nodule(s) in a contra lateral lobe; tumor with pleural nodules or. malignant pleural (or pericardial) effusion * M1b Distant metastasis


50 Surgical management of pleural effusion M1a Palliative Aggressive Chemotherapy. Pleural drainage & pleurodesis. Trap Lung treated with ambulatory pleural tap or insertion of pleural catheter as part of home care support. Diagnostic Thoracosecopic surgery with talc insertion. Radiotherapy or surgery in rare cases for Painful recurrence in chest wall

51 Advanced Lung Cancer M1b Brain Brain metastasis M1b Surgery versus radiation Synchronized or metastatic Solitary Primary lung is resectable

52 Advanced Lung Cancer M1b Adrenal Adrenal metastasis M1b Best if ipsilateral with lower lobe Enblock resection trans diaphragmatic Resectable lung Curative resection

53 Advanced Lung Cancer M1b Bone Bone metastasis M1b Post operative finding Resection and radiotherapy Relatively poor results Same for liver or multiple sites
54 surgery in Advanced NSCLC Never as routine A tumor board decision Specialized centers Part of the guidelines Supported with adjuvant therapy Patient counseling
55 Role of surgery in current stages Stage 0 Tis N0 M0 Surgery Stage IA T1a,b N0 M0 Surgery Stage IB T2a N0 M0 Surgery Stage IIA Stage IIB Stage IIIA Stage IIIB T1a,b T2a T2b T2b T3 T1,T2 T3 T4 T4 Any T N1 N0 N1 N0 N2 N1,N2 N0,N1 N2 N3 M0 M0 M0 M0 M0 M0 M0 M0 M0 Surgery Surgery Chemo/Radio +/-Surgery??Surgery Stage IV Any T Any N M1a,b???Surgery
56
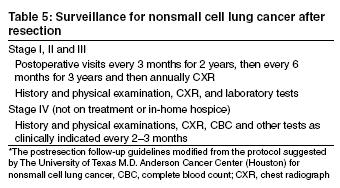
57 Post-resection Follow-up for Non-Small Cell Lung Cancer
58 Thank you
Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010
 LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer
 THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer [Based on WOSCAN NSCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED
THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer [Based on WOSCAN NSCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED
Slide 1. Slide 2. Slide 3. Investigation and management of lung cancer Robert Rintoul. Epidemiology. Risk factors/aetiology
 Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
Thoracic Surgery; An Overview
 Thoracic Surgery What we see Thoracic Surgery; An Overview James P. Locher, Jr, MD Methodist Cardiovascular and Thoracic Surgery Lung cancer Mets Fungus and TB Lung abcess and empyema Pleural based disease
Thoracic Surgery What we see Thoracic Surgery; An Overview James P. Locher, Jr, MD Methodist Cardiovascular and Thoracic Surgery Lung cancer Mets Fungus and TB Lung abcess and empyema Pleural based disease
Mediastinal Staging. Samer Kanaan, M.D.
 Mediastinal Staging Samer Kanaan, M.D. Overview Importance of accurate nodal staging Accuracy of radiographic staging Mediastinoscopy EUS EBUS Staging TNM Definitions T Stage Size of the Primary Tumor
Mediastinal Staging Samer Kanaan, M.D. Overview Importance of accurate nodal staging Accuracy of radiographic staging Mediastinoscopy EUS EBUS Staging TNM Definitions T Stage Size of the Primary Tumor
An Update: Lung Cancer
 An Update: Lung Cancer Andy Barlow Consultant in Respiratory Medicine Lead Clinician for Lung Cancer (West Herts Hospitals NHS Trust) Lead for EBUS-Harefield Hospital (RB&HFT) Summary Lung cancer epidemiology
An Update: Lung Cancer Andy Barlow Consultant in Respiratory Medicine Lead Clinician for Lung Cancer (West Herts Hospitals NHS Trust) Lead for EBUS-Harefield Hospital (RB&HFT) Summary Lung cancer epidemiology
LA RADIOTERAPIA NEL TRATTAMENTO INTEGRATO DEL CANCRO DEL POLMONE NON MICROCITOMA NSCLC I-II
 AUSL BA/4 Ospedale S. Paolo Bari U.O. Complessa di Chirurgia Toracica LA RADIOTERAPIA NEL TRATTAMENTO INTEGRATO DEL CANCRO DEL POLMONE NON MICROCITOMA NSCLC I-II stadio L opinione del chirurgo Francesco
AUSL BA/4 Ospedale S. Paolo Bari U.O. Complessa di Chirurgia Toracica LA RADIOTERAPIA NEL TRATTAMENTO INTEGRATO DEL CANCRO DEL POLMONE NON MICROCITOMA NSCLC I-II stadio L opinione del chirurgo Francesco
Charles Mulligan, MD, FACS, FCCP 26 March 2015
 Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
Bronchogenic Carcinoma
 A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
THORACIC MALIGNANCIES
 THORACIC MALIGNANCIES Summary for Malignant Malignancies. Lung Ca 1 Lung Cancer Non-Small Cell Lung Cancer Diagnostic Evaluation for Non-Small Lung Cancer 1. History and Physical examination. 2. CBCDE,
THORACIC MALIGNANCIES Summary for Malignant Malignancies. Lung Ca 1 Lung Cancer Non-Small Cell Lung Cancer Diagnostic Evaluation for Non-Small Lung Cancer 1. History and Physical examination. 2. CBCDE,
AJCC-NCRA Education Needs Assessment Results
 AJCC-NCRA Education Needs Assessment Results Donna M. Gress, RHIT, CTR Survey Tool 1 Survey Development, Delivery, Analysis THANKS to NCRA for the following work Developed survey with input from partners
AJCC-NCRA Education Needs Assessment Results Donna M. Gress, RHIT, CTR Survey Tool 1 Survey Development, Delivery, Analysis THANKS to NCRA for the following work Developed survey with input from partners
Surgical management of lung cancer
 Surgical management of lung cancer Nick Roubos FRACS Cardiothoracic Surgeon Box Hill Hospital, Epworth Eastern Thoracic Oncology Non Small Cell Lung Cancer (NSCLC) Small Cell Lung Cancer Mesothelioma Pulmonary
