Annals of Oncology Advance Access published August 12, 2014
|
|
|
- Henry Pearson
- 5 years ago
- Views:
Transcription
1 Annals of Oncology Advance Access published August 12, Extended RAS mutations and anti-egfr monoclonal antibody survival benefit in metastatic colorectal cancer: a meta-analysis of randomized controlled trials M. J. Sorich 1, M. D. Wiese 2, A. Rowland 1, G. Kichenadasse 3, R. A. McKinnon 3, C. S. Karapetis 3 1 Department of Clinical Pharmacology, School of Medicine, Flinders University, Adelaide, Australia 2 School of Pharmacy and Medical Sciences, University of South Australia, Adelaide, Australia 3 Flinders Centre for Innovation in Cancer, School of Medicine, Flinders University, Adelaide, Australia; Corresponding author: A/Prof Michael J Sorich, Department of Clinical Pharmacology, School of Medicine, Flinders University, Bedford Park SA, 5042, Australia, Tel: , michael.sorich@flinders.edu.au The Author Published by Oxford University Press on behalf of the European Society for Medical Oncology. All rights reserved. For permissions, please journals.permissions@oup.com.
2 2 Abstract Background: Monoclonal antibodies (mabs) targeting the epidermal growth factor receptor (EGFR) prolong survival in metastatic colorectal cancer KRAS exon 2 wild-type tumors. Recent evidence has suggested that other RAS mutations (in exons 3 and 4 of KRAS and exons 2, 3 and 4 of a related gene, NRAS) may also be predictive of resistance. Methods: Systematic review and meta-analysis of randomized controlled trials (RCTs) evaluating anti-egfr mabs that have assessed tumors for new RAS mutations. Tumors with the new RAS mutations were compared to both tumors without any RAS mutations and tumors with KRAS exon 2 mutations with respect to anti-egfr treatment progression-free survival (PFS) and overall survival (OS) benefit. Results: Nine RCTs comprising a total of 5948 participants evaluated for both KRAS exon 2 and new RAS mutations met the inclusion criteria. Approximately 20% of KRAS exon 2 wildtype tumors harbored one of the new RAS mutations. Tumors without any RAS mutations (either KRAS exon 2 or new RAS mutations) were found to have significantly superior anti- EGFR mab PFS (P<0.001) and OS (P=0.008) treatment effect compared to tumors with any of the new RAS mutations. No difference in PFS or OS benefit was evident between tumors with KRAS exon 2 mutations and tumors with the new RAS mutations. Results were consistent between different anti-egfr agents, lines of therapy and chemotherapy partners. Anti-EGFR mab therapy significantly improved both PFS (hazard ratio 0.62 [95% CI; 0.50 to 0.76]) and OS (hazard ratio 0.87 [95% CI; 0.77 to 0.99]) for tumors without any RAS mutations. No PFS or OS benefit was evident with use of anti-egfr mabs for tumors harboring any RAS mutation (P>0.05). Conclusion: Tumors harboring one of the new RAS mutations are unlikely to significantly benefit from anti-egfr mab therapy in metastatic colorectal cancer. Keywords: RAS mutation, pharmacogenomics, cetuximab, panitumumab, predictive biomarker, meta-analysis
3 3 Key Message Not all KRAS exon 2 wild-type tumors are likely to benefit from anti-egfr mabs in metastatic colorectal cancer. Tumors that harbor one of the new RAS mutations (i.e. KRAS exon 3 and 4 and NRAS exon 2, 3 and 4) have significantly inferior survival benefit from anti- EGFR mab therapy compared to tumors without any RAS mutations. Prior to treatment with anti-egfr mabs, tumors should be screened for mutations in exon 2, 3 and 4 of both KRAS and NRAS genes.
4 4 Introduction Cetuximab and panitumumab are monoclonal antibodies (mabs) that target the extracellular domain of the epidermal growth factor receptor (EGFR) and are important treatment options in patients with metastatic colorectal cancer (mcrc). RAS proteins are important downstream effectors within the mitogen-activated protein kinase (MAPK) pathway that couples EGFR with intracellular signaling cascades. The RAS gene is often mutated in mcrc, and the most common of these is Kirsten rat sarcoma viral oncogene (KRAS). Somatic single nucleotide point mutations in codons 12 and 13 of exon 2 of the KRAS gene lead to constitutive activation of the MAPK pathway, and it is well established from randomized controlled trials (RCTs) that these mutations are predictive of treatment resistance to anti-egfr mabs in mcrc. For this reason, only patients with KRAS exon 2 wild-type tumors were initially approved for treatment with this class of agents [1], which minimizes unnecessary patient toxicity and improves cost-effectiveness of treatment [2]. Recent studies, in particular the retrospective analysis of the PRIME trial [3], suggest that other mutations in genes of the RAS family (NRAS mutations and KRAS mutations outside exon 2) are also associated with reduced response to anti-egfr mabs. This study aims to quantitatively synthesize the evidence from RCTs that evaluate whether extended RAS mutations are negative predictive biomarkers for anti-egfr mab therapy in mcrc. Specifically, the primary aim was to evaluate whether the efficacy of anti-egfr mab treatment for tumors with one of the new RAS mutations is most similar to that of tumors with KRAS exon 2 mutations (not eligible for anti-egfr mab treatment) or tumors with no RAS mutations (good responders to anti-egfr mab treatment). The secondary aim was to quantify the survival benefit of anti-egfr mab therapy in patients with tumors that do not harbor any RAS mutations.
5 5 Method Inclusion criteria Inclusion criteria for the systematic review included: a randomized phase II or III study design involving the comparison of an anti-egfr mab (either as monotherapy or in combination with chemotherapy) to an alternative therapy in mcrc; study participants genotyped for at least one of the following in addition to KRAS exon 2: KRAS mutations in exon 3 (codon 59, 61) or exon 4 (codons 117, 146), or NRAS mutations in exon 2, 3 or 4; and follow up for progression free survival (PFS) and/or overall survival (OS). Search strategy and data extraction Embase, Medline and Web of Science (up to 1 April 2014) were searched for the following terms: (colon cancer or colorectal cancer or metastatic colorectal cancer) and (K-RAS or KRAS or mutant KRAS or mutant RAS) and (panitumumab or cetuximab or anti-egfr) and (N-RAS or NRAS or exon 3 or exon 4 or codon 59 or codon 61 or codon 117 or codon 146). No restrictions were placed on the search, and relevant MeSH (Medline) or Emtree (Embase) terms were utilized where possible. Additionally, abstracts from the 2014 ASCO meetings were hand searched to scan for updated data and to identify any new studies. Initially, duplicate titles were removed and then the title of the articles was scanned to determine if the article was irrelevant. The abstract of all remaining articles were then retrieved and reviewed, and irrelevant articles were discarded. Of the remaining articles, fulltext manuscripts and/or conference posters/presentations were obtained, and those that fulfilled the inclusion criteria were documented. After identification of relevant articles, reference lists of the articles that were identified as relevant were hand-searched to identify any additional articles that were missed with the search strategy. Studies reported in conference abstracts and published in languages other than English were included if sufficient information was available in the (English) abstract and the associated posters or presentations. Data was extracted using a data template. If multiple versions of the data were presented, the largest and most recently updated data was preferentially used in the
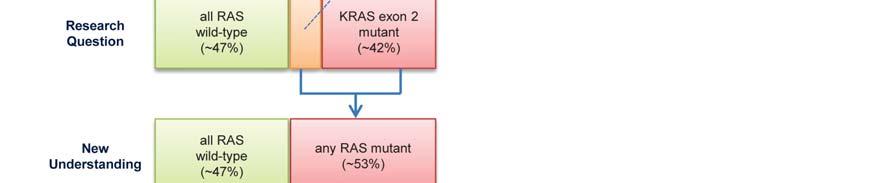
6 6 meta-analysis, and data was cross-checked against other publications were possible. The search strategy and data extraction were undertaken independently by two investigators with any discrepancies resolved by another investigator. RAS subgroups compared Three mutually exclusive RAS subgroups were primarily evaluated (Figure 1). The KRAS exon 2 mutant subgroup represents tumors with a KRAS exon 2 mutation which have previously been shown not to benefit from anti-egfr mabs [4, 5]. In contrast, individuals that are wild-type for KRAS exon 2 have been thought of as likely to benefit from anti-egfr therapy [4, 5]. For the purpose of this study, these individuals with wild-type KRAS exon 2 were divided into two subgroups; the new RAS mutant subgroup (wild-type for KRAS exon 2, but with a KRAS mutation in exons 3 or 4 and/or a NRAS mutation in exons 2, 3 or 4) representing an additional group of patients that potentially do not benefit, and the all RAS wild-type subgroup (no mutations in exons 2, 3 and 4 for either KRAS or NRAS), representing patients that are expected to respond best to anti-egfr therapy. Should the new RAS mutant subgroup be found to have an anti-egfr mab treatment effect that is more similar to the KRAS exon 2 mutant subgroup than the all RAS wild-type subgroup, the new RAS mutant and KRAS exon 2 mutant subgroups would to be merged into an any RAS mutant group for further evaluation. Statistical Analysis Since some anti-egfr mab RCTs have significant cross-over following progression, the pre-specified primary outcome was PFS, and the secondary outcome was OS. The hazard ratio was used to represent the comparative treatment effect on survival outcomes for anti- EGFR mab therapy compared to either no anti-egfr mab therapy or alternative therapy. Studies generally reported hazard ratios derived using Cox proportional-hazards models stratified according to randomization factors (e.g. ECOG performance status). If the hazard
7 7 ratio for a RAS subgroup was not reported, the value was estimated where possible by combining smaller subgroups with a fixed-effect meta-analysis. Evaluation of the primary aim was undertaken based on the comparison of the anti-egfr mab treatment effect (i.e. hazard ratio for survival outcomes) between pairs of RAS subgroups (i.e. all RAS wild-type vs new RAS mutant and KRAS exon 2 mutant vs new RAS mutant ). The interaction hazard ratio (relative size of the treatment effect between subgroups) was calculated by dividing the hazard ratio for the all RAS wild-type or KRAS exon 2 mutant subgroup by the hazard ratio for the new RAS mutant subgroup. A value less than one indicates that the new RAS mutant subgroup has an inferior treatment effect to the other RAS subgroup (and vice-versa). The log of the interaction hazard ratios estimated for each study were pooled using a random-effects model and the inverse variance method. For aim 2, subgroup-specific summary estimates of the treatment effect hazard ratios were pooled using a random-effects model based on the inverse variance method. The treatment effect of the all RAS wild-type and new RAS mutant subgroups were evaluated along with the any RAS mutant group the merged KRAS exon 2 mutant and new RAS mutant subgroups (Figure 1). Analysis was limited to RCTs that assessed the addition of anti-egfr mabs to background therapy (i.e. cytotoxic or best-supportive care) as this was the largest group of studies with sufficiently similar treatment comparison. Hazard ratios for the KRAS exon 2 wild-type subgroup was estimated for reference. Objective response rate was based on the Response Evaluation Criteria in Solid Tumors (RECIST), and response was defined as either a complete or partial response. The effect of treatment on response was measured as an odds ratio (i.e. odds of response with anti- EGFR mab therapy vs odds of response without anti-egfr mab therapy).
