Integration of Surgery And Systemic Therapy In The Treatment of
|
|
|
- Coleen Dickerson
- 5 years ago
- Views:
Transcription


1 Integration of Surgery And Systemic Therapy In The Treatment of Advanced Renal Cell Carcinoma Christopher G. Wood, M. D., FACS Professor and Deputy Chairman Douglas E. Johnson, M. D. Professorship In Urology Department of Urology The University of Texas MD Anderson Cancer Center
2 Therapy of Renal Cell Carcinoma Prior to 2006 Stage I-III: nephrectomy Stage IV: nephrectomy + systemic therapy Common therapies Single-agent and combination regimens containing cytokines (eg, IFN-α, IL-2) and chemotherapeutics Surgery Radiation in selected cases IFN, interferon; IL, interleukin. NCCN Clinical Practice Guidelines in Oncology: Kidney Cancer. Available at: physician_gls/pdf/kidney.pdf. Yang et al. N Engl J Med. 2003;349: Ratain et al. J Clin Oncol. 2006;24: Motzer et al. J Clin Oncol. 2006;24: Motzer et al. JAMA. 2006;295: Motzer et al. N Engl J Med. 2007;356:


 2 Sorafenib (Dec 2005)")
 6")
 5 Everolimus (Mar 2009)")




3 Treatment options for RCC have been revolutionized in a short period of time FDA approvals High dose interleukin-2 Sunitinib (Jan 2006) 2 Sorafenib (Dec 2005) 1 Temsirolimus (May 2007) 3 Pazopanib (Oct 2009) 6 Bevacizumab + IFN-α (Jul 2009) 5 Everolimus (Mar 2009) 4 Axitinib (Jan 2012) US FDA. Sorafenib US FDA. Sunitinib malate US FDA. Temsirolimus US FDA. Everolimus US FDA. Bevacizumab US FDA. Pazopanib US FDA. Axitinib
4 RCC Treatment Algorithm: 2014 * Regimen Setting Therapy Options Treatment Naïve Patient MSK Risk : Good or Intermediate MSK Risk : Poor Sunitinib Bevacizumab ± IFNα Pazopanib Temsirolimus Sunitinib HD IL-2? Sorafenib?Sorafenib Treatment Refractory Patient ( 2 d i ) Ctki Cytokine Refractory ( 2 nd Line) Refractory to VEGF/VEGFR or mtor Inhibitors Sorafenib Pazopanib Axitinib Everolimus Axitinib Sunitinib?Sequential TKI s or VEGFInhibitor *Adapted from M Atkins, ASCO 2006 Non clear cell: Temsirolimus
5 Mechanisms of Therapeutic Effect and Angiogenic Escape Rini, B Clin Cancer Res, 2010
6 What is the proper integration of surgery and systemic therapy in the setting of advanced disease?
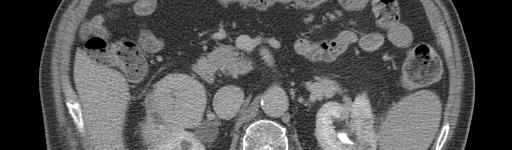
7 62 y/o WM with hematuria PMH: DM, Htn PSH: Appy, Knee surgery SH: Denies Tobacco/ETOH use PE: unremarkable PS = 1 CT abdomen Locally advanced right renal mass CT chest Bilateral pulmonary nodules
8 62 y/o WM with hematuria








9 62 y/o WM with hematuria
10 62 y/o WM with hematuria Hb 9.8 LDH 1000 All other labs WNL Bone scan/mri brain negative for mets
11 62 y/o WM with hematuria Patient undergoes cytoreductive nephrectomy T3aN0M1 Clear cell RCC, FG 4 Follow-up scans at 6 weeks show modest progression of pulmonary metastases Started on Sunitinib 4 weeks/2 weeks 50 mg Required dose reduction at 6 months to 37.5 mg due to toxicity
12 62 y/o WM with hematuria Disease progression at 14 months out from surgery Changed to everolimus Currently stable disease 2 years out from surgery
13 73 y/o WF presents with fatigue and anemia PS = 1 PMH: Htn, Hypothyroidism, MVP, CKD (egfr 36) CT chest: Bilateral pulmonary nodules Labs: Hb 9.5 (after transfusion), LDH 868, all other labs WNL Brain MRI and Bone Scan negative





14 73 y/o WF presents with fatigue and anemia







15 73 y/o WF presents with fatigue and anemia
16 73 y/o WF presents with fatigue and anemia Undergoes right radical nephrectomy with RPLND. Mass noted in right fallopian tube (metastatic renal cell carcinoma) T3aN1M1 ccrcc with 30 40% sarcomatoid and rhabdoid features, FG 4 3/10 LN s positive All surgical margins negative
17 73 y/o WF presents with fatigue and anemia Returns 1 month later, PS = 4 Admitted through the emergency center for failure to thrive Hb 8.2, LDH 1094, Ca , egfr 33




18 73 y/o WF presents with fatigue and anemia







19 73 y/o WF presents with fatigue and anemia
20 73 y/o WF presents with fatigue and anemia Patient never received therapy due to poor performance status Died of disease 45 days after surgery
21 Is there still a role for cytoreductive surgery in the setting of metastatic disease?
22 100 Metastatic RCC Nephrectomy & Immunotherapy UCLA % Surv vival P<0.05 IMT NX Nx + IMT Months J UROL 166: 1611, 2001
23 Effect of Nephrectomy on Survival in Metastatic RCC Radical Nephrectomy + IFN- Patients with metastatic t ti RCC with PS 0-1 (SWOG, N=241) (EORTC, N=83) (SWOG, N=120) (EORTC, N=42) IFN- (SWOG, N=121) (EORTC, N=43) IFN = interferon Flanigan RC et al. N Eng J Med. 2001;345:1655. Mickisch GH et al. Lancet. 2001;358:966.
24 Role of Cytoreductive Nephrectomy in the Setting of Metastatic Disease: EORTC Time to Progression Overall Survival IFN + Nx 5 CR, 3 PR (19%) IFN 1CR, 4 PR (12%) Mickisch G et al. Lancet, 2001
25 Role of Cytoreductive Nephrectomy in the Setting of Metastatic Disease: SWOG 8949 IFN+Nx3PR(3%) Nx IFN 1 CR, 2 PR (4%) Flanigan R et al., NEJM, 2001
26 2001 SWOG vs. UCLA 100 Retrospective. 80 P<0.05 Surviv val Pantuck et al; NEJM, 2001 Nx + IL-2 Nx + IFN IFN Months
27 RCC Treatment Algorithm: 2014 * Regimen Setting Therapy Options Treatment Naïve Patient MSK Risk : Good or Intermediate MSK Risk : Poor Sunitinib Bevacizumab ± IFNα Pazopanib Temsirolimus Sunitinib HD IL-2? Sorafenib?Sorafenib Treatment Refractory Patient ( 2 d i ) Ctki Cytokine Refractory ( 2 nd Line) Refractory to VEGF/VEGFR or mtor Inhibitors Sorafenib Pazopanib Axitinib Everolimus Axitinib Sunitinib?Sequential TKI s or VEGFInhibitor *Adapted from M Atkins, ASCO 2006 Non clear cell: Temsirolimus
28 Cytoreductive Nephrectomy Utilization Tsao CK et. al., Clinical GU Cancer, 2011
29 How Does It Work? Reduction in major portion of tumor burden Immunologic: Surgery induces exposure of new tumor antigens or removal of immunologic i sink Altering the metabolic milieu: Relative renal insufficiency induces metabolic acidosis which is somehow anti-tumoral Endocrine/Paracrine: Removal of secreted factor that promotes progression/metastasis
30 Arguments Against Cytoreductive Nephrectomy Surgical morbidity/mortality significant Only proven benefit in combination with IFN (an inferior therapy) Spend majority of time left on this earth recovering from surgery Significant disease progression or morbidity during post-operative operative recovery period may preclude systemic therapy Newer therapies may result in primary tumor regression
31 Phase 3 Randomized Study Comparing Nephrectomy plus Sunitinib versus Sunitinib without Nephrectomy in 1st line Metastatic RCC Randomization N = 576 Nephrectomy Sunitinib 50 mg 4/2 Sunitinib 50 mg 4/2 - Primary Objective: - To show thatt Sunitinib ib alone is not inferior i to Nephrectomy plus Sunitinib (non inferiority study) in terms of Overall Survival (OS) - Hypothesis: - Median OS expected in the nephrectomy plus Sunitinib = 24 months - Sunitinib alone will be considered as a clinically valid option if median OS > 19,9 months CARMENA Study Pr Arnaud Mejean (CCAFU Necker Hospital Paris, France) Pr Alain Ravaud (GETUG Saint-André Hospital Bordeaux, France)
32 Sunitinib in Patient With or Without Prior Nephrectomy in an Expanded Access Trial of mrcc: Response Response, n (%) Patients with prior Patients without Nx (n=3014*) prior Nx (N=192)* Objective response rate Complete response 538 (18) 31 (1) 17 (9) 0 Partial response 507 (17) 17 (9) Stable disease >3 months 1764 (59) 118 (61) Clinical benefit 2302 (76) 135 (70) Nx=nephrectomy *Only patients with evaluable efficacy data included Clinical benefit=orr + SD 3 months Szczylik et al. ASCO Abstract 5124
33 Sunitinib in Patients With or Without Prior Nephrectomy in an Expanded Access Trial of mrcc: PFS (No Prior Cytokine Treatment) PFS proba ability Patients with prior nephrectomy (n=1020) Median = 12.0 mo (95% CI, ) Patients without prior nephrectomy (n=146) Median = 6.5 mo (95% CI, ) P= Months mrcc = metastatic renal cell carcinoma; PFS = progression free survival Szczylik et al. ASCO, Abstract 5124.
