The speaker has no financial relationships with a commercial interest to disclose and no conflicts of interest to resolve.
|
|
|
- Hector Williams
- 5 years ago
- Views:
Transcription

1 Hana Safah MD Professor of Medicine Tulane University School of Medicine Director of the SCT program, Tulane Medical Center The speaker has no financial relationships with a commercial interest to disclose and no conflicts of interest to resolve. 1
2 Overview of CML Epidemiology Diagnosis Treatment options Managing patients under therapy Epidemiology of CML 15% of adult leukemia About 5,920 new cases estimated in deaths in per 100,000 Median age is 67 years No clear genetic or environmental risk factors; there may be an increased risk with radiation exposure Fatal until 1980s 2

3 Clues to the diagnosis of CML Unexplained & persistent leukocytosis Unexplained thrombocytosis 30-50% Leukocyte alkaline phosphatase decreased Vitamin B12 increased Increased uric acid & LDH 3
4 Bone marrow biopsy Hyper cellular marrow, 75-90% Myeloid to erythroid ratio 10-30:1 WBC maturation stages present with myeloid predominance Megakaryocytes increased and may be dysplastic Fibrosis may be seen with disease progression The Philadelphia chromosome Chromosome translocation t(9;22)(q34;q11) BCR-ABL: fusion between BCR gene on chr 22 and ABL gene on chr 9 (p210 protein with deregulated tyrosine kinase activity in CML, p190 in ALL) 95% of CML patients have the Ph chromosome by Karyotype or FISH 30-40% of the 5% negative for Ph chr, are positive by PCR for BCR-ABL gene 4

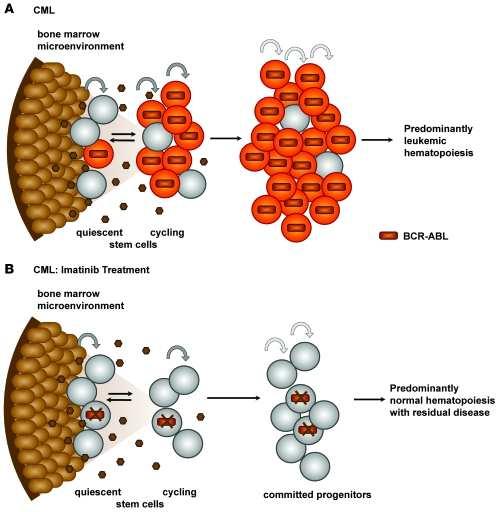
5 Philadelphia chromosome BCR-ABL: 1. ABL protein becomes constitutively active as a protein tyrosine kinase enzyme 2. DNA protein binding activity of ABL is attenuated 3. The binding of ABL to the cytoskeletal actin microfilament is enhanced which increases proliferation, affects differentiation, and blocks apoptosis Hence the potential of tyrosine kinase inhibitor therapy 5
6 Phases of CML Chronic Phase 25-60% are asymptomatic Fatigue Left upper quadrant pain/mass Weight loss Splenomegaly in 30-70% Hyper viscosity: visual or mental status changes and priapism Median survival of untreated patients: years Accelerated phase 10-19% blasts, PB or BM Platelets <100 x10 9 /L (not related to therapy) 20% basophils in peripheral blood Clonal evolution Increasing in spleen size and increase in WBC count unresponsive to therapy 6
7 Blast phase 20% blasts in bone marrow, peripheral blood or both Extramedullary infiltrates with leukemic cells OS 3-6 months 70% have myeloid phenotype (25% have lymphoid phenotype and 5% are undifferentiated). Prognostic factors Age Spleen size WBC Platelet count Blast, eosinophil, basophil % in peripheral blood Deletion of chromosome 9, which is seen in 10-15%, is associated with a worse prognosis 7


8 Prognostic groups low, intermediate, high: Sokol score: age in years, spleen size, platelet count, blast cells. More commonly used especially in imatinib trials. Hasford score: age, spleen size, platelet count, blasts, basophils, eosinophil count Can calculate at Both predict the probability of response to tyrosine kinase inhibitors Trends in cancer treatment: 16 8
9 Historical Treatment Hydroxyurea : to control the WBC count. Interferon alpha: 70-80% may achieve a complete hematologic response % have cytogenetic response Interferon + Cytarabine: showed higher response than IFN alone Imatinib (Gleevec) Dasatinib (Sprycel) Nilotinib (Tasigna) Bosutinib (Bosulif) Ponatinib ( Iclusig) Other Omacetaxin ( Synribo) Allogeneic Stem Cell transplantation 9

10 10

11 CML 11
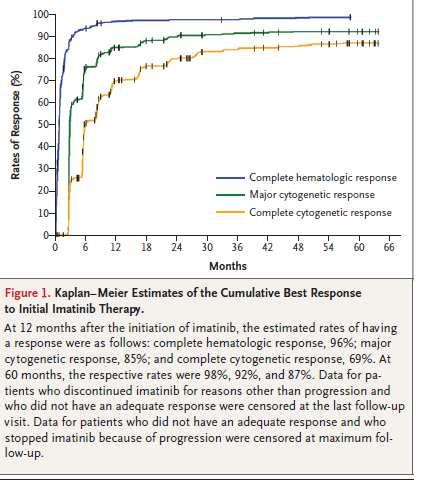
12 Imatinib Selective inhibitor of BCR-ABL tyrosine kinase Also inhibits PDGF-R (platelet derived growth factor receptor) & ckit Effective in all phases of CML Oral therapy, 400 mg/day in chronic phase, 600 mg/day in blast crisis & accelerated phases Approved by FDA 12/2002 for 1 st line treatment of CML based on IRIS Imatinib IRIS trial NEJM 2003: Randomized imatinib vs. IFN + cytarabine in chronic CML Imatinib was associated with lower toxicity and better quality of life 19 month CCyR 73.8 vs. 8.5% favoring Imatinib Only 7% of patients progressed to accelerated or blast crisis Overall survival 89% at 60 months 12

13 13
14 Imatinib toxicity Nausea Peripheral/ peri-orbital edema Diarrhea Rash Fatigue Muscle cramps Myelosuppresion: neutropenia in 45%, thrombocytopenia in 25%, anemia 10% CHF: 1.7% Imatinib failure Primary resistance, failure to achieve hematologic remission at 3 months 15-25% may have cytogenetic resistance (no cytogenetic response at 6 months, or major cytogenetic response at 12 months or complete cytogenetic response at 18 months) 40-60% is due to mutation of ABL T3151 is the most resistant mutation 14
15 Treatment of Imatinib failure Increase dose up to 800 mg QD More effective in those who had previously achieved cytogenetic response with prior standard dose Second generation TKI Dasatinib 2 nd generation BCR-ABL kinase inhibitor 325 x more potent than imatinib, dual inhibitor of ABL and SRC family of kinases, active against the active and inactive conformation of the ABL gene active against all mutations in vitro except the T315I FDA approved it in October 2010 as first line therapy, chronic phase CML Chronic phase: 100 mg daily. AP and BC: 140 mg daily 15
16 Dasatinib START C trial: Chronic phase, imatinib resistant or intolerant, at 24 month follow up: 91% CHR, 53% CCyR, 47% MMR. OS 94%, START- A trial: Accelerated phase, imatinib resistant or intolerant patients, 12 PFS 66%, OS 82% START B trial: CML in blast crisis. PFS 6.7 months, OS 11.8 months Naïve CML Patients: 519 patients randomized to dasatinib 100 mg vs. imatinib 400 mg PO daily, at 12 months, CCyR dasatinib 77% vs. Imatinib 66% (P=0.001) Adverse effects of dasatinib Reversible inhibition of platelet aggregation Pleural effusions (29% of chronic CML, 50% of accelerated CML, 33% with blast phase CML) Prior cardiac history or HTN are risk factors for pleural effusion, also 70 mg BID dosing Lymphocytosis with clonal expansion of NK/T cells 16
17 Nilotinib Selective inhibitor of BCR-ABL tyrosine kinase x more potent than imatinib resistant cell lines, 3-7 x more potent in sensitive lines FDA approved October 2007 (400 mg BID) for chronic & accelerated CML resistant or intolerant to imatinib FDA approved June 2010 (300 mg BID) for newly diagnosed chronic CML Nilotinib phase III multicenter study compared nilotinib 300 mg or 400 mg BID vs. imatinib 400 mg QD in newly diagnosed chronic CML MMR 43% at 300 mg vs. 43% at 400 mg for nilotinib vs. 22% for imatinib at 12 months CCyR 80% 300 mg vs. 78% 400 mg for Nilotinib vs. 65% for imatinib at 12 months Patients with high Sokal risk, the MMR rate at 3 years was 67% for nilotinib vs. 39% for imatinib with a lower progression rate 17

18 Nilotinib Phase II study in blast phase CML showed responses, but they were not durable If used in the 2 nd line setting, performance status & prior cytogenetic response to imatinib are associated with a better prognosis on 2 nd generations TKIs 18
19 Nilotinib toxicity QT prolongation & sudden cardiac death: a black box warning. Monitor EKG, avoid other drugs that prolong QT, replace electrolyte abnormalities prior to start Rare fluid retention, edema, muscle cramps Neutropenia, thrombocytopenia grade 3-4 in 29% Asymptomatic increase in lipase, bilirubin, glucose, hypophosphatemia Peripheral arterial occlusive disease (PAOD) Bosutinib Dual ABL/SRC Kinases Active against mutations that are resistant to imatinib, dasatinib, and nilotinib except for T315I and minimal inhibition of KIT and PDGFR Not recommended as first line therapy As second line of therapy in resistant/ intolerant CP-CML: CHR 86%, MCyR 53%, CCyR 41% at 24 months Effective in AP-CML and BP-CML Approved for all phases of CML, resistant or intolerant to prior TKI. QTc prolongation, diarrhea, otherwise well tolerated. 19
20 Ponatinib Multi-targeted Kinase inhibitor Active against many kinase domain mutations including T315I CCyR, in patient intolerant/ resistant in CP-CML were 46%, AP-CML 50% and 30% in BP-CML, response rate was higher in the T315I patients Approved for all phases of CML, resistant or intolerant to prior TKI. Arterial thrombosis, PE, MI, hepatotoxicity, pancreatitis Test Recommendation Bone marrow cytogenetics 2 At diagnosis to establish the disease phase. If collection of bone marrow is not feasible, FISH on peripheral blood specimen using dual probes for the BCR and ABL genes is an acceptable method of confirming the diagnosis of CML. At 3 months from initation of therapy, if QPCR using IS is not available At 12 months from initation of therapy, if there is no CCyR or MMR. At 18 months form initiation of therapy, if not in MMR and lack of CCyR at 12 months Rising levels of BCR-ABL transcript (1-log increase) without a MMR. Quantitative RT-PCR (QPCR) At diagnosis. Every 3 months when a patient is responding to treatment. After CCyR has been achieved, every 3 months for 3 years and every 3-6 months thereafter. If there is a rising level of BCR-ABL transcript (1-log increase) with a MMR, QPCR analysis should be repeated in 1-3 months. BCR-ABL kinase domain mutation analysis Chronic phase inadequate initial response (failure to achieve PCyR or BCR- ABL/ABL 10% (IS) at 3 months or CCyR at 12 and 18 months). Any sign of loss of response ( Hematologic or cytogenetic relapse) Disease progression to accelerated or blast phase. Version 1, 2014, 09/09/13 NCCN, Network, Inc. 20
