COLPOSCOPY MADE EASY AND SIMPLE
|
|
|
- Alaina Morgan
- 5 years ago
- Views:
Transcription



1 COLPOSCOPY MADE EASY AND SIMPLE Burton Brodsky M.D. Husband, father of four kids Chief of gynecology University of Toledo Assistant residency director University of Toledo Associate professor university of Toledo, director of MIS OBJECTIVES OF SCREENING Prevent morbidity and mortality of cervical cancer Prevent overzealous management of lesions that will most likely regress or disappear Risk of management also outweigh benefits Describe Describe the anatomy, cytology, histology and colposcopic findings of the normal and abnormal cervix and genital tract Describe Describe and understand the pathophysiology of lower genital and tract dysplasia including HPV and its role understand OBJECTIVES Apply Apply new standards for cervical cancer screening including HPV Recognize Recognize the diagnostic characteristics of cervical abnormalities on cytology, colposcopic and histologic exam. See See anatomic changes of the lower genital tract and recognize them and know treatment options 1

2 PRE-TEST CERVICAL SCREENING MANAGEMENT, COLPOSCOPY, PATHOLOGIC DIAGNOSIS AND TREATMENT QUESTION #1 WHICH OF THE FOLLOWING IS NOT A RISK FACTOR FOR CERVICAL CANCER? A. HIGH RISK HPV B. CIGARETTE SMOKING C. MULTIPARITY D. FAMILY HISTORY OF CERVICAL CANCER E. EARLY AGE AT FIRST SEXUAL INTERCOURSE QUESTION #2 WHICH OF THE FOLLOWING IS THE HIGHEST RISK FOR ADENOCARCINOMA OF THE CERVIX? A. HPV 18 B. HPV 31 C. HPV 16 D. HPV 33 E. HPV 22 2
3 QUESTION #3 HOW SHOULD WOMEN WITH UNSATISFACTORY CYTOLOGY TEST RESULTS BE MANAGED? A. REPEAT PAP SMEAR IN ONE YEAR B. REPEAT PAP IMMEDIATELY C. NO NEED TO REPEAT PAP D. REPEAT PAP SMEAR IN 2-4 MONTHS E. IMMEDIATE COLPOSCOPY QUESTION #4 FOR EACH OF THE FOLLOWING SCENARIOS, INDICATE THE APPROPRIATED FOLLOW UP TESTING A 38 YO WITH 2 CONSECUTIVES UNSATISFACTORY CYTOLOGY RESULTS A. REPEAT CYTOLOGY IN ONE YEAR B. REPEAT CO-TESTING IN ONE YEAR C. ROUTINE SCREENING D. COLPOSCOPY QUESTION #5 FOR EACH OF THE FOLLOWING SCENARIOS, INDICATE THE APPROPRIATED FOLLOW UP TESTING A 36 YO WITH NEGATIVE CYTOLOGY AND A POSITIVE HPV CO TEST A. REPEAT CYTOLOGY IN ONE YEAR B. REPEAT CO-TESTING IN ONE YEAR C. ROUTINE SCREENING D. COLPOSCOPY 3
4 QUESTION #6 FOR EACH OF THE FOLLOWING SCENARIOS, INDICATE THE APPROPRIATED FOLLOW UP TESTING A 24YO WITH TWO LGSIL PAPS 12 MONTHS APART AND NEGATIVE REFLEX HPV TESTING A. REPEAT CYTOLOGY IN ONE YEAR B. REPEAT CO-TESTING IN ONE YEAR C. ROUTINE SCREENING D. COLPOSCOPY QUESTION #7 FOR EACH OF THE FOLLOWING SCENARIOS, INDICATE THE APPROPRIATED FOLLOW UP TESTING A 32 YO WOMAN WITH NEGATIVE CYTOLOGY HPV POSITIVE CONTESTING, AND REFLEX GENOTYPING POSITIVE FOR HPV 16 A. REPEAT CYTOLOGY IN ONE YEAR B. REPEAT CO-TESTING IN ONE YEAR C. ROUTINE SCREENING D. COLPOSCOPY QUESTION #8 FOR EACH OF THE FOLLOWING SCENARIOS, INDICATE THE APPROPRIATED FOLLOW UP TESTING A 19YO WITH HGSIL A. REPEAT CYTOLOGY IN ONE YEAR B. REPEAT CO-TESTING IN ONE YEAR C. ROUTINE SCREENING D. COLPOSCOPY 4

5 QUESTION #9 FOR EACH OF THE FOLLOWING SCENARIOS, INDICATE THE APPROPRIATED FOLLOW UP TESTING A 24YO WITH ASCUS-US CYTOLOGY AND NEGATIVE REFLEX HPV TESTING A. REPEAT CYTOLOGY IN ONE YEAR B. REPEAT CO-TESTING IN ONE YEAR C. ROUTINE SCREENING D. COLPOSCOPY QUESTION #10 FOR EACH OF THE FOLLOWING SCENARIOS, INDICATE THE APPROPRIATED FOLLOW UP MANAGEMENT A 62 YO WITH AGC CYTOLOGY A. COLPOSCOPY B. COLPOSCOPY + EMB C. REFLEX HPV TESTING D. REPEAT CYTOLOGY IN 1 YEAR QUESTION A 54-YEAR-OLD MULTIPAROUS WOMAN WAS REFERRED FOR COLPOSCOPY BECAUSE OF AN ABNORMAL CERVICAL CYTOLOGIC SMEAR. THE CERVIX APPEARED GROSSLY NORMAL. AFTER APPLICATION OF 3% ACETIC ACID, COLPOSCOPICALLY-DIRECTED BIOPSY WAS TAKEN OF AN AREA OF ACETOWHITE EPITHELIUM WITH MOSAICISM AND PUNCTATION. THE BIOPSY SPECIMEN MEASURED 2.8 MM FROM THE EPITHELIAL SURFACE TO THE DEEP MARGIN. (PLEASE SEE ILLUSTRATION). WHICH OF THE FOLLOWING IS THE MOST LIKELY DIAGNOSIS? A. CHRONIC CERVICITIS B. LOW-GRADE SQUAMOUS INTRAEPITHELIAL LESION (LSIL) C. HIGH-GRADE SQUAMOUS INTRAEPITHELIAL LESION (HSIL) D. INVASIVE CERVICAL CANCER 5

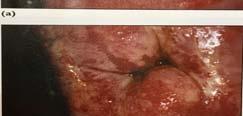
6 QUESTION WHICH HUMAN PAPILLOMA VIRUS (HPV) SUBTYPE IS MOST COMMONLY ASSOCIATED WITH THIS LESION? A. 6 B. 11 C. 16 D. 33 QUESTIONS WHAT IS THE MOST APPROPRIATE NEXT STEP IN MANAGEMENT OF THIS PATIENT? A. REPEAT CERVICAL CYTOLOGY IN 4 MONTHS B. HPV DNA TESTING FOR HIGH-RISK SUBTYPES C. CERVICAL CONIZATION D. RADICAL HYSTERECTOMY WITH PELVIC AND PARAAORTIC LYMPHADENECTOMY QUESTION #14 A 63-YEAR-OLD WOMAN, G 5 P 4014 REQUESTS EVALUATION BECAUSE OF A CHRONIC HISTORY OF VULVAR AND PERINEAL PRURITUS AND PAIN. SHE HAS BEEN TREATED WITH SHORT COURSES OF MEDICATION FOR RECURRENT YEAST INFECTIONS, WHICH HAS RESULTED IN PARTIAL RELIEF OF HER SYMPTOMS. THE PHOTOGRAPH ILLUSTRATES THE PRESENT APPEARANCE OF HER VULVA. WHICH OF THE FOLLOWING IS THE MOST APPROPRIATE NEXT STEP IN MANAGEMENT OF THIS PATIENT? A. COLPOSCOPY B. LONG-TERM ANTIFUNGAL MEDICATION C. HIGH POTENCY TOPICAL STEROIDS D. MULTIPLE PUNCH BIOPSIES E. WIDE LOCAL EXCISION 6

7 QUESTIONS #15-17 A 45 YEAR OLD WOMAN, P3003 PRESENTED WITH A "FLESHY BULGE" PROTRUDING FROM HER VAGINA. SHE ALSO REPORTED OCCASIONAL INTERMENSTRUAL AND POSTCOITAL SPOTTING. OTHERWISE, SHE HAD REGULAR MENSES AND NO HISTORY OF ABNORMAL PAP SMEARS. HER LAST PAP SMEAR WAS 13 MONTHS AGO, AND HER URINE PREGNANCY TEST WAS NEGATIVE. ON SPECULUM EXAMINATION, A SMOOTH, SOFT, ERYTHEMATOUS 8 CM X 1 CM LESION (SEE FIGURE 1) PROTRUDED FROM THE CERVICAL OS AND EXTENDED TO THE INTROITUS. THE REST OF THE VAGINA AND CERVIX APPEARED NORMAL. THE EXTERNAL OS WAS DILATED APPROXIMATELY 1 CM, AND THE BASE OF THE STALK OF THE LESION WAS PALPATED APPROXIMATELY 2 CM DISTAL TO THE CERVICAL OS. ON BIMANUAL EXAMINATION, HER UTERUS, CERVIX, AND ADNEXAE WERE NONTENDER. QUESTIONS #15-17 WHICH ONE OF THE FOLLOWING LESIONS IS THE LEAST LIKELY DIAGNOSIS? A. RETAINED PRODUCTS OF CONCEPTION B. ENDOCERVICAL POLYP C. ENDOMETRIAL POLYP D. PROLAPSING MYOMA E. CERVICAL CANCER 7
8 QUESTONS WHICH OF THE FOLLOWING SHOULD NOT BE PART OF THE INITIAL MANAGEMENT OF THIS PATIENT? A. PAP SMEAR B. COLPOSCOPY C. AVULSION OF THE POLYP WITH A FORCEPS AND HISTOLOGIC EVALUATION D. ENDOMETRIAL BIOPSY QUESTIONS WHAT IS THE APPROXIMATE PROBABILITY THAT THIS LESION IS MALIGNANT? A. 25% B. 14% C. 5% D. 0.5% QUESTIONS #18-21 A 40-YEAR-OLD WOMAN PRESENTS TO YOUR OFFICE WITH A COMPLAINT OF POSTCOITAL SPOTTING. HER EXTERNAL GENITALIA AND VAGINAL AND CERVICAL MUCOSA APPEAR GROSSLY NORMAL ON EXAMINATION. BIMANUAL EXAMINATION DEMONSTRATES A NON-TENDER, AXIAL, FREELY MOBILE UTERUS, APPROXIMATELY 10 WEEKS SIZE, AND NO ADNEXAL MASSES OR TENDERNESS. THE PAP SMEAR AND CULTURES THAT YOU PERFORM ARE NEGATIVE. THE PATIENT CONTINUES TO COMPLAIN OF POSTCOITAL SPOTTING, AND YOU PERFORM A HYSTEROSCOPY. THE KEY INTRAOPERATIVE FINDING IS SHOWN IN THE PHOTOGRAPH. 8