34 Sunitinib in Patients With or Without Prior Nephrectomy in an Expanded Access Trial of mrcc: OS (No Prior Cytokine Treatment) lity OS probabi Patients with prior nephrectomy (n=1020) Median = 19.0 mo (95% CI, ) Patients without prior nephrectomy (n=146) Median = 11.1 mo (95% CI, ) P< OS = overall survival Months Szczylik et al. ASCO, Abstract 5124.
35 Cytoreductive Nephrectomy In The Era of Targeted Therapy: What do we do until the prospective trials are completed? Yes= 201 No = 113 KPS 80 KPS < 80 Choueiri, T et al., J Urol, 2011
36 Cytoreductive Nephrectomy In The Era of Targeted Therapy (SEER ) Culp and Wood, Submitted
37 Cytoreductive Surgery For Metastatic Renal Cell Carcinoma: It s Not For Everyone! Patient Selection Is CRITICAL!!!!!
38 Cytoreductive Nephrectomy: Tufts University 28 highly selected patients (61 pts. deferred) >75% debulking, absence of CNS, Liver, Bone mets, PS 0-1, clear cell histology 93% received systemic therapy Response rate 39%» 18% CR» 21% PR Median survival: 20.5 months Systemic therapy: IL-2 J Urol, 1997
39 Identifying Patients who will Not Benefit from Cytoreductive Nephrectomy: MDACC 566 pts undergoing CN between 1991 and pts undergoing g medical therapy only Compared survival between groups and identified when survival diverged between surgical and non-surgical groups Identified pre-operative variables that differed between surgical groups based on follow-up Pre-operative Risk Factors based on significance in multivariate analysis Culp et al., Cancer, 2010
40 Surgery vs. No Surgery Overall Survival Overall Survival Basedon Follow up of 8.5 months Culp et al., Cancer, 2010
41 Pre-operative Risk Factors Serum albumin < lower limit of normal Serum LDH > upper limit of normal Liver metastasis Symptoms at presentation due to metastasis Retroperitoneal lymph node involvement Supra-diaphragmatic lymph node involvement Clinical T stage 3 or 4 Culp et al., Cancer, 2010
42 Pre-operative Assessment HR (95% CI) P Median Survival (mos) Medical Therapy Only CN - # of risk factors Referent (0.15, 0.30) < (0.25, 0.57) < (0.34, 0.57) < (0.48, 0.84) ( (0.54, 109) 1.09) (0.88, 2.80) (0.24, 4.00) Culp et al., Cancer, 2010
43 Pre-operative Assessment HR (95% CI) P Median Survival (mos) Medical Therapy Only CN - # of risk factors Referent (0.15, 0.30) < (0.25, 0.57) < (0.34, 0.57) < (0.48, 0.84) ( (0.54, 109) 1.09) (0.88, 2.80) (0.24, 4.00) Culp et al., Cancer, 2010
44 Pre-operative Assessment Culp et al., Cancer, 2010
45 Cytoreductive Nephrectomy In The Era of Targeted Therapy (SEER ) Predictive Clinical Factors 1. Size > 7 cm 2. ct3 or ct4 Stage 3. High grade (3 or 4) 4. Clinically + LN s 5. Sarcomatoid Histology Culp and Wood, Submitted
46 Canwedobetter? Is the relevant question whether or not surgery should be incorporated into the management of locally advanced/metastatic renal cell carcinoma?
47 Neoadjuvant (Pre-surgical) Therapy for Renal Cell Carcinoma Potential Benefits Primary tumor downstaging/sizing Decrease surgical morbidity Increase utilization of nephron sparing Make the unresectable become resectable Improve prognosis Eliminate/Downsize metastatic tumor burden Operate on responding patients (litmus test) Potential Risks May increase surgical morbidity Disease may progress (locally or metastatic) on therapy Therapy may alter biology of metastatic disease adversely VEGF rebound may actually cause rapid disease progression
48 Bevacizumab Presurgical Trial Metastatic disease, no prior nephrectomy or therapy Bevacizumab 10 mg/kg IV Q14 days Opened 4/05 Accrual to date: 50 Response Or Stable Progressive, Good PS Progressive, Poor PS 50 patients Clear Cell Histology Nephrectomy, Continue Bevacizumab Nephrectomy, New Chemo New Chemo, or Best Supportive Care Jonasch E et al., JCO, 2009
49 Sunitinib Presurgical Trial Metastatic disease, no prior nephrectomy or therapy Sunitinib 50mg Stable/Respond: Nephrectomy Mid By mouth 2 nd Continue Course 2 Courses Sunitinib June patients Clear Cell Histology
50 Rules of the Game in RCC Surgical Therapy Advances Neoadjuvant Therapy Advances 1. Oncologic equipoise 1. Safety (Lack of disease 2. Nephron sparing progression/increased surgical morbidity) 3. Minimally invasive 2. Improved patient t outcomes (DFS/CSS) 3. Primary tumor downstaging/downsizing
51 Is Neoadjuvant Therapy Safe?
52 Pre-Surgical Therapy: Is it safe? Retrospective review Synchronous M1 disease. Stratified by timing of initiation of targeted systemic therapies. Pre-operative systemic targeted therapy was administered to 70 patients (Pre-surgical). Immediate CN was performed in 103 patients, (Immediate). Complications occurring within 12 months of CN were assessed. Chapin et al. Eur Urol, 2011
53 Complications from cytoreductive nephrectomy by timing of nephrectomy. No. (%) Event All Patients Immediate CN Pre-surgical (n=173) (n=103) Therapy (n=73) p-value Any Complication (by patient) 99 (57.2) 53 (53.4) 39 (55.7) Clavien > 3 (by event) 69 (29.7) 32 (30.2.) 37 (29.4) Complication > 90 days (by event) 24 (10.3) 4 (3.8) 20 (15.9) >1 Complications (by event) 62 (62.6) 27 (50.9) 35 (76.1) Wound Complications+ 27 (15.6) 8 (7.8) 19 (27.1) <0.001 Superficial Wound Dehiscence 23 (13.3) 6 (5.8) 17 (24.3) <0.001 Wound Infection 12 (6.9) 3 (2.9) 9 (12.9) Fascial Dehiscence 2 (1.2) 0 (0) 2 (2.9) Incisional Hernia 3 (1.7) 0 (0) 3 (4.3) DVT 7 (4) 2 (1.9) 5 (7.1) PE 13 (7.5) 6 (5.8) 7(10) Wound Complications = Superficial wound dehiscence, wound infection and fascial dehiscence Chapin et al. Eur Urol, 2011
54 Predictors of Wound Complications After Cytoreductive Nephrectomy Characteristic Univariable Multivariate Odds Ratio (95% CI) p-value Odds Ratio (95% CI) p-value Pre-surgical Targeted Therapy* 4.42 ( ) < ( ) BMI 30* 2.46 ( ) ( ) Diabetic* 1.35 ( ) ( ) Smoker* 1.03 ( ) ( ) Duration of surgery* (per minute increase) 100( ( ) 0) ( ( ) 00) Clinical N1 or N2* 1.84 ( ) ( ) * included in multivariate analysis Chapin et al. Eur Urol, 2011
55 Predictors of Overall Post-operative Complications After Cytoreductive Nephrectomy Analysis of Preoperative and Post-operative Characteristics by risk of overall complications for all patients undergoing cytoreductive ti nephrectomy. Univariable Multivariate Characteristic Odds Ratio (95% CI) p-value Odds Ratio (95% CI) p-value ECOG 2* 9.1 ( ) ( ) Clinical N1 or N2* 2.5 ( ) ( ) Clinical T3 or T4* 20(1138) 2.0 ( ) ( ( ) Pre-surgical Targeted Therapy* 1.8 ( ) ( ) BMI ( ) * included in multivariate analysis Chapin et al. Eur Urol, 2011
56 Predictors of Overall Complications in Patients Receiving Pre-Surgical Targeted Therapy Characteristic i Univariable Multivariate Odds Ratio (95% CI) p-value Odds Ratio (95% CI) p-value Decline in Serum Albumin* 4.3 ( ) ( ) BMI 30* 38( ( ) (0689) 2.35 ( ) Clinical T3 or T4* 2.7 ( ) ( ) ECOG 2* 3.5 ( ) ( ) Charlson ( ) Received bevacizumab 1.4 ( ) * included in multivariate analysis Chapin et al. Eur Urol, 2011
57 Predictors of Overall Survival Characteristic Univariable Multivariate Odds Ratio (95% CI) p-value Odds Ratio (95% CI) p-value Pre-surgical Targeted Therapy* 0.96 ( ) ( ) T-Stage 3 or 4* 1.97 ( ) < ( ) Pathologic Node Positive* 2.53( ) < ( ) 26) < Sarcomatoid Histology* 2.53 ( ) < ( ) Post-operative Complication* 2.23( ) < ( ) ECOG>1 (at presentation) * included in multivariate analysis Chapin et al. Eur Urol, 2011




58 Accelerated Metastasis after Short-Term Treatment with a Potent Inhibitor of Tumor Angiogenesis John M.L. Ebos1, 2, Christina R. Lee1, William Cruz-Munoz1, Georg A. Bjarnason3, James G. Christensen4 and Robert S. Kerbel1, 2,, 1Molecular and Cellular Biology Research, Sunnybrook Health Sciences Centre, Toronto, ON M4N 3M5, Canada 2Department of Medical Biophysics, University of Toronto, Toronto, ON M5G 2M9, Canada 3Sunnybrook Odette Cancer Centre, Toronto, ON M5G 2M9, Canada 4Pfizer Global Research and Development, La Jolla Labs, La Jolla, CA 92121, USA