21 Follow-up Response Treatment Recommendations FCR-ABL/ABL 10% (IS) or PCyR Continue the same dose of TKI 3 months BCR-ABL/ABL 10% (IS) or less than PCyR 1,2 Switch to alternate TKI 3 Evaluate for allogeneic HSCT depending on response to TKI therapy. CCyR Continue the same dose of TKI PCyR1 Switch to alternate TKI (preferred)3 Continue same dose of TKI Dose escalation of imatinib to maximum of 800 mg, as tolerated (if not a candidate for dasatinib, nilotinib, bosutinib, ponatinib or omacetaxine) 12 months Minor or no cytogenetic response 1-2 Switch to alternate TKI (preferred)3 Evaluate for allogeneic HSCT depending on response to TKI therapy Cytogenetic relapse 1-2 Switch to alternate TKI (preferred)3 Dose escalation of imatinib to a maximum of 800 mg, as tolerated (if not a candidate for dasatinib, nilotinib, bosutinib, ponatinib or omacetaxine) Evaluate for allogeneic HSCT depending on response to TKI therapy CCyR Continue the same dose of TKI 18 months PCyR or cytogenetic relapse 1-2 Switch to alternate TKI Evaluate for allogeneic HSCT depending on response to TKI therapy Version 1, 2014, 09/09/13 NCCN, Network, Inc Treatment Options Based on BCR-ABL Kinase Domain Mutation Status Mutation Treatment Options T3151 Ponatinib (preferred) or omacetaxine, HSCT or clinical trial V299L Consider ponatinib, nilotinib or omacetacine 4 T315A Consider ponatinib, nilotinib, imatinib 5, bosutinib, or omacetaxine 4 F317L/V/I/C Consider ponatinib, nilotinib, bosutinib or omacetaxine 4 Y253H, E255K/V, F359V/C/I Any other mutation Consider ponatinib, dasatinib, bosutinib or omacetaxine 4 Consider ponatinib, high-dose imatinib 6, dasatinib, nilotinib, bosutinib or omacetaxine 4 21

22 NCCN guidelines key points Imatinib, nilotinib, dasatinib are all category 1 recommendations for 1 st line treatment in chronic phase 2 nd generation TKIs may be better for intermediate or high risk patients If patient has failed 1 st line treatment with a 2 nd generation TKI, use the alternate 2 nd generation TKI as opposed to imatinib Patients with T3151 mutations should be considered for clinical trials or stem cell transplant 22
23 Allogeneic Stem Cell Transplantation Potentially curative More successful in first chronic phase as opposed to accelerated, blast phase ; 5-yr OS 75%,40%, 10% Faithfull monitoring of disease not to miss the chronic phase window. GVHD is the major morbidity 100 Probability of Survival after HLA-identical Sibling Donor Transplants for CML, By Disease Status and Transplant Year Probability of Survival, % AP, (N=333) AP, (N=300) CP, (N=2,524) CP, (N=2,291) P < Years 10 0 Slide 30 SUM-WW11_29.ppt 23
 Intolerant to all TKIs 2-yr OS : 44% ( T315I) vs.")
24 Indications for allogeneic SCT Not a 1 st line therapy of chronic CML due to excellent results with TKIs Appropriate for patient with T315I mutations and other BCR-ABL mutations that are resistant to all TKIs Disease progression to accelerated phase and blast phase, de novo or on TKI therapy ( use alternate TKI as a bridge to SCT) Intolerant to all TKIs 2-yr OS : 44% ( T315I) vs. 76% (TKI intolerance with out the mutation) 24
25 BCR-ABL positivity post transplant Timing of testing is important: if positive 6-12 months post transplant, there is a high rate of relapse (42% if positive vs. 3% PCR negative), 8% if positive > 36 months But late PCR + may have lower risk of relapse (14 %) Study of 379 patients with CML alive at >18 months post transplant showed 90 (24%) had at least 1 positive BCR- ABL (Radich et al) TKIs and allogeneic SCT Imatinib has shown a complete hematologic response in >70% with cytogenetic response in 58% after failure of BMT Imatinib probably not helpful if patients failed it prior to transplant 25
26 TKIs and allogeneic SCT Consider dasatinib or nilotinib if imatinib used prior to transplant TKIs may be used as maintenance for 1 yr post transplant for CML in Accelerated phase/blast phase to prevent relapse Donor lymphocyte infusion (DLI) Induces durable molecular remission More helpful in chronic phase vs. advanced phases Disease free survival appears higher with donor lymphocyte infusion vs. imatinib, but needs to be confirmed in randomized clinical trials Risk of graft vs. host disease and aplasia 26
27 Causes of Death after Transplants performed in HLA-identical Sibling Primary Disease (47%) New Malignancy (1%) GVHD (14%) Primary Disease (33%) Unrelated Donor New Malignancy (1%) GVHD (15%) Infection (12%) Organ Failure (4%) Other (21%) Primary Disease (73%) Autologous New Malignancy (1%) Other (29%) Organ Failure (6%) Infection (16%) Infection (8%) Organ Failure (2%) Other (16%) Slide 18 SUM-WW11_17.ppt Mortality, % day Mortality after Unrelated Donor Transplants, Early Disease Intermediate Disease Advanced Disease Chronic Phase Accelerated Phase Blast Phase Other 20 0 AML ALL CML MDS/MPS Aplastic Anemia Immune Deficiency Slide 17 SUM-WW11_16.ppt 27

28 Mortality, % day Mortality after HLA-identical Sibling Transplants, Early Disease Intermediate Disease Advanced Disease Chronic Phase Accelerated Phase Blast Phase Other 20 0 AML ALL CML MDS/MPS Aplastic Anemia Immune Deficiency Slide 16 SUM-WW11_15.ppt Infectious complication 28

29 Marrow and Blood Transplantation Complications: GVHD Acute GVHD become apparent in the first few weeks following transplantation -Affects 10% - 80% of allogeneic transplant recipients -Graded from I-IV according to number of organs involved Chronic GVHD become apparent at 100 to 400 days post transplant -Affect 30% - 50% of allogeneic transplant recipients -Classified as limited or extensive organ involvement Djubegovic B, et al.cancer Contol.2003 ASH Education Book, Jan 1,
30 Guidelines for screening for common cancers after SCT Site Breast Screening recommendations Mammogram annually starting at age 40 ; begin at age 25 or 8 years after radiation, which ever occurs later, in women who have received 20 Gy to the chest region Cervix PAP smear every year (for regular PAP test) or every 2 years (for liquid-based PAP test); after age 30, if patient has had 3 consecutive normal tests, may screen every 2-3 years Colorectal Beginning at age 50, fecal occult blood annually and/or flexible sigmoidoscopy every 5 years, or double contrast barium enema every 5 years, or colonoscopy every 10 years; certain high-risk groups (e.g., patients with inflammatory bowel disease) may need earlier initiation and more frequent screening Lung Oral Thyroid Skin Yearly pulmonary exam with imaging as appropriate Yearly oral cavity exam Yearly thyroid exam Skin exam as a part of periodic health exam *Adapted from Children s Oncology Group 25 and EBMT/CIBMTR/ASBMT Guidelines 42 Similar to American Cancer Society recommendations for general population cancer screening 30
31 Solid Cancers 3-5 years, increases with time Incidence at 5, 10, and 15yrs is 0.7%, 2.2%, and 6.7% compared to 0.3%, 0.6% and 0.8% in general population Risk Factor Young age, TBI, cgvhd (severity and >24 months use of immunosuppression) TBI solid cancers (Breast 17% in 25 yrs, thyroid, melanoma) cgvhd: cancer of the bucal mucosa, squamous cell cancer PTLD Incidence 1-2%, 80% within the 1 st year Arises in donor cells Early benign, polymorphic, monomorphic PTLD and Hodgkin s Lymphoma PTLD Risk Factors: EBV, T-Cell depletion, ATG, a GVHD, Graft from mismatched unrelated donor, cgvhd (>1yr) Follow copies of EBV, >1000 preemptive Rituximab 50-80% Response with Rituximab Multiple extra nodal disease and late onset, R-CHOP 31


32 MDS/AML 5-15% in Autologous SCT, 2-5 years (11q23, 5q and 7q) Risk factors, alkylating agents, TBI in conditioning regimen <1% post allo PBSCT Lingering Questions Are tyrosine kinase inhibitors better than allogeneic stem cell transplant in terms of survival? Will 2 nd generation TKIs have an improved survival benefit compared to imatinib? Cost of therapy vs. cancer survival? 32


33 Nowell & Hungerford (photo from Penn Medicine) 33
The BCR-ABL1 fusion. Epidemiology. At the center of advances in hematology and molecular medicine
 At the center of advances in hematology and molecular medicine Philadelphia chromosome-positive chronic myeloid leukemia Robert E. Richard MD PhD rrichard@uw.edu robert.richard@va.gov Philadelphia chromosome
At the center of advances in hematology and molecular medicine Philadelphia chromosome-positive chronic myeloid leukemia Robert E. Richard MD PhD rrichard@uw.edu robert.richard@va.gov Philadelphia chromosome
Chronic myeloid leukemia (CML) Warunsuda Sripakdee, BCOP,BCP Prince of Songkla University
 Warunsuda Sripakdee, BCOP,BCP Prince of Songkla University") Chronic myeloid leukemia (CML) 1 Warunsuda Sripakdee, BCOP,BCP Prince of Songkla University Hematologic malignancies CML ALL AML 2 CML CD34+ results from an acquired mutation that affects hematopoietic
Chronic myeloid leukemia (CML) 1 Warunsuda Sripakdee, BCOP,BCP Prince of Songkla University Hematologic malignancies CML ALL AML 2 CML CD34+ results from an acquired mutation that affects hematopoietic
A 34-year old women came because of abdominal discomfort. Vital sign was stable. Spleen tip was palpable.
