PATOFIZIOLOŠKA DIJAGNOSTIKA POREMEĆAJA BELE KRVNE LOZE
|
|
|
- Ernest Dorsey
- 5 years ago
- Views:
Transcription

1 UNIVERZITET U NOVOM SADU POLJOPRIVREDNI FAKULTET DEPARTMAN ZA A VETERINARSKU MEDICINU PREDMET: PATOLOŠKA FIZIOLOGIJA IOLOGIJA VEŽBA 4. PATOFIZIOLOŠKA DIJAGNOSTIKA POREMEĆAJA BELE KRVNE LOZE Dr vet. Marko R. Cincović
2 PLAN IZLAGANJA PREGLED LEUKOPOEZE PATOFIZIOLOŠKI POREMEĆAJI BELE KRVNE LOZE MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE
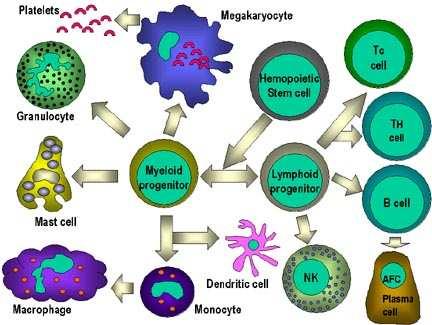
3 PREGLED LEUKOPOEZE
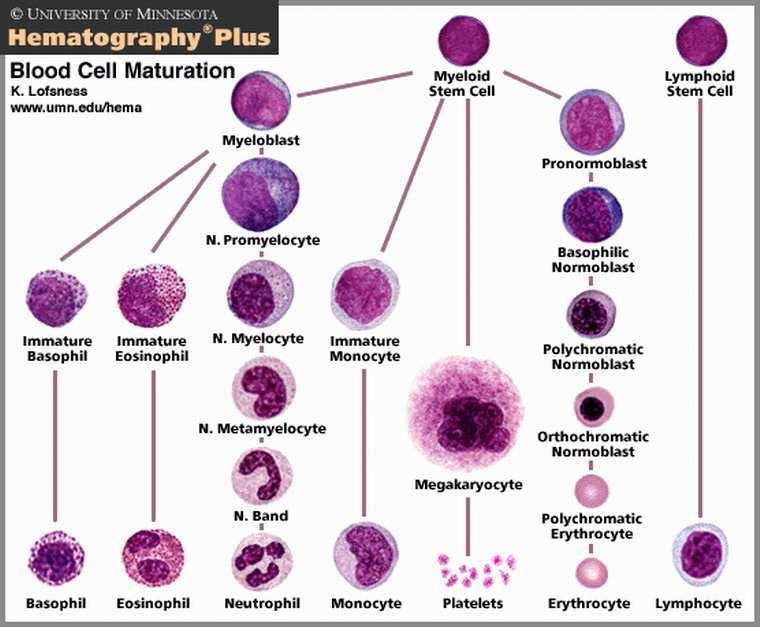
4 PREGLED LEUKOPOEZE