Surgical management of lung cancer Nick Roubos FRACS Cardiothoracic Surgeon Box Hill Hospital, Epworth Eastern Thoracic Oncology Non Small Cell Lung Cancer (NSCLC) Small Cell Lung Cancer Mesothelioma Pulmonary
Collaborative Stage. Site-Specific Instructions - LUNG
 Slide 1 Collaborative Stage Site-Specific Instructions - LUNG In this presentation, we are going to review the AJCC Cancer Staging criteria for the lung primary site. Slide 2 Reading Assignments As each
Slide 1 Collaborative Stage Site-Specific Instructions - LUNG In this presentation, we are going to review the AJCC Cancer Staging criteria for the lung primary site. Slide 2 Reading Assignments As each
Video-Mediastinoscopy Thoracoscopy (VATS)
") Surgical techniques Video-Mediastinoscopy Thoracoscopy (VATS) Gunda Leschber Department of Thoracic Surgery ELK Berlin Chest Hospital, Berlin, Germany Teaching Hospital of Charité Universitätsmedizin Berlin
Surgical techniques Video-Mediastinoscopy Thoracoscopy (VATS) Gunda Leschber Department of Thoracic Surgery ELK Berlin Chest Hospital, Berlin, Germany Teaching Hospital of Charité Universitätsmedizin Berlin
FDG PET/CT in Lung Cancer Read with the experts. Homer A. Macapinlac, M.D.
 FDG PET/CT in Lung Cancer Read with the experts Homer A. Macapinlac, M.D. Patient with suspected lung cancer presents with left sided chest pain T3 What is the T stage of this patient? A) T2a B) T2b C)
FDG PET/CT in Lung Cancer Read with the experts Homer A. Macapinlac, M.D. Patient with suspected lung cancer presents with left sided chest pain T3 What is the T stage of this patient? A) T2a B) T2b C)
GUIDELINES FOR CANCER IMAGING Lung Cancer
 GUIDELINES FOR CANCER IMAGING Lung Cancer Greater Manchester and Cheshire Cancer Network Cancer Imaging Cross-Cutting Group April 2010 1 INTRODUCTION This document is intended as a ready reference for
GUIDELINES FOR CANCER IMAGING Lung Cancer Greater Manchester and Cheshire Cancer Network Cancer Imaging Cross-Cutting Group April 2010 1 INTRODUCTION This document is intended as a ready reference for
Lung Cancer Clinical Guidelines: Surgery
 Lung Cancer Clinical Guidelines: Surgery 1 Scope of guidelines All Trusts within Manchester Cancer are expected to follow this guideline. This guideline is relevant to: Adults (18 years and older) with
Lung Cancer Clinical Guidelines: Surgery 1 Scope of guidelines All Trusts within Manchester Cancer are expected to follow this guideline. This guideline is relevant to: Adults (18 years and older) with
The 8th Edition Lung Cancer Stage Classification
 The 8th Edition Lung Cancer Stage Classification Elwyn Cabebe, M.D. Medical Oncology, Hematology, and Hospice and Palliative Care Valley Medical Oncology Consultants Director of Quality, Medical Oncology
The 8th Edition Lung Cancer Stage Classification Elwyn Cabebe, M.D. Medical Oncology, Hematology, and Hospice and Palliative Care Valley Medical Oncology Consultants Director of Quality, Medical Oncology
Lung 8/7/14. Collecting Cancer Data: Lung NAACCR Webinar Series. August 7, 2014
 Collecting Cancer Data: Lung 2013 2014 NAACCR Webinar Series August 7, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Lung 2013 2014 NAACCR Webinar Series August 7, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Lung Cancer: Determining Resectability
 Lung Cancer: Determining Resectability Leslie E. Quint lequint@umich.edu No disclosures Lung Cancer: Determining Resectability AIM: Review imaging features that suggest resectability / unresectability
Lung Cancer: Determining Resectability Leslie E. Quint lequint@umich.edu No disclosures Lung Cancer: Determining Resectability AIM: Review imaging features that suggest resectability / unresectability
Outcomes Report: Accountability Measures and Quality Improvements
 Outcomes Report: Accountability Measures and Quality Improvements The s Cancer Committee ensures that patients with cancer are treated according to the nationally accepted measures. Because we are an accredited
Outcomes Report: Accountability Measures and Quality Improvements The s Cancer Committee ensures that patients with cancer are treated according to the nationally accepted measures. Because we are an accredited
Collecting Cancer Data: Lung
 Collecting Cancer Data: Lung NAACCR 2011 2012 Webinar Series 2/2/2012 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this
Collecting Cancer Data: Lung NAACCR 2011 2012 Webinar Series 2/2/2012 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this
HISTORY SURGERY FOR TUMORS WITH INVASION OF THE APEX 15/11/2018
 30 EACTS Annual Meeting Barcelona, Spain 1-5 October 2016 SURGERY FOR TUMORS WITH INVASION OF THE APEX lung cancer of the apex of the chest involving any structure of the apical chest wall irrespective
30 EACTS Annual Meeting Barcelona, Spain 1-5 October 2016 SURGERY FOR TUMORS WITH INVASION OF THE APEX lung cancer of the apex of the chest involving any structure of the apical chest wall irrespective
The International Association for the Study of Lung Cancer (IASLC) Lung Cancer Staging Project, Data Elements
 Lung Cancer Staging Project, Data Elements") Page 1 Contents 1.1. Registration... 2 1.2. Patient Characteristics... 3 1.3. Laboratory Values at Diagnosis... 5 1.4. Lung Cancers with Multiple Lesions... 6 1.5. Primary Tumour Description... 10 1.6.