 1 Case 1 A 34-year old women came because of abdominal discomfort. Vital sign was stable. Spleen tip was palpable. CBC and bone marrow aspiration and biopsy were done. Chromosome study showed she had t(9;22)
1 Case 1 A 34-year old women came because of abdominal discomfort. Vital sign was stable. Spleen tip was palpable. CBC and bone marrow aspiration and biopsy were done. Chromosome study showed she had t(9;22)
Stopping TKI s in CML- Are we There Yet? Joseph O. Moore, MD Duke Cancer Institute
 Stopping TKI s in CML- Are we There Yet? Joseph O. Moore, MD Duke Cancer Institute Natural History of CML Accumulation of immature myeloid cells New cytogenetic changes Chronic Phase Accelerated Phase
Stopping TKI s in CML- Are we There Yet? Joseph O. Moore, MD Duke Cancer Institute Natural History of CML Accumulation of immature myeloid cells New cytogenetic changes Chronic Phase Accelerated Phase
Welcome and Introductions
 Living with Chronic Myeloid Leukemia Welcome and Introductions Living with Chronic Myeloid Leukemia Living with Chronic Myeloid Leukemia (CML) Neil P. Shah, MD, PhD Edward S. Ageno Distinguished Professor
Living with Chronic Myeloid Leukemia Welcome and Introductions Living with Chronic Myeloid Leukemia Living with Chronic Myeloid Leukemia (CML) Neil P. Shah, MD, PhD Edward S. Ageno Distinguished Professor
What is the optimal management strategy for younger CP-CML patients with matched, related donors who fail to achieve CCyR
 What is the optimal management strategy for younger CP-CML patients with matched, related donors who fail to achieve CCyR after 18 months of imatinib? Second generation TKIs as a bridge to allogeneic SCT
What is the optimal management strategy for younger CP-CML patients with matched, related donors who fail to achieve CCyR after 18 months of imatinib? Second generation TKIs as a bridge to allogeneic SCT
CML TREATMENT GUIDELINES
 CML TREATMENT GUIDELINES INITIAL INVESTIGATION Propose enrolment in the CML Registry of the CML-MPN Quebec Research Group. Medical history : Question for cardio-respiratory disorders, diabetes, pancreatitis,
CML TREATMENT GUIDELINES INITIAL INVESTIGATION Propose enrolment in the CML Registry of the CML-MPN Quebec Research Group. Medical history : Question for cardio-respiratory disorders, diabetes, pancreatitis,
CML Clinical Case Scenario
 CML Clinical Case Scenario Neil Shah, MD, PhD Edward S. Ageno Distinguished Professor in Hematology/Oncology Leader, Hematopoietic Malignancies Program Helen Diller Family Comprehensive Cancer Center at
CML Clinical Case Scenario Neil Shah, MD, PhD Edward S. Ageno Distinguished Professor in Hematology/Oncology Leader, Hematopoietic Malignancies Program Helen Diller Family Comprehensive Cancer Center at
CML David L Porter, MD University of Pennsylvania Medical Center Abramson Cancer Center CML Current treatment options for CML
 1 CML 2012 LLS Jan 26, 2012 David L Porter, MD University of Pennsylvania Medical Center Abramson Cancer Center CML 2012 Current treatment options for CML patients Emerging therapies for CML treatment
1 CML 2012 LLS Jan 26, 2012 David L Porter, MD University of Pennsylvania Medical Center Abramson Cancer Center CML 2012 Current treatment options for CML patients Emerging therapies for CML treatment
Contemporary and Future Approaches in CML. Emory Meeting; Sea Island August 2014 Hagop Kantarjian, M.D.
 Contemporary and Future Approaches in CML Emory Meeting; Sea Island August 2014 Hagop Kantarjian, M.D. 1 CML. Historical vs. Modern Perspective Parameter Historical Modern Course Fatal Indolent Prognosis
Contemporary and Future Approaches in CML Emory Meeting; Sea Island August 2014 Hagop Kantarjian, M.D. 1 CML. Historical vs. Modern Perspective Parameter Historical Modern Course Fatal Indolent Prognosis
Myeloproliferative Disorders - D Savage - 9 Jan 2002
 Disease Usual phenotype acute leukemia precursor chronic leukemia low grade lymphoma myeloma differentiated Total WBC > 60 leukemoid reaction acute leukemia Blast Pro Myel Meta Band Seg Lymph 0 0 0 2
Disease Usual phenotype acute leukemia precursor chronic leukemia low grade lymphoma myeloma differentiated Total WBC > 60 leukemoid reaction acute leukemia Blast Pro Myel Meta Band Seg Lymph 0 0 0 2
2 nd Generation TKI Frontline Therapy in CML
 2 nd Generation TKI Frontline Therapy in CML Elias Jabbour, M.D. April 212 New York Frontline Therapy of CML in 212 - imatinib 4 mg daily - nilotinib 3 mg BID - dasatinib 1 mg daily Second / third line
2 nd Generation TKI Frontline Therapy in CML Elias Jabbour, M.D. April 212 New York Frontline Therapy of CML in 212 - imatinib 4 mg daily - nilotinib 3 mg BID - dasatinib 1 mg daily Second / third line
What is New in CML in Hagop Kantarjian, M.D. February 2011
 What is New in CML in 2011 Hagop Kantarjian, M.D. February 2011 1 CML. Historical vs. Modern Perspective Parameter Historical Modern Course Fatal Indolent Prognosis Poor Excellent 10-yr survival 10% 84-90%
What is New in CML in 2011 Hagop Kantarjian, M.D. February 2011 1 CML. Historical vs. Modern Perspective Parameter Historical Modern Course Fatal Indolent Prognosis Poor Excellent 10-yr survival 10% 84-90%
Tasigna. Tasigna (nilotinib) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.77 Subject: Tasigna Page: 1 of 6 Last Review Date: March 16, 2018 Tasigna Description Tasigna (nilotinib)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.77 Subject: Tasigna Page: 1 of 6 Last Review Date: March 16, 2018 Tasigna Description Tasigna (nilotinib)
HOW I TREAT CML. 4. KONGRES HEMATOLOGOV IN TRANSFUZIOLOGOV SLOVENIJE Z MEDNARODNO UDELEŽBO Terme Olimia, Podčetrtek,
 HOW I TREAT CML 4. KONGRES HEMATOLOGOV IN TRANSFUZIOLOGOV SLOVENIJE Z MEDNARODNO UDELEŽBO Terme Olimia, Podčetrtek, 12. - 14. april, 2012 Gianantonio Rosti Dpt of Hematology and Oncological Sciences S.
HOW I TREAT CML 4. KONGRES HEMATOLOGOV IN TRANSFUZIOLOGOV SLOVENIJE Z MEDNARODNO UDELEŽBO Terme Olimia, Podčetrtek, 12. - 14. april, 2012 Gianantonio Rosti Dpt of Hematology and Oncological Sciences S.