59 Neoadjuvant Therapy: Axitinib 81 y/o WM s/p 12 weeks Axitinib Bilateral T1b Gr 2
60 What about primary tumor downstaging/sizing?
61 Results of Therapy with Primary Tumor in Place Institution Number of patients Response Rate Response in Primary Tumor Median Survival (mos) NCI 51 6% 0% 13 Netherlands Cancer Institute % 0% 3
62 Presurgical targeted therapy 63 yo male treated with sunitinib prior to nephrectomy
63 Are These Anecdotes Or Can We Rely On These Agents To Reliably Downstage Tumors?
64 Response of Primary Tumor Sunitinib 17 Evaluable Patients 4PR 12 SD 1 PD Response Rate in Primary Tumor: 23% Mean Volume Reduction: 31% Van der Veldt et al., CCR, 2008
65 Response of Primary Tumor Sunitinib Thomas AA et al., J Urol 2009
66 Pre-Surgical Bevacizumab Therapy Primary Tumor Regression N=45 (%) >20% growth 1 (2) 10-20% %g growth 2 (4) 0-10% growth 19 (42) 1-10% shrinkage 13 (29) 11-20% shrinkage 7 (16) 20-30% shrinkage 3 (7) Jonasch E et al., JCO, 2009
67 Pre-surgical Sorafenib *4 patients downstaged from T2 to T1 *2 patients with RV thrombus on imaging were neg. on path *Median tumor shrinkage 96% 9.6% Cowey et al., JCO, 2010
68 Patient characteristics 168 patients Tumor size e96c 9.6 cm ( ) Age 59.1 ( ) Follow- up 11.6 months ( ) ECOG PS (73.2) 2 29 (16.1) 3 16 (9.5) Abel at al., Eur Urol, 2011
69 Clinical rationale for treatment with primary tumor in situ Widespread metastatic disease 52 (30.1) Enrolled in clinical trial 46 (27.4) Brain metastasis, sarcomatoid or non-clear histology in biopsy 30 (17.9) Doctor/ patient preference 17 (10.1) Poor PS/ comorbidities 16 (9.5) Unresectable primary 7 (4.2) Abel at al., Eur Urol, 2011
70 Types of targeted therapy RESULTS N % sunitinib bevicizumab bevicizumab/ erlotinib sorafenib temsirolimus bevicizumab/ chemo erlotinib pazopanib Sunitinib Bevacizumab + Erlotinib Temsirolimus Erlotinib Bevacizumab Sorafenib Bevacizumab + Chemo Pazopanib Total Abel at al., Eur Urol, 2011
71 Maximum overall response in primary tumor Median -7.1% Abel at al., Eur Urol, 2011
72 Impact of Pre-Surgical Targeted Therapy On Venous Tumor Thrombus Delacroix S et al., ASCO GU 2011
73 Clinically meaningful changes occurred in 25% of patients (12/48) table 3 Stable Disease in 75% 36/48 Progression occurred in 14.5% (7/48) Regression in 10.4% (5/48). No Cases of Pulmonary Embolism Delacroix S et al., ASCO GU 2011
74 Initial body of evidence would suggest that significant primary tumor downstaging will not be realized with the current generation of targeted therapy agents. The jury is still out with regards to the newer generation of agents in the pp pipeline.
75 Presurgical/Neoadjuvant Therapy 1. Is it safe? 2. Does it reliably downsize/downstage tumors? 3. Is this treatment paradigm an advancement in the care of patients?
76 Presurgical Bevacizumab Therapy 50 patients were enrolled in the trial 42 patients underwent nephrectomy 6 patients had disease progression and went on to salvage systemic therapy rather than nephrectomy Med PFS 11 mos; Overall Survival 25.4 mos Jonasch et al, J Clin Oncol
77 Is an Early Minor (>=10%) Primary Tumor Response Associated with Overall Survival? OBJECTIVE: to evaluate whether an early minor PT response was associated with improved overall survival in patients undergoing treatment with sunitinib Abel et al., Eur Urol, 2011
78 Maximum rate of decrease is early in therapy Pe ercent Respons se Days of Treatment Abel et al., Eur Urol, 2011
79 Early response associated with higher maximum primary tumor response Patients with Multiple Imaging Points 10% response in 1 st <10% response in 1 st 60 days 60 days (N=18) (N=43) Maximum response (range) % -7.2 % (-53.4, -14.3) (-33.8, 9.8) Time to maximum response (days) (range) 175 (54, 839) 154 (37, 531) Abel EJ, Culp SH et al. Eur Urol. 2011
80 Study Population 75 patients treated with sunitinib for metastatic RCC with primary tumor in place Median follow-up of 15 mos (IQR: 7.5, 30.2) Median treatment time of 160 days (IQR: 83, 260) Abel et al., Eur Urol, 2011
81 Significant predictors of overall survival from univariable analysis HR 95% CI PT response (decrease in diameter) <10% Referent. 10% and > 60 days , % and 60 days , 0.82 Venous thrombus , 1.73 Radiographic retroperitoneal lymphadenopathy , 3.59 Local symptoms at presentation , 3.77 ECOG performance status >= , 4.00 Liver metastases , 4.08 Multiple bone metastases , 4.29 Lactate dehydrogenase > ULN , 4.26 Absolute lymphocyte count < LLN , 5.14 Number of metastatic sites > , 5.18 Abel et al., Eur Urol, 2011
82 Independent predictors of overall survival on multivariable analysis HR 95% CI 10% PT response se in 60 days* , 08, 0.89 Renal vein or IVC thrombus , 1.63 Multiple bone metastases , 4.21 Lactate dehydrogenase > ULN , 4.63 Local symptoms at presentation , 5.84 Number of metastatic sites > , 6.52 Abel et al., Eur Urol, 2011
83 In targeted therapy: PT response better than established prognostic criteria at estimating overall survival Abel EJ and Culp SH, European Urology December 2011

84 Phase II Presurgical Sunitinib: Response in Primary Tumor Predicts Survival 2 cycles of Sunitinib N = 22 Bex A, et al., Urology 2011
85 Cytoreductive Nephrectomy For Metastatic Renal Cell Carcinoma in The Era of Targeted Therapy: Not a question of if but when?
86 Timing Of Cytoreductive Nephrectomy In Metastatic Renal Cell Carcinoma Untreated Metastatic Renal Cell Carcinoma With Primary Tumor In Place (PS 0-1, Surgical Candidate) Non Clear Cell Histology; Sarcomatoid Managed By Standard of Care or Other Clinical Protocol Biopsy To Establish Clear Cell Histology; Lack of Sarcomatoid Cytoreductive ti Sunitinib ib Nephrectomy 4/2 Sunitinib 4/2 X 2 cycles Primary: PFS Secondary: OS, Response Rate, Surgical morbidity/mortality Cytoreductive Nephrectomy A. Bex, EORTC
87 Integration Of Targeted Therapy With Surgery In RCC Targeted therapy has dramatically improved the outcomes for patients with metastatic RCC Efficacy in the adjuvant and neoadjuvant setting is still under investigation Without complete responses, surgery remains integral part of multi-disciplinary approach in metastatic disease Control of primary tumor Metastasectomy Reliable complete responses with any agent will force re-examination of current paradigm Presurgical approach may have merit but needs further study and validation Not clear when it is most appropriate to integrate surgery
Cytoreductive Nephrectomy
 Cytoreductive Nephrectomy Stephen H. Culp, M.D., Ph.D. Assistant Professor, Department of Urology Outline The Historics of CN The current status of CN The importance of patient selection Cytoreductive
Cytoreductive Nephrectomy Stephen H. Culp, M.D., Ph.D. Assistant Professor, Department of Urology Outline The Historics of CN The current status of CN The importance of patient selection Cytoreductive
Management of High Risk Renal Cell Carcinoma
 Management of High Risk Renal Cell Carcinoma Peter E. Clark, MD Professor and Chair, Department of Urology Carolinas HealthCare System Chair, Urologic Oncology Levine Cancer Institute October 14, 2017
Management of High Risk Renal Cell Carcinoma Peter E. Clark, MD Professor and Chair, Department of Urology Carolinas HealthCare System Chair, Urologic Oncology Levine Cancer Institute October 14, 2017
Multidisciplinary approach for renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute
 Multidisciplinary approach for renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute 20 April, Antalya, Turkey RCC European Union 60.000 new diagnoses/year 26.000 Cancer related deaths
Multidisciplinary approach for renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute 20 April, Antalya, Turkey RCC European Union 60.000 new diagnoses/year 26.000 Cancer related deaths
Surgical Management of Metastatic and Locally Recurrent Kidney Cancer: Does it Make Sense?
