MDS overview 전남대학교김여경
|
|
|
- Darleen Farmer
- 5 years ago
- Views:
Transcription

1 MDS overview 전남대학교김여경
2 2008 WHO Classification of MDS Name Abbreviation Key Feature Pts, % Refractory cytopenia, with unlineage, dysplasia Refractory anemia with ring sideroblasts RA Anemia and erythroid dysplasia 10 RN Neutropenia and granulocytic dysplasia < 1 RT Thrombocytopenia and megak. dysplasia < 1 RARS 15% ring sideroblasts 5 5q- syndrome del(5q) Isolated 5q31 deletion, anemia, hypolobated megakaryocytes Refractory cytopenia with multilineage dysplasia Refractory anemia with excess blasts, type 1 Refractory anemia with excess blasts, type 2 RCMD Multilineage dysplasia with > 1 cytopenia With or without ring sideroblasts RAEB-1 5% to 9% blasts 20 RAEB-2 10% to 19% blasts ± Auer rods 20 Unclassifiable MDS-U Does not fit other categories 10 Childhood MDS RCC Often hypocellular; pancytopenia Rare 5 20
3 Case 2000 Isolated thrombocytopenia BM: Dx: Tx: Normocellular marrow, 46, XY ITP corticosteroid, splenectomy 2009 Isolated thrombocytopenia 지속 6,000 /ul (4,200/uL), 13.4 g/dl, 2,000/uL, LDH 600 IU/L Spleen scan: asplenia (+) PBS: H-J body (+) 다음단계의검사혹은치료는? 1. Danazol 2. Cyclosporin 3. Rituximab 4. Eltrombopag / Romiplostim 5. BM reexamination
4 Diagnosis 10~20% : hypocellular marrow (+) 60 세미만환자 : <30%, 60 세이상환자 : <20% 형태학적이상만으로골수형성이상증후군을확진하기어려울때 : 핵형이상을확인. 처음부터진단이어려운경우 : 수개월간의간격을두고반복적으로세포유전학검사를포함하여골수생검을시행. 이형성혹은세포유전학적이상이없는경우이나지속적으로말초혈액혈구감소증이있는경우 : 주기적으로말초혈구검사및세포유전학검사를포함한골수생검을추적검사.
5 Differential Diagnosis 골수내이형성증이반드시클론성질환이라는증거는되지않기때 문에진단전골수이형성증을유발할수있는다른원인들에대한확 인이반드시필요 Vit. B12, folate def. Toxic agents : As, alcohol, chemotherpeutic agents, 조혈촉진인자치료병력 감염 : HIV, parvovirus B19 선천성적혈구이형성빈혈 Paroxysmal nocturnal hemoglobinuria (PNH)
6 Case 2009 Isolated thrombocytopenia BM: Blast 2%, Megakaryocytes dysplasia, Cellularity 70%, 46, XY Dx: ITP, R/O MDS, RT 치료는? (1) Danazol (2) Cyclosporin (3) Rituximab (4) Eltrombopag / Romiplostim (5) Azacitidine

7 Romiplostim in LR-MDS Some pts: increase in the blast proportion!! 1. Kantarjian HM, et al. Blood. 2010;116: Lyons et al. ASH Abstract Kantarjian HM, et al. J Clin Oncol. 2010;28:
8 Case ,000 /ul (1,600/uL), 8.0 g/dl, 1,000/uL BM: blast 7.2%, cellularity 92-95%, 47,XY,+8 Dx: MDS, RAEB-1 치료는? (1) Darbepoietin (2) ATG / Cycloporin (3) Lenalidomide (4) Azacitidine / Decitabine (5) Allo SCT
9 Case ,000 /ul (1,600/uL), 8.0 g/dl, 1,000/uL BM: blast 7.2%, cellularity 92-95%, 47,XY,+8 Dx: MDS, RAEB-1 Tx: decitabine 4 cycles and allo SCT Relapse Pending state of AML Tx: RI induction chemotx and allo SCT
10 International Prognostic Scoring system (IPSS) 1997 Score value Variable Marrow blasts (%) < 5 5~10 11~20 21~30 Karyotype* Good Intermediate Poor Cytotpenia** 0, 1 2, 3 *Good = normal, -Y alone, del(5q) alone, del(20q) alone; Poor = complex ( 3 abnormalities) or chromosome 7 anomalies; Intermediate = other **Neutrophil < 1,800/uL, platelets < 100,000/uL, Hb < 10 g/dl Risk category Overall score Median survival (y) 25% AML progression (y) Low Intermediate-1 0.5~ Intermediate-2 1.5~ HIgh Greenberg P, et al. Blood. 1997;89: ; correction: 1998;91:1100.
11 Limitations of IPSS Not validated in numerous patient subsets Secondary MDS CMML with WBC > 12 x 10 9 /L Previously treated patients Children Limited number of karyotypes Only 3 categories Many common karyotypes omitted Does not account for molecular heterogeneity Omits validated prognostically relevant information LDH Mutations (eg, TP53, TET2) Performance score Marrow fibrosis, ALIP Absolute lymphocyte count
12 WHO-based Prognostic Scoring System (WPSS) Variable Scores WHO category RCUD, RARS, RCMD RAEB-1 RAEB-2 MDS with isolated del(5q) Karyotype* Good Intermediate Poor Severe anemia Absent Present (Hb < 9 g/dl, male; < 8g/dL, female) *Good = normal, -Y alone, del(5q) alone, del(20q) alone; poor = complex ( 3 abnorm alities) or chromosome 7 anomalies; Intermediate = other WPSS risk Sum of individual variable scores Very low 0 Low 1 Intermediate 2 High 3~4 Very high 5~6
13 Revised International Prognostic Scoring system (IPSS-R) 2012 Score value Variable Cytogenetics* Very good Good Intermediate Poor Very poor Marrow blasts (%) 2 > 2~< 5 5~10 > 10 Hemoglobin (g/dl) 10 8~<10 < 8 Platelets (x 10 9 /L) ~< 100 < 50 ANC (x 10 9 /L) 0.8 < New marrow blast categories 2. Refined cytogenetic abnormalities & risk groups : 16 (vs. 6) specific abnormalities, 5 (vs 3) subgroups 3. Evaluation of depth of cytopenias : clinically & statistically relevant cut-points used 4. Inclusion of differentiating features (for survival) : Age, PS, s-ferritin, LDH, B2-mg (provisional) 5. Prognostic model with 5 (vs 4) risk categories : improved predictive power Schanz J, et al. J Clin Oncol. 2012;30:
14 IPSS-R: Cytogenetic scoring & risk group Subgroup Cytogenetics OS AML evolution yrs 25%, yrs Very good -Y, del(11q) 5.4 NR Good normal, del(5q), del(12p), del(20q), double including del(5q) Intermediate del(7q), +8, +19, i(17q), any other single or double independent clones Poor -7, inv(3)/t(3q)/del(3q), double including -7/del(7q) complex (3 abnormalities) Very poor complex (> 3 abnormalities) IPSS-R Overall score Median 25% AML risk category survival (y) progression (y) Very low not reached Low > 1.5 ~ Intermediate > 3 ~ High > 4.5 ~ Very high > Greenberg P, et al. Blood in press
15 IPSS-R Survival related to Age Formula to generate the age-adjusted risk score in the figure: (yrs - 70) x [0.05 (IPSS-R risk score x 0.005)] Greenberg P, et al. Blood in press
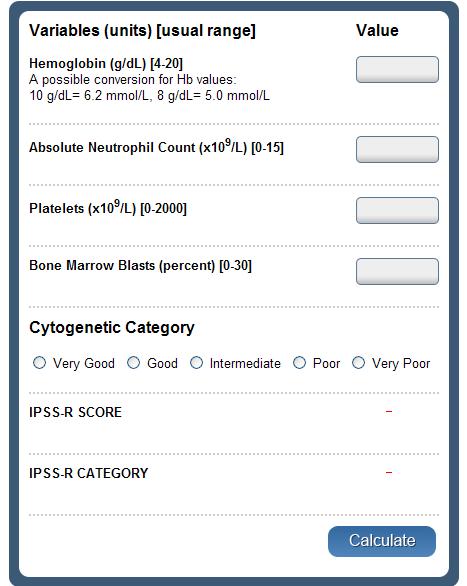
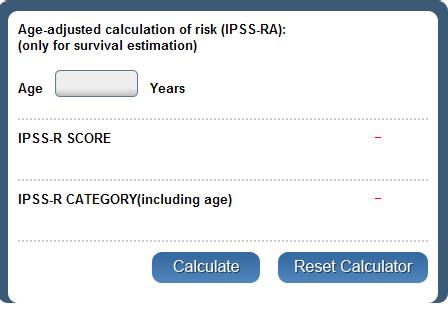
16 IPSS-R calculator
17 Fraction Survival Fraction AML-Free Survival IPSS-R and MDS outcome OS Transformation to AML 1.0 Very good (n = 81; events: 34) Good (n = 1809; events: 890) Intermediate (n = 529; events: 312) Poor (n = 148; events: 109) Very poor (n = 187; events: 158) 1.0 Very good (n = 72; events: 6) Good (n = 1611; events: 284) Intermediate (n = 457; events: 145) Poor (n = 129; events: 56) Very poor (n = 167; events: 47) 0.8 Log-rank P < Log-rank P < Mos Mos Schanz J, et al. J Clin Oncol. 2012;30:
18 Goals of MDS Therapy Select best treatment -Response according to predictive variables -Consider type and severity of cytopenia(s), age, and possible comorbidities LR-risk -Improve blood counts, quality of life; decrease infections -Decrease transfusion requirement, potentially improve survival HR-risk -Prolong survival, delay progression to AML Cheson BD, et al. Blood. 2000;96:
19 Treatment: LR-MDS NCCN Clinical Practice Guidelines ver
20 Treatment: LR-MDS NCCN Clinical Practice Guidelines ver
21 Treatment: HR-MDS NCCN Clinical Practice Guidelines ver
 Sanz GF, 2013")
22 GESMD Therapeutic algorithm for LR-MDS Grupo Espanol de Sindromes Mielodisplasicos (GESMD) Sanz GF, 2013 EHA

23 GESMD Therapeutic algorithm for HR-MDS Sanz GF, 2013 EHA
24 Predictive variables for ESA response in MDS Biological Clinical Endogeneous EPO levels < 500 U/L Marrow blast < 10% IPSS low, Int-1 Diagnosis of RA Normal karyotype Transfusion independence Short duration of Disease Santini, et al. The Oncologist 2011;16:35-42
25 IST of LR-MDS predictors of response Age < 60 yrs Normal karyotype Hypoplastic marrow HLA-DRB1-15 Ag Molldren 2002, Sauntaragiah 2002, 2003, Lim 2007, Sloand 2008
26 Phase III EPIC Trial: Mean Deferasirox Dose & Median Change in s-ferritin Cappellini MD, et Cappellini al. Haematologica. MD, et al. Haematologica. 2010;95:
27 Deferasirox in Transfusion-Dependent MDS (Prospective Study): Results Improvement in serum ferritin levels from baseline (-264 ng/ml) Deferasirox associated with 15% probability of achieving transfusion independence Caveat: only 45% of patients completed planned 1 yr of treatment Toxicity profile consistent with previous studies : 70% experienced toxicity (27% grade 3) Angelucci E, et al. ASH Abstract 425.
