Metastatic disease of the Spine
|
|
|
- Marjory Day
- 5 years ago
- Views:
Transcription
; MCh (Orth); D Orth; FRCS (Tr")

1 Metastatic disease of the Spine Jwalant S. Mehta MS (Orth); MCh (Orth); D Orth; FRCS (Tr & Orth) Consultant Spine Surgeon The Royal Orthopaedic Hospital Birmingham Children s Hospital
2 MSCC Metastatic Spinal Cord Compression
3 Prevalence Bone metastasis seen in 150,000 patients with solid tumours in England and Wales Common sites of metastasis: Lung; Liver; Bone Aaron AD JAMA 1994; 272:
4 Prevalence Spine is the commonest site of bone metastasis 30-70% Cancer patients have spine mets on autopsy 5-10% patients with cancer develop spinal cord compression Jacobs, Perin Neurosurg Focus 2001 As survival rates for primary cancers improve, the prevalence of spinal metastasis will rise.
5 Common sites of primaries Adults: Breast, Lung, Prostate, Renal, Melanoma, Thyroid, Colorectal, Haematologic (MM; Lymphoma) Constans J Neurosurg 1983; 59: Children: Neuroblastomas, Sarcomas Choi ESJ :
6 Pathology Reaching the spine: Haematogenous spread Direct extension / invasion Seeding of CSF Thoracic Spine 70% Lumbar spine 20% Cervical and Sacrum 10%

7 Pathology Vertebral body 80% Posterior elements 20% Most are osteolytic 95% Breast and Prostate are osteoblatic Usually do not cross dural barrier exc sarcomas, recurrence, post radiotherapy



8 Grades of MSCC Grade Bone Epidural Theca Cord deformation Cord compression a b c CSF seen No CSF
9 Patient evaluation 1. Medical condition 2. Clinical presentation: Neurology, Pain, Instability 3. Oncologic status
10 Patient evaluation: Medical condition Overall health; previous treatment with chemo / radio, steroids; Nutritional status Poor outcome factors: age, obesity, malnutrition, Diabetes, low bone density, chronic steroid use, bone marrow suppression Haematologic staus: Leukopenia, thrombocytopaenia, coagulopathy
11 Patient evaluation 1. Medical condition 2. Clinical presentation: Neurology, Pain, Instability 3. Oncologic status
12 Patient evaluation: Neurology Sensory (including fine touch, pin prick, vibration, temperature) Motor Reflexes (including pathologic reflexes) Autonomic
13 Patient evaluation: Neurology Cord v nerve root Myelopathy v radiculopathy Ambulation status (important predictor) Degree of cord compression 5-10% of all MSCC
14 Patient evaluation: Pain 83-95% pain precedes neurology Sciubba J Neurol Spine 2010; 13: Types of pain patterns: Local Radicular Mechanical
15 Patient evaluation: Local Pain Causes: Periosteal strech, endosteal pressure, inflammation by tumour growth Gokaslan Curr Opin Oncol 1996 Localised, constant, not related to activities, deep ache Responds to: NSIAD s, Steroids, radiotherapy
16 Patient evaluation: Radicular Pain Root compression alongs its course (Dermatomal pattern) Sharp, shooting, stabbing Constant, not related to activity Response to NSAID s, steroids, chemo and radiotherapy (tumour shrinkage)
17 Patient evaluation: Mechanical Pain Severe, movement related Worse with loading the spinal column Improves with lying down Refractory to medications, chemo or radiotherapy Instability
18 Patient evaluation: Instability loss of spinal integrity as a result of a neoplastic process that is associated with movement related pain, symptomatic or progressive deformity and / or neural compromise under physiologic loads

19 Spinal Instability Neoplastic Score (SINS) 0-6 Stable 7-12 Intermediate Unstable

20 Spinal Instability Neoplastic Score (SINS) Mobile No pain Mixed Normal alignment No collapse No PL involvement Stable 7-12 Intermediate Unstable
 Lytic Normal")

21 Spinal Instability Neoplastic Score (SINS) Junctional Pain (not mech) Lytic Normal alignment < 50% collapse Right pedicle Stable 7-12 Intermediate Unstable

22 Spinal Instability Neoplastic Score (SINS) Mobile Mech pain Lytic Kyphotic > 50% collapse Bil PL involced Stable 7-12 Intermediate Unstable
23 Biomechanics of collapse Cancellous involvement with intact cortical shell may not lead to instability Taneichi Risk factors: Multivariate logistic regression model Thoracic: Costo-vertebral joint destruction v size of lesion TL / L: Size of lesion and pedicle involvement Bone mineral density v size of lesion
24 Patient evaluation 1. Medical condition 2. Clinical presentation: Neurology, Pain, Instability 3. Oncologic status
25 Patient evaluation Oncologic status Tumour histology Single strongest predictor of survival Vascularity: Renal, Thyroid, Hepato-cellular, Melanoma, GCT (hypervascular; prep embolisation) Tomita stratification of tumour histology
26 Systemic staging Tomita score Tokuhashi score
27 Tomita stratification of tumour histology Slow growing: Breast, Prostate, Thyroid, Carcinoid Moderately growing: Kidney, Uterus Rapidly growing: Lung, Liver, Stomach, Sarcoma, Pancreas, Bladder, Oesophagus, Unknown

28 Tomita surgical classification


29 Weinstein - Boriani - Biagini surgical staging

30 Systemic staging: Tomita

31 Systemic staging: Tokuhashi Parameters General condition Poor Moderate Good Extra-spinal skeletal metastasis >3 1 to 2 0 Metastasis to internal organs Un-removable Removable None Number of spinal metastasis >3 2 1 Spinal cord palsy Complete Incomplete None

32 Systemic staging: Tokuhashi
33 Treatment options Chemotherapy Radiotherapy (CXT, IMRT) Surgery (en bloc, palliative) End of life pathway
34 Treatment options: Chemotherapy Asymptomatic / minimal symptoms Haematologic malignancies Hormone sensitive tumours (if no surgical indication) Newer drugs (named clinical oncologist)


35 51 F B cell lymphoma Large right lung upper lobe mass Chemotherapy Chest pain, SOB CTPA r/o PE (T3 lesion identified)


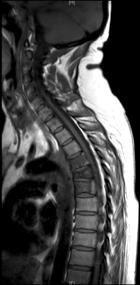
36 T3, 4, 5 lesion No cord compression Encasing thoracic aorta
37 Treatment options: Radiotherapy Conventional (CRT) CRT limited by cord tolerance Radio-sensitive: Response to doses within the cord tolerance Radio-resistant: Requires higher doses than cord tolerance
38 Treatment options: Radiotherapy Intensity-modulated radiation therapy Higher dose of conformal radiation Easing of distinction between sensitive and resistant tumours Sensitive: Breast, prostate, ovarian, neuro-endocrine cancers Resistant: Renal, Thyroid, Hepato-cellular, Non Small cell, Colon, Melanoma, Sarcomas
39 Treatment options: Radiotherapy Problems: Compression fractures Pain flare: Transient increase after CRT Visceral (esophagus), plexus / root susceptible to collateral damage

40 55 M Recent diagnosis of Lung Ca Pre-morbid normal mobility Neurology: Right L2 - S1 4/5 Left L2 - S1 3/5 Normal PR, Sensory level ill defined Palliation Radiotherapy IV Steroids Pain management
41 Treatment options: Surgery En-bloc Stabilisation / decompression Goals and timing of surgery Role of fusion Complications
42 Treatment options: Goals of Surgery Manage expectations Discuss with patient and family Discuss with oncologist Reduce pain Protect, restore neurology Maintain stability for rest of the life (QoL)
43 Treatment options: En Bloc Resection Single level lesion (look for skip lesions) Vertebrectomy, sagittal resection, posterior arch resection, spondylectomy Pre-operative embolisation Assess epidural spread Ligate Hoffmann s ligaments
44 Treatment options: Palliative Surgery Stabilisation, Decompression Anaesthetic assessments Surgical risk stratifications Anterior column reconstruction Minimally invasive options