9 QUESTIONS QUESTIONS # THIS TYPE OF UTERINE LESION IS MOST COMMON IN WHAT AGE GROUP? A. 10 TO 19 YEARS OLD B. 20 TO 29 YEARS OLD C. 40 TO 49 YEARS OLD D. OVER 60 YEARS OLD QUESTIONS # FROM WHAT AREA OF THE UTERUS ARE THESE LESIONS MOST LIKELY TO ARISE? A. FUNDUS B. CORPUS C. CERVIX 9
10 QUESTIONS WHICH MEDICATION IS MOST LIKELY TO BE ASSOCIATED WITH THIS LESION? A. ORAL CONTRACEPTIVES B. DEPOT-LUPRON C. TAMOXIFEN D. MEDROXYPROGESTERONE ACETATE QUESTIONS # IF MALIGNANT CHANGE OCCURS WITHIN THIS LESION, IT IS USUALLY ASSOCIATED WITH WHAT STAGE/GRADE OF ENDOMETRIAL CANCER? A. IA B. IC C. II D. IV QUESTIONS # A 58-YEAR-OLD WOMAN, G 3 P 2103, REQUESTED EVALUATION BECAUSE OF POSTMENOPAUSAL BLEEDING. HER PHYSICAL EXAMINATION WAS NORMAL. HER PAP SMEAR IS SHOWN IN FIGURE 1. HER ENDOMETRIAL BIOPSY IS SHOWN IN FIGURE 2 10

11 QUESTIONS #22-24 WHAT TYPE OF CELLS ARE SEEN IN THE PAP SMEAR? A. MALIGNANT SQUAMOUS CELLS B. MALIGNANT ENDOMETRIAL CELLS C. DYSPLASTIC SQUAMOUS CELLS D. NORMAL ENDOCERVICAL CELLS QUESTIONS WHAT FINDING IS ILLUSTRATED ON THE ENDOMETRIAL BIOPSY? A. ENDOMETRIAL CARCINOMA B. CLEAR CELL CARCINOMA C. PAPILLARY SEROUS CARCINOMA D. ADENOSQUAMOUS CARCINOMA QUESTIONS # WHICH OF THE FOLLOWING IS THE MOST APPROPRIATE TREATMENT FOR THIS PATIENT? A. TAH, BSO, OMENTECTOMY B. TAH, BSO, PELVIC LYMPHADENECTOMY C. TAH, BSO, PELVIC AND AORTIC LYMPHADENECTOMY D. TAH, BSO, OMENTAL BIOPSY, PELVIC AND AORTIC LYMPHADENECTOMY 11

12 CERVICAL CANCER FACTS Cervical cancer is the most common gyn cancer in women worldwide, Most of these cancers stem from HPV infections 99.7% HPV 16 most common and most oncogenic for squamous and HPV 18 for adenocarcinoma Genital HPV is the most common STD in the united states Most sexually active adults will have it at some point in their lives Of women with cervical cancer 60% have never been screened or have not had a pap smear in over 5 years Cervical cancer incidence has decreased more than 50% over past 30 years and mortality has decreased about the same CERVICAL CANCER FACTS Most cases of cervical cancer occur in women who were either never screened or screened inadequately Over 50% cervical cancers never had cytology and another 10% had not been screened within 5 years before diagnosis In the u.s. approx. 12,000 cervical cancers a year and around 4100 deaths In the countries with no screening programs 525,00 cases and 265,000 deaths 12
13 CERVICAL RISK FACTORS HPV Smoking HIV Immunocompromised Chlamydia Obesity Multiparity Early age of first pregnancy less than 17yo DES High risk sexual activity Divided into 2 portions, lower portio or vaginal cervix extends into the vagina. The upper or supracervical cervix extends from the vaginal attachment to the lower uterine segment. THE CERVIX Cervix is 3cm in length and 2cm in diameter in nulliparous patients Cervix is supported by uterosacral and cardinal ligaments Cervix is perfused by the descending cervico-vaginal branches of the uterine art. Innvervation from paracervical and uterosacral plexes (Frankenhausers) and S2-4. There is a relative lack of ectocervical innervation which may account for the minimal discomfort associated with cryotherapy or ectocervical biopsy than that from ECC or LEEP THE CERVIX HISTOLOGY MAJORITY OF THE CERVIX IS COVERED BY STRATIFIED SQUAMOUS EPITHELIUM. CERVIX IS DIVIDED INTO 4 DISTINCT LAYERS A SINGLE LAYER OF TALL COLUMNAR CELLS LINES THE ENDOCERVICAL CANAL. OFTEN REFERRED TO AS GLANDULAR CELLS ENDOCERVICAL CELLS PROTRUDE INTO THE CERVICAL STROMA TO A DEPTH OF 5-8MM THE AREA WHERE THE STRATIFIED SQUAMOUS AND COLUMNAR CELLS MEET IS KNOWN AS THE SQUAMOCOLUMNAR JUNCTION (SCJ) 13



14 14


15 NATURAL HISTORY OF CIN Infection of HPV is a necessary factor for the development of cervical neoplasia Only a small fraction of women infected with HPV will develop HGSIL and cancer, HPV is either transient or persistent Most HPV infection is transient and poses little risk of infection Few infections persist but persistence at 1 year and 2 years strongly predicts subsequent risk of HGSIL regardless of age NATURAL HISTORY OF CIN WHAT HPV INFECTIONS PERSIST Hpv genotype appears to be the most important determinant of persistence and infection HPV 16 has the highest carcinogenic potential accounting for 55-60% of all cervical cancer cases worldwide, HPV 18 is next responsible for 10-15% ca. Hpv 18 is most commonly associated with adenocarcinoma of the cervix. Other risk factors that increase likelihood of persistence include: Cigarette smoking Immunocompromised HIV 15

16 Hpv is most common in teenagers and women in their early 20 s, in some studies approx. 60% young women had hpv infection over 3 year period HPV PROGRESSION AND PERSISTENCE HPV infection decreases with age, lifetime risk of infection is at least 80% Most young patients can clear the infection in an average of 8 months hence most cervical neoplasia will also spontaneously resolve in this population HPV TESTING High risk oncogenic testing no need for low risk testing Only used FDA approved testing for HPV NATURAL HISTORY OF CIN LESIONS Regression % Persistence % Progression to cis % Progression to invasion % CIN CIN CIN 3 32 <56 - >12 16
17 CERVICAL CANCER INCIDENCE BY AGE Age Rate per 100, All ages 9.4 CERVICAL CYTOLOGY SCREENING TECHNIQUES Liquid base and conventional methods of cervical cytology collection are acceptable Blood, discharge, and some lubricants may interfere with interpretation Overall 0.4% tests had obscuring material that caused misinterpretation Exfoliated cells are collected from the TZ of the cervix and transferred to vial of liquid A small amount of water based lubricant on the speculum does not decrease the quality of cervical cytology testing Liquid based specimens has the advantage of allowing a single specimen for cytology, HPV, and testing for STI s. COLPOSCOPY Gold standard to evaluate abnormal cervical cytology Lower sensitivity 50-80%, interobserver agreement, and reproducibility are less than we think. Use acetic acid or lugols solution to accentuate areas of dysplasia Directed biopsies as needed and ECC 17
18 PREPARATION FOR COLPOSCOPY Best to do during days 8-12 of menses but can be done anytime Avoid intravaginal products, medications, douching, or sexual intercourse for 24 hours prior to exam Informed consent Pregnancy testing Remove blood and mucous COLPOSCOPY 3 components of the colposcopic examination Cervical visualization SCJ visibility TZ classification PERFORMING THE COLPOSCOPIC EXAM Clear visualization of the cervix Wipe off blood and mucous Apply acetic acid 3-5% Wait at least 1-2 minutes a common mistake Increase magnification Use vascular lights as needed 18
19 PERFORMING THE COLPOSCOPIC EXAM Document what you did, pictures taken or drawn Helps immensely for future colposcopic exams if needed CLINICAL CONSIDERATIONS DIRECTING COLPOSCOPY Clinical objectives Provide a magnified view of LGT Identify cervical squamocolumnar junction Detect lesions suspicious for neoplasia Direct lesion biopsy Monitor patients with current or past LGT neoplasias Contraindications none Relative contraindications upper or lower tract infection uncontrolled severe HTN Clinical indications Grossly visible LGT lesions Abnormal cervical cytology screening DES exposure uncooperative or anxious pt Acetowhite changes Mosaic pattern Punctation COLPOSCOPY WHAT ARE WE LOOKING FOR Leukoplakia Distance between the capillaries and intensity of color Sharpness of the borders The surface pattern irregular or regular Angles of the vessels Full visualization of TZ and cervix 19