IRIS 8-Year Update. Management of TKI Resistance Will KD mutations matter? Sustained CCyR on study. 37% Unacceptable Outcome 17% 53% 15%
 Management of TKI Resistance Will KD mutations matter? IRIS 8-Year Update 17% 53% 5% 15% 37% Unacceptable Outcome No CCyR Lost CCyR CCyR Other 3% 7% Safety Lost-regained CCyR Sustained CCyR on study Deininger
Management of TKI Resistance Will KD mutations matter? IRIS 8-Year Update 17% 53% 5% 15% 37% Unacceptable Outcome No CCyR Lost CCyR CCyR Other 3% 7% Safety Lost-regained CCyR Sustained CCyR on study Deininger
Tasigna. Tasigna (nilotinib) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.77 Subject: Tasigna Page: 1of 5 Last Review Date: September 15, 2017 Tasigna Description Tasigna (nilotinib)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.77 Subject: Tasigna Page: 1of 5 Last Review Date: September 15, 2017 Tasigna Description Tasigna (nilotinib)
CML: Yesterday, Today and Tomorrow. Jorge Cortes, MD Chief CML Section Department of Leukemia The University of Texas, M.D. Anderson Cancer Center
 CML: Yesterday, Today and Tomorrow Jorge Cortes, MD Chief CML Section Department of Leukemia The University of Texas, M.D. Anderson Cancer Center Five Years of Signal Transduction Inhibition The Beginning
CML: Yesterday, Today and Tomorrow Jorge Cortes, MD Chief CML Section Department of Leukemia The University of Texas, M.D. Anderson Cancer Center Five Years of Signal Transduction Inhibition The Beginning
Form 2012 R3.0: Chronic Myelogenous Leukemia (CML) Pre-Infusion Data
 Pre-Infusion Data") Form 2012 R3.0: Chronic Myelogeus Leukemia (CML) Pre-Infusion Data Key Fields Sequence Number: Date Received: - - CIBMTR Center Number: CIBMTR Research ID: Event date: - - HCT type: (check all that apply)
Form 2012 R3.0: Chronic Myelogeus Leukemia (CML) Pre-Infusion Data Key Fields Sequence Number: Date Received: - - CIBMTR Center Number: CIBMTR Research ID: Event date: - - HCT type: (check all that apply)
Long-Term Outcomes After Hematopoietic Cell Transplantation
 Long-Term Outcomes After Hematopoietic Cell Transplantation Conflicts of Interest No relevant financial conflicts of interest Navneet Majhail, MD, MS Medical Director, NMDP Assistant Scientific Director,
Long-Term Outcomes After Hematopoietic Cell Transplantation Conflicts of Interest No relevant financial conflicts of interest Navneet Majhail, MD, MS Medical Director, NMDP Assistant Scientific Director,
C Longer follow up on IRIS data
 hronic Myeloid Leukemia Drs. Rena Buckstein, Mervat Mahrous & Eugenia Piliotis with input from Dr. J. Lipton (PMH) Updated August 2008* Updates: C Longer follow up on IRIS data Guidelines for monitoring
hronic Myeloid Leukemia Drs. Rena Buckstein, Mervat Mahrous & Eugenia Piliotis with input from Dr. J. Lipton (PMH) Updated August 2008* Updates: C Longer follow up on IRIS data Guidelines for monitoring
CML: Living with a Chronic Disease
 CML: Living with a Chronic Disease Jorge Cortes, MD Chief, CML and AML Sections Department of Leukemia M. D. Anderson Cancer Center Houston, Texas Survival in Early Chronic Phase CML TKI Interferon Chemotherapy
CML: Living with a Chronic Disease Jorge Cortes, MD Chief, CML and AML Sections Department of Leukemia M. D. Anderson Cancer Center Houston, Texas Survival in Early Chronic Phase CML TKI Interferon Chemotherapy
A COMPARATIVE EFFECTIVENESS ANALYSIS OF PATIENTS NEWLY INITIATING TYROSINE KINASE INHIBITOR THERAPY FOR CHRONIC MYELOID LEUKEMIA.
 A COMPARATIVE EFFECTIVENESS ANALYSIS OF PATIENTS NEWLY INITIATING TYROSINE KINASE INHIBITOR THERAPY FOR CHRONIC MYELOID LEUKEMIA Melea Ward A dissertation submitted to the faculty of the University of
A COMPARATIVE EFFECTIVENESS ANALYSIS OF PATIENTS NEWLY INITIATING TYROSINE KINASE INHIBITOR THERAPY FOR CHRONIC MYELOID LEUKEMIA Melea Ward A dissertation submitted to the faculty of the University of
Molecular Detection of BCR/ABL1 for the Diagnosis and Monitoring of CML
 Molecular Detection of BCR/ABL1 for the Diagnosis and Monitoring of CML Imran Mirza, MD, MS, FRCPC Pathology & Laboratory Medicine Institute Sheikh Khalifa Medical City, Abu Dhabi, UAE. imirza@skmc.ae
Molecular Detection of BCR/ABL1 for the Diagnosis and Monitoring of CML Imran Mirza, MD, MS, FRCPC Pathology & Laboratory Medicine Institute Sheikh Khalifa Medical City, Abu Dhabi, UAE. imirza@skmc.ae
Chronic Myeloid Leukemia A Disease of Young at Heart but Not of Body
 Chronic Myeloid Leukemia A Disease of Young at Heart but Not of Body Jeffrey H Lipton, PhD MD FRCPC Staff Physician, Princess Margaret Cancer Centre Professor of Medicine University of Toronto POGO November,
Chronic Myeloid Leukemia A Disease of Young at Heart but Not of Body Jeffrey H Lipton, PhD MD FRCPC Staff Physician, Princess Margaret Cancer Centre Professor of Medicine University of Toronto POGO November,
Bosulif. Bosulif (bosutinib) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.22 Section: Prescription Drugs Effective Date: April 1,2018 Subject: Bosulif Page: 1 of 5 Last Review
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.22 Section: Prescription Drugs Effective Date: April 1,2018 Subject: Bosulif Page: 1 of 5 Last Review
Hull and East Yorkshire and North Lincolnshire NHS Trusts Haematology Multidisciplinary Team Guideline and Pathway. Chronic Myeloid Leukaemia
 Hull and East Yorkshire and North Lincolnshire NHS Trusts Haematology Multidisciplinary Team Guideline and Pathway Chronic Myeloid Leukaemia 1 BACKGROUND The Hull and North Lincolnshire Haematology Multidisciplinary
Hull and East Yorkshire and North Lincolnshire NHS Trusts Haematology Multidisciplinary Team Guideline and Pathway Chronic Myeloid Leukaemia 1 BACKGROUND The Hull and North Lincolnshire Haematology Multidisciplinary
New drugs and trials. Andreas Hochhaus
 New drugs and trials. Andreas Hochhaus Hadera I Oct 2018 Introduction ABL001 is a potent, specific inhibitor of BCR-ABL1 with a distinct allosteric mechanism of action BCR-ABL1 Protein Binds a distinct
New drugs and trials. Andreas Hochhaus Hadera I Oct 2018 Introduction ABL001 is a potent, specific inhibitor of BCR-ABL1 with a distinct allosteric mechanism of action BCR-ABL1 Protein Binds a distinct
2nd generation TKIs to first line therapy
 New Horizons 2011 Newly diagnosed CML moving 2nd generation TKIs to first line therapy Gianantonio Rosti Dept. Of Hematology and Oncology St. Orsola-Malpighi University Hospital Bologna (Italy) GIMEMA
New Horizons 2011 Newly diagnosed CML moving 2nd generation TKIs to first line therapy Gianantonio Rosti Dept. Of Hematology and Oncology St. Orsola-Malpighi University Hospital Bologna (Italy) GIMEMA
Discontinuation of Tyrosine Kinase Inhibitors in Chronic Myeloid Leukemia: What s Stopping us from Stopping?
 Discontinuation of Tyrosine Kinase Inhibitors in Chronic Myeloid Leukemia: What s Stopping us from Stopping? David Pham, PharmD PGY2 Hematology/Oncology Pharmacy Resident South Texas VA Health Care System
Discontinuation of Tyrosine Kinase Inhibitors in Chronic Myeloid Leukemia: What s Stopping us from Stopping? David Pham, PharmD PGY2 Hematology/Oncology Pharmacy Resident South Texas VA Health Care System
TKIs ( Tyrosine Kinase Inhibitors ) Mechanism of action and toxicity in CML Patients. Moustafa Sameer Hematology Medical Advsior,Novartis oncology
 Mechanism of action and toxicity in CML Patients. Moustafa Sameer Hematology Medical Advsior,Novartis oncology") TKIs ( Tyrosine Kinase Inhibitors ) Mechanism of action and toxicity in CML Patients Moustafa Sameer Hematology Medical Advsior,Novartis oncology Introduction In people with chronic myeloid leukemia, A
TKIs ( Tyrosine Kinase Inhibitors ) Mechanism of action and toxicity in CML Patients Moustafa Sameer Hematology Medical Advsior,Novartis oncology Introduction In people with chronic myeloid leukemia, A
BOSULIF (bosutinib) oral tablet
 oral tablet") BOSULIF (bosutinib) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
BOSULIF (bosutinib) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
Chronic Myelogenous Leukemia
 NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Chronic Myelogenous Leukemia Version 1.2015 NCCN.org Continue Version 1.2015, 08/28/14 National Comprehensive Cancer Network, Inc. 2014,
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Chronic Myelogenous Leukemia Version 1.2015 NCCN.org Continue Version 1.2015, 08/28/14 National Comprehensive Cancer Network, Inc. 2014,
Chronic Leukemia Review and Update Todd Kliewer, MD Optim Oncology
 Chronic Leukemia Review and Update 2013 Todd Kliewer, MD Optim Oncology Leukemia A myeloproliferative malignancy arising from the bone marrow. Cells exhibit both rapid clonal division and biologic immortality.