45



46 58 M Ca Prostate Acute (< 24 h) drop in neurology Previously ambulant 3 weeks of back pain


47 3 contiguous levels Epidural spread Cord saving


48 New lesions within 3 months
49 Treatment options: Surgery: Role of fusion Life expectancy Adjuvant therapies Quality of host bone, nutritional status Allografts Avoid autografts: may be involved in pathology
50 Patchell Study RCT 101 patients with MSCC Surgery (stabilisation, decompression and radiotherapy) v Radiotherapy Did not include radio / chemo sensitive tumours ie myeloma, lymphoma, small cell lung
51 Patchell Study Ambulation better in surgery group (84%) than in radiotherapy group (57%) OR 6.2 p = Maintained ambulation for longer in surgery group (122 d) v radiotherapy (13d) p = 0.003
52 Patchell Study Highly sensitive radio / chemo sensitive tumours may respond to cord compression without surgery Solid tumours with cord compression (grade 2, 3) require surgery and radiotherapy Grade 1 MSCC may not require surgery (unless unstable)
53 Treatment options: Vertebral augmentation Reduce instability pain Image guidance; Minimally invasive Local control of pain



54 59, F Ca Cervix Feb cycles of chemo, local recurrence Chest pain, SOB, CTPA to r/o PE L3 lesion (incidental finding) Normal neurology Biopsy, Vertebroplasty
 5 mo later new neurologic deficit")
55 67 M Ca Prostate mets Presented with acute neurology and 1 week history of back pain Posterior stabilisation, decompression Post-op improved neurology (ambulant) 5 mo later new neurologic deficit New lesions
56 Treatment options: Complications of Surgery Haemorrhage Neurologic injury Visceral / Vascular injury Wound healing Medical and Haematologic optimisation pre-operatively
57 Initial management Pain, Neurology, Suspected MSCC: Nurse flat TEDS, Flowtrons, Steroids, Bloods Maintain and update neurologic assessments Discuss with Family, Oncologists, Spinal Surgeon and Anaesthetists Identify imaging requirements and related logistics
58 Imaging and Transfer Imaging: MRI Full Spine: T1, STIR: Other lesions T2: Destruction, compression Axials: CSF at site of compression CT scan: Staging Thorax, Abdomen, Pelvis (TAP) Reformat the lesion: size and type Plain Xrays not recommended
59 Imaging and Transfer Discuss urgency of transfer / MDT (MSCC) co-ordinator Transfer images Clearly documented current neurology Medical and Oncologic information
60 Selected references Fischer CG et al Spine 2010; 35: E Tomita K et al Spine 2001; 26: Tokuhashi Y et al Spine 2005; 30: Fourney DR, et al J Clin Ocol 2011; 29: Enneking Clin Orth Rel Res 1986; 204: 9 24 Boriani S et al Spine 1997; 22: Patchell RA et al Lancet 2005; 366: Gokaslan ZL, et al J Neurosurg 1998; 89:
Metastatic Spinal Disease
 Metastatic Spinal Disease Mr Neil Chiverton Consultant Spinal Surgeon, Sheffield Objectives The scale and nature of the problem NICE recommendations Surgical decision making Case illustrations Incidence
Metastatic Spinal Disease Mr Neil Chiverton Consultant Spinal Surgeon, Sheffield Objectives The scale and nature of the problem NICE recommendations Surgical decision making Case illustrations Incidence
Disclosures. Disclosures 27/01/2019. Modern approach and pitfalls in metastatic spine surgery. None.. Jeremy Reynolds
 Modern approach and pitfalls in metastatic spine surgery Jeremy Reynolds Spine Lead Oxford Bone and Soft Tissue Sarcoma Service MSCC Lead Thames Valley Cancer Network Clinical Lead Oxford Spine 1 Disclosures
Modern approach and pitfalls in metastatic spine surgery Jeremy Reynolds Spine Lead Oxford Bone and Soft Tissue Sarcoma Service MSCC Lead Thames Valley Cancer Network Clinical Lead Oxford Spine 1 Disclosures
The use of surgery in the elderly. for management of metastatic epidural spinal cord compression
 The use of surgery in the elderly Bone Tumor Simulators for management of metastatic epidural spinal cord compression Justin E. Bird, M.D. Assistant Professor Orthopaedic Oncology and Spine Surgery Epidemiology
The use of surgery in the elderly Bone Tumor Simulators for management of metastatic epidural spinal cord compression Justin E. Bird, M.D. Assistant Professor Orthopaedic Oncology and Spine Surgery Epidemiology
Surgical Treatment of Spine Surgery Experience Primary Spinal Neoplasms ( ) Ziya L. Gokaslan, MD, FACS Approximately 3500 spine tumor
 Ziya L. Gokaslan, MD, FACS Approximately 3500 spine tumor") Surgical Treatment of Primary Spinal Neoplasms Ziya L. Gokaslan, MD, FACS Donlin M. Long Professor Professor of Neurosurgery, Oncology & Orthopaedic Surgery Vice Chairman Director of Spine Program Department
Surgical Treatment of Primary Spinal Neoplasms Ziya L. Gokaslan, MD, FACS Donlin M. Long Professor Professor of Neurosurgery, Oncology & Orthopaedic Surgery Vice Chairman Director of Spine Program Department
MSCC CARE PATHWAYS & CASE STUDIES. By Michael Balloch Spine CNS
 MSCC CARE PATHWAYS & CASE STUDIES By Michael Balloch Spine CNS Aims To be familiar with the routes of MSCC prentaion How the guidelines work in practice Routes of presentation Generic intervention Managing
MSCC CARE PATHWAYS & CASE STUDIES By Michael Balloch Spine CNS Aims To be familiar with the routes of MSCC prentaion How the guidelines work in practice Routes of presentation Generic intervention Managing
GUIDELINES FOR RADIOTHERAPY IN SPINAL CORD COMPRESSION THE CHRISTIE, GREATER MANCHESTER & CHESHIRE. Version:
 GUIDELINES FOR RADIOTHERAPY IN SPINAL CORD COMPRESSION THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Dr V. Misra Version: Accountable Committee: V4 Acute Oncology Group
GUIDELINES FOR RADIOTHERAPY IN SPINAL CORD COMPRESSION THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Dr V. Misra Version: Accountable Committee: V4 Acute Oncology Group
Recognition & Treatment of Malignant Spinal Cord Compression Study Day
 Recognition & Treatment of Malignant Spinal Cord Compression Study Day 16 th October 2014 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk
Recognition & Treatment of Malignant Spinal Cord Compression Study Day 16 th October 2014 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk
Update on Management of Malignant Spinal Cord Compression. Heino Hugel Consultant in Palliative Medicine University Hospital Aintree
 Update on Management of Malignant Spinal Cord Compression Heino Hugel Consultant in Palliative Medicine University Hospital Aintree Current Guidelines The symptoms of MSCC may be subtle and therefore careful
Update on Management of Malignant Spinal Cord Compression Heino Hugel Consultant in Palliative Medicine University Hospital Aintree Current Guidelines The symptoms of MSCC may be subtle and therefore careful
Modern management in vertebral metastasis
 43 B. Costachescu, C.E. Popescu Modern management in vertebral metastasis Modern management in vertebral metastasis B. Costachescu, C.E. Popescu Department of Neurosurgery, Division of Spine Surgery, University
43 B. Costachescu, C.E. Popescu Modern management in vertebral metastasis Modern management in vertebral metastasis B. Costachescu, C.E. Popescu Department of Neurosurgery, Division of Spine Surgery, University