Page 1 Contents 1.1. Registration... 2 1.2. Patient Characteristics... 3 1.3. Laboratory Values at Diagnosis... 5 1.4. Lung Cancers with Multiple Lesions... 6 1.5. Primary Tumour Description... 10 1.6.
Special Treatment Issues in Non-small Cell Lung Cancer
 CHEST Supplement DIAGNOSIS AND MANAGEMENT OF LUNG CANCER, 3RD ED: ACCP GUIDELINES Special Treatment Issues in Non-small Cell Lung Cancer Diagnosis and Management of Lung Cancer, 3rd ed: American College
CHEST Supplement DIAGNOSIS AND MANAGEMENT OF LUNG CANCER, 3RD ED: ACCP GUIDELINES Special Treatment Issues in Non-small Cell Lung Cancer Diagnosis and Management of Lung Cancer, 3rd ed: American College
Lung Cancer Imaging. Terence Z. Wong, MD,PhD. Department of Radiology Duke University Medical Center Durham, NC 9/9/09
 Lung Cancer Imaging Terence Z. Wong, MD,PhD Department of Radiology Duke University Medical Center Durham, NC 9/9/09 Acknowledgements Edward F. Patz, Jr., MD Jenny Hoang, MD Ellen L. Jones, MD, PhD Lung
Lung Cancer Imaging Terence Z. Wong, MD,PhD Department of Radiology Duke University Medical Center Durham, NC 9/9/09 Acknowledgements Edward F. Patz, Jr., MD Jenny Hoang, MD Ellen L. Jones, MD, PhD Lung
Outcomes Report: Accountability Measures and Quality Improvements
 Outcomes Report: Accountability Measures and Quality Improvements The FH Memorial Medical Center s Cancer Committee ensures that patients with cancer are treated according to the nationally accepted measures.
Outcomes Report: Accountability Measures and Quality Improvements The FH Memorial Medical Center s Cancer Committee ensures that patients with cancer are treated according to the nationally accepted measures.
Non-Small Cell Lung Cancer: Disease Spectrum and Management in a Tertiary Care Hospital
 Non-Small Cell Lung Cancer: Disease Spectrum and Management in a Tertiary Care Hospital Muhammad Rizwan Khan,Sulaiman B. Hasan,Shahid A. Sami ( Department of Surgery, The Aga Khan University Hospital,
Non-Small Cell Lung Cancer: Disease Spectrum and Management in a Tertiary Care Hospital Muhammad Rizwan Khan,Sulaiman B. Hasan,Shahid A. Sami ( Department of Surgery, The Aga Khan University Hospital,
Dr. Andres Wiernik. Lung Cancer
 Dr. Andres Wiernik Lung Cancer Lung Cancer Facts - Demographics World Incidence: 1 8 million / year World Mortality: 1 6 million / year 5-year survival rates vary from 4 17% depending on stage and regional
Dr. Andres Wiernik Lung Cancer Lung Cancer Facts - Demographics World Incidence: 1 8 million / year World Mortality: 1 6 million / year 5-year survival rates vary from 4 17% depending on stage and regional
According to the current International Union
 Treatment of Stage II Non-small Cell Lung Cancer* Walter J. Scott, MD, FCCP; John Howington, MD, FCCP; and Benjamin Movsas, MD Based on clinical assessment alone, patients with stage II non-small cell
Treatment of Stage II Non-small Cell Lung Cancer* Walter J. Scott, MD, FCCP; John Howington, MD, FCCP; and Benjamin Movsas, MD Based on clinical assessment alone, patients with stage II non-small cell
Case Scenario 1. The patient agreed to a CT guided biopsy of the left upper lobe mass. This was performed and confirmed non-small cell carcinoma.
 Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
Lung Cancer Epidemiology. AJCC Staging 6 th edition
 Surgery for stage IIIA NSCLC? Sometimes! Anne S. Tsao, M.D. Associate Professor Director, Mesothelioma Program Director, Thoracic Chemo-Radiation Program May 7, 2011 The University of Texas MD ANDERSON
Surgery for stage IIIA NSCLC? Sometimes! Anne S. Tsao, M.D. Associate Professor Director, Mesothelioma Program Director, Thoracic Chemo-Radiation Program May 7, 2011 The University of Texas MD ANDERSON
The Itracacies of Staging Patients with Suspected Lung Cancer
 The Itracacies of Staging Patients with Suspected Lung Cancer Gerard A. Silvestri, MD,MS, FCCP Professor of Medicine Medical University of South Carolina Charleston, SC silvestri@musc.edu Staging Lung
The Itracacies of Staging Patients with Suspected Lung Cancer Gerard A. Silvestri, MD,MS, FCCP Professor of Medicine Medical University of South Carolina Charleston, SC silvestri@musc.edu Staging Lung
Treatment of oligometastatic NSCLC
 Treatment of oligometastatic NSCLC Jarosław Kużdżał Department of Thoracic Surgery Jagiellonian University Collegium Medicum, John Paul II Hospital, Cracow New idea? 14 NSCLC patients with solitary extrathoracic
Treatment of oligometastatic NSCLC Jarosław Kużdżał Department of Thoracic Surgery Jagiellonian University Collegium Medicum, John Paul II Hospital, Cracow New idea? 14 NSCLC patients with solitary extrathoracic
Surgery for early stage NSCLC
 1-3 March 2017, Manchester, UK Surgery for early stage NSCLC Dominique H. Grunenwald, MD, PhD Professor Emeritus in Thoracic and Cardiovascular surgery Pierre & Marie Curie University. Paris. France what
1-3 March 2017, Manchester, UK Surgery for early stage NSCLC Dominique H. Grunenwald, MD, PhD Professor Emeritus in Thoracic and Cardiovascular surgery Pierre & Marie Curie University. Paris. France what
MEDIASTINAL STAGING surgical pro
 MEDIASTINAL STAGING surgical pro Paul E. Van Schil, MD, PhD Department of Thoracic and Vascular Surgery University of Antwerp, Belgium Mediastinal staging Invasive techniques lymph node mapping cervical
MEDIASTINAL STAGING surgical pro Paul E. Van Schil, MD, PhD Department of Thoracic and Vascular Surgery University of Antwerp, Belgium Mediastinal staging Invasive techniques lymph node mapping cervical
FDG PET/CT STAGING OF LUNG CANCER. Dr Shakher Ramdave
 FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
Video-assisted thoracoscopic surgery in lung cancer staging
 Review Article on Thoracic Surgery Page 1 of 7 Video-assisted thoracoscopic surgery in lung cancer staging Frederico Krieger Martins, Guilherme Augusto Oliveira, Juliano Cé Coelho, Márcio Chmelnitsky Kruter,
Review Article on Thoracic Surgery Page 1 of 7 Video-assisted thoracoscopic surgery in lung cancer staging Frederico Krieger Martins, Guilherme Augusto Oliveira, Juliano Cé Coelho, Márcio Chmelnitsky Kruter,
Lung Cancer in Women: A Different Disease? James J. Stark, MD, FACP
 Lung Cancer in Women: A Different Disease? James J. Stark, MD, FACP Medical Director, Cancer Program and Director of Palliative Care Maryview Medical Center Professor of Medicine Eastern Virginia Medical
Lung Cancer in Women: A Different Disease? James J. Stark, MD, FACP Medical Director, Cancer Program and Director of Palliative Care Maryview Medical Center Professor of Medicine Eastern Virginia Medical
WHITE PAPER - SRS for Non Small Cell Lung Cancer
 WHITE PAPER - SRS for Non Small Cell Lung Cancer I. Introduction This white paper will focus on non-small cell lung carcinoma with sections one though six comprising a general review of lung cancer from
WHITE PAPER - SRS for Non Small Cell Lung Cancer I. Introduction This white paper will focus on non-small cell lung carcinoma with sections one though six comprising a general review of lung cancer from
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón
 Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
Case presentation. Paul De Leyn, MD, PhD Thoracic Surgery University Hospitals Leuven Belgium
 Case presentation Paul De Leyn, MD, PhD Thoracic Surgery University Hospitals Leuven Belgium Perspectives in Lung Cancer Brussels 6-7 march 2009 LEUVEN LUNG CANCER GROUP Department of Thoracic Surgery
Case presentation Paul De Leyn, MD, PhD Thoracic Surgery University Hospitals Leuven Belgium Perspectives in Lung Cancer Brussels 6-7 march 2009 LEUVEN LUNG CANCER GROUP Department of Thoracic Surgery
North of Scotland Cancer Network Clinical Management Guideline for Carcinoma of the Uterine Cervix
 THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
Lymph node dissection for lung cancer is both an old
 LOBE-SPECIFIC EXTENT OF SYSTEMATIC LYMPH NODE DISSECTION FOR NON SMALL CELL LUNG CARCINOMAS ACCORDING TO A RETROSPECTIVE STUDY OF METASTASIS AND PROGNOSIS Hisao Asamura, MD Haruhiko Nakayama, MD Haruhiko
LOBE-SPECIFIC EXTENT OF SYSTEMATIC LYMPH NODE DISSECTION FOR NON SMALL CELL LUNG CARCINOMAS ACCORDING TO A RETROSPECTIVE STUDY OF METASTASIS AND PROGNOSIS Hisao Asamura, MD Haruhiko Nakayama, MD Haruhiko
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER
 MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
NAACCR Webinar Series 1
 Collecting Cancer Data: Lung 2013 2014 NAACCR Webinar Series August 7, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Lung 2013 2014 NAACCR Webinar Series August 7, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Marcel Th. M. van Rens, MD; Aart Brutel de la Rivière, MD, PhD, FCCP; Hans R. J. Elbers, MD, PhD; and Jules M. M. van den Bosch, MD, PhD, FCCP
 Prognostic Assessment of 2,361 Patients Who Underwent Pulmonary Resection for Non-small Cell Lung Cancer, Stage I, II, and IIIA* Marcel Th. M. van Rens, MD; Aart Brutel de la Rivière, MD, PhD, FCCP; Hans
Prognostic Assessment of 2,361 Patients Who Underwent Pulmonary Resection for Non-small Cell Lung Cancer, Stage I, II, and IIIA* Marcel Th. M. van Rens, MD; Aart Brutel de la Rivière, MD, PhD, FCCP; Hans
