* * * * Supplementary Figure 1. DS Lv CK HSA CK HSA. CK Col-3. CK Col-3. See overleaf for figure legend. Cancer cells
|
|
|
- Kerry Wilkerson
- 5 years ago
- Views:
Transcription
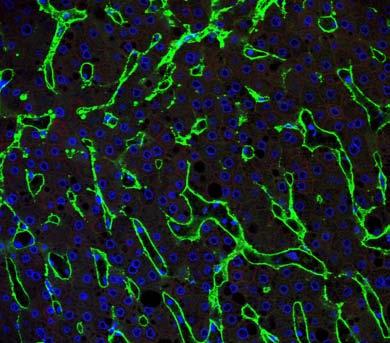
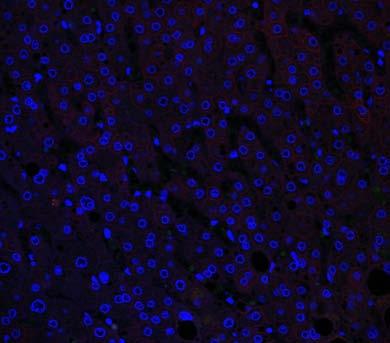
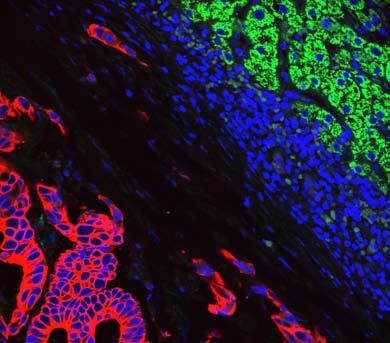
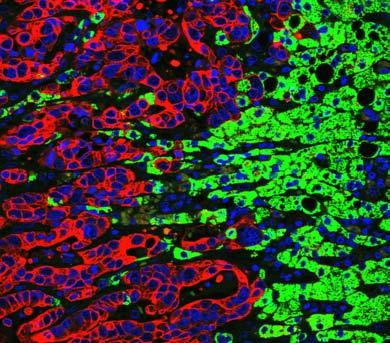
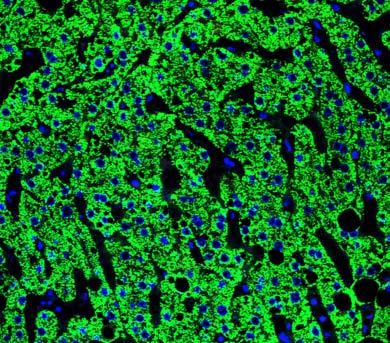
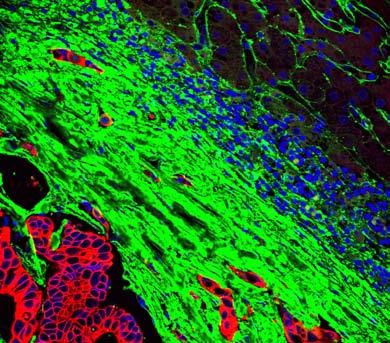
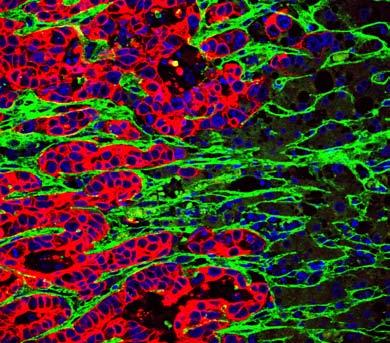
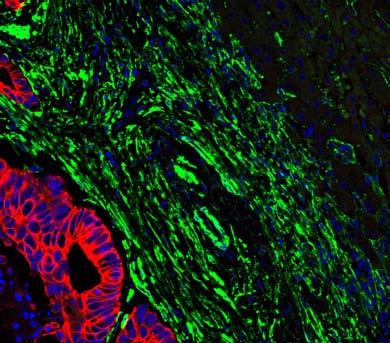
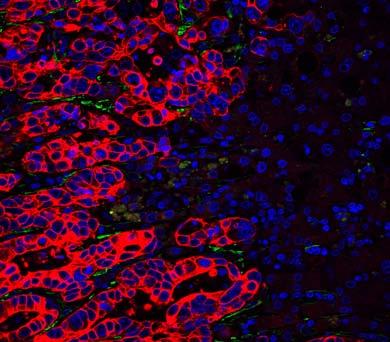
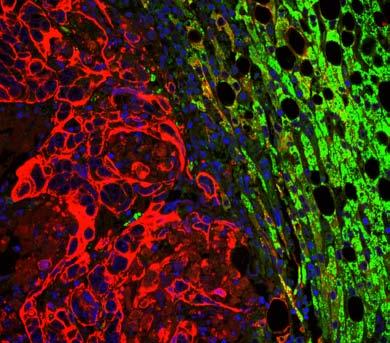
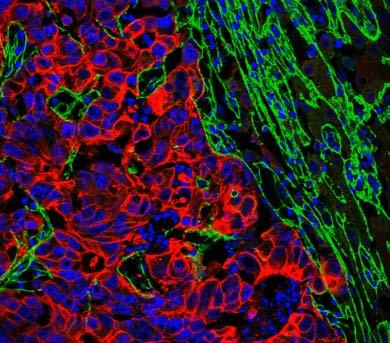
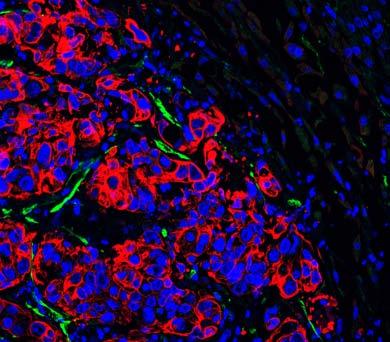
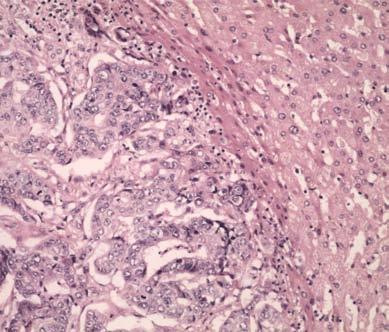
1 Supplementary Figure 1 Cancer cells Desmoplastic stroma Hepatocytes Pre-existing sinusoidal blood vessel New blood vessel a Normal liver b Desmoplastic HGP c Pushing HGP d Replacement HGP e f g h i DS * DS j k * * * l * * * * m CK HSA n CK HSA o CK HSA p CK HSA CK Col-3 CK Col-3 CK Col-3 CK Col-3 q r s t CK αsma See overleaf for figure legend CK αsma CK αsma CK αsma
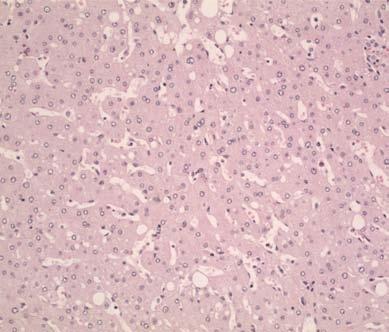
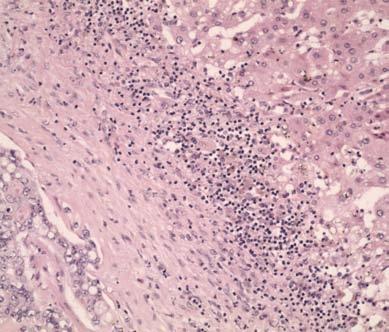
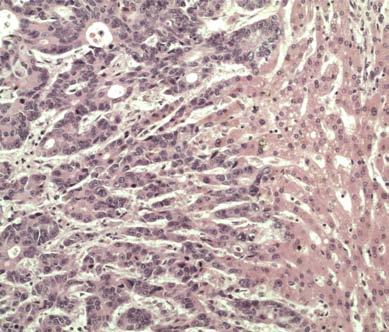
2 Supplementary Figure 1 Morphology of the three histopathological growth patterns (HGPs) of colorectal cancer liver metastases a h. Diagrams and H&E stainings illustrate the morphology of normal liver or the morphology of the tumor normal liver interface in human CRC liver metastases with a desmoplastic, pushing or replacement HGP. i t. To confirm the distinct tumor stroma interaction that occurs in each HGP, we performed additional staining for hepatocyte specific antigen (HSA), collagen 3 (col 3) and alpha smooth muscle actin (αsma). In normal liver, HSA labeled hepatocytes (i), col 3 labeled sinusoidal blood vessels (m), whilst αsma labeled neither hepatocytes nor sinusoidal blood vessels (q). In the desmoplastic HGP, a desmoplastic stroma physically separates cancer cells from normal liver (b,f). Co staining for pan cytokeratin (CK) to detect cancer cells and HSA to detect hepatocytes confirmed physical separation of cancer cells and normal liver (j), whilst co staining for pan cytokeratin and col 3, or pan cytokeratin and αsma, confirmed the presence of a desmoplastic stroma abundant in collagen (n) and αsma positive fibroblasts (r), respectively. In the pushing HGP, cancer cells and normal liver are in close contact with no intervening desmoplastic stroma (c,g) which was confirmed by co staining for CK and HSA (k) or CK and αsma (s). Another feature of the pushing HGP, physical compression of sinusoidal vessels in adjacent normal liver tissue, was confirmed by co staining for pan cytokeratin and col 3 (o). In the replacement HGP, cancer cells infiltrate the liver parenchyma and replace hepatocytes without disturbing the vascular architecture of the liver; no desmoplastic stroma is observed (d,h). Supporting this, co staining for CK and HSA confirmed the invasion of cancer cells into liver parenchyma (l). Co staining for CK and col 3 showed that the vascular architecture of the adjacent liver was preserved at the tumor liver interface (p). Lack of αsma staining confirmed the absence of a desmoplastic stroma (t). Asterisk, cancer cells. DS, desmoplastic stroma., normal liver. Scale bars, 5 µm.
3 Supplementary Figure 2 CRC liver resections performed after preoperative treatment with bev chemo at RM during the period : n = 11 lesions from 47 patients Liver lesions that were absent from baseline pre-treatment scans, but presented after the initiation of bev chemo treatment: n = 5 lesions from 1 patient Recovery of FFPE tissue blocks Tissue not available for assessment: n = 16 lesions FFPE tissue blocks assessed by pathologists for presence of tumour tissue Liver lesions were excluded from further histopathological analysis for the following reasons: Tissue block(s) did not contain any tumour tissue (n = 12 lesions) Analysis of pathological response by pathology team: Tissue was too poor quality for reliable assessment (n = 1 lesion) n = 67 lesions from 37 patients Liver lesions were excluded from assessment of histopathogical growth pattern because a complete pathological response was scored: Analysis of histopathogical growth pattern by pathology team: n = 59 lesions from 33 patients Analysis of morphological response criteria from CT scans: n = 8 lesions Liver lesions were excluded from morphological response criteria assessment because CT scans were of insufficient quality or because the pre and post treatment scans were performed at different sites: n = 7 lesions n = 52 lesions from 31 patients Supplementary Figure 2 Consort diagram for RM cohort Consort diagram to illustrate how cases of CRC liver metastases from patients treated preoperatively with bev chemo at RM were selected for inclusion in the study or excluded.
4 Supplementary Figure 3 1 Poor pathological response Good pathological response >75% viable 5-75% viable 25-49% viable <25% viable Replacement (R) Desmoplastic (D) Pushing (P) 8 Response Poor Good Total HGP (%) 6 4 No. of lesions <5% R 5% R Total 6 (35.3%) 11 (64.7%) 17 (1%) 16 (1%) (%) 16 (1%) 22 (66.7%) 11 (33.3%) 33 (1%) P <.1 2 Response Poor Good Total Individual CRC liver metastases (RM cohort) No. of lesions <5% D 5% D Total 18 (1%) (%) 18 (1%) 4 (26.7%) 11 (73.3%) 15 (1%) 22 (66.7%) 11 (33.3%) 33 (1%) P <.1 Supplementary Figure 3 Correlation between HGP and pathological response in an analysis restricted to one lesion per patient (RM cohort) Data are presented from the same series of 33 patients as depicted in Figure 1b, but for this analysis only one lesion per patient was used. The graph shows the % HGP (replacement, desmoplastic, pushing) scored in the largest lesion from each patient. Lesions scored as >75%, 5-75% or 25-49% viable were considered to be poor responders, whilst lesions scored as <25% viable were considered good responders. Lesions with a substantial ( 5%) replacement HGP were significantly enriched in the poor responder group when compared with good responders (P <.1), whilst lesions with a substantial ( 5%) desmoplastic HGP were significantly enriched in the good responder group when compared with poor responders (P <.1). The χ 2 test was used to determine statistical significance (see 2x2 contingency tables).