5 PREGLED LEUKOPOEZE Mijeloblast

6 PREGLED LEUKOPOEZE Neutrofilni promijelocit

7 PREGLED LEUKOPOEZE Neutrofilni mijelocit

8 PREGLED LEUKOPOEZE Neutrofilni metamijelocit

9 PREGLED LEUKOPOEZE Neutrofil sa nesegmentiranim jedrom

10 PREGLED LEUKOPOEZE Neutrofil sa segmentiranim jedrom

11 PREGLED LEUKOPOEZE EOZINOFILNI PROMIJELOCIT

12 PREGLED LEUKOPOEZE EOZINOFILNI MIJELOCIT

13 PREGLED LEUKOPOEZE EOZINOFILNI METAMIJELOCITI

14 PREGLED LEUKOPOEZE NESEGMENTIRANI - ŠTAPASTI EOZINOFIL

15 PREGLED LEUKOPOEZE SEGMENTIRANI EOZINOFIL

16 PREGLED LEUKOPOEZE BAZOFILNI MIJELOCIT

17 PREGLED LEUKOPOEZE SEGMENTIRANI BAZOFIL

18 PREGLED LEUKOPOEZE MONOBLAST

19 PREGLED LEUKOPOEZE PROMONOCIT
20 PREGLED LEUKOPOEZE MONOCIT

21 PREGLED LEUKOPOEZE LIMFOCIT
22 PATOFIZIOLOŠKI POREMEĆAJI BELE KRVNE LOZE LEUKOCITOZA LEUKOPENIJA NEUTROFILIJA NEUTROPENIJA EOZINOFILIJA EOZINOPENIJA LIMFOCITOZA LIMFOCITOPENIJA
23 TREBA ZNATI: SKRETANJE U LEVO: Ako se u perifernoj krvi javljaju mlađi oblici razvoja granulocitne loze, sa velikim brojom štapastih granulocita i metamijelocita, onda se takva pojava zove skretanje u levo. SKRETANJE U LEVO, UZ LEUKOPENIJU JE PROGNOSTIČKI LOŠ ZNAK!!!
24 TREBA ZNATI: Ako je skretanje u levo jače izraženo, tako da se u perifernoj krvi pojavljuju mijelociti u većem broju, uz pojavu promijelocita i mijeloblasta, onda se ta pojava naziva mijeloidna leukemična reakcija. Ovo stanje se razlikuje od mijeloproliferativnih bolesti na osnovu: 1. nalaza niskih vrednosti alkalne fosfataze u granulocitima 2. prisustvo filadelfijskog hromozoma 3. veliki % mladih ćelija granulocitne loze 4. eozinofilija i bazofilija u perifernoj krvi govori u prilog hronične granulocitne leukoze
25 PATOFIZIOLOŠKI POREMEĆAJI BELE KRVNE LOZE Klasifikacija oboljenja bele krvne loze: LEUKEMIJE MIJELOPROLIFERATIVNE BOLESTI MIJELODISPLASTIČNI SINDROM LIMFOMI MALIGNA PROLIFERACIJA HISTIOCITNIH I DENDRITIČKIH ĆELIJA (APĆ) MULTIPLI MIJELOMI I DRUGE MONOKLONALNE GAMOPATIJE
26 PATOFIZIOLOŠKI POREMEĆAJI BELE KRVNE LOZE LEUKEMIJE DEFINICIJA Leukemije su maligne bolesti krvi kod kojih postoji progresivno i nesvrsishodno razmnožavanje ćelija jedne od leukocitnih loza, koje je često praćeno povećanjem leukocita u perifernoj krvi, kao i povećanjem leukocitne mase u organizmu.
27 PATOFIZIOLOŠKI POREMEĆAJI BELE KRVNE LOZE LEUKEMIJE Kod leukemijske proliferacije se zapaža izraziti poremećaj u diferentovanju i sazrevanju belih krvnih ćelija. Ovaj proces je izraženiji što je leukemija akutnija!!!
28 PATOFIZIOLOŠKI POREMEĆAJI BELE KRVNE LOZE LEUKEMIJE PROLIFERACIJA LEUKEMIČNIH ĆELIJA U KOSTNOJ SRŽI POTISKIVANJE NORMALNIH MATIČNIH ĆELIJA U KOŠTANOJ SRŽI KVALITATIVNE I KVANTITATIVNE PROMENE U KRVNIM ĆELIJAMA Naročito u akutnim leukemijama ANEMIJA INFEKCIJA KRVARENJE
29 PATOFIZIOLOŠKI POREMEĆAJI BELE KRVNE LOZE LEUKEMIJE Klinički stadijumi bolesti u Hroničnoj limfocitnoj leukemiji (po Rai-u) Stadijum 0 I II III IV Kliničke osobine Limfocitoza u perifernoj krvi i kostnoj srži Limfocitoza sa uvećanjem limfnih žlezda Limfocitoza sa uvećanjem jetre i/ili slezine Limfocitoza sa anemijom Hb ispod 100g/l Limfocitoza sa trombocitopenijom Rizična grupa Niska Srednja Srednja Visoka Visoka
30 PATOFIZIOLOŠKI POREMEĆAJI BELE KRVNE LOZE LEUKEMIJE PODELA LEUKEMIJA PO TIPU ĆELIJA GRANULOCITNE LIMFOCITNE MONOCITNE PODELA LEUKEMIJA U ODNOSU NA BROJ LEUKOCITA U PERIF. KRVI LEUKEMIČNE SUBLEUKEMIČNE ALEUKEMIČNE PODELA LEUKEMIJA PO TOKU AKUTNE HRONIČNE
31 PATOFIZIOLOŠKI POREMEĆAJI BELE KRVNE LOZE LEUKEMIJE AKUTNE LEUKEMIJE L1 L2 ALL Akutna limfoblasna leukemija L3 (Burkitt's s leukemija) AML Akutna mijeloblasna leukemija M0 AML sa minimalnom diferencijacijom M1 AML bez diferencijacije M2 AML sa diferencijacijom M3 Akutna promijelocitna leukemija M4 Akutna mijelomonocitna (Naegeli's( acute leukemia) Akutna monoblasna leukemija M5 Akutna monocitna leukemija Schilling's AL, AMoL M6 Akut. Eritroidna leukemija, diguglielmo's syndrome M7 Akut. Megakariocitna leukemija
32 PATOFIZIOLOŠKI POREMEĆAJI BELE KRVNE LOZE MIJELOPROLIFERATIVNE BOLESTI Klonalna proliferacija mijeloidnih progenitora. Mada od ovih progenitora nastaju Različite linije krvnih ćelija u okviru mijeloproliferativnih bolesti dolazi do poremećaja u jednoj liniji ćelija. Razlikujemo: Polycythemia vera (PV)- Predominantna proliferacija eritroidne loze Esencijalna trombocitemija (ET)- Predominantna proliferacija megakariocitne linije Myelofibrosis sa mijeloidnom metaplazijom (MF) (primarna ili idiopatska mijelofibroza)- Predominantna proliferacija megakariocitne linije, ali se nalazi i fibroza u koštanoj srži. Hronična mijelocitna leukemija (CML)- Predominantna proliferacija granulocitne, primarno neutrofilne linije. Ostale varijante: Hipereozinofilni sindrom Sistemska mastocitoza Mijeloproliferativna-mijelodisplastična bolest Juvenilna mijelomonocitna leukemija.
33 PATOFIZIOLOŠKI POREMEĆAJI BELE KRVNE LOZE MIJELODISPLASTIČNI SINDROM Mijelodisplastični sindrom predstavlja proliferaciju mijeloidnih progenitora, a odlikuje se neefikasnom hematopoezom. Koštana srž je normocelularna ili hipercelularna, a posmatrana diferencijacija nije kompletna. Ćelije su displastične. Klasifikacija poremećaja (FAB klasifikacija): Refraktorna anemija Refraktorna anemija sa prstenastim sideroblastima Refraktorna anemija sa viškom blastnih ćelija (5-20% blast ćel. u srži) Refraktorna anemija sa 21-30% blastnih ćelija u koštanoj srži Transformacija u akutnu leukemiju sa preko 30% blastnih ćelija u srži Hronična mijelomonocitna leukemija
34 PATOFIZIOLOŠKI POREMEĆAJI BELE KRVNE LOZE MIJELODISPLASTIČNI SINDROM KADA POMISLITI NA MIJELODISPLASTIČNI SINDROM? Veterinar mora pomisliti na mijelodisplastični sindrom u uslovima neobjašnjive anemije, neutropenije, trombocitopenije ili monocitoze, sa ili bez znakova insuficijencije koštane srži. U peničnim situacijama razmaz krvi i srži moraju biti detaljno pregledani.
35 PATOFIZIOLOŠKI POREMEĆAJI BELE KRVNE LOZE LIMFOMI Ne-Hodkinsovi limfomi B Cell Lymphomas Precursor B cell lymphoma Precursor B lymphoblastic lymphoma Mature B cell lymphoma Small lymphocytic lymphoma Lymphoplasmacytic lymphoma Splenic marginal zone lymphoma Marginal zone B cell lymphoma of mucosa associated lymphoid tissue (MALT lymphoma, maltoma) Nodal marginal zone B cell lymphoma (monocytoid B cell lymphoma) Follicular lymphoma Mantle cell lymphoma Diffuse large B cell lymphoma Primary mediastinal large B cell lymphoma Intravascular large B cell lymphoma EBV positive senile large cell B cell lymphoma Primary effusion lymphoma Burkitt's lymphoma T/NK Cell Lymphomas Precursor T cell lymphoma Precursor T cell lymphoblastic lymphoma Blastic NK cell lymphoma Mature T/NK cell lymphoma Adult T cell leukemia/lymphoma Extranodal NK/T cell lymphoma, nasal type Enteropathy-associated associated T cell lymphoma Hepatosplenic gamma-delta T cell lymphoma Subcutaneous panniculitis-like like T cell lymphoma Mycosis fungoides Sezary syndrome Primary cutaneous anaplastic large cell lymphoma Peripheral T cell lymphoma, unspecified Angioimmunoblastic T cell lymphoma Anaplastic large cell lymphoma
36 PATOFIZIOLOŠKI POREMEĆAJI BELE KRVNE LOZE LIMFOMI Hodkinsovi limfomi Nodular lymphocyte predominant Hodgkin's lymphoma Classical Hodgkin's lymphoma which includes Nodular schlerosing classical Hodgkin's lymphoma Mixed cellularity classical Hodgkin's lymphoma Lymphocyte-rich classical Hodgkin's lymphoma Lymphocyte-depleted classical Hodgkin's lymphoma
37 PATOFIZIOLOŠKI POREMEĆAJI BELE KRVNE LOZE MALIGNA PROLIFERACIJA HISTIOCITNIH I DENDRITIČKIH ĆELIJA (APĆ) Langerhans cell histiocytosis (Histiocytosis X, Eosinophilic granuloma, Hand-Schiiller-Christian disease, Letterer-Siwe disease) Langerhans cell sarcoma (malignant neoplasma) Histiocytic sarcoma (malignant neoplasm) Erdheim-Chester disease Interdigitating dendritic cell sarcoma (malignant neoplasm) Follicular dendritic cell sarcoma (malignant neoplasm)
38 PATOFIZIOLOŠKI POREMEĆAJI BELE KRVNE LOZE MULTIPLI MIJELOMI I DRUGE MONOKLONALNE GAMOPATIJE Multiple myeloma Plasmacytomas Waldenstrom's macroglobulinemia Primary amyloidosis Heavy chain diseases IgG heavy chain disease IgA heavy chain disease IgM heavy chain disease Monoclonal gammopathy of undetermined significance (MGUS)
39 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 1. Pregled punktata limfne žlezde 2. Određivanje broja leukocita 3. Određivanje leukocitne formule 4. Pregled razmaza periferne krvi i koštane srži 5. Citohemijske osobine ćelija u bolestima bele loze
40 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 1. Pregled punktata limfne žlezde Napraviti razmaz uvećane limfne žlezde i posmatrati najpre na malom pa na velikom uveličanju. REZULTATI Uvećanje l.č. je bitan nalaz u benignim i malignim bolestima limfocitne loze. U toku baterijske infekcije vidi se infiltracija neutrofilnih granulocita, kada se vidi slika piogenog limfadenitisa. U TBC-u u vide se džinovske Langhansove ćelije. U malgnim bolestima može se primetiti da maligne ćelije u potpunosti osti ili delimično potiskuju zdravo tkivo limfnog čvora.
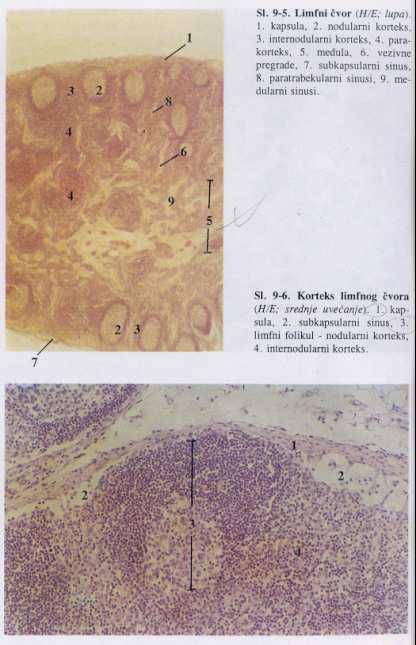
41

42 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 1. Pregled punktata limfne žlezde Zahvatanje limfnih čvorova u limfomima i leukemijama Nodularna infiltracija Nodularna i difuzna infiltracija Difuzna infiltracija Parakortikalna infiltracija Infiltracija mantl zone

43 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 1. Pregled punktata limfne žlezde Neoplastične ćelije limfoma Mali limfocit Centrocit Pleomorfne ćelije Sezary ćelije Centroblast Ćelije Burkittovog NHL Imunoblast Reed-Sternbergova ćelija Limfoplazmocit i plazmocit Varijante RS ćelija Limfoblasti Histiociti

44 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 1. Pregled punktata limfne žlezde Morfologija Reed- Sternbergovi h ćelija u Hodginovom limfomu
45 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 2. Određivanje broja leukocita POTREBAN MATERIJAL Melanžer za leukocita,turkov rastvor,neubauerov hemocitometar, Mikroskop IZVOĐENJE Uvući kap krvi u melanžer za leukocite do ozanke 1. Obrisati vrh melanžera i potom uvući Turkov rastvor do nivoa 11. Tako je postignuto razblaženje 1:10. Lagano mućkati melanžer nekoliko minuta. Na komoricu staviti pokrovno staklo,tako da bude dobro fiksiran (trebaju da se vide Newtonovi obojeni koturovi)


46 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 2. Određivanje broja leukocita IZVOĐENJE Br.leu./µL L = N/4 x 10 x 10 Br leukocita u jednom kvadratiću Razređenje enje Br. LEU u 1mm³ U Litri - red veličina je 10^9 Neubauerova komorica
47 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 3. Određivanje leukocitne formule Izvaditi krv i napraviti razmaz periferne krvi, koji će biti posmatran na uvećanju od 1000x. Diferenciranje leukocita se vrši na 100 ili 200 ćelija. Broji se kao što je dato na donjoj šemi, a rezultate upisujemo prema p datoj tabeli.
48 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 3. Određivanje leukocitne formule Vrsta leukocita BROJANJE Ukupno % Neutrofili 65 65/100 Eozinofili Bazofili Limfociti Monociti
49 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 3. Određivanje leukocitne formule Vrsta Ukupan broj leukocita u 1l krvi Procenat pojedinih vrsta leukocita (%) Neutrofili Eozinofili Bazofili Limfociti Monociti (x 10^9) Čovek Konj Svinja Ovca Koza Pas Mačka Kokoš
50 DIJAGNOSTIKA LEUKOZE GOVEDA PREMA BROJU LEUKOCITA I DIERENCIJALNOJ BELOJ LOZI!!! Maksimalno 30% goveda ispolji limfocitozu Starost goveda Do 3 godine Preko 3 godine Leukozni ključ po Götzeu i sar. (1953) Broj leukocita x10^9 Do 12,0 12,0-18,0 18,0 Preko 18 Do 10,0 10,0-18,0 18,0 Preko 18,0 % limfocita Do Preko 75 Do Preko 75 Prosuđivanje Normalna Sumnjiva Leukozna Normalna Sumnjiva Leukozna
51 DIJAGNOSTIKA LEUKOZE GOVEDA PREMA BROJU LEUKOCITA I DIFERENCIJALNOJ BELOJ LOZI Leukozni ključ za članice Evropske ekonomske zajednice (1978) Starost u godinama Broj limfocita u 10^9/l periferne krvi Normalna Sumljiva Leukozna Do 11,0 11,0-13,0 Preko 13,0 Do 10,0 10,0-12,0 Preko 12,0 Do 8,5 8,5-10,5 Preko 10,5 Do 7,5 7,5-9,5 Preko 9,5 Do 6,5 6,5-8,5 Preko 8,5 Do 6,0 6,0-8,0 Preko 8,0 Do 5,5 5,5-7,5 Preko 7,5 Sličan je i Jugoslovenski leukozni ključ po Stamatoviću iz 1979.