The surgical treatment of metastatic disease of the spine
 The surgical treatment of metastatic disease of the spine Péter Banczerowski National Institute of Neurosurgery, Budapest Spine tumours 15% of the primary tumours of the CNS affect the spine The spine
The surgical treatment of metastatic disease of the spine Péter Banczerowski National Institute of Neurosurgery, Budapest Spine tumours 15% of the primary tumours of the CNS affect the spine The spine
Decision Making Flowchart for Metastatic Spinal Cord Compression and Pathological Spinal Fractures
 Decision Making Flowchart for Metastatic Spinal Cord Compression and Pathological Spinal Fractures All Referrals (see notes): Spinal Surgeons Locally or Trauma SpR at UHW Oncology SpR at Velindre / Singleton
Decision Making Flowchart for Metastatic Spinal Cord Compression and Pathological Spinal Fractures All Referrals (see notes): Spinal Surgeons Locally or Trauma SpR at UHW Oncology SpR at Velindre / Singleton
Malignant Spinal cord Compression. Dr. Thiru Thirukkumaran Palliative Care Services - Northwest Tasmania
 Malignant Spinal cord Compression Dr. Thiru Thirukkumaran Palliative Care Services - Northwest Tasmania Background Statistics of SCC -1 Incidence of SCC Vertebral body metastases 85 % Para-vertebral (Lymphoma)
Malignant Spinal cord Compression Dr. Thiru Thirukkumaran Palliative Care Services - Northwest Tasmania Background Statistics of SCC -1 Incidence of SCC Vertebral body metastases 85 % Para-vertebral (Lymphoma)
Oncologic Emergencies: When to call the Radiation Oncologist
 Oncologic Emergencies: When to call the Radiation Oncologist Dr. Shrinivas Rathod Radiation Oncologist Radiation Oncology Program CancerCare Manitoba and University of Manitoba Disclosures Speaker s name:
Oncologic Emergencies: When to call the Radiation Oncologist Dr. Shrinivas Rathod Radiation Oncologist Radiation Oncology Program CancerCare Manitoba and University of Manitoba Disclosures Speaker s name:
Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2
 Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2 Case 79 yo M with hx of T3N0 colon cancer diagnosed in 2008 metastatic liver disease s/p liver segmentectomy 2009
Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2 Case 79 yo M with hx of T3N0 colon cancer diagnosed in 2008 metastatic liver disease s/p liver segmentectomy 2009
Imaging of bone metastases
 Imaging of bone metastases Antoine Feydy Service de Radiologie B Hôpital Cochin APHP Université Paris Descartes antoine.feydy@aphp.fr MEXICO 2016 INTRODUCTION Diagnostic Imaging Imaging Modalities Strengths,
Imaging of bone metastases Antoine Feydy Service de Radiologie B Hôpital Cochin APHP Université Paris Descartes antoine.feydy@aphp.fr MEXICO 2016 INTRODUCTION Diagnostic Imaging Imaging Modalities Strengths,
Radiotherapy symptoms control in bone mets. Francesco Cellini GemelliART. Ernesto Maranzano,MD. Session 5: Symptoms management
 Session 5: Symptoms management Radiotherapy symptoms control in bone mets Francesco Cellini GemelliART Ernesto Maranzano,MD Director of Oncology Department Chief of Radiation Oncology Centre S. Maria Hospital
Session 5: Symptoms management Radiotherapy symptoms control in bone mets Francesco Cellini GemelliART Ernesto Maranzano,MD Director of Oncology Department Chief of Radiation Oncology Centre S. Maria Hospital
Bone Metastases. Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital
 Bone Metastases Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital 1 Outline Pathophysiology Signs & Symptoms Diagnosis Treatment Spinal Cord Compression 2 General Information
Bone Metastases Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital 1 Outline Pathophysiology Signs & Symptoms Diagnosis Treatment Spinal Cord Compression 2 General Information
Suspecting Tumors, or Could it be cancer?
 Suspecting Tumors, or Could it be cancer? Donna E. Reece, M.D. Princess Margaret Cancer Centre University Health Network Toronto, ON CANADA 07 February 2018 Background Low back pain is common However,
Suspecting Tumors, or Could it be cancer? Donna E. Reece, M.D. Princess Margaret Cancer Centre University Health Network Toronto, ON CANADA 07 February 2018 Background Low back pain is common However,
Managing Bone Pain in Metastatic Disease. Rachel Schacht PA-C Medical Oncology and Hematology Associates Presented on 11/2/2018
 Managing Bone Pain in Metastatic Disease Rachel Schacht PA-C Medical Oncology and Hematology Associates Presented on 11/2/2018 None Disclosures Managing Bone Pain in Metastatic Disease This lecture will
Managing Bone Pain in Metastatic Disease Rachel Schacht PA-C Medical Oncology and Hematology Associates Presented on 11/2/2018 None Disclosures Managing Bone Pain in Metastatic Disease This lecture will
Minimally Invasive Radiofrequency Ablation Treatment of Metastatic Spinal Tumors
 Minimally Invasive Radiofrequency Ablation Treatment of Metastatic Spinal Tumors 1 Objectives Demographics of spinal tumors Treatment options and goals Adoption of RF ablation for pain palliation by NCCN
Minimally Invasive Radiofrequency Ablation Treatment of Metastatic Spinal Tumors 1 Objectives Demographics of spinal tumors Treatment options and goals Adoption of RF ablation for pain palliation by NCCN
PRIMARY STUDIES EN BLOC VERSUS DEBULKING
 PRIMARY STUDIES EN BLOC VERSUS DEBULKING I Study ID II Method III Patient characteristics IV Intervention(s) V Results primary outcome VI Results secondary and other outcome(s) VII Critical appraisal of
PRIMARY STUDIES EN BLOC VERSUS DEBULKING I Study ID II Method III Patient characteristics IV Intervention(s) V Results primary outcome VI Results secondary and other outcome(s) VII Critical appraisal of
Recognition & Treatment of Malignant Spinal Cord Compression
 Recognition & Treatment of Malignant Spinal Cord Compression Acute Oncology Study Day 15 th March 2018 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Yorkshire & the Humber Weston
Recognition & Treatment of Malignant Spinal Cord Compression Acute Oncology Study Day 15 th March 2018 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Yorkshire & the Humber Weston
agreed MSCC pathways and guidelines).
.") Referral of Patients with Spinal Metastatic Disease and Suspected Metastatic Spinal Cord Compression (to be used in association with locally West Midlands Clinical Networks and Clinical Senate Coversheet
Referral of Patients with Spinal Metastatic Disease and Suspected Metastatic Spinal Cord Compression (to be used in association with locally West Midlands Clinical Networks and Clinical Senate Coversheet
En bloc spondylectomy for spinal metastases: a review of techniques
 Neurosurg Focus 15 (5):Article 6, 2003, Click here to return to Table of Contents En bloc spondylectomy for spinal metastases: a review of techniques KEVIN C. YAO, M.D., STEFANO BORIANI, M.D., ZIYA L.
Neurosurg Focus 15 (5):Article 6, 2003, Click here to return to Table of Contents En bloc spondylectomy for spinal metastases: a review of techniques KEVIN C. YAO, M.D., STEFANO BORIANI, M.D., ZIYA L.
Objectives. Comprehension of the common spine disorder