THORACIK RICK. Lungs. Outline and objectives Richard A. Malthaner MD MSc FRCSC FACS
 THORACIK RICK Outline and objectives Lungs Management of a solitary lung nodule Mediastinum Management of a mediastinal mass Pleura Management of a pleural fluid & pneumothorax Esophagus & Stomach Management
THORACIK RICK Outline and objectives Lungs Management of a solitary lung nodule Mediastinum Management of a mediastinal mass Pleura Management of a pleural fluid & pneumothorax Esophagus & Stomach Management
EVIDENCE BASED MANAGEMENT OF STAGE III NSCLC MILIND BALDI
 EVIDENCE BASED MANAGEMENT OF STAGE III NSCLC MILIND BALDI Overview Introduction Diagnostic work up Treatment Group 1 Group 2 Group 3 Stage III lung cancer Historically was defined as locoregionally advanced
EVIDENCE BASED MANAGEMENT OF STAGE III NSCLC MILIND BALDI Overview Introduction Diagnostic work up Treatment Group 1 Group 2 Group 3 Stage III lung cancer Historically was defined as locoregionally advanced
Radiological staging of lung cancer. Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh
 Radiological staging of lung cancer Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh Bronchogenic Carcinoma Accounts for 14% of new cancer diagnoses in 2012. Estimated to kill ~150,000
Radiological staging of lung cancer Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh Bronchogenic Carcinoma Accounts for 14% of new cancer diagnoses in 2012. Estimated to kill ~150,000
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma
 Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
VATS after induction therapy: Effective and Beneficial Tips on Strategy
 VATS after induction therapy: Effective and Beneficial Tips on Strategy AATS Focus on Thoracic Surgery Mastering Surgical Innovation Las Vegas Nevada Oct. 27-28 2017 Scott J. Swanson, M.D. Professor of
VATS after induction therapy: Effective and Beneficial Tips on Strategy AATS Focus on Thoracic Surgery Mastering Surgical Innovation Las Vegas Nevada Oct. 27-28 2017 Scott J. Swanson, M.D. Professor of
Chirurgie beim oligo-metastatischen NSCLC
 24. Ärzte-Fortbildungskurs in Klinischer Onkologie 20.-22. Februar 2014, Kantonsspital St. Gallen Chirurgie beim oligo-metastatischen NSCLC Prof. Dr. med. Walter Weder Klinikdirektor Thoraxchirurgie, UniversitätsSpital
24. Ärzte-Fortbildungskurs in Klinischer Onkologie 20.-22. Februar 2014, Kantonsspital St. Gallen Chirurgie beim oligo-metastatischen NSCLC Prof. Dr. med. Walter Weder Klinikdirektor Thoraxchirurgie, UniversitätsSpital
Adam J. Hansen, MD UHC Thoracic Surgery
 Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER
 10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
Superior and Basal Segment Lung Cancers in the Lower Lobe Have Different Lymph Node Metastatic Pathways and Prognosis
 ORIGINAL ARTICLES: Superior and Basal Segment Lung Cancers in the Lower Lobe Have Different Lymph Node Metastatic Pathways and Prognosis Shun-ichi Watanabe, MD, Kenji Suzuki, MD, and Hisao Asamura, MD
ORIGINAL ARTICLES: Superior and Basal Segment Lung Cancers in the Lower Lobe Have Different Lymph Node Metastatic Pathways and Prognosis Shun-ichi Watanabe, MD, Kenji Suzuki, MD, and Hisao Asamura, MD
Lung /1/16. Please submit all questions concerning webinar content through the Q&A panel. Reminder:
 1 NAACCR 2015-2016 Webinar Series Collecting Cancer Data: Lung NAACCR 2015 2016 Webinar Series Presented by: Angela Martin amartin@naaccr.org Jim Hofferkamp jhofferkamp@naaccr.org Q&A Please submit all
1 NAACCR 2015-2016 Webinar Series Collecting Cancer Data: Lung NAACCR 2015 2016 Webinar Series Presented by: Angela Martin amartin@naaccr.org Jim Hofferkamp jhofferkamp@naaccr.org Q&A Please submit all
B REAST STAGING FORM. PATHOLOGIC Extent of disease through completion of definitive surgery. CLINICAL Extent of disease before any treatment
 B REAST STAGING FORM CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery (DCIS) (LCIS) (Paget s) mi c a b c d TUMOR SIZE:
B REAST STAGING FORM CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery (DCIS) (LCIS) (Paget s) mi c a b c d TUMOR SIZE:
Lung cancer Surgery. 17 TH ESO-ESMO MASTERCLASS IN CLINICAL ONCOLOGY March, 2017 Berlin, Germany
 17 TH ESO-ESMO MASTERCLASS IN CLINICAL ONCOLOGY 24-29 March, 2017 Berlin, Germany Lung cancer Surgery Sven Hillinger MD, Thoracic Surgery, University Hospital Zurich Case 1 59 y, female, 40 py, incidental
17 TH ESO-ESMO MASTERCLASS IN CLINICAL ONCOLOGY 24-29 March, 2017 Berlin, Germany Lung cancer Surgery Sven Hillinger MD, Thoracic Surgery, University Hospital Zurich Case 1 59 y, female, 40 py, incidental
Early and locally advanced non-small-cell lung cancer (NSCLC)
") Early and locally advanced non-small-cell lung cancer (NSCLC) ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up P. E. Postmus, K. M. Kerr, M. Oudkerk, S. Senan, D. A. Waller, J.
Early and locally advanced non-small-cell lung cancer (NSCLC) ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up P. E. Postmus, K. M. Kerr, M. Oudkerk, S. Senan, D. A. Waller, J.
B REAST STAGING FORM. PATHOLOGIC Extent of disease through completion of definitive surgery. CLINICAL Extent of disease before any treatment
 B REAST STAGING FORM Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery (DCIS) (LCIS) (Paget s) mi a b c a b c d TUMOR SIZE: S TAGE
B REAST STAGING FORM Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery (DCIS) (LCIS) (Paget s) mi a b c a b c d TUMOR SIZE: S TAGE
Cervical cancer presentation
 Carcinoma of the cervix: Carcinoma of the cervix is the second commonest cancer among women worldwide, with only breast cancer occurring more commonly. Worldwide, cervical cancer accounts for about 500,000
Carcinoma of the cervix: Carcinoma of the cervix is the second commonest cancer among women worldwide, with only breast cancer occurring more commonly. Worldwide, cervical cancer accounts for about 500,000
Gynecologic Cancer InterGroup Cervix Cancer Research Network. Management of Cervical Cancer in Resource Limited Settings.