5 Supplementary Figure 4 CRC liver resections performed after preoperative treatment with bev-chemo at MUHC during the period : n = 191 lesions from 65 patients Liver lesions that were absent from baseline pre-treatment scans, but presented after the initiation of bev-chemo treatment (new CRCLMs): n = 35 lesions from 13 patients Recovery of FFPE tissue blocks Tissue not available for assessment: n = 1 lesion FFPE tissue blocks assessed by pathologists for presence of tumour tissue Liver lesions were excluded from further histopathological analysis for the following reasons: Tissue block(s) did not contain any tumour tissue: n = 15 lesions Analysis of pathological response by pathology team: Tissue was too poor quality for reliable assessment: n = 3 lesions n = 137 lesions from 61 patients Liver lesions were excluded from assessment of histopathogical growth pattern because a complete pathological response was scored: n = 9 lesions Analysis of histopathogical growth pattern by pathology team: n = 128 lesions from 59 patients Supplementary Figure 4 Consort diagram for MUHC cohort Consort diagram to illustrate how cases of CRC liver metastases from patients treated preoperatively with bev-chemo at MUHC were selected for inclusion in the study or excluded.
6 Supplementary Figure 5 1 Poor pathological response Good pathological response >75% viable 5-75% viable 25-49% viable <25% viable Replacement (R) Desmoplastic (D) Pushing (P) 8 Response Poor Good Total HGP (%) 6 4 No. of lesions <5% R 5% R Total 14 (4%) 21 (6%) 35 (1%) 21 (87.5%) 3 (12.5%) 24 (1%) 35 (59.3%) 24 (4.7%) 59 (1%) P <.1 2 Response Poor Good Total Individual CRC liver metastases (MUHC cohort) No. of lesions <5% D 5% D Total 14 (4%) 21 (6%) 35 (1%) 21 (87.5%) 3 (12.5%) 24 (1%) 35 (59.3%) 24 (4.7%) 59 (1%) P <.1 Supplementary Figure 5 Correlation between HGP and pathological response in an analysis restricted to one lesion per patient (MUHC cohort) Data are presented from the same series of 59 patients as depicted in Figure 1f, but for this analysis only one lesion per patient was used. The graph shows the % HGP (replacement, desmoplastic, pushing) scored in the largest lesion from each patient. Lesions scored as >75%, 5-75% or 25-49% viable were considered to be poor responders, whilst lesions scored as <25% viable were considered good responders. Lesions with a substantial ( 5%) replacement HGP were significantly enriched in the poor responder group when compared with good responders (P <.1), whilst lesions with a substantial ( 5%) desmoplastic HGP were significantly enriched in the good responder group when compared with poor responders (P <.1). The χ 2 test was used to determine statistical significance (see 2x2 contingency tables).
7 Supplementary Figure 6 1 >75% viable Poor pathological response 5-75% viable 25-49% viable Good pathological response <25% viable Replacement (R) Desmoplastic (D) Pushing (P) Response HGP (%) No. of lesions <5% R 5% R Total Poor Good Total 9 (45%) 11 (55%) 8 (88.9%) 1 (11.1%) 2 (1%) 9 (1%) 17 (58.6%) 12 (41.4%) 29 (1%) P =.264 Response Poor Good Total 2 Individual CRC liver metastases No. of lesions <5% D 5% D Total 9 (9%) 1 (1%) 1 (1%) 8 (42.1%) 11 (57.8%) 19 (1%) 17 (58.6%) 12 (41.4%) 29 (1%) P =.128 Supplementary Figure 6 The HGPs correlate with pathological response in patients presenting with a single lesion only The graph shows the HGPs and pathological response in 29 patients that presented with a single lesion only. Graph shows the % HGP (replacement, desmoplastic, pushing) scored in each lesion from each patient. Lesions scored as >75%, 5-75% or 25-49% viable were considered to be poor responders, whilst lesions scored as <25% viable were considered good responders. Lesions with a substantial ( 5%) replacement HGP were significantly enriched in the poor responder group when compared with good responders (P=.264). Lesions with a substantial ( 5%) desmoplastic HGP were significantly enriched in the good responder group when compared with poor responders (P=.128). The χ 2 test was used to determine statistical significance (see 2x2 contingency table).
8 Supplementary Figure 7 1 Poor morphological response Good morphological response AR PR OR Replacement (R) Desmoplastic (D) Pushing (P) 8 HGP (%) 6 4 No. of lesions <5% R 5% R Total Response Poor Good Total 7 (41.2%) 1 (58.8%) 17 (1%) 11 (78.6%) 3 (21.4%) 14 (1%) 18 (58.1%) 13 (41.9%) 31 (1%) P = Individual CRC liver metastases (RM cohort) Supplementary Figure 7 Correlation between HGP and morphological response in an analysis restricted to one lesion per patient (RM cohort) Data are presented from the same series of 31 patients as depicted in Figure 2g, but for this analysis only one lesion per patient was used. The graph shows the % HGP (replacement, desmoplastic, pushing) scored in the largest lesion from each patient. Lesions scored as having an absent morphological response (AR) were considered to be poor responders, whilst those undergoing a partial (PR) or optimal (OR) morphological response were considered to be good responders. Lesions with 5% replacement HGP were significantly enriched in poor responders compared to good responders (P =.357). The χ 2 test was used to determine statistical significance (see 2x2 contingency table).
9 Supplementary Figure 8 1 Poor RECIST response Good RECIST response PD SD PR Replacement (R) Desmoplastic (D) Pushing (P) 8 HGP (%) 6 4 No. of lesions <5% R 5% R Total Response Poor Good Total 12 (37.5%) 2 (62.5%) 32 (1%) 13 (48.1%) 14 (51.9%) 27 (1%) 25 (42.4%) 34 (57.6%) 59 (1%) P =.44 2 Individual CRC liver metastases (RM cohort) Supplementary Figure 8 The HGPs do not correlate with response when using RECIST criteria as a response measure Response to bev-chemo was scored using RECIST criteria in order to categorise individual lesions as: progressive disease (PD), stable disease (SD) or partial response (PR). Graph shows the % HGP scored in each individual lesion (replacement, desmoplastic, pushing) with lesions grouped according to response: PD, SD or PR (n = 59 liver metastases from 33 patients). Lesions scored as PD or SD were considered to be poor responders, whilst lesions scored as PR were considered to be good responders. Lesions with a substantial ( 5%) replacement HGP were not significantly enriched in the poor responder group when compared with good responders (P=.44). The χ 2 test was used to determine statistical significance (see 2x2 contingency table).

 to identify cancer cells (brown) and CD31 to identify vessels")




10 Supplementary Figure 9 a b c d DS DS e f CK2 CD31 Supplementary Figure 9 Staining for blood vessels in the different histopathological growth patterns Resection specimens of CRCLMs corresponding to the three different HGPs were stained for cytokeratin 2 (CK2) to identify cancer cells (brown) and CD31 to identify vessels (blue). a,b. Replacement HGP. Co-option of sinusoidal vessels by invading cancer cells is observed. c,d. Desmoplastic HGP. Co-option of sinusoidal vessels by cancer cells is physically precluded by the desmoplastic stroma (DS) that separates cancer cells from the normal liver (). Dashed line indicates where the desmoplastic rim of the tumor meets the normal liver. e,f. Pushing HGP. Sinusoidal vessels that are present in the normal liver adjacent to the tumor are compressed, highly elongated and run in parallel with the tumor-liver interface, a topology that physically precludes the co-option of these vessels by invading cancer cells. DS, desmoplastic stroma., normal liver. Scale bar, 5 μm.

 and CD31 to identify")


11 Supplementary Figure 1 a b Tumor c DS d Tumor HSA CD31 Supplementary Figure 1 Co-staining for blood vessels and hepatocytes in the different histopathological growth patterns Resection specimens of CRCLMs were stained for HSA to identify hepatocytes (brown) and CD31 to identify vessels (blue). a. Normal liver, b. replacement HGP, c. desmoplastic HGP, and d. pushing HGP. Dashed line indicates the interface where the tumor meets the normal liver. Arrowheads indicate co-opted sinsuoidal vessels that are still associated with hepatocytes. DS, desmoplastic stroma., normal liver. Scale bar, 5 μm.
 f Can ARPC3 (replacement HGP BCLM) g Can Negative control h ARPC3 staining intensity (H-score) 3 2")


.")



12 Supplementary Figure 11 a b Control shrna sharpc3-3 c d e DS Can Can Can DS Can ARPC3 (normal liver) ARPC3 (replacement HGP CRCLM) ARPC3 (desmoplastic HGP CRCLM) f Can ARPC3 (replacement HGP BCLM) g Can Negative control h ARPC3 staining intensity (H-score) P =.16 P =.31 Replacement HGP CRCLM Desmoplastic HGP CRCLM Replacement HGP BCLM Supplementary Figure 11 Expression of the Arp2/3 subunit ARPC3 in human liver metastases a,b. Validation of anti-arpc3 antibody staining specificity HT29 cells stably transfected with a control non-targeting shrna (control shrna) (a) or an ARPC3-targeted shrna (sharpc3-3) (b) were prepared for FFPE sections and then stained using an anti-arpc3 antibody (MABT95, Millipore). Loss of antigenicity in the knockdown cells (b) compared to the control cells (a) indicates that this antibody is specific for ARPC3. c-e. Examples of ARPC3 staining in human liver metastasis specimens Samples of human liver metastasis were stained using the anti-arpc3 antibody. c. ARPC3 staining in normal liver. ARPC3 staining is limited to Kuppfer cells and immune cells within the lumen of vessels (arrowheads) and staining is absent / weak in hepatocytes. d-f. ARPC3 staining in cancer cells (Can) of a replacement HGP CRCLM (d), a desmoplastic HGP CRCLM (e) and a replacement HGP breast cancer liver metastasis (BCLM) (f). Panel g shows a negative control, where the same staining protocol was performed but the primary antibody was omitted. Can, cancer cells., normal liver parenchyma. DS, desmoplastic stroma. h. Quantification of ARPC3 staining in human liver metastasis specimens The intensity of ARPC3 staining was scored in replacement HGP CRCLMs (n = 1), desmoplastic HGP CRCLMs (n = 1) and replacement HGP BCLMs (n = 9). Each data point on the graph is the intensity (H-score) for an individual


13 Supplementary Figure 12 a b * * Supplementary Figure S12 Preclinical model of advanced liver metastasis a. Macroscopic appearance of tumor formation in the left main lobe of the mouse liver after injection of HT29 cells. b. Macroscopic appearance of a human CRC liver metastasis resected from a patient (picture is courtesy of Mr Ali Majeed). Scale bar, 5 mm (a) or 5 cm (b). Tumor is indicated by an asterisk. Supplementary Figure 13 1 n.s. n.s. Relative cell viability n.s. n.s. n.s. n.s. n.s. n.s. n.s. Parent Control shrna sharpc3-1 sharpc3-2 sharpc Time after seeding cells (hours) Supplementary Figure 13 Knockdown of ARPC3 in HT29 cells does not alter cell proliferation Proliferation of parental HT29 cells (Parent) and HT29 cells stably transduced with control shrna, sharpc3-1, sharpc3-2 or sharpc3-3. The quantity of viable cells is expressed relative to the quantity measured at 24 hours ± SEM (n = 3 independent experiments). n.s., no significant difference (Student s t-test).




14 Supplementary Figure 14 a b c d Supplementary Figure 14 Staining for CD31 in HT29 tumours treated with B and capecitabine in vivo a-d. HT29 tumors with normal ARPC3 levels (Control shrna) or ARPC3 knockdown (sharpc3-3) were established in the livers of mice and treated with B plus capecitabine (BC) or vehicle (Vh) alone. Liver specimens harvested after two weeks of treatment were stained for CK2 to label tumor cells and CD31 to label blood vessels. Representative images of the tumour-liver interface are shown for Control shrna tumors treated with Vh (a) or B/C (b) and for ARPC3 knockdown tumors treated with Vh (c) or BC (d). Dashed line in panels c and d indicates where the desmoplastic rim of the tumor meets the normal liver., normal liver. Scale bar, 6 μm.
15 cvessels per mm2 Supplementary Figure 15 a Mean HGP (%) ** ** ** ** b Lesion area (mm 2 ) 1 5 n.s. n.s n.s. n.s. R D P R D P R D P R D P Vh C Vh C Control shrna sharpc3-3 Vh Control shrna C Vh C Vh C Vh sharpc3-3 Control shrna C sharpc3-3 Supplementary Figure 15 Knockdown of ARPC3 does not effect tumor burden or tumor vessel density in mice treated with capecitabine alone a-c. Tumors with normal ARPC3 levels (Control shrna) or ARPC3 knockdown (sharpc3-3) were established in the livers of mice. Mice were then treated with capecitabine (C) or vehicle alone (Vh) for two weeks followed by histopathological analysis of the liver tumors (n = 8 mice per group). Graph in a shows the % HGP per group ± SEM. Graph in b shows liver tumor burden expressed in terms of lesion area ± SEM. Graph in c shows tumor vessel density in terms of vessels per mm 2 ± SEM. For statistical analysis, Mann Whitney U-test (panel a) or Student s t-test (panels b,c) were used. **P<.1. n.s., no significant difference.