 Surgical Management of Metastatic and Locally Recurrent Kidney Cancer: Does it Make Sense? Philippe E. Spiess, MD, FACS Associate Member Department of GU Oncology Department of Tumor Biology Moffitt Cancer
Surgical Management of Metastatic and Locally Recurrent Kidney Cancer: Does it Make Sense? Philippe E. Spiess, MD, FACS Associate Member Department of GU Oncology Department of Tumor Biology Moffitt Cancer
Winship Cancer Institute of Emory University Neoadjuvant Systemic Therapy in Metastatic Renal Cell Carcinoma Patients
 Winship Cancer Institute of Emory University Neoadjuvant Systemic Therapy in Metastatic Renal Cell Carcinoma Patients Bradley Carthon, MD, PhD Assistant Professor, Genitourinary Medical Oncology Winship
Winship Cancer Institute of Emory University Neoadjuvant Systemic Therapy in Metastatic Renal Cell Carcinoma Patients Bradley Carthon, MD, PhD Assistant Professor, Genitourinary Medical Oncology Winship
Medical Management of Renal Cell Carcinoma
 Medical Management of Renal Cell Carcinoma Lin Mei, MD Hematology-Oncology Fellow Hematology, Oncology and Palliative Care Virginia Commonwealth University Educational Objectives Background of RCC (epidemiology,
Medical Management of Renal Cell Carcinoma Lin Mei, MD Hematology-Oncology Fellow Hematology, Oncology and Palliative Care Virginia Commonwealth University Educational Objectives Background of RCC (epidemiology,
David N. Robinson, MD
 David N. Robinson, MD Background and Treatment of mrcc Background ~ 64,770 new cases of kidney/renal pelvis cancers will be diagnosed in the US in 2012 with an estimated 13,570 deaths [1] ~ 75% are clear-cell
David N. Robinson, MD Background and Treatment of mrcc Background ~ 64,770 new cases of kidney/renal pelvis cancers will be diagnosed in the US in 2012 with an estimated 13,570 deaths [1] ~ 75% are clear-cell
Surgery of Renal Cell Carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute
 Surgery of Renal Cell Carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute 23 March 2012, Sao Paulo, Brazil Surgery of RCC Locally confined (small) renal tumours Locally advanced disease Metastatic
Surgery of Renal Cell Carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute 23 March 2012, Sao Paulo, Brazil Surgery of RCC Locally confined (small) renal tumours Locally advanced disease Metastatic
Metastatic renal cancer (mrcc): Evidence-based treatment
: Evidence-based treatment") Metastatic renal cancer (mrcc): Evidence-based treatment José M. Ruiz Morales, M.D. Hospital Médica Sur April 18th, 2018 4th ESO-ESMO Latin American Masterclass in Clinical Oncology Disclosures Consulting:
Metastatic renal cancer (mrcc): Evidence-based treatment José M. Ruiz Morales, M.D. Hospital Médica Sur April 18th, 2018 4th ESO-ESMO Latin American Masterclass in Clinical Oncology Disclosures Consulting:
Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors?
 Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors? Bernard Escudier Institut Gustave Roussy Villejuif, France EIKCS Lyon April 2015 What is the current role of mtor inhibitors?
Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors? Bernard Escudier Institut Gustave Roussy Villejuif, France EIKCS Lyon April 2015 What is the current role of mtor inhibitors?
Evidenze cliniche nel trattamento del RCC
 Criteri di scelta nel trattamento sistemico del carcinoma renale Evidenze cliniche nel trattamento del RCC Alessandro Morabito Unità Sperimentazioni Cliniche Istituto Nazionale Tumori di Napoli Napoli,
Criteri di scelta nel trattamento sistemico del carcinoma renale Evidenze cliniche nel trattamento del RCC Alessandro Morabito Unità Sperimentazioni Cliniche Istituto Nazionale Tumori di Napoli Napoli,
Lymphadenectomy in RCC: Yes, No, Clinical Trial?
 Lymphadenectomy in RCC: Yes, No, Clinical Trial? Viraj Master MD PhD FACS Professor Associate Chair for Clinical Affairs and Quality Director of Clinical Research Unit Department of Urology Emory University
Lymphadenectomy in RCC: Yes, No, Clinical Trial? Viraj Master MD PhD FACS Professor Associate Chair for Clinical Affairs and Quality Director of Clinical Research Unit Department of Urology Emory University
INTEGRATION OF SURGERY AND SYSTEMIC THERAPY FOR ADVANCED RENAL CELL CARCINOMA IN THE TARGETED THERAPY ERA
 INTEGRATION OF SURGERY AND SYSTEMIC THERAPY FOR ADVANCED RENAL CELL CARCINOMA IN THE TARGETED THERAPY ERA Dr. Michael J. Metcalfe PGY-4 Department of Urologic Sciences University of British Columbia October
INTEGRATION OF SURGERY AND SYSTEMIC THERAPY FOR ADVANCED RENAL CELL CARCINOMA IN THE TARGETED THERAPY ERA Dr. Michael J. Metcalfe PGY-4 Department of Urologic Sciences University of British Columbia October
Immunotherapy versus targeted treatments in metastatic renal cell carcinoma: The return game?
 Immunotherapy versus targeted treatments in metastatic renal cell carcinoma: The return game? Sylvie NEGRIER MD, PhD Centre Léon Bérard, Lyon Université Lyon I IMMUNOTHERAPY: A LONG AND WIDING ROAD! WHERE
Immunotherapy versus targeted treatments in metastatic renal cell carcinoma: The return game? Sylvie NEGRIER MD, PhD Centre Léon Bérard, Lyon Université Lyon I IMMUNOTHERAPY: A LONG AND WIDING ROAD! WHERE
Sequencing of therapies in mrcc. Ari Hakimi MD Assistant Professor Urology Service, Department of Surgery MSKCC
 Sequencing of therapies in mrcc Ari Hakimi MD Assistant Professor Urology Service, Department of Surgery MSKCC Old Paradigm Sequencing approved agents VEGF TKI Sunitinib Pazopanib Axitinib TKI TKI MTORi
Sequencing of therapies in mrcc Ari Hakimi MD Assistant Professor Urology Service, Department of Surgery MSKCC Old Paradigm Sequencing approved agents VEGF TKI Sunitinib Pazopanib Axitinib TKI TKI MTORi
I Kid(ney) You Not: Updates on Renal Cell Carcinoma
 You Not: Updates on Renal Cell Carcinoma") Disclosures I Kid(ney) You Not: Updates on Renal Cell Carcinoma Nothing to disclose Renee McAlister, PharmD, BCOP Clinical Pharmacist, GU/Melanoma Vanderbilt Ingram Cancer Center September 29, 2018 Objectives
Disclosures I Kid(ney) You Not: Updates on Renal Cell Carcinoma Nothing to disclose Renee McAlister, PharmD, BCOP Clinical Pharmacist, GU/Melanoma Vanderbilt Ingram Cancer Center September 29, 2018 Objectives
Adjuvant therapy: Additional cancer treatment given after the primary treatment to lower the risk that the cancer will come back
 Adjuvant therapy: Additional cancer treatment given after the primary treatment to lower the risk that the cancer will come back Neo adjuvant therapy: Treatment given as a first step to shrink a tumor
Adjuvant therapy: Additional cancer treatment given after the primary treatment to lower the risk that the cancer will come back Neo adjuvant therapy: Treatment given as a first step to shrink a tumor
Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better?
 Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better? 9 th European Kidney Cancer Symposium, Dublin, April 2014 Tim Eisen Tim Eisen - Disclosures Company Research Support Advisory Board Trial
Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better? 9 th European Kidney Cancer Symposium, Dublin, April 2014 Tim Eisen Tim Eisen - Disclosures Company Research Support Advisory Board Trial
Debate: Lymphadenectomy is Important in mrcc, CON P. Mulder, M.D., Ph.D. JJ. Patard, MD, Ph.D.
 Debate: Lymphadenectomy is Important in mrcc, CON P. Mulder, M.D., Ph.D. JJ. Patard, MD, Ph.D.. Eighth European International Kidney Cancer Symposium Budapest 03-04 May 2013 The role of LND In organ confined
Debate: Lymphadenectomy is Important in mrcc, CON P. Mulder, M.D., Ph.D. JJ. Patard, MD, Ph.D.. Eighth European International Kidney Cancer Symposium Budapest 03-04 May 2013 The role of LND In organ confined
Complex case Presentations
 Complex case Presentations Case Presentations April 2016 Lisa M Pickering Case presentations: chromophobe renal carcinoma 60 year old man. ECOG PS 0 No significant comorbodities August 2009: L radical
Complex case Presentations Case Presentations April 2016 Lisa M Pickering Case presentations: chromophobe renal carcinoma 60 year old man. ECOG PS 0 No significant comorbodities August 2009: L radical
Patient Selection for Surgery in RCC with Thrombus. E. Jason Abel, M.D.
 Patient Selection for Surgery in RCC with Thrombus E. Jason Abel, M.D. RCC with venous invasion Venous invasion occurs in ~10% of RCC Surgery more complex Increased risk for morbidity Thrombus may be confined
Patient Selection for Surgery in RCC with Thrombus E. Jason Abel, M.D. RCC with venous invasion Venous invasion occurs in ~10% of RCC Surgery more complex Increased risk for morbidity Thrombus may be confined
When to Integrate Surgery for Metatstatic Urothelial Cancers
 When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
Tratamiento adyuvante y neoadyuvante del cáncer renal en Xavier Garcia del Muro Solans Institut Català d Oncologia Hospitalet.