28 AZA-001: Trial Design Physician choice of 1 of 3 CCRs 1. BSC only 2. LDAC (20 mg/m 2 /day SC x 14 day q28-42 days) chemotherapy (induction consolidation cycles) Stratified by FAB: RAEB, RAEB-T IPSS: int-2, high R A N D O M I Z E Azacitidine + BSC (75 mg/m 2 /day x 7 days SC q28 days) CCR (Conventional care) (n = 179) (n = 179) Treatment continued until unacceptable toxicity or AML transformation or disease progression Fenaux P, et al. Lancet Oncol. 2009;10:
29 Proportion Surviving AZA-001 Trial: Azacitidine Significantly Improves OS mos HR: 0.58 (95% CI: ; log-rank P =.0001) 24.5 mos CCR Mos From Randomization Azacitidine Fenaux P, et al. Lancet Oncol. 2009;10:
30 Decitabine Phase III MDS Trial: Study Design Open-label, multicenter, 1:1 randomized study IPSS: int-1, int-2, and high-risk MDS patients eligible Primary endpoints: response, time to AML/death IWG response criteria utilized for assessment Eligible patients (N = 170) R A N D O M I Z E D Stratification IPSS Type of MDS (primary or secondary) Decitabine + Supportive Care 15 mg/m 2 / over 3 hrs q8h x 3 days q6w (n = 89) Supportive Care ABX, GFs, and/or transfusions (n = 81) Kantarjian H, et al. Cancer. 2006;106:
 Kantarjian H, et al. Cancer.")
31 Decitabine Phase III Trial: Response to Decitabine (ITT) *For patients with a confirmed date of progression. Best response observed after 2 cycles (median number of cycles = 3) Kantarjian H, et al. Cancer. 2006;106:
32 Phase III EORTC 06011: LD Decitabine vs BSC in Elderly, Int- or High-Risk MDS 3-day inpatient schedule Stratified by IPSS score, primary vs secondary disease, cytogenetic risk, study center Stop at 2 cycles beyond CR or max of 8 cycles Patients with intermediate- or hi gh-risk MDS or CMML, 60 yrs of age or older, 11% to 20 % blasts or < 11% with poor cyto genetics or 21% to 30% with stab le disease for 1 mo (N = 233) Decitabine 15 mg/m 2 IV over 4 hrs q8h x 9 q6w (n = 119) Best Supportive Care (n = 114) Primary endpoint: OS Lübbert M, et al. J Clin Oncol. 2011;29:
33 Phase III Study of LD Decitabine vs BSC in Elderly, Int- or High-Risk MDS: Results Median cycles of decitabine: 4 2 cycles: 38% Compare with a median of 9 cycles in AZA-001 study Responses in treatment arm (IWG 2000 criteria): 34% 13% CR, 6% PR, 15% HI Median time to best response: 3.8 mos Median time to CR: 5.8 mos; PR: 2.9 mos; HI: 3.8 mos Lübbert M, et al. J Clin Oncol. 2011;29:
34 Overall Survival: EORTC No difference in median OS: 10.1 mos for decitabine vs 8.5 mos for supportive care (P =.38) Supportive care Decitabine Median (mos): 10.1 vs 8.5 HR: 0.88 (95% CI: ; log rank P =.3 8) Mos O N Patients at Risk, n Wijermans P, et al. ASH Abstract 226.
35 Progression-Free Survival: EORTC Supportive care No difference in progression to AML: 8.8 mos for decitabine vs 6.1 mos for supportive care (P =.24) Decitabine Modestly but significantly improved median PFS (including higher-risk MDS) : 6.6 mos for decitabine vs 3.0 mos for supportive care (P =.004) Mos O N Patients at Risk, n Wijermans P, et al. ASH Abstract 226.
36 LD-Decitabine & OS in elderly MDS Not optimal decitabine schedule (3-day inpatient vs 5-day outpatient treatment) Small numbers of cycles 40% received 2 cycles or less Median of 4 cycles vs 9 cycles in AZA-001 Higher-risk patient group Control arm lived median of 15 mos in AZA-001 vs 8.5 mos in EORTC study Lübbert M, et al. J Clin Oncol. 2011;29:
37 Hypomethylating Agents Relative merits of azacitidine vs decitabine Role for 1 hypomethylating agent when the other has failed Is there a survival advantage when decitabine is administered using current c ommon practice (ie, 5-day regimen, more cycles)? Optimal dose/schedule What to do once patient achieves CR (ie, maintenance dosing question; need for maintenance seems to be established) What to do in patients without a response Molecular predictors of response Use in combination therapies Actual mechanism of action
38 Predictive factors for response to hypomethylaing agents Clinical Positive Negative Doubling platelets BM blasts > 15% Previous therapy Transfusion dependency Marrow fibrosis gr 3 Molecular Positive Negative Mutated TET2 Mutated p53 Mutated DNMT3a Abnormal/complex karyotype Mutated IDH1/2 Mutated ASXL1 Mutated EZH2 Santini V ASH
39 TET2 mutations & response to azacitidine Itzykson et al. Leukemia 2011

40 Mutational status in LR-MDS Bejar et al. JCO 2012
: low risk = 0, intermediate risk = 1-3, high risk = 4-5 R-IPSS used to examine response to azacitidine and OS GFM: Groupe Francais des Myelodysplasies Ades L, et al. ASH 2012.")
41 IPSS-R in Azacitidine-Treated MDS Retrospective study of 265 patients with intermediate-2- or high-risk MDS treated in French tertiary care centers AZA prognostic scoring system (reported previously by GFM): low risk = 0, intermediate risk = 1-3, high risk = 4-5 R-IPSS used to examine response to azacitidine and OS GFM: Groupe Francais des Myelodysplasies Ades L, et al. ASH Abstract 422.