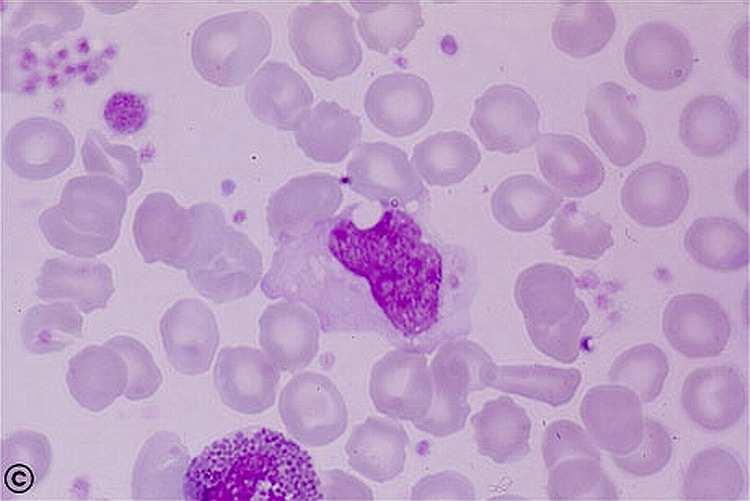
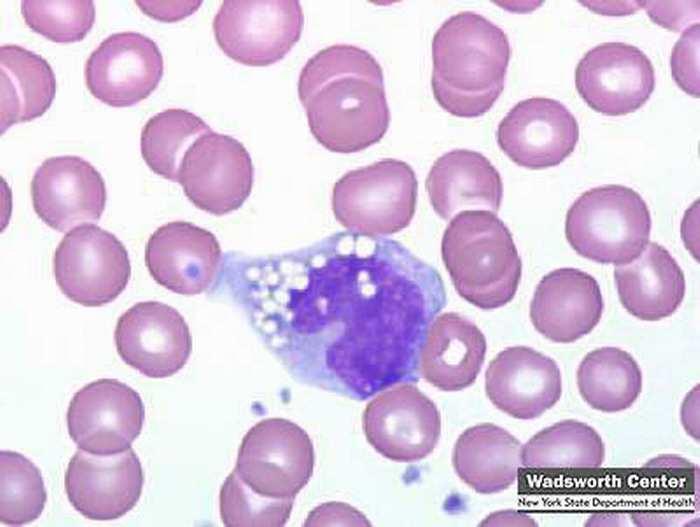
52 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 4. Pregled razmaza periferne krvi i koštane srži

53 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 4. Pregled razmaza periferne krvi i koštane srži
54 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 4. Pregled razmaza periferne krvi i koštane srži Diferencijalna dijagnoza ALL prema obliku ćelija L1 L2 L3 Ćelije Male Uniformne Velike Nejednake Velike, Jednake Citoplazma Oskudna Umerena bazofilija Raznolike u količini i stepenu bazofilije Umereno obilna, Bazofilna, Izražene vakuole Jedro Pravlnog oblika Diskretni nukleolusi Nepravilnog oblika, Izraženi nukleolusi Pravilnog oblika, Izraženi nukleolusi
 Mikroblastična AML Hematogoni Reaktivna limfocitoza AL-L1, aspirat koštane srži")
55 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 4. Pregled razmaza periferne krvi i koštane srži DIFERENCIJALNA DIJAGNOZA Mikromegakariocitna akutna leukemija (M7) Mikroblastična AML Hematogoni Reaktivna limfocitoza AL-L1, aspirat koštane srži Blastne ćelije tipa L1 su male, često po dimenziji slične normalnim perifernim limfocitima. Jedro je okruglo do ovalno sa jednako raspoređenim hromatinom. Nukleolusi načelno nisu vidljivi. Citoplazma je svetlo plava, sa rasutim i nevidljivim granulama. Površine ćelije je ravna ili sa finim membranskim projekcijama.

56 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 4. Pregled razmaza periferne krvi i koštane srži DIFERENCIJALNA DIJAGNOZA Blastična varijanta mantle Limfoma Blastična varijanta NK ćelijske leukemije Blastična varijanta NK/T ćelijske leukemije Male ćelije nehematopoeznih kancera AL-L2, L2, aspirat koštane srži Slične predhodnom osim što su 1,5-2 2 puta veće. Hromatin može biti grupisan, a nukleolus vidljiv. Membrana može biti sa raznim perforacijama.

57 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 4. Pregled razmaza periferne krvi i koštane srži DIFERENCIJALNA DIJAGNOZA Pleomorfni limfomi B i T ćelijske linije L2 ALL M0 i M1 AML Nehematološki tumori AL-L3, Burkitt's Leukemia/Lymphoma, aspirat koštane srži Nešto veće od AL-L1 i prilično uniformnog izgleda. Citoplazma je izrazito bazofilna, i sadrži lipidne vakuole. Moguće je primetiti nukleoluse.

58 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 4. Pregled razmaza periferne krvi i koštane srži AML-M0, aspirat koštane srži Dimenzija kao i neutrofili. Minimalna dierencijacija. Oskudna citolazma siva do svetlo plava. Visok odnos jedro:citoplazma.
59 AML M0 Cytochemistry The blasts are myeloperoxidase (MPO), Sudan black B, and nonspecific esterase (NSE) negative. Immunophenotype Stem cell and hematopoietic progenitor cell markers: CD34+, HLA- DR+, and TdT+ Myeloid lineage markers: CD117+, CD13+ and CD33+. Note that the cytochemistry stain for MPO is usually negative, but positive by immunophenotyping. T cell markers: CD7 is frequently positive, and is an example of what has been designated bilineage, biphenotypic, mixed lineage, or hybrid acute leukemias. Cytogenetics Although no signature abnormality has been identified, complex karyotypes and abnormalities of chromosomes 5, 7, and 11 are relatively common.

60 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 4. Pregled razmaza periferne krvi i koštane srži AML-M1, aspirat koštane srži Dimenzija kao i neutrofili. Minimalna dierencijacija. Oskudna citolazma siva do svetlo plava. Visok odnos jedro:citoplazma.
61 AML M1 Cytochemistry: The blasts are positive for myeloperoxidase (MPO) and Sudan black B, but negative for non-specific esterase (NSE). Immunophenotype: Stem cell and early hematopoietic progenitor markers: CD34+, HLA-DR+, Tdt+ Myeloid lineage markers: CD117+, CD13+, CD33+, MPO+



62 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 4. Pregled razmaza periferne krvi i koštane srži AML-M2, aspirat koštane srži AML-M2 sa eozinofilijom AML-M2 sa bazofilijom
63 AML M2 Cytochemistry: The blasts are positive for myeloperoxidase (MPO), Sudan black B, and chloroacetate esterase (reflecting the abortive maturation effort). The nonspecific esterase stain is negative in the agranular blasts. In acute basophilic leukemia, the diagnostic finding is metachromatic positivity with toluidine blue. Immunophenotype: Stem cell and early hematopoietic progenitor cell markers: CD34+, HLA-DR+, Tdt±. Myeloid lineage markers: CD117+, CD13+, CD33+ Lymphoid lineage markers: CD19, a B cell marker, is usually weakly positive, except in the acute basophilic subtype, and CD56± Cytogenetics: A signature cytogenetic abnormality, t(8;21) is seen in 30% or more of cases, and is seen more in the younger adults with this subtype. No signature cytogenetic abnormality has been identified in the acute basophilic subtype.


64 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 4. Pregled razmaza periferne krvi i koštane srži M3 AML with "angel wings" AML-M3, aspirat koštane srži
65 AML M3 Cytochemistry: The cells are strongly myeloperoxidase, Sudan black B and chloroacetate esterase positive. Immunophenotype: Stem cell and hematopoietic progenitor cell markers: CD34-, HLA-DR- Myeloid lineage markers: CD13+ and CD33+; CD117- and CD15-. Cytogenetics: The signature and diagnostic cytogenetic abnormality is the t(15;17), and has the same diagnostic significance as the t(9;22) in chronic myelocytic leukemia. It is a balanced translocation from the long arm of chromosome 17, the locus of the retinoic acid receptor-α gene, to a site on the long arm of chromosome 15 which is the locus for the promyelocytic leukemia (PML) gene.



66 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 4. Pregled razmaza periferne krvi i koštane srži Atipični, mladi eozinofil AML-M4, aspirat koštane srži


67 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 4. Pregled razmaza periferne krvi i koštane srži Mijeloperoksidaza bojenje Nespecifična esetraza bojenje AML-M4, aspirat koštane srži
68 AML M4 Cytochemistry: The clonal cells stain positive for the myeloid markers, myeloperoxidase (MPO) (d)and chloroacetate esterase, and the monocytic marker, non-specific esterase (NSE) (e) which is not inhibited by flouride. The cells with features of myeloblasts show more MPO positivity while those with features of monocytes show more NSE positivity- some cells stain with both. In the M4Eo subtype, the eosinophils stain like normal neutrophils (e.g. MPO+, Sudan black B+, NSE+) and not normal eosinophils. Immunophenotype: Stem cell and hematopoietic progenitor cell markers- CD34 positivity variable in the M4 subtype, but usually strongly positive in M4Eo subtype Myeloid lineage markers- CD13+, CD33± Monocyte lineage markers- CD14+, CD116±, CD11c±, CD4± Cytogenetics: The signature cytogenetic abnormality found in the M4Eo subtype is inv(16).


69 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 4. Pregled razmaza periferne krvi i koštane srži AML-M5, aspirat koštane srži
70 AML M5 Cytochemistry: In the M5a variant, the non-specific esterase (NSE) is positive (c), and myeloperoxidase (MPO) and Sudan black B are negative. In addition to a positive MSE stain, the Sudan black B may be positive in M5b variant. Immunophenotype: Stem cell and hematopoietic progenitor cell markers- CD34-, HLA-DR - Monocytic lineage markers- CD14±, CD116±, CD11c±, CD64±, CD68±, CD4±, and lysozyme± Myeloid lineage markers- CD33±, CD13±, CD117± Note: In general the M5b subtype shows more positivity with more mature monocyte markers. Cytogenetics: Cytogenetic abnormalities are found in most cases, but a signature abnormality has not been identified. Abnormalities involving the 11q23 are not infrequent, including those cases that occur following exposure to the topisomerase II inhibitors (VP-16 and VM-26).