8 8 Heterogeneity between studies was assessed using the Cochrane s Q statistic and I 2 statistic. Small-study effects (and risk of publication bias) were assessed by visual inspection of funnel plots and Egger s linear regression test. Pre-specified analyses were undertaken by grouping trials according to the anti-egfr mab evaluated (cetuximab or panitumumab), the line of therapy and the background chemotherapy regimen (oxaliplatin-based vs irinotecan based). A sensitivity analysis was undertaken that excluded studies with fluropyrimidine backbone therapy other than infusional 5FU, on the basis of a potential interaction between fluropyrimidine backbone and anti-egfr mab efficacy [6]. All reported P-values are two-sided. Analyses were carried out R (The R Foundation for Statistical Computing, Vienna, Austria). Results Overview of studies included Nine RCTs comprising a total of 5948 participants evaluated for both established and new RAS mutations met the inclusion criteria (Table 1, Figure S1) [3, 7-18]. Seven studies evaluated the addition of an anti-egfr mab to background therapy (FOLFOX, FOLFIRI, irinotecan, oxaliplatin and fluoropyrimidine chemotherapy, or best supportive care), and two studies compared the addition of anti-egfr mab or bevacizumab to cytotoxic therapy (FOLFOX or FOLFIRI). Five RCTs studied panitumumab and three studied cetuximab. All studies other than the COIN study reported data sufficient to estimate PFS and OS treatment effects for the three RAS subgroups. The COIN study only reported sufficient data for the OS treatment hazard ratio for the all RAS wild-type subgroup. Details of ascertainment, specific mutations evaluated, and proportions of study participants evaluated to be KRAS exon 2 wild-type and RAS wild-type are summarized in Table 1. The risk of bias of the trial intention-to-treat (ITT) populations was generally similar between studies with respect to inclusion criteria, randomization, allocation concealment, blinding, outcome reporting and loss to follow-up [4, 5]. KRAS exon 2 mutation status was evaluable in 79% to
9 9 100% of the ITT populations, and new RAS mutations were evaluable in 65% to 100% of KRAS exon 2 wild-type tumor populations. Other than the COIN study (which genotyped only KRAS codon 61, and NRAS codons 12 and 61), all studies genotyped the majority of the new RAS codons (Table 1, Figure 2). The methods used to detect KRAS and NRAS mutations varied between studies, and included bidirectional Sanger sequencing, pyrosequencing, MALDI-ToF analysis and WAVE-based SURVEYOR analysis (Table S1). Based on random-effects meta-analysis of 5 studies that had genotyped for new RAS mutations in all 10 codons (N=1911) it was estimated that 19.9% (95% CI; 16.7% to 23.4%) of KRAS exon 2 wild-type tumors harbored at least one of the new RAS mutations. Significant heterogeneity between study estimates of the prevalence was identified (P=0.016, I 2 =67%). The estimated prevalence of new RAS mutations in each exon is summarized in Figure 2. Comparison of anti-egfr mab treatment effect size between RAS subgroups Eight studies reported sufficient data to evaluate whether anti-egfr mab efficacy differed between the three RAS subgroups. Anti-EGFR mab efficacy was found to be significantly superior for tumors in the all RAS wild-type subgroup compared to tumors in the new RAS mutant subgroup with respect to both PFS (interaction test P<0.001, Figure 3a) and OS (interaction test P =0.008, Figure 3a). However, no significant difference in anti-egfr mab treatment effect with respect to either PFS (interaction test P =0.88) or OS (interaction test P =0.35) was apparent between tumors in the new RAS mutant and KRAS exon 2 mutant subgroups (Figure 3b). No or minimal heterogeneity was evident between studies for the test of interaction between RAS subgroups, and there was no indication that the differences in treatment effect between RAS subgroups differed significantly on the basis of the anti-egfr mab studied, line of therapy, or chemotherapy partner (Table S2). Visual inspection and regression tests did not indicate significant funnel plot asymmetry or small study bias.
10 10 Analysis based on response rates indicated similar findings to those for the survival outcomes. Specifically, the size of the anti-egfr mab treatment effect on response rates was significantly greater for all RAS wild-type tumors than for new RAS mutant tumors (interaction test P=0.001) Additionally, no significant difference in treatment effect, as measured by response rates, was apparent between KRAS exon 2 mutant tumors and the new RAS mutant tumors (interaction test P=0.32). Anti-EGFR mab treatment effect size for the all RAS wild-type subgroup A significant PFS benefit of anti-egfr mab therapy was evident for tumors without any RAS mutations (hazard ratio 0.62 [95% CI; 0.50 to 0.76], Figure 4a). By way of comparison, based on the same set of studies, the PFS hazard ratio for tumors without any KRAS exon 2 mutations (i.e. before exclusion of tumors with the new RAS mutations) was estimated to be 0.68 [0.58 to 0.80]. Similarly, tumors without any RAS mutations gained significant OS benefit with anti-egfr mab therapy (hazard ratio 0.87 [0.77 to 0.99], Figure 4b). In comparison, tumors without any KRAS exon 2 mutations were estimated to have a hazard ratio of 0.90 [0.83 to 0.98]. A sensitivity analysis excluding studies with fluropyrimidine backbone therapy other than infusional 5FU, resulted in For the PFS outcome, significant heterogeneity in anti-egfr treatment effect estimates was apparent between studies (I 2 =67%, P =0.009). No significant small study effects were apparent for either PFS or OS outcomes. No significant differences in the anti-egfr mab PFS and OS treatment effect for RAS wild-type tumors were evident between cetuximab and panitumumab, or between irinotecan-based and oxaliplatin-based background chemotherapy (Table S3). Anti-EGFR mab third-line monotherapy (based on a single study [10, 19]) was estimated to have significantly greater benefit than first/second line anti-egfr mab therapy in combination with chemotherapy with respect to PFS (P=0.002), but not OS (P=0.66). Specifically, the PFS hazard ratio was 0.36 [0.25 to 0.52] for all RAS wild-type
11 11 tumors (compared to PFS hazard ratio of 0.45 [0.34 to 0.59] for KRAS exon 2 wild-type tumors) [10, 19]. A significant increase in response rate (odds ratio of 3.71 [2.16 to 6.36]) was observed via addition of anti-egfr mab therapy for all RAS wild-type tumors (Figure S2). Anti-EGFR mab treatment effect size for mutant RAS tumors Based on 6 studies, no improvement in PFS (hazard ratio 0.99 [0.77 to 1.27) or OS (hazard ratio 1.16 [0.91 to 1.47]) from anti-egfr mab therapy was apparent for tumors with the new RAS mutations. For tumors with any RAS mutation (KRAS exon 2 mutation or new RAS mutation) there was also no improvement in PFS (hazard ratio 1.12 [0.94 to 1.34) or OS (hazard ratio 1.08 [0.97 to 1.21]) with anti-egfr mab therapy (Figure 5). For tumors with any RAS mutation, significant heterogeneity in anti-egfr treatment effect was apparent between studies with respect to PFS (I 2 =63%, P =0.02), but not OS (I 2 =19%, P =0.29). Discussion The current meta-analysis establishes that individuals with tumors that are KRAS exon 2 wild-type (which includes both the all RAS wild-type and new RAS mutant subgroups) should not be considered to be a single homogenous group with respect to anti-egfr mab efficacy. The all RAS wild-type subgroup had a significantly superior anti-egfr mab efficacy compared to the new RAS mutant subgroup, whereas the anti-egfr mab efficacy of the KRAS exon 2 mutant and new RAS mutant subgroups where not distinguishable. This indicates that tumors with one of the new RAS mutations are more appropriately grouped with the tumors with a KRAS exon 2 mutation (forming the any RAS mutant group), rather than with tumors that do not have any RAS mutations. A significant PFS and OS benefit was observed with addition of anti-egfr mab therapy for tumors without any RAS mutations, whereas no PFS or OS benefit was observed for tumors that harbored any RAS mutation. Hence, approximately 53% of mcrc tumors (~42% with
12 12 KRAS exon 2 mutations and ~11% with KRAS exon 3 or 4 or NRAS exons 2, 3, or 4 mutations) are likely resistant to anti-egfr mabs. Some studies, most notably the PRIME trial [3] have indicated that anti-egfr mab treatment for tumors with RAS mutations may lead to a detrimental effect on PFS and OS. Although the detrimental effect of anti-egfr mab therapy for RAS mutant tumors was not statistically significant in the current analysis, significant heterogeneity between studies was apparent. It is currently uncertain why some, but not all studies report a detrimental effect of anti-egfr mabs when used for RAS mutant tumors. To the authors knowledge, this is the first meta-analysis to systematically and quantitatively summarize the evidence from RCTs with respect to the predictive value of the new RAS mutations. The meta-analysis includes panitumumab and cetuximab, different lines of therapy and a range of background chemotherapy. There was little evidence to suggest that the effects of RAS mutations differ between mabs, line of therapy, or background chemotherapy, although the power to detect important heterogeneity was relatively limited due to the relatively small number of studies included in the analysis. There was significant heterogeneity in the frequency of new RAS mutations between studies, which could be explained, at least in part, by the different methods used to detect RAS mutations. We acknowledge that the trial results included in this meta-analysis were extracted from published data rather than being based on an individual patient data meta-analysis. An additional potential limitation of the study is that some of the studies included in the analysis have only been reported in conference presentations rather than full published manuscripts. Although it is possible that the results may differ modestly between the conference presentations and future full publication due to updated data, such differences are likely to be relatively modest. Due to the clear differences observed in this study, modest updating prior to publication is unlikely to substantively alter the results reported here. In addition, for