42 IPSS-R in Azacitidine-Treated MDS R-IPSS strongly prognostic for OS in azacitidine-treated patients with Overall Sruvival high-risk MDS 1.00 Not predictive of response to azacitidine Prognostic value refined with use of azacitidine scoring systems P = Months Ades L, et al. ASH Abstract 422
43 Continued Azacitidine treatment after first response? Time to 1 st response in HR-MDS Silverman LR et al. Cancer 2011;117:
44 Continued Azacitidine treatment after first response? Continued azacitidine Tx after 1 st response improves quality of response in HR-MDS 52%: 1 st response = best response 48%: improvement in their 1 st response with continued therapy (1 st R: HI -> PR or CR) Silverman LR et al. Cancer 2011;117:
45 Combination therapy with hypomethylating agents in MDS N ORR Azacitidine Phenylbutyrate 32 34% Azacitidine Valproic acid, ATRA 62 46% Azacitidine Entinostate % Azacitidine Lenalidomide 18 71% Azacitidine Thalidomide 36 58% Decitabine G. O % Azacitidine Entanercept 32 72% Azacitidine Erythropoietin 32 44% Azacitidine Romiplostim 40 23% Decitabine Romiplostim 40 16% Santini V ASH

46 Outcome After Azcitidine Failure in MDS *Includes AZA001, GFM, and JHU studies. Decitabine only. 1. Lin K, et al. ASH Abstract Prebet T, et al. ASH Abstract Jabbour E, et al. Cancer. 2010;116:
47 Survival after Azacitidine failure with Salvage treatments in HR-MDS/AML Palliative care vs. Intensive CTx p=0.04 vs. Investigational Tx. p<0.001 vs. AlloHSCT p< Intensive CTx vs. IT p=0.05 vs. ASCT p=0.008 IT vs. ASCT p=0.09 Prebet et al. J Clin Oncol 2011; 29: 3322
48 AlloSCT in MDS Transplantation is the only curative method in MDS Best results with young age, marrow blasts < 5%, absence marrow fibrosis, interval to SCT < 5 years, matched sibling donor Very limited donor availability, advanced age 75% of pts with MDS >60 Treatment-related mortality 34-55% Relapse 19-34% High treatment-related morbidity : Patients may have RFS, but not truly DFS 25% 33% 42% TRM DFS Relapse
49 HSCT outcomes in MDS Ghulam J. M. et al. ASH 2012
50 Timing of Transplantation Approximate Life Expectancy (Yrs) for Ablative Allogeneic Transplantation Transplantation at Diagnosis Transplantation in 2 Yrs Transplantation at Progression Low Int Int High Low & Int-1 : benefit for delaying SCT Int-2 & high : delay in time to SCT is associated with a loss in survivorship Cutler et al. Blood 2004

51 Timing of Transplantation Gain in expected survival since diagnosis according to IPSS & WPSS models under different policies with respect to a non-transplantation policy Alessandrino E. P. et al. GITMO, Am J Hematol 2013 in press

52 Timing of Transplantation Allo SCT offers optimal survival benefit when it is performed early in INT-1 IPSS or Intermediate WPSS Alessandrino E. P. et al. GITMO, Am J Hematol 2013 in press
53 Induction prior to allosct Disease stage & cytogenetics: predictors of OS, relapse and NRM Before allosct -decrease pre-transplant disease burden -time to find optimal donor Infection or comorbidity -lose a chance for transplantation
54 Pre-transplant Azacitidine 3 yr OS Relapse Damaj et al, JCO 2012;30:


55 Pre-transplant Azacitidine agvhd: N-S extensive cgvhd: higher in AZA-ICT group (p=0.049) TRM For the purpose of reducing tumor burden before allosct AZA showed comparative OS, EFS, relapse and NRM compare with ICT Damaj et al, JCO 2012;30:
56 Pre-transplant Hypomethylating Agents 2yr DFS 49 AZA, 4 DEC, 3 AZA-DEC Response to HMT G-COR: continued response G-NoC: no change G-LOR: loss of response G-DP: progression G-stable Yahng SA et al. Eur J Haematol 2013;90:11-20
57 Pre-transplant Hypomethylating Agents Independent risk factor for DFS, relapse : Response to HMA & Karyotype at HSCT Yahng SA et al. Eur J Haematol 2013;90:11-20
58 Post-transplant Salvage Usually relapse within 1 or 2 years after HSCT Number of patients relapsing after allosct as a function of time elapsed from transplantation > 900 Days post Transplant
59 Post-transplant Salvage MRD based preemptive 5-Aza Tx in MDS/AML after allosct (RELAZA trial) (n=20) DC, donor chimerism Platzbecker U. et al. Leukemia 2012;26:
 Hematologic Relapse: 65% Relapse was delayed median 231 days")
60 Post-transplant Salvage Platzbecker U. et al. Leukemia 2012;26: Major R Minor R no Response Relapse no Relapse Relapse Response: 16/20 (80%) Hematologic Relapse: 65% Relapse was delayed median 231 days after initial decrease of CD34+ chimerism to <80% Preemptive AZA: acceptable safety & prevent or delay hematologic relapse
 DLI: every 2 nd AZA cycle ORR: 30% (CR 23%, 2 PR) agvhd 37%, cgvhd 17% CR or CRi : longer OS Schroeder et al.")
61 Post-transplant Salvage Azacitidine + DLI in AML (28) or MDS (2) relapsing after allosct (AZARELAR trial) AZA: 8 cycles, D1-5 (median 3) DLI: every 2 nd AZA cycle ORR: 30% (CR 23%, 2 PR) agvhd 37%, cgvhd 17% CR or CRi : longer OS Schroeder et al. Leukemia 2013
62 감사합니다!!
Treating Higher-Risk MDS. Case presentation. Defining higher risk MDS. IPSS WHO IPSS: WPSS MD Anderson PSS
 Treating Higher-Risk MDS Eyal Attar, M.D. Massachusetts General Hospital Cancer Center eattar@partners.org 617-724-1124 Case presentation 72 year old man, prior acoustic neuroma WBC (X10 3 /ul) 11/08 12/08
Treating Higher-Risk MDS Eyal Attar, M.D. Massachusetts General Hospital Cancer Center eattar@partners.org 617-724-1124 Case presentation 72 year old man, prior acoustic neuroma WBC (X10 3 /ul) 11/08 12/08
Myelodysplastic Syndromes. Post-ASH meeting 2014 Marie-Christiane Vekemans
 Myelodysplastic Syndromes Post-ASH meeting 2014 Marie-Christiane Vekemans Agenda New biological developments Risk assessment and prognostic factors New therapeutic options Agenda New biological developments
Myelodysplastic Syndromes Post-ASH meeting 2014 Marie-Christiane Vekemans Agenda New biological developments Risk assessment and prognostic factors New therapeutic options Agenda New biological developments
Table 1: biological tests in SMD
 Table 1: biological tests in SMD Tests Mandatory Recommended Under validation Morphology Marrow aspirate Marrow biopsy 1 Iron staining Quantification of dysplasia WHO 2008 Classification Cytogenetics Conventional
Table 1: biological tests in SMD Tests Mandatory Recommended Under validation Morphology Marrow aspirate Marrow biopsy 1 Iron staining Quantification of dysplasia WHO 2008 Classification Cytogenetics Conventional
Emerging Treatment Options for Myelodysplastic Syndromes
 Emerging Treatment Options for Myelodysplastic Syndromes James K. Mangan, MD, PhD Assistant Professor of Clinical Medicine Abramson Cancer Center, University of Pennsylvania Please note that some of the
Emerging Treatment Options for Myelodysplastic Syndromes James K. Mangan, MD, PhD Assistant Professor of Clinical Medicine Abramson Cancer Center, University of Pennsylvania Please note that some of the
Management of low and high risk MDS
 Management of low and high risk MDS D.Selleslag AZ Sint-Jan Brugge, Belgium Brussels, 4th October 2014 Low / int 1 risk MDS Improve QOL Improve cytopenia Int 2 / high risk MDS Delay progression To AML
Management of low and high risk MDS D.Selleslag AZ Sint-Jan Brugge, Belgium Brussels, 4th October 2014 Low / int 1 risk MDS Improve QOL Improve cytopenia Int 2 / high risk MDS Delay progression To AML
La lenalidomide: meccanismo d azione e risultati terapeutici. F. Ferrara
 La lenalidomide: meccanismo d azione e risultati terapeutici F. Ferrara MDS: new treatment goals Emerging treatment options expected to facilitate shift from supportive care to active therapy in MDS New
La lenalidomide: meccanismo d azione e risultati terapeutici F. Ferrara MDS: new treatment goals Emerging treatment options expected to facilitate shift from supportive care to active therapy in MDS New
Low Risk MDS Scoring System. Prognosis in Low Risk MDS. LR-PSS Validation 9/19/2012
 Advances in MDS What s on the Horizon Tapan M. Kadia, MD Department of Leukemia MD Anderson Cancer Center Outline Newer Prognostic Systems Hypomethylating agent failures Newer Treatment approaches Role
Advances in MDS What s on the Horizon Tapan M. Kadia, MD Department of Leukemia MD Anderson Cancer Center Outline Newer Prognostic Systems Hypomethylating agent failures Newer Treatment approaches Role
Myelodysplastic Syndromes (MDS) Enhancing the Nurses Role in Management
 Enhancing the Nurses Role in Management") Myelodysplastic Syndromes (MDS) Enhancing the Nurses Role in Management Christa Roe, RN, BS, OCN Malignant Hematology Department H Lee Moffitt Cancer Center & Research Tampa, Florida Agenda MDS Disease
Myelodysplastic Syndromes (MDS) Enhancing the Nurses Role in Management Christa Roe, RN, BS, OCN Malignant Hematology Department H Lee Moffitt Cancer Center & Research Tampa, Florida Agenda MDS Disease
myelodysplastic syndrome MDS MDS MDS
 myelodysplastic syndrome MDS MDS 15 10 3 2004 15 MDS 400 2 65 61 70 MDS MDS 1 1 2 3 3 4 1 4 2 3 4 MDS 1982 Bennett French- American-BritishFAB 1 2 WHO 1999 3 2001 4 2002 Vardiman MDS 5 2WHO FAB refractory
myelodysplastic syndrome MDS MDS 15 10 3 2004 15 MDS 400 2 65 61 70 MDS MDS 1 1 2 3 3 4 1 4 2 3 4 MDS 1982 Bennett French- American-BritishFAB 1 2 WHO 1999 3 2001 4 2002 Vardiman MDS 5 2WHO FAB refractory
MYELODYSPLASTIC SYNDROMES: A diagnosis often missed
 MYELODYSPLASTIC SYNDROMES: A diagnosis often missed D R. EMMA W YPKEMA C O N S U LTA N T H A E M AT O L O G I S T L A N C E T L A B O R AT O R I E S THE MYELODYSPLASTIC SYNDROMES DEFINITION The Myelodysplastic
MYELODYSPLASTIC SYNDROMES: A diagnosis often missed D R. EMMA W YPKEMA C O N S U LTA N T H A E M AT O L O G I S T L A N C E T L A B O R AT O R I E S THE MYELODYSPLASTIC SYNDROMES DEFINITION The Myelodysplastic
Emerging Treatment Options for Myelodysplastic Syndromes
 Emerging Treatment Options for Myelodysplastic Syndromes James K. Mangan, MD, PhD Assistant Professor of Clinical Medicine Abramson Cancer Center, University of Pennsylvania Please note that some of the
Emerging Treatment Options for Myelodysplastic Syndromes James K. Mangan, MD, PhD Assistant Professor of Clinical Medicine Abramson Cancer Center, University of Pennsylvania Please note that some of the
MDS-004 Study: REVLIMID (lenalidomide) versus Placebo in Myelodysplastic Syndromes with Deletion (5q) Abnormality
 versus Placebo in Myelodysplastic Syndromes with Deletion (5q) Abnormality") MDS-4 Study: REVLIMID (lenalidomide) versus Placebo in Myelodysplastic Syndromes with Deletion (5q) Abnormality TABLE OF CONTENTS Section 1. Executive Summary Section 2. Background Section
MDS-4 Study: REVLIMID (lenalidomide) versus Placebo in Myelodysplastic Syndromes with Deletion (5q) Abnormality TABLE OF CONTENTS Section 1. Executive Summary Section 2. Background Section
Myelodysplastic syndromes post ASH Dominik Selleslag AZ Sint-Jan Brugge
 Myelodysplastic syndromes post ASH 2016 Dominik Selleslag AZ Sint-Jan Brugge Why did they put MDS at the end of the meeting? Possible explanations Least fascinating disease without progress? Poor speaker?