16 Supplementary Figure 16 a Difference (A1-A2) b c Difference (A1-B1) Difference (B1-B2) Case number 5 1 Case number d Difference (A2-B2) Case number 5 1 Case number Supplementary Figure 16 Difference in % HGP scores between observers for the intra-observer and inter-observer agreement of HGP scoring Two observers scored the HGP (% replacement, % desmoplastic, % pushing) in 15 tissue sections of colorectal cancer liver metastasis. The graphs show the difference between the two % replacement scores for every case for the following comparisons: a. intra-observer agreement: observer A first score (A1) minus observer A second score (A2), b. intra-observer agreement: observer B first score (B1) minus observer B second score (B2), c. inter-observer agreement: observer A first score (A1) minus observer B first score (B1) and d. inter-observer agreement: observer A second score (A2) minus observer B second score (B2). Data points which lie on the red line indicate cases for which there was complete agreement between the two scores, whilst data points either side of the line are cases for which there was disagreement between the two scores.
17 Supplementary Figure 17 a b c d Difference (A1-A2) Difference (B1-B2) Difference (A1-B1) Difference (A2-B2) Average (A1+A2) / Average (B1+B2) / Average (A1+B1) / Average (A2+B2) / 2 Supplementary Figure 17 Bland-Altman plots for intra-observer and inter-observer agreement of HGP scoring Two observers scored the HGP (% replacement, % desmoplastic, % pushing) in 15 tissue sections of colorectal cancer liver metastasis. Bland-Altman plots show the difference between the two % replacement scores plotted against the average of the two % replacement scores for the following comparisons: a. Intra-observer agreement: observer A first score (A1) versus observer A second score (A2). Mean difference between scores (-.33) and limits of agreement ( to 7.497). b. Intra-observer agreement: observer B first score (B1) versus observer B second score (B2). Mean difference between scores (-.633) and limits of agreement ( to ). c. Inter-observer agreement: observer A first score (A1) versus observer B first score (B1). Mean difference between scores (-1.5) and limits of agreement ( to 19.88). d. Inter-observer agreement: observer A second score (A2) versus observer B second score (B2). Mean difference between scores (-2.167) and limits of agreement ( to 2.953). Bold dashed line indicates the mean difference between scores whilst the flanking dotted lines show the limits of agreement. Note: since a large proportion of the 15 data points in each graph have identical x and y co-ordinates, many of the data points depicted constitute multiple overlaping data points.
18 Supplementary Table 1 Characteristics of bev chemo treated CRC patients in the RM cohort Characteristics of 33 patients (n = 59 lesions) treated preoperatively with bev-chemo prior to liver resection at RM. Demographics Gender, number of patients (%) Male 21 (63.6) Female 12 (36.4) Age, median (range) 63 (29 79) Primary tumor Site of primary tumor, number of patients (%) Rectum Recto sigmoid Colon Lymph node status, number of patients (%) Positive Negative Histological grade, number of patients (%) High grade Low grade Adjuvant therapy, number of patients (%) Yes No Liver metastasis No. of liver lesions at presentation, number of patients (%) Solitary lesion Multiple lesions No. of liver lesions utilised for histopathological analysis per patient, number of patients (%) 1 lesion 2 lesions 3 lesions 4 lesions 7 (21.2) 14 (42.4) 12 (36.4) 26 (78.8) 7 (21.2) 4 (12.1) 29 (87.9) 1 (3.3) 23 (69.7) 11 (33.3) 22 (66.7) 17 (51.5) 1 (3.3) 2 (6.1) 4 (12.1) Baseline lesion size, median (range) 21 mm (5 11) Preoperative therapy administered, number of patients (%) CAPOX + bevacizumab FOLFOX + bevacizumab FOLFIRI + bevacizumab 21 (63.6) 5 (15.2) 7 (21.2) Cycles of preoperative therapy, median (range) 6 (4 12) Interval between last bevacizumab dose and resection, median (range) 76 days (41 362) Footnote: CAPOX, capecitabine and oxaliplatin; FOLFOX, infusional 5 fluorouracil and oxaliplatin; FOLFIRI, infusional 5 fluorouracil and irinotecan.
19 Supplementary Table 2 Univariate analysis of clinical characteristics associated with pathological response in RM patients treated preoperatively with bev chemo Analysis was performed using data for 59 lesions from 33 patients treated preoperatively with bev-chemo prior to liver resection (RM cohort). The χ 2 test was used to determine statistical significance. Variables Demographics Gender Male Female Age <6 years 6 years Primary tumor Site of primary tumor Rectum Recto sigmoid Colon Lymph node status Positive Negative Histological grade High grade Low grade Adjuvant therapy Yes No Liver metastasis No. of liver lesions at presentation Solitary Multiple Baseline lesion size <2 mm 2 mm Preoperative therapy administered CAPOX + bevacizumab FOLFOX + bevacizumab FOLFIRI + bevacizumab Cycles of preoperative therapy 6 cycles >6 cycles Interval between last bevacizumab dose and resection <7 days 7 days Total number of lesions Lesions with <25% viable tumor, no. (%) 12 (35.3) 1 (4) 6 (35.3) 16 (38.1) 4 (3.8) 8 (33.3) 1 (45.5) 19 (39.6) 3 (27.3) 5 (62.5) 17 (33.3) 4 (22.2) 18 (43.9) 5 (45.5) 17 (35.4) 11 (45.8) 11 (31.4) 16 (42.1) 2 (22.2) 4 (3.8) 16 (36.4) 6 (4.) 1 (41.7) 12 (34.3) P value Table continues overleaf
20 Supplementary Table 2 continued Variables Response measures Change in lesion size by RECIST PR SD or PD Morphological response on CT Yes (OR or PR) No (AR) Histopathological growth pattern Replacement HGP <25% 25% Replacement HGP <5% 5% Desmoplastic HGP <25% 25% Desmoplastic HGP <5% 5% Total number of lesions Lesions with <25% viable tumor, no (%) 15 (44.1) 7 (28.) 11 (57.9) 1 (3.3) 2 (71.4) 2 (6.5) 21 (65.6) 1 (3.7) () 22 (64.7) 1 (3.6) 21 (67.7) P value <.1 <.1 <.1 <.1 Footnote: CAPOX, capecitabine and oxaliplatin; FOLFOX, infusional 5 fluorouracil and oxaliplatin; FOLFIRI, infusional 5 fluorouracil and irinotecan; N/A, data not available.
21 Supplementary Table 3 Characteristics of bev chemo treated CRC patients in the MUHC cohort Characteristics of 59 patients (n = 128 lesions) treated preoperatively with bev-chemo at MUHC. Demographics Gender, number of patients (%) Male 35 (59.3) Female 24 (4.7) Age, median (range) 63 (3 85) Primary tumor Site of primary tumor, number of patients (%) Rectum Recto sigmoid Colon Lymph node status, number of patients (%) Positive Negative N/A Histological grade, number of patients (%) High grade Low grade N/A Adjuvant therapy, number of patients (%) Yes No N/A Liver metastasis No. of liver lesions at presentation, number of patients (%) Solitary lesion Multiple lesions No. of liver lesions utilised for histopathological analysis per patient, number of patients (%) 1 lesion 2 lesions 3 lesions 4 lesions 5 lesions 6 lesions 8 lesions 12 lesions 11 (18.6) 9 (15.3) 39 (66.1) 32 (54.2) 8 (13.6) 19 (32.2) 4 (6.8) 36 (61.) 19 (32.2) 12 (2.3) 46 (78.) 1 (1.7) 18 (3.5) 41 (69.5) 29 (49.2) 15 (25.4) 7 (11.8) 3 (5.1) 2 (3.4) 1 (1.7) 1 (1.7) 1 (1.7) Baseline lesion size, median (range) 26 (5 19)* Preoperative therapy administered, number of patients (%) FOLFOX + bevacizumab FOLFIRI + bevacizumab 47 (79.7) 12 (2.3) Cycles of preoperative therapy, median (range) 6 (2 13) Interval between last bevacizumab dose and resection, median (range) 64 (23 237) Footnote: FOLFOX, infusional 5 fluorouracil and oxaliplatin; FOLFIRI, infusional 5 fluorouracil and irinotecan; N/A, data not available. *Information on baseline lesion size was available for 113 out of 128 lesions.
22 Supplementary Table 4 Univariate analysis of clinical characteristics associated with pathological response in MUHC patients treated preoperatively with bev chemo Analysis was performed using data for 128 lesions from 59 patients treated preoperatively with bev-chemo prior to liver resection (MUHC cohort). The χ 2 test was used to determine statistical significance. Variables Demographic Gender Male Female Age <6 years 6 years Primary tumor Site of primary tumor Rectum Recto sigmoid Colon Lymph node status Positive Negative Histological grade High grade Low grade Adjuvant therapy Yes No Liver metastasis No. of liver lesions at presentation Solitary Multiple Baseline lesion size <2 mm 2 mm Preoperative therapy administered FOLFOX + bevacizumab FOLFIRI + bevacizumab Cycles of preoperative therapy 6 cycles >6 cycles Interval between last bevacizumab dose and resection <7 days 7 days Total number of lesions Lesions with <25% viable tumor, no. (%) 29 (32.9) 17 (42.5) 18 (34.) 28 (37.3) 5 (23.8) 8 (57.1) 33 (35.5) 2 (3.3) 7 (63.6) 1 (16.7) 28 (38.9) 6 (25) 4 (38.8) 7 (38.9) 39 (35.4) 13 (32.5) 29 (39.7) 42 (38.9) 4 (2.) 37 (43) 9 (21.4) 22 (37.9) 24 (34.3) P value Table continues overleaf
23 Supplementary Table 4 continued Variables Response measures Change in lesion size by RECIST PR SD or PD Histopathological growth pattern Replacement HGP <25% 25% Replacement HGP <5% 5% Desmoplastic HGP <25% 25% Desmoplastic HGP <5% 5% Total number of lesions Lesions with <25% viable tumor, no (%) 22 (5) 2 (29) 34 (56.7) 23 (17.7) 4 (57.1) 6 (1.3) 2 (4.2) 44 (55) 6 (9.7) 4 (6.6) P value.24 <.1 <.1 <.1 <.1 Footnote: FOLFOX, infusional 5 fluorouracil and oxaliplatin; FOLFIRI, infusional 5 fluorouracil and irinotecan; N/A, data not available.
24 Supplementary Table 5 Univariate and multivariate analysis of clinical characteristics associated with pathological response in lesions treated preoperatively with bev chemo Data from patients that received preoperative therapy with bev chemo were used to determine clinical variables associated with a good pathological response (lesions were pooled from RM and MUHC). Only lesions with 5% replacement HGP (85 lesions) or 5% desmoplastic HGP (96 lesions) were included. Lesions with 5% pushing HGP were excluded (6 lesions). The final analysis was therefore performed on 181 lesions from 9 patients. Both the univariate analysis and the multivariate analysis were performed using a generalized estimating equation. Only 5 variables that met a pre defined threshold of P<.25 in the univariate analysis were included in the subsequent multivariate analysis. Univariate analysis Multivariate analysis Demographics Gender Male Female Age <6 years 6 years Primary tumour Site of primary tumor Rectum Colon / recto sigmoid Lymph node status Positive Negative Histological grade High grade Low grade Adjuvant therapy Yes No Liver metastasis Number of lesions at presentation Solitary Multiple Baseline lesion size <2 mm 2 mm Preoperative therapy administered CAPOX + bev / FOLFOX + bev FOLFIRI + bev Cycles of preoperative therapy 6 cycles >6 cycles Interval between last bevacizumab dose and resection <7 days 7 days HGP 5% replacement 5% desmoplastic OR (95% CI) P value OR (95% CI) P value.83 (.69 1.) 1.21 ( ) 1.3 ( ).97 ( ).91 ( ) 1.1 ( ).68 ( ) 1.47 ( ) 1.16 ( ).86 ( ).85 (.7 1.3) 1.17 ( ) 1.7 ( ).93 ( ).99 ( ) 1.1 (.5 2.4) 2.9 ( ).48 ( ) 2.3 ( ).49 ( ) 1.41 ( ).71 ( ).7 (.3.16) 15.6 ( ).57.8 (.32 2.) 1.25 ( ) ( ) 2.7 ( ) ( ).88 ( ) ( ).57 ( ) <.1.6 (.3.15) ( ) <.1 Footnote: For every variable tested, we present the odds ratio in both directions e.g. male vs female (OR=.83) and its reverse, female vs male (OR=1.21), etc. bev, bevacizumab; CAPOX, capecitabine and oxaliplatin; FOLFOX, infusional 5 fluorouracil and oxaliplatin; FOLFIRI, infusional 5 fluorouracil and irinotecan.