20 REID COLPOSCOPIC INDEX Colposcopic sign Zero points 1 point 2 points margin Condymomatous Micropapillary Feathery Satellite lesions Smooth Straight Rolled Peeling Internal border acetowhitening vessels Shiny Snowy Translucent Fine patterns Uniform caliber and patterns Duller white absent Dull white Gray Iodine staining positive partial negative Coarse patterns Dilated with variable caliber and intercapillary distances 20




21 21





22 Sample Footer Text 11/29/



23 23


24 Colposcopy is inadequate or colposcopy is adequate but no lesion is identified RECOMMENDATIONS FOR ECC ACOG BULLETIN 2013 Initial evaluation of ASC-H, HSIL, AGC, or AIS cytology results Surveillance 4 to 6 months after excisional therapy if specific margins are positive for hsil Surveillance after conization for AIS has been perfomed in women wishing fertility preservation 24
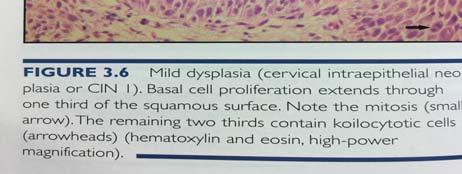
25 In women with ASC-us or LGSIL cervical cytology, ECC is preferred when no lesion is identified on colpo, or colpo is unsatisfactory, or in women with previous excision or ablation of TZ When a lesion is identified in the TZ ECC is also acceptable ENDOCERVICAL SAMPLING ASCCP In women with ASCUS cannot exclude HGSIL AGUS AIS HISTOLOGY OF THE CERVIX CIN 1 Koilocyte formation Basal cell proliferation extends through 1/3 squamous surface CIN 2 Basal cell proliferation extends through ½ of the surface epithelium Mitoses are present at the epithelial surface CIN 3 CIS PROLIFERATION OF IMMATURE DYSPLASTIC CELLS THROUGHOUT THE SQUAMOUS EPITHELIUM FROM BASE TO SURFACE BASEMENT MEMBRANE REMAINS INTACT HISTOLOGY OF THE CERVIX INVASIVE CANCER IRREGULAR BORDERS, SMALL MALIGNANT NESTS, IF LESS THAN 5X7MM ( DEPTH AND HORIZONTAL SPREAD) THEN MICROINVASION CYTOPLASM IS EOSINOPHILIC AND CONTAINS KERATIN SOMETIMES 25




26 26

27 KEY POINTS CERVICAL INTRAEPITHELIAL NEOPLASIA 1 (CIN 1) HAVE LITTLE PREMALIGNANT POTENTIAL MANIFESTATION OF ACUTE HPV INFECTION HIGH RATE OF REGRESSION KEY POINTS Generally, LSIL cytology is associated with transient HPV infection such as CIN I But up to 28% of LSIL have CIN 2 or 3 identified on colpo Bottom line: Transient = GOOD Persistent = BAD High-grade squamous intraepithelial lesion (HSIL) is associated with persistent and transforming infection and cancer risk 27


28 KEY POINTS CIN 2 SEEM TO REPRESENT A MIX OF LOW GRADE AND HIGH GRADE LESIONS NOT AN INTERMEDIATE GRADE LESION CONSIDERED A CANCER PRECURSOR KEY POINTS CIN 3 AND ADENOCARCINOMA IN SITU CLEAR CANCER PRECURSORS ALTHOUGH PROGRESSION FROM PERSISTENT INFECTION TO CANCER IS SLOW TIME FROM CIN 3 TO INVASIVE CANCER AVERAGES 8.1 TO 12.6 YRS 28




29 29

30 Colposcopy and ECC is recommended regardless of hpv status AGUS Endometrial sampling is recommended in pts greater than 35yo or less than 35 if clinical conditions exist bleeding or anovulation If NO CIN 2 is identified co testing at 12 months and 24 months is recommended, then continue with repeat co testing in 3 years AGUS 9-38% of women with agus have cin % have invasive cancer 30
31 AGUS (FAVOR NEOPLASIA) OR AIS If invasive disease is not identified during initial colposcopic work up, a diagnostic excisional procedure is recommended Ecc sampling after excision is preferred Type of diagnostic excisional procedure used provides specimen with interpretable margins Difficult to identify on colposcopy EMB AND ECC CONSIDER COLPOSCOPY AND IF NO ENDOMETRIAL ABNORMALITY IS IDENTIFIED THEN PROCEED WITH COLPOSCOPY ATYPICAL ENDOMETRIAL CELLS No further evaluation in premenopausal women ENDOMETRIAL CELLS ON PAP For menopausal women endometrial assessment is recommended regardless of symptoms Endometrial adenocarcinoma in 5% of postmenopausal women 31

32 SCREENING FOR AGES Cytology alone every 3 years HPV testing not used as part of screen RATIONAL FOR LONGER SCREENING INTERVALS Sensitivity of single pap 50-70% Cancer risk 18mo after 3 neg paps: 1.5/100,000 Cancer risk 36mo after 3 neg paps: 4.7/100,000 Risk of HSIL/cancer <3 yrs after negative pap not significantly higher than risk after 1 year Screening can be harmful: lifetime risk of colpo Screening q3yrs: 760 colpo/1000 women Screening annually: 2000 colpo/1000 women 99,997 women screened unnecessarily to help 3 WHY AVOID HPV TESTING AGES 21-29? Prevalence of carcinogenic HPV approaches 20% in teens and early 20s Most carcinogenic HPV infections resolve without intervention Can lead to repeated call backs, anxiety, and interventions WITHOUT benefit 32




33 SCREENING FOR AGES Cytology + HPV testing (cotesting) every 5 years is PREFERRED Cytology alone every 3 years is acceptable Increased detection of CIN 3 RATIONALE FOR COTESTING Decreased CIN3 in subsequent screening Achieves risk of detecting CIN3 equal to cytology alone at 1-3 yr intervals Enhances detection of AIS/Adenocarcinoma Minimizes increased number of colposcopies WHY NOT ANNUAL COTESTING? High NPV of one cotest means most abnormal screens at 1-3 year intervals are TRANSIENT HPV infection and not precancer Potential harms are amplified (invasive management) that has not benefit to the patient 33
34 WHEN TO STOP SCREENING Stop at age 65 for those with adequate negative prior screening Definition of adequate negative screening Stop after hysterectomy with removal of cervix and no history of CIN2+ NO CIN2+ within last 20 years 3 consecutive negative Paps or Evidence of adequate negative prior screen is not required 2 consecutive negative HPV tests STOP SCREENING AT AGE 65 SCREENING SHOULD NOT RESUME FOR ANY REASON, EVEN IF A WOMAN REPORTS HAVING A NEW PARTNER RATIONALE FOR STOPPING AT AGE 65 CIN2+ IS RARE AFTER AGE 65 MOST ABNORMAL SCREENS, EVEN HPV+ ARE FALSE POSITIVES AND DO NOT REFLECT PRECANCER HPV RISK REMAINS 5-10% COLPOSCOPY/BIOPSY/TREATMENT ARE MORE DIFFICULT THUS HARMS ARE MAGNIFIED INCIDENTAL HPV INFECTION UNLIKELY LEAD TO CANCER WITHIN REMAINING LIFETIME 34
35 HISTORY OF CIN 2, CIN 3 OR AIS CONTINUE ROUTINE SCREENING FOR AT LEAST 20 YEARS SINCE THE DIAGNOSIS EVEN IF THIS EXTENDS SCREENING PAST THE AGE OF 65 Vaginal cancer rate is 7/million/year 663 vag cuff paps needed to find 1 VAIN RATIONALE FOR STOPPING AFTER HYST 2066 women followed after hyst for average of 89 months 3% had VAIN, 0 had cancer Risk of Pap abnormality after hyst is 1% Compare this risk to risk of breast cancer in men (we do not screen men with MMG) HPV VACCINE Does NOT change screening Reduces CIN3+ by 17-33% Reduces colposcopy by 10% Reduces treatment by 25-30% 35
36 3 FDA approved vaccines now a 9- valent vaccine with more to come, covers 20% more high risk Hpv infections HPV VACCINE Ages 9-26? Now later ages If you have been vaccinated with bivalent or quadvalent you do NOT need re-vaccination HPV AS A PRIMARY SCREENING TEST IT MAY REPLACE COTESTING IN THE FUTURE HIGH NPV BUT SPECIFICITY IS LACKING UNCLEAR FOLLOWUP TO HPV+ TEST HPV STATUS BIASES CYTOLOGY REPORTS TO ABNORMAL AT THIS TIME, IN MOST CLINICAL SETTINGS, WOMEN SHOULD NOT BE SCREENED WITH HPV TESTING ALONE SPECIAL POPULATIONS HIV + screen twice in the first year after dx Then annually Initiate year of diagnosis even if younger than 21 (ACOG rec) Immunocompromised (e.g. transplant pts) No major committee recs Reasonable to start screen at 21 ya then annually 36