Myelodysplastic syndromes post ASH 2016 Dominik Selleslag AZ Sint-Jan Brugge Why did they put MDS at the end of the meeting? Possible explanations Least fascinating disease without progress? Poor speaker?
Outline. Case Study 5/17/2010. Treating Lower-Risk Myelodysplastic Syndrome (MDS) Tapan M. Kadia, MD Department of Leukemia MD Anderson Cancer Center
 Tapan M. Kadia, MD Department of Leukemia MD Anderson Cancer Center") Treating Lower-Risk Myelodysplastic Syndrome (MDS) Tapan M. Kadia, MD Department of Leukemia MD Anderson Cancer Center Outline Case Study What is lower-risk MDS? Classification systems Prognosis Treatment
Treating Lower-Risk Myelodysplastic Syndrome (MDS) Tapan M. Kadia, MD Department of Leukemia MD Anderson Cancer Center Outline Case Study What is lower-risk MDS? Classification systems Prognosis Treatment
Dr Kavita Raj Consultant Haematologist Guys and St Thomas Hospital
 Dr Kavita Raj Consultant Haematologist Guys and St Thomas Hospital IPSS scoring system Blood counts Bone marrow blast percentage Cytogenetics Age as a modulator of median survival IPSS Group Median Survival
Dr Kavita Raj Consultant Haematologist Guys and St Thomas Hospital IPSS scoring system Blood counts Bone marrow blast percentage Cytogenetics Age as a modulator of median survival IPSS Group Median Survival
Emerging Treatment Options for Myelodysplastic Syndromes
 Emerging Treatment Options for Myelodysplastic Syndromes James K. Mangan, MD, PhD Assistant Professor of Clinical Medicine Abramson Cancer Center, University of Pennsylvania Please note that some of the
Emerging Treatment Options for Myelodysplastic Syndromes James K. Mangan, MD, PhD Assistant Professor of Clinical Medicine Abramson Cancer Center, University of Pennsylvania Please note that some of the
MYELODYSPLASTIC SYNDROME. Vivienne Fairley Clinical Nurse Specialist Sheffield
 MYELODYSPLASTIC SYNDROME Vivienne Fairley Clinical Nurse Specialist Sheffield MDS INCIDENCE 1/100,000/YEAR 3,250/YEAR MEDIAN AGE 70 MDS HYPO OR HYPERCELLULAR BONE MARROW BLOOD CYTOPENIAS (EARLY STAGES
MYELODYSPLASTIC SYNDROME Vivienne Fairley Clinical Nurse Specialist Sheffield MDS INCIDENCE 1/100,000/YEAR 3,250/YEAR MEDIAN AGE 70 MDS HYPO OR HYPERCELLULAR BONE MARROW BLOOD CYTOPENIAS (EARLY STAGES
Let s Look at Our Blood
 Let s Look at Our Blood Casey O Connell, MD Associate Professor of Clinical Medicine Jane Anne Nohl Division of Hematology Keck School of Medicine of USC 10,000,000,000 WBCs/day Bone Marrow: The Blood
Let s Look at Our Blood Casey O Connell, MD Associate Professor of Clinical Medicine Jane Anne Nohl Division of Hematology Keck School of Medicine of USC 10,000,000,000 WBCs/day Bone Marrow: The Blood
Myelodysplastic syndrome. Jeanne Palmer, MD Mayo Clinic, Arizona
 Myelodysplastic syndrome Jeanne Palmer, MD Mayo Clinic, Arizona What is Myelodysplastic syndrome? A disease where the bone marrow doesn t work appropriately What does that mean?? Red blood cells Carry
Myelodysplastic syndrome Jeanne Palmer, MD Mayo Clinic, Arizona What is Myelodysplastic syndrome? A disease where the bone marrow doesn t work appropriately What does that mean?? Red blood cells Carry
ACCME/Disclosures. History. Hematopathology Specialty Conference Case #4 4/13/2016
 Hematopathology Specialty Conference Case #4 Sherrie L. Perkins MD, PhD University of Utah ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose
Hematopathology Specialty Conference Case #4 Sherrie L. Perkins MD, PhD University of Utah ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose
Should patients with higher risk MDS (or AML in «early relapse») proceed directly to allo SCT without prior chemotherapy?
 proceed directly to allo SCT without prior chemotherapy?") Should patients with higher risk MDS (or AML in «early relapse») proceed directly to allo SCT without prior chemotherapy? Pierre Fenaux Cohem 2012 Barcelona Should patients with higher risk MDS (or AML
Should patients with higher risk MDS (or AML in «early relapse») proceed directly to allo SCT without prior chemotherapy? Pierre Fenaux Cohem 2012 Barcelona Should patients with higher risk MDS (or AML
Impact of Comorbidity on Quality of Life and Clinical Outcomes in MDS
 Current Therapeutic and Biologic Advances in MDS A Symposium of The MDS Foundation ASH 2014 Impact of Comorbidity on Quality of Life and Clinical Outcomes in MDS Peter Valent Medical University of Vienna
Current Therapeutic and Biologic Advances in MDS A Symposium of The MDS Foundation ASH 2014 Impact of Comorbidity on Quality of Life and Clinical Outcomes in MDS Peter Valent Medical University of Vienna
MDS FDA-approved Drugs
 MDS: Current Thinking on the Disease, Diagnosis, and Treatment Mikkael A. Sekeres, MD, MS Associate Professor of Medicine Director, Leukemia Program Dept of Hematologic Oncology and Blood Disorders Taussig
MDS: Current Thinking on the Disease, Diagnosis, and Treatment Mikkael A. Sekeres, MD, MS Associate Professor of Medicine Director, Leukemia Program Dept of Hematologic Oncology and Blood Disorders Taussig
Should lower-risk myelodysplastic syndrome patients be transplanted upfront? YES Ibrahim Yakoub-Agha France
 Should lower-risk myelodysplastic syndrome patients be transplanted upfront? YES Ibrahim Yakoub-Agha France Myelodysplastic syndromes (MDS) are heterogeneous disorders that range from conditions with a
Should lower-risk myelodysplastic syndrome patients be transplanted upfront? YES Ibrahim Yakoub-Agha France Myelodysplastic syndromes (MDS) are heterogeneous disorders that range from conditions with a
Acute Myeloid Leukemia
 Acute Myeloid Leukemia Pimjai Niparuck Division of Hematology, Department of Medicine Ramathibodi Hospital, Mahidol University Outline Molecular biology Chemotherapy and Hypomethylating agent Novel Therapy
Acute Myeloid Leukemia Pimjai Niparuck Division of Hematology, Department of Medicine Ramathibodi Hospital, Mahidol University Outline Molecular biology Chemotherapy and Hypomethylating agent Novel Therapy
Non-transplant Therapy for MDS. Bart Scott, MD Associate Member, FHCRC Associate Professor, UWMC
 Non-transplant Therapy for MDS Bart Scott, MD Associate Member, FHCRC Associate Professor, UWMC MDS Treatment Algorithm Asymptomatic Symptomatic Bone Marrow Function Low/Int-1 Int-2/High Observation Cytokine
Non-transplant Therapy for MDS Bart Scott, MD Associate Member, FHCRC Associate Professor, UWMC MDS Treatment Algorithm Asymptomatic Symptomatic Bone Marrow Function Low/Int-1 Int-2/High Observation Cytokine
Prognostic Scoring Systems for Therapeutic Decision Making in MDS. Peter Greenberg, MD Stanford University Cancer Center Stanford, CA
 Prognostic Scoring Systems for Therapeutic Decision Making in MDS Peter Greenberg, MD Stanford University Cancer Center Stanford, CA DISCLOSURE I have no relevant financial relationships to disclose. MDSs:
Prognostic Scoring Systems for Therapeutic Decision Making in MDS Peter Greenberg, MD Stanford University Cancer Center Stanford, CA DISCLOSURE I have no relevant financial relationships to disclose. MDSs:
Refining Prognosis. Overview. Low Blood Counts. Low Blood Counts. High Risk MDS and Novel Therapy: What s on the Horizon? 3/2/2016
 High Risk MDS and Novel Therapy: What s on the Horizon? Rafael Bejar MD, PhD Aplastic Anemia & MDS International Foundation Regional Patient and Family Conference March 19 th, 216 Overview Refining Prognosis
High Risk MDS and Novel Therapy: What s on the Horizon? Rafael Bejar MD, PhD Aplastic Anemia & MDS International Foundation Regional Patient and Family Conference March 19 th, 216 Overview Refining Prognosis
Treatment of low risk MDS
 Treatment of low risk MDS Matteo G Della Porta Cancer Center IRCCS Humanitas Research Hospital & Humanitas University Rozzano Milano, Italy matteo.della_porta@hunimed.eu International Prognostic Scoring
Treatment of low risk MDS Matteo G Della Porta Cancer Center IRCCS Humanitas Research Hospital & Humanitas University Rozzano Milano, Italy matteo.della_porta@hunimed.eu International Prognostic Scoring
Myelodysplastic Syndromes: Understanding your diagnosis and current and emerging treatments
 Myelodysplastic Syndromes: Understanding your diagnosis and current and emerging treatments Shyamala Navada, M.D., MSCR Assistant Professor Icahn School of Medicine at Mount Sinai Tisch Cancer Institute
Myelodysplastic Syndromes: Understanding your diagnosis and current and emerging treatments Shyamala Navada, M.D., MSCR Assistant Professor Icahn School of Medicine at Mount Sinai Tisch Cancer Institute
Treatment of Low-Blast Count AML. Maria Teresa Voso Dipartimento di Biomedicina e Prevenzione Università di Roma Tor Vergata
 Treatment of Low-Blast Count AML Maria Teresa Voso Dipartimento di Biomedicina e Prevenzione Università di Roma Tor Vergata Definition of Low-Blast Count AML Blast counts 20-30%, or > 10%? v Retrospective
Treatment of Low-Blast Count AML Maria Teresa Voso Dipartimento di Biomedicina e Prevenzione Università di Roma Tor Vergata Definition of Low-Blast Count AML Blast counts 20-30%, or > 10%? v Retrospective
Network Guidance Document. Oncological treatment of Haematology. Myelodysplastic Syndromes (MDS) Final. Status: November 2012.