 Objectives Comprehension of the common spine disorder Disc degeneration/hernia Spinal stenosis Common spinal deformity (Spondylolisthesis, Scoliosis) Osteoporotic fracture Destructive spinal lesions Anatomy
Objectives Comprehension of the common spine disorder Disc degeneration/hernia Spinal stenosis Common spinal deformity (Spondylolisthesis, Scoliosis) Osteoporotic fracture Destructive spinal lesions Anatomy
How a fully integrated Acute Oncology Service can benefit the busy medical unit
 How a fully integrated Acute Oncology Service can benefit the busy medical unit Dr. Pauline Leonard MD FRCP Consultant Medical Oncologist Whittington Health Over the next 35 mins Briefly remind you of
How a fully integrated Acute Oncology Service can benefit the busy medical unit Dr. Pauline Leonard MD FRCP Consultant Medical Oncologist Whittington Health Over the next 35 mins Briefly remind you of
Louisa Fleure. Advanced Prostate Cancer Clinical Nurse Specialist. Guys and St Thomas NHS Trust
 Louisa Fleure Advanced Prostate Cancer Clinical Nurse Specialist Guys and St Thomas NHS Trust The classification of advanced prostate cancer The incidence of patients presenting with, or developing advanced
Louisa Fleure Advanced Prostate Cancer Clinical Nurse Specialist Guys and St Thomas NHS Trust The classification of advanced prostate cancer The incidence of patients presenting with, or developing advanced
Appendix 4 Urology Care Pathways
 Appendix 4 Urology Care Pathways Cancer Care Pathways outline the steps and stages in the patient journey from referral through to diagnostics, staging, treatment, follow up, rehabilitation and if applicable
Appendix 4 Urology Care Pathways Cancer Care Pathways outline the steps and stages in the patient journey from referral through to diagnostics, staging, treatment, follow up, rehabilitation and if applicable
Management of Acute Oncological emergencies
 Management of Acute Oncological emergencies Malignant Spinal cord compression (MSCC) Neutropenic sepsis Superior vena caval obstruction Hypercalcemia Hyponatremia Bowel obstruction Brain Metastasis with
Management of Acute Oncological emergencies Malignant Spinal cord compression (MSCC) Neutropenic sepsis Superior vena caval obstruction Hypercalcemia Hyponatremia Bowel obstruction Brain Metastasis with
Louisa Fleure. Advanced Prostate Cancer Clinical Nurse Specialist. Guys and St Thomas NHS Trust
 Louisa Fleure Advanced Prostate Cancer Clinical Nurse Specialist Guys and St Thomas NHS Trust The classification of advanced prostate cancer The incidence of patients presenting with, or developing advanced
Louisa Fleure Advanced Prostate Cancer Clinical Nurse Specialist Guys and St Thomas NHS Trust The classification of advanced prostate cancer The incidence of patients presenting with, or developing advanced
MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION
 CLINICAL POLICY MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION DOCUMENT REF: PCLASCORD (Version No. 1.4) Name and designation of policy author(s) Approved by (committee, group, manager)
CLINICAL POLICY MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION DOCUMENT REF: PCLASCORD (Version No. 1.4) Name and designation of policy author(s) Approved by (committee, group, manager)
EVALUATE, TREAT AND WHEN TO REFER RED FLAGS Mid Atlantic Occupational Regional Conference and Environmental Medicine October 6, 2018
 EVALUATE, TREAT AND WHEN TO REFER RED FLAGS Mid Atlantic Occupational Regional Conference and Environmental Medicine October 6, 2018 Marc J. Levine, MD Rothman Institute Director Spine Surgery Program
EVALUATE, TREAT AND WHEN TO REFER RED FLAGS Mid Atlantic Occupational Regional Conference and Environmental Medicine October 6, 2018 Marc J. Levine, MD Rothman Institute Director Spine Surgery Program
VAriation. Orthotics and Me (?surgeons) Greg Etherington Spine Surgeon. Orthopaedic & Neurosurgery backgrounds. Subspeciality training
 Greg Etherington Spine Surgeon. Orthopaedic & Neurosurgery backgrounds. Subspeciality training") Orthotics and Me (?surgeons) Greg Etherington Spine Surgeon Orthopaedic & Neurosurgery backgrounds Subspeciality training spine, upper limb, trauma, pelvis. What do you do in spine? Lumbar Cervical Trauma
Orthotics and Me (?surgeons) Greg Etherington Spine Surgeon Orthopaedic & Neurosurgery backgrounds Subspeciality training spine, upper limb, trauma, pelvis. What do you do in spine? Lumbar Cervical Trauma
Spinal Cord Compression Diagnosis and Management. Information for Shared Care Centres and Community Staff
 Reference: CG1412 Written by: Dr Daniel Yeomanson Peer reviewer Dr Jeanette Payne Approved: August 2016 Approved by D&TC: 10 th June 2016 Review Due: August 2019 Intended Audience This document contains
Reference: CG1412 Written by: Dr Daniel Yeomanson Peer reviewer Dr Jeanette Payne Approved: August 2016 Approved by D&TC: 10 th June 2016 Review Due: August 2019 Intended Audience This document contains
Recommendations for cross-sectional imaging in cancer management, Second edition
 www.rcr.ac.uk Recommendations for cross-sectional imaging in cancer management, Second edition Tumours of the spinal cord Faculty of Clinical Radiology www.rcr.ac.uk Contents Primary spinal cord tumours
www.rcr.ac.uk Recommendations for cross-sectional imaging in cancer management, Second edition Tumours of the spinal cord Faculty of Clinical Radiology www.rcr.ac.uk Contents Primary spinal cord tumours
Recognition & Treatment of Malignant Spinal Cord Compression Study Day
 Recognition & Treatment of Malignant Spinal Cord Compression Study Day 11 th May 2017 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk Clinical
Recognition & Treatment of Malignant Spinal Cord Compression Study Day 11 th May 2017 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk Clinical
Guidelines for the Management. Malignant Spinal Cord Compression. Final Guideline
 Guidelines for the Management Of Malignant Spinal Cord Compression Final Guideline 1. Introduction 1.1 Aetiology of MSCC 1.2 Use of the guidelines 2. Summary of Pathway 2.1 Algorithms 2.2 Role of the MSCC
Guidelines for the Management Of Malignant Spinal Cord Compression Final Guideline 1. Introduction 1.1 Aetiology of MSCC 1.2 Use of the guidelines 2. Summary of Pathway 2.1 Algorithms 2.2 Role of the MSCC
Review Article Chondrosarcoma of the Mobile Spine and Sacrum
 Sarcoma Volume 2011, Article ID 274281, 4 pages doi:10.1155/2011/274281 Review Article Chondrosarcoma of the Mobile Spine and Sacrum Ryan M. Stuckey and Rex A. W. Marco Department of Orthopaedics, University
Sarcoma Volume 2011, Article ID 274281, 4 pages doi:10.1155/2011/274281 Review Article Chondrosarcoma of the Mobile Spine and Sacrum Ryan M. Stuckey and Rex A. W. Marco Department of Orthopaedics, University
Metastatic Spinal Cord Compression (MSCC) Clinical guidelines and pathway
 Clinical guidelines and pathway") Metastatic Spinal Cord Compression (MSCC) Clinical guidelines and pathway Version 2: May 2012 To be read in conjunction with NICE CG75 Developed by consensus by: Dr Peter Robson, Consultant Oncologist,