37 SPECIAL POPULATIONS Women who were exposed to des in-utero Women previously treated for CIN 2, cin 3 or cancer 37

38 38


39 39
40 40

41 41
PRE TEST CERVICAL SCREENING MANAGEMENT COLPOSCOPY PATHOLOGIC DIAGNOSIS AND TREATMENT
 PRE TEST CERVICAL SCREENING MANAGEMENT COLPOSCOPY PATHOLOGIC DIAGNOSIS AND TREATMENT QUESTION #1 WHICH OF THE FOLLOWING IS NOT A RISK FACTOR FOR CERVICAL CANCER? A. HIGH RISK HPV B. CIGARETTE SMOKING C.
PRE TEST CERVICAL SCREENING MANAGEMENT COLPOSCOPY PATHOLOGIC DIAGNOSIS AND TREATMENT QUESTION #1 WHICH OF THE FOLLOWING IS NOT A RISK FACTOR FOR CERVICAL CANCER? A. HIGH RISK HPV B. CIGARETTE SMOKING C.
Making Sense of Cervical Cancer Screening
 Making Sense of Cervical Cancer Screening New Guidelines published November 2012 Tammie Koehler DO, FACOG The incidence of cervical cancer in the US has decreased more than 50% in the past 30 years because
Making Sense of Cervical Cancer Screening New Guidelines published November 2012 Tammie Koehler DO, FACOG The incidence of cervical cancer in the US has decreased more than 50% in the past 30 years because
Appropriate Use of Cytology and HPV Testing in the New Cervical Cancer Screening Guidelines
 Appropriate Use of Cytology and HPV Testing in the New Cervical Cancer Screening Guidelines Tim Kremer, MD Ralph Anderson, MD 1 Objectives Describe the natural history of HPV particularly as it relates
Appropriate Use of Cytology and HPV Testing in the New Cervical Cancer Screening Guidelines Tim Kremer, MD Ralph Anderson, MD 1 Objectives Describe the natural history of HPV particularly as it relates
HPV and Cervical Cancer, Screening and Prevention. John Ragsdale, MD July 12, 2018 CME Lecture Series
 HPV and Cervical Cancer, Screening and Prevention John Ragsdale, MD July 12, 2018 CME Lecture Series We have come a long Way Prevalence HPV in Young Adults in U.S HPV genotypes 55-60% of All cancers 20%
HPV and Cervical Cancer, Screening and Prevention John Ragsdale, MD July 12, 2018 CME Lecture Series We have come a long Way Prevalence HPV in Young Adults in U.S HPV genotypes 55-60% of All cancers 20%
Cervical Dysplasia and HPV
 Cervical Dysplasia and HPV J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse HPV Double stranded DNA virus The HPV infect epithelial cells of the skin and mucous membranes Highest risk
Cervical Dysplasia and HPV J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse HPV Double stranded DNA virus The HPV infect epithelial cells of the skin and mucous membranes Highest risk
Samuel B. Wolf, D.O., F.A.C.O.G. Emerald Coast Obstetrics and Gynecology Panama City Florida
 Making sense of the new Pap smear screening guidelines. Samuel B. Wolf, D.O., F.A.C.O.G. Emerald Coast Obstetrics and Gynecology Panama City Florida Case 17 year old G1P0010 with first sexual encounter
Making sense of the new Pap smear screening guidelines. Samuel B. Wolf, D.O., F.A.C.O.G. Emerald Coast Obstetrics and Gynecology Panama City Florida Case 17 year old G1P0010 with first sexual encounter
Faculty Pap Smear Guidelines: Family Planning Update 2008 Part Two
 Faculty Pap Smear Guidelines: Family Planning Update 2008 Part Two Seshu P. Sarma, MD, FAAP Emory University Regional Training Center Atlanta, Georgia Produced by the Alabama Department of Public Health
Faculty Pap Smear Guidelines: Family Planning Update 2008 Part Two Seshu P. Sarma, MD, FAAP Emory University Regional Training Center Atlanta, Georgia Produced by the Alabama Department of Public Health
Becoming a colposcopist: Colposcope case studies
 Becoming a colposcopist: Colposcope case studies Seon-Kyung Lee, M.D. Department of Obstetrics and Gynecology College of Medicine, Kyung Hee University Value of Colposcopy Cytology is an effective screening
Becoming a colposcopist: Colposcope case studies Seon-Kyung Lee, M.D. Department of Obstetrics and Gynecology College of Medicine, Kyung Hee University Value of Colposcopy Cytology is an effective screening
I have no financial interests in any product I will discuss today.
 Cervical Cancer Screening Update and Implications for Annual Exams George F. Sawaya, MD Professor Department of Obstetrics, Gynecology and Reproductive Sciences Department of Epidemiology and Biostatistics
Cervical Cancer Screening Update and Implications for Annual Exams George F. Sawaya, MD Professor Department of Obstetrics, Gynecology and Reproductive Sciences Department of Epidemiology and Biostatistics
Management Algorithms for Abnormal Cervical Cytology and Colposcopy
 Management Algorithms for Abnormal Cervical Cytology and Colposcopy Table of Contents Standard Colposcopic Definitions... 1 Guidelines for the Assessment of Abnormal Cervical Cytology... 2 Ia: Persistent
Management Algorithms for Abnormal Cervical Cytology and Colposcopy Table of Contents Standard Colposcopic Definitions... 1 Guidelines for the Assessment of Abnormal Cervical Cytology... 2 Ia: Persistent
ASCCP 2013 Guidelines for Managing Abnormal Cervical Cancer Screening Tests
 ASCCP 2013 Guidelines for Managing Abnormal Cervical Cancer Screening Tests www.treatmentok.com Barbara S. Apgar, MD, MS Professor of Family Medicine University of Michigan Ann Arbor, Michigan Disclosures
ASCCP 2013 Guidelines for Managing Abnormal Cervical Cancer Screening Tests www.treatmentok.com Barbara S. Apgar, MD, MS Professor of Family Medicine University of Michigan Ann Arbor, Michigan Disclosures
Cervical Cancer 4/27/2016
 Guidelines for Cervical Cancer Screening and Prevention Management of Abnormal Results Kathy A. King, MD Assistant Professor of OB/GYN Medical College of Wisconsin May 6, 2016 Cervical Cancer In US about
Guidelines for Cervical Cancer Screening and Prevention Management of Abnormal Results Kathy A. King, MD Assistant Professor of OB/GYN Medical College of Wisconsin May 6, 2016 Cervical Cancer In US about
Lauren O Sullivan, D.O. February 19, 2015
 Lauren O Sullivan, D.O. February 19, 2015 1. Review basics of Pap smear, cervical dysplasia/cancer and HPV infection. 2. Review 2012 updated screening guidelines. 3. Discuss how and where to find updated
Lauren O Sullivan, D.O. February 19, 2015 1. Review basics of Pap smear, cervical dysplasia/cancer and HPV infection. 2. Review 2012 updated screening guidelines. 3. Discuss how and where to find updated
Cervical Cancer Screening Update. Melissa Hartman, DO Women s Health
 Cervical Cancer Screening Update Melissa Hartman, DO Women s Health Previous Cervical Cancer Screening Organization Recommendation ACS (2011) ACP (2008) NCI (2003) Age 21 or 3 years after first intercourse
Cervical Cancer Screening Update Melissa Hartman, DO Women s Health Previous Cervical Cancer Screening Organization Recommendation ACS (2011) ACP (2008) NCI (2003) Age 21 or 3 years after first intercourse
Human Papillomavirus (HPV) and Cervical Cancer Prevention
 and Cervical Cancer Prevention") Human Papillomavirus (HPV) and Cervical Cancer Prevention MOA Autumn Convention November 3, 2017 David J Boes, DO, FACOOG (Dist.) Associate Professor, MSU-COM 1 Disclosures None relative to this presentation
Human Papillomavirus (HPV) and Cervical Cancer Prevention MOA Autumn Convention November 3, 2017 David J Boes, DO, FACOOG (Dist.) Associate Professor, MSU-COM 1 Disclosures None relative to this presentation
Clinical Guidance: Recommended Best Practices for Delivery of Colposcopy Services in Ontario Best Practice Pathway Summary
 Clinical Guidance: Recommended Best Practices for Delivery of Colposcopy Services in Ontario Best Practice Pathway Summary Glossary of Terms Colposcopy is the examination of the cervix, vagina and, in
Clinical Guidance: Recommended Best Practices for Delivery of Colposcopy Services in Ontario Best Practice Pathway Summary Glossary of Terms Colposcopy is the examination of the cervix, vagina and, in
The society for lower genital tract disorders since 1964.
 The society for lower genital tract disorders since 1964. Updated Consensus Guidelines for Managing Abnormal Cervical Cancer Screening Tests and Cancer Precursors American Society for and Cervical Pathology
The society for lower genital tract disorders since 1964. Updated Consensus Guidelines for Managing Abnormal Cervical Cancer Screening Tests and Cancer Precursors American Society for and Cervical Pathology
Introduction to Colposcopy
 Introduction to Colposcopy Papanicolaou smear (Pap smear) screening test Colposcopy diagnostic test Introduction to Colposcopy Acetic acid and Lugol s iodine applied Cervix examined under magnification
Introduction to Colposcopy Papanicolaou smear (Pap smear) screening test Colposcopy diagnostic test Introduction to Colposcopy Acetic acid and Lugol s iodine applied Cervix examined under magnification
!"#$%&'(#)*$+&,$-&.#,$/#0()1-$ ),1')$2(%&,2#,%$%(0'#$34567$
*$+&,$-&.#,$/#0()1-$ ),1')$2(%&,2#,%$%(0'#$34567$") !"#$%&'(#)*$+&,$-&.#,$/#0()1-$ ),1')$2(%&,2#,%$%(0'#$34567$ Updated Consensus Guidelines for Managing Abnormal Cervical Cancer Screening Tests and Cancer Precursors American Society for and Cervical Pathology
!"#$%&'(#)*$+&,$-&.#,$/#0()1-$ ),1')$2(%&,2#,%$%(0'#$34567$ Updated Consensus Guidelines for Managing Abnormal Cervical Cancer Screening Tests and Cancer Precursors American Society for and Cervical Pathology
Eradicating Mortality from Cervical Cancer
 Eradicating Mortality from Cervical Cancer Michelle Berlin, MD, MPH Vice Chair, Obstetrics & Gynecology Associate Director, Center for Women s Health June 2, 2009 Overview Prevention Human Papilloma Virus