 Final. Status: November 2012.") Network Guidance Document Oncological treatment of Haematology Myelodysplastic Syndromes (MDS) Status: Final Expiry Date: November 2012 Version Number: 1 Publication Date: November 2010 Page 1 of 14T:\DOG
Network Guidance Document Oncological treatment of Haematology Myelodysplastic Syndromes (MDS) Status: Final Expiry Date: November 2012 Version Number: 1 Publication Date: November 2010 Page 1 of 14T:\DOG
Your Speaker. Outline 10/2/2017. Myelodysplastic Syndromes and Myeloid Neoplasms. Introduction and classifications Epidemiology Presentation Workup
 Myelodysplastic Syndromes and Myeloid Neoplasms Abdulraheem Yacoub, MD Associate Professor Of Medicine Clinical Director of Ambulatory Hematology clinics The University of Kansas Cancer Center Your Speaker
Myelodysplastic Syndromes and Myeloid Neoplasms Abdulraheem Yacoub, MD Associate Professor Of Medicine Clinical Director of Ambulatory Hematology clinics The University of Kansas Cancer Center Your Speaker
No benefit of hypomethylating agents compared to supportive care for higher risk myelodysplastic syndrome
 ORIGINAL ARTICLE Korean J Intern Med 2018;33:1194-1202 No benefit of hypomethylating agents compared to supportive care for higher risk myelodysplastic syndrome Sang Kyun Sohn 1, Joon Ho Moon 1, In Hee
ORIGINAL ARTICLE Korean J Intern Med 2018;33:1194-1202 No benefit of hypomethylating agents compared to supportive care for higher risk myelodysplastic syndrome Sang Kyun Sohn 1, Joon Ho Moon 1, In Hee
AML IN OLDER PATIENTS Whenever possible, intensive induction therapy should be considered
 AML IN OLDER PATIENTS Whenever possible, intensive induction therapy should be considered Charles A. Schiffer, M.D. Karmanos Cancer Institute Wayne State University School of Medicine Detroit, MI WHY ARE
AML IN OLDER PATIENTS Whenever possible, intensive induction therapy should be considered Charles A. Schiffer, M.D. Karmanos Cancer Institute Wayne State University School of Medicine Detroit, MI WHY ARE
What is MDS? Epidemiology, Diagnosis, Classification & Risk Stratification
 What is MDS? Epidemiology, Diagnosis, Classification & Risk Stratification Rami Komrokji, MD Clinical Director Malignant Hematology Moffitt Cancer Center Normal Blood and Bone Marrow What is MDS Myelodysplastic
What is MDS? Epidemiology, Diagnosis, Classification & Risk Stratification Rami Komrokji, MD Clinical Director Malignant Hematology Moffitt Cancer Center Normal Blood and Bone Marrow What is MDS Myelodysplastic
Disclosure Slide. Research Support: Onconova Therapeutics, Celgene
 Oral Rigosertib Combined with Azacitidine in Patients with Acute Myeloid Leukemia (AML) and Myelodysplastic Syndromes (MDS): Effects in Treatment Naïve and Relapsed- Refractory Patients Shyamala C. Navada,
Oral Rigosertib Combined with Azacitidine in Patients with Acute Myeloid Leukemia (AML) and Myelodysplastic Syndromes (MDS): Effects in Treatment Naïve and Relapsed- Refractory Patients Shyamala C. Navada,
Overview. Myelodysplastic Syndromes: What s on the Horizon? Molecular Mutations in MDS. Refining Risk Models. Incorporating Mutational Data
 Myelodysplastic Syndromes: What s on the Horizon? Vu H. Duong, MD, MS Assistant Professor of Medicine University of Maryland July 16, 2016 Overview Refining Risk models Specific Therapeutic Areas of Need
Myelodysplastic Syndromes: What s on the Horizon? Vu H. Duong, MD, MS Assistant Professor of Medicine University of Maryland July 16, 2016 Overview Refining Risk models Specific Therapeutic Areas of Need
LENALIDOMIDA EN EL SMD 5Q-
 LENALIDOMIDA EN EL SMD 5Q- EXPERIENCIA ESPAÑOLA 37 Diada Internacional 7 de Junio de 2013 M. Díez Campelo Hematología HOSPITAL UNIVERSITARIO 15-30% MDS Introduction Sole anomaly or in addition to 1 cytogenetics
LENALIDOMIDA EN EL SMD 5Q- EXPERIENCIA ESPAÑOLA 37 Diada Internacional 7 de Junio de 2013 M. Díez Campelo Hematología HOSPITAL UNIVERSITARIO 15-30% MDS Introduction Sole anomaly or in addition to 1 cytogenetics
IPSS Modified 7/27/2011. WHO-Based Prognostic Scoring System (WPSS)
") Advances in MDS Treatment: What s on the Horizon? New Prognostic Models and Therapies Jason Gotlib, MD, MS Assistant Professor of Medicine (Hematology) Stanford Cancer Center AA&MDSIF July 3, 011 WHO-Based
Advances in MDS Treatment: What s on the Horizon? New Prognostic Models and Therapies Jason Gotlib, MD, MS Assistant Professor of Medicine (Hematology) Stanford Cancer Center AA&MDSIF July 3, 011 WHO-Based
Myelodysplastic syndromes: 2018 update on diagnosis, risk-stratification and management
 Received: 2 October 2017 Accepted: 2 October 2017 DOI: 10.1002/ajh.24930 ANNUAL CLINICAL UPDATES IN HEMATOLOGICAL MALIGNANCIES Myelodysplastic syndromes: 2018 update on diagnosis, risk-stratification and
Received: 2 October 2017 Accepted: 2 October 2017 DOI: 10.1002/ajh.24930 ANNUAL CLINICAL UPDATES IN HEMATOLOGICAL MALIGNANCIES Myelodysplastic syndromes: 2018 update on diagnosis, risk-stratification and
Myelodysplastic syndromes and the new WHO 2016 classification
 Myelodysplastic syndromes and the new WHO 2016 classification 32nd General Annual Meeting of the Belgian Hematology Society 10-11 February 2017 Gregor Verhoef, Departement of Hematology, University Hospital
Myelodysplastic syndromes and the new WHO 2016 classification 32nd General Annual Meeting of the Belgian Hematology Society 10-11 February 2017 Gregor Verhoef, Departement of Hematology, University Hospital
Clinical Roundtable Monograph
 Clinical Roundtable Monograph C l i n i c a l A d v a n c e s i n H e m a t o l o g y & O n c o l o g y J u l y 2 0 0 9 Treatment Selection for Myelodysplastic Syndrome Patients in the Community Setting
Clinical Roundtable Monograph C l i n i c a l A d v a n c e s i n H e m a t o l o g y & O n c o l o g y J u l y 2 0 0 9 Treatment Selection for Myelodysplastic Syndrome Patients in the Community Setting
AML in elderly. D.Selleslag AZ Sint-Jan Brugge, Belgium 14 December 2013
 AML in elderly D.Selleslag AZ Sint-Jan Brugge, Belgium 14 December 2013 AML is predominantly a disease of the elderly incidence 2 3/100.000 SEER Cancer Statistics, National Cancer Institute, USA 2002 2006
AML in elderly D.Selleslag AZ Sint-Jan Brugge, Belgium 14 December 2013 AML is predominantly a disease of the elderly incidence 2 3/100.000 SEER Cancer Statistics, National Cancer Institute, USA 2002 2006
Understanding & Treating Myelodysplastic Syndrome (MDS)
") Understanding & Treating Myelodysplastic Syndrome (MDS) Casey O Connell, MD Associate Professor of Clinical Medicine Jane Anne Nohl Division of Hematology Keck School of Medicine of USC Let s Look at Our
Understanding & Treating Myelodysplastic Syndrome (MDS) Casey O Connell, MD Associate Professor of Clinical Medicine Jane Anne Nohl Division of Hematology Keck School of Medicine of USC Let s Look at Our
ASBMT MDS/MPN Update Sunil Abhyankar, MD
 ASBMT MDS/MPN Update Sunil Abhyankar, MD Professor of Medicine Medical Director, Pheresis and Cell Processing Division of Hematologic Malignancies and Cellular Therapeutics Department of Internal Medicine
ASBMT MDS/MPN Update Sunil Abhyankar, MD Professor of Medicine Medical Director, Pheresis and Cell Processing Division of Hematologic Malignancies and Cellular Therapeutics Department of Internal Medicine
NOVEL APPROACHES IN THE CLASSIFICATION AND RISK ASSESSMENT OF PATIENTS WITH MYELODYSPLASTIC SYNDROMES-CLINICAL IMPLICATION
 ORIGINAL ARTICLES NOVEL APPROACHES IN THE CLASSIFICATION AND RISK ASSESSMENT OF PATIENTS WITH MYELODYSPLASTIC SYNDROMES-CLINICAL IMPLICATION Ilina Micheva 1, Rosen Rachev 1, Hinco Varbanov 1, Vladimir
ORIGINAL ARTICLES NOVEL APPROACHES IN THE CLASSIFICATION AND RISK ASSESSMENT OF PATIENTS WITH MYELODYSPLASTIC SYNDROMES-CLINICAL IMPLICATION Ilina Micheva 1, Rosen Rachev 1, Hinco Varbanov 1, Vladimir
Allogeneic Hematopoietic Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Neoplasms
 Allogeneic Hematopoietic Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Neoplasms Policy Number: 8.01.21 Last Review: 1/2019 Origination: 12/2001 Next Review: 1/2020 Policy Blue
Allogeneic Hematopoietic Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Neoplasms Policy Number: 8.01.21 Last Review: 1/2019 Origination: 12/2001 Next Review: 1/2020 Policy Blue
Myelodysplastic syndromes
 Myelodysplastic syndromes Robert P Hasserjian Massachusetts General Hospital, Boston, MA Disclosure of Relevant Financial Relationships Dr. Hasserjian declares he has no conflict(s) of interest to disclose.