13 13 most studies results were confirmed through second sources such as the European Medicines Agency assessment documents [8, 9]. Although results of nine RCTs are included in this analysis, there are a small number of additional trials (NCIC CTG CO.17 [20], CALGB/SWOG [21], NORDIC VII [22], EPIC [23]) that could potentially be retrospectively analyzed for the additional RAS mutations in the future. New information from these trials could potentially alter the results of the current analysis. A potential direction of future research is the evaluation of individual RAS mutations to understand whether the magnitude of effect on anti-egfr mab efficacy varies from mutation to mutation, including if some RAS mutations but not others are associated with worse PFS and OS when treated with anti-egfr mab therapy. Data was not reported in a manner to enable such an analysis to be performed in this study and a collaborative meta-analysis based on patient-level data will likely be required. As the prevalence of individual mutations is low, the power to detect differences between individual mutations may be limiting. An additional direction for future research is the further evaluation of mutations and expression of genes within the MAPK pathway but outside the RAS family such as PTEN, PIK3CA and EREG [24-26]. Moreover, in order to confirm that RAS subgroup estimates of treatment effect are unbiased, future patient-level analyses of the trial data should aim to further evaluate the balance of prognostic factors within RAS subgroups and the impact of excluding trial participants with insufficient tumor sample for RAS mutation status ascertainment. In conclusion, meta-analysis analysis of nine RCTs indicates that not all KRAS exon 2 wildtype tumors benefit from anti-egfr mab treatment in mcrc. Individuals who are KRAS exon 2 wild-type, but have one of the new RAS mutations, have distinctly inferior anti-egfr mab treatment benefit compared to individuals without any RAS mutations. Rather, individuals with one of the new RAS mutations appear to be much more similar to individuals with a KRAS exon 2 mutation in that both groups have little evidence of a significant survival benefit from anti-egfr mabs. These results suggest that extended RAS mutation testing
14 14 (KRAS exon 3 and 4 and NRAS exon 2, 3 and 4, in addition to KRAS exon 2 currently undertaken) should be undertaken prior to the administration of an anti-egfr mab. The weight of current evidence indicates that both cetuximab and panitumumab should only be prescribed for patients with mcrc that are wild-type for all known RAS activating mutations. Funding: No funding was used for this project Disclosures: CSK is an Advisory Board member for Amgen and Merck Serono. GK is an honorary Advisory Board member for Bayer. All other authors declare no conflicts of interest
15 15 References 1. Dahabreh IJ, Terasawa T, Castaldi PJ, Trikalinos TA. Systematic review: Anti epidermal growth factor receptor treatment effect modification by KRAS mutations. Ann Intern Med 2011; 154: Behl AS, Goddard KAB, Flottemesch TJ et al. Cost-effectiveness analysis of screening for KRAS and BRAF mutations in metastatic colorectal cancer. J Natl Cancer Inst 2012; 104: Douillard JY, Oliner KS, Siena S et al. Panitumumab-FOLFOX4 treatment and RAS mutations in colorectal cancer. N Engl J Med 2013; 369: Adelstein B-A, Dobbins TA, Harris CA et al. A systematic review and meta-analysis of KRAS status as the determinant of response to anti-egfr antibodies and the impact of partner chemotherapy in metastatic colorectal cancer. Eur J Cancer 2011; 47: Vale CL, Tierney JF, Fisher D et al. Does anti-egfr therapy improve outcome in advanced colorectal cancer? A systematic review and meta-analysis. Cancer Treat Rev 2012; 38: Grothey A, Lenz H-J. Explaining the Unexplainable: EGFR Antibodies in Colorectal Cancer. J Clin Oncol 2012; 30: Maughan TS, Adams RA, Smith CG et al. Addition of cetuximab to oxaliplatin-based first-line combination chemotherapy for treatment of advanced colorectal cancer: results of the randomised phase 3 MRC COIN trial. The Lancet 377: European Medicines Agency, Committee for Medicinal Products for Human Use. Erbitux Assessment report EMA/CHMP/701107/ _Variation/human/000558/WC pdf (accessed 8 April 2014). 9. European Medicines Agency, Committee for Medicinal Products for Human Use. Vectibix Assessment report EMA/413562/ _Variation/human/000741/WC pdf (accessed 8 April 2014). 10. Patterson S, D., Peeters M, Siena S et al. Comprehensive analysis of KRAS and NRAS mutations as predictive biomarkers for single agent panitumumab (pmab) response in a randomized, phase III metastatic colorectal cancer (mcrc) study ( ). J Clin Oncol 2013; 31: abstr Peeters M, Oliner KS, Price TJ et al. Analysis of KRAS/NRAS mutations in phase 3 study of panitumumab (pmab) plus FOLFIRI versus FOLFIRI for second-line treatment (tx) of metastatic colorectal cancer (mcrc). J Clin Oncol 2014; 32: abstr LBA Peeters M, Douillard JY, Van Cutsem E et al. Mutant KRAS Codon 12 and 13 Alleles in Patients With mcrc: assessment as biomarkers of Response to Panitumumab. J Clin Oncol 2013; 31: Seymour MT, Brown SR, Middleton G et al. Panitumumab and irinotecan versus irinotecan alone for patients with KRAS wild-type, fluorouracil-resistant advanced colorectal cancer (PICCOLO): A prospectively stratified randomised trial. Lancet Oncol 2013; 14: Stintzing S, Jung A, Rossius L et al. Mutations within the EGFR signaling pathway: Influence on efficacy in FIRE-3-A randomized phase III study of FOLFIRI plus cetuximab or bevacizumab as first-line treatment for wild-type (WT) KRAS (exon 2) metastatic colorectal cancer (mcrc) patients. J Clin Oncol 2014; 32: abstr Bokemeyer C, Kohne CH, Ciardiello F et al. Treatment outcome according to tumor RAS mutation status in OPUS study patients with metastatic colorectal cancer (mcrc) randomized to FOLFOX4 with/without cetuximab. J Clin Oncol 2014; 32: abstr Schwartzberg LS, Rivera F, Karthaus M et al. PEAK: A Randomized, Multicenter Phase II Study of Panitumumab Plus Modified Fluorouracil, Leucovorin, and Oxaliplatin
16 16 (mfolfox6) or Bevacizumab Plus mfolfox6 in Patients With Previously Untreated, Unresectable, Wild-Type KRAS Exon 2 Metastatic Colorectal Cancer. J Clin Oncol Karthaus M, Schwartzberg L, Rivera F et al. Updated overall survival (OS) analysis of novel predictive KRAS/NRAS mutations beyond KRAS exon 2 in PEAK: A 1st-line phase 2 study of FOLFOX6 plus panitumumab (pmab) or bevacizumab (bev) in metastatic colorectal cancer (mcrc). Eur J Cancer 2013; 49: S Ciardiello F, Lenz HJ, Kohne CH et al. Treatment outcome according to tumor RAS mutation status in CRYSTAL study patients with metastatic colorectal cancer (mcrc) randomized to FOLFIRI with/without cetuximab.. J Clin Oncol 2014; 32: abstr Amado RG, Wolf M, Peeters M et al. Wild-type KRAS is required for panitumumab efficacy in patients with metastatic colorectal cancer. J Clin Oncol 2008; 26: Jonker DJ, O'Callaghan CJ, Karapetis CS et al. Cetuximab for the Treatment of Colorectal Cancer. N Engl J Med 2007; 357: Venook AP, Niedzwiecki D, Lenz HJ et al. CALGB/SWOG 80405: Phase III trial of irinotecan/5-fu/leucovorin (FOLFIRI) or oxaliplatin/5-fu/leucovorin (mfolfox6) with bevacizumab (BV) or cetuximab (CET) for patients (pts) with KRAS wild-type (wt) untreated metastatic adenocarcinoma of the colon or rectum (MCRC). J Clin Oncol 2014; 32: abstr LBA Tveit K GT, Glimelius B et al.. Randomized phase III study of 5- fluorouracil/folinate/oxaliplatin given continuously or intermittently with or without cetuximab, as first-line treatment of metastatic colorectal cancer: The NORDIC VII study (NCT ), by the Nordic Colorectal Cancer Biomodulation Group. Ann Oncol 2010; viii Sobrero AF, Maurel J, Fehrenbacher L et al. EPIC: Phase III Trial of Cetuximab Plus Irinotecan After Fluoropyrimidine and Oxaliplatin Failure in Patients With Metastatic Colorectal Cancer. J Clin Oncol 2008; 26: Jonker DJ, Karapetis C, Harbison CT. Epiregulin gene expression as a biomarker of benefit from cetuximab in the treatment of advanced colorectal cancer. Br J Cancer 2014; 110: Sartore-Bianchi A, Martini M, Molinari F et al. PIK3CA Mutations in Colorectal Cancer Are Associated with Clinical Resistance to EGFR-Targeted antibodies. Cancer Res 2009; 69: De Roock W, De Vriendt V, Normanno N et al. KRAS, BRAF, PIK3CA, and PTEN mutations: implications for targeted therapies in metastatic colorectal cancer. Lancet Oncol 2010; 12:
17 17 Table 1. Summary of studies included in the meta-analysis Figure 1. Grouping of tumors by KRAS exon 2 mutations and extended RAS mutations. Figure 2. Prevalence of new RAS mutations across studies NA; not applicable, NE; not evaluated, NR; evaluated but not reported a New RAS mutations are reported as a proportion of the KRAS exon 2 wild-type group. b KRAS and NRAS codon 59 mutation not evaluated. c KRAS codon 117 mutation not evaluated d includes exon 3 codon 61 mutations in addition to the exon 2 mutations e only NRAS mutation G12C evaluated f Random-effects meta-analysis summary estimates (95% confidence interval) based on studies that have evaluated all relevant codons Figure 3. The relative size of the anti-egfr treatment effect for tumors with one of the new RAS mutations compared to (A) tumors without any RAS mutations, and (B) tumors with any KRAS exon 2 mutations. Figure 4. Anti-EGFR treatment benefit for tumors without any RAS mutations (all RAS wildtype) and tumors without any KRAS exon 2 mutations (KRAS exon 2 wild-type) with respect to (A) progression-free survival, and (B) overall survival. cmab; cetuximab, OS; overall survival, PFS; progression-free survival, pmab; panitumumab
18 18 Figure 5. Anti-EGFR treatment benefit for tumors with any RAS mutations and tumors with any KRAS exon 2 mutations with respect to (A) progression-free survival, and (B) overall survival. cmab; cetuximab, OS; overall survival, PFS; progression-free survival, pmab; panitumumab

19 19
20 20
21 21
22 22
23 23
24 24
25 25
26 26
27 Table 1. Summary of studies included in the meta-analysis Anti-EGFR Agent Vs. Comparator Trial Name Line, Background Treatment N (ITT) Exons Evaluated a KRAS NRAS Ascertainment KRAS exon 2 / New RAS b exons Wild-type Proportion c KRAS exon 2 / All RAS exons OPUS 1 st line, FOLFOX % / 66% 57% / 42% Cetuximab Vs. No Cetuximab COIN 1 st line, OxFp 1630 d 79% / 100% 56% / 53% CRYSTAL 1 st line, FOLFIRI % / 65% 63% / 54% Panitumumab Vs. No Panitumumab Cetuximab Vs. Bevacizumab Panitumumab Vs. Bevacizumab Notes: PRIME PICCOLO FIRE-3 PEAK 1 st line, FOLFOX 2 nd line, FOLFIRI 2 nd line, Irinotecan 3 rd line, BSC 1 st line, FOLFIRI 1 st line, FOLFOX % / 95% 60% / 51% % / 87% 55% / 44% 615 d 92% / ~81% NA % / 68% 57% / 47% % / 69% NA % / 79% NA BSC: best supportive care, FOLFIRI: folinic acid, fluorouracil and irinotecan, FOLFOX: folinic acid, fluorouracil and oxaliplatin, ITT: overall intention-to-treat population, NA: not applicable, OxFp; oxaliplatin and fluoropyrimidine chemotherapy a dark grey shading indicates that all codons within the specified exon were assessed, and light grey shading indicates some but not all codons were assessed. b Ascertainment of the new RAS mutations refers to the proportion of KRAS exon 2 wild-type participants that were evaluable for the new RAS mutations
Validated and promising predictive factors in mcrc: Recent updates on RAS testing Fotios Loupakis, MD PhD
 Validated and promising predictive factors in mcrc: Recent updates on RAS testing Fotios Loupakis, MD PhD U.O. Oncologia 2 Universitaria Azienda Ospedaliero-Universitaria Pisana Pisa, Italy Learning Objectives
Validated and promising predictive factors in mcrc: Recent updates on RAS testing Fotios Loupakis, MD PhD U.O. Oncologia 2 Universitaria Azienda Ospedaliero-Universitaria Pisana Pisa, Italy Learning Objectives
Related Policies None