25 Supplementary Table 6 Characteristics of MUHC patients that presented with new CRC liver metastases after bev chemo treatment was initiated (new CRCLMs) Demographics Gender, number of patients (%) Male 9 (69.2) Female 4 (3.8) Age, median (range) 65 (46 78) Primary tumor Site of primary tumor, number of patients (%) Rectum Recto sigmoid Colon Lymph node status, number of patients (%) Positive Negative N/A Histological grade, number of patients (%) High grade Low grade N/A Adjuvant therapy, number of patients (%) Yes No Liver metastasis Quantity of liver lesions present when treatment started, number of patients (%) No lesion* Solitary lesion Multiple lesions Quantity of new liver lesions presenting after treatment started, number of patients (%) Solitary lesion Multiple lesions No. of liver lesions utilised for histopathological analysis per patient, number of patients (%) 1 lesion 2 lesions 3 lesions 5 lesions 14 lesions Preoperative therapy administered, number of patients (%) FOLFOX + bevacizumab FOLFIRI + bevacizumab 2 (15.4) 3 (23.1) 8 (61.5) 1 (76.9) 3 (23.1) 2 (15.4) 8 (61.5) 3 (23.1) 4 (3.8) 9 (69.2) 2 (15.4) 2 (15.4) 9 (69.2) 7 (53.8) 6 (46.2) 7 (53.8) 3 (23.1) 1(7.7) 1 (7.7) 1 (7.7) 9 (69.2) 4 (3.8) Cycles of preoperative therapy, median (range) 6 (5 12) Interval between last bevacizumab dose and resection, median (range) 67 days (43 126) Footnote: *Two patients were administered bev-chemo prior to detection of liver metastases: one patient was receiving adjuvant bev-chemo when liver disease was detected and a second patient was receiving bev-chemo for CRC lung metastasis when liver disease was detected. bev, bevacizumab; CAPOX, capecitabine and oxaliplatin; FOLFOX, infusional 5 fluorouracil and oxaliplatin; FOLFIRI, infusional 5 fluorouracil and irinotecan. N/A, data not available.
26 Supplementary Table 7 Characteristics of MUHC patients that received no preoperative therapy prior to resection of CRC liver metastases (untreated CRCLMs) Demographics Gender, number of patients (%) Male 11 (57.9) Female 8 (42.1) Age, median (range) 7 (33 8) Primary tumor Site of primary tumor, number of patients (%) Rectum Recto sigmoid Colon Lymph node status, number of patients (%) Positive Negative N/A Histological grade, number of patients (%) High grade Low grade N/A Adjuvant therapy, number of patients (%) Yes* No (completely chemonaive) Baseline features of the liver metastases No. of liver lesions at presentation, number of patients (%) Solitary lesion Multiple lesions No. of liver lesions utilised for histopathological analysis per patient, number of patients (%) 1 lesion 2 lesions 4 lesions 6 lesions 5 (26.3) 1 (5.3) 13 (68.4) 1 (52.6) 5 (26.3) 4 (21.1) 1 (5.3) 1 (52.6) 8 (42.1) 4 (21.1) 15 (78.9) 12 (63.2) 7 (36.8) 12 (61.1) 5 (26.3) 1 (5.3) 1 (5.3) Baseline lesion size, median (range) 13.5 mm (4 77) Footnote: *patients were only included if the last dose of adjuvant therapy was administered 365 days prior to diagnosis of liver metastasis (median interval between last dose of adjuvant therapy and diagnosis of liver metastasis in these 4 patients was 1161 days, range was days). Adjuvant therapy consisted of chemotherapy only and no patients received adjuvant bevacizumab. N/A, data not available.
27 Supplementary Table 8 Univariate and multivariate analysis of clinical characteristics associated with overall survival in patients treated preoperatively with bev chemo Data from patients that received preoperative therapy with bev chemo at MUHC were used to determine clinical variables associated with overall survival. Only patients in the predominant replacement subgroup (26 patients) or the predominant desmoplastic subgroup (35 patients) were included in the analysis. The predominant pushing subgroup (1 patient) was excluded from the analysis. The final analysis was therefore performed on 61 patients. Both the univariate analysis and the multivariate analysis were performed using Cox proportional hazards regression. Only 2 variables that met a pre defined threshold of P<.25 in the univariate analysis were included in the subsequent multivariate analysis. Univariate analysis Multivariate analysis Demographics Gender Male Female Age <6 years 6 years Primary tumour Site of primary tumor Rectum Colon / recto sigmoid Lymph node status Positive Negative Histological grade High grade Low grade Adjuvant therapy Yes No Liver metastasis Number of lesions at presentation Solitary Multiple Mean baseline lesion size <2 mm 2 mm Preoperative therapy administered CAPOX+bev / FOLFOX+bev FOLFIRI+bev Cycles of preoperative therapy 6 cycles >6 cycles Interval between last bevacizumab dose and resection <7 days 7 days HGP 5% replacement 5% desmoplastic HR (95% CI) P value HR (95% CI) P value 1.14 ( ).88 ( ) 1.8 ( ).93 ( ) 1.28 ( ).78 ( ).72 ( ) 1.38 ( ) 1.25 ( ).8 ( ) 1.5 ( ).95 ( ).41 ( ) 2.44 ( ) 1.63 ( ).61 ( ).91 ( ) 1.1 ( ).67 ( ) 1.49 ( ) 1.3 ( ).97 ( ).29 (.12.67) 3.5 ( ) ( ) 1.96 ( ) (.14.8) 3.3 ( ).135 Footnote: For each variable tested, we present the odds ratio in both directions e.g. male vs female (HR=1.14) and its reverse, female vs male (HR=.88), etc. bev, bevacizumab; CAPOX, capecitabine and oxaliplatin; FOLFOX, infusional 5 fluorouracil and oxaliplatin; FOLFIRI, infusional 5 fluorouracil and irinotecan.
28 Supplementary Table 9 Analysis for differences in characteristics between patients with a predominant replacement HGP and patients with a predominant desmoplastic HGP Analysis was performed on 89 patients from MUHC that received preoperative therapy with bev chemo or chemotherapy alone. Clinical characteristics were compared between 38 predominant replacement HGP patients and 51 predominant desmoplastic HGP patients. The χ 2 test was used to determine statistical significance. Demographics Gender Male Female Age <6 years 6 years Primary tumour Primary tumour site Rectum Recto sigmoid Colon Lymph nodes Positive Negative Histological grade High grade Low grade Treated with adjuvant therapy Yes No Liver metastasis Number of lesions at presentation No lesion* Solitary lesion Multiple lesions Mean baseline lesion size <2 mm 2 mm Therapy administered FOLFOX FOLFIRI FOLFIRINOX 5 FU FOLFOX + bev FOLFIRI + bev Total number of patients Number of replacement patients (%) 28 (5) 1 (3.3) 15 (42.9) 23 (42.6) 7 (35) 9 (52.9) 22 (68.8) 2 (45.5) 5 (35.7) 4 (66.7) 2 (36.4) 8 (5) 3 (41.7) 3 (1) 8 (29.6) 27 (45.8) 9 (36) 23 (41.1) 11 (45.8) () 1 (5) 19 (38.8) 7 (58.3) Number of desmoplastic patients (%) 28 (5) 23 (69.7) 2 (57.1) 31 (57.4) 13 (65) 8 (47.1) 1 (31.2) 24 (54.5) 9 (64.3) 2 (33.3) 35 (63.6) 8 (5) 42 (58.3) () 19 (7.4) 32 (54.2) 16 (64) 33 (58.9) 13 (54.2) 1 (1) 1 (5) 1 (1) 3 (61.2) 5 (41.7) P value Table continues overleaf
29 Supplementary Table 9 continued Cycles of preoperative therapy 6 cycles >6 cycles Interval between last therapy dose and resection <7 days 7 days (41.9) 12 (44.4) 15 (31.9) 21 (55.3) 36 (58.1) 15 (55.6) 32 (68.1) 17 (44.7) Footnote: *Three patients were administered therapy prior to detection of liver metastases: one patient was receiving adjuvant bev-chemo when liver disease was detected, one patient was receiving bev-chemo for CRC lung metastasis when liver disease was detected and one patient was receiving adjuvant chemotherapy alone when liver disease was detected. FOLFOX, infusional 5 fluorouracil and oxaliplatin; FOLFIRI, infusional 5 fluorouracil and irinotecan; FOLFIRINOX, infusional 5 fluorouracil and irinotecan and oxaliplatin; 5 FU, infusional 5 FU only.
30 Supplementary Table 1 Analysis for differences in characteristics between patients that received bev chemo and patients that received chemotherapy alone Analysis was performed on 91 patients from MUHC. Clinical characteristics were compared between 62 patients that received pre operative bev chemo and 29 patients that received preoperative chemotherapy only). The χ 2 test was used to determine statistical significance. Demographics Gender Male Female Age <6 years 6 years Primary tumor Primary tumour site Rectum Recto sigmoid Colon Lymph nodes Positive Negative Histological grade High grade Low grade Treated with adjuvant therapy Yes No Liver metastases Number of lesions at presentation No lesion* Solitary lesion Multiple lesions Mean baseline lesion size <2 mm 2 mm Therapy administered FOLFOX FOLFIRI FOLFIRINOX 5 FU Total number of patients Number of bev chemo patients (%) 37 (64.9) 25 (73.5) 25 (69.4) 37 (67.3) 12 (57.1) 1 (58.8) 4 (75.5) 35 (77.8) 8 (57.1) 5 (83.3) 38 (69.1) 13 (72.2) 48 (66.7) 2 (5) 18 (66.7) 42 (7) 14 (56) 41 (73.2) 5 (66.7) 12 (92.3) () () Number of chemo alone patients (%) 2 (35.1) 9 (26.5) 11 (3.6) 18 (32.7) 9 (42.9) 7 (41.2) 13 (24.5) 1 (22.2) 6 (42.9) 1 (16.7) 17 (3.9) 5 (27.8) 24 (33.3) 2 (5) 9 (33.3) 18 (3) 11 (44) 15 (26.8) 25 (33.3) 1 (7.7) 2 (1) 1 (1) P value Table continues overleaf
31 Supplementary Table 1 continued Cycles of preoperative therapy 6 cycles >6 cycles Interval between last therapy dose & resection <7 days 7 days (65.1) 21 (75) 35 (72.9) 26 (66.7) 22 (34.9) 7 (25) 13 (27.1) 13 (33.3) Footnote: *Four patients were administered therapy prior to detection of liver metastases: one patient was receiving adjuvant bev chemo when liver disease was detected, one patient was receiving bev chemo for CRC lung metastasis when liver disease was detected and two patients were receiving adjuvant chemotherapy alone when liver disease was detected. FOLFOX, infusional 5 fluorouracil and oxaliplatin; FOLFIRI, infusional 5 fluorouracil and irinotecan; FOLFIRINOX, infusional 5 fluorouracil and irinotecan and oxaliplatin; infusional 5 FU.
32 Supplementary Table 11 Characteristics of 17 patients from whom samples of breast cancer liver metastasis were obtained Details of primary Age at diagnosis of primary breast cancer, median (range) 47 (36 77) Primary was resected, number of patients (%) Yes No Ductal or lobular histology, number of patients (%) Ductal Lobular Mixed T stage, number of patients (%) T1 T2 T3 T4 N/A Lymph nodes, number of patients (%) Positive Negative N/A Treatment received prior to obtaining liver metastasis sample Form of treatment received, number of patients (%) Endocrine therapy Chemotherapy Herceptin Everolimus Iressa Zometa 15 (88.2) 2 (11.8) 13 (76.5) 3 (17.6) 1 (5.9) 6 (35.3) 6 (35.3) 2 (11.8) 1 (5.9) 2 (11.8) 9 (52.9) 6 (35.3) 2 (11.8) 14 (82.4) 12 (7.6) 2 (11.8) 1 (5.9) 1 (5.9) 1 (5.9) Details of liver metastasis sample Age when sample was obtained, median (range) 54 (43 81) Source of material, number of patients (%) Resection Autopsy Intrinsic subtype, number of patients (%) Luminal A Luminal B HER2 negative Luminal B HER2 positive HER2 positive (non luminal) Triple negative Footnote: N/A, data not available. 11 (64.7) 6 (35.3) 5 (29.4) 5 (29.4) 3 (17.7) () 4 (23.5)
33 Supplementary Table 12 Results of the intra and inter observer agreement study for scoring the HGPs of liver metastases Measurement of intra observer agreement for HGP scoring Comparison Correlation co efficient Mean difference Observer A (1st score) versus Observer A (2nd score) Observer B (1st score) versus Observer B (2nd score) Limits of agreement ( to 7.497) ( to ) Measurement of inter observer agreement for HGP scoring Comparison Correlation co efficient Mean difference Observer A (1st score) versus Observer B (1st score) Observer A (2nd score) versus Observer B (2nd score) Limits of agreement ( to 19.88) ( to 2.953) Supplementary Table 13 Criteria for scoring the intrinsic subtypes of breast cancer Intrinsic subtype Luminal A Luminal B HER2 negative Luminal B HER2 positive HER2 positive (non luminal) Triple negative Criteria ER and PgR positive HER2 negative Ki67 low ER positive HER2 negative Ki67 high ER positive HER2 positive Any Ki67 Any PgR HER2 positive ER and PgR absent ER negative PgR negative HER2 negative Footnote: Table was adapted from: Goldhirsch, A., et al. Personalizing the treatment of women with early breast cancer: highlights of the St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 213. Ann Oncol 24, (213). ER, estrogen receptor; PgR, progesterone receptor.