Myelodysplastic syndromes Robert P Hasserjian Massachusetts General Hospital, Boston, MA Disclosure of Relevant Financial Relationships Dr. Hasserjian declares he has no conflict(s) of interest to disclose.
What you need to know about MDS. The Myelodysplastic Syndromes. Stuart Goldberg MD
 What you need to know about MDS The Myelodysplastic Syndromes Stuart Goldberg MD The Myelodysplastic Syndromes are a group of bone marrow failure diseases The bone marrow is the factory that makes blood
What you need to know about MDS The Myelodysplastic Syndromes Stuart Goldberg MD The Myelodysplastic Syndromes are a group of bone marrow failure diseases The bone marrow is the factory that makes blood
Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Neoplasms. Policy Specific Section:
 Medical Policy Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Type: Medical Necessity and Investigational / Experimental Policy Specific Section:
Medical Policy Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Type: Medical Necessity and Investigational / Experimental Policy Specific Section:
HCT for Myelofibrosis
 Allogeneic HSCT for MDS and Myelofibrosis Sunil Abhyankar, MD Professor Medicine, Medical Director, Pheresis and Cell Processing University of Kansas Hospital BMT Program April 27 th, 213 HCT for Myelofibrosis
Allogeneic HSCT for MDS and Myelofibrosis Sunil Abhyankar, MD Professor Medicine, Medical Director, Pheresis and Cell Processing University of Kansas Hospital BMT Program April 27 th, 213 HCT for Myelofibrosis
CREDIT DESIGNATION STATEMENT
 CME Information LEARNING OBJECTIVES Recall the dose-limiting toxicity and preliminary clinical response results with 14- and 21-day extended treatment schedules of daily oral azacitidine. Apply new research
CME Information LEARNING OBJECTIVES Recall the dose-limiting toxicity and preliminary clinical response results with 14- and 21-day extended treatment schedules of daily oral azacitidine. Apply new research
The Changing Face of MDS: Advances in Treatment
 Thank you very much again for listening to me. We are going to be talking now in terms of therapy of MDS or The Changing Face of MDS Advances in Treatment. My name is Guillermo Garcia-Manero. I am a Professor
Thank you very much again for listening to me. We are going to be talking now in terms of therapy of MDS or The Changing Face of MDS Advances in Treatment. My name is Guillermo Garcia-Manero. I am a Professor
Selinexor is an oral, slowly-reversible, first-inclass Selective Inhibitor of Nuclear Export (SINE)
") Selinexor, a First-in-Class XPO1 Inhibitor, Is Efficacious and Tolerable in Patients with Myelodysplastic Syndromes (MDS) Refractory to Hypomethylating Agents Justin Taylor, MD, Morgan Coleman, MPH, Kelsey
Selinexor, a First-in-Class XPO1 Inhibitor, Is Efficacious and Tolerable in Patients with Myelodysplastic Syndromes (MDS) Refractory to Hypomethylating Agents Justin Taylor, MD, Morgan Coleman, MPH, Kelsey
Agenti ipometilanti e trapianto nelle sindromi mielodisplastiche e nelle leucemie mieloidi acute
 Agenti ipometilanti e trapianto nelle sindromi mielodisplastiche e nelle leucemie mieloidi acute Francesco Onida Università degli Studi di Milano Centro Trapianti di Midollo/Oncoematologia Fondazione IRCCS
Agenti ipometilanti e trapianto nelle sindromi mielodisplastiche e nelle leucemie mieloidi acute Francesco Onida Università degli Studi di Milano Centro Trapianti di Midollo/Oncoematologia Fondazione IRCCS
Dr Shankara Paneesha. ASH Highlights Department of Haematology & Stem cell Transplantation
 ASH Highlights 2015 Themes of ASH 2015 Novel therapies - Myeloma AML Lymphoma Pd-L1 & PD-l inhibitors Emerging concepts in biology HIF-1a pathway Cautionary tales ASH Choosing Wisely list IFM/DFCI
ASH Highlights 2015 Themes of ASH 2015 Novel therapies - Myeloma AML Lymphoma Pd-L1 & PD-l inhibitors Emerging concepts in biology HIF-1a pathway Cautionary tales ASH Choosing Wisely list IFM/DFCI
Myelodysplastic Syndrome
 Myelodysplastic Syndrome A Family-Oriented Approach on Diagnosis and Treatment Options Cecilia Arana Yi, MD Assistant Professor MDS Patient & Family/Caregiver Forum March 3, 2018 Quote of the Day There
Myelodysplastic Syndrome A Family-Oriented Approach on Diagnosis and Treatment Options Cecilia Arana Yi, MD Assistant Professor MDS Patient & Family/Caregiver Forum March 3, 2018 Quote of the Day There
A Phase II Study of the Combination of Oral Rigosertib and Azacitidine in Patients with Myelodysplastic Syndromes (MDS)
") A Phase II Study of the Combination of Oral Rigosertib and Azacitidine in Patients with Myelodysplastic Syndromes (MDS) Shyamala C. Navada, MD 1, Lewis R. Silverman, MD 1, Katherine Hearn, RN 2, Rosalie
A Phase II Study of the Combination of Oral Rigosertib and Azacitidine in Patients with Myelodysplastic Syndromes (MDS) Shyamala C. Navada, MD 1, Lewis R. Silverman, MD 1, Katherine Hearn, RN 2, Rosalie
Clinical Overview: MRD in CLL. Dr. Matthias Ritgen UKSH, Medizinische Klinik II, Campus Kiel
 Clinical Overview: MRD in CLL Dr. Matthias Ritgen UKSH, Medizinische Klinik II, Campus Kiel m.ritgen@med2.uni-kiel.de Remission in CLL Clinical criteria (NCI->WHO) Lymphadenopathy Splenomegaly Hepatomegaly
Clinical Overview: MRD in CLL Dr. Matthias Ritgen UKSH, Medizinische Klinik II, Campus Kiel m.ritgen@med2.uni-kiel.de Remission in CLL Clinical criteria (NCI->WHO) Lymphadenopathy Splenomegaly Hepatomegaly
Enhancing Survival Outcomes in the Management of Patients With Higher-Risk Myelodysplastic Syndromes
 The classification, diagnosis, treatment goals, clinical experience, guidelines, and therapeutic options for higher-risk MDS patients are reviewed. Anne Silber. Ha Long Bay, Vietnam (detail). Limited edition
The classification, diagnosis, treatment goals, clinical experience, guidelines, and therapeutic options for higher-risk MDS patients are reviewed. Anne Silber. Ha Long Bay, Vietnam (detail). Limited edition
The immunomodulatory agents lenalidomide and thalidomide for treatment of the myelodysplastic syndromes: A clinical practice guideline
 Critical Reviews in Oncology/Hematology 85 (2013) 162 192 The immunomodulatory agents lenalidomide and thalidomide for treatment of the myelodysplastic syndromes: A clinical practice guideline Heather
Critical Reviews in Oncology/Hematology 85 (2013) 162 192 The immunomodulatory agents lenalidomide and thalidomide for treatment of the myelodysplastic syndromes: A clinical practice guideline Heather
Treatment of Myelodysplastic Syndromes in Elderly Patients
 Adv Ther (2011) 28(Suppl.2):1-9. DOI 10.1007/s12325-011-0001-9 REVIEW Treatment of Myelodysplastic Syndromes in Elderly Patients Jesus Feliu Sanchez Received: December 14, 2010 / Published online: March
Adv Ther (2011) 28(Suppl.2):1-9. DOI 10.1007/s12325-011-0001-9 REVIEW Treatment of Myelodysplastic Syndromes in Elderly Patients Jesus Feliu Sanchez Received: December 14, 2010 / Published online: March
Myelodysplastic Syndromes: Update in Diagnosis and Therapy. Peter Valent
 Myelodysplastic Syndromes: Update in Diagnosis and Therapy Peter Valent MDS: Typical Features - Dysplasia in one or more Cell Lineages in the BM - Peripheral Cytopenia (unilineage, bi-, or pan-cp) - Quality
Myelodysplastic Syndromes: Update in Diagnosis and Therapy Peter Valent MDS: Typical Features - Dysplasia in one or more Cell Lineages in the BM - Peripheral Cytopenia (unilineage, bi-, or pan-cp) - Quality
New treatment strategies in myelodysplastic syndromes and acute myeloid leukemia van der Helm, Lidia Henrieke
 University of Groningen New treatment strategies in myelodysplastic syndromes and acute myeloid leukemia van der Helm, Lidia Henrieke IMPORTANT NOTE: You are advised to consult the publisher's version
University of Groningen New treatment strategies in myelodysplastic syndromes and acute myeloid leukemia van der Helm, Lidia Henrieke IMPORTANT NOTE: You are advised to consult the publisher's version