 Medical Policy MP 2.04.53 BCBSA Ref. Policy: 2.04.53 Last Review: 07/25/2018 Effective Date: 07/25/2018 Section: Medicine Related Policies None DISCLAIMER Our medical policies are designed for informational
Medical Policy MP 2.04.53 BCBSA Ref. Policy: 2.04.53 Last Review: 07/25/2018 Effective Date: 07/25/2018 Section: Medicine Related Policies None DISCLAIMER Our medical policies are designed for informational
Extended RAS testing in metastatic colorectal cancer Refining the predictive molecular biomarkers
 Review Article Extended RAS testing in metastatic colorectal cancer Refining the predictive molecular biomarkers Humaid O. Al-Shamsi 1, Waleed Alhazzani 2, Robert A. Wolff 1 1 Department of Gastrointestinal
Review Article Extended RAS testing in metastatic colorectal cancer Refining the predictive molecular biomarkers Humaid O. Al-Shamsi 1, Waleed Alhazzani 2, Robert A. Wolff 1 1 Department of Gastrointestinal
KRAS, NRAS, and BRAF Variant Analysis in Metastatic Colorectal Cancer
 KRAS, NRAS, and BRAF Variant Analysis in Metastatic Colorectal Cancer Policy Number: 2.04.53 Last Review: 5/2018 Origination: 1/2011 Next Review: 5/2019 Policy Blue Cross and Blue Shield of Kansas City
KRAS, NRAS, and BRAF Variant Analysis in Metastatic Colorectal Cancer Policy Number: 2.04.53 Last Review: 5/2018 Origination: 1/2011 Next Review: 5/2019 Policy Blue Cross and Blue Shield of Kansas City
Page: 1 of 17. KRAS, NRAS and BRAF Mutation Analysis in Metastatic Colorectal Cancer
 Page: 1 of 17 Last Review Status/Date: March 2015 Analysis in Metastatic Colorectal Cancer Description This policy summarizes the evidence for using tumor cell KRAS, NRAS and BRAF mutational status as
Page: 1 of 17 Last Review Status/Date: March 2015 Analysis in Metastatic Colorectal Cancer Description This policy summarizes the evidence for using tumor cell KRAS, NRAS and BRAF mutational status as
ADVANCED COLORECTAL CANCER: UNRESECTABLE OR BORDERLINE RESECTABLE (GROUP 1) CHEMOTHERAPY +/- TARGETED AGENTS. Andrés Cervantes. Professor of Medicine
 CHEMOTHERAPY +/- TARGETED AGENTS. Andrés Cervantes. Professor of Medicine") ADVANCED COLORECTAL CANCER: UNRESECTABLE OR BORDERLINE RESECTABLE (GROUP 1) CHEMOTHERAPY +/- TARGETED AGENTS Andrés Cervantes Professor of Medicine 1995 One option Advances in the treatment of mcrc 2000
ADVANCED COLORECTAL CANCER: UNRESECTABLE OR BORDERLINE RESECTABLE (GROUP 1) CHEMOTHERAPY +/- TARGETED AGENTS Andrés Cervantes Professor of Medicine 1995 One option Advances in the treatment of mcrc 2000
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 KRAS, NRAS, and BRAF Variant Analysis in Metastatic Colorectal Cancer Page 1 of 25 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: KRAS, NRAS, and BRAF Variant Analysis
KRAS, NRAS, and BRAF Variant Analysis in Metastatic Colorectal Cancer Page 1 of 25 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: KRAS, NRAS, and BRAF Variant Analysis
Description of Procedure or Service. Policy. Benefits Application
 Corporate Medical Policy KRAS, NRAS, BRAF Mutation Analysis and Related File Name: Origination: Last CAP Review: Next CAP Review: Last Review: kras_nras_braf_mutation_analysis_and_related_treatment_in_metastatic_colorectal_cancer
Corporate Medical Policy KRAS, NRAS, BRAF Mutation Analysis and Related File Name: Origination: Last CAP Review: Next CAP Review: Last Review: kras_nras_braf_mutation_analysis_and_related_treatment_in_metastatic_colorectal_cancer
First line treatment in metastatic colorectal cancer
 First line treatment in metastatic colorectal cancer Claus-Henning Köhne University Clinic Onkology and Haematology North West German Cancer Center (NWTZ) A non authorised version of ESMO guidelines was
First line treatment in metastatic colorectal cancer Claus-Henning Köhne University Clinic Onkology and Haematology North West German Cancer Center (NWTZ) A non authorised version of ESMO guidelines was
Populations Interventions Comparators Outcomes Individuals: With metastatic colorectal cancer
 Metastatic Colorectal Cancer (20453) Medical Benefit Effective Date: 07/01/17 Next Review Date: 05/18 Preauthorization Yes Review Dates: 05/12, 05/13, 05/14, 05/15, 05/16, 07/16, 05/17 Preauthorization
Metastatic Colorectal Cancer (20453) Medical Benefit Effective Date: 07/01/17 Next Review Date: 05/18 Preauthorization Yes Review Dates: 05/12, 05/13, 05/14, 05/15, 05/16, 07/16, 05/17 Preauthorization
Κίκα Πλοιαρχοπούλου. Παθολόγος Ογκολόγος Ευρωκλινική Αθηνών
 Κίκα Πλοιαρχοπούλου Παθολόγος Ογκολόγος Ευρωκλινική Αθηνών Time (months) Survival outcomes in mcrc have progressively improved over the past two decades Treatment options for many patients Multidisciplinary
Κίκα Πλοιαρχοπούλου Παθολόγος Ογκολόγος Ευρωκλινική Αθηνών Time (months) Survival outcomes in mcrc have progressively improved over the past two decades Treatment options for many patients Multidisciplinary
METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD
 METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD INTRODUCTION Second leading cause of cancer related death in the United States. 136,830 cases in 2014
METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD INTRODUCTION Second leading cause of cancer related death in the United States. 136,830 cases in 2014
MEDICAL POLICY. SUBJECT: GENOTYPING - RAS MUTATION ANALYSIS IN METASTATIC COLORECTAL CANCER (KRAS/NRAS) POLICY NUMBER: CATEGORY: Laboratory
 POLICY NUMBER: CATEGORY: Laboratory") MEDICAL POLICY Clinical criteria used to make utilization review decisions are based on credible scientific evidence published in peer reviewed medical literature generally recognized by the medical community.
MEDICAL POLICY Clinical criteria used to make utilization review decisions are based on credible scientific evidence published in peer reviewed medical literature generally recognized by the medical community.
Prognostic significance of K-Ras mutation rate in metastatic colorectal cancer patients. Bruno Vincenzi Università Campus Bio-Medico di Roma
 Prognostic significance of K-Ras mutation rate in metastatic colorectal cancer patients Bruno Vincenzi Università Campus Bio-Medico di Roma Colorectal cancer 3 rd most common cancer worldwide Approximately
Prognostic significance of K-Ras mutation rate in metastatic colorectal cancer patients Bruno Vincenzi Università Campus Bio-Medico di Roma Colorectal cancer 3 rd most common cancer worldwide Approximately
Supplementary Online Content
 Supplementary Online Content Venook AP, Niedzwiecki D, Lenz H-J, et al. Effect of first-line chemotherapy combined with cetuximab or bevacizumab on overall survival in patients with KRAS wild-type advanced
Supplementary Online Content Venook AP, Niedzwiecki D, Lenz H-J, et al. Effect of first-line chemotherapy combined with cetuximab or bevacizumab on overall survival in patients with KRAS wild-type advanced
Targeted therapies in colorectal cancer: the dos, don ts, and future directions
 Editorial Targeted therapies in colorectal cancer: the dos, don ts, and future directions Marwan Fakih City of Hope Comprehensive Cancer Center, 1500 E Duarte St, Duarte, CA 91010, USA Corresponding to:
Editorial Targeted therapies in colorectal cancer: the dos, don ts, and future directions Marwan Fakih City of Hope Comprehensive Cancer Center, 1500 E Duarte St, Duarte, CA 91010, USA Corresponding to:
EGFR-targeted therapy in metastatic colorectal cancer
 EGFR-targeted therapy in metastatic colorectal cancer What do we know and where are we going? Hagen Kennecke, MD, MHA, FRCPC Abstract N umerous Phase III studies have documented the benefit of panitumumab
EGFR-targeted therapy in metastatic colorectal cancer What do we know and where are we going? Hagen Kennecke, MD, MHA, FRCPC Abstract N umerous Phase III studies have documented the benefit of panitumumab
Does it matter which chemotherapy regimen you partner with the biologic agents?
 Does it matter which chemotherapy regimen you partner with the biologic agents? Yes, it does matter! Axel Grothey Disclosures Research Funding to MAYO Clinic Genentech Bayer Eisai Pfizer Imclone Potential
Does it matter which chemotherapy regimen you partner with the biologic agents? Yes, it does matter! Axel Grothey Disclosures Research Funding to MAYO Clinic Genentech Bayer Eisai Pfizer Imclone Potential
CURRENT STANDARD OF CARE OF COLORECTAL CANCER: THE EVOLUTION OF ESMO CLINICAL PRACTICE GUIDELINES
 CURRENT STANDARD OF CARE OF COLORECTAL CANCER: THE EVOLUTION OF ESMO CLINICAL PRACTICE GUIDELINES Fortunato Ciardiello ESMO Past-President 2018-2019 Dipartimento di Medicina di Precisione Università degli
CURRENT STANDARD OF CARE OF COLORECTAL CANCER: THE EVOLUTION OF ESMO CLINICAL PRACTICE GUIDELINES Fortunato Ciardiello ESMO Past-President 2018-2019 Dipartimento di Medicina di Precisione Università degli
Review of the ESMO consensus conference on metastatic CRC Basis strategies ad groups (RAS, BRAF, etc) Michel Ducreux
 Michel Ducreux") Review of the ESMO consensus conference on metastatic CRC Basis strategies ad groups (RAS, BRAF, etc) Michel Ducreux 2 ESMO consensus on mcrc 2016 Chairs: Co-Chairs of working groups E Van Cutsem A Sobrero
Review of the ESMO consensus conference on metastatic CRC Basis strategies ad groups (RAS, BRAF, etc) Michel Ducreux 2 ESMO consensus on mcrc 2016 Chairs: Co-Chairs of working groups E Van Cutsem A Sobrero
RAS and BRAF in metastatic colorectal cancer management
 Review Article RAS and BRAF in metastatic colorectal cancer management Jun Gong 1, May Cho 1, Marwan Fakih 2 1 Department of Medical Oncology, City of Hope National Medical Center, Duarte, CA, USA; 2 Medical
Review Article RAS and BRAF in metastatic colorectal cancer management Jun Gong 1, May Cho 1, Marwan Fakih 2 1 Department of Medical Oncology, City of Hope National Medical Center, Duarte, CA, USA; 2 Medical
Conflicts of Interest GI Malignancies: An Update on Current Treatment Options
 Conflicts of Interest GI Malignancies: An Update on Current Treatment Options Nothing to disclose Trevor McKibbin, PharmD, MS, BCOP Clinical Specialist, Hematology/Oncology Winship Cancer Institute of
Conflicts of Interest GI Malignancies: An Update on Current Treatment Options Nothing to disclose Trevor McKibbin, PharmD, MS, BCOP Clinical Specialist, Hematology/Oncology Winship Cancer Institute of
Colon Cancer Molecular Target Agents
 Colon Cancer Molecular Target Agents Ci Caio Max SR S. Rocha Lima, M.D. MD Professor of Medicine CDi CoDiretor Cl Colorectal tlheptobiliary, Pancreatic SDG, and Phase I Unit University of Miami & Silvester
Colon Cancer Molecular Target Agents Ci Caio Max SR S. Rocha Lima, M.D. MD Professor of Medicine CDi CoDiretor Cl Colorectal tlheptobiliary, Pancreatic SDG, and Phase I Unit University of Miami & Silvester
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan
 State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
OPTIMISING OUTCOMES FOR PATIENTS WITH ADVANCED COLORECTAL CANCER
 OPTIMISING OUTCOMES FOR PATIENTS WITH ADVANCED COLORECTAL CANCER E-Learning Module Stavros Gkolfinopoulos 1, Demetris Papamichael 1, George Pentheroudakis 2 1. Cyprus Oncology Centre, Nicosia, Cyprus 2.