71 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 4. Pregled razmaza periferne krvi i koštane srži Mijeloblast i eritroblast Atipični eritroblast Ćelije sa vakuolama AML-M6, aspirat koštane srži



72 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 4. Pregled razmaza periferne krvi i koštane srži PAS + bojenje AML-M6, aspirat koštane srži Bojenje Fe, prusko plavo
73 AML M6 Cytochemistry: The myeloperoxidase (MPO), Sudan black B, and nonspecific esterase (NSE) stains are negative in the proerythroblasts. The myeloblastic elements may be MPO, Sudan black B or NSE positive depending on the lineage of the myeloblastic leukemia component. The periodic acid-schiff (PAS) stain frequently shows large PAS positive cytoplasmic granules in the erythroblastic elements (g-h). Immunophenotype: Stem cell and hematopoietic progenitor cell markers- CD34-, HLA-DR- Erythroid lineage markers- The erythroid cells ae positive for glycoforin A Myeloid lineage markers- The myeloblasts are variably positive for CD13, CD33, and CD117. Monocytic lineage markers- Depending on the number of monolytic elements present, CD14, CD11b and 11a, CD4, and CD64 are variably positive. Cytogenetics: No signature cytogenetic abnormality has been identified in this subtype. Complex abnormalities, usually involving chromosomes 5 and 7 are most common, similar to those seen in the myelodysplastic syndromes.


74 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 4. Pregled razmaza periferne krvi i koštane srži Veliki nezreo megakarioblast AML-M7, aspirat koštane srži
75 AML M7 Cytochemistry: May show positivity with acid phosphatase, PAS and NSE stains. Myeloperoxidase and Sudan black B stains are negative. Immunophenotype: Stem cell and hematopoietic progenitor markers- CD34- and HLA-DR- ; a unique feature is that the leukocyte common antigen (CD45) is negative Megakaryocyte lineage markers- CD41 (glycoprotein IIb/IIIa) and/or CD61 (glycoprotein IIIA) usually positive. CD36 (glycoprotein IIIb) is positive. Myeloid lineage markers- CD13 and CD33 may be positive Cytogenetics: No signature cytogenetic abnormality has been identified. In infants under one year of age the t(1;22) often is present.
76 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 4. Pregled razmaza periferne krvi i koštane srži Kvalitativne nenormalnosti krvnih loza u mijelodisplastičnom sindromu Ćelijska loza Eritron Granulociti Megakariociti Monociti Blasti Periferna krv Dimorfija, makrocitoza, anizopoikilocitoza, bazofilno punktirani eritroblasti, retki dakriociti, displastični er-blasti Pseude-pelger neutrof., hipersegmentisani neutrof., Ring- neutrof. sa prstenastim jedrom, Döhleova tela, agranulisanost (kompletna ili segmentirana) Džinovski trombociti, fragmenti megakariocita, sivi (gray) trombociti, mikrotrombociti Česti promonociti, vakuolisani monociti, multilobarni monociti, dvojedarne dendritičke ćelije Koštana srž Eritroidna hiperplazija, ring (prstenasti) sideroblasti, displazni eritroblasti Promijelociti sa retkim ili odsutnim azorpfilnim granulama, hipo ili agranulirani mijelociti i neutrofili, džinovski metamijelociti i mikro i makro-neutrofili Mikro-megakariociti, hipo ili asegmentisani megakariociti, polinuklearni megakariociti Češći promonociti, dvo ili tro-jedarne dendritičke ćelije, sea-blue histiociti. Emperipoleza limfocita u retikuloendotelskim ćelijama Najčešće mali mononuklearni tipa I (1-3 3 azurofilne granule), tipa II (do 15 azurofilnih granula) i tipa III (izrazito granulisani blasti sa ili bez Auerovih štapića)
77 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE Kriterijumi za odvajanje hronične granulocitne leukemije (HGL) od o atipične HGL i hronične mijelomonocitne leukemije (CMML) HGL Vrhovi neutrofila i mijelocita+metamijelocita u leukocitnoj formuli Monociti čine manje od 3% leukocitne formule Znaci dishematopoeze ne postoje ili su minimalni Bazofilija Atipična HGL Promijelociti, mijelociti i metamijelociti čine više od 15% leukocita u perifernoj krvi Monociti čine više od 3% svih leukocita u krvi Postoji disgranulopoeza na nivou mijelocita, metamijelocita i zrelih neutrofila CMML 4. Pregled razmaza periferne krvi i koštane srži Promijelociti, mijelociti i metamijelociti čine zajedno manje od 15% leukocita periferne krvi (tipično je manje od 5%) Monociti čine više od 1x10^9/l leukocita Disgranulopoeza uobičajena ali ne i obavezna
78 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 5. Citohemijske i imunološke osobine ćelija u leukemiji Određivanje broja Leu i diferencijacije bele krvne slike, uz detaljno uzimanje anamneze i fizikalni pregled mogu ukazati na leukemički status. Ipak, konačna dijagnoza se postavlja imuno-citohemijskim metodama pomoću određivanja ćelijskih markera, primenom tehnike rozeta, imunofluorescentna tehnika, tehnika monoklonskih At i dr.
79 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 5. Citohemijske i imunološke osobine ćelija u leukemiji Citohemijska ispitivanja omogućuju dokazivanje prisustva specifičnih enzima i drugih materija u pojedinim ćelijama, jer bojenjem po Pappenheimu nije moguće lako diferentirati blastne ćelije i različite nezrele forme; što je značajno za dijagnostiku akutnih leukemija. Vrši se ispitivanje aktivnosti mijeloperoksidaze bojenjem sudan crnim B. Perjodnom kiselinom (Schiffova PAS reakcija) se boje ćelije u cilju dokazivanja glikogena. Dokazivanje kisele fosfataze, alkalne fosfataze, nespecifične alfa-naftol butirat esteraze, dokazanje muramidaze (lizozomske aktivnsti). Takođe e se vrši i diferenciranje ćelija na osnovu prisustva karakterističnih antigena na površini ćelija ili antigena u samoj ćeliji, pomoću monoklonskih At.
80 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 5. Citohemijske i imunološke osobine ćelija u leukemiji Vrsta leukemije M-1 M-2 M-3 M-4 M-5 M-6 Peroksidaza Sudan B +/ /+ + -/+ + PAS + + +/+ + +/ ± Hloracetat esteraza /+ + +/ ± + Nespecifična butirat- esteraza - ± ± +/ Kisela fosfataza +/- + +/+ + +/ ± Muramidaza - - ± +/++ ±/
81 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 5. Citohemijske i imunološke osobine ćelija u leukemiji Vrsta leukemije 0-ALL CALLA T-ALL B-ALL FAB PODELA L1-L2 L2 L1-L2 L2 L1-L2 L2 L3 PAS Kisela fosfataza Peroksidaza Sudan B Muramidaza - / / / / / / O-ALL = Ni B ni T akutna limfoblasna leukemija CALLA = akutna limfoblasna leukemija sa prisutnim zajedničkim antigenom T-ALL = Akutna T limfoblasna leukemija B-ALL = Akutna B limfoblasna leukemija
82 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 5. Citohemijske i imunološke osobine ćelija u leukemiji Imunofenotipska klasifikacija ALL Tip leukemije Membrana Citoplazma Jedro B-ALL Rana B-prekursor ALL CD19 CD22 TdT Common-B ALL CD19/CD10 CD22 TdT Pre-B ALL CD19 µ TdT B-ALL CD19/CD22 Ig / / T-ALL Pre T-ALL CD7 CD3 TdT T-ALL CD7/CD2 CD3 TdT
83 MARKERI PATOFIZIOLOŠKE PROCENE BELE KRVNE LOZE 5. Citohemijske i imunološke osobine ćelija u leukemiji Osnovni panel monoklonalnih antitela za dijagnostiku limfoma ANTITELO CD20 CD79a CD3 CD45RO CD30 Kappa Lambda ĆELIJA B-ćelije B-ćelije T-ćelije T-ćelije i nezrele B-ćelije RS ćelije B-ćelije B-ćelije BOJENJE Membrana Citoplazma Membrana Membrana Goldžijeva zona Citoplazma Citoplazma