ADVANCES IN THE MANAGEMENT OF MYELODYSPLASTIC SYNDROMES
 ADVANCES IN THE MANAGEMENT OF MYELODYSPLASTIC SYNDROMES Corey Cutler, MD MPH FRCPC Associate Professor of Medicine, Harvard Medical School Dana-Farber Cancer Institute, Boston, MA HCT Outcomes - MDS 2001-2011
ADVANCES IN THE MANAGEMENT OF MYELODYSPLASTIC SYNDROMES Corey Cutler, MD MPH FRCPC Associate Professor of Medicine, Harvard Medical School Dana-Farber Cancer Institute, Boston, MA HCT Outcomes - MDS 2001-2011
Summary of Key AML Abstracts Presented at the European Hematology Association (EHA) June 22-25, 2017 Madrid, Spain
 June 22-25, 2017 Madrid, Spain") Summary of Key AML Abstracts Presented at the European Hematology Association (EHA) June 22-25, 2017 Madrid, Spain EHA 2017 ANNUAL MEETING: ABSTRACT SEARCH PAGE: https://learningcenter.ehaweb.org/eha/#!*listing=3*browseby=2*sortby=1*media=3*ce_id=1181*label=15531
Summary of Key AML Abstracts Presented at the European Hematology Association (EHA) June 22-25, 2017 Madrid, Spain EHA 2017 ANNUAL MEETING: ABSTRACT SEARCH PAGE: https://learningcenter.ehaweb.org/eha/#!*listing=3*browseby=2*sortby=1*media=3*ce_id=1181*label=15531
Department of Leukemia, The University of Texas M.D. Anderson Cancer Center, Houston, Texas; 2 Sunesis Pharmaceuticals, Inc, South San Francisco
 Phase I/II Study of Vosaroxin and Decitabine in Newly Diagnosed Older Patients with Acute Myeloid Leukemia (AML) and High Risk Myelodysplastic Syndrome (MDS) Naval Daver 1, Hagop Kantarjian 1, Guillermo
Phase I/II Study of Vosaroxin and Decitabine in Newly Diagnosed Older Patients with Acute Myeloid Leukemia (AML) and High Risk Myelodysplastic Syndrome (MDS) Naval Daver 1, Hagop Kantarjian 1, Guillermo
Blast transformation in chronic myelomonocytic leukemia: Risk factors, genetic features, survival, and treatment outcome
 RESEARCH ARTICLE Blast transformation in chronic myelomonocytic leukemia: Risk factors, genetic features, survival, and treatment outcome AJH Mrinal M. Patnaik, 1 Emnet A. Wassie, 1 Terra L. Lasho, 2 Curtis
RESEARCH ARTICLE Blast transformation in chronic myelomonocytic leukemia: Risk factors, genetic features, survival, and treatment outcome AJH Mrinal M. Patnaik, 1 Emnet A. Wassie, 1 Terra L. Lasho, 2 Curtis
Reduced-intensity Conditioning Transplantation
 Reduced-intensity Conditioning Transplantation Current Role and Future Prospect He Huang M.D., Ph.D. Bone Marrow Transplantation Center The First Affiliated Hospital Zhejiang University School of Medicine,
Reduced-intensity Conditioning Transplantation Current Role and Future Prospect He Huang M.D., Ph.D. Bone Marrow Transplantation Center The First Affiliated Hospital Zhejiang University School of Medicine,
Acute Myeloid Leukemia: State of the Art in 2018
 Acute Myeloid Leukemia: State of the Art in 2018 Harry P. Erba, MD, PhD Professor, Department of Medicine Director, Leukemia Program Duke University Durham, NC Treatment Paradigm of Adults with AML Fit
Acute Myeloid Leukemia: State of the Art in 2018 Harry P. Erba, MD, PhD Professor, Department of Medicine Director, Leukemia Program Duke University Durham, NC Treatment Paradigm of Adults with AML Fit
A paradigm shift in the therapy of low blast count acute myeloid leukemia. Valeria Santini UF Ematologia, Università di Firenze
 A paradigm shift in the therapy of low blast count acute myeloid leukemia Valeria Santini UF Ematologia, Università di Firenze Patients (%) AML is predominantly a disease of the elderly 40 69% of patients
A paradigm shift in the therapy of low blast count acute myeloid leukemia Valeria Santini UF Ematologia, Università di Firenze Patients (%) AML is predominantly a disease of the elderly 40 69% of patients
Myelodysplastic Syndrome: Let s build a definition
 1 MDS: Diagnosis and Treatment Update Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine Weill Medical College of Cornell University The New York Presbyterian Hospital Myelodysplastic
1 MDS: Diagnosis and Treatment Update Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine Weill Medical College of Cornell University The New York Presbyterian Hospital Myelodysplastic
Myelodysplastic Syndromes:
 Incidence Rate per 100,000 7/21/2015 Myelodysplastic Syndromes: Current Thinking on the Disease, Diagnosis and Treatment Rafael Bejar MD, PhD Aplastic Anemia & MDS International Foundation Regional Patient
Incidence Rate per 100,000 7/21/2015 Myelodysplastic Syndromes: Current Thinking on the Disease, Diagnosis and Treatment Rafael Bejar MD, PhD Aplastic Anemia & MDS International Foundation Regional Patient
ASBMT MDS/MPN UPDATE
 ASBMT MDS/MPN UPDATE Sunil Abhyankar, MD Professor of Medicine Medical Director, Pheresis and Cell Processing Division of Hematologic Malignancies and Cellular Therapeutics Department of Internal Medicine
ASBMT MDS/MPN UPDATE Sunil Abhyankar, MD Professor of Medicine Medical Director, Pheresis and Cell Processing Division of Hematologic Malignancies and Cellular Therapeutics Department of Internal Medicine
Molecular Genetic Testing to Predict Response to Therapy in MDS
 Molecular Genetic Testing to Predict Response to Therapy in MDS Rafael Bejar MD, PhD Bone Marrow Failure Disease Scientific Symposium Rockville, MD March 18 th, 2016 Overview Response Criteria Lenalidomide
Molecular Genetic Testing to Predict Response to Therapy in MDS Rafael Bejar MD, PhD Bone Marrow Failure Disease Scientific Symposium Rockville, MD March 18 th, 2016 Overview Response Criteria Lenalidomide
New and Emerging Strategies in the Treatment of Patients with Higher risk Myelodysplastic Syndromes (MDS)
") Welcome to Managing Myelodysplastic Syndromes. My name is David Steensma. I am an Associate Professor of Medicine at Harvard Medical School and a faculty member in the Adult Leukemia Program at Dana Farber
Welcome to Managing Myelodysplastic Syndromes. My name is David Steensma. I am an Associate Professor of Medicine at Harvard Medical School and a faculty member in the Adult Leukemia Program at Dana Farber
Etiology. Definition MYELODYSPLASTIC SYNDROMES. De novo. Secondary MDS (10 years earlier than primary) transformation
 transformation") MYELODYSPLASTIC SYNDROMES Rashmi Kanagal-Shamanna, MD Assistant Professor Hematopathology & Molecular Diagnostics The University of Texas M.D. Anderson Cancer Center Houston, Texas No relevant COIs to
MYELODYSPLASTIC SYNDROMES Rashmi Kanagal-Shamanna, MD Assistant Professor Hematopathology & Molecular Diagnostics The University of Texas M.D. Anderson Cancer Center Houston, Texas No relevant COIs to
The function of the bone marrow. Living with Aplastic Anemia. A Case Study - I. Hypocellular bone marrow failure 5/14/2018
 The function of the bone marrow Larry D. Cripe, MD Indiana University Simon Cancer Center Bone Marrow Stem Cells Mature into Blood Cells Mature Blood Cells and Health Type Function Term Red Cells Carry
The function of the bone marrow Larry D. Cripe, MD Indiana University Simon Cancer Center Bone Marrow Stem Cells Mature into Blood Cells Mature Blood Cells and Health Type Function Term Red Cells Carry
SWOG ONCOLOGY RESEARCH PROFESSIONAL (ORP) MANUAL LEUKEMIA FORMS CHAPTER 16A REVISED: DECEMBER 2017
 MANUAL LEUKEMIA FORMS CHAPTER 16A REVISED: DECEMBER 2017") LEUKEMIA FORMS The guidelines and figures below are specific to Leukemia studies. The information in this manual does NOT represent a complete set of required forms for any leukemia study. Please refer
LEUKEMIA FORMS The guidelines and figures below are specific to Leukemia studies. The information in this manual does NOT represent a complete set of required forms for any leukemia study. Please refer
MDS 101. What is bone marrow? Myelodysplastic Syndrome: Let s build a definition. Dysplastic? Syndrome? 5/22/2014. What does bone marrow do?