Vessel co-option mediates resistance to anti-angiogenic therapy in liver metastases
 A r t i c l e s Vessel co-option mediates resistance to anti-angiogenic therapy in liver metastases 216 Nature America, Inc., part of Springer Nature. All rights reserved. Sophia Frentzas 1,2,11, Eve Simoneau
A r t i c l e s Vessel co-option mediates resistance to anti-angiogenic therapy in liver metastases 216 Nature America, Inc., part of Springer Nature. All rights reserved. Sophia Frentzas 1,2,11, Eve Simoneau
Prognostic significance of stroma tumorinfiltrating lymphocytes according to molecular subtypes of breast cancer
 Prognostic significance of stroma tumorinfiltrating lymphocytes according to molecular subtypes of breast cancer Hee Jung Kwon, Nuri Jang, Min Hui Park, Young Kyung Bae Department of Pathology, Yeungnam
Prognostic significance of stroma tumorinfiltrating lymphocytes according to molecular subtypes of breast cancer Hee Jung Kwon, Nuri Jang, Min Hui Park, Young Kyung Bae Department of Pathology, Yeungnam
Indeterminate Pulmonary Nodules in Patients with Colorectal Cancer
 Indeterminate Pulmonary Nodules in Patients with Colorectal Cancer Jai Sule 1, Kah Wai Cheong 2, Stella Bee 2, Bettina Lieske 2,3 1 Dept of Cardiothoracic and Vascular Surgery, University Surgical Cluster,
Indeterminate Pulmonary Nodules in Patients with Colorectal Cancer Jai Sule 1, Kah Wai Cheong 2, Stella Bee 2, Bettina Lieske 2,3 1 Dept of Cardiothoracic and Vascular Surgery, University Surgical Cluster,
Surgical Management of Metastatic Colon Cancer: analysis of the Surveillance, Epidemiology and End Results (SEER) database
 database") Surgical Management of Metastatic Colon Cancer: analysis of the Surveillance, Epidemiology and End Results (SEER) database Hadi Khan, MD 1, Adam J. Olszewski, MD 2 and Ponnandai S. Somasundar, MD 1 1 Department
Surgical Management of Metastatic Colon Cancer: analysis of the Surveillance, Epidemiology and End Results (SEER) database Hadi Khan, MD 1, Adam J. Olszewski, MD 2 and Ponnandai S. Somasundar, MD 1 1 Department
Breast cancer: Molecular STAGING classification and testing. Korourian A : AP,CP ; MD,PHD(Molecular medicine)
") Breast cancer: Molecular STAGING classification and testing Korourian A : AP,CP ; MD,PHD(Molecular medicine) Breast Cancer Theory: Halsted Operative breast cancer is a local-regional disease The positive
Breast cancer: Molecular STAGING classification and testing Korourian A : AP,CP ; MD,PHD(Molecular medicine) Breast Cancer Theory: Halsted Operative breast cancer is a local-regional disease The positive
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan
 State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
Chemotherapy for resectable liver mets: Options and Issues. Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA
 Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Colorectal Cancer Therapy and Associated Toxicity
 Colorectal Cancer Therapy and Associated Toxicity Mountain States Cancer Conference November 6, 2010 Colin D. Weekes, M.D., Ph.D Assistant Professor University of Colorado GI Cancers Are Common 2009 Estimated
Colorectal Cancer Therapy and Associated Toxicity Mountain States Cancer Conference November 6, 2010 Colin D. Weekes, M.D., Ph.D Assistant Professor University of Colorado GI Cancers Are Common 2009 Estimated
Implications of Progesterone Receptor Status for the Biology and Prognosis of Breast Cancers
 日大医誌 75 (1): 10 15 (2016) 10 Original Article Implications of Progesterone Receptor Status for the Biology and Prognosis of Breast Cancers Naotaka Uchida 1), Yasuki Matsui 1), Takeshi Notsu 1) and Manabu
日大医誌 75 (1): 10 15 (2016) 10 Original Article Implications of Progesterone Receptor Status for the Biology and Prognosis of Breast Cancers Naotaka Uchida 1), Yasuki Matsui 1), Takeshi Notsu 1) and Manabu
Supplementary Fig. 1: ATM is phosphorylated in HER2 breast cancer cell lines. (A) ATM is phosphorylated in SKBR3 cells depending on ATM and HER2
 ATM is phosphorylated in SKBR3 cells depending on ATM and HER2") Supplementary Fig. 1: ATM is phosphorylated in HER2 breast cancer cell lines. (A) ATM is phosphorylated in SKBR3 cells depending on ATM and HER2 activity. Upper panel: Representative histograms for FACS
Supplementary Fig. 1: ATM is phosphorylated in HER2 breast cancer cell lines. (A) ATM is phosphorylated in SKBR3 cells depending on ATM and HER2 activity. Upper panel: Representative histograms for FACS
Breast cancer in elderly patients (70 years and older): The University of Tennessee Medical Center at Knoxville 10 year experience
: The University of Tennessee Medical Center at Knoxville 10 year experience") Breast cancer in elderly patients (70 years and older): The University of Tennessee Medical Center at Knoxville 10 year experience Curzon M, Curzon C, Heidel RE, Desai P, McLoughlin J, Panella T, Bell
Breast cancer in elderly patients (70 years and older): The University of Tennessee Medical Center at Knoxville 10 year experience Curzon M, Curzon C, Heidel RE, Desai P, McLoughlin J, Panella T, Bell
Cover Page. The handle holds various files of this Leiden University dissertation
 Cover Page The handle http://hdl.handle.net/1887/55957 holds various files of this Leiden University dissertation Author: Dekker T.J.A. Title: Optimizing breast cancer survival models based on conventional
Cover Page The handle http://hdl.handle.net/1887/55957 holds various files of this Leiden University dissertation Author: Dekker T.J.A. Title: Optimizing breast cancer survival models based on conventional
Contemporary Classification of Breast Cancer
 Contemporary Classification of Breast Cancer Laura C. Collins, M.D. Vice Chair of Anatomic Pathology Professor of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Outline
Contemporary Classification of Breast Cancer Laura C. Collins, M.D. Vice Chair of Anatomic Pathology Professor of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Outline
Molecular in vitro diagnostic test for the quantitative detection of the mrna expression of ERBB2, ESR1, PGR and MKI67 in breast cancer tissue.
 Innovation for your breast cancer diagnostics PGR G ATA G C G A C G AT C G A A A G A A G T TA G ATA G C G A C G AT C G A A A G A A G T TA G ATA G C G A C G AT C G A A A G A A G T TA G ATA G C G A C ERBB2
Innovation for your breast cancer diagnostics PGR G ATA G C G A C G AT C G A A A G A A G T TA G ATA G C G A C G AT C G A A A G A A G T TA G ATA G C G A C G AT C G A A A G A A G T TA G ATA G C G A C ERBB2
COLORECTAL CANCER 44
 COLORECTAL CANCER 44 Colorectal Cancer Highlights from the 2009 Annual Meeting of the American Society of Clinical Oncology Edited by Stuart M. Lichtman, MD Memorial Sloan-Kettering Cancer Center Commack,
COLORECTAL CANCER 44 Colorectal Cancer Highlights from the 2009 Annual Meeting of the American Society of Clinical Oncology Edited by Stuart M. Lichtman, MD Memorial Sloan-Kettering Cancer Center Commack,
UK Interdisciplinary Breast Cancer Symposium. Should lobular phenotype be considered when deciding treatment? Michael J Kerin
 UK Interdisciplinary Breast Cancer Symposium Should lobular phenotype be considered when deciding treatment? Michael J Kerin Professor of Surgery National University of Ireland, Galway and Galway University
UK Interdisciplinary Breast Cancer Symposium Should lobular phenotype be considered when deciding treatment? Michael J Kerin Professor of Surgery National University of Ireland, Galway and Galway University
Molecular in vitro diagnostic test for the quantitative detection of the mrna expression of ERBB2, ESR1, PGR and MKI67 in breast cancer tissue.
 Innovation for your breast cancer diagnostics Now valid ated on: -Roche cob as z 480 A nalyzer -Roche L ightcycle r 480 II - ABI 750 0 Fast -Versant kpcr Cyc ler PGR ESR1 MKI67 Molecular in vitro diagnostic
Innovation for your breast cancer diagnostics Now valid ated on: -Roche cob as z 480 A nalyzer -Roche L ightcycle r 480 II - ABI 750 0 Fast -Versant kpcr Cyc ler PGR ESR1 MKI67 Molecular in vitro diagnostic
Only Estrogen receptor positive is not enough to predict the prognosis of breast cancer
 Young Investigator Award, Global Breast Cancer Conference 2018 Only Estrogen receptor positive is not enough to predict the prognosis of breast cancer ㅑ Running head: Revisiting estrogen positive tumors
Young Investigator Award, Global Breast Cancer Conference 2018 Only Estrogen receptor positive is not enough to predict the prognosis of breast cancer ㅑ Running head: Revisiting estrogen positive tumors
Locally Advanced Colon Cancer. Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery
 Locally Advanced Colon Cancer Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery Case 34 yo man presented with severe RLQ abdominal pain X 24 hrs. No nausea/vomiting/fever. + flatus.
Locally Advanced Colon Cancer Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery Case 34 yo man presented with severe RLQ abdominal pain X 24 hrs. No nausea/vomiting/fever. + flatus.
Supplementary Figure 1. Double-staining immunofluorescence analysis of invasive colon and breast cancers. Specimens from invasive ductal breast
 Supplementary Figure 1. Double-staining immunofluorescence analysis of invasive colon and breast cancers. Specimens from invasive ductal breast carcinoma (a) and colon adenocarcinoma (b) were staining
Supplementary Figure 1. Double-staining immunofluorescence analysis of invasive colon and breast cancers. Specimens from invasive ductal breast carcinoma (a) and colon adenocarcinoma (b) were staining
Supplementary Figures
 Supplementary Figures Supplementary Figure 1 DOT1L regulates the expression of epithelial and mesenchymal markers. (a) The expression levels and cellular localizations of EMT markers were confirmed by
Supplementary Figures Supplementary Figure 1 DOT1L regulates the expression of epithelial and mesenchymal markers. (a) The expression levels and cellular localizations of EMT markers were confirmed by
RNA preparation from extracted paraffin cores:
 Supplementary methods, Nielsen et al., A comparison of PAM50 intrinsic subtyping with immunohistochemistry and clinical prognostic factors in tamoxifen-treated estrogen receptor positive breast cancer.
Supplementary methods, Nielsen et al., A comparison of PAM50 intrinsic subtyping with immunohistochemistry and clinical prognostic factors in tamoxifen-treated estrogen receptor positive breast cancer.
Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS
 Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS Survival Rates of by Stage of Adenocarcinoma of the Colon Liver Resection New Perspective Colorectal cancer liver
Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS Survival Rates of by Stage of Adenocarcinoma of the Colon Liver Resection New Perspective Colorectal cancer liver
Management Of Patients With Metastatic Colorectal Cancer in Lebanese Hospitals and Associated Direct Cost: A Multicenter Cohort Study
 Management Of Patients With Metastatic Colorectal Cancer in Lebanese Hospitals and Associated Direct Cost: A Multicenter Cohort Study Henaine AM; Chahine G; Massoud M; Salameh P; Awada S; Lahoud N; El
Management Of Patients With Metastatic Colorectal Cancer in Lebanese Hospitals and Associated Direct Cost: A Multicenter Cohort Study Henaine AM; Chahine G; Massoud M; Salameh P; Awada S; Lahoud N; El
Targeted Therapies in Metastatic Colorectal Cancer: An Update
 Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
MammaPrint, the story of the 70-gene profile
 MammaPrint, the story of the 70-gene profile René Bernards Professor of Molecular Carcinogenesis The Netherlands Cancer Institute Amsterdam Chief Scientific Officer Agendia Amsterdam The breast cancer
MammaPrint, the story of the 70-gene profile René Bernards Professor of Molecular Carcinogenesis The Netherlands Cancer Institute Amsterdam Chief Scientific Officer Agendia Amsterdam The breast cancer
Adjuvant endocrine therapy (essentials in ER positive early breast cancer)
") Adjuvant endocrine therapy (essentials in ER positive early breast cancer) Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Experimental Therapeutics Outline Picking optimal adjuvant endocrine
Adjuvant endocrine therapy (essentials in ER positive early breast cancer) Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Experimental Therapeutics Outline Picking optimal adjuvant endocrine
COLORECTAL CANCER CASES
 COLORECTAL CANCER CASES Case #1 Case #2 Colorectal Cancer Case 1 A 52 year-old female attends her family physician for her yearly complete physical examination. Her past medical history is significant
COLORECTAL CANCER CASES Case #1 Case #2 Colorectal Cancer Case 1 A 52 year-old female attends her family physician for her yearly complete physical examination. Her past medical history is significant
Multigene Testing in NCCN Breast Cancer Treatment Guidelines, v1.2011
 Multigene Testing in NCCN Breast Cancer Treatment Guidelines, v1.2011 Robert W. Carlson, M.D. Professor of Medicine Stanford University Chair, NCCN Breast Cancer Treatment Guidelines Panel Selection of
Multigene Testing in NCCN Breast Cancer Treatment Guidelines, v1.2011 Robert W. Carlson, M.D. Professor of Medicine Stanford University Chair, NCCN Breast Cancer Treatment Guidelines Panel Selection of
Layered-IHC (L-IHC): A novel and robust approach to multiplexed immunohistochemistry So many markers and so little tissue
: A novel and robust approach to multiplexed immunohistochemistry So many markers and so little tissue") Page 1 The need for multiplex detection of tissue biomarkers. There is a constant and growing demand for increased biomarker analysis in human tissue specimens. Analysis of tissue biomarkers is key to
Page 1 The need for multiplex detection of tissue biomarkers. There is a constant and growing demand for increased biomarker analysis in human tissue specimens. Analysis of tissue biomarkers is key to
Advances in Chemotherapy of Colorectal Cancer
 Advances in Chemotherapy of Colorectal Cancer Richard M. Goldberg Lineberger Comprehensive Cancer Center University of North Carolina at Chapel Hill Disease Settings Adjuvant Therapy MOSAIC, FOLFOX Andre
Advances in Chemotherapy of Colorectal Cancer Richard M. Goldberg Lineberger Comprehensive Cancer Center University of North Carolina at Chapel Hill Disease Settings Adjuvant Therapy MOSAIC, FOLFOX Andre
Breast Cancer: ASCO Poster Review
 Breast Cancer: ASCO Poster Review Carmen Criscitiello, MD, PhD Istituto Europeo di Oncologia Milano HER2+ SUBTYPE Research questions in early HER2+ BC De-escalation of toxicity without compromising efficacy
Breast Cancer: ASCO Poster Review Carmen Criscitiello, MD, PhD Istituto Europeo di Oncologia Milano HER2+ SUBTYPE Research questions in early HER2+ BC De-escalation of toxicity without compromising efficacy
Behandeling van colorectale levermetastasen. Rol van beeldvorming van de lever bij colorectaal carcinoom
 Behandeling van colorectale levermetastasen Rol van beeldvorming van de lever bij colorectaal carcinoom B. Op de Beeck Universitair Ziekenhuis Antwerpen bart.op.de.beeck@uza.be 10.12.2016 AZ Turnhout campus
Behandeling van colorectale levermetastasen Rol van beeldvorming van de lever bij colorectaal carcinoom B. Op de Beeck Universitair Ziekenhuis Antwerpen bart.op.de.beeck@uza.be 10.12.2016 AZ Turnhout campus
Controversies in Breast Pathology ELENA PROVENZANO ADDENBROOKES HOSPITAL, CAMBRIDGE
 Controversies in Breast Pathology ELENA PROVENZANO ADDENBROOKES HOSPITAL, CAMBRIDGE Neoadjuvant Chemotherapy Indications: Management of locally advanced invasive breast cancers including inflammatory breast
Controversies in Breast Pathology ELENA PROVENZANO ADDENBROOKES HOSPITAL, CAMBRIDGE Neoadjuvant Chemotherapy Indications: Management of locally advanced invasive breast cancers including inflammatory breast
SUPPLEMENTARY INFORMATION
 DOI: 10.1038/ncb3021 Supplementary figure 1 Characterisation of TIMPless fibroblasts. a) Relative gene expression of TIMPs1-4 by real time quantitative PCR (RT-qPCR) in WT or ΔTimp fibroblasts (mean ±
DOI: 10.1038/ncb3021 Supplementary figure 1 Characterisation of TIMPless fibroblasts. a) Relative gene expression of TIMPs1-4 by real time quantitative PCR (RT-qPCR) in WT or ΔTimp fibroblasts (mean ±
What s New in Colon Cancer? Therapy over the last decade
 What s New in Colon Cancer? 9/19/2014 Michael McNamara, MD Therapy over the last decade Cytotoxic chemotherapy - 5FU ( Mayo, Roswell, Infusional) - Xeloda (01 ) - Oxaliplatin (02 ) - Irinotecan (96 ) Anti-
What s New in Colon Cancer? 9/19/2014 Michael McNamara, MD Therapy over the last decade Cytotoxic chemotherapy - 5FU ( Mayo, Roswell, Infusional) - Xeloda (01 ) - Oxaliplatin (02 ) - Irinotecan (96 ) Anti-
Supplemental Figures. Amylase. Glucose. Pancreas FAP-WT FAP-KO weight (g) mg/dl U/L 0.
 mg/dl U/L 0.") Supplemental Figures A.2 3.1 2 2 1 1.5. 3 U/L 4 mg/dl weight (g).25.15 Amylase Glucose Pancreas B Trichrome HABP PAS H&E Supplemental Figure 1. FAP is dispensable for pancreatic development. (A) The pancreas
Supplemental Figures A.2 3.1 2 2 1 1.5. 3 U/L 4 mg/dl weight (g).25.15 Amylase Glucose Pancreas B Trichrome HABP PAS H&E Supplemental Figure 1. FAP is dispensable for pancreatic development. (A) The pancreas
Surgical Management of Advanced Stage Colon Cancer. Nathan Huber, MD 6/11/14
 Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
SSM signature genes are highly expressed in residual scar tissues after preoperative radiotherapy of rectal cancer.
 Supplementary Figure 1 SSM signature genes are highly expressed in residual scar tissues after preoperative radiotherapy of rectal cancer. Scatter plots comparing expression profiles of matched pretreatment
Supplementary Figure 1 SSM signature genes are highly expressed in residual scar tissues after preoperative radiotherapy of rectal cancer. Scatter plots comparing expression profiles of matched pretreatment
Recent advances in breast cancers
 Recent advances in breast cancers Breast cancer is a hetrogenous disease due to distinct genetic alterations. Similar morphological subtypes show variation in clinical behaviour especially in response
Recent advances in breast cancers Breast cancer is a hetrogenous disease due to distinct genetic alterations. Similar morphological subtypes show variation in clinical behaviour especially in response
CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION
 CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION PROVIDED AS AN EDUCATIONAL SERVICE BY THE INSTITUTE FOR CONTINUING HEALTHCARE EDUCATION SUPPORTED BY AN EDUCATIONAL GRANT FROM GENENTECH LEARNING
CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION PROVIDED AS AN EDUCATIONAL SERVICE BY THE INSTITUTE FOR CONTINUING HEALTHCARE EDUCATION SUPPORTED BY AN EDUCATIONAL GRANT FROM GENENTECH LEARNING
Supplementary Figure 1. Characterization of NMuMG-ErbB2 and NIC breast cancer cells expressing shrnas targeting LPP. NMuMG-ErbB2 cells (a) and NIC
 and NIC") Supplementary Figure 1. Characterization of NMuMG-ErbB2 and NIC breast cancer cells expressing shrnas targeting LPP. NMuMG-ErbB2 cells (a) and NIC cells (b) were engineered to stably express either a LucA-shRNA
Supplementary Figure 1. Characterization of NMuMG-ErbB2 and NIC breast cancer cells expressing shrnas targeting LPP. NMuMG-ErbB2 cells (a) and NIC cells (b) were engineered to stably express either a LucA-shRNA
Supplementary Online Content
 Supplementary Online Content Venook AP, Niedzwiecki D, Lenz H-J, et al. Effect of first-line chemotherapy combined with cetuximab or bevacizumab on overall survival in patients with KRAS wild-type advanced
Supplementary Online Content Venook AP, Niedzwiecki D, Lenz H-J, et al. Effect of first-line chemotherapy combined with cetuximab or bevacizumab on overall survival in patients with KRAS wild-type advanced
SFSPM Novembre Valeur prédictive et pronostique de l infiltrat immunitaire dans les cancers du sein traités par chimiothérapie néoadjuvante
 SFSPM Novembre 217 Valeur prédictive et pronostique de l infiltrat immunitaire dans les cancers du sein traités par chimiothérapie néoadjuvante Dr Fabien REYAL Service de Chirurgie INSERM U932 Immunity
SFSPM Novembre 217 Valeur prédictive et pronostique de l infiltrat immunitaire dans les cancers du sein traités par chimiothérapie néoadjuvante Dr Fabien REYAL Service de Chirurgie INSERM U932 Immunity
Evaluation the Correlation between Ki67 and 5 Years Disease Free Survival of Breast Cancer Patients
 BIOSCIENCES BIOTECHNOLOGY RESEARCH ASIA, December 2015. Vol. 12(3), 2221-2225 Evaluation the Correlation between Ki67 and 5 Years Disease Free Survival of Breast Cancer Patients S.M. Hosseini¹, H. Shahbaziyan
BIOSCIENCES BIOTECHNOLOGY RESEARCH ASIA, December 2015. Vol. 12(3), 2221-2225 Evaluation the Correlation between Ki67 and 5 Years Disease Free Survival of Breast Cancer Patients S.M. Hosseini¹, H. Shahbaziyan
Impact of BMI on pathologic complete response (pcr) following neo adjuvant chemotherapy (NAC) for locally advanced breast cancer
 following neo adjuvant chemotherapy (NAC) for locally advanced breast cancer") Impact of BMI on pathologic complete response (pcr) following neo adjuvant chemotherapy (NAC) for locally advanced breast cancer Rachna Raman, MD, MS Fellow physician University of Iowa hospitals and clinics
Impact of BMI on pathologic complete response (pcr) following neo adjuvant chemotherapy (NAC) for locally advanced breast cancer Rachna Raman, MD, MS Fellow physician University of Iowa hospitals and clinics
Good Old clinical markers have similar power in breast cancer prognosis as microarray gene expression profilers q
 European Journal of Cancer 40 (2004) 1837 1841 European Journal of Cancer www.ejconline.com Good Old clinical markers have similar power in breast cancer prognosis as microarray gene expression profilers
European Journal of Cancer 40 (2004) 1837 1841 European Journal of Cancer www.ejconline.com Good Old clinical markers have similar power in breast cancer prognosis as microarray gene expression profilers
Adjuvant/neoadjuvant systemic treatment of colorectal cancer
 5th ESO-ESMO Eastern Europe and Balkan Region Masterclass in Medical Oncology Belgrade, June 19 th 2018 Adjuvant/neoadjuvant systemic treatment of colorectal cancer Carlotta Antoniotti Polo Oncologico
5th ESO-ESMO Eastern Europe and Balkan Region Masterclass in Medical Oncology Belgrade, June 19 th 2018 Adjuvant/neoadjuvant systemic treatment of colorectal cancer Carlotta Antoniotti Polo Oncologico
A new way of looking at breast cancer tumour biology
 A new way of looking at breast cancer tumour biology Contents Intrinsic subtypes of breast cancer 3 Gene expression assays 3 Basis of the Prosigna test 4 Information provided by Prosigna 5 The accuracy
A new way of looking at breast cancer tumour biology Contents Intrinsic subtypes of breast cancer 3 Gene expression assays 3 Basis of the Prosigna test 4 Information provided by Prosigna 5 The accuracy
Immunohistochemical classification of breast tumours
 Immunohistochemical classification of breast tumours Workshop in Diagnostic Immunohistochemistry September 19 th - 21 th 2018 Anne-Vibeke Lænkholm Department of Surgical Pathology, Zealand University Hospital,
Immunohistochemical classification of breast tumours Workshop in Diagnostic Immunohistochemistry September 19 th - 21 th 2018 Anne-Vibeke Lænkholm Department of Surgical Pathology, Zealand University Hospital,
Current Status of Biomarkers (including DNA Tumor Markers and Immunohistochemistry in the Laboratory Diagnosis of Tumors)
") Current Status of Biomarkers (including DNA Tumor Markers and Immunohistochemistry in the Laboratory Diagnosis of Tumors) Kael Mikesell, DO McKay-Dee Hospital May 14, 2015 Outline Update to DNA Testing
Current Status of Biomarkers (including DNA Tumor Markers and Immunohistochemistry in the Laboratory Diagnosis of Tumors) Kael Mikesell, DO McKay-Dee Hospital May 14, 2015 Outline Update to DNA Testing
Risk factors for cancer recurrence or death within 6 months after liver resection in patients with colorectal cancer liver metastasis
 ORIGINAL ARTICLE pissn 2288-6575 eissn 2288-6796 http://dx.doi.org/10.4174/astr.2016.90.5.257 Annals of Surgical Treatment and Research Risk factors for cancer recurrence or death within 6 months after
ORIGINAL ARTICLE pissn 2288-6575 eissn 2288-6796 http://dx.doi.org/10.4174/astr.2016.90.5.257 Annals of Surgical Treatment and Research Risk factors for cancer recurrence or death within 6 months after
ANALYTISCHE STRATEGIE Tissue Imaging. Bernd Bodenmiller Institute of Molecular Life Sciences University of Zurich
 ANALYTISCHE STRATEGIE Tissue Imaging Bernd Bodenmiller Institute of Molecular Life Sciences University of Zurich Quantitative Breast single cancer cell analysis Switzerland Brain Breast Lung Colon-rectum
ANALYTISCHE STRATEGIE Tissue Imaging Bernd Bodenmiller Institute of Molecular Life Sciences University of Zurich Quantitative Breast single cancer cell analysis Switzerland Brain Breast Lung Colon-rectum
RECTAL CANCER CLINICAL CASE PRESENTATION
 RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
Radiation Therapy for the Oncologist in Breast Cancer
 REVIEW ARTICLE Chonnam National University Medical School Sung-Ja Ahn, M.D. Adjuvant Tamoxifen with or without in Patients 70 Years of Age with Stage I ER-Positive Breast Cancer: Efficacy Outcomes (10
REVIEW ARTICLE Chonnam National University Medical School Sung-Ja Ahn, M.D. Adjuvant Tamoxifen with or without in Patients 70 Years of Age with Stage I ER-Positive Breast Cancer: Efficacy Outcomes (10
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress?
 Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Triple Negative Breast Cancer
 Triple Negative Breast Cancer Prof. Dr. Pornchai O-charoenrat Division of Head-Neck & Breast Surgery Department of Surgery Faculty of Medicine Siriraj Hospital Breast Cancer Classification Traditional
Triple Negative Breast Cancer Prof. Dr. Pornchai O-charoenrat Division of Head-Neck & Breast Surgery Department of Surgery Faculty of Medicine Siriraj Hospital Breast Cancer Classification Traditional
SHREE ET AL, SUPPLEMENTAL MATERIALS. (A) Workflow for tumor cell line derivation and orthotopic implantation.
 Workflow for tumor cell line derivation and orthotopic implantation.") SHREE ET AL, SUPPLEMENTAL MATERIALS SUPPLEMENTAL FIGURE AND TABLE LEGENDS Supplemental Figure 1. Derivation and characterization of TS1-TGL and TS2-TGL PyMT cell lines and development of an orthotopic
SHREE ET AL, SUPPLEMENTAL MATERIALS SUPPLEMENTAL FIGURE AND TABLE LEGENDS Supplemental Figure 1. Derivation and characterization of TS1-TGL and TS2-TGL PyMT cell lines and development of an orthotopic
Surgical resection improves survival in pancreatic cancer patients without vascular invasion- a population based study
 Original article Annals of Gastroenterology (2013) 26, 346-352 Surgical resection improves survival in pancreatic cancer patients without vascular invasion- a population based study Subhankar Chakraborty
Original article Annals of Gastroenterology (2013) 26, 346-352 Surgical resection improves survival in pancreatic cancer patients without vascular invasion- a population based study Subhankar Chakraborty
Third Line and Beyond: Management of Refractory Colorectal Cancer
 Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
ADJUVANT CHEMOTHERAPY...
 Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
ADVANCED COLORECTAL CANCER: UNRESECTABLE OR BORDERLINE RESECTABLE (GROUP 1) CHEMOTHERAPY +/- TARGETED AGENTS. Andrés Cervantes. Professor of Medicine
 CHEMOTHERAPY +/- TARGETED AGENTS. Andrés Cervantes. Professor of Medicine") ADVANCED COLORECTAL CANCER: UNRESECTABLE OR BORDERLINE RESECTABLE (GROUP 1) CHEMOTHERAPY +/- TARGETED AGENTS Andrés Cervantes Professor of Medicine 1995 One option Advances in the treatment of mcrc 2000
ADVANCED COLORECTAL CANCER: UNRESECTABLE OR BORDERLINE RESECTABLE (GROUP 1) CHEMOTHERAPY +/- TARGETED AGENTS Andrés Cervantes Professor of Medicine 1995 One option Advances in the treatment of mcrc 2000
Present Role of Immunohistochemistry in the. Subtypes. Beppe Viale European Institute of Oncology University of Milan Milan-Italy
 Present Role of Immunohistochemistry in the Classification of Molecular Subtypes Beppe Viale European Institute of Oncology University of Milan Milan-Italy We know it is many diseases Breast cancer is
Present Role of Immunohistochemistry in the Classification of Molecular Subtypes Beppe Viale European Institute of Oncology University of Milan Milan-Italy We know it is many diseases Breast cancer is
Supplementary Figures
 Supplementary Figures Supplementary Fig. 1. Galectin-3 is present within tumors. (A) mrna expression levels of Lgals3 (galectin-3) and Lgals8 (galectin-8) in the four classes of cell lines as determined
Supplementary Figures Supplementary Fig. 1. Galectin-3 is present within tumors. (A) mrna expression levels of Lgals3 (galectin-3) and Lgals8 (galectin-8) in the four classes of cell lines as determined
Clinicopathological Factors Affecting Distant Metastasis Following Loco-Regional Recurrence of breast cancer. Cheol Min Kang 2018/04/05
 Abstract No.: ABS-0075 Clinicopathological Factors Affecting Distant Metastasis Following Loco-Regional Recurrence of breast cancer 2018/04/05 Cheol Min Kang Department of surgery, University of Ulsan
Abstract No.: ABS-0075 Clinicopathological Factors Affecting Distant Metastasis Following Loco-Regional Recurrence of breast cancer 2018/04/05 Cheol Min Kang Department of surgery, University of Ulsan
Prediction of Postoperative Tumor Size in Breast Cancer Patients by Clinical Assessment, Mammography and Ultrasonography
 Prediction of Postoperative Tumor Size in Breast Cancer Patients by Clinical Assessment, Mammography and Ultrasonography Eyad Fawzi AlSaeed 1 and Mutahir A. Tunio 2* 1 Consultant Radiation Oncology, Chairman
Prediction of Postoperative Tumor Size in Breast Cancer Patients by Clinical Assessment, Mammography and Ultrasonography Eyad Fawzi AlSaeed 1 and Mutahir A. Tunio 2* 1 Consultant Radiation Oncology, Chairman
GI Tumor Board 3/8/2018. Case #1 IDEA. Case #1 Question #1 What is the next step in management?
 GI Tumor Board Edward Kim George Poultsides Naseem Esteghamat Kenzo Hirose May Cho Alan Venook Arta Monjazeb Margaret Tempero George Fisher Andrew Ko Daniel Chang Thomas Semrad Sisi Haraldsdottir Case
GI Tumor Board Edward Kim George Poultsides Naseem Esteghamat Kenzo Hirose May Cho Alan Venook Arta Monjazeb Margaret Tempero George Fisher Andrew Ko Daniel Chang Thomas Semrad Sisi Haraldsdottir Case
Morphological and Molecular Typing of breast Cancer
 Morphological and Molecular Typing of breast Cancer Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology, Nottingham University Hospitals NHS Trust Histological
Morphological and Molecular Typing of breast Cancer Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology, Nottingham University Hospitals NHS Trust Histological
Jonathan Dickinson, LCL Xeloda
 Xeloda A blockbuster in the making Jonathan Dickinson, LCL Xeloda Xeloda unique tumor-activated mechanism Delivering more cancer-killing agent straight into cancer Highly effective comparable efficacy
Xeloda A blockbuster in the making Jonathan Dickinson, LCL Xeloda Xeloda unique tumor-activated mechanism Delivering more cancer-killing agent straight into cancer Highly effective comparable efficacy
Breast cancer (screening) in older individuals: the oncologist s viewpoint for the geriatrician
 in older individuals: the oncologist s viewpoint for the geriatrician") Breast cancer (screening) in older individuals: the oncologist s viewpoint for the geriatrician Hans Wildiers Medical oncologist, Leuven, Belgium Past chairman of the EORTC elderly task force President-elect
Breast cancer (screening) in older individuals: the oncologist s viewpoint for the geriatrician Hans Wildiers Medical oncologist, Leuven, Belgium Past chairman of the EORTC elderly task force President-elect
An epithelial-to-mesenchymal transition-inducing potential of. granulocyte macrophage colony-stimulating factor in colon. cancer
 An epithelial-to-mesenchymal transition-inducing potential of granulocyte macrophage colony-stimulating factor in colon cancer Yaqiong Chen, Zhi Zhao, Yu Chen, Zhonglin Lv, Xin Ding, Renxi Wang, He Xiao,
An epithelial-to-mesenchymal transition-inducing potential of granulocyte macrophage colony-stimulating factor in colon cancer Yaqiong Chen, Zhi Zhao, Yu Chen, Zhonglin Lv, Xin Ding, Renxi Wang, He Xiao,
Cetuximab plus 5-FU/FA/oxaliplatin (FOLFOX-4) in the first-line treatment of metastatic colorectal cancer: a large-scale Phase II study (OPUS)
 in the first-line treatment of metastatic colorectal cancer: a large-scale Phase II study (OPUS)") Cetuximab plus 5-FU/FA/oxaliplatin (FOLFOX-4) in the first-line treatment of metastatic colorectal cancer: a large-scale Phase II study (OPUS) C Bokemeyer, E Staroslawska, A Makhson, I Bondarenko, JT Hartmann,
Cetuximab plus 5-FU/FA/oxaliplatin (FOLFOX-4) in the first-line treatment of metastatic colorectal cancer: a large-scale Phase II study (OPUS) C Bokemeyer, E Staroslawska, A Makhson, I Bondarenko, JT Hartmann,
Clinical Research in Rare Cancers. Friday 10 th February Matt Seymour & Nicola Keat
 Clinical Research in Rare Cancers Friday 10 th February 2012 Matt Seymour & Nicola Keat Rare cancer is a common disease Rare Cancer : [prevalence
Clinical Research in Rare Cancers Friday 10 th February 2012 Matt Seymour & Nicola Keat Rare cancer is a common disease Rare Cancer : [prevalence
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Technology Appraisals. Patient Access Scheme Submission Template
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Technology Appraisals Patient Access Scheme Submission Template Bevacizumab in combination with fluoropyrimidine-based chemotherapy for the first-line
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Technology Appraisals Patient Access Scheme Submission Template Bevacizumab in combination with fluoropyrimidine-based chemotherapy for the first-line
Lower lymph node yield following neoadjuvant therapy for rectal cancer has no clinical significance
 Original Article Lower lymph node yield following neoadjuvant therapy for rectal cancer has no clinical significance Dedrick Kok Hong Chan 1,2, Ker-Kan Tan 1,2 1 Division of Colorectal Surgery, University
Original Article Lower lymph node yield following neoadjuvant therapy for rectal cancer has no clinical significance Dedrick Kok Hong Chan 1,2, Ker-Kan Tan 1,2 1 Division of Colorectal Surgery, University
Disclosures. Outline. What IS tumor budding?? Tumor Budding in Colorectal Carcinoma: What, Why, and How. I have nothing to disclose
 Tumor Budding in Colorectal Carcinoma: What, Why, and How Disclosures I have nothing to disclose Soo-Jin Cho, MD, PhD Assistant Professor UCSF Dept of Pathology Current Issues in Anatomic Pathology 2017
Tumor Budding in Colorectal Carcinoma: What, Why, and How Disclosures I have nothing to disclose Soo-Jin Cho, MD, PhD Assistant Professor UCSF Dept of Pathology Current Issues in Anatomic Pathology 2017
What is new in HR+ Breast Cancer? Olivia Pagani Breast Unit and Institute of oncology of Southern Switzerland
 What is new in HR+ Breast Cancer? Olivia Pagani Breast Unit and Institute of oncology of Southern Switzerland Outline Early breast cancer Advanced breast cancer Open questions Outline Early breast cancer
What is new in HR+ Breast Cancer? Olivia Pagani Breast Unit and Institute of oncology of Southern Switzerland Outline Early breast cancer Advanced breast cancer Open questions Outline Early breast cancer
How to Use MRI Following Neoadjuvant Chemotherapy (NAC) in Locally Advanced Breast Cancer
 in Locally Advanced Breast Cancer") Global Breast Cancer Conference 2016 & 5 th International Breast Cancer Symposium April 29 th 2016, 09:40-10:50 How to Use MRI Following Neoadjuvant Chemotherapy (NAC) in Locally Advanced Breast Cancer
Global Breast Cancer Conference 2016 & 5 th International Breast Cancer Symposium April 29 th 2016, 09:40-10:50 How to Use MRI Following Neoadjuvant Chemotherapy (NAC) in Locally Advanced Breast Cancer