84 PITANJA?
85
Bone Marrow. Procedures Blood Film Aspirate, Cell Block Trephine Biopsy, Touch Imprint
 Bone Marrow Protocol applies to acute leukemias, myelodysplastic syndromes, myeloproliferative disorders, chronic lymphoproliferative disorders, malignant lymphomas, plasma cell dyscrasias, histiocytic
Bone Marrow Protocol applies to acute leukemias, myelodysplastic syndromes, myeloproliferative disorders, chronic lymphoproliferative disorders, malignant lymphomas, plasma cell dyscrasias, histiocytic
2010 Hematopoietic and Lymphoid ICD-O Codes - Alphabetical List THIS TABLE REPLACES ALL ICD-O-3 Codes
 Acute basophilic leukemia 9870/3 Acute biphenotypic leukemia [OBS] 9805/3 Acute erythroid leukemia 9840/3 Acute megakaryoblastic leukemia 9910/3 Acute monoblastic and monocytic leukemia 9891/3 Acute myeloid
Acute basophilic leukemia 9870/3 Acute biphenotypic leukemia [OBS] 9805/3 Acute erythroid leukemia 9840/3 Acute megakaryoblastic leukemia 9910/3 Acute monoblastic and monocytic leukemia 9891/3 Acute myeloid
2012 Hematopoietic and Lymphoid ICD-O Codes - Numerical List THIS TABLE REPLACES ALL ICD-O-3 Codes
 Malignant lymphoma, NOS 9590/3 Non-Hodgkin lymphoma, NOS 9591/3 B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and classical Hodgkin lymphoma 9596/3 Primary
Malignant lymphoma, NOS 9590/3 Non-Hodgkin lymphoma, NOS 9591/3 B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and classical Hodgkin lymphoma 9596/3 Primary
Combinations of morphology codes of haematological malignancies (HM) referring to the same tumour or to a potential transformation
 referring to the same tumour or to a potential transformation") Major subgroups according to the World Health Organisation (WHO) Classification Myeloproliferative neoplasms (MPN) Myeloid and lymphoid neoplasms with eosinophilia and abnormalities of PDGFRA, PDGFRB or
Major subgroups according to the World Health Organisation (WHO) Classification Myeloproliferative neoplasms (MPN) Myeloid and lymphoid neoplasms with eosinophilia and abnormalities of PDGFRA, PDGFRB or
WHO Classification. B-cell chronic lymphocytic leukemia/small T-cell granular lymphocytic leukemia
 Blood Malignancies-II Prof. Dr. Herman Hariman, a Ph.D, SpPK (KH). Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. of Clinical Pathology, School of Medicine, University of North Sumatra WHO classification
Blood Malignancies-II Prof. Dr. Herman Hariman, a Ph.D, SpPK (KH). Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. of Clinical Pathology, School of Medicine, University of North Sumatra WHO classification
The spectrum of flow cytometry of the bone marrow
 The spectrum of flow cytometry of the bone marrow Anna Porwit Lund University Faculty of Medicine Dept. of Clinical Sciences Div. Oncology and Pathology anna.porwit@med.lu.se Disclosure of speaker s interests
The spectrum of flow cytometry of the bone marrow Anna Porwit Lund University Faculty of Medicine Dept. of Clinical Sciences Div. Oncology and Pathology anna.porwit@med.lu.se Disclosure of speaker s interests
Integrated Hematopathology. Morphology and FCI with IHC
 Integrated Hematopathology Morphology and FCI with IHC FrontMatter.indd i 9/6/2009 9:30:12 PM FrontMatter.indd ii 9/6/2009 9:30:18 PM Integrated Hematopathology Morphology and FCI with IHC Cherie H Dunphy,
Integrated Hematopathology Morphology and FCI with IHC FrontMatter.indd i 9/6/2009 9:30:12 PM FrontMatter.indd ii 9/6/2009 9:30:18 PM Integrated Hematopathology Morphology and FCI with IHC Cherie H Dunphy,
Classifications of lymphomas
 Classifications of lymphomas Lukes and Collins Kiel classification Working formulation REAL classification (1994) WHO classification (2000) WHO CLASSIFICATIONF OF NEOPLASMS HAEMATOPETIC AND LYMPHOID TISSUES
Classifications of lymphomas Lukes and Collins Kiel classification Working formulation REAL classification (1994) WHO classification (2000) WHO CLASSIFICATIONF OF NEOPLASMS HAEMATOPETIC AND LYMPHOID TISSUES
Clinical Policy: Bendamustine (Bendeka, Treanda) Reference Number: PA.CP.PHAR.307
 Reference Number: PA.CP.PHAR.307") Clinical Policy: (Bendeka, Treanda) Reference Number: PA.CP.PHAR.307 Effective Date: 01/18 Last Review Date: 11/17 Coding Implications Revision Log Description The intent of the criteria is to ensure that
Clinical Policy: (Bendeka, Treanda) Reference Number: PA.CP.PHAR.307 Effective Date: 01/18 Last Review Date: 11/17 Coding Implications Revision Log Description The intent of the criteria is to ensure that
Lymphoma/CLL 101: Know your Subtype. Dr. David Macdonald Hematologist, The Ottawa Hospital
 Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Non-Hodgkin Lymphoma. Protocol applies to non-hodgkin lymphoma involving any organ system except the gastrointestinal tract.
 Non-Hodgkin Lymphoma Protocol applies to non-hodgkin lymphoma involving any organ system except the gastrointestinal tract. Protocol revision date: January 2005 No AJCC/UICC staging system Procedures Cytology
Non-Hodgkin Lymphoma Protocol applies to non-hodgkin lymphoma involving any organ system except the gastrointestinal tract. Protocol revision date: January 2005 No AJCC/UICC staging system Procedures Cytology
Reviewing the ICD-10 classification of haematological neoplasms on its way to ICD-11
 WHO-FIC NETWORK MEETING Tokyo, Japan haematological neoplasms on its way to ICD-11 Ulrich Vogel, Robert Jakob, Michael Schopen, Harald Stein, Stefan Krause Abstract: haematological neoplasms on its way
WHO-FIC NETWORK MEETING Tokyo, Japan haematological neoplasms on its way to ICD-11 Ulrich Vogel, Robert Jakob, Michael Schopen, Harald Stein, Stefan Krause Abstract: haematological neoplasms on its way
Contents. vii. Preface... Acknowledgments... v xiii
 Contents Preface... Acknowledgments... v xiii SECTION I 1. Introduction... 3 Knowledge-Based Diagnosis... 4 Systematic Examination of the Lymph Node... 7 Cell Type Identification... 9 Cell Size and Cellularity...
Contents Preface... Acknowledgments... v xiii SECTION I 1. Introduction... 3 Knowledge-Based Diagnosis... 4 Systematic Examination of the Lymph Node... 7 Cell Type Identification... 9 Cell Size and Cellularity...
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells. Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital
 Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Classification of Hematologic Malignancies. Patricia Aoun MD MPH
 Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
Hematology Unit Lab 2 Review Material
 Objectives Hematology Unit Lab 2 Review Material - 2018 Laboratory Instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Objectives Hematology Unit Lab 2 Review Material - 2018 Laboratory Instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Hepatic Lymphoma Diagnosis An Algorithmic Approach
 Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
Plasma cell myeloma (multiple myeloma)
") Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
Bone Marrow. Procedures Blood Film Aspirate, Cell Block Trephine Biopsy, Touch Imprint
 Bone Marrow Protocol applies to acute leukemias, myelodysplastic syndromes, myeloproliferative disorders, chronic lymphoproliferative disorders, malignant lymphomas, plasma cell dyscrasias, histiocytic
Bone Marrow Protocol applies to acute leukemias, myelodysplastic syndromes, myeloproliferative disorders, chronic lymphoproliferative disorders, malignant lymphomas, plasma cell dyscrasias, histiocytic
Burkitt lymphoma. Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8
 Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Bone Marrow. Procedures Blood Film Aspirate, Cell Block Trephine Biopsy, Touch Imprint
 Bone Marrow Protocol applies to acute leukemias, myelodysplastic syndromes, myeloproliferative disorders, chronic lymphoproliferative disorders, malignant lymphomas, plasma cell dyscrasias, histiocytic
Bone Marrow Protocol applies to acute leukemias, myelodysplastic syndromes, myeloproliferative disorders, chronic lymphoproliferative disorders, malignant lymphomas, plasma cell dyscrasias, histiocytic
Introduction: The Revised (4 th Edition) World Health Organization (WHO) Classification of Tumors of Hematopoietic and Lymphoid Tissues
 World Health Organization (WHO) Classification of Tumors of Hematopoietic and Lymphoid Tissues") Society for Hematopathology Scientific Symposium USCAP Companion Meeting, Boston, MA March 8, 2009 Boston, MA Steven H. Swerdlow and James Vardiman, Moderators Introduction: The Revised (4 th Edition)
Society for Hematopathology Scientific Symposium USCAP Companion Meeting, Boston, MA March 8, 2009 Boston, MA Steven H. Swerdlow and James Vardiman, Moderators Introduction: The Revised (4 th Edition)
Hematology Page 1 of 8
 Hematology Page 1 of 8 Hematology Major Category Code Headings Revised 12/17 1 Basic methodology and test armamentarium 20000 2 Normal hematopoiesis & hemostasis 20100 3 RBC disorders, non-neoplastic 20340
Hematology Page 1 of 8 Hematology Major Category Code Headings Revised 12/17 1 Basic methodology and test armamentarium 20000 2 Normal hematopoiesis & hemostasis 20100 3 RBC disorders, non-neoplastic 20340
DETERMINATION OF A LYMPHOID PROCESS
 Chapter 2 Applications of Touch Preparation Cytology to Intraoperative Consultations: Lymph Nodes and Extranodal Tissues for Evaluation of Hematolymphoid Disorders INTRODUCTION As discussed in Chap. 1,
Chapter 2 Applications of Touch Preparation Cytology to Intraoperative Consultations: Lymph Nodes and Extranodal Tissues for Evaluation of Hematolymphoid Disorders INTRODUCTION As discussed in Chap. 1,
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL)
 Hodgkin lymphoma )HL)") Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and
 Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and / or peripheral blood Classified based on cell type
Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and / or peripheral blood Classified based on cell type
Small B-cell (Histologically Low Grade) Lymphoma
 Lymphoma") Frequency of Lymphoid Neoplasms Small B-cell (Histologically Low Grade) Lymphoma Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital B-cell neoplasms 88% Diffuse large B-cell lymphoma