 Management of Cervical Cancer in Resource Limited Settings Linus Chuang MD Conflict of Interests None Cervical cancer is the fourth most common malignancy in women worldwide 530,000 new cases per year
Management of Cervical Cancer in Resource Limited Settings Linus Chuang MD Conflict of Interests None Cervical cancer is the fourth most common malignancy in women worldwide 530,000 new cases per year
11/21/ M with LUL Mass Case Presentation / Round Table Discussion. Multiple-choice question What stage is this tumor?
 MS 62M with LUL Mass Case Presentation / Round Table Discussion Dr. Jasleen Kukreja and Johannes Kratz Department of Thoracic Surgery University of California, San Francisco 62M, presented to clinic 6/2009
MS 62M with LUL Mass Case Presentation / Round Table Discussion Dr. Jasleen Kukreja and Johannes Kratz Department of Thoracic Surgery University of California, San Francisco 62M, presented to clinic 6/2009
Seventh Edition of the Cancer Staging Manual and Stage Grouping of Lung Cancer. Quick Reference Chart and Diagrams
 CHEST Special Features Seventh Edition of the Cancer Staging Manual and Stage Grouping of Lung Cancer Quick Reference Chart and Diagrams Omar Lababede, MD ; Moulay Meziane, MD ; and Thomas Rice, MD, FCCP
CHEST Special Features Seventh Edition of the Cancer Staging Manual and Stage Grouping of Lung Cancer Quick Reference Chart and Diagrams Omar Lababede, MD ; Moulay Meziane, MD ; and Thomas Rice, MD, FCCP
The Role of Radiation Therapy
 The Role of Radiation Therapy and Surgery in the Treatment of Bronchogenic Carcinoma R Adams Cowley, M.D., Morris J. Wizenberg, M.D., and Eugene J. Linberg, M.D. A study of the combined use of preoperative
The Role of Radiation Therapy and Surgery in the Treatment of Bronchogenic Carcinoma R Adams Cowley, M.D., Morris J. Wizenberg, M.D., and Eugene J. Linberg, M.D. A study of the combined use of preoperative
T3 NSCLC: Chest Wall, Diaphragm, Mediastinum
 for T3 NSCLC: Chest Wall, Diaphragm, Mediastinum AATS Postgraduate Course April 29, 2012 Thomas A. D Amico MD Professor of Surgery, Chief of Thoracic Surgery Duke University Health System Disclosure No
for T3 NSCLC: Chest Wall, Diaphragm, Mediastinum AATS Postgraduate Course April 29, 2012 Thomas A. D Amico MD Professor of Surgery, Chief of Thoracic Surgery Duke University Health System Disclosure No
The Value of Adjuvant Radiotherapy in Pulmonary and Chest Wall Resection for Bronchogenic Carcinoma
 The Value of Adjuvant Radiotherapy in Pulmonary and Chest Wall Resection for Bronchogenic Carcinoma G. A. Patterson, M.D., R. Ilves, M.D., R. J. Ginsberg, M.D., J. D. Cooper, M.D., T. R. J. Todd, M.D.,
The Value of Adjuvant Radiotherapy in Pulmonary and Chest Wall Resection for Bronchogenic Carcinoma G. A. Patterson, M.D., R. Ilves, M.D., R. J. Ginsberg, M.D., J. D. Cooper, M.D., T. R. J. Todd, M.D.,
PET CT for Staging Lung Cancer
 PET CT for Staging Lung Cancer Rohit Kochhar Consultant Radiologist Disclosures Neither I nor my immediate family members have financial relationships with commercial organizations that may have a direct
PET CT for Staging Lung Cancer Rohit Kochhar Consultant Radiologist Disclosures Neither I nor my immediate family members have financial relationships with commercial organizations that may have a direct
Prognostic Factors for Survival of Stage IB Upper Lobe Non-small Cell Lung Cancer Patients: A Retrospective Study in Shanghai, China
 www.springerlink.com Chin J Cancer Res 23(4):265 270, 2011 265 Original Article Prognostic Factors for Survival of Stage IB Upper Lobe Non-small Cell Lung Cancer Patients: A Retrospective Study in Shanghai,
www.springerlink.com Chin J Cancer Res 23(4):265 270, 2011 265 Original Article Prognostic Factors for Survival of Stage IB Upper Lobe Non-small Cell Lung Cancer Patients: A Retrospective Study in Shanghai,
Educational Objectives. Managing Lung Cancer From the Solitary Pulmonary Nodule to Complex Cases: A Multidisciplinary Approach.
 Managing Lung Cancer From the Solitary Pulmonary Nodule to Complex Cases: A Multidisciplinary Approach Robert A. Meguid, MD, MPH, FACS Assistant Professor of Cardiothoracic Surgery Surgical Director, Surgical
Managing Lung Cancer From the Solitary Pulmonary Nodule to Complex Cases: A Multidisciplinary Approach Robert A. Meguid, MD, MPH, FACS Assistant Professor of Cardiothoracic Surgery Surgical Director, Surgical
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Ablative therapy, nonsurgical, for pulmonary metastases of soft tissue sarcoma, 279 280 Adipocytic tumors, atypical lipomatous tumor vs. well-differentiated
Note: Page numbers of article titles are in boldface type. A Ablative therapy, nonsurgical, for pulmonary metastases of soft tissue sarcoma, 279 280 Adipocytic tumors, atypical lipomatous tumor vs. well-differentiated
Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease
 Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease Jennifer E. Tseng, MD UFHealth Cancer Center-Orlando Health Sep 12, 2014 Background Approximately
Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease Jennifer E. Tseng, MD UFHealth Cancer Center-Orlando Health Sep 12, 2014 Background Approximately
is time consuming and expensive. An intra-operative assessment is not going to be helpful if there is no more tissue that can be taken to improve the
 My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
Treatment of Clinical Stage I Lung Cancer: Thoracoscopic Lobectomy is the Standard
 Treatment of Clinical Stage I Lung Cancer: Thoracoscopic Lobectomy is the Standard AATS General Thoracic Surgery Symposium May 5, 2010 Thomas A. D Amico MD Professor of Surgery, Duke University Medical
Treatment of Clinical Stage I Lung Cancer: Thoracoscopic Lobectomy is the Standard AATS General Thoracic Surgery Symposium May 5, 2010 Thomas A. D Amico MD Professor of Surgery, Duke University Medical
came from a carcinoma and in 12 from a sarcoma. Ninety lesions were intrapulmonary and the as the chest wall and pleura. Details of the primary
 Thorax 1982;37:366-370 Thoracic metastases MARY P SHEPHERD From the Thoracic Surgical Unit, Harefield Hospital, Harefield ABSTRACI One hundred and four patients are reviewed who were found to have thoracic
Thorax 1982;37:366-370 Thoracic metastases MARY P SHEPHERD From the Thoracic Surgical Unit, Harefield Hospital, Harefield ABSTRACI One hundred and four patients are reviewed who were found to have thoracic
Satellite Pulmonary Nodule in the Same Lobe (T4N0) Should Not Be Staged as IIIB Non Small Cell Lung Cancer
 Should Not Be Staged as IIIB Non Small Cell Lung Cancer") Satellite Pulmonary Nodule in the Same Lobe (T4N0) Should Not Be Staged as IIIB Non Small Cell Lung Cancer Ayesha S. Bryant, MSPH, MD, Sara J. Pereira, MD, Daniel L. Miller, MD, and Robert James Cerfolio,
Satellite Pulmonary Nodule in the Same Lobe (T4N0) Should Not Be Staged as IIIB Non Small Cell Lung Cancer Ayesha S. Bryant, MSPH, MD, Sara J. Pereira, MD, Daniel L. Miller, MD, and Robert James Cerfolio,
Impact of Radical Systematic Mediastinal Lymphadenectomy on Tumor Staging in Lung Cancer
 Impact of Radical Systematic Mediastinal Lymphadenectomy on Tumor Staging in Lung Cancer Jakob R. Izbicki, MD, Bernward Passlick, MD, Ortrud Karg, MD, Christian Bloechle, MD, Klaus Pantel, MD, Wolfram
Impact of Radical Systematic Mediastinal Lymphadenectomy on Tumor Staging in Lung Cancer Jakob R. Izbicki, MD, Bernward Passlick, MD, Ortrud Karg, MD, Christian Bloechle, MD, Klaus Pantel, MD, Wolfram
Boot Camp Case Scenarios
 Boot Camp Case Scenarios Case Scenario 1 Patient is a 69-year-old white female. She presents with dyspnea on exertion, cough, and right rib pain. Patient is a smoker. 9/21/12 CT Chest FINDINGS: There is
Boot Camp Case Scenarios Case Scenario 1 Patient is a 69-year-old white female. She presents with dyspnea on exertion, cough, and right rib pain. Patient is a smoker. 9/21/12 CT Chest FINDINGS: There is
Oncology 101. Cancer Basics
 Oncology 101 Cancer Basics What Will You Learn? What is Cancer and How Does It Develop? Cancer Diagnosis and Staging Cancer Treatment What is Cancer? Cancer is a group of more than 100 different diseases
Oncology 101 Cancer Basics What Will You Learn? What is Cancer and How Does It Develop? Cancer Diagnosis and Staging Cancer Treatment What is Cancer? Cancer is a group of more than 100 different diseases
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS
 Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Radiology Pathology Conference
 Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Cervical Cancer 3/25/2019. Abnormal vaginal bleeding
 Cervical Cancer Abnormal vaginal bleeding Postcoital, intermenstrual or postmenopausal Vaginal discharge Pelvic pain or pressure Asymptomatic In most patients who are not sexually active due to symptoms
Cervical Cancer Abnormal vaginal bleeding Postcoital, intermenstrual or postmenopausal Vaginal discharge Pelvic pain or pressure Asymptomatic In most patients who are not sexually active due to symptoms
Complex Thoracoscopic Resections for Locally Advanced Lung Cancer
 Complex Thoracoscopic Resections for Locally Advanced Lung Cancer Duke Thoracoscopic Lobectomy Workshop March 21, 2018 Thomas A. D Amico MD Gary Hock Professor of Surgery Section Chief, Thoracic Surgery,
Complex Thoracoscopic Resections for Locally Advanced Lung Cancer Duke Thoracoscopic Lobectomy Workshop March 21, 2018 Thomas A. D Amico MD Gary Hock Professor of Surgery Section Chief, Thoracic Surgery,