Chronic Leukemia Review and Update 2013 Todd Kliewer, MD Optim Oncology Leukemia A myeloproliferative malignancy arising from the bone marrow. Cells exhibit both rapid clonal division and biologic immortality.
Contemporary and Future Approaches in Management of CML. Disclosures
 Winship Cancer Institute of Emory University Contemporary and Future Approaches in Management of CML Hagop Kantarjian, MD Chairman and Professor, Department of Leukemia University of Texas M. D. Anderson
Winship Cancer Institute of Emory University Contemporary and Future Approaches in Management of CML Hagop Kantarjian, MD Chairman and Professor, Department of Leukemia University of Texas M. D. Anderson
t(9;22)(q34;q11) as part of a single or complex translocation, or BCR-ABL transcripts must be present in every case
(q34;q11) as part of a single or complex translocation, or BCR-ABL transcripts must be present in every case") CHRONIC MYELOID LEUKAEMIA Diagnostic Criteria Chronic phase CML t(9;22)(q34;q11) as part of a single or complex translocation, or BCR-ABL transcripts must be present in every case Maximally cellular marrow
CHRONIC MYELOID LEUKAEMIA Diagnostic Criteria Chronic phase CML t(9;22)(q34;q11) as part of a single or complex translocation, or BCR-ABL transcripts must be present in every case Maximally cellular marrow
Role of Second Generation Tyrosine Kinase Inhibitors in Newly Diagnosed CML. GIUSEPPE SAGLIO, MD University of Torino, Italy
 Role of Second Generation Tyrosine Kinase Inhibitors in Newly Diagnosed CML GIUSEPPE SAGLIO, MD University of Torino, Italy Outcome in 282 Patients Treated with Imatinib First Line in Hammersmith Hospital
Role of Second Generation Tyrosine Kinase Inhibitors in Newly Diagnosed CML GIUSEPPE SAGLIO, MD University of Torino, Italy Outcome in 282 Patients Treated with Imatinib First Line in Hammersmith Hospital
History of CML Treatment
 History of CML Treatment Eduardo Olavarria No conflict of interest Lisbon, 20th March 2018 #EBMT18 www.ebmt.or What is CML? The mystery of chronic myeloid leukaemia Chronic myeloid leukaemia Often diagnosed
History of CML Treatment Eduardo Olavarria No conflict of interest Lisbon, 20th March 2018 #EBMT18 www.ebmt.or What is CML? The mystery of chronic myeloid leukaemia Chronic myeloid leukaemia Often diagnosed
BCCA Protocol Summary for Treatment of Chronic Myeloid Leukemia and Ph+ Acute Lymphoblastic Leukemia Using PONAtinib
 BCCA Protocol Summary for Treatment of Chronic Myeloid Leukemia and Ph+ Acute Lymphoblastic Leukemia Using PONAtinib Protocol Code Tumour Group Contact Physician ULKCMLP Leukemia Dr. Donna Forrest ELIGIBILITY:
BCCA Protocol Summary for Treatment of Chronic Myeloid Leukemia and Ph+ Acute Lymphoblastic Leukemia Using PONAtinib Protocol Code Tumour Group Contact Physician ULKCMLP Leukemia Dr. Donna Forrest ELIGIBILITY:
Chronic Myelogenous Leukemia
 NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Chronic Myelogenous Leukemia Version 3.2014 NCCN.org Continue Version 3.2014, 01/15/14 National Comprehensive Cancer Network, Inc. 2014,
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Chronic Myelogenous Leukemia Version 3.2014 NCCN.org Continue Version 3.2014, 01/15/14 National Comprehensive Cancer Network, Inc. 2014,
CHRONIC MYELOID LEUKEMIA. Dr.M SAI SRAVANTHI POST GRADUATE DEPT OF GENERAL MEDICINE KAMINENI INSTITUTE OF MEDICAL SCIENCES
 CHRONIC MYELOID LEUKEMIA Dr.M SAI SRAVANTHI POST GRADUATE DEPT OF GENERAL MEDICINE KAMINENI INSTITUTE OF MEDICAL SCIENCES CHRONIC MYELOID LEUKEMIA INCIDENCE The incidence of CML is 1.5 per 100,000 people
CHRONIC MYELOID LEUKEMIA Dr.M SAI SRAVANTHI POST GRADUATE DEPT OF GENERAL MEDICINE KAMINENI INSTITUTE OF MEDICAL SCIENCES CHRONIC MYELOID LEUKEMIA INCIDENCE The incidence of CML is 1.5 per 100,000 people
ICLUSIG (ponatinib) oral tablet
 oral tablet") ICLUSIG (ponatinib) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
ICLUSIG (ponatinib) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
Guidelines and real World: Management of CML in chronic and advanced phases. Carolina Pavlovsky. FUNDALEU May 2017 Frankfurt
 Guidelines and real World: Management of CML in chronic and advanced phases Carolina Pavlovsky. FUNDALEU 26-28 May 217 Frankfurt Some Issues in CML 217 First Line treatment: Imatinib vs 2nd generation
Guidelines and real World: Management of CML in chronic and advanced phases Carolina Pavlovsky. FUNDALEU 26-28 May 217 Frankfurt Some Issues in CML 217 First Line treatment: Imatinib vs 2nd generation
SESSION III: Chronic myeloid leukemia PONATINIB. Gianantonio Rosti, MD, Department of Hematology, University of Bologna, Italy
 SESSION III: Chronic myeloid leukemia PONATINIB Gianantonio Rosti, MD, Department of Hematology, University of Bologna, Italy Ponatinib A Pan-BCR-ABL Inhibitor Rationally designed inhibitor of BCR- ABL
SESSION III: Chronic myeloid leukemia PONATINIB Gianantonio Rosti, MD, Department of Hematology, University of Bologna, Italy Ponatinib A Pan-BCR-ABL Inhibitor Rationally designed inhibitor of BCR- ABL
Chronic Myeloid Leukaemia
 Chronic Myeloid Leukaemia Molecular Response: What is really important? Jeff Szer The Royal Melbourne Hospital PROBABILITY, % PROBABILITY OF SURVIVAL AFTER MYELOABLATIVE TRANSPLANTS FOR CML IN CHRONIC
Chronic Myeloid Leukaemia Molecular Response: What is really important? Jeff Szer The Royal Melbourne Hospital PROBABILITY, % PROBABILITY OF SURVIVAL AFTER MYELOABLATIVE TRANSPLANTS FOR CML IN CHRONIC
pan-canadian Oncology Drug Review Final Clinical Guidance Report Bosutinib (Bosulif) for Chronic Myelogenous Leukemia April 21, 2015
 for Chronic Myelogenous Leukemia April 21, 2015") pan-canadian Oncology Drug Review Final Clinical Guidance Report Bosutinib (Bosulif) for Chronic Myelogenous Leukemia April 21, 2015 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Clinical Guidance Report Bosutinib (Bosulif) for Chronic Myelogenous Leukemia April 21, 2015 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
HSCT for Myeloproliferative Disorders. Jane Apperley
 HSCT for Myeloproliferative Disorders Jane Apperley Myeloproliferative disorders CML Polycythemia vera Essential thrombocythemia Primary myelofibrosis bcr-abl + bcr-abl - JAK2 (valine to phenylalanin an
HSCT for Myeloproliferative Disorders Jane Apperley Myeloproliferative disorders CML Polycythemia vera Essential thrombocythemia Primary myelofibrosis bcr-abl + bcr-abl - JAK2 (valine to phenylalanin an
CIBMTR Center Number: CIBMTR Recipient ID: Today s Date: Date of HSCT for which this form is being completed:
 Chronic Myelogenous Leukemia (CML) Post-HSCT Data Sequence Number: Date Received: Registry Use Only Today s Date: Date of HSCT for which this form is being completed: HSCT type: autologous allogeneic,
Chronic Myelogenous Leukemia (CML) Post-HSCT Data Sequence Number: Date Received: Registry Use Only Today s Date: Date of HSCT for which this form is being completed: HSCT type: autologous allogeneic,
Allogeneic SCT for. 1st TKI. Vienna Austria. Dr. Eduardo Olavarría Complejo Hospitalario de Navarra
 The International Congress on Controversies in Stem Cell Transplantation and Cellular Therapies (COSTEM) Berlin, Germany September 8-11, 2011 Vienna Austria Allogeneic SCT for CML Allogeneic after failure
The International Congress on Controversies in Stem Cell Transplantation and Cellular Therapies (COSTEM) Berlin, Germany September 8-11, 2011 Vienna Austria Allogeneic SCT for CML Allogeneic after failure
CML and Future Perspective. Hani Al-Hashmi, MD
 CML and Future Perspective Hani Al-Hashmi, MD Objectives Learning from CML history Outcome of interest to clinician Patient and community interest!! Learning from CML history Survival Probability (All