 Tratamiento adyuvante y neoadyuvante del cáncer renal en 2017 Xavier Garcia del Muro Solans Institut Català d Oncologia Hospitalet. Barcelona Pronóstico del CR mediante un sistema integrado en 468 pts
Tratamiento adyuvante y neoadyuvante del cáncer renal en 2017 Xavier Garcia del Muro Solans Institut Català d Oncologia Hospitalet. Barcelona Pronóstico del CR mediante un sistema integrado en 468 pts
Timing of targeted therapy in patients with low volume mrcc. Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital
 1 Timing of targeted therapy in patients with low volume mrcc Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital 2 Wont be discussing: Symptomatic patients High volume disease Rapidly growing metastases
1 Timing of targeted therapy in patients with low volume mrcc Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital 2 Wont be discussing: Symptomatic patients High volume disease Rapidly growing metastases
Atezolizumab Adjuvant Study: Medical Oncologist Perspective. Sumanta K. Pal, MD City of Hope Comprehensive Cancer Center
 Atezolizumab Adjuvant Study: Medical Oncologist Perspective Sumanta K. Pal, MD City of Hope Comprehensive Cancer Center Trial overview Key issues Outline Challenges with neoadjuvant therapy Placebo control
Atezolizumab Adjuvant Study: Medical Oncologist Perspective Sumanta K. Pal, MD City of Hope Comprehensive Cancer Center Trial overview Key issues Outline Challenges with neoadjuvant therapy Placebo control
Fifteenth International Kidney Cancer Symposium
 The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
Oncology A Phase II Study of Presurgical Sunitinib in Patients with Metastatic Clear-cell Renal Carcinoma and the Primary Tumor In Situ
 Oncology A Phase II Study of Presurgical Sunitinib in Patients with Metastatic Clear-cell Renal Carcinoma and the Primary Tumor In Situ Axel Bex, Christian Blank, Wim Meinhardt, Harm van Tinteren, Simon
Oncology A Phase II Study of Presurgical Sunitinib in Patients with Metastatic Clear-cell Renal Carcinoma and the Primary Tumor In Situ Axel Bex, Christian Blank, Wim Meinhardt, Harm van Tinteren, Simon
The Really Important Questions Current Immunotherapy Trials are Not Answering
 The Really Important Questions Current Immunotherapy Trials are Not Answering David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/Harvard Cancer Center Harvard Medical School PD-1 Pathway
The Really Important Questions Current Immunotherapy Trials are Not Answering David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/Harvard Cancer Center Harvard Medical School PD-1 Pathway
Targeted and immunotherapy in RCC
 Targeted and immunotherapy in RCC Treatment options Surgery (radical VS partial nephrectomy) Thermal ablation therapy Surveillance Immunotherapy Molecular targeted therapy Molecular targeted therapy Targeted
Targeted and immunotherapy in RCC Treatment options Surgery (radical VS partial nephrectomy) Thermal ablation therapy Surveillance Immunotherapy Molecular targeted therapy Molecular targeted therapy Targeted
Renal Cell Carcinoma: Status of Medical and Surgical Therapy. Ronald M. Bukowski Emeritus Physician Cleveland Clinic Foundation
 Renal Cell Carcinoma: Status of Medical and Surgical Therapy Ronald M. Bukowski Emeritus Physician Cleveland Clinic Foundation Metastatic Renal Cell Carcinoma: Evolution of Current Therapeutic Approaches
Renal Cell Carcinoma: Status of Medical and Surgical Therapy Ronald M. Bukowski Emeritus Physician Cleveland Clinic Foundation Metastatic Renal Cell Carcinoma: Evolution of Current Therapeutic Approaches
Indications For Partial
 Indications For Partial Nephrectomy Christopher G. Wood, M. D., FACS Professor and Deputy Chairman Douglas E. Johnson, M. D. Endowed Professorship in Urology Department of Urology The University of Texas
Indications For Partial Nephrectomy Christopher G. Wood, M. D., FACS Professor and Deputy Chairman Douglas E. Johnson, M. D. Endowed Professorship in Urology Department of Urology The University of Texas
Linee guida terapeutiche oncologiche. Francesco Massari U.O.C. di Oncologia Medica d.u. Azienda Ospedaliera Universitaria Integrata Verona
 Linee guida terapeutiche oncologiche Francesco Massari U.O.C. di Oncologia Medica d.u. Azienda Ospedaliera Universitaria Integrata Verona 1 YOUNG SPECIALIST RENAL CARE Verona, 07-08 Marzo 2014 Clinical
Linee guida terapeutiche oncologiche Francesco Massari U.O.C. di Oncologia Medica d.u. Azienda Ospedaliera Universitaria Integrata Verona 1 YOUNG SPECIALIST RENAL CARE Verona, 07-08 Marzo 2014 Clinical
Complete Remission is a Reachable Goal in mrcc L. Albiges Institut Gustave Roussy
 Complete Remission is a Reachable Goal in mrcc L. Albiges Institut Gustave Roussy Is complete remission an achievable goal in mrcc? Lessons from observation Lessons from immunotherapy Current status in
Complete Remission is a Reachable Goal in mrcc L. Albiges Institut Gustave Roussy Is complete remission an achievable goal in mrcc? Lessons from observation Lessons from immunotherapy Current status in
Metastatic Renal Cancer Medical Treatment
 Metastatic Renal Cancer Medical Treatment Bohuslav Melichar, M.D., Ph.D. Professor and Head Department of Oncology Palacký University Medical School and Teaching Hospital Olomouc, Czech Republic Peculiarities
Metastatic Renal Cancer Medical Treatment Bohuslav Melichar, M.D., Ph.D. Professor and Head Department of Oncology Palacký University Medical School and Teaching Hospital Olomouc, Czech Republic Peculiarities
New strategies and future of target therapy in advanced kidney cancer
 New strategies and future of target therapy in advanced kidney cancer VHL Gene Inactivation VHL Complex Disrupted VHL Protein HIF1-a, HIF2-a Accumulation VEGF PDGF TGF-α, CXCR4 Angiogenesis Endothelial
New strategies and future of target therapy in advanced kidney cancer VHL Gene Inactivation VHL Complex Disrupted VHL Protein HIF1-a, HIF2-a Accumulation VEGF PDGF TGF-α, CXCR4 Angiogenesis Endothelial
CLINICAL CHALLENGES IN METASTATIC RENAL CELL CARCINOMA: THE RIGHT THERAPY FOR THE RIGHT PATIENT
 Daniel Heng, MD, MPH, FRCPC @DrDanielHeng Chair GU Tumour Group, Tom Baker Cancer Centre Clinical Professor, University of Calgary CLINICAL CHALLENGES IN METASTATIC RENAL CELL CARCINOMA: THE RIGHT THERAPY
Daniel Heng, MD, MPH, FRCPC @DrDanielHeng Chair GU Tumour Group, Tom Baker Cancer Centre Clinical Professor, University of Calgary CLINICAL CHALLENGES IN METASTATIC RENAL CELL CARCINOMA: THE RIGHT THERAPY
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy
 Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Dose individualization of sunitinib in mrcc: Toxicity-adjusted dose or Therapeutic drug monitoring
 Dose individualization of sunitinib in mrcc: Toxicity-adjusted dose or Therapeutic drug monitoring Alison Zhang 1, Peter Fox 1, Sally Coulter 4, Val Gebski 5, Bavanthi Balakrishnar 1, Christopher Liddle
Dose individualization of sunitinib in mrcc: Toxicity-adjusted dose or Therapeutic drug monitoring Alison Zhang 1, Peter Fox 1, Sally Coulter 4, Val Gebski 5, Bavanthi Balakrishnar 1, Christopher Liddle
Renal Cell Carcinoma: Systemic Therapy Progress and Promise
 Renal Cell Carcinoma: Systemic Therapy Progress and Promise Michael B. Atkins, M.D. Deputy Director, Lombardi Comprehensive Cancer Ctr Georgetown University Medical Center Everolimus Rini, Campbell, Escudier.
Renal Cell Carcinoma: Systemic Therapy Progress and Promise Michael B. Atkins, M.D. Deputy Director, Lombardi Comprehensive Cancer Ctr Georgetown University Medical Center Everolimus Rini, Campbell, Escudier.