Metastatic Spinal Cord Compression (MSCC) Clinical guidelines and pathway Version 2: May 2012 To be read in conjunction with NICE CG75 Developed by consensus by: Dr Peter Robson, Consultant Oncologist,
Case Report Four-Rod Stabilization of Severely Destabilized Lumbar Spine Caused by Metastatic Tumor
 Volume 2013, Article ID 254684, 6 pages http://dx.doi.org/10.1155/2013/254684 Case Report Four-Rod Stabilization of Severely Destabilized Lumbar Spine Caused by Metastatic Tumor Isao Shibuya, Koichi Sairyo,
Volume 2013, Article ID 254684, 6 pages http://dx.doi.org/10.1155/2013/254684 Case Report Four-Rod Stabilization of Severely Destabilized Lumbar Spine Caused by Metastatic Tumor Isao Shibuya, Koichi Sairyo,
Benefits of Radiation Therapy in the Palliative Cancer Patient
 Benefits of Radiation Therapy in the Palliative Cancer Patient Dr Joshua Sappiatzer Radiation Oncologist Page 1 Overview Why we should aim for better palliative radiotherapy treatment Bone metastases Rapid
Benefits of Radiation Therapy in the Palliative Cancer Patient Dr Joshua Sappiatzer Radiation Oncologist Page 1 Overview Why we should aim for better palliative radiotherapy treatment Bone metastases Rapid
factor for identifying unstable thoracolumbar fractures. There are clinical and radiological criteria
 NMJ-Vol :2/ Issue:1/ Jan June 2013 Case Report Medical Sciences Progressive subluxation of thoracic wedge compression fracture with unidentified PLC injury Dr.Thalluri.Gopala krishnaiah* Dr.Voleti.Surya
NMJ-Vol :2/ Issue:1/ Jan June 2013 Case Report Medical Sciences Progressive subluxation of thoracic wedge compression fracture with unidentified PLC injury Dr.Thalluri.Gopala krishnaiah* Dr.Voleti.Surya
Spinal cord compression as a first presentation of cancer: A case report
 J Pain Manage 2013;6(4):319-322 ISSN: 1939-5914 Nova Science Publishers, Inc. Spinal cord compression as a first presentation of cancer: A case report Nicholas Lao, BMSc(C), Michael Poon, MD(C), Marko
J Pain Manage 2013;6(4):319-322 ISSN: 1939-5914 Nova Science Publishers, Inc. Spinal cord compression as a first presentation of cancer: A case report Nicholas Lao, BMSc(C), Michael Poon, MD(C), Marko
9:00-9:10 am Metastatic Epidural Cervical Spinal Cord Compression CSRS San Diego, 2015 Michael G. Fehlings, MD
 9:00-9:10 am Metastatic Epidural Cervical Spinal Cord Compression CSRS San Diego, 2015 Michael G. Fehlings, MD 1 BACKGROUND After the lungs and the liver, metastases most frequently arise in osseous tissues;
9:00-9:10 am Metastatic Epidural Cervical Spinal Cord Compression CSRS San Diego, 2015 Michael G. Fehlings, MD 1 BACKGROUND After the lungs and the liver, metastases most frequently arise in osseous tissues;
Acute Oncology Services Clinical Forum: Metastatic Spinal Cord Compression. Tuesday 17 th September 2013
 Acute Oncology Services Clinical Forum: Metastatic Spinal Cord Compression Tuesday 17 th September 2013 Welcome, Introduction and Aims of the Event Dr Tom Newsom-Davis, LCA AOS Pathway Chair Why MSCC?
Acute Oncology Services Clinical Forum: Metastatic Spinal Cord Compression Tuesday 17 th September 2013 Welcome, Introduction and Aims of the Event Dr Tom Newsom-Davis, LCA AOS Pathway Chair Why MSCC?
Primary Bone Tumors: Spine Surgery Live -Video Techniques Mobile Spine
 Primary Bone Tumors: Spine Surgery Live -Video Techniques Mobile Spine Christopher Ames MD Professor of Neurosurgery and Orthopedic Surgery Director of Spine Tumor And Deformity Surgery UCSF Department
Primary Bone Tumors: Spine Surgery Live -Video Techniques Mobile Spine Christopher Ames MD Professor of Neurosurgery and Orthopedic Surgery Director of Spine Tumor And Deformity Surgery UCSF Department
CASE REPORT TOTAL EN BLOC SPONDYLECTOMY FOR L2 CHORDOMA: A CASE REPORT
 Nagoya J. Med. Sci. 73. 197 ~ 203, 2011 CASE REPORT TOTAL EN BLOC SPONDYLECTOMY FOR L2 CHORDOMA: A CASE REPORT NORIMITSU WAKAO 1, SHIRO IMAGAMA 1, ZENYA ITO 1, KEI ANDO 1, KENICHI HIRANO 1, RYOJI TAUCHI
Nagoya J. Med. Sci. 73. 197 ~ 203, 2011 CASE REPORT TOTAL EN BLOC SPONDYLECTOMY FOR L2 CHORDOMA: A CASE REPORT NORIMITSU WAKAO 1, SHIRO IMAGAMA 1, ZENYA ITO 1, KEI ANDO 1, KENICHI HIRANO 1, RYOJI TAUCHI
Metastatic Spinal Cord Compression
 Metastatic Spinal Cord Compression Dr Zacharias Tasigiannopoulos Clinical Oncologist Colney centre Department of Oncology Norwich, UK Introduction 2-5% of cancer patients have an episode of MSCC Initial
Metastatic Spinal Cord Compression Dr Zacharias Tasigiannopoulos Clinical Oncologist Colney centre Department of Oncology Norwich, UK Introduction 2-5% of cancer patients have an episode of MSCC Initial
Surgical and orthotic possibilities of bone tumour pain management
 Surgical and orthotic possibilities of bone tumour pain management Chaloupka, R., Grosman, R., Repko, M., Tichý, V. Ortopedická klinika FN Brno-Bohunice Ortopedická klinika, FN Brno, Jihlavská 20, 625
Surgical and orthotic possibilities of bone tumour pain management Chaloupka, R., Grosman, R., Repko, M., Tichý, V. Ortopedická klinika FN Brno-Bohunice Ortopedická klinika, FN Brno, Jihlavská 20, 625
Comprehension of the common spine disorder.
 Objectives Comprehension of the common spine disorder. Disc degeneration/hernia. Spinal stenosis. Common spinal deformity (Spondylolisthesis, Scoliosis). Osteoporotic fracture. Anatomy Anatomy Anatomy
Objectives Comprehension of the common spine disorder. Disc degeneration/hernia. Spinal stenosis. Common spinal deformity (Spondylolisthesis, Scoliosis). Osteoporotic fracture. Anatomy Anatomy Anatomy
Outcomes Report: Accountability Measures and Quality Improvements
 Outcomes Report: Accountability Measures and Quality Improvements The FH Memorial Medical Center s Cancer Committee ensures that patients with cancer are treated according to the nationally accepted measures.
Outcomes Report: Accountability Measures and Quality Improvements The FH Memorial Medical Center s Cancer Committee ensures that patients with cancer are treated according to the nationally accepted measures.
BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Cancer is a group of more than 100 different diseases that are characterized by uncontrolled cellular growth,
BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Cancer is a group of more than 100 different diseases that are characterized by uncontrolled cellular growth,
HIGH LEVEL - Science
 Learning Outcomes HIGH LEVEL - Science Describe the structure and function of the back and spine (8a) Outline the functional anatomy and physiology of the spinal cord and peripheral nerves (8a) Describe
Learning Outcomes HIGH LEVEL - Science Describe the structure and function of the back and spine (8a) Outline the functional anatomy and physiology of the spinal cord and peripheral nerves (8a) Describe
Palliative RT. Jiraporn Setakornnukul, M.D. Radiation Oncology Division Siriraj Hospital, Mahidol University
 Palliative RT Jiraporn Setakornnukul, M.D. Radiation Oncology Division Siriraj Hospital, Mahidol University Scope Brain metastasis Metastasis epidural spinal cord compression SVC obstruction Bone pain
Palliative RT Jiraporn Setakornnukul, M.D. Radiation Oncology Division Siriraj Hospital, Mahidol University Scope Brain metastasis Metastasis epidural spinal cord compression SVC obstruction Bone pain