 101 May 17, 2014 Myelodysplastic Syndrome: Let s build a definition Myelo bone marrow Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine What is bone marrow? What does bone
101 May 17, 2014 Myelodysplastic Syndrome: Let s build a definition Myelo bone marrow Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine What is bone marrow? What does bone
Department of Leukemia, The University of Texas M.D. Anderson Cancer Center, Houston, Texas; 2 Sunesis Pharmaceuticals, Inc, South San Francisco
 Phase I/II Study of Vosaroxin and Decitabine in Newly Diagnosed Older Patients with Acute Myeloid Leukemia (AML) and High Risk Myelodysplastic Syndrome (MDS) Naval Daver 1, Hagop Kantarjian 1, Guillermo
Phase I/II Study of Vosaroxin and Decitabine in Newly Diagnosed Older Patients with Acute Myeloid Leukemia (AML) and High Risk Myelodysplastic Syndrome (MDS) Naval Daver 1, Hagop Kantarjian 1, Guillermo
Current guidelines for management of INT- 2/high risk MDS
 ELASTIC Current guidelines for management of INT- 2/high risk MDS If fit (i.e. HCT-CI and performance status< 3), consider for early allo BMT with/without prior AML induction therapy If unfit consider
ELASTIC Current guidelines for management of INT- 2/high risk MDS If fit (i.e. HCT-CI and performance status< 3), consider for early allo BMT with/without prior AML induction therapy If unfit consider
Acute Myeloid Leukemia Progress at last
 Acute Myeloid Leukemia Progress at last Bruno C. Medeiros, MD September 9, 217 Introduction Mechanisms of leukemogenesis Emerging therapies in AML Previously untreated AML Relapsed and refractory patients
Acute Myeloid Leukemia Progress at last Bruno C. Medeiros, MD September 9, 217 Introduction Mechanisms of leukemogenesis Emerging therapies in AML Previously untreated AML Relapsed and refractory patients
Better Prognosis for Patients With Del(7q) Than for Patients With Monosomy 7 in Myelodysplastic Syndrome
 Than for Patients With Monosomy 7 in Myelodysplastic Syndrome") Better Prognosis for Patients With Del(7q) Than for Patients With Monosomy 7 in Myelodysplastic Syndrome Iris Cordoba, MD 1 ; José R. González-Porras, MD 1 ; Benet Nomdedeu, MD 2 ; Elisa Luño, MD 3 ; Raquel
Better Prognosis for Patients With Del(7q) Than for Patients With Monosomy 7 in Myelodysplastic Syndrome Iris Cordoba, MD 1 ; José R. González-Porras, MD 1 ; Benet Nomdedeu, MD 2 ; Elisa Luño, MD 3 ; Raquel
APPROACH TO MYELODYSPLASTIC SYNDROMES IN THE ERA OF PRECISION MEDICINE
 APPROACH TO MYELODYSPLASTIC SYNDROMES IN THE ERA OF PRECISION MEDICINE Rashmi Kanagal-Shamanna, MD Assistant Professor Hematopathology & Molecular Diagnostics Department of Hematopathology The University
APPROACH TO MYELODYSPLASTIC SYNDROMES IN THE ERA OF PRECISION MEDICINE Rashmi Kanagal-Shamanna, MD Assistant Professor Hematopathology & Molecular Diagnostics Department of Hematopathology The University
A prospective, multicenter European Registry for newly diagnosed patients with Myelodysplastic Syndromes of IPSS low and intermediate-1 subtypes.
 Protocol Synopsis Study Title A prospective, multicenter European Registry for newly diagnosed patients with Myelodysplastic Syndromes of IPSS low and intermediate-1 subtypes. Short Title European MDS
Protocol Synopsis Study Title A prospective, multicenter European Registry for newly diagnosed patients with Myelodysplastic Syndromes of IPSS low and intermediate-1 subtypes. Short Title European MDS
Disrupting the Cell Cycle to Treat AML and MDS Rodman & Renshaw Conference
 CYC 682 Disrupting the Cell Cycle to Treat AML and MDS Rodman & Renshaw Conference September 2014 Disclaimer This presentation contains forward-looking statements within the meaning of the safe harbor
CYC 682 Disrupting the Cell Cycle to Treat AML and MDS Rodman & Renshaw Conference September 2014 Disclaimer This presentation contains forward-looking statements within the meaning of the safe harbor
2013 AAIM Pathology Workshop
 2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone
2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone
3/31/2014. New Directions in Aplastic Anemia Treatment: What s on the Horizon? Objectives
 New Directions in Aplastic Anemia Treatment: What s on the Horizon? AA & MDS International Foundation Living with, MDS, or PNH Patient and Family Conferences in 2014 April 5, 2014 Objectives To provide
New Directions in Aplastic Anemia Treatment: What s on the Horizon? AA & MDS International Foundation Living with, MDS, or PNH Patient and Family Conferences in 2014 April 5, 2014 Objectives To provide
LAM 20-30% Cristina Papayannidis, MD, PhD DIMES, Istituto di Ematologia L. e A. Seràgnoli Università di Bologna
 LAM 20-30% Cristina Papayannidis, MD, PhD DIMES, Istituto di Ematologia L. e A. Seràgnoli Università di Bologna FAB CLASSIFICATION OF MYELODYSPLASTIC SYNDROME Subtype % Blood Myeloblasts Bone Marrow Myeloblasts
LAM 20-30% Cristina Papayannidis, MD, PhD DIMES, Istituto di Ematologia L. e A. Seràgnoli Università di Bologna FAB CLASSIFICATION OF MYELODYSPLASTIC SYNDROME Subtype % Blood Myeloblasts Bone Marrow Myeloblasts
Kevin Kelly, MD, Phd Acute Myeloid and Lymphoid Leukemias
 Kevin Kelly, MD, Phd Acute Myeloid and Lymphoid Leukemias Relevant financial relationships in the past twelve months by presenter or spouse/partner. Speakers bureau: Novartis, Janssen, Gilead, Bayer The
Kevin Kelly, MD, Phd Acute Myeloid and Lymphoid Leukemias Relevant financial relationships in the past twelve months by presenter or spouse/partner. Speakers bureau: Novartis, Janssen, Gilead, Bayer The
MDS - Diagnosis and Treatments. Dr Helen Enright, Adelaide and Meath Hospital Dr Catherine Flynn, St James Hospital
 MDS - Diagnosis and Treatments Dr Helen Enright, Adelaide and Meath Hospital Dr Catherine Flynn, St James Hospital Overview What is myelodysplasia? Symptoms Diagnosis and prognosis Myelodysplasia therapy
MDS - Diagnosis and Treatments Dr Helen Enright, Adelaide and Meath Hospital Dr Catherine Flynn, St James Hospital Overview What is myelodysplasia? Symptoms Diagnosis and prognosis Myelodysplasia therapy
Anemia (2): 4 MS/18/02/2019
: 4 MS/18/02/2019") Anemia (2): 4 MS/18/02/2019 Case 2 65 yr old male had gradual onset of odd behavior with psychotic symptoms, irritability and parasthesia in hands and feet He was noticed to have imbalanced gait. Examination
Anemia (2): 4 MS/18/02/2019 Case 2 65 yr old male had gradual onset of odd behavior with psychotic symptoms, irritability and parasthesia in hands and feet He was noticed to have imbalanced gait. Examination
MANAGEMENT OF ADULT PATIENTS WITH MYELODYSPLASTIC SYNDROMES
 MANAGEMENT OF ADULT PATIENTS WITH MYELODYSPLASTIC SYNDROMES *Nicolas Bonadies Department of Haematology and Central Haematology Laboratory, Inselspital Bern, University Hospital, University of Bern, Bern,
MANAGEMENT OF ADULT PATIENTS WITH MYELODYSPLASTIC SYNDROMES *Nicolas Bonadies Department of Haematology and Central Haematology Laboratory, Inselspital Bern, University Hospital, University of Bern, Bern,
Myelodysplastic syndromes
 Haematology 601 Myelodysplastic syndromes The myelodysplastic syndromes are a group of disorders predominantly affecting elderly people, leading to ineffective haematopoiesis, and they have the potential
Haematology 601 Myelodysplastic syndromes The myelodysplastic syndromes are a group of disorders predominantly affecting elderly people, leading to ineffective haematopoiesis, and they have the potential
Maintaining Long-Term Efficacy in the Elderly MDS Patient with Poor Performance Status
 Hi, my name is Dr. Hetty Carraway. I am a staff physician at the Taussig Cancer Institute at the Cleveland Clinic. Welcome to Managing MDS. 1 As you all are aware, many of our patients with MDS are in
Hi, my name is Dr. Hetty Carraway. I am a staff physician at the Taussig Cancer Institute at the Cleveland Clinic. Welcome to Managing MDS. 1 As you all are aware, many of our patients with MDS are in
Myelodysplastic Syndromes
 NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Myelodysplastic Syndromes Version 2.2017 November 10, 2016 NCCN.org NCCN Guidelines for Patients available at www.nccn.org/patients Continue
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Myelodysplastic Syndromes Version 2.2017 November 10, 2016 NCCN.org NCCN Guidelines for Patients available at www.nccn.org/patients Continue
[ NASDAQ: MEIP ] Analyst & Investor Event December 8, 2014
![[ NASDAQ: MEIP ] Analyst & Investor Event December 8, 2014](/thumbs/73/68853651.jpg "[ NASDAQ: MEIP ] Analyst & Investor Event December 8, 2014") [ NASDAQ: MEIP ] Analyst & Investor Event December 8, 2014 Forward-Looking Statements These slides and the accompanying oral presentation contain forward-looking statements. Actual events or results may
[ NASDAQ: MEIP ] Analyst & Investor Event December 8, 2014 Forward-Looking Statements These slides and the accompanying oral presentation contain forward-looking statements. Actual events or results may
Use of TPO mimetics for Indications Other Than ITP
 Use of TPO mimetics for Indications Other Than ITP Mazyar Shadman, MD, MPH Discussant: Siobán Keel, MD Hematology Fellows Conference June 28, 2013 Thrombopoietin (TPO) and other c mpl ligands TPO mimetics
Use of TPO mimetics for Indications Other Than ITP Mazyar Shadman, MD, MPH Discussant: Siobán Keel, MD Hematology Fellows Conference June 28, 2013 Thrombopoietin (TPO) and other c mpl ligands TPO mimetics