Master Class: Fundamentals of Lung Cancer
 This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
Proposed All Wales Vulval Cancer Guidelines. Dr Amanda Tristram
 Proposed All Wales Vulval Cancer Guidelines Dr Amanda Tristram Previous FIGO staging FIGO Stage Features TNM Ia Lesion confined to vulva with
Proposed All Wales Vulval Cancer Guidelines Dr Amanda Tristram Previous FIGO staging FIGO Stage Features TNM Ia Lesion confined to vulva with
UICC TNM 8 th Edition Errata
 UICC TNM 8 th Edition Errata ions are in italics Page 28 Oropharynx p16 positive Pathological Stage II,T2 N2 M0 T3 N0,N1 M0 Stage II,T2 N2 M0 T3,T4 N0,N1 M0 Page 61 Oesophagus Adenocarcinoma Pathological
UICC TNM 8 th Edition Errata ions are in italics Page 28 Oropharynx p16 positive Pathological Stage II,T2 N2 M0 T3 N0,N1 M0 Stage II,T2 N2 M0 T3,T4 N0,N1 M0 Page 61 Oesophagus Adenocarcinoma Pathological
Surgery for nonsmall cell lung cancer
 SERIES TOPICS IN THORACIC ONCOLOGY Surgery for nonsmall cell lung cancer Loïc Lang-Lazdunski Number 3 in the Series Topics in Thoracic Oncology Edited by G. Zalcman and N. Girard Affiliations: Dept of
SERIES TOPICS IN THORACIC ONCOLOGY Surgery for nonsmall cell lung cancer Loïc Lang-Lazdunski Number 3 in the Series Topics in Thoracic Oncology Edited by G. Zalcman and N. Girard Affiliations: Dept of
and Strength of Recommendations
 ASTRO with ASCO Qualifying Statements in Bold Italics s patients with T1-2, N0 non-small cell lung cancer who are medically operable? 1A: Patients with stage I NSCLC should be evaluated by a thoracic surgeon,
ASTRO with ASCO Qualifying Statements in Bold Italics s patients with T1-2, N0 non-small cell lung cancer who are medically operable? 1A: Patients with stage I NSCLC should be evaluated by a thoracic surgeon,
ACOS Inquiry and Response Selected Inquires CS Tumor Size/Extension Evaluation, CS Lymph Nodes Evaluation, CS Metastasis at Diagnosis Evaluation *
 ACOS Inquiry and Response Selected Inquires CS Tumor Size/Extension Evaluation, CS Lymph Nodes Evaluation, CS Metastasis at Diagnosis Evaluation * CS Tumor Size/Extension Evaluation 24842 12/11/2007: Q:
ACOS Inquiry and Response Selected Inquires CS Tumor Size/Extension Evaluation, CS Lymph Nodes Evaluation, CS Metastasis at Diagnosis Evaluation * CS Tumor Size/Extension Evaluation 24842 12/11/2007: Q:
Lung Cancer-a primer. Sai Yendamuri, MD Professor and Chair, Dept of Thoracic Surgery,RPCI,Buffalo
 Lung Cancer-a primer Sai Yendamuri, MD Professor and Chair, Dept of Thoracic Surgery,RPCI,Buffalo CLINICAL CATEGORIES THE SOLITARY PULMONARY NODULE MULTIPLE PULMONARY NODULES Differential Diagnosis Malignant
Lung Cancer-a primer Sai Yendamuri, MD Professor and Chair, Dept of Thoracic Surgery,RPCI,Buffalo CLINICAL CATEGORIES THE SOLITARY PULMONARY NODULE MULTIPLE PULMONARY NODULES Differential Diagnosis Malignant
Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours?
 Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours? Question #2: How are cardia tumours managed? Michael F. Humer December 3, 2005 Vancouver, BC Case
Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours? Question #2: How are cardia tumours managed? Michael F. Humer December 3, 2005 Vancouver, BC Case
Tumour size as a prognostic factor after resection of lung carcinoma
 Tumour size as a prognostic factor after resection of lung carcinoma A. S. SOORAE AND R. ABBEY SMITH Thorax, 1977, 32, 19-25 From the Cardio-Thoracic Unit, Walsgrave Hospital, Clifford Bridge Road, Coventry
Tumour size as a prognostic factor after resection of lung carcinoma A. S. SOORAE AND R. ABBEY SMITH Thorax, 1977, 32, 19-25 From the Cardio-Thoracic Unit, Walsgrave Hospital, Clifford Bridge Road, Coventry
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
The 7th Edition of TNM in Lung Cancer.
 10th European Conference Perspectives in Lung Cancer. Brussels, March 2009. The 7th Edition of TNM in Lung Cancer. Peter Goldstraw, Consultant Thoracic Surgeon, Royal Brompton Hospital, Professor of Thoracic
10th European Conference Perspectives in Lung Cancer. Brussels, March 2009. The 7th Edition of TNM in Lung Cancer. Peter Goldstraw, Consultant Thoracic Surgeon, Royal Brompton Hospital, Professor of Thoracic
Lung. 10/24/13 Chest X-ray: 2.9 cm mass like density in the inferior lingular segment worrisome for neoplasm. Malignancy cannot be excluded.
 Lung Case Scenario 1 A 54 year white male presents with a recent abnormal CT of the chest. The patient has a history of melanoma, kidney, and prostate cancers. 10/24/13 Chest X-ray: 2.9 cm mass like density
Lung Case Scenario 1 A 54 year white male presents with a recent abnormal CT of the chest. The patient has a history of melanoma, kidney, and prostate cancers. 10/24/13 Chest X-ray: 2.9 cm mass like density
Case Scenario year-old white male presented to personal physician with dyspepsia with reflux.
 Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
The right middle lobe is the smallest lobe in the lung, and
 ORIGINAL ARTICLE The Impact of Superior Mediastinal Lymph Node Metastases on Prognosis in Non-small Cell Lung Cancer Located in the Right Middle Lobe Yukinori Sakao, MD, PhD,* Sakae Okumura, MD,* Mun Mingyon,
ORIGINAL ARTICLE The Impact of Superior Mediastinal Lymph Node Metastases on Prognosis in Non-small Cell Lung Cancer Located in the Right Middle Lobe Yukinori Sakao, MD, PhD,* Sakae Okumura, MD,* Mun Mingyon,