Common fracture & dislocation of the cervical spine. Theerachai Apivatthakakul Department of Orthopaedic Chiangmai University
 Common fracture & dislocation of the cervical spine Theerachai Apivatthakakul Department of Orthopaedic Chiangmai University Objective Anatomy Mechanism and type of injury PE.and radiographic evaluation
Common fracture & dislocation of the cervical spine Theerachai Apivatthakakul Department of Orthopaedic Chiangmai University Objective Anatomy Mechanism and type of injury PE.and radiographic evaluation
A PATIENT WITH TWO EPISODES OF THORACIC SPINAL CORD COMPRESSION CAUSED BY PRIMARY LYMPHOMA AND METASTATIC CARCINOMA OF THE PROSTATE, 11 YEARS APART
 A PATIENT WITH TWO EPISODES OF THORACIC SPINAL CORD COMPRESSION CAUSED BY PRIMARY LYMPHOMA AND METASTATIC CARCINOMA OF THE PROSTATE, 11 YEARS APART Shih-Huang Tai, 1 Yu-Chang Hung, 1 Jian-Chin Chen, 2
A PATIENT WITH TWO EPISODES OF THORACIC SPINAL CORD COMPRESSION CAUSED BY PRIMARY LYMPHOMA AND METASTATIC CARCINOMA OF THE PROSTATE, 11 YEARS APART Shih-Huang Tai, 1 Yu-Chang Hung, 1 Jian-Chin Chen, 2
Adult Spinal Deformity Robert Hart. Dept. Orthopaedics and Rehab OHSU
 Adult Spinal Deformity 2010 Robert Hart Dept. Orthopaedics and Rehab OHSU What is Adult Spinal Deformity? Untreated Idiopathic Scoliosis Flat Back Syndrome Adjacent Segment Stenosis Non-Union Degenerative
Adult Spinal Deformity 2010 Robert Hart Dept. Orthopaedics and Rehab OHSU What is Adult Spinal Deformity? Untreated Idiopathic Scoliosis Flat Back Syndrome Adjacent Segment Stenosis Non-Union Degenerative
Malignant Peripheral Nerve Sheath Tumor post Wide Excision with Multiple Lung Metastases: the Role and Treatment Consideration of RT
 Malignant Peripheral Nerve Sheath Tumor post Wide Excision with Multiple Lung Metastases: the Role and Treatment Consideration of RT Case Number: RT2009-64(M) Potential Audiences: Intent Doctor, Oncology
Malignant Peripheral Nerve Sheath Tumor post Wide Excision with Multiple Lung Metastases: the Role and Treatment Consideration of RT Case Number: RT2009-64(M) Potential Audiences: Intent Doctor, Oncology
Considerations for surgical intervention in metastatic cancer to the spine: Catherine Sarah Hibberd
 Considerations for surgical intervention in metastatic cancer to the spine: Evaluation of risk factors for pathologic fracture and spinal cord compression, and analysis of pre-operative scoring systems
Considerations for surgical intervention in metastatic cancer to the spine: Evaluation of risk factors for pathologic fracture and spinal cord compression, and analysis of pre-operative scoring systems
Cancer of Unknown Primary (CUP) Protocol
 Protocol") 1 Department of Oncology. Cancer of Unknown Primary (CUP) Protocol Version: Document type: Document sponsor Designation Document author [ s] Designation[s] Approving committee / Group Ratified by: Date
1 Department of Oncology. Cancer of Unknown Primary (CUP) Protocol Version: Document type: Document sponsor Designation Document author [ s] Designation[s] Approving committee / Group Ratified by: Date
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R
 Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
PATHWAY MANAGEMENT OF METASTATIC SPINAL CORD COMPRESSION (MSCC) THE CHRISTIE, GREATER MANCHESTER & CHESHIRE
 THE CHRISTIE, GREATER MANCHESTER & CHESHIRE") PATHWAY MANAGEMENT OF METASTATIC SPINAL CORD COMPRESSION (MSCC) THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Dr V. Misra Version: Accountable Committee: V3 MSCC Network
PATHWAY MANAGEMENT OF METASTATIC SPINAL CORD COMPRESSION (MSCC) THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Dr V. Misra Version: Accountable Committee: V3 MSCC Network
ESCOME Pre-Course Outline (v1.09)
") ESCOME Pre-Course Outline (v1.09) 1. Basics of Spinal Disorders Introduction to Spinal Surgery Spinal Anatomy Introduction to Vertebral Anatomical Concepts Anatomy and Function of Joints and Ligaments
ESCOME Pre-Course Outline (v1.09) 1. Basics of Spinal Disorders Introduction to Spinal Surgery Spinal Anatomy Introduction to Vertebral Anatomical Concepts Anatomy and Function of Joints and Ligaments
The Role of Radiotherapy in Metastatic Breast Cancer. Shilpen Patel MD, FACRO Associate Professor Departments of Radiation Oncology and Global Health
 The Role of Radiotherapy in Metastatic Breast Cancer Shilpen Patel MD, FACRO Associate Professor Departments of Radiation Oncology and Global Health Indications for Palliative Pain Control Radiation Bone
The Role of Radiotherapy in Metastatic Breast Cancer Shilpen Patel MD, FACRO Associate Professor Departments of Radiation Oncology and Global Health Indications for Palliative Pain Control Radiation Bone
Revised Dec Spine MR Protocols
 Spine MR Protocols Sp 1: Cervical spine MRI without contrast Sp 2: Pre- and post-contrast cervical spine MRI Sp 3: Pre- and post-contrast cervical spine MRI (multiple sclerosis protocol) Sp 4: Thoracic
Spine MR Protocols Sp 1: Cervical spine MRI without contrast Sp 2: Pre- and post-contrast cervical spine MRI Sp 3: Pre- and post-contrast cervical spine MRI (multiple sclerosis protocol) Sp 4: Thoracic
Harrington rod stabilization for pathological fractures of the spine NARAYAN SUNDARESAN, M.D., JOSEPH H. GALICICH, M.D., AND JOSEPH M. LANE, M.D.
 J Neurosurg 60:282-286, 1984 Harrington rod stabilization for pathological fractures of the spine NARAYAN SUNDARESAN, M.D., JOSEPH H. GALICICH, M.D., AND JOSEPH M. LANE, M.D. Neurosurgery and Orthopedic
J Neurosurg 60:282-286, 1984 Harrington rod stabilization for pathological fractures of the spine NARAYAN SUNDARESAN, M.D., JOSEPH H. GALICICH, M.D., AND JOSEPH M. LANE, M.D. Neurosurgery and Orthopedic
Departement of Neurosurgery A.O.R.N A. Cardarelli- Naples.
 Percutaneous posterior pedicle screw fixation in the treatment of thoracic, lumbar and thoraco-lumbar junction (T12-L1) traumatic and pathological spine fractures. Report of 45 cases. G. Vitale, A. Punzo,
Percutaneous posterior pedicle screw fixation in the treatment of thoracic, lumbar and thoraco-lumbar junction (T12-L1) traumatic and pathological spine fractures. Report of 45 cases. G. Vitale, A. Punzo,
Brain Tumors. What is a brain tumor?
 Scan for mobile link. Brain Tumors A brain tumor is a collection of abnormal cells that grows in or around the brain. It poses a risk to the healthy brain by either invading or destroying normal brain
Scan for mobile link. Brain Tumors A brain tumor is a collection of abnormal cells that grows in or around the brain. It poses a risk to the healthy brain by either invading or destroying normal brain
Lumbar disc herniation
 Lumbar disc herniation Thomas Kishen Spine Surgeon Sparsh Hospital for Advanced Surgeries Bangalore Symptoms and Signs Radicular Pain in the distribution of the involved nerve Neurological deficit motor,
Lumbar disc herniation Thomas Kishen Spine Surgeon Sparsh Hospital for Advanced Surgeries Bangalore Symptoms and Signs Radicular Pain in the distribution of the involved nerve Neurological deficit motor,
National Cancer Registration and Analysis Service Short Report: Chemotherapy, Radiotherapy and Surgical Tumour Resections in England: (V2)