Molecular Characterization of Breast Cancer: The Clinical Significance
 Molecular Characterization of : The Clinical Significance Shahla Masood, M.D. Professor and Chair Department of Pathology and Laboratory Medicine University of Florida College of Medicine-Jacksonville
Molecular Characterization of : The Clinical Significance Shahla Masood, M.D. Professor and Chair Department of Pathology and Laboratory Medicine University of Florida College of Medicine-Jacksonville
Breast Imaging: Multidisciplinary Approach. Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina
 Breast Imaging: Multidisciplinary Approach Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina No Disclosures Objectives Discuss a multidisciplinary breast
Breast Imaging: Multidisciplinary Approach Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina No Disclosures Objectives Discuss a multidisciplinary breast
Aintree University Hospital
 Aintree University Hospital Liverpool, UK Evolving role of DEBIRI with DC Bead - TACE in mcrc Hassan Z Malik MD FRCS Consultant Hepatobiliary Surgeon Hassan Z Malik is a consultant to Biocompatibles UK
Aintree University Hospital Liverpool, UK Evolving role of DEBIRI with DC Bead - TACE in mcrc Hassan Z Malik MD FRCS Consultant Hepatobiliary Surgeon Hassan Z Malik is a consultant to Biocompatibles UK
SUPPLEMENTARY INFORMATION
 DOI: 1.138/ncb3355 a S1A8 + cells/ total.1.8.6.4.2 b S1A8/?-Actin c % T-cell proliferation 3 25 2 15 1 5 T cells Supplementary Figure 1 Inter-tumoral heterogeneity of MDSC accumulation in mammary tumor
DOI: 1.138/ncb3355 a S1A8 + cells/ total.1.8.6.4.2 b S1A8/?-Actin c % T-cell proliferation 3 25 2 15 1 5 T cells Supplementary Figure 1 Inter-tumoral heterogeneity of MDSC accumulation in mammary tumor
Supplementary Figure 2
 100 10 1 0.1 Supplementary Figure 2 ** ** ** * * ** ACTA2 CD34 CSPG4 NCAM TGF-b1 VEGFa Fold-change variation relative to normal tissue Piera Balzarini et al Supplementary Table 1 Pathological features
100 10 1 0.1 Supplementary Figure 2 ** ** ** * * ** ACTA2 CD34 CSPG4 NCAM TGF-b1 VEGFa Fold-change variation relative to normal tissue Piera Balzarini et al Supplementary Table 1 Pathological features
SCIENCE CHINA Life Sciences
 SCIENCE CHINA Life Sciences RESEARCH PAPER April 2013 Vol.56 No.4: 335 340 doi: 10.1007/s11427-013-4435-y Risk factors of recurrence in small-sized, node negative breast cancer in young women: a retrospective
SCIENCE CHINA Life Sciences RESEARCH PAPER April 2013 Vol.56 No.4: 335 340 doi: 10.1007/s11427-013-4435-y Risk factors of recurrence in small-sized, node negative breast cancer in young women: a retrospective
Clinical Features and Survival Analysis of T1mic, a, bn0m0 Breast Cancer
 Original Articles Jpn J Clin Oncol 2012;42(6)471 476 doi:10.1093/jjco/hys046 Advance Access Publication 3 April 2012 Clinical Features and Survival Analysis of T1mic, a, bn0m0 Breast Cancer Junnan Li,
Original Articles Jpn J Clin Oncol 2012;42(6)471 476 doi:10.1093/jjco/hys046 Advance Access Publication 3 April 2012 Clinical Features and Survival Analysis of T1mic, a, bn0m0 Breast Cancer Junnan Li,
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Health Technology Appraisal Nivolumab for previously treated metastatic colorectal cancer with high microsatellite instability or mismatch repair deficiency
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Health Technology Appraisal Nivolumab for previously treated metastatic colorectal cancer with high microsatellite instability or mismatch repair deficiency
Mismatch repair status, inflammation and outcome in patients with primary operable colorectal cancer
 Mismatch repair status, inflammation and outcome in patients with primary operable colorectal cancer Park JH, Powell AG, Roxburgh CSD, Richards CH, Horgan PG, McMillan DC, Edwards J James Park Clinical
Mismatch repair status, inflammation and outcome in patients with primary operable colorectal cancer Park JH, Powell AG, Roxburgh CSD, Richards CH, Horgan PG, McMillan DC, Edwards J James Park Clinical
Dr. Iain Tan. Senior Consultant GI Medical Oncologist National Cancer Centre Singapore
 ESMO-ASIA 2017 Preceptorship (GI cancers) Session: Metastatic colorectal cancer, liver limited metastases Topic: Unresectable or borderline resectable : chemotherapy +/- targeted agents Dr. Iain Tan Senior
ESMO-ASIA 2017 Preceptorship (GI cancers) Session: Metastatic colorectal cancer, liver limited metastases Topic: Unresectable or borderline resectable : chemotherapy +/- targeted agents Dr. Iain Tan Senior
Colon Cancer Liver Metastases: Liver-Directed Therapy
 Colon Cancer Liver Metastases: Liver-Directed Therapy Shishir K. Maithel, MD FACS Assistant Professor of Surgery Division of Surgical Oncology Winship Cancer Institute Emory University August 10, 2014
Colon Cancer Liver Metastases: Liver-Directed Therapy Shishir K. Maithel, MD FACS Assistant Professor of Surgery Division of Surgical Oncology Winship Cancer Institute Emory University August 10, 2014
Does it matter which chemotherapy regimen you partner with the biologic agents?
 Does it matter which chemotherapy regimen you partner with the biologic agents? Yes, it does matter! Axel Grothey Disclosures Research Funding to MAYO Clinic Genentech Bayer Eisai Pfizer Imclone Potential
Does it matter which chemotherapy regimen you partner with the biologic agents? Yes, it does matter! Axel Grothey Disclosures Research Funding to MAYO Clinic Genentech Bayer Eisai Pfizer Imclone Potential
Techniques to Improve Resectability of Colorectal Liver Metastases Ching-Wei D. Tzeng, M.D.
 Techniques to Improve Resectability of Colorectal Liver Metastases Ching-Wei D. Tzeng, M.D. Department of Surgery Grand Rounds University of Kentucky January 15, 2014 Metastatic Colorectal Cancer (CRC)
Techniques to Improve Resectability of Colorectal Liver Metastases Ching-Wei D. Tzeng, M.D. Department of Surgery Grand Rounds University of Kentucky January 15, 2014 Metastatic Colorectal Cancer (CRC)
(a) Schematic diagram of the FS mutation of UVRAG in exon 8 containing the highly instable
 Schematic diagram of the FS mutation of UVRAG in exon 8 containing the highly instable") Supplementary Figure 1. Frameshift (FS) mutation in UVRAG. (a) Schematic diagram of the FS mutation of UVRAG in exon 8 containing the highly instable A 10 DNA repeat, generating a premature stop codon
Supplementary Figure 1. Frameshift (FS) mutation in UVRAG. (a) Schematic diagram of the FS mutation of UVRAG in exon 8 containing the highly instable A 10 DNA repeat, generating a premature stop codon
Present Status and Perspectives of Colorectal Cancer in Asia: Colorectal Cancer Working Group Report in 30th Asia-Pacific Cancer Conference
 Present Status and Perspectives of Colorectal Cancer in Asia: Colorectal Cancer Working Group Report in 30th Asia-Pacific Cancer Conference Jpn J Clin Oncol 2010;40(Supplement 1)i38 i43 doi:10.1093/jjco/hyq125
Present Status and Perspectives of Colorectal Cancer in Asia: Colorectal Cancer Working Group Report in 30th Asia-Pacific Cancer Conference Jpn J Clin Oncol 2010;40(Supplement 1)i38 i43 doi:10.1093/jjco/hyq125
38 years old, premenopausal, had L+snbx. Pathology: IDC Gr.II T-1.9cm N+2/4sn ER+100%st, PR+60%st, Her2-neg, KI %
 38 years old, premenopausal, had L+snbx Pathology: IDC Gr.II T-1.9cm N+2/4sn ER+100%st, PR+60%st, Her2-neg, KI67 5-10% Question: What will you do now? 1. Give adjuvant chemotherapy 2. Send for Oncotype
38 years old, premenopausal, had L+snbx Pathology: IDC Gr.II T-1.9cm N+2/4sn ER+100%st, PR+60%st, Her2-neg, KI67 5-10% Question: What will you do now? 1. Give adjuvant chemotherapy 2. Send for Oncotype
TEB. Id4 p63 DAPI Merge. Id4 CK8 DAPI Merge
 a Duct TEB b Id4 p63 DAPI Merge Id4 CK8 DAPI Merge c d e Supplementary Figure 1. Identification of Id4-positive MECs and characterization of the Comma-D model. (a) IHC analysis of ID4 expression in the
a Duct TEB b Id4 p63 DAPI Merge Id4 CK8 DAPI Merge c d e Supplementary Figure 1. Identification of Id4-positive MECs and characterization of the Comma-D model. (a) IHC analysis of ID4 expression in the
Can we prevent metastasis?
 Can we prevent metastasis? A research example to translate from the bench to the bedside Diane Palmieri, Ph.D. Women s Cancers Section Laboratory of Molecular Pharmacology CCR, NCI Some Basic Truths Most
Can we prevent metastasis? A research example to translate from the bench to the bedside Diane Palmieri, Ph.D. Women s Cancers Section Laboratory of Molecular Pharmacology CCR, NCI Some Basic Truths Most
Circulating Tumor Cells in non- Metastatic Triple Negative Breast Cancer
 Circulating Tumor Cells in non- Metastatic Triple Negative Breast Cancer Carolyn Hall, Ph.D. Department of Surgical Oncology The University of Texas MD Anderson Cancer Center Triple Negative Breast Cancer
Circulating Tumor Cells in non- Metastatic Triple Negative Breast Cancer Carolyn Hall, Ph.D. Department of Surgical Oncology The University of Texas MD Anderson Cancer Center Triple Negative Breast Cancer
Role of Primary Resection for Patients with Oligometastatic Disease
 GBCC 2018, April 6, Songdo ConvensiA, Incheon, Korea Panel Discussion 4, How Can We Better Treat Patients with Metastatic Disease? Role of Primary Resection for Patients with Oligometastatic Disease Tadahiko
GBCC 2018, April 6, Songdo ConvensiA, Incheon, Korea Panel Discussion 4, How Can We Better Treat Patients with Metastatic Disease? Role of Primary Resection for Patients with Oligometastatic Disease Tadahiko
Rationale for VEGFR-targeted Therapy in RCC
 Rationale for VEGFR-targeted Therapy in RCC EIKCS, Budapest, May 2013 Tim Eisen Tim Eisen - Disclosures Company Research Support Advisory Board Trial Management Group Honoraria Astra Zeneca + + + Astellas
Rationale for VEGFR-targeted Therapy in RCC EIKCS, Budapest, May 2013 Tim Eisen Tim Eisen - Disclosures Company Research Support Advisory Board Trial Management Group Honoraria Astra Zeneca + + + Astellas
(A) RT-PCR for components of the Shh/Gli pathway in normal fetus cell (MRC-5) and a
 RT-PCR for components of the Shh/Gli pathway in normal fetus cell (MRC-5) and a") Supplementary figure legends Supplementary Figure 1. Expression of Shh signaling components in a panel of gastric cancer. (A) RT-PCR for components of the Shh/Gli pathway in normal fetus cell (MRC-5) and
Supplementary figure legends Supplementary Figure 1. Expression of Shh signaling components in a panel of gastric cancer. (A) RT-PCR for components of the Shh/Gli pathway in normal fetus cell (MRC-5) and