OPTIMISING OUTCOMES FOR PATIENTS WITH ADVANCED COLORECTAL CANCER E-Learning Module Stavros Gkolfinopoulos 1, Demetris Papamichael 1, George Pentheroudakis 2 1. Cyprus Oncology Centre, Nicosia, Cyprus 2.
Efficacy of cetuximab based chemotherapy in metastatic colorectal cancer according to RAS and BRAF mutation subgroups: A meta analysis
 MOLECULAR AND CLINICAL ONCOLOGY 4: 1017-1024, 2016 Efficacy of cetuximab based chemotherapy in metastatic colorectal cancer according to RAS and BRAF mutation subgroups: A meta analysis LI LIN 1,2*, LU
MOLECULAR AND CLINICAL ONCOLOGY 4: 1017-1024, 2016 Efficacy of cetuximab based chemotherapy in metastatic colorectal cancer according to RAS and BRAF mutation subgroups: A meta analysis LI LIN 1,2*, LU
Author's response to reviews
 Author's response to reviews Title:FCGR2A and FCGR3A polymorphisms and clinical outcome in metastatic colorectal cancer patients treated with 1st line 5-fluorouracil/folinic acid and oxaliplatin +/- cetuximab
Author's response to reviews Title:FCGR2A and FCGR3A polymorphisms and clinical outcome in metastatic colorectal cancer patients treated with 1st line 5-fluorouracil/folinic acid and oxaliplatin +/- cetuximab
Metastatik Kolorektal Kanser Tedavisinde Yeni Biyobelirteçler Sonrası Panitumumab. Prof. Dr. N. Faruk Aykan Antalya 22 Mart 2014
 Metastatik Kolorektal Kanser Tedavisinde Yeni Biyobelirteçler Sonrası Panitumumab Prof. Dr. N. Faruk Aykan Antalya 22 Mart 2014 1952-1953 St. Louis, ABD Kinase growth factor pathway Activated receptor
Metastatik Kolorektal Kanser Tedavisinde Yeni Biyobelirteçler Sonrası Panitumumab Prof. Dr. N. Faruk Aykan Antalya 22 Mart 2014 1952-1953 St. Louis, ABD Kinase growth factor pathway Activated receptor
KRAS G13D mutation testing and anti-egfr therapy
 KRAS G13D mutation testing and anti-egfr therapy KRAS G13D mutation and anti-egfr therapy Current data do not support a need to specifically identify this mutation for assessing anti-egfr eligibility in
KRAS G13D mutation testing and anti-egfr therapy KRAS G13D mutation and anti-egfr therapy Current data do not support a need to specifically identify this mutation for assessing anti-egfr eligibility in
ANTI-EGFR IN MCRC? Assoc. Prof. Gerald Prager, Medical University of Vienna, Austria
 IS IT TIME TO RE-CHALLENGE ANTI-EGFR IN MCRC? Assoc. Prof. Gerald Prager, Medical University of Vienna, Austria Dr. Andrea Sartore-Bianchi, Oncologia Clinica Molecolare, Niguarda Cancer Center, Milano,
IS IT TIME TO RE-CHALLENGE ANTI-EGFR IN MCRC? Assoc. Prof. Gerald Prager, Medical University of Vienna, Austria Dr. Andrea Sartore-Bianchi, Oncologia Clinica Molecolare, Niguarda Cancer Center, Milano,
What s New in Colon Cancer? Therapy over the last decade
 What s New in Colon Cancer? 9/19/2014 Michael McNamara, MD Therapy over the last decade Cytotoxic chemotherapy - 5FU ( Mayo, Roswell, Infusional) - Xeloda (01 ) - Oxaliplatin (02 ) - Irinotecan (96 ) Anti-
What s New in Colon Cancer? 9/19/2014 Michael McNamara, MD Therapy over the last decade Cytotoxic chemotherapy - 5FU ( Mayo, Roswell, Infusional) - Xeloda (01 ) - Oxaliplatin (02 ) - Irinotecan (96 ) Anti-
MÁS ALLA DE LA PRIMERA LÍNEA: SECUENCIA DE TRATAMIENTO. Dra. Ruth Vera Complejo Hospitalario de Navarra
 MÁS ALLA DE LA PRIMERA LÍNEA: SECUENCIA DE TRATAMIENTO Dra. Ruth Vera Complejo Hospitalario de Navarra GOALS Prolongation of survival Cure Improving tumour-related symptoms Stopping tumour progression
MÁS ALLA DE LA PRIMERA LÍNEA: SECUENCIA DE TRATAMIENTO Dra. Ruth Vera Complejo Hospitalario de Navarra GOALS Prolongation of survival Cure Improving tumour-related symptoms Stopping tumour progression
Panitumumab: The KRAS Story. Chrissie Fletcher, MSc. BSc. CStat. CSci. Director Biostatistics, Amgen Ltd
 Panitumumab: The KRAS Story Chrissie Fletcher, MSc. BSc. CStat. CSci. Director Biostatistics, Amgen Ltd Clinical Background: panitumumab in mcrc Panitumumab is a fully human IgG2 monoclonal antibody directed
Panitumumab: The KRAS Story Chrissie Fletcher, MSc. BSc. CStat. CSci. Director Biostatistics, Amgen Ltd Clinical Background: panitumumab in mcrc Panitumumab is a fully human IgG2 monoclonal antibody directed
JY Douillard MD, PhD Professor of Medical Oncology
 Colorectal Cancer ESMO Preceptorship Program Prague May 22-23rd 2014 Review of the ESMO Consensus Conference on metastatic colo-rectal cancer Basic strategy and groups (RASwt/mut, BRAF mut) JY Douillard
Colorectal Cancer ESMO Preceptorship Program Prague May 22-23rd 2014 Review of the ESMO Consensus Conference on metastatic colo-rectal cancer Basic strategy and groups (RASwt/mut, BRAF mut) JY Douillard
Daniele Santini University Campus Bio-Medico Rome, Italy
 Daniele Santini University Campus Bio-Medico Rome, Italy Anti EGFR therapy and colorectal cancer Cetuximab or Panitumumab Adapted from Ciardiello F. and Tortora G. NEJM 2008;358:1160-74 Who will benefit
Daniele Santini University Campus Bio-Medico Rome, Italy Anti EGFR therapy and colorectal cancer Cetuximab or Panitumumab Adapted from Ciardiello F. and Tortora G. NEJM 2008;358:1160-74 Who will benefit
Vectibix. Vectibix (panitumumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.85 Subject: Vectibix Page: 1 of 5 Last Review Date: December 2, 2016 Vectibix Description Vectibix
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.85 Subject: Vectibix Page: 1 of 5 Last Review Date: December 2, 2016 Vectibix Description Vectibix
TRANSPARENCY COMMITTEE
 The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 3 September 2014 VECTIBIX, 20 mg/ml, concentrate for solution for infusion B/1 5 ml vial (CIP: 34009 571 818 5 7)
The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 3 September 2014 VECTIBIX, 20 mg/ml, concentrate for solution for infusion B/1 5 ml vial (CIP: 34009 571 818 5 7)
Q11: WHAT IS THE CURRENT STANDARD FIRST LINE TREATMENT FOR METASTATIC INOPERABLE COLORECTAL CANCER?
 Q11: WHAT IS THE CURRENT STANDARD FIRST LINE TREATMENT FOR METASTATIC INOPERABLE COLORECTAL CANCER? Version 11/24/2011 3:08 PM Q11 TABLE OF CONTENTS SCIENTIFIC REPORT... 6 1 INTRODUCTION... 6 1.1 PICO...
Q11: WHAT IS THE CURRENT STANDARD FIRST LINE TREATMENT FOR METASTATIC INOPERABLE COLORECTAL CANCER? Version 11/24/2011 3:08 PM Q11 TABLE OF CONTENTS SCIENTIFIC REPORT... 6 1 INTRODUCTION... 6 1.1 PICO...
JY Douillard MD, PhD Professor of Medical Oncology
 ESMO Preceptorship Colorectal Cancer Colorectal ESMO Cancer Preceptorship Vienna 26-27 Program October 2015 Prague May 22-23rd 2014 Review of the ESMO Consensus Conference on metastatic colo-rectal cancer
ESMO Preceptorship Colorectal Cancer Colorectal ESMO Cancer Preceptorship Vienna 26-27 Program October 2015 Prague May 22-23rd 2014 Review of the ESMO Consensus Conference on metastatic colo-rectal cancer
Understanding predictive and prognostic markers
 Understanding predictive and prognostic markers Professor Aimery de Gramont Chairman of ARCAD Foundation and GERCOR, Paris FRANCE Understanding predictive and prognostic markers Aimery de Gramont Prognostic
Understanding predictive and prognostic markers Professor Aimery de Gramont Chairman of ARCAD Foundation and GERCOR, Paris FRANCE Understanding predictive and prognostic markers Aimery de Gramont Prognostic
Cetuximab in third-line therapy of patients with metastatic colorectal cancer: A single institution experience
 JBUON 2016; 21(1): 70-79 ISSN: 1107-0625, online ISSN: 2241-6293 www.jbuon.com E-mail: editorial_office@jbuon.com ORIGINAL ARTICLE Cetuximab in third-line therapy of patients with metastatic colorectal
JBUON 2016; 21(1): 70-79 ISSN: 1107-0625, online ISSN: 2241-6293 www.jbuon.com E-mail: editorial_office@jbuon.com ORIGINAL ARTICLE Cetuximab in third-line therapy of patients with metastatic colorectal
Available at journal homepage:
 European Journal of Cancer (212) 48, 1466 1475 Available at www.sciencedirect.com journal homepage: www.ejconline.com Addition of cetuximab to chemotherapy as first-line treatment for KRAS wild-type metastatic
European Journal of Cancer (212) 48, 1466 1475 Available at www.sciencedirect.com journal homepage: www.ejconline.com Addition of cetuximab to chemotherapy as first-line treatment for KRAS wild-type metastatic
Kolorektalni karcinom- novosti u liječenju. PANEL: Maja Banjin, Janja Ocvirk, Borislav Belev, Ivan Nikolić, Anes Pašić
 Kolorektalni karcinom- novosti u liječenju PANEL: Maja Banjin, Janja Ocvirk, Borislav Belev, Ivan Nikolić, Anes Pašić Kolorektalni karcinomnovosti u liječenju PANEL : Maja Banjin, Janja Ocvirk, Borislav
Kolorektalni karcinom- novosti u liječenju PANEL: Maja Banjin, Janja Ocvirk, Borislav Belev, Ivan Nikolić, Anes Pašić Kolorektalni karcinomnovosti u liječenju PANEL : Maja Banjin, Janja Ocvirk, Borislav
The left versus right colon cancer story What is the truth?