Eradicating Mortality from Cervical Cancer Michelle Berlin, MD, MPH Vice Chair, Obstetrics & Gynecology Associate Director, Center for Women s Health June 2, 2009 Overview Prevention Human Papilloma Virus
Objectives. I have no financial interests in any product I will discuss today. Cervical Cancer Screening Guidelines: Updates and Controversies
 Cervical Cancer Screening Guidelines: Updates and Controversies I have no financial interests in any product I will discuss today. Jody Steinauer, MD, MAS University of California, San Francisco Objectives
Cervical Cancer Screening Guidelines: Updates and Controversies I have no financial interests in any product I will discuss today. Jody Steinauer, MD, MAS University of California, San Francisco Objectives
Cervical Cancer Screening for the Primary Care Physician for Average Risk Individuals Clinical Practice Guidelines. June 2013
 Cervical Cancer Screening for the Primary Care Physician for Average Risk Individuals Clinical Practice Guidelines General Principles: Since its introduction in 1943, Papanicolaou (Pap) smear is widely
Cervical Cancer Screening for the Primary Care Physician for Average Risk Individuals Clinical Practice Guidelines General Principles: Since its introduction in 1943, Papanicolaou (Pap) smear is widely
I have no financial interests in any product I will discuss today.
 Cervical Cancer Screening Update and Implications for Annual Exams George F. Sawaya, MD Professor Department of Obstetrics, Gynecology and Reproductive Sciences Department of Epidemiology and Biostatistics
Cervical Cancer Screening Update and Implications for Annual Exams George F. Sawaya, MD Professor Department of Obstetrics, Gynecology and Reproductive Sciences Department of Epidemiology and Biostatistics
Cervical Cancer Screening
 Cervical Cancer Screening MEGAN CHENEY, MD MPH MEDICAL DIRECTOR, THE WOMEN S CENTER ASSISTANT DIRECTOR, BGSMC OBGYN RESIDENCY PROGRAM SECTION CHIEF, THE WOMEN S HEALTH INSTITUTE Objectives Understand proper
Cervical Cancer Screening MEGAN CHENEY, MD MPH MEDICAL DIRECTOR, THE WOMEN S CENTER ASSISTANT DIRECTOR, BGSMC OBGYN RESIDENCY PROGRAM SECTION CHIEF, THE WOMEN S HEALTH INSTITUTE Objectives Understand proper
I have no financial interests to disclose.
 Workshop: Case Management of Abnormal Pap Smears and Colposcopies Rebecca Jackson, MD Professor Obstetrics, Gynecology & Reproductive Sciences and Epidemiology & Biostatistics I have no financial interests
Workshop: Case Management of Abnormal Pap Smears and Colposcopies Rebecca Jackson, MD Professor Obstetrics, Gynecology & Reproductive Sciences and Epidemiology & Biostatistics I have no financial interests
I have no financial interests in any product I will discuss today.
 Cervical Cancer Prevention: 2012 and Beyond George F. Sawaya, MD Professor Department of Obstetrics, Gynecology and Reproductive Sciences Department of Epidemiology and Biostatistics University of California,
Cervical Cancer Prevention: 2012 and Beyond George F. Sawaya, MD Professor Department of Obstetrics, Gynecology and Reproductive Sciences Department of Epidemiology and Biostatistics University of California,
Dysplasia: layer of the cervical CIN. Intraepithelial Neoplasia. p16 immunostaining. 1, Cervical. Higher-risk, requires CIN.
 CLINICAL PRACTICE GUIDELINE Guideline Number: DHMP_DHMC_PG1015 Guideline Subject: Routine Cervical Cancer Screening Effective Date: 9/2018 Revision Date: 9/2019 Pages: 2 of 2 Quality Management Committee
CLINICAL PRACTICE GUIDELINE Guideline Number: DHMP_DHMC_PG1015 Guideline Subject: Routine Cervical Cancer Screening Effective Date: 9/2018 Revision Date: 9/2019 Pages: 2 of 2 Quality Management Committee
No Disclosures. Updated Guidelines for Cervical Cancer Screening and Prevention Management of Abnormal Results. Objectives 5/9/2016
 Updated Guidelines for Cervical Cancer Screening and Prevention Management of Abnormal Results Kathy A. King, MD Assistant Professor of OB/GYN Medical Director, PPWI Medical College of Wisconsin May 6,
Updated Guidelines for Cervical Cancer Screening and Prevention Management of Abnormal Results Kathy A. King, MD Assistant Professor of OB/GYN Medical Director, PPWI Medical College of Wisconsin May 6,
Cervical Screening for Dysplasia and Cancer in Patients with HIV
 Cervical Screening for Dysplasia and Cancer in Patients with HIV Adult Clinical Guideline from the New York State Department of Health AIDS Institute w w w.hivg uidelines.org Purpose of the Guideline Increase
Cervical Screening for Dysplasia and Cancer in Patients with HIV Adult Clinical Guideline from the New York State Department of Health AIDS Institute w w w.hivg uidelines.org Purpose of the Guideline Increase
CERVICAL INTRAEPITHELIAL NEOPLASIA (CIN)
") CERVICAL INTRAEPITHELIAL NEOPLASIA (CIN) The cervix constitutes the lower third of the uterus. It is in two parts, the endocervix and the ectocervix. Ectocervix is covered with squamous epithelium. Endocervix
CERVICAL INTRAEPITHELIAL NEOPLASIA (CIN) The cervix constitutes the lower third of the uterus. It is in two parts, the endocervix and the ectocervix. Ectocervix is covered with squamous epithelium. Endocervix
Human Papillomavirus
 Human Papillomavirus Dawn Palaszewski, MD Assistant Professor of Obstetrics and Gynecology University of February 18, 2018 9:40 am Dawn Palaszewski, MD Assistant Professor Department of Obstetrics and
Human Papillomavirus Dawn Palaszewski, MD Assistant Professor of Obstetrics and Gynecology University of February 18, 2018 9:40 am Dawn Palaszewski, MD Assistant Professor Department of Obstetrics and
Colposcopy. Attila L Major, MD, PhD
 Colposcopy Attila L Major, MD, PhD Histology Colposcopy Cytology It has been estimated that annual Pap smear testing reduces a woman s chance of dying of cervical cancer from 4 in 1000 to about 5 in 10,000
Colposcopy Attila L Major, MD, PhD Histology Colposcopy Cytology It has been estimated that annual Pap smear testing reduces a woman s chance of dying of cervical cancer from 4 in 1000 to about 5 in 10,000
Cervical Conization. 1
 Cervical Conization www.zohrehyousefi.com 1 Cone Biopsy is a surgical procedure with removal of a cone shaped portion of the cervix The extent of involvement of epithelium on the ectocervix has been clearly
Cervical Conization www.zohrehyousefi.com 1 Cone Biopsy is a surgical procedure with removal of a cone shaped portion of the cervix The extent of involvement of epithelium on the ectocervix has been clearly
SESSION J4. What's Next? Managing Abnormal PAPs in 2014
 37th Annual Advanced Practice in Primary and Acute Care Conference: October 9-11, 2014 2:45 SESSION J4 What's Next? Managing Abnormal PAPs in 2014 Session Description: Linda Eckert, MD Review current guidelines
37th Annual Advanced Practice in Primary and Acute Care Conference: October 9-11, 2014 2:45 SESSION J4 What's Next? Managing Abnormal PAPs in 2014 Session Description: Linda Eckert, MD Review current guidelines
Case Based Problems. Recommended Guidelines. Workshop: Case Management of Abnormal Pap Smears and Colposcopies. Disclosure
 Disclosure Workshop: Case Management of Abnormal Pap Smears and Colposcopies Rebecca Jackson, MD Associate Professor Obstetrics, Gynecology & Reproductive Sciences and Epidemiology & Biostatistics This
Disclosure Workshop: Case Management of Abnormal Pap Smears and Colposcopies Rebecca Jackson, MD Associate Professor Obstetrics, Gynecology & Reproductive Sciences and Epidemiology & Biostatistics This
Cervical Cancer : Pap smear
 Taking a PAP SMEAR Cervical Cancer : Pap smear George N Papanicolaou introduced cervical cytology in clinical practice in 1940 In 1945, PAP smear was endorsed by American cancer society as an effective
Taking a PAP SMEAR Cervical Cancer : Pap smear George N Papanicolaou introduced cervical cytology in clinical practice in 1940 In 1945, PAP smear was endorsed by American cancer society as an effective
1.Acute and Chronic Cervicitis - At the onset of menarche, the production of estrogens by the ovary stimulates maturation of the cervical and vaginal
 Diseases of cervix I. Inflammations 1.Acute and Chronic Cervicitis - At the onset of menarche, the production of estrogens by the ovary stimulates maturation of the cervical and vaginal squamous mucosa
Diseases of cervix I. Inflammations 1.Acute and Chronic Cervicitis - At the onset of menarche, the production of estrogens by the ovary stimulates maturation of the cervical and vaginal squamous mucosa
Screening for Cervical Cancer: Demystifying the Guidelines DR. NEERJA SHARMA
 Screening for Cervical Cancer: Demystifying the Guidelines DR. NEERJA SHARMA Cancer Care Ontario Cervical Cancer Screening Goals Increase patient participation in cervical screening Increase primary care
Screening for Cervical Cancer: Demystifying the Guidelines DR. NEERJA SHARMA Cancer Care Ontario Cervical Cancer Screening Goals Increase patient participation in cervical screening Increase primary care
Chapter 10: Pap Test Results
 Chapter 10: Pap Test Results On completion of this section, the learner will be able to: 1. Identify how Pap test results are interpreted and the reasons for normal and abnormal results. 2. Describe the
Chapter 10: Pap Test Results On completion of this section, the learner will be able to: 1. Identify how Pap test results are interpreted and the reasons for normal and abnormal results. 2. Describe the
VIN/VAIN O C T O B E R 3 RD J M O R G A N