Frequency of Lymphoid Neoplasms Small B-cell (Histologically Low Grade) Lymphoma Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital B-cell neoplasms 88% Diffuse large B-cell lymphoma
Immunopathology of Lymphoma
 Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
Lymphoma: What You Need to Know. Richard van der Jagt MD, FRCPC
 Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
During past decades, because of the lack of knowledge
 Staging and Classification of Lymphoma Ping Lu, MD In 2004, new cases of non-hodgkin s in the United States were estimated at 54,370, representing 4% of all cancers and resulting 4% of all cancer deaths,
Staging and Classification of Lymphoma Ping Lu, MD In 2004, new cases of non-hodgkin s in the United States were estimated at 54,370, representing 4% of all cancers and resulting 4% of all cancer deaths,
The College of American Pathologists offers these protocols
 Strategies for Laboratory and Patient Management Protocol for the Examination of Specimens From Patients With Hematopoietic Neoplasms of the Bone Marrow A Basis for Checklists LoAnn C. Peterson, MD; Steven
Strategies for Laboratory and Patient Management Protocol for the Examination of Specimens From Patients With Hematopoietic Neoplasms of the Bone Marrow A Basis for Checklists LoAnn C. Peterson, MD; Steven
88-year-old Female with Lymphadenopathy. Faizi Ali, MD
 88-year-old Female with Lymphadenopathy Faizi Ali, MD Clinical History A 88-year-old caucasian female presented to our hospital with the complaints of nausea, vomiting,diarrhea, shortness of breath and
88-year-old Female with Lymphadenopathy Faizi Ali, MD Clinical History A 88-year-old caucasian female presented to our hospital with the complaints of nausea, vomiting,diarrhea, shortness of breath and
Change Summary - Form 2018 (R3) 1 of 12
 1 of 12") Summary - Form 2018 (R3) 1 of 12 Form Question Number (r3) Type Description New Text Previous Text Today's date was removed 2018 N/A Today's Date Removed from Key Fields 2018 N/A HCT Type 2018 N/A Product
Summary - Form 2018 (R3) 1 of 12 Form Question Number (r3) Type Description New Text Previous Text Today's date was removed 2018 N/A Today's Date Removed from Key Fields 2018 N/A HCT Type 2018 N/A Product
HEMATOPATHOLOGY (SHANDS HOSPITAL AT THE UNIVERSITY OF FLORIDA): Rotation Director: Ying Li, M.D., Ph.D., Assistant Professor
: Rotation Director: Ying Li, M.D., Ph.D., Assistant Professor") HEMATOPATHOLOGY (SHANDS HOSPITAL AT THE UNIVERSITY OF FLORIDA): Rotation Director: Ying Li, M.D., Ph.D., Assistant Professor I. Description of the rotation: During this rotation, the resident will gain
HEMATOPATHOLOGY (SHANDS HOSPITAL AT THE UNIVERSITY OF FLORIDA): Rotation Director: Ying Li, M.D., Ph.D., Assistant Professor I. Description of the rotation: During this rotation, the resident will gain
Large cell immunoblastic Diffuse histiocytic (DHL) Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s
 Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s") Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Mixed Phenotype Acute Leukemias
 Mixed Phenotype Acute Leukemias CHEN GAO; AMY M. SANDS; JIANLAN SUN NORTH AMERICAN JOURNAL OF MEDICINE AND SCIENCE APR 2012 VOL 5 NO.2 INTRODUCTION Most cases of acute leukemia can be classified based
Mixed Phenotype Acute Leukemias CHEN GAO; AMY M. SANDS; JIANLAN SUN NORTH AMERICAN JOURNAL OF MEDICINE AND SCIENCE APR 2012 VOL 5 NO.2 INTRODUCTION Most cases of acute leukemia can be classified based
Pathology. #11 Acute Leukemias. Farah Banyhany. Dr. Sohaib Al- Khatib 23/2/16
 35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
Contractor Name: Novitas Solutions, Inc. Contractor Number: Contractor Type: MAC A. LCD ID Number: L35032 Status: A-Approved
 LCD for Flow Cytometry (L35032) Contractor Name: Novitas Solutions, Inc. Contractor Number: 12501 Contractor Type: MAC A LCD ID Number: L35032 Status: A-Approved Contractor Information LCD Information
LCD for Flow Cytometry (L35032) Contractor Name: Novitas Solutions, Inc. Contractor Number: 12501 Contractor Type: MAC A LCD ID Number: L35032 Status: A-Approved Contractor Information LCD Information
Changes to the Hematopoietic and Lymphoid Neoplasm Coding Manual
 Changes to the Hematopoietic and Lymphoid Neoplasm Coding Manual KCR 2018 SPRING TRAINING 2018 Hematopoietic Database Updates Updates were done to the Hematopoietic Database based on the WHO Hematopoietic
Changes to the Hematopoietic and Lymphoid Neoplasm Coding Manual KCR 2018 SPRING TRAINING 2018 Hematopoietic Database Updates Updates were done to the Hematopoietic Database based on the WHO Hematopoietic
Non-Hodgkin s Lymphomas Version
 NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Non-Hodgkin s Lymphomas Version 2.2015 NCCN.org Continue Use of Immunophenotyping/ Genetic Testing in Differential Diagnosis of Mature B-Cell
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Non-Hodgkin s Lymphomas Version 2.2015 NCCN.org Continue Use of Immunophenotyping/ Genetic Testing in Differential Diagnosis of Mature B-Cell
Tim R. Randolph. PhD, MT(ASCP) Chair and Associate Professor Department of Biomedical Laboratory Science Saint Louis University
 Chair and Associate Professor Department of Biomedical Laboratory Science Saint Louis University") Tim R. Randolph. PhD, MT(ASCP) Chair and Associate Professor Department of Biomedical Laboratory Science Saint Louis University Anemias Over 30 types Myeloproliferative Neoplasm Polycythemia Leukemia AML:M6
Tim R. Randolph. PhD, MT(ASCP) Chair and Associate Professor Department of Biomedical Laboratory Science Saint Louis University Anemias Over 30 types Myeloproliferative Neoplasm Polycythemia Leukemia AML:M6
Acute myeloid leukemia. M. Kaźmierczak 2016
 Acute myeloid leukemia M. Kaźmierczak 2016 Acute myeloid leukemia Malignant clonal disorder of immature hematopoietic cells characterized by clonal proliferation of abnormal blast cells and impaired production
Acute myeloid leukemia M. Kaźmierczak 2016 Acute myeloid leukemia Malignant clonal disorder of immature hematopoietic cells characterized by clonal proliferation of abnormal blast cells and impaired production
Acute Myeloid Leukemia with Recurrent Cytogenetic Abnormalities
 Acute Myeloid Leukemia with Recurrent Cytogenetic Abnormalities Acute Myeloid Leukemia with recurrent cytogenetic Abnormalities -t(8;21)(q22;q22)(aml/eto) -inv(16) or t(16;16) -t(15;17) -11q23 Acute Myeloid
Acute Myeloid Leukemia with Recurrent Cytogenetic Abnormalities Acute Myeloid Leukemia with recurrent cytogenetic Abnormalities -t(8;21)(q22;q22)(aml/eto) -inv(16) or t(16;16) -t(15;17) -11q23 Acute Myeloid
Clinical Policy: Bendamustine (Bendeka, Treanda) Reference Number: CP.PHAR.307
 Reference Number: CP.PHAR.307") Clinical Policy: (Bendeka, Treanda) Reference Number: CP.PHAR.307 Effective Date: 02/17 Last Review Date: 02/17 Coding Implications Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Bendeka, Treanda) Reference Number: CP.PHAR.307 Effective Date: 02/17 Last Review Date: 02/17 Coding Implications Revision Log See Important Reminder at the end of this policy for important
Lymphoid Neoplasms. Sylvie Freeman Department of Clinical Immunology, University of Birmingham
 Lymphoid Neoplasms Sylvie Freeman Department of Clinical Immunology, University of Birmingham Incidence of Haematological Malignancies UK2001 (CRUK) Malignancy New Cases All Cancers 271,000 Leukaemia 6,760
Lymphoid Neoplasms Sylvie Freeman Department of Clinical Immunology, University of Birmingham Incidence of Haematological Malignancies UK2001 (CRUK) Malignancy New Cases All Cancers 271,000 Leukaemia 6,760
Corrigenda. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (revised 4th edition): corrections made in second print run
: corrections made in second print run") Corrigenda WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (revised 4th edition): corrections made in second print run In addition to corrections of minor typographical errors, corrections
Corrigenda WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (revised 4th edition): corrections made in second print run In addition to corrections of minor typographical errors, corrections
Bone marrow aspiration as the initial diagnostic tool in the diagnosis of leukemia - A case study
 Original Research Article Bone marrow aspiration as the initial diagnostic tool in the diagnosis of leukemia - A case study Priyanka Poonam 1*, N.K. Bariar 2 1 Tutor, Department of Pathology, Patna Medical
Original Research Article Bone marrow aspiration as the initial diagnostic tool in the diagnosis of leukemia - A case study Priyanka Poonam 1*, N.K. Bariar 2 1 Tutor, Department of Pathology, Patna Medical
Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED
 Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED Acute Myeloid Leukemia Firstly we ll start with this introduction then enter the title of the lecture, so be ready and let s begin by the name of Allah : We
Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED Acute Myeloid Leukemia Firstly we ll start with this introduction then enter the title of the lecture, so be ready and let s begin by the name of Allah : We
7 Omar Abu Reesh. Dr. Ahmad Mansour Dr. Ahmad Mansour
 7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
3/5/2013. Hematopoiesis: Red and white marrow. Hematopoiesis. Bone marrow aspirate and core biopsy. Gartner, Color Textbook of Histology, 3 rd Edition
 Hematopoiesis Hematopoiesis: Red and white marrow Bone marrow aspirate and core biopsy Gartner, Color Textbook of Histology, 3 rd Edition 1 reticulocytes elliptocytes schistocytes spheroctyes target cells
Hematopoiesis Hematopoiesis: Red and white marrow Bone marrow aspirate and core biopsy Gartner, Color Textbook of Histology, 3 rd Edition 1 reticulocytes elliptocytes schistocytes spheroctyes target cells
2007 Workshop of Society for Hematopathology & European Association for Hematopathology Indianapolis, IN, USA Case # 228
 2007 Workshop of Society for Hematopathology & European Association for Hematopathology Indianapolis, IN, USA Case # 228 Vishnu V. B Reddy, MD University of Alabama at Birmingham Birmingham, AL USA 11/03/07
2007 Workshop of Society for Hematopathology & European Association for Hematopathology Indianapolis, IN, USA Case # 228 Vishnu V. B Reddy, MD University of Alabama at Birmingham Birmingham, AL USA 11/03/07
2 nd step do Bone Marrow Study If possible both the aspiration and
 Blood Malignancies-I Prof. Herman Hariman,SpPK a (KH). Ph.D.(U.K) Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. Clinpath, FK-USU First do the Full Blood Count Hb, WBCS, Platelets Morphology!! Such as blasts,
Blood Malignancies-I Prof. Herman Hariman,SpPK a (KH). Ph.D.(U.K) Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. Clinpath, FK-USU First do the Full Blood Count Hb, WBCS, Platelets Morphology!! Such as blasts,
HEMATOPATHOLOGY DIAGNOSIS & SUBTYPING. Use of IHC. Use of Polymerase Chain Reaction (PCR) Use of Flow Cytometry
 Use of Flow Cytometry") HEMATOPATHOLOGY DIAGNOSIS & SUBTYPING HEMATOPATHOLOGY DIAGNOSIS & SUBTYPING The 2008 WHO classification system for tumors of hematopoietic and lymphoid tissues specifies that various combinations of immunophenotypic
HEMATOPATHOLOGY DIAGNOSIS & SUBTYPING HEMATOPATHOLOGY DIAGNOSIS & SUBTYPING The 2008 WHO classification system for tumors of hematopoietic and lymphoid tissues specifies that various combinations of immunophenotypic
The primary medical content categories of the blueprint are shown below, with the percentage assigned to each for a typical exam:
 Hematology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified hematologist
Hematology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified hematologist
MOC HEM - General Hematopathology (Mandatory 50-Question Module)
") MOC HEM - General Hematopathology (Mandatory 50-Question Module) acute monoblastic/monocytic leukemia infectious mononucleosis adult T cell leukemia/lymphoma in situ follicular lymphoma ALL; phenotypes
MOC HEM - General Hematopathology (Mandatory 50-Question Module) acute monoblastic/monocytic leukemia infectious mononucleosis adult T cell leukemia/lymphoma in situ follicular lymphoma ALL; phenotypes
MOC HEM - General Hematopathology (Mandatory 50-Question Module)
") MOC HEM - General Hematopathology (Mandatory 50-Question Module) acute monoblastic/monocytic leukemia infectious mononucleosis adult T cell leukemia/lymphoma in situ follicular lymphoma ALL; phenotypes
MOC HEM - General Hematopathology (Mandatory 50-Question Module) acute monoblastic/monocytic leukemia infectious mononucleosis adult T cell leukemia/lymphoma in situ follicular lymphoma ALL; phenotypes
Case 3. Ann T. Moriarty,MD
 Case 3 Ann T. Moriarty,MD Case 3 59 year old male with asymptomatic cervical lymphadenopathy. These images are from a fine needle biopsy of a left cervical lymph node. Image 1 Papanicolaou Stained smear,100x.
Case 3 Ann T. Moriarty,MD Case 3 59 year old male with asymptomatic cervical lymphadenopathy. These images are from a fine needle biopsy of a left cervical lymph node. Image 1 Papanicolaou Stained smear,100x.
HEMATOLOGIC MALIGNANCIES BIOLOGY
 HEMATOLOGIC MALIGNANCIES BIOLOGY Failure of terminal differentiation Failure of differentiated cells to undergo apoptosis Failure to control growth Neoplastic stem cell FAILURE OF TERMINAL DIFFERENTIATION
HEMATOLOGIC MALIGNANCIES BIOLOGY Failure of terminal differentiation Failure of differentiated cells to undergo apoptosis Failure to control growth Neoplastic stem cell FAILURE OF TERMINAL DIFFERENTIATION
WBCs Disorders 1. Dr. Nabila Hamdi MD, PhD
 WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
ADx Bone Marrow Report. Patient Information Referring Physician Specimen Information
 ADx Bone Marrow Report Patient Information Referring Physician Specimen Information Patient Name: Specimen: Bone Marrow Site: Left iliac Physician: Accession #: ID#: Reported: 08/19/2014 - CHRONIC MYELOGENOUS
ADx Bone Marrow Report Patient Information Referring Physician Specimen Information Patient Name: Specimen: Bone Marrow Site: Left iliac Physician: Accession #: ID#: Reported: 08/19/2014 - CHRONIC MYELOGENOUS
HEMATOPATHOLOGY. 2017/2018 2nd semester
 HEMATOPATHOLOGY 2017/2018 2nd semester NORMAL HAEMOPOESIS COMMON MYELOID PRGENITOR HEMATOPOIETIC STEM CELL COMMON LYMPHOID PROGENITOR NK T B MEGAKARYO- BLAST PRONORMO- BLAST MONOBLAST MYELOBLAST PRO NK
HEMATOPATHOLOGY 2017/2018 2nd semester NORMAL HAEMOPOESIS COMMON MYELOID PRGENITOR HEMATOPOIETIC STEM CELL COMMON LYMPHOID PROGENITOR NK T B MEGAKARYO- BLAST PRONORMO- BLAST MONOBLAST MYELOBLAST PRO NK
WBCs Disorders. Dr. Nabila Hamdi MD, PhD
 WBCs Disorders Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features and
WBCs Disorders Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features and
LYMPHOMAS an overview of some subtypes of NHLs
 One of the confusing aspects of the lymphoid neoplasms concerns the use of the descriptive terms "leukemia" and "lymphoma." LYMPHOMAS an overview of some subtypes of NHLs Leukemia is used for lymphoid
One of the confusing aspects of the lymphoid neoplasms concerns the use of the descriptive terms "leukemia" and "lymphoma." LYMPHOMAS an overview of some subtypes of NHLs Leukemia is used for lymphoid
Myeloproliferative Disorders - D Savage - 9 Jan 2002
 Disease Usual phenotype acute leukemia precursor chronic leukemia low grade lymphoma myeloma differentiated Total WBC > 60 leukemoid reaction acute leukemia Blast Pro Myel Meta Band Seg Lymph 0 0 0 2
Disease Usual phenotype acute leukemia precursor chronic leukemia low grade lymphoma myeloma differentiated Total WBC > 60 leukemoid reaction acute leukemia Blast Pro Myel Meta Band Seg Lymph 0 0 0 2
Case year old male with abdominal lymphadenopathy Treated with 8 cycles of R-CHOP One year later B-symptoms and progressive disease
 Codirectors Tsieh Sun, M.D., FASCP Francisco Vega, M.D., Ph.D. Department of Hematopathology UT MD Anderson Cancer Center Houston Texas There is no conflict of interest involved in the content and presentation
Codirectors Tsieh Sun, M.D., FASCP Francisco Vega, M.D., Ph.D. Department of Hematopathology UT MD Anderson Cancer Center Houston Texas There is no conflict of interest involved in the content and presentation
Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies
 Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies Megan S. Lim MD PhD University of Pennsylvania October 8, 2018 Objectives To understand how the trend toward less invasive lymph
Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies Megan S. Lim MD PhD University of Pennsylvania October 8, 2018 Objectives To understand how the trend toward less invasive lymph
Pathology of Hematopoietic and Lymphoid tissue
 CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
B980 B968. C836 Diffuse non-hodgkin's lymphoma, undifferentiated (diffuse) C839 Non-follicular diffuse non-hodgkin lymphoma, unspecified
 C839 Non-follicular diffuse non-hodgkin lymphoma, unspecified") รหะส ICD ท ยกเล ก (ตาม DRG 5.1.1) รหะสท ยกเล ก Description รหะสท ใช Description A090 Other and unspecified gastroenteritis and colitis of infectious origin A09 Diarrhoea and gastroenteritis of presumed
รหะส ICD ท ยกเล ก (ตาม DRG 5.1.1) รหะสท ยกเล ก Description รหะสท ใช Description A090 Other and unspecified gastroenteritis and colitis of infectious origin A09 Diarrhoea and gastroenteritis of presumed
Bone Marrow Pathology. Part 1. R.S. Riley, M.D., Ph.D.
 Bone Marrow Pathology Part 1 R.S. Riley, M.D., Ph.D. Bone Marrow Pathology Bone marrow basics Red cell diseases White cell diseases Other diseases Bone Marrow Pathology Bone marrow basics Hematopoiesis
Bone Marrow Pathology Part 1 R.S. Riley, M.D., Ph.D. Bone Marrow Pathology Bone marrow basics Red cell diseases White cell diseases Other diseases Bone Marrow Pathology Bone marrow basics Hematopoiesis
155.2 Malignant neoplasm of liver not specified as primary or secondary. C22.9 Malignant neoplasm of liver, not specified as primary or secondary
 ICD-9 TO ICD-10 Reference ICD-9 150.9 Malignant neoplasm of esophagus unspecified site C15.9 Malignant neoplasm of esophagus, unspecified 151.9 Malignant neoplasm of stomach unspecified site C16.9 Malignant
ICD-9 TO ICD-10 Reference ICD-9 150.9 Malignant neoplasm of esophagus unspecified site C15.9 Malignant neoplasm of esophagus, unspecified 151.9 Malignant neoplasm of stomach unspecified site C16.9 Malignant
Laboratory Diagnosis for WBC Pathology
 CLINICAL PATHOLOGY Dr. Araceli Jacoba WBC Parameters WBC Count Differential count Absolute count Leukocyte Alkaline Phosphatase (LAP) Special stains of WBC Cluster designation Types of WBC Counts WBC Count
CLINICAL PATHOLOGY Dr. Araceli Jacoba WBC Parameters WBC Count Differential count Absolute count Leukocyte Alkaline Phosphatase (LAP) Special stains of WBC Cluster designation Types of WBC Counts WBC Count
THE SOCIETY FOR Hematopathology and the European
 SPECIAL ARTICLE World Health Organization Classification of Neoplastic Diseases of the Hematopoietic and Lymphoid Tissues: Report of the Clinical Advisory Committee Meeting Airlie House, Virginia, November
SPECIAL ARTICLE World Health Organization Classification of Neoplastic Diseases of the Hematopoietic and Lymphoid Tissues: Report of the Clinical Advisory Committee Meeting Airlie House, Virginia, November
Citomorfološka dijagnostika akutnih mijeloičnih leukemija podjela prema Svjetskoj zdravstvenoj organizaciji
 Kratki pregledni članak/mini-review Citomorfološka dijagnostika akutnih mijeloičnih leukemija podjela prema Svjetskoj zdravstvenoj organizaciji Cytomorphologic diagnostics of acute myeloid leukemia the
Kratki pregledni članak/mini-review Citomorfološka dijagnostika akutnih mijeloičnih leukemija podjela prema Svjetskoj zdravstvenoj organizaciji Cytomorphologic diagnostics of acute myeloid leukemia the
3.1 Introduction. It is emphasised that not all tests are necessarily required in every case. 3.2 Taxonomic structure
 CHAPTER 3 CLASSIFICATION 3.1 Introduction Accurate diagnosis underpins lymphoma management. Historically, competing lymphoma classifications have been a source of frustration to pathologists, clinicians
CHAPTER 3 CLASSIFICATION 3.1 Introduction Accurate diagnosis underpins lymphoma management. Historically, competing lymphoma classifications have been a source of frustration to pathologists, clinicians
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology. Songlin Zhang, MD, PhD LSUHSC-Shreveport
 From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
Practical Diagnosis of Hematologic Disorders. Vol 2 Malignant Disorders
 5 th ed Practical Diagnosis of Hematologic Disorders Vol 2 Malignant Disorders Vol2_FrontMatter_v03_0804 final.indd i 8/6/2009 10:00:11 PM Authors Carl R Kjeldsberg, MD Professor of Pathology, University
5 th ed Practical Diagnosis of Hematologic Disorders Vol 2 Malignant Disorders Vol2_FrontMatter_v03_0804 final.indd i 8/6/2009 10:00:11 PM Authors Carl R Kjeldsberg, MD Professor of Pathology, University
Many of the hematolymphoid disorders are derived
 REVIEW ARTICLE Practical Immunohistochemistry in Hematopathology: A Review of Useful Antibodies for Diagnosis Ji Lu, MD and Karen L. Chang, MD Abstract: This review article offers some useful panels of
REVIEW ARTICLE Practical Immunohistochemistry in Hematopathology: A Review of Useful Antibodies for Diagnosis Ji Lu, MD and Karen L. Chang, MD Abstract: This review article offers some useful panels of
Immunohistochemical classification of haematolymphoid tumours. Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital
 Immunohistochemical classification of haematolymphoid tumours Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital Malignant lymphoproliferative diseases What are they? Haematolymphoid
Immunohistochemical classification of haematolymphoid tumours Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital Malignant lymphoproliferative diseases What are they? Haematolymphoid
New Haven, Connecticut
 New Haven, Connecticut Yale University Main Campus Yale mascot: Handsome Dan Cutaneous Lymphomas Tony Subtil, MD, MBA Associate Professor Yale University Cutaneous Lymphomas: 1. Intro 2. CTCL/NK 3. CBCL
New Haven, Connecticut Yale University Main Campus Yale mascot: Handsome Dan Cutaneous Lymphomas Tony Subtil, MD, MBA Associate Professor Yale University Cutaneous Lymphomas: 1. Intro 2. CTCL/NK 3. CBCL
Participants Identification No. % Evaluation. Mitotic figure Educational Erythrocyte precursor, abnormal 1 0.
 Cell Identification Mitotic figure 212 99.5 Educational Erythrocyte precursor, abnormal BMD-02 The arrowed cell is a mitotic figure. It was correctly identified by 99.5% of the participants. A cell containing
Cell Identification Mitotic figure 212 99.5 Educational Erythrocyte precursor, abnormal BMD-02 The arrowed cell is a mitotic figure. It was correctly identified by 99.5% of the participants. A cell containing
Evaluation of Bone Marrow Biopsies and Aspirates ANNA PORWIT DEPARTMENT OF PATHOLOGY, LUND UNIVERSITY
 Evaluation of Bone Marrow Biopsies and Aspirates ANNA PORWIT DEPARTMENT OF PATHOLOGY, LUND UNIVERSITY DISCLOSURES NONE Learning objectives To review the rules of BMA evaluation To review the main issues
Evaluation of Bone Marrow Biopsies and Aspirates ANNA PORWIT DEPARTMENT OF PATHOLOGY, LUND UNIVERSITY DISCLOSURES NONE Learning objectives To review the rules of BMA evaluation To review the main issues
Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU
 Rex K.H. Au-Yeung Department of Pathology, HKU") Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU Lecture outline Time 10:00 11:00 11:15 12:10 12:20 13:15 Content Introduction to lymphoma Review of lymphocyte biology
Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU Lecture outline Time 10:00 11:00 11:15 12:10 12:20 13:15 Content Introduction to lymphoma Review of lymphocyte biology
12 Dynamic Interactions between Hematopoietic Stem and Progenitor Cells and the Bone Marrow: Current Biology of Stem Cell Homing and Mobilization
 Table of Contents: PART I: Molecular and Cellular Basis of Hematology 1 Anatomy and Pathophysiology of the Gene 2 Genomic Approaches to Hematology 3 Regulation of Gene Expression, Transcription, Splicing,
Table of Contents: PART I: Molecular and Cellular Basis of Hematology 1 Anatomy and Pathophysiology of the Gene 2 Genomic Approaches to Hematology 3 Regulation of Gene Expression, Transcription, Splicing,
2/13/2015. Hematopoiesis: Red and white marrow. Fluorescent in situ hybridization for chromosomal translocation. Hematopoiesis
 Fluorescent in situ hybridization for chromosomal translocation Hematopoiesis Hematopoiesis: Red and white marrow 1 Bone marrow aspirate and core biopsy Gartner, Color Textbook of Histology, 3 rd Edition
Fluorescent in situ hybridization for chromosomal translocation Hematopoiesis Hematopoiesis: Red and white marrow 1 Bone marrow aspirate and core biopsy Gartner, Color Textbook of Histology, 3 rd Edition
Flow cytometry leukocyte differential : a critical appraisal
 Flow cytometry leukocyte differential : a critical appraisal Francis Lacombe Flow cytometry department University Hospital of Bordeaux, Pessac, France francis.lacombe@chu-bordeaux.fr 2008 HORIBA ABX, All
Flow cytometry leukocyte differential : a critical appraisal Francis Lacombe Flow cytometry department University Hospital of Bordeaux, Pessac, France francis.lacombe@chu-bordeaux.fr 2008 HORIBA ABX, All
Lymphoma Immunophenotyping: A New Era in Paraffin-Section Immunohistochemistry
 Advances in Anatomic Pathology Vol. 8, No. 4, pp. 218 239 2001 Lippincott Williams & Wilkins, Inc., Philadelphia Lymphoma Immunophenotyping: A New Era in Paraffin-Section Immunohistochemistry Eric D. Hsi
Advances in Anatomic Pathology Vol. 8, No. 4, pp. 218 239 2001 Lippincott Williams & Wilkins, Inc., Philadelphia Lymphoma Immunophenotyping: A New Era in Paraffin-Section Immunohistochemistry Eric D. Hsi
CME/SAM. Mixed Phenotype Acute Leukemia
 AJCP / Original Article Mixed Phenotype Acute Leukemia A Study of 61 Cases Using World Health Organization and European Group for the Immunological Classification of Leukaemias Criteria Olga K. Weinberg,
AJCP / Original Article Mixed Phenotype Acute Leukemia A Study of 61 Cases Using World Health Organization and European Group for the Immunological Classification of Leukaemias Criteria Olga K. Weinberg,
LEUKAEMIA and LYMPHOMA. Dr Mubarak Abdelrahman Assistant Professor Jazan University
 LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish
LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish
Hematology 101. Rachid Baz, M.D. 5/16/2014
 Hematology 101 Rachid Baz, M.D. 5/16/2014 Florida 101 Epidemiology Estimated prevalence 8,000 individuals in U.S (compare with 80,000 MM patients) Annual age adjusted incidence 3-8/million-year 1 More
Hematology 101 Rachid Baz, M.D. 5/16/2014 Florida 101 Epidemiology Estimated prevalence 8,000 individuals in U.S (compare with 80,000 MM patients) Annual age adjusted incidence 3-8/million-year 1 More
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure
 Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
2016 US Lymphoid Malignancy Statistics by World Health Organization Subtypes
 2016 US Lymphoid Malignancy Statistics by World Health Organization Subtypes Lauren R. Teras, PhD 1 ; Carol E. DeSantis, MPH 2 ; James R. Cerhan, MD, PhD 3 ; Lindsay M. Morton, PhD 4 ; Ahmedin Jemal, DVM,
2016 US Lymphoid Malignancy Statistics by World Health Organization Subtypes Lauren R. Teras, PhD 1 ; Carol E. DeSantis, MPH 2 ; James R. Cerhan, MD, PhD 3 ; Lindsay M. Morton, PhD 4 ; Ahmedin Jemal, DVM,
Pathology of Hematopoietic and Lymphoid tissue
 Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
INDEX. Numbers in italics refer to pages on which tables appear. Numbers in boldface refer to pages on which images appear.
 INDEX Numbers in italics refer to pages on which tables appear. Numbers in boldface refer to pages on which images appear. A acetic acid-zinc-formalin fixation time and implications, 4 sample results,
INDEX Numbers in italics refer to pages on which tables appear. Numbers in boldface refer to pages on which images appear. A acetic acid-zinc-formalin fixation time and implications, 4 sample results,
Heme 9 Myeloid neoplasms
 Heme 9 Myeloid neoplasms The minimum number of blasts to diagnose acute myeloid leukemia is 5% 10% 20% 50% 80% AML with the best prognosis is AML with recurrent cytogenetic abnormality AML with myelodysplasia
Heme 9 Myeloid neoplasms The minimum number of blasts to diagnose acute myeloid leukemia is 5% 10% 20% 50% 80% AML with the best prognosis is AML with recurrent cytogenetic abnormality AML with myelodysplasia
HEMATOLOGY Maintenance of Certification (MOC) Examination Blueprint
 Examination Blueprint") HEMATOLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Hematology MOC exam blueprint Based on feedback from physicians that MOC assessments should
HEMATOLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Hematology MOC exam blueprint Based on feedback from physicians that MOC assessments should
2016 WHO CLASSIFICATION OF TUMOURS OF HAEMATOPOIETIC AND LYMPHOID TISSUES, 4TH ED., VOL FCDS WEBCAST SERIES OCTOBER 19, 2017
 2016 WHO CLASSIFICATION OF TUMOURS OF HAEMATOPOIETIC AND LYMPHOID TISSUES, 4TH ED., VOL 2 2017-2018 FCDS WEBCAST SERIES OCTOBER 19, 2017 STEVEN PEACE, CTR 1 CDC & Florida DOH Attribution We acknowledge
2016 WHO CLASSIFICATION OF TUMOURS OF HAEMATOPOIETIC AND LYMPHOID TISSUES, 4TH ED., VOL 2 2017-2018 FCDS WEBCAST SERIES OCTOBER 19, 2017 STEVEN PEACE, CTR 1 CDC & Florida DOH Attribution We acknowledge
Myeloid neoplasms. Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories:
 Myeloid neoplasms Note: Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories: 1. AML : Acute myeloid leukemia(stem cell with myeloid
Myeloid neoplasms Note: Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories: 1. AML : Acute myeloid leukemia(stem cell with myeloid
AML: WHO classification, biology and prognosis. Dimitri Breems, MD, PhD Internist-Hematoloog Ziekenhuis Netwerk Antwerpen
 AML: WHO classification, biology and prognosis Dimitri Breems, MD, PhD Internist-Hematoloog Ziekenhuis Netwerk Antwerpen Acute myeloid leukemia Clonal expansion of undifferentiated myeloid precursors Impaired
AML: WHO classification, biology and prognosis Dimitri Breems, MD, PhD Internist-Hematoloog Ziekenhuis Netwerk Antwerpen Acute myeloid leukemia Clonal expansion of undifferentiated myeloid precursors Impaired