 The left versus right colon cancer story What is the truth? Prof. V. Heinemann CCC LMU, Klinikum Grosshadern Ludwig-Maximilian-University of Munich, Germany Three stages of truth (Schopenhauer) Ridicule
The left versus right colon cancer story What is the truth? Prof. V. Heinemann CCC LMU, Klinikum Grosshadern Ludwig-Maximilian-University of Munich, Germany Three stages of truth (Schopenhauer) Ridicule
Targeted Therapies in Metastatic Colorectal Cancer: An Update
 Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
Populations Interventions Comparators Outcomes Individuals: With metastatic colorectal cancer. Comparators of interest. are:
 KRAS, NRAS, and BRAF Variant Analysis in Metastatic Colorectal (20453) (Formerly KRAS, NRAS, and BRAF Mutation Analysis in Metastatic Colorectal ) Medical Benefit Effective Date: 07/01/18 Next Review Date:
KRAS, NRAS, and BRAF Variant Analysis in Metastatic Colorectal (20453) (Formerly KRAS, NRAS, and BRAF Mutation Analysis in Metastatic Colorectal ) Medical Benefit Effective Date: 07/01/18 Next Review Date:
KRAS MUTATION ANALYSIS IN METASTATIC COLORECTAL CANCER
 KRAS MUTATION ANALYSIS IN METASTATIC COLORECTAL CANCER Protocol: GEN004 Effective Date: September 1, 2017 Table of Contents Page COMMERCIAL AND MEDICAID COVERAGE RATIONALE... 1 MEDICARE COVERAGE RATIONALE...
KRAS MUTATION ANALYSIS IN METASTATIC COLORECTAL CANCER Protocol: GEN004 Effective Date: September 1, 2017 Table of Contents Page COMMERCIAL AND MEDICAID COVERAGE RATIONALE... 1 MEDICARE COVERAGE RATIONALE...
FEP Medical Policy Manual
 FEP Medical Policy Manual FEP 2.04.53 KRAS, NRAS, and BRAF Variant Analysis in Effective Date: April 15, 2018 Related Policies: 5.21.84 Erbitux (cetuximab) 5.21.85 Vectibix (panitumamab) KRAS, NRAS, and
FEP Medical Policy Manual FEP 2.04.53 KRAS, NRAS, and BRAF Variant Analysis in Effective Date: April 15, 2018 Related Policies: 5.21.84 Erbitux (cetuximab) 5.21.85 Vectibix (panitumamab) KRAS, NRAS, and
Cetuximab with Chemotherapy as Treatment for Stage III Colon or Metastatic Colorectal Cancer
 Cetuximab with Chemotherapy as Treatment for Stage III Colon or Metastatic Colorectal Cancer Cetuximab with Chemotherapy (CT) as First-Line Treatment for Metastatic Colorectal Cancer (mcrc): Analysis of
Cetuximab with Chemotherapy as Treatment for Stage III Colon or Metastatic Colorectal Cancer Cetuximab with Chemotherapy (CT) as First-Line Treatment for Metastatic Colorectal Cancer (mcrc): Analysis of
COLORECTAL CANCER. Bert H. O Neil, MD Jackie and Joseph Cusick Professor of Oncology Director, GI Malignancies and Phase I Program
 COLORECTAL CANCER Bert H. O Neil, MD Jackie and Joseph Cusick Professor of Oncology Director, GI Malignancies and Phase I Program Rectal Cancer Adjuvant therapy No single study specific to rectal cancer
COLORECTAL CANCER Bert H. O Neil, MD Jackie and Joseph Cusick Professor of Oncology Director, GI Malignancies and Phase I Program Rectal Cancer Adjuvant therapy No single study specific to rectal cancer
Name of Policy: Panitumumab, Vectibix
 Name of Policy: Panitumumab, Vectibix Policy #: 369 Latest Review Date: June 2014 Category: Pharmacology Policy Grade: B Background/Definitions: As a general rule, benefits are payable under Blue Cross
Name of Policy: Panitumumab, Vectibix Policy #: 369 Latest Review Date: June 2014 Category: Pharmacology Policy Grade: B Background/Definitions: As a general rule, benefits are payable under Blue Cross
Published Ahead of Print on November 26, 2012 as /JCO J Clin Oncol by American Society of Clinical Oncology
 Published Ahead of Print on November 26, 202 as.200/jco.202.45.492 The latest version is at http://jco.ascopubs.org/cgi/doi/.200/jco.202.45.492 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T
Published Ahead of Print on November 26, 202 as.200/jco.202.45.492 The latest version is at http://jco.ascopubs.org/cgi/doi/.200/jco.202.45.492 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T
MEET ROY*: A PATIENT WITH LIVER-LIMITED mcrc
 MEET ROY*: A PATIENT WITH LIVER-LIMITED mcrc * A hypothetical case study of a patient eligible for first-line mcrc therapy. mcrc = metastatic colorectal cancer. WHAT CLINICAL CHARACTERISTICS AFFECT YOUR
MEET ROY*: A PATIENT WITH LIVER-LIMITED mcrc * A hypothetical case study of a patient eligible for first-line mcrc therapy. mcrc = metastatic colorectal cancer. WHAT CLINICAL CHARACTERISTICS AFFECT YOUR
Reprint requests: American Society of Clinical Oncology Mill Road, Suite 800. Alexandria, VA
 American Society of Clinical Oncology Provisional Clinical Opinion: Testing for KRAS Gene Mutations in Patients with Metastatic Colorectal Carcinoma to Predict Response to Anti Epidermal Growth Factor
American Society of Clinical Oncology Provisional Clinical Opinion: Testing for KRAS Gene Mutations in Patients with Metastatic Colorectal Carcinoma to Predict Response to Anti Epidermal Growth Factor
DOSING AND INFORMATION GUIDE LEAPS AHEAD
 DOSING AND INFORMATION GUIDE In patients with WT RAS* mcrc 1 VECTIBIX (panitumumab) LEAPS AHEAD 5.6-month increase in median OS with FOLFOX vs FOLFOX alone 1 Spot the difference. CHOOSE VECTIBIX PRIME
DOSING AND INFORMATION GUIDE In patients with WT RAS* mcrc 1 VECTIBIX (panitumumab) LEAPS AHEAD 5.6-month increase in median OS with FOLFOX vs FOLFOX alone 1 Spot the difference. CHOOSE VECTIBIX PRIME
DOES LOCATION MATTER IN COLORECTAL CANCER: LEFT VS RIGHT?
 DOES LOCATION MATTER IN COLORECTAL CANCER: LEFT VS RIGHT? By: Dr. Dominik Modest, Medical Department III, Hospital of the University of Munich, Germany Dr. Andrea Sartore-Bianchi, Niguarda Cancer Center,
DOES LOCATION MATTER IN COLORECTAL CANCER: LEFT VS RIGHT? By: Dr. Dominik Modest, Medical Department III, Hospital of the University of Munich, Germany Dr. Andrea Sartore-Bianchi, Niguarda Cancer Center,
Development of Conventional Chemotherapy in mcrc BSC vs. Chemo, Biochemical modulation, Oral fluoropyrimidines, Developmentof combination chemotherapy
 ESMO Preceptorship Colorectal Cancer Colorectal ESMO Cancer Preceptorship Valencia May Program 20-21st 2016 Prague May 22-23rd 2014 Development of Conventional Chemotherapy in mcrc BSC vs. Chemo, Biochemical
ESMO Preceptorship Colorectal Cancer Colorectal ESMO Cancer Preceptorship Valencia May Program 20-21st 2016 Prague May 22-23rd 2014 Development of Conventional Chemotherapy in mcrc BSC vs. Chemo, Biochemical
INDICATION: COMPENDIA TRANSPARENCY TRACKING FORM
 COMPENDIA TRANSPARENCY TRACKING FORM DRUG: Panitumumab INDICATION: Metastatic colorectal cancer, wild-type KRAS mutation, first-line therapy, in combination with infusional fluorouracil, leucovorin, and
COMPENDIA TRANSPARENCY TRACKING FORM DRUG: Panitumumab INDICATION: Metastatic colorectal cancer, wild-type KRAS mutation, first-line therapy, in combination with infusional fluorouracil, leucovorin, and
COMETS: COlorectal MEtastatic Two Sequences
 COMETS: COlorectal MEtastatic Two Sequences A Phase III Multicenter Trial Comparing Two Different Sequences of Second/Third Line Therapy (Irinotecan/Cetuximab Followed By FOLFOX-4 vs. FOLFOX-4 Followed
COMETS: COlorectal MEtastatic Two Sequences A Phase III Multicenter Trial Comparing Two Different Sequences of Second/Third Line Therapy (Irinotecan/Cetuximab Followed By FOLFOX-4 vs. FOLFOX-4 Followed
K-Ras mutational status and response to EGFR inhibitors for treatment of advanced CRC. Monica Bertagnolli, MD. CRA Continuing Education, November 2008
 K-Ras mutational status and response to EGFR inhibitors for treatment of advanced CRC Monica Bertagnolli, MD CRA Continuing Education, November 2008 The Ras Oncogene Kirsten and Harvey: 1964 Identification
K-Ras mutational status and response to EGFR inhibitors for treatment of advanced CRC Monica Bertagnolli, MD CRA Continuing Education, November 2008 The Ras Oncogene Kirsten and Harvey: 1964 Identification
MEETING SUMMARY ESMO 2018, Munich, Germany. Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER
 MEETING SUMMARY ESMO 2018, Munich, Germany Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER DISCLAIMER Please note: The views expressed within this presentation are the personal
MEETING SUMMARY ESMO 2018, Munich, Germany Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER DISCLAIMER Please note: The views expressed within this presentation are the personal
Fluorouracil, Leucovorin, and Irinotecan Plus Cetuximab Treatment and RAS Mutations in Colorectal Cancer
 VOLUME NUMBER 7 MARCH 5 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Fluorouracil, Leucovorin, and Irinotecan Plus Treatment and RAS Mutations in Colorectal Cancer Eric Van Cutsem, Heinz-Josef
VOLUME NUMBER 7 MARCH 5 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Fluorouracil, Leucovorin, and Irinotecan Plus Treatment and RAS Mutations in Colorectal Cancer Eric Van Cutsem, Heinz-Josef