CML and Future Perspective Hani Al-Hashmi, MD Objectives Learning from CML history Outcome of interest to clinician Patient and community interest!! Learning from CML history Survival Probability (All
ELN Recommendations on treatment choice and response. Gianantonio Rosti, MD, Department of Hematology, University of Bologna, Italy
 ELN Recommendations on treatment choice and response Gianantonio Rosti, MD, Department of Hematology, University of Bologna, Italy ELN 2013 Response to Front-line Treatment Baseline 3 months 6 months OPTIMAL
ELN Recommendations on treatment choice and response Gianantonio Rosti, MD, Department of Hematology, University of Bologna, Italy ELN 2013 Response to Front-line Treatment Baseline 3 months 6 months OPTIMAL
New drugs in first-line therapy
 New drugs in first-line therapy Gianantonio Rosti Dept of Hematology and Oncology Seràgnoli, Bologna University (Italy) GIMEMA (Gruppo Italiano Malattie Ematologiche dell Adulto) CML WORKING PARTY IRIS
New drugs in first-line therapy Gianantonio Rosti Dept of Hematology and Oncology Seràgnoli, Bologna University (Italy) GIMEMA (Gruppo Italiano Malattie Ematologiche dell Adulto) CML WORKING PARTY IRIS
CML: definition. CML epidemiology. CML diagnosis. CML: peripheralbloodsmear. Cytogenetic abnormality of CML
 MolecularDiagnostic.be Third Scientific Meeting Molecular Diagnostics.be t(9;22) CML: definition Management of CML patients treated with TKI: the place of molecular monitoring Antwerp, December 13 th 11
MolecularDiagnostic.be Third Scientific Meeting Molecular Diagnostics.be t(9;22) CML: definition Management of CML patients treated with TKI: the place of molecular monitoring Antwerp, December 13 th 11
CML HORIZONS 101 AND CML 101
 CML HORIZONS 101 AND CML 101 by Pat Garcia-Gonzalez, USA May 1, 2015 Barcelona, Spain Goals of this Session Everything you ever wanted to know and were afraid of asking Help you navigate the conference
CML HORIZONS 101 AND CML 101 by Pat Garcia-Gonzalez, USA May 1, 2015 Barcelona, Spain Goals of this Session Everything you ever wanted to know and were afraid of asking Help you navigate the conference
10 YEARS EXPERIENCE OF TYROSINE KINASE INHIBITOR THERAPY FOR CML IN OXFORD
 10 YEARS EXPERIENCE OF TYROSINE KINASE INHIBITOR THERAPY FOR CML IN OXFORD Dalia Khan 1, Noemi Roy 1, Vasha Bari 1, Grant Vallance 1, Helene Dreau 1, Timothy Littlewood 1, Andrew Peniket 1, Paresh Vyas
10 YEARS EXPERIENCE OF TYROSINE KINASE INHIBITOR THERAPY FOR CML IN OXFORD Dalia Khan 1, Noemi Roy 1, Vasha Bari 1, Grant Vallance 1, Helene Dreau 1, Timothy Littlewood 1, Andrew Peniket 1, Paresh Vyas
pan-canadian Oncology Drug Review Final Clinical Guidance Report Ponatinib (Iclusig) for Chronic Myeloid Leukemia / Acute Lymphoblastic Leukemia
 for Chronic Myeloid Leukemia / Acute Lymphoblastic Leukemia") pan-canadian Oncology Drug Review Final Clinical Guidance Report Ponatinib (Iclusig) for Chronic Myeloid Leukemia / Acute Lymphoblastic Leukemia October 1, 2015 DISCLAIMER Not a Substitute for Professional
pan-canadian Oncology Drug Review Final Clinical Guidance Report Ponatinib (Iclusig) for Chronic Myeloid Leukemia / Acute Lymphoblastic Leukemia October 1, 2015 DISCLAIMER Not a Substitute for Professional
MRD in CML (BCR-ABL1)
") MRD in CML (BCR-ABL1) Moleculaire Biologie en Cytometrie cursus Barbara Denys LAbo Hematologie UZ Gent 6 mei 2011 2008 Universitair Ziekenhuis Gent 1 Myeloproliferative Neoplasms o WHO classification 2008:
MRD in CML (BCR-ABL1) Moleculaire Biologie en Cytometrie cursus Barbara Denys LAbo Hematologie UZ Gent 6 mei 2011 2008 Universitair Ziekenhuis Gent 1 Myeloproliferative Neoplasms o WHO classification 2008:
Gleevec. Gleevec (imatinib) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.74 Subject: Gleevec Page: 1 of 6 Last Review Date: June 24, 2016 Gleevec Description Gleevec (imatinib)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.74 Subject: Gleevec Page: 1 of 6 Last Review Date: June 24, 2016 Gleevec Description Gleevec (imatinib)
Taiwan Guidelines for the Management of Chronic Myeloid Leukemia
 Taiwan Guidelines for the Management of Chronic Myeloid Leukemia Taiwan CML Study Group Coordinator: Lee-Yung Shih 2013/11/30 1 Contents Initial work-up at diagnosis and define baseline prognostic factors
Taiwan Guidelines for the Management of Chronic Myeloid Leukemia Taiwan CML Study Group Coordinator: Lee-Yung Shih 2013/11/30 1 Contents Initial work-up at diagnosis and define baseline prognostic factors
State of the Art Therapy and Monitoring of CML Hagop Kantarjian, M.D. Grand Rounds Hackensack, New Jersey. September 22, 2010
 State of the Art Therapy and Monitoring of CML - 2010 Hagop Kantarjian, M.D. Grand Rounds Hackensack, ew Jersey September 22, 2010 1 CML. Historical vs. Modern Perspective Parameter Historical Modern Course
State of the Art Therapy and Monitoring of CML - 2010 Hagop Kantarjian, M.D. Grand Rounds Hackensack, ew Jersey September 22, 2010 1 CML. Historical vs. Modern Perspective Parameter Historical Modern Course
screening procedures Disease resistant to full-dose imatinib ( 600 mg/day) or intolerant to any dose of imatinib
 or intolerant to any dose of imatinib") Table S1. Study inclusion and exclusion criteria Inclusion criteria Aged 18 years Signed and dated informed consent form prior to protocol-specific screening procedures Cytogenetic- or PCR-based diagnosis
Table S1. Study inclusion and exclusion criteria Inclusion criteria Aged 18 years Signed and dated informed consent form prior to protocol-specific screening procedures Cytogenetic- or PCR-based diagnosis
CML CML CML. tyrosine kinase inhibitor CML. 22 t(9;22)(q34;q11) chronic myeloid leukemia CML ABL. BCR-ABL c- imatinib mesylate CML CML BCR-ABL
(q34;q11) chronic myeloid leukemia CML ABL. BCR-ABL c- imatinib mesylate CML CML BCR-ABL") 1 Key Wordschronic myeloid leukemiaimatinib mesylate tyrosine kinase inhibitor chronic myeloid leukemia CML imatinib mesylate CML CML CML CML Ph 10 1 30 50 3 5 CML α IFNα Ph Ph cytogenetic response CRmajor
1 Key Wordschronic myeloid leukemiaimatinib mesylate tyrosine kinase inhibitor chronic myeloid leukemia CML imatinib mesylate CML CML CML CML Ph 10 1 30 50 3 5 CML α IFNα Ph Ph cytogenetic response CRmajor
Subject: Dasatinib (Sprycel ) Tablets
 Tablets") 09-J1000-43 Original Effective Date: 01/01/12 Reviewed: 01/10/18 Revised: 02/15/18 Subject: Dasatinib (Sprycel ) Tablets THIS MEDICAL COVERAGE GUIDELINE IS NOT AN AUTHORIZATION, CERTIFICATION, EXPLANATION
09-J1000-43 Original Effective Date: 01/01/12 Reviewed: 01/10/18 Revised: 02/15/18 Subject: Dasatinib (Sprycel ) Tablets THIS MEDICAL COVERAGE GUIDELINE IS NOT AN AUTHORIZATION, CERTIFICATION, EXPLANATION
CML 301 SOME INTRODUCTION INTO CML, CML SCIENCE, DRUG DEVELOPMENT AND INFORMATION RESOURCES. by Sarunas Narbutas Jan Geissler.
 CML 301 SOME INTRODUCTION INTO CML, CML SCIENCE, DRUG DEVELOPMENT AND INFORMATION RESOURCES by Sarunas Narbutas Jan Geissler 4 May 2018 CML 101 / BASICS: UNDERSTANDING THE DISCUSSIONS IN CML SESSIONS What
CML 301 SOME INTRODUCTION INTO CML, CML SCIENCE, DRUG DEVELOPMENT AND INFORMATION RESOURCES by Sarunas Narbutas Jan Geissler 4 May 2018 CML 101 / BASICS: UNDERSTANDING THE DISCUSSIONS IN CML SESSIONS What
Chronic myeloid leukemia: 2018 update on diagnosis, therapy and monitoring
 Received: 13 December 2017 Accepted: 17 December 2017 DOI: 10.1002/ajh.25011 ANNUAL CLINICAL UPDATES IN HEMATOLOGICAL MALIGNANCIES Chronic myeloid leukemia: 2018 update on diagnosis, therapy and monitoring
Received: 13 December 2017 Accepted: 17 December 2017 DOI: 10.1002/ajh.25011 ANNUAL CLINICAL UPDATES IN HEMATOLOGICAL MALIGNANCIES Chronic myeloid leukemia: 2018 update on diagnosis, therapy and monitoring
Advancing CML Patient Care: Closing in on a Cure?