Treatment Algorithm and Therapy Management in mrcc. Manuela Schmidinger Medical University of Vienna Austria
 Treatment Algorithm and Therapy Management in mrcc Manuela Schmidinger Medical University of Vienna Austria A Paradigm Shift in the Treatment of mrcc 1. Sunitinib 2. Sorafenib 3. Bevacizumab+IFN-alpha
Treatment Algorithm and Therapy Management in mrcc Manuela Schmidinger Medical University of Vienna Austria A Paradigm Shift in the Treatment of mrcc 1. Sunitinib 2. Sorafenib 3. Bevacizumab+IFN-alpha
Innovaciones en el tratamiento del ca ncer renal. Enrique Grande
 Innovaciones en el tratamiento del ca ncer renal Enrique Grande The enriched inflammatory environment of RCC Chen Z, et al. Nat Rev Cancer 2014 Available agents are expanding across the three eras of arcc
Innovaciones en el tratamiento del ca ncer renal Enrique Grande The enriched inflammatory environment of RCC Chen Z, et al. Nat Rev Cancer 2014 Available agents are expanding across the three eras of arcc
Reference No: Author(s) Approval date: June Committee. Operational Date: July Review:
 Approval date: June Committee. Operational Date: July Review:") Reference No: Title: Author(s) Systemic anti-cancer therapy (SACT) guidelines for renal cell cancer Dr Alison Clayton Consultant Medical Oncologist & Dr Jane Hurwitz Consultant Medical Oncologist, Cancer
Reference No: Title: Author(s) Systemic anti-cancer therapy (SACT) guidelines for renal cell cancer Dr Alison Clayton Consultant Medical Oncologist & Dr Jane Hurwitz Consultant Medical Oncologist, Cancer
Cytoreductive nephrectomy and its role in the present-day period of targeted therapy
 585501TAU0010.1177/1756287215585501Therapeutic Advances in UrologySH Culp review-article2015 Therapeutic Advances in Urology Review Cytoreductive nephrectomy and its role in the present-day period of targeted
585501TAU0010.1177/1756287215585501Therapeutic Advances in UrologySH Culp review-article2015 Therapeutic Advances in Urology Review Cytoreductive nephrectomy and its role in the present-day period of targeted
Emerging Biomarkers of VEGF and mtor Inhibitors in 2015
 Emerging Biomarkers of VEGF and mtor Inhibitors in 2015 Laurence Albiges Institut Gustave Roussy, France Fourteenth International Kidney Cancer Symposium Miami, Florida, USA November 6-7, 2015 www.kidneycancersymposium.com
Emerging Biomarkers of VEGF and mtor Inhibitors in 2015 Laurence Albiges Institut Gustave Roussy, France Fourteenth International Kidney Cancer Symposium Miami, Florida, USA November 6-7, 2015 www.kidneycancersymposium.com
RCC in Adolescents and Young Adults (AYAs): Diagnosis and Management
: Diagnosis and Management") RCC in Adolescents and Young Adults (AYAs): Diagnosis and Management Nicholas G. Cost, M.D. Assistant Professor, Department of Surgery, Division of Urology University of Colorado Cancer Center Fifteenth
RCC in Adolescents and Young Adults (AYAs): Diagnosis and Management Nicholas G. Cost, M.D. Assistant Professor, Department of Surgery, Division of Urology University of Colorado Cancer Center Fifteenth
Prognostic Factors for mrcc: Relevance in Clinical Practice
 Prognostic Factors for mrcc: Relevance in Clinical Practice Daniel Heng MD MPH FRCPC Chair, GU Tumor Group Tom Baker Cancer Center University of Calgary Prognostic Factors Patient Factors Performance Status
Prognostic Factors for mrcc: Relevance in Clinical Practice Daniel Heng MD MPH FRCPC Chair, GU Tumor Group Tom Baker Cancer Center University of Calgary Prognostic Factors Patient Factors Performance Status
Cytoreductive Nephrectomy vs Medical Therapy as Initial Treatment: A Rational Approach to the Sequence Question in Metastatic Renal Cell Carcinoma
 Clinical factors challenge the multidisciplinary team to reach a personalized treatment decision algorithm. Dorothy Fox. Soweto Woman. Watercolor on paper, 30 36. Cytoreductive Nephrectomy vs Medical Therapy
Clinical factors challenge the multidisciplinary team to reach a personalized treatment decision algorithm. Dorothy Fox. Soweto Woman. Watercolor on paper, 30 36. Cytoreductive Nephrectomy vs Medical Therapy
Surgeons Perspective: LN as a Draining Pattern. Jose A. Karam, MD, FACS Associate Professor Department of Urology
 Surgeons Perspective: LN as a Draining Pattern Jose A. Karam, MD, FACS Associate Professor Department of Urology Disclosures EMD Serono, Pfizer, Novartis: Advisory board/consultant Disclosures I perform
Surgeons Perspective: LN as a Draining Pattern Jose A. Karam, MD, FACS Associate Professor Department of Urology Disclosures EMD Serono, Pfizer, Novartis: Advisory board/consultant Disclosures I perform
Renal Cell Cancer. Clinical case study 1 & 2. Petri Bono MD PhD Helsinki University Hospital Helsinki, Finland
 Renal Cell Cancer Clinical case study 1 & 2 Petri Bono MD PhD Helsinki University Hospital Helsinki, Finland 1 Case study 1 - RCC and Lung Metastases Case study 1: Patient History Male, 63 years old Mild
Renal Cell Cancer Clinical case study 1 & 2 Petri Bono MD PhD Helsinki University Hospital Helsinki, Finland 1 Case study 1 - RCC and Lung Metastases Case study 1: Patient History Male, 63 years old Mild
SBRT for lung metastases: Case report
 SBRT for lung metastases: Case report Guillermo de Velasco MD, PhD University Hospital 12 de Octubre @H12O_GUCancer @g_develasco Case report 71 years old man Smoker DM 2005 Right radical nephrectomy Histology:
SBRT for lung metastases: Case report Guillermo de Velasco MD, PhD University Hospital 12 de Octubre @H12O_GUCancer @g_develasco Case report 71 years old man Smoker DM 2005 Right radical nephrectomy Histology:
Developping the next generation of studies in RCC
 Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
A Review in the Treatment Options for Renal Cell Cancer
 A Review in the Treatment Options for Renal Cell Cancer Ali McBride, PharmD, MS BCPS, BCOP Clinical Coordinator Hematology/Oncology Department of Pharmacy The University of Arizona Cancer Center RENAL
A Review in the Treatment Options for Renal Cell Cancer Ali McBride, PharmD, MS BCPS, BCOP Clinical Coordinator Hematology/Oncology Department of Pharmacy The University of Arizona Cancer Center RENAL
Treatment of Renal Cell Carcinoma (RCC) in the Era of Targeted Agents
 in the Era of Targeted Agents") Conflict of Interest Treatment of Renal Cell Carcinoma (RCC) in the Era of Targeted Agents None Patrick Medina, PharmD, BCOP Associate Professor University of Oklahoma OKC, OK Learning Objectives Epidemiology
Conflict of Interest Treatment of Renal Cell Carcinoma (RCC) in the Era of Targeted Agents None Patrick Medina, PharmD, BCOP Associate Professor University of Oklahoma OKC, OK Learning Objectives Epidemiology
Prognostic Factors: Does It Really Matter if New Drugs for Targeted Therapy Will Be Used?
 european urology supplements 8 (2009) 478 482 available at www.sciencedirect.com journal homepage: www.europeanurology.com Prognostic Factors: Does It Really Matter if New Drugs for Targeted Therapy Will
european urology supplements 8 (2009) 478 482 available at www.sciencedirect.com journal homepage: www.europeanurology.com Prognostic Factors: Does It Really Matter if New Drugs for Targeted Therapy Will
Guidelines on Renal Cell
 Guidelines on Renal Cell Carcinoma (Text update March 2009) B. Ljungberg (Chairman), D.C. Hanbury, M.A. Kuczyk, A.S. Merseburger, P.F.A. Mulders, J-J. Patard, I.C. Sinescu Introduction Renal cell carcinoma
Guidelines on Renal Cell Carcinoma (Text update March 2009) B. Ljungberg (Chairman), D.C. Hanbury, M.A. Kuczyk, A.S. Merseburger, P.F.A. Mulders, J-J. Patard, I.C. Sinescu Introduction Renal cell carcinoma
Sergio Bracarda MD. Head, Medical Oncology Department of Oncology AUSL-8 Istituto Toscano Tumori (ITT) San Donato Hospital Arezzo, Italy
 San Donato Hospital Arezzo, Italy") Sergio Bracarda MD Head, Medical Oncology Department of Oncology AUSL-8 Istituto Toscano Tumori (ITT) San Donato Hospital Arezzo, Italy Ninth European International Kidney Cancer Symposium Dublin 25-26
Sergio Bracarda MD Head, Medical Oncology Department of Oncology AUSL-8 Istituto Toscano Tumori (ITT) San Donato Hospital Arezzo, Italy Ninth European International Kidney Cancer Symposium Dublin 25-26
pan-canadian Oncology Drug Review Stakeholder Feedback on a pcodr Request for Advice Axitinib (Inlyta) for Metastatic Renal Cell Carcinoma
 for Metastatic Renal Cell Carcinoma") pan-canadian Oncology Drug Review Stakeholder Feedback on a pcodr Request for Advice Axitinib (Inlyta) for Metastatic Renal Cell Carcinoma Pfizer Canada Inc. June 29, 2017 3 Stakeholder Feedback on a pcodr
pan-canadian Oncology Drug Review Stakeholder Feedback on a pcodr Request for Advice Axitinib (Inlyta) for Metastatic Renal Cell Carcinoma Pfizer Canada Inc. June 29, 2017 3 Stakeholder Feedback on a pcodr
Neoadjuvant vs. Adjuvant Chemotherapy for Muscle-Invasive Bladder Cancer
 Neoadjuvant vs. Adjuvant Chemotherapy for Muscle-Invasive Bladder Cancer Andrew J. Stephenson, MD, FRCSC, FACS Director, Urologic Oncology Associate Professor of Surgery Glickman Urological and Kidney
Neoadjuvant vs. Adjuvant Chemotherapy for Muscle-Invasive Bladder Cancer Andrew J. Stephenson, MD, FRCSC, FACS Director, Urologic Oncology Associate Professor of Surgery Glickman Urological and Kidney
CANCER UROLOGY VOL. 12. P. S. Borisov 1, M. I. Shkol nik 2, R. V. Orlova 3, P. A. Karlov 1 DOI: /
 CANCER UROLOGY 3 6 VOL. The use of targeted therapies and selection of the optimal treatment sequence in heterogeneous population of patients with metastatic kidney cancer. Results of retrospective study
CANCER UROLOGY 3 6 VOL. The use of targeted therapies and selection of the optimal treatment sequence in heterogeneous population of patients with metastatic kidney cancer. Results of retrospective study
CON: Removal of the Breast Primary in Patients with Metastatic Breast Cancer
 CON: Removal of the Breast Primary in Patients with Metastatic Breast Cancer Amelia B. Zelnak, M.D., M.Sc. Assistant Professor of Hematology and Medical Oncology Winship Cancer Institute Emory University
CON: Removal of the Breast Primary in Patients with Metastatic Breast Cancer Amelia B. Zelnak, M.D., M.Sc. Assistant Professor of Hematology and Medical Oncology Winship Cancer Institute Emory University
Angiogenesis Targeted Therapies in Renal Cell Carcinoma
 Angiogenesis Targeted Therapies in Renal Cell Carcinoma John S. Lam, MD Department of Urology David Geffen School of Medicine University of California-Los Angeles Patient Case CC: Abdominal pain VS: T
Angiogenesis Targeted Therapies in Renal Cell Carcinoma John S. Lam, MD Department of Urology David Geffen School of Medicine University of California-Los Angeles Patient Case CC: Abdominal pain VS: T
Management of Locally Reccurent Renal Cell Carcinoma. Jose A. Karam, MD, FACS Assistant Professor Department of Urology
 Management of Locally Reccurent Renal Cell Carcinoma Jose A. Karam, MD, FACS Assistant Professor Department of Urology DefiniAons Defini&ve treatment Aiming for cure Abla&on therapy Radiofrequency abla&on
Management of Locally Reccurent Renal Cell Carcinoma Jose A. Karam, MD, FACS Assistant Professor Department of Urology DefiniAons Defini&ve treatment Aiming for cure Abla&on therapy Radiofrequency abla&on
Medical treatment of metastatic renal cell carcinoma (mrcc) in the elderly ( 65y): Position of a SIOG Taskforce
 in the elderly ( 65y): Position of a SIOG Taskforce") Medical treatment of metastatic renal cell carcinoma (mrcc) in the elderly ( 65y): Position of a SIOG Taskforce Medical treatment of metastatic RCC in the elderly ( 65y): Members of the SIOG Taskforce
Medical treatment of metastatic renal cell carcinoma (mrcc) in the elderly ( 65y): Position of a SIOG Taskforce Medical treatment of metastatic RCC in the elderly ( 65y): Members of the SIOG Taskforce
Carcinoma renale (I): Posters Review. Elena Verzoni Oncologia Medica 1 SS.Oncologia Genitourinaria Fondazione IRCCS Istituto Nazionale Tumori Milano
: Posters Review. Elena Verzoni Oncologia Medica 1 SS.Oncologia Genitourinaria Fondazione IRCCS Istituto Nazionale Tumori Milano") Carcinoma renale (I): Posters Review Elena Verzoni Oncologia Medica 1 SS.Oncologia Genitourinaria Fondazione IRCCS Istituto Nazionale Tumori Milano Agenda: Best Posters in Localized RCC Surgery: CN (#
Carcinoma renale (I): Posters Review Elena Verzoni Oncologia Medica 1 SS.Oncologia Genitourinaria Fondazione IRCCS Istituto Nazionale Tumori Milano Agenda: Best Posters in Localized RCC Surgery: CN (#
Second - Line Debate: Axitinib
 Second - Line Debate: Axitinib Alain Ravaud, MD PhD Bordeaux, France DISCLOSURES Member of Global, European and/or French advisory board in RCC and/or GU tumors for Pfizer, Novartis, GSK, Roche, BMS, Merck.