Managing mcrc Across Disease Continuum: Front-Line Therapy and Treatment Beyond Progression
 Managing mcrc Across Disease Continuum: Front-Line Therapy and Treatment Beyond Progression Guillermo Méndez, MD Sección Oncología Hospital de Gastroenterología Bonorino Udaondo Carlos B. Udaondo y Fundación
Managing mcrc Across Disease Continuum: Front-Line Therapy and Treatment Beyond Progression Guillermo Méndez, MD Sección Oncología Hospital de Gastroenterología Bonorino Udaondo Carlos B. Udaondo y Fundación
OHTAC Recommendation. KRAS Testing for Anti-EGFR Therapy in Advanced Colorectal Cancer
 OHTAC Recommendation KRAS Testing for Anti-EGFR Therapy in Advanced Colorectal Cancer Presented to the Ontario Health Technology Advisory Committee in August, 2010 December 2010 Issue Background In February
OHTAC Recommendation KRAS Testing for Anti-EGFR Therapy in Advanced Colorectal Cancer Presented to the Ontario Health Technology Advisory Committee in August, 2010 December 2010 Issue Background In February
Colorectal cancer is the second most common cause of
 SYSTEMIC TREATMENT FOR METASTATIC COLORECTAL CANCER Systemic Treatment: Maintenance Compared with Holiday Cornelis J.A. Punt, MD, PhD, Lieke H.J. Simkens, MD, and Miriam Koopman, MD, PhD OVERVIEW With
SYSTEMIC TREATMENT FOR METASTATIC COLORECTAL CANCER Systemic Treatment: Maintenance Compared with Holiday Cornelis J.A. Punt, MD, PhD, Lieke H.J. Simkens, MD, and Miriam Koopman, MD, PhD OVERVIEW With
Horizon Scanning in Oncology
 Horizon Scanning in Oncology Panitumumab (Vectibix ) for the first-line treatment of metastatic colorectal cancer DSD: Horizon Scanning in Oncology Nr. 011 ISSN online 2076-5940 Horizon Scanning in Oncology
Horizon Scanning in Oncology Panitumumab (Vectibix ) for the first-line treatment of metastatic colorectal cancer DSD: Horizon Scanning in Oncology Nr. 011 ISSN online 2076-5940 Horizon Scanning in Oncology
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Stivarga) Reference Number: CP.CPA.157 Effective Date: 11.16.17 Last Review Date: 11.17 Line of Business: Medicaid Medi-Cal Revision Log See Important Reminder at the end of this policy
Clinical Policy: (Stivarga) Reference Number: CP.CPA.157 Effective Date: 11.16.17 Last Review Date: 11.17 Line of Business: Medicaid Medi-Cal Revision Log See Important Reminder at the end of this policy
Cost-effectiveness of Cetuximab and Panitumumab in First-line Treatment for Patients with KRAS Wild-Type Metastatic Colorectal Cancer in Ontario
 Cost-effectiveness of Cetuximab and Panitumumab in First-line Treatment for Patients with KRAS Wild-Type Metastatic Colorectal Cancer in Ontario Emmanuel Ewara, Dr. Greg Zaric, Dr. Stephen Welch, Dr. Sisira
Cost-effectiveness of Cetuximab and Panitumumab in First-line Treatment for Patients with KRAS Wild-Type Metastatic Colorectal Cancer in Ontario Emmanuel Ewara, Dr. Greg Zaric, Dr. Stephen Welch, Dr. Sisira
/m 2 Oxaliplatin 85 1 Q2W 1-3 Leucovorin Q2W 5-FU Q2W 5-FU Q2W
 癌症診療指引33 Adjuvant therapy of colon cancer mfolfox6 Oxaliplatin 85 1 Q2W 1-3 FOLFOX4 Oxaliplatin 85 1 Q2W 9 Leucovorin 200 1-2 Q2W 5-FU 400 1-2 Q2W 5-FU 600 1-2 Q2W FLOX Oxaliplatin 85 1,15,29 Q8W 4 Leucovorin
癌症診療指引33 Adjuvant therapy of colon cancer mfolfox6 Oxaliplatin 85 1 Q2W 1-3 FOLFOX4 Oxaliplatin 85 1 Q2W 9 Leucovorin 200 1-2 Q2W 5-FU 400 1-2 Q2W 5-FU 600 1-2 Q2W FLOX Oxaliplatin 85 1,15,29 Q8W 4 Leucovorin
EXAMPLE. ratio (%) Contraindication for treatment with panitumumab or cetuximab
 Contraindication for treatment with panitumumab or cetuximab") Dr Kate Goodhealth Goodhealth Medical Clinic 123 Address Road SUBURBTOWN NSW 2000 Referring Doctor Your ref Address Dr John Medico 123 Main Street, SUBURBTOWN NSW 2000 Phone 02 9999 9999 Requested 17 May
Dr Kate Goodhealth Goodhealth Medical Clinic 123 Address Road SUBURBTOWN NSW 2000 Referring Doctor Your ref Address Dr John Medico 123 Main Street, SUBURBTOWN NSW 2000 Phone 02 9999 9999 Requested 17 May
RECONSIDERING THE BENEFIT OF INTERMITTENT VERSUS CONTINUOUS TREATMENT IN THE MAINTENANCE TREATMENT SETTING OF METASTATIC COLORECTAL CANCER
 RECONSIDERING THE BENEFIT OF INTERMITTENT VERSUS CONTINUOUS TREATMENT IN THE MAINTENANCE TREATMENT SETTING OF METASTATIC COLORECTAL CANCER SUNAKAWA, Y, 1 BEKAIISAAB, T, 2 AND STINTZING, S. 3 SELECTED HIGHLIGHTS
RECONSIDERING THE BENEFIT OF INTERMITTENT VERSUS CONTINUOUS TREATMENT IN THE MAINTENANCE TREATMENT SETTING OF METASTATIC COLORECTAL CANCER SUNAKAWA, Y, 1 BEKAIISAAB, T, 2 AND STINTZING, S. 3 SELECTED HIGHLIGHTS
Panitumumab 6mg/kg Therapy
 Panitumumab 6mg/kg Therapy INDICATIONS FOR USE: INDICATION Treatment of adult patients with wild-type RAS metastatic colorectal cancer (mcrc) ICD10 Protocol Code In first line in combination with FOLFOX
Panitumumab 6mg/kg Therapy INDICATIONS FOR USE: INDICATION Treatment of adult patients with wild-type RAS metastatic colorectal cancer (mcrc) ICD10 Protocol Code In first line in combination with FOLFOX
Pharmacy Management Drug Policy
 11/13, 10/12, 11/11, 1, 6/10, Page 1 of 5 DESCRIPTION: Cetuximab is a recombinant humanized monoclonal antibody that binds specifically to the extracellular domain of the human epidermal growth factor
11/13, 10/12, 11/11, 1, 6/10, Page 1 of 5 DESCRIPTION: Cetuximab is a recombinant humanized monoclonal antibody that binds specifically to the extracellular domain of the human epidermal growth factor
J Cancer Res Clin Oncol (2014) 140: DOI /s
 140: DOI /s") J Cancer Res Clin Oncol (2014) 140:1607 1614 DOI 10.1007/s00432-014-1678-3 Original Article Clinical Oncology Left sided primary tumors are associated with favorable prognosis in patients with KRAS codon
J Cancer Res Clin Oncol (2014) 140:1607 1614 DOI 10.1007/s00432-014-1678-3 Original Article Clinical Oncology Left sided primary tumors are associated with favorable prognosis in patients with KRAS codon
Therapeutic Options for Patients with BRAF-mutant Metastatic Colorectal Cancer
 Therapeutic Options for Patients with BRAF-mutant Metastatic Colorectal Cancer Axel Grothey, M.D., Professor of Oncology, Clinical and Translational Science Division of Medical Oncology Mayo Clinic, Rochester,
Therapeutic Options for Patients with BRAF-mutant Metastatic Colorectal Cancer Axel Grothey, M.D., Professor of Oncology, Clinical and Translational Science Division of Medical Oncology Mayo Clinic, Rochester,
Metastatic colorectal cancer: treatment with panitumumab
 GUIDELINES IN FOCUS Metastatic colorectal cancer: treatment with panitumumab Author: Brazilian Medical Association Participants: Antonio Silvinato; Isabela da Silveira Pedreira; João Conrado Bueno dos
GUIDELINES IN FOCUS Metastatic colorectal cancer: treatment with panitumumab Author: Brazilian Medical Association Participants: Antonio Silvinato; Isabela da Silveira Pedreira; João Conrado Bueno dos
Opinion 17 October 2012
 The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 17 October 2012 VECTIBIX 20 mg/ml, concentrate for solution for infusion B/1 vial of 5 ml (CIP code: 3400957181857)
The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 17 October 2012 VECTIBIX 20 mg/ml, concentrate for solution for infusion B/1 vial of 5 ml (CIP code: 3400957181857)
Integrating anti-egfr therapies in metastatic colorectal cancer
 Review Article Integrating anti-egfr therapies in metastatic colorectal cancer Sigurdis Haraldsdottir, Tanios Bekaii-Saab The Ohio State University Comprehensive Cancer Center, Columbus, Ohio, USA Corresponding
Review Article Integrating anti-egfr therapies in metastatic colorectal cancer Sigurdis Haraldsdottir, Tanios Bekaii-Saab The Ohio State University Comprehensive Cancer Center, Columbus, Ohio, USA Corresponding
AIOM GIOVANI Perugia, Luglio 2017
 AIOM GIOVANI 2017 Perugia, 07-08 Luglio 2017 Scelta delle linee successive nel paziente RAS e BRAF wild-type con particolare accento su nuovi bersagli terapeutici Francesca Battaglin U.O.C. Oncologia Medica
AIOM GIOVANI 2017 Perugia, 07-08 Luglio 2017 Scelta delle linee successive nel paziente RAS e BRAF wild-type con particolare accento su nuovi bersagli terapeutici Francesca Battaglin U.O.C. Oncologia Medica
ASCO 2017 updates in Colorectal and Gastric Cancers. May Cho, M.D.
 ASCO 2017 updates in Colorectal and Gastric Cancers May Cho, M.D. Relevant financial relationships in the past twelve months by presenter or spouse/partner: None The speaker will directly disclosure the
ASCO 2017 updates in Colorectal and Gastric Cancers May Cho, M.D. Relevant financial relationships in the past twelve months by presenter or spouse/partner: None The speaker will directly disclosure the
BRAF Testing In The Elderly: Same As in Younger Patients?