 VIN/VAIN O C T O B E R 3 RD 2 0 1 8 J M O R G A N Vaginal Intraepithelial Neoplasia VAIN I, II, III Incidence 0.1/100,000 women in US Mean age 50s (J Womens Health (Larchmt) 2009:18:1731) (J Obstet Gynaecol
VIN/VAIN O C T O B E R 3 RD 2 0 1 8 J M O R G A N Vaginal Intraepithelial Neoplasia VAIN I, II, III Incidence 0.1/100,000 women in US Mean age 50s (J Womens Health (Larchmt) 2009:18:1731) (J Obstet Gynaecol
Management of Abnormal Cervical Cytology and Histology
 Management of Abnormal Cervical Cytology and Histology Assoc. Prof. Gökhan Tulunay Etlik Zübeyde Hanım Women s Diseases Teaching & Research Hospital Gynecologic Oncology Clinic Universally accepted guideline
Management of Abnormal Cervical Cytology and Histology Assoc. Prof. Gökhan Tulunay Etlik Zübeyde Hanım Women s Diseases Teaching & Research Hospital Gynecologic Oncology Clinic Universally accepted guideline
Objectives. Background. Background. Background. Background 9/26/16. Update on Cervical and HPV Screening Guidelines: To pap or not to pap?
 Update on Cervical and HPV Screening Guidelines: To pap or not to pap? Marina Delazari Miller MD Clinical Assistant Professor Department of Obstetrics & Gynecology University of Iowa Hospitals and Clinics
Update on Cervical and HPV Screening Guidelines: To pap or not to pap? Marina Delazari Miller MD Clinical Assistant Professor Department of Obstetrics & Gynecology University of Iowa Hospitals and Clinics
Cervical Testing and Results Management. An Evidenced-Based Approach April 22nd, Debora Bear, MSN, MPH
 Cervical Testing and Results Management An Evidenced-Based Approach April 22nd, 2010 Debora Bear, MSN, MPH Assistant Medical Director for Planned Parenthood of New Mexico, Inc. Burden of cervical cancer
Cervical Testing and Results Management An Evidenced-Based Approach April 22nd, 2010 Debora Bear, MSN, MPH Assistant Medical Director for Planned Parenthood of New Mexico, Inc. Burden of cervical cancer
Cervical Cancer Screening. David Quinlan December 2013
 Cervical Cancer Screening David Quinlan December 2013 Cervix Cervical Cancer Screening Modest variation provincially WHO and UK begin at 25 stop at 60 Finland begin at 30 stop at 60 Rationale for
Cervical Cancer Screening David Quinlan December 2013 Cervix Cervical Cancer Screening Modest variation provincially WHO and UK begin at 25 stop at 60 Finland begin at 30 stop at 60 Rationale for
Clinical Practice Guidelines June 2013
 Clinical Practice Guidelines June 2013 General Principles: The Papanicolaou (Pap) smear is widely credited with reducing mortality from cervical cancer, and remains the single best method for the early
Clinical Practice Guidelines June 2013 General Principles: The Papanicolaou (Pap) smear is widely credited with reducing mortality from cervical cancer, and remains the single best method for the early
Histopathology: Cervical HPV and neoplasia
 Histopathology: Cervical HPV and neoplasia These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you need to learn about
Histopathology: Cervical HPV and neoplasia These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you need to learn about
Your Colposcopy Visit
 Introduction Welcome to the colposcopy clinic. This booklet tells you about. The colposcopy examination.. Tests that are done in the colposcopy clinic.. What these tests look for Take a few minutes to
Introduction Welcome to the colposcopy clinic. This booklet tells you about. The colposcopy examination.. Tests that are done in the colposcopy clinic.. What these tests look for Take a few minutes to
To further assess abnormalities detected on cervical cytological sample. To guide colposcopically directed biopsy
 1 To further assess abnormalities detected on cervical cytological sample To guide colposcopically directed biopsy To exclude invasive disease To aid in outpatient management and treatment of precancerous
1 To further assess abnormalities detected on cervical cytological sample To guide colposcopically directed biopsy To exclude invasive disease To aid in outpatient management and treatment of precancerous
Conflict of Interest Disclosure. Anita L. Nelson, MD. Principles Underlying Screening Recommendations. Learning Objectives
 Advanced Colposcopy Conflict of Interest Disclosure Anita L. Nelson, MD Anita L. Nelson, MD Professor OB-GYN David Geffen School of Medicine at UCLA CFHC s 2014 Women s Health Update Berkeley, CA May 20,
Advanced Colposcopy Conflict of Interest Disclosure Anita L. Nelson, MD Anita L. Nelson, MD Professor OB-GYN David Geffen School of Medicine at UCLA CFHC s 2014 Women s Health Update Berkeley, CA May 20,
Update on Cervical Cancer Screening. Rahmouna Farez M.D. Assistant Professor, Medical College of Wisconsin 5/2/2014
 Update on Cervical Cancer Screening Rahmouna Farez M.D. Assistant Professor, Medical College of Wisconsin 5/2/2014 Objectives Review the natural history of HPV as it relates to cervical cancer screening
Update on Cervical Cancer Screening Rahmouna Farez M.D. Assistant Professor, Medical College of Wisconsin 5/2/2014 Objectives Review the natural history of HPV as it relates to cervical cancer screening
Update on Cervical Cancer Screening
 Update on Cervical Cancer Screening Rahmouna Farez M.D. Assistant Professor, Medical College of Wisconsin 5/2/2014 Objectives Review the natural history of HPV as it relates to cervical cancer screening
Update on Cervical Cancer Screening Rahmouna Farez M.D. Assistant Professor, Medical College of Wisconsin 5/2/2014 Objectives Review the natural history of HPV as it relates to cervical cancer screening
Updated ASCCP Consensus Guidelines For Managing Diagnosed Cervical Cancer Precursors Michael A. Gold, M.D.
 Updated ASCCP Consensus Guidelines For Managing Diagnosed Cervical Cancer Precursors Michael A. Gold, M.D. 27 May, 2014 London, England Faculty Disclosure X No, nothing to disclose Yes, please specify
Updated ASCCP Consensus Guidelines For Managing Diagnosed Cervical Cancer Precursors Michael A. Gold, M.D. 27 May, 2014 London, England Faculty Disclosure X No, nothing to disclose Yes, please specify
Management that provides continuity of care for women
 Management that provides continuity of care for women If women are diagnosed with reproductive tract infection, prompt treatment should be instituted according to the WHO guidelines. Though it may be preferred
Management that provides continuity of care for women If women are diagnosed with reproductive tract infection, prompt treatment should be instituted according to the WHO guidelines. Though it may be preferred
Cervical cancer presentation
 Carcinoma of the cervix: Carcinoma of the cervix is the second commonest cancer among women worldwide, with only breast cancer occurring more commonly. Worldwide, cervical cancer accounts for about 500,000
Carcinoma of the cervix: Carcinoma of the cervix is the second commonest cancer among women worldwide, with only breast cancer occurring more commonly. Worldwide, cervical cancer accounts for about 500,000
Cervical Skills. Dr Margaret Laing Queen Elizabeth University Hospital
 Cervical Skills Dr Margaret Laing Queen Elizabeth University Hospital What is screening? Screening is a test offered to an apparently well person with the possibility of detecting a serious disease before
Cervical Skills Dr Margaret Laing Queen Elizabeth University Hospital What is screening? Screening is a test offered to an apparently well person with the possibility of detecting a serious disease before
Understanding Your Pap Test Results
 Understanding Your Pap Test Results Most laboratories in the United States use a standard set of terms called the Bethesda System to report pap test results. Normal: Pap samples that have no cell abnormalities
Understanding Your Pap Test Results Most laboratories in the United States use a standard set of terms called the Bethesda System to report pap test results. Normal: Pap samples that have no cell abnormalities
Cervical Cancer Screening Guidelines Update
 Frontier AIDS Education and Training Center Cervical Cancer Screening Guidelines Update Hillary Liss, MD Harborview Medical Center, Madison and Adult Medicine Clinics Frontier AETC, Medical Program Director
Frontier AIDS Education and Training Center Cervical Cancer Screening Guidelines Update Hillary Liss, MD Harborview Medical Center, Madison and Adult Medicine Clinics Frontier AETC, Medical Program Director
 1 Cervical Cancer Prevention and Screening: Update 2010 Michael S. Policar, MD, MPH Clinical Professor of Ob, Gyn, and RS UCSF School of Medicine policarm@obgyn.ucsf.edu No commercial disclosures for this
1 Cervical Cancer Prevention and Screening: Update 2010 Michael S. Policar, MD, MPH Clinical Professor of Ob, Gyn, and RS UCSF School of Medicine policarm@obgyn.ucsf.edu No commercial disclosures for this
Colposcopic Principles. Simon Leeson Consultant Obstetrician/ Gynaecologist Betsi Cadwaladr University Health Board UK
 Colposcopic Principles Simon Leeson Consultant Obstetrician/ Gynaecologist Betsi Cadwaladr University Health Board UK The cervix topics discussed are: original squamous epithelium endocervical epithelium
Colposcopic Principles Simon Leeson Consultant Obstetrician/ Gynaecologist Betsi Cadwaladr University Health Board UK The cervix topics discussed are: original squamous epithelium endocervical epithelium
GLANDULAR LESIONS PITFALLS IN MANAGEMENT. Dr Li Wai Hon HKSCCP The 15 th Anniversary Symposium 10 December 2016
 GLANDULAR LESIONS PITFALLS IN MANAGEMENT Dr Li Wai Hon HKSCCP The 15 th Anniversary Symposium 10 December 2016 Introduction Cervical glandular lesions are much less common than squamous lesion Incidence
GLANDULAR LESIONS PITFALLS IN MANAGEMENT Dr Li Wai Hon HKSCCP The 15 th Anniversary Symposium 10 December 2016 Introduction Cervical glandular lesions are much less common than squamous lesion Incidence
Done by khozama jehad. Neoplasia of the cervix
 Done by khozama jehad Neoplasia of the cervix An overview of cervical neoplasia very import. Most tumors of the cervix are of epithelial origin and are caused by oncogenic strains of human papillomavirus
Done by khozama jehad Neoplasia of the cervix An overview of cervical neoplasia very import. Most tumors of the cervix are of epithelial origin and are caused by oncogenic strains of human papillomavirus
Gynecologic Cancers. What is Gynecologic Cancer. Who is at risk for GYN cancer? 3/1/2018 1
 What is Gynecologic Cancer Gynecologic Cancers Marge Ramsdell RN, MN, OCN Madigan Army Medical Center Any cancer that starts in a woman s reproductive organs Each GYN cancer is unique 5 main types Cervical
What is Gynecologic Cancer Gynecologic Cancers Marge Ramsdell RN, MN, OCN Madigan Army Medical Center Any cancer that starts in a woman s reproductive organs Each GYN cancer is unique 5 main types Cervical
Cervical Cancer Screening
 Todd R. Jenkins, MD, MSHA Senior Vice Chair Director, Division of Women s Reproductive Healthcare Learning Objectives Describe the etiology, natural history, and usage of the human papillomavirus (HPV)
Todd R. Jenkins, MD, MSHA Senior Vice Chair Director, Division of Women s Reproductive Healthcare Learning Objectives Describe the etiology, natural history, and usage of the human papillomavirus (HPV)
Managament of Abnormal Cervical Cytology and Histology
 Managament of Abnormal Cervical Cytology and Histology Ali Ayhan, M.D Başkent University Faculty of Medicine Department of Gynecology and Obstetrics Division of Gynecologic Oncology Abnormal Cytologic
Managament of Abnormal Cervical Cytology and Histology Ali Ayhan, M.D Başkent University Faculty of Medicine Department of Gynecology and Obstetrics Division of Gynecologic Oncology Abnormal Cytologic
Pap Smears Pelvic Examinations Well Woman Examinations. When should you have them performed???
 Pap Smears Pelvic Examinations Well Woman Examinations. When should you have them performed??? Arlene Evans-DeBeverly, PA-C Copyright 2012 There are always ongoing changes in gynecology, including the
Pap Smears Pelvic Examinations Well Woman Examinations. When should you have them performed??? Arlene Evans-DeBeverly, PA-C Copyright 2012 There are always ongoing changes in gynecology, including the
Over-diagnoses in Cytopathology: Is histology the gold standard?
 Over-diagnoses in Cytopathology: Is histology the gold standard? Teresa M. Darragh, MD UCSF Departments of Pathology and Obstetrics, Gynecology & Reproductive Sciences Faculty Disclosures: Teresa M. Darragh,
Over-diagnoses in Cytopathology: Is histology the gold standard? Teresa M. Darragh, MD UCSF Departments of Pathology and Obstetrics, Gynecology & Reproductive Sciences Faculty Disclosures: Teresa M. Darragh,
HIV and AIDS Related Cancers DR GORDON AMBAYO UHS
 HIV and AIDS Related Cancers DR GORDON AMBAYO UHS INTRODUCTION People with HIV/AIDS are at high risk for developing certain cancers, such as: Kaposi's sarcoma, non-hodgkin lymphoma, and cervical cancer.
HIV and AIDS Related Cancers DR GORDON AMBAYO UHS INTRODUCTION People with HIV/AIDS are at high risk for developing certain cancers, such as: Kaposi's sarcoma, non-hodgkin lymphoma, and cervical cancer.
Estimated New Cancers Cases 2003
 Harvard-MIT Division of Health Sciences and Technology HST.071: Human Reproductive Biology Course Director: Professor Henry Klapholz Estimated New Cancers Cases 2003 Images removed due to copyright reasons.
Harvard-MIT Division of Health Sciences and Technology HST.071: Human Reproductive Biology Course Director: Professor Henry Klapholz Estimated New Cancers Cases 2003 Images removed due to copyright reasons.
International Federation of Gynecology and Obstetrics
 International Federation of Gynecology and Obstetrics Treatment of Cervical Precancerous Lesions using Thermocoagulation(Cold Coagulation) and Cryotherapy General Principles All high grade CIN should be
International Federation of Gynecology and Obstetrics Treatment of Cervical Precancerous Lesions using Thermocoagulation(Cold Coagulation) and Cryotherapy General Principles All high grade CIN should be
Disclosures. Learning objectives. George F. Sawaya, MD. I have nothing to disclose.
 Well Woman Visits in 2018: How Should We Approach Cervical Cancer Screening and Routine Pelvic Examinations? George F. Sawaya, MD Disclosures I have nothing to disclose. Professor, Obstetrics, Gynecology
Well Woman Visits in 2018: How Should We Approach Cervical Cancer Screening and Routine Pelvic Examinations? George F. Sawaya, MD Disclosures I have nothing to disclose. Professor, Obstetrics, Gynecology
WOMEN S INTERAGENCY HIV STUDY LABORATORY - PELVIC EXAM STUDIES COLPOSCOPY RESULTS FORM L14
 WOMEN S INTERAGENCY HIV STUDY LABORATORY - PELVIC EXAM STUDIES COLPOSCOPY RESULTS FORM L4 ID LABEL HERE ---> - - - VISIT #: FORM COMPLETED BY: VERSION DATE: 0 / 0 / 6 ANY MISSING OR INCOMPLETE TEST RESULTS
WOMEN S INTERAGENCY HIV STUDY LABORATORY - PELVIC EXAM STUDIES COLPOSCOPY RESULTS FORM L4 ID LABEL HERE ---> - - - VISIT #: FORM COMPLETED BY: VERSION DATE: 0 / 0 / 6 ANY MISSING OR INCOMPLETE TEST RESULTS
Screening for Cervical Cancer. Grand Rounds 1/16/13 Meggan Linck
 Screening for Cervical Cancer Grand Rounds 1/16/13 Meggan Linck Cervical Cancer Worldwide 2 nd most common and 5 th deadliest U.S. 8 th most common 80% occur in developing world Median age at diagnosis
Screening for Cervical Cancer Grand Rounds 1/16/13 Meggan Linck Cervical Cancer Worldwide 2 nd most common and 5 th deadliest U.S. 8 th most common 80% occur in developing world Median age at diagnosis
LABORATORY - PELVIC EXAM STUDIES COLPOSCOPY RESULTS FORM L14
 LABORATORY - PELVIC EXAM STUDIES COLPOSCOPY RESULTS FORM L4 ID LABEL HERE ---> - - - VISIT #: FORM COMPLETED BY: VERSION DATE: 0/0/0 ANY MISSING OR INCOMPLETE TEST RESULTS MUST BE EXPLAINED ON THIS FORM.
LABORATORY - PELVIC EXAM STUDIES COLPOSCOPY RESULTS FORM L4 ID LABEL HERE ---> - - - VISIT #: FORM COMPLETED BY: VERSION DATE: 0/0/0 ANY MISSING OR INCOMPLETE TEST RESULTS MUST BE EXPLAINED ON THIS FORM.
LABORATORY - PELVIC EXAM STUDIES COLPOSCOPY RESULTS FORM L14
 LABORATORY - PELVIC EXAM STUDIES COLPOSCOPY RESULTS FORM L4 ID LABEL HERE ---> - - - VISIT #: FORM COMPLETED BY: VERSION DATE: 09/5/95 ANY MISSING OR INCOMPLETE TEST RESULTS MUST BE EXPLAINED ON THIS FORM.
LABORATORY - PELVIC EXAM STUDIES COLPOSCOPY RESULTS FORM L4 ID LABEL HERE ---> - - - VISIT #: FORM COMPLETED BY: VERSION DATE: 09/5/95 ANY MISSING OR INCOMPLETE TEST RESULTS MUST BE EXPLAINED ON THIS FORM.
The Pap Smear Test. The Lebanese Society of Obstetrics and Gynecology. Women s health promotion series
 The Lebanese Society of Obstetrics and Gynecology Women s health promotion series The Pap Smear Test Since the Pap smear test started to be used the number of cases of cervical cancer was greatly reduced.
The Lebanese Society of Obstetrics and Gynecology Women s health promotion series The Pap Smear Test Since the Pap smear test started to be used the number of cases of cervical cancer was greatly reduced.
Proposed new national cervical screening program. Dr Elizabeth Jackson Obstetrician Gynaecologist Cairns
 Proposed new national cervical screening program Dr Elizabeth Jackson Obstetrician Gynaecologist Cairns www.drelizabethjackson.com Cervical cancer in Australia 12th most common cancer affecting Australian
Proposed new national cervical screening program Dr Elizabeth Jackson Obstetrician Gynaecologist Cairns www.drelizabethjackson.com Cervical cancer in Australia 12th most common cancer affecting Australian
PREVENTION OF CERVICAL CANCER
 PREVENTION OF CERVICAL CANCER Author: Dr R. Fuentes MBchb, Havana Spec. OB,GY-Havana- 2011 CONTENT TABLE Abbreviations 2 Introduction 4 The natural history of Cervical cancer 4 Risk Factors 4 Incidence
PREVENTION OF CERVICAL CANCER Author: Dr R. Fuentes MBchb, Havana Spec. OB,GY-Havana- 2011 CONTENT TABLE Abbreviations 2 Introduction 4 The natural history of Cervical cancer 4 Risk Factors 4 Incidence
Twenty-first refresher course. Chan Kit Sheung
 Twenty-first refresher course Chan Kit Sheung 7-5-2015 Case 1 Case 1, 29y old, G3P2, referred from MCHC Cervical smear on 27-9-2013: LGSIL, defaulted appointment Cervical smear in 12/2014: negative Colposcopy
Twenty-first refresher course Chan Kit Sheung 7-5-2015 Case 1 Case 1, 29y old, G3P2, referred from MCHC Cervical smear on 27-9-2013: LGSIL, defaulted appointment Cervical smear in 12/2014: negative Colposcopy
Cytology/Biopsy/Leep Gynecologic Correlation: Practical Considerations and Approaches.
 Cytology/Biopsy/Leep Gynecologic Correlation: Practical Considerations and Approaches. Fadi W. Abdul-Karim MD MEd. Professor of Pathology. Vice chair for education. Robert Tomsich Pathology and Lab Med
Cytology/Biopsy/Leep Gynecologic Correlation: Practical Considerations and Approaches. Fadi W. Abdul-Karim MD MEd. Professor of Pathology. Vice chair for education. Robert Tomsich Pathology and Lab Med
X-Treme Primary Care: HPV and STIs. Arti Barnes MD MPH Clinical Director South Central AIDS Education and Training Centers