") National Cancer Registration and Analysis Service Short Report: Chemotherapy, Radiotherapy and Surgical Tumour Resections in England: 13-14 (V2) Produced as part of the Cancer Research UK - Public Health
National Cancer Registration and Analysis Service Short Report: Chemotherapy, Radiotherapy and Surgical Tumour Resections in England: 13-14 (V2) Produced as part of the Cancer Research UK - Public Health
Role of Posterior Fixation Technique in Surgeries for Pathological Fractures of the Dorsal and Lumbar Spine Secondary to Neoplastic Causes
 Med. J. Cairo Univ., Vol. 83, No. 1, March: 293-298, 2015 www.medicaljournalofcairouniversity.net Role of Posterior Fixation Technique in Surgeries for Pathological Fractures of the Dorsal and Lumbar Spine
Med. J. Cairo Univ., Vol. 83, No. 1, March: 293-298, 2015 www.medicaljournalofcairouniversity.net Role of Posterior Fixation Technique in Surgeries for Pathological Fractures of the Dorsal and Lumbar Spine
CERVICAL SPINE TIPS A
 CERVICAL SPINE TIPS A Musculoskeletal Approach to managing Neck Pain An ALGORITHM, as a management guide Rick Bernau & Ian Wallbridge June 2010 THE PROCESS An interactive approach to the management of
CERVICAL SPINE TIPS A Musculoskeletal Approach to managing Neck Pain An ALGORITHM, as a management guide Rick Bernau & Ian Wallbridge June 2010 THE PROCESS An interactive approach to the management of
Spine Pain Management Program
 Spine Pain Management Program Please complete the following information: Patient Name: Patient ID Number: Patient DOB: The procedure being requested: Epidural Injection Please check the indication (reason)
Spine Pain Management Program Please complete the following information: Patient Name: Patient ID Number: Patient DOB: The procedure being requested: Epidural Injection Please check the indication (reason)
CT PET SCANNING for GIT Malignancies A clinician s perspective
 CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
Original Date: October 2015 LUMBAR SPINAL FUSION FOR
 National Imaging Associates, Inc. Clinical guidelines Original Date: October 2015 LUMBAR SPINAL FUSION FOR Page 1 of 9 INSTABILITY AND DEGENERATIVE DISC CONDITIONS FOR CMS (MEDICARE) MEMBERS ONLY CPT4
National Imaging Associates, Inc. Clinical guidelines Original Date: October 2015 LUMBAR SPINAL FUSION FOR Page 1 of 9 INSTABILITY AND DEGENERATIVE DISC CONDITIONS FOR CMS (MEDICARE) MEMBERS ONLY CPT4
SUBAXIAL CERVICAL SPINE TRAUMA- DIAGNOSIS AND MANAGEMENT
 SUBAXIAL CERVICAL SPINE TRAUMA- DIAGNOSIS AND MANAGEMENT 1 Anatomy 3 columns- Anterior, middle and Posterior Anterior- ALL, Anterior 2/3 rd body & disc. Middle- Posterior 1/3 rd of body & disc, PLL Posterior-
SUBAXIAL CERVICAL SPINE TRAUMA- DIAGNOSIS AND MANAGEMENT 1 Anatomy 3 columns- Anterior, middle and Posterior Anterior- ALL, Anterior 2/3 rd body & disc. Middle- Posterior 1/3 rd of body & disc, PLL Posterior-
Advanced Pelvic Malignancy: Defining Resectability Be Aggressive. Lloyd A. Mack September 19, 2015
 Advanced Pelvic Malignancy: Defining Resectability Be Aggressive Lloyd A. Mack September 19, 2015 CONFLICT OF INTEREST DECLARATION I have no conflicts of interest Advanced Pelvic Malignancies Locally Advanced
Advanced Pelvic Malignancy: Defining Resectability Be Aggressive Lloyd A. Mack September 19, 2015 CONFLICT OF INTEREST DECLARATION I have no conflicts of interest Advanced Pelvic Malignancies Locally Advanced
Evaluation of prognostic scoring systems for bone metastases using single center data
 MOLECULAR AND CLINICAL ONCOLOGY 3: 1361-1370, 2015 Evaluation of prognostic scoring systems for bone metastases using single center data HIROFUMI SHIMADA 1, TAKAO SETOGUCHI 2, SHUNSUKE NAKAMURA 1, MASAHIRO
MOLECULAR AND CLINICAL ONCOLOGY 3: 1361-1370, 2015 Evaluation of prognostic scoring systems for bone metastases using single center data HIROFUMI SHIMADA 1, TAKAO SETOGUCHI 2, SHUNSUKE NAKAMURA 1, MASAHIRO
Brain and Central Nervous System Cancers
 Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
Kim, Hyoungmin 1 ; Lee, Choon-Ki 1 ; Yeom, Jin S. 1 ; Lee, Jae Hyup 1 ; Lee, Suk- Joong 2 ; Chang, Bong-Soon 1
 The Predictive Value of the Spinal Instability Neoplastic Score (SINS) System for Adverse Events of Pathologic Fracture and Spinal Cord Compression in Patients with Single Spinal Metas tasis. Kim, Hyoungmin
The Predictive Value of the Spinal Instability Neoplastic Score (SINS) System for Adverse Events of Pathologic Fracture and Spinal Cord Compression in Patients with Single Spinal Metas tasis. Kim, Hyoungmin
Disclosures. Overview 8/3/2016. SRS: Cranial and Spine
 SRS: Cranial and Spine Brian Winey, Ph.D. Department of Radiation Oncology Massachusetts General Hospital Harvard Medical School Disclosures Travel and research funds from Elekta Travel funds from IBA
SRS: Cranial and Spine Brian Winey, Ph.D. Department of Radiation Oncology Massachusetts General Hospital Harvard Medical School Disclosures Travel and research funds from Elekta Travel funds from IBA
Anterior Cervical Discectomy and Fusion Surgery
 Disclaimer This movie is an educational resource only and should not be used to manage orthopaedic health. All decisions about the management of orthopaedic conditions must be made in conjunction with
Disclaimer This movie is an educational resource only and should not be used to manage orthopaedic health. All decisions about the management of orthopaedic conditions must be made in conjunction with
Pedicle Subtraction Osteotomy. Case JB. Antonio Castellvi 5/19/2017
 Pedicle Subtraction Osteotomy John M. Small MD Florida Orthopedic Institute University South Florida Department Orthopedic Surgery Castellvi Spine May 11, 2017 Case JB 66 y/o male 74 235 lbs Retired police
Pedicle Subtraction Osteotomy John M. Small MD Florida Orthopedic Institute University South Florida Department Orthopedic Surgery Castellvi Spine May 11, 2017 Case JB 66 y/o male 74 235 lbs Retired police
National Imaging Associates, Inc. Clinical guidelines
 National Imaging Associates, Inc. Clinical guidelines Original Date: September 1997 THORACIC SPINE CT Page 1 of 5 CPT Codes: 72128, 72129, 72130 Last Review Date: May 2013 Guideline Number: NIA_CG_043
National Imaging Associates, Inc. Clinical guidelines Original Date: September 1997 THORACIC SPINE CT Page 1 of 5 CPT Codes: 72128, 72129, 72130 Last Review Date: May 2013 Guideline Number: NIA_CG_043
1105 two (2) vertebrae... 1, add on per additional vertebra
 vertebrae... 1, add on per additional vertebra") SPINE STAGE OPERATIONS Staged operations shall be paid at 100% for the first stage and 85% for the second stage. Where the second stage pays a higher fee 100% shall be paid and the first stage shall be
SPINE STAGE OPERATIONS Staged operations shall be paid at 100% for the first stage and 85% for the second stage. Where the second stage pays a higher fee 100% shall be paid and the first stage shall be
Clinical indications for positron emission tomography
 Clinical indications for positron emission tomography Oncology applications Brain and spinal cord Parotid Suspected tumour recurrence when anatomical imaging is difficult or equivocal and management will