 EGFR, K-RAS, K BRAF Testing In The Elderly: Same As in Younger Patients? Nadine Jackson McCleary MD MPH Gastrointestinal Oncology Dana-Farber/Harvard Cancer Care Boston, MA, USA Outline Colorectal cancer
EGFR, K-RAS, K BRAF Testing In The Elderly: Same As in Younger Patients? Nadine Jackson McCleary MD MPH Gastrointestinal Oncology Dana-Farber/Harvard Cancer Care Boston, MA, USA Outline Colorectal cancer
療指引 34 Adjuvant Therapy of Colon Cancer
 療指引 34 Adjuvant Therapy of Colon Cancer mfolfox6 Oxaliplatin 85 1 Q2W 1~3, 10 FLOX Oxaliplatin 85 1,15,29 Q8W 4 Leucovorin 500 1,8,15,22,29,35 Q8W 5-FU 500 1,8,15,22,29,35 Q8W Capecitabine Capecitabine
療指引 34 Adjuvant Therapy of Colon Cancer mfolfox6 Oxaliplatin 85 1 Q2W 1~3, 10 FLOX Oxaliplatin 85 1,15,29 Q8W 4 Leucovorin 500 1,8,15,22,29,35 Q8W 5-FU 500 1,8,15,22,29,35 Q8W Capecitabine Capecitabine
Personalised Medicine
 Personalised Medicine Panacea or Pandora s box? Dr Tom Lillie Oncology Therapeutic Area Head Amgen October 2012 Amgen is the world s leading biotechnology company employs more than 17,000 staff in 39 countries
Personalised Medicine Panacea or Pandora s box? Dr Tom Lillie Oncology Therapeutic Area Head Amgen October 2012 Amgen is the world s leading biotechnology company employs more than 17,000 staff in 39 countries
Dr. Iain Tan. Senior Consultant GI Medical Oncologist National Cancer Centre Singapore
 ESMO-ASIA 2017 Preceptorship (GI cancers) Session: Metastatic colorectal cancer, liver limited metastases Topic: Unresectable or borderline resectable : chemotherapy +/- targeted agents Dr. Iain Tan Senior
ESMO-ASIA 2017 Preceptorship (GI cancers) Session: Metastatic colorectal cancer, liver limited metastases Topic: Unresectable or borderline resectable : chemotherapy +/- targeted agents Dr. Iain Tan Senior
The Use of Epidermal Growth Factor Receptor Inhibitors in Advanced Colorectal Cancer
 CED-CCO Special Advice Report 8 EDUCATION AND INFORMATION 2012 The Use of Epidermal Growth Factor Receptor Inhibitors in Advanced Colorectal Cancer D. Jonker, J. Biagi, and A.E. Haynes Report Date: July
CED-CCO Special Advice Report 8 EDUCATION AND INFORMATION 2012 The Use of Epidermal Growth Factor Receptor Inhibitors in Advanced Colorectal Cancer D. Jonker, J. Biagi, and A.E. Haynes Report Date: July
Signifıcant progress has been made in the last decade in the
 BIOLOGIC THERAPIES IN COLORECTAL CANCER Biologic Therapies in Colorectal Cancer: Indications and Contraindications Marwan Fakih, MD OVERVIEW The role of antiangiogenic and anti-epidermal growth factor
BIOLOGIC THERAPIES IN COLORECTAL CANCER Biologic Therapies in Colorectal Cancer: Indications and Contraindications Marwan Fakih, MD OVERVIEW The role of antiangiogenic and anti-epidermal growth factor
The ESMO consensus conference on metastatic colorectal cancer
 ESMO Preceptorship Programme Colorectal cancer Prague July, 6-7 2016 The ESMO consensus conference on metastatic colorectal cancer Andres Cervantes ESMO consensus on mcrc 2016 Chairs: Co-Chairs of working
ESMO Preceptorship Programme Colorectal cancer Prague July, 6-7 2016 The ESMO consensus conference on metastatic colorectal cancer Andres Cervantes ESMO consensus on mcrc 2016 Chairs: Co-Chairs of working
Oncologist. The. Gastrointestinal Cancer
 The Oncologist Gastrointestinal Cancer The Clinical Benefit of Bevacizumab in Metastatic Colorectal Cancer Is Independent of K-ras Mutation Status: Analysis of a Phase III Study of Bevacizumab with Chemotherapy
The Oncologist Gastrointestinal Cancer The Clinical Benefit of Bevacizumab in Metastatic Colorectal Cancer Is Independent of K-ras Mutation Status: Analysis of a Phase III Study of Bevacizumab with Chemotherapy
RESEARCH ARTICLE. Value of KRAS, BRAF, and PIK3CA Mutations and Survival Benefit from Systemic Chemotherapy in Colorectal Peritoneal Carcinomatosis
 RESEARCH ARTICLE Value of KRAS, BRAF, and PIK3CA Mutations and Survival Benefit from Systemic Chemotherapy in Colorectal Peritoneal Carcinomatosis Yusuke Sasaki 1,2, Tetsuya Hamaguchi 1 *, Yasuhide Yamada
RESEARCH ARTICLE Value of KRAS, BRAF, and PIK3CA Mutations and Survival Benefit from Systemic Chemotherapy in Colorectal Peritoneal Carcinomatosis Yusuke Sasaki 1,2, Tetsuya Hamaguchi 1 *, Yasuhide Yamada
Review Article Advances of Targeted Therapy in Treatment of Unresectable Metastatic Colorectal Cancer
 BioMed Research International Volume 2016, Article ID 7590245, 14 pages http://dx.doi.org/10.1155/2016/7590245 Review Article Advances of Targeted Therapy in Treatment of Unresectable Metastatic Colorectal
BioMed Research International Volume 2016, Article ID 7590245, 14 pages http://dx.doi.org/10.1155/2016/7590245 Review Article Advances of Targeted Therapy in Treatment of Unresectable Metastatic Colorectal
Clinical Policy: Panitumumab (Vectibix) Reference Number: CP.PHAR.321
 Reference Number: CP.PHAR.321") Clinical Policy: (Vectibix) Reference Number: CP.PHAR.321 Effective Date: 03/17 Last Review Date: 03/17 Coding Implications Revision Log See Important Reminder at the end of this policy for important regulatory
Clinical Policy: (Vectibix) Reference Number: CP.PHAR.321 Effective Date: 03/17 Last Review Date: 03/17 Coding Implications Revision Log See Important Reminder at the end of this policy for important regulatory
Clinical Trials in the Era of Personalised Medicine and Biomarkers. Chris Karapetis New Zealand Society of Oncology Conference 2 nd July 2012
 Clinical Trials in the Era of Personalised Medicine and Biomarkers Chris Karapetis New Zealand Society of Oncology Conference 2 nd July 2012 The EGFR Signaling Network is Vast and Complicated EGFR activation
Clinical Trials in the Era of Personalised Medicine and Biomarkers Chris Karapetis New Zealand Society of Oncology Conference 2 nd July 2012 The EGFR Signaling Network is Vast and Complicated EGFR activation
Bevacizumab is currently licensed for the following indication relevant for this NICE review:
 Roche Executive Summary Context Bevacizumab (Avastin) is a humanized (93% human) murine monoclonal antibody which binds to and neutralizes VEGF, a powerful pro-angiogenic glycoprotein produced by both
Roche Executive Summary Context Bevacizumab (Avastin) is a humanized (93% human) murine monoclonal antibody which binds to and neutralizes VEGF, a powerful pro-angiogenic glycoprotein produced by both
Perioperative chemotherapy for colorectal cancer livermetastases: what is the optimal strategy?
 Perioperative chemotherapy for colorectal cancer livermetastases: what is the optimal strategy? Prof Eric Van Cutsem, MD, PhD Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be A classical case
Perioperative chemotherapy for colorectal cancer livermetastases: what is the optimal strategy? Prof Eric Van Cutsem, MD, PhD Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be A classical case
Ashita Waterston Beatson West of Scotland Cancer Centre
 Ashita Waterston Beatson West of Scotland Cancer Centre Aim of treatment Scheduling and choice of treatments are dictated by aim: Down staging for resectability: upfront intensive Prolong survival: combination
Ashita Waterston Beatson West of Scotland Cancer Centre Aim of treatment Scheduling and choice of treatments are dictated by aim: Down staging for resectability: upfront intensive Prolong survival: combination
Worst outcomes according to RAS mutation variants: an analysis in patients with metastatic colorectal adenocarcinoma
 JBUON 2018; 23(4): 925-935 ISSN: 1107-0625, online ISSN: 2241-6293 www.jbuon.com E-mail: editorial_office@jbuon.com ORIGINAL ARTICLE Worst outcomes according to RAS mutation variants: an analysis in patients
JBUON 2018; 23(4): 925-935 ISSN: 1107-0625, online ISSN: 2241-6293 www.jbuon.com E-mail: editorial_office@jbuon.com ORIGINAL ARTICLE Worst outcomes according to RAS mutation variants: an analysis in patients
clinical practice guidelines
 Annals of Oncology 21 (Supplement 5): v93 v97, 2010 doi:10.1093/annonc/mdq222 Advanced colorectal cancer: ESMO Clinical Practice Guidelines for treatment E. Van Cutsem 1, B. Nordlinger 2 & A. Cervantes
Annals of Oncology 21 (Supplement 5): v93 v97, 2010 doi:10.1093/annonc/mdq222 Advanced colorectal cancer: ESMO Clinical Practice Guidelines for treatment E. Van Cutsem 1, B. Nordlinger 2 & A. Cervantes
Published Ahead of Print on April 18, 2011 as /JCO J Clin Oncol by American Society of Clinical Oncology INTRODUCTION
 Published Ahead of Print on April 18, 211 as 1.12/JCO.21.33.591 The latest version is at http://jco.ascopubs.org/cgi/doi/1.12/jco.21.33.591 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T From
Published Ahead of Print on April 18, 211 as 1.12/JCO.21.33.591 The latest version is at http://jco.ascopubs.org/cgi/doi/1.12/jco.21.33.591 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T From
Toxicity by Age Group. Old Factor 1: Age. Disclosures. Predicting survival in metastatic colorectal cancer. Personalized Medicine - Decision Tools -
 Disclosures Predicting survival in metastatic colorectal cancer Daniel Sargent, PhD Mayo Clinic Consulting activities Amgen Pfizer Roche/Genentech Sanofi-Aventis Genomic Health Personalized Medicine -
Disclosures Predicting survival in metastatic colorectal cancer Daniel Sargent, PhD Mayo Clinic Consulting activities Amgen Pfizer Roche/Genentech Sanofi-Aventis Genomic Health Personalized Medicine -
Novel Molecularly Targeted Therapies and Biomarkers in Advanced Colorectal Cancer. Objectives
 Novel Molecularly Targeted Therapies and Biomarkers in Advanced Colorectal Cancer Michael S. Lee, MD Assistant Professor of Medicine University of North Carolina Objectives Discuss important clinicopathologic
Novel Molecularly Targeted Therapies and Biomarkers in Advanced Colorectal Cancer Michael S. Lee, MD Assistant Professor of Medicine University of North Carolina Objectives Discuss important clinicopathologic