 X-Treme Primary Care: HPV and STIs Arti Barnes MD MPH Clinical Director South Central AIDS Education and Training Centers Learning Objectives Review recommendations for HPV related cancer screening in
X-Treme Primary Care: HPV and STIs Arti Barnes MD MPH Clinical Director South Central AIDS Education and Training Centers Learning Objectives Review recommendations for HPV related cancer screening in
Lessons From Cases of Screened Women Who Developed Cervical Carcinoma
 Lessons From Cases of Screened Women Who Developed Cervical Carcinoma R. Marshall Austin MD,PhD Magee-Womens Hospital of University of Pittsburgh Medical Center raustin@magee.edu Why Focus Study On Cases
Lessons From Cases of Screened Women Who Developed Cervical Carcinoma R. Marshall Austin MD,PhD Magee-Womens Hospital of University of Pittsburgh Medical Center raustin@magee.edu Why Focus Study On Cases
What is a Pap smear?
 Pap smear What is a Pap smear? A Pap smear is a test that checks for changes in the cells of your cervix. The cervix is the lower part of the uterus that opens into the vagina. Developed over forty years
Pap smear What is a Pap smear? A Pap smear is a test that checks for changes in the cells of your cervix. The cervix is the lower part of the uterus that opens into the vagina. Developed over forty years
Human Papillomavirus. Kathryn Thiessen, ARNP, ACRN The Kansas AIDS Education and Training Center The University of Kansas School of Medicine Wichita
 Human Papillomavirus Kathryn Thiessen, ARNP, ACRN The Kansas AIDS Education and Training Center The University of Kansas School of Medicine Wichita What is Genital HPV Infection Human papillomavirus is
Human Papillomavirus Kathryn Thiessen, ARNP, ACRN The Kansas AIDS Education and Training Center The University of Kansas School of Medicine Wichita What is Genital HPV Infection Human papillomavirus is
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
What is cervical cancer?
 What is cervical cancer? The cervix is the bottom part, or neck, of the uterus. Cervical cancer happens when normal cells in the cervix change into abnormal cells, and grow out of control. Most women whose
What is cervical cancer? The cervix is the bottom part, or neck, of the uterus. Cervical cancer happens when normal cells in the cervix change into abnormal cells, and grow out of control. Most women whose
CERVICAL CANCER FACTSHEET. What is cervical cancer?
 CERVICAL CANCER FACTSHEET What is cervical cancer? ENGAGe is releasing a series of factsheets to raise awareness of gynaecological cancers and to support its network to work at a grassroots level. Take-up
CERVICAL CANCER FACTSHEET What is cervical cancer? ENGAGe is releasing a series of factsheets to raise awareness of gynaecological cancers and to support its network to work at a grassroots level. Take-up
Cervical Cancer Prevention in the 21 st Century Changing Paradigms
 Cervical Cancer Prevention in the 21 st Century Changing Paradigms Teresa M. Darragh, MD UCSF Departments of Pathology and Obstetrics, Gynecology & Reproductive Sciences Faculty Disclosures: Teresa M.
Cervical Cancer Prevention in the 21 st Century Changing Paradigms Teresa M. Darragh, MD UCSF Departments of Pathology and Obstetrics, Gynecology & Reproductive Sciences Faculty Disclosures: Teresa M.
Treatment of Cervical Intraepithelial Neoplasia. Case. How would you manage this woman?
 Treatment of Cervical Intraepithelial Neoplasia Karen Smith-McCune Professor, Department of Obstetrics, Gynecology and Reproductive Sciences I have no conflicts of interest Case How would you manage this
Treatment of Cervical Intraepithelial Neoplasia Karen Smith-McCune Professor, Department of Obstetrics, Gynecology and Reproductive Sciences I have no conflicts of interest Case How would you manage this
Gynecologic Malignancies. Kristen D Starbuck 4/20/18
 Gynecologic Malignancies Kristen D Starbuck 4/20/18 Outline Female Cancer Statistics Uterine Cancer Adnexal Cancer Cervical Cancer Vulvar Cancer Uterine Cancer Endometrial Cancer Uterine Sarcoma Endometrial
Gynecologic Malignancies Kristen D Starbuck 4/20/18 Outline Female Cancer Statistics Uterine Cancer Adnexal Cancer Cervical Cancer Vulvar Cancer Uterine Cancer Endometrial Cancer Uterine Sarcoma Endometrial
HPV the silent killer, Prevention and diagnosis
 HPV the silent killer, Prevention and diagnosis HPV Human Papilloma Virus is a name given for a silent virus transmitted sexually most of the time, a virus that spreads in the name of love, passion, and
HPV the silent killer, Prevention and diagnosis HPV Human Papilloma Virus is a name given for a silent virus transmitted sexually most of the time, a virus that spreads in the name of love, passion, and
CERVIX. MLS Basic histological diagnosis MLS HIST 422 Semester 8- batch 7 L12 : Dr. Ali Eltayb.
 CERVIX MLS Basic histological diagnosis MLS HIST 422 Semester 8- batch 7 L12 : Dr. Ali Eltayb. CERVIX Most cervical lesions are: Most are Cervicitis. cancers ( common in women worldwide). CERVICITIS Extremely
CERVIX MLS Basic histological diagnosis MLS HIST 422 Semester 8- batch 7 L12 : Dr. Ali Eltayb. CERVIX Most cervical lesions are: Most are Cervicitis. cancers ( common in women worldwide). CERVICITIS Extremely
Cytyc Corporation - Case Presentation Archive - July 2002
 ThinPrep Pap Test History: 34 Year Old Female LMP: Day 20 Specimen Type: Cervical/Vaginal Case provided by Mark Tulecke, M.D. and Gabrielle Trawinski CT (ASCP), Mount Auburn Hospital, Cambridge, Massachusetts.
ThinPrep Pap Test History: 34 Year Old Female LMP: Day 20 Specimen Type: Cervical/Vaginal Case provided by Mark Tulecke, M.D. and Gabrielle Trawinski CT (ASCP), Mount Auburn Hospital, Cambridge, Massachusetts.
SOGC / SCC Clinical Practice Guideline
 SOGC / SCC Clinical Practice Guideline Colposcopic Management of Abnormal Cervical Cancer Screening and Histology These Clinical Practice Guidelines have been prepared and approved by the Executive and
SOGC / SCC Clinical Practice Guideline Colposcopic Management of Abnormal Cervical Cancer Screening and Histology These Clinical Practice Guidelines have been prepared and approved by the Executive and
An Update on Cervical Cancer Screening Recommendations and on the DOH BCC Program
 An Update on Cervical Cancer Screening Recommendations and on the DOH BCC Program Susan Baum, MD, MPH NM Nurse Practitioner Council Annual Conference April 20, 2012 I have no commercial relationships related
An Update on Cervical Cancer Screening Recommendations and on the DOH BCC Program Susan Baum, MD, MPH NM Nurse Practitioner Council Annual Conference April 20, 2012 I have no commercial relationships related
6 Week Course Agenda. Today s Agenda. Ovarian Cancer: Risk Factors. Winning the War 11/30/2016 on Women s Cancer Gynecologic Cancer Prevention
 6 Week Course Agenda Winning the War 11/30/2016 on Women s Cancer Gynecologic Cancer Prevention Lee-may Chen, MD Director, Division of Gynecologic Oncology Professor Department of Obstetrics, Gynecology
6 Week Course Agenda Winning the War 11/30/2016 on Women s Cancer Gynecologic Cancer Prevention Lee-may Chen, MD Director, Division of Gynecologic Oncology Professor Department of Obstetrics, Gynecology
What Causes Cervical Cancer? Symptoms of Cervical Cancer
 Cervical Health Awareness Month is a chance to raise awareness about how women can protect themselves from HPV (human papillomavirus) and cervical cancer. HPV is a very common infection that spreads through
Cervical Health Awareness Month is a chance to raise awareness about how women can protect themselves from HPV (human papillomavirus) and cervical cancer. HPV is a very common infection that spreads through
Cytology Update M Laing QEUH
 Cytology Update M Laing QEUH Age change to 25 to 65 Age 25 to 50 Three yearly smear invitation Age 50 to 65 Five yearly smear invitation Women on non routine screening will be invited up to age 70 OUTCOME
Cytology Update M Laing QEUH Age change to 25 to 65 Age 25 to 50 Three yearly smear invitation Age 50 to 65 Five yearly smear invitation Women on non routine screening will be invited up to age 70 OUTCOME
Jacqui Morgan March 6, 2019
 Jacqui Morgan March 6, 2019 Case 1 25yo, G2P1 Here for WWE, no problems, healthy, needs refill on OCPs. Pap- Abnormal Glandular Cells-NOS Now What?? Case 1 Colposcopy What findings? Case 1 ECC Cervical
Jacqui Morgan March 6, 2019 Case 1 25yo, G2P1 Here for WWE, no problems, healthy, needs refill on OCPs. Pap- Abnormal Glandular Cells-NOS Now What?? Case 1 Colposcopy What findings? Case 1 ECC Cervical
Gynecological Cancers
 Gynecological Cancers Outline Ovarian Cancer Uterine (Endometrial) Cancer Cervical Cancer Vulvar Cancer Vaginal Cancer Overian Cancer Ovarian cancer is cancer that forms in the tissue of the ovary and
Gynecological Cancers Outline Ovarian Cancer Uterine (Endometrial) Cancer Cervical Cancer Vulvar Cancer Vaginal Cancer Overian Cancer Ovarian cancer is cancer that forms in the tissue of the ovary and
I have no financial interests in any product I will discuss today.
 How Should We Approach Cervical Cancer Screening and Routine Pelvic Examinations in 2019? Michael Policar, MD, MPH Professor Emeritus Department of Obstetrics, Gynecology and Reproductive Sciences University
How Should We Approach Cervical Cancer Screening and Routine Pelvic Examinations in 2019? Michael Policar, MD, MPH Professor Emeritus Department of Obstetrics, Gynecology and Reproductive Sciences University