Second - Line Debate: Axitinib Alain Ravaud, MD PhD Bordeaux, France DISCLOSURES Member of Global, European and/or French advisory board in RCC and/or GU tumors for Pfizer, Novartis, GSK, Roche, BMS, Merck.
The Therapeutic Landscape in Advanced Renal Cell Carcinoma
 The Therapeutic Landscape in Advanced Renal Cell Carcinoma Cora Sternberg, MD, FACP Chairman, Department of Medical Oncology San Camillo-Forlanini Hospital Rome, Italy What best describes the change in
The Therapeutic Landscape in Advanced Renal Cell Carcinoma Cora Sternberg, MD, FACP Chairman, Department of Medical Oncology San Camillo-Forlanini Hospital Rome, Italy What best describes the change in
The High-Dose Aldesleukin (IL-2) Select Trial in Patients with Metastatic RCC
 Select Trial in Patients with Metastatic RCC") The High-Dose Aldesleukin (IL-2) Select Trial in Patients with Metastatic RCC D McDermott, M Ghebremichael, S Signoretti, K Margolin, J Clark, J Sosman, J Dutcher, T Logan, R Figlin and M Atkins on behalf
The High-Dose Aldesleukin (IL-2) Select Trial in Patients with Metastatic RCC D McDermott, M Ghebremichael, S Signoretti, K Margolin, J Clark, J Sosman, J Dutcher, T Logan, R Figlin and M Atkins on behalf
The role of cytoreductive. nephrectomy in elderly patients. with metastatic renal cell. carcinoma in an era of targeted. therapy
 The role of cytoreductive nephrectomy in elderly patients with metastatic renal cell carcinoma in an era of targeted therapy Dipesh Uprety, MD Amir Bista, MD Yazhini Vallatharasu, MD Angela Smith, MA David
The role of cytoreductive nephrectomy in elderly patients with metastatic renal cell carcinoma in an era of targeted therapy Dipesh Uprety, MD Amir Bista, MD Yazhini Vallatharasu, MD Angela Smith, MA David
Case(s): How to Deal with Mixed Response Giuseppe Procopio
: How to Deal with Mixed Response Giuseppe Procopio") Case(s): How to Deal with Mixed Response Giuseppe Procopio Fondazione IRCCS Istituto Nazionale dei Tumori, Milano Disclosures Advisory: Astellas, Bayer, GSK Consultant: Pfizer, Novartis Background Mixed
Case(s): How to Deal with Mixed Response Giuseppe Procopio Fondazione IRCCS Istituto Nazionale dei Tumori, Milano Disclosures Advisory: Astellas, Bayer, GSK Consultant: Pfizer, Novartis Background Mixed
Characterization of Patients with Poor-
 Characterization of Patients with Poor- Risk Metastatic Renal Cell Carcinoma Hamieh L 1 *, McKay RR 1 *, Lin X 2, Simantov R 2, Choueiri TK 1 *Equal contributions 1 Dana-Farber Cancer Institute, Boston,
Characterization of Patients with Poor- Risk Metastatic Renal Cell Carcinoma Hamieh L 1 *, McKay RR 1 *, Lin X 2, Simantov R 2, Choueiri TK 1 *Equal contributions 1 Dana-Farber Cancer Institute, Boston,
Sequential Therapy in Renal Cell Carcinoma*
 Sequential Therapy in Renal Cell Carcinoma* Bernard Escudier, MD, Marine Gross Goupil, MD, Christophe Massard, MD, and Karim Fizazi, MD, PhD Because of the recent approval of several drugs for the treatment
Sequential Therapy in Renal Cell Carcinoma* Bernard Escudier, MD, Marine Gross Goupil, MD, Christophe Massard, MD, and Karim Fizazi, MD, PhD Because of the recent approval of several drugs for the treatment
The Rationale for Immunotherapy as an Adjuvant Treatment for Locally Advanced BC
 The Rationale for Immunotherapy as an Adjuvant Treatment for Locally Advanced BC Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology Baylor College
The Rationale for Immunotherapy as an Adjuvant Treatment for Locally Advanced BC Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology Baylor College
GUIDELINES ON RENAL CELL CARCINOMA
 GUIDELINES ON RENAL CELL CARCINOMA B. Ljungberg (chairman), D.C. Hanbury, M.A. Kuczyk, A.S. Merseburger, P.F.A. Mulders, J-J. Patard, I.C. Sinescu Introduction This EAU guideline was prepared to help urologists
GUIDELINES ON RENAL CELL CARCINOMA B. Ljungberg (chairman), D.C. Hanbury, M.A. Kuczyk, A.S. Merseburger, P.F.A. Mulders, J-J. Patard, I.C. Sinescu Introduction This EAU guideline was prepared to help urologists
Targeted Therapy in Advanced Renal Cell Carcinoma
 Targeted Therapy in Advanced Renal Cell Carcinoma Brian I. Rini, M.D. Department of Solid Tumor Oncology Glickman Urologic and Kidney Institute Cleveland Clinic Taussig Cancer Institute Cleveland, Ohio
Targeted Therapy in Advanced Renal Cell Carcinoma Brian I. Rini, M.D. Department of Solid Tumor Oncology Glickman Urologic and Kidney Institute Cleveland Clinic Taussig Cancer Institute Cleveland, Ohio
Integrating novel therapy in advanced renal cell carcinoma
 Integrating novel therapy in advanced renal cell carcinoma Tian Zhang, MD Assistant Professor of Medicine GU Oncology Duke Cancer Institute March 11, 2017 Disclosures Research Funding Janssen Pfizer Consultant
Integrating novel therapy in advanced renal cell carcinoma Tian Zhang, MD Assistant Professor of Medicine GU Oncology Duke Cancer Institute March 11, 2017 Disclosures Research Funding Janssen Pfizer Consultant
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD
 La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
Surgical Management of Renal Cancer. David Nicol Consultant Urologist
 Surgical Management of Renal Cancer David Nicol Consultant Urologist Roles of Surgery 1. Curative intervention localised disease 2. Symptomatic control advanced disease 3. Augmentation of efficacy of systemic
Surgical Management of Renal Cancer David Nicol Consultant Urologist Roles of Surgery 1. Curative intervention localised disease 2. Symptomatic control advanced disease 3. Augmentation of efficacy of systemic
ASCO 2011 Genitourinary Cancer
 ASCO 2011 Genitourinary Cancer Expanding Options for Chronic Diseases? Walter Stadler, MD, FACP University of Chicago Disclosures (All Non-University &/or Financial Dealings with Potential, Real, or Perceived
ASCO 2011 Genitourinary Cancer Expanding Options for Chronic Diseases? Walter Stadler, MD, FACP University of Chicago Disclosures (All Non-University &/or Financial Dealings with Potential, Real, or Perceived
Prostate cancer Management of metastatic castration sensitive cancer
 18 th Annual Advances in Oncology - 2017 Prostate cancer Management of metastatic castration sensitive cancer Urothelial carcinoma Non-muscle invasive urothelial carcinoma Updates in metastatic urothelial
18 th Annual Advances in Oncology - 2017 Prostate cancer Management of metastatic castration sensitive cancer Urothelial carcinoma Non-muscle invasive urothelial carcinoma Updates in metastatic urothelial
Clinical/Surgical trials that will change my practice
 Clinical/Surgical trials that will change my practice Mr Jim M Adshead Herts and Beds Urological Cancer Centre, Lister Hospital What s changed and where do I feel we are clutching at straws? Regional Specialist
Clinical/Surgical trials that will change my practice Mr Jim M Adshead Herts and Beds Urological Cancer Centre, Lister Hospital What s changed and where do I feel we are clutching at straws? Regional Specialist
How does histology alter treatment? Cora N. Sternberg, MD, FACP Department of Medical Oncology San Camillo and Forlanini Hospitals Rome, Italy
 How does histology alter treatment? Cora N. Sternberg, MD, FACP Department of Medical Oncology San Camillo and Forlanini Hospitals Rome, Italy Targeting VHL/HIF in Clear Cell RCC VHL Bevacizumab (Antibody)
How does histology alter treatment? Cora N. Sternberg, MD, FACP Department of Medical Oncology San Camillo and Forlanini Hospitals Rome, Italy Targeting VHL/HIF in Clear Cell RCC VHL Bevacizumab (Antibody)
Metastasectomy After Targeted Therapy in Patients With Advanced Renal Cell Carcinoma