 J a n u a r y 2 0 0 9 w w w. c l i n i c a l a d v a n c e s. c o m V o l u m e 7, I s s u e 1, S u p p l e m e n t 1 Faculty Francis J. Giles, MB, MD, FRCPI, FRCPath Professor of Medicine Chief, Division
J a n u a r y 2 0 0 9 w w w. c l i n i c a l a d v a n c e s. c o m V o l u m e 7, I s s u e 1, S u p p l e m e n t 1 Faculty Francis J. Giles, MB, MD, FRCPI, FRCPath Professor of Medicine Chief, Division
Venice Meeting Highlights: Key lessons. Conclusions Michele Baccarani Rüdiger Hehlmann
 Venice Meeting Highlights: Key lessons Conclusions Michele Baccarani Rüdiger Hehlmann CML therapy in the imatinib era CML prognosis has improved dramatically Cellular and molecular biology studies help
Venice Meeting Highlights: Key lessons Conclusions Michele Baccarani Rüdiger Hehlmann CML therapy in the imatinib era CML prognosis has improved dramatically Cellular and molecular biology studies help
Chronic Myeloid Leukaemia Guidelines
 Chronic Myeloid Leukaemia Guidelines Approved by Pathway Board for Haematological Malignancies Coordinating author: Heather Oakervee, Bart s Health NHST Date of issue: 12.03.2015 Version number:v1.0 These
Chronic Myeloid Leukaemia Guidelines Approved by Pathway Board for Haematological Malignancies Coordinating author: Heather Oakervee, Bart s Health NHST Date of issue: 12.03.2015 Version number:v1.0 These
Accepted Manuscript. Improving Outcomes in Chronic Myeloid Leukemia Over Time in the Era of Tyrosine Kinase Inhibitors. Pradnya Chopade, Luke P.
 Accepted Manuscript Improving Outcomes in Chronic Myeloid Leukemia Over Time in the Era of Tyrosine Kinase Inhibitors Pradnya Chopade, Luke P. Akard PII: S2152-2650(18)30343-4 DOI: 10.1016/j.clml.2018.06.029
Accepted Manuscript Improving Outcomes in Chronic Myeloid Leukemia Over Time in the Era of Tyrosine Kinase Inhibitors Pradnya Chopade, Luke P. Akard PII: S2152-2650(18)30343-4 DOI: 10.1016/j.clml.2018.06.029
Greater Manchester and Cheshire Cancer Network Chronic Myeloid Leukaemia v3 2012
 Greater Manchester and Cheshire Cancer Network Chronic Myeloid Leukaemia v3 2012 Dr Simon Watt Dr Shiva Natarajan 1.0 Introduction The landscape in chronic myeloid leukaemia (CML) has changed dramatically
Greater Manchester and Cheshire Cancer Network Chronic Myeloid Leukaemia v3 2012 Dr Simon Watt Dr Shiva Natarajan 1.0 Introduction The landscape in chronic myeloid leukaemia (CML) has changed dramatically
Should nilotinib replace imatinib as first line treatment of chronic myeloid leukemia in chronic phase (CML-CP)?
?") Should nilotinib replace imatinib as first line treatment of chronic myeloid leukemia in chronic phase (CML-CP)? http://test.metromomsblog.org/wp-content/uploads/2010/02/tortoise-and-the-hare.jpg D. Van
Should nilotinib replace imatinib as first line treatment of chronic myeloid leukemia in chronic phase (CML-CP)? http://test.metromomsblog.org/wp-content/uploads/2010/02/tortoise-and-the-hare.jpg D. Van
Imatinib Mesylate in the Treatment of Chronic Myeloid Leukemia: A Local Experience
 ORIGINAL ARTICLE Imatinib Mesylate in the Treatment of Chronic Myeloid Leukemia: A Local Experience PC Bee, MMed*, G G Gan, MRCP*, A Teh, FRCP**, A R Haris, MRCP* *Department of Medicine, Faculty of Medicine,
ORIGINAL ARTICLE Imatinib Mesylate in the Treatment of Chronic Myeloid Leukemia: A Local Experience PC Bee, MMed*, G G Gan, MRCP*, A Teh, FRCP**, A R Haris, MRCP* *Department of Medicine, Faculty of Medicine,
BMS Satellite Symposium
 ICKSH 2018 BMS Satellite Symposium Emerging Trends in CML Management CHAIRMAN The Head of Catholic Hematology Hospital The Director of the Catholic Leukemia Research Institute at the Catholic University
ICKSH 2018 BMS Satellite Symposium Emerging Trends in CML Management CHAIRMAN The Head of Catholic Hematology Hospital The Director of the Catholic Leukemia Research Institute at the Catholic University
HEMATOPOIETIC CELL TRANSPLANTATION FOR CHRONIC MYELOID LEUKEMIA
 LEUKEMIA Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs are dependent
LEUKEMIA Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs are dependent
Chronic Myeloid Leukemia
 NCCN GUIDELINES FOR PATIENTS 2018 Please complete our online survey at NCCN.org/patients/survey Chronic Myeloid Leukemia Presented with support from: Available online at NCCN.org/patients Ü Chronic Myeloid
NCCN GUIDELINES FOR PATIENTS 2018 Please complete our online survey at NCCN.org/patients/survey Chronic Myeloid Leukemia Presented with support from: Available online at NCCN.org/patients Ü Chronic Myeloid
Starting & stopping therapy in Chronic Myeloid Leukemia: What more is needed? Richard A. Larson, MD University of Chicago March 2019
 Starting & stopping therapy in Chronic Myeloid Leukemia: What more is needed? Richard A. Larson, MD University of Chicago March 2019 Disclosures Richard A. Larson, MD Research funding to the University
Starting & stopping therapy in Chronic Myeloid Leukemia: What more is needed? Richard A. Larson, MD University of Chicago March 2019 Disclosures Richard A. Larson, MD Research funding to the University
What is New in CML Jorge Cortes, MD Chief, CML and AML Sections Department of Leukemia MD Anderson Cancer Center Houston, Texas
 What is New in CML 2018 Jorge Cortes, MD Chief, CML and AML Sections Department of Leukemia MD Anderson Cancer Center Houston, Texas Final Results CML-IV Molecular Response with Imatinib 1538 pts newly
What is New in CML 2018 Jorge Cortes, MD Chief, CML and AML Sections Department of Leukemia MD Anderson Cancer Center Houston, Texas Final Results CML-IV Molecular Response with Imatinib 1538 pts newly
Chronic Myelogenous Leukemia
 Small Cell NCCN Lung Table Guidelines of Contents Index Staging,, CML Table of References Contents NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Chronic Myelogenous Leukemia Version
Small Cell NCCN Lung Table Guidelines of Contents Index Staging,, CML Table of References Contents NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Chronic Myelogenous Leukemia Version
Blast Phase Chronic Myelogenous Leukemia
 Blast Phase Chronic Myelogenous Leukemia Benjamin Powers, MD; and Suman Kambhampati, MD The dramatic improvement in survival with tyrosine kinase inhibitors has not been demonstrated in the advanced blast
Blast Phase Chronic Myelogenous Leukemia Benjamin Powers, MD; and Suman Kambhampati, MD The dramatic improvement in survival with tyrosine kinase inhibitors has not been demonstrated in the advanced blast
Juan Luis Steegmann Hospital de la Princesa. Madrid. JL Steegmann
 Juan Luis Steegmann Hospital de la Princesa. Madrid. Juan Luis Steegmann Hospital de la Princesa. Madrid No rush,at least in Chronic Phase Blast Phase*: SCT asap, after restablishing CP with TKI Accelerated
Juan Luis Steegmann Hospital de la Princesa. Madrid. Juan Luis Steegmann Hospital de la Princesa. Madrid No rush,at least in Chronic Phase Blast Phase*: SCT asap, after restablishing CP with TKI Accelerated
Outlook CML 2016: What is being done on the way to cure
 New Horizons 2011 Outlook CML 2016: What is being done on the way to cure Gianantonio Rosti Dept. Of Hematology and Oncology St. Orsola-Malpighi University Hospital Bologna (Italy) GIMEMA CML Working Party
New Horizons 2011 Outlook CML 2016: What is being done on the way to cure Gianantonio Rosti Dept. Of Hematology and Oncology St. Orsola-Malpighi University Hospital Bologna (Italy) GIMEMA CML Working Party
NCCP Chemotherapy Protocol. Bosutinib Monotherapy
 Bosutinib Monotherapy INDICATIONS FOR USE: INDICATION Treatment of adult patients with chronic phase (CP), accelerated phase (AP), and blast phase (BP) Philadelphia chromosome positive chronic myelogenous
Bosutinib Monotherapy INDICATIONS FOR USE: INDICATION Treatment of adult patients with chronic phase (CP), accelerated phase (AP), and blast phase (BP) Philadelphia chromosome positive chronic myelogenous
What Can We Expect from Imatinib? CML Case Presentation. Presenter Disclosure Information. CML Case Presentation (cont)? Session 2: 8:15 AM - 9:00 AM
? Session 2: 8:15 AM - 9:00 AM") Welcome to Master Class for Oncologists Session 2: 8:15 AM - 9: AM Miami, FL December 18, 29 Chronic Myelocytic Leukemia: Imatinib and Beyond Speaker: Daniel J. DeAngelo, MD, PhD Dana-Farber Cancer Institute