Clinical indications for positron emission tomography Oncology applications Brain and spinal cord Parotid Suspected tumour recurrence when anatomical imaging is difficult or equivocal and management will
Department of Orthopedic Surgery, Henan Province People s Hospital, Henan, People s Republic of China; 2
 Int J Clin Exp Med 2018;11(3):2465-2470 www.ijcem.com /ISSN:1940-5901/IJCEM0060812 Original Article Validation of a scoring system predicting survival and function outcome in patients with metastatic epidural
Int J Clin Exp Med 2018;11(3):2465-2470 www.ijcem.com /ISSN:1940-5901/IJCEM0060812 Original Article Validation of a scoring system predicting survival and function outcome in patients with metastatic epidural
Case Report Treatment of Renal Cell Carcinoma with 2-Stage Total en bloc Spondylectomy after Marked Response to Molecular Target Drugs
 Case Reports in Orthopedics Volume 2013, Article ID 916501, 4 pages http://dx.doi.org/10.1155/2013/916501 Case Report Treatment of Renal Cell Carcinoma with 2-Stage Total en bloc Spondylectomy after Marked
Case Reports in Orthopedics Volume 2013, Article ID 916501, 4 pages http://dx.doi.org/10.1155/2013/916501 Case Report Treatment of Renal Cell Carcinoma with 2-Stage Total en bloc Spondylectomy after Marked
Fractures of the thoracic and lumbar spine and thoracolumbar transition
 Most spinal column injuries occur in the thoracolumbar transition, the area between the lower thoracic spine and the upper lumbar spine; over half of all vertebral fractures involve the 12 th thoracic
Most spinal column injuries occur in the thoracolumbar transition, the area between the lower thoracic spine and the upper lumbar spine; over half of all vertebral fractures involve the 12 th thoracic
STAGING, BIOPSY AND NATURAL HISTORY OF TUMORS SCOTT D WEINER MD
 STAGING, BIOPSY AND NATURAL HISTORY OF TUMORS SCOTT D WEINER MD WHAT DO YOU DO WHEN THIS SHOWS UP IN YOUR OFFICE? besides panicking KEY PRINCIPLE!!! Reactive zone is the edema, neovascularity and inflammation
STAGING, BIOPSY AND NATURAL HISTORY OF TUMORS SCOTT D WEINER MD WHAT DO YOU DO WHEN THIS SHOWS UP IN YOUR OFFICE? besides panicking KEY PRINCIPLE!!! Reactive zone is the edema, neovascularity and inflammation
The vertebral column is the primary osseous target of
 spine clinical article J Neurosurg Spine 23:228 232, 2015 Predictors of delayed failure of structural kyphoplasty for pathological compression fractures in cancer patients Gary Rajah, MD, 1 David Altshuler,
spine clinical article J Neurosurg Spine 23:228 232, 2015 Predictors of delayed failure of structural kyphoplasty for pathological compression fractures in cancer patients Gary Rajah, MD, 1 David Altshuler,
Malignant Spinal Cord Compression (MSCC) Clinical Advisor Coordinator
 Clinical Advisor Coordinator") Malignant Spinal Cord Compression (MSCC) Clinical Advisor Coordinator Induction Training 2016 Version Control This is a controlled document please destroy all previous versions on receipt of a new version.
Malignant Spinal Cord Compression (MSCC) Clinical Advisor Coordinator Induction Training 2016 Version Control This is a controlled document please destroy all previous versions on receipt of a new version.
The management and treatment options for secondary bone disease. Omi Parikh July 2013
 The management and treatment options for secondary bone disease Omi Parikh July 2013 Learning Objectives: The assessment and diagnostic process of patients with suspected bone metastases e.g bone scan,
The management and treatment options for secondary bone disease Omi Parikh July 2013 Learning Objectives: The assessment and diagnostic process of patients with suspected bone metastases e.g bone scan,
A rare case of cervical epidural extramedullary plasmacytoma presenting with monoparesis
 Romanian Neurosurgery Volume XXXI Number 1 2017 January - March Article A rare case of cervical epidural extramedullary plasmacytoma presenting with monoparesis Okan Turk, Ibrahim Burak Atci, Hakan Yilmaz,
Romanian Neurosurgery Volume XXXI Number 1 2017 January - March Article A rare case of cervical epidural extramedullary plasmacytoma presenting with monoparesis Okan Turk, Ibrahim Burak Atci, Hakan Yilmaz,
Gillian Wooldridge, DO Houston Methodist Willowbrook Hospital Primary Care Sports Medicine Fellowship May 3, 2018
 Gillian Wooldridge, DO Houston Methodist Willowbrook Hospital Primary Care Sports Medicine Fellowship May 3, 2018 Disclosures Neither I nor any family members have financial disclosures Special thanks
Gillian Wooldridge, DO Houston Methodist Willowbrook Hospital Primary Care Sports Medicine Fellowship May 3, 2018 Disclosures Neither I nor any family members have financial disclosures Special thanks
Vertebral Augmentation for Compression Fractures. Scott Magnuson, MD Pain Management of North Idaho, PLLC
 Vertebral Augmentation for Compression Fractures Scott Magnuson, MD Pain Management of North Idaho, PLLC OVCFs are most common type of fragility fracture 20-25% Caucasian women and men over 50 yrs have
Vertebral Augmentation for Compression Fractures Scott Magnuson, MD Pain Management of North Idaho, PLLC OVCFs are most common type of fragility fracture 20-25% Caucasian women and men over 50 yrs have
Module 1: Basic Comprehensive Course
 The Hellenic Spine Society organize 5 modules according to the following program, which is based on the Eurospine program Module 1: Basic Comprehensive Course SESSION1: SPINE THE BIGGER PICTURE Evidence
The Hellenic Spine Society organize 5 modules according to the following program, which is based on the Eurospine program Module 1: Basic Comprehensive Course SESSION1: SPINE THE BIGGER PICTURE Evidence
APPROPRIATE USE GUIDELINES
 APPROPRIATE USE GUIDELINES Appropriateness of Advanced Imaging Procedures (MRI, CT, Bone Scan/PET) in Patients with Neck Pain CDI QUALITY INSTITUTE: PROVIDER LED ENTITY (PLE) Updated June, 2017 Contents
APPROPRIATE USE GUIDELINES Appropriateness of Advanced Imaging Procedures (MRI, CT, Bone Scan/PET) in Patients with Neck Pain CDI QUALITY INSTITUTE: PROVIDER LED ENTITY (PLE) Updated June, 2017 Contents
Clinical Case Conference
 Clinical Case Conference Palliative radiation therapy for bone metastasis Jeff Burkeen, MD, PGY2 7/20/2015 1 Overview Epidemiology Pathophysiology Common presentations and symptoms Imaging Surgery Radiation
Clinical Case Conference Palliative radiation therapy for bone metastasis Jeff Burkeen, MD, PGY2 7/20/2015 1 Overview Epidemiology Pathophysiology Common presentations and symptoms Imaging Surgery Radiation
CP80 Version: V01. Acute Oncology Management Service Date approved: 8 th May 2015 Date ratified: 1 st June 2015 Review date: 1 st June 2017
 STANDARD OPERATING PROCEDURE (SOP) AND PATHWAY FOR THE MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION (MSCC) WITHIN THE CHRISTIE (Refer to the Manchester Cancer Network MSCC Pathway flowchart)
STANDARD OPERATING PROCEDURE (SOP) AND PATHWAY FOR THE MANAGEMENT OF PATIENTS WITH METASTATIC SPINAL CORD COMPRESSION (MSCC) WITHIN THE CHRISTIE (Refer to the Manchester Cancer Network MSCC Pathway flowchart)