 Metastasectomy After Targeted Therapy in Patients With Advanced Renal Cell Carcinoma Jose A. Karam, Brian I. Rini,* Leticia Varella, Jorge A. Garcia, Robert Dreicer, Toni K. Choueiri, Eric Jonasch, Surena
Metastasectomy After Targeted Therapy in Patients With Advanced Renal Cell Carcinoma Jose A. Karam, Brian I. Rini,* Leticia Varella, Jorge A. Garcia, Robert Dreicer, Toni K. Choueiri, Eric Jonasch, Surena
CLINICAL POLICY Department: Medical Management Document Name: Inlyta Reference Number: NH.PHAR.100 Effective Date: 05/12
 Page: 1 of 5 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of generally accepted
Page: 1 of 5 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of generally accepted
EAU GUIDELINES ON RENAL CELL CARCINOMA
 EAU GUIDELINES ON RENAL ELL ARINOMA (Limited text update March 2016) B. Ljungberg (hair), K. Bensalah, A. Bex (Vice-chair), S. anfield, R.H. Giles (Patient Organisation Representative), M. Hora, M.A. Kuczyk,
EAU GUIDELINES ON RENAL ELL ARINOMA (Limited text update March 2016) B. Ljungberg (hair), K. Bensalah, A. Bex (Vice-chair), S. anfield, R.H. Giles (Patient Organisation Representative), M. Hora, M.A. Kuczyk,
Recent Developments in Research on Kidney Cancer: Highlights from Urological and Oncological Congresses in 2007
 european urology supplements 7 (2008) 494 507 available at www.sciencedirect.com journal homepage: www.europeanurology.com Recent Developments in Research on Kidney Cancer: Highlights from Urological and
european urology supplements 7 (2008) 494 507 available at www.sciencedirect.com journal homepage: www.europeanurology.com Recent Developments in Research on Kidney Cancer: Highlights from Urological and
REAL WORLD PRACTICE: ADJUVANT THERAPY READY FOR PRIME TIME? PRO
 REAL WORLD PRACTICE: ADJUVANT THERAPY READY FOR PRIME TIME? PRO Alain Ravaud, MD.PhD Bordeaux. France DISCLOSURES Consultant for: Pfizer, Novartis, GlaxoSmithKline, Roche, Bristol-Myers Squibb Institutional
REAL WORLD PRACTICE: ADJUVANT THERAPY READY FOR PRIME TIME? PRO Alain Ravaud, MD.PhD Bordeaux. France DISCLOSURES Consultant for: Pfizer, Novartis, GlaxoSmithKline, Roche, Bristol-Myers Squibb Institutional
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease
 Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
Revisione Oral Abstracts
 Revisione Oral Abstracts Francesco Massari Oncologia Medica Azienda Ospedaliero Universitaria di Bologna Policlinico S. Orsola-Malpighi UPDATES and NEWS from the Genitourinary Cancers Symposium - Milano,
Revisione Oral Abstracts Francesco Massari Oncologia Medica Azienda Ospedaliero Universitaria di Bologna Policlinico S. Orsola-Malpighi UPDATES and NEWS from the Genitourinary Cancers Symposium - Milano,
Why was HOPE 205 a Positive After Years of Negative Studies?
 Why was HOPE 205 a Positive After Years of Negative Studies? Prof. Dr. med. Viktor Grünwald Klinik für Hämatologie, Hämostaseologie, Onkologie und Stammzelltransplantation Why do we pursue combinations?
Why was HOPE 205 a Positive After Years of Negative Studies? Prof. Dr. med. Viktor Grünwald Klinik für Hämatologie, Hämostaseologie, Onkologie und Stammzelltransplantation Why do we pursue combinations?
Kidney Cancer Session
 New Frontiers in Urologic Oncology September 12 th, 2015 Kidney Cancer Session Moderator: Philippe E. Spiess, M.D. Invited Faculty Members: Wade J. Sexton, MD Jeremiah J. Morrissey, PhD Agenda for Session
New Frontiers in Urologic Oncology September 12 th, 2015 Kidney Cancer Session Moderator: Philippe E. Spiess, M.D. Invited Faculty Members: Wade J. Sexton, MD Jeremiah J. Morrissey, PhD Agenda for Session
UPDATE FROM ASCO GU FEBRUARY 2018, SAN FRANCISCO, USA. Prof. David Pfister University Hospital of Cologne Germany RENAL CELL CARCINOMA
 UPDATE FROM ASCO GU FEBRUARY 2018, SAN FRANCISCO, USA Prof. David Pfister University Hospital of Cologne Germany RENAL CELL CARCINOMA DISCLAIMER Please note: The views expressed within this presentation
UPDATE FROM ASCO GU FEBRUARY 2018, SAN FRANCISCO, USA Prof. David Pfister University Hospital of Cologne Germany RENAL CELL CARCINOMA DISCLAIMER Please note: The views expressed within this presentation
Metastasectomy for Melanoma What s the Evidence and When Do We Stop?
 Metastasectomy for Melanoma What s the Evidence and When Do We Stop? Vernon K. Sondak, M D Chair, Moffitt Cancer Center Tampa, Florida Focus on Melanoma London, UK October 15, 2013 Disclosures Dr. Sondak
Metastasectomy for Melanoma What s the Evidence and When Do We Stop? Vernon K. Sondak, M D Chair, Moffitt Cancer Center Tampa, Florida Focus on Melanoma London, UK October 15, 2013 Disclosures Dr. Sondak
Is Immune Therapy the Holy Grail in Metastatic Kidney Cancer?
 Is Immune Therapy the Holy Grail in Metastatic Kidney Cancer? New Frontiers in Urologic Oncology 8-2016 Mayer Fishman, MD PhD Member, Moffitt Cancer Center Department of Genitourinary Oncology Professor,
Is Immune Therapy the Holy Grail in Metastatic Kidney Cancer? New Frontiers in Urologic Oncology 8-2016 Mayer Fishman, MD PhD Member, Moffitt Cancer Center Department of Genitourinary Oncology Professor,
Fifteenth International Kidney Cancer Symposium
 The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
Immunotherapy for the Treatment of Cancer
 Immunotherapy for the Treatment of Cancer Jason Muhitch, PhD Assistant Professor Department of Urology Department of Immunology Roswell Park Comprehensive Cancer Center Oncology for Scientists March 15,
Immunotherapy for the Treatment of Cancer Jason Muhitch, PhD Assistant Professor Department of Urology Department of Immunology Roswell Park Comprehensive Cancer Center Oncology for Scientists March 15,
The Met Pathway as a Target in RCC
 The Met Pathway as a Target in RCC Harriet Kluger, M.D. Associate Professor Yale Cancer Center Disclosures pertinent to this presentation - none c-met Pathway (Biocarta) Rationale for c-met targeting in
The Met Pathway as a Target in RCC Harriet Kluger, M.D. Associate Professor Yale Cancer Center Disclosures pertinent to this presentation - none c-met Pathway (Biocarta) Rationale for c-met targeting in
Early Chemotherapy for Metastatic Prostate Cancer
 Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
Sustained Response to Temsirolimus in Chromophobe variant of Metastatic Renal Cell Carcinoma
 JOURNAL OF CASE REPORTS 2015;5(1):280-284 Sustained Response to Temsirolimus in Chromophobe variant of Metastatic Renal Cell Carcinoma Chanchal Goswami, Aditi Mandal B. P. Poddar Hospital & Medical Research
JOURNAL OF CASE REPORTS 2015;5(1):280-284 Sustained Response to Temsirolimus in Chromophobe variant of Metastatic Renal Cell Carcinoma Chanchal Goswami, Aditi Mandal B. P. Poddar Hospital & Medical Research
Renal Mass Biopsy: Needed Now More than Ever
 Renal Mass Biopsy: Needed Now More than Ever Stuart G. Silverman, MD, FACR Professor of Radiology Harvard Medical School Director, Abdominal Imaging and Intervention Brigham and Women s Hospital Boston,
Renal Mass Biopsy: Needed Now More than Ever Stuart G. Silverman, MD, FACR Professor of Radiology Harvard Medical School Director, Abdominal Imaging and Intervention Brigham and Women s Hospital Boston,
A randomized phase 2 trial of CRLX101 in combination with bevacizumab in patients with metastatic renal cell carcinoma (mrcc) vs standard of care
 vs standard of care") A randomized phase 2 trial of CRLX101 in combination with bevacizumab in patients with metastatic renal cell carcinoma (mrcc) vs standard of care Martin H. Voss 1, Thomas Hutson 2, Arif Hussain 3, Ulka
A randomized phase 2 trial of CRLX101 in combination with bevacizumab in patients with metastatic renal cell carcinoma (mrcc) vs standard of care Martin H. Voss 1, Thomas Hutson 2, Arif Hussain 3, Ulka