Welcome to Master Class for Oncologists Session 2: 8:15 AM - 9: AM Miami, FL December 18, 29 Chronic Myelocytic Leukemia: Imatinib and Beyond Speaker: Daniel J. DeAngelo, MD, PhD Dana-Farber Cancer Institute
The CML Guide. Information for Patients and Caregivers. Chronic Myeloid Leukemia. Matthew, CML survivor. This publication was supported by
 The CML Guide Information for Patients and Caregivers Chronic Myeloid Leukemia Matthew, CML survivor This publication was supported by Revised 2017 Booklet Updates The Leukemia & Lymphoma Society wants
The CML Guide Information for Patients and Caregivers Chronic Myeloid Leukemia Matthew, CML survivor This publication was supported by Revised 2017 Booklet Updates The Leukemia & Lymphoma Society wants
Form 2011 R4.0: Acute Lymphoblastic Leukemia (ALL) Pre-HCT Data
 Pre-HCT Data") Key Fields Sequence Number: Date Received: - - CIBMTR Center Number: CIBMTR Recipient ID: Date of HCT for which this form is being completed: - - HCT type: (check all that apply) Autologous Allogeneic,
Key Fields Sequence Number: Date Received: - - CIBMTR Center Number: CIBMTR Recipient ID: Date of HCT for which this form is being completed: - - HCT type: (check all that apply) Autologous Allogeneic,
Summary 1. Comparative effectiveness of ponatinib
 Cost-effectiveness of ponatinib (Iclusig ) as indicated for adult patients with: (i) CP-, AP-, or BP- chronic myeloid leukaemia (CML) who are resistant to dasatinib or nilotinib; who are intolerant to
Cost-effectiveness of ponatinib (Iclusig ) as indicated for adult patients with: (i) CP-, AP-, or BP- chronic myeloid leukaemia (CML) who are resistant to dasatinib or nilotinib; who are intolerant to
MP BCR-ABL1 Testing in Chronic Myelogenous Leukemia and Acute Lymphoblastic Leukemia
 Medical Policy BCBSA Ref. Policy: 2.04.85 Last Review: 10/18/2018 Effective Date: 10/18/2018 Section: Medicine Related Policies 8.01.30 Hematopoietic Cell Transplantation for Chronic Myelogenous Leukemia
Medical Policy BCBSA Ref. Policy: 2.04.85 Last Review: 10/18/2018 Effective Date: 10/18/2018 Section: Medicine Related Policies 8.01.30 Hematopoietic Cell Transplantation for Chronic Myelogenous Leukemia
Chronic Myeloid Leukemia
 Chronic Myeloid Leukemia Paula, CML survivor This publication was supported by Revised 2014 A Message from Louis J. DeGennaro, PhD President and CEO of The Leukemia & Lymphoma Society The Leukemia & Lymphoma
Chronic Myeloid Leukemia Paula, CML survivor This publication was supported by Revised 2014 A Message from Louis J. DeGennaro, PhD President and CEO of The Leukemia & Lymphoma Society The Leukemia & Lymphoma
The future of HSCT. John Barrett, MD, NHBLI, NIH Bethesda MD
 The future of HSCT John Barrett, MD, NHBLI, NIH Bethesda MD Transplants today Current approaches to improve SCT outcome Optimize stem cell dose and source BMT? PBSCT? Adjusting post transplant I/S to minimize
The future of HSCT John Barrett, MD, NHBLI, NIH Bethesda MD Transplants today Current approaches to improve SCT outcome Optimize stem cell dose and source BMT? PBSCT? Adjusting post transplant I/S to minimize
La terapia della LMC: è possibile guarire senza trapianto? Fabrizio Pane
 La terapia della LMC: è possibile guarire senza trapianto? Fabrizio Pane What could be the concept of Cure in CML? Sustained DMR with or without TKI therapy And 100% CML-related survival And QoL comparable
La terapia della LMC: è possibile guarire senza trapianto? Fabrizio Pane What could be the concept of Cure in CML? Sustained DMR with or without TKI therapy And 100% CML-related survival And QoL comparable
Sede Amministrativa: Università degli Studi di Padova
 Sede Amministrativa: Università degli Studi di Padova Dipartimento di Scienze del Farmaco CORSO DI DOTTORATO DI RICERCA IN SCIENZE FARMACOLOGICHE CURRICOLO: FARMACOLOGIA, TOSSICOLOGIA E TERAPIA XXX CICLO
Sede Amministrativa: Università degli Studi di Padova Dipartimento di Scienze del Farmaco CORSO DI DOTTORATO DI RICERCA IN SCIENZE FARMACOLOGICHE CURRICOLO: FARMACOLOGIA, TOSSICOLOGIA E TERAPIA XXX CICLO
Executive summary Overview
 Executive summary Overview In this appraisal, we have demonstrated that dasatinib is clinically more effective, as well as more cost effective, than imatinib, the current standard of care. In the pivotal
Executive summary Overview In this appraisal, we have demonstrated that dasatinib is clinically more effective, as well as more cost effective, than imatinib, the current standard of care. In the pivotal
One Day BMT Course by Thai Society of Hematology. Management of Graft Failure and Relapsed Diseases
 One Day BMT Course by Thai Society of Hematology Management of Graft Failure and Relapsed Diseases Piya Rujkijyanont, MD Division of Hematology-Oncology Department of Pediatrics Phramongkutklao Hospital
One Day BMT Course by Thai Society of Hematology Management of Graft Failure and Relapsed Diseases Piya Rujkijyanont, MD Division of Hematology-Oncology Department of Pediatrics Phramongkutklao Hospital
Low doses of tyrosine kinase inhibitors in CML
 CML Horizons Conference Warsaw 4-6 May 2018 Low doses of tyrosine kinase inhibitors in CML Delphine Rea, MD, PhD Pôle Hématologie Oncologie Radiothérapie INSERM UMR-1160 Centre Hospitalo-Universitaire
CML Horizons Conference Warsaw 4-6 May 2018 Low doses of tyrosine kinase inhibitors in CML Delphine Rea, MD, PhD Pôle Hématologie Oncologie Radiothérapie INSERM UMR-1160 Centre Hospitalo-Universitaire
Reduced-intensity Conditioning Transplantation
 Reduced-intensity Conditioning Transplantation Current Role and Future Prospect He Huang M.D., Ph.D. Bone Marrow Transplantation Center The First Affiliated Hospital Zhejiang University School of Medicine,
Reduced-intensity Conditioning Transplantation Current Role and Future Prospect He Huang M.D., Ph.D. Bone Marrow Transplantation Center The First Affiliated Hospital Zhejiang University School of Medicine,
Does Generic Imatinib Change the Treatment Approach in CML?
 Does Generic Imatinib Change the Treatment Approach in CML? Jerald P. Radich, MD Fred Hutchinson Cancer Research Center/ Seattle Cancer Care Alliance NCCN.org For Clinicians NCCN.org/patients For Patients
Does Generic Imatinib Change the Treatment Approach in CML? Jerald P. Radich, MD Fred Hutchinson Cancer Research Center/ Seattle Cancer Care Alliance NCCN.org For Clinicians NCCN.org/patients For Patients
State of the Art Therapy and Monitoring of CML Hagop Kantarjian, M.D. Grand Rounds UT Southwestern. October 28, 2010
 State of the Art Therapy and Monitoring of CML - 2010 Hagop Kantarjian, M.D. Grand Rounds UT Southwestern October 28, 2010 1 CML. Historical vs. Modern Perspective Parameter Historical Modern Course Fatal
State of the Art Therapy and Monitoring of CML - 2010 Hagop Kantarjian, M.D. Grand Rounds UT Southwestern October 28, 2010 1 CML. Historical vs. Modern Perspective Parameter Historical Modern Course Fatal
35 Current Trends in the
 35 Current Trends in the Management of Chronic Myelogenous Leukemia Abstract: CML is a hematopoietic stem cell disease which is characterized by the presence of Philadelphia chromosome (Ph-chromosome)
35 Current Trends in the Management of Chronic Myelogenous Leukemia Abstract: CML is a hematopoietic stem cell disease which is characterized by the presence of Philadelphia chromosome (Ph-chromosome)
The legally binding text is the original French version
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 14 March 2007 SPRYCEL 20 mg, film-coated tablet, blister (377 637-9) SPRYCEL 20 mg, film-coated tablet, bottle (377
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 14 March 2007 SPRYCEL 20 mg, film-coated tablet, blister (377 637-9) SPRYCEL 20 mg, film-coated tablet, bottle (377
How I treat high risck CML
 Torino, September 14, 2018 How I treat high risck CML Patrizia Pregno Hematology Dept. Citta della Salute e della Scienza Torino Disclosures Advisory Board: Novartis, Pfizer, Incyte Speaker Honoraria:
Torino, September 14, 2018 How I treat high risck CML Patrizia Pregno Hematology Dept. Citta della Salute e della Scienza Torino Disclosures Advisory Board: Novartis, Pfizer, Incyte Speaker Honoraria: